The Children’s Early Warning Tool (PDF 1470 KB) · The Children’s Early Warning Tool ... CEWT...
30
The Children’s Early Warning Tool Kevin McCaffery Staff Specialist in Paediatric Intensive Care, Brisbane Senior Medical Advisor, Patient Safety Centre, Brisbane
Transcript of The Children’s Early Warning Tool (PDF 1470 KB) · The Children’s Early Warning Tool ... CEWT...
The Children’s Early Warning Tool
Kevin McCaffery
Staff Specialist in Paediatric Intensive Care, BrisbaneSenior Medical Advisor, Patient Safety Centre, Brisbane

Objective• To design a suite of tools to meet the needs of
bedside clinicians
• Observation chart
• Reference ranges for age
• Early warning score
• Clinical escalation
• Tool to assess interventions
• Triage tool
• Customisable

Design
• Blank canvas
• What observations predict deterioration?• Normal ranges for age?
• Single point vs. cumulative score? (both…?)
• Weighting of observations
• What observations – pragmatic
• Human factors approach to design



Validation• Retrospective
• All patients admitted PICU from ward in 2007• CEWT detected patients before PICU admission
• Prospective• Twelve pilot sites (tertiary / regional / rural)• Two month trial• Phased roll-out
• Retrieval population
• Root Cause Analysis
• Semi-qualitative implementation study

Retrospective validationICU admissions
0
1
2
3
4
5
6
7
8
9
10
11
-48 -45 -42 -39 -36 -33 -30 -27 -24 -21 -18 -15 -12 -9 -6 -3 0
time (hours)
CEW
T sc
ore
bronchiolitis n=20pneumonia n=5reactive airways n=4sepsis n=14

CEWT – BronchiolitisICU admissions: bronchiolitis
0
1
2
3
4
5
6
7
8
-48 -45 -42 -39 -36 -33 -30 -27 -24 -21 -18 -15 -12 -9 -6 -3 0
time (hours)
CEW
T sc
ore
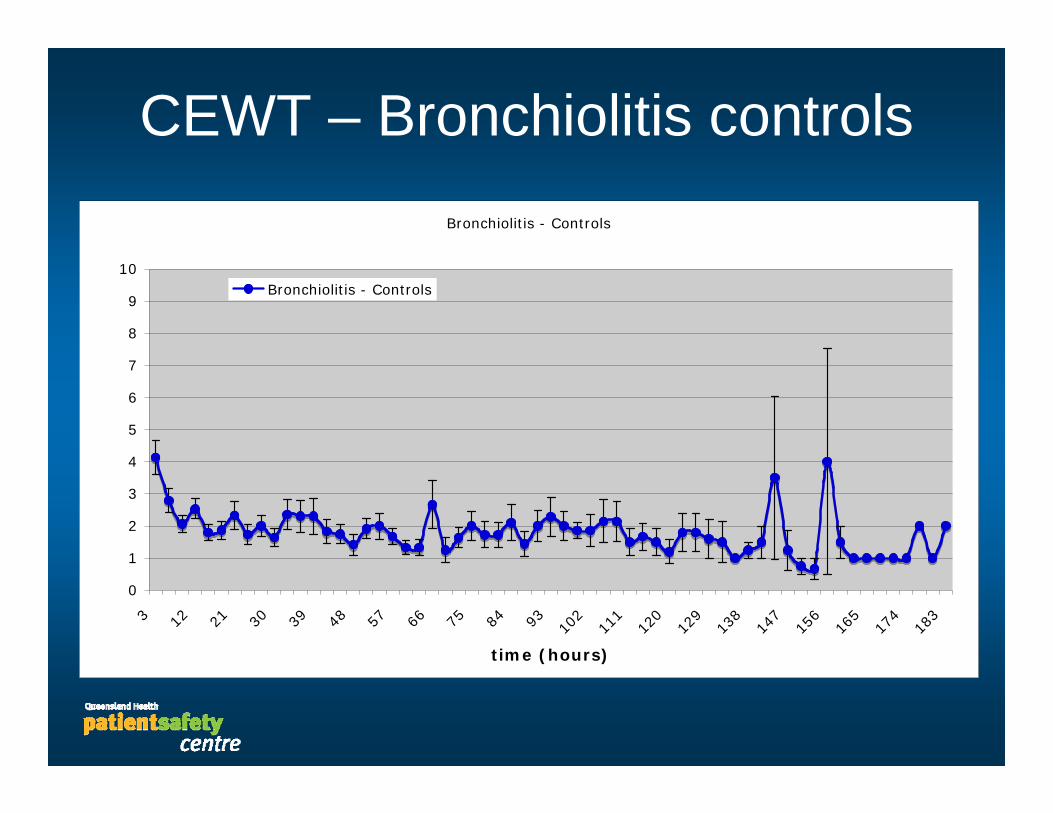
CEWT – Bronchiolitis controlsBronchiolitis - Controls
0
1
2
3
4
5
6
7
8
9
10
3 12 21 30 39 48 57 66 75 84 93 102
111
120
129
138
147
156
165
174
183
time (hours)
Bronchiolitis - Controls

Prospective trial
• Approximately 1900 patients
• Currently analysing data• Optimise physiological weighting
• Optimise action box (for different institutional capabilities)
• Impression is that scoring seems appropriate
• Two critical incidents• Patients had respiratory arrests
• In both cases, CEWT had been overruled by registrar
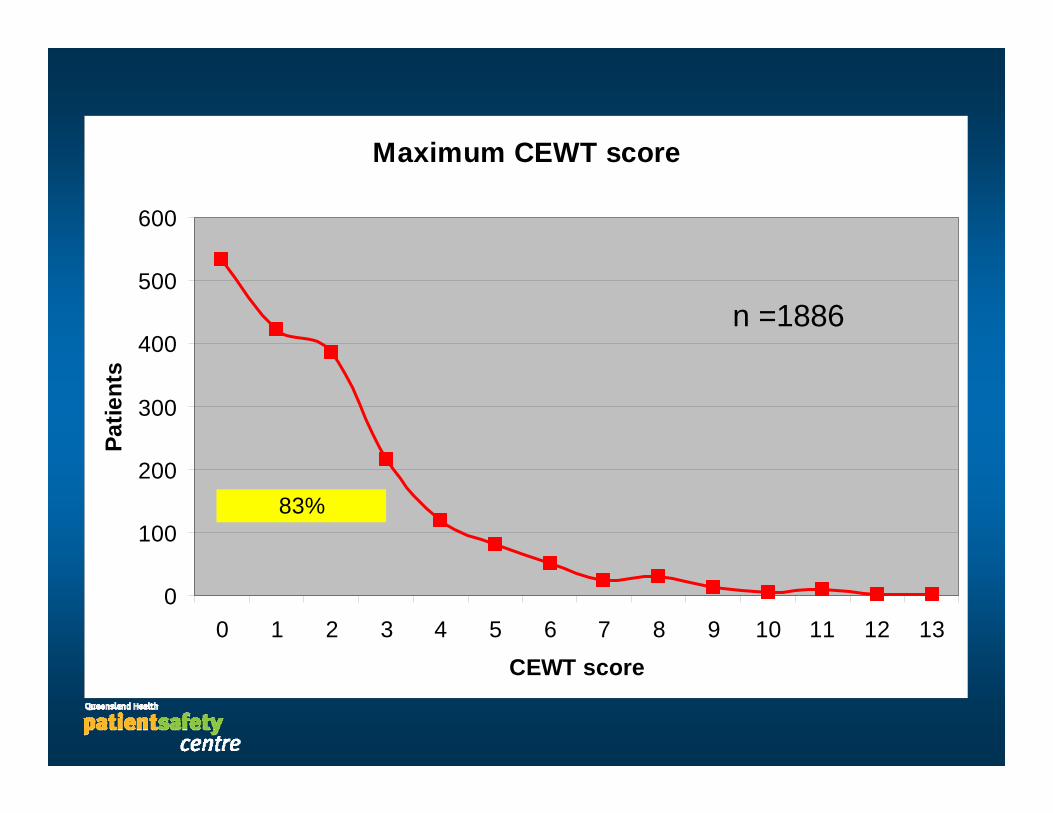
Maximum CEWT score
0
100
200
300
400
500
600
0 1 2 3 4 5 6 7 8 9 10 11 12 13CEWT score
Patie
nts
83%
n =1886

CEWT scores by centre
0
20
40
60
80
100
120
140
160
0 1 2 3 4 5 6 7 8 9 10 11 12 13
CEWT score
Patie
nts
TertiaryRegional 1Regional 2Regional 3Regional 4Regional 5Rural
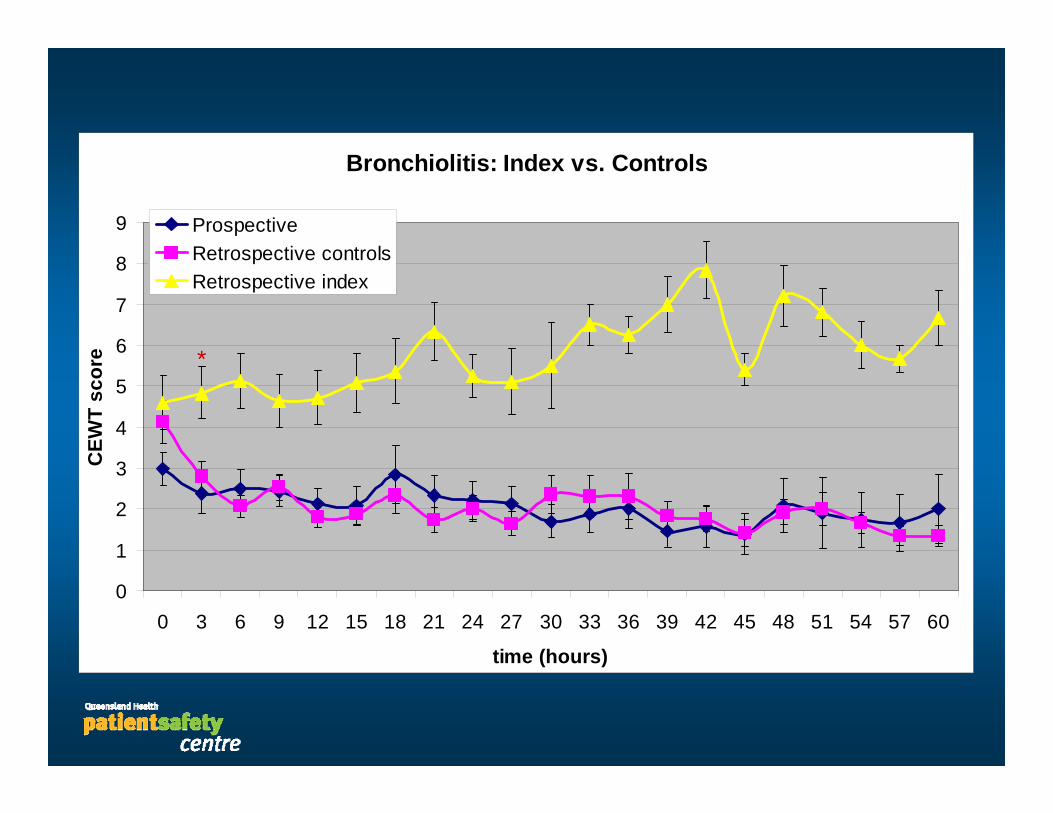
Bronchiolitis: Index vs. Controls
0
1
2
3
4
5
6
7
8
9
0 3 6 9 12 15 18 21 24 27 30 33 36 39 42 45 48 51 54 57 60
time (hours)
CEW
T sc
ore
ProspectiveRetrospective controlsRetrospective index
*
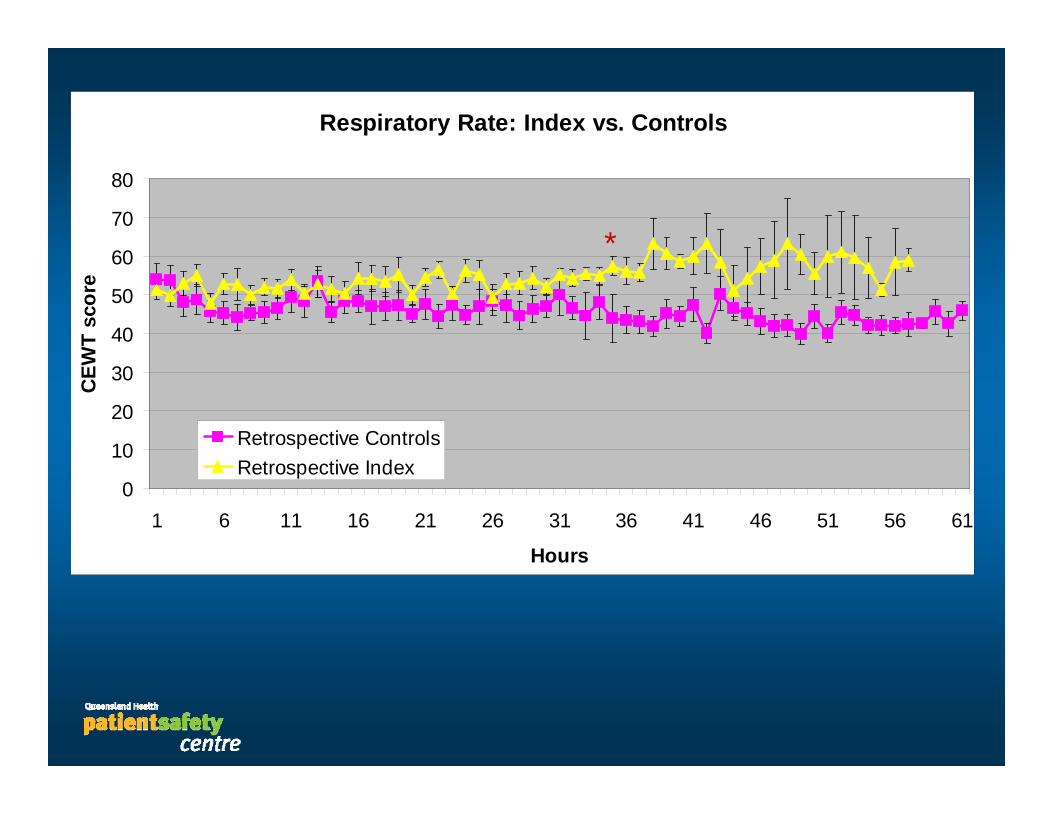
Respiratory Rate: Index vs. Controls
0
10
20
30
40
50
60
70
80
1 6 11 16 21 26 31 36 41 46 51 56 61
Hours
CEW
T sc
ore
Retrospective ControlsRetrospective Index
*


Retrieval CEWT
• 4 month convenience sample of retrieval referrals
• Evaluate state-wide implemetation
• Identify early and late referrers
• Improve objectivity in co-ordination

Retrieval patients - CEWT score
0
5
10
15
20
25
30
35
40
45
50
0 1 2 3 4 5 6 7 8 9 10 11 12 13
n = 204
23%
51%

CEWT score by diagnostic group
0
5
10
15
20
25
0 1 to 3 4,5 6,7 ³ 8
Trauma Gen SurgeryResp infection AsthmaSepsis DKASeizure

Retrieval team composition vs. CEWT
0
5
10
15
20
25
30
0 1 2 3 4 5 6 7 8 9 10 11 12 13
CEWT score
Nurse / ICP
Doctor / nurse

Root Cause Analysis
• Currently reviewing state-wide data in last 3 years
• 20 cases filed (RCAs not total deaths)
• 1 late identification spinal injury
• 2 – haemorrhage during / post surgery
• 1 out-of-hospital arrest (discharged that day)
• 1 SUDEP


Semi-quantitative implementation study
• Questionnaire at end of prospective trial period
• Evaluation of trial-site experience• Staff demographics• Impact on perceived ability to care for hospitalised children• Ease of use• Educational material / support
• Inform design of state-wide implementation strategy

Children's Early Warning Tool - Respondents
0
5
10
15
20
25
30
35
40
45
50
Paed Nurse<3 yr
Paed Nurse>3yr
Adult / PaedNurse
Paedresident
Paedregistrar
Paedconsultant
GP
n = 115

What impact has CEWT had on your ability to care for children in hospital?
1
1.5
2
2.5
3
3.5
4
4.5
5
TertiaryHDU
TertiaryOncology
TertiaryMedical /Surgical
Regional1
Regional2
Regional3
Regional4
Regional5
Rural 1 Rural 2 Rural 3 Rural 4 Rural 5
No change
Improved
Worsened

How difficult was the CEWT chart to use?
1
1.5
2
2.5
3
3.5
4
4.5
5
Tertiar
y HDU
Tertiar
y Onc
ology
Tertiar
y Med
ical /
Surgica
lReg
ional
1Reg
ional
2Reg
ional
3Reg
ional
4Reg
ional
5
Rural 1
Rural 2
Rural 3
Rural 4
Rural 5
Very easy
Very hard

How did you rate the educational material and support?
1
1.5
2
2.5
3
3.5
4
4.5
5
TertiaryHDU
TertiaryOncology
TertiaryMedical /Surgical
Regional1
Regional2
Regional3
Regional4
Regional5
Rural 1 Rural 2 Rural 3 Rural 4 Rural 5Poor
Acceptable
Excellent
What next…• Complete prospective analysis• Optimise CEWT• Design state-wide implementation• Work collaboratively across borders• Further projects
• Other charts• Telemedicine• Computers

?

Acknowledgements
• The staff of the Patient Safety Centre, Brisbane• John Wakefield, Jillann Farmer, Rowena Richardson,
Hayden Scotter, Lynette Adams
• The other members of the CEWT team• Jo-Anne Stephens• Ruth McCaffery
• The staff who participated in the prospective trial