The Digestive System or tract extends from the · PDF fileThe Digestive System or tract...
44
-
Upload
phungduong -
Category
Documents
-
view
221 -
download
6
Transcript of The Digestive System or tract extends from the · PDF fileThe Digestive System or tract...


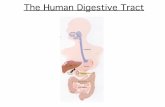
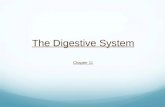
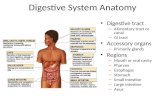
The Digestive System or tract extends from themouth to the anus.
FUNCTION The Digestive System breaks down and
absorbs food materials e.g. amino acids, glucose

DEFINITIONS:
Ingestion: Ingestion is the taking in of food, liquids or
drugs by mouth.
Digestion: Digestion is the mechanical and chemical
breakdown of food to simple molecules that can be absorbed by the body.

Absorption:
The movement of molecules across gastrointestinal epithelial membranes into the body fluids.
90 % of the absorption of all nutrients takes place in the small intestine. The other 10 % take place in the stomach and large intestine.

Absorption takes place through the villi and depends on diffusion, facilitated diffusion, osmosis and active transport.

BASIC TISSUE LAYERS
From the inside out:
Mucous membrane - epithelial layer
Submucosa - connective tissue
Smooth muscle
Serous membrane - peritoneum

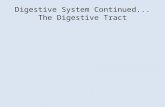
THE PROCESS OF DIGESTION:
Food enters the mouth and mastication occurs (chewing the food)
The food becomes a bolus and deglutition occurs (swallowing)

The bolus enters the stomach aided by peristaltic action and gravity. The bolus is churned by the process of peristalsis and mixed with gastric juice to become chyme and digestion continues aided by HCl & enzymes found in the gastric juice
Peristalsis moves the chyme to the small intestine where absorption of vitamins, minerals & nutrients occurs through the
villi.

DEFAECATORY SYSTEM
Function: Elimination of faeces from the rectum
through the anus Faeces is composed of undigested food
stuffs, inorganic materials and bacteria. Faecal matter is about 75% fluid and 25%
solid material. The brown colour of faeces is due to the
breakdown of bile by the intestinal bacteria.

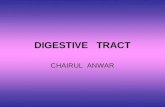
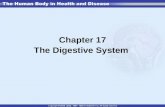
Large intestine
STRUCTURE Caecum, ascending
colon, transverse colon, descending colon and sigmoid colon
Rectum Anal canal, anus
FUNCTION Re absorption of
water, secretion of mucous, vitamin production (bacteria)
Storage Elimination


Physiology of Defaecation: Distension of the rectum initiates
contractions. This process is aided after meals when the large intestine increases in motility.
Rectal pressure rises the internal sphincter of the anal canal relaxes and this gives rise to the desire to defecate
During defecation the longitudinal rectal muscles contract to increase pressure and the external sphincter muscle begins to relax

Excretion is aided by contractions of abdominal and pelvic skeletal muscles, which raise intra-abdominal pressure and help push the faeces from the rectum through the anal canal and out the anus
Defecation is a reflex action that can be voluntarily inhibited by keeping the external sphincter contracted.

NORMAL CHANGES ASSOCIATED WITH AGEING:
Sensation of taste and smell diminish (associated with neurological function).
Loss of teeth Decreased saliva production (not associated with all older people and usually associated with disease process or drug therapy)
Weakened gag reflex.

Decreased appetite Muscle wall of digestive tract loses tone.
Secretion of digestive enzymes decreases.
Liver shrinks and receives less blood supply.
Peristalsis of the oesophagus decreases (may be due to high prevalence of neurological disease).
Decreased absorption rate. Decreased large bowel motility

Dysphagia:
In older people in long term care about one third have some dysphagia. This is due to vascular, structural or neurological causes.
Vascular:
May be due to dilatation or aneurysm of the aorta.
Presenter
Presentation Notes
Myasthenia gravis is a chronic autoimmune neuromuscular disease characterized by varying degrees of weakness of the skeletal (voluntary) muscles of the body. What are the symptoms of myasthenia gravis?�� Although myasthenia gravis may affect any voluntary muscle, muscles that control eye and eyelid movement, facial expression, and swallowing are most frequently affected. The onset of the disorder may be sudden. Symptoms often are not immediately recognized as myasthenia gravis. In most cases, the first noticeable symptom is weakness of the eye muscles. In others, difficulty in swallowing and slurred speech may be the first signs. The degree of muscle weakness involved in myasthenia gravis varies greatly among patients, ranging from a localized form, limited to eye muscles (ocular myasthenia), to a severe or generalized form in which many muscles - sometimes including those that control breathing - are affected. Symptoms, which vary in type and severity, may include a drooping of one or both eyelids (ptosis), blurred or double vision (diplopia) due to weakness of the muscles that control eye movements, unstable or waddling gait, weakness in arms, hands, fingers, legs, and neck, a change in facial expression, difficulty in swallowing and shortness of breath, and impaired speech (dysarthria).

Structural: Structural problems are usually associated with
neurogenic disorders and may affect any part of the oesophagus. The oesophagus may be dilated or restricted.
Neurological: Can result from stroke, Parkinson's Disease,
myasthenia gravis.





Management:
Evaluation by a speech pathologist is necessary and treatment may involve correction of the underlying disorder, swallowing therapy, dilatation or surgery.
Impaired oesophageal motility may be treated with drugs.
Prolonged enteral feeding is sometimes necessary

Hiatus Hernia
This occurs when the stomach moves up through the diaphragm at the hiatus.
A hiatus hernia can cause regurgitation, flatulence and acid vomiting.

Treatment is usually conservative involving weight loss, elevation of the head of the bed, eating small, frequent meals, antacids and avoiding eating before going to bed. Although dilatation and corrective surgery can be used

Gastritis Usually results from a decrease in
hydrochloric acid secretion, which leads to a decreased absorption of iron and vitamin B12. This results in bacterial over growth resulting in mild to severe epigastric pain, dyspepsia, distension, nausea and vomiting
Management: Frequent meals of a diet that is bland
and spice free but containing vitamins and iron

Gastric Ulcers This cause may be related to chronic use of
drugs such as steroids and aspirin. This occurs even with decreased hydrochloric acid production and is thought to be related to decreasing gastric mucosal blood flow
Management: As gastric ulcers may lead to cancer, they
should be biopsied. Surgery may be preformed if complications such as bleeding or obstruction occur. However, treatment is usually conservative with bed rest and drug therapy

Constipation Constipation results from decreased
frequency of bowel movements, hard difficult defecation and a feeling of incomplete evacuation. It is associated with decreased motility, malignancy, obstruction, poor nutrition, decreased fluid intake, hypothyroidism, hypercalcaemia, depression, or medications
A major complication of constipation is faecal impaction and mega colon
Management: Increased physical activity, a high fibre diet,
increased fluids, laxatives and enemas

Retention with overflow
Impaction


Soap and water (evacuation by lubrication) Disposable- Microlax (5 mL)- Travenol (RN only)
Retention enemas- olive oil (RN only)- fluid (for rehydration)- medicated (RN only)

Diarrhoea Diarrhoea results from increased fluidity,
or frequency of bowel movements. The most common cause in older people
is faecal impactions, bacterial or viral infections, diet, and medications.
Diarrhoea can also result from diseases such as diverticulitis, thyrotoxicosis, diabetes, gastric and liver disease

Management
A complete assessment should be made, stool cultures, fluid balance chart and adequate hydration (under medical supervision) undertaken. Treatment will depend on the cause

TECHNIQUES FOR FEEDING ACLIENT
Some residents may require feeding due to weakness, paralysis, casts, confusion and so on. It is important to do so in a relaxed manner so that the resident does not feel rushed.

Steps:
Consult the nursing care plan so that you are aware of feeding requirements.
Ask the resident about the order in which foods and fluids are offered.
Spoons are usually used, as there is less risk of injury. The spoon should be about 1/3 full as this portion is easy chewed and swallowed.
Encourage the residents to feed themselves if possible. This fosters independence and helps decrease feelings of helplessness. Use finger foods if possible.

Visually impaired residents require you to describe what you are feeding them. If they are able to feed themselves, describe the foods and fluids and their place on the plate/tray using the numbers of the clock.

Meals should be a time of social interaction, encourage conversation and interaction.
Sit so that you face the resident. This allows you to converse, observe any difficulties swallowing and conveys that you have time to relax

The aims of bowel management are todevelop regular bowel habits and to prevent uninhibited bowel elimination. A bowel training program can achieve regular emptying of the lower bowel.

Bowel training programs: Take advantage of the client’s natural
reflexes. regularity, timing, nutrition, fluids, exercise and correct positioning promote predictable defecation.
Steps include: recording defecation time, character of the
stool, nutritional intake, cognitive abilities and functional self care toileting abilities for 5 to 7 days

analysis of this record to establish a program for the client
Establishment of a regular time for defecation consistency is essential.
30 minutes after a meal natural defecation reflexes occur
Therefore after a meal is one of the best times to plan bowel evacuation (or if there is a previously established habit pattern at a different time of the day, then this should be followed).

Rectal suppository or mechanical stimulation e.g. digital stimulation with a gloved finger may stimulate the anorectal reflex.
Suppository should be inserted 30 mins before the scheduled bowel elimination time.

Time between insertion of the suppository and defecation time should be noted for future modification of the bowel program. Once the bowel routine is well established, stimulation with a suppository may not be necessary

The resident should assume the normal squatting position
To promote regular elimination, the diet should be high in fibre with adequate fluid. Natural stimulants such as prunes, fruits, vegetables and whole grains are preferred laxatives.

ASSISTING A CLIENT MAINTAINFAECAL CONTINENCEDevices used to manage bowel incontinence:
Pads, liners, disposable briefs, protective underwear (washable incontinence pants, ancillary products e.g. odour eliminator spray s (ConvaTec Pro System Incontinence Care Training Manual.)
Also help may be sought from: Continence Foundation of Australia

Implications for Nursing Assistants:
It is important to report any changes to a resident's eating patterns or patterns of elimination.
Constipation can cause confusion in the elderly client.
Diarrhoea if severe has been known to cause death in the frail elderly