The Changing Face of Heart Transplantation Hari R. Mallidi, MD, FRCSC Stanford Cardiothoracic...
51
The Changing Face of Heart Transplantation Hari R. Mallidi, MD, FRCSC Stanford Cardiothoracic Surgery 7 th International Symposium on Stem Cell Therapy & Cardiovascular Innovations
-
Upload
maud-summers -
Category
Documents
-
view
214 -
download
1
Transcript of The Changing Face of Heart Transplantation Hari R. Mallidi, MD, FRCSC Stanford Cardiothoracic...

The Changing Face of Heart Transplantation
Hari R. Mallidi, MD, FRCSCStanford Cardiothoracic Surgery
7th International Symposium on Stem Cell Therapy & Cardiovascular Innovations

Oldest Record
Legendary Pien Ch’iao
Performed the “Legendary Exchange of Hearts.”
Balance between the spirit and the will

Earlier Experimental Work

Overview of the History of Heart Transplantation
“A parable of regenerative medicine” K. Chien, Nature, 2008

NUMBER OF HEART TRANSPLANTS REPORTED BY YEAR
189 320667
1190
2172
2728
31513381
40204199 4229
4395 4460 4427 4283 42063898
3642 3508 3469 3372 3346 3271 3341 3362 3355
0
500
1000
1500
2000
2500
3000
3500
4000
4500
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
2006
2007
Nu
mb
er
of
Tra
ns
pla
nts
ISHLTNOTE: This figure includes only the heart transplants that are reported to the ISHLT Transplant Registry. As such, the presented data may not mirror the changes in the number of heart transplants performed worldwide
2009

NUMBER OF HEART TRANSPLANTS REPORTED BY YEAR
0
500
1000
1500
2000
2500
3000
3500
4000
4500
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
2006
2007
Nu
mb
er
of
Tra
ns
pla
nts
Other
EuropeNorth America
ISHLTNOTE: This figure includes only the heart transplants that are reported to the ISHLT Transplant Registry. As such, the presented data may not mirror the changes in the number of heart transplants performed worldwide
2009

Current Challenges
• Changing recipient population• Decreasing donor population• Increasing recipient sensitization
– Desensitization protocols– Acute cellular rejection– Acute humoral rejection

Patient Population
- Better management of advanced heart failure
- Patient population is older and sicker
- Other options to heart transplantation: Mechanical Support

Recipient Selection
Indications• Advanced heart failure
– NYHA Class III or IV– VO2 max ≤12 cc/kg/min (on β-blockers)
and ≤14 cc/kg/min (intolerant β-blockers)
• Incessant VT or high risk of sudden death
• Refractory, severe angina• Congenital heart disease
– Failed Fontan conduit– Failing systemic right ventricle
• Cardiac tumors– Low likelihood of metastasis
Contra-indications (most relative)• Advanced age (>70)• Active systemic infection• Fixed pulmonary hypertension
– PVR > 5 Wood Units or PVRI > 6– TPG > 15-20 mmHg– PAs > 50-60 mmHg or >50% systemic
• Severe renal*, hepatic*, or pulmonary disease
• Obesity (BMI > 30 or >140% IBW)• Severe PVD• Diabetes mellitus
– End-organ damage– Poor glycemic control (HbA1c >7.5)
• Active or recent malignancy• Recent pulmonary infarction• Ongoing substance abuse• Psychosocial:
– Poor compliance– Inadequate social support

Age > 70
• Increasingly older patient population being transplanted
• Oldest transplant currently alive at Stanford was 76yo at the time of his transplant
0
5
10
15
20
25
30
35
40
0-9 10-19 20-29 30-39 40-49 50-59 60-69 70+
Recipient Age
% o
f tra
nspl
ants
1982-1991 (N = 21,126)
1992-2001 (N = 40,356)
2002-6/2008 (N = 21,609)

Fixed Pulmonary Hypertension
• High fixed PVR– Might remain a transplant candidate– Will elect to bridge the patient with an LVAD
• Should be an in-patient on inotropic therapy• Not likely to be discharged without LVAD implant
– Follow closely PVR during period of LVAD support
– When/If PVR drops below 2.5 then would reconsider transplant eligibility

Severe non-cardiac organ failure
• Renal failure– Incidence of combined heart-kidney transplant
increasing• 5 Heart-Kidney Transplants in 2009
• Liver failure– Usually a contraindication in acute situation– In young patients with severe 'cardiac' cirrhosis have
done combined transplant
• Pulmonary failure– Combined Heart-Lung Transplant
• Average 5-10 Heart-Lung Transplants per year at Stanford

Obesity (BMI > 30 or > 140% IBW)
• Expanded the acceptance criteria– Accept up to BMI of 35– If BMI > 35
• Consider LVAD implant• Intense exercise and weight loss program• Reconsider transplant eligibility if weight loss
occurs

Diabetes Mellitus
• No longer considered a contraindication unless patient has significant functional limitation
• Poor glycemic control– Hb
A1c >7.5% remains a contraindication
• Patients with poor diabetic control are considered for LVAD therapy

Congenital2%
ReTX2%
Myopathy46%
Misc.3%
Valvular3%
CAD44%
1/1982-6/2008
DIAGNOSIS IN ADULT HEART TRANSPLANTS
203040506070
% o
f Cas
es Myopathy CAD
CAD38%
Valvular2%
Misc.4%
Myopathy51%
ReTX3%
Congenital2%
1/2005-6/2008
ISHLT
2009

Changing Patient Population
Re-transplantation candidates LVAD recipients Multiple previous operations
Complex congenital patients
• New challenges–Sensitized Patients–Surgical challenges–Ethical issues

Sensitized patients
When the magnitude and likelihood of a heightened response can be assertained
When they show >10% panel reactive antibodies (PRA)
More important than high PRA is the presence of donor specific antibodies (DSA) or antibodies directed against the donor heart.
Mehra MR. Curr Opin Cardiol. 2003;18:153-8.

Methods of Assessment

De-sensitization protocols
• All patients with a cPRA > 10%– Goal: Reduce levels of circulating antibodies
• Pre-transplant– IVIG– Rituximab
• Intra-operative– Plasmapheresis
• Post-operative– IVIG– Close monitoring for DSA

ADULT HEART TRANSPLANTS (1989-6/1993) Relative Risk of 15 Year Mortality with 95% Confidence Limits
Recipient Pre-Transplant PRA
0
0.5
1
1.5
2
0 10 20 30
PRA
p = 0.0100
Re
lati
ve
Ris
k o
f 1
5 Y
ea
r M
ort
ali
ty
(N=7,478)2009ISHLT

Matching Donors & Recipients
Matching is based upon:• ABO blood group• Body size compatibility (±
20% body weight)• Antibody screen (PRA)• No HLA prospective
matching done unless high levels of pre-formed antibodies on screening (PRA > 10-20%)
Allocation is determined by:
• Recipient’s priority on waiting list– Status code (1A, 1B, 2)– Time accrued within a status
• Geographic location from donor

Advances in Surgical Technique
Goals:
- Improve surgical technique and preserve cardiac anatomy
- Decrease Ischemic Time
- Improve Myocardial Protection

Organ Preservation
• Decreased organ ischemic time
• Continuous perfusion of organ
• Better organ function
• Recovery of organ function in borderline cases

Biatrial Technique

Bicaval Technique

ADULT HEART TRANSPLANTS (1/2002-6/2007) Relative Risk of 1 Year Mortality with 95% Confidence Limits
Ischemia Time
0
0.5
1
1.5
2
2.5
3
30 60 90 120 150 180 210 240 270 300 330 360
Ischemia Time (minutes)
p = 0.0004Re
lati
ve
Ris
k o
f 1
Ye
ar
Mo
rta
lity
2009ISHLT (N=10,705)

POST-TRANSPLANT ISSUES

What to Expect Post-Transplant
• Immunocompromised due to anti-rejection medications– Bacterial, fungal, viral, atypical organisms
• The transplanted heart is denervated– Sinus tachycardia (HR 110-120 may be normal)– May not experience angina– Exercise intolerance, fatigue
• Abnormal ECG• Subtle symptoms (lethargy, nausea) may be the
only signs of rejection or early infection

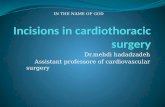
ADULT HEART TRANSPLANT RECIPIENTS: Relative Incidence of Leading Causes of Death
(Deaths: January 1992 - June 2008)
0
10
20
30
40
50
0-30 Days (N= 3,531)
31 Days – 1Year (N =
3,513)
>1 Year – 3Years (N =
2,716)
>3 Years – 5Years (N =
2,356)
>5 Years – 10Years (N =
5,335 )
>10 Years (N= 3,677)
CAV Acute Rejection
Malignancy (non-Lymph/PTLD) Infection (non-CMV)
Graft Failure
Pe
rce
nta
ge
of
De
ath
s
ISHLT
2009

ADULT HEART TRANSPLANT RECIPIENTS: Cumulative Incidence of Leading Causes of Death
(Transplants: January 1992 - June 2007)
0%
1%
2%
3%
4%
5%
6%
7%
8%
9%
10%
0 1 2 3 4 5 6 7 8 9 10
Time (years)
CAV Acute Rejection
Malignancy (non-Lymph/PTLD) Graft Failure
CMV Infection (non-CMV)
Inc
ide
nc
e o
f C
au
se
-Sp
ec
ific
De
ath
s
ISHLT
2009

Routine Surveillance

Immunosuppression: General Principles
- Immune reactivity and risk of rejection is highest early (first 6 months) after graft implantation and decreases with time therefore the doses are higher early on.
- Most modern regimens employ low doses of several drugs without overlapping toxicities in preference to higher doses of fewer drugs.

Immunosuppressive Agents

Immunosuppressive Drugs
• Induction therapy with T-cell cytolitic agent– 50% of centers give induction therapy– Multiple agents: OKT3, rATG
• Corticosteroids– Solumedrol 500 mg IV coming off bypass, then 125
mg IV q8h x 3 doses– Prednisone 1 mg/kg divided BID (Day 1-14)– Gradually taper dosage with goal of complete wean
by 6-9 months

Immunosuppression Regimens
Pre-1980’s Typical Graft CAD Renal Sparing
CyclosporinTacrolimus
CyclosporinTacrolimus
Sirolimus
ImuranMMF
ImuranSirolimus MMF
PrednisonePrednisone(month 0-6)

0
20
40
60
80
100
Cyclosporine Tacrolimus Rapamycin MMF Azathioprine Prednisone
% o
f P
atie
nts
2000 (N = 1,503) 2003 (N = 1,610) July 2007 - June 2008 (N = 1,705)
ADULT HEART RECIPIENTS Maintenance Immunosuppression at Time of 1 Year Follow-up
NOTE: Different patients are analyzed in each time frame.
ISHLT
Analysis is limited to patients who were alive at the time of the follow-up
2009

Rejection
• 30-50% of patients will experience rejection within the 1st year
• Most cases are cellular (T-lymphocyte mediated). Up to 20% are humoral (antibody mediated).
• Presentation:– Asymptomatic (most)– Malaise, fatigue, atrial arrhythmias, pericardial
effusion, low grade fever, GI symptoms– Heart failure, ventricular arrhythmias, and conduction
delays occur late

Identifying Allograft RejectionDisease Progression
Alloimmune activation Cellular invasion
Multiple genes and pathways
Cellular inflamationand myocyte necrosis
Graft Dysfunction
Heart failure andarrhythmias
Diagnostic Indicators
Gene Expression ProfilingImmune Function Assays
Endomyocardial Biopsy(intermediate)
Functional Assessment(late)

Endomyocardial Biopsy

Biopsy Grading (ISHLT)
Old (1990) New (2004) Histology
0 0 No rejection
1A
1R (Mild)Interstitial and/or perivascular lymphocitic infiltrate with up to one focus of myocyte damage
1B
2
3A
3B
4

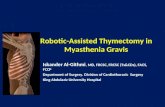
Biopsy Pathology: AMR
CD28 highlights intravascularMacrophages
C4d staining ofcapillaries

Pham et al., NEJM, Apr 22, 2010

Management of Rejection
• Cellular: dependent upon histology grade and presence of hemodynamic compromise (HDC).– Moderate without HDC: Solumedrol 1 gm IV daily x 3,
augmentation of baseline immunosuppression– Severe or moderate with HDC: As above + antibody
cytolytic therapy– Recurrent or refractory: Total lymphoid irradiation
• Antibody mediated: Plasmapheresis, IVIg, Rituximab, Photopheresis

Cardiac Allograft VasculopathyCoronary Angiogram
Intravascular Ultrasound (IVUS)
Histology(autopsy)
Diagnosis: coronary angiogram, IVUS, Dobutamine stressEchocardiography (DSE), myocardial perfusion imaging (MPS)

1 Mehra et al., JHLT 1995; 2 Rickenbacker et al., Circ 1995
Significance of Intimal Thickening
0
5
10
15
20
25
30
Ca
rdia
c e
ve
nt
rate
(%
)
MIT > 0.5 MIT ≤ 0.5
Intimal thickening
7/31
1/43
P=0.006
Sudden death, MI, or need forrevascularization
MIT ≤ 0.3mm
MIT > 0.3mm
MIT ≤ 0.3mm
MIT > 0.3mm

Kobashigawa et al, Multicenter IVUS Validay Study, JACC 2005
Effects of MIT change on long-term cardiac outcomes
• 125 Heart Tx patients• 5 centers• Baseline vs 1 year IVUS• 5-year follow-up
DeathGraft lossAcute MICHFNeed for PCI/CABGICD placementCVA, PVDAngiographic CAV

Eisen et al., NEJM 2003; Keogh et al., Circ 2004, Mancini et al., Circ 2003
Effects of PSI on CAV
Rapamycin
Control P<0.01
Patients with established CAVDe novo after OHT
Primary endpoint: death, angioplasty, MI,or >25% increase in catheterization score

Infection
Fishman, NEJM 2007

The Journey Continues

Challenges for the future
• Better define the role of MCS• Improve organ storage / resuscitation• Improved assessment of immunological
risks• Improved rejection surveillance• Improved immunosuppression regimens• Improved prophylaxis against infection and
malignancy

Acknowledgements
Robert C. Robbins, MD
Philip E. Oyer, MD, PhD
Bruce A. Reitz, MD
Sharon A Hunt, MD
Hannah Valantine, MD
Michael Pham, MD, MPH
Francois Haddad, MD
Michael B. Fowler, MD