
A National Collaboration Initiative for the Canadian Aerospace Industry Funding partner:

the Canadian Heart Health Initiative
Building Block towards a
Countrywide Integrated
Chronic Disease Prevention
Action
NON COMMUNICABLE DISEASE SEMINAR, THL, Helsinki, FinlandN
Sylvie Stachenko

About Canada
A Federated System
• 10 Provinces, 3 Territories and Federal
Government
• Provinces and territories primary
responsibility for health services– Adherence to Canada Health Act
– Federal transfers support provincial/territorial services
– Shared decision-making
• Universal health insurance: medical and
hospital care

The Burden of Chronic Disease in
Canada
Individuals and families
18,000,000 live with chronic illness
Chronic disease accounts for 87% of disability
High risk groups
Increased prevalence in vulnerable communities (e.g. Aboriginals) and in socio-economically disadvantaged groups.
Economy
Direct health care costs: 67% of total direct costs are expended on chronic diseases
Indirect costs: 60% of total indirect costs), e.g, loss of productivity and foregone income
All these numbers are increasing
Aging, increased prevalence of some risk factors, e.g. obesity
A rich history in health
promotion
Incremental Investment in Chronic
Disease Prevention
• Single diseases
• Single risk factors
• Specific population groups
Towards an integrated
approach to NCD prevention…
at the core of the CINDI concept...
Commonality of risk factors for major NCD’s
Systems approach to delivery
Partnerships

National Disease / Risk Factor
Strategies
Partnership models
Good foundation for integrated
chronic disease policies / programs
Canadian Strategy for Tobacco
Control
Governance
- Multisectoral Partnerships
Multi-pronged Strategy
- Access
- Advertising and Promotion
- Packaging and Labelling
- Product Regulations
- Taxes
- Smuggling
- Enforcement and Education
Sustained over time

Some successes...

Trends in Smoking Current Smokers,
12+ years, 2001-2009, Canada
Source::Canadian Community Health Survey
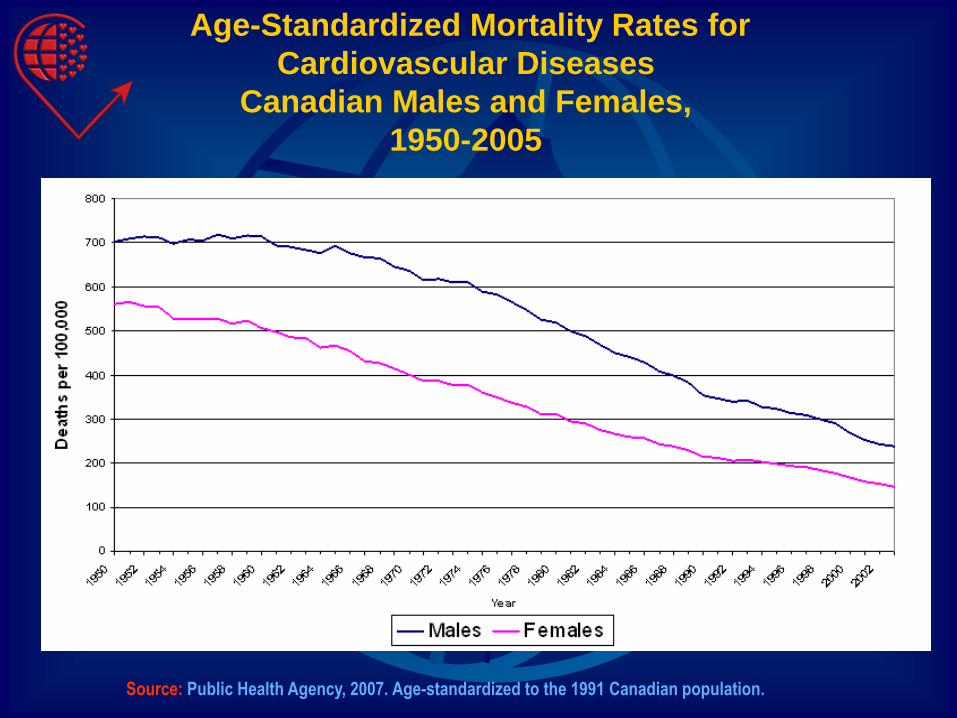
Age-Standardized Mortality Rates for
Cardiovascular Diseases
Canadian Males and Females,
1950-2005
Source: Public Health Agency, 2007. Age-standardized to the 1991 Canadian population.

Some Emerging Trends

Source: Why Health Care Renewal Matters: Lessons from Diabetes,
The Health Council of Canada, March 2007
More and More
Canadians are Obese
CANADA overall*
23% obese in 2007
15% obese in 1992*No data available for the Territories
YUKON*
NORTHWEST
TERRITORIES*NUNAVUT*
BRITISH
COLUMBIA
19%
14%ALBERTA
25%
15% SASKATCHEWAN
31%
16%
MANITOBA
28%
17%ONTARIO
23%
13%
QUÉBEC
22%
13%
NEWFOUNDLAND
and LABRADOR
34%
22%
NEW
BRUNSWICK
29%
18%
NOVA
SCOTIA
25%
19%
PRINCE
EDWARD
ISLAND
26%
16%

Self-Reported Risk Factor Prevalence,
2007
Source: Source: Centre for Chronic Disease Prevention and Control, Public Health Agency of Canada, 2007 using
Statistics Canada, Canadian Community Health Survey Data.
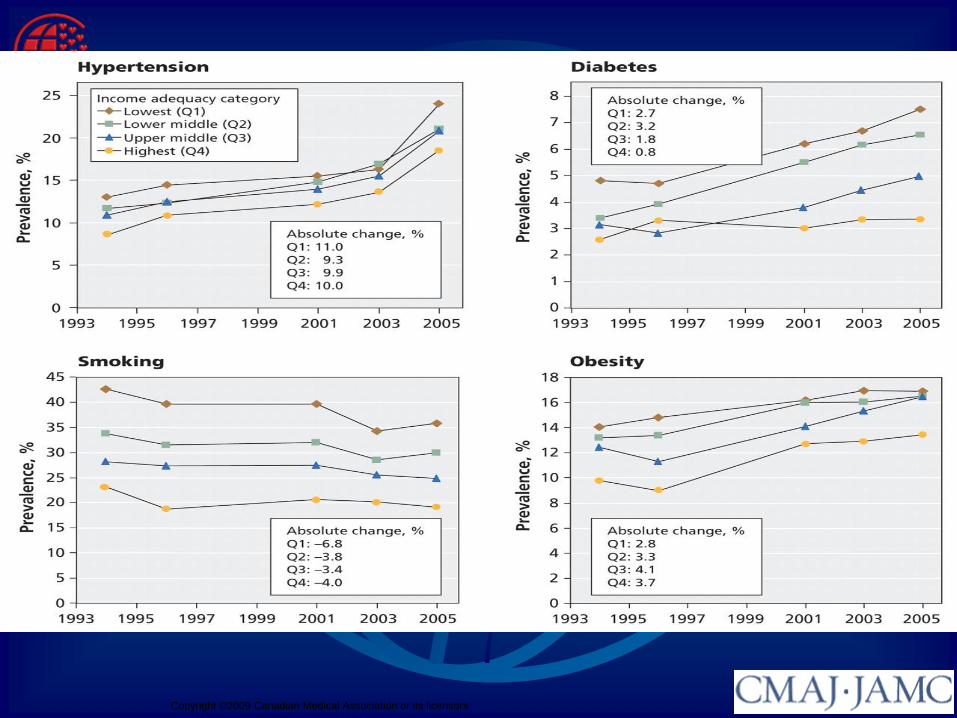
Copyright ©2009 Canadian Medical Association or its licensors

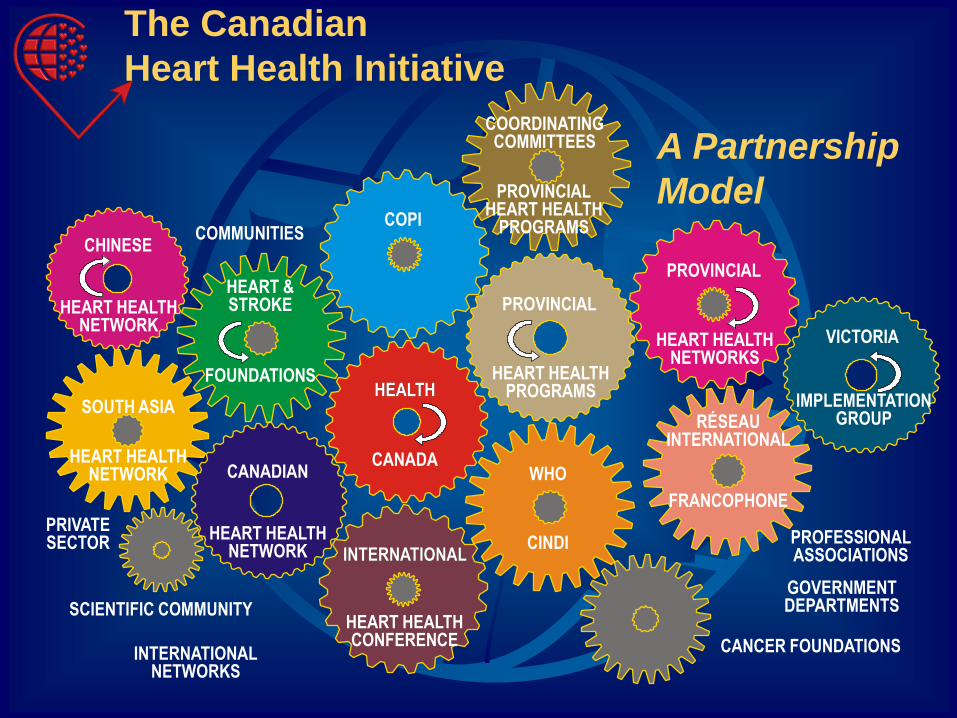
The Canadian Heart Health Initiative
Entry point for an
integrated approach to
chronic disease
prevention

Common Risk Factor Approach

Canadian Heart Health Initiative
Co funded by theNational Health Research Development
Programand National Department of Health
Provide practical and evidence based know how on integrated action
Conceived in 1987 as per the Ottawa Charter
to strengthen public health capacity in health
promotion and implement integrated approaches
interventions to address CVD
To apply the existing available knowledge on CVD
prevention in diverse systems across Canada
Uses heart health as entry point with a view to expand
to other NCDs that share common risk factors
Canadian Heart Health Initiative
backbone of CINDI

Integration as a Principle of
Program Design
• Organizing Principle• Working together to address risk factors and their
underlying determinants
• Maximizing the preventive dose
• In Practice – Partnership approaches and
modern governance arrangements• Concerted and coordinated action around:
• Policy and program
• Surveillance and evaluation
• Funding systems
• Research agenda
• Dissemination
CHINESECOMMUNITIES
SOUTH ASIA
FOUNDATIONS
CANADIAN
COPI
CANADA
HEALTHHEALTH
SCIENTIFIC COMMUNITY
INTERNATIONALINTERNATIONAL
WHO
CINDI
PROVINCIAL
PROVINCIAL
VICTORIA
IMPLEMENTATIONGROUP
CANCER FOUNDATIONS
RÉSEAUINTERNATIONAL
FRANCOPHONE
The Canadian
Heart Health Initiative
A Partnership
ModelPROVINCIALHEART HEALTH
PROGRAMS
COORDINATINGCOMMITTEES
HEART HEALTHPROGRAMS
HEART HEALTHNETWORKS
PROFESSIONALASSOCIATIONS
GOVERNMENTDEPARTMENTS
HEART HEALTHCONFERENCE
HEART HEALTHNETWORK
HEART HEALTHNETWORK
HEART HEALTHNETWORK
INTERNATIONALNETWORKS
PRIVATESECTOR
HEART &STROKE
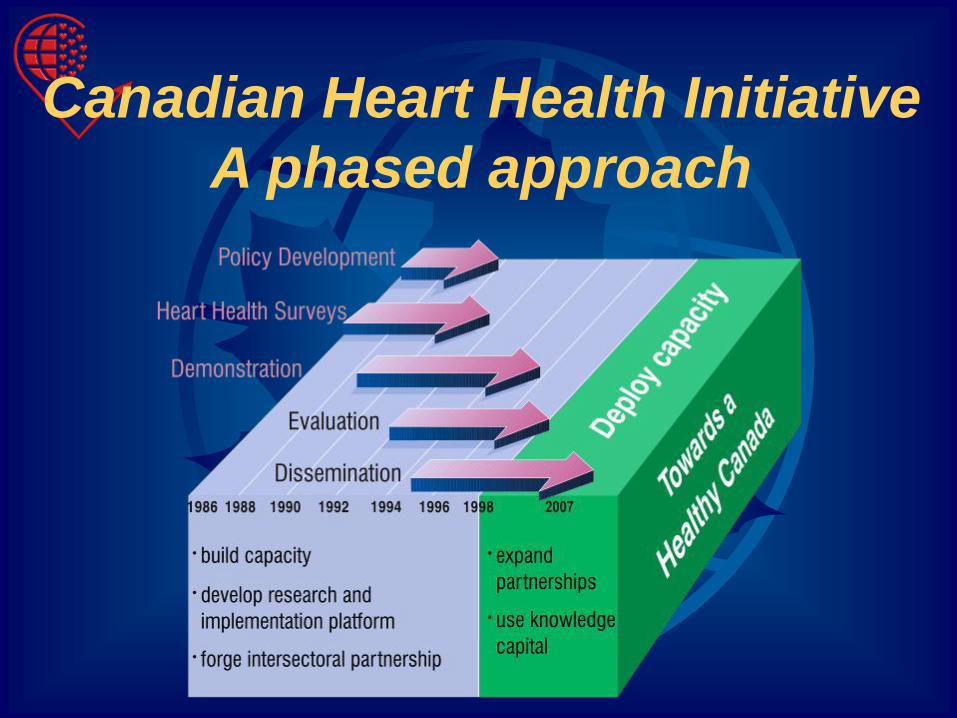
Canadian Heart Health Initiative
A phased approach

Policy Development
(1986-88)
• Federal / Provincial working group
recommendations
• Consultations with stakeholders
• Consensus approach to Policy
Framework
• “Promoting Heart Health in Canada”
(1987)

Provincial Heart Health Surveys
(1986-92)
• 10 provincially-based surveys were
conducted
• Built provincial capacity
• Risk factor data and physical
measurement
• Media / Marketing for visibility
• Consolidated into one national database
– The Canadian Heart Health Database
Demonstration Phase
(1989-97)
• To determine feasibility of implementing
a comprehensive approach to CVD
prevention at the community level
• 311 community-based provincial heart
health multifactorial demonstration
programs in 10 provinces
• Common risk factor focus: tobacco,
physical activity, nutrition eg fat intake

A focus on evaluation
• Outcome evaluation on a focused set of risk factors through risk factor surveys
• Process evaluation guidelines developed• common process indicators for
heart health strategies
• increased capacity of public health departments to monitor and implement prevention programs
• Canadian Heart Health Evaluation Database
• CHHI - Process Evaluation of the Demonstration Phase

• Rich experience on integrated action at the
community level across the country
• Broadened experience on community
mobilization and participation in Canada
… coalition building, partnership approaches
Canadian Heart Health InitiativeKey Achievements

• New skills for public health practitioners:
• Organizational development
• Leadership development
• Conflict resolution
• Marketing
• Political process
• Advocacy and communication
• Capacity was transferable to other issues
Canadian Heart Health Initiative

Other Achievements
• First national database on behavioural and physical risk factors which is ongoing
• Linkage to mortality and morbidity data
• Flexible network management model for pan-Canadian initiatives in a decentralized environment
• Knowledgeable trained teams at all levels
with skills in planning and evaluation in the
delivery of integrated approaches
• Link to international efforts such as WHO CINDI/CARMEN

Learnings from the
Demonstration Phase
• Combination of science and practice powerful
force to advance the prevention agenda –visible
results are critical to secure political
commitment
• Focused mainly on community mobilization and
formal public health infrastructure – health care
system not fully mobilized…..insufficient
supportive policy changes in other sectors
• Need to link up with other targeted prevention
initiatives and combine strategies whenever
possible (CHHI, Diabetes, Canadian Strategy on
Cancer Control…)

Dissemination Phase
• Research dissemination projects
• Building on the learnings of the CHHI
– Towards an integrated approach to
chronic disease prevention

Canadian Heart Health
Dissemination Project
• Description
and synthesis
of 9 provincial
dissemination
projects
- published
http://www.science.mcmaster.ca/chhdp/CHHDP_IE.html
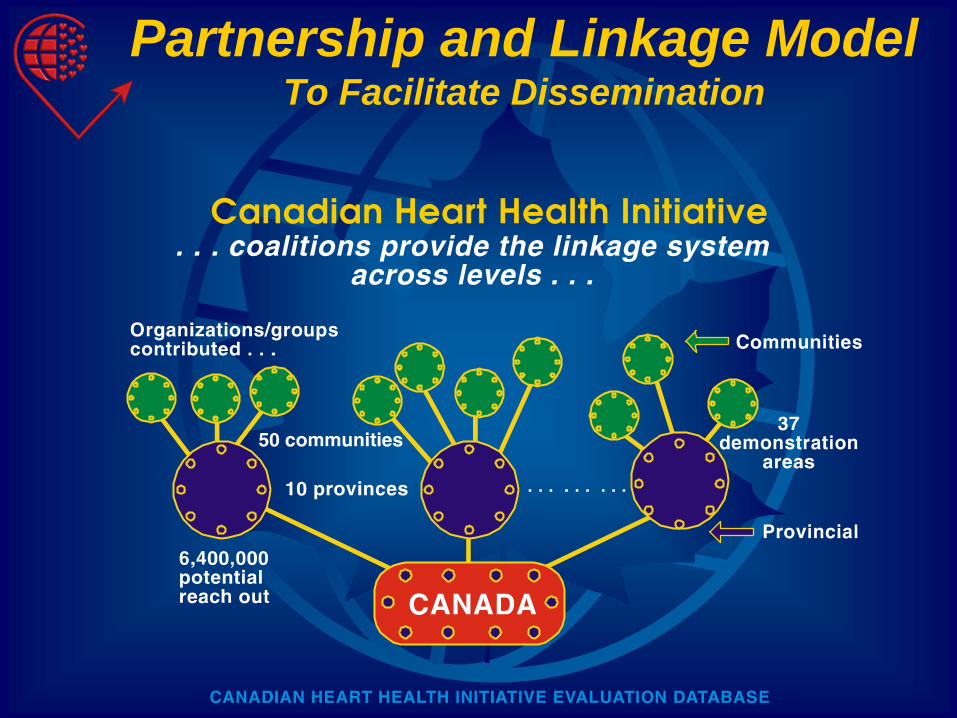
Partnership and Linkage ModelTo Facilitate Dissemination

Dissemination PhaseTowards an Integrated Approach to
Chronic Disease Prevention
• Expanding existing heart health coalitions
to chronic disease alliances at national,
provincial and community levels
– Chronic Disease Prevention Alliance
of Canada
. . . . . . . . .
– Provincial alliances
– … Important role of civil society
Building on the
Heart Health Platforms to
Guide Integrated Action
• Knowledge Synthesis
and exchange
• Surveillance
• New National Governance
Mechanisms
Knowledge Synthesis and
Exchange
• Comprehensive learning system• National Best Practice Consortium for Integrated Chronic
Disease Prevention and Control • www.phac.gc.ca/cbpp
• Observatory of Chronic Disease Policy • www.phac-aspc.gc.ca/ccdpc-cpcmc
• Supportive infrastructure for NCD preventive
research• Canadian Institutes for Health Research
• Health Promotion Research Consortium
• Knowledge networks
• New “demonstration sites” to evaluate and monitor
intersectoral NCD prevention approaches• Alberta WHO CINDI demonstration site
… … …

Surveillance
• Towards a comprehensive surveillance
system for chronic diseases
• Accommodates existing initiatives building on
disease and risk factor surveillance but focus on
coordination among different levels and
jurisdictions
• Stronger emphasis on data analysis, interpretation
and dissemination
• National ongoing risk factor surveys extended to
capture information on determinants
… … …

New Governance Mechanisms
to support
integrated Chronic Disease
Prevention• Centre for Chronic disease Prevention and
Control (PHAC)
• Public Health Network (cross jurisdictional)• Expert group on chronic diseases
• Intersectoral Healthy Living Network… Moving towards “Whole of Government
Approaches” at the national level
• Chronic Disease Prevention Alliance of Canada
Federal Integrated Chronic
Disease Prevention Strategy
• Combines:• Inter-sectoral action on diet and physical activity
with disease-specific actions related to cancer,
diabetes and cardiovascular disease
• Three pronged:• Promote health through inter-sectoral action
• Minimize risk of chronic disease and injury
• Detect early and effectively manage
chronic health problems and injuries
• Implemented by:• Combining actions of public health and
primary health care
• Involving multiple sectors and acting in
multiple settings
Provincial Territorial Chronic
Disease EffortsMoving towards … Whole of government approaches
Some reflections on moving
knowledge into NCD action
Value Added of a Policy Framework
• Articulation of policy principles, issues, strategies
• Informed/focused debate
• Make complexity clear
• Additional information research needs?
• Link various levels: national, regional, community
• Identify stakeholders: health and non-health sectors
basis for partnerships
political support
towards an action plan

The importance of building
capacity• Demonstration projects, evaluation,
tools and resources, surveillance
Role of Knowledge Brokers
• Knowledge brokering links
researchers and decision
makers, facilitating their
interaction so that they are
able to:
• better understand each other's
goals and professional culture,
• influence each other's work,
• forge new partnerships, and
• use evidence into decision
making.
• Individuals or organizations
can be knowledge brokers
adapted from Murphy, 2006

Role of Credible champions and
leaders• People and their interactions
matter more than the message
• On-going liaison and institution
inter-connections
• Personal contact and trust-
building through quality
relationships over time can
offer systems change potential
• Necessary for:
– Access to decision-making
settings
– Credibility
In memoriam Dr. Andrés PetrasovitsFebruary 11, 1937 – July 24, 2001
• Engage the media
• Use of local case studies– “Stories” make issues real
• Use of visuals
– Geographic Information Systems (GIS)
• Visuals and Colors (rather than stats)
to communicate urgency
Use Effective Communication Strategies
Effective Communication Strategies
• Customise the message
– Politicians and policy makers:
key points, implications, policy direction
and costs
– Informed user:
access to data for manipulation e.g.
Chronic Disease Infobase on Web
– General public:
packaged information
Create public demand but takes
time, reliable
information
Gosmokefree!

Partnerships with nongovernmental
organizations
• Chronic Disease Prevention
Alliance of Canada

Involve the End Users
• Meaningful engagement of stakeholders
that will use the data
e.g. risk factor surveys
Address Concerns of
Decision Makers
• Focused on solutions and cost of policies
• Need to supplement data with cost
effectiveness studies,consumer research,etc
• Timing and policy window
– Include short term objectives
Make the economic argument
• Work with economists to assess
economic impact of trends – important
for government
• Projections to make the case for status
quo

Use of projections and
economic modeling
The Business Case: British Columbia
100
90
80
70
60
50
40
30
20
10
0
-10
Revenue Growth – 3%
Education Growth 3%
Health Growth 8%
Balanced Budget
–
–
Other spending reaches zero by 17/18
Percent
TOTAL 100.0%
71.3%
27.0%
-0.6%
41.6%
28.4%
27.0%
53.6%
27.0%
16.6%
Health
Education
Other
04/05 05/06 06/07 07/08 08/09 09/10 10/11 11/12 12/13 13/14 14/15 15/16 16/17 17/18
Year

Document innovation and learn
from a variety
of models• ActNow! BC
• Quebec Public Health Act
• Intersectoral community initiatives

Develop mechanisms for
sharing and
disseminating innovation

Thank you
Kiitos


















