THE DIABETIC EYE - Postgraduate Medical JournalTHE DIABETIC EYE D. W. HILL, F.R.C.S. Institute of...
11
POSTGRAD. MED. J. (1964), 40, 696 THE DIABETIC EYE D. W. HILL, F.R.C.S. Institute of Ophthalmology, London, W.C.I. THE INTRODUCTION of insulin has transformed the management of diabetes mellitus bringing a greatly increased expectation of life with the result that a number of complications, some taking many years to develop, have become manitest. At the present time the impact of this revolution is being felt as a large popula- tion of patients with long established diabetes collects. Blindness due to diabetes has increased and diabetic retinopathy accounted for 11.3% of those under 60 years old regis- tered blind in Great Britain in 1962 (Mooney, 1963). It seems appropriate in this article to deal at length with diabetic retinopathy and review the other ocular manifestations of diabetes briefly. For the sake of orientation the ocular changes in diabetes are listed in Table 1, while Table 2 indicates how various events may affect the eyes. RETINOPATHY Clinical Manifestations Diabetic retinopathy is a disease of con- siderable variation both in severity, clinical appearance, and progress. It is seldom seen in the young diabetic of less than five years' duration (Collyer and Hazlett, 1961), but is often present at diagnosis in the maturity onset diabetic and may be the presenting lesion. The earliest clinical manifestations comprise a cen- tral punctate retinopathy (Ballantyne, 1947) with microaneurisms, dot haemorrhages and small white spots grouped around the posterior pole of the eye. After a time larger haemorrha- ges develop which have been likened to blots, round in shape with crenated poorly defined margins; set deeply in the retina in the inner molecular and nuclear layers, they contrast with the more superficial flame shaped haemorrhages of hypertensive retinopathy which are moulded by the nerve fibre layer. Accompanying these hemorrhages are small patches of waxy exudate. The retinopathy advances and spreads to involve larger areas of the retina but seldom affects the periphery of the fundus. Larger and more irregular hemorrhages are seen which break through the layers of the retina to lie on its surface, TABLE 1 OCULAR MANIFESTATIONS IN DIABETES External Lid and conjunctival infections. Ophthalmoplegia Anterior segment Pigmentary migration Pupillary changes poor dilatation Argyll Robertson pupil Rubeosis iridis haemorrhagic glaucoma Cataract transient changes diabetic (juvenile) senile Hypotension, in diabetic coma Posterior segment Vitreous hemorrhage Retinopathy Lipwemia retinalis Optic neuritis Subjective Transient changes in refraction phenomena Weakness of accommodation Aura of hypoglycaemia TABLE 2 OCULAR MANIFESTATIONS ON CERTAIN OCCASIONS Presenting signs Retinopathy and symptoms Cataract Transient refractive changes Ophthalmoplegia Optic neuritis Diabetic coma Ocular hypotension Transient lens opacities Lipaemia retinalis Hypoglycaemia Subjective visual phenomena (early) preretinal haemorrhages, or in a pocket between the retina and vitreous, subhyaloid haemorrhages; the latter have a semi-circular outline with a fluid level above; the haemorrhages absorb slowly over a period of weeks leaving few residual signs. Some of the larger hemorrhages may break through into the vitreous causing opacities and reducing vision. by copyright. on March 2, 2020 by guest. Protected http://pmj.bmj.com/ Postgrad Med J: first published as 10.1136/pgmj.40.470.696 on 1 December 1964. Downloaded from
Transcript of THE DIABETIC EYE - Postgraduate Medical JournalTHE DIABETIC EYE D. W. HILL, F.R.C.S. Institute of...

POSTGRAD. MED. J. (1964), 40, 696
THE DIABETIC EYE
D. W. HILL, F.R.C.S.Institute of Ophthalmology, London, W.C.I.
THE INTRODUCTION of insulin has transformedthe management of diabetes mellitus bringing agreatly increased expectation of life with theresult that a number of complications, sometaking many years to develop, have becomemanitest. At the present time the impact ofthis revolution is being felt as a large popula-tion of patients with long established diabetescollects. Blindness due to diabetes hasincreased and diabetic retinopathy accountedfor 11.3% of those under 60 years old regis-tered blind in Great Britain in 1962 (Mooney,1963). It seems appropriate in this article todeal at length with diabetic retinopathy andreview the other ocular manifestations ofdiabetes briefly. For the sake of orientationthe ocular changes in diabetes are listed inTable 1, while Table 2 indicates how variousevents may affect the eyes.
RETINOPATHYClinical Manifestations
Diabetic retinopathy is a disease of con-siderable variation both in severity, clinicalappearance, and progress. It is seldom seen inthe young diabetic of less than five years'duration (Collyer and Hazlett, 1961), but isoften present at diagnosis in the maturity onsetdiabetic and may be the presenting lesion. Theearliest clinical manifestations comprise a cen-tral punctate retinopathy (Ballantyne, 1947)with microaneurisms, dot haemorrhages andsmall white spots grouped around the posteriorpole of the eye. After a time larger haemorrha-ges develop which have been likened to blots,round in shape with crenated poorly definedmargins; set deeply in the retina in the innermolecular and nuclear layers, they contrastwith the more superficial flame shapedhaemorrhages of hypertensive retinopathywhich are moulded by the nerve fibre layer.Accompanying these hemorrhages are smallpatches of waxy exudate. The retinopathyadvances and spreads to involve larger areasof the retina but seldom affects the peripheryof the fundus. Larger and more irregularhemorrhages are seen which break throughthe layers of the retina to lie on its surface,
TABLE 1OCULAR MANIFESTATIONS IN DIABETES
External Lid and conjunctival infections.Ophthalmoplegia
Anterior segment Pigmentary migrationPupillary changespoor dilatationArgyll Robertson pupil
Rubeosis iridishaemorrhagic glaucoma
Cataracttransient changesdiabetic (juvenile)senile
Hypotension, in diabetic coma
Posterior segment Vitreous hemorrhageRetinopathyLipwemia retinalisOptic neuritis
Subjective Transient changes in refractionphenomena Weakness of accommodation
Aura of hypoglycaemia
TABLE 2OCULAR MANIFESTATIONS ON CERTAIN
OCCASIONSPresenting signs Retinopathyand symptoms Cataract
Transient refractive changesOphthalmoplegiaOptic neuritis
Diabetic coma Ocular hypotensionTransient lens opacitiesLipaemia retinalis
Hypoglycaemia Subjective visual phenomena(early)
preretinal haemorrhages, or in a pocketbetween the retina and vitreous, subhyaloidhaemorrhages; the latter have a semi-circularoutline with a fluid level above; thehaemorrhages absorb slowly over a period ofweeks leaving few residual signs. Some of thelarger hemorrhages may break through intothe vitreous causing opacities and reducingvision.
by copyright. on M
arch 2, 2020 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.40.470.696 on 1 D
ecember 1964. D
ownloaded from

December, 1964 HILL: The Diabetic Eye 697
The extent to which venous changes occur indiabetic retinopathy varies considerably; a slightgeneral dilatation is said to be the earliest signof retinopathy but is difficult to detect. Moredefinite are dilated segments, and these may befollowed by the appearance of irregular beadingof the veins, tortuosity and bizarre loops lyingon the retina and projecting from its surface.The term proliferative retinopathy implies
the development of new vessels, a serious prog-nostic sign, for the majority of cases deteriorateand many become blind. Beetham (1963) foundthat five years elapsed on average between theonset and final stages of proliferative retino-pathy. The stage at which proliferation com-mences varies from case to case, but there isalways some venous abnormality present. Newvessels grow in the plane of the retinal vesselsand spread forwards into the vitreous to formdelicate fronds, rete mirabile, commonlyarising from the optic disc but also seenelsewhere taking origin from the retinal veins,Their walls are fragile so that bleeding fre-quently occurs into the retina and vitreous. Ata later stage the fronds thicken with connectivetissue to form retinitis proliferans, and in severecases sheets of preretinal connective tissue form.Retinitis proliferans may also arise from thedirect organisation of vitreous hemorrhage(Ballantvne, 1947). Contraction of the retinitisoroliferans and preretinal connective tissuesleads to traction on the retina, shown by stresslines on the posterior vitreous face, and laterretinal detachment.Permanent loss of central vision in diabetic
retinopathv is due to involvement of the maculaby haemorrhage, hard exudate or retinal detach-ment. Occasionally a frond of retinitis prolife-rans may spread in front of the maculaobscuring vision. Complete blindness occursfrom massive vitreous haemorrhage, retinaldetachment or intercurrent haemorrhagicglaucoma.
It is difficult to summarise succinctly thenatural history of diabetic retinopathy but threeelements can be recognised, haemorrhagic,venous and proliferative. Onset is usuallymarked by slight haemorrhagic changes whichprogress and recruit hard exudates. venouschanges run concurrently in varving decree. ata later stage proliferative changes may develop.An intricate clinical classification DroDosed byScott (1951) expresses this variability. Larsen(1960b) makes a distinction between the retino-nathv in middle-aged, older and iuvenile dia-betics. The middle-aged diabetic, 20-40 yearsold at the onset of diabetes, shows the evolu-
tion just described, passing from a punctateretinopathy to increasing haemorrhage and con-fluent exudates, and in a small proportion ofcases to proliferative retinopathy. The olderdiabetic aged over 50 years at onset has amarked tendency to develop exudative changesat the macula with the formation of confluentplaques; later, glistening crystals form and thewhole plaque gradually disperses to leave ascarred area; central vision fails as the plaquedevelops. Juvenile diabetics with onset ofdisease in the first 20 years of life show severaldiffering patterns of retinopathy. It maydevelop along the lines of the middle-ageddiabetic, or there may be an early onset ofproliferative retinopathy initiated by vitreousdetachment with preretinal and subhyaloidhaemorrhages; other cases progress very slowlybut develop severe arteriosclerosis over a periodof 20-30 years.
Hypertension frequently complicates diabetes,and the retinopathy of hypertension may com-Plicate the appearance of diabetic retinopathy,but there is no doubt that diabetic retinopathyis a separate entity not dependent on hyper-tension for its existence (Duke Elder, 1940a).Soft exudates are seen from time to time inthe course of diabetic retinopathy but are lessconspicuous than those of hypertensive retino-pathy.Development of a fine stippled pigmentation
of the macula (Jensen and Lundbaek, 1955) isoccasionally encountered in iuvenile diabetics,the significance of the condition being that it isharmless and not associated with any loss ofvision.The differentiation of microaneurisms and
punctate haemorrhages can be difficult. If thelesion has a well defined spherical outline with alight reflex from the summit this is indicativeof an aneurism, but such an appearance is notalways seen. In other instances the durationof the lesion may help as haemorrhages usuallyclear within a few weeks whilst aneurisms per-sist for long periods.Fluorescence retinal photography (Dollery,
Hodge and Engel, 1962) is a form of angio-graphy in which the contrast medium,fluorescein, is injected intravenously and photo-graphed as it passes through the retina. Studiesof diabetic retinopathy (Scott, Dollery, Hill,Hodge and Fraser, 1964) reveal many moremicroaneurisms and new vessels than seemevident clinically (Figs. 1 and 2). Aneurismsare usually grouped and in severe cases appearlike bunches of grapes clustered round avenule. After the passage of fluorescein some
by copyright. on M
arch 2, 2020 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.40.470.696 on 1 D
ecember 1964. D
ownloaded from

698 POSTGRADUATE MEDICAL JOURNAL December, 1964
............··:.
·:::: i~i~l............ .......~i~f~
.......................... ·i:: .··. ··· ·.·...
..........:
:: j::j:::`.: w
...·.:~ .....: ,:: . ::::: ffilliii
i~~pl~ii~~i:~i:":: :........:::, :..::....:w:::·;...........:i:~: ·.·1·
...........''··:··'
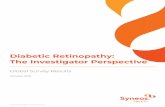
FIG. 1.-Reproduction of a colour transparency ofthe fundus oculi showing the right superiortemporal field, from a patient with diabeticretinopathy. There are numerous hemorrhagesand some small exudates. This figure should becarefully compared with Figure 2.
aneurisms empty promptly, others more slowly,while others remain fluorescent for as long asten minutes with leakage of the dye into thesurrounding tissues. Similar leakage occursfrom some new vessels, and to a marked extentfrom fronds of retinitis proliferans, whence dyepasses into the vitreous. It is conjectured thatthis abnormal permeability may be associatedwith the haze in the vitreous found in activeproliferative retinopathy.IncidenceThe incidence of diabetic retinopathy rises
with the duration of diabetes. In a group ofdiabetics of all ages Larsen ,(1960a) found it torise slowly during the first five years after thedisease was diagnosed, then sharply; by tenyears there was an equal incidence in nearly allage groups apart from patients under the ageof 16 years in whom the complication was rare.Figures for the incidence of retinopathy varywidely depending in part on the criteria adoptedfor diagnosis; Larsen (1960a) notes an incidencereported in the literature of 30-80% after 15years and 60-100% after 20 years.
It is difficult to ascertain how control of thediabetes is related to retinopathy. Keiding,Root and Marble (1952) found a reduced Inci-dence in patients with good clinical control ascompared to those with bad control, in groups
.iP:'i8is·:···.....·:·; ··· -·:···:····
.·.; :::..::::i'''"l:; I:I·''::': ::::. ·:.'·:·:· :··: :·..·. .::ii,:::::i:·· : :i:i::'.:.··'·'-'·'· ·'·'·;`'·`··-·····-·...i.i(iZlili.i'aiii'::::i''"::.. ··:·· ·:::":· ..'.l.'ai.;i;. :::.·ii:i.::::. ::i.iiliiiiiiiii:iiiin::. ..:.i.::::.·.Li..aiiWiii:.iii:ia: I:·::::·::::.::I:i-::·'''''. ''i:.41.1111. :1I:i:i:i.:·:::-·Lisiliiki:iiai!iii.:r::i:ii: ··!:·-·::·: ···'""'''''''''; ::i:i':::ifil:I:1···:·· :.i::: ::::·;-.·:···:··;::::::::::+::.pri:#::::::: '.::,·:I:: ·:''·' ::.:..:::...:..:··I:I-' ::C:i:T:iq'.'i.iiii''iii.ii".iiiCiii."::ii;i:··: ·.:.-.·.· ·':'·.i::iii.iQ;ai.·.i.,,;.:.a:ii-.::I...:·.·:;::-:.' ··· ··· ··· '·' ':I:::-:::: :i:i:;..:...:::::. ···, ,, ·:·:\I: :I, .,F:li
,:,::::i:::.::, 'I:: :·'::::::':i:: ·:l..ii·'': .·. ::::.II:'::.: ··:: '''' '''::::':'i·:::::::I:: ,,..:iii:':iii,''ii'I.:··j.:.:.:-·:: :::::::*·l.p:-.'i::'iIil ::::: -:::;ii:::l;"·;:i·::-, ::la..F .V. . ...I:··:::-·::-:·· ·:iaiqn.ni.9.i. 'iiEii.i.i.iii.:: ia.::....:I:i;'c.i:.:.::-:-:a:.:,:.::-·:· ::::I··:·: ·:·.·.·:::::::I-j.:':-i:i41::1 :::.:.:.::j::·''·::I· ··· :':''·'·:·:.i.·:·::· ····::' ':···" .-i::·:·:·:;.L:ni:19I:r ·::·:i::-:I·:::::lsl::.::I:i:;::I:.:::-:-:::' $%ri:·:::·iii.ii.:''i.lilb .:-::iici5ii:S'. :i;:·· :II::"i.w:-::::;,:. :.:'..ii.ii.lliii.ii 'I:·.·.··' ""' ::: ·:
·r.·:·:·:·:·:·:·;··r.,;-Billllliiii:i:i::,;. ;. " '::":'i:::· ;i.. j:::::::·'·li: 6·1·j::·rBi.i.i:: I·:·:::::'::i:i::i8Z:·:· ·p·:.Il::',':::- ::::r::::a::::: ·:· ··::-:JG..·::::lii:';:li;;·!:l.......r'k;l::^.iii:''::"::: ::;.:.:: '::y:·:·:1!1,'·:;:;·::::i::·I::::::·::-··::::-::::2:ri.\;-:\i:t:: 'I: :::::r:.j::.··::i·:iE':'.'.:i.;.-;.i.:j:-.i.:j..: ,ii::`:::':::::;.....iiiBII\-';Y:di:·i:I::j..li-:'i:I:.I':t:ij.::::·.1.:"·j`:;::::::;·:::::·.,:·:·:·::::;j:-:.::';:.::·.:::i:':;':::... b.-i:: :::···.'·.'i-::·:::_I:I·:jl:W:i:.:I:: ::':..':::::.:::j li,:iilij.ii.ii.i..iii.i.:.il.l:·A:.43:··:·:.:i..:.a.:n·· ii:.,::I:.: ::i::iY:..:..illsl:::·-.:· :'::·::::::II:::X:ilj.i:i::-.ilili!P:::::`::I .i.a.n i.ai:I::Iiiliiiiilili:iiI:iii:':ili'llll:.:i ':.9.:.::'' :::·::: .;_,, ,,i::8·:··i-::uc.n.bj..it.:il..i·:j''iiiii.;.i;·.cf·.l:.::i;i:i:,i i:···:.::·:·:::::::::·. ..:
;i.:.c.::-_::i-·:·r: ···:·: r:·; :,::: :.i'::;:::::.:::I ·::;:'::':·:·:: ·:·i:.i:::si:i·i·i::·::::::-.'::i:i:i:·:i:::-:::· ·'·'·'·:':' :·- Qii.:"iii.i8ilia,;,:,:,:::: ::IP':::. ..:·i:·::.i::::··::::··::::...··-············
:·:·rr;-;::::·;·· -;;-- ·"':--;.:::.9 :i ··:·.-::-·-····:·· ··:·:;···:-:·:·: :· :::::·i::::-i:.:·:·:· .·::: ::.·.u·::::a:::i·:;i:·:·:::; :::·-:::"::-:·:·····:l-::i I.C ':::::'j. ····-:·:·; t.i:.i
iki....:.·..i8ii!' ··:·' if it;c:· ··· .:::·:·· ··-·:·.:----:-:·-··· ···-
·':':-:':':''''':i.- -·:·"r':· ".·:..:'.j::j::::':::::"·'-::::i::; :i3:':: :I.::.ip..iP :::r-.·:;·::.:c:::a·::-j:::::j,:·:wl
;;·-·;.::: :. ::::):.:.:·::::::';:::"'::Eij.::liZ ::-i::::-.:::::::S::':
FIG. 2.--Early venous phase flourescein photographof the same area as Figure 1. The fluoresceinappears white filling the whole of the arteriolesbut only the edges of the veins, because theblood from the periphery of the retina is not yetfluorescent. Numerous micrpaneurisms can beseen appearing as small white dots, many of themare invisible in Figure 1. The haemorrhagesappear as dark patches obscuring the back-ground fluorescence.
of differing duration of disease. A prospectivesurvey of degenerative disease in growth onsetdiabetics entering the second decade of diag-nosed diabetes was undertaken by Hardin,Jackson, Johnston and Kelly (1956) who cal-culated an index of control, taking into accountboth the strictness of control and the durationof treatment. When this index was plottedagainst the severity of retinopathy there was aclose correlation for the whole group of patientswith diabetes of 10-29 years' duration. Plot-ting merely duration of disease againstseverity of retinopathy produced a moderatecorrelation for cases of less than 15 years dura-tion, an expression of the latent period requiredfor the retinopathy to become manifest. How-ever after that period the duration of diseasewas of little importance in determining theseverity of retinopathy. Control was related toseverity of retinopathy over the whole periodof the investigation, in the sense that bad con-trol was associated with severe retinopathy; thelonger the duration of bad control the worsethe retinopathy was likely to be. These con-clusions are supported by Collyer and Hazlett(1961) who found in a survey of 100 growthonset diabetics that all cases of severe retino-pathy were poorly controlled.
by copyright. on M
arch 2, 2020 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.40.470.696 on 1 D
ecember 1964. D
ownloaded from

December, 1964 HILL: The Diabetic Eye 699
:. Ri ::·.·s'::: ;'·1:'·:: sgii.:::ip r:e:61
.i.ii.i'i..F..i..:I:ii.r:i:li.ij.lji.iiiiril::: i::·:
I:; :·: :.:::::.i·.6 ''': ···· t:::'ii,.ia :::: :: :·:P.:·i.:::::::..:, :: :::il.::::::·:i:: :.::: :· .·:::.:IB:·:- " ( ·:6: -;..W :::···: :·: :' :::i·: ·:· ·- ;: :,:,:·:· .·.·:;::: .....·::'::I::.'iiB: ·::::-. ::. :.::::::: i:i.(:i:::'ii:::..:··r '·:: .:::·:·:··:i·:::: :·· ::i::
·;:::··.··: :il:::.::: ':· ·:: :·:·:::::':::::':.::':: :·:·::::.:..·...·::;.ii· ·:· :·:·.:::,jii:i.:.i::· '. ''.:. :::::i:.:i:i :.i: :::.:·::::: :. ...:...·::· ·:··:· ::: ''' :::::'::::' :::::::::::: h.::: ::.':···:::r.,::··· "·iii:l:·:··· ·:;:::. ::::::·.:. ::::·::·::::
.iil :':: :·:·:···:·'8j·:''·: ·:::::I::·:::·:'.: r::.::.··:BS
·:· .·:·:·ii::::.-.::·::i.:'.' ::.·:::::.: ::·::.'::: ·.:.·.:· ·::· ·:::''::'':''':':: ·:··:···::::D
.::: x ·P:':'''::·· i· ..:"..·:· ·.:.·:·:·:i:. :· ": ·:·.::ig:. ···:::::·-::· '·::'·'····:··. ·:···:· ··:· ·:· ·:·.::··:· ·:· ·:·: ·:· :·:·iiii::·ilai:···. c:i: ...:. ·:· ;·
::: ':· ...: :i.i:i::·" :·..·:· i.;.L. "·.*L...."*;rrC.Cjki.·. %.:.:.j*.*.;$.·b.!.···::'ii:i::i·.I '::::::···:::':I::'j: ·a ·· ·::.:·· ···:·:·: ·:·:
FIG. 3.-An injected specimen of retina showing anarea of capillary closure in the centre of thephotograph. A few dilated tortuous capillariesremain open; microaneurisms are seen on thesevessels and those bordering the area of closure.Photograph supplied by Professor N. Ashton.
PathologyInvestigation of the pathology of diabetic
retinopathy has been assisted by the develop-ment of new methods of histological examina-tion. During the past 20 years a considerableamount of energy has been devoted to theproblem. Ballantyne (1947) studying flat pre-parations of the whole retina rediscovered themicroaneurisms. Ashton (1953) using injectiontechniques drew attention to the areas ofcapillary closure. More recently Kuwabaraand Cogan (1960) using controlled tryptic diges-tion were able to isolate the blood vessels fromthe retinal tissue and study their histology ingreater detail.The use of injected preparations (Fig. 3) has
revealed scattered areas of capillary closurerelated to the arterioles, but not localized to anyone part of the retina; in these areas a few largedilated capillaries persist. Microaneurisms arefound on these capillaries and also borderingthe area of closure. Around the edge newloops of dilated capillaries form, derived fromthe venous capillaries. (Ashton, 1963).
Digest preparations allow study of theendothelial cells. In normal capillaries they aredistributed regularly as a lining to the basementmembrane, which splits to enclose the muralcells or pericytes scattered along the capillary.Ashton (1963) has studied the behaviour of theendothelial cells and finds that in areas ofcapillary closure the empty vessels are reducedto thin tubes of basement membrane, the
endothelial cells having migrated to the nearbyopen capillaries. Endothelial cells proliferatein response to hypoxia, a change seen in thenew capillary loops bordering areas of closureand in microaneurisms.
Microaneurisms are not specific lesions ofdiabetic retinopathy for they are also encoun-tered in a number of other conditions in whichretinal hypoxia occurs, for example venousthrombosis, macroglobulinamia and Eales'disease. They appear confined to the retina, forthough superficially similar lesions are seen inthe kidney in intercapillary glomerulosclerosis,Volk (1956) considers them to differ fromretinal microaneurisms. Controversy existsabout the origin of microaneurisms; mostappear to come from outpouchings on the capil-lary wall though some at least start from dilatedcapillary loops (Ashton, 1951) whose contiguouswalls adhere and break down. They passthrough a cycle of changes (Cogan, Toussaintand Kuwabara, 1961), endothelial proliferation,deposit of PAS staining material on the base-ment membrane, lipoid infiltration and disinte-gration.So far attention has been focussed on the
vascular changes occurring in diabetic retino-,pathy, but Wolter (1961) and Bloodworth (1962)both stress the extent of neuronal degeneration,and Wolter claims to have demonstrated aproliferation and degeneration of antidromalnerves. Ashton (1963) has shown that areas ofneuronal degeneration are closely related toareas of capillary closure.The basic lesion in diabetic retinopathy
would appear to be capillary closure. Mostauthorities would agree that new vessel for-mation is a secondary process induced byprolonged tissue anoxia; but the mechanism ofcapillary closure is still obscure. Earlierthoughts that this might have been due to tissueswelling resulting from a primary metabolicinjury (Ashton, 1959) have not been supported(Ashton, 1963). A gradual hyaline thickeningof the basement membrane of arterioles through-out the Ibody in diabetes affects the retinalvessels and may Ibe responsible for producinga slow ischaemia with lowered capillary pressureand closure (Ashton, 1963). Cogan and others(1961) have noted that the mural cells in thewalls of the retinal capillaries are frequentlydegenerate in diabetic retinopathy; they pos-tulate a specific lesion and consider thatmicroaneurisms arise from these sites throughweakening of the basement membrane. Lossof pericytes may also result in failure to controlcapillary tone with redistribution of the retinal
by copyright. on M
arch 2, 2020 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.40.470.696 on 1 D
ecember 1964. D
ownloaded from

700 POSTGRADUATE MEDICAL JOURNAL December, 1964
circulation and closure of some capillaries.Increased permeability of the capillaries due toendothelial injury (Ballantyne, 1945), andembarrassment of the venous outflow are otherpossible factors in the development of retino-pathy. Finally the question remains whetherthe vascular changes, by no means specific,are primary or secondary to the neuronal lesionsalready mentioned (Toussaint, Cogan andKuwabara, 1962).From a discussion of the pathogenesis of
diabetic retinopathy arises the further problemof the factors in the diabetic state which deter-mine the onset of the retinopathy. Anassociation between adrenocortical hyper-function and diabetic retinopathy has beensuggested Iby Becker, Maengwyn Davies, Rosen,Friedenwald and Winter (1954) based onclinical, biochemical and pathological evidence.During pregnancy hormonal changes occurwhich include adrenocortical hyperactivity; theonset of diabetic retinopathy and its resolutionafter delivery have been observed, also theworsening of established retinopathy during thelast trimester followed by improvement afterpregnancy. The development of retinal micro-aneurisms has 'been noted as a result ofprolonged administration of intravenous ACTHto patients without diabetes. The associationof deterioration of retinopathy with poor controlof the diabetes can be interpreted in terms ofthe increase of adrenocortical activity whichaccompanies infection and ketosis. There isno direct test for adrenocortical hyperfunction,but the Thorn test (depression of circulatingeosinophils in response to a test dose of ACTH)is negative in hypofunction. A negative testwas obtained in 50% of a group of diabeticswithout retinopathy, but the response couldbe obtained with a test dose of cortisone sug-gesting that adrenocortical hypofunction wasresponsible for the failure. In contrast allpatients with retinopathy gave a positive res-ponse. Indirect evidence of adrenal hyper-function in diabetics with retinopathy, andhypofunction in those without retinopathy,comes from a determination of the free oxy-steroid excretion which is raised in cases ofretinopathy and lowered in those withoutretinopathy. The excretion of 17-hydroxy-corticosteroids is similarly altered but thechanges are less marked (Maengwyn Davies,Lerman, Pogell, Stone, and Friedenwald 1956).The therapeutic response to pituitary ablation,adrenalectomy and testosterone will be dis-cussed later; all of these measures result in areduction of adrenocortical function.
The renal lesions of the Kimmelsteil Wilson(KW) kidney, are found in many cases of severeretinopathy; Ashton (1958) found them presentin all cases examined by autopsy. Becker andothers (1954) demonstrated evidence of adreno-cortical hyperfunction in cases of KW kidneyat autopsy. There was an increase in weightof the adrenals by 24%, lipoid vacuolisationin the zona fasciculata in 86% of cases and agreater incidence of adrenal adenomas.Experimental evidence from rabbits shows thatadministration of anterior pituitary extractsand cortisone in healthy and alloxan diabeticanimals results in the production of renal lesionsconsidered similar to those of KW kidney.Becker (1952) reported a rise from 30% to70/, in the incidence of these lesions aftercortisone injection when the animals werealloxan diabetic. Rosen (1956) reviewing theevidence for adrenal hyperfunction in diabeticretinopathy concluded that the failure to pro-duce capillary microaneurisms consistently inexperimental animals, and their infrequency inman after prolonged steroid therapy, constituteda weakness in the hypothesis.
Poulsen and Larsen (1961) have investigatedthe changes of intraocular pressure whichaccompany the fluctuation of blood sugar levels.Both hyperglycemia and hypoglycaemia mayproduce a fall in the ocular tension. Hyper-glycemia due to insulin lack is a more potentfactor than alimentary hyperglycaemia and mayproduce a 10% fall. Acute hypoglycaemia mayresult in a fall of as much as 20%. Thevariations are more marked in severe diabetics.It is argued that these changes put a mechanicalstress on the walls of the retinal blood vesselsdepriving them of their normal support. Mooney(1963) reports two clinical observations in sup-port of this idea. In a patient with mild diabeticretinopathy the second eye which was blindfrom glaucoma was free of retinopathy. Anotherpatient with severe retinopathy was observed tohave low ocular tension in association withvitreous haemorrhage, which rose to normal asthe haemorrhage resolved.A rise in the level of serum lipids is found
in many diabetics. It increases in patients withretinopathy and is even higher in those withnephropathy, but as it occurs in other diseasesunaccompanied by retinopathy it must be con-sidered a non-specific change (Larsen, 1960).The same can be said of the protein-boundcarbohydrate and hexosamine fractions whichare increased in diabetic retinopathy. Ashton(1959) has drawn attention to the fact that noneof these biochemical changes can be invoked
by copyright. on M
arch 2, 2020 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.40.470.696 on 1 D
ecember 1964. D
ownloaded from

December, 1964 HILL: The Diabetic Eye 701
to explain the localisation of the lesions to theretina.
TreatmentThe legion of treatments advocated at various
times for this complication is a sure indicationof the unsatisfactory results obtained, so muchso that many consider the condition untreatable.A fundamental difficulty lies in deciding thecriteria on which treatment may be assessed.Some of the manifestations of retinopathy, forexample retinitis proliferans, are consequent onextensive injury to the tissues, whilst others,haemorrhages and microaneurisms, are muchcloser to the primary lesion of diabetic retino-pathy. Because the natural evolution of theretinopathy is slow it is important to look forimprovement in those clinical manifestationswhich are close to the primary lesion, as theothers may continue to progress under themomentum of the injury already inflicted.This applies particularly to retinitis proliferanswhich is a connective tissue reaction, and pos-sibly also to exudates which are never seen inthe absence of established retinopathy.A comparison of the results of different
workers is difficult because of the lack ofuniformity in their criteria of assessment.Repeated estimation of the visual acuity whichhas the advantage of a close relationship tothe amount of useful vision experienced bythe patient, is unfortunately a poor guide tothe progress of the retinopathy; in cases wherevitreous hemorrhage is occurring wide fluc-tuations are encountered in the visual acuity,irrespective of the trend of the disease. Changesin refraction, cataract, and intercurrent oculardisease can also upset the visual acuity. Joplin,Hill, Scott and Fraser (1962) have studied serialretinal photographs of selected areas of theretina, assessing them in terms of five com-ponents, haemorrhages and microaneurisms,venous dilatation, new vessel formation, retinitisproliferans and exudates. Using a four-pointscale of severity they were able to demonstratethe trend of retinopathy in treated and un-treated cases. It is not possible to study thewhole fundus by photography so Contreras,Field, Hall and Sweet (1962) preferred todocument their cases by repeated fundus draw-ings made with the aid of the binocular indirectophthalmoscope, affording a diagram of thewhole fundus and vitreous but losing theaccurate detail of the retinal photograph.The natural history of diabetic retinopathy
is very variable both in the rate of deteriorationand the incidence of periods of inactivity,
sometimes of arrest. Beetham (1963) hasobserved spontaneous arrest for periods of 1-9years in 10% of a group of patients withproliferative retinopathy who received nospecific treatment for the complication. Theseobservations cast grave doubt on the significanceof treatment in isolated cases of improvement,and indicate the need for some form of controlin any therapeutic trial relating to diabeticretinopathy.Three lines of treatment will be discussed,
pituitary ablation, anabolic steroids, and lowfat diets; in addition light coagulation will bementioned. Other methods of treatment haveincluded the exhibition of vitamin B12, rutin,lipotropic substances, and cestrogens but withlittle success. The impetus for pituitary ablationcame from the observation by Poulsen (1953)of remission and eventual clearing of retino-pathy in a woman who suffered from post-partum necrosis of the pituitary, with clinicalSimmonds disease and increased sensitivity toinsulin. Ablation can be produced by hypophy-sectomy (Luft, Olivecrona, Ikkos, Kornerup,and Ljunggren, 1955; Kinsell, 1957; Schimek,1956; Javid, Gordon and Erickson, 1958;Vannas, Hernberg and Bjorkesten, 1959) per-formed transcranially or trans-sphenoidally;alternatively the pituitary stalk may be dividedand a diaphragm inserted to prevent healingof the portal venous system (Contreras andothers, 1962). Irradiation with a neutron beam(Sangalli, 1961), and implantation of radio-active Yttrium-90 seeds through a cannulapassed across the top of the nasal cavity underradiographic control (Fraser and Joplin, 1961)are alternative methods. Intracranial surgeryin diabetic patients is fraught with more riskthan usual from thrombosis and infarction ofthe retracted lobes of the brain; for that reasonthe nasal approach is sometimes preferred.Surgical hypophysectomies produce completeablation of immediate onset in the majority ofpatients. After an Yttrium implant the first signof decreased activity is a sharp drop in theinsulin requirement, usually manifest on thefifth day (Joplin and others, 1962). Irradiationfrom the cyclotron takes longer to act and isnot free from risk of damage to surroundingstructures. Stalk section like Yttrium implantproduces a proportion of incomplete ablations,but present evidence though not conclusivesuggests that there may be little difference inthe effect on retinopathy of partial or completeablation. Improvement in nearly all aspectsof retinopathy was reported by Contreras andothers (1962), but Joplin and others (1962)
by copyright. on M
arch 2, 2020 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.40.470.696 on 1 D
ecember 1964. D
ownloaded from

702 POSTGRADUATE MEDICAL JOURNAL December, 1964
found only dilated veins, hemorrhages and newvessels favourably influenced. This series ofpatients has been followed and additionalpatients recruited; in 1963 Hill reported thatabout one-third of them showed improvementin respect of dilated veins, hemorrhages andnew vessels, none was worse; but retinitisproliferans deteriorated in half the cases andexudates showed little change. By contrast acomparable unimplanted group showed nosignificant change in respect of venous dilata-tion, hemorrhages and new vessels. At a recentsymposium held to consider the effects ofhypophysectomy and adrenalectomy on diabeticretinopathy (Luft, 1962) most speakers reportedarrest or improvement in about half their cases.Operative mortality was not serious but therewas a considerable mortality in the years offollow-up due in many cases to renal failure.Gordon and Javid (1962) reviewed themetabolic effects of hypophysectomy and con-sidered that patients could be maintained inthe Houssay state for at least five years. Limitedrenal function was the major hazard.Anabolic steroids have been given to coun-
teract the changes in serum proteins occurringin diabetic retinopathy, a fall in serum albuminand a rise in the alpha-2 globulins which containlipoproteins and mucopolysaccharides (Dar-denne, 1961). These changes are consideredto be due to the action of glucocorticoids,consequent on pituitary and adrenal hyper-function. Dardenne Ihas treated 48 patientsfor periods of eighteen months and longer withDecadurabolin and Orgabolin, following theeffect with retinal photographs; 8 patientsimproved, 34 were stationary and 6 deteriorated.Saskin, Waldman and Pelner (1951) treated28 patients with testosterone propionate, andfound that 11 showed no fresh hemorrhages,10 were improved and 7 unchanged afterperiods of two to six months. Valk (1960)reported a single case of improvement. Theduration of these trials was too short to forman opinion about the effectiveness of treatment,and in the series of cases presented by Dar-denne no mention is made of the criteria bywhich the results were judged.The extent to which hard exudates are due
to intracellular fat liberated by necrosis, orserum lipid infiltration, is uncertain (Van Eck,1959), but of 10 patients on a low fat diet(20 grams a day) for an average period of oneyear exudates were reduced in 5 cases andslightly reduced in a further 3; vascular changesand hemorrhages were uninfluenced. King,Dobree, Kok, Foulds and Dangerfield (1963)
treated their patients on a low fat diet to whichunsaturated vegetable fats were added; therewas a reduction of the total serum lipids andan improvement in exudates in 21 out of 26cases. In a comparable group of untreatedcases 11 improved, 4 were unchanged and 22were worse. Unfortunately the disappearanceof exudates left a permanent scotoma so thatthere was no significant improvement in vision.
Light coagulation of areas of active retino-pathy (producing a controlled local coagulationnecrosis by means of a high intensity lightsource, an effect similar to the natural pheno-menon of an eclipse burn) has been advocatedby Wetzig and Worlton (1963), and the pre-liminary results show moderate success.The results of treatment are unsatisfactory
though superior to comparable untreatedgroups; the management of patients must beassessed in this context. Pituitary ablationproduces considerable general effects and re-quires careful replacement therapy withadequate medical supervision always available.It is likely to be superseded when the cause ofretinopathy is better understood, but for thepresent should be considered when the retino-pathy is severe and active -but not too advanced,provided there is no renal impairment.
OTHER OCULAR MANIFESTATIONS
IncidenceAn extensive survey of the ocular com-
plications of diabetes was made by Waite andBeetham (1935) who examined 2,002 diabeticpatients on the occasion of their first admissionto hospital. The series included many newcases and some already under treatment for aperiod. To obtain an estimate of the incidenceof these ocular conditions in patients not suffer-ing from diabetes they examined concurrentlyanother series of 457 patients also admitted tohospital for the first time. Mild chronic in-fections of the external eye were more commonin the diabetic group and included squamousblepharitis and conjunctivitis from whichstaphylococci were often cultured; surprisinglymeibomian cysts and styes were not common.Xanthelasma occurred more frequently indiabetics, but xanthoma diabetica was notencountered. Weakness of accommodation wasfound in 21% of patients under 50 years ofage; it was never severe and was associated in40% of the cases with a history of transientrefractive changes suggesting that it was len-ticular in origin. Evidence of depigmentationof the iris was found in 6% of the diabetic
by copyright. on M
arch 2, 2020 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.40.470.696 on 1 D
ecember 1964. D
ownloaded from

December, 1964 HILL: The Diabetic Eye 703
patients as compared to 2% of the other group.Poor dilatation of the pupils following theinstillation of mydriatics for routine examina-tion was found in 4% of the diabetic cases, thepatients having normal pupillary reactions.Argyll-Robertson pupils occurred in 2.8% ofthe diabetes, in half of the cases there wasno clear indication of syphilitic origin.Iridocyclitis occurred with equal frequency inboth groups, 1.3% of cases. Senile cataract wasfound to have a similar incidence in the twoseries of patients in all age groups. Amongstjuvenile diabetics cataract was found in 4%of cases of which half were poorly controlled,it progressed at varying rates and once estab-lished was uninfluenced ,by diabetic control.Transient refractive changes were reported in6% of patients. 7 male diabetic patients werefound to have changes typical of tobaccoamblyopia, but in no case was an affection ofthe optic nerve found specific to diabetes.Ocular muscle palsies occurred in 0.8% ofthe diabetic patients.
Leopold (1945) reviewed a series of 100patients who had had 10 years careful diabeticmanagement and compared his findings withthose of Waite and Beetham (1935); he foundlittle significant change save that the incidenceof retinopathy had increased.
Changes in the Lens and RefractionBecause of the widely fluctuating blood
sugar levels, and alteration in the state ofhydration of the tissues, changes in the re-fraction of the eye are frequent in uncontrolleddiabetes. A change towards myopia is usualin uncontrolled patients with a rapid swingtowards hypermetropia when the blood sugaris brought under control. There is a diversityof opinion about the mechanism of thesechanges (Lawrence, Oakley and Barne, 1942;Duke Elder, 1949) though they appear to beosmotic effects acting on the crystalline lens.A change of 2-3 dioptres is usual but it maybe exceeded; it is often astigmatic affecting onemeridian more than another. With the onsetof hypermetropia the patient may be consider-ably inconvenienced particularly when attempt-ing to read, but it is seldom necessary toprescribe glasses as the changes are transientlasting only a week or two when the diabetesis adequately controlled.
Transient changes are seen in the crystallinelens of the eye in diabetic coma (Lawrence andothers, 1942), due to the intense dehydrationwhich also produces profound ocular hypo-tension, they disappear rapidly when the
condition is brought under control. In thesecases the globe of the eye feels very soft to thefingers and with the ophthalmoscope opacitiescan be seen in the crystalline lens which takethe form of wavy lines due to capsular folding,with vacuoles and clefts, and occasionallydenser opacities. Transient lens changes havealso been noted following the control of severediabetes; they take differing forms. Lawrence(1946) reported two cases in which radial cort-ical opacities appeared and lasted 2-4 weeks.Diabetic cataract is a rare entity occurringbilaterally in young patients. Snowflakeopacities appear in the anterior and posteriorcortex under the lens capsule and progress tocomplete opacity sometimes within a few weeks;its incidence and relation to diabetic controlhave been noted. Senile cataract though nomore common in the diabetic probably maturesfaster (Scott, 1953) so that the total incidencemay be higher. In any event a routine urinetest is essential in all cases of cataract, both forthe detection of undiagnosed diabetes and toensure that the disease is adequately controlledbefore operation. Both types of cataract canbe removed surgically with reasonable prospectsof useful vision provided the eye is otherwisehealthy, especially free from new vessels on theiris and serious retinopathy. Post-operativehamorrhage and iridocyclitis are more liableto occur in the diabetic patient and form themajor hazards to successful cataract extraction(Nutt, 1953).
Changes in the IrisOedema and vesiculation of the pigment
epithelium on the posterior surface of the irisresults from infiltration of the cells with gly-cogen and their consequent degeneration.Ultimately the pigment is liberated and de-posited on the structures bounding the anteriorchamber of the eye, the posterior surface ofthe cornea and the anterior capsule of the lens.These deposits and the depigmentation of theiris can be detected with the slit lampmicroscope. The gross thickening of the pig-ment epithelium is probably the basis of thepoor dilatation of the pupil in response tomydriatic drugs which has already beenmentioned.The growth of new vessels on the surface
of the iris is often associated with severeproliferative retinopathy; they are first seenon the anterior surface just beyond the pupil-lary margin, appearing as a dull red patchwhich spreads round the pupil and peripherally.New vessels also develop in the angle of the
by copyright. on M
arch 2, 2020 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.40.470.696 on 1 D
ecember 1964. D
ownloaded from

704 POSTGRADUATE MEDICAL JOURNAL December, 1964
anterior chamber at the same time; they areonly visible by gonioscopy using a specialcontact lens, and block the filtration angleleading to haemorrhagic glaucoma. The termrulbeosis iridis is given to this neovascularisation.
Diabetes does not influence the incidenceof iridocyclitis (Waite and Beetham, 1935), andin a recent review of the concept of diabeticiritis Woods (1961) came to the conclusionthat there was no form of iridocyclitis specificto diabetes, nor could the disease be consideredan aetiological factor in uveitis.
Optic NeuritisSkillern and Lockhart (1959) report 14 cases
of optic neuritis in patients with uncontrolleddiabetes. The onset was gradual and the con-dition bilateral in most cases, papillitis wasobserved in some cases and optic atrophy inothers; a central scotoma or peripheral con-traction of the field of vision was found.Control of the diabetes prevented furtherdeterioration but only 3 patients experiencedany improvement of vision. The condition wasconsidered to be due to the toxic effects ofdiabetes on the optic nerve in susceptiblesubjects; the low incidence of neuropathy,present in only 3 of the cases, and the shortduration of the diabetes were thought todifferentiate it from neuropathic and vasculardisturbances. Duke Elder (1940b) describedthe condition as of sudden onset, often bilateral,more common in males and showing a densesharp-edged scotoma which was central, peri-central or caecocentral (that is, a loss of visualfield centred on or around the fixation point,or lying between it and the blind spot); theprognosis was uncertain, rapid resolution orpersistence with consequent optic atrophy mightoccur. Scott (1953) drew attention to theacknowledged sensitivity of diabetic patientsto the toxic effects of tobacco as manifest bytobacco amblyopia, and agreed with otherauthors (Waite and Beetham, 1935; Walsh,1947) in doubting the existence of a specificdiabetic optic neuritis. In assessing the evidenceit should be remembered that there arenumerous causes of optic neuritis and somecases remain unassigned despite full investiga-tion. The possibility of a genetic factor insome of these cases is suggested by the report
of primary optic atrophy in two patients, maleand female siblings with longstanding diabetesunsatisfactorily controlled (Tunbridge andPaley, 1956).
Ocular PalsiesDiabetic ophthalmoplegia affects the third or
sixth cranial nerves, rarely the fourth (King,1959), and often occurs against a backgroundof previous cranial monoplegia which hasrecovered spontaneously without further com-plication. It is a complication of middle agedpatients with controlled diabetes or mild un-recognised disease; peripheral neuropathy andretinopathy are not necessarily associated.Goldstein and Cogan (1960) reviewed 22 casesof third nerve palsy considered after inves-tigation to be due to diabetes, and comparedthem with 39 other cases due to various causes.The onset of diabetic ophthalmoplegia wassudden, often preceded or accompanied by ahomolateral headache, closely resembling theclinical presentation of an intracranial aneurism.Paralysis of the external muscles was partialor complete but the pupil was usually sparedand internal ophthalmoplegia occurred in only5 cases, being incomplete in 2. By contrast29 out of the 39 other cases which includedseveral due to aneurism, were affected byinternal ophthallmoplegia. All the diabeticcases recovered, the time varied from six daysto four months, but repeated attacks werefound in several patients.
Other ComplicationsIt remains to mention briefly two other
complications of diabetes: subjective visualsymptoms in hypoglycemia, which take variousforms, for example blurring of near vision,diplopia or luminous scotomata, which areusually constant for each patient; and therare condition of lipaemia retinalis seen whenthe fat content of the blood is grossly raisedin severe untreated diabetes, so that the retinalvessels present a peculiar milky pallor turningto pink near the optic disc.
I wish to thank Professor N. Ashton of theInstitute of Ophthalmology for his kindness in supply-ing the photograph of the injected preparation ofretina (Fig. 3), and Mrs. M. Engel of the Hammer-smith Hospital who prepared the retinal photographs.
REFERENCESASHTON, N. (1951: Diabetic Retinopathy, Proc. roy. Soc. Med., 44, 747.ASHTON, N. (1958): Diabetic Micro-Angiopathy, Bibl. ophthal. (Basel), 52, 1.ASHTON, N. (1959): Diabetic Retinopathy, Lancet, ii, 625.ASHTON, N. (1962): Diabetic Retinopathy in Disorders of Carbohydrate Metabolism, p. 195, ed. D. A. Pyke,London: Pitman Medical.
by copyright. on M
arch 2, 2020 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.40.470.696 on 1 D
ecember 1964. D
ownloaded from

December, 1964 HILL: The Diabetic Eye 705
ASHTON, N. (1963): Studies of the Retinal Capillaries in Relation to Diabetic and other Retinopathies, Brit.J. Ophthal., 47, 521.
BALLANTYNE, A. J. (1945): Retinal Changes associated with Diabetes and with Hypertension, Arch. Ophthal.(Chicago), 33, 97-quoted by Ashton (1963).
BALLANTYNE, A. J. (1947): The State of the Retina in Diabetes Mellitus, Trans. ophthal. Soc. U.K., 66, 503.BECKER, B. (1952): Diabetic Retinopathy, Ann. Intern. Med., 37, 273.BECKER, B., MAENGWYN DAVIES, G. D., ROSEN, D., PRIEDENWALD, J. S., and WINTER, F. C. (1954): The
Adrenal Cortex and B-Vitamins in Diabetic Retinopathy, Diabetes, 3, 175.BEETHAM, W. P. (1963): Visual Prognosis of Proliferating Diabetic Retinopathy, Brit. J. Ophthal., 47, 611.BLOODWORTH, J. M. B. (1962): Diabetic Retinopathy, Diabetes, 11, 1.COGAN, D. G., TOUSSAINT, D., and KUWABARA, T. (1961): Retinal Vascular Patterns: Diabetic Retinopathy,
A.M.A. Arch. Ophthal., 66, 366.COLLYER, R. T., and HAZLETT, B. E. (1961): Retinopathy and Neuropathy in one hundred Growth-onset
Diabetic Patients, Canad. med. Ass. J., 85, 1328.CONTRERAS, J. S., FIELD, R. A., HALL, W. A., and SWEET, W. H. (1962): Ophthalmological Observations in
Hypophyseal Stalk Section: Report of 8 Gases of Advancing Diabetic Retinopathy, A.M.A. Arch. Ophthal.,67, 428.
DARDENNE, U. (1961): The Therapeutic Applications of Anabolic Steroids in Ophthalmology, Acta Endocr.(Kbh.), 39, Suppl. 63, p. 143.
DOLLERY, C. T., HODGE, J. V., and ENGEL, M. (1962): Studies of the Retinal Circulation with Fluorescein,Brit. med. J., ii, 1210.
DUKE ELDER, W. S. (1940a): Diabetic Retinopathy: Textbook of Ophthalmology, Vol. III, p. 2729, London:Kimpton.
DUKE ELDER, W. S. (1940b): Endogenous Toxins, ibid, p, 3005.DUKE ELDER, W. S. (1949): Changes of Refraotion in Diabetes Mellitus: Textbook of Ophthalmology, Vol.
IV, p. 4364, London: Kimpton.FRASER, R., and JOPLIN, G. F. (1961): Modem Trends in Endocrinology, ed. H. Gardiner Hill, London:
Butterworth-quoted by Joplin and others (1962).GOLDSTEIN, J. E., and COGAN, D. G. (1960): Diabetic Ophthalmoplegia with special Reference to the Pupil,A.M.A. Arch. Ophthal., 64, 592.GORDON, E. S., and JAVID, M. 1(1962): Metabolic Studies in Hypophysectomy for Diabetic Vascular Disease,Diabetes, 11, 470.HARDIN, R. C., JACKSON, R. L., JOHNSTON, T. L., and KELLY, H. G. (1956): The Development of Diabetic
Retinopathy. Effects of Duration and Control of Diabetes: Diabetes, 5, 397.HILL, D. W. (1963): Unpublished communication.JAVID, M., GORDON, E. S., and ERICKSON, T. C. (1958): Hypophyseotomy in Severe Diabetes: 1, Neuro-
surgical Aspects, J. Neurosurg., 15, 504.JENSEN, V. A., and LUNDBAEK, K. (1955): Diabetic Pigmentopathy of the Macula Lutea: A pew Ophthal-imological Anomaly in long-term Diabetes, Ophthal. (Basel), 129. 89-quoted by Larsen (1960b).JOPLIN, G. F., HILL, D. W., SCOTT, D. J., and FRASER, T. C. R. (1962): Pituitary Ablation in the Treatment
of Diabetic Retinopathy in Disorders of Carbohydrate Metabolism, p. 207, ed. D. A. Pyke, London:Pitman Medical.
KEIDING, N. R., ROOT, H. F., and MARBLE, A. (1952): Importance of Control of Diabetes in Prevention ofVascular Complications, J. Amer. med. Ass., 150, 964-quoted by Larsen (1960a).KING, F. P. (1959): Paralyses of the Extraocular Muscles m Diabetes, A.M.A. Arch. intern. Med., 104, 318.KING, R. C., DOBREE, J. H., D'A KOK, FOULDS, W. S., and DANGERFIELD, W. G. (1963): Exudative DiabeticRetinopathy, Brit. J. Ophthal., 47, 666.KINSELL, L. W. (1957): Hypophysectomy in Unstable Diabetics with Progressive Retinal and Renal VascularDisease, Bull. N.Y. Acad. Med., 33, 171.KUWABARA, T., and COGAN, D. G. (1960): Studies of Retinal Vascular Patterns: Part I Normal Architecture,A.M.A. Arch. Ophthal., 64, 904.LARSEN, H. W. (1960a): Incidence of Diabetic Retinopathy, Acta ophthal. (Kbh.), 38, Suppl. 60, p. 17.LARSEN, H. W. (1960b): Development and Course of Diabetic Retinopathy, ibid, p. 21.LAWRENCE, R. D., OAKLEY, W., and BARNE, I. C. (1942): Temporary Lens Changes in Diabetic Coma, Lancet,ii, 63.LAWRENCE, R. D. (1946): Temporary Cataracts in Diabetes, Brit. J. Ophthal., 30, 78.LEOPOLD, I. H. (1945): Diabetes Mellitus as Observed in 100 Cases for 10 or more Years: III Ocularfindings, Amer. J. med. Sci., 209, 16.LEOPOLD, I. H., ed. (1961): Survey, Ophthal., 6, 498.LUFT, R., OLIVECRONA, H., IKKOS, D., KORNERUP, T., and LJUNGGREN, H. (1955): Hypophysectomy in Man:Further Experiences in Severe Diabetes Mellitus, Brit. med. J., ii, 752.LUFT, R. (1962): The Use of Hypophysectomy in Juvenile Diabetes Mellitus with Vascular Complications,Symposium on the Influence of Hypophysectomy and of Adrenalectomy on Diabetic Retinopathy, Diabetes,11, 461.MAENGWYN DAVIES, G. D., LERMAN, S., POGELL, B. M., STONE, H. H., and FRIEDENWALD, J. S. (1956): TheAdrenal Cortex in Diabetic Retinopathy: Urinary 17-hydroxycorticosteroid Excretion Studies, Bull. JohnsHopk. Hosp., 99, 16.MOONEY, A. J. (1963): Diabetic Retinopathy-A Challenge, Brit. J. Ophthal., 47, 513.Nurr, A. B. (1953): Lens Extraction in Diabetic Patients, ibid, 37, 725.POULSEN, J. E. (1953): Recovery from Retinopathy in a Case of Diabetes with Simmonds' Disease, Diabetes,2, 7.
by copyright. on M
arch 2, 2020 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.40.470.696 on 1 D
ecember 1964. D
ownloaded from

706 POSTGRADUATE MEDICAL JOURNAL December, 1964
POULSEN, J. E., and LARSEN, H. W. (1961): Variations of the Intraocular Tension as a Pathogenetic Factorin Diabetic Retinopathy. Proc. 4th Congress de la Federation international du Diabete, p. 536, ed.M. Demole, Geneve: Editions Medicine et Hygiene.
ROSEN, D. A. (1956): Trans. Canad. ophthal. Soc., 8, 122.SANGALLI (1961): see Leopold (1961).SASKIN, E., WALDMAN, S., and PELNER, L. (1951): Diabetic Retinopathy: A New Approach to Therapy with
a Steroid Hormone-Testosterone Propionate, Amer. J. Ophthal., 34, 613.SCHIMEK, R. A. (1956): Hypophysectomy for Diabetic Retinopathy, A.M.A. Arch. Ophthal., 56, 416.SCOTT, D. J., DOLLERY, C. T., HILL, D. W., HODGE, J. V., and FRASER, T. C. R. (1964): Fluorescein Studies
of Diabetic Retinopathy, Brit. med. J., i, 811.SCOTT, G. I. (1951): Diabetic Retinopathy, Proc. roy. Soc. Med., 44, 743.SCOTT, G. I. (1953): Ocular Complications of Diabetes Mellitus, Brit. J. Ophthal., 37, 705.SKILLERN, P. G., and LOCKHART, G. (1959): Optic Neuritis and Uncontrolled Diabetes Mellitus in 14 Patients,
Ann. intern. Med., 51, 468.TOUSSAINT, D., COGAN, D. G., and KUWABARA, T. (1962): Extravascular Lesions of Diabetic Retinopathy,
A.M.A. Arch. Ophthal., 67, 42.TUNBRIDGE, R. E., and PALEY, R. G. (1956): Primary Optic Atrophy in Diabetes Mellitus, Diabetes, 5, 295.VANNAS, S., HERNBERG, C. A., and BJORKESTEN, G. (1959): Hypophyseotomy as a Therapeutic Method for
Proliferative Diabetic Retinopathy, A.M.A. Arch. Ophthal., 62, 370.VALK, L. E. M. (1960): Favourable Tffect of Durabolin (19-nor-androstenolon-phenyl-propionate) on Diabetic
Retinopathy, Ophthal. (Basel), 139, 480.VAN ECK, W. F. (1959): The Effect of a Low Fat Diet on the Serum Lipids in Diabetes and its Significancein Diabetic Retinopathy, Amer. J. Med., 27, 196.VOLK, D. (1956): Dissimilarity of Retinal Microaneurysm and Glomerular Nodule in Diabetes, A.M.A. Arch.Ophthal., 56, 188.WAITE, J. H., and BEETHAM, W. P. (1935): The Visual Mechanism in Diabetes Mellitus, New Engl. J. Med.,212, 367.WALSH, F. B. (1947): Clinical Neuro-ophthalmology, 1st. ed., Baltimore: Williams & Wilkins-quoted by Scott(1953).WETZIG, P. C., and WORLTON, J. T. (1963): Treatment of Diabetic Retinopathy by Light-coagulation, Brit. J.Ophthal., 47, 539.WOLTER, J. R. (1961): Diabetic Retinopathy, Amer. J. Ophthal., 51, 1123.WOODS, A. C. (1961): Endogenous Inflammations of the Uveal Tract, p. 304, Baltimore: Williams & Wilkins.by copyright.
on March 2, 2020 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.40.470.696 on 1 Decem
ber 1964. Dow
nloaded from