The Cardiologist’s Guide to the Cardiovascular Consequences of Smoking and the Benefits of...
64
The Cardiologist’s Guide to the The Cardiologist’s Guide to the Cardiovascular Consequences of Cardiovascular Consequences of Smoking and the Benefits of Smoking and the Benefits of Cessation Cessation
-
Upload
julius-burns -
Category
Documents
-
view
219 -
download
2
Transcript of The Cardiologist’s Guide to the Cardiovascular Consequences of Smoking and the Benefits of...

The Cardiologist’s Guide to the The Cardiologist’s Guide to the Cardiovascular Consequences of Cardiovascular Consequences of
Smoking and the Benefits of CessationSmoking and the Benefits of Cessation

OverviewOverview
Coronary artery diseaseCoronary artery disease
Peripheral vascular disease Peripheral vascular disease
Abdominal aortic aneurysmAbdominal aortic aneurysm
StrokeStroke
Cardiovascular disease and environmental Cardiovascular disease and environmental tobacco smoketobacco smoke
Cardiovascular benefits of smoking cessationCardiovascular benefits of smoking cessation

Smoking and Coronary Artery DiseaseSmoking and Coronary Artery Disease (CAD) (CAD)

Smoking: Role in the Pathogenesis of Smoking: Role in the Pathogenesis of Cardiovascular EventsCardiovascular Events
Endothelial dysfunctionEndothelial dysfunction
Increased hematologic Increased hematologic thrombogenicitythrombogenicity
Enhanced inflammatory Enhanced inflammatory responseresponse
Oxidative modificationOxidative modification
Lavi et al. Circulation. 2007;115:2621-2627; http://www.texasheartinstitute.org/HIC/Topics/Diag/diangio.cfm. Accessed June 14, 2007.
Atherosclerotic Disease Right Coronary Artery
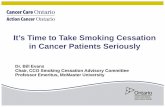
Smoking: Increased ThrombogenicitySmoking: Increased Thrombogenicity
Tissue factor (TF) is highly Tissue factor (TF) is highly expressed in atherosclerotic expressed in atherosclerotic plaques and may play a role plaques and may play a role in thrombosisin thrombosis
TF was assessed by adding TF was assessed by adding factor Xa (FXa)factor Xa (FXa)
Current smokers have Current smokers have significantly higher levels of significantly higher levels of circulating TF activity than circulating TF activity than nonsmokersnonsmokers
Sambola et al. Circulation. 2003;107:973-977.
217
283
0
100
200
300
400
CurrentSmokers Priorto Smoking 2
Cigarettes
CurrentSmokers After
Smoking 2Cigarettes
Fac
tor
Xa
(FX
a) p
mo
l/L
/min
P=.003

Smoking: Impaired Endothelial Vasodilator FunctionSmoking: Impaired Endothelial Vasodilator Function
Zeiher et al. Circulation. 1995;92:1094-1100.
Flo
w-D
epen
den
t D
ilat
ion
(%
)
0
20
30
40
60
50
10
–10
P<.01
P<.001
P<.01
Current Smokers
P<.01
Nonsmokers
P<.01
Flow-dependent dilation was Flow-dependent dilation was significantly blunted in current significantly blunted in current smokers compared with nonsmokers smokers compared with nonsmokers Angiographically normal smokers
Angiographically irregular smokers
Angiographically normal nonsmokers
Angiographically irregular nonsmokers
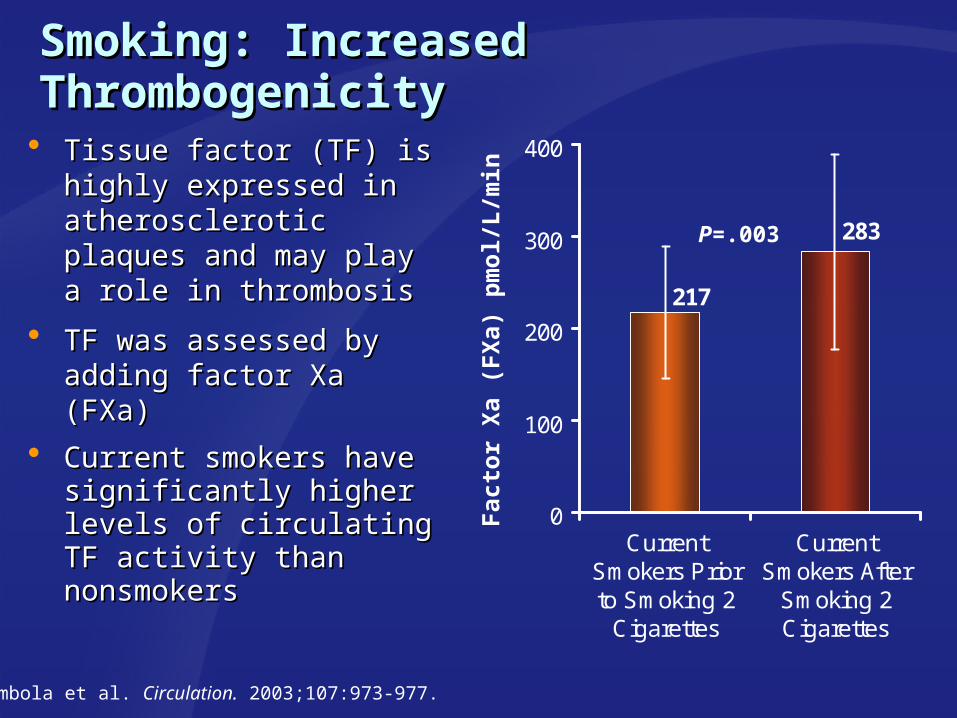
Smoking: Epicardial Endothelial Smoking: Epicardial Endothelial DysfunctionDysfunction
Lavi et al. Circulation. 2007;115:2621-2627.
Current smokers are more likely to have epicardial endothelial Current smokers are more likely to have epicardial endothelial dysfunction than nonsmokersdysfunction than nonsmokers
En
do
thel
ial
Dys
fun
ctio
n (
%)
P=.0360
45
30
15
0Nonsmokers Ex-smokers Current
Smokers
46%
34%35%

Smoking: Elevated White Blood Cell CountSmoking: Elevated White Blood Cell Count Elevated white blood cell (WBC) count has been associated with a greater Elevated white blood cell (WBC) count has been associated with a greater
risk of cardiovascular eventsrisk of cardiovascular events
Current smokers have significantly increased WBC counts compared with Current smokers have significantly increased WBC counts compared with nonsmokersnonsmokers
Lavi et al. Circulation. 2007;115:2621-2627; Stewart et al. Circulation. 2005;111:1756-1762
8
6
4
2
0
P<.0001
P=.03
P<.0001
P<.0001Cel
l C
ou
nts
(10
9 /L
)
Current Smokers
Ex-smokers
WBC Neutrophils Lymphocytes Monocytes
Nonsmokers
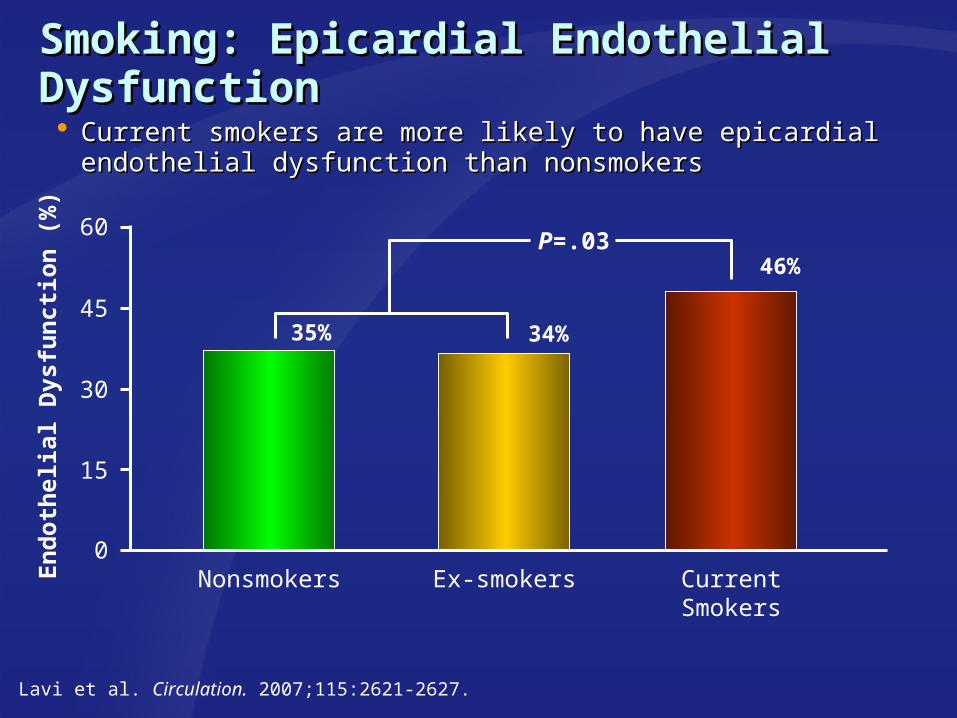
Smoking: Increased Oxidative ModificationSmoking: Increased Oxidative Modification
aF2-isoprostane level is an index of lipid peroxidation in vivo. The dots representing subjects who smoked are each connected to a dot representing a nonsmoker matched to the subject for age and sex.Adapted from Morrow et al. N Engl J Med. 1995;332(18):1198-1203.
640
560
480
400
320
240
160
80
Current Smokers
Nonsmokers
Fre
e F
2-Is
op
rost
anes
a (p
mo
l/L
) 1000
900
800
700
600
500
400
300
Current Smokers
Nonsmokers
Est
erif
ied
F2-
Iso
pro
stan
esa
(pm
ol/
L)

Smoking: Reduced Nitric Oxide (NO) Smoking: Reduced Nitric Oxide (NO) BiosynthesisBiosynthesis
Barua et al. Circulation. 2001;104:1905-1910.
5000
0Nonsmokers Current Smokers
4000
3000
2000
1000
NO
Co
nce
ntr
atio
n (
nm
ol/
L) P<.0001
1266
3613

Smoking: Multiplicative Risk Factor for Smoking: Multiplicative Risk Factor for Coronary Artery DiseaseCoronary Artery Disease
a All rates were age-adjusted by 10-year age groups to the US white male population in 1980. Hypercholesterolemia defined as cholesterol 250 mg/dL. Hypertension defined as a diastolic blood pressure 90 mm Hg. Burns. Prog Cardiovasc Dis. 2003;46(1): 11-29; Source: Pooling Project Research Group, 1978.
Smoking PlusElevated Cholesterol
or Hypertension
Risk Factor Status at Entry Into the Study
ElevatedCholesterol Plus
Hypertension
All 3 Risk Factors Present
Smoking, Elevated Cholesterol, or
Hypertension Alone
No RiskFactors
Rat
es p
er 1
000a
23
54
10392
189
0
50
100
150
200
250

Smoking: Increased Coronary Artery Smoking: Increased Coronary Artery Disease (CAD) MortalityDisease (CAD) Mortality
a The probability of an event (developing a disease) occurring in exposed people compared with the probability of the event in nonexposed people. Adjusted for age.Willett et al. N Engl J Med. 1987;317(21):1303-1309.
1.0
5.4
3.7
1.7
0
2
4
6
8
10
12
Rel
ativ
e R
isk
(95%
CI)
Rel
ativ
e R
isk
(95%
CI)
a
Fatal CADFatal CAD
1-14/Day1-14/DayNonsmokersNonsmokers 15-24/Day15-24/Day 25/Day25/DayCigarettes/Day
Current Smokers

Smoking: Effect on Coronary Artery Smoking: Effect on Coronary Artery DiseaseDisease
Waters et al. Circulation. 1996;94:614-621.
0
10
20
30
40
50
60
Progression of Existing Lesions
Pat
ien
ts (
%)
Current Smokers
Nonsmokers0
10
20
30
40
50
60
Formation of New Lesions
Pat
ien
ts (
%)
Current Smokers
Nonsmokers
P=.002 P=.007
5757
3737 3636
2020

Smoking: Increased Risk of AnginaSmoking: Increased Risk of Angina
aThe probability of an event (developing a disease) occurring in exposed people compared with the probability of the event in nonexposed people. Adjusted for age.Willett et al. N Engl J Med. 1987;317(1):1303-1309.
0
1
2
3
4
5
Rel
ativ
e R
isk
(95%
CI)
Rel
ativ
e R
isk
(95%
CI)
aa
1.01.0
1.61.6
2.62.6
2.02.0
1-14/Day1-14/DayNonsmokersNonsmokers 15-24/Day15-24/Day 25/Day25/DayCigarettes/Day
Current Smokers

Smoking: Increased Risk of Acute Smoking: Increased Risk of Acute Nonfatal Myocardial InfarctionNonfatal Myocardial Infarction Current smoking was associated with a 3-fold increase in odds of a Current smoking was associated with a 3-fold increase in odds of a
nonfatal acute myocardial infarction compared with nonsmokersnonfatal acute myocardial infarction compared with nonsmokers
aThe ratio of the odds of development of disease in exposed persons to the odds of development of disease in nonexposed persons.Teo. Lancet. 2006;368:647-658.
Odd
s R
atio
(95%
CI)
Odd
s R
atio
(95%
CI)aa
101099887766554433221100
Age <40 y Age <40 y Age 40-49 y Age 40-49 y Age 50-59 y Age 50-59 y Age 60-69 y Age 60-69 y Age >70 y Age >70 y
2200
NonsmokersNonsmokers Ex-smokersEx-smokers 1-191-19

Smoking: Increased Risk of Sudden Smoking: Increased Risk of Sudden Cardiac DeathCardiac Death
aThe probability of an event (developing a disease) occurring in exposed people compared with the probability of the event in nonexposed people. Adjusted for age.Wannamethee et al. Circulation. 1995;91:1749-1756.
1.0
2.3
0.0
1.0
2.0
3.0
4.0
Nonsmokers Current Smokers
Rel
ativ
e R
isk
(95%
CI)
Rel
ativ
e R
isk
(95%
CI)
aa

Smoking: Increased Risk of Q-Wave MI After Smoking: Increased Risk of Q-Wave MI After Percutaneous Coronary RevascularizationPercutaneous Coronary Revascularization
aThe probability of an event (developing a disease) occurring in exposed people compared with the probability of the event in nonexposed people. Adjusted for the baseline variables significantly associated with each end point.Hasdai et al. N Engl J Med. 1997;336:755-761.
0.0
1.0
2.0
3.0
4.0
Nonsmokers Ex-smokers Current Smokers
Q-wave Myocardial Infarction (MI)
Rel
ativ
e R
isk
(95%
CI)
a
1.01.01.281.28
2.082.08

Summary: Smoking and Coronary Artery Summary: Smoking and Coronary Artery Disease (CAD)Disease (CAD) Smoking plays a role in the development of CAD via:Smoking plays a role in the development of CAD via:
– Endothelial dysfunctionEndothelial dysfunction– Increased thrombogenicityIncreased thrombogenicity– Elevated WBC countsElevated WBC counts– Increased oxidative stressIncreased oxidative stress– Reduced NO biosynthesisReduced NO biosynthesis
Smoking acts as a multiplicative risk factor for Smoking acts as a multiplicative risk factor for development of CADdevelopment of CAD
Smoking is associated with an increasedSmoking is associated with an increased– Rate of progression of CADRate of progression of CAD– Risk of anginaRisk of angina– Risk of acute myocardial infarctionRisk of acute myocardial infarction– Risk of sudden cardiac deathRisk of sudden cardiac death– Risk of Q-wave myocardial infarction after Percutaneous Risk of Q-wave myocardial infarction after Percutaneous
Coronary RevascularizationCoronary Revascularization

Smoking and Peripheral Vascular DiseaseSmoking and Peripheral Vascular Disease

Peripheral Vascular Disease (PVD)Peripheral Vascular Disease (PVD)
PVD affects approximately PVD affects approximately 20% of adults older than 20% of adults older than age 55age 55
Approximately half of patients Approximately half of patients with PVD are asymptomaticwith PVD are asymptomatic
5% to 10% of asymptomatic 5% to 10% of asymptomatic patients will progress to patients will progress to symptomatic PVD over symptomatic PVD over 5 years 5 years
Patients with symptomatic Patients with symptomatic PVD are at higher risk for PVD are at higher risk for other cardiovascular disease other cardiovascular disease and mortalityand mortality
Hankey et al. JAMA. 2006;295:547-553; Hooi et al. Am J Epidemiol. 2001;153:666-672; Hooi et al. Br J Gen Pract. 1999;49:49-55; Hooi et al. Scand J Prim Health Care. 1998;16:177-182; http://healthguide.howstuffworks.com/peripheral-artery-disease-and-intermittent-claudication-in-depth.htm. Accessed October 8, 2007.
Build-up of atheroscleroticplaque in arterial wall

Asymptomatic Peripheral Vascular Asymptomatic Peripheral Vascular Disease: Increased RiskDisease: Increased Risk
aThe ratio of the odds of development of disease in exposed persons to the odds of development of disease in nonexposed persons. Adjusted for other cardiovascular risk factors. Hooi et al. Scand J Prim Health Care. 1998;16:177-182.
1.0
2.8
1.6
0.0
1.0
2.0
3.0
4.0
Od
ds
Rat
io (
95%
CI)
Od
ds
Rat
io (
95%
CI)
aa
Ex-smokers Current SmokersNonsmokers

Intermittent Claudication (IC): Increased Intermittent Claudication (IC): Increased RiskRisk Rate of development of IC is Rate of development of IC is
approximately 4 times as great in approximately 4 times as great in current smokers than in current smokers than in nonsmokers (OR 4.1[2.3-7.9]) nonsmokers (OR 4.1[2.3-7.9])
Risk tends to increase with the Risk tends to increase with the intensity of smokingintensity of smoking
The 5-year mortality for patients The 5-year mortality for patients with IC who continue to smoke is with IC who continue to smoke is 40% to 50%40% to 50%
Hooi et al. Scand J Prim Health Care. 1998;16:177-182; Kannel et al. Geriatrics. 1973;28:61-68; http://www.radiologyassistant.nl/en/42c2527422d06.
Stenosis of the Left Iliac Artery

Risk of Peripheral Vascular Disease vs Risk of Peripheral Vascular Disease vs Coronary Artery DiseaseCoronary Artery Disease For smokers, the risk of peripheral vascular disease (PVD) is greater For smokers, the risk of peripheral vascular disease (PVD) is greater
than the risk of coronary artery disease (CAD)than the risk of coronary artery disease (CAD)
aThe probability of an event (developing a disease) occurring in exposed people compared with the probability of the event in nonexposed people. Adjusted for age and sex.Price et al. Eur Heart J. 1999;20(5):344-353.
3.94
1.871.661.59
0
2
4
6
8PVD CAD
Rel
ativ
e R
isk
(95%
CI)
a
Moderate Smokers Heavy Smokers
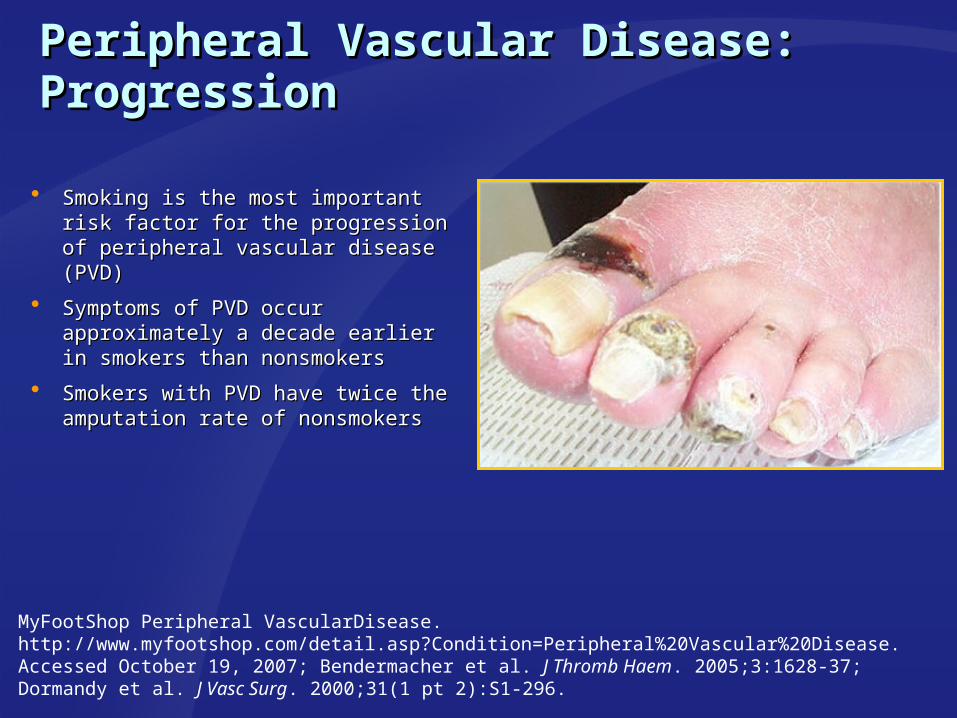
Peripheral Vascular Disease: ProgressionPeripheral Vascular Disease: Progression
Smoking is the most important risk Smoking is the most important risk factor for the progression factor for the progression of peripheral vascular disease (PVD)of peripheral vascular disease (PVD)
Symptoms of PVD occur Symptoms of PVD occur approximately a decade earlier in approximately a decade earlier in smokers than nonsmokerssmokers than nonsmokers
Smokers with PVD have twice the Smokers with PVD have twice the amputation rate of nonsmokersamputation rate of nonsmokers
MyFootShop Peripheral VascularDisease.http://www.myfootshop.com/detail.asp?Condition=Peripheral%20Vascular%20Disease. Accessed October 19, 2007; Bendermacher et al. J Thromb Haem. 2005;3:1628-37; Dormandy et al. J Vasc Surg. 2000;31(1 pt 2):S1-296.
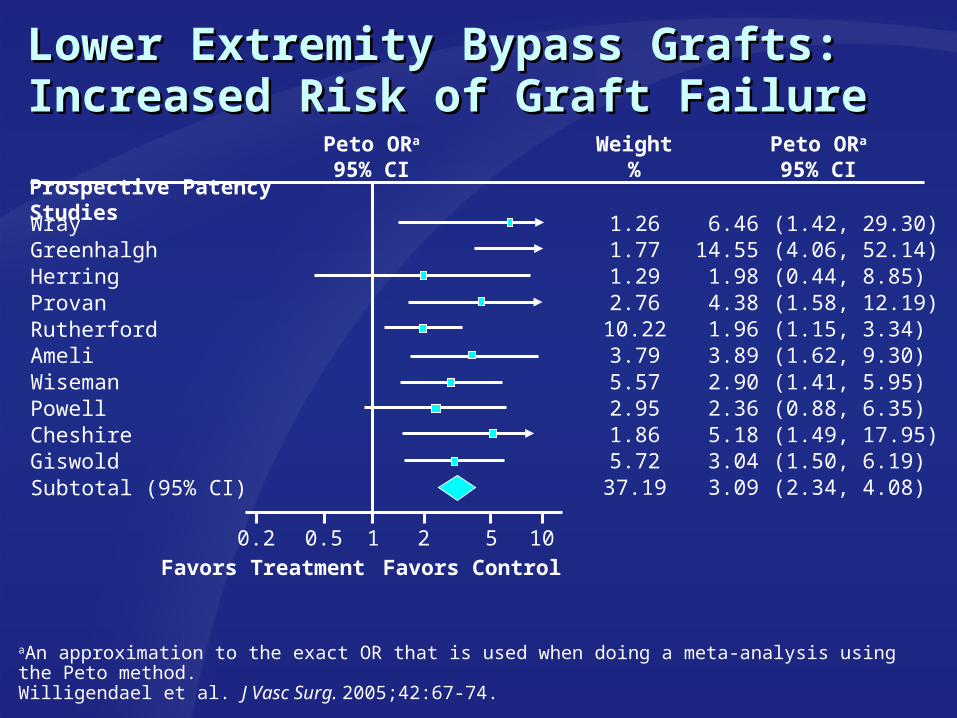
Lower Extremity Bypass Grafts: Increased Lower Extremity Bypass Grafts: Increased Risk of Graft FailureRisk of Graft Failure
Peto ORa
95% CIWeight
%Peto ORa
95% CI
WrayGreenhalghHerringProvanRutherfordAmeliWisemanPowellCheshireGiswoldSubtotal (95% CI)
1.261.771.292.76
10.223.795.572.951.865.72
37.19
6.4614.55
1.984.381.963.892.902.365.183.043.09
(1.42, 29.30)(4.06, 52.14)(0.44, 8.85)(1.58, 12.19)(1.15, 3.34)(1.62, 9.30)(1.41, 5.95)(0.88, 6.35)(1.49, 17.95)(1.50, 6.19)(2.34, 4.08)
Prospective Patency Studies
0.5 1 2 5 10Favors Treatment Favors Control
0.2
aAn approximation to the exact OR that is used when doing a meta-analysis using the Peto method.Willigendael et al. J Vasc Surg. 2005;42:67-74.

Smoking: Increased Mortality After Smoking: Increased Mortality After Vascular SurgeryVascular Surgery
In order to provide very late In order to provide very late survival data, Kazmers et al survival data, Kazmers et al evaluated 310 patients evaluated 310 patients undergoing elective vascular undergoing elective vascular surgerysurgery
Follow-up was 6.64Follow-up was 6.644.62 years4.62 years
Age, diabetes, smoking, and Age, diabetes, smoking, and low ejection fraction were low ejection fraction were independently associated with independently associated with overall mortality postoperatively overall mortality postoperatively
Kazmers et al. J Surg Res. 2002;105:109-114.

Summary: Smoking and Peripheral Summary: Smoking and Peripheral Vascular Disease (PVD)Vascular Disease (PVD)
Smoking is associated with an increased risk of Smoking is associated with an increased risk of – Asymptomatic PVDAsymptomatic PVD– Intermittent claudicationIntermittent claudication– Progression of PVDProgression of PVD– Amputation due to complications of PVDAmputation due to complications of PVD– Femoral-popliteal bypass graft failureFemoral-popliteal bypass graft failure– Mortality after vascular surgeryMortality after vascular surgery
Symptoms of PVD occur approximately a decade earlier Symptoms of PVD occur approximately a decade earlier in smokers than in nonsmokersin smokers than in nonsmokers
Current smokers are at greater risk for developing PVD Current smokers are at greater risk for developing PVD than coronary artery diseasethan coronary artery disease

Smoking and Abdominal Aortic Aneurysm Smoking and Abdominal Aortic Aneurysm (AAA)(AAA)

1.0
4.7
3.0
0
1
2
3
4
5
6
7
8
AAA: Greater Risk in Smokers Than CAD or AAA: Greater Risk in Smokers Than CAD or Cerebrovascular DiseaseCerebrovascular Disease The association between smoking and aortic aneurysm is substantially stronger than The association between smoking and aortic aneurysm is substantially stronger than
the association between smoking and coronary or cerebrovascular diseasethe association between smoking and coronary or cerebrovascular disease
AAA= Abdominal Aortic Aneurysm; CAD=Coronary Artery DiseaseaThe probability of an event (developing a disease) occurring in exposed people compared with the probability of the event in nonexposed people.Lederle et al. J Vasc Surg. 2003(2);38:329-334.
Aortic Aneurysm to CAD
Aortic Aneurysm to Cerebrovascular
Disease
NeverSmokers
Po
ole
d E
stim
ates
of
Rat
io o
f C
urr
ent
Sm
oke
rs’
RR
a
P<.00001
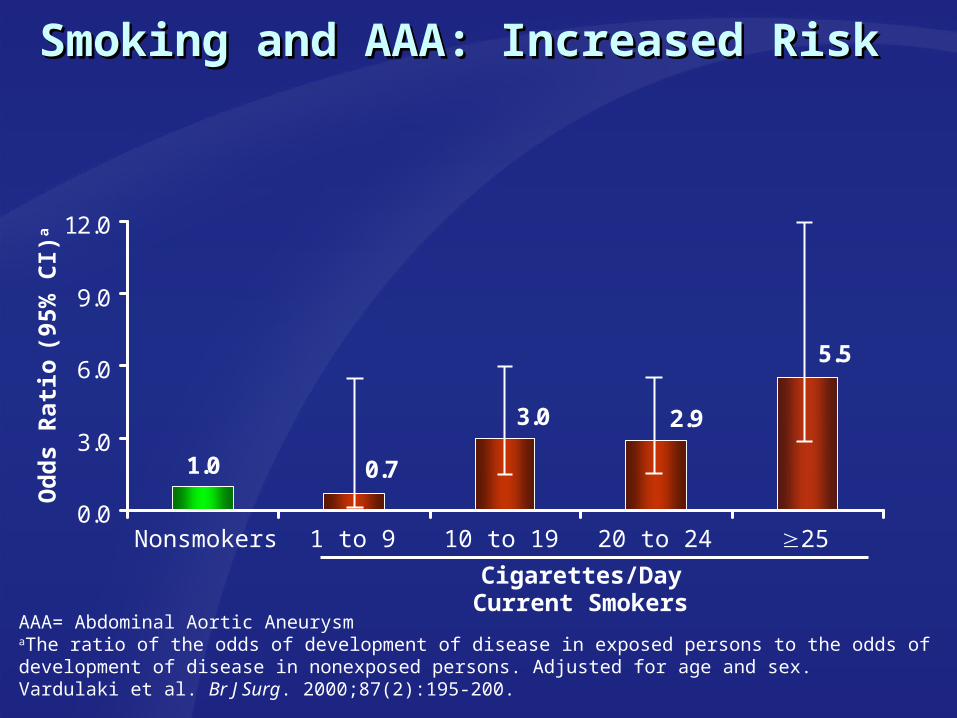
Smoking and AAA: Increased RiskSmoking and AAA: Increased Risk
AAA= Abdominal Aortic AneurysmaThe ratio of the odds of development of disease in exposed persons to the odds of development of disease in nonexposed persons. Adjusted for age and sex.Vardulaki et al. Br J Surg. 2000;87(2):195-200.
1.0
5.5
0.7
3.0 2.9
0.0
3.0
6.0
9.0
12.0
Od
ds
Rat
io (9
5% C
I)a
Nonsmokers 1 to 9 10 to 19 2520 to 24
Cigarettes/DayCurrent Smokers
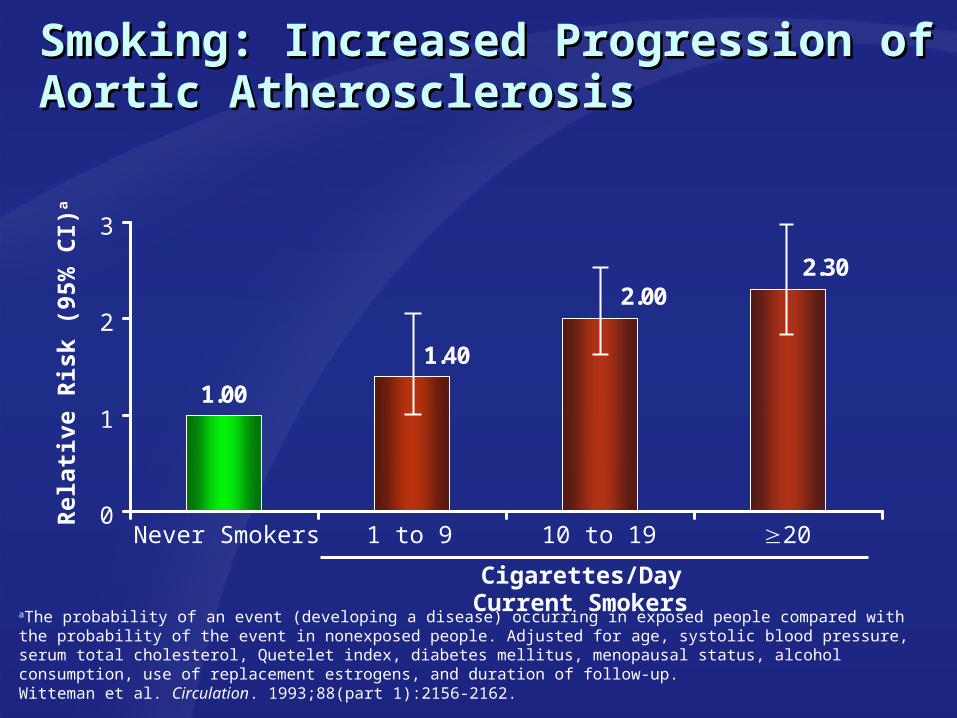
1.00
2.302.00
1.40
0
1
2
3
Smoking: Increased Progression of Smoking: Increased Progression of Aortic AtherosclerosisAortic Atherosclerosis
aThe probability of an event (developing a disease) occurring in exposed people compared with the probability of the event in nonexposed people. Adjusted for age, systolic blood pressure, serum total cholesterol, Quetelet index, diabetes mellitus, menopausal status, alcohol consumption, use of replacement estrogens, and duration of follow-up.Witteman et al. Circulation. 1993;88(part 1):2156-2162.
Rel
ativ
e R
isk
(95%
CI)
a
Never Smokers 1 to 9 10 to 19 20
Cigarettes/DayCurrent Smokers

Smoking: Effect on AAA ExpansionSmoking: Effect on AAA Expansion
AAA= Abdominal Aortic AneurysmBrady. Circulation. 2004;110:16-21.
P<.001
Ave
rag
e L
inea
r G
row
th R
ate
(mm
/yea
r)
2.532.83
0.0
0.5
1.0
1.5
2.0
2.5
3.0
Nonsmokers Current Smokers

Summary: Smoking and Abdominal Summary: Smoking and Abdominal Aortic Aneurysm (AAA)Aortic Aneurysm (AAA)
Current smokers have a higher risk of developing an Current smokers have a higher risk of developing an AAA than either coronary artery disease or AAA than either coronary artery disease or cerebrovascular diseasecerebrovascular disease
Smoking is associated with an increased risk ofSmoking is associated with an increased risk of– Formation of AAAFormation of AAA– Progression of aortic atherosclerosisProgression of aortic atherosclerosis– Expansion of AAAExpansion of AAA

Smoking and StrokeSmoking and Stroke

Smoking and StrokeSmoking and Stroke
Smoking contributes to Smoking contributes to 12% to 14% of all stroke deaths12% to 14% of all stroke deaths
Smoking may potentiate the effects Smoking may potentiate the effects of other stroke risk factorsof other stroke risk factors
Smoking increases stroke riskSmoking increases stroke risk– Acutely: effects on thrombus Acutely: effects on thrombus
formationformation– Chronically: increased burden Chronically: increased burden
of atherosclerotic diseaseof atherosclerotic disease
MRI of BrainWith an Acute Ischemic Stroke
Goldstein et al. Stroke. 2006;37:1583-1633; http://www.ucihs.uci.edu/stroke/whatisastroke.shtml. Accessed October 19, 2007.

20
30
40
50
Smoking: Increased Progression of Smoking: Increased Progression of Carotid AtherosclerosisCarotid Atherosclerosis BBoth active smoking and environmental tobacco smoke exposure are oth active smoking and environmental tobacco smoke exposure are
associated with increased progression of carotid atherosclerosis.associated with increased progression of carotid atherosclerosis.
aAdjusted for demographic characteristics, cardiovascular risk factors, and lifestyle variables (risk factor model and Keys score, education, leisure activity, body mass index, and alcohol use). bTo environmental tobacco smoke.Howard et al. JAMA. 1998;279(2):119-124.
Ex-smokers with
Exposureb
CurrentSmokers
Nonsmokerswithout
Exposureb
Pro
gre
ssio
n o
f In
tim
a-M
edia
l T
hic
knes
s, µ
m/3
y (
95%
CI)
a
Ex-smokerswithout
Exposureb
Nonsmokerswith
Exposureb
43.043.0
38.838.8
31.631.6 32.832.8
25.925.9

Smoking: Increased Risk of Fatal and Smoking: Increased Risk of Fatal and Nonfatal Stroke in WomenNonfatal Stroke in Women
1.0
3.8
2.92.5
0
1
2
3
4
5
6
1-14 15-24Nonsmokers
Rel
ativ
e R
isk
(95%
CI)
a
aThe probability of an event (developing a disease) occurring in exposed people compared with the probability of the event in nonexposed people. Adjusted for age, follow-up period, history of diabetes, hypertension, high cholesterol levels, and relative weight (in 5 categories).Colditz et al. N Engl J Med. 1988;318(15):937-941.
≥25
Cigarettes/DayCurrent Smokers

0
2
4
6
8
10
12
Smoking: Increased Risk of Hemorrhagic Smoking: Increased Risk of Hemorrhagic StrokeStroke
aThe probability of an event (developing a disease) occurring in exposed people compared with the probability of the event in nonexposed people.Adjusted for age, exercise, alcohol consumption, body mass index, history of hypertension, and history of diabetes. Kurth et al. Stroke. 2003;34:2792-2795.
Total Hemorrhagic Stroke
Rel
ativ
e R
isk
(95%
CI)
a
Intracerebral Hemorrhage
Subarachnoid Hemorrhage
Nonsmokers (n=20,339)
<15 Cigarettes/day (n=1914)
15 Cigarettes/day (n=3265)
2.062.06
3.433.43 2.392.39 2.892.891.741.74 4.044.04

Smoking: Increased Stroke MortalitySmoking: Increased Stroke Mortality
Cigarette smoking increases the risk of mortality from stroke in menCigarette smoking increases the risk of mortality from stroke in men
aTwenty-year age-adjusted mortality per 10,000 person-years for men. P<.014 for trend. Hart et al. Stroke. 1999;30:1999-2007.
30.9
39.0
50.6
0
10
20
30
40
50
60
15-241-15
Mo
rtal
ity
Rat
ea
≥25
Cigarettes/DayCurrent Smokers

Summary: Smoking and StrokeSummary: Smoking and Stroke
Smoking contributes to 12% to 14% of all stroke deathsSmoking contributes to 12% to 14% of all stroke deaths
Increased risk ofIncreased risk of– Progression of carotid atherosclerosisProgression of carotid atherosclerosis– StrokeStroke– Hemorrhagic strokeHemorrhagic stroke– Intracerebral hemorrhageIntracerebral hemorrhage– Subarachnoid hemorrhageSubarachnoid hemorrhage
Increased stroke-related mortalityIncreased stroke-related mortality
Cardiovascular Disease (CVD) and Cardiovascular Disease (CVD) and Environmental Tobacco SmokeEnvironmental Tobacco Smoke

Effects of Environmental Tobacco Smoke Effects of Environmental Tobacco Smoke on Cardiovascular Diseaseon Cardiovascular Disease Effects of environmental Effects of environmental
tobacco smoketobacco smoke risk of heart diseaserisk of heart disease platelet and endothelial platelet and endothelial
functionfunction arterial stiffnessarterial stiffness atherosclerosisatherosclerosis oxidative stressoxidative stress inflammationinflammation– ↓↓ heart rate variabilityheart rate variability energy metabolismenergy metabolism infarct sizeinfarct size
American Heart Association. Scientific Position, Risk Factors and Coronary Heart Disease, 2005. http://americanheart.org. Accessed February 2007; Barnoya et al. Circulation. 2005; 111:2684-2698; http://www.istockphoto.com/file_closeup/abuse/smoking/tobacco_products/3383715_cigarette_burning.php?id=3383715. Accessed October 11, 2007.

Environmental Tobacco Smoke: Prevalence of Environmental Tobacco Smoke: Prevalence of Heart DiseaseHeart Disease
Adjusted for age, systolic blood pressure, diastolic blood pressure, total cholesterol, HDL cholesterol, FEV, height, preexisting CAD, body mass index, triglycerides, white cell count, diabetes, physical activity, alcohol intake, and social class. aLight active refers to men smoking 1-9 cigarettes a day. bHeavy passive refers to upper three quarters of cotinine concentration combined (0.8 to 14.0 ng/mL). cLight passive refers to lowest quarter of cotinine concentration among nonsmokers (0-0.07 ng/mL). Whincup et al. BMJ. 2004;329:200-205.
Exposure to environmental tobacco smoke increases the risk of Exposure to environmental tobacco smoke increases the risk of heart disease among nonsmokers by 30%heart disease among nonsmokers by 30%
Years of Follow up
Pro
po
rtio
n W
ith
Maj
or
CA
D
0 5 10 15 200
0.05
0.10
0.15
0.20
Light activea
Heavy passiveb
Light passivec

Environmental Tobacco Smoke: Environmental Tobacco Smoke: Platelet ActivationPlatelet Activation
ns=not significant. a Unless marked as “ns,” differences for each value between groups were statistically significant at a level of P<.05. Schmid et al. Thromb Res. 1996;81:451-460.
Nonsmokers Current Smokers
pg
/mL
a
36.8
34.8
32.8
30.8
28.8
26.8
24.8
22.81 2 3 4 5 12
11-dehydro-thromboxane B2
nsns
ns
Day
Min
/10°
Pla
tele
tsa
1 2 3 4 5 12
Malondialdehyde
Day
5.6
2.5
3.2
3.6
4.0
4.4
4.8
5.2
ns ns nsns
ns
ns
ns
ns
nsns

Environmental Tobacco Smoke: Environmental Tobacco Smoke: Vascular Endothelial DysfunctionVascular Endothelial Dysfunction
CFVR is a measure of endothelial function in the coronary circulation. Otsuka et al. JAMA. 2001;286:436-441.
Acute exposure to environmental tobacco smoke significantly reduces Acute exposure to environmental tobacco smoke significantly reduces mean coronary flow velocity reserve (CFVR) in nonsmokersmean coronary flow velocity reserve (CFVR) in nonsmokers
CF
VR
(M
ean
±S
D)
PP<.001<.001
2.0
2.5
3.0
3.5
4.0
4.5
5.0
5.5 Nonsmokers Current Smokers
Before Acute Exposure After Acute Exposure

Environmental Tobacco Smoke: Environmental Tobacco Smoke: Risk of Acute Myocardial Infarction (MI)Risk of Acute Myocardial Infarction (MI)
aThe ratio of the odds of development of disease in exposed persons to the odds of development of disease in nonexposed persons. Adjusted for age, sex, region, physical activity, and consumption of fruits, vegetables, and alcohol. Adapted from Teo et al. Lancet. 2006;368:647-658.
NonsmokersNonsmokers
Od
ds
Rat
io (
95%
CI)
Od
ds
Rat
io (
95%
CI)
aa
Environmental Tobacco Smoke Exposure (Hours per Week)Environmental Tobacco Smoke Exposure (Hours per Week)
NeverNever 1-71-7 8-148-14 15-2115-21 2222
44
22
11
0.750.75
Exposure to environmental tobacco smoke increased the risk Exposure to environmental tobacco smoke increased the risk of non-fatal acute MI in a graded mannerof non-fatal acute MI in a graded manner

Summary: Cardiovascular Disease and Summary: Cardiovascular Disease and Environmental Tobacco SmokeEnvironmental Tobacco Smoke
Exposure to environmental tobacco smoke increases Exposure to environmental tobacco smoke increases risk ofrisk of– Heart disease, by 30%Heart disease, by 30%– Acute myocardial infarction (MI)Acute myocardial infarction (MI)
Environmental tobacco smoke affects multiple factors Environmental tobacco smoke affects multiple factors associated with the development of coronary artery associated with the development of coronary artery disease, includingdisease, including– Platelet activationPlatelet activation– Vascular endothelial dysfunctionVascular endothelial dysfunction

Cardiovascular Benefits of Cardiovascular Benefits of Smoking CessationSmoking Cessation

Cardiovascular Benefits of Cessation: Cardiovascular Benefits of Cessation: FibrinogenFibrinogen After 2 weeks of cessation by formerly chronic smokers, both fibrinogen After 2 weeks of cessation by formerly chronic smokers, both fibrinogen
concentration and the rate of fibrinogen synthesis are reducedconcentration and the rate of fibrinogen synthesis are reduced
ASR=absolute rate of fibrinogen synthesis. aAbstention period of 2 weeks. Hunter et al. Clin Sci (Lond). 2001;100(4):459-465.
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
0
5
10
15
20
25
30
Fib
rin
og
en A
SR
mg
/kg
Fib
rin
og
en A
SR
mg
/kg
Pla
sma
Fib
rin
og
enP
lasm
a F
ibri
no
gen
Co
nce
ntr
atio
n (
g/L
)C
on
cen
trat
ion
(g
/L)
P<.001 P<.001
SmokingSmoking AbstentionAbstentionaa SmokingSmoking AbstentionAbstentionaa
16.1
24.12.49
3.06

6.1
7.0
0
1
2
3
4
5
6
7
8
Cardiovascular Benefits of Cessation: Cardiovascular Benefits of Cessation: White Blood CellsWhite Blood Cells
aAbstention period of 17 weeks.Eliasson et al. Nicotine Tob Res. 2001;3(3):249-255.
AbstentionaSmoking
Wh
ite
Blo
od
Cel
ls (
×10
9 /l) P<.026

0.420.33
0.0
0.2
0.4
0.6
0.8
1.0
1.321.16
0.0
0.5
1.0
1.5
2.0
2.5
3.0
Cardiovascular Benefits of Cessation: Improved Cardiovascular Benefits of Cessation: Improved Lipid ProfileLipid Profile
HDL=high-density lipoprotein; LDL=low-density lipoprotein. aAbstention period of 17 weeks.Eliasson et al. Nicotine Tob Res. 2001;3(3):249-255.
P<.001
HD
L (
mm
ol/L
) 3.523.78
0.0
1.0
2.0
3.0
4.0
5.0
LD
L (
mm
ol/L
)
Smoking Abstentiona
Smoking Abstentiona
HD
L/L
DL
Rat
io
P<.015
P<.001
Smoking Abstentiona

7276
0
20
40
60
80
100
120
Cardiovascular Benefits of Cessation: Cardiovascular Benefits of Cessation: Hemodynamic ProfileHemodynamic Profile Smoking cessation is associated with an improvement in Smoking cessation is associated with an improvement in
hemodynamic parameters.hemodynamic parameters.
a Abstention period of 6 months. Oren et al. Angiology. 2006;57(5):564-568.
8790
0
20
40
60
80
100
120
Hea
rt R
ate
(Bea
ts/m
in)
P<.05
Mea
n A
rter
ial
Pre
ssu
re (
mm
Hg
)
Smoking
P<.05
SmokingAbstentiona Abstentiona

0
10
20
30
40
50
60
70
80
90
Au
gm
enta
tio
n In
dex
(%
)b
Cardiovascular Benefits of Cessation: Cardiovascular Benefits of Cessation: Hemodynamic Profile (cont’d)Hemodynamic Profile (cont’d) Smoking cessation is associated with an improvement in arterial Smoking cessation is associated with an improvement in arterial
compliancecompliance
aProvides an assessment of small arteriolar compliance. bThe amplitude of the reflected wave depends on the stiffness of the small vessels and large arteries and thus provides a measure of systolic arterial stiffness.cAbstention period of 6 months. Oren et al. Angiology. 2006;57(5):564-568.
6.3
5.1
0
2
4
6
8
10
Osc
illat
ory
Co
mp
lian
ce
(mL
/mm
Hg
× 1
00)a
P<.01
P<.05
Smoking Abstentionc Smoking Abstentionc
63.1
50.6

Cardiovascular Benefits of Cessation: Cardiovascular Benefits of Cessation: Platelet EffectsPlatelet Effects Smoking is associated with reduced platelet volume and enhanced platelet Smoking is associated with reduced platelet volume and enhanced platelet
cAMPcAMPcc response to stimulation of adenylate cyclase with prostaglandin E response to stimulation of adenylate cyclase with prostaglandin E11
aPGE=prostaglandin E1; bMPV=mean platelet volume; ccAMP= cyclic adenosine monophosphate.Terres et al. Am J Med. 1994;97:242-249.
0 1 2 1 4 8 9 1 4 8 9 12Weeks
4
8
10
12
6
cAM
P A
fter P
GE
(nm
ol/L
) (95
% C
I)a
P=.02
MPV
(fL)
(95%
CI)b
Weeks
P<.001
8.2
8.4
8.6
9.0
8.8
0 1 2 1 4 8 9 1 4 8 9 12
NicotineChewing
Gum
Smoking Nonsmoking/Nonchewing
Smoking NicotineChewing
Gum
Nonsmoking/Nonchewing

Cardiovascular Benefits of Cessation: Cardiovascular Benefits of Cessation: Platelet Effects (cont’d)Platelet Effects (cont’d)
aQuit smoking for 28 days. bResumed smoking after quitting for 14 days.ADP=adenosine diphosphate. ADP is a platelet aggregation agonist.Morita et al. J Am Coll Cardiol. 2005;45:589-594.
Smoking abstinence is associated with reduced platelet Smoking abstinence is associated with reduced platelet aggregabilityaggregability
ADP=5.0 µmol/L
Group Aa Group Bb
Pla
tele
t A
gg
reg
atio
n (
%)
0
20
60
100
40
80
Time (Days)
0 7 14 21 28
NS
P<.01
NS
NS
P<.01

Cardiovascular Benefits of Cessation: Cardiovascular Benefits of Cessation: Reduced Risk of Arrhythmic DeathReduced Risk of Arrhythmic Death Cessation of cigarette smoking is associated with a reduction in arrhythmic Cessation of cigarette smoking is associated with a reduction in arrhythmic
death for patients with post-myocardial infarction left ventricular dysfunctiondeath for patients with post-myocardial infarction left ventricular dysfunction
Peters et al. J Am Coll Cardiol. 1995;26(5):1287-1292.
P=.040
Survival in Years
Su
rviv
al (
%)
0
20
40
60
80
100
0 2 31
Ex-smokers
Smokers

Cardiovascular Benefits of Cessation: Cardiovascular Benefits of Cessation: Reduced Risk of Acute Myocardial Reduced Risk of Acute Myocardial Infarction (MI)Infarction (MI)
aThe ratio of the odds of development of disease in exposed persons to the odds of development of disease in nonexposed persons. Adjusted for sex, region, diet, alcohol, physical activity, consumption of fruits, vegetables, and alcohol.Adapted from Teo. Lancet. 2006;368:647-658.
PP<.0001<.0001
CurrentCurrent >1-3>1-3 >5-10>5-10 >10-15>10-15 2020
Ex-smokers (Years Since Cessation)Ex-smokers (Years Since Cessation)
>3-5>3-5 >15-20>15-20
Od
ds
Rat
io (
95%
CI)
Od
ds
Rat
io (
95%
CI)
aa
44
22
11

Cardiovascular Benefits of Citywide Smoke-Cardiovascular Benefits of Citywide Smoke-Free Ordinance: Reduced Incidence of Acute Free Ordinance: Reduced Incidence of Acute MIMI
Bartecchi et al. Circulation. 2006;114:1490-1496.
27% reduction in the incidence of acute myocardial infarction (MI) after 27% reduction in the incidence of acute myocardial infarction (MI) after implementation of a smoke-free ordinance in Pueblo City, Coloradoimplementation of a smoke-free ordinance in Pueblo City, Colorado
AM
I C
ou
nts
per
100
,000
Per
son
-Yea
rs
257
119
187
116
0
50
100
150
200
250
300
Pueblo City El Paso County
Preordinance Postordinance
P<.001

Cardiovascular Benefits of Cessation: Reduced Cardiovascular Benefits of Cessation: Reduced Risk of Recurrent Cardiac ArrestRisk of Recurrent Cardiac Arrest The risk for recurrent cardiac arrest is lower among those who quit smoking The risk for recurrent cardiac arrest is lower among those who quit smoking
than among continuing smokersthan among continuing smokers
aAbstention period of 3 years. Hallstrom et al. N Engl J Med. 1986;314:271-275.
27
19
0
5
10
15
20
25
30
Current Smokers Ex-smokersa
Occ
urr
ence
at
3 Y
ears
(%
)
P=.038
Recurrent Cardiac Arrest

Cardiovascular Benefits of Cessation: Reduced Cardiovascular Benefits of Cessation: Reduced Mortality After Percutaneous Coronary Mortality After Percutaneous Coronary RevascularizationRevascularization Current smokers had a significantly greater risk of overall mortality after Current smokers had a significantly greater risk of overall mortality after
percutaneous coronary revascularizationpercutaneous coronary revascularization
Su
rviv
al (
%)
100
80
60
40
20
00 2 3 4 5 6 7 8 9 10 11 12
Years After Index Procedure
Hasdai. N Engl J Med. 1997;336(11):755-761.
Quitters
Persistent Smokers

Cardiovascular Benefits of Cessation: Reduced Cardiovascular Benefits of Cessation: Reduced Mortality After Coronary Artery Bypass GraftMortality After Coronary Artery Bypass Graft
Estimated survival benefit associated with smoking cessation Estimated survival benefit associated with smoking cessation increased from 3% at 5 years to 10% at 10 years and 15% at 15 yearsincreased from 3% at 5 years to 10% at 10 years and 15% at 15 years
Adapted from van Domburg et al. J Am Coll Cardiol. 2000;36(3):878-883.
Pro
bab
ilit
y o
f S
urv
ival
(%
)
0 5 10 15 20
Years
PP<.0001 (Ex-smokers vs <.0001 (Ex-smokers vs Current Smokers)Current Smokers)
Nonsmokers
Persistent Smokers
100
80
60
40
20
0
Quitters

Cardiovascular Benefits of Cessation: Cardiovascular Benefits of Cessation: Reduced Progression of Peripheral Vascular Reduced Progression of Peripheral Vascular DiseaseDisease
Jonason et al. Acta Med Scand. 1987;221:253-260.
Years
Res
t P
ain
, C
um
ula
tive
(%
)
30
20
10
0
P=.049
2 71 6543
Abstention
Smoking

Cardiovascular Benefits of Cessation: Cardiovascular Benefits of Cessation: Reduced Risk of StrokeReduced Risk of Stroke
aThe probability of an event (developing a disease) occurring in exposed people compared with the probability of the event in nonexposed people. Adjusted for age and treatment assignment.Robbins et al. Ann Intern Med. 1994;120(6):458-462.
1.0
2.5
2.0
1.2
0
1
2
3
4
Nonsmokers Ex-smokers CurrentSmokers
(<20 cig/d)
CurrentSmokers
(≥20 cig/d)
Rel
ativ
e R
isk
(95%
CI)
a
P for trend <.0001

Cardiovascular Benefits of Smoking CessationCardiovascular Benefits of Smoking Cessation
Short-term BenefitsShort-term Benefits fibrinogen concentrationfibrinogen concentration rate of fibrinogen synthesisrate of fibrinogen synthesis WBCsWBCs Improved HDL/LDL ratioImproved HDL/LDL ratio risk of strokerisk of stroke HDL; decreased LDLHDL; decreased LDL arterial pressurearterial pressure HRHR Improved arterial complianceImproved arterial compliance risk of arrhythmic death after MIrisk of arrhythmic death after MI platelet volumeplatelet volume Enhanced platelet cAMP response to Enhanced platelet cAMP response to
stimulation of ADP with prostaglandin E1stimulation of ADP with prostaglandin E1 smoking-induced platelet aggregabilitysmoking-induced platelet aggregability
Long-term BenefitsLong-term Benefits Reduced risk ofReduced risk of
– Stroke Stroke – Repeat CABG Repeat CABG – Recurrent coronary events Recurrent coronary events
after MIafter MI– Arrhythmic death after MIArrhythmic death after MI– Secondary CVD events Secondary CVD events – Revascularization procedure Revascularization procedure
after CABGafter CABG Reduced Reduced
– Mortality after CABGMortality after CABG– Mortality after PTCAMortality after PTCA– Levels of inflammatory Levels of inflammatory
markers associated with markers associated with progression of CVD progression of CVD (C-reactive protein, WBC, and (C-reactive protein, WBC, and fibrinogen)fibrinogen)
Twardella et al. Eur Heart J. 2004;25:2101-2108; Morita et al. J Am Coll Cardiol. 2005;45:589-594; Oren et al. Angiology. 2006;57:564-568; Terres et al. Am J Med. 1994; 97:242-249; Nilsson et al. J Int Med. 1996; 240:189-194; Peters et al. J Am Coll Cardiol. 1995;26:1287-1292; Rea et al. Ann Intern Med. 2002;137: 494-500; Hasdai et al. N Engl J Med. 1997;336:755-761; van Domburg et al. J Am Coll Cardiol. 2000; 36:878-883; Bakhru et al. PLoS Med. 2005;2:e160; Eliasson et al. Nicotine Tob Res. 2001;3 :249-255; Hunter et al . Clin Sci. 2001;100 :459-465; Wannamethee et al. JAMA. 1995;274:155-160.