
The Certification Commission for Healthcare Information Technology (CCHIT) Overview and Update HIT...
23
The Certification Commission for Healthcare Information Technology (CCHIT) Overview and Update HIT Summit West March 8, 2005 Mark Leavitt, MD, PhD Chair, CCHIT Medical Director, HIMSS
-
Upload
ashley-malone -
Category
Documents
-
view
214 -
download
1
Transcript of The Certification Commission for Healthcare Information Technology (CCHIT) Overview and Update HIT...
The Certification Commission for Healthcare Information
Technology (CCHIT)Overview and Update
HIT Summit WestMarch 8, 2005
Mark Leavitt, MD, PhD Chair, CCHIT
Medical Director, HIMSS
Slide 2
Introduction and Overview
• Context and Origin of CCHIT
• Mission and Concept
• Organization
• Stakeholder Relationships
• Guiding Principles and Points to Clarify
• Scope, Timeline and Deliverables
• Q and A
Slide 3
Context for Founding of CCHIT
• The President’s goal:Electronic health records (EHR) for every individual by 2014
• ONCHIT Strategic Framework: Private sector HIT product certification is one of eight key actions
Slide 4
Founding of CCHIT
• Founded by three HIT organizations:• American Health Information Management Assoc (AHIMA)• Healthcare Information and Management Systems Society
(HIMSS)• National Alliance for Health Information Technology
(Alliance)
• Formed panel to nominate first Commissioners
• Provided seed funding for launch• First official meeting Sept 14, 2004

Slide 5
Mission of CCHIT
To accelerate the adoptionof robust, interoperable HIT
throughout the US healthcare system,
by creating an efficient, credible, sustainable mechanism
for the certification of HIT products.
Slide 6
Scope, Timeline, and Deliverables
• Initial scope• Certify EHR products for physician
offices• Timeline
• Pilot process ready in Summer 2005• Deliverables:
• Operational capability for certification • Roadmap forecasting future certification
plans 2-3 years ahead
Slide 7
Ambulatory Care and HIT:A Critical Need
• Primary site for delivery of:• Chronic disease management• Preventive care
• System needs addressable with HIT:• Quality improvement• Patient safety• Portability of patient records
Slide 8
EHR Adoptionin Ambulatory Care
• Clinical IT penetration level is low:1 • Small offices (i.e. most doctors): 7%• Groups of 50 doctors or more: 20%
• Barriers to EHR adoption:• Cost of system• Risk of failure, incompatibility,
obsolescence• Lack of positive incentives
1 Center for Studying Health System Change, Sept 2004
Slide 9
Standards and Certification Create “Tipping Points” in Technology
Adoption
The IBM-standard PC launched the personal computing revolution
The Ethernet networking standardgave those PC’s connectivity
Wi-fi certification made connectivity available almost anywhere
Slide 10
How Product CertificationCan Accelerate HIT
Adoption
• Increase the confidence of providers to invest in and adopt HIT
• Ensure interoperability of HIT products within the emerging health information infrastructure
• Enhance the availability of HIT adoption incentives from public and private purchasers/payers
Slide 11
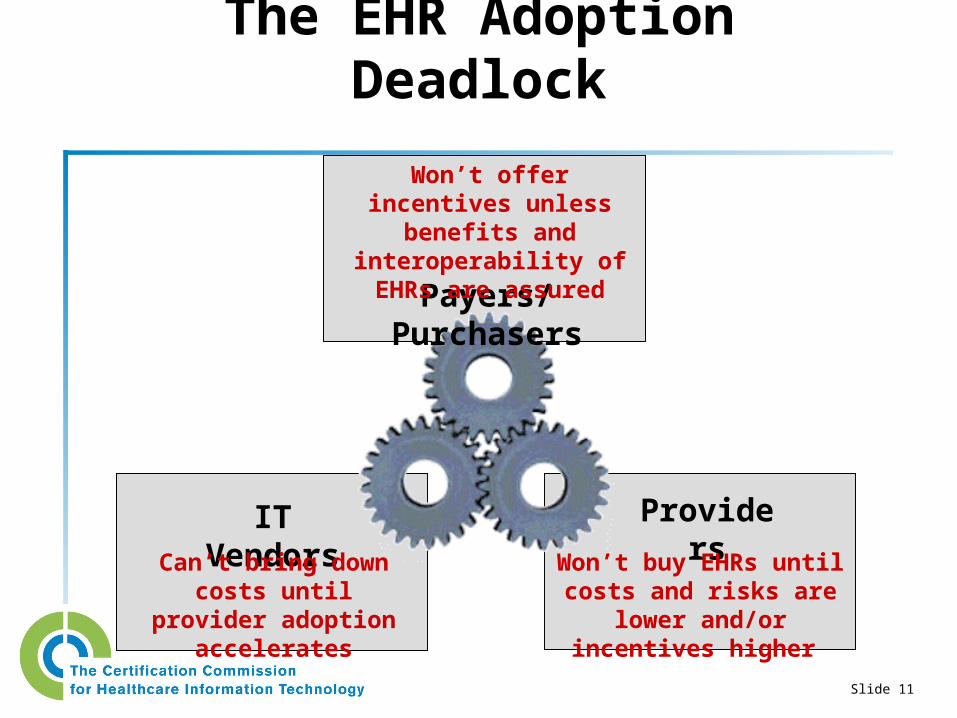
The EHR Adoption Deadlock
Payers/Purchasers
ProvidersIT VendorsWon’t buy EHRs until
costs and risks are lower and/or incentives higher
Can’t bring down costs until provider
adoption accelerates
Won’t offer incentives unless benefits and
interoperability of EHRs are assured
Slide 12
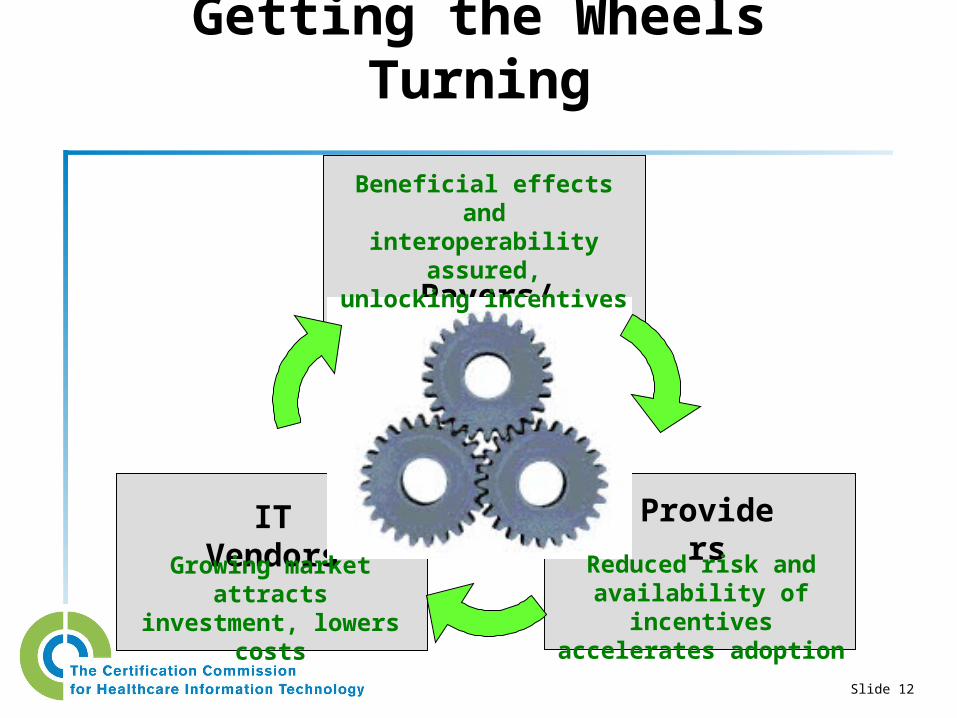
Getting the Wheels Turning
Payers/Purchasers
ProvidersIT Vendors
Beneficial effects andinteroperability assured,
unlocking incentives
Reduced risk andavailability of incentives
accelerates adoption
Growing marketattracts investment,
lowers costs
Slide 13
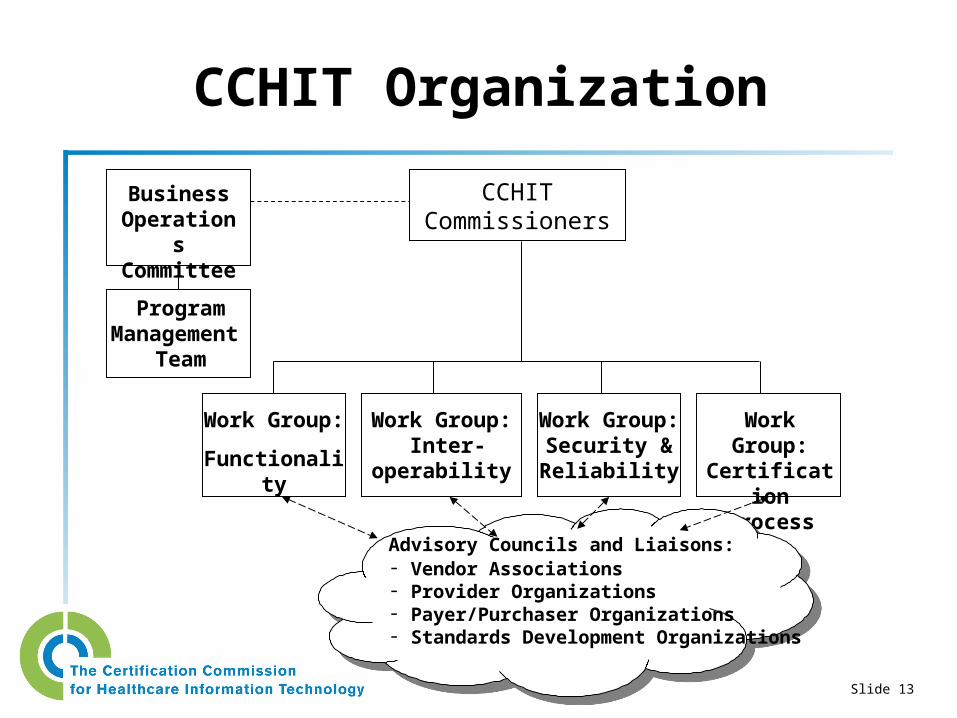
CCHIT Organization
CCHITCommissioners
Business Operations Committee
Program Management
Team
Work Group:
Functionality
Work Group: Inter-
operability
Work Group:Security & Reliability
Work Group:Certification
Process
Advisory Councils and Liaisons:- Vendor Associations- Provider Organizations- Payer/Purchaser Organizations- Standards Development Organizations
Slide 14
Composition of the Commission
• Three key constituencies (2 – 4 from each):
• Providers• Vendors• Purchasers/payers/coalitions
• Other at-large stakeholders (2 – 4 total):• Government HIT leaders (e.g. ONCHIT, CMS) – note:
ex-officio, nonvoting role• Standards development organizations (e.g. HL7)• Others, e.g. healthcare consumer advocates, etc.
Slide 15
Commissioners
• C. Martin Harris, MD – Cleveland Clinic• Douglas Henley, MD – AAFP• John Hummel – Sutter Health• John Tooker, MD – ACP• Graham O. King – McKesson Corp• Jane B. Metzger – First Consulting • Andrew G. Ury, MD – PMSI
• Suzanne Delbanco – Leapfrog• Charles Kennedy, MD - Wellpoint• Reed Tuckson, MD – United Health• Susan Postal – HCA• Sam Karp – CHCF• Wes Rishel – HL7
• Mark Leavitt, MD, PhD (Chair) – HIMSS
• Lori Evans – ONCHIT (nonvoting)• Clay Ackerly – CMS (nonvoting)
Slide 16
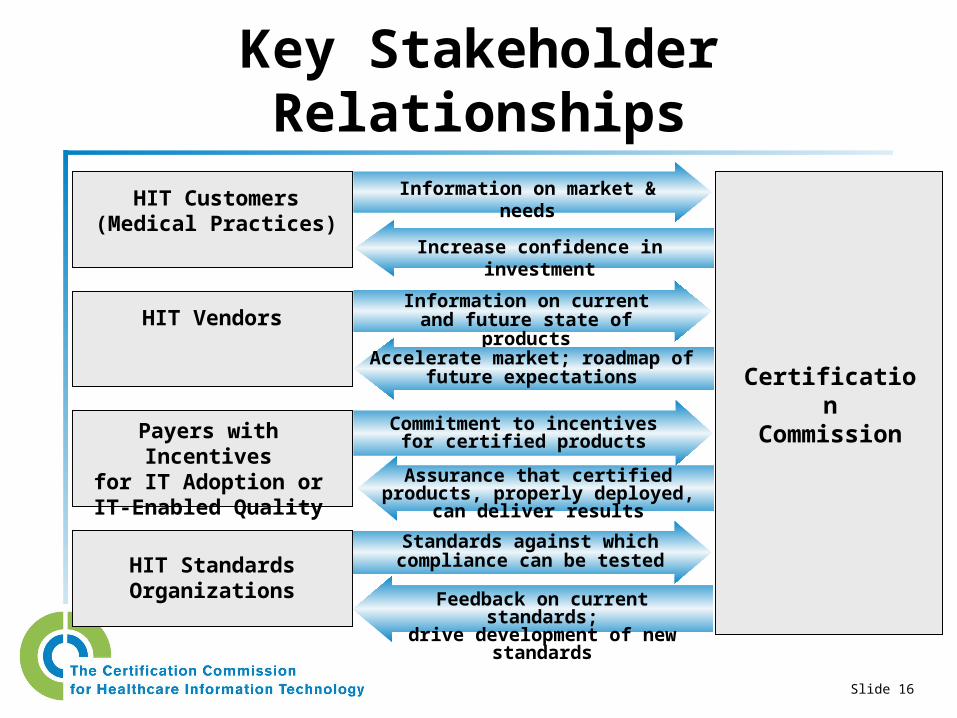
Key Stakeholder Relationships
Payers with Incentivesfor IT Adoption orIT-Enabled Quality
CertificationCommission
HIT Vendors
HIT Customers(Medical Practices)
HIT Standards Organizations
Information on market & needs
Increase confidence in investment
Information on current and future state of products
Accelerate market; roadmap of future expectations
Commitment to incentivesfor certified products
Assurance that certified products, properly deployed, can deliver results
Standards against whichcompliance can be tested
Feedback on current standards;drive development of new standards
Slide 17
Guiding Principles
• Need for decisive private-sector action now• Must seek input and deliver a compelling
value for all key stakeholders and the larger healthcare community
• Most operate in credible, objective, and collaborative manner
• Certification must be objective, laboratory verified to the greatest extent practical
• Must be efficient, fast, and low in cost
Slide 18
Key Points to Clarify
• Product Certification is different from:• Organizational Accreditation• Professional Certification
• Certification is binary, i.e. “pass/fail”• Not a subjective, comparative “points” rating
system• A voluntary process
• Initial requirements must be market reality-based• A forward-looking requirements roadmap provides
the best means to influence market direction
Slide 19
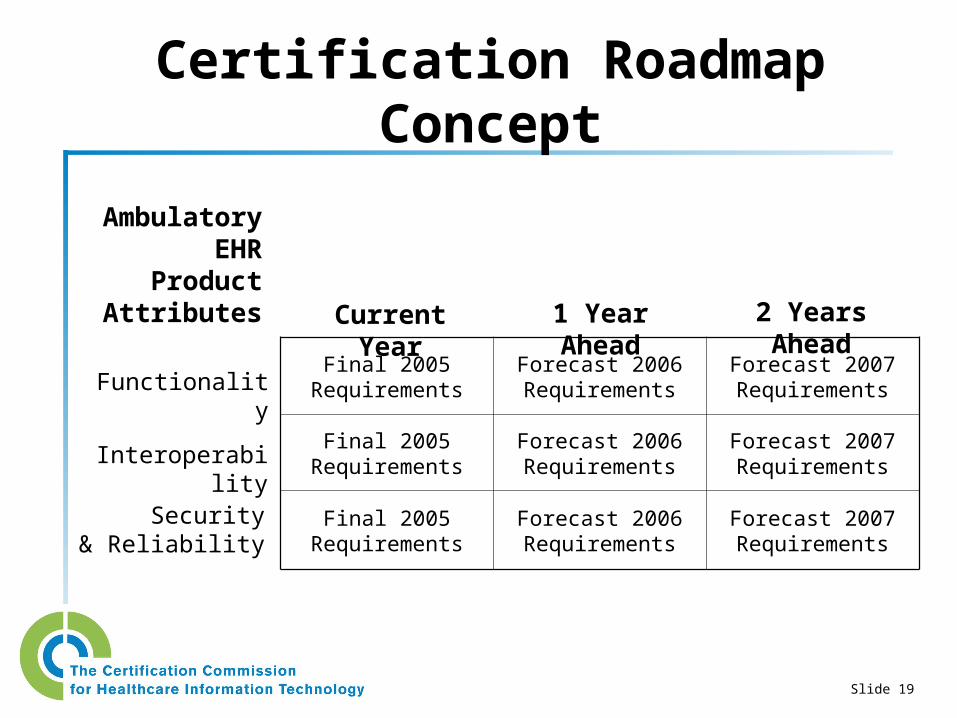
Certification Roadmap Concept
Final 2005 Requirements
Forecast 2006 Requirements
Forecast 2007 Requirements
Final 2005 Requirements
Forecast 2006 Requirements
Forecast 2007 Requirements
Final 2005 Requirements
Forecast 2006 Requirements
Forecast 2007 Requirements
AmbulatoryEHR
ProductAttributes
Functionality
Security& Reliability
Interoperability
Current Year 1 Year Ahead 2 Years Ahead
Slide 20
Project Status
• Work Groups now completing Phase I – Data Gathering
• Reference material on standards and other efforts
• Stakeholder priorities• Availability in marketplace
• Gain broad stakeholder input• Post for public comment (~April)• Conference calls and online comment
mechanisms• Outreach and communications program
Slide 21
Tasks Ahead
• Phase II – Draft Certification Requirements• Balance stakeholder desires, marketplace availability,
testability, burden and cost• Second public comment cycle
• Pilot/beta testing of certification• Confidential testing of initial set of products/vendors• Refine requirements and testing methodology
• Launch 2005 deliverables• Begin accepting applications and granting certification• Release forward-looking roadmap
Slide 22
Summing Up
• CCHIT successfully launched and operating• Goal is to accelerate the adoption of robust,
interoperable HIT -- while delivering value to providers, vendors, and purchasers/payers
• Ambulatory EHR is initial focus, with first step certification in summer 2005
• Commission to also deliver a forward-looking roadmap of certification plans to the industry
Q and A
For more information: www.cchit.org
Submit your questions and comments at the website


















