
The Christie NHS Foundation Trust NZIMRT: Hamilton 30 th Aug 2013 BROOKLYN 2 RADIOTHERAPY Carl...
58
The Christie NHS Foundation Trust NZIMRT: Hamilton 30 th Aug 2013 BROOKLYN 2 RADIOTHERAPY Carl ROWBOTTOM Fri 30 th Aug 2013 Session 4 / Talk 2 15:35 – 16:20 ABSTRACT Image-guided radiotherapy provides a wealth of information regarding how patient anatomy changes during a course of radiotherapy treatment. This fundamentally changes the treatment planning process from a single time-point in the patient pathway to a more reactive process where plans are assessed using new anatomical information as it becomes available, and new treatment plans generated as required. The increased use of image-guided radiotherapy requires much greater co-ordination and communication between treatment planning and treatment delivery staff, as well as software solutions to streamline the workflow necessary for assessment and re-planning during treatment. A review of data at The Christie in Manchester has shown that around 20% of patients receiving image-guided radiotherapy require a review due to patient changes at least once during their treatment. However, every time a treatment plan is generated there is a small risk that there will be a deviation between the treatment delivered and that intended. International estimates show that treatment deviations occur 2-3% of the time. With this in mind a structured workflow and clear decision rules have been developed at The Christie to ensure that new treatment plans are generated for those patients where the benefit to the patient outweighs any potential risks from deviations.
-
Upload
molly-gilmore -
Category
Documents
-
view
217 -
download
0
Transcript of The Christie NHS Foundation Trust NZIMRT: Hamilton 30 th Aug 2013 BROOKLYN 2 RADIOTHERAPY Carl...

The Christie NHS Foundation TrustNZIMRT: Hamilton 30th Aug 2013
BROOKLYN 2
RADIOTHERAPY
Carl ROWBOTTOM
Fri 30th Aug 2013
Session 4 / Talk 2
15:35 – 16:20
ABSTRACTImage-guided radiotherapy provides a wealth of information regarding how patient anatomy changes during a course of radiotherapy treatment. This fundamentally changes the treatment planning process from a single time-point in the patient pathway to a more reactive process where plans are assessed using new anatomical information as it becomes available, and new treatment plans generated as required. The increased use of image-guided radiotherapy requires much greater co-ordination and communication between treatment planning and treatment delivery staff, as well as software solutions to streamline the workflow necessary for assessment and re-planning during treatment. A review of data at The Christie in Manchester has shown that around 20% of patients receiving image-guided radiotherapy require a review due to patient changes at least once during their treatment. However, every time a treatment plan is generated there is a small risk that there will be a deviation between the treatment delivered and that intended. International estimates show that treatment deviations occur 2-3% of the time. With this in mind a structured workflow and clear decision rules have been developed at The Christie to ensure that new treatment plans are generated for those patients where the benefit to the patient outweighs any potential risks from deviations.

The Christie NHS Foundation TrustNZIMRT: Hamilton 30th Aug 2013
Treatment Planning in a Changing World
Carl Rowbottom PhDRadiotherapy Physics Group LeaderThe Christie NHS Foundation Trust,
Manchester

The Christie NHS Foundation TrustNZIMRT: Hamilton 30th Aug 2013
Manchester?

The Christie NHS Foundation TrustNZIMRT: Hamilton 30th Aug 2013
The Christie
• One of only 3 specialist cancer hospitals in England
• Largest single site comprehensive cancer centre in Europe
• One of the largest radiotherapy services in Europe • Serves population of 3.2 million people• Only radiotherapy provider for the catchment area

The Christie NHS Foundation Trust
Radiotherapy in Manchester
• The Radiotherapy department employs:• 35 clinical oncologists• 32 physicists• 34 dosimetrists• 19 linac engineers• 110 treatment radiographers
• Treat ~ 8500 patients per year • ~ 5,500 radical treatments per year• ~100,000 radiotherapy fractions
each year (2-3% growth per year)

The Christie NHS Foundation Trust
Radiotherapy in Manchester
• 16 linear accelerators across three sites• 12 machines at the main site• 2 satellite centres with two
machines each• All treatment planning on main site
• 12 elekta linacs, 4 varian linacs• 12 with IGRT• 10 with VMAT
• All external beam planning on Pinnacle• ~450 treatment plans per month• ~120 inverse planned IMRT per
month • ~ 80 breast IMRT (field-in-field) per
month

The Christie NHS Foundation TrustNZIMRT: Hamilton 30th Aug 2013
The future of medicine & radiotherapy

The Christie NHS Foundation TrustNZIMRT: Hamilton 30th Aug 2013
Traditional Medicine

The Christie NHS Foundation TrustNZIMRT: Hamilton 30th Aug 2013
The Future of Medicine

The Future of Radiotherapy?
Personalised Radiotherapy
• Individualised plan
• Image-guided treatment
• Plan adaptation as required

The Christie NHS Foundation TrustNZIMRT: Hamilton 30th Aug 2013
IGRT creates need for adaptive radiotherapy
• Patient anatomy changes are more easily visualised by IGRT.
• Patient set-up can be corrected for, but what is the dosimetric consequence of the anatomical change?• Requires visualisation of the plan on the new
anatomy. • Drinking from the firehose?

Patients change during treatment shock…….

Patients change during treatment shock…….

Patients change during treatment shock…….

Patients change during treatment shock…….

The Christie NHS Foundation TrustNZIMRT: Hamilton 30th Aug 2013
What is adaptive radiotherapy?

The Christie NHS Foundation TrustNZIMRT: Hamilton 30th Aug 2013
Defining Adaptive Radiotherapy?
• There is no clear definition of adaptive radiotherapy
• My personal view• Any new treatment plan that is created and
used due to physical or biological changes of the patient is adaptive radiotherapy
• Can be either a pro-active or reactive process

The Christie NHS Foundation TrustNZIMRT: Hamilton 30th Aug 2013
How many patients will it affect?

The Christie NHS Foundation TrustNZIMRT: Hamilton 30th Aug 2013
• 160/772 (20.7%) Patients required a review by Radiotherapy Planning
What is the consequence of IGRT based Radiotherapy?
Frequency of Request for Planning Review
213
150
66
86
27 25
45
15
69
359
12 8
12
0
50
100
150
200
250
PROSTATE n= 228 LUNG n= 219 H+N n= 101 OESOPHAGUSn=95
PANCREAS n= 39 BLADDER n= 33 OTHER = 57
Num
ber
of patients
tre
ate
d
Patients NOT requiring review Patients referred for review
6.6%31.5%
34.7% 9.5%
30.8% 24.2%
21.1%

The Christie NHS Foundation TrustNZIMRT: Hamilton 30th Aug 2013
What is the consequence of IGRT based Radiotherapy?
• Tanyi & Fuss……• 34 out of 146 patients required re-planning at least
once during the course of treatment (23.3%)
• Christie experience…..• 35 out of 160 patients required a replan (21.9%)• 35 replans needed from 772 patients (4.5%)
• Why the differences between Tanyi&Fuss and Christie?
Taken from Tanyi & Fuss, Acta Oncologica, 47, 1444-1453 (2008)

The Christie NHS Foundation TrustNZIMRT: Hamilton 30th Aug 2013
Are we increasing risk to the patient with reactive planning?
• International estimates* show deviations from prescribed treatment ~0.5% of fractions• Most errors occur at handover points, e.g. treatment
plan to treatment execution (interpretation of treatment intent to treatment)
• Error rate per treatment course….. 1-3%
• Adaptive radiotherapy ≡ increase in treatment courses?
• How do we ensure adaptive radiotherapy doesn’t lead to 6-fold increase in errors?
*Marks et al, IJROBP, 69(5):1579-1586 (2007)

The Christie NHS Foundation TrustNZIMRT: Hamilton 30th Aug 2013
• Only adapt treatment if it is likely to significantly improve patient outcome• develop clear decision rules…….
• Is (serial-) OAR dose going to exceed tolerance?
• Is tumour dose within ±3%?
• When adapting treatment build quality in to the process (Deming process system approach)• standardise process steps wherever possible
• minimise number of process steps
• do not rely on inspection for quality
Are we increasing risk to the patient with reactive planning?

The Christie NHS Foundation TrustNZIMRT: Hamilton 30th Aug 2013
Improving adaptive radiotherapy workflow

The Christie NHS Foundation TrustNZIMRT: Hamilton 30th Aug 2013
The Goal of Adaptive Radiotherapy - Physical
Patient anatomy information (IGRT)
Fast/Accurate planning(original plan on new anatomy)
Fast/Accurate re-plan (new plan on new anatomy)
New treatment record(accumulated dose of plan to changing anatomy)
Changes belowtrigger level
Changes above
trigger level
Delivery of newplan & new IGRT
New treatment record(including treatmentalready delivered)
Independent/Automaticsafety check (no verification)
Accurate/Reliable plan evaluationincluding previous treatmentfractions (deformable dose
accumulation)

The Christie NHS Foundation TrustNZIMRT: Hamilton 30th Aug 2013
Workflow examples
Example 1: New CT scan & replan at set time point during treatment
(e.g. H&N adaptive planning)

Workflow Headaches – Adaptive planning
Original CT ScanROIs, IMRT objectives, Plan, Dose
New CT Scan
Add new planNew CT Scan as Primary
Original CT Scan as Secondary
Load PlanImport Original CT Scan ROIs
Fuse Images (rigid body registration)Copy ROIs on to New CT Scan
Clinician modifies ROIs on New CT Scan
Start New Plan

The Christie NHS Foundation TrustNZIMRT: Hamilton 30th Aug 2013
Workflow Headaches - ReplanningOriginal CT Scan
ROIs, IMRT objectives, Plan, DoseNew CT Scan
Copy Original Plan to New CT ScanAutomatically fuse images (rigid body registration)
Automatically deform ROIs from Original CT Scan to New CT Scan
Clinician checks ROIs on New CT Scan
Modifies (if necessary)
Plan Modification

The Christie NHS Foundation TrustNZIMRT: Hamilton 30th Aug 2013

The Christie NHS Foundation TrustNZIMRT: Hamilton 30th Aug 2013
Workflow examples
Example 2: Reactive planning (e.g. react to patient changes on
treatment as required – using CBCT)

The Christie NHS Foundation TrustNZIMRT: Hamilton 30th Aug 2013
Workflow examples
Example 2: Reactive planning (e.g. react to patient changes on
treatment as required – using CBCT)
But first an aside on using CBCT for reactive planning........

The Christie NHS Foundation TrustNZIMRT: Hamilton 30th Aug 2013
Why use CBCT-based IGRT for adaptive therapy?
• CBCT is likely to be performed for verification of patient position. • Radiation dose has already been given to the patient.• Patient is definitely in the treatment position.
• Truly adaptive therapy involves assessing patient anatomy on a given fraction and adapting when necessary. • No waiting for new CT scan. • No treatment gaps waiting for new treatment plan.

The Christie NHS Foundation TrustNZIMRT: Hamilton 30th Aug 2013
Challenges with use of CBCT for ART
• Imaging protocols often designed for geometric verification only• Low dose scans (ALARA)
• Is image quality sufficient for delineating normal tissues?
• Small or Medium field of view – incomplete patient outline
• Can the treatment plan be re-calculated?
• Two-stage imaging protocols• Small FoV and low image quality (&dose) if patient
anatomy is stable• Larger FoV and higher image quality (&dose) if
patient anatomy is changing

• Small FOV and half rotation CBCT scan.
• Adequate for verification of patient set-up
• Adequate for treatment planning?

The Christie NHS Foundation TrustNZIMRT: Hamilton 30th Aug 2013
Challenges with use of CBCT for ART
• CT numbers are unreliable for treatment planning purposes• Even with calibration procedures CT numbers from CBCT
are influenced by the patient size compared to the phantom size used for calibration
• If going to use CBCT scans for re-calculation need to have methodology for ensuring accuracy of electron/physical density information

The Christie NHS Foundation TrustNZIMRT: Hamilton 30th Aug 2013
CT Number change due to scatter differences…
• Small FoV• Adding 1.5cm
of bolus around the CatPhan phantom decreases the CBCT pixel value by 60 – 120 in soft tissue range
CT Vs Density
0
500
1000
1500
2000
2500
0 500 1000 1500 2000 2500
CT density values
CB
CT
pix
el v
alu
es
No Bolus
1 layer
3 layers

The Christie NHS Foundation TrustNZIMRT: Hamilton 30th Aug 2013
CT Number change due to scatter differences…
Thing et al, Acta Oncologica, 2013

The Christie NHS Foundation TrustNZIMRT: Hamilton 30th Aug 2013
Improving CBCT Images for use in Adaptive Radiotherapy
Thing et al, Acta Oncologica, 2013
• Pre-processing projections prior to reconstruction• Use monte-carlo to predict scatter per projection &
subtract. • Monte carlo........• (Thing et al, Acta Oncologica, 2013)


Improving CBCT Images for use in Adaptive Radiotherapy
Marchant et al, PMB, 53, pp5719-5733 (2008)
• Post-processing images after reconstruction.• Use the planning CT scan
to provide a coarse correction to the cone-beam images after reconstruction

The Christie NHS Foundation TrustNZIMRT: Hamilton 30th Aug 2013
Workflow examples
Example 2: Reactive planning (e.g. react to patient changes on
treatment as required – using CBCT)
The Christie NHS Foundation TrustNZIMRT: Hamilton 30th Aug 2013
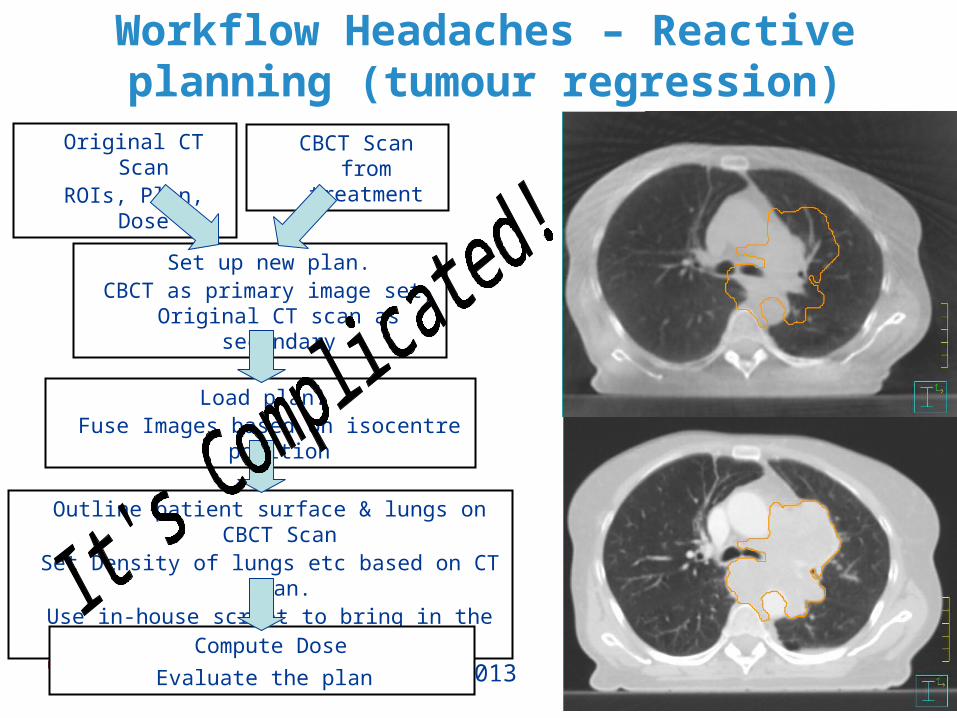
Workflow Headaches – Reactive planning (tumour regression)
Original CT ScanROIs, Plan, Dose
CBCT Scan from treatment
Set up new plan.CBCT as primary image set, Original CT scan as secondary
Load plan. Fuse Images based on isocentre position
Outline patient surface & lungs on CBCT ScanSet Density of lungs etc based on CT Scan.
Use in-house script to bring in the original plan
Compute Dose
Evaluate the plan

The Christie NHS Foundation TrustNZIMRT: Hamilton 30th Aug 2013

The Christie NHS Foundation TrustNZIMRT: Hamilton 30th Aug 2013
Challenges in the adaptive radiotherapy process

The Christie NHS Foundation TrustNZIMRT: Hamilton 30th Aug 2013
• How do we change a treatment plan following tumour regression during radiotherapy treatment?
• Questions to consider• Is microscopic disease still present?• Elastic or non-elastic regression?
Clinical challenge – Reactive planning (tumour regression)

The Christie NHS Foundation TrustNZIMRT: Hamilton 30th Aug 2013
Clinical Challenge – Reactive planning (tumour regression)
Rit et al, ICCR, 2010

The Christie NHS Foundation TrustNZIMRT: Hamilton 30th Aug 2013
Clinical Headaches – Reactive planning (tumour regression)
Sonke & Belderos, Semin Radiat Oncol, 20:94-106, 2010

The Christie NHS Foundation TrustNZIMRT: Hamilton 30th Aug 2013
The Goal of Adaptive Radiotherapy
Patient anatomy information (IGRT)
Fast/Accurate planning(original plan on new anatomy)
Fast/Accurate re-plan (new plan on new anatomy)
New treatment record(accumulated dose of plan to changing anatomy)
Changes belowtrigger level
Changes above
trigger level
Delivery of newplan & new IGRT
New treatment record(including treatmentalready delivered)
Independent/Automaticsafety check (no verification)
Accurate/Reliable plan evaluationincluding previous treatmentfractions (deformable dose
accumulation)

The Christie NHS Foundation TrustNZIMRT: Hamilton 30th Aug 2013
Deformable Registration ≠ Dose Accumulation
• Deformable registration algorithms balance image similarity with physically realistic deformations• No tears or folds in the
image rather than bio-mechanical limitations
• >7% of pixels >3mm in error
• >2% of pixels >7mm in error• Are these error levels
acceptable for use in treatment decisions? Kirby et al, Med Phys, 40(1):011702
(2013)

The Christie NHS Foundation TrustNZIMRT: Hamilton 30th Aug 2013
The Goal of Adaptive Radiotherapy
Patient anatomy information (IGRT)
Fast/Accurate planning(original plan on new anatomy)
Fast/Accurate re-plan (new plan on new anatomy)
New treatment record(accumulated dose of plan to changing anatomy)
Changes belowtrigger level
Changes above
trigger level
Delivery of newplan & new IGRT
New treatment record(including treatmentalready delivered)
Independent/Automaticsafety check (no verification)
Accurate/Reliable plan evaluationincluding previous treatmentfractions (deformable dose
accumulation)

The Christie NHS Foundation TrustNZIMRT: Hamilton 30th Aug 2013
Going beyond anatomical adaptive radiotherapy
• So far adaptive radiotherapy has been performed within the anatomical domain• Mixed success in literature from purely anatomical
approach• Patient heterogeneity may predominant dose variation
• What if adaptive radiotherapy was based on biological changes during treatment?• Is there any supporting evidence for this approach?

• Can we use pre-treatment MR to guide the adaptive RT process?
• Example of prognostic indicator in gynaecological cancer.......• 50 patients with cervix carcinoma• DCE-MRI before radiotherapy
• Measured enhancing fraction (EF) of tumour
Going beyond anatomical adaptive radiotherapy

The Christie NHS Foundation TrustNZIMRT: Hamilton 30th Aug 2013
Going beyond anatomical adaptive radiotherapy

The Christie NHS Foundation TrustNZIMRT: Hamilton 30th Aug 2013
Going beyond anatomical adaptive radiotherapy

The Christie NHS Foundation TrustNZIMRT: Hamilton 30th Aug 2013
Going beyond anatomical adaptive radiotherapy – the Steinbeck study?
• Study of 32 mice with human prostate xenografts. • Receiving androgen deprivation therapy and/or radiotherapy• Repeat DW-MRI and DCE-MRI give apparent diffusion
coefficient (ADC) and vascular biomarker (Ktrans)• Treatment response measured 30 days posts RT (tumour
volume)

The Christie NHS Foundation TrustNZIMRT: Hamilton 30th Aug 2013
Going beyond anatomical adaptive radiotherapy – the Steinbeck study

The Christie NHS Foundation TrustNZIMRT: Hamilton 30th Aug 2013
Going beyond anatomical adaptive radiotherapy – the Steinbeck study

The Christie NHS Foundation TrustNZIMRT: Hamilton 30th Aug 2013
Going beyond anatomical adaptive radiotherapy – the Steinbeck study
(from mice to men)• High-risk prostate cancer patients......• If we can predict tumour response from MR imaging (DW & DCE-MRI)......
• Can we predict normal tissue response?• Can we stratify prostate cancer patients?• Can we modify treatment after 2 weeks of radiotherapy?
• Escalation/de-escalation?• Normal tissue dose modification?
• Pilot study (20 patients) to begin in 2014

The Christie NHS Foundation TrustNZIMRT: Hamilton 30th Aug 2013
“Data is not information, information is not knowledge, knowledge is not understanding, understanding is not wisdom”
Clifford Stoll




![Rowbottom - Liver Function Assessment [2]](https://static.fdocuments.in/doc/165x107/577cc8681a28aba711a2bc56/rowbottom-liver-function-assessment-2.jpg)












