
The case against mandibular condylotomy in the treatment of the painful, deranged temporomandibular...
5
J Oral Maxillofac Surg 54:70-74, 1996 The Case Against in the Treatment Mandibular Condylo tomy of the Painful, Deranged Temporomandibular Joint PETER BANKS, FDSRCS, FFDRCS, FRCS” To paraphrase Dr Johnson the operation of condylot- omy is like the dog walking on its hinder legs; whether or not it is done well, we are surprised to see it done at all. Condylotomy was developed by the late Sir Terence Ward’ in the unit in which I presently work as an operation for the painful, dysfunctional temporo- mandibular joint. There is some myth attached to the rationale for the procedure, there being several claims to the original idea. Dr William Campbell, an excep- tional radiologist who did much original work on the functional anatomy of the temporomandibular joint,233 claims to have suggested the operation on the basis of the incidental observation that symptomatic improve- ment occurred after fracture of the condylar neck. Al- though Ward advocated the procedure,’ his rationale was flawed. He frequently told his trainees, “others modify the occlusion to suit the joint; we change the joint to fit the occlusion.” When McKenzie and I per- formed our retrospective study of the operation, we expected to discredit it on the basis of observed com- plications in a significant number of patients.4,5 It was a surprise at the time to find that long-term pain relief was found in 90% of those interviewed. However, the operation was abandoned as a clinical tool for a number of reasons. In the first place, the operative result was unpredictable, particularly in the hands of the inexperi- enced surgeon for whom the occurrence of fracture dislocation became all too common. Secondly, it was impossible to divorce clinical success from the placebo effect. The case illustrated in Figure 1 had complained of facial pain for 7 years before surgery, which can be seen to have effectively done nothing. However, she had been rendered pain free according to her own ac- count for the ensuing 10 years. * Consultant Oral & Maxillofacial Surgeon, South Thames Re- gional Maxillofacial Unit, Queen Victoria Hospital NHS Trust, East Grinstead, UK. Address correspondence and reprint requests to Dr Banks, The Queen Victoria Hospital, Holtye Rd, East Grinstead, West Sussex RH19 3DZ United Kingdom. 0 1997 American Association of Oral and Maxillofacial Surgeons 027%2391/97/5501-0010$3.00/0 Definition of Terms Any discussion of condylotomy has to be clear as to what is meant by the term. Condylotomy is an opera- tive section of the condylar neck that permits a change in the angulation of the condylar process. What has been described as a modified condylotomy6-9 is not the same operation, and is more correctly described as a vertical ramus osteotomy.” There is an important difference that is evident more from a retrospective analysis of cases than from the initial design of the operative procedure. In 1975 we observed4 that, in spite of the regular attempt to push the condyle forward and medially after blind condylotomy, it consistently remodeled to leave a backward angulation, which in unilateral cases was accompanied by a sustained in- crease in the joint space (Fig 2). It was our considered view that the operation, in effect rather than by design, produced a more favorable angular relationship be- tween the condyle and the disc. The general observa- tion made in that article that “all procedures which reduce the conflict during movement between condyle and disc are likely to be beneficial,” is probably still true today. A repositioned condylar process after a vertical ra- mus osteotomy is designed to place the condyle into the same relationship with the disc as an anterior repo- sitioning appliance, but to make it a permanent change.’ As Solberg has observed,” this is only likely to be successful where there is a reducible anterior disc displacement (RDD). It can be argued that the true condylotomy might be successful in irreducible disc displacement (IRDD), provided the angulation of the condyle can be predictably achieved, something that is not consistently possible with the blind procedure. In our unit, attempts at controlled repositioning by both intraoral and extraoral open operations have been dis- continued because of the unacceptable morbidity in- volving mainly an occasional facial weakness and more frequently a limitation of opening, complications that have been reported by others.12 Osteotomy of the condylar neck or ramus is only 70
-
Upload
peter-banks -
Category
Documents
-
view
215 -
download
0
Transcript of The case against mandibular condylotomy in the treatment of the painful, deranged temporomandibular...
J Oral Maxillofac Surg 54:70-74, 1996
The Case Against in the Treatment
Mandibular Condylo tomy of the Painful, Deranged
Temporomandibular Joint PETER BANKS, FDSRCS, FFDRCS, FRCS”
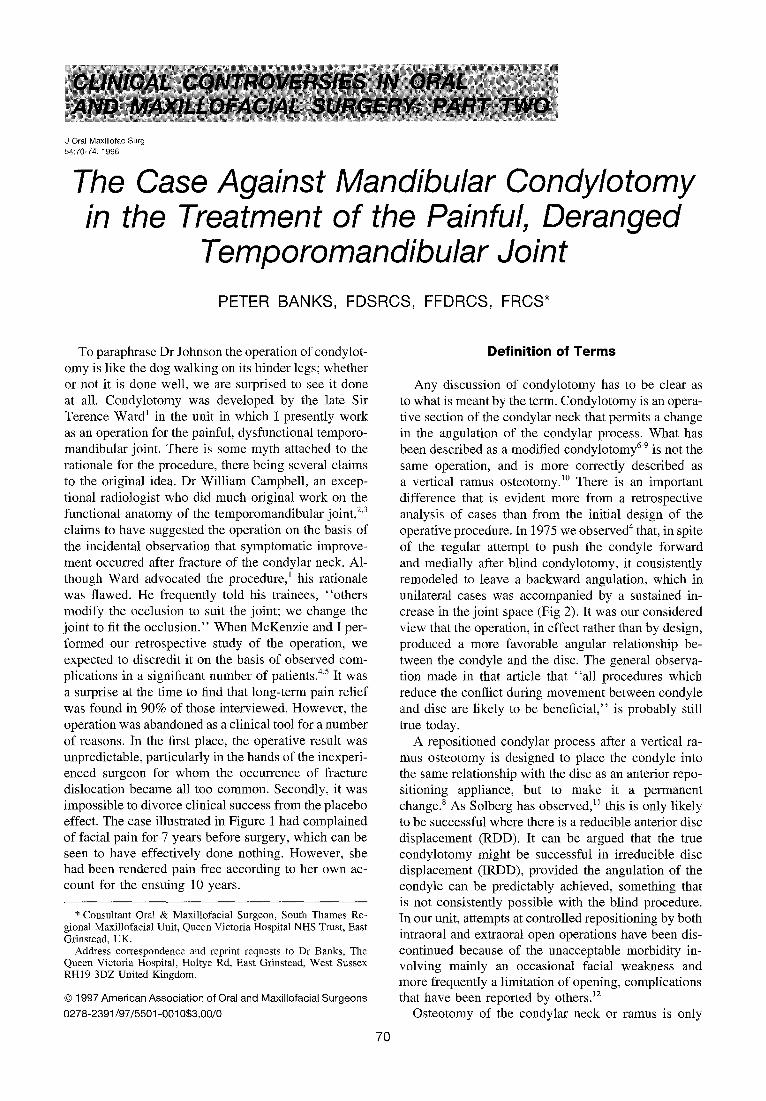
To paraphrase Dr Johnson the operation of condylot- omy is like the dog walking on its hinder legs; whether or not it is done well, we are surprised to see it done at all. Condylotomy was developed by the late Sir Terence Ward’ in the unit in which I presently work as an operation for the painful, dysfunctional temporo- mandibular joint. There is some myth attached to the rationale for the procedure, there being several claims to the original idea. Dr William Campbell, an excep- tional radiologist who did much original work on the functional anatomy of the temporomandibular joint,233 claims to have suggested the operation on the basis of the incidental observation that symptomatic improve- ment occurred after fracture of the condylar neck. Al- though Ward advocated the procedure,’ his rationale was flawed. He frequently told his trainees, “others modify the occlusion to suit the joint; we change the joint to fit the occlusion.” When McKenzie and I per- formed our retrospective study of the operation, we expected to discredit it on the basis of observed com- plications in a significant number of patients.4,5 It was a surprise at the time to find that long-term pain relief was found in 90% of those interviewed. However, the operation was abandoned as a clinical tool for a number of reasons. In the first place, the operative result was unpredictable, particularly in the hands of the inexperi- enced surgeon for whom the occurrence of fracture dislocation became all too common. Secondly, it was impossible to divorce clinical success from the placebo effect. The case illustrated in Figure 1 had complained of facial pain for 7 years before surgery, which can be seen to have effectively done nothing. However, she had been rendered pain free according to her own ac- count for the ensuing 10 years.
* Consultant Oral & Maxillofacial Surgeon, South Thames Re- gional Maxillofacial Unit, Queen Victoria Hospital NHS Trust, East Grinstead, UK.
Address correspondence and reprint requests to Dr Banks, The Queen Victoria Hospital, Holtye Rd, East Grinstead, West Sussex RH19 3DZ United Kingdom.
0 1997 American Association of Oral and Maxillofacial Surgeons
027%2391/97/5501-0010$3.00/0
Definition of Terms
Any discussion of condylotomy has to be clear as to what is meant by the term. Condylotomy is an opera- tive section of the condylar neck that permits a change in the angulation of the condylar process. What has been described as a modified condylotomy6-9 is not the same operation, and is more correctly described as a vertical ramus osteotomy.” There is an important difference that is evident more from a retrospective analysis of cases than from the initial design of the operative procedure. In 1975 we observed4 that, in spite of the regular attempt to push the condyle forward and medially after blind condylotomy, it consistently remodeled to leave a backward angulation, which in unilateral cases was accompanied by a sustained in- crease in the joint space (Fig 2). It was our considered view that the operation, in effect rather than by design, produced a more favorable angular relationship be- tween the condyle and the disc. The general observa- tion made in that article that “all procedures which reduce the conflict during movement between condyle and disc are likely to be beneficial,” is probably still true today.
A repositioned condylar process after a vertical ra- mus osteotomy is designed to place the condyle into the same relationship with the disc as an anterior repo- sitioning appliance, but to make it a permanent change.’ As Solberg has observed,” this is only likely to be successful where there is a reducible anterior disc displacement (RDD). It can be argued that the true condylotomy might be successful in irreducible disc displacement (IRDD), provided the angulation of the condyle can be predictably achieved, something that is not consistently possible with the blind procedure. In our unit, attempts at controlled repositioning by both intraoral and extraoral open operations have been dis- continued because of the unacceptable morbidity in- volving mainly an occasional facial weakness and more frequently a limitation of opening, complications that have been reported by others.12
Osteotomy of the condylar neck or ramus is only
70
PETER BANKS 71
FIGURE 1. An attempted condylotomy. The patient claimed to have suffered pain for 7 years before her “operation.” She claimed equally to have been pain free for the ensuing 10 years.
likely to benefit a patient with a mechanical derange- ment of the temporomandibular joint (TMJ). Two key questions, therefore, need to be addressed. Can a pain- ful, dysfunctional temporomandibular joint present as an uncomplicated cause of facial pain and, if so, is it really a disease?
TMJ Pain/Dysfunction Within the Spectrum of Facial Pain
Simplistically, it seems clear that pain in the face either originates in an end organ such as a tooth or elsewhere in the path to conscious appreciation. Har- ris13 has extensively reviewed the mechanism of idio- pathic facial pain and has suggested possible biochemi- cal changes that might explain the clinical features. He suggested the existence of an enhanced alerting mechanism in response to peripheral stimuli that could be perceived as pain. l4 For example, if the cortex reads its pain signals as originating from healthy teeth, the clinical picture is that of atypical odontalgia. In the face, conscious appreciation of pain of whatever cause will often be accompanied by reflex muscle spasm, which will in turn predispose to incoordination of the temporomandibular joint diarthrosis and clinical dys- function. It is most important to distinguish these disor-
ders from the type of end organ TMJ pain that results from such factors as mechanical trauma. It would equally be foolish to expect mechanical surgical proce- dures to be of benefit other than by a placebo effect. There should then be a much more clearly defined group of patients in whom the dysfunctional TMJ be- comes the only source of end organ pain; it being this group alone that might benefit from surgical reposition- ing of the moving part of the articulation.
Is Dysfunctional TMJ Pain a Disease?
The epidemiology of TMJ dysfunction has been ex- tensively studied and has been reviewed by a number of authors.‘5-‘7 Other than in degree, it is difficult to separate functional disorders of the joint from an inter- nal derangement. It is a fact that there is a high inci- dence of the disorder within the general population and that the incidence decreases with increasing age.‘* Carlsson’7 cites a number of long-term studies, notably that of Greene and Laskin,‘” that show the long-term symptomatic relief of all conservative and placebo treatments to be about 90%. As defined, the disorder is not progressive and does not include degenerative joint disease. It is disturbing, therefore, to find the classification described by Wilkes20X21 used in discus- sion of condylotomy when that classification presumes a spectrum of disease for which there is no evidence.
The disorder that comprises pain and dysfunction of the TMJ may indeed be disarmingly simple in its ori- gin. The TMJ is now accepted as being quite similar in structure, function, and pathology to other joints in the body.‘* It is unique in only one respect; it is one of a bilateral diarthrosis, which means that the two joints are interdependent in all movements. A number of changes in the external environment of the joint may disturb the coordination of this interdependence. Incoordinated action of the flexible capsule of a young person’s TMJ would seem easily to result in unfavor- able displacement of the disc-clinical dysfunction. Thus, trauma, malocclusion, stress, and parafunctional habits, or increased loading on the articulation, could all result in the same clinical endpoint: perverted pro- prioceptive information leading to incoordination and, at this stage, reducible disc displacement. In some cases, persistent deformation of the capsule becomes painful, which in turn evokes an inflammatory re- sponse of variable degree that is now regularly ob- served through the arthroscope. The biochemical inflammatory response (synovitis) impairs joint lubri- cation and movement with eventual formation of adhe- sions and increasing fixation of the disc. The simplest measures that reduce pain, change the proprioceptive input, and allow reeducation of the complex interactive musculature should be the logical methods of treat- ment. The passage of time would also be expected to resolve symptoms. A nonspecific, reversible inflam-

72 CONDYLOTOMY -THE CASE AGAINST
FIGURE 2. The results of the blind condylotomy. A, Immediate postoperative PA radiograph of showing condyle placed in the designed position. B, Immediate postoperative lateral view of the same case. C, Same case showing typical functional remodeling after 9 months. D, Same case at 3 years.
Table I. Data Recorded in Recent Studies of Condylotomy or Vertical Ramus Osteotomy in the Treatment of Dysfunctional TMJ Pain
Authors
separate Length of Type of Analysis of Significant
Patients Conservative Conservative Reducibility of Bilateral Postoperative Length of Treated Treatment Treatment Disc CZiStX Treatment Follow-up Pain Relief
Bell et al, 1990
Upton et al, 1991
Hall et al, 1993
Werther et al; 1995
9 Mean 6.8 yrs Not recorded RDD All bilateral MMF 3 wk 24 to 55 mo 100% Training elastics Orthodontics Exercises
44 1 to 41 months Bile Not recorded NO MMF 3 wk (unilat.) Not recorded 85% (10.8 mean) appliance MMF 6 wk (bilat.)
207 Not recorded Not recorded RDD: Early NRDD No MMF3to6wk 20% of series About 90% Training elastics 3 wk at mean Exercises 3 mo 2.8 yr
51 Not recorded Not recorded MRI proven RDD No Not defined 18 days NIA 4 pts. at 1 yr
PETER BANKS
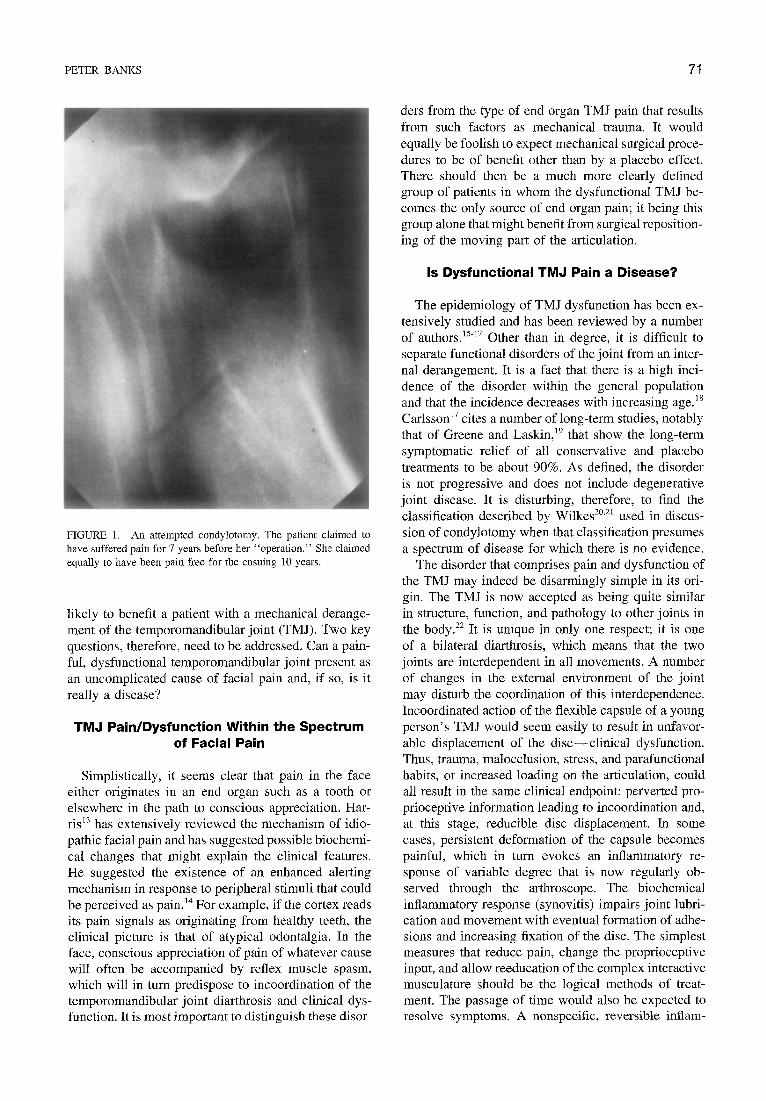
FIGURE 3. A, Right and B, left radiographs of the temporomandibular joints 6 years after a left blind condylotomy. In contrast to bilateral cases, there is a sustained increase in joint space on the operated side
matory response to trauma cannot be defined as a dis- tinct disease.
Is a Surgical Solution Ever Justified?
The case against condylotomy is also to some extent the case against surgery. Logically, repositioning of the condyle in relation to the disc will only be of benefit when it is absolutely certain the patient’s symptoms are solely the result of internal derangement of the joint. It cannot be assumed that some of the observed joint changes, such as disc perforation, are not part of the natural spectrum of joint anatomy, because so little is known of the natural variations in internal anatomy. In the case of reducible displacement of the disc, an operative intervention will probably, at best, provide a short-term solution to a potentially self-correcting situation. It is important to be sure that surgery itself is not of long-term detriment, and the evidence for this is sparse. Those who advocate condylar repositioning either by condylotomy or vertical ramus osteotomy have done little to counter this criticism. Recent articles (Table l), apart from the short series described by Bell et al,” do not consistently define the length or rationale of preoperative management and, within the known timescale of TMJ dysfunction, the follow-up period is inconclusive. In each of the series, a number of uncontrolled variables have been introduced. Postoper- ative fixation, enforced rest, local sensory denervation, and postoperative physiotherapy cannot be discounted in the observed short-term benefit. In fact, all report short-term pain relief in a high percentage of patients,
as indeed we did in our survey in the early 1970~.~ The lack of selection in the cases operated by Ward and his colleagues means that at the stage we examined them the symptomatic improvement might well have occurred with no treatment at all. The significant mor- bidity present in a small number of cases owing to surgical failure is accordingly a significant reason for abandoning the method.
There is no doubt that an inflammatory reaction is detectable in the painful dysfunctional join? that can lead to adhesions and irreducible disc displace- ment. However, recent advocates of condylar reposi- tioning surgery consistently select patients with RDD in whom noninvasive or minimally invasive treatments can be equally successfu1.23S25S26 A nonprogressive, doubtful disease entity in young persons can only jus- tify minimally invasive surgery as a final resort. The logic behind arthrocentesis to accelerate resolution of inflammatory changes seems irrefutable. The chief dis- advantage is that its application is largely confined to the upper compartment.
A final objection to condylar repositioning, and particularly true condylotomy, lies in the mechanical difficulty with bilateral cases. In 1975,4 we were able to demonstrate that the increase in joint space after bilateral condylotomy (Fig 3) was not consistently maintained, and that results in bilateral cases were commensurably worse. It is difficult to believe the bilaterally repositioned condyle will maintain its new relationship any better in the long-term unless adjunctive measures lead to a permanent modifica- tion of occlusal contacts.

74 CONDYLOTOMY-THE CASE AGAINST
Conclusions
There is no convincing evidence that either condylotomy or the so-called modified condylotomy have been tested under acceptable scientific clinical control. As Carlsson17 states: “It is generally not possi- ble to differentiate specific treatment effects from pla- cebo effects or spontaneous fluctuations of signs and symptoms without a careful study design and use of controls. ’ ’ Painful TMJ dysfunction has a natural his- tory of spontaneous fluctuation and placebo response, and that at least is known. Moreover, those who advo- cate surgical treatment signally fail to define diagnostic criteria and treatment protocols, and claim success in a condition with an estimated 90% chance of spontane- ous resolution if true pathology is excluded. Greene and Marbach16 provide two seminal statements with which most experienced surgeons would agree, and which bear restatement: “A vast amount of contempo- rary clinical care is incidental to curing disease, but the damage done by medicine to the health of individu- als and populations is very significant.“27 The advo- cates of condylotomy might further reflect that “sur- gery should be able to improve upon conservative treatments, taking account of the increased incidence of adverse sequelae. No proof has been forthcoming.”
References
1. Ward TG: Surgery of the mandibular joint. J Oral Surg 28:139, 1961
2. Campbell W: Radiology of the mandibular joint. MD Thesis, University of Edinburgh, 1962.
3. Campbell W: Clinical radiological investigations of the mandib- ular joints. Br J Radio1 38401, 1965
4. Banks P, McKenzie I: Condylotomy: A clinical and surgical appraisal of a surgical technique. J Maxillofac Surg 3:170, 1975
5. Banks P, McKenzie I: Criteria for condylotomy. .I Oral Surg 68:601, 1975
6. Nickerson JW, Veaco NS: Condylotomy in surgery of the tem- poromandibular joint. Oral Maxillofac Surg Clin North Am 1:303, 1989
7. Upton LG, Sullivan SM: The treatment of temporomandibular joint internal derangement using a modified open condylot- omy: A preliminary report. J Oral Surg 49578, 1991
8. Hall HD, Nickerson JW, McKenna SJ: Modified condylotomy for treatment of the painful temporomandibular joint with a reducing disc. J Oral Surg 51:133, 1993
9. Werther JR, Hall HD, Gibbs SJ: Disk position before and after modified condylotomy in 80 symptomatic temporomandibu- lar joints. J Oral Surg 79:668, 1995
10. Bell WH, Yamaguchi Y, Poor MR: Treatment of temporoman dibular joint dysfunction by intraoral vertical ramus osteot- omy. Int J Adult Orthodont Orthognath Surg 5:9, 1990
11. Solberg WK: Temporomandibular disorders: Management of internal derangement. Br Dent J 160:379, 1988
12. Shevel E: It&a-oral condylotomy for the treatment of temporo- mandibular joint derangement. J Oral Surg 20:360, 1991
13. Harris M: The surgical management of idiopathic facial pain produces intractable latrogenic pain? Br J Oral Maxillofac Surg 34:1, 1996
14. Derbyshire SWE, Jones AKP, Devani P, et al: Cerebral re- sponses to pain in patients with atypical facial pain measured by Positron Emission Tomography. J Neurol Neurosurg Psychiatr 57: 1166, 1994
15. Agerberg G, Carlsson GE: Functional disorders of the mastica- tory system. Acta Odont Stand 30:597, 1972
16. Greene CS, Marbach JJ: Epidemiologic studies of mandibular dysfunction: A critical review. J Prosthet Dent 48:184, 1982
17. Carlsson GE: Long term effects of treatment of craniomandibu- lar disorders. J Craniomandib Pratt 3:337, 1985
18. Franks AST: Studies related to the temporomandibular joint. DDS Thesis University of Manchester, England, 1964
19. Greene CS, Laskin DM: Long-term evaluation of treatment of myofascial pain-dysfunction syndrome: A comparative anal- ysis. J Oral Surg 107:235, 1983
20. Wilkes CH: Internal derangements of the temporomandibular joint. Arch Otolaryngol Head Neck Surg 115:469, 1989
21. Wilkes CH: Surgical treatment of internal derangements of the temporomandibular joint. Arch Otolatyngol Head Neck Surg 117:64, 1991
22. Israel HA: Synovial fluid analysis. Oral Maxillofac Surg Clin North Am 1:85, 1989
23. Moses JJ, Poker ID: TMJ Arthroscopic surgery: An analysis of 237 patients. Oral Surg Oral Med Oral Path01 47:790, 1989
24. Shafer DM, Assael L, White LB, et al: Tumour necrosis factor- alpha as a biochemical marker of pain and outcome in tempo- romandibular joints with internal derangements. J Oral Maxil- lofac Surg 52:786, 1994
25. Montgomery MT, Gordon SM, Van Sickels JE, et al: Changes in signs and symptoms following temporomandibular joint disc repositioning surgery. J Oral Surg 50:320, 1992
26. Dolwick MF, Dimitroulis G: Is there a role for temporomandibu- lar joint surgery? J Oral Surg 32:307, 1994
27. Illich I: Medical Nemesis. New York, NY, Phantom Books, 1978, p 15












![Temporomandibular Disorders, Head · used to decrease TMJ in ammation[10 12]. Patients who are diagnosed with TMJ in ammation may have altered mandibular dynamics that are](https://static.fdocuments.in/doc/165x107/5bf6b42f09d3f20a768c5edc/temporomandibular-disorders-head-used-to-decrease-tmj-in-ammation10-12-patients.jpg)





