The clinical effectiveness of nurse practitioners' management of minor injuries in an adult...
12
EVIDENCE SYNTHESIS The clinical effectiveness of nurse practitioners’ management of minor injuries in an adult emergency department: a systematic review Anne Wilson PhD, BN, MN, FRCNA, Elizabeth Zwart RN, Cert. Oncology, Cert. Stomal Therapy, Grad Dip Onc Nsg, Iain Everett RN, BN, Cert A&E and Jodie Kernick RN, BN, Grad Dip ICU Grad. Cert. Retrieval Discipline of Nursing, The University of Adelaide, Adelaide, South Australia, Australia Abstract Background The increasing cost of healthcare in Australia demands changes in the way healthcare is delivered. Nurse practitioners have been introduced into specialty areas including emergency departments. Specific interven- tions are known to include the treatment and management of minor injuries, but little has been reported on their work. Objectives Examine the best available evidence to determine the clinical effectiveness of emergency department nurse practitioners in the assessment, treatment and management of minor injuries in adults. Inclusion criteria For inclusion studies had to include adult patients treated for minor injuries by nurse practitioners in emergency departments. All study designs were included. Search strategy English language articles from 1986 onwards were sought using MEDLINE, CINAHL, Embase and Science Citation Index. Methodological quality Two independent reviewers critically appraised the quality of the studies and extracted data using standardised tools. Data collection Two independent reviewers assessed the eligibility of each study for inclusion into the review and the study design used. Where any disagreement occurred, consensus was reached by discussion with an independent researcher. Data synthesis Studies were assessed for homogeneity by considering populations, interventions and outcomes. Where heterogeneity was present, synthesis was undertaken in a narrative format; otherwise a meta-analysis was conducted. For each outcome measure, results were tabulated by intervention type and discussed in a narrative summary. Results from randomised controlled trials were pooled in meta-analyses where appropriate. Results Nine studies from a total of 55 participants met the inclusion criteria. Two were randomised controlled trials. Metasynthesis of research findings generated five synthesised findings derived from 16 study findings aggregated into seven categories. Evidence comparing the clinical effectiveness of nurse practitioners to mainstream management of minor injuries was fair to poor methodological quality. When comparable data were pooled, there were no significant differences (P < 0.05) between nurse practitioners and junior doctors. Conclusions The results emphasise the need for more high-quality research using appropriate outcome measures in the area of clinical effectiveness of nurse practitioners, particularly interventions that improve outcomes for presentations to emergency departments and address issues of waiting and congestion. Key words: adult, emergency department, minor injuries, nurse practitioners, systematic review. Correspondence: Dr Anne Wilson, Discipline of Nursing, School of Population Health & Clinical Practice, Level 3, Eleanor Harold Building, The University of Adelaide, North Terrance, Adelaide, Australia, 5005. Email: [email protected] doi:10.1111/j.1744-1609.2009.00121.x Int J Evid Based Healthc 2009; 7: 3–14 © 2009 The Authors Journal Compilation © Blackwell Publishing Asia Pty Ltd
-
Upload
anne-wilson -
Category
Documents
-
view
213 -
download
0
Transcript of The clinical effectiveness of nurse practitioners' management of minor injuries in an adult...

E V I D E N C E S Y N T H E S I S
The clinical effectiveness of nurse practitioners’ managementof minor injuries in an adult emergency department:a systematic review
Anne Wilson PhD, BN, MN, FRCNA, Elizabeth Zwart RN, Cert. Oncology, Cert. StomalTherapy, Grad Dip Onc Nsg, Iain Everett RN, BN, Cert A&E and Jodie Kernick RN, BN, GradDip ICU Grad. Cert. RetrievalDiscipline of Nursing, The University of Adelaide, Adelaide, South Australia, Australia
AbstractBackground The increasing cost of healthcare in Australia demands changes in the way healthcare is delivered.Nurse practitioners have been introduced into specialty areas including emergency departments. Specific interven-tions are known to include the treatment and management of minor injuries, but little has been reported on theirwork.
Objectives Examine the best available evidence to determine the clinical effectiveness of emergency departmentnurse practitioners in the assessment, treatment and management of minor injuries in adults.
Inclusion criteria For inclusion studies had to include adult patients treated for minor injuries by nursepractitioners in emergency departments. All study designs were included.
Search strategy English language articles from 1986 onwards were sought using MEDLINE, CINAHL, Embaseand Science Citation Index.
Methodological quality Two independent reviewers critically appraised the quality of the studies andextracted data using standardised tools.
Data collection Two independent reviewers assessed the eligibility of each study for inclusion into the reviewand the study design used. Where any disagreement occurred, consensus was reached by discussion with anindependent researcher.
Data synthesis Studies were assessed for homogeneity by considering populations, interventions and outcomes.Where heterogeneity was present, synthesis was undertaken in a narrative format; otherwise a meta-analysis wasconducted. For each outcome measure, results were tabulated by intervention type and discussed in a narrativesummary. Results from randomised controlled trials were pooled in meta-analyses where appropriate.
Results Nine studies from a total of 55 participants met the inclusion criteria. Two were randomised controlledtrials. Metasynthesis of research findings generated five synthesised findings derived from 16 study findingsaggregated into seven categories. Evidence comparing the clinical effectiveness of nurse practitioners to mainstreammanagement of minor injuries was fair to poor methodological quality. When comparable data were pooled, therewere no significant differences (P < 0.05) between nurse practitioners and junior doctors.
Conclusions The results emphasise the need for more high-quality research using appropriate outcome measuresin the area of clinical effectiveness of nurse practitioners, particularly interventions that improve outcomes forpresentations to emergency departments and address issues of waiting and congestion.
Key words: adult, emergency department, minor injuries, nurse practitioners, systematic review.
Correspondence: Dr Anne Wilson, Discipline of Nursing, School ofPopulation Health & Clinical Practice, Level 3, Eleanor HaroldBuilding, The University of Adelaide, North Terrance, Adelaide,Australia, 5005. Email: [email protected]
doi:10.1111/j.1744-1609.2009.00121.x Int J Evid Based Healthc 2009; 7: 3–14
© 2009 The AuthorsJournal Compilation © Blackwell Publishing Asia Pty Ltd

Background
The increasing cost of healthcare in Australia demandschanges in the way healthcare is delivered. In other coun-tries, nurse practitioner (NP) roles have evolved from theneed to provide improved access and affordable qualityhealthcare to increasingly complex patients.1–3 In Australia,as in other countries, the title ‘nurse practitioner’ is assignedthrough an application and certification process managedby the state nurses boards. Worldwide, these credentialsmight go by different titles that describe the status of nursesworking in extended and expanded roles, for example,advance practice nurse and nurse specialist.4
Nurse practitioners, working in an expanded scope ofpractice using extended repertoire of skill, are able to coordi-nate patients’ care both within and beyond the hospitalsetting, complementing the current clinical care already pro-vided.5 They might expand the hospital’s ability to respondeffectively and efficiently to evolving demands on the health-care system and act as the driving force for collaborationbetween the patient’s general practitioner and other health-care professionals to best meet the needs of the patient.6
Nurse practitioners have recently been introduced intospecialty areas including emergency departments. Specificinterventions are known to include the treatment and man-agement of minor injuries, but little has been reported on thework of emergency department nurse practitioners (ENP).Introducing NP is an approach that aims to improve patientaccess to interventions and decrease the demand on hospitalmedical services.7 Consequently, it is anticipated that inter-vention by an NP will decrease the amount of time spent byemergency department medical practitioners on specifiedpresentations.8 A report from one major Australian metropoli-tan hospital has indicated that although initiatives within theemergency department have shown dramatic improvementin waiting times to be seen by a medical officer, triagethresholds are still not meeting the agreed national accessperformance indicators under the Australasian Triage Scale.9
Increased waiting times can affect patients’ total length ofhospital stay, leading to issues of violence/aggression andemergency department overcrowding. Overcrowding has adetrimental effect on stress levels for all emergency depart-ment staff, affecting staff retention and ultimately the qualityof patient care that can be provided. The reason for extendedwaits is always due to the patient’s needing to wait for anavailable medical officer to assess them and commence theappropriate investigations and treatment. An appropriatelytrained and educated NP would be able to target a specificgroup of patients to address waiting times and assist theemergency department to decrease overcrowding andincrease patient flow through the department.10,11
With international trends, Australian Departments ofHealth have been actively involved in the development ofthe role of the NP through the implementation of state-based projects.12 Within the Final South Australian NursePractitioner Project Report, a number of key issues and rec-ommendations arose from the defining features of an NP.12
These defining features combine the subroles of educator,
mentor, provider, manager and researcher. It is envisagedthat, in order for these roles to evolve, the setting in whichthe NP wishes to be accredited must be specified. The NPshould accordingly develop in areas where gaps in servicesexist, continually consulting with other healthcare profes-sionals to ensure services are productive and healthcarefacilities and clients are benefiting. Implementing ENP aimsto facilitate best practice, cost-effective patient care in col-laboration with medical and allied healthcare professionals,and to contribute to the safe, efficient and best possible careof patients whom fall within the defined scope of practice.13
This systematic review has generated new knowledgerelating to the contemporary role of NP in emergencydepartment patient care. As such, there is a need to ascertainwhether or not services provided by NP are an effectiveadjunct to current practice, reducing waiting times, readmis-sion rates and total length of stay. With this in mind, theobjective of this systematic review is to present the bestavailable evidence related to the clinical effectiveness of NPin the management of adults referred for treatment by themin an emergency department.
Objectives
The objective of this review was to examine the best avail-able evidence to determine the clinical effectiveness of ENPin the assessment, treatment and management of minorinjuries in adults and their effect on waiting times. Thespecific review questions addressed were:
Are ENP effective in:1 Reducing waiting times to be assessed2 Reducing waiting times for treatment3 Reducing overall length of stay times4 Reducing the amount of medical officer time spent on
specified presentations5 Improving patient access to interventions6 Reducing issues of emergency department overcrowding
Criteria for considering studies forthis review
Types of studiesThis review considered randomised controlled trials (RCTs),non-randomised clinical trials, case-series, case–control andcohort studies where the effectiveness of NP was comparedfor the assessment, treatment and management of emer-gency department presentations for minor injuries in adults.In the absence of large numbers of RCTs, other researchmethods, such as descriptive exploratory designs, wereused.
Types of participantsParticipants included adult (16 years and over) presentationsto an emergency department for treatment by an NP of aminor injury.
Types of interventionsThe phenomena of interest were the scope of practice of theENP and included activities of:
4 A Wilson et al.
© 2009 The AuthorsJournal Compilation © Blackwell Publishing Asia Pty Ltd

• Assessment• Diagnosis• Consultation• Treatment• Referral• Patient education
Types of outcome measuresThe primary outcome of interest was the management ofminor injuries by NP in an adult emergency department.Given the wide range of presentations to an emergencydepartment and the breadth of nurses’ work, the authorsincluded studies that reported on the effectiveness of NP’smanagement of any presentation, including, but notlimited to:• Effect on waiting times• Referral (internal or external) to other practitioners or
services within the emergency department and/or hospi-tal or to practitioners or services in the community
• Representations to the emergency department within48 h
• Perceived or identified cost reduction• Patient satisfaction
Search strategy for identificationof studies
A comprehensive search strategy was developed to find bothpublished and unpublished studies in English from 1986onwards. An initial search of the Cochrane Database ofSystematic Reviews, Joanna Briggs Institute (JBI) and theDatabase of Abstracts of Reviews of Effect (DARE) weresearched for any systematic review publication on this topic.No such reviews were found at the commencement of thereview.
A three-step search strategy was used in each componentof this review. Initial keywords used were: emergencydepartment, nurse practitioner, nurse specialist, advancedpractice, expanded practice and extended practice. MeSHterminology and keywords were adapted to suit the needs ofthe different databases.
Step oneAn initial limited search of MEDLINE and CINAHL was under-taken followed by analysis of the text words contained in thetitle and abstract, and of the index terms used to describearticle. The databases searched included MEDLINE, CINAHL,Embase and DARE.
Step twoA second extensive search using all identified keywords andindex terms was then undertaken across all included data-bases. A second extensive search was undertaken using theidentified keywords and index terms. Databases searched inthe second stage included:1 PubMed2 PsycInfo3 Academic Search Elite
4 Expanded Academic Index5 Web of Science6 AustHealth7 Health and Society8 CINAHL9 Cochrane Library (incorporating DARE and CENTRAL)
10 ISI Current ContentsThe search for unpublished studies was conducted using
Dissertation Abstracts International and included proceed-ings, dissertations, abstracts and reports.
An electronic search of Google and Google Scholar assearch engines for relevant conference proceedings, reportsand unpublished studies was also conducted in an attemptto identify further trials, although no additional studies werelocated by this approach.
Step threeThird, the reference list of all identified reports and articleswas searched for additional studies. Key journals which con-sistently appear in searches were hand-searched to capturerelevant research-based articles which fall outside theidentified search terms. In order to avoid publication bias,hand-searching was also undertaken in journals which arenot listed on databases but are known to contain works inour field of investigation. A search of the reference listsand bibliographies of all relevant articles was conducted tofind additional articles not found in the preceding searchstrategies.
The initial search of the above-mentioned electronic data-bases elicited 385 articles. These 385 articles were assessedby two reviewers for relevance to the review based on theinformation provided in the title and abstract using theinclusion/exclusion criteria. Articles identified as potentialinclusions were retrieved and then assessed for inclusionbased on the full text. The reference lists of all studiesdeemed to match the inclusion criteria were searched forany further possible inclusions.
Those studies that were of poor methodological quality ordid not meet the inclusion criteria were excluded from thereview. The identification of articles for inclusion and exclu-sion is outline in Figure 1. The included articles are presentedin Appendix I and the basis for the excluded articles isoutlined in Appendix II.
Methods of the review
Assessment of methodological qualityPapers selected for retrieval were assessed independently bytwo reviewers for methodological validity before inclusion inthe review using standardised critical appraisal instrumentsfrom the Joanna Briggs Institute Meta Analysis of StatisticsAssessment and Review Instrument (JBI-MAStARI).14 Descrip-tive papers of survey research and case-note audit selectedfor retrieval were assessed independently by two reviewersfor methodological validity before inclusion in the reviewusing the critical appraisal tool for observational studiesfrom JBI.14
Effective management of minor injuries 5
© 2009 The AuthorsJournal Compilation © Blackwell Publishing Asia Pty Ltd

Where no comparative studies are identified, opinion andtext papers selected for retrieval were assessed by two inde-pendent reviewers for authenticity before inclusion in thereview. Any disagreements that arose between the reviewerswere resolved through discussion or with a third reviewer.
Data extractionData extraction of the eligible studies was undertaken inde-pendently by two reviewers using the data extraction toolsfrom JBI-MAStARI.14 Any disagreement was resolved by dis-cussion between the reviewers. The data extracted includedspecific details about the interventions, populations, studymethods and outcomes of significance to the review ques-tion and specific objectives.
Data synthesisTwo independent reviewers entered data. The findings/conclusions from descriptive studies were categorised andsynthesised. This involved the aggregation or synthesis offindings to generate a set of statements representing thataggregation, through assembling the findings (level 1 find-ings) with their quality, and categorising these findings onthe basis of similarity in meaning (level 2 findings).
These categories were then subjected to a metasynthesisin order to produce a single comprehensive set of synthe-
sised findings (level 3 findings) that can be used as a basis forevidence-based practice. Where textual pooling was notpossible the findings are presented in narrative form.14
Where possible, papers were pooled in statistical meta-analysis using the JBI-MAStARI.14 All data entered into JBI-MAStARI were subject to double data entry. Odds ratio (forcategorical data), weighted mean differences (for continu-ous data) and their 95% confidence intervals were calcu-lated for analysis. Heterogeneity was assessed using thestandard c2. Where statistical pooling was not possible, thefindings are presented in narrative form.
The included studies in this review were assessed for fea-sibility of meta-analyses of primary and secondary outcomes.As only one study was found on the primary outcome (thatof clinical effectiveness of emergency NP’s management ofadults with minor injuries), analysis was not possible.However, it was possible to extract data relating to thereduction of waiting time in the emergency department andpatients satisfaction with care received.
Two RCTs were identified that used care by junior doctorsas the measure of the comparison against ENP.15,16 Wherecount data were present, numbers needed to treat, relativerisk and 95% confidence intervals have been calculated inorder to provide a treatment effect.
A single study17 was identified that compared the clinicaland cost-effectiveness of ENP, but as this was the case meta-analysis was not possible. Therefore, the data from theincluded study have been combined in a narrative review.
Results
Description of studiesSelection of studiesOver 385 titles were identified from the search criteria. Ofthese, 55 were retrieved on the basis that the title and/orabstract appeared relevant to the review. Two independentreviewers individually assessed these articles against thereview criteria. Twenty retrieved articles were found to meetthe inclusion criteria. Of the 35 excluded, reasons for exclu-sion were as follows: 10 articles were not studies, 16 did notdescribe an intervention study, two articles did not meet theparticipant inclusion criteria, and seven were unclear in theirreporting. Of the studies retrieved only two were RCTs andthe remainder descriptive studies predominantly usingsurvey design.
InterventionsThe focus of reported interventions in the included studieswas the reduction in waiting times, referral to other practi-tioners or services, provision of medication, radiographs andother treatment, such as bandaging and suturing.
Patient satisfaction with treatment by an NP was reportedin few studies and is reported as an outcome. In one study,some participants reported they would have preferred to beseen by a medical officer.18 In all other studies, satisfactionwith NP services was reportedly over 70%.
Articles excluded not retrieved n=330
Articles that met all inclusion criteria n=20
Experimental studies included in review n=8
Descriptive studies included in the review n=12
Experimental studies n=5
Articles excluded n=35 10 not a study 16 no intervention 2 did not meet participant
inclusion criteria 7 unclear reporting
Descriptive studies for synthesis n=4
Descriptive studies excluded n=8
Experimental studies excluded n=3
Articles from search strategy n=385
Articles retrieved n=55
Figure 1 Flow chart for identification of papers included in a sys-tematic review of the clinical effectiveness of nurse practitioners’management of adults in an emergency department.
6 A Wilson et al.
© 2009 The AuthorsJournal Compilation © Blackwell Publishing Asia Pty Ltd

Methodological quality of included studiesOf the 12 survey research and case-note studies criticallyappraised, four studies were included and eight studiesexcluded because of meeting less than 60% of the assess-ment criteria. No studies were able to fulfil all requirementsof the critical appraisal form. The four included studies wereable to meet more than 60% of assessment criteria.10,18–20
Of eight other quantitative studies critically appraised, onestudy was able to fulfil all requirements of the criticalappraisal form.15 Four studies were able to meet more than60% of requirements.2,16,17,21 Of the three excluded, twostudies were excluded after finding one did not have com-parable groups22 and another23 included paediatrics beingtreated by NP’s and junior doctors did not fit the inclusioncriteria. Additionally, Considine examined NP and theirspecific scope of practice only.24
Results of metasynthesis of the research findingsOther than the four survey and case-note studies,10,18–20 twostudies were RCTs.15,16 The remaining studies were a retro-spective case-series study,21 a satisfaction survey2 and abefore- and after-cohort study.17 The RCTs reported on theeffectiveness of the ENP in comparison with the role of thejunior medical officer in relation to length of stay, waitingtimes, follow-up and significant error. Results of the synthesisof the descriptive studies are presented below as narrativefindings. Results of the meta-analysis of the two RCT arereported separately.
Narrative findingsWaiting times. In examining waiting times, the study byJennings et al. was a retrospective case-series study thatclearly showed a significant reduction in waiting time andlength of stay for patients managed by the NP in comparisonwith the traditional medical model (TM) of care.21 Theoverall median waiting time for emergency patients to beseen by the ENP was less than the traditional model(junior doctors): ENP 12 min (5.5–28 min), TM 31 min(11.5–76 min) (P < 0.001).
This is supported by Byrne et al., who report that patientsmanaged through the traditional care pathways waited sig-nificantly longer to be seen than patients seen by the ENP(t177 = 43.23, P < 0.001).2
Length of stay. Length of stay was also significantlyreduced in patients managed by the ENP. Jennings et al.found median times for length of stay for those seen by theENP were 94 min (53.5–163.5 min) and for those seen in theTM 170 min (100–274 min) (P < 0.001).21 This is also sup-ported by Byrne et al., who reported that patients managedthrough the traditional model of care (managed by doctors)spent an average of 33 min longer than those managed bythe ENP (t177 = 19.94, P < 0.001).2
Patient satisfaction. Cooper et al.15 found from outcomesmeasured over a period of 2 months using patient satisfac-tion scores that patients overall were more satisfied with thetreatment and information provided by the ENP. The samefindings are confirmed by Byrne et al.2 who report that ENPsignificantly provide more health promotion and advice cor-relating with patient satisfaction support.
Meta-analysisFollow up. A meta-analysis was conducted for the twoRCT15,16 comparing care provided by ENP and junior doctors(Table 1; Fig. 2). The studies were shown to be homogenous(c2 = 2.63, P = 0.10.).
It was found that there was no significance differencebetween the two groups overall (Z = 0.87, P = 0.38), there-fore showing that the follow up provided by the ENP com-pared with the junior doctor was equal or just the same. In
Table 1 Summary of two randomised controlled trials comparingfollow up of patients managed by emergency department nursepractitioners (ENP) or managed in a minor injuries unit (MIU) withjunior doctors or patients managed in a traditional accident andemergency department (A&E). The table includes the number ofpatients (n) followed up in each group and the total (N) in eachgroup
Study ENP or MIU(follow up)
Junior doctors orA&E (follow up)
n N n N
Cooper et al. (2002)15 63 128 65 128Sakr et al. (1999)16 618 1315 391 1447
Cooper et al. (2002)
DerSimonian and Laird Relative Risk (Risk Ratio) Weight (confidence interval 95% random)
62.51% 0.97 (0.76, 1.24)
37.49% 0.61 (0.35, 1.04)
100.00% 0.81 (0.51, 1.30)
Favours ControlFavours Treatment 000
Heterogeneity χ2 = 2.63, P = 0.1055245
88.0
Sakr et al. (1999)
Overall
Overall Z = 0.87, P = 0.3898
Study
Figure 2 Forest plot of two randomised controlled trials comparing follow up of patients managed by emergency department nursepractitioners or managed in a minor injuries unit with junior doctors or patients managed in a traditional accident and emergency departmentfollow up.
Effective management of minor injuries 7
© 2009 The AuthorsJournal Compilation © Blackwell Publishing Asia Pty Ltd

Byrne et al.’s2 study, it found that patients seen by ENP hadreceived more printed information at discharge related tofollow up if required, as well as health advice than those seenin traditional models of care.
Significant error. A meta-analysis was conducted for thetwo RCTs15,16 comparing ENP and junior doctors (Table 2;Fig. 3). The studies were shown to be homogenous(c2 = 0.01, P = 0.92.).
It was found that there was no significant differencebetween the two groups overall (Z = 0.91, P = 0.36).
Metasynthesis of survey research and case-note auditstudies included in the review generated five synthesisedfindings. These synthesised findings were derived from 16study findings that were subsequently aggregated intoseven categories. The five synthesised findings are presentedbelow.
Effect on waiting times. Two studies reported that careprovided by ENP was effective in reducing waiting times fortreatment and overall length of stay in the emergencydepartment.10,20 In Wilson et al.’s study, 96.3% of presenta-tions triaged level 4, and 94.4% of those triaged level 5 wereseen within the time frame recommended by the Australa-sian Triage Scale.10 Patients’ acceptance of being treated byNP was high, and they considered ENP to be a good servicefor minor injuries and were happy to be offered appoint-
ments with them rather than waiting for long periods, espe-cially if it meant waiting all night.20
Scope of practice. In examining diagnostic interventionsprovided, one study found that 51% (n = 51) of patients didnot require any diagnostic treatment.10
Specific treatment provided by emergency NP included:• Pain relief20
• Radiographs: Meek et al. reported that of 49 majordepartments with official NP, 29 (59%) allowed them torequest certain radiographs. All were restricted to limbs,and in all situations there was a minimum age limit.19 Inanother study, 47% (n = 41) of patients required X-raysonly, and 2% (n = 2) required blood investigations inaddition to X-rays.10
• Prescribing: Of 49 major departments in a study by Meeket al., 40 (82%) allowed limited prescribing (dispens-ing).19 Of the 40, all could prescribe tetanus toxoid, 30allowed ‘over the counter’ medication, such as paraceta-mol, and nine allowed ‘prescription only’ items, such asoral antibiotics.19
• Referrals: Incidental data were recorded by Megahy andLloyd as they became apparent during their study.18 Theyincluded the number of X-rays taken, the number ofpositive fractures, the amount of orthopaedic referrals afterX-ray and the number of referrals to the accident andemergency clinic. Referral was found to be appropriateafter accurate diagnosis by the ENP. Their report concludedthat ENP with appropriate training managed minor injuriesappropriately and effectively. Wilson et al. found thatpatients were referred to consultants within the hospital,outpatient clinics and general practitioner for follow up.10
However, 20% of patients did not require referral.Additional procedures reportedly carried out by ENP
included suturing and suture removal, plaster cast applica-tion, dressings, ice-compress and incision and drainage.10
Restrictions to practice. Several papers reported that theENP positions were ‘unofficial’ and that other professionalgroups restricted NP activities.19 Investigating prevalence ofthe role, Meek et al. found that in 202 replies from majordepartments, 60 (30%) used NP. Of the 60, 49 (82%)were ‘official’ NP, and11 were ‘unofficial.’19 Of 140 minor
Cooper et al. (2002)
DerSimonian and Laird Relative Risk (Risk Ratio) Weight (confidence interval 95% random)
1.25% 1.01 (0.06, 15.93)
98.75% 0.86 (0.63, 1.18)
100.00% 0.87 (0.64, 1.18)
Favours ControlFavours Treatment 000
Heterogeneity χ2 = 0.01, P = 0.9203443
88.0
Sakr et al. (1999)
Overall
Overall Z = 0.91, P = 0.3628
Study
Figure 3 Forest plot of significant error in care for patients managed by emergency department nurse practitioners or managed in a minorinjuries unit with junior doctors or patients managed in a traditional accident and emergency department.
Table 2 Summary of two randomised controlled trials comparingsignificant error in care for patients managed by emergency depart-ment nurse practitioners (ENP) or managed in a minor injuries unit(MIU) with junior doctors or patients managed in a traditionalaccident and emergency department (A&E). The table includes thenumber of patients (n) with significant error in each group and thetotal (N) in each group
Study ENP or MIU(significant error)
Junior doctors orA&E (significant error)
n N n N
Cooper et al. (2002)15 1 99 1.00 100Sakr et al. (1999)16 126 1315 191 1447
8 A Wilson et al.
© 2009 The AuthorsJournal Compilation © Blackwell Publishing Asia Pty Ltd

departments which responded, 89 (64%) used NP of which15 (17%) were officially recognised as NP. Major depart-ments were those with 24-h medical cover and receivingambulance trauma cases. All other departments were con-sidered minor.
Meek et al. reported that the NP could prescribe a limitedrange of drugs in 82% of major departments with ‘official’NP, but radiograph requesting was permitted in only 57% ofsuch departments: of those not able to request radiographs,95% blamed radiographers for preventing this.19
One study examining 60 major departments to determinethe professional groups and activities reported to restrict NPactivities the most found that radiographers (n = 31, 52%),legal considerations (n = 14, 23%), doctors in accident andemergency department (A&E) (n = 6, 10%), hospital or trustmanagement practices (n = 4, 6.7%), nurses in A&E (n = 1,1.7%) and other unspecified factors (n = 6, 10%) contrib-uted to restrictions.19 Interestingly, patients were not foundto restrict ENP practice at all.
Satisfaction with care received. Patient satisfaction withthe care received and acceptance of being treated by NPwas generally high in all the studies reporting on thisoutcome.10,18–20 Wilson et al. found patients were pleasedwith the ENP caring attitude, the intent of their listening,kindness, support shown and friendliness. Two studies foundENP to be friendly, understanding, attentive and providehelpful advice.10,20 One study found that over 80% attendingwith minor injuries were happy to be seen by an NP only.19
Another reported patients would use the service again.20
All respondents (n = 151, 83%) to 181 questionnaires inone of the studies agreed that NP introduced themselvesclearly and that they were happy with their treatment andhappy to be seen by an NP again, were given helpful advice,were satisfied with the care received from the NP, and woulduse the service again.18,20 The perception was that staff werehappy, helpful and friendly. In Megahy and Lloyd’s study, sixpeople (4%) commented they would prefer to see a doctor.18
Patients’ confidence in the ENP ability to treat them was highin one of the studies.10 Results showed 84.2% had no doubts,5.3% had some doubts, and 10.5% were uncertain.
Representation within 48 h. One of the studies includedrepresentation within 48 h after the visit with the NP as anoutcome.10 Out of 100 patients, it was noted that six (6%)had revisited within 48 h of their initial treatment.10
Cost-effectiveness. In a prospective study comparing theclinical effectiveness and costs of minor injury services pro-vided by NP, Sakr et al.17 used routine data collected pro-spectively and configured to assess the costs and costconsequences of both models of care. They found therevenue costs were slightly greater in the minor injuries unit(MIU) (£41.10) compared with the A&E (£40.01). With ahigher rate of referral by the ENP, the authors concluded thatthe costs and consequences were greater for MIU cases(£12.7 per minor injury case) compared with A&E depart-ment (£9.66 per minor injury case).
In contrast, Wilson et al. compared patient pathways afterthe implementation of ENP.10 Although the study did notseek to show cost-effectiveness, mapping of patient path-ways showed a greater number of steps and personnelinvolved in the traditional medical assessment.
Discussion
Quality of included studiesThe overall quality of the included studies appears to begenerally low based on the JBI critical appraisal forms. This isbecause the review included study designs other than RCT,which reduced the number of studies that were randomisedand blinded. However, the aim of the review was to identifyhow effective within emergency departments in the hospitalNP could be and if only RCT were included the review wouldonly include comparisons with medical officers. The justifi-cation of including non-RCT was based on developing amore comprehensive understanding of the effectiveness ofNP treating minor injuries.
The overall quality of the included studies was alsoaffected by very few of the included studies comparing likegroups in both characteristics and interventions. This couldbe because in reality only very large and funded studiescould accomplish this. In a field that is hungry for knowledgeand investigation, it is not uncommon for descriptive studiesto dominate. In addition, the differences in role betweencountries of NP do not lend easily to reviews includinginternational works.
Effectiveness of emergency NP managingminor injuriesBased on evidence from nine studies included in this system-atic review, there is no significant difference between theeffectiveness of ENP and junior doctors. There were no com-parative studies between ENP and other health professionalsin the management of minor injuries that could be included.A study comparing ENP with physiotherapists and doctorsdid not meet the inclusion criteria.22 Therefore, this conclu-sion must be interpreted with caution because of the poor tofair methodological study designs used and variable types ofoutcome measures used.
Anecdotally, there does appear to be a significance in thereduction of waiting times for patients to be assessed,waiting times for treatment and overall length of stay times,consequently improving the flow of patients through emer-gency departments.
Reducing the amount of medical officer time spent onspecified presentations logically has an effect in improvingpatient access to interventions, reducing issues of emer-gency department overcrowding and improving patientsatisfaction with health services.
Restrictions to ENP practice were not reported in morecurrent studies, the reason for this being unclear. It is pos-sible that as the roles have become more established andfamiliar organisations and other health professionals aremore comfortable with the nurses’ extended role.
Effective management of minor injuries 9
© 2009 The AuthorsJournal Compilation © Blackwell Publishing Asia Pty Ltd

Limitations of the reviewThe results of this systematic review have been restricted bymultiple factors.
Terminology pertaining to NP and their incumbent roles isambiguous. NP have been active in the USA for over20 years and similarly in the UK, whereas their introductionin Australia is only recent. Commonly, the major character-istic of the role is for the provision of advanced emergencypractice. However, there is a lack of clarity in the works as towhat this entails, the terminology used and the formalappointment and qualifications required to fulfil the role.Whereas every endeavour was made to optimise inclusivity,the heterogeneity made selection of works and comparativeanalysis and synthesis of the data challenging. This issue hasbeen reiterated in a systematic review of the NP role inprimary care.6
Terminology pertaining to the roles within the emergencydepartment and the category of patients reviewed is alsoproblematic. The aim of this review was to investigate therole of the NP in the management of ‘minor injuries’ withinthe emergency department setting. Because of differingtriage scoring systems and diagnostic categories used inemergency departments internationally, collating compa-rable data were again difficult. Even with interventionsgrouped into subcategories, there were still dissimilaritiesamong interventions including how interventions areadministered, recorded and examined. A broad search strat-egy and terms based on a review of known works endeav-oured to address this issue.
The stipulation for inclusion in the review that practicemust only pertain to the treatment of adults in the emer-gency department might be perceived as another limitationof the review. A large case–control study23 found that therewas no difference in median waiting times, treatment timesand length of stay in the emergency department betweenemergency NP care and patients managed by traditionalprocesses. This study might have influenced the overall find-ings of the review; however, the study included children andwas therefore excluded. Similarly, a study by Ball et al. wasexcluded for including children in one of the comparisongroups.22
Horrocks, Anderson and Salisbury identified that the lackof recent RCTs and high-quality observational studiesrestricted their review.6 Our review was also significantlylimited by the lack of large rigorous, carefully designedstudies which evaluated the effectiveness of the NP role.Whereas focus was given to the included RCTs, the data fromobservational and interpretive studies were also included asthese particularly focussed on patient satisfaction, a keyoutcome for investigation. Rigorous and comprehensiveevaluation is pivotal for the development of the NP role inthe emergency department and a body of knowledge whichinforms policy and practice.
Economic analysis of the cost of implementing an NPservice in comparison with standard emergency departmenttreatment was unable to be formally conducted because ofthere being only one study available for inclusion. This is anarea for future research focus as the impetus for implemen-
tation of many NP run minor injuries clinics in the emer-gency department is a reduction of cost. Justification of thisis important if endorsement of the role within the healthsector is to continue.
Conclusion
This systematic review showed that there is no statisticallysignificant difference between the effectiveness of care byENP and junior doctors. Furthermore, no significant differ-ence was evident when various interventions used in theincluded studies were separately compared between TM andemergency NP. It would appear that ENP are effective inreducing patients’ waiting time and length of stay in emer-gency departments and that patients are satisfied with thecare they received. Although some of the studies includedin this review have methodological weaknesses, we haveincluded them as they do provide useful and interestinginformation for clinicians and managers looking at optionsfor improving service delivery.
Implications for practiceThe number of limited quality studies comparing the effec-tiveness of ENP managing minor injury presentations makesit difficult to draw conclusions regarding the most effectivemanagement strategies. The findings of the present reviewsupport the use of NP for the management and treatment ofminor injuries in adults. The results also confirm that imple-menting care by NP can reduce waiting times in the emer-gency department and therefore alleviate complications thatarise from people becoming agitated from waiting for treat-ment. Of importance is that those of greater need are morelikely to be seen by a medical practitioner earlier. The prioritytherefore remains for healthcare to find effective ways ofimproving patient outcomes. Finally, the review emphasisesthe need to ensure in both practice and research that effec-tive nursing practice is implemented.
Implications for researchThe results of the systematic review emphasise the need formore research to assess the effectiveness of interventionsaimed at effective healthcare in emergency departments andin particular that by nurses. Management of minor injuries ispotentially an area where effectiveness both in costs andhealth delivery remains unclear. Research should be of thehighest-quality practicable and explore useful outcomes,such as time saving, minimisation of health personnel andreduction in stress for staff. This will allow for more detailedunderstanding of the feasibility, cost and efficacy of particu-lar interventions.
Acknowledgements
We would like to thank Dr Tim Schultz and Dr Rick Wiechulafor assistance with conducting the systematic reviewprocess.
10 A Wilson et al.
© 2009 The AuthorsJournal Compilation © Blackwell Publishing Asia Pty Ltd

Conflict of interest
The impetus for this review arose from a grant received bythe first author to conduct an evaluation of the RoyalAdelaide Hospital Emergency Department Nurse PractitionerInitiative.
References1. Blunt E. Role and productivity of nurse practitioners in one
urban emergency department. J Emerg Nurs 1998; 24: 234–9.2. Byrne G, Richardson M, Brunsdon J, Patel A. An evaluation of
the care of patients with minor injuries in emergency settings.Accid Emerg Nurs 2000; 8: 101–9.
3. Cole FL, Ramirez E, Mickanin J. ED nurse practitioners’ employ-ment by a physician group versus hospital: pros and cons. JEmerg Nurs 1999; 25: 183–6.
4. Driscoll A, Worrall-Carter L, O’Reilly J, Stewart S. A historicalreview of the nurse practitioner role in Australia. Clin Excell NursePract 2005; 9: 141–52.
5. American Academy of Nurse Practitioners. Position Statementon the Quality of Nurse Practitioner Practice. 2007. Available at:http://www.aanp.org
6. Horrocks S, Anderson E, Salisbury C. Systematic review ofwhether nurse practitioners working in primary care canprovide equivalent care to doctors. BMJ 2002; 324: 819–23.
7. Cole FL, Kleinpell R. Expanding acute care nurse practitionerpractice: focus on emergency department practice. J Am AcadNurse Pract 2006; 18: 187–9.
8. Department of Human Services. Nurse practitioner projectreport (South Australia – Nu Prac Project). Project Report. Ade-laide, SA: Department of Human Services, 1999.
9. Royal Adelaide Hospital. Introduction of an Emergency NursePractitioner. Adelaide, SA: Royal Adelaide Hospital, 2004.
10. Wilson A, Shifaza F. An evaluation of the effectiveness andacceptability of nurse practitioners in an adult emergencydepartment. Int J Nurs Pract 2008; 14: 149–56.
11. Nash K, Zachariah B, Nitschmann J, Psencik B. Evaluation of thefast track unit of a university emergency department. J EmergNurs 2007; 33: 14–20.
12. Pustejovsky A. The growing need for emergency nurse practi-tioners. J Emerg Nurs 1996; 22: 10.
13. American Academy of Nurse Practitioners. Position StatementNurse Practitioner Cost-Effectiveness. 2007. Available at: http://www.aanp.org
14. Pearson A, Porritt KA, Doran D et al. A comprehensive system-atic review of evidence on the structure, process, characteristicsand composition of a nursing team that fosters a healthy workenvironment. Int J Evid Based Healthc 2006; 4: 118–59.
15. Cooper MA, Lindsay GM, Kinn S, Swann IJ. Evaluating emer-gency nurse practitioner services: a randomized controlled trial.J Adv Nurs 2002; 40: 721–30.
16. Sakr M, Angus J, Perrin J, Nixon C, Nicholl J, Wardrope J. Careof minor injuries by emergency nurse practitioners or juniordoctors: a randomised controlled trial. Lancet 1999; 354:1321–6.
17. Sakr M, Kendall R, Angus J, Saunders A, Nicholl J, Wardrope J.Emergency nurse practitioners: a three part study in clinical andcost-effectiveness. Emerg Med J 2003; 20: 158–63.
18. Megahy A, Lloyd M. Managing minor injuries. Emerg Nurse2004; 12: 14–16.
19. Meek SJ, Ruffles G, Anderson J, Ohiorenoya D. Nurse practitio-ners in major accident and emergency departments – a nationalsurvey. J Accid Emerg Med 1995; 12: 177–81.
20. Ritchie L, Dawood M, Whibley P, Sprules V. Meeting the chal-lenge: an evaluation of the ENP clinic. Emerg Nurse 2004; 12:10–13.
21. Jennings N, O’Reilly G, Lee G, Cameron P, Free B, Bailey M.Evaluating outcomes of the emergency nurse practitioner rolein a major urban emergency department, Melbourne, Australia.J Clin Nurs 2008; 17: 1044–50.
22. Ball S, Walton K, Hawes S. Do emergency department physio-therapy practitioner’s, emergency nurse practitioners anddoctors investigate, treat and refer patients with closed muscu-loskeletal injuries differently? Emerg Med J 2007; 24: 185–8.
23. Jjcnoa C, Martin R, Smit D, Winter C, Jenkins J. Emergency nursepractitioner care and emergency department patient flow: casecontrol study. Emerg Med Australas 2006; 18: 385–90.
24. Considine J, Martin R, Smit D, Jenkins J, Winter C. Defining thescope of practice of the emergency nurse practitioner role in ametropolitan emergency department. Int J Nurs Pract 2006; 12:205–13.
Effective management of minor injuries 11
© 2009 The AuthorsJournal Compilation © Blackwell Publishing Asia Pty Ltd

Ap
pen
dix
I–
Incl
ud
edSt
ud
ies
Des
crip
tive
stu
die
s
Stud
yM
etho
dsPa
rtic
ipan
tsM
easu
res
Con
clus
ions
Not
es
Mee
ket
al.,
(199
5)19
Que
stio
nnai
res
nurs
e-in
-cha
rge
Rep
lies
from
357
of46
5fu
nctio
ning
maj
oror
min
orde
par
tmen
ts(7
7%).
Som
enu
rses
wor
kun
offic
ially
asnu
rse
pra
ctiti
oner
sw
ithou
tac
tual
lyho
ldin
gth
etit
le(p
.17
7).
Dep
artm
ents
wer
eas
ked
whe
ther
nurs
esw
ere
‘offi
cial
’or
‘uno
ffici
al’.
Dat
aw
asco
llate
din
tom
ajor
orm
inor
dep
artm
ents
;sp
ecia
lists
dep
artm
ents
wer
eno
tst
udie
das
they
have
alo
ngtr
aditi
onof
nurs
ep
ract
ition
ers
and
asp
ecifi
cca
selo
ad.
Maj
or:
thos
ede
par
tmen
tsha
ving
24hr
resi
dent
med
ical
cove
ran
dre
ceiv
ing
ambu
lanc
etr
aum
aca
ses
–al
loth
ers
cons
ider
edm
inor
.
The
use
ofnu
rse
pra
ctiti
oner
sin
A&
Ede
par
tmen
tsis
incr
easi
ngra
pid
ly.
The
prin
cip
alre
ason
bein
gto
redu
cew
aitin
gtim
es;
how
ever
the
pub
lishe
dev
iden
ceto
sup
por
tth
ison
lyde
mon
stra
tes
atim
esa
ving
inth
ose
pat
ient
sse
ntfo
rra
diog
rap
hs,
alth
ough
41%
ofde
par
tmen
tsw
ithof
ficia
lnur
sep
ract
ition
ers
dono
tal
low
them
tore
que
stra
diol
ogy.
The
grea
tm
ajor
ityof
nurs
ep
ract
ition
ers
have
been
form
ally
trai
ned
for
the
role
.
Old
stud
ybu
tre
leva
ntto
our
obje
ctiv
es.
Seem
sth
atA
ustr
alia
isap
pro
xim
atel
yin
the
pos
ition
ofes
tabl
ishi
ngA
&E
Nur
sep
ract
ition
ersi
mila
rto
the
UK
10ye
ars
ago.
Mog
ahy
and
Lloy
d(2
004)
18Q
uest
ionn
aire
sG
roup
1.A
llp
atie
nts
over
age
of16
,w
hoat
tend
edA
&E
over
one
mon
than
dtr
eate
dby
anu
rse
pra
ctiti
oner
.10
8p
atie
nts
give
nq
uest
ionn
aire
son
com
ple
tion
oftr
eatm
ent
and
befo
redi
scha
rge.
They
hand
edth
emin
asth
eyle
ftth
ede
pt.
Ap
ilot
of25
pat
ient
s.G
roup
2–
A&
Eco
nsul
tant
sin
the
revi
ewcl
inic
who
also
revi
ewed
docu
men
tatio
n.in
terp
reta
tion.
Patie
ntsa
tisfa
ctio
n.W
heth
erm
inor
inju
ries
wer
ebe
ing
man
aged
app
rop
riate
lyan
def
fect
ivel
y.A
ccur
acy
ofra
diog
ragr
aph
inte
rpre
tatio
n
Nur
sep
ract
ition
ers
with
app
rop
riate
trai
ning
man
age
min
orin
jurie
sap
pro
pria
tely
and
effe
ctiv
ely.
With
initi
alan
don
goin
gsu
pp
ort
and
trai
ning
,nu
rse
pra
ctiti
oner
sw
ere
com
pet
ent
inm
anag
ing
inju
ries,
refe
rrin
gto
clin
ics,
req
uest
ing
x-ra
ysap
pro
pria
tely
and
inte
rpre
ting
the
film
sac
cura
tely
.
Tabl
esdi
fficu
ltto
extr
act
resu
lts.
Dat
aco
uld
have
been
mor
ecl
early
pre
sent
ed.
Tabl
eon
clin
ical
refe
rral
audi
tre
sults
show
s57
–60%
agre
emen
tre
ferr
al,
wou
ndm
anag
men
t,x-
ray
req
uest
,cl
ear
&co
ncis
edo
cum
enta
tion
and
accu
rate
x-ra
y
Ritc
hie
etal
.(2
004)
20Q
uest
ionn
aire
sC
ateg
ory
4p
atie
nts
with
min
orin
jurie
sTh
ecl
inic
has
been
asu
cces
san
dha
sco
ntrib
uted
tore
duce
dw
aitin
gtim
esin
Cat
egor
y1
pat
ient
s.It
isal
sore
gard
edw
ellb
yst
aff
who
app
reci
ate
bein
gab
leto
offe
ra
choi
ceof
care
.Th
isle
ssen
the
pot
entia
lfor
ange
ran
dag
gres
sion
This
isa
low
leve
lrep
ort
with
out
desc
riptio
nof
anal
ysis
pro
cedu
res,
ethi
csap
pro
valo
rq
uest
ionn
aire
desi
gnm
etho
ds.
Wils
onan
dSh
ifaza
(200
8)10
Que
stio
nnai
resu
rvey
and
case
note
audi
t.Re
tros
pec
tive
desi
gn
100
Patie
nts
trea
ted
byth
enu
rse
pra
ctiti
oner
tria
ged
with
ATS
cate
gorie
s3–
5in
the
min
orin
jurie
sar
eaof
the
ED.
Con
duct
edca
se-n
ote
audi
tsan
dex
plo
red
pat
ient
satis
fact
ion
with
afte
r-ca
req
uest
ionn
aire
s.O
nehu
ndre
dca
seno
tes
ofp
atie
nts
trea
ted
byth
enu
rse
pra
ctiti
oner
wer
eau
dite
dan
d57
pat
ient
sco
mp
lete
dq
uest
ionn
aire
sex
plo
ring
thei
rsa
tisfa
ctio
nan
dp
erce
ptio
nof
the
care
rece
ived
.
Ana
lysi
sof
the
case
-not
eda
tain
dica
ted
that
the
maj
ority
ofp
rese
ntin
gco
mp
lain
tsw
ere
min
orin
jurie
s.O
fth
ese
inju
ries,
96.3
%of
pre
sent
atio
nstr
iage
dle
vel4
and
94.4
%of
thos
etr
iage
dle
vel5
wer
ese
enw
ithin
the
time
fram
ere
com
men
ded
byth
eA
ustr
alas
ian
Tria
geSc
ale.
46%
ofp
atie
nts
req
uire
dX
-ray
san
d2%
req
uire
dp
atho
logy
test
sdu
ring
thei
rem
erge
ncy
dep
artm
ent
stay
.Th
em
ajor
ityof
pat
ient
sw
ere
satis
fied
with
the
trea
tmen
tre
ceiv
edfr
omth
enu
rse
pra
ctiti
oner
The
stud
yco
nclu
ded
nurs
ep
ract
ition
ers
pro
vide
dan
acce
pta
ble
leve
lof
care
with
asi
gnifi
cant
leve
lof
Incl
uded
asit
addr
ess
the
set
crite
riap
atie
ntsa
tisfa
ctio
n.It
was
note
dth
atnu
rse
pra
ctiti
oner
sp
rovi
dea
diffe
renc
eby
imp
rovi
ngw
aitin
gtim
esan
din
crea
sing
pat
ient
flow
.
12 A Wilson et al.
© 2009 The AuthorsJournal Compilation © Blackwell Publishing Asia Pty Ltd
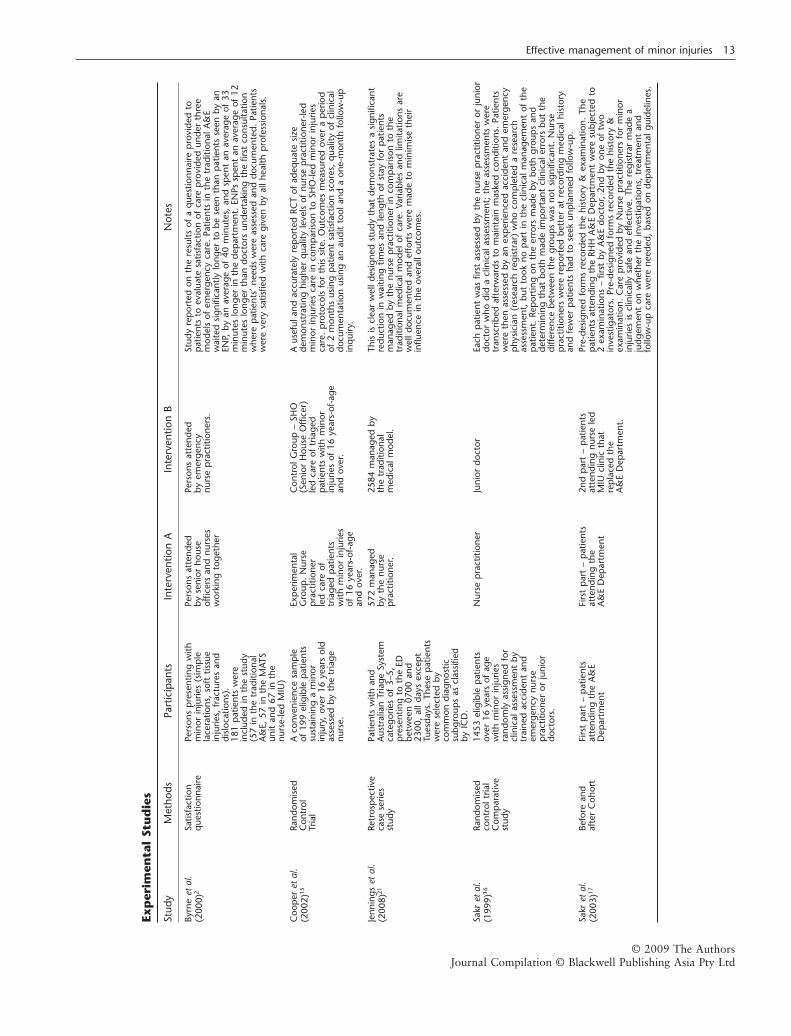
Exp
erim
enta
lSt
ud
ies
Stud
yM
etho
dsPa
rtic
ipan
tsIn
terv
entio
nA
Inte
rven
tion
BN
otes
Byrn
eet
al.
(200
0)2
Satis
fact
ion
que
stio
nnai
rePe
rson
sp
rese
ntin
gw
ithm
inor
inju
ries
(sim
ple
lace
ratio
ns,
soft
tissu
ein
jurie
s,fr
actu
res
and
disl
ocat
ions
).18
1p
atie
nts
wer
ein
clud
edin
the
stud
y(5
7in
the
trad
ition
alA
&E,
57in
the
MAT
Sun
itan
d67
inth
enu
rse-
led
MIU
)
Pers
ons
atte
nded
byse
nior
hous
eof
ficer
san
dnu
rses
wor
king
toge
ther
Pers
ons
atte
nded
byem
erge
ncy
nurs
ep
ract
ition
ers.
Stud
yre
por
ted
onth
ere
sults
ofa
que
stio
nnai
rep
rovi
ded
top
atie
nts
toev
alua
tesa
tisfa
ctio
nof
care
pro
vide
dun
der
thre
em
odel
sof
emer
genc
yca
re.
Patie
nts
inth
etr
aditi
onal
A&
Ew
aite
dsi
gnifi
cant
lylo
nger
tobe
seen
than
pat
ient
sse
enby
anEN
P,by
anav
erag
eof
40m
inut
es,
and
spen
tan
aver
age
of33
min
utes
long
erin
the
dep
artm
ent.
ENPs
spen
tan
aver
age
of12
min
utes
long
erth
ando
ctor
sun
dert
akin
gth
efir
stco
nsul
tatio
nw
here
pat
ient
s’ne
eds
wer
eas
sess
edan
ddo
cum
ente
d.Pa
tient
sw
ere
very
satis
fied
with
care
give
nby
allh
ealth
pro
fess
iona
ls.
Coo
per
etal
.(2
002)
15Ra
ndom
ised
Con
trol
Tria
l
Aco
nven
ienc
esa
mp
leof
199
elig
ible
pat
ient
ssu
stai
ning
am
inor
inju
ry,
over
16ye
ars
old
asse
ssed
byth
etr
iage
nurs
e.
Exp
erim
enta
lG
roup
.N
urse
pra
ctiti
oner
led
care
oftr
iage
dp
atie
nts
with
min
orin
jurie
sof
16ye
ars-
of-a
gean
dov
er.
Con
trol
Gro
up–
SHO
(Sen
ior
Hou
seO
ffice
r)le
dca
reof
tria
ged
pat
ient
sw
ithm
inor
inju
ries
of16
year
s-of
-age
and
over
.
Aus
eful
and
accu
rate
lyre
por
ted
RCT
ofad
equa
tesi
zede
mon
stra
ting
high
erq
ualit
yle
vels
ofnu
rse
pra
ctiti
oner
-led
min
orin
jurie
sca
rein
com
par
ison
toSH
O-le
dm
inor
inju
ries
care
.p
roto
cols
for
this
site
.O
utco
mes
mea
sure
dov
era
per
iod
of2
mon
ths
usin
gp
atie
ntsa
tisfa
ctio
nsc
ores
,q
ualit
yof
clin
ical
docu
men
tatio
nus
ing
anau
dit
tool
and
aon
e-m
onth
follo
w-u
pin
qui
ry.
Jenn
ings
etal
.(2
008)
21Re
tros
pec
tive
case
serie
sst
udy
Patie
nts
with
and
Aus
tral
ian
Tria
geSy
stem
cate
gorie
sof
3–5,
pre
sent
ing
toth
eED
betw
een
0700
and
2300
,al
lday
sex
cep
tTu
esda
ys.
Thes
ep
atie
nts
wer
ese
lect
edby
com
mon
diag
nost
icsu
bgro
ups
ascl
assi
fied
byIC
D.
572
man
aged
byth
enu
rse
pra
ctiti
oner
.
2584
man
aged
byth
etr
aditi
onal
med
ical
mod
el.
This
iscl
ear
wel
ldes
igne
dst
udy
that
dem
onst
rate
sa
sign
ifica
ntre
duct
ion
inw
aitin
gtim
esan
dle
ngth
ofst
ayfo
rp
atie
nts
man
aged
byth
enu
rse
pra
ctiti
oner
inco
mp
aris
onto
the
trad
ition
alm
edic
alm
odel
ofca
re.
Varia
bles
and
limita
tions
are
wel
ldoc
umen
ted
and
effo
rts
wer
em
ade
tom
inim
ise
thei
rin
fluen
cein
the
over
allo
utco
mes
.
Sakr
etal
.(1
999)
16Ra
ndom
ised
cont
rolt
rial
Com
par
ativ
est
udy
1453
elig
ible
pat
ient
sov
er16
year
sof
age
with
min
orin
jurie
sra
ndom
lyas
sign
edfo
rcl
inic
alas
sess
men
tby
trai
ned
acci
dent
and
emer
genc
ynu
rse
pra
ctiti
oner
orju
nior
doct
ors.
Nur
sep
ract
ition
erJu
nior
doct
orEa
chp
atie
ntw
asfir
stas
sess
edby
the
nurs
ep
ract
ition
eror
juni
ordo
ctor
who
did
acl
inic
alas
sess
men
t;th
eas
sess
men
tsw
ere
tran
scrib
edaf
terw
ards
tom
aint
ain
mas
ked
cond
ition
s.Pa
tient
sw
ere
then
asse
ssed
byan
exp
erie
nced
acci
dent
and
emer
genc
yp
hysi
cian
(res
earc
hre
gist
rar)
who
com
ple
ted
are
sear
chas
sess
men
t,bu
tto
okno
par
tin
the
clin
ical
man
agem
ent
ofth
ep
atie
nt.
Rep
ortin
gon
the
erro
rsm
ade
bybo
thgr
oup
san
dde
term
inin
gth
atbo
thm
ade
imp
orta
ntcl
inic
aler
rors
but
the
diffe
renc
ebe
twee
nth
egr
oup
sw
asno
tsi
gnifi
cant
.N
urse
pra
ctiti
oner
sw
ere
rep
orte
dbe
tter
atre
cord
ing
med
ical
hist
ory
and
few
erp
atie
nts
had
tose
ekun
pla
nned
follo
w-u
p.
Sakr
etal
.(2
003)
17Be
fore
and
afte
rC
ohor
tFi
rst
par
t–
pat
ient
sat
tend
ing
the
A&
ED
epar
tmen
t
Firs
tp
art
–p
atie
nts
atte
ndin
gth
eA
&E
Dep
artm
ent
2nd
par
t–
pat
ient
sat
tend
ing
nurs
ele
dM
IUcl
inic
that
rep
lace
dth
eA
&E
Dep
artm
ent.
Pre-
desi
gned
form
sre
cord
edth
ehi
stor
y&
exam
inat
ion.
The
pat
ient
sat
tend
ing
the
RHH
A&
ED
epar
tmen
tw
ere
subj
ecte
dto
2ex
amin
atio
ns–
first
byA
&E
doct
or,
2nd
byon
eof
two
inve
stig
ator
s.Pr
e-de
sign
edfo
rms
reco
rded
the
hist
ory
&ex
amin
atio
n.C
are
pro
vide
dby
Nur
sep
ract
ition
ers
for
min
orin
jurie
sis
clin
ical
lysa
fean
def
fect
ive.
The
regi
stra
rm
ade
aju
dgem
ent
onw
heth
erth
ein
vest
igat
ions
,tr
eatm
ent
and
follo
w-u
pca
rew
ere
need
ed,
base
don
dep
artm
enta
lgui
delin
es.
Effective management of minor injuries 13
© 2009 The AuthorsJournal Compilation © Blackwell Publishing Asia Pty Ltd

Appendix II – Excluded Studies
Descriptive StudiesMarr S, Steele K, Swallow V, Craggs S, Procter S, Newton J, Sen B,
McNabb A. Mapping the range and scope of emergency nursepractitioner services in the Northern and Yorkshire Region: atelephone survey.
Reason for Exclusion: Doesn’t address the effect on patientoutcomes of nurse practitioner services.
Meite S, Moser MS, Riyad BA, van Beek CA. Attitude of EmergencyDepartment Patients with Minor Problems to being Treated bya Nurse Practitioner.
Reason for Exclusion: Survey of opinion- they had a hypotheti-cal willingness to be treated. But none were actually treated bynurse practitioners.
Mills AC, McSweeney M. Primary Reasons for Emergency Depart-ment Visits and Procedures Performed for Patients who sawNurse practitioners.
Reason for Exclusion: identifies presenting complaints – ascoping study of types of injuries seen by nurse practitioners.
Norris T, Melby V. The Acute Care Nurse practitioner: challengingexisting boundaries of emergency nurses in the UnitedKingdom.
Reason for Exclusion: Opinion study only.Read S, Jones NMB, Williams BT. Nurse practitioners in Accident and
Emergency Departments: what do they do?Reason for Exclusion: Comparative study of nurse practitioners
and MDs over 2 days in an emergency department-noeffectiveness.
Rhee KJ, Dermyer AL. Patient satisfaction with a nurse practitioner ina university emergency service.
Reason for Exclusion: Minimal reporting on the data and howconclusions were reached; low level analysis.
Sheahan SL. Documentation of Health Risks and Health PromotionCounseling by Emergency Department Nurse practitioners andPhysicians.
Reason for Exclusion: Does not meet our review question/objectives – focuses on identification of health risks and healthpromotion counselling by emergency department nurse prac-titioner.
Wright, Erwin, Blanton & Covington, Fast Track in the EmergencyDepartment: A one-year experience with nurse practitioners.
Reason for Exclusion: Poor research design. Conclusions inad-equately supported.
Experimental StudiesBall, STE, Walton, K and Hawes, S. Do emergency department
physiotherapy practitioners, emergency nurse practitioners,and doctors investigate, treat and refer patients with closedmusculoskeletal injuries differently?
Reason for Exclusion: Focused on the role of the physiotherapypractitioner in comparison with the emergency nurse practitio-ner and the medical officer.
Considine, J., R. Martin, et al. Emergency nurse practitioner care andemergency department patient flow: case-control study.
Reason for Exclusion: Paediatric inclusion and the study was areview of the new role of nurse practitioners rather than aeffectiveness study.
Considine, J., R. Martin, et al. Defining the scope of practice of theemergency nurse practitioner role in a metropolitan emergencydepartment.
Reason for Exclusion: Did not fit inclusion criteria.
14 A Wilson et al.
© 2009 The AuthorsJournal Compilation © Blackwell Publishing Asia Pty Ltd