
The contractility enhancing effect of the calcium sensitiser levosimendan is not attenuated by...
4
PHARMACODYNAMICS Lasse Lehtonen Stig Sundberg The contractility enhancing effect of the calcium sensitiser levosimendan is not attenuated by carvedilol in healthy subjects Received: 19 March 2002 / Accepted: 2 July 2002 / Published online: 23 August 2002 Ó Springer-Verlag 2002 Abstract Objective: It was assessed whether the con- tractility enhancing effect of the calcium sensitiser levo- simendan is altered by carvedilol. Methods: Twelve healthy subjects received 2 mg levo- simendan i.v. both alone and in addition to a 7–9-day treatment with 25 mg carvedilol orally, twice daily, in a cross-over, placebo-controlled, double-blind, rando- mised study. Systolic time intervals, heart rate, and blood pressure were measured at baseline and up to 2 h after drug administration. Results: When levosimendan was administered in addi- tion to carvedilol, the shortening of electromechanical systole QS2i (indicating increased contractility) was similar to that found with levosimendan alone (P=0.475). Also, the maximum heart rate change was similar, although a statistically significant difference in heart rate was detected due to minor differences at two time points during the 2-h follow-up (P=0.018). There were no differences in diastolic blood pressure response (P=0.962), but the systolic blood pressure response was attenuated by about 4 mmHg with the combination (P=0.013). Conclusions: The contractility enhancing effect of levo- simendan was not altered in healthy subjects who had received carvedilol for at least 1 week. Heart rate and diastolic blood pressure responses were not altered ei- ther, while the systolic blood pressure response was blunted. Keywords Levosimendan Calcium sensitisation Carvedilol Beta-blockade Contractility Introduction Levosimendan is a novel calcium sensitiser developed for short-term intravenous treatment of decompensated heart failure [1]. The drug enhances cardiac contractility by binding to troponin C in a calcium-dependent way [2, 3], and causes vasodilation by opening ATP-sensitive potassium channels in vascular smooth muscle cells [4]. Levosimendan has been shown to improve both hae- modynamics and symptoms in patients with decom- pensated heart failure [5, 6]. Carvedilol is a non-selective b-antagonist and a se- lective a 1 -antagonist, which improves the prognosis of patients with heart failure [7]. However, b-blockers have limitations in their general application in severe heart failure, due to concomitant myocardial depression that may complicate the initiation of therapy [8]. In this pa- tient population, concomitant use of levosimendan and b-blockers could be of potential value, because the contractility enhancing effect of levosimendan could facilitate the initiation and maintenance of b-blocker therapy. In patients with heart failure, who decompensate during b-blocker therapy, levosimendan is used con- comitantly with carvedilol. It is therefore important to clarify if carvedilol alters the contractility enhancing effect of levosimendan. We used a study design where the subjects were given levosimendan intravenously at the end of a treatment period with carvedilol. The aim of the study was to assess if carvedilol alters the contractility enhancing effect of levosimendan in young healthy subjects, using systolic time intervals as indices of contractility. Methods Subjects Twelve healthy male subjects were included. Their mean age was 24 years (range 21–29 years), and mean weight 76 kg (range 68– 85 kg). All subjects gave written informed consent to participation Eur J Clin Pharmacol (2002) 58: 449–452 DOI 10.1007/s00228-002-0500-3 S. Sundberg (&) Orion Pharma, Clinical Research, Cardiovascular Projects, Espoo, Finland E-mail: [email protected] Tel.: +358-10-4292875 Fax: +358-10-4292896 L. Lehtonen Department of Clinical Pharmacology, University of Helsinki, Helsinki, Finland
Transcript of The contractility enhancing effect of the calcium sensitiser levosimendan is not attenuated by...

PHARMACODYNAMICS
Lasse Lehtonen Æ Stig Sundberg
The contractility enhancing effect of the calcium sensitiserlevosimendan is not attenuated by carvedilol in healthy subjects
Received: 19 March 2002 /Accepted: 2 July 2002 / Published online: 23 August 2002� Springer-Verlag 2002
Abstract Objective: It was assessed whether the con-tractility enhancing effect of the calcium sensitiser levo-simendan is altered by carvedilol.Methods: Twelve healthy subjects received 2 mg levo-simendan i.v. both alone and in addition to a 7–9-daytreatment with 25 mg carvedilol orally, twice daily, in across-over, placebo-controlled, double-blind, rando-mised study. Systolic time intervals, heart rate, andblood pressure were measured at baseline and up to 2 hafter drug administration.Results: When levosimendan was administered in addi-tion to carvedilol, the shortening of electromechanicalsystole QS2i (indicating increased contractility) wassimilar to that found with levosimendan alone(P=0.475). Also, the maximum heart rate change wassimilar, although a statistically significant difference inheart rate was detected due to minor differences at twotime points during the 2-h follow-up (P=0.018). Therewere no differences in diastolic blood pressure response(P=0.962), but the systolic blood pressure response wasattenuated by about 4 mmHg with the combination(P=0.013).Conclusions: The contractility enhancing effect of levo-simendan was not altered in healthy subjects who hadreceived carvedilol for at least 1 week. Heart rate anddiastolic blood pressure responses were not altered ei-ther, while the systolic blood pressure response wasblunted.
Keywords Levosimendan Æ Calcium sensitisation ÆCarvedilol Æ Beta-blockade Æ Contractility
Introduction
Levosimendan is a novel calcium sensitiser developedfor short-term intravenous treatment of decompensatedheart failure [1]. The drug enhances cardiac contractilityby binding to troponin C in a calcium-dependent way [2,3], and causes vasodilation by opening ATP-sensitivepotassium channels in vascular smooth muscle cells [4].Levosimendan has been shown to improve both hae-modynamics and symptoms in patients with decom-pensated heart failure [5, 6].
Carvedilol is a non-selective b-antagonist and a se-lective a1-antagonist, which improves the prognosis ofpatients with heart failure [7]. However, b-blockers havelimitations in their general application in severe heartfailure, due to concomitant myocardial depression thatmay complicate the initiation of therapy [8]. In this pa-tient population, concomitant use of levosimendan andb-blockers could be of potential value, because thecontractility enhancing effect of levosimendan couldfacilitate the initiation and maintenance of b-blockertherapy.
In patients with heart failure, who decompensateduring b-blocker therapy, levosimendan is used con-comitantly with carvedilol. It is therefore important toclarify if carvedilol alters the contractility enhancingeffect of levosimendan. We used a study design wherethe subjects were given levosimendan intravenously atthe end of a treatment period with carvedilol.
The aim of the study was to assess if carvedilol altersthe contractility enhancing effect of levosimendan inyoung healthy subjects, using systolic time intervals asindices of contractility.
Methods
Subjects
Twelve healthy male subjects were included. Their mean age was24 years (range 21–29 years), and mean weight 76 kg (range 68–85 kg). All subjects gave written informed consent to participation
Eur J Clin Pharmacol (2002) 58: 449–452DOI 10.1007/s00228-002-0500-3
S. Sundberg (&)Orion Pharma, Clinical Research,Cardiovascular Projects, Espoo, FinlandE-mail: [email protected].: +358-10-4292875Fax: +358-10-4292896
L. LehtonenDepartment of Clinical Pharmacology,University of Helsinki, Helsinki, Finland

in the study. The study protocol was approved by the local ethicscommittee. The study was conducted in accordance with the Dec-laration of Helsinki (Hong Kong revision 1989).
Study design
The study was a placebo-controlled, double-blind (with regard tolevosimendan), randomised, cross-over study (Fig. 1). First thesubjects received 2 mg levosimendan and placebo i.v. blindly inrandomised order on two consecutive days (days 1 and 2). At theend of an open-label period of 7–9 days with 2·25 mg carvedilolorally daily, the subjects again received 2 mg levosimendan andplacebo i.v. blindly in randomised order on two consecutive days(days 3 and 4). Levosimendan and placebo were given as a 5-mini.v. infusion.
Assessments
After a 15-min supine rest, baseline systolic time intervals, heartrate, and blood pressure were recorded twice with an interval ofabout 5 min (the mean of the two readings was used as the baselinevalue). The assessments were repeated at the end of the infusion(0 min), and 10, 30, 60, and 120 min afterwards, with the subjectsremaining supine all the time. Recordings were made with a six-channel ECG (Mingograf 62, Siemens-Elema) at a paper speed of100 mm/s. For the measurement of systolic time intervals, five toten cardiac cycles were averaged using a digitizer (Bitpad, Sum-magraphics). The electromechanical systole (QS2) was measuredfrom the beginning of the Q-wave in the ECG to the beginning ofthe second heart sound in the phonocardiogram. To calculate thepre-ejection period (PEP), the equation PEP=QS2–LVET (LVET,left ventricular ejection time) was used. LVET was measured fromthe beginning of the upstroke to the incisura of the dicrotic notch inthe ear densitogram first derivative (Hewlett-Packard 780-16). QS2was corrected for heart rate according to Weissler et al. [9] anddesignated QS2i, while PEP was not corrected.
The heart rate was recorded from the same beats used whendigitising the systolic time intervals. The blood pressure was mea-sured with an automatic device (Dinamap 8100, Critikon) fromeither arm.
Statistical analysis
Treatment effects were evaluated using analysis of covariance(ANCOVA) for repeated measurements with post hoc pairwisecomparisons according to the method of Tukey. Baseline mea-surements were utilised as covariates in the analysis. Estimates ofthe treatment differences with 95% confidence intervals were alsocalculated. The comparison between the combination (levosimen-dan+carvedilol) and levosimendan was the primary one. A two-sided P<0.05 was considered statistically significant.
Results
The 7–9-day treatment with carvedilol had no effect onQS2i, the mean values being 520–523 ms both before
and at the end of the carvedilol period. When levo-simendan was administered in addition to carvedilol,the shortening of QS2i, indicating increased contrac-tility, was similar to that with levosimendan alone(P=0.475) (Fig. 2). The maximum shortening of QS2iwas 18 ms with levosimendan alone and 13 ms whenlevosimendan was given in addition to carvedilol(P=0.0006 and P=0.0047, respectively, compared withplacebo).
Both levosimendan and the 7–9-day treatment withcarvedilol shortened PEP by 13 and 8 ms, respectively,but the difference was not significant between levosim-endan alone compared with levosimendan given in ad-dition to carvedilol (P=0.105). Levosimendanshortened PEP from 63 (13) to 50 (13) ms [mean(SD)](P=0.0001). When levosimendan was administered inaddition to carvedilol, PEP shortened from 61 (10) to 59(11) ms compared with placebo (P=0.0115).
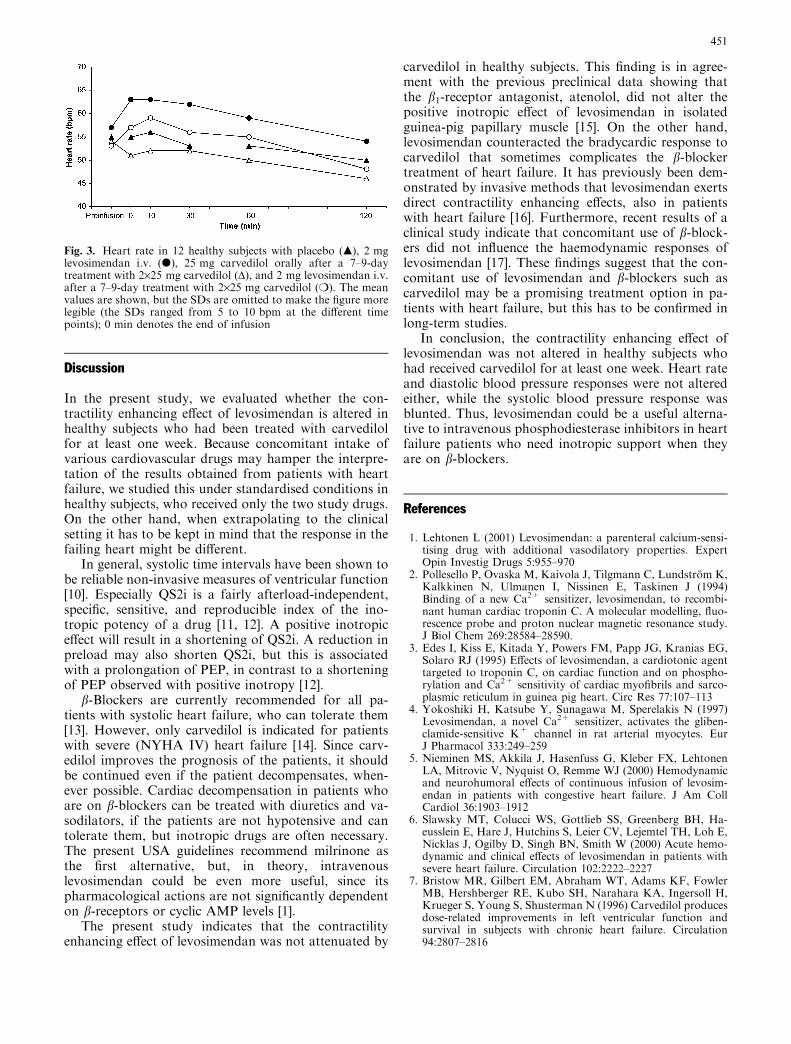
When levosimendan was administered in addition tocarvedilol, the maximum increase in the heart rate was6 bpm, from 53 (6) to 59 (6) bpm, which was the same aswith levosimendan alone, from 57 (10) to 63 (9) bpm.However, although the shape of the heart rate responsecurves were very similar (Fig. 3), the estimated differ-ence was statistically significant (P=0.018). This differ-ence was totally attributable to numerically minordifferences (about 2–3 bpm) at the time points 0 minand 120 min.
Levosimendan increased the systolic blood pressureby 5 mmHg, from 121 (6) to 126 (8) mmHg, and de-creased diastolic blood pressure by 3 mmHg, from 62(5) to 59 (7) mmHg. When levosimendan was admin-istered in addition to carvedilol, the diastolic bloodpressure response did not differ from that with levo-simendan alone (P=0.962), but the systolic bloodpressure response was attenuated by about 4 mmHg(P=0.013).
Fig. 1. Flow chart of the study; L, levosimendan; P, placebo
Fig. 2. Electromechanical systole (QS2i) in 12 healthy subjectswith placebo treatment (m), 2 mg levosimendan i.v. (d), 25 mgcarvedilol orally after a 7–9-day treatment with 2·25 mg carvedilol(D), and 2 mg levosimendan i.v. after a 7–9-day treatment with2·25 mg carvedilol (m). The mean values are shown, but the SDsare omitted to make the figure more legible (the SDs ranged from11 to 18 ms at the different time points); 0 min denotes the end ofinfusion
450
Discussion
In the present study, we evaluated whether the con-tractility enhancing effect of levosimendan is altered inhealthy subjects who had been treated with carvedilolfor at least one week. Because concomitant intake ofvarious cardiovascular drugs may hamper the interpre-tation of the results obtained from patients with heartfailure, we studied this under standardised conditions inhealthy subjects, who received only the two study drugs.On the other hand, when extrapolating to the clinicalsetting it has to be kept in mind that the response in thefailing heart might be different.
In general, systolic time intervals have been shown tobe reliable non-invasive measures of ventricular function[10]. Especially QS2i is a fairly afterload-independent,specific, sensitive, and reproducible index of the ino-tropic potency of a drug [11, 12]. A positive inotropiceffect will result in a shortening of QS2i. A reduction inpreload may also shorten QS2i, but this is associatedwith a prolongation of PEP, in contrast to a shorteningof PEP observed with positive inotropy [12].
b-Blockers are currently recommended for all pa-tients with systolic heart failure, who can tolerate them[13]. However, only carvedilol is indicated for patientswith severe (NYHA IV) heart failure [14]. Since carv-edilol improves the prognosis of the patients, it shouldbe continued even if the patient decompensates, when-ever possible. Cardiac decompensation in patients whoare on b-blockers can be treated with diuretics and va-sodilators, if the patients are not hypotensive and cantolerate them, but inotropic drugs are often necessary.The present USA guidelines recommend milrinone asthe first alternative, but, in theory, intravenouslevosimendan could be even more useful, since itspharmacological actions are not significantly dependenton b-receptors or cyclic AMP levels [1].
The present study indicates that the contractilityenhancing effect of levosimendan was not attenuated by
carvedilol in healthy subjects. This finding is in agree-ment with the previous preclinical data showing thatthe b1-receptor antagonist, atenolol, did not alter thepositive inotropic effect of levosimendan in isolatedguinea-pig papillary muscle [15]. On the other hand,levosimendan counteracted the bradycardic response tocarvedilol that sometimes complicates the b-blockertreatment of heart failure. It has previously been dem-onstrated by invasive methods that levosimendan exertsdirect contractility enhancing effects, also in patientswith heart failure [16]. Furthermore, recent results of aclinical study indicate that concomitant use of b-block-ers did not influence the haemodynamic responses oflevosimendan [17]. These findings suggest that the con-comitant use of levosimendan and b-blockers such ascarvedilol may be a promising treatment option in pa-tients with heart failure, but this has to be confirmed inlong-term studies.
In conclusion, the contractility enhancing effect oflevosimendan was not altered in healthy subjects whohad received carvedilol for at least one week. Heart rateand diastolic blood pressure responses were not alteredeither, while the systolic blood pressure response wasblunted. Thus, levosimendan could be a useful alterna-tive to intravenous phosphodiesterase inhibitors in heartfailure patients who need inotropic support when theyare on b-blockers.
References
1. Lehtonen L (2001) Levosimendan: a parenteral calcium-sensi-tising drug with additional vasodilatory properties. ExpertOpin Investig Drugs 5:955–970
2. Pollesello P, Ovaska M, Kaivola J, Tilgmann C, Lundstrom K,Kalkkinen N, Ulmanen I, Nissinen E, Taskinen J (1994)Binding of a new Ca2+ sensitizer, levosimendan, to recombi-nant human cardiac troponin C. A molecular modelling, fluo-rescence probe and proton nuclear magnetic resonance study.J Biol Chem 269:28584–28590.
3. Edes I, Kiss E, Kitada Y, Powers FM, Papp JG, Kranias EG,Solaro RJ (1995) Effects of levosimendan, a cardiotonic agenttargeted to troponin C, on cardiac function and on phospho-rylation and Ca2+ sensitivity of cardiac myofibrils and sarco-plasmic reticulum in guinea pig heart. Circ Res 77:107–113
4. Yokoshiki H, Katsube Y, Sunagawa M, Sperelakis N (1997)Levosimendan, a novel Ca2+ sensitizer, activates the gliben-clamide-sensitive K+ channel in rat arterial myocytes. EurJ Pharmacol 333:249–259
5. Nieminen MS, Akkila J, Hasenfuss G, Kleber FX, LehtonenLA, Mitrovic V, Nyquist O, Remme WJ (2000) Hemodynamicand neurohumoral effects of continuous infusion of levosim-endan in patients with congestive heart failure. J Am CollCardiol 36:1903–1912
6. Slawsky MT, Colucci WS, Gottlieb SS, Greenberg BH, Ha-eusslein E, Hare J, Hutchins S, Leier CV, Lejemtel TH, Loh E,Nicklas J, Ogilby D, Singh BN, Smith W (2000) Acute hemo-dynamic and clinical effects of levosimendan in patients withsevere heart failure. Circulation 102:2222–2227
7. Bristow MR, Gilbert EM, Abraham WT, Adams KF, FowlerMB, Hershberger RE, Kubo SH, Narahara KA, Ingersoll H,Krueger S, Young S, Shusterman N (1996) Carvedilol producesdose-related improvements in left ventricular function andsurvival in subjects with chronic heart failure. Circulation94:2807–2816
Fig. 3. Heart rate in 12 healthy subjects with placebo (m), 2 mglevosimendan i.v. (d), 25 mg carvedilol orally after a 7–9-daytreatment with 2·25 mg carvedilol (D), and 2 mg levosimendan i.v.after a 7–9-day treatment with 2·25 mg carvedilol (m). The meanvalues are shown, but the SDs are omitted to make the figure morelegible (the SDs ranged from 5 to 10 bpm at the different timepoints); 0 min denotes the end of infusion
451

8. Bristow MR (2000) b-adrenergic receptor blockade in chronicheart failure. Circulation 101:558–569
9. Weissler AM, Harris WS, Schoenfeld CD (1968) Systolic timeintervals in heart failure in man. Circulation 37:149–159
10. Martin CE, Shaver JA, Thompson ME, Reddy PS, Leonard JJ(1971) Direct correlation of external systolic time intervals withinternal indices of left ventricular function in man. Circulation44:419–431
11. Nakamura Y, Wiegner AW, Gaasch WH, Bing OHL (1983)Systolic time intervals: assessment by isolated cardiac musclestudies. J Am Coll Cardiol 2:973–978
12. Li Q, Belz GG (1993) Systolic time intervals in clinical phar-macology. Eur J Clin Pharmacol 44:415–421
13. Hunt HA, Baker DW, Chin MH, Cinquegrani MP, Feld-manmd AM, Francis GS, Ganiats TG, Goldstein S, Gregora-tos G, Jessup ML, Noble RJ, Packer M, Silver MA, StevensonLW, Gibbons RJ, Antman EM, Alpert JS, Faxon DP, FusterV, Gregoratos G, Jacobs AK, Hiratzka LF, Russell RO, SmithSC Jr (2001) ACC/AHA Guidelines for the Evaluation andManagement of Chronic Heart Failure in the Adult. Circula-tion 104:2996–3007
14. Packer M, Coats AJ, Fowler MB, Katus HA, Krum H,Mohacsi P, Rouleau JL, Tendera M, Castaigne A, Roecker EB,Schultz MK, DeMets DL (2001) Effect of carvedilol on survivalin severe chronic heart failure. N Engl J Med 344:1651–1658
15. Haikala H, Kaheinen P, Levijoki J, Linden I-B (1997) The roleof cAMP- and cGMP-dependent protein kinases in the cardiacactions of the new calcium sensitizer, levosimendan. Cardio-vasc Res 34:536–546
16. Givertz MM, Conrad CH, Andreou C (1998) Direct myocar-dial effects of levosimendan, a novel calcium sensitizing agent,in humans with left ventricular dysfunction. Circulation (17Suppl):I-579
17. Follath F, Cleland JG, Just H, Papp JG, Scholz H, Peuhkuri-nen K, Harjola VP, Mitrovic V, Abdalla M, Sandell EP, Le-htonen L (2002) Efficacy and safety of intravenouslevosimendan compared with dobutamine in severe low-outputheart failure (the LIDO study): a randomised double-blindtrial. Lancet 360(9328):196–202
452


















