The Diabetic Kidney… What to do? - WVAFP...CME Information This Live activity, Diabetic Kidney......
46
The Diabetic Kidney… What to do? Michael Cobble, MD, FNLA Director Canyon Medical Center Sandy, Utah Adjunct Faculty University of Utah Salt Lake City, Utah
Transcript of The Diabetic Kidney… What to do? - WVAFP...CME Information This Live activity, Diabetic Kidney......

The Diabetic Kidney… What to do?
Michael Cobble, MD, FNLA Director
Canyon Medical Center Sandy, Utah
Adjunct Faculty University of Utah
Salt Lake City, Utah

Statement of Sponsorship and Support This CME Symposium is sponsored by and supported by an educational grant from Janssen Biotech, Inc., administered by Janssen Scientific Affairs, LLC.

In collaboration with
Join at http://www.pcmg-us.org for free resources, CME opportunities and information about metabolic issues.

CME Information
This Live activity, Diabetic Kidney... What to Do, from 06/01/2019 - 05/31/2020, has been reviewed and is acceptable for up to 1.00 Prescribed credit(s) by the American Academy of Family Physicians. Physicians should claim only the credit commensurate with the extent of their participation in the activity.

Faculty Disclosure Statement Primary Care Education Consortium adheres to the conflict of interest policy of the ACCME and the AMA. It is the policy of PCEC to ensure balance, independence, objectivity, and scientific rigor in all of its educational activities. All individuals in a position to control the content in our programs are expected to disclose any relationships they may have with commercial companies whose products or services may be mentioned so that participants may evaluate the objectivity of the presentations. In addition, any discussion of off-label, experimental, or investigational use of drugs or devices will be disclosed by the faculty. Only those participants who have no conflict of interest or who agree to an identified resolution process prior to their participation were involved in the CME activity.

Disclosures Michael Cobble, MD, has disclosed that he is on the speakers bureau for Amarin, Amgen, AstraZeneca and Regeneron for the clinical conditions of Lipids, CAD and Diabetes. Stephen Brunton, MD, has disclosed that he is on the advisory board for Abbott Diabetes, AstraZeneca, Bayer, Janssen, Novo Nordisk, Sanofi and Xeris Pharmaceuticals; as well as on the speakers bureau for AstraZeneca, Bayer, Janssen, Lilly, and Novo Nordisk. Gregory Scott, PharmD, RPh, Editorial Support, disclosed no relevant financial relationship or interest with a proprietary entity producing, marketing, reselling or distributing health care goods or services.

Learning Objectives After participating in the activity, the clinician should be able to: • Appropriately screen for the presence of chronic kidney disease in
patients with T2DM. • Identify chronic kidney disease at an early stage in patients with
T2DM. • Individualize evidence-based therapy to slow the progression of
kidney disease in patients with T2DM and chronic kidney disease.

Chronic Kidney Disease Is Common • Prevalence: 30 million US adults (15%)1
• 1-in-3 US adults with diabetes • 1-in-5 US adults with hypertension
• 45% of new cases of ESRD are due to diabetes2 • 48% of those with severely reduced kidney function but not on
dialysis are not aware of having CKD1
1. US Centers for Disease Control and Prevention. https://www.cdc.gov/diabetes/pubs/pdf/kidney_factsheet.pdf. Accessed March 25, 2019. 2. United States Renal Data System. https://www.usrds.org/2017/download/2017_Volume_2_ESRD_in_the_US.pdf. Accessed March 25, 2019.
CKD, chronic kidney disease; ESRD, end-stage renal disease

End-Stage Renal Disease, United States
0
50
100
150
200
250
300
350
400
1980
1985
1990
1995
2000
2005
2010
2015
Inci
denc
e pe
r mill
ion/
year
, sta
ndar
dize
d
Year
Incidence Rate of ESRD
2017
United States Renal Data System. https://usrds.org/2019/download/USRDS_2019_ES_final.pdf. Accessed November 19, 2019.
341

End-Stage Renal Disease, United States, 2017 (cont)
124,500
108,131
12,572 3666
0
25,000
50,000
75,000
100,000
125,000
Total ESRD Hemodialysis Peritoneal Dialysis Transplant
Num
ber o
f new
cas
es
Incidence, 2017
United States Renal Data System. https://usrds.org/2019/download/USRDS_2019_ES_final.pdf. Accessed November 19, 2019.

Prevalence Is Increasing in Adults with Diabetes and Low eGFR in the Absence of Albuminuria
0
0.5
1
1.5
2
2.5
3
UACR <30 mg/g UACR 30-299 mg/g UACR ≥300 mg/g
Popu
latio
n es
timat
e (m
illio
ns)
Persons with Diabetes and eGFR <60 mL/min/1.73 m2
1988-1994 1999-2002 2003-2006 2007-2010
Kramer H, et al. Diabetes Care. 2018;41:775-781.
UACR, urine albumin-to-creatinine ratio

Mortality Is Increasing in Adults with Diabetes and Low eGFR in the Absence of Albuminuria
35
51
0
10
20
30
40
50
60
Mor
talit
y ra
te p
er 1
,000
per
son-
year
s
Mortality Rate in Persons with Diabetes with eGFR <60 mL/min/1.73 m2 and UACR <30 mg/g
1988-1994 2003-2006
Kramer H, et al. Diabetes Care. 2018;41:775-781.

From 1988-1994 to 2003-2006, the mortality rate in adults with diabetes and low eGFR in the absence of albuminuria has increased.
Presenter
Presentation Notes
Answer: 3/Increased

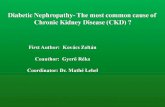
Slower Rate of Decline in eGFR with Nonalbuminuric CKD
1.00 1.00 1.00
1.72 1.82 1.88
4.52
2.38 2.37
0.76
1.42 1.44
0.00
1.00
2.00
3.00
4.00
5.00
End-Stage Kidney Disease All-Cause Mortality MACE
Haza
rd R
atio
*
Risk of ESKD, All-Cause Mortality, MACE by CKD Status
No CKD** Albuminuric non-CKD Albuminuric CKD Non-abuminuric CKD
M=10,185 patients with T2DM in the ACCORD study CKD=eGFR <60 mL/min/1.73 m2; albuminuria=UACR > 30 mg/g *Adjusted for age, sex, race/ethnicity, duration of diabetes, smoking, history of cardiovascular disease, serum lipid levels, systolic blood pressure, body mass index, glycated hemoglobin, use of RAAS inhibitor therapy **eGFR 90-120 mL/min/1.73 m2
Buyadaa O, et al. Diabetes Care. 2019;doi:10.2337/dc19-1438/-/DC1.
Presenter
Presentation Notes
OBJECTIVE We aimed to investigate the rate of progression of nonalbuminuric chronic kidney disease (CKD) to end-stage kidney disease (ESKD) or death or major cardiovascular events (MACE) compared with albuminuric and nonalbuminuric phenotypes. RESEARCH DESIGN AND METHODS We included 10,185 participants with type 2 diabetes enrolled in the Action to Control Cardiovascular Risk in Diabetes (ACCORD) study. Based on baseline albuminuria and estimated glomerular filtration rate (eGFR), participants were classified as having: no kidney disease (no CKD), albuminuria only (albuminuric non-CKD), reduced eGFR only (nonalbuminuric CKD), or both albuminuria and reduced eGFR(albuminuric CKD). The rate of eGFR decline and hazard ratios (HRs) for ESKD or death or MACE were calculated. RESULTS For individuals with no CKD and those with nonalbuminuric CKD, the rates of eGFR decline were21.31 and20.60 mL/min/year, respectively (P<0.001). In competing risks analysis (no CKD as the reference), HRs for ESKD indicated no increased risk for nonalbuminuric CKD (0.76 [95% CI 0.34, 1.70]) and greatest risk for albuminuric CKD (4.52 [2.91, 7.01]). In adjusted Cox models, HRs for death and MACE were highest for albumuniuric CKD (2.38 [1.92, 2.90] and 2.37 [1.89, 2.97], respectively) and were higher for albuminuric non-CKD (1.82 [1.59, 2.08] and 1.88 [1.63, 2.16], respectively) than for those with nonalbuminuric CKD (1.42 [1.14, 1.78] and 1.44 [1.13, 1.84], respectively). CONCLUSIONS Those with nonalbuminuric CKD showed a slower rate of decline in eGFR than did any other group; however, these individuals still carry a greater risk for death and MACE than do those with no CKD.

Risk Factors for CKD • Diabetes mellitus (uncontrolled)
• Hypertension (uncontrolled)
• Obesity • Heart failure • Age >60 years • Tobacco use • Family history • Ethnicity • Prior history of acute kidney injury
Gatwood J, et al. PLoS One. 2018;13(2):e0192712.

All-Cause Mortality Based on eGFR and UACR
0
1
2
3
4
5
6
7
8
9
15-30 30-45 45-60 60-75 75-90 90-105 >105
Rela
tive
risk
eGFR (mL/min/1.73 m2)
<10 10-29 30-299 300+
UACR (mg/g)
KDIGO. Kidney Int Suppl (2011). 2013;3(1):19-62.
UACR, urine albumin-to-creatinine ratio

Cardiovascular Mortality Based on eGFR and UACR
0
1
2
3
4
5
6
7
8
9
15-30 30-45 45-60 60-75 75-90 90-105 >105
Rela
tive
risk
eGFR (mL/min/1.73 m2)
<10 10-29 30-299 300+
UACR (mg/g)
KDIGO. Kidney Int Suppl (2011). 2013;3(1):19-62.
UACR, urine albumin-to-creatinine ratio

Cognitive Impairment in CKD Chronic Kidney
Disease
Reduced •●Processing •●Attention •●Response speed •●Short-term memory
Early stage
Deficits in ●Executive functioning ●Verbal fluency ●Logical memory ●Orientation ●Concentration
Moderate stage
Early stage + Moderate stage +
Deficits in ●Cognitive control ●Delayed/Immediate memory ●Visuospatial impairment ●Overall cognition
End stage
Brodski J, et al. J Int Neuropsychol Soc. 2019;25(1):101-114.

Case Scenario • Julio is a 63-yo male
diagnosed with T2DM x 7y • A1c had ranged from 6.8%
to 7.4% since diagnosis • Now 7.8%
• PMH: angina pectoris x 2y; stable
• Vital signs WNL • eGFR 64 mL/min/1.73 m2 • UACR 90 mg/g
• Current meds: • Metformin 1 g BID • Pioglitazone 45 mg
qAM • Atorvastatin 40 mg
qPM • Ramipril 10 mg qPM • Aspirin 81 mg qPM • NTG 0.3 mg SL prn
What change would you make to his antidiabetic therapy?

Intensive Therapy Results in Reduced Nephropathy
0
5
10
15
20
25
30
35
40
At 4 Years At 8 Years Post-Trial At 13 Years At 13 Years
Num
ber o
f Pat
ient
s
Intensive Therapy
Conventional Therapy
Diabetic Nephropathy ESRD
Requiring Dialysis
HR 0.44 95% CI: 0.25-0.77 P=0.004
P=0.04
• Patients with T2DM and persistent microalbuminuria
• 160 randomized • 130 continued
follow up
• Intensive* or conventional therapy for 7.8 y
• Follow-up for 5.5 y
Gaede P, et al. N Engl J Med. 2008;358:580-591.
*To achieve A1c <6.5%, total cholesterol <175 mg/dL, triglyceride <150 mg/dL, BP <130/80 mmHg; included renin-angiotensin-aldosterone inhibitor, low-dose aspirin

Effect of Intensive Glucose Lowering vs Standard Therapy on Renal Outcomes
Risk Ratio (intensive vs
standard therapy)
95% CI P
Microalbuminuria 0.86 0.76-0.96 0.009
Macroalbuminuria 0.74 0.65-0.85 0.001
Doubling of the SCr 1.06 0.92-1.22 0.44
ESRD 0.69 0.46-1.05 0.09
Death from renal disease 0.99 0.55-1.79 0.98
Systematic review of 7 trials involving 28,065 adults; 2-15 years of follow up Target A1C (or FPG) in the intensive group in each trial: A1c <7; 7.1; <6; ≤6.5; <6 and 1.5% less than standard; FPG <6 mg/dL; FPG <6 mg/dL Target A1C (or FPG) in the standard group in each trial: A1c 7-7.9; <9 and 1.5% higher than intensive; FPG 6.1-15 mg/dL; 6.1-15 mg/dL; not reported; local standards; avoidance of excessive hyperglycemia
Coca SG, et al. Arch Intern Med. 2012;172(10):761-769.

Screening for CKD in Diabetes Adults Children/Adolescents
Who? T1DM: Duration ≥5 years
T2DM: All
Comorbid hypertension: All with T1DM or T2DM
At puberty or age >10 years, whichever is earlier, once the child has had diabetes ≥5 years
How? Urinary albumin (eg, spot UACR)
and
eGFR
Urinary albumin (morning preferred) with spot UACR
When? At least once a year At least once a year
American Diabetes Association. Diabetes Care. 2019;42(Suppl 1):S124-S138. American Diabetes Association. Diabetes Care. 2019;42(Suppl 1):S148-S164.

This is correct regarding screening for kidney dysfunction in patients with type 2 diabetes: Measure estimated glomerular filtration rate and urine albumin-to-creatinine ratio annually.
Presenter
Presentation Notes
Answer: 3/Measure estimated glomerular filtration rate and urine albumin-to-creatinine ratio annually

Diabetic CKD vs non-Diabetic CKD Non-DKD DKD
Onset of proteinuria Rapid Gradual
Progression of CKD Rapid Gradual
Duration of diabetes <5 years >10 years
Urinalysis Active sediment (hematuria, pyuria, casts)
Bland sediment (crystals, protein, hyaline casts)
Retinopathy Absent Usually present
Republished with permission of American Society of Nephrology from Diagnosis and Management of Type 2 Diabetic Kidney Disease, Doshi SM, Friedman AN, volume 12, © 2017; permission conveyed through Copyright Clearance Center, Inc. Doshi SM, et al. Clin J Am Soc Nephrol. 2017;12:1366-1373.

Characteristics of CKD* in Adults with T2DM
45%
19%
28% 30%
0%
20%
40%
60%
80%
100%
Microalbuminuria Macroalbuminuria Retinopathy No retinopathy ormicro/macroalbuminuria
Perc
ent o
f Pat
ient
s with
CKD
*eGFR <60 mL/min/1.73 m2 13% (171/1197) of patients with T2DM had CKD
Kramer HJ, et al. JAMA. 2003;289:3273-3277.
n=171

Management Goals for DKD
• Identify patients at risk for CKD/DKD • Intervene early • Prevent further deterioration in kidney function

Treatment Principles for DKD • Control blood glucose, blood pressure, blood lipids • Tobacco cessation • Manage diet/lifestyle- reduce salt intake • Consider RAAS inhibitor (ACE-I or ARB) • Consider referral, especially for dialysis/transplantation • Monitor potentially nephrotoxic medications • Monitor medications cleared by the kidney • Implement shared decision-making • Provide patient education
American Diabetes Association. Diabetes Care. 2019;42(Suppl 1):S124-S138.

DKD Management Therapeutic Option Recommendation
Glycemic control A1c ≤7% reduces risk or slow the progression of CKD. Consider SGLT-2i or GLP-1RA shown to reduce CKD progression, CV events, or both
BP control 10-y ASCVD risk <15%: <140/90 mmHg 10-y ASCVD risk >15%: <130/80 mmHg
RAAS blockade ACE-I or ARB (nonpregnant with diabetes + HTN) -recommended if UACR 30-299 mg/24 h -strongly recommended if UACR ≥300 mg/24 h and/or
eGFR <60 mL/min/1.73 m2 -not recommended for 1° prevention if normal BP, UACR,
eGFR
Weight loss Demonstrated benefit
Close monitoring for disease progression and treatment-related complications is advised
American Diabetes Association. Diabetes Care. 2019;42(Suppl 1):S124-S138. Doshi SM, et al. Clin J Am Soc Nephrol. 2017;12:1366-1373.

Management Issues Clinicians Should Master
• Screen using eGFR and UACR • Utilize glucose-lowering medications shown to reduce
cardiovascular risk • Consider SGLT2i > GLP-1RA, DPP-4i depending on CV risk factor
• Achieve and maintain good control of blood glucose, blood pressure, blood lipids
• Consider renin-angiotensin-aldosterone inhibitor therapy • Facilitate/Support tobacco cessation

Considerations for Referral to Nephrology • Acute kidney injury or abrupt sustained fall in eGFR • eGFR <30 mL/min/1.73 m2 (G4-G5) • Consistent UACR ≥300 mg/g or AER ≥300 mg/24h • Progression of CKD • Urinary red cell casts, RBC >20 hpf sustained and not readily
explained • CKD and HTN refractory to ≥4 antihypertensive agents • Persistent abnormalities of serum K+ • Recurrent or extensive nephrolithiasis • Hereditary kidney disease • Progressive CKD with risk of kidney failure within 1 y ≥10% to 20%
KDIGO. Kidney Int Suppl (2011). 2013;3(1):19-62. AER, albumin excretion rate; hpf, high-power field; HTN, hypertension

*Referral threshold may vary †Anemia, metabolic bone disease, secondary hyperparathyroidism, resistant hypertension, electrolyte disturbances
American Diabetes Association. Diabetes Care. 2020;43(Suppl. 1):S135-S151.
Considerations for Nephrology Referral – ADA*
Uncertain etiology of kidney disease
Difficult management
issues†
eGFR <30 mL/min/1.73 m2
Rapidly progressing kidney disease

Results of CV Outcomes Trials
CV Safety
CV Benefit Renal Benefit
Dipeptidyl peptidase-4 inhibitors
Alogliptin
Linagliptin
Saxagliptin
Sitagliptin
Glucagon-like peptide-1 receptor agonists
Albiglutide*
Dulaglutide
Exenatide BID NR
Exenatide QW
Liraglutide
Lixisenatide
Semaglutide
Sodium glucose cotransporter-2 inhibitors
Canagliflozin Dapagliflozin Empagliflozin Ertugliflozin
CV safety • Non-inferiority • Not more than 30% increase in CV
risk compared to placebo as part of standard therapy
CV benefit • If non-inferiority is demonstrated,
can look for superiority • Superiority- CV risk significantly
reduced compared to placebo as part of standard therapy
*Will no longer be available as of December 2019.

Saxagliptin Improves UACR
*P value is based on a 2-tailed normal distribution approximation test for the proportion of patients who worsened. **P value is based on a χ2 test for independence. ***P value is based on a 2-tailed normal distribution approximation test for the proportion of patients who improved.
Mosenzon O, et al. Diabetes Care. 2017;40:69-76.
84% 82%
29% 23%
4% 3%
15% 17%
60%
60%
28% 23%
1% 1% 12%
17%
68% 74%
0%
20%
40%
60%
80%
100%
120%
Saxagliptin Placebo Saxagliptin Placebo Saxagliptin Placebo
<30 30-300 >300
Change in categorical UACR from baseline to end of treatment by baseline UACR category
P=0.021* P<0.001** P=0.049***
UACR <30 mg/g at baseline UACR 30-300 mg/g at baseline UACR >300 mg/g at baseline

Effect of GLP-1 Receptor Agonists on Renal Endpoints
GLP-1 Receptor Agonists- Liraglutide
Rate/100 patient-years
Hazard Ratio
(95% CI)
P
Active Placebo New onset of persistent macroalbuminuria or a doubling of SCr and eGFR ≤45 mL/min/1.73 m2, need for continuous renal-replacement therapy, or death from renal disease
1.5 1.9 0.78 (0.67-0.92)
0.003
New onset of persistent macroalbuminuria 0.9 1.21 0.74
(0.60-0.91) 0.004
Marso SP, et al. N Engl J Med. 2016;375(4):311-322. Mann JFE, et al. N Engl J Med. 2017;377(9):839-848.

Effect of GLP-1 Receptor Agonists on Renal Endpoints
GLP-1 Receptor Agonists- Semaglutide
Rate/100 patient-years
Hazard Ratio
(95% CI)
P
Active Placebo
Persistent macroalbuminuria or a doubling of SCr and eGFR ≤45 mL/min/1.73 m2, need for continuous renal-replacement therapy
1.86 3.06 0.64 (0.46-0.88)
0.005
Marso SP, et al. N Engl J Med. 2016;375(19):1834-1844.

Canagliflozin CREDENCE Trial • 4401 patients with T2DM
• Age ≥30 y • A1c 6.5% to 12.0% • eGFR 30 to <90 mL/min/1.73
m2 • UACR >300 to 5000 mg/g • Stabilized on ACE-I or ARB
therapy • 2-week, single-blind, placebo
run-in • Randomized (1:1) to
(stratified by eGFR): • Canagliflozin 100 mg or
placebo daily
Perkovic V, et al. N Engl J Med. 2019;380(24):2295-2306.
• Treatment continued until: • Trial completion • Initiation of dialysis • Kidney transplantation • Occurrence of diabetic
ketoacidosis • Pregnancy • Receipt of disallowed therapy
• Results suggested that there was no difference in amputation risk or fracture risk between canagliflozin and placebo
• Contrary to CANVAS

Effect of SGLT-2 Inhibitors on Renal Endpoints
SGLT-2 Inhibitors- Canagliflozin Rate/100 patient-years
Hazard Ratio
(95% CI)
P
Active Placebo
Dialysis, transplantation, sustained eGFR <15 mL/min/1.73 m2, doubling of SCr, or renal or CV death
4.32 6.12 0.70 (0.59-0.82)
0.00001
Doubling of SCr 2.07 3.38 0.60 (0.48-0.76)
<0.001
ESRD 2.04 2.94 0.68 (0.54-0.86)
0.002
ESRD, doubling of SCr, or renal death 2.70 4.04 0.66 (0.53-0.81)
<0.001
Dialysis, kidney transplantation, or renal death
1.36 1.86 0.72 (0.54-0.97)
–
Perkovic V, et al. N Engl J Med. 2019;380(24):2295-2306.

Canagliflozin in T2DM and Pre-existing Nephropathy: CREDENCE
N=4401 patients with T2DM, eGFR 30 to <90 mL/min/1.73 m2 and UACR >300 to 5000 mg/g Median follow-up 2.62 y NNT=22 for primary composite NNT=28 for renal-specific composite NNT=43 for ESKD
From The New England Journal of Medicine, Perkovic V, Jardine MJ, Neal B, Bompoint S, Heerspink HJL, Charytan DM, Edwards R, Agarwal R, Bakris G, Bull S, Cannon CP, Capuano G, Chu PL, de Zeeuw D, Greene T, Levin A, Pollock C, Wheeler DC, Yavin Y, Zhang H, Zinman B, Meininger G, Brenner BM, Mahaffey KW, Canagliflozin and Renal Outcomes in Type 2 Diabetes and Nephropathy, volume 380, pages 2295-2306, Copyright © 2001 Massachusetts Medical Society. Reprinted with permission from Massachusetts Medical Society. Perkovic V, et al. N Engl J Med. 2019;380(24):2295-2306.
Presenter
Presentation Notes
METHODS In this double-blind, randomized trial, we assigned patients with type 2 diabetes and albuminuric chronic kidney disease to receive canagliflozin, an oral SGLT2 inhibitor, at a dose of 100 mg daily or placebo. All the patients had an estimated glomerular filtration rate (GFR) of 30 to <90 ml per minute per 1.73 m2 of body-surface area and albuminuria (ratio of albumin [mg] to creatinine [g], >300 to 5000) and were treated with renin–angiotensin system blockade. The primary outcome was a composite of end-stage kidney disease (dialysis, transplantation, or a sustained estimated GFR of <15 ml per minute per 1.73 m2), a doubling of the serum creatinine level, or death from renal or cardiovascular causes. Prespecified secondary outcomes were tested hierarchically. RESULTS The trial was stopped early after a planned interim analysis on the recommendation of the data and safety monitoring committee. At that time, 4401 patients had undergone randomization, with a median follow-up of 2.62 years. The relative risk of the primary outcome was 30% lower in the canagliflozin group than in the placebo group, with event rates of 43.2 and 61.2 per 1000 patient-years, respectively (hazard ratio, 0.70; 95% confidence interval [CI], 0.59 to 0.82; P = 0.00001). The relative risk of the renal-specific composite of end-stage kidney disease, a doubling of the creatinine level, or death from renal causes was lower by 34% (hazard ratio, 0.66; 95% CI, 0.53 to 0.81; P<0.001), and the relative risk of end-stage kidney disease was lower by 32% (hazard ratio, 0.68; 95% CI, 0.54 to 0.86; P = 0.002). The canagliflozin group also had a lower risk of cardiovascular death, myocardial infarction, or stroke (hazard ratio, 0.80; 95% CI, 0.67 to 0.95; P = 0.01) and hospitalization for heart failure (hazard ratio, 0.61; 95% CI, 0.47 to 0.80; P<0.001). There were no significant differences in rates of amputation or fracture. CONCLUSIONS In patients with type 2 diabetes and kidney disease, the risk of kidney failure and cardiovascular events was lower in the canagliflozin group than in the placebo group at a median follow-up of 2.62 years. (Funded by Janssen Research and Development; CREDENCE ClinicalTrials.gov number, NCT02065791.)

Effect of SGLT-2 Inhibitors on Renal Endpoints
SGLT-2 Inhibitors- Dapagliflozin
Kaplan-Meier event rate (4 y)
Hazard Ratio
(95% CI)
P
Active Placebo Sustained decrease in eGFR ≥40% to <60 mL/min/1.73 m2, ESRD, or CV or renal death
4.2% 5.3% 0.76 (0.67-0.87)
<0.0001
Sustained decrease in eGFR ≥40% to <60 mL/min/1.73 m2, ESRD, or renal death
1.5% 2.6% 0.53 (0.43-0.66)
<0.0001
Sustained decrease in eGFR ≥40% to <60 mL/min/1.73 m2 1.4% 2.5% 0.54
(0.43-0.67) <0.0001
ESRD 0.1% 0.2% 0.31 (0.13-0.79)
0.013
ESRD or renal death 0.1% 0.3% 0.41 (0.20-0.82)
0.012
Mosenzon O, et al. Lancet. Diabetes Endocrinol 2019;doi:10.1016/S2213-8587(19)30180-9

SGLT-2 Inhibitors- Empagliflozin Rate/100 patient-years
Hazard Ratio
(95% CI)
P
Active Placebo
Doubling of SCr, ESRD, or renal death 0.63 1.15 0.54 <0.001
Doubling of SCr and eGFR ≤45 mL/min/1.73 m2
1.0.55 0.97 0.56 (0.39-0.79)
<0.001
Doubling of SCr and eGFR ≤45 mL/min/1.73 m2, initiation of renal-replacement therapy, or renal death
0.63 1.15 0.54 (0.40-0.75)
<0.001
Initiation of renal-replacement therapy 0.10 0.21 0.45 (0.21-0.97)
0.04
Progression to macroalbuminuria 4.18 6.49 0.62 (0.54-0.72)
<0.001
Incident or worsening nephropathy 4.78 7.60 0.61 (0.53-0.70
<0.001
Wanner C, et al. N Engl J Med. 2016;375(4):323-334.
Effect of SGLT-2 Inhibitors on Renal Endpoints

As a class of medications, dipeptidyl peptidase-4 inhibitors are supported by little, if any, evidence demonstrating a cardiovascular benefit in a patient with T2DM and chronic kidney disease.
Presenter
Presentation Notes
Answer: 1/Dipeptidyl peptidase-4 inhibitor

Updated Prescribing Information to Reflect CV Outcomes Trials MACE FDA Labeling Regarding CV Risk
GLP-1 Receptor Agonists
Albiglutide* –
Dulaglutide –
Exenatide once-weekly
Liraglutide …to reduce the risk of major adverse CV events (CV death, non-fatal myocardial infarction, or non-fatal
stroke) in adults with T2DM and established CV disease
Lixisenatide
Semaglutide –
SGLT-2 Inhibitors
Canagliflozin
…to reduce the risk of major adverse CV events in adults with T2DM and established CV disease …to reduce the risk of end-stage kidney disease (ESKD), doubling of serum creatinine, cardiovascular
(CV) death, and hospitalization for heart failure in adults with T2DM and diabetic nephropathy with albuminuria ˃ 300 mg/d
Dapagliflozin …to reduce the risk of hospitalization for heart failure in adults with T2DM and established CV disease or
multiple CV risk factors
Empagliflozin …to reduce the risk of CV death in adults with T2DM and established CV disease
Ertugliflozin
*No longer available as of December 2019
Tanzeum [package insert]. Research Triangle, NC: GlaxoSmithKline; December 2017. Trulicity [package insert]. Indianapolis, IN: Eli Lilly and Co.; September 2019. Bydureon [package insert]. Wilmington, DE: AstraZeneca Pharmaceuticals LP; February 2019. Victoza [package insert]. Plainsboro, NJ: Novo Nordisk Inc.; September 2019. Adlyxin [package insert]. Bridgewater, NJ: Sanofi-aventis U.S., LLC; January 2019. Ozempic [package insert]. Plainsboro, NJ: Novo Nordisk Inc.; November 2019. Rybelsus [package insert]. Plainsboro, NJ: Novo Nordisk Inc.; September 2019. Invokana [package insert]. Titusville, NJ: Janssen Pharmaceuticals, Inc.; December 2019. Farxiga [package insert]. Wilmington, DE: AstraZeneca Pharmaceuticals LP; October 2019. Jardiance [package insert]. Ridgefield, CT: Boehringer Ingelheim Pharmaceuticals, Inc.; January 2019. Steglatro [package insert]. Whitehouse Station, NJ: Merck Sharp

American Diabetes Association. Diabetes Care. 2020;43(Suppl 1):S98-S110. American Diabetes Association. Standards of medical care in diabetes-2020, American Diabetes Association, 2020. Copyright and all rights reserved. Material from this publication has been used with the permission of American Diabetes Association.
New Paradigm in T2DM Treatment

Patients with T2DM and Established ASCVD or CKD
American Diabetes Association. Diabetes Care. 2020;43(Suppl 1):S98-S110. American Diabetes Association. Standards of medical care in diabetes-2020, American Diabetes Association, 2020. Copyright and all rights reserved. Material from this publication has been used with the permission of American Diabetes Association.

Implications for Patient Care • CKD is common in patients with T2DM causing
significant increases in: • CV mortality • All-cause mortality
• Annual screening for CKD in patients with T2DM is critical
• Measure both eGFR and UACR
• Controlling blood glucose, blood pressure, and blood lipids is critical
• Recent clinical trial evidence demonstrates reduced renal events with several SGLT-2 inhibitors and GLP-1 receptor agonists
• Presents an additional opportunity to individualize therapy • Patient affordability may be a limiting factor

The Diabetic Kidney… What to do?
Thank you!