The changing landscape of health reform: The imperative for new payment models Presented by: Joel...
28
The changing landscape of health reform: The imperative for new payment models Presented by: Joel Gilbertson Jack Friedman Senior Vice President Senior Vice President Community Partnerships Accountable Care Services and External Affairs and Payor Relations
-
Upload
stanley-foster -
Category
Documents
-
view
213 -
download
0
Transcript of The changing landscape of health reform: The imperative for new payment models Presented by: Joel...

The changing landscape of health reform: The imperative for new payment models
Presented by: Joel Gilbertson Jack FriedmanSenior Vice President Senior Vice PresidentCommunity Partnerships Accountable Care Services and External Affairs and Payor Relations

Our presentation today
• Update on health care reform• Policy trends: The case for new models• 2014 advocacy priorities
Legislative environment
• Early lessons from health care reform• Paradigm shifts and the new imperatives• The role of governance
Accountable care
Providence Health & Services | 2014 GOVERNANCE CONFERENCE

Our voice in the long reform journey
Providence Health & Services | 2014 GOVERNANCE CONFERENCE
Mission: Revealing God’s love for all, especially the poor and vulnerable.
Proverbs 31:9: Defend the rights of the poor and needy.
Our calling Our advocacy
Health care is a basic human right.
For decades we have advocated for a more just health care system with coverage for all.
While not perfect, the Affordable Care Act increases coverage for millions of uninsured, reducing their vulnerability to illness and financial distress.
Health care reform

The ACA: What’s in place, pending and to come
QualityHospital -acquired
conditions
Value-based purchasing
Readmissions
Efficiency/ geographic variation
Payment
CMS Innovation
Center
Accountable Care
Organizations
Bundled payments
Physician payments
Coverage
Immediate consumer
protections
Private insurance reforms
Medicaid expansion
Health insurance exchanges
Individual mandate
Finance Post-acute care
Payment reductions and
restraints
Waste, fraudand abuse
Independent Payment
Advisory Board
4Providence Health & Services | 2014 GOVERNANCE CONFERENCE

WA OR CA MT AK0%
20%
40%
60%
80%
100%
120%
140%
160%
EnrolledProjected
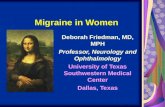
Medicaid expansion exceeds projections in three states
Total actual enrollment:
1,285,254No expansion
202,168 206,086
877,000
Projected136,000
Projected136,000
Projected700,000
100%
Data reflects only newly eligible enrollments and is current as of March 11, 2014

WA OR CA MT AK0%
20%
40%
60%
80%
100%
120%ProjectedEnrolled
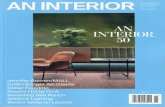
Exchange enrollment has mostly slower start
Total actual enrollmentacross our five states:
1,044,212107,262
38,806
868,936
22,542
6,666
100%
Data current as of March 11, 2014
Projected 280,000
Projected183,000
Projected 37,626
Projected19,311
Projected691,000

Exchanges: Early enrollment observations
Income levels are lower
85 percent of enrollees are eligible
for subsidies
Similar in all five of our states
Mid-range coverage
Most popular choice are silver level plans
with 70/30 cost share
Lower premiums of narrow networks
preferred
Ages skewing older
Nearly one third of enrollees in our
states are 55-64 years of age
Adds risk for insurers, complexity for
providers

Five issues we are watching as exchanges roll out
2014 through 2015
New coverage models, uneven enrollment and risk management may increase market segmentation
Narrow networks control cost but consumers and legislators want more choice
Lower enrollment may delay ability of exchanges to become self-sustaining
A weak individual mandate may not drive enough future enrollment
Uncertainty about consumer ability to pay premiums and the impact on insurers and providers

2014 policy: The case for new business models
Providence Health & Services | 2014 GOVERNANCE CONFERENCE
Health care costs stretch government budgets and drive
down reimbursement
Private and public payers turn to
alternative payment models
Consumer empowerment drives scrutiny and greater
transparency

Fee-for-service payments continuedownward trend
Medicare Parts A and BAnnual growth in per-beneficiary spending

Further cuts expected in 2014 and beyond
Medicare physician payment• Must be reformed; timing
uncertain• 24 percent cut set for
March 31• Cost of one-year patch:
$22 billion• Cost of overhaul or 10-
year patch: $128 billion
Medicare Advantage payment• CMS recently proposed an
estimated 6 percent reduction for 2015
• MA quality bonus ends in 2014, reducing payment for high performers (PHP) by about6 percent
Medicare hospital payment• 2 percent across-the-
board payment cut from budget will continue through 2023
• New “two-midnight” admissions criteria will reduce hospital payment if implemented in October
Providence Health & Services | 2014 GOVERNANCE CONFERENCE

Reform of sustainable growth rate brings opportunity and risk
Current proposal encourages alternative payment models for Medicare physiciansProvides annual payment update of 0.5 percent from 2014 to 2018
• Two new tracks for payment increases in 2018 and beyond• Up to a 5 percent bonus for adoption of medical home model
1. A merit-based incentive payment system with rewards and penalties2. Rewards participation in alternative payment models
Risk: no source identified to fund the $128 billion cost of this plan, leaving hospital reimbursement open for more cuts
Risk: Other Medicare programs known as “extenders” not funded

Opposing political forces may drive consensus on shared-risk models
DemocratsFinancial realities of broken fee-for-service
system lead to support of shared risk models
Medicare reformer on deck:
New Senate Finance Committee Chair Ron Wyden (D-Ore.)
Providence Health & Services | 2014 GOVERNANCE CONFERENCE

Alternative payment models on the rise
Oregon’s coordinated care model
Strong enrollment and financial incentives
90 percent of Oregon’s Medicaid enrollees are in CCOs
Total enrollment 727,000 with 400,000 more expected by 2022
Federal waiver requires 2 percent reduction in Medicaid spending trend
If 2 percent achieved, federal funds of nearly $2 billion available over 5 years
Coordinated care model attributes
Sustainable rate of cost growth
Providers, plans share risk
Core set of quality measures
Price, quality transparency and standard reporting
Integrated payment and delivery reform

Public wants less cost, more value and access
Providence Health & Services | 2014 GOVERNANCE CONFERENCE
Health care = 17% GDP
Focus on mergers, affiliations
Scrutiny of community benefit
Tax exemption questionedDemand for
transparency Chargemasters indefensible

Our 2014 advocacy priorities
o Redesigning how clinical care is organized and paid for
o Ensuring coverage expansions are fair and sustainable
o Preserving flexibility to serve the unique needs of our communities
o Ensuring access for the most vulnerable among us
Providence Health & Services | 2014 GOVERNANCE CONFERENCE 16

Providence Health & Services | 2014 GOVERNANCE CONFERENCE
Accountable care
Health reform and our shifting business model

Early lessons from health reform
• Cost over choice• Payor negotiations fierce• Provider networks narrowing• Government programs: total cost of care incentives• Primary care central: new incentives to manage
downstream costs• Marketplace seeing some relief

2012 health spending: Lowest increase in 53 years!
• $2.8 trillion• +3.7% over 2011• +4.6% general economy• 17.2% GDP in 2012• 17.3% in 2011• Hospitals +4.9%• Physicians +4.6%• Rx +.4% (generics!)• Out-of-pocket +3.8%

Fundamental paradigm shifts
• We cannot be at mercy of health plans• We must be upstream of the premium• Providence/Swedish-centric provider networks• Direct contracts with large employers• We influence employee health benefit design• At risk for episodes/total cost of care• At risk for three years or moreProvidence Health & Services | 2014 GOVERNANCE CONFERENCE

Fundamental paradigm shifts (cont’d)
• We’re cost centers first• Revenue centers second• Marginally effective care is waste• Everything, now………to• Most good for most people at least amount of cost
Providence Health & Services | 2014 GOVERNANCE CONFERENCE

The new imperatives
• Form ACOs to capture covered lives• Measure lives, not admissions• Commit to total cost of care over time• Put PCMHs on steroids• Find and train population health management leaders• Continuously improve cost structure• Reserve capital for future losses• Get Triple Aim better—FASTProvidence Health & Services | 2014 GOVERNANCE CONFERENCE

Providence responding to new environment
• ACOs in WA, CA, MT • Providence/Swedish-centric networks• Boeing and Intel direct—total cost of care• Joints and heart surgery bundles• Managed Medicaid readiness• Partnering with plans for upside risk• Converting FFS Medicare to Medicare AdvantageProvidence Health & Services | 2014 GOVERNANCE CONFERENCE

Providence responding to new environment(cont’d)
• Medicare Advantage partnerships: PHP, Premera and United
• Medical groups preparing: coding, analytics, case management
Providence Health & Services | 2014 GOVERNANCE CONFERENCE

The new math

Role of governance: Push management to be better!!
• Number of covered lives dedicated to our network• PMPM trend on employee health spend• Percent of low acuity ED visits going down or up• Risk returns in new MA products• HEDIS and CAHPS scores• Percent of medical admissions for ambulatory sensitive
conditions
Providence Health & Services | 2014 GOVERNANCE CONFERENCE

Role of governance: Push management to be better!!(cont’d)
• C-section rate: Medicaid and commercial• Health care costs in last six months of life• Specialty referral rates/1000• Hospital bed days/1000
Providence Health & Services | 2014 GOVERNANCE CONFERENCE

Thank you
Together, we answer the call of every person we serve: Know me, care for me, ease my way