The Diagnosis and Management of Benign Hepatic Tumors › wp-content › uploads › 2013 › 07 ›...
12
LIVER, PANCREAS, AND BILIARY TRACT: CLINICAL REVIEW The Diagnosis and Management of Benign Hepatic Tumors Bo Yoon Choi, MD and Mindie H Nguyen, MD, MAS Abstract: Benign hepatic tumors include a broad spectrum of re- generative and true neoplastic processes. Because of advances in imaging studies such as computed tomography (CT) and magnetic resonance imaging (MRI) as well as progress in immunohistochem- istry, accurate diagnosis can now be made in a large percentage of patients without surgical laparotomy or resection. This article will focus on the pathogenesis, diagnosis, and management of focal benign lesions ofthe liver. Many ofthese tumors present with typical features in various imaging studies. On occasions, biopsies are re- quired and/or surgical removal is needed. The most common benign hepatic tumors include cavemous hemangioma, focal nodular hy- perplasia, hepatic adenoma, and nodular regenerative hyperplasia. In the majority of cases of benign hepatic tumors, patients are asymp- tomatic, and no treatment is indicated. The main indication for treatment is the presence of significant cIinical symptoms or sus- picion of malignancy or fear of malignant transformation. Key Words: liver, benign tumor, diagnosis, review (J Clin GastroenteroI2005;39:401-412) B enign hepatic tumors are increasingly reported with the widespread use of sensitive imaging studies and occa- sionally present significant diagnostic and therapeutic chal- lenges. They usually occur in asymptomatic patients with or without underlying liver disease. Using simple imaging tech- niques such as ultrasound (US), benign hepatic tumors can be categorized as solitary or multiple and as solid or cystic as shown in Table 1.1-3 In general, a single imaging study is insufficient for a definitive diagnosis, and further studies may be necessary. Most benign hepatic tumors follow a fairly indolent clinical course. However, some ofthem are associated with serious complications. Thus, the understanding of clinical, radiologic, and pathologic characteristics of each tumor is important for accurate diagnosis and appropriate treatrnent of these tumors. This article will review several benign hepatic tumors that are commonly encountered in adults. We will categorize them as solid or cystic tumors and describe key differential diagnostic criteria for each tumor. We will also propose a stepwise approach for diagnosis and From the Oivision of Gastroenterology and Hepatology, Oepartment of Medicine, Stanford University Medical Center, Stanford, CA. Reprints: Mindie H. Nguyen, MO, MAS, Oivision of Gastroenterology and Hepatology, Stanford University Medical Center, 750 Welch Road, Suite 210, PaIo Alto, CA 94304-1509 (e-mail: [email protected]). Copyright @ 2005 by Lippincott Williams & Wilkins I C/in Gastroentero/. Volume 39, Number 5, MaY/June 2005 treatrnent of asymptomatic patients with benign hepatic tumors (Fig. I). SOLlD HEPATIC TUMORS Hemangioma Pathogenesis and Pathology Hemangioma is the most common benign hepatic tumor. The pathogenesis is not well understood. Some ofthese tumors have estrogen receptors, and accelerated growth has been observed with high estrogen states such as those associated with puberty, pregnancy, oral contraceptive use, and with androgen treatrnent. These findings suggest that hormonal effect may be one ofthe pathogenic mechanisms.4-<>Growth of hemangioma is thought to be due to ectasia rather than hy- pertrophy or hyperplasia.7 According to autopsy series, the prevalence ofhemangioma ranges from 3% to 20%, and most of them are seen in middle-aged women. The female-to-male ratio is 5 to 6:I.5,S Hemangiomas are usually located in the subcapsular region of the right lobe, with size ranging from less than I cm to more than 20 cm. Grossly, it is a well-circumscribed and compressible tumor with dark color.7 Microscopically, it arises from the endothelial cells that line the blood vessels and consists of multiple, large vascular channels lined by a single layer of endothelial cells and supported by collagenous walls.s,9 Their blood supply arises from the hepatic artery.1 Clinical Presentation The most common clinical presentation of hemangio- mas is an incidental finding during ultrasonographic exam- ination of the abdomen for unrelated reasons.5 Hemangiomas are usually less than 5 cm. Only a few patients with large tu- mors (>5 cm) may present with nonspecific abdominal symp- toms. Intermittent symptoms can also occur when there is necrosis, infarction, or thrombosis of the tumor.7 Although hemangiomas can occur at any age, most of them grow very slowly and are rarely diagnosed during childhood. Major complications such as spontaneous hemorrhage are distinc- tively rare in even large hemangiomas.5 Kasaback-Merritt syndrome is arare clinical entity with thrombocytopenia and disseminated intravascular coagulopathy associated with giant hemangioma. These patients can present with upper abdom- inal pain and bleeding due to progressive consumptive coagulopathy, which is often triggered by a surgical or dental procedure.1O 401 70
Transcript of The Diagnosis and Management of Benign Hepatic Tumors › wp-content › uploads › 2013 › 07 ›...

LIVER, PANCREAS, AND BILIARY TRACT: CLINICAL REVIEW
The Diagnosis and Management ofBenign Hepatic Tumors
Bo Yoon Choi, MD and Mindie H Nguyen, MD, MAS
Abstract: Benign hepatic tumors include a broad spectrum of re-generative and true neoplastic processes. Because of advances inimaging studies such as computed tomography (CT) and magneticresonance imaging (MRI) as well as progress in immunohistochem-istry, accurate diagnosis can now be made in a large percentage ofpatients without surgical laparotomy or resection. This article willfocus on the pathogenesis, diagnosis, and management of focalbenign lesions ofthe liver. Many ofthese tumors present with typicalfeatures in various imaging studies. On occasions, biopsies are re-quired and/or surgical removal is needed. The most common benignhepatic tumors include cavemous hemangioma, focal nodular hy-perplasia, hepatic adenoma, and nodular regenerative hyperplasia. Inthe majority of cases of benign hepatic tumors, patients are asymp-tomatic, and no treatment is indicated. The main indication for
treatment is the presence of significant cIinical symptoms or sus-picion of malignancy or fear of malignant transformation.
Key Words: liver, benign tumor, diagnosis, review
(J Clin GastroenteroI2005;39:401-412)
B enign hepatic tumors are increasingly reported with thewidespread use of sensitive imaging studies and occa-
sionally present significant diagnostic and therapeutic chal-lenges. They usually occur in asymptomatic patients with orwithout underlying liver disease. Using simple imaging tech-niques such as ultrasound (US), benign hepatic tumors can becategorized as solitary or multiple and as solid or cystic asshown in Table 1.1-3 In general, a single imaging study isinsufficient for a definitive diagnosis, and further studies maybe necessary. Most benign hepatic tumors follow a fairlyindolent clinical course. However, some ofthem are associatedwith serious complications. Thus, the understanding ofclinical, radiologic, and pathologic characteristics of eachtumor is important for accurate diagnosis and appropriatetreatrnent of these tumors. This article will review severalbenign hepatic tumors that are commonly encountered inadults. We will categorize them as solid or cystic tumors anddescribe key differential diagnostic criteria for each tumor. Wewill also propose a stepwise approach for diagnosis and
From the Oivision of Gastroenterology and Hepatology, Oepartment ofMedicine, Stanford University Medical Center, Stanford, CA.
Reprints: Mindie H. Nguyen, MO, MAS, Oivision of Gastroenterology andHepatology, Stanford University Medical Center, 750 Welch Road, Suite210, PaIo Alto, CA 94304-1509 (e-mail: [email protected]).
Copyright @ 2005 by Lippincott Williams & Wilkins
I C/in Gastroentero/. Volume 39, Number 5, MaY/June 2005
treatrnent of asymptomatic patients with benign hepatictumors (Fig. I).
SOLlD HEPATIC TUMORS
HemangiomaPathogenesis and Pathology
Hemangioma is the most common benign hepatic tumor.The pathogenesis is not well understood. Some ofthese tumorshave estrogen receptors, and accelerated growth has beenobserved with high estrogen states such as those associatedwith puberty, pregnancy, oral contraceptive use, and withandrogen treatrnent. These findings suggest that hormonaleffect may be one ofthe pathogenic mechanisms.4-<>Growth ofhemangioma is thought to be due to ectasia rather than hy-pertrophy or hyperplasia.7 According to autopsy series, theprevalence ofhemangioma ranges from 3% to 20%, and mostof them are seen in middle-aged women. The female-to-maleratio is 5 to 6: I.5,S
Hemangiomas are usually located in the subcapsularregion of the right lobe, with size ranging from less than I cmto more than 20 cm. Grossly, it is a well-circumscribed andcompressible tumor with dark color.7 Microscopically, it arisesfrom the endothelial cells that line the blood vessels andconsists of multiple, large vascular channels lined by a singlelayer of endothelial cells and supported by collagenouswalls.s,9 Their blood supply arises from the hepatic artery.1
Clinical PresentationThe most common clinical presentation of hemangio-
mas is an incidental finding during ultrasonographic exam-ination of the abdomen for unrelated reasons.5 Hemangiomasare usually less than 5 cm. Only a few patients with large tu-mors (>5 cm) may present with nonspecific abdominal symp-toms. Intermittent symptoms can also occur when there isnecrosis, infarction, or thrombosis of the tumor.7 Althoughhemangiomas can occur at any age, most of them grow veryslowly and are rarely diagnosed during childhood. Majorcomplications such as spontaneous hemorrhage are distinc-tively rare in even large hemangiomas.5 Kasaback-Merrittsyndrome is arare clinical entity with thrombocytopenia anddisseminated intravascular coagulopathy associated with gianthemangioma. These patients can present with upper abdom-inal pain and bleeding due to progressive consumptivecoagulopathy, which is often triggered by a surgical or dentalprocedure.1O
401
70

Choi and Nguyen J Clin Gastroentero/. Volume 39, Number 5, MaY/June 2005
TABLE 1. DifferentialDiagnosisof BenignHepaticTumorsSolitary MuItiple or DilTuse
Hemangioma HemangiomaFocal nodular Focal nodular
hyperplasia hyperplasiaHepatic adenoma Hepatic adenomaMacroregenerative Macroregenerative
nodule nodule
Focal fatty change Focal fatty changeIntrahepatic bile duct Nodular regenerative
adenoma hyperplasiaMesenchymal
hamartoma
Lipomatous tumorInflammatory
pseudotumorSimple hepatic cyst
Solid
Cystic Polycystic liverdisease
Echinococcal cyst
Von Meyenburgcomplexes
Peliosis hepatis
Echinococcal cyst
Choledochal cyst
Biliary cystadenomaCaroli disease
ImagingThe majority of hemangiomas can be diagnosed accu-
rately by imaging studies alone since hemangiomas usuallyhave characteristic imaging features. They may be isolated ormultiple as in up to 50% of patients.9 On US, hemangiomatypically appears as a well-defined, lobulated, homogeneoushyperechoic mass, but it may also have hypoechoic portiondue to hemorrhage, fibrosis, or calcification. The accuracyof US is reported to be 70% to 80%.28 Contrast-enhancedharmonic US imaging demonstrates peripheral nodular en-hancement in the portal phase and the absence of intratumoralvesse\s in the arterial phase, which is often present inhepatocellular carcinoma (HCC).11.12
Hemangiomas are ftequently missed on standard CT, buttheycan often be diagnosed by multiphasic CT.In early enhancedimages, they show peripheral nodular or globular enhancement.As time goes by, contrast enhancement progresses centripetally.In delayed enhanced images, they appear as uniformly enhancedtumors.13The best, although most expensive, imaging study forhemangiomas is MRI with sensitivity and specificity between85% and 95%. Bright signal intensity on T2-weighted imagesand similar enhancement pattem to enhanced CT are veryspecific and effective for accurate diagnosis (Fig. 2).14.15Singlephoton emission computed tomography (SPECT) with techne-tium-Iabeled red blood cell has similar sensitivity and specificityto MRI for hemangioma only if the tumor is larger than 3 cmand close to the surface.4.5Because ofthese limitations, SPECTshould be used as a supplementary test.
However, there are also atypical findings of hemangio-mas such as cystic hemangiomas or small hemangiomas withimmediate homogeneous enhancement.16.17 In these cases,pathologic conformation via needle biopsy is required, al-though it is still debatable whether needle biopsy can be safelyperformed in hypervascular tumors such as hemangioma. One
402
retrospective study of percutaneous biopsy of 38 patients withsuspected hemangiomas using 20-gauge needles reported thatit is safe and effective for establishing the diagnosis of hem-angiomas. In that study, hemangiomas range in size from 1 cmto 13.5 cm, with a mean of 3 cm.4
ManagementTreatment is not indicated for asymptomatic patients
with hemangiomas that are less than 5 cm after the diagnosis isestablished and stability can be demonstrated on at least onefollow-up study at 6-month interval.4 Asymptomatic patientswith giant hemangiomas may need to be monitored moreclosely. Indications for treatment include severe symptoms,complications, and inability to exclude malignancy.18 Treat-ment includes surgical enucleation, resection, transarterialcatheter chemoembolization, hepatic irradiation, and trans-plantation.5.19 Surgical resection and enucleation are applica-ble for single hemangioma. Transplantation may be necessaryin large umesectable lesions, multiple lesions, or thoseinvolving the hepatic hilum.
SummaryHemangiomas are the most common benign tumors
of the liver. They are often asymptomatic and are foundincidentally on imaging studies. Complicationsare uncom-monoDiagnosisis usuallymadeby characteristicradiographicfeatures,and MRI is themost sensitiveand specificdiagnosticmodality. Treatment depends on the patient's clinicalpresentation.
Focal Nodular HyperplasiaPathogenesis and Pathology
Focal nodular hyperplasia (FNH) is the second mostcommon benign solid tumor of the liver and makes upapproximately 8% of ali primary hepatic tumors.4.9ThepathogenesisofFNH is not wellunderstood.In the past, FNHwasthoughtto be eithera hamartomaor a neoplasmthat formsin response to ischemia. However,more recently, it is con-sidereda nonneoplastic,hyperplasticresponseto a congenitalvascular malformation.7Histologically,FNH is defined asa tumor consisting of benign-appearinghepatocytes occurr-ing in the liver that is normal or nearly normal.20FNH isencountered in as many as 3% of general population,predominantly in childbearing-agedwomen with a female-to-male ratio of 6 to 8:1.5 Oral contraceptive use may beassociated with FNH, but its association is not clear. Mostinvestigatorsagree that the use of oral contraceptivedoes notinducethe formationof FNH,but it acts onlyto acceleratethegrowthof already formedtumors.21FNH most often presentsas a solitary,less than 5-cm nodule near the hepatic surface,although large masses up to 15 cm in diameter have beenreported:4
On gross pathology,it is usually a well-circumscribed,globular, lobulated but not encapsulated tumor.21The char-acteristichistologic featuresof FNH include a dense, centralstellate scar and septa that radiate from the central scar. Thesepta divide the tumor into severalnodules. Microscopically,this scar is composed of bile ductules, cholangiolar
@ 2005 Lippincott Williams & Wilkins
71

J C/in Gastroenterol. Volume 39, Number 5, May/june 2005 Benign Hepatic Tumors
Characteristic increased uptake
I \No Yes
I tBiopsy __ Probablefocalnodular
hyperplasia
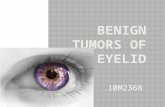
Liver mass in an asymptomatic patient
~
LFTs, Viral serology, AFP, CBC
/ \Normal or nonspecific LFT
~Ultrasound
Cystic
~Simple cystic structure
,/ \
Solid
~
Dynamic CT or MRI
~
Characteristic imaging ofhemangioma
,/ \Yes
~Observe
Yes
99mTc scintigraphy
~
I \Nondiagnostic Focal nodular hyperplasia
~ ~Resection Observe
FIGURE 1. Evaluationfor asymptomaticlivermasses.
proliferation with surrounding inflammatory infiltrates, andmalfonned vessels including arteries and capillaries but noportal veins.20 All of these proliferating bile ductules are ofhepatocellular origin, not the prefonned biliary tree.7 Thehepatic parenchyma between the septa is nonnally arrangedinto hepatic cords composed of hepatocytes, sinusoids, andKupffer cells.
Clinical PresentationA1though FNH may grow to more that 10 cm in
diameter,patientsare rarelysymptomatic.8Clinicalsymptoms
@ 2005 Lippincott Williams & Wilkins
Abnormal
Further evaluation for
probable HCC or metastasis
No
~Central scar on CT or MRI
I \No
tProbable hepatic adenoma
tHistologic exam with biopsy
IHepatic adenoma
~
Focal nodular hyperplasia
1
Observe
Consider resection Observe
(especially if> 5 cm)versus watchful observation
such as epigastric or right upper quadrant pain are found in lessthan one third of patients, and pain is usually not acute.22Spontaneous rupture leading to hemorrhage is extremely rare.Most patients have nonnal liver function test. Malignanttransfonnation of FNH has not been clearly described.Fibrolamellar variant of HCC is one of malignant hepatictumors that also has a central scar similar to that of FNH, butthere is no definite evidence that FNH is a precursor offibrolamellar HCC.23 Because of its benign clinical course,distinction between FNH and other hypervascular hepatictumors, such as hepatic adenoma, HCC, and hypervascular
403
72
Yes No
Observe Furtherevaluation

Choi and Nguyen J C/in Gastroenterol- Volume 39, Number 5, MaY/June 2005
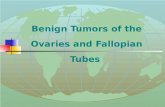
FIGURE2. Hemangioma.A, EarlyenhancedTl-weightedimage reveals peripheral nodülar enhancement of the tumor.B, Delayed enhanced Tl-weighted image shows homoge-neous enhancement of the tumor.
metastasis, is critical to ensure appropriate treatment andfollow-up.
ImagingAs in the case with histologic study, the central fibrous
scar is the most characteristic finding in imaging studies. US isoften the initial imaging modality that indicates a focal hepaticlesion, but FNH is not well demonstrated by simple sono-graphic technique. There is only a subtle difference ofechogenicity between FNH and the surrounding normal liver.FNH may be slightly hypoechoic, isoechoic, or slightlyhyperechoic. Some of them may show a hypoechoic halosurrounding the tumor,z° Color and power Doppler US may behelpful for detecting the vascularity in suspected FNH. Inaddition, use of US contrast media has been reported. Afterinjection of contrast media (Levovist; Schering AG, Berlin,Germany), FNH demonstrates strong homogeneous activitysimilar to adjacent hepatic parenchyma. The mechanism of itsuptake is thought to be related to Kupffer cell activity. This canbe a differential point ITomother malignant hepatic tumors thattypically demonstrate no uptake as focal defects.24 Despites
404
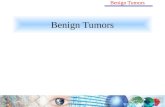
FIGURE3. FNH.A, UnenhancedTl-weighted image demon-strates a smoothly marginated isointense tumor with a hyper-intense portion. B, Fat saturation T2-weighted image revealsslightly hyperintense tumor with a central scar and its intenselybright signal. C, Enhanced Tl-weighted image shows a homo-geneous enhanced tumor with hypointense central scar.
these possibilities, US is currently not considered the modalityof choice for characterization of FNH.
On multiphasic CT and enhanced MRI, typical featuresofFNH are very characteristic (Fig. 3).1.22On multiphasic CT,
@ 2005 Lippincott Williams & Wilkins
73

J C/in Gastroenterol- Volume 39, Number 5, MaY/June 2005 Benign Hepatic Tumors
FNH is usually homogeneous and iso-attenuating to thenonnal liver before contrast injection. At late arterial phase,FNH typically presents with a bright homogeneous enhance-ment and a hypodense central scar. The radiating hypodensefibrous bands or septa, arising from the scar, are infrequent butquite characteristic. At portal phase, FNH retums to iso-attenuating to the nonnalliver and may be difficult to detect.Delayed phase often shows hyperattenuation ofthe central scarand septa due to the late opacification of the fibrotic com-ponents. Dilated feeding arteries penetrating central scar anddraining veins running at the surface of the tumor may berecognized in large FNH.13Because early hyperattenuation ofthe tumor is the most reliable sign, multidetector computedtomography (MDCT), which allows the rapid scanning of theentire liver at the late arterial phase, can facilitate thecharacterization of FNH. \3
On MRI, FNH is slightly hypointense on Tl-weightedimages and slight1yhyperintense on T2-weighted images. FNHmay also be nearly isointense on both Tl- and T2-weightedimages. Unlike hepatic adenoma, FNH rarely has higher signalintensity than the liver on Tl-weighted images.25 The centralscar is usually hyperintense on T2-weighted images. Ondynamic contrast-enhanced MR images, FNH shows similarenhancement pattem to multiphasic CT (Fig. 3). Superpara-magnetic iron oxide (SPIO) is an MR contrast agent thatundergoes phagocytosis by the RES system (Kupffer cell). OnSPIO-enhanced T2-weighted images, FNH is hypointense,whereas the central scar is more conspicuous.9.21 On MR imageswith hepatobiliary contrast agents, FNH appears hyperintense inrelation to the nonnal liver, and the central scar remainshypointense.8 In addition to these typical imaging features,atypical CT and MRI findings also OCCUf.These include multiplelesions, heterogeneity or fat component within the tumor, non-visualization of the central scar, and pseudo-capsular enhance-ment.26
On hepatic scintigraphy with 99m Tc-sulfur-colloid,FNH shows nonnal (30%), increased (30%), and decreased(30%) colloid uptake compared with the nonnalliver. In 10%of cases, uptake is intense, and this is a very specific finding forFNH.21Hepatic adenoma usually has decreased uptake.27 Theamount of uptake depends on the size and number of Kupfferand fibrous cells. Radiologically, FNH is sometimes mistakenas fibrolamellar HCC, but the fibrous scar of fibrolamellarHCC is usually large and eccentric with broad fibrous bandsand ca1cifications.8If all of the imaging studies fail to establisha finn diagnosis, histologic examination is warranted. Bycombining different imaging modalities, especially by usingMRI, a precise diagnosis of FNH can be achieved in 70% to90% of cases in centers with expertise in the appropriateimaging techniques.8
ManagementIn asymptomaticpatientswith FNH,treatmentgenerally
includes clinical follow-up to observe for the developmentof symptoms and radiologic follow-up with US to detectenlarging tumors.z9Most of resected cases are due to theundetenninednature of the tumor, the presenceof symptoms,or suspicionof metastasisin patients previouslyoperatedfor
@ 2005 Lippincott Williams & Wilkins
malignant diseases.28 When surgical resection is not possible,FNH may be treated by transarterial embolization.3.21 Onespecial concem in the management of FNH is the fear ofaccelerated growth of FNH with high-estrogen state such aspregnancy. Although the association between pregnancy andtumor enlargement or development of significant symptomsincluding tumor rupture have not been clearly established forFNH,6 it may be prudent to observe pregnant patients withFNH with more frequent US during pregnancy and the post-partum period.
SnmmaryFNH is the second most common benign tumor of the
liver, next to hemangioma. Patients are rarely symptomatic.Multiphasic CT and enhanced MRI are the most useful diag-nostic modalities. Definitive diagnosis may require histologicexamination in selected cases. Treatrnent includes conserva-tive clinical follow-up in asymptomatic patients. Surgicalresection is indicated for those with significant symptoms or inwhom malignancy cannot be excluded by radiologic and his-tologic studies.
Hepatic Adenoma
Pathogenesis and PathologyHepatic adenoma (HA) is arare hepatic tumor that is
pathologically characterized by the benign proliferation ofhepatocytes. As seen with FNH, HA also occurs predomi-nant1y in young women with a female-to-male ratio of 4: 1.5The pathogenesis of HA remains disputed, but the strongassociation with oral contraceptive use has been documented.HA was extremely rare before the introduction of oralcontraceptives in the 1960s. Since 1960s, the incidence hasgreat1y increased, and HA occurs more frequent1y in patientswith a history of long-tenn and high-dose estrogen use.30Withdrawal of oral contraceptives is reported to induce theregression of the tumor, although this may take severalmonths.22 In addition to oral contraceptives, anabolicandrogen-containing steroid medications also may increasethe incidence, number, and size of HA. Another risk group forHA includes patients with glycogen storage disease. Theprevalence is 50% in patients with Type I glycogen storagedisease (von Gierke) and 25% with Type III disease.4 In thesepatients, adenomas are also more likely to be multiple and toundergo malignant transfonnation, although the latter is stillrare.31
Macroscopically, HA is usually solitary (70%-80%), well-circumscribed, round, unencapsulated, but it often fonnspseudo-capsules by compressing adjacent hepatic tissue. Theyhave yellow-tan color with diameter ranging from 5 to 15 cm,and up to 30 cm on rare occasions.4 Grossly, intratumoral fat,necrosis, hemorrhage, or large subcapsular vessels are com-monly observed. Microscopically, HA includes large plates ofcells that resemble nonnal hepatocytes and are separated bydilated sinusoids. These sinusoids are perfused by feedingarteries, which contribute to the hypervascularity of HA. Thepresence of hypervascularity, loosely organized connective
405
74

T
Choi and Nguyen J Clin Gastroenterol. Volume 39, Number 5, MaY/June 2005
tissues, the absence of a true capsule, and the subcapsularlocation ofHA explain its propensity for rupture and bleeding.HA does not contain bile ductules, a key histologic finding thatdistinguishes it from FNH.30 Kupffer cells may be present butare often few.26
Clinical Presentation
Most patients with no more than a few small adenomasare asymptomatic. In I case series with 44 patients, 48% ofpatients are detected incidentally and 44% have symptoms.5Large HA may cause a sensation of right upper quadrantfullness or discomfort. HA is of clinical importance because ofits tendency to spontaneous rupture, hemorrhage. Therefore,acute abdominal pain and catastrophic intraperitoneal hemor-rhage are not uncommon presentation of HA.22 Rare cases ofmalignant transformation have also been reported, particularlyin patients with large or multiple tumors.8 In the absence ofmalignancy, serum alpha-fetoprotein and liver function testsare usually normal in patients with HA.
ImagingOn US, hepatic adenomas have variable and nonspecific
appearances depending on the character of the tumor.Hypoechoic, hyperechoic, and mixed-echoic patterns repre-sent simple adenoma, adenoma with fatty metamorphosis,hemorrhage, and necrosis, respectively.32 Color Doppler USsometimes demonstrates peripheral peritumoral and intra-tumoral vessels with a flat continuous or uncommonly, tripha-sic waveform. These findings are absent in FNH, so it can beused to differentiate between these 2 types of tumors.30 USfindings with contrast enhancement using Levovist may alsobe helpful. In the hepatic phase, 5 minutes following contrastinjection, the tumor shows relatively low uptake incomparison with the surrounding liver. Other benign tumorsthat have strong Kupffer cell activity such as FNH and somehemangiomas demonstrate strong homogeneous activity sim-ilar to adjacent hepatic parenchyma, while malignant tumorssuch as HCC and metastasis demonstrate no uptake.24.33
On multiphasic CT and MRI, HA may show morespecific findings. Unlike FNH, HA is frequent\y heteroge-neous due to intratumoral hemorrhage, necrosis, and fatcomponents on CT. HA containing none of these componentsis nearly iso-attenuating to normalliver on unenhanced phaseas well as portal-venous and delayed phases. HA shows earlyenhancement because of their rich arterial supply. Peripheralenhancement with centripetally progression is often detected,reflecting the presence of the large subcapsular feedingvessels.26
MRI findings can also be very characteristic. On TI-weighted images, adenomas have been described variously ashyperintense, isointense, or hypointense due to the presence ofhemorrhage, necrosis, or fat components. However, 35% to77% of cases are described as hyperintense. On T2-weightedimages, 47% to 74% of adenomas are also predominant\yhyperintense.30 On dynamic contrast-enhanced MR images,HA demonstrates early arterial enhancement. SPIO-enhancedMR is useful to distinguish adenomas from HCC. In contrastto HA, which typically shows signalloss on T2-weighted im-ages, malignant hepatic tumors generally lack Kupffer cells
406
and show no signal IOSS.34As discussed earlier, hepaticscintigraphy with 99mTc-sulfur-colloid demonstrates HA withabsent or decreased uptake, reflecting decreased number orfunction of Kupffer cells.
ManagementBecause ofthe risk of spontaneous rupture and malignant
transformation, HA must be identified and treated prompt\y.After the diagnosis of HA, the most common recommendedtreatrnent is a surgical resection due to the above complica-tions.29.30However, especially in small «5 em) HA, discontin-uation of estrogen and follow-up with US can also beconsidered.35 The treatrnent options include surgical enucle-ation, resection, transplantation, and hepatic arterial emboliza-tion, which is also an effective option for the treatrnent of HAwith acute hemorrhage.30 Liver transplantation is required forpatients with diffuse or multifocal adenomas. Laparoscopicsurgery offers an alternative modality for small HA with goodsurgical outcomes according to one case series with 17 patientsof HA.28
SummaryHA is arare benign tumor; however, it is important to
recognize this tumor and to differentiate it from other hepatictumors because of the risk of hemorrhage and malignanttransformation. HA is usually detected with US, but it has nospecific features on US. Color Doppler US, multiphasic CT,and MR can offer better characterization of HA. Criteria thatguide treatrnent include the number and size ofthe lesions, thepresence of symptoms, and the surgical risk incurred bypatients.
Other Types of Hepatic Adenoma
Hepatic Adenomatosis
Hepatic adenomatosis is defined as more than 10adenomas, and it is considered a distinct disease entity due todifferent clinical features.36It has been reported in the absenceof oral contraceptive use or glycogen storage disease with M:Fratio of I: 1. Patients often present with clinical symptoms suchas abdominal pain, hepatomegaly, and impaired liver function.Adenomatosis has higher tendency toward rupture, hemor-rhage, and malignant transformation, leading to a poorerprognosis.36 The imaging and histologic features are similar toadenomas. Diagnosis is usually made by exclusion of otherhepatic tumors, since multifocal HCC or metastasis is muchmore common in the presence of multiple solid hepaticlesions. Close follow-up is warranted and liver transplantationis sometimes necessary.37
Intrahepatic Bife Duct AdenomaBile duct adenoma is a benign and asymptomatic mass
that is typically discovered incidentally at imaging studies,surgery, or at autopsy. I It is usually a well-circumscribed, sub-capsular mass with a diameter ofless than I em and composedof bile ductules, inflammatory cell, and fibrosis. Radiologicimaging findings are nonspecific. Histologic analysis is the keyin differentiating intrahepatic bile duct adenoma from otherhepatic malignancy such as cholangiocarcinoma or metastasis.Treatrnent is usually not required.
@ 2005 Lippincott Williams & Wilkins
75

I CIin Gastroenterol. Volume 39, Number 5, MaY/June 2005
Nodular Regenerative HyperplasiaPathogenesis and Pathology
Nodular regenerative hyperplasia (NRH) is a benignproliferative lesion, which has been referred to by many namesin the literature including nodular transformation, noncirrhoticnodulation, and partial nodular transformation. It is a distinctdisease entity characterized by diffuse involvement ofthe liverwith nodules composed of hyperplastic hepatocytes, and itshould not be confused with the regenerative nodules ofcirrhosis or FNH.9 Macroscopically, NRH is characterized bymultiple bulging regenerative nodules in clusters with rangingsizes ITom0.1 to 4 cm. This gross finding may not be differentITom micronodular cirrhosis.5 However, microscopic featuresare very characteristic and readily distinguishable ITomcirrhosis. Histologic examination reveals the regeneration ofhepatocytes with multinucleated hepatocytes and thickenedregenerating hepatocytes with centrilobular atrophy. Theseregenerating nodules also compress the central veinscurvilinearly, and there is a lack of fibrotic reactions. On theother hand, NRH and HA share similar benign process andhistologic eIements and are difficult to be distinguished ITomeach other based on a single-needle biopsy. Multiple biopsiesare often helpful as NRH is a diffuse or multinodular process,whereas HA is a solitary process in which the remainder oftheliver is normal.22
The pathogenesis ofNRH is not well known. One oftheproposed theories hypothesizes that a primary vascular processleads to obliteration of portal vein, which in tum inducesischemia, atrophy of hepatocytes in the central zone, and theproliferation of hepatocytes.38 The other theory proposes thata preneoplastic process leads to NRH due to the reported highprevalence of hepatocyte dysplasia (200/0-42%) and HCCformed in livers of patients with NRH.39 According to twolarge case series, the prevalence of NRH was reported to be2.1% and 2.6%.4 NRH mostIy affects patients older than50 years of age, and the gender distribution of NRH isvariable.
Wide spectrum of systemic diseases and drugs are alsoassociated with NRH such as myeloproliferative disorders,Iymphoproliferative disorders, chronic vascular disorders, rheu-matologic and collagen vascular diseases (rheumatoid arthritis,Felty's syndrome, polyarteritis nodosa, amyloidosis, and pri-mary biliary cirrhosis), solid organ transplantation (renal andliver transplantation), and use of steroids or chemotherapeuticagents.22
Clinical Presentation
Clinically, NRH usually cause no symptoms and arediscovered incidentally during imaging studies or surgery.Some patients present mainly with symptoms of portal hy-pertension such as hepatomegaly, splenomegaly, ascites, oresophageal varices due to the compression of the main portalvein at the hepatic hilum. Other cholestatic symptoms can alsooccur.40Mild and nonspecific eIevated liver function tests maybe seen. Rarely, hepatic failure, rupture of the liver, or malig-nant transformation can occur.39 Because of these clinicalfeatures, the diagnosis of NRH should be considered inpatients with clinical signs of portal hypertension and normal
@ 2005 Lippincott Wil/iams & Wilkins
Benign Hepatic Tumors
or mildly abnormalliver function test, in whom other causes ofportal hypertension have been excluded.
ImagingImaging findings are not specific, and histologic
examination is often warranted. In most cases, US showsnormal hepatic parenchyma. In a few cases, well-delineatedhypoechoic or isoechoic nodules can be depicted. Hyperechoicnodules have been reported in very rare cases.41On enhancedCT, NRH shows normal findings or hypoattenuating nodules.Hyperattenuating portion of nodule represents hemorrhage orarterioportal shunting.22,41There are only a few reports on theMR findings. Lesions are described as hyperintense on Tl-weighted images and iso- or hypointense to normal liver onT2-weighted images.42.43
ManagementAccurate diagnosis should be confirmed with histologic
examination prior to treatment. In highly suspicious cases,open biopsy is indicated to obtain adequate sample of hepatictissue since percutaneous needle biopsies may give falselynormal results.4 Management depends on the cIinical symp-toms. In asymptomatic patients, no treatment is recommendedexcept for periodic follow-up to monitor for development ofHCC, although this is very rare. In patients with complicationsofportal hypertension, appropriate management including drugtherapy, endoscopic therapy, or portocaval shunt is necessary.4Rarely, patients may progress to liver failure and finally requireliver transplantation.5
SummaryNRH is another benign hepatic tumor that is often
detected as incidental findings. The diagnosis ofNRH usuallyrequires clinical, radiologic, and histologic examinations. Accu-rate diagnosis is the key, and treatment is indicated based on thepatient's cIinical presentations.
Macroregenerative Nodule
Pathogenesis and PathologyMacroregenerative nodule (MRN) was previously
cIassified as adenomatous hyperplasia or high-grade dysplasticnodule (> I cm).25 MRN occurs on the background of thecirrhotic liver, acute massive or submassive necrotic liver.Nowadays, MRNs are more ITequentIy detected in liverexplants after orthotropic liver transplantation.44 Clinicalimportance of MRN is its malignant transformation toHCC, although it is not cIear how what percentage of MRNwill progress to malignancy. The reported prevalence of MRNvaries between 14.2% and 25% on autopsy series.44 In acutemassive or submassive necrosis, remaining hepatic parenchymashows compensatory lobular hyperplasia after parenchymalloss. In cirrhotic liver, the hyperplastic reactions occur asa result of even a larger amount of cellloss. Regenerating isletsof viable cells are formed between destructed areas, and theseislets make up the nodular structures.7
Macroscopically, MRN has a greener or paler colorcompared with the surrounding cirrhotic liver. As comparedwith HCC, MRN has lower proliferation indices, which is nogreater than three-cell thickness.23 At times, MRN may
407
76

TChoi and Nguyen J Clin Gastroenterol·Volume 39, Number 5, MaY/June 2005
demonstrate ischemic coagulative necrosis and hemorrhage,nuclear crowding, and microacinal formation that herald thedevelopment ofHCC. MRN usually has variable atypia. Morespecifically, MRN without atypia is classified as Type I andMRN with atypia as Type 11.
Clínical Presentation and ImagingPatients have no specific symptoms since MRN is
usually discovered by imaging studies in patients with cir-rhosis or advanced fibrosis for evaluation of HCC. Liverfunction test with viral markers study shows the etiology andseverity of underlying liver disease.
MRN is rarely detected on screening US.45 On CT, thepresence of MRN can be suggested by nodular hepatic contour,and nodules are iso-attenuating to surrounding liver duringarterial and portal phases.46 On MRI, lesions show variablesignal intensities on Tl-weighted images and typically hypo-intensity on T2-weighted images with no enhancement onarterial enhanced phase. These are distinguishable features fromHCC, which typically are hyperintense on T2-weighted imageswith strong enhancement during the arterial phase.45.47Sparsecentral or peripheral blood supply is found on angiographywithout neovascularity. HCC emerging from MRN can bedemonstrated as nodule-in-nodule pattem on imaging studiesdue to their histologic uneven growth.48
Management and SummaryMRN is a benign but premalignant lesion found in
cirrhotic or fibrotic livers. Imaging findings are not charac-teristic, but MRI findings are useful for the differentiation fromHCC. Because of its malignant potential, surgical resection ofMRN is sometimes advocated, especially in those with atypia.Optimal management of MRN remains unknown pendingongoing investigation.
Other Solid Tumors
Mesenchymal Hamartoma
Mesenchymal hamartoma of the liver is an uncommonbenign lesion composed ofbile ducts, immature mesenchymalcells, and hepatocytes.49 Most of them are diagnosed duringchildhood, although a few cases have been reported in adults.50The clinical presentation is nonspecific, and imaging findingsreveal solid or multicystic lesions.51 Although hamartoma canbe diagnosed by percutaneous biopsy, diagnosis is usuallyestablished after surgical excision.
Focal Fatty ChangeHepatic steatosis is generally a diffuse process, but focal
distribution offat is quite common in the liver called focal fattychange.52 The pathogenesis is not well understood, butregional hypoxia of hepatic tissue is thought to play a roleaccording to one theory.53 The majority of patients haveunderlying disease such as diabetes, obesity, and malnutrition.Lesions are often discovered incidentally on imaging studiesand characteristically show a fan-shaped or geographic pattemmainly in subcapsular areas or regions adjacent to thefaIciform ligamento54 Focal fatty change can be found assingle or multiple lesions with variable sizes in a few cen-
408
timeters up to 10 cm. These tumor-like lesions may bemistaken for other hepatic tumors, and liver biopsy is oftenrequired for a definitive diagnosis.53
Lipomatous TumorLipomatous tumors such as hepatic angiomyolipoma or
hepatic lipoma are very rare benign tumors. Patients areusually asymptomatic, and lesions are often encountered inpatients with tuberous sclerosis.8 As their names imply, on theimaging studies, lipoma shows uniform fat component,whereas angiomyolipoma also contains intratumoral vesseland smooth muscle component. Atypical cases should becarefully differentiated from other hypervascular tumorsincluding HCC, FNH, and hemangioma.55 Fine-needle as-piration is occasionally required and reveals fat cells,epithelioid smooth muscle cells, and blood vessels.56 Theprognosis is good, and surgical resection may be needed ifpatients have symptoms related to mass effect.57,58
lnjlammatory PseudotumorInflammatory pseudotumor is an extremely rare benign
hepatic tumor. It has the appearance of a malignant tumor buthas a benign histology and clinical course.59 The etiology isunclear, but underlying infectious agents are strongly sug-gested as the pathologic process.60 The clinical presentation isnonspecific. Patients may have fever, malaise, weight loss, andsymptoms related to a mass effect. Routine imaging proceduresare not sufficient to make the diagnosis, and a biopsy isnecessary to differentiate it from other tumors.61 Histologicexamination reveals myofibroblasts, polyclonal plasma cell, andfibrous tissue. The course of the disease is unpredictable. Inmost of the reported cases, the patients underwent resection.62
CYSTIC TUMORS
Sim pie Cyst
Pathogenesis and PathologyHepatic cysts are relatively common and most often
discovered incidentally. Simple hepatic cysts are usually con-genital. During embryogenesis, abnormal or excessive intra-hepatic bile ducts develop. These ducts are obstructed or fail toconnect with extrahepatic ducts and eventually form hepaticcysts. Despite their pathogenesis, communication with thebiliary duct is very rare, and simple cysts usually contain clearfluid with a similar composition to serum.63 Hepatic cysts arerecognized with increasing frequency as imaging modalitiesadvance. The US prevalence is reported to be 5%. There is astrong female predominance and presentations occur mostfrequently in the fifth decade.64 Histologically, simple cysts arelined by simple cuboidal epithelium, identical to that of bileducts and thin underlying rim of fibrous stroma.
Clínical Presentation and ImagingPatients are usually asymptomatic, and solitary cysts
that become symptomatic are generally larger than 5 cm.These can cause mass effects such as right upper quadrantpain. Rarely,other complicationssuch as intracystichemor-rhage and infection may develop and present a diagnosticchallenge.65Hepaticcystscanusuallybe diagnosedby USoOn
@ 2005 Lippincott Williams & Wilkins
77

I Clin Gastroenterol. Volume 39, Number 5, May/june 2005 Benign Hepatic Tumors
CT and MR1, simple cysts have water attenuation, withimperceptibleand small thin wall, withoutseptations,or withenhancementof its wall or content.64ln cases of intracystichemorrhage,the signal intensityis high, with fluid-fluidlevei,on the both Tl- and T2-weightedimages when mixed bloodproducts are present. 2
ManagementMost simple hepatic cysts do not cause any symptom
and are best managed conservatively. The preferred treatmentof symptomatic cases is US- or CT-guided percutaneous cystaspiration followed by sc1erotherapy with a1cohol (or doxy-cyc1ine). Surgical treatment is indicated if it is difficult toexclude malignancy or if there is biliary communication orinfection.66 Laparoscopic fenestration and deroofing have beendocumented to be safe and effective.67,68The choice between
open and laparoscopic surgery depends on the location of thecyst in the liver.
SummaryHepaticcysts are commonbenign tumors,especiallyin
older patients and female patients. They are usually asymp-tomatic and found incidentally. lmaging features are verytypicaL Complications such as intracystic hemorrhage orinfection are very rare. Management inc1udesconservativeobservation,laparoscopicor open surgical treatment.
Polycystic Liver DiseasePolycystic liver disease is an autosomal dominant
disorder often found in association with renal polycysticdisease. Patients are usually asymptomatic, but advanceddisease can result in hepatomegaly, liver failure, or Budd-Chiari syndrome.2,68 Although the diagnosis is easily madewith both CT and MR imaging, MR imaging is more sensitivefor the detection of complicated cysts.2
Choledochal CystPathogenesis and Pathology
Choledochal cysts are congenital bile duct anomalies.These cystic dilatations of the biliary tree can involve theextrahepatic biliary ducts, the intrahepatic biliary ducts, orboth.69 Choledochal cysts are more prevalent in Asia than inthe United States or other Westem countries. No strongunifying etiologic theory exists for choledochal cysts. Thepathogenesis may be multifactoriaL ln many patients withcholedochal cysts, an anomalous junction between the com-mon bile duct and pancreatic duct can be demonstrated. Thisabnormal union allows pancreatic secretions to reflux into thecommon bile duct, where the pancreatic proenzymes becomeactivated, thereby damaging and weakening the bile duct wall.Defects in epithelialization and recanalization of the de-veloping bile ducts and congenital weakness ofthe ductal wallhave also been implicated.70
Clinical Presentation and ImagingThe c1inicalhistory and presentationof patients with a
choledochal cyst vary with the patient's age. The classicpresentationsof adultpatientsarejaundice, pain, and palpable
@ 2005 Lippincott Williams & Wilkins
mass, but some patients also present with cholangitissymptoms including fever or vague dyspeptic symptoms.71
For diagnosing choledochal cysts, US is the modality ofchoice. The communication with the biliary ductal systemmust be demonstrated. Depending on the type of choledochalcysts, dilatation of the intrahepatic ducts and the presence ofintrahepatic cysts may or may not be demonstrated. CT, MR1,and magnetic resonance cholangiopancreatography (MRCP)help to delineate the anatomy of the lesion and of thesurrounding structures. These tests can also assist in definingthe presence and extent of potential intrahepatic ductalinvolvement. lnvasive studies inc1uding percutaneous trans-hepatic cholangiography (PTC) or endoscopic retrogradecholangiopancreatography (ERCP) are particularly helpful indemonstrating the presence of an anomalous pancreaticobili-ary junction and in delineating associated extrahepatic orintrahepatic strictures and stones.
ManagementThe treatment of choice for choledochal cysts is the
complete excision of the cyst with a biliary-entericanasto-mosis to restore continuity with the gastrointestinal tract. 72
Appropriate antibiotic therapy and supportive care should begiven to patients presenting with cholangitis. Laparoscopicresection of choledochal cyst and reconstruction has beenreported to be technically feasible.73
SummaryCholedochal cyst is a congenital bile duct anomaly, US
findings are diagnostic in many patients; however, comple-mentary studies such as CT, MRI!MRCp, or PTC/ERCP maybe helpful in the preoperative period for delineating details ofthe surrounding anatomy. The best treatment is completeexcision with biliary-enteric reconstruction.
Echinococcal Cyst
Pathogenesis and PathologyHydatid cysts or echinococcal cysts are still endemic in
certain parts of the world and caused by the tapewormsEchinococcus granulosus or Echinococcus multilocularis.74Humans can become infected upon ingesting the eggs of theparasite direct1y,through contact with sheep, cats, dogs, cattle,or by contaminated water or food.75 The liver parenchymafilters out most of the embryos, and those that are not de-stroyed transform into small cysts that grow over time.Depending on the condition of the parasite and the hostreaction, the cyst can degenerate and may eventually collapse,leaving an area of calcification in the liver. After the initialhepatic involvement, local extension or metastatic spread tothe lungs, brain, bones, or bulbous oculi may be seen inEchinococcus multilocularis infection,76
Microscopically, hydatid cyst is composed of threelayers: the outer pericyst, which corresponds to compressedhepatic tissue; the endocyst, an inner germinal layer; and theectocyst, a translucent thin interleaved membrane. Maturationof a cyst is characterized by the development of daughter cystsin the periphery as a result of endocyst invagination, Peripheralcalcifications are common in both viable and nonviable cysts.2
409
78

Choi and Nguyen
Clinical Presentation and ImagingThe majority of patients are asymptomatic, but some
may present with abdominal pain, fever, or hepatomegaly.Anaphylactic shock may occur due to rupture of cysts into theperitoneal cavity. Helpful diagnostic features include eosin-ophilia, positive serologic tests, and radiologic imaging.
On US or CT, hydatid cysts appear as well-definedlesions with distinguishable walls. AIso, calcified rims,intracystic septations, and daughter cysts can be seen.77.78MR images clearly demonstrate the pericyst, the matrix, anddaughter cysts. The pericyst is seen as a hypointense rim onboth Tl- and T2-weighted images because of its fibrouscomponent and the presence of calcification. The hydatidmatrix (hydatid "sand") appears hypointense on Tl- andmarkedly hyperintense on T2-weighted images. Daughtercysts are more hypointense than the matrix on T2-weightedimages.2.74On the contrast-enhanced images, solid compo-nents of the cysts are weakly enhanced?4
ManagementSurgical treatment can cure the patients ifthe entire cysts
are removed. Special care should be taken not to spill thehydatid fluid during surgery because spillage of the hydatidfluid can induce anaphylactic reaction.79 Laparoscopic treat-ments including simple drainage, unroofing, and pericystec-tomy have been reported to be safe and effective.80 Medicaltreatment with albendazole or mebendazole only is noteffective but can be used as an adjuvant therapy.
SummaryHydatid cysts are caused by tapeworm infection, which
has a worldwide distribution. Most patients are asymptomatic.Diagnosis is made by eosinophilia, positive serologic tests, andcharacteristic imaging features. Treatments include medical,surgical, and laparoscopic procedures.
Other Cystic Tumors
Biliary Cystadenoma
Biliary cystadenoma is an uncommon, slow-growingtumor and is considered a premalignant lesion.81 Malignanttransformation to cystadenocarcinoma is not uncommon. Itoccurs predominantly in female patients between 30 and 50years of age. Histologically, the tumor emerges as multilocularcyst with a single layer ofbiliary epithelium. On enhanced CT,it is a multilocular cystic lesion with typical enhancement ofthe cystic walls, internal septations, and mural nodules. I TheMRI findings vary depending on the protein content of thefluid and the presence of an intracystic soft-tissue component.Imaging findings are similar to cystadenocarcinoma, althoughthe polypoid projection with pedunculated excrescence ismore common in cystadenocarcinoma.2 For treatment, surgicalresection is mandatory if cystadenocarcinoma is suspected.82After surgical resection, recurrence is quite common.
Von Meyenburg ComplexBile duct hamartomas, also known as von Meyenburg
complex, are relatively common benign lesions composed ofdisorganized proliferation of bile ductules and fibrocollage-nous stroma.83 Radiologic imagings are nonspecific, revealing
410
/ CIinGastroenterol·Volume 39, Number 5, MaY/June 2005
multiple subcentimeter nonenhanced lesions.84 von Meyen-burg complex is of no clinical importance, except for mim-icking metastasis or microabscess.85 Further evaluation ortreatment is not required.
Caroli Disease
Caroli disease is arare, autosomal-recessive develop-mental disorder characterized by nonobstructive sacculardilatation of intrahepatic bile ducts, multiple intrahepaticcalculi, and is associated with polycystic renal disease.86Clinical symptoms include recurrent attacks of fever, rightupper quadrant pain, and rarely jaundice. US is the best initialimaging study because it reveals the irregular dilatation ofthelarge intrahepatic ducts. On enhanced CT and MRI, thepresence of tiny dots with strong enhancement within dilatedintrahepatic ducts ("central dot" sign), reflecting intraluminalportal vein radicles, is very suggestive finding of Carolidisease.87 Surgical treatment may be necessary for recurrent orrefractory cholangitis. Broad-spectrum antibiotic coverage isindicated in cases of cholangitis.
Peliosis HepaticaPeliosis hepatis is arare benign lesion that is char-
acterized by the presence of diffuse blood-filled cystic spaces.It can occur in the liver, spleen, bone marrow, and lungs.88 Ithas been reported to associate with long-term treatment ofsteroid, estrogen, tamoxifen, immunoglobulin, malignancy(hepatocellular carcinoma and adenoma), hematologic disease(Hodgkin disease, multiple myeloma), renal transplantation,and infections (tuberculosis, AIDS). Radiologic imagingfindings are cystic lesions with variable sizes. Sometimes,very smalllesions are detected as noncystic or diffuse hepaticlesions.88.89Treatment should include withdrawal of the pos-sible causative agents and specific treatment such as antibioticsin patients with either primary or secondary infections.
REFERENCESI. Horton KM, Bluemke DA, Hruban RH, et aI. CT and MR imaging of
benign hepatic and biliary tumors. Radiographics. 1999;19:431-451.
2. Mortele lU, Ros PR. Cystic focalliver lesions in the adult: differential CT
and MR imaging features. Radiographics. 2001;21:895-910.
3. De Rave S, Hussain SM. A liver tumour as an incidental finding:differential diagnosis and treatment. Scand J Gastroenterol. 2002;236(suppl):81-86.
4. Biecker E, Fischer HP, Strunk H, et aI. Benign hepatic tumours. Z Gas-troenterol. 2003;41: 191-200.
5. Trotter JF, Everson GT. Benign focallesions ofthe liver. Clin Liver Dis.200 1;5: 17-42.
6. Cobey FC, Salem RR. A review of liver masses in pregnancy anda proposed algorithm for their diagnosis and management. Am J Surg.2004;187: 181-191.
7. Colombo M. Malignant neoplasm ofthe liver. ln: SchiffER, Sorrell MF,Maddrey WC, eds. Schifl's Diseases of the Liver, 9th ed. Philadelphia:Lippincott WilIiams & Wilkins, 2002:1377-1403.
8. Mergo PJ, Ros PR. Benign lesions of the liver. Radiol Clin North Am.1998;36:319-331.
9. Federle MP, Brancatelli G. lmaging ofbenign hepatic masses. Semin LiverDis.2001;21:237-249.
10. Hochwald SN, Blumgart LH. Giant hepatic hemangioma with Kasabach-Merritt syndrome: is the appropriate treatment enucleation or livertransplantation? HPB Surg. 2000;11:413-419.
11. Isozaki T, Numata K, Kiba T, et aI. Differential diagnosis of hepatictumors by using contrast enhancement patterns at USo Radiology. 2003;229:798-805.
@ 2005 Lippincott Williams & Wilkins
79

J C/in Gastroenterol. Volume 39, Number 5, MaY/June 2005 Benign Hepatic Tumors
12. Lee JY, Choi Bl, Han JK, et aI. lmproved sonographic imaging ofhepatic
hemangioma with contrast-enhanced coded hannonic angiography:comparison with MR imaging. Ultrasound Med Biol. 2002;28:287-295.
13. Valette PJ, PiIleul F, Crombe-Ternamian A. MOCTofbenign livertumorsand metastases. Eur Radiol. 2003;13:31-41.
14. Olcott EW, Li KC, Wright GA, et aI. Oifferentiation of hepatic
malignancies from hemangiomas and cysts by T2 relaxation times: early
experience with multiply refocused four-echo imaging at 1.5 T. J MagnReson Imaging. 1999;9:81-86.
15. Unal 0, Sakarya ME, Arslan H, et aI. Hepatic cavernous hemangiomas:
patterns of contrast enhancement on MR fluoroscopy imaging. ClinImaging. 2002;26:39-42.
16. Kim T, Federle MP, Baron RL, et aI. Oiscrimination of small hepatichemangiomas from hypervascular malignant tumors smaller than 3 cm
with three-phase helical CT. Radiology. 200 I ;219:699-706.
17. Jang HJ, Kim TK, Lim HK, et aI. Hepatic hemangioma: atypical
appearances on CT, MR imaging, and sonography. AJR Am J Roentgenol.2003;180:135-141.
18. Yoon SS, Charny CK, Fong Y, et aI. Oiagnosis, management, and
outcomes of 115 patients with hepatic hemangioma. J Am Col/ Surg.2003; 197:392-402.
19. Srivastava ON, Gandhi O, Seith A, et aI. Transcatheter arterialembolization in the treatment of symptomatic cavernous hemangiomasofthe liver: a prospective study. Abdom Imaging. 2001;26:510-514.
20. Hussain SM, Terkivatan T, Zondervan PE, et aI. Focal nodularhyperplasia: findings at state-of-the-art MR imaging, US, CT, andpathologic analysis. Radiographics. 2004;24:3-17.
21. Kehagias O, Moulopoulos L, Antoniou A, et aI. Focal nodularhyperplasia: imaging findings. Eur Radiol. 2001;11:202-212.
22. Mortele KJ, Ros PR. Benign liver neoplasms. Clin Liver Dis. 2002;6: 119-145.
23. Brunt EM. Benign tumors ofthe liver. Clin Liver Dis. 2001;5:1-15.24. Von Herbay A, Vogt C, Haussinger O. Oifferentiation between benign and
malignant hepatic lesions: utility of color stimulated acoustic emissionwith the microbubble contrast agent Levovist. J Ultrasound Med. 2004;23:207-215.
25. Hussain SM, Zondervan PE, Uzermans JN, et aI. Benign versus malignanthepatic nodules: MR imaging findings with pathologic correlation.Radiographics. 2002;22: 1023-1036.
26. Fulcher AS, Sterling RK. Hepatic neoplasms: computed tomography andmagnetic resonance features. J Clin Gastroenterol. 2002;34:463-471.
27. Herman P, Pugliese V, Machado MA, et aI. Hepatic adenoma and focalnodular hyperplasia: differential diagnosis and treatment. World J Surg.2000;24:372-376.
28. Oescottes B, Glineur O, Lachachi F, et aI. Laparoscopic liver resection ofbenign liver tumors. Surg Endosc. 2003;17:23-30.
29. Kim J, Ahmad SA, Lowy AM, et aI. An algorithm for the accurateidentification ofbenign liver lesions. Am J Surg. 2004;187:274-279.
30. Grazioli L, Federle MP, Brancatelli G, et aI. Hepatic adenomas: imagingand pathologic findings. Radiographics. 200 1;21:877-892.
31. Lee P1. Glycogen storage disease type I: pathophysiology of liver ade-nomas. Eur J Pediatr. 2002;161(suppl):46-49.
32. Hung CH, Changchien CS, Lu SN, et aI. Sonographic features ofhepaticadenomas with pathologic correlation. Abdom Imaging. 2001;26:500-506.
33. Lim AK, Patel N, Gedroyc WM, et aI. Hepatocellular adenoma: diagnosticdifficulties and novel imaging techniques. Br J Radiol. 2002;75:695-699.
34. Beets-Tan RG, Van Engelshoven JM, Greve Jw. Hepatic adenoma andfocal nodular hyperplasia: MR findings with superparamagnetic ironoxide-enhanced MRI. Clin Imaging. 1998;22:211-215.
35. Terkivatan T, de Wilt JH, de Man RA, et aI. Indications and long-termoutcome of treatment for benign hepatic tumors: a critical appraisal. ArchSurg.2001;136:1033-1038.
36. Grazioli L, Federle MP, Ichikawa T, et aI. Liver adenomatosis: clinical,histopathologic, and imaging findings in 15 patients. Radiology. 2000;216:395-402.
37. Chiche L, Oao T, Salame E, et aI. Liver adenomatosis: reappraisal,diagnosis, and surgical management: eight new cases and review of theliterature. Ann Surg. 2000;231 :74-81.
38. AI-Mukhaizeem KA, Rosenberg A, Sherker AH. Nodular regenerativehyperplasia ofthe liver: an under-recognized cause ofportal hypertensionin hematological disorders. Am J Hematol. 2004;75:225-230.
@ 2005 Lippincott Wi//iams & Wilkins
39. Oogan E, Ozgur R, Ercan V, et aI. Nodular regenerative hyperplasia oftheliver: a case reporto Turk J Gastroenterol. 2003;14:64-67.
40. Arvanitaki M, Adler M. Nodular regenera tive hyperplasia of the liver:
a review of 14 cases. Hepatogastroenterology. 2001;48:1425-1429.
41. Clouet M, Boulay I, Boudiaf M, et aI. Imaging features of nodular
regenerative hyperplasia of the liver mimicking hepatic metastases.Abdom Imaging. 1999;24:258-261.
42. Casillas C, Marti-Bonmati L, Galant 1. Pseudotumoral presentation of
nodular regenerative hyperplasia of the liver: imaging in five patientsincluding MR imaging. Eur Radiol. 1997;7:654-658.
43. Horita T, Tsutsumi A, Takeda T, et aI. Significance ofmagnetic resonance
imaging in the diagnosis of nodular regenerative hyperplasia of the liver
complicated with systemic lupus erythematosus: a case report and reviewof the literature. Lupus. 2002; 11: 193-196.
44. Gurkan A, Sherlock MF, Chui AK, et aI. A giant multiacinarmacroregenerative nodule in an explanted liver. Transplantation. 200 I;72:538-539.
45. Rode A, Bancel B, Oouek P, et aI. Small nodule detection in cirrhoticlivers: evaluation with US, spiral CT, and MRJ and correlation withpathologic examination of explanted liver. J Comput Assist Tomogr. 200 I;25:327-336.
46. de Ledinghen V, Laharie O, Lecesne R, et aI. Oetection of nodules in liver
cirrhosis: spiral computed tomography or magnetic resonance imaging?A prospective study of 88 nodules in 34 patients. Eur J GastroenterolHepatol.2002;14:159-165.
47. Krinsky GA, Lee VS, Theise NO, et aI. Hepatocellular carcinoma anddysplastic nodules in patients with cirrhosis: prospective diagnosis withMR imaging and explantation correlation. Radiology. 200 I;219:445-454.
48. Serra C, Piscaglia F. Nodule in nodule: malignant transformationof a macroregenerative nodule in cirrhosis revealed by duplex-Ooppler.J Hepatol. 1999;30:955.
49. Cook JR, Pfeifer JD, Oehner LP. Mesenchymal hamartoma of the liver inthe adult: association with distinct clinical features and histologicalchanges. Hum Pathol. 2002;33:893-898.
50. Brkic T, Hrstic I, Vucelic B, et aI. Benign mesenchymalliver hamartomain an adult male: a case report and review of the literature. Acta MedAustriaca.2003;30:134-137.
51. Papastratis G, Margaris H, Zografos GN, et aI. Mesenchymal hamartomaofthe liver in an adult: a review ofthe literature. Int J Clin Pract. 2000;54:552-554.
52. Wanless IR. Benign liver tumors. Clin Liver Dis. 2002;6:513-526.53. Zeppa P, Anniciello A, Vetrani A, et aI. Fine needle aspiration biopsy of
hepatic focal fatty change: a report oftwo cases. Acta Cytol. 2002;46:567-570.
54. Itai Y, Saida Y. Pitfalls in liver imaging. Eur Radiol. 2002;12: 1162-1174.55. Yan F, Zeng M, Zhou K, et aI. Hepatic angiomyolipoma: various ap-
pearances on two-phase contrast scanning of spiral CT. Eur J Radiol.2002;41: 12-18.
56. Hogemann O, Flemming P, Kreipe H, et aI. Correlation of MRI and CTfindings with histopathology in hepatic angiomyolipoma. Eur Radiol.2001;11: 1389-1395.
57. Ren N, Qin LX, Tang ZY, et aI. Oiagnosis and treatment of hepaticangiomyolipoma in 26 cases. World J Gastroenterol. 2003;9:1856-1858.
58. Yeh CN, Chen MF, Hung CF, et aI. Angiomyolipoma of the liver. J SurgOncol. 200 I;77: 195-200.
59. Sakai T, Shiraki K, Yamamoto N, et aI. Oiagnosis of inflammatorypseudotumor ofthe liver. Int J Moi Med. 2002;10:281-285.
60. Koea JB, Broadhurst GW, Rodgers MS, et aI. lnflammatory pseudotumorof the liver: demographics, diagnosis, and the case for nonoperativemanagement. J Am Col/ Surg. 2003;196:226-235.
61. Choi BY, Kim WS, Cheon JE, et aI. Inflammatory myofibroblastic tumourofthe liver in a child: CT and MR findings. Pediatr Radiol. 2003;33:30-33.
62. Biecker E, Zimmermann A, Oufour JE Spontaneous regression of aninflammatory pseudotumor of the liver. Z Gastroenterol. 2003;41 :991-994.
63. Karavias DO, Tsamandas AC, Payatakes AH, et aI. Simple (non-parasitic)
liver cysts: clinical presentation and outcome. Hepatogastroenterology.2000;47: 1439-1443.
64. Carrim ZI, Murchison JT. The prevalence of simple renal and hepaticcysts detected by spiral computed tomography. Clin Radiol. 2003;58:626-629.
411
80

Choi and Nguyen J C/in Gastroenterol. Volume 39, Number 5, May/june 2005
65. Kitajima Y, Okayama Y, Hirai M, et aI. Intracystic hemorrhage of a simple
liver cyst mimicking a biliary cystadenocarcinoma. J Gastroenterol. 2003;38: 190-193.
66. Moorthy K, Mihssin N, Houghton pw. The management ofsimple hepatic
cysts: scIerotherapy or laparoscopic fenestration. Ann R Coll Surg Engl.2001;83:409-414.
67. Fiamingo P, Tedeschi U, Veroux M, et aI. Laparoscopic treatment of
simple hepatic cysts and polycystic liver disease. Surg Endosc. 2003; 17:623-626.
68. Hansman MF, Ryan JA Jr, Holmes JH 4th, et aI. Management and long-
terrn foIlow-up of hepatic cysts. Am J Surg. 200 I; I 81 :404-410.
69. Weyant MJ, Maluccio MA, BertagnoIli MM, et aI. Choledochal cysts inadults: a report of two cases and review of the literature. Am JGastroenterol. 1998;93:2580-2583.
70. Miyano T, Yamataka A. Choledochal cysts. Curr Opin Pediatr. 1997;9:283-288.
71. Durgun AV, Gorgun E, Kapan M, et aI. Choledochal cysts in adults and the
importance of ditferential diagnosis. J Hepatobiliary Pancreat Surg.2002;9:738-74 I.
72. Lipsett PA, Pitt HA. Surgical treatment of choledochal cysts. J Hepato-
biliary Pancreat Surg. 2003;10:352-359.
73. Tanaka M, Shimizu S, Mizumoto K, et aI. LaparoscopicaIly assisted re-
section of choledochal cyst and Roux-en- Y reconstruction. Surg Endosc.2001 ;15:545-552.
74. Kodama Y, Fujita N, Shimizu T, et aI. Alveolar echinococcosis: MR
findings in the liver. Radiology. 2003;228:172-177.
75. Kumar MJ, Toe K, BaneIjee RD. Hydatid cyst of liver. Postgrad Med J.2003;79:1 I3-1 14.
76. Harrnan M, Arslan H, Kotan C, et aI. MRI findings of hepatic alveolar
echinococcosis. Clin lmaging. 2003;27:411-416.
77. Caremani M, Lapini L, Caremani D, et aI. Sonographic diagnosis of
hydatidosis: the sign ofthe cyst waIl. Eur J Ultrasound. 2003; 16:217-223.
78. Haddad MC, BiIjawi GA, Khouzami RA, et aI. Unilocular hepaticechinococcal cysts: sonography and computed tomography findings. ClinRadiol.2001;56:746--750.
79. Buttenschoen K, Carli Buttenschoen D. Echinococcus granulosusinfection: the chaIlenge of surgi cal treatment. Langenbecks Arch Surg.2003;388:218-230.
80. Seven R, Berber E, Mercan S, et aI. Laparoscopic treatment of hepatichydatid cysts. Surgery. 2000; 128:36-40.
81. Kinoshita H, Tanimura H, Osishi H, et aI. Clinical features and imagingdiagnosis of biliary cystadenocarcinoma of the liver. Hepatogastroenter-ology.2001;48:250-252.
82. Hai S, Hirohashi K, Uenishi T, et aI. Surgical management of cystichepatic neoplasms. J Gastroenterol. 2003;38:759-764.
83. Mortele B, Mortele K, Seynaeve P, et aI. Hepatic bile duct hamartomas(von Meyenburg Complexes): MR and MR cholangiography findings.J Comput Assist Tomogr. 2002;26:438-443.
84. Motohara T, Semelka RC, Nagase L. MR imaging of benign hepatictumors. Magn Reson Imaging Clin North Am. 2002;10:1-14.
85. Neri S, Mauceri B, Cilio D, et aI. Biliary hamartomas (von Mayenburgcomplex): magnetic resonance imaging in a case reporto Intern Med 1.2004;34:71-72.
86. De Tommaso AM, Santos DS, Hessel G. Caroli's disease: 6 case studies.Acta Gastroenterol Latinoam. 2003;33:47-5 I.
87. Levy AD, Rohrrnann CA Jr, Murakata LA, et aI. Caroli's disease:radiologic spectrum with pathologic correlation. AJR Am J Roentgenol.2002; 179: 1053-1057.
88. Verswijvel G, Janssens F, CoIla P, et aI. Peliosis hepatis presenting asa multifocal hepatic pseudotumor: MR findings in two cases. Eur Radiol.2003; 13:40-44.
89. Gouya H, Vignaux O, Legmann P, et aI. Peliosis hepatis: triphasichelical CT and dynamic MRl findings. Abdom Imaging. 2001;26:507-509.
Reprinted from the Joumal ofClinical Gastroenterology (2005) 39(5):401-412, Choi BY, Nguyen MH, TheDiagnosis and Management of Benign Hepatic Tumors, Copyright @ 2005 with permission from Wolters
Kluwer, Lippincott Williams & Wilkins.412 @ 2005 Lippincott Williams & Wilkins
81