The Best for Every Child - Public Health Agency · A consensus has development amongst...
216
A report on the potential to transform disadvantaged communities in Lisburn through early intervention The Best for Every Child Researched and written by Barnardo’s NI, commissioned by Resurgam Trust Dr Roger Courtney Public Health Agency
Transcript of The Best for Every Child - Public Health Agency · A consensus has development amongst...

A report on the potential to transform disadvantaged communities in Lisburn through early intervention
The Best forEvery Child
Researched and written by Barnardo’s NI, commissioned by Resurgam TrustDr Roger Courtney
Public HealthAgency


Page 1
Contents
Page
i. ExecutiveSummary 2
1. Introduction 6
2. TheNeedsofDisadvantagedCommunitiesinLisburn 10
3. WhyEarlyIntervention? 37
4. PublicPolicyContext 46
5. TheoryofChange 75
6. OperatingModel 95
7. ImplementationPlan 102
8. Bibliography 108
Appendices
1. TermsofReference 114
2. MembershipoftheEarlyInterventionSteeringGroup 116
3. Summariesofprovenearlyinterventionprogrammes 117
4. EarlyInterventionSites&programmesintheUKandIreland 198 (Nottingham,youngballymunandWestTallaghtCDI)
Thetitleofthisreport,“Thebestforeverychild”isaquotefromoneoftheparentswhoparticipatedintheconsultationsduringtheresearchphaseindevelopingthisreport

Page 2
1. IntroductionThisfeasibilitystudyandconsultationwascommissionedfromBarnardo’swithfundingfromthePublicHealthAgency,byResurgamDevelopmentTrustrepresentingcommunityandyouthorganisationsindisadvantagedcommunitiesintheCityofLisburn,includingOldWarren,Hilden,Hillhall,Tonagh,KnockmoreandLaganValley.Itinvolvedconsultationswithaverywiderangeofcommunityorganisations,schoolsandprofessionalagenciesworkinginLisburn.Italsoincludedresearchinto:theneedsofthetargetareas;thedesiredoutcomesforchildrenandyoungpeople;theevidenceandargumentsfortakinganearlyinterventionapproachtotheissues;thepublicpolicycontextandtheextentthatitmightsupportanearlyinterventionapproach;andtheevidenceofthepotentialimpactofdeliveringparticularprovenprogrammesinthetargetareasofLisburn.
2. TheneedsofdisadvantagedcommunitiesinLisburnResearchintotheneedsofdisadvantagedareasofLisburncomplementedbyconsultationswithlocalcommunitygroupsandprofessionalsworkinginthetargetareasidentifiedverysignificantissuesconcerningthehealth,wellbeing,safetyandsecurityofthepopulationintheseareas,whichhaveaverydetrimentaleffectonthelivesofmanyfamilies.Concernsaboutparentingwerealsoveryprominentinmostoftheconsultations.Thesefindingsareconsistentwiththeinternationalliteratureoninequalityanddeprivationonarangeofwellbeingindicators.
Whatwasmoreshockingwastheverypooreducationaloutcomesofthechildrenandyoungpeople,rightfromprimaryschool.Ofthoseattendingthethreepost-primarycontrolledandintegratedsecondaryschoolsinLisburn,three-quartersleaveschoolwithout5+GCSEswithEnglishandMathsandveryfewgoontouniversityorcollege.Therewassignificantevidenceofeducationalunder-achievementbeingreplicateddownthegenerations.Thenatureofemploymentinthe21stCenturywouldsuggestthat,asaresultofpooreducationalachievement,thelevelofdeprivation,andtheextentofpoorhealthandwellbeing,intheseareaswill,ifnotarrestedbyamajorintervention,increasefurtherinfutureyears.Itwasclearfromtheresearchthattinkeringattheedgesoftheproblemwillnotbeenoughtotacklethischronicproblem:asubstantialandcomprehensiveinitiativeisurgentlyrequiredifthenextgenerationoflivesofchildrenandyoungpeopleisnottobeblighted.
3. WhyEarlyIntervention?Aconsensushasdevelopmentamongstneuro-scientists,psychologists,economistsandothersconcernedwiththedevelopmentofchildrenandyoungpeoplethat:■ 80%ofbraindevelopmenthappensbeforeachildisthreeyearsoldandsothese
arethemostcriticalyearstoinvestinthedevelopmentofthechild;
Executive Summary

Page 3
■ investingintheseearlyyearsandintheearlystageswhenchallengesinachild’slifearebecomingevidentarebothmoreeffectivethaninvestingindealingwiththechroniclaterphasesoftheseproblems;
■ investingintheearlyyearsofachild’slifeandtheearlystagesofsocialproblemsbeforetheybecomechroniccanproduceverysubstantialsavingstothepublicpurseinlateryears;
■ preventionscienceiscriticallyimportantindemonstrating,throughrobustresearch,usuallyinvolvingrandomcontroltrials,whatinterventionsactuallywork;and
■ beingclearaboutthespecificoutcomesthatanyinterventionisdesignedtoimpactonisvitallyimportant.
4. PublicPolicyContextAlthoughtheconceptsaroundanearlyinterventionapproachhaveonlybecomecommonlydiscussedinternationallyinthelastdecade,theyhavenowhadasignificantimpactonthestrategicthinkingofarangeofgovernmentdepartmentsandagenciesinNorthernIreland,whichnowemphasiseprevention,earlyinterventionandevidence-basedpractice,althoughactualimplementationoftheapproachisstillataveryearlystage.Itrequiresalonger-termperspectiveinrealisingthesavingstothepublicpurseofsuchanapproachandthebreakingdownofdepartmentalsilos,asthepositiveoutcomesofaninvestmentfromonedepartmentmayaccruetoanotherdepartment.
5. TheoryofChangeThereportoutlinesalogicmodelwhichdemonstratesthelinksbetweentheinvestmentofresources;theprogrammestobedelivered;theoutputsfromtheseprogrammes;theoutcomesintermsofchangedlives;andhoweachofthesecanbemeasured.Thelogicmodelsuggeststhatthefollowingoutcomesshouldbeaddressed:■ Reducednumberofteenagepregnancies■ Reducedlevelofsmokingduringpregnancy■ Improvedparentingskillsandconfidence■ Improvedparent-childattachmentfor0-2yearolds■ Improvedschoolreadinessamongst3&4yearolds■ Improvedliteracyandnumeracyinchildrenaged4-11■ Improvedsocialandemotionalskillsandresilienceof4-11yearolds■ Improvedschoolattendance■ Improvededucationalaspirationsandattainmentonleavingschool■ Reducedbehavioural/conductproblems■ Reducedsmoking,alcoholanddrugconsumptionamongstyoungpeople■ Reducedcrimeandanti-socialbehaviouramongstyoungpeople

Page 4
Effectiveinterventionsneedtocommencewithafamilybeforeachildisbornandcontinueatleastthroughprimaryschoolage.Theyneedtoincludeuniversalprogrammesaswellastargetedservices.
Inordertoaddressthis,theapproachproposedhastwokeyelements:
1) AlthoughLisburnisunder-servedinrelationtosupportforchildrenandfamilies,asitdoesnotreceiveregenerationfundingsuchasNeighbourhoodRenewal,despitehavingareaswithinthe10%mostdeprivedinthe2010MDMfiguresandhasmuchworseeducationaloutcomesthanareaswithintheworst10%,thereisstillaneedimprovetheco-ordination,effectivenessandintegrationofexistingservicesforchildren,youngpeopleandfamiliesintheLisburnareabydevelopingacommonoutcomesframework(whichwillenableimpacttobemeasured),creatingasharedfocusonqualityachievedthroughjointreflectivepractice,trainingandpeerlearning,wherebydifferentorganisationscanlearnfromoneanother.Inaddition,allexistingorganisationswillneedtoworktogethertotransformtheculturewithintheCityofLisburn,especiallywithinareasofdeprivation,toemphasiseaspirationandachievement(particularlyinrelationtoeducation).
2) ThescaleoftheprobleminLisburn,whereby75%ofpupilsfromallofthethreecontrolled/integratedschoolsleavewithouttheminimum5CGSEwithMathsandEnglish,issuchthatsignificantnewsustainableinvestmentisneededinnewinterventionstobreakthecycleofpooroutcomes,whichislikelytoonlygetworse.TheseneworenhancedinterventionsmustcomplimentandworkalongsideexistingcommunityserviceswithinLisburnsothatallservicesareworkingtogetherunderacommonoutcomesframework.Theneworenhancedinterventionsshouldalsohaveclearlydemonstratedeffectivenesssothatconfidencecanbegainedthattheywilldeliverthelevelofimprovementrequired.
Specificinterventionswillbeidentifiedbythemulti-agencyEarlyIntervention
LisburnConsortiumoncefundingisinplace,butarelikelytoincludeinterventionsbasedon:■ intensivehomevisiting;■ parentingtraining;■ pre-schoolearlyyearschilddevelopment;■ additionalliteracysupportintheprimaryyears;■ socialandemotionaldevelopment;and■ mentoringsupport.
Executive Summary

Page 5
6. OperatingModelThereportoutlinesanoperatingmodelfordeliveringtherecommendedprogrammesinLisburnwhichwillbebothownedbythelocalcommunity;fullyengageallthekeystakeholderswhohaveaninterestinoutcomesforchildrenandyoungpeopleinthetargetareasinacollaborativeapproach;andbedeliveredbyanagencywithstrongexperienceindeliveringearlyinterventionprogrammesforchildrenandfamilies.
TherearealsoconsiderableadvantagesindevelopingacloserelationshipwithotherareasthathavedevelopedanEarlyInterventionapproach.ApartnershipwiththeEarlyInterventioninitiativeinDerry-Londonderry,whichisatasimilarstagewouldhaveparticularadvantages.
7. ImplementationPlanThereportoutlinesamedium-termimplementationplaninphasesfortakingforwardtherecommendationsinthereport.ThephasedapproachedallowsforthepotentialfindingsfromthelargenumberofRCTevaluationsthatwillreportoverthenextfouryearsinfuturephasestobetakenonboard.

Page 6
CHAPTER ONE
Introduction
ThisreporthasbeencommissionedbyResurgamDevelopmentTrustandfundedbythePublicHealthAgencytoexplorethefeasibilityofanearlyinterventioninitiativetobreakthecycleofunder-achievementamongstchildrenandyoungpeopleindisadvantagedcommunitiesinLisburn.TheconceptofEarlyInterventionLisburnhasbeenpioneeredbytherecentlycreatedResurgamDevelopmentTrustrepresentingawiderangeofcommunityandyouthorganisationsindisadvantagedareasinLisburn.
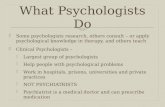
Lisburnisarecentlydesignatedcitytothesouth-westofBelfastontheRiverLagan.Ithasagrowingpopulationof117,836.Itisanareaofsharpcontrasts.ItcontainssomeofthemostprosperousareasinNorthernIreland(includingWallacePark–themostprosperous),aswellasaseriesofdisadvantagedhousingestatesbuiltinphasesbetweentheendofWWIIandthe1970stoencouragepopulationgrowthawayfromBelfast.TheseestatesincludethepredominatelyProtestant/Unionist/LoyalistOldWarren,Hillhall,HildenandthemoremixedKnockmoreand
10 11
12 1315
1416
189
8
7 17
1 Knockmore2 Old Warren3 Tonagh4 Lagan Valley5 Hilden6 Hillhall
7 Ballinderry8 Maghaberry9 Maze10 Ballymacross11 Ballymacash12 Lisnagarvey
13 Wallace Park14 Magheralave15 Harmony Hill16 Lambeg17 Drumbo18 Blaris
1 2 34
5 6

Page 7
Tonaghestates.TherearealsosignificantsmallerpocketsofdeprivationaroundLisburn,includinginBallymacashandMilltown/Derriaghy.
Twinbrook,Poleglass,KilweeandColinGlen,whilecurrentlywithintheLisburnLocalGovernmentArea,identifymorewithWestBelfast;willbecomepartofBelfastCouncilareafollowingtheimplementationoftheReviewofPublicAdministration;andarealreadypartofthesuccessfulColinEarlyInterventionCommunityandsohavenotbeenincludedinthisstudy.Theprocessofdevelopingthisreporthasinvolved,inadditiontoextensivedeskresearch,aseriesofconsultationmeetingsandworkshopswithcommunities,schoolprincipals,voluntaryorganisationsandstatutoryagenciesworkingwithindisadvantagedareasinLisburn.Participantsinconsultationworkshopsandinterviewshaveincludedthefollowingwhohavemadeavaluablecontributiontothedevelopmentofthestrategy:
AdrianArbuthnot–DepartmentofEducationNIAnnieArmstrong-ColinNeighbourhoodPartnershipAdieBird–ChairoftheEarlyInterventionLisburnSteeringGroup/ResurgamOwenBrady–NorthernIrelandHousingExecutiveSoniaBrown–HildenCommunityAssociationCaitlinBurns-HillhallRegenerationGroupTonyCanavan–DepartmentofJusticeNILouiseClarke–HildenCommunityAssociationRosieColquhoun–KnockmoreCommunityAssociationPatriciaConnelly–TonaghWomen’sGroupJonathonCraigMLA–MemberoftheNIAssemblyEducationCommitteeEvelynCurran-EasternChildcarePartnershipMichaelDevine–SouthEasternEducationandLibraryBoardMartinDevlin–SouthEasternHealth&SocialCareTrustSharonDickson–LisburnYMCAKieranDrayne-ColinEarlyInterventionCommunityFrancisFerris–TrainingForWomenNetworkandHillhallCommunityAssociationSharonGibson–Resurgam/LisburnPSPPaulGivanMLA–ChairofAssemblyJusticeCommitteeSamHamilton-OldWarrenCommunityAssociationAnnHardy–Children&YoungPerson’sStrategicPartnershipJulieHealy–Barnardo’sSharonHeazley–NorthernIrelandHousingExecutiveHildenWomen’sGroupFionaIrvine–TonaghWomen’sGroupIngridIrvine–TonaghWomen’sGroup

Page 8
PamelaJames-KnockmorePrimarySchoolMaureenJamison–SouthEasternHealth&SocialCareTrustMauraJohn-OldWarrenCommunityAssociationSheenaKerr–TonaghWomen’sGroupTommyKynes-OldWarrenCommunityAssociationAliceLennon-SouthEasternEducationandLibraryBoardJulieLenaghan–TonaghWomen’sGroupHelenLewis-BrownleePrimarySchoolMonicaMcCann–Barnardo’sEamonMcCarthy–DerryHealthyCitiesPatriciaMcCormick–HildenCommunityAssociationJimMcLaughlin–DerriaghyCommunityAssociationMargaretMcCormick-FortHillCollegeNeilMcGivern–SEELBPaulineMcMillan-LisburnYMCAJamesMartin-LaurelhillCommunityCollegeMonicaMeehan–SouthEasternEducationandLibraryBoardYouthServiceEdwardMilliken–HillhallRegenerationGroupLawrenceMilliken–HillhallRegenerationGroupJasonMilliken–HillhallRegenerationGroupTonyMorgan–UniversityofUlsterGailMullan-HillhallRegenerationGroupAshleyMulligan-KillowenPrimarySchoolOldWarrenWomen’sGroupDenisPaisley–OldWarrenYouthInitiativesSarahJanePatterson–CommunityworkerKnockmore/TonaghHeatherPhillips–HildenCommunityAssociationPaulPorter–LisburnCityCouncilorTanyaPorter–HildenCommunityAssociationMarianQuinnandotherstaff–TallaghtWestChildhoodDevelopmentInitiativeSeamusQuinn-StPatrick’sAcademyGordonRea–HildenCommunityAssociationJimRose–LisburnCityCouncilMabelScullion–PublicHealthAgencyJimSheerin-LisnagarveyHighSchoolDavidSmith-SouthEasternRegionalCollegeClaireSpiers-TonaghPrimarySchoolJulieStephenson–DepartmentofEducationNIHarryStewart-LargymorePrimarySchoolIanSutherland-SouthEasternHealth&SocialCareTrustFionaTeague–DerryHealthCitiesJohnTodd–DepartmentofJusticeNI
CHAPTER ONE
Introduction

Page 9
ChrisTotten–PublicHealthAgencyLisaTucker–RaggedyBapLauraTurner–Ballymacoss/NorthLisburnAnneWatsonKnockmoreCommunityAssociationJasonWhite–SouthEasternHealth&SocialCareTrustAndrewWilliamson-OldWarrenPrimarySchool
TheresearchandconsultationswereguidedbytheEarlyInterventionLisburnSteeringGroup(listofmembersofthesteeringgroupareshowninAppendix1).
Thereportisinsixmainsections:
Section 2 looksattheneedsofdisadvantagedcommunitiesinLisburninrelationtohealth,wellbeing,parenting,safety,securityandeducation.
Section3explorestheconceptofEarlyInterventionandwhyithasbecomecriticalinthedevelopmentofthinkingaboutsocialprogrammesinternationallyaswellasintheUKandIreland.
Section 4explorestherelevantNorthernIrelandpublicpolicycontextanditsrelevancetotheEarlyInterventionevidence-basedapproach
Section 5outlinesaTheoryofChangeandLogicModelandassessesandhighlightstheevidence-basedprogrammesthathavebeenshowntomakeasignificantimpactontheoutcomeswhichareappropriateforEarlyInterventionLisburn
Section 6exploresthemostappropriateoperatingmodelforengagingallthekeystakeholdersindeliveringtheEarlyInterventionLisburnvision
Section 7providesasuggestedimplementationplanfortakingforwardtheearlyInterventioninitiative.

Page 10
CHAPTER TWO
The needs of disadvantagedcommunities in Lisburn
2.1IntroductionThefollowingsectionoutlinestheissuesofconcernthatwerehighlightedincommunityconsultations,alongwithananalysisandsummaryoftheavailabledataonvariousformsofdisadvantageinthetargetareasinLisburnwhichpreventchildrenandyoungpeopleachievingtheirpotential.
TheNorthernIrelandStatisticsandResearchAgency(NISRA)gathersdataonallwardsandSuperOutputAreas(SOAs)inNorthernIrelandfromavarietyofsources,whichitdisseminatesthroughitsNINISdatabase.ThisdataprovidesarangeofimportantinformationaboutthetargetdisadvantagedcommunitiesinLisburn.
SomeoftheanalysisbelowreferstoelectoralwardsandotherstoSuperOutputAreas(SOA),wheretheinformationisavailable.SomeSOAsareco-terminuswiththeelectoralwards(e.g.OldWarrenandTonagh).InHillhall,HildenandKnockmorewards,however,therearetwoSOAsineachward.TheboundariesofwardsorSOAsmaynotbethesameastheboundariesofacommunityasperceivedbytheresidentswithinthoseboundaries.TheKnockmoreestate,forexample,isinOldWarrenratherthantheKnockmoreward.PartoftheOldWarrenestateisinLaganValleyward.
SignificantpocketsofdeprivationcanalsobecontainedwithinawardorSOAthatalsocontainscomparativeaffluence,sothatthescores/rankingsfortheward/SOAmaymasktheexistenceofthesesmallerpocketsofdeprivationaroundLisburn,includinginBallymacoshandMilltown/Derriaghy.

Page 11
Population(bywardandSOAs)*Theestimatedpopulations(andreligiousbreakdown)ofeachofthetargetwardsandSOAsin2011areasfollows:
OldWarren(70.4%Protestantand24.9%Catholic) 2,401
Tonagh(62%Protestantand35.4%Catholic) 2,537
Hillhall(90.2%Protestantand5%Catholic 2,815
Hillhall1(88.7%Protestantand5.9%Catholic) 1,412
Hillhall2(76.1%Protestantand18.4%Catholic) 1,403
Knockmore(76.1%Protestantand18.4%Catholic) 3,537
Knockmore1(73.4%Protestantand22.8%Catholic) 1,862
Knockmore2(79.2%Protestantand13.6%Catholic) 1,675
Hilden(89.5%Protestantand5.4%Catholic) 2,826
Hilden1(84.2%Protestantand8.7%Catholic) 1,351
Hilden2(94.4%Protestantand2.4%Catholic) 1,475
LaganValley 2,967
LaganValley1SOA(84.6%Protestant;8.9%Catholic) 1,379
Totalpopulation 17,083
NumberofChildren(under16)*Theestimatedtotalnumberofchildreninthetargetareasin2010areasfollows:
Ward SOA Totalno.ofchildren
0-2yearolds 3-5yearolds
OldWarren OldWarren 600 116 128
Tonagh Tonagh 512 79 97
Hillhall 611 122 115
Hillhall1 296
Hillhall2 316
Knockmore 757 157 242
Knockmore1 329
Knockmore2 427
Hilden 588 110 112
Hilden1 293
Hilden2 294
LaganValley 573 98 119
Alltargetareas 3,641 682 717
*NINISwardandSOAprofiles(www.ninis.nisra.gov.uk–lastupdatedOctober2011)

Page 12
Births*Therewerethefollowingnumberofbirthsinthetargetareasduring2009/10:
Derryaghy1 119(2010/11)
Knockmore 73
Hilden 57
Tonagh 44
OldWarren 41(46in2010/11)
Hillhall 37(23inHillhall1SOAin2010/11)
LaganValley 36
Totalnumberofbirths: 288
2.2MultipleDeprivationThissectionlooksattheNINIScompositemeasureofdeprivation*andsomeoftheviewsthatemergedfromthecommunityconsultations.
Multi-deprivation2010rankings*ThefollowingaretheMDMrankingsforthetargetareasofLisburnoutof582wardsand890SOAs:
Ward MDM ranking CommentsOldWarren 32nd Withinthe10%mostdeprivedwards
Tonagh 103rd Withinthe20%mostdeprivedwards
Hilden 154th Withinthe30%mostdeprivedwards.Hilden1SOAisranked299thoutof890SAOs;Hilden2isranked227th
LaganValley 156th Withinthe30%mostdeprivedwards;SOALaganValley1isranked231stoutof890,justoutsidetheworst25%mostdeprivedSOAs
Hillhall 203rd SuperOutputAreaHillhall1isoneofthe20%mostdeprivedSOAsinNI–ranked145th
Knockmore 285th SOAKnockmore1isranked550thoutof890;Knockmore2SOAisranked310th
*NINISwardandSOAprofiles(www.ninis.nisra.gov.uk–lastupdatedOctober2011)
CHAPTER TWO
The needs of disadvantagedcommunities in Lisburn

Page 13
Economicwellbeing–incomesupport(2011)*
OldWarren ConsistentlymuchworsethantheNIaverageonallincomesupportindicators.ItismorethantwicetheNIaverageforthenumberofchildrenlivinginincomesupporthouseholds.Itistwoandthree-quarterstimestheNIaverageforloneparentsclaimingincomesupport
Tonagh WorsethantheNIaveragefornumberofchildreninincomesupporthouseholdsandnumberofloneparentsclaimingincomesupport
Hilden ConsistentlyworsethantheNIaverageonallincomesupportindicators
Hillhall WorsethantheNIaverageonthenumberofchildreninincomesupporthouseholdsandloneparentsclaimingincomesupport
Knockmore 18%abovetheNIaverageofnumberofincomesupportclaimantsandincomesupportclaimantswithadisabilitypremium
LaganValley 20%abovetheNIaverageforincomesupportclaimants;athirdabovetheNIaveragefornumberofchildreninincomesupporthouseholds;and57%abovetheNIaverageforloneparentsclaimingincomesupport
CommunityConsultationsConsultationswithcommunitiesandprofessionalsworkinginthetargetareas(seethelistofconsulteesintheIntroduction)highlightedtheseriousimpactofsocio-economicdisadvantageonfamiliesinthetargetcommunities.
Onecommunityrepresentativedescribedthesenseofeconomicexclusionfromlocalfacilities,suchasthenearbyleisurecentreandactivitycentre,whichareunaffordabletomanyfamiliesonlowincomes.Thesamerepresentativealsodescribedthechallengesforlowincomefamilieswhohaveachildwhogainsaplaceinagrammarschoolwhichexpectsparentstopaya“voluntary”fee,plusthecostoftheuniform,schooltrips,tuition,etc.Middleclassfamiliescanaffordtopayforspecialtutorstohelpensurethechildpassesthe11+tests,andgainsextrahelpwithkeysubjectsiftheyrequireit,aswelltheotheradditionalcontributionsexpectedbygrammarschools.
Thecommunityconsultationshighlightedconcernsaboutincreasinglevelsofunemployment(althoughlowerthanmanyotherareasofsignificantdeprivation);theincreasingnumberofjobswhicharetemporary,part-timeand/orlowpaid;andproblemsofunemployabilityduetothelowlevelsofeducationalachievement,discussedbelow.
Theconsultationsalsohighlightedtheimpactofa“benefitsculture”particularlyforfamilieswhereno-oneisworking,where,toenhancetheirmeagreincomes,theireffortsareoftenfocusedonmaximizingbenefitsclaimsformedical
*NINISwardandSOAprofiles(www.ninis.nisra.gov.uk–lastupdatedOctober2011)

Page 14
conditionsordisabilitiesamongsttheparentsandchildren.Thebenefitstrapwhichmakesitdisadvantageousforparentstotakeuplowpaidemploymentbecausetheywillbeworseoffwasalsohighlighted.
Thelackofaffordablechildcarewasalsocitedasanotherbarrierinparentsgainingpaidemploymentduringvariousoftheconsultationswithcommunityandwomen’sgroupsinthetargetareas.Itissupportedbythelackofidentifiableall-daychildcareprovisionintheareas.
2.3EducationThissectionexplorestherelevantdataoneducationalperformance(basedon2009/10statisticsfromDENI).IthighlightstheinadequateeducationaloutcomesformanychildrenindisadvantagedcommunitiesinLisburn,muchofitreflectingtheenvironmentalfactorsinthelivesofthechildren.
PleasenotethatstatisticalinformationbywardprovidedbyNINISisfromtheyear2009/10.StatisticalinformationfromtheDepartmentofEducationonschoolperformanceisfortheyear2010/11
Percentageofpost-primarypupilsentitledtofreeschoolmealsMostlyconsistentwiththeMultipleDeprivationMeasuresforeachward,highlightedabove,thefollowingarethepercentageofchildrenentitledtofreeschoolmealsineachward:
0 10 20 30 40 50 60 70 80 90 100
Knockmore
Hilden
Hillhall
Lagan Vallet
Tonagh
Old Warren 39.9%
(a much lower % than would be suggested by the ward’s multiple deprivation ranking)
26.4%
23.8%
17.6%
17.6%
11.1%
NI average 16.7%
CHAPTER TWO
The needs of disadvantagedcommunities in Lisburn

Page 15
Percentageofpupilsstatemented/SENyears1-7AllthetargetwardsareabovetheNIaverageof18.9%,intermsofthepercentageofpupilsinschoolyears1to7,whohavebeenstatementedasaresultoflearningdifficultiesordesignatedashavingspecialeducationalneeds,exceptforKnockmorewhichisbelowaverage(15.4%):
Atpost-primarylevel,morethanonequarter(27.7%)ofstudentsatLaurelhillCommunityCollegehavespecialeducationalneeds;20.9%atFortHillCollege.and13.3%atLisnagarveySecondarySchool.
SpeechandlanguagedifficultiesThenumberofspeechandlanguagereferralsforchildrenagedunder16atthetimeofreferralinthetargetareasareshowninthetablebelow:
LISBURN WARD New Review Group Contact
Can C Did not respond /attend
Grand Total
Multiple Deprivation Ranking
BALLYMACOSS 45 705 353 112 46 1261 395
DERRYAGHY 64 667 289 89 68 1177 198
HILDEN 17 315 254 36 30 652 154
LAGANVALLEY 16 375 194 35 19 639 156
TONAGH 15 318 230 31 15 609 103
BALLYMACASH 20 371 146 28 25 590 575
BLARIS 12 376 156 25 15 584 470
OLDWARREN 17 243 261 31 19 571 32
HILLHALL 17 282 220 22 25 566 203
KNOCKMORE 27 239 92 47 35 440 285
TWINBROOK 12 243 116 19 34 424 10
POLEGLASS 30 213 90 39 42 414 80
WALLACEPARK 11 174 54 15 14 268 582
LISBURN(allwards)Total
619 9230 4736 1191 753 16529
Twinbrook,PoleglassandWallaceParkwardshavebeenincludedbywayofcontrast.
0 10 20 30 40 50 60 70 80 90 100
Knockmore
Hillhall
Hilden
Tonagh
Lagan Valley
Old Warren 41.8%
28.8%
26.2%
23.9%
21.8%
15.4%
NI average 18.9%

Page 16
Itmighthavebeenexpectedthatchildrenfrommoredeprivedwardsarelikelytoexperiencegreaterproblemswiththeirspeech/language.Thistable,however,doesnotconfirmanyrelationshipbetweenthelevelofdeprivationofawardandthenumberofreferralsofchildrenwithspeechandlanguagedifficulties.Thelackofanyexpectedrelationshipmaybetodowiththeconfidenceofmoremiddle-classparentstoaccesstheservicestheyfeeltheirchild,whoisexperiencingspeechorlanguagedelays,requires,counterbalancinganyrelationshipwithdeprivation.
Percentageofpoorattendance(lessthan85%)atprimaryschoolAllthetargetwardsareworsethantheNIaverageof5.5%intermsofchildrennotachieving85%attendanceatprimaryschool:
Sub-domain for primary school rankingNINIScalculatesasub-domainscoreandranking,basedindatafrom2006/7-2007/8.Itiscalculatedusingthreesetsofindicators:■ The%ofchildrenachievinglevel4orhigheratkeystage2■ The%ofchildrenwithspecialeducationalneeds■ Thelevelofabsenteeism
ThegeneralrelationshipbetweentheSOANINASprimaryschoolsub-domainrankingsandtheMultipleDeprivationrankingsishighlightedinthetablebelow.However,theHildenSOAs(withamultipledeprivationrankingsof227and299)haveprimaryschoolsub-domainrankingsof117thand119th,whicharemuchworsethanwouldbeexpected.Tonagh,LaganValley1,Knockmore1andHillhall2arealsoworsethanwouldbeexpectedfromtheMultipleDeprivationRankings.OldWarrenandHillhall1arebetterthanwouldbeexpected.
0 10 20 30 40 50 60 70 80 90 100
Knockmore
Tonagh
Hillhall
Old Warren
Lagan Valley
Hilden
NI average 5.5%
12.1%
11.6%
8.4%
7.0%
6.9%
5.5%
CHAPTER TWO
The needs of disadvantagedcommunities in Lisburn

Page 17
SOA Primary School Ranking MDM Ranking CommentsHilden2 117th 227 Withintheworst15%ofSOAs
Hilden1 119th 299 Withintheworst15%ofSOAs
OldWarren 129th 85 Withintheworst15%ofSOAs
Tonagh 138th 192 Withintheworst15%ofSOAs
LaganValley1 187th 231 Withintheworst25%ofSOAs
Knockmore2 312th 310
Knockmore1 383rd 550
Hillhall1 397th 145
Hillhall2 430th 612
PrimarySchoolPerformanceatKeystage1and2(EnglishandMaths)1
Theexpectationisthatallprimaryschoolpupilswillachieveatleastlevel2EnglishandMathsatkeystage1andlevel4inEnglishandMathsatKeyStage2.
ThetablebelowshowsthenumberofprimaryschoolsinLisburnthatdonotenable90%oftheirpupilstoachievethesestandards,outofapossiblemaximumof14schools.Theyarepartlybasedonsubjectiveteacherassessmentssotheyneedtobetreatedwithsomecaution.
Stage and Level
The number of primary schools not achieving 90% of the target
The number of primary schools in Lisburn achieving below the NI average for that band of free school meal entitlement
Comments
KeyStage1Level2English
5 6 3oftheschoolsnotachieving90%haveafreeschoolentitlementof30%+.ThreearecurrentlyExtendedSchools2,twoofwhichhavenurseryclasses.Twoarebelowtheirtargetintake
KeyStage1Level2Maths
3 8 Only1oftheschoolsnotachieving90%hasafreeschoolentitlementof30%+.ItiscurrentlyanExtendedSchoolwithanurseryclass.Itbelowitsintaketarget
KeyStage2Level2English
8 6 4oftheschoolsnotachieving90%haveafreeschoolentitlementof30%+,allofwhicharecurrentlyExtendedSchools,twoofwhichhaveanurseryclassandoneareceptionclass.Twoarebelowtheirtargetintake.
KeyStage2Level2Maths
8 7 4oftheschoolsnotachieving90%haveafreeschoolentitlementof30%+,allofwhicharecurrentlyExtendedSchools,twoofwhichhaveanurseryclassandoneareceptionclass.Twoarebelowtheirtargetintake.
1 FromKeyStageOne&TwoAssessmentsforschoolsintheLisburnAreain2010/11–DepartmentofEducation
2 The2012/13ExtendedSchoolentitlementwillbedeterminedpriortoSeptember2012.

Page 18
TheseprimaryschoolKeyStage1&2findingswouldsuggestseriousconcernsabouttheStage1resultsinfiveoftheprimaryschools(fiveinEnglishandthreeinMaths)andKeyStage2resultsinsevenprimaryschoolsinbothEnglishandMaths.Surprisingly,fouroftheseschoolshavelessthan20%ofpupilsentitledtofreeschoolmeals.
Twooftheprimaryschoolslistedsend70%+oftheirpupilstoagrammarschool.Fiveprimaryschools(includingtheabovetwo)sendmorethanhalfoftheirpupilstoagrammarschool.Sixoftheschoolssent20%orlessoftheirpupilstoagrammarschool.ThefindingsalsoshowthatgoodresultsatKeyStage1donotnecessarilymeangoodresultsatKeyStage2andvisa-versa.
Thesestatisticsonprimaryschoolperformanceareveryinteresting,becausethereisaweakerlinkbetweentheassessmentscoresandthepercentageofpupilsentitledtofreeschoolmeals(ameasureofdeprivation)thantheliteraturewouldsuggest.Thisimpliesthat,inadditiontotheroleofparents,theroleoftheschoolisveryimportantinincreasingtheaspirationsandachievementofchildren.
Byward,thenumbers(notpercentage)ofpupilswhoareresidentinthetargetareasandattendagrammarschoolareasfollows:
Bywayofcontrast,thefigureforWallaceParkis175andthefigureforPoleglassis125.
Theresultssuggestthat,onaverage,atKeyStage2,aboutonequarterofpupilsinLisburnExtendedSchoolsarenotachievingtheminimumacceptablestandardatKeyStage2EnglishorMaths.However,theactualpercentagevariesbetweenschoolsandsubjects:from19.45%to53.55%.These25%ofprimaryschoolpupils(andtheworstperformingschools)shouldbeanimportantfocusofanyEarlyInterventioninitiativeandthegenerationswhicharelikelytofollowintheirfootsteps,unlessdecisiveactionistaken.
0 10 20 30 40 50 60 70 80 90 100
Knockmore
Hillhall
Lambeg
Lagan Valley
Tonagh
Hilden
Old Warren 21
31
36
59
68
72
88
CHAPTER TWO
The needs of disadvantagedcommunities in Lisburn

Page 19
Theseprimaryschoolresultswouldsuggest,subjecttotheoutcomeoftheauditofschoolsthatiscurrentlytakingplace,whichmayresultinfurtherschoolclosures,anyprimaryschoolsinitiativeshould,perhaps,beconcentratedontheschoolsdesignatedasExtendedSchools(3ofwhichhavenurseryclassesand1whichhasareceptionclass),oronthefouroftheExtendedSchoolswiththelowestkeystageresults(twooftheExtendedSchoolshaveimpressiveKeyStage1&2results).
TheevaluationoftheExtendedSchoolprogrammedidnotdemonstratearelationshipbetweenExtendedSchoolfundingandPrimarySchoolperformance,butrecommendedacloserrelationshipbetweentheactivitiesfundedundertheExtendedSchoolprogrammeandtheeducationalaimsoftheschool.
Post-PrimaryPerformance
Percentageofpoorattendance(lessthan85%)atpost-primaryschoolAllthetargetwardsinLisburnareworsethantheNIaverageof12.7%fornotachieving85%attendanceatpost-primaryschools:
0 10 20 30 40 50 60 70 80 90 100
Knockmore
Hillhall
Hilden
Lagan Valley
Tonagh
Old Warren
NI average 12.7%
30.0%
25.6%
25.1%
23.7%
21.2%
20.3%

Page 20
Leavingschoolwith5+GCSEsatgradeA*-C(2009/10)*AllthetargetwardsareconsistentlywellbelowtheNIaverageof72%foryoungpeopleleavingschoolwithatleast5GCSEsatgradeA*toC,includingthemoreaffluentLambegward:
AveragenumberofpupilsleavingcontrolledandintegratedschoolsinLisburnin2010/11with5+GCSEs(DeptofEducation)
Average and Range 2010/11
Comment
%ofcontrolledandintegratedsecondaryschoolpupilsinIisburnachieving5+GCSEsA*-CwithEnglishandMaths(2010/11)
Average:24.27%
Range:19.6–26.7%
TheaverageforallNIschoolsis60%.(and36%forallNInon-grammarschools).TheNIgovernment’sPfGtargetisanaverageof66%forallpupilsand49%fordisadvantagedpupilsby2014/15
%ofcontrolledandintegratedsecondaryschoolpupilsinLisburnachieving5+GCSEsA*-C(2010/11)
Average:44.57%
Range:43.5–46.4%
TheaverageforallLisburnschoolsis75.1%.(96.8%forLisburngrammarschools)Theaveragefornon-grammarschoolsinNorthernIrelandis57.3%.
OneoftheLisburnsecondaryschoolscurrentlyhasExtendedSchoolsfunding.Anotherhadthefundingunderapreviousround.TwoofthesecondaryschoolsarecurrentsubjecttoFormalIntervention.
0 10 20 30 40 50 60 70 80 90 100
Knockmore
Hilden
Hillhall
Lagan Valley
Lambeg
Old Warren
Tonagh
NI average 12.7%
20%
40%
48%
53.1%
55%
57%
58%
* NINISwardandSOAprofiles(www.ninis.nisra.gov.uk–lastupdatedOctober2011)
CHAPTER TWO
The needs of disadvantagedcommunities in Lisburn

Page 21
Leavingschoolwith2ormoreAlevelsAllthetargetwardsareconsistentlylowerthantheNIaverageof53.6%foryoungpeopleleavingschoolwith2ormoreAlevels(56%inLisburn).EventhemoreaffluentLambegWardhasapoorrecordintermsofAlevelresults:
A level results of post-primary schools TheNIaverageforallpost-primaryschoolsAlevelresultsin2010/11is51.5%leavingschoolwith3+AlevelsA*-C(DepartmentofEducation).TheaverageforthesecondaryschoolsinLisburnis35.1%(48.4%achieved5+GCSEs).
Percentageofschoolleaversinhighereducation*AllthetargetwardsareworsethantheNIaverageof42%foryoungpeoplegoingontohighereducationi.e.university:
TheNIaverageforyoungpeopleleavingnon-grammarschoolsandgoingontouniversityorequivalentis19.2%.TheNIaverageforyoungpeopleentitledtofreeschoolmealsgoingontouniversityorequivalentis18.3%.Againboystendtodomuchworsethangirls.
0 10 20 30 40 50 60 70 80 90 100
Knockmore
Hillhall
Lagan Valley
Hilden
Tonagh
Lambeg
Old Warren
NI average 53.6% Lisburn average 56%
12%
14%
20%
32%
34%
38%
44%
0 10 20 30 40 50 60 70 80 90 100
Knockmore
Hilden
Tonagh
Old Warren
Hillhall
Lagan Valley
NI average 42%
9.4%
10%
12%
20%
29%
30%
* NINISwardandSOAprofiles(www.ninis.nisra.gov.uk–lastupdatedOctober2011)

Page 22
Percentageofschoolleaversinfurthereducation*AllthetargetwardsareworsethantheNIaverageof33%(andtheNInon-grammaraverageof43.7%)foryoungpeoplegoingontofurthereducation(i.e.college):
Education,skills&trainingdeprivationdomainrankingforSOAs*TheoverallNINIS2010education,skills&trainingrankingsforallthetargetSOAsareasaremuchworsethantheiroverallmultipledeprivationranking.Someofthedifferencesarestriking.
CommunityConsultationsThefindings,above,fromthestatisticsoneducationalachievement,wereechoedbythefindingsfromthecommunityconsultations.Muchofthediscussionaroundeducationalunderachievementhighlightedaviciouscircleinvolving:
0 10 20 30 40 50 60 70 80 90 100
Hillhall
Knockmore
Lagan Valley
Tonagh
Old Warren
Hilden
NI average 33%
11%
12%
20%
25%
30%
31%
0 100 200 300 400 500 600 700 800 900 1000Hillhall 2
Knockmore 1
Knockmore 2
Laganvalley 1
Tonagh
Hilden 1
Hillhall 1
Hilden 2
Old Warren 5995109
128134
173181
393512
within the worst 10% of SOAs (MDM ranking of 85)
within the worst 15% of SOAs (MDM ranking of 227)
within the worst 15% of SOAs (MDM ranking of 145)
within the worst 15% of SOAs (MDM ranking of 299)
within the worst 15% of SOAs (MDM ranking of 192)
within the worst 20% of SOAs (MDM ranking of 231)
within the worst 25% of SOAs (MDM ranking of 310)
(MDM ranking of 550)
(MDM ranking of 612)
* NINISwardandSOAprofiles(www.ninis.nisra.gov.uk–lastupdatedOctober2011)
CHAPTER TWO
The needs of disadvantagedcommunities in Lisburn

Page 23
■ parentswhooftenthemselveshadpoorexperiencesintheeducationsystemandthereforedonotvalueeducation;
■ povertyrestrictingtheabilityofmanyfamiliestoencouragetheirchildrentogotoagrammarschool,getextratuitionwhentheyneedit,and/orgoontouniversityinsteadofgettingajob;
■ parentsfacingoverwhelmingpersonaldifficulties(mentalhealth,physicalhealth,carerresponsibilities,addiction,domesticviolence,etc)themselves;
■ parentshavinglowambitionsforthemselvesandtheirchildren;■ parentswithpoorliteracyandnumeracy;■ parentsnotreadingtotheirchildren;■ thetendencyofchildrentofollowinthefootstepsoftheirparents,older
siblingsand/orfriends,includingthosewhohavelesspotential;■ lackofconsistentboundariessetforchildrene.g.lettingchildrenstayuplate
andarelateortiredthenextdayinschool,ornotensuringthechildrenattendschool;
■ lackofconsistentpositivediscipline,orveryharshdiscipline,leadingtopoorbehaviour/conduct;
■ lackoffocusedsupportforchildrenwithlearningdifficulties/developmentdelay,butnotstatemented;
■ thelackofcommunityrolemodelschampioningtheimportanceofeducation;■ thelackofavailablejobswhichcouldcreateamotivatortoobtain
qualifications;■ lackofparentalengagementwithschoolsparticularlyafterP1&P2;and■ parentsandteachersviewingmanychildrenas“notacademic”andtreating
themaccordingly(incontrasttomiddle-classparentswhowilltendtoseekoutandpayforappropriateprivatetuitionorsupportservice,toensuretheirchildwillfulfilltheirambitions/potential.
Parentsconsultedwhoareworkingtendedtoresenttheprioritygiventoparentsonincomesupportorjobseekersallowanceinobtainingplacesinnurseryschools;aswellasnurseryplacesbeingallocatedtomiddle-classchildrenfromoutsideofthearea.
Theconsultationsalsohighlightedtheparticularchallengesfacedbytheincreasingnumberofloneparents.Oneteacherhighlightedaparticularclassintheirschoolwhichhadnofatherslivingwiththeirchildren.Thevastmajorityofprimaryschoolteachersarealsowomen,raisingconcernsaboutthelackofpositivemalerolemodelsinthelivesofboys.

Page 24
ConsequencesofpooreducationaloutcomesLeavingschoolwithfewornoqualificationshasverysignificantimplicationsfortheoutcomesforthatchildinlaterlife.OfthosewholeftschoolwithnoqualificationsinNorthernIreland,only45%arecurrentlyinanyformofemployment.Thequalificationsgainedalsohaveamajorimpactontheincomeoftheindividual,asshownbythegraphbelow.
WageRatesbyQualificationLevel
Thosewithathird/tertiary(degree)levelqualificationearnedmorethan40%abovetheaverage.Thosewithnoqualificationsearnedonlyc.75%oftheaverageandthereforeareathighriskofpoverty.
CommentoneducationaldisadvantageThesefindingsshowclearlythatonalleducationalindicatorsthemajorityofchildrenandyoungpeopleinthetargetareasarefailingtoachievetheirpotentialintermsofeducationaloutcomes.Evenattendanceatschoolisasignificantproblem,rightfromprimaryschool(andmuchworseatpost-primary).Outcomesintermsofgoingontoagrammarschool,achievingGCSEs,AlevelsandgoingontocollegeoruniversityareverysignificantlylowerthantheNIaverage.
Theextentofeducationaldisadvantageismuchworsethanwouldbeanticipatedfromthedataoneconomicdisadvantage(seeabove)aloneandcomparespoorlywithothermoreeconomicallydisadvantagedpredominantlyCatholic/Republicanareas.
0%
20%
40%
60%
80%
100%
120%
140%
160%
180%
2011201020092008200720062005
Tertiary A-level No Quals
CHAPTER TWO
The needs of disadvantagedcommunities in Lisburn

Page 25
IftheevidenceinrelationtogenderforNorthernIrelandasawholeisthesameinLisburn,itisalsolikelythatboysinLisburnareperformingmorepoorlythangirls.
ThesefindingsareconsistentwiththefindingsofthePWCNI-widestudycommissionedbytheDepartmentofEducationin2008,whichshowedthatatKeyStage2EnglishandMathematics,proportionatelyfourtimesasmanycontrolledschoolswereunderperforminginNIcomparedtomaintainedschools.AtGCSEEnglishandMathematics,14%ofcontrolledschoolsinNIwereunderperforming,comparedwith4%ofmaintainedschools.TheyalsosupporttheconclusionsofthePurvisReviewinrelationtounder-achievementofProtestantworking-classchildren.
Itiscommonforschoolstobeblamedforthisunder-achievement.However,theresearchevidenceshowsthat75-90%ofthedifferencebetweenchildrenwhoachieveandunder-achieveisduetofactorsoutsideofthecontrolofschools,particularlyinrelationtoparentswhothemselveshaveunder-achievededucationallyand,asaresult,donotvalueeducation.
2.4Health&WellbeingThissectionlooksatsomeofthemeasurableindicatorsofhealthwithinthetargetdisadvantagedcommunitiesinLisburnandtheviewsofthoseinvolvedinthecommunityconsultations.
Dentalregistrationsofyoungchildren1Thelevelsofdentalregistrationsof0-2and3-5yearoldsin2011areconsistentlylowerthantheNIaverage(27.8%for0-2yearoldsand63.6%for3-5yearolds)inallthetargetareas,exceptfor0-2yearoldsinHillhall.
Ward Dental registrations of 0-2 year olds
Dental registrations of 3-5 year olds
Comment
OldWarren 19.6% 43.2% 68%and70%respectivelyoftheaverage
LaganValley 17.9% 46.7% 64%and73%respectivelyoftheaverage
Tonagh 21.6% 40.2% 78%and63%respectivelyoftheaverage
Hilden 24.8% 49.5% 89%and78%respectivelyoftheaverage
Knockmore 24.4% 54.3% 88%and85%respectivelyoftheaverage
Hillhall 27.9% 51.8% ThesameastheNIaveragefor0-2yearoldsbutonly81%oftheaveragefor3-5yearolds
NIAverage 27.8% 63.6%
1 DentalRegistrations2011CSA

Page 26
SmokingduringpregnancyMothersinmostofthetargetareasaremuchmorelikelytosmokeduringpregnancythantheNIaverageof16%:
Percentageofbirthstounmarriedmothers2
MostofthetargetareasaresubstantiallyabovetheNIaverageof39.8%forthepercentageofbirthstounmarriedmothersin2009,exceptforKnockmore1.TheSOAswiththehighest%ofbirthstounmarriedmothersareOldWarren,LaganValley1andHillhall1.
0 10 20 30 40 50 60 70 80 90 100
Hillhall
Hilden
Lagan Valley
Tonagh
Knockmore
Old Warren
NI average 16%
34%
29%
25%
24%
19%
16%
(more than twice the NI average)
(87% above the NI average)
(56% above the NI average)
(50% above average)
(19% above the NI average)
Hillhall is the same as the NI average
0 10 20 30 40 50 60 70 80 90 100
Knockmore 2Knockmore 1
KnockmoreHillhall 2Hillhall 1
HillhallTonagh
Hilden 2Hilden 1
HildenLagan Valley 1
Old Warren 72.5%63.2%
52.9%55.6%
50%48.7%
43.5%60.9%
26.1%33%
29.2%42.3%
(82% above the NI average)
(58.8% above the NI average)
(33% above the NI average)
(40% above the NI average)
(26% above the NI average)
(22% above the NI average)
(11% above the NI average)
(53% above the NI average)
(below the NI average)
(below the NI average)
(below the NI average)
(11% above the NI average)
2 NINISwardandSOAprofiles(www.ninis.nisra.gov.uk–lastupdatedOctober2011)
CHAPTER TWO
The needs of disadvantagedcommunities in Lisburn

Page 27
Medianageofmothersofnew-bornbabies(notavailablebySOA)TheNIaverageageformothersofnew-bornbabiesis29.TheaverageinOldWarren,HillhallandHildenisyoungerthantheNIaverage.
LifeExpectancyLifeexpectancy(seemedianageatdeath,below)isbelowtheNIaverageforbothmenandwomeninOldWarrenandTonagh.ItisalsobelowtheNIaverageformeninHillhallandforwomeninKnockmore.
Medianageatdeath(notavailablebySOA)MostofthetargetwardshaveanaveragelifespanbelowtheNIaverageof79.OfparticularconcernisOldWarrenwherethedifferenceis6years.
0 10 20 30 40 50 60 70 80 90 100
Tonagh
Knockmore
Lagan Valley
Hilden
Hillhall
Old Warren
NI average 29
26
27
27
27
29
30
(3 years below the NI average)
(2 years below the NI average)
(2 years younger than the NI average)
(2 years below the NI average)
(same as the NI average)
(1 year older than the NI average)
0 10 20 30 40 50 60 70 80 90 100
Lagan Valley
Knockmore
Hilden
Tonagh
Hillhall
Old Warren
NI average 79
73
77
78
78
81
82
(6 years below the NI average)
(2 years below the NI average)
(1 year below the NI average)
(1 year below the NI average)
(above the NI average)
(above the NI average)

Page 28
Percentagedeathsunderage75*OldWarrenandKnockmore2arewellabovetheNIaverageof38.4%forthepercentageofdeathsin2009forpeopleundertheageof75.
CommunityConsultationsThecommunityconsultationsalsohighlightedarangeofphysical,mentalandsexualhealthrelatedissuesofconcern,which,intheresearchliterature,areoftenassociatedwithgeographicalareasofsignificantdisadvantage.Theseinter-relatedissuesincludethefollowing:
■ Smoking(includingsmokingduringpregnancy)■ Heavydrinking(includingdrinkingduringpregnancy)■ Druguse,especiallyprescriptiondrugs■ Depressionandothermentalhealthdifficulties■ Self-harmandsuicide■ Unhealthyeating■ Obesity■ Lackofexercise
CommentsonhealthandwellbeingissuesThestatisticsandcommunityconsultationsraisesignificantconcernsabouthealthandwellbeingissuesinthetargetareas.ThelevelofearlydeathinOldWarrenandKnockmore2isparticularlydisturbing.Thefactthatthemajorityofbirthsaretounmarriedmothersreflectschangesinsociety,butismuchhigherthanotherpartsofNorthernIreland(andLisburn).Itreinforcestheevidencefromschoolsofthehighlevelofloneparents,whichcanhavesignificantimplicationsforparenting.Thehighlevelofsmokingduringpregnancyisonecontributing
0 10 20 30 40 50 60 70 80 90 100
Lagan Valley 1Lagan Valley
Hilden 2Hilden 1
HildenKnockmore 2Knockmore 1
KnockmoreTonagh
Hillhall 2Hillhall 1
HillhallOld Warren 52%
37.5%36.4%
40%
35%38.5%
27%20%
57.1%26.1%
15.4%17.5%
41.7%
(35% above the NI average)
(just below the NI average)
(just below the NI average)
(the same as the NI average)
(below the NI average)
(70% of the NI average)
(half the NI average)
(almost 50% above the NI average)
(two-thirds of the NI average)
(4% above the NI average)
(40% below the NI average)
(less than half the NI average)
(9% above average)
* NINISwardandSOAprofiles(www.ninis.nisra.gov.uk–lastupdatedOctober2011)
CHAPTER TWO
The needs of disadvantagedcommunities in Lisburn

Page 29
factortopassingondisadvantagetothenextgeneration.Thelevelofdentalregistrationsisafurtherindicationofsomeparents’knowledgeorlackofconcernforthehealthandwellbeingoftheirchildren.
2.5SafetyandStabilityThissectionexploresissuesofsafetyandstabilityindisadvantagedcommunitiesinLisburn,includingprotectionofchildren,anti-socialbehaviourandcrime.
ChildProtectionThefollowingtableshowsthenumberofchildrenwhowerereferredtosocialservicesinrelationtochildprotectionissueslastyearand,aschildrenmoveinandoutoftheChildProtectionRegisterovertime,thenumberofchildrenwhoarecurrentlyonthechildprotectionregisterineachofthetargetSOAs:
SOA Number of children referred (2011)
Number of children currently on the child protection register (a
particular point in time in 2012)Derryaghy1 113(the2ndhighestSOAin
theSEHSCTarea)10
OldWarren 78 15
Tonagh 53 18(thehighestofanySOAintheSEHSCTarea
Hilden1 34 *
Hilhall1 33 10
LaganValley1 30 7
LaganValley2 27 *
Hilden2 5 *
*Lessthan5
ThesestatisticssuggestparticularchildprotectionconcernsinDerryaghy1,OldWarren,TonaghandHillhall1.

Page 30
Numberofanti-socialbehaviourincidentsAllthetargetwardsarewellabovetheNIaverageof141forthenumberofanti-socialbehaviourincidentsreported,exceptforHillhall(91):
Numberofcriminaloffencesper10,000ofthepopulation(2010/11)1
AllthetargetwardsarewellabovetheNIaverageforcrime,exceptforHillhallandKnockmore.ViolentcrimesaremorethantwicetheNIaverageinHildenandTonagh.
Violent crimes
Criminal damage
Burglary Other theft offences
Vehicle offences
Totals
Hilden 502.4 303.6 150 376.8 41.9 1573.6
Tonagh 477 278.9 32.3 319.3 68.7 1321.7
Laganvalley 310 330 73.3 190 40 1126.7
OldWarren 252.5 332.7 80.2 64.1 36.1 853.7
Hillhall 126.6 94 32.5 94 36.2 470.2
Knockmore 110 107.7 60.9 67.9 70.2 461.1
NIaverage 165.6 138.9 65.9 102.8 38.5 583.8
0 100 200 300 400 500 600 700 800 900 1000
Hillhall
Knockmore
Old Warren
Laganvalley
Hilden
Tonagh
NI average 141
(two and a third times the NI average)
(two and a third times the NI average)
(two and a quarter times the NI average)
(one and a half times the NI average)
(a third above the NI average)
(below average)
331
330
316
220
190
91
1 NINISwardandSOAprofiles(www.ninis.nisra.gov.uk–lastupdatedOctober2011)
CHAPTER TWO
The needs of disadvantagedcommunities in Lisburn

Page 31
NumberofdomesticabuseoffencesAllthetargetwardsareabovetheNIaverageof17forthenumberofdomesticabusecasesreportedin2010:
CommunityConsultationsTheconsultationswithlocalcommunities,schoolsandprofessionalsworkinginthearea,alsohighlightedconcernsinrelationtosafetyandstability,inparticular:■ youngpeopleengaginginanti-socialbehaviourandcriminalactivity,
includingviolence■ domesticviolence
However,insomeareastherealsoseemstohavebeenimportantimprovementsinrelationshipswiththepoliceinstartingtotrytotacklesomeoftheseissues.
CommentsonsafetyandstabilityThestatisticsfromthetargetareasreflectverysignificantconcernsaboutchildprotectionissues,anti-socialbehaviourandcrime,includingdomesticviolence,inmanyofthetargetareas,whichwerereinforcedduringthecommunityconsultations.
2.6ParentingAkeyunderlyingissueinallthecommunityconsultationswasamajorconcernaboutparenting,which,initself,hasanimpactontheotherissueshighlightedaboveof:educationalunder-achievement;lackofambition;unhealthylifestyles,etc.ensuringthatthecycleofdisadvantageandunder-achievementispassedongenerationtogeneration.
Parentingissuesarehardertoquantifyinstatisticalinformationandcanoftenonlybequantifiedindirectlye.g.throughissueslikethelevelofdental
0 10 20 30 40 50 60 70 80 90 100
Hillhall
Laganvalley
Knockmore
Hilden
Tonagh
Old Warren
NI average 17
36
36
34
33
32
20
(more than twice the NI average)
(more than twice the NI average)
(twice the NI average)
(twice the NI average)
(88% above the NI average)
(18% above the NI average)

Page 32
registrations(highlightedunder“health”above),childaccidentsorhospitaladmissions,orchildrenontheriskregister,orincare.
However,parentingcameupasthemajorthemeinnearlyallthecommunityconsultations.Someofthekeyissueshighlightedintheconsultationswereasfollows:
■ Havingchildrenwhentheparentsweretooyoung■ Parentingskillsnolongerpasseddownthroughthegenerations■ Lackofparentingknowledge■ Lackofaparentingculture■ Lackofownershipoftheeducationanddevelopmentoftheirchildren(theyare
perceivedasotherpeople’sresponsibilities)■ Lackofambitionfortheirchildren■ Wanttobetheirchildren’sfriends–lackofdiscipline■ Lackofengagementoffathers■ Lackofmalerolemodels
Otherissuesparticularlyconcernedwithparentingandhealth,alreadyhighlightedabove,wereasfollows:■ Feedingtheirchildrenunhealthyfood■ Obesity■ Smokinganddrinking■ Exercise■ Mentalhealthissuesforparentsaffectingthechildren■ Medicalproblemsforparentsaffectingthechildren
Otherissuesconcernedprimarilywithparentingandeducation,alreadyhighlightedabove,wereasfollows:■ Badexperienceofeducationthemselves■ Notreadingtotheirchildren■ Parentsnotstakeholdersinoureducationsystem■ Notengagingenoughwithschool■ ParentsonlyinterestedinbeinginvolvedinP1&P2andloseinterestafterthat■ Nothelpingchildrenwiththeirhomework■ Lackofambitionorexpectationfortheirchildren■ Childrenbeingallowedtostayuplate–childrentiredandlatethenext
morning■ Thereareparentswhoinotherwaysaregoodparentsbutdon’tvalue
education■ Poordisciplineathomeleadingtoconductproblemsatschool
CHAPTER TWO
The needs of disadvantagedcommunities in Lisburn

Page 33
2.7ProvisionforChildrenandYoungPeople
OldWarrenThereisoneplaygroup(asatelliteoftheColinSurestart)inOldWarren,withamorningcrèchefor10children,whiletheirparentsparticipateinaprogrammeandanafternoonprogrammefor2yearolds.
RaggedyBapplaygroupforchildrenaged2yearsand10months,inaformerNIHEhouseinAvonmoreParkOldWarren,ismanagedbyOldWarrenCommunityAssociation.Therearemorningandafternoonsessions.RaggedyBapisamemberofEarlyYears.
OldWarrenPrimarySchoolhasaNurseryClass.
KnockmoreThereisaplaygroupeachmorninginGroveActivityCentreforchildrenbetween2yearsand10monthsto4yearsold.StAloysiusPrimarySchoolinKnockmoreestate(OldWarrenward)hasanurseryclass.
TonaghTonaghPrimarySchoolhasareceptionclass.ThereisamotherandtoddlersgroupinachurchhallinTonagh.ThereisacrècheinStColumbasPresbyterian-MethodistChurch.
HilhallTheColinSureStarthasanoutreachprogrammebasedinanoldshopunitinHillhall,butwillbemovingintoanewcommunityfacility.Thereisanursery(BarbourNursery)inHilhallEstate.Localresidentshaveconcernsaboutthecriteriaforprioritizingadmissiontothenurserywhich,intheirview,favoursthechildrenofmiddle-classfamiliesfromoutsidethearea,andtheunemployedfromwithinthearea.ThereisalsoastatutorynurseryinLargymorePrimarySchool.
HildenBarnardosrunaParentInfantProgrammeinHilden.ThereisamothersandtoddlersagroupmintheGospelHall.After-schoolsprogrammesareruninthecommunityhousefor5-11,12-18and14/15yearolds.SomeyoungpeopletendtheFusionYouthProgrammeinLisburnCathedral.
LaganValleyInLaganValleythereisoneplaygroup,1daynursery(intheHospital)and1After-schoolclub.

Page 34
BallymacashThereisaplaygroupinBallymacashPrimarySchool(memberofEarlyYears)andanurseryclassinKillowenPrimarySchool.
Incontrasttotheaboveprovision,thereare3playgroups,1after-schoolscluband1crecheinWallacePark;3playgroupsinTwinbrook;and3creches,2daynurseriesand1after-schoolsclubinPoleglass.
YouthWorkSEELBisfundingaqualifiedyouthworkertoprovide6contactsessionswithyoungpeopleinOldWarren,throughOldWarrenYouthInitiativesandStreetsAhead(inOldWarren,HillhallandHilden).TheStreetsAheadfundingendsin18months.
AqualifiedyouthworkerisalsofundedbytheBoardtoprovide6hoursyouthworkinOldWarrenand6hoursinHillhall.TheBoardalsofundsasecond6houryouthoutreachpostinHillhallandoneinHilden.
SEELBisalsofundingfullandpart-timeyouthworkersintheYMCAincentralLisburn.TheBoardYouthServicehasaskedthemtofocusonKnockmore.
Thereisafull-timeyouthcentreaspartofLaurelhillCommunityCollege,withamaincatchmentareaofKnockmoreandBallymacash,plusLaurelhillschoolstudentsfromotherareas.
FollowingtheclosureofDerriaghyPrimarySchool,thesiteisbeingturnedintoayouthandcommunityfacility,withafull-timeyouthworker.
SEELByouthworkersdelivertheschool-based“NewBeginnings”programmefornewyear1pupils.
ManychurchesareinvolvedinyouthworkinLisburn.SixLisburnchurcheshavefull-timeyouthworkers.LisburnYMCA,inadditionto1.1familyworkandwrap-aroundsupport,providesyouthprovisionincentralLisburnfournightsandoneafternoonaweek,inadditiontoworkwithyoungpeopleatriskofschoolexclusion,inpost-primaryschools;analcoholprogrammeinpost-primaryschools;adviceonsexualandmentalhealth;andtrainingandemploymentforNEETS.
TheDepartmentofEducationplantoissuethelong-awaited“PrioritiesforYouth”draftyouthworkstrategyforNorthernIrelandbeforethesummer2012.
CHAPTER TWO
The needs of disadvantagedcommunities in Lisburn

Page 35
2.8ConclusionsinrelationtoindicatorsofneedinthetargetcommunitiesinLisburn
Thestatisticsinrelationtoneedsinthetargetcommunities,insomerespects,showapatternthatiscommontomanyworkingclasscommunitiesandconfirmedbymanyresearchstudies,withlowincomes;dependenceonbenefits;youngunmarriedmothers;smokingduringpregnancy;emotionalandmentalhealthdifficulties;anddifficultieswithanti-socialbehaviourandcrime,includingdomesticviolence.
Thefindingsthatarebothshockingandunexpectedfromanacademicperspective,aretheverypooreducationaloutcomesofaverysignificantnumberofchildrenandyoungpeople,thevastmajorityofwhomdonotevenachieve5GCSEswithEnglishandMaths,andthereforedonotachieveAlevelsorgoontheuniversityorcollege.Concernsaboutattendanceatschoolandunder-achievementareevidentfromprimaryschoolonwards.
Cycleofdeprivationandunder-achievementThesefindings,inadditiontotheviewsexpressedduringtheconsultationswithcommunitiesandprofessionalsinthetargetareas,suggestaviciouscycleofdeprivationandunder-achievement,that,astheliteraturewouldsuggest,ispasseddownthroughthegenerationsandwhichisnotbrokenbythecurrentsetofagencies,servicesandprogrammesworkingintheareas.Thiscyclepresentsmajorchallengesintryingtobringaboutchange.Intermsofinterventions,discussedlater,itispossibletoattempttointerveneatanypointinthecycle.

Page 36
CycleofDeprivationandUnder-Achievement
Difficult transition to nearest secondary school; poor nutrition; poor numeracy and literacy; low aspirations; behavioural problems; poor attendance at school; poor test results; lack of parental engagement with the school or homework; anti-social behaviour; drinking; smoking; early sexual experiences.
Poor nutrition; poor numeracy and literacy; low aspirations; behavioural problems; poor attendance at school; poor test results; lack of parental engagement with the school or homework; poor transfer test results or not entered in transfer test.
Educational under-achievement (leave school early with few or no
qualifications); unemployed or in low paid employment; low aspirations; poor
relationships with parents; anti-social behaviour and/or crime; engagement
with the criminal justice system; risky sexual experiences – multiple
partners; increasing experience of alcohol and drugs;
teenage/unplanned pregnancy; smoking
and/or drinking during pregnancy.
Lack of breast-feeding;
poor parenting; poor infant brain
development; poor parental attachment; parents
not talking to, playing with, or reading to children; lack of
boundaries established; behavioural problems; poor early
cognitive abilities; parents experiencing mental health difficulties
and/or problems with alcohol and/or drugs (including prescription drugs); children not ready for primary school.
AGE 11-14
AGE 5-11
AGE 14-18
AGE 0-4
CHAPTER TWO
The needs of disadvantagedcommunities in Lisburn

Page 37
3.1IntroductionTheCentreforExcellenceandOutcomesforChildrenandYoungPeople(CE04)definesEarlyInterventionas“interveningearlyandassoonaspossibletotackleproblemsemergingforchildren,youngpeopleandtheirfamiliesorwithapopulationatriskofdevelopingproblems.Earlyinterventionmayoccuratanypointinachild’slife”(GraspingtheNettle’Report2009).Anearlyinterventionapproachsuggestsinterventions:
■ intheearlyyearsofachild’slife,where,theevidencesuggests,manyproblemsinlaterlifearecreatedandatwhichstagebraindevelopmentismoulded;
■ attheearlystageofdifficulty,whenachildmaybevulnerabletopoordevelopmentaloutcomes;
■ basedonwholesocietyapproachtoearlyinterventionthroughanetworkofsupportsandservicesandmulti-agencyworking;
■ whichareevidence-basedthroughrigorousevaluation(eitheradoptingevidence-basedprogrammeswhichhavepreviouslybeenrigorouslyevaluated,orinnovatingevidence-informedprogrammeswhicharethenrobustlyevaluated;
■ arefocusedonclearlymeasurableoutcomes;■ supportingandempoweringparents,familiesandinformalsupportnetworks;■ whicharelong-term/sustainable(notshort-termfundedprojectswhichend
whenthefundingends);■ whichcombineuniversal(allchildren)preventionprogrammesandnon-
stigmatisingtargetedearlyinterventiononthosemostatrisk;■ areaccessibleandflexible;and■ promoteparticipationandinclusion.
3.2WhyisEarlyInterventionImportant?Theinternationalevidencefromaverywiderangeofsourcesanddisciplinesisallpointingtowardsthecrucialimportanceofearlyinterventionintacklingdisadvantageandunder-achievement.Themainreasonsareasfollows:
■ Aseriesofnationalandinternationalstudieshaveshownthatproblemsinchildrenasyoungasthreecanpredictmoreseriousproblemsintheteenageyearsandtwenties.
■ Agapincapabilitiesofachildagedthreeyearsoldfromalowsocio-economicgroup,comparedwithonefromahighsocio-economicgroup,willtendtoincreasecontinuallythroughoutthechild’sschoolyears.
CHAPTER THREE
Why early intervention

Page 38
■ Brainstudieshaveshownthatthemajorityofthedevelopmentofthehumanbraintakesplaceinthefirstthreeyears.Howthebraindevelopshashugeimplicationsforthedevelopmentofthechild.
■ Itismorecost-effectivetointerveneatayoungage.NobeleconomistJimHeckmanhasshownthatresourcesinvestedintheearlyyears(0-4)islikelyonaveragetoresultinseventimesthatamountinthelaterlifeofthechildintermsofreducedmentalhealthcosts,justicesystemcosts,etc.
3.3TheLinkbetweenPovertyandEducationalDisadvantageintheUKIn2010theJosephRowntreeFoundationpublishedastudyofchildren’seducationalattainment(AlisaGoodmanandPaulGregg26March2010),basedonfourlarge-scalelongitudinalsourcesofdataonchildrengrowingupintheUKtoday.TheseweretheMillenniumCohortStudy(UK-wide),theAvonLongitudinalstudyofParentsandChildren,theLongitudinalStudyofYoungPeopleinEnglandandtheChildrenoftheBritishCohortStudy.Thechildreninthesestudiesrangedfromearlychildhoodthroughtolateadolescence.
Theresearchshowedthateducationaldeficitsemergeearlyinchildren’slives,evenbeforeentryintoschool,andwidenthroughoutchildhood.Evenbytheageofthreethereisaconsiderablegapincognitivetestscoresbetweenchildreninthepoorestfifthofthepopulationcomparedwiththosefrombetter-offbackgrounds.Thisgapwidensaschildrenenterandmovethroughtheschoolingsystem,especiallyduringprimaryschoolyears.
AnalysisoftheMillenniumCohortStudyshowedbigdifferencesincognitivedevelopmentbetweenchildrenfromrichandpoorbackgroundsattheageofthree,andthisgapwidenedbyagefive.Thereweresimilarlylargegapsinyoungchildren’ssocialandemotionalwell-beingattheseages.Childrenfrompoorerbackgroundsalsofacedmuchlessadvantageous‘earlychildhoodcaringenvironments’thanchildrenfrombetter-offfamilies.Forexample,comparedwithchildrenfrombetter-offbackgrounds,thereweresignificantdifferencesinpoorerchildren’sandtheirmothers’:
■ healthandwell-being(e.g.birth-weight,breastfeeding,andmaternaldepression);
■ familyinteractions(e.g.mother–childcloseness);■ thehomelearningenvironment(e.g.readingregularlytothechild);and■ parentingstylesandrules(e.g.regularbed-timesandmeal-times).
Differencesinthehomelearningenvironment,particularlyattheageofthree,haveanimportantroletoplayinexplainingwhychildrenfrompoorerbackgroundshave
CHAPTER THREE
Why early intervention

Page 39
lowertestscoresthanchildrenfrombetter-offfamilies.However,alargeproportionofthegapremainsunexplained,orappearsdirectlyrelatedtootheraspectsoffamilybackground(suchasmother’sage,andfamilysize).
Thissuggeststhatpoliciestoimproveparentingskillsandhomelearningenvironmentscannot,ontheirown,eliminatethecognitiveskillsgapbetweenrichandpooryoungchildren.Ontheotherhand,manyaspectsoftheearlychildhoodcaringenvironmentdohaveapositiveeffectonchildren’ssocialandemotionaldevelopmentandresilience,meaningthatpoliciesaimedatimprovinghealth,parentingskillsandthehomelearningenvironmentcouldstillbeveryimportant.
AnalysisoftheAvonLongitudinalStudyofParentsandChildrensuggestedthatthegapinattainmentbetweenchildrenfromthepoorestandrichestbackgrounds,alreadylargeatagefive,grewparticularlyfastduringtheprimaryschoolyears.Byageeleven,onlyaroundthree-quartersofchildrenfromthepoorestfifthoffamiliesreachedtheexpectedlevelatKeyStage2,comparedwith97percentofchildrenfromtherichestfifth.PoorerchildrenwhoperformedwellinKeyStagetestsatagesevenweremorelikelythanbetter-offchildrentofallbehindbyageeleven,andpoorerchildrenwhoperformedbadlyatsevenwerelesslikelytoimprovetheirrankingcomparedwithchildrenfrombetter-offbackgrounds–animportantfactorbehindthewideninggap.
Someofthefactorsthatappeartoexplainthewideninggapduringprimaryschoolare:■ parentalaspirationsforhighereducation;■ howfarparentsandchildrenbelievetheirownactionscanaffecttheirlives
(self-efficacy);and■ children’sbehaviouralproblems,includinglevelsofhyperactivity,conduct
issuesandproblemsrelatingtotheirpeers.
Parentalaspirationsandattitudestoeducationvarystronglybysocio-economicposition,with81percentoftherichestmotherssayingtheyhopedtheirnine-year-oldwouldgotouniversity,comparedwithonly37percentofthepoorestmothers.Suchadverseattitudestoeducationofdisadvantagedmothersareoneofthesinglemostimportantfactorsassociatedwithlowereducationalattainmentatageeleven.Thefindingssuggestthatgovernmentpoliciesaimingtochangemothers’andchildren’sattitudesandbehaviourduringprimaryschoolingcouldbeeffectiveinreducingthegrowthintherich–poorgapthattakesplaceduringthistime.
AnalysisoftheLongitudinalStudyofYoungPeopleinEnglandfoundthatattainmentgapsatageelevenwerealreadylargeandfurtherwideningwasrelativelysmallintheteenyearscomparedwithearlierinchildhood.Bythetime

Page 40
youngpeopletaketheirGCSEs,thegapbetweenrichandpoorisverylarge.Forexample,only21percentofthepoorestfifthmanagedtogainfivegoodGCSEs(gradesA*-C,includingEnglishandMaths),comparedwith75percentoftherichestfifth(seethepreviouschapterforsimilarfindingsinNorthernIreland).
Itbecomeshardertoreversepatternsofunder-achievementbytheteenageyearsbuttherearesomewaysthatdisadvantageandpoorschoolresultscontinuetobelinked.Evenaftercontrollingforlong-runfamilybackgroundfactorsandpriorattainment,youngpeoplearemorelikelytodowellatGCSEiftheirparents:■ thinkitlikelythattheyoungpersonwillgoontohighereducation;■ devotematerialresourcestowardseducationincludingprivatetuition,
computerandinternetaccess;■ spendtimesharingfamilymealsandoutings;and■ quarrelwiththeirchildrelativelyinfrequently.
ThestudyalsofoundthatyoungpeoplearemorelikelytodowellatGCSEiftheyoungpersonhim/herself:■ hasagreaterbeliefinhis/herownabilityatschool;■ believesthateventsresultprimarilyfromhis/herownbehaviourandactions;■ findsschoolworthwhile;■ thinksitislikelythathe/shewillapplyto,andgetinto,highereducation;■ avoidsriskybehavioursuchasfrequentsmoking,cannabisuse,anti-social
behaviour,truancy,suspensionandexclusion;and■ doesnotexperiencebullying.
Sinceyoungpeoplegrowingupinpoorfamiliesdolesswellinalltheserespectscomparedwiththoseinbetter-offfamilies,thisprovidessomeexplanationfortheirpoorereducationalattainmentbytheendofcompulsoryschooling.Whileinterveningearlierinchildhoodislikelytobemosteffective,policiesaimedatimprovingattitudesandbehaviouramongteenagerscouldalsohavesomebeneficialeffectsinpreventingchildrenfrompoorbackgroundsfallingyetfurtherbehindduringthesecondaryschoolyears.
TheanalysisofchildrenoftheBritishCohortStudyfoundthatchildren’stestscoreswerelowestwhenpovertyhadpersistedacrossthegenerations,and,attheotherendofthespectrum,highestwhenmaterialadvantagewaslong-lasting.
Parents’cognitiveabilitiesandotherchildhoodcircumstancesplayaveryimportantroleinexplainingthegapbetweenthetestscoresofricherandpoorerchildrentoday.Nearlyone-fifthofthegapintestscoresbetweentherichestandpoorestchildrencouldbeexplainedbyanapparent‘direct’linkbetweenthechildhoodcognitiveabilityofparentsandthatoftheirchildren.Thiswasfound
CHAPTER THREE
Why early intervention

Page 41
evenaftercontrollingforawiderangeofenvironmentalfactors,andaftertakingintoaccountmanyofthechannelsthroughwhichcognitiveabilitymightoperate,suchasparents’subsequenteducationalattainment,adultsocio-economicpositionandattitudestoeducation.Overfour-fifthsofthegapinthetestscoresofricherandpoorerchildren,however,isnotexplainedbythedirectlinkbetweenthecognitiveabilityofparentsandthatoftheirchildren.
Ontheotherhand,whilegoodsocialskillsalsoappearedtobelinkedacrossgenerationsi.e.parenttochild,thesedonotmakeasignificantdirectcontributiontothecurrentgapincognitivetestscoresbetweenrichandpoorchildren.
Therewasalsoastrongintergenerationalcorrelationbetweenawidevarietyofotherattitudesandbehaviours,suchaswhetheraparentreadstotheirchildeveryday,andparentalexpectationsforadvancededucation.Thepassingofsuchtraitsacrossgenerationsalsohelpstoexplainthepersistentdisadvantagethatchildrenfrompoorbackgroundsfaceintheireducationalattainment.
Thesefindingssuggestthatattitudesandbehaviourarepotentiallyimportantlinksbetweensocio-economicdisadvantageandchildren’seducationalattainmentandhaveshowntwomajorareaswherepolicymighthelptoreduceeducationalinequalities.
Parentsandthefamilyhome:■ Improvingthehomelearningenvironmentinpoorerfamilies(e.g.booksand
readingpre-school,computersinteenyears).■ Helpingparentsfrompoorerfamiliestobelievethattheirownactionsand
effortscanleadtohighereducation.■ Raisingfamilies’aspirationsanddesireforadvancededucation,fromprimary
schoolonwards.
Thechild’sownattitudesandbehaviours:■ Reducingchildren’sbehaviouralproblems,andengagementinrisky
behaviours.■ Helpingchildrenfrompoorerfamiliestobelievethattheirownactionsand
effortscanleadtohighereducation.■ Raisingchildren’saspirationsandexpectationsforadvancededucation,from
primaryschoolonwards.
Therehasbeenamarkedshiftingovernmentpolicyemphasisinrecentyearsawayfromanarrowerfocusoneducationaloutcomes,andtowardsthewideremotionalandsocialwell-beingofchildren(atleastinEngland,WalesandScotland).

Page 42
However,someoftheareashighlightedbytheJRFstudyabove(GoodmanandGregg2010)arebettercoveredbyexistingpolicyandevidencethanothers.Forexample:
■ Therehasbeenincreasingemphasisonparentingprogrammesandimprovingchildbehaviourintheearlyyearsbeforeschoolingstarts,butmuchlesssointheprimaryschoolyears(andevenlessinsecondary).TheJRFresearch(GoodmanandGregg2010)suggeststhatreachingfamilieswhilechildrenareofschoolagemightcontinuetobeuseful.
■ Intensiveprogrammesthatfocusonhelpingsmallnumbersofchildrenmostinneedtendtohavethestrongestevidencebehindthem.However,educationaldisadvantageaffectsaverylargenumberofchildrenfromlow-incomefamilies,butwithlowerintensitythanthoseattheextreme,anditmaybethatpolicyneedstofocusmoreonthese.
■ Programmestoraiseeducationalaspirations(suchasAimHigherinEnglandandWales)typicallystartinthesecondaryschoolyears,whilethisresearchsuggeststhatsuchinterventionscouldbeworthwhileatayoungerage–forexampleinprimaryschools.
■ Theevidenceonschoolandlocal-basedinterventionstoimproveyoungpeople’ssocialandemotionalskills,behaviour,andparticipationinpositiveactivitiesneedstobestrengthenedthroughrobustevaluation.
■ Educationalbodiesandschoolshaveasignificantroletoplayintacklingmanyoftheissuesraisedhere.Relevantpoliciesarelikelytoincludehowfundsareallocatedtowardspupilsfromthepoorestbackgrounds,andthedirectteachingsupportprovidedtochildrenwhentheystarttofallbehind.Ifsuccessful,thesesuggestedchangesmightatleasthelptopreventchildrenfrompoorbackgroundsfromslippingfurtherbehindtheirbetter-offpeersthroughouttheirschooling,andindeedcouldgosomewaytowardsclosingtherich–poorgap.
ThefindingsoftheJRFstudy(GoodmanandGregg2010)maybeparticularlyimportantintryingtounderstandwhythedataforworkingclassProtestant/LoyalistcommunitiesinLisburn(andNorthernIrelandmoregenerally)showssuchpooreducationaloutcomes,comparedtoevenmoredeprivedCatholic/Republicanareas.Akeyissuemaybeparentalattitudesandaspirations.
TheindependentreportfromDawnPurvisMLA(Purvis2011)suggeststhatitmaybearesultofdifferentattitudestoeducationwithinworkingclassProtestant/
CHAPTER THREE
Why early intervention

Page 43
Loyalistcommunitiesthathistoricallyreliedonchildrenfollowingtheirparentsfootstepsintolarge-scaleindustrialemployment(e.g.linenmills,threadmills,ropeworks,shipyard,aircraftmanufacture,etc),atrade,orthesecurityservices,forwhicheducationalrequirementswerelow.Whilemuchofthesekindsofjobshavegoneandtheroutesintoemploymentarenowbasedonpublicadvertisementswithclearselectioncriteriaincreasinglybasedonqualificationsandexperienceobtained.However,thecultureandattitudesthatexistedinpreviousgenerationsmaybestillinfluencingattitudestowardseducationandaspirationsinProtestant/Loyalistworkingclasscommunities.
3.4AllenReportsWorkinEnglandbyGrahamAllenMPandIanDuncanSmithMPin2008(EarlyIntervention:GoodParents,GreatKids,BetterCitizensAllen&DuncanSmith2008)andGrahamAllenin2011(EarlyIntervention–theNextStepsAllen2011)hashighlightedtheneedforanemphasisonearlyinterventiontomakesurechildrengetthebeststartinlife.Forexample,theirreviewoftheinternationalliteraturefoundthat:
■ Achild’sdevelopmentscoreatjust22monthsofagecanserveasanaccuratepredictorofeducationaloutcomesatage26
■ Boysassessedasbeing“atrisk”bynursesattheageof3were2.5timesaslikelytohavecriminalconvictions(55%forviolentoffences)attheageof21asthosedeemednotatrisk
TheAllenreportshighlighttheinternationalevidencewhichshowsthatbraindevelopmentintheearlyyearsisacriticalfactorinthedevelopmentofchildren.Babiesarebornwithone-quarteroftheirbraindeveloped.Thereisthenveryrapiddevelopmentofthebrain,sothatbytheageofthree,80%oftheirbrainshavebeendeveloped.Duringthiscriticalperiod,neglect,thewrongtypeofparentingorotheradverseexperiencescanhaveaprofoundeffectonhowchildrenareemotionally“wired”,whichwilldeeplyinfluencefutureresponsestoeventsandtheirabilitytoempathisewithotherpeople.
TheAllenreportsdemonstrate,fromtheliterature,thatearlyinterventiontopromotesocialandemotionaldevelopmentcansignificantlyimprovementalandphysicalhealth,educationalattainmentandemploymentopportunitiesandthatitcanalsohelppreventcriminalbehaviour(especiallyviolentbehaviour),drugandalcoholmisuseandteenagepregnancy.

Page 44
Allenconcludesthattherightkindofparentingisabiggerinfluenceonchildren’sfuturethanwealth,socialclass,educationoranyothersocialfactorandsoparentsneedtobegiventheinformationandsupportthattheyneedtohelptheirchildren.
Thereportsalsorecommendtheintroductionofearlyinterventionprogrammeswhichhavebeenshowntoworkinimprovingoutcomesforchildren.Helists72ofthemostpromisingearlyinterventionprogrammes,19ofwhichalreadyhaveverysignificantevidencefortheireffectiveness.
Hisreviewoftheliteraturealsodemonstratesthecosteffectivenessofinterveningearlyinachild’slifetotackleasocialproblemasopposedtointerveninglateron.Economicevaluationsofsomeofthemosteffectiveearlyinterventionprogrammeshaveshownthatinvestinginthefirstfewyears(frompregnancy)ofachild’slifecansavemultiplesofthatinvestmentinlatercostsofprison,welfarebenefits,justiceservices,treatmentprogrammes,mentalhealthservices,etc.Ithasbeenshown,forexample,thatLifeSkillsTrainingprogrammescanproducesavingsof25timesthecostoftheprogramme.
ResearchontheConsequencesofChildhoodDisadvantageinNorthernIrelandSullivanetal(2010)publishedaresearchreport*ontheConsequencesofChildhoodDisadvantageinNorthernIrelandatage5,basedontheNIpartoftheUKMillenniumCohortStudy,in2010.Theresearchfoundthat:
■ Health-relatedindicatorsamongparents,suchassmoking,breastfeedingandBMIwerelessfavourableinNIthaninGB
■ Parents’BodyMassIndex(BMI)islinkedtothechild’sBMIandalsotothechild’seducationalandbehaviouralscores
■ Povertyislinkedtoalltheoutcomes.However,cognitiveandeducationaloutcomesaremorestronglystructuredbypovertythanthehealthandbehaviouraloutcomes.Parentaleducationandsocialclassareparticularlypowerfulpredictorsofeducationalandcognitiveoutcomes.Theirimpacthowevercanonlypartiallyaccountedfordespitethelargenumberofpotentialmediatorsincludingrichinformationonparentingpractices
■ Variablesreflectinggoodparentingpractices,regularityandastronghomelearningenvironmentpredictpositivecognitive,educationalandbehaviouraloutcomes.Father’sinvolvementhasexplanatorypowerforcognitiveandeducationaloutcomes
CHAPTER THREE
Why early intervention
* Sullivan,A.,Cara,O.,Joshi,H.Ketende,S.andObelenskaya,P.(2010)The Consequences of Childhood Disdvantage in Northern Ireland at Age 5OFMDFM

Page 45
■ Parents’longstandingillnessesandmentaldistressarelinkedtopoorercognitive,educationalandbehaviouralassessmentsandgeneralhealthinthechild
3.5ConclusionsinrelationtoEarlyInterventionAlltheevidencefromtheUKandinternationalsourcespointstotheimpactofparents’educationandsocialclassontheoutcomesfortheirchildren.Thegapbetweenchildrenofdifferentbackgroundsisevidenteveninthefirsttwoyearsoflifeandwidenscontinuouslythroughouttheirchildhood.
Theevidencedemonstratesboththeeffectivenessandcost-effectivenessofinterveninginthefirstcoupleofyearsofachild’slife.Thereareconsiderablesavingsforthestateininvestinginearlychildrenratherthantryingtotacklethesocialproblemsthatemergelaterinlife.
Theliteraturealsohighlightstheimportanceofbasinginterventionsonrealevidenceofwhatworks,especiallyevidencegatheredfromwellrunlargescaleRandomControlTrials.
Theresearchonearlyinterventionalsohighlightsvariousotherissues,includingthefollowing:
■ Parents’obesity,physicalillnessandmentalhealthproblemscanhaveasignificantimpactontheoutcomesfortheirchildren.
■ Parentingiscriticaltothedevelopmentofchildrenandyoungpeople.Effortstoimproveparentingneedtostartfrombeforebirthandcontinueinprimaryschool.
■ Interventionsneedtobeprioritizedonthe0-12agegroup,especiallythe0-2yearoldsandtheirparents
■ Increasingeducationalaspirations,sothateducationisvalued,iscriticaltoimprovingeducationalachievement.
■ Programmesthattargetaverysmallnumberofvulnerablefamiliese.g.thosefocusedonchildprotection,missthelargenumberofchildrenindisadvantagedcommunitieswhoarelikelytounderachieveandinturnfacearangeofeconomic,personalandsocialproblems

Page 46
CHAPTER FOUR
The Northern Ireland public policy context that supports the need for change
4.1IntroductionThefollowingsectionhighlightssomeofthekeypublicpolicydocumentsthatarehelpingtodrivethechangeinemphasistowardspreventionandearlyintervention.Thesepublicpolicydocumentscomeunderthebroadheadingofpublichealth;children,youngpeopleandfamilies;education;area-basedinitiatives;andtheProgrammeforGovernment.However,itisimportantnottoreinforcethefragmentationofpolicyandservicesthathasdevelopedfromsilothinkinginpolicydevelopment.
Relevantquotesthatspecificallysupportanearlyinterventionapproachareunderlinedbelow.
4.2PublicHealth
InvestingforHealthIn2002theDHSSPSpublisheditsInvestingforHealthstrategywhichrecognisesthathealthandwellbeingarecruciallydeterminedbythesocial,economic,physicalandculturalenvironmentandseekstoshifttheemphasisfromaconcentrationonthemedicaltreatmentofill-healthtowardstacklingthefactorswhichadverselyaffecthealthandperpetuatehealthinequalities.Thestrategyhighlightstheconsistentinternationalevidencethatthelowerthesocio-economiccircumstancesoffamilies,theworsethehealthandwellbeingofmembersofthefamilyarelikelytobe.Itstatesthat“investinginthecrucialearlyyearsandeducationcanbreakthecycleofdeprivation”.
Thestrategysetouttwooverarchinggoals:■ Toimprovethehealthofourpeoplebyincreasingthelengthoftheirlives
andincreasingthenumberofyearstheyspendfreefromdisease,illnessanddisability
■ Toreduceinequalitiesinhealthbetweengeographicareas,socio-economicandminoritygroups
Italsoestablishedanumberofobjectivesincluding:■ Toreducepovertyinfamilieswithchildren■ Toenableallpeopleandyoungpeopleinparticulartodeveloptheskillsand
attitudesthatwillgivethemthecapacitytoreachtheirfullpotentialandmakehealthychoices.
Thestrategyrecognisesthat■ responsibilitiesforachievingthesegoalsrestswitharangeofdifferent
governmentdepartments■ Actionsneedtobecarriedinpartnershipsbetweenalltherelevantbodies

Page 47
■ Thatcommunitiesneedtobeengagedthroughacommunitydevelopmentapproach
AHealthierFutureIn2005theDHSSPSpublisheda20yearvisionforhealthandwellbeinginNorthernIreland2005–2015entitled,AHealthierFuture,to“improvethephysicalandmentalhealthandsocialwellbeingofthepeopleofNorthernIreland”.
Thevisionexplicitlyrecognisesthat“themostimportantfactorsindeterminingthehealthandsocialwellbeingofthepopulationaredeterminedbythecircumstancesinwhichweliveandwork,suchas:• disadvantageandsocialexclusion• poverty• unemployment• loweducationalachievement• socialandcommunityenvironment• housingandlivingconditions• workingconditions• thewiderenvironment.
Ithighlightsthatpoorersocio-economicgroupsarelikelytohavehigherincidenceofcancer,diabetesandotherlong-standingillnesses.
TheVisionrecognisesthatthereneedstobe“anewemphasisonreducingsmoking(esp.amongstchildren),reducingalcohol-relatedharm,tacklinglevelsofobesity,increasinglevelsofphysicalactivityandpromotinggoodmentalhealth.
Itsetsanoutcometo“reducebytwothirdsthegapinlifeexpectancybetweenthoselivinginthemostdeprived20%ofelectoralwardsandtheaveragelifeexpectancyhereforbothmenandwomenbetween2000and2015.
MarmotReviewInNovember2008,ProfessorSirMichaelMarmotwasaskedbythethenSecretaryofStateforHealthtochairanindependentreviewtoproposethemosteffectiveevidence-basedstrategiesforreducinghealthinequalitiesinEnglandfrom2010.Thefinalreport,‘FairSocietyHealthyLives’,waspublishedinFebruary2010,andconcludedthat
■ Reducinghealthinequalitiesisamatteroffairnessandsocialjustice.Themanypeoplewhoarecurrentlydyingprematurelyeachyearasaresultofhealthinequalitieswouldotherwisehaveenjoyed,intotal,between1.3and2.5millionextrayearsoflife.

Page 48
■ Thereisasocialgradientinhealth–theloweraperson’ssocialposition,theworsehisorherhealth.Actionshouldfocusonreducingthegradientinhealth.
■ Healthinequalitiesresultfromsocialinequalities.Actiononhealthinequalitiesrequiresactionacrossallthesocialdeterminantsofhealth.
■ Focusingsolelyonthemostdisadvantagedwillnotreducehealthinequalitiessufficiently.
■ Toreducethesteepnessofthesocialgradientinhealth,actionsmustbeuniversal,butwithascaleandintensitythatisproportionatetothelevelofdisadvantage.(proportionateuniversalism).
■ Actiontakentoreducehealthinequalitieswillbenefitsocietyinmanyways.Itwillhaveeconomicbenefitsinreducinglossesfromillnessassociatedwithhealthinequalities.Thesecurrentlyaccountforproductivitylosses,reducedtaxrevenue,higherwelfarepaymentsandincreasedtreatmentcosts.
■ Economicgrowthisnotthemostimportantmeasureofourcountry’ssuccess.Thefairdistributionofhealth,well-beingandsustainabilityareimportantsocialgoals.Tacklingsocialinequalitiesinhealthandtacklingclimatechangemustgotogether.
Thereportrecommendsthatreducinghealthinequalitieswillrequireactiononsixpolicyobjectives:■ Giveeverychildthebeststartinlife■ Enableallchildren,youngpeopleandadultstomaximisetheircapabilitiesand
havecontrolovertheirlives■ Createfairemploymentandgoodworkforall■ Ensurehealthystandardoflivingforall■ Createanddevelophealthyandsustainableplacesandcommunities■ Strengthentheroleandimpactofill-healthprevention.
Itarguesthat:deliveringthesepolicyobjectiveswillrequireactionbycentralandlocalgovernment,theNHS,thethirdandprivatesectorsandcommunitygroups;nationalpolicieswillnotworkwithouteffectivelocaldeliverysystemsfocusedonhealthequityinallpolicies;andeffectivelocaldeliveryrequireseffectiveparticipatorydecision-makingatlocallevel,byempoweringindividualsandlocalcommunities.
CHAPTER FOUR
The Northern Ireland public policy context that supports the need for change

Page 49
PHACorporateStrategyThisreporthashadasignificantimpactonthecorporatestrategyofthePublicHealthAgency(PHA)inNorthernIreland,Realising the health and wellbeing potential of people,whichhasfourprioritiesforimprovinghealthandwellbeing:
■ Giveeverychildthebeststartinlife■ Workwithotherstoensureadecentstandardofliving■ BuildsustainableCommunities■ Makehealthierchoiceseasier
Actionstopromotetheseprioritiesinclude■ CommissioningFamilyNursePartnershipsandotherevidence-basedfamily
supportforfamilieswhodonotqualifyforFNP■ Reviewingantenataleducationtopromoteparentchildinteractionandinfant
brainandemotionaldevelopment■ Breastfeedingpeersupportprogrammes■ RootsofEmpathyprogrammesinschools■ Supportingsocialeconomybusinessesandcommunityskillsdevelopment■ Supportincrementalexpansionofprogrammestodevelopthetop20%most
disadvantagedcommunities■ ImplementtheFitterFuturesforAllframeworktoaddressobesity■ StopSmokingSupportservicesespeciallyforpregnantwomen■ Putinplaceintegratedplanstopreventsuicideandpromoteemotionalhealth
PHACommunityDevelopmentThematicActionPlanThePublicHealthAgencyrecognizesthecrucialimportanceofusinganasset-basedcommunitydevelopmentapproach,whichlooksbeyondthemedicalmodelinimprovinghealthandwellbeingandclosinghealthinequalities.Therearefourmainstreams:
■ Directcommunitydevelopmentsupporttoorganizationsandcommunities■ Commisioningofserviceswhichpromotesustainablecommunities■ Commissioningofhealthandwellbeingimprovementservicesfrom
community-basedorganisations■ Innovationandtestingoutnewwaysofworking.
MentalHealthReviewIn2006acomprehensiveReviewofMentalHealthandLearningDisabilitywascarriedoutbyBamfordmakingawideRangeofrecommendationsforhowservicesinthisareacouldbeimproved.In2009theNIExecutivepublisheda2009-2011ActionPlaninresponsetotheReview,includinganaimtopromote“positivehealth,well-beingandearlyintervention”.Theseplannedactionsincluded:

Page 50
■ Publisharevisedcross-sectoralPromotingMentalHealthandWellbeingStrategy
■ Develop,consultonandimplementanEarlyYearsStrategy■ Introducearevisedcurriculumwhichprovidesopportunitiesthroughpersonal
developmentandotherareasforyoungpeopletodeveloptheskillstheyneedtocopewithchallengingpersonalsituationssuchasviolenceagainstwomenandchildren;self-harmetc.
■ Sustainindependentcounselingsupportserviceinpost-primaryschools■ Produceguidanceforpost-primaryschoolsonproactivelypromotingpositive
emotionalhealthandwellbeingamongstaffandpupils
SexualHealthPromotionInNovember2008DHSSPSpublishedaSexualHealthPromotionStrategyandActionPlan,inordertoimprove,protectandpromotethesexualhealthandwellbeingofthepopulationinNorthernIreland”.Itsobjectivesinclude:■ Toreducethenumberofunplannedbirthstoteenagemothers■ Topromoteopportunitiestoenableyoungpeopletomakeinformedchoices
beforeengaginginsexualactivity,especially,empoweringthemtodelayfirstintercourseuntilanappropriatetimeoftheirchoosing.
Theapproachofthestrategyincludesensuringthatservicesareaccessibleandresponsivetoneed,includetheneedsofdisadvantagedgroupsandthoseathighestrisk;andactiontotacklethedeterminantsofsexualhealthbasedonanevidencedbasedapproach.
TheStrategyacknowledgesthatthereisa“stronglinkbetweensocialdeprivationandSTIs,abortionsandteenagepregnancyandearlymotherhoodisassociatedwithpooreducationalachievement,poorphysicalandmentalhealth,socialisolationandpoverty”.ResearchinNorthernIrelandhasshownthat“respondentsfromapartlyskilledsocio-economicbackgroundweretwiceaslikelyasthosefromaprofessional/managerialbackgroundtohavehadsexualintercoursebeforetheageofsixteen”.
AcrucialaspectoftheSexualHealthPromotionStrategyisPrevention,including“everyonehavingthelifeskillsandaccesstoservicestoenablethemtomakeinformedchoicesandtodeterthedevelopmentofhealthcompromisingbehaviours.Thisisparticularlyimportantforyoungpeopleasthemajorityofparents,healthandeducationalprofessionalsagreethatsexualrelationsarebestdelayeduntilayoungpersonissufficientlymaturetoparticipateinamutuallyrespectfulrelationship”.
CHAPTER FOUR
The Northern Ireland public policy context that supports the need for change

Page 51
Italsostressestheimportanceofparentsandcarershavingthe“skillsandknowledgetotalktotheirchildren,asgoodparent/childcommunicationandsexualhealthissuescanhelpdelayfirstsexualexperienceandlimitpoorsexualhealthoutcomes”IthighlightsthepotentialroleofSureStart,HealthySchools,HealthActionZonesandHealthyLivingCentresinpromotingpartnerships.
Thestrategyalsoacknowledgesthat“schoolshaveanimportantcontributiontomakeininfluencinganddevelopingyoungpeople’ssexualhealthandwellbeingthroughthedeliveryofeffectivePersonaldevelopment,includingRelationshipandSexualEducation”.
Thestrategysetsspecifictargetsincludingthefollowing:■ 92%of11-16yearoldsshouldnothaveexperiencedsexualintercourseby
2013■ Areductionof25%intherateofbirthstoteenagemothersunder17yearsof
ageby2013.
SpecificactivitiesintheActionPlanincludethefollowing:■ TocontinuetoimplementguidelinesonRelationshipsandSexualEducation■ Toprovideopportunitiestoyoungpeopleinschoolandyouthsettings
todeveloptheskillstheyneedforlifetosupporttheminappropriatelymanagingtheirrelationships,includingsexuallifestyles
■ Tofurtherdevelop,particularlyinareasofsocio-economicdeprivationandruralareas,communitybasedteenagepersonaldevelopmentprogrammesthatwillincorporatesexualhealthissuesandrisktalkingbehaviour
SuicidePreventionIn2006theDHSSPSissuedits5-yearSuicidePreventionStrategyandActionPlan,Protect Life,followingverysignificantconcernaboutthenumberofsuicidesinNorthernIreland,particularlyamongstyoungpeople.Actionstobedeliveredbyvariouspartnersincludedwere:■ Toprovidefamilieswiththeopportunitytoavailofnon-stigmatising
practicalinterventionstohelpconsolidateparenting,copingandlifeskills■ Topromotetheinclusionofpromotingpositivementalhealthasakey
elementofthe“HealthyScvhools”programmeandensurethatchildrenandyoungpeopleareprotectedfromallformsofbullying
■ Toraiseawarenessofandensureavailabilityandtimelyaccesstoappropriateinterventionservices(e.g.ChildandAdolscentMentalHealthServices,mentoringschemesandotherappropriatestatutoryandvoluntaryservices).
■ Encouragetheinclusionofcopingandlifeskills,emotionalliteracy,andprogrammesthatpromotepositivementalhealthintheschoolcurriculum
■ TodevelopenhancedlinkagesbetweentheHealthandSocalServicesandthe

Page 52
community/voluntarycounselingandsupportnetwork,particularlyinrelationtotransitionservicesandtobridgeanygapsinserviceprovision
■ Toenhancetheroleofthecommunity/voluntarysectorconcerningtheprovisionofmentoringsupportforyoungpeopleatriskofsuicideandself-harm
■ Toensurethatappropriatesupportservicesreachouttoallmarginalizedanddisadvantagedgroups,inparticularlesbian,gay,bi-sexual,andtrans-gendergroups,ruralcommunities,ethnicminorities,andthosepeoplewhoareeconomicallydeprived.
AlcoholandDrugsIn2006theDHSSPSpublisheda5-yearcross-sectoralstrategy,New Strategic Direction for Alcohol and Drugs,thatsoughttoreducetheharmrelatedtobothalcoholanddrugmisuseinNorthernIreland(seeoutlineofdraftPhase2below).
In2008theDHSSSPSpublishedaRegional Hidden Harm Action PlantorespondtotheneedsofchildrenborntoandlivingwithparentalalcoholanddrugmisuseinNorthernIreland.ThePlanhighlightssomeofthepotentialimpactsforachildoflivingwithparentalalcoholordrugabuse,including:■ Harmfulphysicaleffectsonunbornandnewbornbabies■ Impairedpatternsofparentalcareandroutineswhichmayleadtoearly
behaviouralandemotionalproblemsinchildren■ Higherriskofemotionalandphysicalneglectorabuse■ Lackofadequatesupervision■ Povertyandmaterialdeprivation■ Repeatedseparationfromparents…■ Childrentakingoninappropriatesubstitutecaringrolesandresponsibilities
forsiblingsandparents■ Socialisolation■ Disruptiontoschoolingandschoollife■ Earlyexposuretoalcoholanddrugmisusingcultureandassociatedillegal
activitiesandlifestyles■ Poorphysicalandmentalhealthinadulthood
Theprinciplesunderpinningtheactionplaninclude“Afocusonpreventionandearlyidentification”andthatservicesneedtobebasedon“evaluationofeffectiveness”,aswellaswhatchildrenandparents/carerssaytheyneed.
TheActionPlanoutlineswhatshouldbeincludedinacontinuumofspecialistservices,including:■ Familyplanningservices■ Maternityservices
CHAPTER FOUR
The Northern Ireland public policy context that supports the need for change

Page 53
■ Post-natalandearlyYears■ Specialistservicesandsupportforchildren(andprovidessomeUKexamples)■ Confidentialhelpandadvice■ Parentinginterventions,including“well-evaluatedparentingprogrammes,
suchasWebster-Stratton,andspecificprogrammestargetedtosubstancemisusingparents(andgives3UKexamplesofservices)
■ Familyfocusedservices,includingfamilytherapies,parentingwork,1:1workincludingcounselingwithchildrenandwithparents
■ practicalsupport■ Art,dramaandplaytherapy
In2009theDepartmentissuedanActionPlan,Addressing Young People’s Drinking in Northern Ireland,tosupporttheNew Direction for Alcohol and Drugs.ThePlanaimstoreduceboththesupplyof,anddemandfor,alcoholamongstyoungpeople;preventandreducetheharmsfromalcoholuse;andidentifyandprovidetheappropriatesupportforthosemostvulnerableoratrisk.TheprincipleswhichunderpinthePlanincludetheroleoffamilies,theneedforevidence-basedinformation,theidentificationoflocalneeds,andafocusonthemostdisadvantagedareasthroughtheNeighbourhoodRenewalAreas.Actionsinclude:■ Delivery,inaconsistentmanner,alcoholeducationtoallyoungpeoplein
schools;develop,and/orenhancelocalpeerlearning/informationprojectsandinitiatives
■ Localcommunitiestoidentifyanddevelopsupport/diversionaryactivitieswhereyoungpeople’sdrinkingisidentifiedasanissue
■ Continuetoprovideinformation,interventionsandprogrammesonsafesexualpractices,promotingmentalhealth,suicideandself-harm,homeaccidents,trafficaccidents–particularlytargetingyoungdrinkersandthoseyoungpeoplelivinginNeighbourhoodRenewalAreas
■ Developaresearchprogrammeonyoungpeopleandalcohol,andensureallinitiativesarerobustlyevaluated
■ Commissionandpublisharangeofresearchandevaluationstouncoverwhichinterventionsmosteffectivelyaddressthisissue…
■ LocalHiddenHarmActionplansdevelopedandeffectivelyimplemented andthattakefullaccountofissuesrelatingtoalcoholmisuse…fromconception
to18
InJanuary2011theDepartmentissuedaconsultationdocumenttoreviseandextendtheoriginalstrategy(New Strategic Direction for Alcohol and Drugs Phase 2 2011-2016)ratherthanproduceanewstrategy.Objectivesintherevisedstrategyincludeto“promoteopportunitiesforthoseundertheageof18yearstodevelopappropriateskills,attitudesandbehaviourstoenablethemtoresistsocietalpressurestodrinkalcoholand/ormisusedrugs.

Page 54
SomeoftheemergingissueshighlightedbytheDraftNewStrategicDirectioninclude:■ Familiesandhiddenharm■ Mentalhealth,suicideanddrugsandalcoholmisuse■ Alcohol■ Linkswithsexualviolenceandabuse,anddomesticviolence.
Theprinciplessetoutintakingthestrategyforwardinclude:■ Evaluation,EvidenceandGoodPracticeBasede.g.informedbyevidenceof
theproblemsand“whatworks”andimprovingtheevidencebasethroughevaluation
■ Partnershipandworkingtogether■ Addressinglocalneed■ CommunityBased■ Long-termfocus
ThedraftNew Strategic DirectionhighlightsPreventionandEarlyInterventionasoneofthecriticalsupportpillars.Itstatesthat“PreventionandearlyInterventionislargelyconcernedwithencouraginganddevelopingwaystosupportandempowerindividuals,familiesandcommunitiesintheacquisitionofknowledge,attitudesandskills”.Itrecommendsthat“aparticularfocusshouldbeputontheimportanceofearlyintervention(especiallyyoungchildrenandfamilies)andtheadoptionoftargeted,aswellasuniversaltypesofpreventionwhichwillleadtothereductionofriskfactorsandthedevelopmentofprotectivefactorsassociatedwiththepreventionofalcoholanddrug-relatedharm”.Italsoarguesthat“interventionsmustbetailoredtoparticularsettingssuchastheschool,communityandworkplace…Theimportanceofformalandinformaleducationandcommunity-basedapproachesisacknowledged.”
ItrecommendsthatresourcestodelivertheNew Strategic Directionshouldbe“properlytargetedatactivitiesandprogrammesthathavebeenshownbypreviousresearchandevaluationtobeeffective”.
ThesuggestedKeyPrioritiesinclude:■ Targetingthoseatriskandvulnerable,includingvulnerableyoungpeople(e.g.
childrenandalcohol/drugusingparents;andschoolexcludees)■ Promotinggoodpracticeinrespectofalcoholanddrug-relatededucation
andprevention,basedon“soundconceptualprinciplesand…evidencedgoodpractice”
CHAPTER FOUR
The Northern Ireland public policy context that supports the need for change

Page 55
TheDraftStrategyoutlinesshorttolongtemoutcomes,includingreducingtheproportionofyoungpeoplewhodrinkonaregularbasis;whogetdrunk;whotakedrugs.
MaternityStrategyIn2011DHSSPSissuedadraftMaternityStrategyforconsultation,whichrecognisesthat“disadvantagestartsbeforebirthandaccumulatesthroughoutlife”.Ithighlightsthefactthatthoseindeprivedcommunities,youngermothers,motherswhodonotbreastfeed,motherswhosmoke,drinkheavily,usedrugs,orareobesearemorelikelytohavepoorerpregnancyoutcomes.Itacknowledgesthatifhealthinequalitiescanbereducedbefore,duringandafterpregnancythiswillimpactonthefuturehealthofthepopulation.
TacklingHealthinequalityatasub-regionallevelTheSouthEasternHealth&SocialCareTrust(SEHSCT)hasitsownHealthInequalityActionPlan2011/12,whichfocusesonthemostdeprived20%ofareaswithintheTrust(whichincludesOldWarrenandTonagh)includingthefollowingobjectives:■ SupporttheEmotionalDevelopmentofyoungchildreninthe20%most
deprived(NeighbourhoodRenewal/SureStart)areas–• throughthedeliveryofRootsofEmpathyprogramme“withastrong
evidenceforeffectiveness”• Supportingparentsindevelopingtheirchildren’semotionalfoundations
throughtheNewParentProgramme,IncredibleYearsParentingProgrammeandMellowParents/MellowBabiesprogrammes
■ Reducesmokinginthe20%mostdeprivedareasincludingananti-natalincentiveandsupportscheme
■ Reducechildhoodobesityinthe20%mostdeprivedareas,throughMini-Mendfor2-4yearoldsinSurestart
■ Mentalhealth,Suicidepreventionandselfharmby• Deliveringamentalhealthprogrammeinsecondaryschoolsinthe20%
mostdeprivedareas• Acommunicationandtrainingprogrammeinthe20%mostdeprived
communities■ Drugsandalcoholbydevelopinganddeliveringanewprogrammeaimedatthe
familiesofteenagedrinkers■ Supportsocialenterprise/employmentschemesinneighbourhoodrenewal
arease.g.Kilkooley,ColinBridgeandBallymote■ Improveoutcomesforlookedafterchildren

Page 56
4.3Children,YoungPeople&Families
TheGovernment’s10-yearStrategyforChildrenandYoungPeopleIn2006,OFMDFMpublisheditsinter-departmental10-yearstrategyforchildrenandyoungpeople-Our Children and Young People – Our Pledge(OFMDFM2006)settingout6highleveloutcomesforchildrenandyoungpeoplethatallagenciesinNorthernIrelandshouldbeworkingtowards:Childrenandyoungpeopleshouldbe:
■ Healthy■ Enjoying,learningandachieving■ Livinginsafetyandwithstability■ Experiencingeconomicandenvironmentalwellbeing■ Contributingpositivelytocommunityandsociety■ Livinginasocietywhichrespectstheirrights
Thesupportingthemesofthe10yearstrategyincludethefollowing:■ Theneedtoadopta“whole-child”approach,whichgivesrecognitiontothe
complexnatureofourchildren’sandyoungpeople’slives■ Workinginpartnershipwiththosewhoprovideandcommissionchildren’s
services…■ Securingandharnessingthesupportofparents,carersandthecommunities
inwhichourchildrenandyoungpeoplelive■ Makingagradualshifttopreventativeandearlyinterventionapproaches
withoutcompromisingthosechildrenandyoungpeoplewhocurrentlyneedourservicesmost
TheStrategycontainsaspecificpledge“wewillpromoteamovetopreventativeandearlyinterventionpracticewithouttakingattentionawayfromourchildrenandyoungpeoplecurrentlymostinneedofmoretargetedservices.
Italsocontainsapledgeto“deliverimprovedoutcomesforallchildrenandyoungpeople,wewillensurethatallfuturepoliciesdevelopedandservicesofferedto,andaccessedby,childrenandyoungpeople,arebasedonidentifiedneedandonevidenceaboutwhatworks”.
Implementationandresourcingofthe10-yearstrategyhasbeendisappointingtomanyoftheorganisationsconcernedwithchildoutcomes.TheOFMdFMChildren’sUnithasbeenincorporatedintoawiderdepartment.
CHAPTER FOUR
The Northern Ireland public policy context that supports the need for change

Page 57
ChildrenandYoungPeople’sStrategicPartnershipIn2011aChildrenandYoungPeople’sStrategicPartnership(CYPSP)wasestablishedtoimproveoutcomesforchildrenandyoungpeoplethroughintegratedplanning.
TheCYPSPisthefirstChiefExecutiveledcrossagency,crosssectoralintegratedplanningandcommissioningprocessforNorthernIreland.ThisincludesALLstatutorysectororganisationswithresponsibilityforchildrenandyoungpeopleandrepresentativesfromVoluntaryandCommunityandBMEsectors.WithafocusonearlyinterventiontheChildrenandYoungPeople’sPlanisthekeydriverforthiswork.
ThePartnershiphasdevelopeda“NorthernIrelandChildrenandYoungPeople’sPlan2011-2014,whichsetsouthowintegratedplanningandcommissioningarrangementswillbeputinplacetosecureimprovementsinthe6highleveloutcomesforchildrenandyoungpeople(highlightedabove).OneofthefourthemesofthestrategyisEarlyIntervention–inparticular,seekingdesignationofNorthernIrelandasasiteforearlyinterventionandsupportingallagenciestoworktogetherinrelationtotheintegratedplanningandcommissioningofearlyintervention.Theotherthemesare“CommunicatingwithGovernment”,“IntegrationofPlanning”and“OptimisationofResources”.
ApartfromthedefinitionofearlyinterventionandhowtheCYPSPhasagreedtotakeforwardearlyintervention.OneoftheactionswithintheChildrenandYoungPeople’sPlanincludesthedevelopmentofastandardisedresilienceframeworkfortheevaluationofearlyinterventionprogrammesacrossNorthernIreland.
Outcomegroupshavebeenestablishedineachsub-region.TheSouthEasternOutcomesGroup,whichawidemembershipfromthestatutory,voluntaryandcommunitysectors,hasbeenmandatedbythePartnershiptoimplementoutcomesbasedplanningforLisburn&DownandNorthDown&Ards.ThepurposeoftheSouthEasternOutcomesGroupisto“carryoutintegratedplanningandcommissioningforchildrenandyoungpeopleinthearea,withspecificemphasisonsharingresourcesacrossagenciestoimproveoutcomesforchildrenandyoungpeople”.TheOutcomesGroupiscurrentlylookingattheestablishmentordesignationofmorelocalLocalityGroups(suchasColinEarlyInterventionCommunityandEarlyInterventionLisburn)tocarryoutoutcomesbasedplanningatthelevelofgeographywhichmakessenselocally.
TheSouthEasternOutcomesGrouphasalsosetinplacethefoundationsforageographicallybasedFamilySupportHubtoengagewithfamilieswhodonotmeetthethresholdforstatutorysocialworksupportandimproveco-ordinationof

Page 58
servicedeliverytoindividualfamilies.Barnardo’shasbeencontractedtodeliverthefamilysupportservicethroughthreefamilysupportworkersinLisburn.Itiscurrentlydealingwithc.50referralspermonth.
DHPSSPSFamiliesMatter(2009)TheDHSSPSFamilysupportstrategy,Families Matterisbasedonthesixoutcomesinthe10yearstrategyforchildrenandyoungpeopleandafamilysupport(Hardiker)modelwithfourlevels:
Level1:AllchildrenLevel2:ChildrenwhoarevulnerableLevel3:ChildreninneedinthecommunityLevel4:Childreninneedofrehabilitation
Thestrategyacknowledgesthat“earlyinterventionproducespositivedividendsintermsofchildrenandfamiliesnotneedingmorespecialistservicesatalaterdate”andthe“currentinequityinresourcingearlyinterventionservicescomparedtothoseofhigherneedsandthismustbeaddressed”.
ThestrategyhighlightsfourprioritythemesforDHSSPS:■ Informationforparentsandserviceplanners■ Access,includingavoidingstigma,language,etc■ SupportingFamiliesandParents,includingParentingEducation,Positive
Parenting,localitybasedservicese.g.extendedschools,children’scentres,relationshipsupport/mediationandSurestart
■ WorkingTogetherforfamiliesandCommunities,includingmulti-agencyworkingandcommonassessment
HealthChild,HealthyFutureTheDHSSPSpublishedaFrameworkfortheUniversalChildHealthPromotionProgrammeinNorthernIrelandfrompregnancyto19years,in2010.Itisbasedontheconceptofprogressiveuniversalismi.e.everychild/familyreceivesastandarduniversalservicei.e.setcontactsbythemidwife,healthvisitorandschoolnurse,etc.tothestandardsintheframework.However,acomprehensiveassessmentofneed(UNOCINI)shouldidentifywhereadditionalearlyinterventionsupportandinterventionsaretobeofferedtoamelioratethepotentialearlynegativeimpactofanyphysical,socialoremotionalfactor,suchasSurestart,breastfeedingsupport,counseling,evidence-basedparenting,thusreducinginequalities.Wherethisearlyinterventionisunabletoaddresstheneed,children/familiesareescalatedtoamoreprogressivelevelofinterventiontosafeguardthewelfareofthechild.
CHAPTER FOUR
The Northern Ireland public policy context that supports the need for change

Page 59
Thestrategyrecognisestheparticularimportanceofprovidingadditionalsupporttopregnantteenagersduetothehigherriskoflowbreastfeeding,lowbirthweight,highinfantmortality,highchildaccidents,highpostnataldepression.
TheFrameworkrecognisesthedevelopedunderstandingoftheneurologicaldevelopmentofachild’sbrain,theimportanceofparent-childattachmentinthefirstfewyearsoflife,andthenegativeimpactofmaternalstressinpregnancy.AmajoremphasisintheFrameworkisontheprovisionofparentingsupportandpositiveparentinge.g.usingagreedevidence-basedprogrammestosupportspecificworke.g.Solihullapproach,IncredibleYears,MellowParenting,theSocialBabyBook/Video,andBabyExpressNewsletters.
TheFrameworkaimstoachieve10specificoutcomes:■ Strongparent-childattachmentandpositiveparenting,leadingtobettersocial
andemotionalwellbeingamongchildren■ Carethathelpskeepchildrenhealthyandsafe■ Healthyeatingandincreasedactivity■ Preventionandreductionofsomeseriousdiseasesandcommunicablediseases■ Increasedratesofinitiationandcontinuationofbreastfeeding■ Readinessforschoolandimprovedlearning■ Earlyrecognitionofgrowthdisordersandriskfactorsforobesity■ Earlydetectionandactions(includingearlyintervention/referral)toaddress
developmentaldelayandillhealthandconcernsaboutsafety■ Identificationoffactorsthatcouldinfluencehealthandwellbeinginfamilies■ Bettershortandlongtermoutcomesforchildrenwhoareatriskofsocial
exclusion
TheFrameworkincludesthefollowingcoreelements:
■ Healthimprovement• Supportforparenting:EarlyInterventionandpreventionprogrammesfor
childrenandfamilies• Engagingfathers/partners• Healthpromotionincluding“stronglinksandclosercommunication
withcommunitydevelopmentprogrammesandotherinitiativesaimedatreducinginequalities,socialexclusion,eliminatingpovertyandimprovingeducationaloutcomes”
• PromotionofSocialandEmotionalDevelopment• Safeguarding
1 Theevidencebaseforsomeoftheseinterventionsisweakerthanothers

Page 60
• Schoolhealthprofiling,inorderto“developpreventionandearlyinterventionprogrammestoaddresstheneedsofthispopulationwiththeschoolsettingandwithinlocalcommunities”(Note:PHAtoleadtodeveloponetoolsupportedbyICT)
■ Healthprotection• Surveillance• Screening• Immunisation
DiscussionswithcommunitygroupsandthoseinvolvedinhealthvisitinghashighlightedthelackofresourcesavailableinNorthernIrelandtoeffectivelydeliverytheHealthy Child, Healthy Futureframework.Although,perhapsbetterintheSETrustareathanotherTrustareas,ahealthvisitorintheSETrustareaislikelytohaveacaseloadof300-400+families.Tobeabletoprovidemoreintensivesupportforthemostvulnerablenewmothers(fromthe20thweekofthepregnancytotwoyearsold)theTrusthasintroducedtheevidence-informedNew Parenting Programme.AnadditionalhealthvisitorisemployedinbothOldWarrenandHilhall,withacaseloadof25familieseach.ThedeliveryoftheserviceisbeingevaluatedbyQUB(notwithacontrolgroup).AsimilarmodelisbeingdeliveredintheColinarea,withahealthvisitorplustwosupportworkers.Theevidence-informed(butnotaprovenprogramme)10-14weekparentingskillsprogramme,Mellow Parents,developedinScotland,isalsobeingdeliveredinOldWarrenbytheTrust.
ChildPovertyStrategyTheChildPovertyAct2010placesastatutoryobligationontheNIExecutivetodevelopachildpovertystrategy.TheExecutive’sstrategyisdesignedtotryandbreakthecycleofpovertyandunderachievementby“raisingaspirations,increasingaccesstoopportunitiesthrougheducation,supportingparentsintowork,and,providingthenecessarysupporttothosemostinneedsuchaschildrenwithdisabilities,loneparentsandothers”.
Thecross-departmentalStrategysetsoutthekeyareasthattheExecutivebelievesarecrucialinaddressingthecausesandconsequencesofchildpovertyandinmeetingtheGovernment’sobligationsinTheAct.TheStrategyhastwokeystrandsofworkrelevanttothecausesandtheconsequencesofchildpoverty:
1. reducingworklessnessamongstadultswithchildren2. promotelongertermoutcomesthroughchildbasedinterventionswhichare
designedtotacklethecyclicalnatureofchildpoverty
CHAPTER FOUR
The Northern Ireland public policy context that supports the need for change

Page 61
TheStrategyhighlightsanumberofprinciplesthatunderpinandshouldsupportthedeliveryofthestrategy:■ Ashifttowardstacklingtherootcausesofpovertyandnotjusttreatingits
symptoms.■ PuttingchildrenatthecentreoftheStrategyandtakingintoaccounttheir
viewswhendevelopingpoliciesandprogrammestotacklechildpoverty.■ AdoptingaLifeCycleapproach,breakingthecyclethatresultsinchildren
bornintopovertybecomingworkingageadultsinlowincome.■ Promotingexcellenceinsupportacrossarangeofkeypolicyareasincluding
employmentandskills,education,childcare,healthandfamilysupport,housingandneighbourhoods,andfinancialsupport.
■ Agradualshifttowardstheuseofpreventativemeasurestotacklechildpovertyand,whenfamiliesfacedifficulties,interventionatanearlystage,reducingthelikelihoodofmoreseriousproblemsdevelopinginthefuture
■ Applyinganevidencebasedapproach.■ Adoptingawholefamilyapproachwhichconcentratesonallmembersofthe
family-children,youngpeople,andtheirparentsandsupportingfamilylife.■ Empoweringandenablingparentsonlowincomeintoworkandmakework
payforthoseonlowpay.■ Promotingpartnershipworkingacrossallsectorsincludingpublic,private,
voluntary,andcommunitysectors.■ RecognisingthecurrenteconomicclimateandtheneedfortheStrategytobe
balancedagainstexistingfinanciallimits.
TheKeyStrategicPrioritiesintheStrategyareasfollows:■ Ensure,asfaraspossible,thatpovertyanddisadvantageinchildhooddoesnot
translateintopooreroutcomesforchildrenastheymoveintoadulthood.■ Supportmoreparentstobeinworkthatpays.■ Ensurethechild’senvironmentsupportsthemtothrive.■ Targetfinancialsupporttoberesponsivetofamilysituations.
SomeoftherelevantActionAreasundertwoofthesepriorities,whicharerelevanttoanearlyinterventionapproachareasfollows:
Ensure,asfaraspossible,thatpovertyinchildhooddoesnottranslateintopooroutcomesforchildrenastheymoveintoadultlife■ Provideallchildrenandyoungpeoplewithopportunitiestoreachtheir
educationalattainmentregardlessofbackgroundandaddressbarrierstopupilsachievingtheirfullpotential.
■ Supportdisadvantagedfamiliestopromotethephysical,social,intellectualandemotionaldevelopmentoftheirchildrensothattheyflourishathomeandwhentheygettoschool.

Page 62
■ Supportthedeliveryofanaccessible,flexibleandqualitychildcaresector,sothatitiseffectiveinreducingbarrierstoemployment,particularlythoseexperiencedbydisadvantagedgroups,andsupportschilddevelopmentandwellbeing”.
■ Improvehealthoutcomesandtargetthosegroupswhoareparticularlyatriskorvulnerable,inordertotacklehealthinequalitiesofchildrenandyoungpeople.
■ Strengthenandimprovepreventionandearlyinterventionforallchildrenandtheirfamilies,particularlyinthefirstthreeyearsoflifetomaximisefutureoutcomesinhealthandwellbeing.
■ Providefamilysupportandinterventionservicestochildreninvulnerablefamilies.
■ Improveschoolreadinessandincreaseparticipationinformalandnon-formaleducation,youthservicesandsportsthroughaccessibleandaffordableculture,artsandleisureservices.
■ Addresssocio-economicdisadvantageinchildrenandmaximiseaccesstokeyservicesforchildrenandyoungpeople.
Ensurethechild’senvironmentsupportsthemtothrive:■ Promoteaffordable,accessibleplayandleisureprovisionforallchildrenand
youngpeople.■ Providedifferentlearningenvironmentsthroughyouthserviceswhich
complementformallearningandarefocusedonthepersonalandsocialdevelopmentofchildrenandyoungpeople.
■ Toimproveopportunitiesforlowincomefamiliestoparticipateinarts,cultural,sportingandleisureactivities.
■ Ensurethatparentscanaccessinformationandservices,includingtheRegionalFamilySupportDatabaseintheirlocalareastosupportthemincarryingouttheirparentalresponsibilities.
■ Makepublictransportmoreaccessibleandaffordabletoallchildrenincludingthosewithadisabilityinbothurbanandruralareas.
■ Continuetotakeactiontoaddressfuelpovertyinvulnerablehouseholds.■ Ensurechildrenandyoungpeoplearelivinginhomeswhichachievethe
DecentHomesStandard.■ Supportstatutoryandvoluntaryagencies,includinglocalcouncils,to
provideservicesandprogrammeswhichmeettheneedsoflocalcommunities,particularlydisadvantagedcommunities.
■ Continuetoaddresstheunderlyingcausesofdisadvantageandimprovethephysicalenvironmentofthemostdeprivedneighbourhoods.
AnactionplantoimplementtheChildPovertystrategyisexpectedtobepublishedbytheSummer2012.
CHAPTER FOUR
The Northern Ireland public policy context that supports the need for change

Page 63
4.4Education
Everyschoolagoodschool–apolicyforschoolimprovementTheDepartmentofEducationundertookareviewofthepreviousschoolimprovementpolicyandissuedthefindingsofthisreviewandproposalsforthewayforwardforpublicconsultationinJanuary2008.Followingconsultation,thefinalisedpolicydocument,EverySchoolAGoodSchool-APolicyforSchoolImprovementwaslaunchedbythethenEducationMinister,CaitrionaRuaneinApril2009.
TheDepartment’svisionis“toensurethateverylearnerfulfillshisorherpotentialateachstageofherorhisdevelopment”.
Thepolicyrecognisesthat“therearestilltoomanyyoungpeoplefinishingtheir12yearsofcompulsoryschoolingwithoutreaching”5+GCSEsgradeA*-C,especiallythosewhoareeconomicallyandsociallydisadvantaged,sothat“schoolsservingdisadvantagedcommunities,andcommunitieswherethevalueplacedoneducationmaynotbeashighasitmightbe,willneedmuchgreaterlevelsofsupport”.Inspectorshavereportedthatinone-thirdofprimaryschoolsinspectedthequalityofprovisionwasnotgoodenough(ChiefInspector’sReport2006-2008).
Thepolicyhighlightsthecharacteristicsandindicatorsofagoodschoolwitheffectiveperformance,inrelationto:■ Child-Centredprovision■ Highqualityteachingandlearning■ Effectiveleadership■ Aschoolconnectedtothelocalcommunity
TheDepartmentcommits,amongstarangeofthings,to“maintainingaparticularfocusontacklingthebarrierstolearningthatmanyyoungpeopleface”andinparticularto“continuetosupportworkthroughthedevelopingpupil’semotionalhealthandwellbeingprogrammeandthecounsellingprovisioninschoolsinordertobuildpupil’sresiliencetodealwithchallengesintheirlivesandimprovetheirreadinesstolearn”;andtoplanandtrackliteracyandnumeracybetterthroughcleareroutcomes.
ThePolicyalsorecognisestheimportanceof“increasingengagementbetweenschoolandparents,familiesandcommunitiestheyserve”,through■ TheExtendedSchoolsProgrammewhichsupportsover400schoolsin
disadvantagedcommunities,will“continuetoensurethatthoseschoolsservingthemostdisadvantagedcommunitiesreceiveadditionalsupportto

Page 64
provideactivitiesoutsideofnormalschoolhoursthatreflectandrespondtotheneedsoftheirpupilsandthelocalcommunity”
■ Fullserviceextendedschools(alreadybeingpilotedin3Belfastschool)–theDepartmentwill“publishastrategyforthefurtherdevelopmentofthisconcept”
■ Healthpromotingschools(200schoolsalreadyengaged)■ Identifyinganddisseminating“goodpracticewithaparticularfocuson
communityuseofschoolstohelpschoolsinbuildingstrongerlinkswiththeirparentsandlocalcommunities”
ExtendedSchoolsTheExtendedSchoolsconceptwasoriginallyintroducedinNorthernIrelandin2006,basedonExtended Schools: schools, families, communities – working togetherdocumentpublishedbytheDepartmentofEducation.ExtendedSchoolsweretobeschoolswhich:
■ viewsworkingwithitspupils,familiesandcommunityasanessentialelementinraisingthestandardofpupilsachievement;
■ buildspartnershipswithneighbouringschools,thefurthereducationsectorandotherstatutory,voluntary,businessandcommunityorganizationstodevelopanddeliverbetterservicesforthecommunityasawholeandforchildrenandyoungpeopleandtheirfamiliesinparticular;
■ helpstostrengthenfamiliesandcommunitiesthroughprovidingopportunitiesforlifelonglearningandpersonaldevelopment;and
■ usesitsaccommodationflexiblyandoutsideofschoolhoursforthegoodoflearnersandthecommunity.
Thedocumenthighlightsalargenumberofpotentialbenefitsforpupils,schools,familiesandcommunitiesfromengagementwithExtendedSchools.
ThecriteriaforreceivingExtendedSchoolsfundingforprimaryandnurseryschoolswasinclusioninaneighbourhoodrenewalarea;beinthe30%lowestrankingwardsorSOAsinrelationtotheEducationdomain;orFreeSchoolmealsentitlementof37%ofhigher.Intermsoffundingschoolsweretoreceiveablockallocation,plusanamountperpupil,basedonaslidingscale,plusanextraallowanceforbeingpartofacluster.SchoolswererequiredtosubmitaproposedExtendedSchoolactionplan.
FollowingETIevaluationsoftheExtendedSchoolsProgrammein2009and2010,whichshowedprogressbutrequiredbetterintegrationwithwhole-schoolimprovementplanningandmoreattentiontoraisingstandardsandtheachievementofspecifichighleveloutcomes,inNovember2010theDepartment
CHAPTER FOUR
The Northern Ireland public policy context that supports the need for change

Page 65
issuedarevisedCircularonExtended Schools – Building on Good Practice.Itstatesthat“theprimaryfunctionofanExtendedSchoolmustbetoraisestandardsthroughtheprovisionoftargetedsupportserviceswhichhaveafocusonlearning,developmentandprogress”and“topromote,supportandsustainthedrivetomaximizelearningandachievementforthosechildrenandyoungpeoplemostinneedorwhoareatriskofloweducationalattainment”.Itstaesthat“Aboveeverythingelse,itmustberememberedthattheactivitiesandservicesprovidedbyExtendedSchoolsmustbefocusedonthecorepurposeofimprovingchildren’slearningandlevelsofeducationalattainment”.
TheCircularstatesthateffectiveExtendedSchoolsprogrammeshave:■ Mappedprovisioninrelationtodataandanalysisofneed;■ Joinedupplanswithotherprovisionsuchastheyouthservice,health,
neighbourhoodrenewal,andcommunityrelations;■ Activelyparticipatedinaclusterworkingtopromotethesharingofprovision
andexpertisebetweenschoolsandpromotedcrosscommunitycollaborationwherepossible;and
■ Engagedwiththevoluntaryandcommunitysectorinthedeliveryofservicesandactivitiesallowingschoolstobuildtheircapacity.
PuttingPupilsFirst:ShapingOurFutureInhisfirstpublicpolicystatement,inSeptember2011,whichwaspublishedasPuttingPupilsFirst:ShapingOurFuture’JohnO’Dowdsetouthisvisionforeducation.Thisincludedthefollowingstatement:
“Infocusingontheneedsofallchildren,wemuststartbylayingtherightfoundationsforlearninginthoseall-importantearlyyears”
ItalsoincludedacommitmenttofinalisingtheEarlyYearsStrategy.Thedraftstrategysetoutto,amongstotherobjectives,“promotingbetterlearningoutcomesforchildrenbytheendoftheFoundationstage,especiallyinlanguageandnumber;andinthechildren’spersonalandsocialdevelopment,emotionalwell-beingandreadinesstolearn”.Thedraftstrategyalsoidentifiesthefollowingissues:■ identifyingbestpractice■ earlyinterventionwherenecessary■ tacklingbarrierstolearning■ developingstronglinkswithfamiliesandcommunities
Thedraftstrategyalsoproposesreviewingthepre-schoolcurriculum,reflectingthecentralityofthecurriculumtoliteracyandnumeracy.Italsoproposessettingoutthemilestonestobeexpectedinachild’sdevelopment.

Page 66
In2012theDepartmentaskedtheEducationandLibraryBoards,inpartnershipwiththeothereducationalmanagementbodiestoproduceanauditofallschoolsandproduceplansforthefutureofthepost-primary(endofMarch2012)andprimary(endofJune2012)sectors.Thisislikelytoresultintheclosureofbothprimaryandpost-primaryschoolsinLisburn,andelsewhere.
LiteracyandNumeracyIn2011theGovernmentpublisheditsstrategytoimproveoutcomesinliteracyandnumeracy,Count,read:succeed.Amongstothermeasurestosupportpupils,teachers,schoolleadersandgovernors,includingthedevelopmentofguidanceforparentsrepre=schoolchildrenthestrategyhighlightstheimportanceof“earlyinterventionwherenecessaryforpupilsofanyage,informedbytheeffectiveuseofdata,toaddresstheneedsofthosewhoarestruggling”,especiallyintheearlyyearsand“ensuringearlyinterventiontoaddressactualorpotentialunderachievement”.TheActionPlanstatesthat“Extendedschoolswillensuretheirextendedschoolsactivitiesorservicesareintegratedintotheirplanningforraisingstandards.
ThestrategysaysthataDirectoratewillbecreatedinDElinkingwithparents,familiesandcommunitiestohelpthemsupporttheirchildren,particularlyinnumeracyandliteracy.
ChildcareTheDepartmentofEducationhasalsocommittedtoproducingaChildcareStrategyfor0-6yearsoldsandhascarriedoutaconsultationprocess.
4.5Area-basedInitiatives
NeighbourhoodRenewalInJune2003,GovernmentlaunchedPeopleandPlace–AstrategyforNeighbourhoodRenewal.Thislongterm(7–10year)strategytargetsthosecommunitiesthroughoutNorthernIrelandsufferingthehighestlevelsofdeprivation.NeighbourhoodRenewalisacrossgovernmentstrategyandaimstobringtogethertheworkofallGovernmentDepartmentsinpartnershipwithlocalpeopletotackledisadvantageanddeprivationinallaspectsofeverydaylife.Neighbourhoodsinthemostdeprived10%ofwardsacrossNorthernIrelandwereidentifiedusingtheNobleMultipleDeprivationMeasure.Followingextensiveconsultation,thisresultedinatotalof36areas,andapopulationofapproximately280,000(onepersonin6inNorthernIreland),beingtargetedforintervention.Theareasinclude:■ 15inBelfast,■ 6inLondonderryand
CHAPTER FOUR
The Northern Ireland public policy context that supports the need for change

Page 67
■ 15inothertownsandcitiesacrossNorthernIreland(includingColinincorporatingPoleglassandTwinbrook).
NeighbourhoodPartnershipshavebeenestablishedineachNeighbourhoodRenewalAreaasavehicleforlocalplanningandimplementation.EachNeighbourhoodPartnershipincludesrepresentativesofkeypolitical,statutory,voluntary,communityandprivatesectorstakeholders.Together,theyhavedevelopedlongtermvisionsandactionplansdesignedtoimprovethequalityoflifeforthoselivinginthearea.
ThekeystrategicobjectiveofNeighbourhoodRenewalis:Totacklethecomplex,multi-dimensionalnatureofdeprivationinanintegratedway,throughthefollowing:■ CommunityRenewal-todevelopconfidentcommunitiesthatareableand
committedtoimprovingthequalityoflifeintheirareas■ EconomicRenewal-todevelopeconomicactivityinthemostdeprived
neighbourhoodsandconnectthemtothewiderurbaneconomy■ SocialRenewal-toimprovesocialconditionsforthepeoplewholiveinthe
mostdeprivedneighbourhoodsthroughbetterco-ordinatedpublicservicesandthecreationofsaferenvironments
■ PhysicalRenewal-tohelpcreateattractive,safe,sustainableenvironmentsinthemostdeprivedneighbourhoods.
NoneofthetargetareasinEarlyInterventionLisburnareconsideredtobeNeighbourhoodRenewalareas,basedonthe2001multipledeprivationdata.
AreasAtRiskTheAreas at RiskPilotProgrammewasestablishedin2006toidentifyandinterveneinareasconsideredatriskofslippingintoaspiralofdecline.TheDepartment,throughtheVoluntaryandCommunityUnit,inconjunctionwitharangeofotherpartners,willhelptosupportthesecommunities,whichperhapsfeelneglectedorisolatedinordertohelpbuildconfidenceandasenseofbelonging.Thetypesofareasthattheprogrammeoperateswithinincludeforexample:■ ‘Interface’areasthatlieoutsideofNeighbourhoodRenewalareas■ Areasineconomicdecline■ Areasat‘riskofdecline’forexample,thoseareasthatwithouttargetedsupport
maymoveintothetop10%asdefinedbyNoble■ Areasatriskof‘descendingintoinstabilityandcrisis’orareasinwhichthere
isadeclineincommunitycohesionwhichthreatenspeaceandstability■ Areaswherethelossoftheserviceprovidedbyorganisationswouldhavea
significantnegativeimpactonthelocalcommunity.

Page 68
ProgrammeObjectives-ThekeyobjectivesoftheProgrammeareto:■ reducethelevel,frequencyandimpactofinterfaceviolencewithinthe
community;■ increaselevelsofeconomicactivitywithinthetargetedareas;■ stabilisetargetedareastothepointthattheareaiseithernolongerconsidered
asan‘areaatrisk’,orthattheriskoftheareaslippingintodeclineisprevented;
■ increasecommunitycohesionandcapacity;■ strengthencommunityinfrastructureinthoseareaswhereitisweak;and■ achieveamoresustainableapproachtocommunityparticipationand
development.
Inordertoensurethatthecommunitiesparticipatinginthisprogrammemeetthecriteriaastrategicpartnershipwasestablished,chairedbytheVoluntaryandCommunityUnit.PermanentpartnersaretheDevelopmentOffices(BRO;RDO;NWDO)andtheNorthernIrelandHousingExecutive,inbothcasesinvolvementisdevolvedtolocaloffices.Otherstatutorybodiesareinvitedtojoinonanadhocbasisasandwhentheirexpertisewouldlendsignificancetotheprogramme.
Potentialareasforinclusionintheprogrammeweresoughtfromthepermanentpartners,whoalsohavetoprovideanevidentialbasisforinclusion.OthersourcesofreferenceincludedlocalpoliticiansincludingCouncillorsandMLA’s.EachnominatedareawasconsideredagainstcriteriabeforebeingsenttoMinisterforconsiderationandapproval.
Onceanareawasincludedalocalvoluntaryorganisationwasnominated(bythepermanentpartners)toactastheleadorganization,chargedwithassistingtocarryoutacommunityaudit.TheDepartmenttakestheleadinappointingaconsultanttocarryouttheauditwhichcanbesupportedthroughprogrammefunds,beforesubmittingaprojectproposal.Theprojectproposalwasconsideredbyallpartnerorganisationsandsubjecttounanimousagreement.
Thepilotprogrammeiscurrentlyoperatinginthefollowingareas:
Phase One: Sydenham(EastBelfast);Taughmonagh(SouthBelfast;Seacourt(Larne);WestPortadown;Rathenraw(Antrim);Dunclug(Ballymena;Limavady;DhuVarren(Portrush);Ballynashallog(Londonderry)
Phase Two: (Announced13November2007byMinisterMargaretRitchie):LowerWhitewell(NorthBelfast);Ballybeen(Dundonald);Gilford(Banbridge);Annadale(SouthBelfast);Scrabo(Newtownards);Killicomaine(Portadown);Alexander/Lisanally(Armagh);AshfieldGardens(Fintona);SeymourHill(Dunmurry);
CHAPTER FOUR
The Northern Ireland public policy context that supports the need for change

Page 69
CraigyhillandAntivlle(Larne);Harryville(Ballymena);Caw/NelsonDrive/LincolnCourts(Derry/Londonderry)
Phase Three: (Announced28January2009byMinisterMargaretRitchie):Beechfield(Donaghadee);Lettershandoney(Derry/Londonderry);Strathfoyle(Derry/Londonderry);FerrisPark(LarneTown);DouryRoad(Ballymena).
NoneoftheEarlyInterventionLisburntargetareashavebeendesignatedasAreasAtRisk.
CommunitySafetyStrategyInJanuary2011thenewDepartmentofJusticeissuedforconsultation“Buildingsafer,SharedandConfidentCommunities–aconsultationonanewcommunitysafetystrategyforNorthernIreland”designedtohelpbuild:■ Safercommunities:withlowerlevelsofcrimeandanti-socialbehaviour,
includingsupportingearlyinterventionforlong-termcrimereduction■ Sharedcommunities:whereeveryone’srightsarerespectedinashared,and
cohesivecommunity■ Confidentcommunities:inwhichpeoplefeelsafeandhaveconfidenceinthe
justiceagenciesthatservethem
Thedraftprinciplesfordeliveringthestrategyincludeboth■ early intervention,“recognizingtheimportanceofearlyinterventionsto
helpaddresstheunderlyingriskfactorsthatcanleadtocrimeandanti-socialbehaviour”;and
■ Evidence-based solutions,“focusingonsolutionsthatpreventandreducecrimewhichareevidence-based,innovativeandresponsivetolocalneeds.
InordertobuildsaferCommunitiesthestrategywould“buildonwhatworksinreducingandpreventingcrime,andworkingreaterpartnershipwithotherExecutiveDepartmentstocreatesafercommunitiesoverthelongtermparticularlyintheareasofhealth,educationandaddressinginequalityandsocialdisadvantage”.
Section5.4outlinestherelationshipbetweencrimeandtheunderlyingcausesandriskfactorsandtherationaleforanearlyinterventionapproach.Itprovidestwoevidence-basedearlyinterventionapproachesincludingthePerryPreschoolProject.
ThedraftstrategycommitstheDepartmentofJusticeto“workwithotherExecutiveDepartmentstoconsiderhowwecansupportearlyinterventionandpromoteitatlocalpartnershiplevelwhereappropriate.Wewillcontinueto

Page 70
supportanddevelopearlystageinterventionprojects,andreviewwhatworksinearlystageprovision.
TheDepartmentofJusticehasdevelopedaStrategicFrameworkforReducingOffendingwhichwillbegoingoutforconsultationbeforetheSummer2012forapprovalbytheendoftheyear.Thisframework,amongstotherthings,highlightstheimportanceoftacklingsocialdeterminantsofcrimesuchasimprovingeducationalattainmentandreducingpoverty,aswellaspreventionanddiversionactivitiesincludingEarlyInterventions,tacklingdrugsandalcoholmisuseandrespondingtomentalhealthissues
4.6ProgrammeforGovernment2011–2016InMarch2012theGovernmentlauncheditsProgrammeforGovernment(PfG),followingaperiodofconsultation.TheProgrammehasfiveaims:■ Growingasustainableeconomyandinvestinginthefuture■ Creatingopportunities,tacklingdisadvantageandimprovinghealthand
wellbeing■ Protectingourpeople,theenvironmentandcreatingsafercommunities■ Buildingastrongandsharedcommunity■ Deliveringhighqualityandefficientpublicservices
TheProgrammecontainsthefollowingrelevantcommitments:■ Introduceandsupportarangeofinitiativesaimedatreducingfuelpoverty
acrossNIincludingpreventiveinterventions■ Provide£40milliontoimprovepathwaystoemployment,tacklesystemicissues
linkedtodeprivationandincreasecommunityservicesthroughtheSocialInvestmentFund(in8regionsofdisadvantageandpoverty)
■ Publishandimplementastrategyforintegratedandaffordablechildcare■ Deliverarangeofmeasurestotacklepovertyandsocialexclusion,throughthe
DeliveringSocialChangedeliveryframework■ UsetheSocialProtectionFundtohelpindividualsandfamiliesfacinghardship
duetothecurrenteconomicdownturn■ FulfillourcommitmentsundertheChildPovertyActtoreducechildpoverty■ Improvecommunitysafetybytacklinganti-socialbehaviour■ Increasetheproportionofyoungpeoplewhoachieveatleast5GCSEsatA*-C
orequivalentincludingGCSEsinMathsandEnglishbythetimetheyleaveschool
■ Improveliteracyandnumeracylevelsamongschoolleavers,withadditionalsupporttargetedatunderachievingpupils
■ Ensurethatatleastoneyearofpre-schooleducationisavailabletoeveryfamilythatwantsit
■ Allocateanincreasingpercentageoftheoverallhealthbudgettopublichealth
CHAPTER FOUR
The Northern Ireland public policy context that supports the need for change

Page 71
■ Invest£7.8millioninprogrammestotackleobesity■ Provide£40milliontoaddressderelictionandpromoteinvestmentinthe
physicalregenerationofdeprivedareasthroughtheSocialInvestmentFund.
TheProgrammedoesnotspecificallyincludeacommitmenttoearlyinterventionortoevidence-basedapproaches.InFebruary2012theChildren’sCommissioner’s(NICCY)responsetotheDraftProgrammeforGovernmentrecommendedincludingaspecificcommitmentinthePfG“toearlyinterventionandpreventionforchildrenandyoungpeople,linkingfundingandjointworkingacrossdepartments”.
SocialInvestmentFundTheExecutiveagreedon22March2011totheestablishmentoftheSocialInvestmentFund(SIF)andmoniestotaling£80millionoverafouryearperiodweresubsequentlyallocatedintheBudget.thePfG,highlightedabove,includesarenewedcommitmenttotheFund.
ThehighlevelaimoftheSocialInvestmentFundistoreducepoverty,unemploymentandphysicaldeteriorationinareasthroughareabasedinterventionsofsignificantscalewhichwillbedeliveredinpartnershipwithcommunities.TheFundwilltoencouragecommunities,statutoryagencies,businessanddepartmentstoworktogetherinaco-ordinatedway,reducingduplication,sharingbestpracticeandenhancingexistingprovisionforthebenefitsofthosecommunitiesmostinneed.
TheSIF’sstrategicobjectivesaretosupportcommunitiesto:■ buildPathwaystoEmployment;■ tacklethesystemicissueslinkedtodeprivation;■ increasecommunityservices;and■ addressdereliction.
A“prediscussion”paperwaspublishedinMarch2011andoutlinesthehighlevelstrategicconcept,objectivesandoverallmethodologyoftheFund.AconsultationdocumentwaspublishedtoseekviewsontheproposedoperationoftheSocialInvestmentFund(SIF),includingoptionsforapplyingtotheFund,application/assessmentcriteria,howtheFundshouldbemanagedandthestructurestosupportitsdelivery.TheConsultationontheproposedoperationoftheSocialInvestmentFund(SIF)closedonthe23December2011.
SocialProtectionFundTheNIExecutivehasalsoestablishedaSocialProtectionFund(SPF)to“assistthosemostinneedinthewidercommunity”.Thisyear(2011/12)theyagreed

Page 72
toprioritisefuelpovertythroughthefund,andcommittedthefull£20millionbudgettoawinterfuelpovertypaymentschemethroughtheDepartmentforSocialDevelopmentandtheDepartmentofHealth,SocialServicesandPublicSafety(DHSSPS)undertheFinancialAssistanceAct(NorthernIreland)2009.Throughthescheme,aone-offpaymentof£75hasbeenmadetopersonsinreceiptofincome-basedmeans-testedbenefits,includingincomesupport,income-relatedemploymentandsupportallowanceandincome-basedjobseeker’sallowance.PensioncreditrecipientsandpeopleinreceiptofcancertreatmentinlinewithcriteriadeterminedbyDHSSPSarereceivingone-offpaymentsof£100.Althoughfundingfortheprogrammewassecuredforonlyonefinancialyear,theExecutivearecommittedtosecuringmoneysforfutureSPFprogrammesduringtheremainderofthecurrentBudgetperiod.
4.7ConclusionsinrelationtothePublicPolicyContextThepublicpolicycontextpresentsaconsistentsenseoftransitiontowardsanearlyinterventionandevidence-basedapproachtoaddressingmanyofthedifficultiesfacingchildren,youngpeopleandfamiliesinNorthernIreland.Thereisaclearunderstandingoftheimplicationsofdeprivationandwiderinequalitiesfortheoutcomesforchildrenandyoungpeopleandastatedcommitmenttotacklingtheseinequalities.Thepolicycontextsuggeststheprinciplesthatshoulddrivethisearlyinterventionapproachareasfollows:
Interventionsshould:■ focusontacklingrootcausesandnotjusttreatingsymptoms;■ takeplaceintheearlyyearsofachild’slife,where,theevidencesuggests,
manyproblemsinlaterlifearecreatedandatwhichstagebraindevelopmentismoulded,and/orattheearlieststageofdifficulty,whenachildmaybevulnerabletopoordevelopmentaloutcomes;
■ adoptawholechildapproach,whichgivesrecognitiontothecomplexnatureofourchildren’sandyoungpeople’slives;
■ adoptawholefamilyapproachwhichconcentratesonallmembersofthefamily-children,youngpeople,andtheirparentsandsupportingfamilylife;
■ adoptawholesocietyapproachtoearlyinterventionthroughanetworkofintegratedsupportsandservicesandmulti-agencyworking;
■ buildonthestrengthsandresilienceofchildren,youngpeopleandfamiliesandnotonlyrespondtotheirneeds;
■ beevidence-basedthroughimplementingprogrammeswhichhavebeensubjecttorigorousevaluation(esp.RCTs).Innovationsthathavenotbeenrobustlyevaluatedbeforeshouldberigorouslyevaluated;
■ befocusedonachievingclearmeasurableoutcomes;■ Beimplementedwithfidelitybyskilledandtrainedstaff;■ be“owned”bythecommunitythroughacommunitydevelopmentapproach;
CHAPTER FOUR
The Northern Ireland public policy context that supports the need for change

Page 73
■ beaccessibleandpromoteparticipationandinclusion;■ besustainedandlong-term;■ combine
• Level1support:universal(allchildren);• Level2support:targetcommunitiesandgroups/categoriesoffamilies
whicharemostvulnerableduetodeprivation,etc.;and• Level3support:non-stigmatisingtargetedearlyinterventiononparticular
familiesassessedtobemostatrisk.
Thepolicycontextraisesotherimportantissuestobeconsidered:
IdentificationofareasofdeprivationTherecognitionoftheimportanceofdeprivationindeterminingoutcomesforchildrenandyoungpeoplehasresultedinthedevelopmentofthevaluableMultipleDeprivationMeasure(MDM)torankwardsandSuperOutputAreas.Thishasbeenusedbyarangeofinitiativestotargetthose“mostinneed”.NeighbourhoodRenewalhasfocusedawiderangeofservicesandresourcesinthe10%ofmostdeprivedcommunities(basedonthe2001MDM.Thisapproachhassignificantshortcomings,including:
■ ThemajorityofpoorfamiliesliveoutsideNeighbourhoodRenewalareas■ ManybetterofffamiliesliveinthemostdisadvantagedSOAs■ Resourcesavailabletocommunitieswhichrankjustoutsidethe200110%
rankinghavebeendivertedtowardsNeighbourhoodRenewalAreas■ Deprivationchangesovertime.Ifcalculatednow,OldWarrenwouldbea
NeighbourhoodRenewalArea■ MDMincludesproximitytoahospital,inthiscase,LaganValleyHospital
whichisveryclosetoTonagh/OldWarren/Knockmore,butisnolongerafullacutehospital
■ AveragingDeprivationthroughanaggregatemeasuresuchasMDMignorestheimportanceofindicatorswhichmayshowaverydifferentpicture.Forexample,theverylowlevelofeducationalattainmentinProtestantworkingclassareasinLisburn(andotherpartsofNorthernIreland)isverydisturbing,requiringurgentaction,butismaskedbyafocusedonMDM.
ResourcingandImplementationManyofthestrategiesaboveexpressagoodunderstandingoftheissuestobeaddressedverypositiveaimsandprinciples.However,thelong-termresourcingandimplementationhasbeenpoor.Despitethesepositivesoundingstrategydocuments,littlehaschangedfordisadvantagedfamiliesinthetargetareasofLisburncharacterisedbypovertyand,evenmoreso,byeducationalunderachievement.Manyevidence-basedinitiativeshavebeenintroducedina

Page 74
half-heartedwaywithinadequateand/orshort-termresources.Thereneedstobeaclearcommitmenttoeffectivelong-termresourcingofrobustlyevidence-basedprogrammes,otherwisetheinequalitieswillcontinuetowiden.
Theeconomicevidencethatearlyinterventionprogrammescan,ratherthancostmoney,overthelonger-term,saveconsiderableamountsofmoneyforthestate,butthenatureofshort-termfundingdecisionsmeansthatthecriteriausedtomakethesedecisionsdonottakeintoaccounttheselong-termsavings.
PartnershipworkingThemantraofcross-sectoralandintegratedpartnershipworking,basedonawholechildmodel,cannotbedeliveredthroughtraditionalsilomodelsandstructures.EarlyInterventionoftenmeansinvestmentsbyoneDepartmentoragencyinordertoproducedesiredoutcomesforadifferentDepartmentoragency.
Hopefully,thenewChildrenandYoungPeople’sStrategicPartnershipandthesub-regionalOutcomeandLocalityGroupspresenttheopportunitytomakeaseriouscommitmenttopartnershipworkinganddevelopingtrulyintegratedservices.
Thereisstillabiggapbetweentheworkofpublichealthandsocialcareagenciesandworkinschools.TheExtendedSchoolsinitiativehasmadeasmallcontributiontowardsmoreintegration,butthisisonlyattheearlystages.Forearlyinterventiontobesuccessfulthereneedstoseamlessworkingbetweenschools(whichnearlyallchildrenattend),community-basedinitiatives,andthehealthandsocialcaresector.
CHAPTER FOUR
The Northern Ireland public policy context that supports the need for change

Page 75
5.1OutcomesTheprevioussectionshave:■ analysedtheneedsofthetargetcommunitiesinLisburn,asidentifiedbothby
deskresearchandthroughtheconsultationswithcommunityrepresentatives,schoolsandthosefromtherelevantprofessionalagenciesworkingintheareas;
■ examinedtheconcepts,andrationale,aroundearlyintervention;and■ summarisedtherelevantpublicpolicycontext.
These,together,suggestthatthespecificoutcomeswhichtheEarlyInterventionLisburnInitiativeshouldtarget,tohaveanimpactontheGovernment’shighleveloutcomesforchildrenofbeing:Healthy;Enjoying,learningandachieving;Livinginsafetyandwithstability;Experiencingeconomicandenvironmentalwellbeing;Contributingpositivelytocommunityandsociety;andLivinginasocietywhichrespectstheirrights,shouldbeasfollows:
■ Reducednumberofteenagepregnancies■ Reducedlevelofsmokingduringpregnancy■ Improvedparentingskillsandconfidence■ Improvedparent-childattachmentfor0-2yearolds■ Improvedschoolreadinessamongst3&4yearolds■ Improvedliteracyandnumeracyinchildrenaged4-11■ Improvedsocialandemotionalskillsandresilienceof4-11yearolds■ Improvedschoolattendance■ Improvededucationalaspirationsandattainmentonleavingschool■ Reducedbehavioural/conductproblems■ Reducedsmoking,alcoholanddrugconsumptionamongstyoungpeople■ Reducedcrimeandanti-socialbehaviouramongstyoungpeople■ Reducedchildhoodandteenageobesity■ Increasedengagementoffathersintheirchildren’slearning
Thereisbroadagreementthattheseareimportantoutcomestobeaddressedtoimprovethelivesofthepeopleofthetargetareas.However,thekeyquestionishowbesttoachievetheseoutcomes.Thisinturnsuggestsanumberofotherquestions,whichneedtobeaddressed,asfollows:
■ Whatimpactdocurrentprogrammesandservicesmakeontheseoutcomesandhowcouldtheymakeagreaterimpact?
■ Whatarethemosteffectiveinterventionstoachievetheseoutcomes?andhowrobustistheevidenceforthepotentialimpactoftheinterventions?
CHAPTER FIVE
Theory of change

Page 76
■ Whatarethemostcost-effectiveinterventionsi.e.whichinterventionswillcreatethegreatestlong-termsavingstothepublicpurse?
■ Whichinterventionsshouldbeuniversal,targetedonparticularcommunities/populations,ortargetedonparticularfamilies?
■ Whereshouldinterventionstakeplace:inthehome,communityvenuesand/orschools?
■ Howcanprogressagainsttheagreedoutcomesbemeasured?
■ Whatresourcesarerequiredtoimplementtheevidence-basedprogrammesthatwillhaveasignificantimpactontheagreedoutcomes?
5.2AligningexistingprogrammesandservicesAlthoughLisburnisunderservedintermsofsupportforchildrenandfamilies,asitdoesnotreceiveregenerationfundingsuchasNeighbourhoodRenewal,despitehavingareaswithinthe10%mostdeprivedinthe2010MDMfiguresandconsiderablyworseeducationaloutcomesthanmanyotherareaswithintheworst10%,therearesomeexistingservicesandprogrammesthatoperateinoneormoreofthetargetareas,deliveredbydifferentstatutoryandvoluntaryagencies.Asafirststepitwillbeimportantto:■ increasetheawarenessof,andfocuson,preventionandearlyintervention;■ mapandimprovetheco-ordinationandintegrationofexistingservicesfor
childrenandfamilies,towardsachievingtheagreedoutcomes;■ supportexistingcommunityservicesforchildren,youngpeopleandfamilies
intheLisburnareabydevelopingacommonoutcomesframework(whichwillenableimpacttobemeasured);
■ helpprogrammes/servicestosetandmeasurespecificoutcomes;learnfromtheinternationalliterature;andmanualiseprogrammes/services;
■ developasharedfocusonqualityachievedthroughjointreflectivepractice,trainingandpeerlearning,wherebydifferentorganisationscanlearnfromoneanother;and
■ encourageandsupportexistingorganisationstoworktogethertotransformtheculturewithintheCityofLisburn,especiallywithinareasofdeprivation,toemphasiseaspirationandachievement(particularlyinrelationtoeducation).Thiscanbedonethroughlocalmedia,doortodoorconsultations,celebratinglocalchampionsetc.
5.3WhatWorks?Therehasbeenextensiveworkcarriedoutaroundtheworldtoevaluatewhichofthemanyearlyinterventionsocialprogrammesactuallyworki.e.havea
CHAPTER FIVE
Theory of change

Page 77
significantpositiveimpactonthedesiredoutcomes.Thestrongestevidenceisfromevaluations,carriedoutbyexperiencedindependentevaluators,whichinvolvelargenumbersofchildren,familiesand/oryoungpeoplereceivingamanualised(standardised)programme;wherethereisaRandomControlTrial(RCT)witharandomisedcontrolgroupnotreceivingtheprogrammewhichisthereforeverysimilartothegroupreceivingtheprogramme;andtestingiscarriedoutbothbeforeandaftertheintervention,usingwell-establishedmeasurementinstruments.
Therearevariousorganisationsinternationallywhichspecialiseinanalysingthequalityandrobustnessofevaluationinformationfromsocialprogrammesaroundtheworldinordertohighlightprogrammeswhichare“proven”or“promising”,includingBlueprintsandtheWhat Works Clearing House.WorkisnowunderwaytodevelopanequivalentoftheBlueprintsdatabaseforEurope.DartingtonSocialResearchUnitinEnglandhaveworkedwithSteveAosfromWashingtonStateUSAtocreateacostbenefitmodelforEnglandwhichwillformpartofasoontobelaunched“BlueprintsforEurope”(seehttp://www.dartington.org.uk/investinginchildren).GrahamAllenMP,inhisreports,hashighlightedtheprogrammeswhichhehasbeenadvisedbyUKexpertshavethestrongestevidencebase.
Theimpactofsomeofthebestprogrammeshasalsobeenevaluatedintermsofthelong-termcostsandbenefits.Thesehaveshownthatinvestmentintherightevidence-basedearlyinterventionprogrammescanproduceverysubstantiallonger-termsavingsinissueslike:welfarebenefits,medicalandmentalhealthservices,prisonandotherjusticeservices,etc.ThismeansthatfortheGovernmentinNorthernIrelandtoinvestintherecommendedprogrammesinLisburnislikelytoresultinlong-termsavingsmanytimestheamountoftheinvestmentthatisrequirednow.
NobellaureateeconomistJimHeckmanhasanalysedalargenumberofcost-effectivenessstudiesandshownthattheyoungertheageofchildrenengagedintheprogrammesthemoreeffectivetheyareinreducinginequalitiesandmorecost-effectivetheprogrammesareingeneratinglong-termsavings.ThissuggeststhatthebedrockoftheEarlyInterventionLisburnprogrammeshouldbefamilyinterventionsfrompregnancytoage3.Hissubsequentwork,however,alsoshowsthattheseinterventionsneedtobesustainedasthechildrengetolder,particularlyduringtheirprimaryschoolyears,topreventinequalitiesbeingstrengthenedagain.Thisindicatestheimportanceofprogrammesthataddresstheneedsof3-11yearoldsandthosewhomakethedifficulttransitiontopost-primaryschool,aswellasthecrucialprogrammesforchildrenaged0-3andtheirparents.

Page 78
5.3ProvenEarlyInterventionProgrammesWhatworksinmeetingthecomplexneedsoffamiliesisarangeofapproaches.Inordertogiveanindicativelistofpotentialprogrammes,thefollowingaresomeofthemostrobustlyevaluated“proven”programmes(i.e.havebeensubjecttoatleasttworobustRCTevaluationswhichproducedstatisticallysignificantresults)mostofwhichhavebeenshowntoresultinsubstantiallatersavings,inrelationtoeachoftheimportantoutcomesforEarlyInterventionLisburn,highlightedabove:
Reducednumberofteenagepregnancies■ FamilyNursePartnership*(pregnancy–age2)–deliveredbyatrained
healthvisitororothernursetotargetedparentsinthehome–whichhasbeenshowntoreduceanddelaysubsequentbirths–ItiscurrentlybeingdeliveredinNorthernIrelandbytheWesternHealth&SocialCareTrustinDerry/Londonderryand,althoughPHAidentifiedLisburnasapriorityareaintheSouthEast,BelfastandtheSouthernTrustareashavebeenchosenfornewFamilyNursePartnershipprogrammes,ratherthanLisburn.ItisalsobeingdeliveredinScotlandinEdinburghandTaysideandinEnglandbyNottinghamlocalauthority.ThereiscurrentlyamajorRCTtrialbeingcarriedoutonFamily
0-3 4-5pre-school
School Post-school
Preschool programs
Schooling
Programmes targeted towards the earliest years
Age
Job training
Rat
e of
Ret
urn
to
Inve
stm
ent
in H
um
an C
apit
al
* KnownasNurseFamilyPartnershipsintheUSAwheretheprogrammeoriginated
CHAPTER FIVE
Theory of change
The Hockman Curve

Page 79
NursePartnershipsinGB.Previousevaluationsshowthattheparentandchildprogrammescombinedaremoreeffectthaneitherdeliveredontheirown.
Reducedlevelofsmoking,drinkinganddruguseduringpregnancy■ FamilyNursePartnership(pregnancy–age2)–seeabove
Improvedparentingskillsandconfidence■ IncredibleYears(aged0-9)ParentsProgramme:Basic(12-14weeks);Advanced
(10-12weeks);andSCHOOLandDinaDinasaur(anhourtwiceaweek(ortwohoursonceaweekfor20-22weeks)forchildrenwithconductproblems)–Targetedonidentifiedfamilies–ItiscurrentlybeingdeliveredintheRepublicofIreland(Youngballymun/Archways)andvariousaspectsofIncredibleYearsisbeingdeliveredinvariousplacesinNorthernIreland(IFIarefundingacross-communityinitiativeintheSEELBareatodeliverIncredibleYearsin16schools,includinginOldWarrenPrimarySchool)
■ Parent-ChildInteractionTherapy(age2-7yearolds)–Targetedonpre-schoolchildrenwithevidenceofaconductdisorderandtheirparents
Improvedparent-childattachmentfor0-2yearolds■ FamilyNursePartnership(pregnancy–age2)–seeabove
■ IncredibleYears(aged0-12)–seeabove
Improvedliteracyandnumeracyinchildrenaged4-11■ DoodleDen–aliteracyprogrammefor5/6yearolds,withadditionalparent
andfamilysessions.Itisdeliveredfor90minutesthreetimesaweekafterschool(inschoolandcommunityvenues)byaspeciallytrainedteacherandyouthworkertoagroupof15children.TheRCTofthepilotinWestTallaghtDublinhasdemonstrateditsimpact.
■ SuccessforAll,includingCuriosityCorner(age3-11yearolds)–Universal-school-based-InstituteofEffectiveEducationUniversityofYork.Therearemodulesforeachkeystagefromfoundationtokeystage3
■ TimetoRead(age8–10yearolds)–developedinNIbyBusinessintheCommunity,usingvolunteersfromcompaniestoreadfor30minuteseachweekwithchildreninaprimaryschoolsetting.Arandomcontroltrialevaluationhasindicateditseffectiveness,esp.forthosechildrenwhosereadingdevelopmentisonlyslightlydelayed.ReadingRecoveryislikelytobemoreeffectiveforthelowest20%ofreaders.TimetoReadisfreetotheschools.ThekeyissueisBITCbeingabletoidentifyappropriatevolunteerstodeliverthe

Page 80
programme.ItisalreadybeingdeliveredinOldWarrenandKillowenPrimarySchools
Improvedsocialandemotionalskills,conductandresilienceof4-11yearolds■ PATHS(4/5-11yearolds)–Universal-school-based–Barnardo’sinNorthern
Ireland(aroundCraigavon)andlocalauthoritiesinBirmingham,NorfolkandManchester
■ IncredibleYearsforchildren,parents(seeabove)andteachers(6daytrainingworkshoponclassroombehaviourmanagement)–seeaboveandAppendixfordetails
Reducedbehavioural/conductproblems■ IncredibleYears(aged0-12)–childprogramme(incDinaDinosaur)–universal
preventionprogrammeandtreatmentprogrammeforsmallgroupsofparticularlyatriskchildren–seeaboveandAppendixfordetails
■ TripleP(aged0-16)–Bothuniversalandtargeted(4levels)–onlyprovenifthewholeprogrammeatthe4levelsisdelivered(onlya“promising”BlueprintsProgramme).IsbeingpilotedinLongfordWestMeathParentingPartnershipintheRepublicofIrelandandEngland
Improvedschoolattendance■ BigBrothers/BigSisters(6-18yearolds)–Targeted-mentoringdeliveredby
carefullyselectedandtrainedvolunteers–beingdeliveredinvariouspartsoftheRepublicofIrelandthroughForoige.
Reducedsmoking,alcoholanddrugconsumptionamongstyoungpeople■ BigBrothers/BigSisters(6-18yearolds)–seeabove
■ LifeSkillsTraining(9-15yearolds)–Universal–3-yearschool-basedprogramme(15sessionsinyear1;10inyear2;and5inyear3)–currentlybeingdeliveredinNottingham.Barnardo’shaveBigLotteryfundingtodeliverLSTintheUK,includingNorthernIreland
■ FunctionalFamilyTherapy(10-18yearolds)–Targeted-family-based–deliveredbyaspeciallytrainedqualifiedsocialworker-currentlybeingdeliveredbyArchwaysinDublinandbeingtrialedinBrighton.ActionforChildrenareplanningtodeliveritinNorthernIrelandwithBigLotteryfunding
■ Nurse-FamilyPartnerships–seeabove
CHAPTER FIVE
Theory of change

Page 81
Reducedcrimeandanti-socialbehaviouramongstyoungpeople■ Nurse-FamilyPartnerships–seeabove
■ FunctionalFamilyTherapy(10-18yearolds)–seeabove
■ MultisystemicTherapy–Targetedonatriskyoungpeople(aged12-17)-familyandcommunity-based.ExternhavebeenpilotingMSTinNorthernIrelandandareplanningtoexpandtheprogrammewithfundingfromtheBigLottery
Increasedengagementoffatherswiththeirchild’slearningNo“proven”programmes.TheUSprogrammeFather’sReadingEveryDay(FRED)looksasifithaspotentialandengagesLibrariesinearlyintervention.AllagreedprogrammesshouldfollowtheFatherhoodInstituteguidelinesonengagingfathers.
Improvededucationalattainmentonleavingschool■ BigBrothers/BigSisters(6-18yearolds)–seeabove
Reducedchildhoodandteenageobesity■ Therehavebeenfewstudiesthathavedemonstratedeffectivenessin
preventingobesity.Effortstotackleobesityinschoolhavehadpoorresults.Thefocusofcurrentresearchisontheante-natal,post-natalandpre-schoolperiods.SureStartseemstohaveanimpactonchildren’sBMIbutnotonthelevelofobesity.PHAareinvolvedinarangeofprogrammestotryandimprovephysicalfitnessandreduceobesity
OtherProgrammesThereareotherprogrammeswhichaddresstheoutcomeshighlightedabove,buttheylacktherobustevidence-basetobeconfidentthatimplementingtheseotherprogrammesinLisburnwouldhaveasignificantimpactontheagreedoutcomes.
OtherpopularprogrammesarealreadybeingdeliveredinLisburn,includingtheNewParentingProgramme,ParentInfantProgramme(PIP)andMellowParents/Fathers/Bumps.TherearealsoanumberofyouthworkprogrammesinthetargetareasofLisburn.TheEarlyInterventionapproachdoesnotmeanthatthese“unproven”programmesshouldimmediatelybeabandoned,unlesstherearealternative“proven”programmesthatcanreplacethem,butthat,wheretheyarealreadymanualised,deliveredtoasignificantnumberofchildren/familiesandfocusedonspecificoutcomes,theyshouldberobustlyevaluatedusinganRCTmethodologyassoonaspossible.Othercurrentprogrammeswhicharenotyetatthisstageofdevelopment,suchasyouthwork,shouldbefurtherdeveloped,usingtherobustinternationalresearchevidence,tocreatemoreclearlydesired

Page 82
outcomes,andbemanualisedandevaluated.ThecurrentpartnershipwiththeUniversityofUlstershouldassistinthisprocess.
SureStartSureStart,whichisakeyGovernmentearlyinterventionindisadvantagedcommunitiesandwhichcurrentlyoperatesinOldWarrenandHillhall,hasnotyetbeendiscussedinanydetailinthisreport.
SureStartisagovernmentledinitiativeaimedatgivingeverychildthebestpossiblestartinlifeandwhichoffersabroadrangeofservicesfocusingonFamilyHealth,EarlyYearsCareandEducationandImprovedWellBeingProgrammestochildrenaged4andunder.TheSureStartProgrammeissupportedbyanumberofkeyprinciples:■ Toco-ordinate,streamlineandaddvaluetoexistingservicesforyoung
childrenandtheirfamiliesinlocalcommunities■ Toinvolveparents■ Toavoidstigma■ Toensurelastingsupport■ Tobesensitivetolocalfamiliesneeds■ Topromotetheparticipationofalllocalfamilies
Servicesprovidedbyprojectsmust:■ Addvaluetoexisting/plannedservices■ Bebaseduponevidenceofwhatinterventionsaresuccessful■ Imaginativelyrespondtolocalneed■ Beinformedbystrategicdirection
SureStartworkisfocusedon6highleveloutcomestoensurechildrenare:■ BeingHealthy■ EnjoyingLearningandAchieving■ LivinginSafetyandwithStability■ LivinginaSocietywhichRespectstheirRights■ ExperiencingEconomicandEnvironmentalWell-being■ ContributingPositivelytoCommunityandSociety
ThecoreservicesofSureStartare:■ OutreachandHomeVisitingServices-tomakecontactasearlyaspossiblein
thechild’slifeanddrawfamiliesintousingotherservices■ FamilySupportandParentingInformation-bothgroupandhomebased■ GoodQualityPlay,LearningandChildCareExperiences-forchildren,both
groupandhomebased■ PrimaryandCommunityHealthcareandAdvice
CHAPTER FIVE
Theory of change

Page 83
■ SupportforChildrenwithSpecialNeeds-throughsignpostingtomorespecialisedserviceswherenecessary
Examplesofspecificservicesofferedthroughprojectsinclude:■ Homebasedantenatalcare■ BreastfeedingSupportGroups■ Advice,supportandinformationonhealthrelatedtopics■ EarlyLanguageDevelopmentProgrammes■ Playdevelopmentforallagesandstages■ Ageappropriatephysicaldevelopmentopportunities■ Highqualitycrèchesessions■ Promotionofthecreativearts■ Supportforsmoothtransitionsbetweenpreschoolandschool
SureStartservicesarecurrentlyavailableinatleastthetop20percentwardareasofdisadvantageinNorthernIreland,andthetop20percentSuperOutputareas,asdefinedbytheNorthernIrelandMultipleDeprivationMeasure2010.Therearenow34SureStartprogrammesacrossNorthernIrelandwhichcoverawidegeographicspreadandhaveagoodurbanandruralmix.Over30,000childrenagedunderfouryearsandtheirfamilieshaveaccesstotheservicesprovidedthroughtheprogramme.Outofthe32programmesoperatinghere,approximatelyone-thirdarebasedinruralsettings.
SureStartprogrammeshavebeendesignedspecificallytoreflectandrespondtolocalneeds.Forthatreason,eachSureStartprogrammeisuniqueintermsoftheservicesitprovidesandthemannerinwhichitprovidesthem.However,allSureStartprojectsnowprovideaDevelopmentalProgrammefortwotothreeyearoldswhichaimstoenhancesocialandemotionaldevelopment,buildoncommunicationandlanguageskillsandencourageimaginationthroughplay.Thiscanhelpsomechildrentobepreparedforstartingpre-schooleducation.TheProgrammeisnotintendedtobeauniversalserviceforallchildrenintheyearbeforestartingpre-schooleducationbutisaimedprimarilyatthosechildrenwhoarelikelytobenefitmostfromthissupport.
ThereisamajornationalevaluationoftheSureStartprogrammeinEngland,whichshouldproduceaclearerunderstandingoftheimpactoftheprogrammebytheendof2012.InterimevaluationshaveshownthatchildreninSurestartareasarelikelytohavebetterphysicalhealththantheequivalentnon-SureStartareas.Mothersalsoreportedprovidingamorecognitivelystimulatingandlesschaotichomelearningenvironmentfortheirchildren;experiencinggreaterlifesatisfaction;andengaginginlessharshdiscipline.Howeverthemothersalso

Page 84
reportedmoredepressivesymptomsandlessengagementwiththeirchild’sschool(althoughitwaslowoverallalready).
TheSureStartevaluator,onthebasisoftheinitialevidencehasrecommended,intheGrahamAllen2011EarlyInterventionreport(Allen2011),thatSureStart,deliveredtoahighstandard,shouldbeakeycomponentinanyearlyinterventioninitiative,althoughnotsufficientinitself.
ThereisalsoanimportantquestionastothenumberoffamiliesthatanyparticularSureStartschemewillbeabletosupportinlightofthefundingmadeavailable.Theevidence,highlightedabove,isthatthemajorityofchildreninthetargetareasofLisburnarelikelytosignificantlyunderachieveeducationally,withveryimportantimplicationsforotheraspectsoftheirlives.CurrentschemesinOldWarrenandHillhall(currentlypartoftheColinNeighbourhoodinitiative)canonlysupportaverysmallnumberoffamilies.IfSureStartistomakeasignificantimpactinthetargetareas,itneedstoreachamuchlargernumberoffamilieswithhighqualityservicesdeliveredbywelltrainedstaff.OnthecurrentDENIcriteria,TonaghshouldalsohaveaSureStartscheme.Fromthestatisticalevidence,oneducationalgrounds,thereisastrongcaseforalsohavingaSureStartschemeinHildenandLaganValley.
5.4CriteriatouseinselectingearlyinterventionprogrammestodeliverHavingsuggestedalong-listofevidence-basedprogrammeswhichwouldhaveanimpactonthedesiredoutcomes,itisimportanttobeclearaboutthecriteriathatwillbeusedtoselectasmallernumberofprogrammesfromthislist.Itisrecommendedthattheseshort-listingcriteriaareasfollows:
NumberofoutcomeseachoftheprogrammesislikelytohaveanimpactonEachoftheevidence-basedinterventionshighlightedabovehaveanimpactonadifferentnumberofthedesiredoutcomes.Allthingsbeingequal,priorityshouldthereforebegiventoprogrammesthathaveapositiveimpactonthelargestnumberofdesiredoutcomes.Thenumberofoutcomesthatwouldbeaffectedbythelong-listedprogrammesareasfollows:
ThereisevidencethataFamilyNursePartnershipprogrammecouldhaveapositiveimpactonatleastfiveofthedesiredoutcomes.
IncredibleYearsprogrammeforparents,childrenandteachersislikelytohaveanimpactonatleastfourofthedesiredoutcomes.
CHAPTER FIVE
Theory of change

Page 85
BigBrothers/BigSistersislikelytohaveanimpactonatleastthreeofthedesiredoutcomes,includingschoolattendanceandeducationalattainmentwhichareclearlycriticaloutcomesinLisburn.
FunctionalFamilyTherapyislikelytohaveanimpactonatleasttwoofthedesiredoutcomes
Thefollowingprogrammesarelikelytohaveanimpactonatleastoneoftheoutcomesabove:■ PATHS■ Parent-ChildInteractionTherapy■ SuccessforAllincludingcuriositycorner■ TripleP■ LifeSkillsTraining■ MultisystemicTherapy■ DoodleDen■ TimetoRead
AgegrouptobeaddressedTheevidenceisthattheearliertheageoftherecipientsofaprogrammethemoreeffectiveandcost-effectiveitislikelytobe.However,itisalsoimportantthatprogrammestoenhancethelifechancesofdisadvantagedchildrenandyoungpeoplecontinueaftertheearlyyearsprogrammesthroughprimaryschoolandthetransitiontosecondaryschool.Thetargetagegroupsofeachoftheprogrammesareasfollows:
Frombirth:■ FamilyNursePartnership-pregnancy–age2(targeted–home-based)■ IncredibleYears-age0-12(community-basedinc.schools)■ TripleP-age0-16
Fromage2/3:■ SuccessforAll,includingCuriosityCorner-age3-11(universalinprimary)■ Parent-ChildInteractionTherapy-age2-7(targetedhome-based)
Fromage4-6■ PATHS–age4/5-11(universalinprimaryschools)■ BigBrothers/BigSisters–age6-18(targeted–community-based)■ DoodleDen–age5/6(targetedinprimaryschools)

Page 86
Fromage8-12■ TimetoRead–aged8-10■ LifeSkillsTrainingage9-15(universalinprimaryandpost-primaryschools)■ StrengtheningFamiliesage10-14(targetedhome-based)■ FunctionalFamilyTherapy–age10-18(targetedhome-based)■ MultisystemicTherapy-age12-17(targetedhome-based)
TheappropriatelocationofprogrammesEachoftheprogrammesaredesignedtobedeliveredindifferenttypesoflocations.Theabilityofonetypeofvenuetotakeonmorethanonenewprogrammeatatimewouldsuggestthatprogrammesshouldcoverarangeofdifferentvenues.Thesepotentialtypesofvenuesarehighlightedbelow:
Universalinprimaryschools■ PATHS(4/5-11yearolds)■ SuccessforAll,includingcuriositycorner(3-11yearolds)■ LifeSkillsTraining(9-15yearolds)
Targetedinprimaryschool■ TimetoRead(6-8yearolds)■ DoodleDen(5/6yearolds)
Universalinpost-primarySchools■ LifeSkillsTraining(9-15yearolds)
Targeted–basedinacommunityvenue(includingschoolsandlibraries)■ IncredibleYears(0-12)■ BigBrothers/BigSisters(6-18yearolds)
Targeted–home-based■ FamilyNursePartnership(pregnancy–2yearolds)■ Parent-ChildInteractionTherapy(2-7yearolds)■ FunctionalFamilyTherapy(10-18yearolds)■ MultisystemicTherapy(12-17yearolds)
CapacitytodeliverThechoiceofthemostappropriateinterventionsandthetimingoftheirintroductionwillalsodependonthelocalcapacitytointroduceanddelivertheprogrammewithfidelity.AprogrammedevelopedintheUSA,forexample,thathasneverbeenusedintheUKorIrelandislikelytoneedtobeadaptedinawaythatisappropriateforthelocallanguageandcultureandtheadaptationwillneedtobeapprovedbytheprogrammelicense-holder(s)oftheprogramme.Onthepositive
CHAPTER FIVE
Theory of change

Page 87
sidethereisarapidlyincreasingskillandexperienceindeliveringarangeofevidence-basedprogrammesintheUKandIreland,includingNorthernIreland.
ProgrammesalreadybeingdeliveredinNorthernIreland■ IncredibleYears■ FamilyNursePartnerships■ PATHS■ Multi-systemicTherapy
ProgrammesalreadyplannedforNorthernIreland■ LifeSkillsTraining
ProgrammesalreadybeingdeliveredintheUKorIreland(inadditiontothosedeliveredinNorthernIreland,whichareallalsobeingdeliveredinUKand/orIreland)■ BigBrothers/BigSisters■ SuccessforAll■ FunctionalFamilyTherapy■ TripleP
Otherprogrammes■ Parent-ChildInteractionTherapy■ MultisystemicTherapy
Short-listedevidence-basedprogrammesTheaboveselectioncriteriawouldsuggestthatthemosteffectiveandpracticallydeliverableinterventionstoimpactonthedesiredoutcomesabovewouldbeasfollows:
■ IncredibleYears(parentandchildprogrammes-throughtheprimaryschoolswiththepooresttestresultsatstages1&2andthroughSurestart)
■ FamilyNursePartnerships■ BigBrothers/BigSistersmentoringprogramme■ PATHS■ LifeSkillsTraining■ MultisystemicTherapy■ SuccessforAll■ DoodleDen■ TimetoRead
Note:FunctionalFamilyTherapyandMultisystemicTherapyareeffectivelyalternativestoeachother.OncostgroundsMultisystemicTherapyisbeingrecommendedhere.

Page 88
Itisimportanttosaythattheamountofrobustevaluationevidence,bothpositiveandnegative,onprogrammesforchildren,youngpeopleandfamiliesisincreasingrapidly.WithintwoyearstherewillbeovertwentyRCTevaluationsofsuchprogrammesintheUKandIreland,whichwillfurtherenhancetheabilityofEILtoidentifythemostappropriateinitiativestoachievetheagreedoutcomes.Theshortlisted“proven”programmesrecommendedinthisreportarebasedonthecurrentbestevidence.ResurgamandEarlyInterventionLisburnSteeringGroup/Consortium,inconsultationwiththemainstakeholders/funders,willneedtomakefinaldecisionsastotheprogrammestoprioritiseinphase1,aswellascontinuingtoexaminetheemergingnationalandinternationalefficacyevidence(theCYPSPparticularlyrecommends*trackingtheoutcomesofRCTevaluationsinNorthernIreland);buildinglocalcapacity,sothatthereisanongoingsustainedefforttochangeoutcomesforchildren,youngpeopleandfamilies.;promotinginnovationandtheinclusionoflocalcommunities,childrenandyoungpeopleinbuildingontheirassets,promotingtheirrightsandrespondingtotheirneeds.
5.5CostsoftheEarlyInterventionProgrammesTheevidenceonthecostsofdeliveringthelong-listedevidence-basedprogrammesisasfollows:
Programme Target group Total cost** to deliverIncredibleYears
Parentsand3-8yearolds
Parentprogramme:£4,833perschooleachyear;SchoolReadiness(enhancedparentingprogramme):£1,500perschool;DinaChildren’sProgramme:£6,253perschool
£12,586perschool/venue(inc.all3IYSprogrammes)
PATHS 4-6yearolds Costof£10,000peryearperschool(totalcosts)
£10,000perschool
FamilyNursePartnership
Pregnancy–age2
Costof£3,000perclientfamilyperyear,inc.nursetraining
£669,000for10%offamiliesintargetareas
BigBrothers/BigSisters
6-18yearolds Costperyoungpersonperyearc.£627
£140,000for10%ofallchildrenaged6+inthetargetareas
LifeSkillsTraining
9-15yearolds Costofc.£4.40perstudentplusthecostoftraining:£2,508
£7,000.00forallyoungpeopleaged9-15
MultisystemicTherapy
12-17yearolds c.£2,821peryoungperson £282,100for10%ofyoungpeopleage12-17
SuccessforAll,includingcuriositycorner
3-11yearolds £3,467forKeyStage1and£7,280forKeyStage2,perschool(allcosts)£3,526forthenursery/receptionprogramme
£10,747perschool(£14,273foraschoolwithanurseryorreception)
* CYPSP2012Recommendations“HowtomakeNorthernIrelandanEarlyInterventionRegion”**Willneedtobeadjustedeachyearforinflation
CHAPTER FIVE
Theory of change

Page 89
DoodleDen 5/6yearolds £18,000sitecostsplus£4,200pergroupof15children
£35,000todeliverinfourprimaryschools(15pupilseach)
TimetoRead 6-8yearolds Free.Thecriticalresourcearethevolunteerstodelivertheprogramme
Free
TotalCosts(assumingschool-basedprogrammesaredeliveredinfourschools/venues):£1,312,777
5.6CostsoftheCo-ordinationInfrastructureInadditiontoprogrammerelatedcosts,EarlyInterventionLisburnwouldrequirefundingforitsinfrastructure,inordertodevelopandimplementprogrammes;ensureprogrammefidelity/quality;co-ordinaterelationshipswiththevariousstakeholders;managefinance;ensureeffectivecommunityengagement,etc..
Cost Headings Annual Cost (need to adjust for inflation)
EarlyInterventionCommunityCo-ordinator(salary&relatedcosts)-Resurgam £35,000
EarlyInterventionDeliveryManager(salary&relatedcosts)–DeliveryPartner £45,000
EarlyInterventionQuality&MonitoringOfficer(salary&relatedcosts)–DeliveryPartner
£35,000
AdministrationandservicingoftheEarlyInterventionConsortium-Resurgam £3,000
Programme-relatedFinance/Administration £15,000
Travel(local,nationalandinternational),phonecosts £8,000
Officeandenergycosts-Resurgam £7,500
Officeandenergycosts–Deliverypartner £7,500
Stationary,PRandmarketingcosts(incNewsletter) £6,000
Governancecosts-Resurgam £3,000
Evaluation(seebelow) £50,000
CommunityConsultations-Resurgam £2,000
OneProject-TwoCitieswithEarlyInterventionDerry-LondonderryandeffectivepartnershipworkingwithotherEarlyInterventionsites
£10,000
Thecostofparent-friendlyeventsandactivitiestohelpbuildtherelationshipswithparentsandattractthemtoparticipateinmorerigorousprogrammes
£3,000
TotalAnnualCosts £230,000
Thetotalannualcostofimplementingtherecommendedprogrammesandtherelatedinfrastructurecostswouldthereforebec.£1,540,000.However,itislikelytobeseveralyearsbeforetheinvestmentcanbeputinplacetodeliveralltherecommendedprogrammes,sothefundingrequiredinyear1islikelytobeconsiderablylower.
ThecostsofSureStarthavenotbeenincludedinthesecalculations,astheyaresubjecttoseparatenegotiationswiththeEasternChildcarePartnership.

Page 90
Therearealsopotentialissuesconcerningcommunitypremiseswhereprogrammesaregoingtobedeleivered,whicharehardtocalculateatthisstage.Insomeofthetargetareastherearegoodcommunitybuildings;otherareasarelikelytobeabletoaccessgreatlyimprovedcommunitypremisesinthenearfuture.Therearealsosomeareaswithverypoorfacilities,whichcurrentlyprovidelittlescopeforadditionalearlyinterventionservices.
5.7EvaluationThereisanimportantissueconcerningtheevaluation(s)ofanyagreedprogrammesimplemented.Iftheprogrammeshavealreadybeenrobustlyevaluatedatleasttwice(as“proven”Blueprintsprogrammesare,oriftheyarealreadysubjecttoamajorRCTtrialelsewhereintheUKorIreland,itmaynotbenecessarytocommissionanRCTevaluation.However,programmesthathavesomepromisingevidence,suchasMellowParents,theParentInfantProgramme(PIP)andtheNewParentingProgramme,buthavenotyetbeensubjecttoalarge-scaleRCTshouldbesubjecttoaRCTtrial.Inadditionitisstillimportanttocommissionanobjectiveformativeandsummativeassessmentofhowwelltheprogrammeshavebeenimplemented,whatprogressisbeingmadeinachievingtheagreedoutcomes,andidentifyanylessonsthatcanbelearnt.
Itwouldalsobeincrediblyvaluabletocommissionalong-termassessment,againstdatafromcomparableareas,astotheextentthattheagreedsetofEarlyInterventionLisburnprogrammesoverallhavebeenabletoimpactonthemeasurableoutcomeindicators.Ideallythisshouldbeoveratleast15years.
Therearealsovariousexistingprogrammesandservicesforchildren,youngpeopleandfamiliescurrentlybeingdeliveredinsomeofthetargetareas.Theevidencefromthisreportwouldsuggestthatcollectivelytheseprogrammesandservicesarenotenablingthechildrenandyoungpeoplefromthetargetareastoachievetheirpotential.However,perhapstheseoutcomeswouldbeevenworseiftheseprogrammesandservices,orsomeofthem,didnotexist.Theseprogrammesandservicesneedtobeeffectivelymappedandassessedagainsttheevidencefortheimpacttheyaremakingonthedesiredoutcomes,highlightedabove.Itwouldthenbepossibletomakeinformeddecisionsonwaysof:
■ clarifyingoutcomesofexistingprogrammesandservicesandevaluatingtheirimpactontheseoutcomes;
■ focusingexistingprogrammesandservicestoimprovethedesiredservices;■ expandingexistingprogrammesandservices;■ co-ordinatingthevariousprogrammesandservicesbetter;■ reducingorclosingexistingservices;and/or■ fillingthegapsidentified.
CHAPTER FIVE
Theory of change

Page 91
5.8PerformanceManagementInadditiontoexternalevaluationthereneedstobeaneffectiveperformancemanagementandqualityassurancesystemthatensuresthatallprogrammesaredeliveredwithfidelity(assetdownbytheownersofthelicense)andinaccordancewiththeobjectivesandcommitmentsagreedwithfunders.Somelicensedprogrammeshaveverytightfidelityandqualityassurancerequirementse.g.PATHS,othersarelesstightlyspecifiede.g.IncredibleYears.ThedangerinthelatteristhatprogrammmesmaybeimplementedinawaythatfailstoachievetheoutcomeswhichRCTevaluationshaveshowntheycanachieve.AnyprogrammesimplementedthroughEILneedtobedemonstrateaveryhighstandardoffidelity.
Therealsoneedstoaneffectiveprocessforgathering,measuring,analyzingandreportingonrelevantdatafromeachprogramme.
ThisissueisdiscussedmoreundertheOperatingModelbelow.
5.9PotentialSourcesofFunding:Fromthescanofpublicpolicydocuments,thefollowingareGovernmentDepartmentsandagencieswhichhaverelevantpublicpolicyobjectivesinrelationtotheagreedoutcomesandshouldthereforebepotentialsourcesoffundingfortheEarlyInterventionLisburnprogrammes:
■ OFMdFM–SocialInvestmentFund■ DHSSPS■ Health&SocialCareBoard■ PublicHealthAgency■ SouthEasternHealth&SocialCareTrust■ Children&YoungPersonsStrategicPartnership■ DepartmentofEducation■ SouthEasternEducation&LibraryBoard–schoolsbudget■ SouthEasternEducation&LibraryBoard–youthservicebudget■ Schools’ExtendedSchoolsbudget■ DepartmentofJustice■ YouthJusticeAgency■ ProbationBoard■ PSNI■ DepartmentofSocialDevelopment■ Departmentalresearchbudgetsreevaluations■ LisburnCityCouncil■ NIHousingExecutive■ BigLottery–e.g.SupportingFamilies■ Charitabletrusts/foundations

Page 92
5.10 TheoryofChangeLinkagesAtheoryofchangehighlightsthelogicoftheapproachtobeadoptedi.e.betweeninputs,activities,outputsandoutcomes.ThefollowinghighlightstheoveralllogicofthesuggestedEarlyInterventionLisburnapproach:
TheoverarchingobjectiveofEarlyInterventionLisburnis:ToimprovetheoutcomesforchildrenandyoungpeopleindisadvantagesareasofLisburn
Thisistobeachievedby:Puttinginplaceandeffectivelyimplementingprovenuniversalandtargetedprogrammeswhichhavebeenshowntoimproveoutcomesforchildrenandyoungpeopleoverasustainedperiod.
Thisistobeachievedby:BeingclearabouttheoutcomeswherechildrenandyoungpeopleindisadvantagedcommunitiesinLisburnfallsignificantlyshortoftheNorthernIrelandaverage.AND
IdentifyingthoseprovenuniversalandtargetedprogrammeswhichhavebeenshowntoimprovethespecificagreedoutcomesforchildrenandyoungpeopleindisadvantagedcommunitiesAND
Eitherrobustlyevaluating,and/orstopdelivering,existingprogrammesthatdonotdemonstrateclearlytheirpositiveimpactontheagreedoutcomesAND
Gainingeffectivecommunity,politicalandstatutorycommitmenttoandsupportfortheimplementationofacomprehensivesustainedearlyinterventionprogrammeandtoworkingeffectivelytogetherAND
Gainingsufficientlong-termfundingtosupportasustainedearlyinterventionprogrammeAND
Implementingagreeevidence-basedprogrammeswithfidelityAND
AttractingandretainingtheparticipationofthetargetparentsandchildrenintheprogrammesimplementedAND
Effectivelyevaluatingtheprogrammesagainstagreedoutcomes
CHAPTER FIVE
Theory of change

Page 93
5.11 LogicModelThefollowinglogicmodelarticulatesinmoredetailthepotentialrelationshipbetweeninputs,activities,outputs,intermediateandfinaloutcomesandhowtheycanbemeasured.
Inputs Activities Outputs Intermediate outcomes
Final outcomes
==> ==> ==> ==>
AnnualFinancialsupportof£1.5Mfromstat.sources:• Co-ordinator
&programmestaff
• Programmecosts
• Governance&m’mentcosts
• Evaluation• Acommitment
fromagenciestoworktogethertoachievetheoutcomes
• Engagementoftargetlocalcommunities
• Supportfrompoliticalreps
• Contributionfromschoolstopromoteeffectivedelivery&liaison
• ContributionfromeachpartnertoparticipateintheConsort-ium&deliveragreedprogrammes
• Contributionfromparents&childrentoparticipate
• Qualityassurancere.programmefidelity
• Evaluationexpertise
UniversalinPrimarySchools
• PATHS(4-6yearolds)
• SuccessforAllinc.curiositycorner(age3-11)
• TimetoRead(8-10yrolds)
• LifeSkillsTraining(9-15yearolds)
UniversalinPost-PrimarySchools• LifeSkills
Training(9-15yearolds)
Targetedincommunityvenues• Incredible
Years(age0-12)
• BigBrothers/BigSisters(BB/BS)(6-18yearolds)
Targetedhome-based• FamilyNurse
P’ship(NFP)(pregnancy-2)
• MultisystemicTherapy(12-17yearolds
• PATHS(xsessionsforychildrenoverzmonths)
• SuccessforAll(xsessionsforychildrenoverzmonths)
• LifeSkillsTraining(xsessionsforychildrenoverzmonths)
• IncredibleYears(xsessionsforychildrenoverzmonths)in
• BB/BS(xsessionsforychildrenoverzmonths)
• FNP(xsessionsforychildrenoverzmonths)
• MultisystemicTherapy(xsessionsforychildrenoverzmonths)
• Reducednumberofteenagepregnancies
• Reducedlevelofsmokingduringpregnancy
• Improvedparentingskillsandconfidence
• Improvedparent-childattachmentfor0-2yearolds
• Improvedschoolattendance
• Improvedschoolreadinessamongst3&4yearolds
• Improvedthesocialandemotionalskillsandresilienceof4-11yearolds
• Improvedliteracy&numeracyinchildrenaged4-11
• Improvededucationalattainment
• Reducedbehavioural/conductproblems
• Reducedsmoking,alcohol&drugconsumptionamongstyoungpeople
• Reducedcrimeandanti-socialbehaviouramongstyoungpeople
• Improvedphysicalandmentalhealthofchildren

Page 94
How inputs will be measured
How activities will be measured
How outputs will be measured
How intermediate outcomes will be measured
How final outcomes will be measured
==> ==> ==> ==>
Financialbudgetandquarterlymanagementaccounts
Outputsinrelationtoparentandchildparticipation
ParticipationintheearlyYearsLisburnSteeringGroupandsub-groups
Outputs(seecolumntotheright)
Fidelitytotheprogrammemanual
Parentsatisfaction
Youngparticipantsatisfaction
Numberofprogrammesessionsdelivered
Numberofchildrenandyoungpeopleinvolvedintheprogrammes
Numberofparentsinvolvedintheprogrammes
%attendanceatprogrammes
%ofparticipantscompletingtheprogrammes
• %ofmotherssmokingduringpregnancy
• Increasedparentingconfidence(ParentsSenseofCompetenceScale)
• Increasedparentalengagementwiththeirchild’seducation
• Improvedchildbehaviour(TheEybergChildBehaviourInventoryforParentsandtheSutter-EybergBehaviourInventoryforteachers)
• Improvedchildsocial&emotionalskills(SDQforparentsandteachers)
• Literacy&numeracyatKeystages1&2
• Numberofteenagepregnancies
• Improvedparent-childattachmentfor0-2yearolds
• increased%ofchildrenwith85%schoolattendance
%deathsundertheageof75
Averageageatdeath
%youngpeoplegoingontohigherorfurthereducation
%ofyoungpeopleachieving5+GCSEsA*-C
%ofyoungpeopleachieving2+AlevelsA*-C
Numberofcrimesandanti-socialbehaviourincidents
Levelofsmoking,alcoholanddrugconsumptionamongstteenagers
CHAPTER FIVE
Theory of change

Page 95
CHAPTER SIX
Operating model
6.1IntroductionItisvitaltohaveaneffectiveandacceptedoperatingmodeltoplanandimplementacomprehensiveprogrammeofuniversalandtargetedearlyinterventionprogrammesinLisburn.Thestructuresneedtoengageallthekeyagenciesifitistoensureeffectiveco-ordinationandseamlessdeliveryofservices.ItisalsovitallyimportantthatthelocalcommunitieswhichEarlyInterventionLisburnwouldservefeelasenseofownershipoftheprogrammesthataredelivered,otherwise,iftheyareperceivedtobeparachutedinbyexternalagencies,theprogrammesareunlikelytogettheparticipationofthosewhomostneedtheservicesinordertobesuccessful.
6.2ResurgamTrustTheResurgamDevelopmentTrusthasbeenestablishedtocreateacommunity-ownedorganisationdesignedtopromotetheinterestsofthoseindisadvantagedcommunitiesinLisburn.ItwasformallyconstitutedasacompanylimitedbyguaranteeinJanuary2011.IthasbeenacceptedascharitablefortaxpurposesbytheInlandRevenue.ThemembershipofResurgamismadeupofc.1,000individualmembers(adultsandyoungpeople).TheBoardismadeupofrepresentativesfromlocalcommunityandyouthorganisations.
ItisResurgamthatinitiatedthecurrentexplorationofanearlyinterventionapproachtoaddressingmanyoftheproblemsfacedbydisadvantagedcommunitiesinLisburnandcurrentlyco-chairsandservicestheEarlyInterventionLisburnSteeringGroupmadeupofawiderangeofrelevantagencies.
Currently,atthetimeofwritingthisreport,however,Resurgamisaverynewplayeranddoesnotreceiveanycorefunding.ThisisanissuethatwouldneedtoberesolvedifitistohavethecapacitytoplayaleadingroleinthedevelopmentandmanagementofEarlyInterventionLisburn.DiscussionsarecurrentlytakingplacewithDSDinrelationtoResurgamasaflagshipsocialenterpriseinitiative.
ItisalsoimportantthatResurgamhastheorganisationalandfinancialpoliciesandprocedures,andassuredgovernancedevelopmentprocessesthatreflectitspotentialasthecentralco-ordinatingandservicingbodyofEarlyInterventionLisburn.
6.3ChildrenandYoungPeople’sOutcomesGroupAsecondkeyplayeristheinter-agencyinter-sectoralSouthEasternOutcomesGroupoftheChildrenandYoungPeople’sStrategicPartnership,whichisplayingavitalroleindrivingtheearlyinterventionagenda.AllthemainstatutoryandvoluntarybodiesconcernedwithmeetingtheneedsofchildrenandyoungpeoplewithintheSouth-Easternareaarerepresentedonthegroup.

Page 96
TheEarlyInterventionLisburnSteeringGroup,whichhasrepresentativesfromvariouscommunitygroupsandallthekeystatutoryagencies,shouldberefreshedastheEarlyInterventionLisburnConsortiumandberecognisedasaLocalitysub-groupoftheSouth-EasternYoungPeople’sStrategicPartnershipOutcomesGroupandshouldbecomethekeyco-ordinatinginter-agencybody,similartotherolefulfilledbyHealthImprovementorHealthCitiesPartnerships.
6.4OtherImportantPartnersThefollowingaresomeoftheotherkeyplayerswhichneedtobeengagedandcommittedtotheEarlyInterventionLisburnConsortiumifitistobeasuccess:
■ PublicHealthAgency■ SouthEasternHealth&SocialCareTrust■ SouthEasternChildcarePartnership■ DepartmentofEducation■ SouthEasternEducation&LibraryBoard/ESA■ StatutoryYouthService-SouthEasternEducation&LibraryBoard/ESA■ DepartmentofJustice/YouthJusticeAgency■ PSNI■ DepartmentofSocialDevelopment■ LisburnCityCouncil■ NIHousingExecutive■ Electedrepresentatives
6.5DeliveryPartner(s)Deliveringtheportfolioofearlyinterventionprogrammesrecommendedinthisreportwillrequireextensiveexperienceofdeliveringandqualityassuringprogrammesforchildrenandfamilies.ItisthereforevitalthatoneofmoreexperienceddeliverypartnerareappointedbyEarlyInterventionConsortiumLisburnConsortium.
Thereisanimportantquestionastohowmanydeliverypartnersthereshouldbe.Itispossibletomakeanargumentforseveraldifferentarrangements:
Option 1: Separatedeliverypartnersforeveryprogramme(potentiallylargenumberofdifferentdeliverypartners)■ Pros:abletobringinexperienceofdeliveringallthetargetprogrammes;bodies
currentlydeliveringthetargetprogrammeselsewherecanbeincludedinEIL■ Cons:complexstructure;variousdifferentorganisationalculturesand
systems;complex,diffuseaccountability;moredifficulttobuildeffectiverelationshipsandcross-programmeworking;timeandenergyrequiredtoeffectivelyco-ordinatethevariousbodies
CHAPTER SIX
Operating model

Page 97
Option2:Oneexperienceddeliverypartnerwhichtakesresponsibilityfortheimplementationofallprogrammes■ Pros:simplestructure;singleorganisationalcultureandsystems;clear
accountability;easiertobuildeffectiverelationshipsandcross-programmeworking
■ Cons:onebodyisunlikelytohavepreviousexperienceofdeliveringallthetargetprogrammes.
Option 3: Onedeliverypartner,whichcansub-contractdeliveryofprogrammes,ifnecessary■ Pros:Simplestructure;singleorganisationalcultureandsystem;clear
accountabilityandreportinglines;easytobuildeffectiverelationships;canengageotheragenciesindelivery(e.g.SEHSCTindeliveringFNP);sub-contractingcanbequalityassuredbythedeliverypartner;strongeffectiveco-ordinationbetweentheprogrammes
■ Cons:SuccessoftheEILinitiativedependsontheappointmentoftherightdeliverypartnerwhichcandelivercomplexprogrammeswithfidelityandworkwellwiththecommunity
Option3isrecommended.
6.6PotentialroleofResurgamCommunityengagementiscriticaltothesuccessofEarlyInterventionLisburn.Resurgam,asanrepresentativeumbrellacommunitybodyforthetargetareas,has,therefore,acrucialroleinthesuccessoftheinitiative.TheSouth-EasternYoungPeople’sStrategicPartnershipOutcomesGroup,onbehalfoftherelevantagencies,shouldcontractwithResurgumtofulfillthefollowingrolesfortheEarlyInterventionLisburnConsortium/LocalityGroup:
Consortium■ Organiseandco-ordinatemeetingsoftheEarlyInterventionLisburn
Consortium(notlessthan4/5timesayear)■ EnsureallConsortiummeetingsarewellplannedandeffectivelyserviced■ Provideaco-chairfortheConsortium■ EnsuretheEarlyInterventionLisburnConsortiumhastheappropriate
structureandofficers■ EnsuretheConsortiumoperatestothehighestgovernancestandardsand
regularlyreviewsitsperformance
DeliveryPartner■ Drawupthebrief(withexpertassistanceifrequired)fortheappointmentofa
deliverypartner,forapprovalbytheConsortium

Page 98
■ ServicetherecruitmentandselectionofadeliverypartnerbyapanelappointedbytheEILConsortium
■ Maintaineffectiveliaisonwiththedeliverypartner■ Facilitateandsupporttherelationshipbetweenthedeliverypartnerand
relevantcommunitygroups/organisations■ LiaisewiththeDeliveryPartnerinrelationtothedevelopmentoftheportfolio
ofnewevidence-basedearlyinterventionprogrammes,asagreedwiththeConsortium
RiskManagement■ Develop,andkeepup-to-date,ariskregister■ HighlighttotheConsortiumandDeliveryPartneranypotentialbarriersor
challengestoachievingtheagreedplans■ EnsureResurgamandEarlyInterventionInitiativeLisburnConsortium
complywiththehigheststandardsinrelationtogovernanceandpotentialconflictsofinterest
MarketingandPR■ ActivelypromoteandpublicisetheEarlyYearsLisburnInitiative,locallyinthe
targetcommunitiesandwidercommunitynetworks■ Activelysupportthemarketingofrelevantprogrammesinthetargetareas■ ProducearegularEarlyInterventionLisburnNewsletter,inpartnershipwith
theDeliveryPartner,anddisseminatewidelywithinthetargetcommunities
Employment■ EmployandmanageanEarlyInterventionCommunityEngagementOfficer■ Ensuregoodpracticeintherecruitment,selection,inductionandmanagement
ofstaffinallaspectsofEarlyInterventionLisburn■ Contributeasapanelmembertotheselectionofstaffforagreedprogrammes
ProgrammeDevelopment■ Negotiate,withtheConsortium,fundingfortheinitialagreedevidence-based
programmesandinfrastructurecosts■ Facilitate(withexpertassistanceifnecessary)thedevelopment,
implementationandmonitoringofoverallEarlyInterventionLisburnstrategicandannualoperationalplans
QualityAssurance&PerformanceManagement■ ConsiderQualityassurancereportsfromtheDeliveryPartnerinrelationto
ensuringtheeffectivedeliveryoftheoverallprogrammeandensuringthefidelityofevidence-basedprogrammes
CHAPTER SIX
Operating model

Page 99
■ EnsuretheDeliveryPartnerhasappropriatesystemsinplacetomonitorandevaluatetheperformanceofagreedprogrammes;andagainstspecificindicatorsfortheoverallprogrammeinrelationtoeachOutcome
Finance■ Ensurethehigheststandardsoffinancialplanning,accountingandreporting■ Ensureappropriatefinancialreportingmechanismstofunders/contractors
whichareprovidingfundingdirectlytoResurgamand/ortheEarlyInterventionLisburnConsortium
Collaboration■ Collaborateeffectivelywithothercommunityorganisationsengagedinearly
interventioninitiativesinNorthernIreland,GBandIreland■ Buildeffectiverelationshipsandworkpositivelytoresolveanydisputesor
difficulties
Consultation■ Activelypromotetheactiveparticipationofallthelocaltargetcommunitiesin
theagreedprogrammes■ Consultlocaltargetcommunitiesonperceptionsoftheprogrammesand
emergingneedsandissues■ EnsurethereisaneffectivecommunityvoiceontheEarlyInterventionLisburn
Consortium■ Ensureallrelevantlocalcommunitygroupsareeffectivelyrepresentedon
Resurgam
ResearchandEvaluation■ FacilitatetheappointmentandservicingofanExpertAdvisoryCommittee(of
earlyinterventionandevaluationexperts)toadvisetheConsortium■ Drawupabrief(withexpertassistance,ifrequired)fortheappointmentof
evaluators■ Sourceexperiencedevaluatorsthroughadministeringathoroughtender
recruitmentprocessandsitonthepanel(thepaneltobeappointedbyEILConsortium)
■ Ensuretheevaluationcontractiseffectivelymanaged■ Ensureeffectiveliaisonwithevaluators

Page 100
6.7RoleoftheDeliveryPartnerThefollowingissuggestedasappropriateresponsibilitiesoftheDeliveryPartner:
QualityAssurance&PerformanceManagement■ Ensuretheagreedprogrammesaredeliveredwithfidelity,througheffective
qualityassurance■ Ensuregoodpracticeinidentifyingandsourcinganysub-contracteddelivery
bodies■ Ensurethereareappropriatesystemsinplacetointernallymonitorand
evaluatetheperformanceofagreedprogrammes
ProgrammeDevelopment■ Contributetothenegotiationsforfundingofagreedevidence-based
programmesandinfrastructurecosts■ Developtenderbriefsforagreedprogrammestobedeliveredbysub-
contractors,forConsortiumapproval■ Contributetothedevelopment,implementationandmonitoringofoverall
EarlyInterventionLisburnstrategicandannualoperationalplans■ LiaisewiththeEarlyInterventionLisburnConsortiumandResurgamin
relationtothedevelopmentoftheportfolioofnewevidence-basedearlyinterventionprogrammes
RiskManagement■ Develop,andkeepup-to-date,ariskregisterinrelationtotheagreed
programmes■ HighlighttotheConsortiumandResurgam,assoonaspossible,anybarriers
orchallengestoachievingtheagreedplans■ Complywiththehigheststandardsinrelationtogovernanceandpotential
conflictsofinterest
MarketingandPR■ ActivelypromoteandpublicisetheEarlyYearsLisburnInitiative,locallyinthe
targetcommunities,NI-wideandintheUKandIreland■ Activelymarkettherelevantprogrammesinthetargetareas■ ProducearegularEarlyInterventionLisburnNewsletter,inpartnershipwith
Resurgam
Employment■ EmployandmanageanEarlyInterventionManager(notnecessarilythefinal
jobtitle)toleadandco-ordinatethevariousprogrammesandliaisewiththeConsortiumandResurgam
CHAPTER SIX
Operating model

Page 101
■ Ensuregoodpracticeintherecruitment,selection,inductionandmanagementofstaffinallaspectsofEarlyInterventionLisburn
■ Contributetotheselectionofstaffforanyagreedsub-contractedprogrammes■ Ensureallstaffaretrainedtotheappropriatestandard
Finance■ Ensurethehigheststandardsoffinancialplanning,accountingandreporting■ Ensureappropriatefinancialreportingmechanismstofunders/contractors
Collaboration■ EnsureeffectivecollaborationwithSureStart,relevantschools,andother
relevantprogrammes,organisationsandvenues■ Collaborateeffectivelywithotherearlyinterventiondeliverybodiesin
NorthernIrelandandbuildrelationshipswithotherearlyinterventioninitiativesinGBandIreland
■ Liaisecloselywithanysub-contracteddeliveryagenciesandworkpositivelytoresolveanydisputesordifficulties
Consultation■ Activelypromotetheactiveparticipationofthelocaltargetcommunities■ Consultlocaltargetcommunitiesonperceptionsoftheprogrammesand
emergingneedsandissues
ResearchandEvaluation■ KeepuptodatewithemergingevidenceintheUK,Irelandandinternationally
oftheefficacyofrelevantearlyinterventionprogrammes■ Ensurethereisanappropriateperformancemanagementinformationsystem
whichiseffectivelyimplemented■ Ensuretheevaluationcontractiseffectivelymanaged■ Ensureeffectiveliaisonwithevaluators
Reporting■ ProduceareportfortheEarlyInterventionLisburnConsortiumandResurgam
(notlessthan4timesayear)inaformatagreedwiththeConsortium■ Producefinancialandmonitoringreportsasagreedwiththerelevantfunders

Page 102
CHAPTER SEVEN
Implementation plan
7.1IntroductionThisshortsectionwilloutlinethenextstepsintermsofmovingtowardsimplementingtherecommendationsabove.Itisnotpossibletoimplementarangeofnewprogrammesatonce,soitisimportanttophasetheirintroduction.Whichprogrammeswouldbeimplementedbeforeotherprogrammeswouldbepartlydeterminedbyfunding,theavailabilityofaDeliveryPartnerwithrelevantexperience,andthereadinessoftheenvironmente.g.thecommunitiesandschoolstosupporttheimplementationofaprogramme.
7.2TimetableThefollowingoutlinesasuggestedimplementationplanbetweenJune2012andDecember2018:
June–September2012■ EarlyInterventionLisburnSteeringGrouptodiscussthereportandagree
whichrecommendations(ifany)itwishestoendorse
■ Agreetheprocessforprintinganddisseminatingthereport
■ MeetwiththeSouthEastOutcomesGroupoftheChildren&YoungPerson’sStrategicPartnershiptodiscussthereport
■ Agreeaprogrammeofface-to-facepresentationsofasummaryofthereporttoarangeofkeystakeholders,includingcommunityorganisationsandstatutoryagencies
■ Agreetheprocessfordevelopingacommonoutcomesframework(whichwillenableimpacttobemeasured)andasharedfocusonqualityachievedthroughjointreflectivepractice,trainingandpeerlearning,wherebydifferentorganisationscanlearnfromoneanother.
■ BringexistingorganisationstogethertoidentifyhowbesttotransformtheculturewithintheCityofLisburn,especiallywithinareasofdeprivation,toemphasiseaspirationandachievement(particularlyinrelationtoeducation)throughlocalmedia,doortodoorconsultations,celebratinglocalchampionsetc.
■ Agreeaprocessformappingexistingservices/programmesservingdisadvantagedcommunitiesinLisburnandtheevidenceforthecontributiontheymaketowardstheagreedoutcomes

Page 103
■ MeetwiththeprimaryschoolsintheExtendedSchoolsprogrammeinLisburntodiscusswiththemthekindsofsupportandassistancetheyrequiretohelpthemachievetheirobjectivesandthepotentialtohostappropriateprovenmodelsintheschools
■ DrawupabriefandprocessfortheappointmentofaDeliveryPartner.
■ AppointanappropriateDeliveryPartner
■ AgreeaService-LevelAgreementwiththeDeliveryPartner
■ Considerthepotentialforanyoftheprogrammestobedeliveredinpartnershipoverawidergeographicalarea(e.g.theOneProject:TwoCitiesinitiative;SEHSCTarea)
■ Identifythemostappropriatesource(s)ofinfrastructurefinance,andapply,forfundinginaccordancewithappropriateobjectivesandprocedures.
■ Identifythepotentialfundersofrecommendedprogrammesandarrangemeetingswitheachtodiscussthereportandpotentialfunding
■ NegotiateaninitialcontractbetweentheChildren&YoungPerson’sStrategicPartnershipandResurgamtotakeforwardtherecommendationsinthereport
■ DrawupandapprovejobdescriptionsandspecificationsforinfrastructurepostsinResurgamandtheDeliveryPartner
■ ArrangestudyvisitstoseetherecommendedprogrammesintheUKandIrelandinoperation
■ EnsureResurgamhasalltheorganisationalpoliciesandprocedures,financialpoliciesandprocedures,andexternallysupportedgovernancedevelopmentprocessesthatreflectitspotentialastheco-ordinatingandservicingbodyoftheEarlyInterventionLisburnConsortium
■ ConsiderthemostappropriatemembershipoftheEarlyInterventionConsortium
■ Appointtheco-chairsoftheearlyInterventionLisburnConsortium

Page 104
October–December2012■ RecruitandselectaResurgamEarlyInterventionCommunityCo-ordinator
(subjecttofundinghavingbeennegotiated)throughopenrecruitment(inaccordancewithagreedpoliciesandprocedures)
■ TheDeliveryPartnertorecruitandselectanappropriateEarlyInterventionLisburnDeliveryManager
■ Drawup(DeliveryPartner)servicedesignbriefsforeachoftheagreedphase1programmese.g.fromIncredibleYears,FamilyNursePartnerships,BigBrother/BigSisters,PATHS,SuccessforAllandLifeSkillsTraining
■ Putdetailedproposals/applicationstofunders/contractors,inrelationtophase1programmesandinfrastructure,asagreed
■ Meetwiththetargetschoolsconcerningtheirpotentialtohostappropriateprogrammese.g.Incredibleyearsfullparentandchildprogrammes,PATHSandSuccessforAll
■ DrawupanevaluationbrieffortheoverallEarlyInterventionLisburnProgrammeandseekfundingfortheevaluation
January–March2013■ InductandtraintheResurgamEarlyInterventionCommunityCo-ordinator
andDeliveryPartnerEarlyInterventionDeliveryManager
■ RecruitandselectaDeliveryPartnerEarlyInterventionQuality&MonitoringOfficer(subjecttofundinghavingbeennegotiated)throughopenrecruitment(inaccordancewithagreedpoliciesandprocedures)
■ Goouttotenderonthephase1agreedprogrammese.g.fromIncredibleYears,FamilyNursePartnershipsandBigBrothers/BigSisters,PATHS,SuccessforAll,LifeSkillsTraining,whenappropriatefundinghasbeenapproved
■ MeetwithBITCaboutthepotentialtodeliverTimetoReadintheadditionaltargetprimaryschools
■ Putmoredetailedproposals/applicationtofunders/contractors,inrelationtophase1asagreed
■ Agreewhichprogrammestoincludeinphase2e.g.fromthepriorityprogrammesnotimplementedinphase1
CHAPTER SEVEN
Implementation plan

Page 105
■ Goouttotenderforanappropriateevaluationteam
■ Drawupandagreeastrategicplanfor2013-2018andanoperationalplanfor2013/14.
April2013–August2013■ DeliveryPartnertocarryoutthestartup(planning,trainingandrecruitment)
phaseofthefirstearlyinterventionprogrammes
■ Marketthephase1programmeseffectivelytothetargetlocalaudiences
■ Drawupservicedesignbriefsandtenderspecificationsforeachoftheagreedphase2programmes
■ Evaluatorstoagreemeasuresandinstrumentsandcarryoutbaselinemeasurement
■ Putdetailedproposals/applicationtofunders/contractors,inrelationtophase2asagreed
■ EarlyInterventionLisburnConsortiumandResurgamtodiscussannualearlyinterventionreportfromtheDeliveryPartner
September–December2013■ Startdeliveringagreedphase1earlyinterventionprogrammes
■ Evaluatorstoproducebaselinereport
■ Putmoredetailedproposals/applicationtofunders/contractors,inrelationtophase2programmes,asagreed
■ Goouttotenderonthephase2agreedprogrammes,whenappropriatefundinghasbeenapproved
January-June2014■ DeliveryPartnertocarryoutstartupphase(planning,negotiatinglicenses,
training,baselineevaluationandrecruitment)ofphase2earlyinterventionprogrammes
■ Agreewhichprogrammesshouldbepartofphase3

Page 106
■ Putdetailedproposals/applicationtofunders/contractors,inrelationtophase3programmes,asagreed
■ EarlyInterventionConsortiumandResurgamtodiscussannualearlyinterventionreportfromtheDeliveryPartner
July–December2014■ Startdeliveringagreedphase2earlyinterventionprogrammes(community,
homeandschoolbased)
■ Drawupservicedesignbriefsandtenderspecificationsforeachoftheagreedphase3programmes
■ Goouttotenderonthephase3agreedprogrammes
■ ReviewthegovernanceoftheEarlyInterventionLisburninitiativeandagreeactionstofurtherimproveit
■ Putmoredetailedproposals/applicationtofunders/contractors,inrelationtophase3programmes,asagreed
■ Consider1styearformativeevaluationreport(s)andadjustmentsrequiredinthedeliveryoftheprogrammes
January–June2015■ Startup(planning,negotiatinglicenses,training,baselineevaluationand
recruitment)phaseofphase3earlyinterventionprogrammes
■ Agreewhichprogrammesshouldbepartofphase4(considerableadditionalevidenceonwhatworksintermsofearlyinterventionshouldbeavailableatthispoint,incarangeofRCTsinIrelandandGB)
■ Putdetailedproposals/applicationtofunders/contractors,inrelationtophase4programmes,asagreed
■ EarlyInterventionsteeringgrouptodiscussannualearlyinterventionreportfromResurgam
CHAPTER SEVEN
Implementation plan

Page 107
July–December2015■ Startdeliveringagreedphase3earlyinterventionprogrammes
■ Considertheformative2yearevaluationreport(2yearsofphase1and2yearsofphase2)
■ Drawupservicedesignbriefsforeachoftheagreedphase4programmes(wherefundingisagreedandthereisaviabledeliveryagency),whichhavenotbeendevelopedintheprevious3phasesoftheprogramme.
January–June2016■ Startup(planning,negotiatinglicenses,training,baselineevaluationand
recruitment)phaseofphase4earlyinterventionprogrammes
■ EarlyInterventionsteeringgrouptodiscussannualearlyinterventionreportfromResurgam
July–December2016■ Startdeliveringagreedphase4earlyinterventionprogrammes
■ Considerthe3yearevaluationreport(3yearsofphase1;2yearsofphase2;and1yearofphase3)
■ ReviewthegovernanceoftheEarlyInterventionLisburninitiativeandagreeactionstofurtherimprovethem
January–June2018■ EarlyInterventionConsortiumandResurgamtodiscussannualearly
interventionreportfromtheDeliveryPartner
July–December2017■ Considerthe4yearevaluationreport(4yearsofphase1;3yearsofphase2;2
yearsofphase3;and1yearofphase4)
January–June2018■ EarlyInterventionConsortiumandResurgamtodiscussannualearly
interventionreportfromtheDeliveryPartner
July–December2018■ Considerthe5yearevaluationreport(5yearsofphase1;4yearsofphase2;3
yearsofphase3;and2yearsofphase4)

Page 108
Bibliography – Public Policy/Strategy
Children&YoungPerson’sStrategicPartnershipLocalityOutcomeMonitoringSEHSCTArea2005-2010CYPSP
PrioritiestoinformtheActionPlanfortheSouthEasternAreaConsultationDocumentJanuary2012SouthEasternOutcomesGroupCYPSP
South-EasternOutcomesGroupOutcomesIndicators(accessedMay2012)
DepartmentofEducationNIBenchmarkingDataPrimarySchools2008/9DepartmentofEducationNI
Count, Read: Succeed - A Strategy to Improve Outcomes in Literacy and Numeracy (March2011)DepartmentofEducationNI
DENIResponseto“ACallforAction”reportintoEducationalDisadvantageandtheProtestantWorkingClass
Extended Schools – schools, families, communities – working together(2006)DepartmentofEducationNI
Extended Schools – Building on Good PracticeDENI(November2010)CircularNumber2010/21
An Evaluation of Extended Schools(May2009)ETI/DENI
Every School a Good School – a policy for school improvement(April2009)DENI
InCASArrangementsforAutumn2011CircularNumber20011/1530/7/11DepartmentofEducationNI
KeyStageOneAssessmentsforschoolsintheLisburndistrictcouncil2010/11
KeyStageTwoAssessmentsforschoolsintheLisburndistrictcouncil2010/11
DepartmentofEducation(England&Wales)Munro,E.(May2011)The Munro Review of Child ProtectionFinalReportaChild-CentredSystemDepartmentofEducation
DepartmentofHealth,SocialServices&PublicSafety
Addressing Young People’s Drinking in Northern Ireland – action to support the new Strategic Direction for Alcohol and Drugs(June2009)DHSSPS

Page 109
Delivering the Bamford Vision–theresponseoftheNorthernIrelandExecutivetotheBamfordReviewofmentalHealthandLearningDisabilityActionPlan2009-2011(October2009)DHSSPS
Families Matter: Supporting families in Northern Ireland–regionalfamilyandparentingstrategy(March2009)DHSSPS
A Healthier Future-atwentyyearvisionforhealthandwellbeinginNorthernIreland2005-2015DHSSPS
Healthy Child, Healthy Future–aframeworkfortheUniversalChildHealthPromotionProgrammeinNorthernIreland–pregnancyto19years(May2010)DHSSPS
Draft Maternity Strategy for Northern Ireland(2011)DHSSPS
Myths & Reality – teenage pregnancy and parenthood(November2000)DHSSPS
New Strategic Direction for Alcohol and Drugs Phase 2 2011-2016 –aconsultationdocumentJanuary2011DHSSPS
Protect Life-aSharedVision–TheNISuicidePreventionStrategyandActionPlan2006-2011(October2006)DHSSPS
Regional Hidden Harm Action Plan–respondingtotheneedsofchildrenborntoandlivingwithparentalalcoholanddrugmisuseinNorthernIreland(October2008)DHSSPS
Sexual Health Promotion strategy and action plan 2008-2013(November2008)DHSSPS
DepartmentofHealth(England&Wales)Marmot,M.(February2010)Fair Society, Healthy LivesDepartmentofHealth
DepartmentofJusticeNIBuilding Safer, Shared and Confident Communities-aconsultationonanewcommunitysafetystrategyforNorthernIreland(January2011)DepartmentofJusticeNI
Draft Strategic Framework for Reducing OffendingDepartmentofJustice

Page 110
Strategic Framework for Reducing Offending – Evidence-base(March2012)DepartmentofJustice
DepartmentofSocialDevelopmentPeople and Place – a strategy for neighbourhood renewal(2003)DSD
DSD Corporate Plan 2008-2011 Together, tackling disadvantage, building communities-astrategyforneighbourhoodrenewal(2008)DSD
EqualityCommissionEvery Child an Equal Child-AnEqualityCommissionStatementonkeyInequalitiesinEducationandaStrategyforInterventionNovember20087EqualityCommission
HousingExecutiveLisburnHousing&RegenerationStrategy2007/08-2011/12HousingExecutive
NICCYWill the draft Northern Ireland Programme for Government deliver on children’s rights and best interests? an analysis(February2012)NICCY
NorthernIrelandAssemblyProgrammeforGovernmentpre-schoolcommitmentResearch&InformationServiceBriefingpaper(February2012)NIAssembly
FreeSchoolMealEntitlementasameasureofdeprivationResearch&InformationServiceBriefingpaper191/10November2010NIAssembly
NorthernIrelandExecutiveProgrammeforGovernmentBuildingaBetterFuture2011-15NorthernIrelandExecutive
Investing for Health(March2002)NorthernIrelandExecutive
NorthernIrelandOfficeOur Children and Young People – Our PledgeatenyearstrategyforchildrenandyoungpeopleinNorthernIreland2006-2016(2006)
OFMDFMSocialInvestmentFundConsultationPaper(September2011)OFMDFM
Bibliography – Public Policy/Strategy

Page 111
PublicHealthAgencyCommunity Development Health & Social - Wellbeing Improvement Thematic Action Plan 2011-2012 (Draft13)(November2011)PublicHealthAgency
HSCCommissionerSpecificationHealth&SocialWellbeingImprovementMarch2012PublicHealthAgency
PublicHealthAgencyCorporateStrategy2011-2015Realisingthehealthandwellbeingpotentialofpeople(2011)PublicHealthAgency
SouthEasternEducation&LibraryBoardNeedsAssessmentofYoungPeopleinLisburnCityCouncilArea(undated)SEELB
ThreeYearDevelopmentPlan2012/15SEELBYouthServiceLisburnDivision
SouthEasternHealthandSocialCareTrustHealth Inequality Action Plan for the South Eastern Trust Area 2011/12(2011)SEHSCT
NewParentProject(undatedguidancedocument)SEHSCT
YouthJusticeAgencyYouthJusticeAgencyBusinessPlan2011-2012
Bibliography-ResearchAllen,G.(2011)Early Intervention – the Next StepsDepartmentofWork&Pensions
Allen,GandDuncanSmith,I..(2008)EarlyIntervention:Goodparents,GreatKids,BetterCitizens
Bellenge,F.X.G(Fall2002)Measuring the Cost of Reading Recovery: A Practical ApproachJournalofReadingRecovery
Chowdry,H.,Crawford,C.,Dearden,L.,Joyce,R.,Sibieta,L.,Sylva,K.andWashbrook,E.(March2010)PoorerChildren’sEducationalAttainment:HowImportantareAttitudesandBehaviour?JosephRowntreeFoundation
Heckman,J.J.andMasterov,D.V.(October2004)The Productivity Argument for Investing in Young ChildrenNCSL

Page 112
Horgan,G.,Monteith,M.WhatcanwedototacklechildpovertyinNorthernIreland(November2009)SavetheChildrenFund/JosephRowntreeFoundation
Murphy,T.andGuerin,S(2012)How are our FamiliesChildhoodDevelopmentInitiative
Murphy,A.,Murphy,T.andSmith,M.(2011)Quality Services, Better Outcomes – a Quality Framework for Achieving OutcomesChildhoodDevelopmentInitiative
NINISWardandSOAprofiles(lastupdatedOctober2011)NISRA
Purvis,D.(March2011)A Call for ActionreportintoEducationalDisadvantageandtheProtestantWorkingClassDawnPurvisMLA
Sullivan,A.,Cara,O.,Joshi,H.,Ketende,S.andObolenskaya,P.The Consequences of Childhood Disadvantage in Northern Ireland at age 5 – a report to the NIO and OFMDFM(June2010)InstituteofEducationLondon
Growing Up in Ireland–HowfamiliesmatterforSocialandEmotionalOutcomesof9-yearOldChildrenReport4
TheImpactofSureStartLocalProgrammesonfiveyearoldsandtheirfamilies(November2010)NationalEvaluationofSureStart(NESS)TeamResearchBrief
Grasping the Nettle-earlyinterventionforchildren,familiesandcommunities(undated)C4EO2009
Goodman,A.andGregg,P.Educational Disadvantaged – how important are attitudes and behaviour?(March2010)JosephRowntreeFoundation
Bibliography-OtherHandbookofProgrammes(October2011)ColinEarlyInterventionCommunity
OutcomesfortheColinAreaOctober2011ColinEarlyInterventionCommunity
ReportforEasternChildcarePartnershiptoascertainneedsandpossiblestructureofaLisburnCentralSureStart(March2012)ResurgamCommunityDevelopmentTrust
ResurgamTrustStrategicPlan2010-2015(2010)ResurgamDevelopmentTrust
Bibliography – Public Policy/Strategy

Page 113
AComparisonoftheNewParentProjectwithotherhomevisitingprogrammes(February2009)NCBNI
EarlyYearsAllianceEarlyYearsManifesto(undated)EarlyYearsStrategicAlliance

Page 114
APPENDIX ONE
Terms of Reference for the developmentof a detailed model of delivery for Early Intervention Lisburn
BackgroundResurgumDevelopmentTrusthasdevelopedtheconceptofanEarlyInterventionLocalitywithinLisburninordertomeetarangeofdisproportionatelypooroutcomesforchildrenandfamiliesintheLisburnarea.Todevelopthisconceptfurther,ResurgumandthePublicHealthAgencyhavecommissionedBarnadostodeliverspecificdeliverableswhichwillhelptakethisinitaiveforward.Barnadosarealsocontributingfundingtothisprojectinaspiritofcollaborationandhaveallocatedanexperiencedconsultanttooperationallyleadthisworkontheirbehalf.
TimescaleAlldeliverablesshouldbecompletedby31stMay,2012
DeliverablesThemaindeliverablefromthispieceofworkwillbeasinglereporttitled‘TheDevelopmentofanEarlyInterventionLocalitywithinLisburn’.Withinthisreport,severaldistinctelementswillbecovered,asdetailedbelow:
1. TheCaseforChange:thissectionwillarticulatewhyanearlyinterventioninitiativeisrequiredinLisburn.ItwoulddetailoutcomesforchildrenlivingwithinthemostdeprivedestateswithinLisburn,especiallyOldWarren,HillhallandTonagh(althoughitwillalsocoverotherestates)andhowthesecomparewithotherareasinNorthernIreland.ThissectionwillalsodetailthespecificneedswithinLisburn,thecurrentservicesinplace,thegapsandthepotentialoverlapsbetweencurrentservices.
2. SharedOutcomesandPrinciples:ThiskeysectionwillarticulatethesharedOUTCOMESandPRINCIPLESthatallstakeholdersinEarlyInterventionLisburnhavesignedupto.Obviously,togettothispoint,engagementwithcommunity,statutory(includingschools)andvoluntarypartnerswillneedtotakeplace.Thisengagementshouldincludeallkeystakeholdersandshouldbefullyinclusivefromanearlystage.TheengagementprocesswillneedtobedesignedandimplementedtoensuretheviewsofallkeystakeholdersareincludedandthatagreementisreachedbetweenallpartnersastowhichsharedoutcomesandprinciplesshouldunderpinthedevelopmentofEarlyInterventionLisburn.
3. Whatworks–aglobalreviewofevidence:UsingtheOutcomesagreedinsection2,thissectionwilldetailthetypesofprogrammesandpracticeswhichhavebeenproventodelivertheexpectedOutcomese.g.improvedadolescentmentalhealth,reducedteenagedrinking,kidsmorereadyforschoolinP.1,improvedschoolattendanceorbetteracademicachievementetcetc.

Page 115
4. DesignofanintegratedmodelofdeliveryforEarlyInterventionLisburn(EIL):ThiselementwilltakeallthelearningfromtheprevioussectionsandwilldesignasuiteofinterventionswhichcollectivelywillenableEILtoachievetheOutcomesidentifiedinsection2.Thus,eachinterventionwillbeclearlylinkedtospecificOutcomes.Inaddition,clearperformanceindicatorswillbeidentifiedtoensurethatprogresstowardsspecificoutcomescanbemeasurede.g.GCSEresultsforanoutcomeofbetteracademicachievement.Thissectionwillalsoprovideanestimatefortheoverallprojectedcostoftheprogramme.ThiscostshouldincludetherecruitmentbyResurgumofanoverallEILProgrammeManagertooverseetheimplementationoftheEILinitiative.Thissectionwillnotdetailpotentialprovidersbutmayprovideexamplesofwherespecificprogrammeshavebeenproventomakeameasurabledifferenceinotherareas.
5. RoleofResurgumasprogrammeowners:ThissectionwillprovidebackgroundinformationaboutResurgumandwilllayouttherationaleforResurgumtakingresponsibility,asaleadingcommunityorganisationinLisburn,forthedeliveryoftheEarlyInterventionLisburninitiative.SpecificelementsoftheroleofResurgummayinclude:
a. Responsibilityforfinancialmanagementb. Responsibilityforidentifyingandsourcing,viatendering,thebest
providersforeachinterventionc. Monitoringtheperformanceagainstspecificindicatorsfortheoverall
programmeinrelationtoeachOutcomed. Reportingprogresstofunderse. Qualityassuranceofthedeliveryoftheoverallprogramme
6. ImplementationPlan:Thisshortsectionwilloutlinethenextstepsintermsofmovingtowardsimplementationsuchasdesigningadetailedspecificationforeachintervention,leadingtotenderdocumentationandtherecruitmentbyResurgumofanoverallEILProgrammeManager.

Page 116
APPENDIX TWO
Membership of the Early Intervention Lisburn Steering Group:
AdieBird(Chair)DenisPaisleyJasonWhiteAnneHardyMabelScullionCarolineMcGrathIanSutherlandJonathonCraigMartinDevlinNeilMcGivernMonicaMcCannPaulPorterUnaGeelanPaulGivanFrancisFerris

Page 117
APPENDIX THREE
Descriptions of Recommended Early Intervention Programmes
MultisystemicTherapy
BigBrothersBigSisters
FunctionalFamilyTherapy
LifeSkillsTraining
FamilyNursePartnerships
PATHS(PromotingAlternativeThinkingStrategies)
IncredibleYears
TripleP–PositiveParenting
Parent-ChildHome
ReadingRecovery
Parent-ChildInteractionTherapy
FathersReadingEveryDay(FRED)
TimetoRead

Page 118
MULTISYSTEMICTHERAPY(MST)
ProgramSummaryMultisystemicTherapy(MST)isanintensivefamily-andcommunity-basedtreatmentthataddressesthemultipledeterminantsofseriousantisocialbehaviorinjuvenileoffenders.Themultisystemicapproachviewsindividualsasbeingnestedwithinacomplexnetworkofinterconnectedsystemsthatencompassindividual,family,andextrafamilial(peer,school,neighborhood)factors.Interventionmaybenecessaryinanyoneoracombinationofthesesystems.
ProgramTargetsMSTtargetschronic,violent,orsubstanceabusingmaleorfemalejuvenileoffenders,ages12to17,athighriskofout-of-homeplacement,andtheoffenders’families.
ProgramContentMSTaddressesthemultiplefactorsknowntoberelatedtodelinquencyacrossthekeysettings,orsystems,withinwhichyouthareembedded.MSTstrivestopromotebehaviorchangeintheyouth’snaturalenvironment,usingthestrengthsofeachsystem(e.g.,family,peers,school,neighborhood,indigenoussupportnetwork)tofacilitatechange.
ThemajorgoalofMSTistoempowerparentswiththeskillsandresourcesneededtoindependentlyaddressthedifficultiesthatariseinraisingteenagersandtoempoweryouthtocopewithfamily,peer,school,andneighborhoodproblems.Withinacontextofsupportandskillbuilding,thetherapistplacesdevelopmentallyappropriatedemandsontheadolescentandfamilyforresponsiblebehavior.Interventionstrategiesareintegratedintoasocialecologicalcontextandincludestrategicfamilytherapy,structuralfamilytherapy,behavioralparenttraining,andcognitivebehaviortherapies.
MSTisprovidedusingahome-basedmodelofservicesdelivery.Thismodelhelpstoovercomebarrierstoserviceaccess,increasesfamilyretentionintreatment,allowsfortheprovisionofintensiveservices(i.e.,therapistshavelowcaseloads),andenhancesthemaintenanceoftreatmentgains.TheusualdurationofMSTtreatmentisapproximately60hoursofcontactoverfourmonths,butfrequencyanddurationofsessionsaredeterminedbyfamilyneed.
ProgramOutcomesEvaluationsofMSThavedemonstratedforseriousjuvenileoffenders:
■ reductionsof25-70%inlong-termratesofrearrest,
APPENDIX THREE
Descriptions of Recommended Early Intervention Programmes

Page 119
■ reductionsof47-64%inout-of-homeplacements,■ extensiveimprovementsinfamilyfunctioning,and■ decreasedmentalhealthproblemsforseriousjuvenileoffenders.
ProgramCostsMSThasachievedfavorableoutcomesatcostsavingincomparisonwithusualmentalhealthandjuvenilejusticeservices,suchasincarcerationandresidentialtreatment.Atacostof$4,500peryouth,arecentpolicyreportconcludedthatMSTwasthemostcost-effectiveofawiderangeofinterventionprogramsaimedatseriousjuvenileoffenders.
ProgramBackgroundMultisystemicTherapy(MST)wasdevelopedinthelate1970s.Itaddressesseverallimitationsofexistingmentalhealthservicesforseriousjuvenileoffenderswhichincludeminimaleffectiveness,lowaccountabilityofserviceprovidersforoutcomes,andhighcost.
Treatmentefforts,ingeneral,havefailedtoaddressthecomplexityofyouthneeds,beingindividually-oriented,narrowlyfocused,anddeliveredinsettingsthatbearlittlerelationtotheproblemsbeingaddressed(e.g.,residentialtreatmentcenters,outpatientclinics).Givenoverwhelmingempiricalevidencethatseriousantisocialbehaviorisdeterminedbytheinterplayofindividual,family,peer,school,andneighborhoodfactors,itisnotsurprisingthattreatmentsofseriousantisocialbehaviorhavebeenlargelyineffective.Restrictiveout-of-homeplacements,suchasresidentialtreatment,psychiatrichospitalization,andincarceration,failtoaddresstheknowndeterminantsofseriousantisocialbehaviorandfailtoalterthenaturalecologytowhichtheyouthwilleventuallyreturn.Furthermore,mentalhealthandjuvenilejusticeauthoritieshavehadvirtuallynoaccountabilityforoutcome,asituationthatdoesnotenhanceperformance.Theineffectivenessofout-of-homeplacement,coupledwithextremelyhighcosts,haveledmanyyouthadvocatestosearchforviablealternatives.MSTisonetreatmentmodelthathasawell-documentedcapacitytoaddresstheaforementioneddifficultiesinprovidingeffectiveservicesforjuvenileoffenders.
TheoreticalRationale/ConceptualFrameworkConsistentwithsocial-ecologicalmodelsofbehaviorandfindingsfromcausalmodelingstudiesofdelinquencyanddruguse,MSTpositsthatyouthantisocialbehaviorismultideterminedandlinkedwithcharacteristicsoftheindividualyouthandhisorherfamily,peergroup,school,andcommunitycontexts.Assuch,MSTinterventionsaimtoattenuateriskfactorsbybuildingyouthandfamilystrengths(protectivefactors)onahighlyindividualizedandcomprehensivebasis.Theprovisionofhome-basedservicescircumventsbarrierstoserviceaccessthat

Page 120
oftencharacterizefamiliesofseriousjuvenileoffenders.Anemphasisonparentalempowermenttomodifythenaturalsocialnetworkoftheirchildrenfacilitatesthemaintenanceandgeneralizationoftreatmentgains.
BriefDescriptionofInterventionMSTisapragmaticandgoal-orientedtreatmentthatspecificallytargetsthosefactorsineachyouth’ssocialnetworkthatarecontributingtohisorherantisocialbehavior.Thus,MSTinterventionstypicallyaimto:■ improvecaregiverdisciplinepractices;■ enhancefamilyaffectiverelations;■ decreaseyouthassociationwithdeviantpeers;■ increaseyouthassociationwithprosocialpeers;■ improveyouthschoolorvocationalperformance;■ engageyouthinprosocialrecreationaloutlets;and■ developanindigenoussupportnetworkofextendedfamily,neighbors,and
friendstohelpcaregiversachieveandmaintainsuchchanges.
Specifictreatmenttechniquesusedtofacilitatethesegainsareintegratedfromthosetherapiesthathavethemostempiricalsupport,includingcognitivebehavioral,behavioral,andthepragmaticfamilytherapies.
MSTservicesaredeliveredinthenaturalenvironment(e.g.,home,school,andcommunity).Thetreatmentplanisdesignedincollaborationwithfamilymembersandis,therefore,familydrivenratherthantherapistdriven.TheultimategoalofMSTistoempowerfamiliestobuildanenvironment,throughthemobilizationofindigenouschild,family,andcommunityresources,thatpromoteshealth.Thetypicaldurationofhome-basedMSTservicesisapproximatelyfourmonths,withmultipletherapist-familycontactsoccurringeachweek,determinedbyfamilyneed.
AlthoughMSTisafamily-basedtreatmentmodelthathassimilaritieswithotherfamilytherapyapproaches,severalsubstantivedifferencesareevident:
1. MSTplacesconsiderableattentiononfactorsintheadolescentandfamily’ssocialnetworksthatarelinkedwithantisocialbehavior.Hence,forexample,MSTprioritiesincluderemovingoffendersfromdeviantpeergroups,enhancingschoolorvocationalperformance,anddevelopinganindigenoussupportnetworkforthefamilytomaintaintherapeuticgains.MSTprogramshaveanextremelystrongcommitmenttoremovingbarrierstoserviceaccess(e.g.,thehome-basedmodelofservicedelivery).
2. MSTservicesaremoreintensivethantraditionalfamilytherapies(e.g.,severalhoursoftreatmentperweekvs.50minutes).
3. Mostimportantly,MSThaswell-documentedlong-termoutcomeswith
APPENDIX THREE
Descriptions of Recommended Early Intervention Programmes

Page 121
adolescentspresentingseriousantisocialbehaviorandtheadolescents’families.
ThestrongestandmostconsistentsupportfortheeffectivenessofMSTcomesfromcontrolledstudiesthatfocusedonviolentandchronicjuvenileoffenders.Importantly,resultsfromthesestudiesshowedthatMSToutcomesweresimilarforyouthacrosstheadolescentagerange(i.e.,12-17years),formalesandfemales,andforAfricanAmericanaswellasWhiteyouthandfamilies.
EvidenceofProgramEffectivenessThefirstcontrolledstudyofMSTwithjuvenileoffenderswaspublishedin1986,andthreerandomizedclinicaltrialswithviolentandchronicjuvenileoffendershavebeenconductedsincethen.Inthesetrials,MSThasdemonstratedlong-termreductionsincriminalactivity,drug-relatedarrests,violentoffenses,andincarceration.Thissuccesshasledtoseveralrandomizedtrialsandquasi-experimentalstudiesaimedatextendingtheeffectivenessofMSTtootherpopulationsofyouthpresentingseriousclinicalproblemsandtheirfamilies.
Theinformationforthisfactsheetwasexcerptedfrom:
Henggeler,S.W.,Mihalic,S.F.,Rone,L.,Thomas,C.,&Timmons-Mitchell,J.(1998).BlueprintsforViolencePrevention,BookSix:MultisystemicTherapy.Boulder,CO:CenterfortheStudyandPreventionofViolence.

Page 122
BIGBROTHERSBIGSISTERSOFAMERICA(BBBSA)
ProgramSummaryBigBrothersBigSistersofAmerica(BBBSA)hasbeenprovidingadultsupportandfriendshiptoyouthfornearlyacentury.Areportin1991demonstratesthatthroughBBBSA’snetworkofnearly500agenciesacrossthecountry,morethan70,000youthandadultsweresupervisedinone-to-onerelationships.
ProgramTargetsBBBSAtypicallytargetsyouth(aged6to18)fromsingleparenthomes.
ProgramContentServicedeliveryisbyvolunteerswhointeractregularlywithayouthinaone-to-onerelationship.Agenciesuseacasemanagementapproach,followingthroughoneachcasefrominitialinquirythroughclosure.Thecasemanagerscreensapplicants,makesandsupervisesthematches,andclosesthematcheswheneligibilityrequirementsarenolongermetoreitherpartydecidestheycannolongerparticipatefullyintherelationship.
BBBSAdistinguishesitselffromothermentoringprogramsviarigorouspublishedstandardsandrequiredprocedures:
■ Orientationisrequiredforallvolunteers.■ VolunteerScreeningincludesawrittenapplication,abackgroundcheck,an
extensiveinterview,andahomeassessment;itisdesignedtoscreenoutthosewhomayinflictpsychologicalorphysicalharm,lackthecapacitytoformacaringbondwiththechild,orareunlikelytohonortheirtimecommitments.
■ YouthAssessmentinvolvesawrittenapplication,interviewswiththechildandtheparent,andahomeassessment;itisdesignedtohelpthecaseworkerlearnaboutthechildinordertomakethebestpossiblematch,andalsotosecureparentalpermission.
■ Matchesarecarefullyconsideredandbasedupontheneedsoftheyouth,abilitiesofvolunteers,preferencesoftheparent,andthecapacityofprogramstaff.
■ Supervisionisaccomplishedviaaninitialcontactwiththeparent,youth,andvolunteerwithintwoweeksofthematch;monthlytelephonecontactwiththevolunteer,parentand/oryouthduringthefirstyear;andquarterlycontactwithallpartiesduringthedurationofthematch.
ProgramOutcomesAnevaluationoftheBBBSAprogramhasbeenconductedtoassesschildrenwhoparticipatedinBBBSAcomparedtotheirnon-participatingpeers.Afteraneighteenmonthperiod,BBBSAyouth:
APPENDIX THREE
Descriptions of Recommended Early Intervention Programmes

Page 123
■ were46%lesslikelythancontrolyouthtoinitiatedruguseduringthestudyperiod.
■ were27%lesslikelytoinitiatealcoholusethancontrolyouth.■ werealmostone-thirdlesslikelythancontrolyouthtohitsomeone.■ werebetterthancontrolyouthinacademicbehavior,attitudes,andperformance.■ weremorelikelytohavehigherqualityrelationshipswiththeirparentsor
guardiansthancontrolyouth.■ weremorelikelytohavehigherqualityrelationshipswiththeirpeersattheend
ofthestudyperiodthandidcontrolyouth.
ProgramCostsThenationalaveragecostofmakingandsupportingamatchrelationshipis$1,000(£627)peryear.
ProgramBackgroundBigSistersactivitywasinitiatedin1902,whenagroupofwomeninNewYorkCitybeganbefriendinggirlswhocamebeforetheNewYorkChildren’sCourt.KnownthenastheLadiesofCharity,thegrouplaterbecameCatholicBigSistersofNewYork.AstoryintheNewYorkTimesin1902reportedthatajudgeoftheNewYorkChildren’sCourtsecuredpromisesfromagroupofinfluentialmenthateachonewouldbefriendoneboywhohadbeenbeforehiscourt.Hisactivitycouldhaveinfluencedamemberofhiscourt,ClerkErnestK.Coulter,whoiscreditedwithfoundingtheorganizedBigBrothersMovementin1904.ACincinnatibusinessman,IrvinF.Westheimer,andamemberofacloselyknit,charity-mindedJewishcommunity,urgedhisfriendsandbusinessassociatestobefriendtroubledanddisadvantagedyouths,whicheventuallyledtotheorganizationofaBigBrothersagencyinCincinnatiin1910.
BeforeWorldWarI,theBigBrothersandBigSistersMovementwascharacterizedbymanyformsoforganization,underavarietyofsponsors,utilizinganumberofapproaches.Butalloftheeffortswereunitedbyasinglespirit—adesiretohelpchildren,generallyfromone-parenthomes,whosemoral,mental,andphysicaldevelopmentwasendangeredbytheirenvironmentsandbackgrounds.By1922,“standards”(i.e.,basicrequirements)werecreatedandadopted.Theseearlystandardsaddressedtheone-to-onerelationshipasavolunteer’sindividualandpersonaleffortinbehalfofchildren,andassertedtheneedforanagencytomanageitsaffairsinaprofessionalmanner.Bytheearly1930s,thestandardshadbecomemorestringentinsettingforthminimumrequirementsforoperationatthelocallevel.
Inthemid-1930s,theGreatDepressionaffectedtheBigBrothersandBigSistersFederation,andby1937thenationalofficecloseditsdoors,whilelocalagencies

Page 124
continuedtooperate.FollowingWorldWarII,anewfederationwasestablishedonlyforBigBrothersagencies.Outofaconvictionthatwomencouldhelpmeettheneedsofgirls,BigSistersInternationalwascreatedbytheBigSistersagenciesthenoperatingin1970.In1977,BigSistersInternationalandBigBrothersofAmericamergedtobecomeBigBrothersBigSistersofAmerica(BBBSA).
EffortsfocusedonthedevelopmentandpilotingofasetofStandardsandRequiredProceduresforOne-To-OneService(BigBrothersBigSistersofAmerica,1986;asamended,1996),whichwereadoptedin1986.Thisconsistsofcorporatemanagementandprogrammanagementstandards,witheachstandardhavingasetofrequiredproceduresthatweredeemednecessarytofulfilleachstandard.CompliancewiththesestandardsandrequiredproceduresbecamethehallmarkofaneffectiveBigBrothersBigSisters(BBBS)agencyandthebasisforbuildingaconsistentone-to-oneserviceofover500BBBSagenciesacrossall50states.AdescriptionofmanualspublishedbyBBBSAcanbefoundinAppendixB.
Duringmorethan85yearsofnationalorganizationaldevelopmentandlocalizedservicedelivery,theword“mentoring”wasnotapartofthemovement’snomenclature.Infact,itwasnotuntilthelate1980s,whenfundersandresearchersdeterminedthatmentoringmaybeapromisingapproachforchildrenat-risk,thatthewordmentoringfounditswayintotheBBBSA’srhetoricfordescribingtheirservice.TherewasastronginclinationonthepartoflocalBBBSagencies,however,tonotconfuseBBBSA’ssystematicandstructuredvolunteerapproachwiththemorelooselyfashionedmentoringprogramsthatwerebeingdeveloped.Mentoringhasvariousdefinitions,dependingontheemphasisthataparticularcommunityyouthprogramhasasitsgoal.“Mentoring”isoftenusedinterchangeablywith“tutoring,”andsometimes,withthegoalofapprenticeship.Mentoringtendstobeanadd-ontoprogramsthathaveveryspecificgoalsandobjectives,withmentoringbeingseenasonlyoneofmanyingredients.Historically,mentoringhashadahelping-to-learnaspecttoit;forexample,anolderpersonguidingayoungerperson,usuallyaroundsomeprescribedactivityoraspectoflife.BigBrothersBigSisterswork,however,focusesonfriendshipastheprimaryaspectoftherelationship,whichshouldleadtoafeelingoftrustovertime,andwhichthenmayleadtosomeaspectsoflearning,regardlessofthesubjectorbehavior.Buttherelationship—thetrust,themutuallysharedexperiencesofeverydaylife—istheessenceoftheservice.Whilethewordmentoringisnowused,forthemostpart,interchangeablywithBigBrothersBigSisters,BBBSA’semphasiscontinuestobeonthequalityoftherelationshipbetweenthevolunteerandthechild,andnotonasetofprescribedactivities.
APPENDIX THREE
Descriptions of Recommended Early Intervention Programmes

Page 125
TheoreticalRationale/ConceptualFrameworkAlthoughBBBSAwasnotdevelopedwithacademictheoriesofdelinquencyinmind,theproject’srationalemostcloselyresemblessocialcontroltheory.Accordingtothisperspective,attachmentstoprosocialothers,commitmenttosociallyappropriategoals,andinvolvementinconventionalactivitiesrestrainyouthfromengagingindelinquentactivitiesorotherproblembehaviors,becausemoresociallybondedyouthhavemoretolosebymisbehavior.
TherationalethathasguidedBBBSAservicefornearlyacenturyhasbeenthattheconsistentpresenceofanon-familialcaringadultcanmakeadifferenceinthesocial/emotionaldevelopmentofachildoryoungperson,particularlyonegrowingupinasingleparentfamilyorinanadversesituation.OvertheyearsthedevelopmentoftheBBBSservicehasbeenbasedontheoverridingbeliefthataconsistentandfrequentvolunteercontactisapowerfulinfluence.Thisbeliefhasbeenbased,predominantly,onanecdotalreportsfromparents,teachers,casemanagers,andchildrenthemselves.
ThemostrelevantresearchtodatehascomefromtheresiliencystudiescarriedoutbyresearcherssuchasEmmyWerner,andothers,undertherubricof“caringadults.”Werner,ina30yearlongitudinalstudyontheislandofKauai,hasfoundthatthenumberofcaringadultsoutsidethefamilywithwhomthechildlikedtoassociatewasasignificantprotectivefactorforbothhighriskboysandgirlswhomadeasuccessfultransitionintoadulthood.Basedonsuchresearch,BBBSAcontinuesitsgeneralizedapproachandconcentratesonenhancingtheinfrastructuretosupportthedevelopmentandmaintenanceoftherelationshipbetweenthevolunteerandchild.
BriefDescriptionofInterventionBBBSisacommunitymentoringprogramwhichmatchesanadultvolunteer,knownasaBigBrotherorBigSister,toachild,knownasaLittleBrotherorLittleSister,withtheexpectationthatacaringandsupportiverelationshipwilldevelop.Hence,thematchbetweenvolunteerandchildisthemostimportantcomponentoftheintervention.Equallyimportant,however,isthesupportofthatmatchbytheongoingsupervisionandmonitoringofthematchrelationshipbyaprofessionalstaffmember.Theprofessionalstaffmemberselects,matches,monitors,andclosestherelationshipwiththevolunteerandchild,andcommunicateswiththevolunteer,parent/guardian,andthechildthroughoutthematchedrelationship.
Inpractice,thevolunteerinterventioninthetraditionalone-to-onerelationshipwithachildisthreetofivehoursperweek,onaweeklybasis,overthecourseofayearorlonger.Thegeneralizedactivityofthatrelationshipisrelatedtothegoalsthatweresetinitiallywhenthematchwasestablished.Thesegoalsareidentified

Page 126
fromtheextensivecasemanagerinterviewheldwiththeparent/guardianandwiththechild.Theforemostgoalusuallysetistodeveloparelationship—onethatismutuallysatisfying,wherebothpartiescometogetherfreelyonaregularbasis.Morespecificgoalsmightrelatetoschoolattendance,academicperformance,relationshipswithotherchildrenandsiblings,generalhygiene,learningnewskillsordevelopingahobby.Thegoalsestablishedforaspecificmatcharedevelopedintoanindividualizedcaseplan,whichisupdatedbythecasemanagerasprogressismadeandcircumstanceschangeovertime.
Generallyspeaking,BBBSagencystaffdonottellavolunteerspecificallywhatactivitiestoengageinwiththechildduringtheirtimetogether,buttheyguidethevolunteerandmakesuggestionsofpossibleactivitiesandapproaches,basedonthechild’sandvolunteer’sinterestsandneeds.Consistencyintherelationshipovertimeisahigherprioritythanthetypesofactivitiesinwhichtheyparticipate.Oncethematchhasbeeninitiallyagreedupon,inthepresenceofthechild,volunteer,andthechild’sparent/guardian,itisthentheresponsibilityoftheprofessionalstaffmember,knownasthecasemanager,tomaintainon-goingcontactwithallpartiesinthematchrelationship.
TheStandardsandRequiredProceduresforOne-To-OneServiceoutlinesthescheduleofcontactsthecasemanageristohavewiththevolunteer,aswellaswiththeparentand/orchild.Thereistobemorefrequentcontactduringtheearlystagesofthematchwithaninitialcontactwithintwoweeksofmakingthematch,thenmonthlycontactthroughouttherestoftheyear,andthencontacteverythreemonthsafterthefirstyearandthroughoutthedurationofthematch.Thecasemanagercallsthevolunteerandtheparentafterthefirstandsecondweekoftherelationshiptodeterminehowtherelationshipisdeveloping,andmaycontinueonaweeklybasisthroughthefirstsixweeks,dependingonthesituation.However,iteventuallydevelopsintoamonthlycontactwiththevolunteerandtheparent.
Atleastquarterly,thecasemanagerisintouchwiththechildtolearnoftheyouth’sexperiences.Thesesupervisorycontactsinformthecasemanagerhowtherelationshipisdevelopingandprovideanopportunitytogiveadviceandguidancearoundanyissuesthevolunteermighthave,aswellastoencourageandsupportvariousactivities.Formostagencies,theon-goingcasemanagersupervisionwiththevolunteertakesplaceoverthephone.Thecasemanageristoassessthematchgoalsonanannualbasisandmakeappropriateadjustmentstothecaseplan.
EvidenceofProgramEffectivenessIncontrasttopriorresearchonmentoringprogramswhichhasfailedtodemonstratetheeffectivenessofthoseprograms,researchconductedbyPublic/PrivateVentures(P/PV)ontheBBBSmodelprovidesclearevidencethatacaring
APPENDIX THREE
Descriptions of Recommended Early Intervention Programmes

Page 127
relationshipbetweenanadultvolunteerandayoungpersoncanprovideawiderangeoftangiblebenefits.
P/PVconductedacomparativestudyofnearly1,000ten-tosixteen-yearoldsfromeightBBBSagenciesduringtheyears1992-1993.Halfoftheseyoungpeoplewererandomlyassignedtoatreatmentgroup,forwhichBBBSmatchesweremade;theotherhalfwererandomlyassignedtoacontrolgroupandwerenotmatched(thecontrolgroupmemberswereputonawaitinglistfor18months).TheP/PVstudycomparedthesetwogroupsafteran18monthperiodoftime.
Attheconclusionofthe18-monthstudyperiod,itwasfoundthatLittleBrothersandLittleSisters(youthparticipantsintheprogram)werelesslikelytohavestartedusingdrugsoralcohol,werelesslikelytohavehitsomeone,feltmorecompetentaboutdoingschoolwork,attendedschoolmore,gotbettergrades,andhadbetterrelationshipswiththeirparentsandpeersthanthosewhodidnotparticipateintheprogram.
Theinformationforthisfactsheetwasexcerptedfrom:
McGill,D.E.,Mihalic,S.F.,&Grotpeter,J.K.(1998).BlueprintsforViolencePrevention,BookTwo:BigBrothersBigSistersofAmerica.Boulder,CO:CenterfortheStudyandPreventionofViolence.

Page 128
FUNCTIONALFAMILYTHERAPY(FFT)ProgramSummaryFunctionalFamilyTherapy(FFT)isanoutcome-drivenprevention/interventionprogramforyouthwhohavedemonstratedtheentirerangeofmaladaptive,actingoutbehaviorsandrelatedsyndromes.
ProgramTargetsYouth,aged11-18,atriskforand/orpresentingwithdelinquency,violence,substanceuse,ConductDisorder,OppositionalDefiantDisorder,orDisruptiveBehaviorDisorder.Oftentheseyouthpresentwithadditionalcomorbidchallengessuchasdepression.
ProgramContentFFTrequiresasfewas8-15sessionsofdirectservicetimeforcommonlyreferredyouthandtheirfamilies,andgenerallynomorethan26totalsessionsofdirectserviceforthemostsevereproblemsituations.
DeliverymodesFlexibledeliveryofservicebyoneand(rarely)twopersonteamstoclientsin-home,clinic,school,juvenilecourt,communitybasedprograms,andattimeofre-entryfrominstitutionalplacement.
ImplementationWiderangeofinterventionists,includingtrainedprobationofficers,mentalhealthtechnicians,degreedmentalhealthprofessionals(e.g.,M.S.W.,Ph.D.,M.D.,R.N.,M.F.T.,L.C.P.).
FFTeffectivenessderivesfromemphasizingfactorswhichenhanceprotectivefactorsandreducerisk,includingtheriskoftreatmenttermination.Inordertoaccomplishthesechangesinthemosteffectivemanner,FFTisaphasicprogramwithstepswhichbuilduponeachother.Thesephasesconsistof:
■ Engagement,designedtoemphasizewithinyouthandfamilyfactorsthatprotectyouthandfamiliesfromearlyprogramdropout;
■ Motivation,designedtochangemaladaptiveemotionalreactionsandbeliefs,andincreasealliance,trust,hope,andmotivationforlastingchange;
■ Assessment,designedtoclarifyindividual,familysystem,andlargersystemrelationships,especiallytheinterpersonalfunctionsofbehaviorandhowtheyrelatedtochangetechniques;
■ BehaviorChange,whichconsistsofcommunicationtraining,specifictasksandtechnicalaids,basicparentingskills,problemsolvingandconflictmanagementskills,contractingandresponse-costtechniques;and
APPENDIX THREE
Descriptions of Recommended Early Intervention Programmes

Page 129
■ Generalization,duringwhichfamilycasemanagementisguidedbyindividualizedfamilyfunctionalneeds,theirinterfacewithcommunitybasedenvironmentalconstraintsandresources,andthealliancewiththeFFTtherapist/FamilyCaseManager.
ProgramOutcomesClinicaltrialshavedemonstratedthatFFTiscapableof:
■ EffectivelytreatingadolescentswithConductDisorder,OppositionalDefiantDisorder,DisruptiveBehaviorDisorder,alcoholandotherdrugabusedisorders,andwhoaredelinquentand/orviolent;
■ Interruptingthematriculationoftheseadolescentsintomorerestrictive,highercostservices;
■ Reducingtheaccessandpenetrationofothersocialservicesbytheseadolescents;
■ Generatingpositiveoutcomeswiththeentirespectrumofinterventionpersonnel;
■ Preventingfurtherincidenceofthepresentingproblem;■ Preventingyoungerchildreninthefamilyfrompenetratingthesystemofcare;■ Preventingadolescentsfrompenetratingtheadultcriminalsystem;and■ Effectivelytransferringtreatmenteffectsacrosstreatmentsystems.
ProgramCostsThe90-daycostsrangebetween$1,600and$5,000foranaverageof12homevisitsperfamily.Currentcostsvaryandarehighlydependentoncostoflabor.
ProgramBackgroundManytherapiesarenamedtoreflectatheoreticalperspective(e.g.,behavioral,objectrelations)oraprimaryfocus(e.g.,multiplesystems,cognitive).FunctionalFamilyTherapy(FFT)isnamedtoreflectasetofcoretheoreticalprincipleswhichrepresentstheprimaryfocus(family),andanoverridingallegiancetopositiveoutcomeinamodelthatunderstandsbothpositiveandnegativebehaviorasrepresentationsoffamilyrelationalsystems(functional).Thus,FunctionalFamilyTherapyhasadoptedanintegrativestancethatstressesfunctionalityofthefamily,thetherapy,andtheclinicalmodel.
ThedevelopersandreplicatorsofFunctionalFamilyTherapyhaverecognizedthatsolutionsrequireanintegrationofhighqualityscience,testedtheoreticalprinciples,andextensiveclinicalexperienceinpursuitofspecificfunctionalgoalsof:

Page 130
1. Effectivelychangingthemaladaptivebehaviorsofyouthandfamilies,especiallythosewhoattheoutsetmaynotbemotivatedormaynotbelievetheycanchange
2. Reducingthepersonal,societal,andeconomicdevastationthatresultsfromthecontinuationorexacerbationofthevariousdisruptivebehaviordisordersofyouth
3. Doingsowithlesscost,intermsoftimeandmoney,thansomanyofthemoreexpensive(butnotnecessarilyeffective)treatmentscurrentlyavailable.
Unlikeothertherapies,FFTwasnotdevelopedoncollegestudents,neuroticindividuals,orinpatientadults.Instead,FFTgrewoutofaneedtoserveapopulationofat-riskadolescentsandfamiliesthatwereunderserved,hadfewresources,weredifficulttotreat,andwereoftenperceivedbyhelpingprofessionstobetreatmentresistant.Inmanycasesthesefamiliesenteredthe“system”angry,resistant,andunmotivatedtochange.Essentiallythe“helpingprofessions”didnotknowhowtotreatthispopulation.FFTdevelopedoutoftheawarenessthattobesuccessfulintreatmentofthispopulationweneededtobeculturallycompetent,andunderstandwhythisgroupwassotreatmentresistant.Thus,FFTattemptedtodevelopwaystoengagethesefamiliesinordertohelpthemachieveobtainablechangeandbecomemoreadaptableandproductive.Overthelast30years,FFThaslearnedthatitisimportanttodomorethansimplystoppingbadbehaviors.Weknowthatitisimportanttomotivatefamiliestochangeinapositivewaybyuncoveringanddevelopingtheuniquestrengthsofthefamilyinwaysthatenhancethefamilies’self-respectwhileprovidingspecificwaystoimprove.
Sinceitsinceptionin1969,FFThasaccomplisheditsprimarygoalsbyintegratingthemostpromisingtheoreticalperspectives,theempiricaldataavailable,andhoursandhoursofdirectclinicalexperiencewiththetroubledyouthwewantedtohelp.FFTisdesignedtoincreaseefficiency,decreasecosts,andenhanceourabilitytoprovideservicetomoreyouthby:
1. Targetingriskandprotectivefactorsthatwecan,infact,changeandthenprogrammaticallychangingthem;
2. Engagingandmotivatingthefamiliesandyouthsotheyparticipatemoreinthechangeprocess;
3. Enteringeachsessionandphaseofinterventionwithaclearplanandbyusingproventechniquesforimplementation;
4. Constantlymonitoringprocessandoutcomesowedon’tfoolourselvesormakeexcusesforfailure;and
5. Believinginthefamiliesweseeandthenbelievinginourselves.
APPENDIX THREE
Descriptions of Recommended Early Intervention Programmes

Page 131
AtthetimeoftheinceptionofFunctionalFamilyTherapy,themajortheoreticalperspectivesandservicesavailablefortreatingtroubledyouthinafamilycontextwererudimentary,thoughpromising.Earlyon,FFTrepresentedanintegrationofsystemsperspectivesandbehavioraltechniques.ThesystemicbackgroundofFFTemphasizeddynamicandreciprocalprocesseswhichneededtobeidentifiedinreferredfamilies.Thisledtoearlyobservationalresearchontheinteractionsofdelinquentandnon-delinquentfamiliesusingasystemicframework.ThebehavioralbackgroundofFFTprovidednotonlyspecific,manualizeableinterventionssuchascontracting,butitalsofeaturedanurgentawarenessoftheneedforrigoroustreatmentdevelopment-ascientificimperativetosystematicallyexaminetheeffectsofinterventionanddevelopstrategiesforidentifyingpositivechangeprocesses.Theseoriginsledtoacontinuingseriesofstudiesinvolvingcontrolledoutcomeevaluationsandadditionalreplications.Duringthemid-1970’s,FFTalsobeganaddressingissuesoftherapistcharacteristicsandin-sessionprocessesfromanintegratedclinical/researchperspective,bothreflectingandcontributingtothetrainingoftherapistsforsubsequentinterventions.Inthelate1990’sFFTfurtherarticulatedtheclinicalchangemodeladdingacomprehensivesystemofclient,process,andoutcomeassessmentimplementedthroughacomputer-basedclienttrackingandmonitoringsystem(FFT-CSS).
ThroughoutitsdevelopmentFFThasinsistedonstepbystepdescriptionsoftheclinicalchangeprocessaswellasrigorousevaluationofboththeprocessandoutcomesofthiswork.FFThasalsoinsistedonintegratinghighqualityscience(inregardtoevaluationandresearch)withsoundclinicaljudgementandexperienceandcomprehensivetheoreticalprinciples.Thus,overthelast30yearsFFThasbeenadynamicandevolvingclinicalsystemthatretainsitscoreprincipleswhileaddingclinicalfeaturesthatfurtherenhancesuccessfuloutcomes.Initsmostrecentiteration,FFThasdevelopedafunctionalfamilyassessmentsystemtoaidFFTtherapistsintargetingandimplementingtherapeuticchangegoalsinawaythatleadstoaccountabilitythroughprocessandoutcomeevaluation.Thus,FFThasmaturedintoaclinicalinterventionmodelwithsystematictraining,supervision,andprocessandoutcomeassessmentcomponentsalldirectedatenhancingthedeliveryofFFTinlocalcommunities(seeFigure1).
BriefDescriptionofInterventionFunctionalFamilyTherapy(FFT)isawelldocumentedfamilypreventionandinterventionprogramwhichhasbeenappliedsuccessfullytoawiderangeofproblemyouthandtheirfamiliesinvariouscontexts.Whilecommonlyemployedasaninterventionprogram,FFThasdemonstrateditseffectivenessasamethodforthepreventionofmanyoftheproblemsofat-riskadolescentsandtheirfamilies.FunctionalFamilyTherapy(FFT)isanempiricallygroundedinterventionprogram

Page 132
thattargetsyouthbetweentheagesof11and18,althoughyoungersiblingsofreferredadolescentsarealsotreated.FFTisashort-terminterventionwith,onaverage,8to12one-hoursessionsformildcasesandupto26to30hoursofdirectserviceformoredifficultsituations.Inmostprogramssessionsarespreadoverathree-monthperiodoftime.Targetpopulationsrangefromat-riskpreadolescentstoyouthwithveryseriousproblemssuchasconductdisorder.Thedatafromnumerousoutcomestudiessuggeststhatwhenappliedasintended,FFTcanreducerecidivismbetween25%and60%.AdditionalstudiessuggestthatFFTisacost-effectiveinterventionthatcan,whenappropriatelyimplemented,reducetreatmentcostswellbelowthatoftraditionalservicesandotherfamily-basedinterventions.
Practice SitesWashington StateImplementation
CSPV Blueprint Project (8 sites)Nevada
UtahPennsylvania
VirginiaArizonaIndianaKansasFlorida
KentuckyDelwareClinical Practice Training
Supervision
Science
Clinical ServicesSystem
Clinical monitoring/tracking
Family/AdolescentAssessment
ProtocolClient Assessment
Process AssessmentOutcome Assessment
Externship
Clinical Training Supervision
FFT Clinical Model
FFT-PRNPractice Research
Network
Adherence StudiesThe Family Project/
UNLV
Clinical Trials
Effectiveness StudiesThe Family Project/
UNLV
Process StudiesCTRADA Study 2
Univ. Utah
Figure1:MatureClinicalModel
APPENDIX THREE
Descriptions of Recommended Early Intervention Programmes

Page 133
Asitdeveloped,FFThasbeenreadilyadoptedinmanycontextsduetoitsclearidentificationofspecificphases,eachofwhichincludesdescriptionsofgoals,requisitetherapistcharacteristics,andtechniques.Thephasesofintervention,andtheircomponentactivities,havedevelopedinthecontextofmanyclinicalhourswithmanyfamiliesofvariouscharacteristics,coupledwithintensivesupervisionandclinicalcasediscussion.Asaresult,eachphaseinvolvesclinicallyrichandsuccessfulinterventionsthatareorganizedinacoherentmannerandallowclinicianstomaintainfocusinthecontextofconsiderablefamilyandindividualdisruption.Thephasesconsistof:
1. Phase 1: Engagement and Motivation.Duringtheseinitialphases,FFTappliesreattribution(e.g.,reframing)andrelatedtechniquestoimpactmaladaptiveperceptions,beliefs,andemotions.Thisproducesincreasinghopeandexpectationofchange,decreasingresistance,increasingallianceandtrust,reducingtheoppressivenegativitywithinfamilyandbetweenfamilyandcommunity,andincreasingrespectforindividualdifferencesandvalues.
2. Phase 2: Behavior Change.Thisphaseappliesindividualizedanddevelopmentallyappropriatetechniquessuchascommunicationtraining,specifictasksandtechnicalaids,basicparentingskills,andcontractingandresponse-costtechniques.
3. Phase 3: Generalization.Inthisphase,FamilyCaseManagementisguidedbyindividualizedfamilyfunctionalneeds,theirinteractionwithenvironmentalconstraintsandresources,andthealliancewiththetherapist.
Eachofthesephasesinvolvesbothassessmentandinterventioncomponents.Familyassessmentfocusesoncharacteristicsoftheindividualfamilymembers,familyrelationaldynamics,andthemultisystemiccontextinwhichthefamilyoperates.Thefamilyrelationalsystemisdescribedinregardtointerpersonalfunctionsandtheirimpactonpromotingandmaintainingproblembehavior.Interventionisdirectedataccomplishingthegoalsoftherelevanttreatmentphase.Forexample,intheengagementandmotivationphase,assessmentisfocusedondeterminingthedegreetowhichthefamilyoritsmembersarenegativeandblaming.Thecorrespondinginterventionwouldtargetthereductionofnegativityandblaming.Inbehaviorchange,assessmentwouldfocusontargetingtheskillsnecessaryformoreadaptivefamilyfunctioning.Interventionwouldbeaimedathelpingthefamilydevelopthoseskillsinawaythatmatchedtheirrelationalpatterns.Ingeneralization,theassessmentfocusesonthedegreetowhichthefamilycanapplythenewbehaviorinbroadercontexts.Interventionswouldfocusonhelpinggeneralizethefamilybehaviorchangeintosuchcontexts.

Page 134
Asaclinicalmodel,FFThasbeenconductedinvariedclinicalsettingsandasahome-basedmodel.ThefidelityoftheFFTmodelisachievedbyaspecifictrainingmodelandasophisticatedclientassessment,tracking,andmonitoringsystemthatprovidesforspecificclinicalassessmentandoutcomeaccountability(FFT-CSS).TheFFTPracticeResearchNetwork(FFT-PRN)allowsclinicalsitestoparticipateinthedevelopmentanddisseminationofFFTmodelinformation.
EvidenceofProgramEffectivenessTodate,thirteenstudiesinreferencedjournals(plusoneinpreparation)demonstratedramaticandsignificantpositivetreatmenteffects,includingfollow-upperiodsofuptofiveyears.Ratesofoffendingandfostercareorinstitutionalplacementhavebeenreducedatleast25percentandasmuchas60percentincomparisontotherandomlyassignedormatchedalternativetreatments,orbaserates.Onestudyalsodemonstratedapositivethreeyearfollow-upeffectonsiblings.Additionalformalprogramreports(e.g.,countyandfederalfundedprojects)fromcompletedandongoingreplicationsreflectsimilarpositiveoutcomes,andfivecurrentlyfundedtrials(NationalInstituteofDrugAbuse,NationalInstituteofAlcoholAbuseandAlcoholism,GovernmentofSweden)promiseadditionaldataregardinggeneralizationofeffectsforFFTacrossmorecontextsandpopulations.StudieshavealsoidentifiedspecificFFTbasedinterventionsanddirectchangesinfamilyfunctioningwhichrelatetotheoutcomefindings.
OnemajorfactorinthesuccessfulevolutionofFFThasbeenthecontinuous(29year)involvementofitsprogenitorsandmanyofitsco-contributorsinvariousuniversitysettings.Thiscontexthasnotonlymaintainedastandardofscientificscrutiny,buthasalsocontributedtotheconceptualintegrityofthemajorconstructsandtechniques.TheprimeexampleofthisimpactistheextensiveworkonreframinginFFT,informedbyotherwell-developedtheoreticalperspectivessuchasinformationprocessingtheory,socialcognition,andthepsychologyofemotion.Laboratorybasedresearchhasidentifiedspecificcomponentsofthiscriticaltechnique,whichinturnhasledtoappliedresearchoncognitivesetandattributionalprocessesinreferredadolescentfamilies.Further,investigationshaveidentifiedin-sessiontherapistcharacteristicsandfamilyinteractionprocessesrelevanttothephasesofFFTwhicharepredictiveofpositivechange.Mostnotableprocesschangesappeartobeinfamilycommunicationpatterns,andespeciallynegative/blamingcommunicationsand“withholding”typesofsilence.Withrespecttotherapistcharacteristics,processandoutcomedatademonstratethatFFTtherapistsmustbefirstrelationallysensitiveandfocused,thencapableofclearstructuringandteaching,inordertoproducesignificantlyfewerdropoutsduringtreatmentandlowerrecidivism.
APPENDIX THREE
Descriptions of Recommended Early Intervention Programmes

Page 135
Morerecently,FFThasbeenwidelyadoptedbecauseithasevolvedanincreasinglymulticulturalperspective,andhasaddedeffectivehome-basedintervention.Inthehome-basedClarkCounty,Nevada,YouthandFamilyServicesprogram,forexample,referredadolescentsareroughly30percentAfricanAmerican,20percentHispanic/Latino(mostlyMexicanAmerican),andjustunder50percentEuropeanAmericanwithafewAmericanIndianandAsianAmericanyouth.PreliminarydataonthefirstyearofFFTinvolvementindicatenodifferenceinreoffendingrateamongthedifferentethnic/racialgroups,supportingthegeneralizabilityofFFTeffectsacrosscultural/racialgroups.TheFayetteville,NorthCarolina,programhasinvolvedprimarilyWhiteandAfricanAmericanfamiliesandtherapists,includingasignificantnumberofmixedracerelationshipsandoffspring.ThetwoclinicaltrialsbeingconductedinNewMexicoinvolveHispanic/LatinoandWhiteyouth,andthehome-basedprograminurbanWillowRun,Michigan,involvesalargeproportionofAfricanAmericanandmixedfamilies.(Seereplicationinformationinlatersectionsformoredetails.)Asthemodelhasbeenincreasinglyadoptedinmulticulturalcontexts,focusisbeingplacedonissuesofcultureandethnicity,withmuchofthisrecentworkundertakeninthecontextofthemulti-siteNationalInstituteofDrugAbuse(NIDA)fundedCenterforResearchonAdolescentDrugAbuse(CRADA,HowardLiddle,P.I.).
Takentogether,28yearsofdataandclinicalexperiencewithFFTinvolvinghundredsoftherapistsandthousandsoffamilieshaveprovidedstrongempiricalsupportforthisfamily-basedinterventionwithadolescents.Inaddition,theresearchhasdemonstratedthatinterventionmustincludeamajorfocusonchangingemotionalandattributional,especiallyblaming,componentsoffamilyinteraction,thenprovideaprogramofspecificbehaviorchangetechniquesthatareculturallyappropriate,familyappropriate,andconsistentwiththecapabilitiesofeachfamilymember.
Theinformationforthisfactsheetwasexcerptedfrom:
Alexander,J.,Barton,C.,Gordon,D.,Grotpeter,J.,Hansson,K.,Harrison,R.,Mears,S.,Mihalic,S.,Parsons,B.,Pugh,C.,Schulman,S.,Waldron,H.,&Sexton,T.(1998).BlueprintsforViolencePrevention,BookThree:FunctionalFamilyTherapy.Boulder,CO:CenterfortheStudyandPreventionofViolence.

Page 136
LIFESKILLSTRAINING(LST)
ProgramSummaryTheresultsofoveradozenstudiesconsistentlyshowthattheLifeSkillsTraining(LST)programdramaticallyreducestobacco,alcohol,andmarijuanause.Thesestudiesfurthershowthattheprogramworkswithadiverserangeofadolescents,producesresultsthatarelong-lasting,andiseffectivewhentaughtbyteachers,peerleaders,orhealthprofessionals.
ProgramTargetsLSTisaprimaryinterventionthattargetsallmiddle/juniorhighschoolstudents(initialinterventioningrades6or7,dependingontheschoolstructure,withboostersessionsinthetwosubsequentyears).
ProgramContentLSTisathree-yearinterventiondesignedtopreventorreducegatewaydruguse(i.e.,tobacco,alcohol,andmarijuana),primarilyimplementedinschoolclassroomsbyschoolteachers.Theprogramisdeliveredin15sessionsinyearone,10sessionsinyeartwo,and5sessionsinyearthree.Sessions,whichlastanaverageof45minutes,canbedeliveredonceaweekorasanintensivemini-course.Theprogramconsistsofthreemajorcomponentswhichteachstudents(1)generalself-managementskills,(2)socialskills,and(3)informationandskillsspecificallyrelatedtodruguse.Skillsaretaughtusingtrainingtechniquessuchasinstruction,demonstration,feedback,reinforcement,andpractice.
ProgramOutcomesUsingoutcomesaveragedacrossmorethanadozenstudiesconductedwithLST,ithasbeenfoundto:
■ Cuttobacco,alcohol,andmarijuanause50%-75%.
Long-termfollow-upresultsobservedsixyearsfollowingtheinterventionshowthatLST:
■ Cutspolydruguseupto66%;■ Reducespack-a-daysmokingby25%;and■ Decreasesuseofinhalants,narcotics,andhallucinogens.
ProgramCostsLSTcanbeimplementedatacostofapproximately$7perstudentperyear(curriculummaterialsaveragedoverthethree-yearperiod).Thisdoesnotincludethecostoftrainingwhichisaminimumof$2,000perdayforoneortwodays.
APPENDIX THREE
Descriptions of Recommended Early Intervention Programmes

Page 137
ProgramBackgroundTheLifeSkillsTraining(LST)programwasdevelopedtoaddressthemonumentalproblemofsubstanceabuseinthiscountry.Theadversehealth,social,andlegalconsequencesofthisproblemhavebeenwelldocumented.Cigarettesmokingisarisk-factorforheartdisease,variouscancers,andchronicobstructivelungdiseaseandaccountsforover430,000deathsperyear.Alcoholisnotonlyrelatedtochronicdiseasessuchascirrhosisoftheliver,butisalsoamajorfactorinautofatalitiesandhomicides.Beyondthis,adolescentdrugusepredictsanumberofotherundesirableoutcomessuchasreducingtraditionaleducationalaccomplishmentsandjobstability,increasingthelikelihoodofmarryingandhavingchildrenatyoungerages,andincreasingthelikelihoodofengagingincriminalbehavior.
Despiteconsiderablepublicattentionandtheexpenditureofwelloverabilliondollarsinthepastfewyearsalone,littleifanyprogresshasbeenmadetowardreducingdrugabuse.Atpresent,druguseamongAmericanyouthisaproblemofenormousproportionsanditisgettingworse.Since1991,accordingtonationalsurveys,drugusehasincreasedbymorethan30percentleadingsomeexpertstobelievethatweareonthevergeofanewdrugepidemic.Figure1illustratesthistrendinannualprevalence(proportionofusers)ofillicitdrugusefortwelfthgradestudentssince1975.Accordingtothemostrecentnationalsurveydata,thefollowingproportionsofhighschoolstudentshaveusedalcohol,cigarettes,andillicitdrugsatleastonce(Johnston,O’Malley&Bachman,1995):
Alcohol Cigarettes Illicit Drugs8thGraders 56% 46% 26%
10thGraders 71% 57% 37%
12thGraders 80% 62% 46%
Resultsfromthesamesurveyindicatedthatduringthepast30days,thefollowingproportionsofhighschoolstudentsusedthefollowingsubstancesoneormoretimes:
Alcohol Cigarettes Illicit Drugs8thGraders 26% 19% 11%
10thGraders 39% 25% 19%
12thGraders 50% 31% 22%
Forsomeoftheseteens,usemaybediscontinuedafterabriefperiodofexperimentation.However,formany,initiationofcigarettesmoking,drinking,ordrug-takingmayleadtopatternsofusewhichresultinbothpsychologicalandphysicaldependence.Ingeneral,programsdesignedtohelpindividualsquit

Page 138
smoking,drinking,orusingdrugshaveonlybeenmoderatelyeffective.Quitesimply,onceanytypeofsubstanceusehabitisacquireditisextremelydifficulttobreak.Scientificevidencenowsuggeststhatthedevelopmentofeffectivepreventionprogramsmayofferthegreatestpotentialforimpactingthisimportanthealthproblem.
Unfortunately,reviewsofthepreventionresearchliteratureandmeta-analyticstudiesshowthatmanywidelyuseddrugabusepreventionapproachesareineffective.Themostcommonapproachestosubstanceabusepreventionoverthepasttwodecadeshaveinvolvedeitherthepresentationoffactualinformationconcerningthedangersofsubstanceuseorwhathasbeenreferredtoas“affective”education.
Approachesrelyingontheprovisionoffactualinformationarebasedlargelyontheassumptionthatincreasedknowledgeaboutpsychoactivesubstancesandtheiradverseconsequenceswouldbeaneffectivedeterrent.Affectiveeducationapproachesaredesignedtoenrichthepersonalandsocialdevelopmentofstudentsthroughclassdiscussionandexperimentalclassroomactivities.Bothoftheseapproacheshaveproventobelargelyineffectivebecausetheydonotaddressthefactorspromotingtheinitiationandearlystagesofsubstanceuse/abuse.
TheLSTprogramisadrugabusepreventionprogramthatisbasedonanunderstandingofthecausesofsmoking,alcohol,anddruguse/abuse.TheLSTinterventionhasbeendesignedsothatittargetsthepsychosocialfactorsassociatedwiththeonsetofdruginvolvement.Withthisinmind,theprogramimpactsondrug-relatedexpectancies(knowledge,attitudes,andnorms),drug-relatedresistanceskills,andgeneralcompetence(personalself-managementskillsandsocialskills).Increasingprevention-relateddrugknowledgeandresistanceskillscanprovideadolescentswiththeinformationandskillsneededtodevelopanti-drugattitudesandnorms,aswellastoresistpeerandmediapressuretousedrugs.Teachingeffectiveself-managementskillsandsocialskills(improvingpersonalandsocialcompetence)offersthepotentialofproducinganimpactonasetofpsychologicalfactorsassociatedwithdecreaseddrugabuserisk(byreducingintrapersonalmotivationstousedrugsandbyreducingvulnerabilitytopro-drugsocialinfluences).
TheoreticalRationale/ConceptualFrameworkManytheorieshavebeenadvancedtoexplaindrugabuse.Themostprominentamongthesefocusonsociallearning,problembehaviors,self-derogation,persuasivecommunications,peerclusters,andsensation-seeking.However,theetiologyofdrugabuseinvolvesadynamicprocesswhichunfoldsovermanyyears.
APPENDIX THREE
Descriptions of Recommended Early Intervention Programmes

Page 139
Acommonlimitationofmosttheoreticalmodelsisthattheyareessentiallysnap-shotsoftheetiologyofdrugabuseanddonotadequatelycapturethecomplexityoftheproblem.
Wenowknowthattheinitiationofdruguseistheresultofthecomplexcombinationofmanydiversefactors.Thereisnosinglepathwayorsinglevariablewhichservesasanecessaryandsufficientconditionforthedevelopmentofeitherdruguseordrugabuse.Withthisinmind,theLSTapproachtodrugabusepreventionisbasedonaperson-environmentinteractionistmodelofdrugabuse.Likeothertypesofhumanbehavior,drugabuseisconceptualizedasbeingtheresultofadynamicinteractionofanindividualandhis/herenvironment.Socialinfluencestousedrugs(alongwiththeavailabilityofdrugs)interactwithindividualvulnerability.Someindividualsmaybeinfluencedtousedrugsbythemedia(TVshowsandmoviesglamorizingdruguseorsuggestingthatdruguseisnormalorsociallyacceptableaswellasadvertisingeffortstopromotethesaleofalcoholandtobaccoproducts),byfamilymemberswhousedrugsorconveypro-drugattitudes,and/orbyfriendsandacquaintanceswhousedrugsorholdattitudesandbeliefssupportiveofdruguse.Othersmaybepropelledtowarddruguseoradrug-usingpeergroupbecauseofintrapersonalfactorssuchaslowself-esteem,highanxietyorotherdysphoricfeelings,ortheneedforexcitement.
Sincetherearemultiplepathwaysleadinginitiallytodruguseandlatertodrugabuse,amoreusefulwayofconceptualizingdrugabuseisfromarisk-factorperspectivesimilartothatusedintheepidemiologyofchronicdiseasessuchascancerandheartdisease.Fromthisperspective,thepresenceofspecificriskfactorsislessimportantthantheiraccumulation.Asmoreriskfactorsaccumulatesodoesthelikelihoodthatanindividualwillbecomeadruguserandeventuallyadrugabuser.Thus,thepresenceofmultipleriskfactorsisassociatedwithbothinitialdruguseandtheseverityofdruginvolvement.
Ithasalsobeenwellestablishedthattheprevalenceofdrugusegenerallyincreaseswithageandprogressesinawell-definedsequence.Drugusetypicallybeginswiththeuseofalcoholandtobaccofirst,progressinglatertotheuseofmarijuana,and,forsome,totheuseofstimulants,opiates,hallucinogens,andotherillicitsubstances.Notsurprisingly,thisprogressioncorrespondsexactlytotheprevalenceandavailabilityofthesesubstanceswithalcoholbeingthemostprevalentformofdruguseandthemostwidelyavailable,followedbytobacco(cigarettes)andmarijuana.Becausealcohol,tobacco,andmarijuanaareamongthefirstsubstancesused,theyhavebeenreferredtoas“gateway”substances.Theuseofthese“gateway”substancessignificantlyincreasestheriskofusingillicitdrugsotherthanmarijuana.

Page 140
Takingthisintoaccount,theLSTpreventionprogramtargetsthose“gateway”substances(tobacco,alcohol,andmarijuana)thatoccuratthebeginningofthedevelopmentalprogression.Thus,LSToffersthepotentialforinterruptingthenormaldevelopmentalprogressionfromuseofthesesubstancestootherformsofdruguse/abuse.Asecondreasonfortargetingthistypeofdruguseisthattheuseofthesesubstancesaccountsforthelargestportionofdrug-relatedannualmortalityandmorbidity.
BriefDescriptionofIntervention
OverviewTheLSTpreventionprogramisathree-yearinterventiondesignedtobeconductedinschoolclassrooms.Basedonthetheoreticalframeworkdiscussedearlier,theLSTprogramwasdevelopedtoimpactondrug-relatedknowledge,attitudesandnorms;teachskillsforresistingsocialinfluencestousedrugs;andpromotethedevelopmentofgeneralpersonalself-managementskillsandsocialskills.Consistentwiththis,theLSTpreventionprogramcanbestbeconceptualizedasconsistingofthreemajorcomponents.Thefirstcomponentisdesignedtoteachstudentsasetofgeneralself-managementskills.Thesecondcomponentfocusesonteachinggeneralsocialskills.Thethirdcomponentincludesinformationandskillsthatarespecificallyrelatedtotheproblemofdrugabuse.Thefirsttwocomponentsaredesignedtoenhanceoverallpersonalcompetenceanddecreaseboththemotivationstousedrugsandvulnerabilitytodrugusesocialinfluences.Theproblem-specificcomponentisdesignedtoprovidestudentswithmaterialrelatingdirectlytodrugabuse(drugresistanceskills,anti-drugattitudes,andanti-drugnorms).AcompletedescriptionofeachLSTcomponentmaybefoundinthesectionlabeled“ProgramasDesignedandImplemented.”
ProgramStructureTheLSTprogramconsistsoffifteenclassperiods(roughly45minuteseach)andisintendedformiddleorjuniorhighschoolstudents,dependinguponthestructureoftheschool.Aboosterinterventionhasalsobeendevelopedwhichconsistsoftenclassperiodsinthesecondyearandfiveclassperiodsinthethirdyear.Thismeansforschooldistrictswithamiddleschoolstructure,theLSTprogramcanbeimplementedwithstudentsinthesixthgrade,followedbyboostersessionsintheseventhandeighthgrades.IftheLSTprogramisimplementedinajuniorhighschoolsetting,studentsreceivetheprogramintheseventhgrade,andtheboostersessionsintheeighthandninthgrade,respectively.TherationaleforimplementingtheLSTprogramatthispointconcernsavarietyoffactorsconcerningthedevelopmentalprogressionofdruguse,normalcognitiveandpsychosocialchangesoccurringatthistime,theincreasingprominenceofthepeergroup,andissuesrelatedtothetransitionfromprimarytosecondaryschool.
APPENDIX THREE
Descriptions of Recommended Early Intervention Programmes

Page 141
Drugexpertshaveestablishedthatearlyadolescenceisatimeofincreasedriskforexperimentingwithoneormorepsychoactivesubstances.Childrenfirsttypicallyexperimentwithalcoholduringthesixthandseventhgrades.Thegreatestproportionalchangeincigarettesmokingoccursbetweentheseventhandeighthgrades.Correspondingly,thegreatestchangeinmarijuanausetakesplacebetweentheeighthandninthgrades.Adolescenceisalsoatimeofincreasedrelianceonthepeergroup,separationfromparentsastheydevelopasenseofindependenceandautonomy,andchangesinthewayindividualsthink.Forexample,duringthistime,individualsbegintoshiftfromaconcretestyleofthinkingthatincludesaclearsenseofrightandwrongorabsoluterulesofbehaviortoonethatismorerelativeandhypothetical.Thisenablestheadolescenttoacceptdeviationfromestablishedrulesandtorecognizethefrequentlyirrationalandinconsistentnatureofadultbehavior.Inaddition,ithasbeennotedthatthetransitionfromprimarytosecondaryschoolcanbeasourceofstressthatincreasesriskfromproblembehaviorssuchastobacco,alcohol,andillicitdruguse.Finally,thestrongestevidenceconcerningtheeffectivenessofdrugabusepreventionprogramsisbasedonevaluationresearchwithprogramsimplementedwithindividualsduringthisperiod.
Whiletheprogramiseffectivewithjusttheoneyearofprimaryintervention,researchalsohasshownthatpreventioneffectsaregreatlyenhancedwhenboostersessionsareincluded.Forexample,twostudieshaveshownthatoneyearoftheprimaryinterventionofLSTproducedreductionsof56-67percentinsmokingwithoutanyadditionalboostersessions;butforthosestudentsreceivingboostersessions,thesereductionswereashighas87percent.Inaddition,theboostersessionsenhancethedurabilityofpreventioneffects,sothattheydonotdecayasmuchovertime.LSThasbeenshowntobeeffectiveusingavarietyofserviceprovidersincludingoutsidehealthprofessionals,regularclassroomteachers,andpeerleaders.Peercounselorsareoftenslightlyolder(highschool)andalmostalwaysworkinconjunctionwithatrainedadultprovider.
EvidenceofProgramEffectiveness
OverviewConsiderablepreventionresearchhasbeenconductedoverthepasttwentyyears.Despitethebesteffortsofeducators,healthprofessionals,anddrugabusepreventionspecialists,alargenumberofevaluationstudieshavefailedtodemonstratethatthepreventionapproachbeingutilizedwasabletoproduceameasurableimpactondrugusebehavior.Somestudieshavedemonstratedreductionsinattitudestowarddrugsanddruguse.Othershavedemonstratedincreasesinknowledgeaboutdrugsortheconsequencesofusingdrugs.But,effortstodemonstratethatpreventionprogramscouldimpactonactualdrugusehavebeendisappointing.

Page 142
ResearchwiththeLifeSkillsTrainingProgramMorethanoneandahalfdecadesofresearchwiththeLSTprogramhaveconsistentlyshownthatparticipationintheprogramcancutdruguseinhalf.Thesereductions(relativetocontrols)inboththeprevalence(i.e.,proportionofpersonsinapopulationwhohavereportedsomeinvolvementinaparticularoffense)andincidence(i.e.,thenumberofoffenseswhichoccurinagivenpopulationduringaspecifiedtimeinterval)ofdrugusehaveprimarilybeenwithrespecttotobacco,alcohol,andmarijuanause.Thesestudieshavedemonstratedthatthispreventionapproachcanproducereductionsindrugusethatarelong-lastingandclinicallymeaningful.Forexample,long-termfollow-updataindicatethatreductionsindruguseproducedwithseventhgraderscanlastuptotheendofhighschool.EvaluationresearchhasdemonstratedthatthispreventionapproachiseffectivewithabroadrangeofstudentsincludingWhite,middle-classyouthandpoorinner-cityminority(AfricanAmericanandHispanic/Latino)youth.Ithasnotonlydemonstratedreductionsintheuseoftobacco,alcohol,ormarijuanauseofupto80percent,butevaluationstudiesshowthatitalsocanreducemoreseriousformsofdruginvolvementsuchastheweeklyuseofmultipledrugsorreductionsintheprevalenceofpack-a-daysmoking,heavydrinking,orepisodesofdrunkenness.
ResultsfromfourpublishedstudiestestingtheLSTprogramshowthatdruguseamongtheLSTstudentswasatleasthalfthatofthecontrolgroup.
TheinformationforthisfactsheetwasexcerptedfromBotvin,G.J.,Mihalic,S.F.,&Grotpeter,J.K.(1998).BlueprintsforViolencePrevention,BookFive:LifeSkillsTraining.Boulder,CO:CenterfortheStudyandPreventionofViolence.
APPENDIX THREE
Descriptions of Recommended Early Intervention Programmes

Page 143
FAMILYNURSEPARTNERSHIPS(NURSE-FAMILYPARTNERSHIPSINTHEUSA)
ProgramSummaryFamilyNursePartnershipsorNurse-FamilyPartnershipsintheUSA(FormerlyPrenatalandInfancyHomeVisitationbyNurses),guidedbyastrongtheoreticalorientation,consistsofintensiveandcomprehensivehomevisitationbynursesduringawoman’spregnancyandthefirsttwoyearsafterbirthofthewoman’sfirstchild.Whiletheprimarymodeofservicedeliveryishomevisitation,theprogramdependsuponavarietyofotherhealthandhumanservicesinordertoachieveitspositiveeffects.Theprogramisdesignedtoservelow-income,at-riskpregnantwomenbearingtheirfirstchild.
ProgramContentNursehomevisitorsworkwithfamiliesintheirhomesduringpregnancyandthefirsttwoyearsofthechild’slife.Theprogramisdesignedtohelpwomenimprovetheirprenatalhealthandtheoutcomesofpregnancy;improvethecareprovidedtoinfantsandtoddlersinanefforttoimprovethechildren’shealthanddevelopment;andimprovewomen’sownpersonaldevelopment,givingparticularattentiontotheplanningoffuturepregnancies,women’seducationalachievement,andparents’participationintheworkforce.Typically,anursevisitorisassignedtoafamilyandworkswiththatfamilythroughthedurationoftheprogram.
ProgramOutcomesThisprogramhasbeentestedwithbothWhiteandAfricanAmericanfamiliesinruralandurbansettings.Nurse-visitedwomenandchildrenfaredbetterthanthoseassignedtocontrolgroupsineachoftheoutcomedomainsestablishedasgoalsfortheprogram.Ina15-yearfollow-upstudyofprimarilyWhitefamiliesinElmira,NewYork,findingsshowedthatlow-incomeandunmarriedwomenandtheirchildrenprovidedanursehomevisitorhad,incontrasttothoseinacomparisongroup:
■ 79%fewerverifiedreportsofchildabuseorneglect;■ 31%fewersubsequentbirths;■ anaverageofovertwoyears’greaterintervalbetweenthebirthoftheirfirst
andsecondchild;■ 30monthslessreceiptofAidtoFamilieswithDependentChildren;■ 44%fewermaternalbehavioralproblemsduetoalcoholanddrugabuse;■ 69%fewermaternalarrests;■ 60%fewerinstancesofrunningawayonthepartofthe15-year-oldchildren;■ 56%fewerarrestsonthepartofthe15-year-oldchildren;and■ 56%fewerdaysofalcoholconsumptiononthepartofthe15-year-oldchildren.

Page 144
ProgramCostsThecostoftheprogramwasrecoveredbythefirstchild’sfourthbirthday.Substantialsavingstogovernmentandsocietywerecalculatedoverthechildren’slifetimes.In1997,thetwo-and-a-half-yearprogramwasestimatedtocost$3,200peryearperfamilyduringthestart-upphase(thefirstthreeyearsofprogramoperation)and$2,800perfamilyperyearoncethenursesarecompletelytrainedandworkingatfullcapacity.Actualcostoftheprogramwillvarydependingprimarilyuponthesalariesoflocalcommunity-healthnurses.Communitieshaveusedavarietyoflocal,state,andfederalfundingsourcestosupporttheprogram,includingMedicaid,welfare-reform,maternalandchildhealth,andchildabusepreventiondollars.
ProgramBackgroundManyofthemostpervasive,intractable,andcostlyproblemsfacedbyyoungchildrenandparentsinoursocietytodayareaconsequenceofadversematernalhealth-relatedbehaviors(suchascigarettesmoking,drinking,anddruguse)duringpregnancy,dysfunctionalinfantcaregiving,andstressfulenvironmentalconditionsthatinterferewithparentalandfamilyfunctioning.Theseproblemsincludeinfantmortality,pretermdeliveryandlowbirthweight,childabuseandneglect,childhoodinjuries,youthviolence,closelyspacedpregnancy,andthwartedeconomicself-sufficiencyonthepartofparents.Standardindicesofchildhealthandwell-beingindicatethatmanychildreninoursocietyaresuffering.
■ NineinfantsoutofeverythousandintheUnitedStatesdiebeforetheirfirstbirthday.Asaresultofhighratesoflowbirthweight(lessthan2500gramsor5pounds8ounces),ourinfantmortalityrateisworsethan19othernations,inspiteofdramaticreductionsininfantmortalityinthelasttwodecadesduetoimprovementsinnewbornintensivecare.Lowbirthweightbabieswhosurviveare50percentmorelikelytousespecialeducationservicesoncetheyenterschoolthanarenormalbirthweightcontrols.
■ Over2.5millionchildrenwerereportedasbeingabusedorneglectedin1990,andoneinthreeofthevictimsofphysicalabusewereinfantslessthanoneyearofage.Between1,200and1,500childrendieeachyearasaresultofparentorcaregivermaltreatment.Notonlyismaltreatmentmorallyunacceptable,butthesocialconsequencesaresodevastatingthattheU.S.AdvisoryPanelonChildAbuseandNeglecthascalledchildmaltreatmentanationalemergency.
■ Childhoodinjuriesaretheleadingcauseofdeathamongchildrenagedonetofourteen.
■ Highratesofviolenceamongadolescents,bothasvictimsandperpetrators,threatenthesafetyandwell-beingofourneighborhoods.Amongyoungpeopleaged15-24,homicideisaleadingcauseofdeath,andforAfricanAmericansitisthenumberonecause.
APPENDIX THREE
Descriptions of Recommended Early Intervention Programmes

Page 145
■ In1992,52percentofthemothersonAFDChadtheirfirstbirthasteens,costingthegovernmentapproximately$12.8billion.Rapidsuccessivepregnancyincreasesthelikelihoodofcontinuedwelfaredependenceandahostofassociatedproblems.
Evidenceindicatesthatasignificantportionoftheseproblemscanbetracedtoparentalbehavior—inparticular,towomen’shealth-relatedbehaviorsduringpregnancy,tothequalityofcarethatparentsprovidetotheirchildren,andtowomen’slifechoiceswithrespecttofamilyplanning,educationalachievement,andworkforceparticipation.WhiletheseproblemscutacrossallsegmentsofU.S.society,theyaremorecommonamongwomenwhobeginchildbearingaspoor,unmarriedadolescents.Low-income,single,adolescentmotherscanhavegoodpregnancyoutcomesandchildrenwhodowell,buttheircapacitytocareforthemselvesandfortheirchildrenisoftencompromisedbyhistoriesofmaltreatmentintheirownchildhood,psychologicalimmaturityordepression,stressfullivingconditions,andinadequatesocialsupport.Theseconditionscontributetothegreaterlikelihoodthatsociallydisadvantagedparentswillabusecigarettesandotherdrugsduringpregnancyandwillfailtoprovideadequatecarefortheirchildren,oftenwithdevastatingresults.
Womenwhosmokecigarettesanduseothersubstancesduringpregnancy,forexample,areatconsiderableriskforbearinglowbirthweightnewborns,andtheirchildrenareatheightenedriskforneurodevelopmentalimpairment.Evensubtledamagetothefetalbraincanunderminechildren’sintellectualfunctioningandcapacityforemotionalandbehavioralregulation.Parents’capacitiestoreadandrespondtotheirinfants’communicativesignalsformthebasisforchildren’ssenseofsecurityandtrustintheworldandtheirbeliefintheircapacitytoinfluencethatworld.Breachesofthattrusthavelong-termconsequences,especiallywhencaregivingdysfunctioniscombinedwithneurodevelopmentalimpairmentonthepartofthechild.
AlongitudinalstudyofalargeDanishsampleofchildrenandtheirfamiliesfoundthatchildrenwhoexperiencedthecombinationofbirthcomplicationsandparentalrejectioninthefirstyearoflifewereatsubstantiallyincreasedriskforviolentcriminalityatage18incomparisontochildrenwhoexperiencedonlybirthcomplicationsorparentalrejectionalone.Whileonly4.5percentofthesampleexperiencedbothbirthcomplicationsandparentalrejection,thatgroupaccountedfor18percentofallviolentcrimesamongthose18yearsofage.Parentalrejectionorbirthtraumabyitselfdidnotincreasetheriskforviolence.Whenriskfactorsaccumulate,theriskforadverseoutcomesincreases,ofteninsynergisticallyviciousways.

Page 146
Theproblemslistedhavebeenresistivetogovernmentinterventionoverthepastthirtyyears.However,scientificevidenceisaccumulatingthatitispossibletoimprovetheoutcomesofpregnancy,toimproveparents’abilitiestocarefortheirchildren,andtoreducewelfaredependencewithprogramsofprenatalandearlychildhoodhomevisitation,butitisnoteasy.Ouroptimismstandsincontrasttoearlierresearchonhomevisitation.Theearlierresearchwasdifficulttointerpretbecausetheprogramsstudiedwereoftennotdesignedtoaddresstheneedsofparentsinsensibleandpowerfulways,andtheresearchitselffrequentlylackedscientificrigor.
Theprogramofprenatalandinfancyhomevisitationbynursesdescribedhereisdistinguishedfromotherprogramsbyitsfirmfoundationinepidemiologyandtheory.Theprogramisbaseduponananalysisofproximalrisksfortheparticularoutcomesthatitisdesignedtoaffect(usuallyparentalbehaviorsorconditionsinthehomethatincreasethelikelihoodofadverseoutcomesonthepartofthemotherorchild).Italsoisfoundeduponthreeinterrelatedtheoreticalfoundations—self-efficacy,attachment,andhumanecologytheories.Eachofthesetheoriesaddressesdifferentaspectsofthedevelopmentalsystemthatcontributestoadversematernalandchildoutcomesinvulnerablefamilies.
TheoreticalRationale/ConceptualFrameworkTheprogramhasbeengroundedintheoriesofhumanecology(Bronfenbrenner,1979,1992),self-efficacy(Bandura,1977,1982),andhumanattachment(Bowlby,1969).Theearliestformulationsoftheprogramgavegreatestemphasistohumanecology,butastheprogramhasevolved,ithasbeengroundedmoreexplicitlyintheoriesofself-efficacyandhumanattachment.
TheoriginalformulationofthisprogramwasbasedinlargepartonBronfenbrenner’stheoryofhumanecology.Humanecologytheoryemphasizestheimportanceofsocialcontextsasinfluencesonhumandevelopment.Parents’careoftheirinfants,fromthisperspective,isinfluencedbycharacteristicsoftheirfamilies,socialnetworks,neighborhoods,communities,andcultures,andinterrelationsamongthesestructures.Bronfenbrenner’soriginaltheoreticalframeworkhasbeenelaboratedmorerecently(withgreaterattentiontoindividualinfluences)inhisperson-process-contextmodelofresearchonhumandevelopment.
Thepersonelementsofthemodelarereflectedintheprogramcomponentsthathavetodowithbehavioralandpsychologicalcharacteristicsoftheparentandchild.Intheformulationofthetheoreticalfoundationsoftheprogram,parents,andespeciallymothers,areconsideredbothdevelopingpersonsandtheprimaryfocusofthepreventiveintervention.Particularattentionisfocusedonparents’progressivemasteryoftheirrolesasparentsandasadultsresponsiblefortheirownhealthand
APPENDIX THREE
Descriptions of Recommended Early Intervention Programmes

Page 147
economicself-sufficiency.Thisprogramemphasizesparentdevelopmentbecauseparents’behaviorconstitutesthemostpowerfulandpotentiallyalterableinfluenceonthedevelopingchild,particularlygivenparents’controlovertheirchildren’sprenatalenvironment,theirface-to-faceinteractionwiththeirchildrenpostnatally,andtheirinfluenceonthefamily’shomeenvironment.
Theconceptofprocessencompassesparents’interactionwiththeirenvironmentaswellastheintrapsychicchangesthatcharacterizetheirmasteryoftheirrolesasparentsandproviders.Threeaspectsofprocessemphasizedhererelatetoindividuals’functioning:(1)programprocesses(e.g.,thewaysinwhichthevisitorsworkwithparentstostrengthenparents’competencies);(2)processesthattakeplacewithinparents(i.e.,theinfluenceoftheirpsychologicalresources—developmentalhistories,mentalhealth,andcopingstyles—onbehavioraladaptation);and(3)parents’interactionwiththeirchildren,otherfamilymembers,friends,andhealthandhumanserviceproviders.Forthesakeofsimplicity,thediscussionoftheseprocesseshasbeenintegratedbelowintotheperson(parent)partofthemodel.
Thefocusonparentselaboratedhereisnotintendedtominimizetherolethatcontextualfactorssuchaseconomicconditions,culturalpatterns,racism,andsexismplayinshapingtheopportunitiesthatparentsareafforded.Mostofthosefeaturesoftheenvironment,however,areoutsideoftheinfluenceofpreventiveinterventionsprovidedthroughhealthandhumanservicesystems.Certaincontexts,nevertheless,areaffectedbyparents’adaptivecompetencies.Itisthesefeaturesoftheenvironmentthatthecurrentprogramattemptstoaffect,primarilybyenhancingparents’socialskills.Theaspectsofcontextthatwearemostconcernedabouthavetodowithinformalandformalsourcesofsupportforthefamily,characteristicsofcommunitiesthatcansupportorunderminethefunctioningoftheprogramandfamilies,theimpactofgoingtoschoolorworkingonfamilylife,aswellasculturalconditionsthatneedtobetakenintoconsiderationinthedesignandconductoftheprogram.
Oneofthecentralhypothesesofecologicaltheoryisthatthecapacityoftheparent-childrelationshiptofunctioneffectivelyasacontextfordevelopmentdependsontheexistenceandnatureofotherrelationshipsthattheparentmayhave.Theparent-childrelationshipisenhancedasacontextfordevelopmenttotheextentthateachoftheseotherrelationshipsinvolvesmutualpositivefeelingsandthattheotherpartiesaresupportiveofthedevelopmentalactivitiescarriedonintheparent-childrelationship.Conversely,thedevelopmentalpotentialoftheparent-childrelationshipisimpairedtotheextentthateachoftheotherrelationshipsinwhichtheparentisinvolvedconsistsofmutualantagonismorinterferencewiththedevelopmentalactivitiescarriedonintheparent-childrelationship.

Page 148
LimitationsofHumanEcologyTheory.Comparedtootherdevelopmentaltheories,Bronfenbrenner’sframeworkprovidesamoreextendedandelaboratedconceptionoftheenvironment.Theoriginalformulationofthetheory,however,tendedtotreattheimmediatesettingsinwhichchildrenandfamiliesfindthemselvesasshapedbyculturalandstructuralcharacteristicsofthesociety.Littleconsiderationwasgiventotherolethatadults(inparticularparents)playinselectingandshapingthesettingsinwhichtheyfindthemselves.Whilemanyinvestigatorstodayreasonthatthepersonalcharacteristicsthatinfluenceindividuals’selectionandshapingoftheircontextshavegeneticorigins,wehavechosentodeterminetheextenttowhichandthemeansbywhichhealthychoicesandadaptivebehaviorscanbepromoted.
Consequently,self-efficacyandattachmenttheorieswereintegratedintothemodeltoprovideabroaderconceptionoftheparentsettingrelationship.Theintegrationofthesetheoriesallowsforaconceptualizationofdevelopmentthatencompassestrulyreciprocalrelationshipsinwhichsettings,children,andotheradultsinfluenceparentalbehavior,andinwhichparentssimultaneouslyselectandshapetheirsettingsandinterpersonalrelationships.
Self-EfficacyTheorySelf-efficacytheoryprovidesausefulframeworkforpromotingwomen’shealth-relatedbehaviorduringpregnancy,careoftheirchildren,andpersonaldevelopment.AccordingtoBandura,differencesinmotivation,behavior,andpersistenceineffortstochangeawiderangeofsocialbehaviorsareafunctionofindividuals’beliefsabouttheconnectionbetweentheireffortsandtheirdesiredresults.Accordingtothisview,cognitiveprocessesplayacentralroleintheacquisitionandretentionofnewbehaviorpatterns.Inselfefficacytheory,Banduradistinguishesoutcomeexpectationsfromefficacyexpectations.Outcomeexpectationsareindividuals’estimatesthatagivenbehaviorwillleadtoagivenoutcome.Efficacyexpectationsareindividuals’beliefsthattheycansuccessfullycarryoutthebehaviorrequiredtoproducetheoutcome.Itisefficacyexpectationsthataffectboththeinitiationandpersistenceofcopingbehavior.Individuals’perceptionsofself-efficacycaninfluencetheirchoiceofactivitiesandsettings,andcandeterminehowmuchefforttheywillputforthinthefaceofobstacles.
LimitationsofSelf-EfficacyTheory.Whileself-efficacytheoryprovidespowerfulinsightsintohumanmotivationandbehavior,itislimitedinseveralrespects.Thefirstlimitationisthatitisprimarilyacognitive-behavioraltheory.Itattendstotheemotionallifeofthemotherandotherfamilymembersonlythroughtheimpactofbehavioronwomen’sbeliefsorexpectations,whichinturnaffectemotions.Manypeoplehaveexperiencedmultipleadversitiesintheformofoverlyharshparenting,rejection,orneglectthatoftencontributetoasenseofworthlessness,depression,
APPENDIX THREE
Descriptions of Recommended Early Intervention Programmes

Page 149
andcynicismaboutrelationships.Self-efficacygivesinadequateattentiontomethodsofhelpingparentscopewiththesefeaturesoftheirpersonalhistoryortheimpactofthoseearlyexperiencesontheircareoftheirchildren.Wehaveaugmentedthetheoreticalunderpinningsoftheprogramregardingthesesocialandemotionalissueswithattachmenttheory(discussedbelow).
Thesecondlimitationisthatself-efficacyattendstoenvironmentalinfluencesinacursoryway.Peoplecangiveupbecausetheydonotbelievethattheycandowhatisrequired,buttheyalsocangiveupbecausetheyexpectthattheireffortswillmeetwithpunitiveness,resistance,orunresponsiveness.WhileBanduraacknowledgesthatadversityandintractableenvironmentalconditionsareimportantfactorsinthedevelopmentofindividuals’senseoffutility,thestructureofthoseenvironmentalforcesisnotthesubjectofBandura’stheory.Inotherwords,individuals’feelingsofhelplessnessandfutilityarenotsimplyintra-psychicphenomena,butareconnectedtoenvironmentalcontextsthatprovidelimitedopportunitiesandthatfailtonurtureindividuals’growthandwell-being.Thestructureofthoseenvironmentalinfluencesistheprimarysubjectofhumanecologytheory,discussedabove.
AttachmentTheoryHistorically,thisprogramowesmuchtoBowlby’stheoryofattachment.Attachmenttheorypositsthathumanbeings(andotherprimates)haveevolvedarepertoireofbehaviorsthatpromoteinteractionbetweencaregiversandtheirinfants(suchascrying,clinging,smiling,signaling),andthatthesebehaviorstendtokeepspecificcaregiversinproximitytodefenselessyoungsters,thuspromotingtheirsurvival,especiallyinemergencies.Humans(aswellasmanyotherspecies)arebiologicallypredisposedtoseekproximitytospecificcaregiversundertimesofstress,illness,orfatigueinordertopromotesurvival.Thisorganisationofbehaviordirectedtowardthecaregiverisattachment.
Inrecentyears,agrowingbodyofevidenceindicatesthatcaregivers’levelsofresponsivitytotheirchildrencanbetracedtocaregivers’ownchildrearinghistoriesandattachment-relatedexperiences.Caregivers’attachment-relatedexperiencesarethoughttobeencodedin“internalworkingmodels”ofselfandothersthatcreatestylesofemotionalcommunicationandrelationshipsthateitherbuffertheindividualintimesofstressorthatleadtomaladaptivepatternsofaffectregulationandcreatefeelingsofworthlessness.Differencesininternalworkingmodels,accordingtoattachmenttheorists,haveenormousimplicationsformothers’capacitiesfordevelopingsensitiveandresponsiverelationships,especiallywiththeirownchildren.

Page 150
LimitationsofAttachmentTheoryAttachmenttheoryprovidesarichsetofinsightsintotheoriginsofdysfunctionalcare-givingandpossiblepreventiveinterventionsfocusedonparent-visitorandparent-childrelationships.Itgivesscantattentiontotherolethatindividualdifferencesininfantsmayplayasindependentinfluencesonparentalbehavior,anditprovidesinadequateattentiontoissuesofparentalmotivationforchangeincare-giving.Moreover,itminimizestheimportanceofthecurrentsocialandmaterialenvironmentinwhichthefamilyisfunctioningasinfluencesonparents’capacitiestocarefortheirchildren.Formoresystematictreatmentsoftheseissues,weturnedtoself-efficacyandhumanecologytheories(discussedabove).
SummaryoftheRoleofTheoryandEpidemiologyinProgramDesignTheprogramanditsspecificinterventionstrategieshavebeenbuiltupon:
■ theoriesabouthumandevelopmentandchange,and■ asolidunderstandingoftheriskfactorsforparticularnegativeoutcomesand
howtoreducethoserisksbypromotingadaptivebehavior.
BriefDescriptionofInterventionTheprogramofhomevisitationbeginsduringpregnancyandcontinuesthroughthechild’ssecondbirthday.Eachfamilyisassignedanursewhovisitsfamiliesaboutonceeveryotherweekduringpregnancyandthefirsttwoyearsofthechild’slife.Totheextentpossible,programsshouldkeepthesamenurseassignedtoafamilyfortheentiretimetheyparticipateintheprogram.Programprocessstudieshaveshownthatprogrameffectivenesstendstodeclinewhenfamiliesareservedbymorethanonenurseoverthecourseoftheirparticipation.
Thenursesuseprogramprotocolsthataredesignedtoaccomplishthreeoverridinggoals:(1)theimprovementofpregnancyoutcomes;(2)theimprovementofthechild’shealthanddevelopment;and(3)theimprovementofthemothers’ownpersonaldevelopment.Inthehomevisits,thenursespromotethreeaspectsofmaternalfunctioning:(a)health-relatedbehaviorsduringpregnancyandtheearlyyearsofthechild’slife;(b)thecareparentsprovidetotheirchildren;and(c)parents’familyplanning,educationalachievement,andparticipationintheworkforce.Intheserviceofthesethreegoals,thenurseslinkfamilieswithneededhealthandhumanservicesandinvolveotherfamilymembersandfriendsinthepregnancy,birth,andearlycareofthechild.
Thenursesusedetailedassessments,record-keepingforms,andprotocolstoguidetheirworkwithfamiliesbutadaptthecontentoftheirhomevisitstotheindividualneedsofeachfamily.Theyprovideacomprehensiveeducationalprogramdesignedtopromoteparents’andotherfamilymembers’effectivephysicalandemotional
APPENDIX THREE
Descriptions of Recommended Early Intervention Programmes

Page 151
careoftheirchildren.Thenursesalsohelpwomenclarifytheirgoalsanddevelopproblem-solvingskillstoenablethemtocopewiththechallengesofcompletingtheireducation,findingwork,andplanningfuturepregnancies.Developingacloseworkingrelationshipwiththemotherandherfamily,thenurseshelpmothersidentifysmallachievableobjectivesthatcanbeaccomplishedbetweenvisitsthat,ifmet,willbuildmothers’confidenceandmotivationtomanagethedemandsofcare-givingandbecomeeconomicallyself-sufficient.
Theprogramfocusesonspecificparentalbehaviorsandmodifiableenvironmentalconditionsthatareassociatedwithadverseoutcomesineachofthedomainsidentifiedasprogramgoals.Theprotocolsandrecordkeepingsystemaredesignedtoreinforcehomevisitors’focusonprogramgoalsandtheoreticalfoundationsoftheprogram.
Thenursesarescheduledtovisitfamiliesonceaweekforthefirstmonthafterregistrationandtheneveryotherweekthroughdelivery.Afterdeliverythenursesarescheduledtovisitonceaweekforthefirstsixweeksofthebaby’slifeandtheneveryotherweekuntilthe21stmonthpostpartum.From21to24monthspostpartum,thenursesvisitonceamonth.Inthesevisits,whichtypicallylastfrom60-90minutes,thenursesworktoachievethegoalsandobjectivesoutlinedabove,employingclinicalinterventionsthataregroundedintheoriesofhumanecology,attachment,andself-efficacy.Itshouldbenoted,however,thatsomemothersareincrisesthatinterferewiththeirconsistentlykeepingscheduledappointments.Althoughthenursesmakeeveryefforttofollowthespecifiedscheduleofvisits,theyareallowedtovisitmorefrequentlywhenfamiliesexhibitcrisesthatwouldwarrantmoreintensivesupport.Inaddition,althoughtherearespecifieddomainsofprogramcontentthataredevelopmentallyorganizedandexpectedtobecoveredduringparticularperiods,familiesexhibitconsiderablevariationintheirexpressedneeds.Thisleadstosubstantialindividualvariationintheamountoftimethatmaybespentonparticularprogramcontentareas.Allofthisleadstovariationintheamountandcontentoftheprogramexperiencedbyanyonefamily.Theprogramneverthelessadherestoacoresetofprogramgoals,content,andmethods.
EvidenceofProgramEffectivenessForlow-incomewomenandtheirchildren,theprogramhasbeensuccessfulin:
■ improvingwomen’sprenatalhealth-relatedbehaviors(especiallyreducingcigarettesmokingandimprovingdiet);
■ reducingpregnancycomplications,suchashypertensivedisordersandkidneyinfections;

Page 152
■ reducingharmtochildren,asreflectedinfewercasesofchildabuseandneglectandinjuriestochildrenrevealedintheirmedicalrecords;
■ improvingwomen’sownpersonaldevelopment,indicatedbyreductionsintheratesofsubsequentpregnancy,anincreaseinspacingbetweenfirstandsecondbornchildren,areductioninwelfaredependence,andreductionsinbehavioralproblemsduetosubstanceabuseandincriminalbehavioronthepartofmotherswhowereunmarriedandfromlow-incomehouseholdsatregistrationduringpregnancy;and
■ reducingcriminalandantisocialbehavioronthepartofthe15-yearoldchildrenasindicatedbyfewerarrests,convictions/violationsofprobation,anddaysofconsumingalcohol.
Thecostoftheprogram,fromthestandpointofgovernmentspending,isrecoveredbythetimethechildrenreachfouryearsofage,andthecostsavingstogovernmentandsocietyexceedthecostoftheprogrambyafactorofatleast4:1overthechild’slifetime.
IntheUKFamilyNursePartnershipstendstobedeliveredtoyoungparentse.g.uptoage20oruptoage24.
Theinformationforthisfactsheetwasexcerptedfrom:
Olds,D.,Hill,P.,Mihalic,S.,&O’Brien,R.(1998).BlueprintsforViolencePrevention,BookSeven:PrenatalandInfancyHomeVisitationbyNurses.Boulder,CO:CenterfortheStudyandPreventionofViolence.
APPENDIX THREE
Descriptions of Recommended Early Intervention Programmes

Page 153
PROMOTINGALTERNATIVETHINKINGSTRATEGIES(PATHS)
ProgramSummaryThePATHS(PromotingAlternativeTHinkingStrategies)Curriculumisacomprehensiveprogramforpromotingemotionalandsocialcompetenciesandreducingaggressionandbehaviorproblemsinelementaryschool-agedchildrenwhilesimultaneouslyenhancingtheeducationalprocessintheclassroom.Thisinnovativecurriculumisdesignedtobeusedbyeducatorsandcounselorsinamulti-year,universalpreventionmodel.Althoughprimarilyfocusedontheschoolandclassroomsettings,informationandactivitiesarealsoincludedforusewithparents.
ProgramTargetsThePATHSCurriculumwasdevelopedforuseintheclassroomsettingwithallelementaryschoolaged-children.PATHShasbeenfield-testedandresearchedwithchildreninregulareducationclassroomsettings,aswellaswithavarietyofspecialneedsstudents(deaf,hearing-impaired,learningdisabled,emotionallydisturbed,mildlymentallydelayed,andgifted).IdeallyitshouldbeinitiatedattheentrancetoschoolingandcontinuethroughGrade5.
ProgramContentThePATHSCurriculum,taughtthreetimesperweekforaminimumof20-30minutesperday,providesteacherswithsystematic,developmentally-basedlessons,materials,andinstructionsforteachingtheirstudentsemotionalliteracy,self-control,socialcompetence,positivepeerrelations,andinterpersonalproblem-solvingskills.Akeyobjectiveofpromotingthesedevelopmentalskillsistopreventorreducebehavioralandemotionalproblems.PATHSlessonsincludeinstructioninidentifyingandlabelingfeelings,expressingfeelings,assessingtheintensityoffeelings,managingfeelings,understandingthedifferencebetweenfeelingsandbehaviors,delayinggratification,controllingimpulses,reducingstress,self-talk,readingandinterpretingsocialcues,understandingtheperspectivesofothers,usingstepsforproblem-solvinganddecision-making,havingapositiveattitudetowardlife,self-awareness,nonverbalcommunicationskills,andverbalcommunicationskills.Teachersreceivetraininginatwo-tothree-dayworkshopandinbi-weeklymeetingswiththecurriculumconsultant.
ProgramOutcomesThePATHSCurriculumhasbeenshowntoimproveprotectivefactorsandreducebehavioralriskfactors.Evaluationshavedemonstratedsignificantimprovementsforprogramyouth(regulareducation,specialneeds,anddeaf)comparedtocontrolyouthinthefollowingareas:

Page 154
■ Improvedself-control,■ Improvedunderstandingandrecognitionofemotions,■ Increasedabilitytotoleratefrustration,■ Useofmoreeffectiveconflict-resolutionstrategies,■ Improvedthinkingandplanningskills,■ Decreasedanxiety/depressivesymptoms(teacherreportofspecialneeds
students),■ Decreasedconductproblems(teacherreportofspecialneedsstudents),■ Decreasedsymptomsofsadnessanddepression(childreport–specialneeds),
and■ Decreasedreportofconductproblems,includingaggression(childreport).
ProgramCostsProgramcostsoverathree-yearperiodwouldrangefrom$15/student/yearto$45/student/year.Thehighercostwouldincludehiringanon-sitecoordinator,thelowercostwouldincluderedeployingcurrentstaff.
ProgramBackgroundThePATHS(PromotingAlternativeTHinkingStrategies)Curriculumwasdevelopedtofilltheneedforacomprehensive,developmentally-basedcurriculumintendedtopromotesocialandemotionalcompetenceandpreventorreducebehaviorandemotionalproblems.Fromitsinception,thegoalofPATHSwasfocusedonpreventionthroughthedevelopmentofessentialdevelopmentalskillsinemotionalliteracy,positivepeerrelations,andproblem-solving.TheCurriculum(Kusché&Greenberg,1994)isdesignedtobetaughtbyelementaryschoolteachersfromgradeKthroughgrade5.
Twodecadesofpriorresearchhadindicatedanincreasingemphasisontheneedforuniversal,school-basedcurriculaforthepurposesofbothpromotingemotionalcompetenceanddecreasingriskfactorsrelatedtolatermaladjustment.However,althoughpreviousresearchhassuggestedthatsuchapproachesmightbeespeciallyeffectiveduringtheelementaryschoolyears,mostevaluationshadbeenrestrictedinscopeand/orhadinvolvedprogramswithconsiderablelimitations(e.g.,narrowdevelopmentalfocus,shortduration,andunreliableandinvalidoutcomemeasures).Extensivefocusonteachingemotionalcompetency,understanding,andawarenesswasnotablylacking,andcomprehensiveevaluationsandinclusiveprogramswererare.Theseshortcomingsweresurprising,giventhewiderangeofcurriculautilizedinelementaryeducationthatwereintendedtopromotesocialcompetenceandpreventdisorder.Nevertheless,researchstronglysuggestedthatacomprehensivepreventionprogramintheclassroomsettinghadthepotentialtoprovidemuchneededassistanceforbothnormally-adjustedandbehaviorallyat-riskstudents.
APPENDIX THREE
Descriptions of Recommended Early Intervention Programmes

Page 155
Inaddition,webelievedthattherapidandcomplexculturalchangesofthepastfewdecades,aswellasthosepredictedfortheforeseeablefuture,madeemotionalandsocialcompetencycrucialrequirementsforadaptiveandsuccessfulfunctioningofchildrenandfortheircontinuingadaptationasadolescentsandadults.Althoughsocialandemotionalcompetencehadneverbeenconsideredanecessarycomponentofeducationinthepast,wefeltthatithadbecomeascriticalforthebasicknowledgerepertoireofallchildrenasreading,writing,andarithmetic.Teachersacknowledgedthattheyhadlittlebackgroundorestablishedstrategiestodealwithemotionalandsocialcompetency,sowefeltthatitwasnecessarytoprovidedetailedlessons,aswellasmaterialsandinstruction.
Aswithmanyofthemorerecentschool-basedpreventiveinterventions,PATHSwasdesignedtobetaughtbyregularclassroomteachers(initiallywithsupportfromprojectstaff)asanintegratedcomponentoftheregularyear-longcurriculum.However,itisimportanttoensurethatchildrengeneralize(i.e.,applytheskillstonewcontexts)theuseofPATHSskillstotheremainderofthedayandtoothercontexts.Thus,generalizationactivitiesandstrategieswereincorporatedtobeusedin(andoutsideof)theclassroomthroughouteachschoolday,andmaterialswereincludedforusewithparents.
Morerecentliteraturereviewshaveindicatedthatsuccessfulprogramshavethefollowingcharacteristics:(a)utilizingaprogramoflongerduration,(b)synthesizinganumberofsuccessfulapproaches,(c)incorporatingadevelopmentalmodel,(d)providinggreaterfocusontheroleofemotionsandemotionaldevelopment,(e)providingincreasedemphasisongeneralizationtechniques,(f)providingongoingtrainingandsupportforimplementation,and(g)utilizingmultiplemeasuresandfollow-upsforassessingprogrameffectiveness.
Allsevenoftheseunder-emphasizedbutcriticalfactorshavebeenincorporatedintothePATHScurriculum.Furthermore,asPATHShasbeenutilizedwithdifferentcohortsandpopulationsoverthepast15years,multiplefield-testswithextensivefeedbackfromteachershasledtoexpansionandimprovementinPATHSovertime.
TheoreticalRationale/ConceptualFrameworkThePATHSprevention-interventionprogramisbasedonfiveconceptualmodels.Thefirst,theABCD(Affective-Behavioral-Cognitive-Dynamic)ModelofDevelopmentfocusesonthepromotionofoptimaldevelopmentalgrowthforeachindividual.Thesecondmodelincorporatesaneco-behavioralsystemsorientationandemphasizesthemannerinwhichtheteacherusesthecurriculummodelandgeneralizestheskillstobuildahealthyclassroomatmosphere(i.e.,onethatsupportsthechildren’suseandinternalizationofthematerialtheyhavebeentaught).Thethirdmodelinvolvesthedomainsofneurobiologyandbrain

Page 156
structuralization/organization,whilethefourthparadigminvolvespsychodynamiceducation(derivedfromDevelopmentalPsychodynamicTheory).Finally,thefifthmodelincludespsychologicalissuesrelatedtoemotionalawareness,orasitismorepopularlylabeled,emotionalintelligence.
TheABCDModelTheABCDmodelincorporatesaspectsofdiversetheoriesofhumandevelopmentincludingpsychodynamicdevelopmentaltheory,developmentalsocialcognition,cognitivedevelopmentaltheory,cognitivesocial-learningtheory,andattachmenttheory.TheABCDmodelplacesprimaryimportanceonthedevelopmentalintegrationofaffect(i.e.,emotion,feeling,mood)andemotionlanguage,behavior,andcognitiveunderstandingtopromotesocialandemotionalcompetence.Abasicpremiseisthatachild’scoping,asreflectedinhisorherbehaviorandinternalregulation,isafunctionofemotionalawareness,affective-cognitivecontrol,andsocial-cognitiveunderstanding.ImplicitintheABCDmodelistheideathatduringthematurationalprocess,emotionaldevelopmentprecedesmostformsofcognition.Thatis,youngchildrenexperienceemotionsandreactonanemotionallevellongbeforetheycanverbalizetheirexperiences.Inearlylife,affectivedevelopmentisanimportantprecursorofotherwaysofthinkingandlaterneedstobeintegratedwithcognitiveandlinguisticabilities,whichareslowertodevelop.Table1presentsasummaryofstagesintheABCDModel(SeeGreenberg&Kusché,1993forelaboration).
Duringthefirstthreeyearsoflife,theentirerepertoireofemotionalsignalsdevelops,andthesesignals/displaysaresubsequentlyusedthroughouttherestofanindividual’slifetime.Thus,bythetimechildrenarebeginningtoutilizelanguagefluentlytoexpressinternalstatesofbeing(e.g.,feelingsad,happy,jealous),mostoftheiremotionalresponseshavealreadybecomehabitual.
Bytheendofthepreschoolyears,mostchildrenhavebecomeskilledinbothshowingandinterpretingemotionaldisplays,althoughthereareconsiderableindividualdifferencesinchildren’semotionalprofiles.Thechildalsobeginstodemonstrateaffectiveperspective-takingskills(i.e.,theabilitytodifferentiatetheemotions,needs,anddesiresofdifferentpeopleinaparticularcontext).Thepreschoolergraduallyfindsnewwaystocopewithunpleasantemotionsanddiscoversthatinternallyexperiencedaffectscanbedirectlysharedwithothersthroughverbalmeans.Furthermore,thechildbeginstoregulateinternalaffectivestatesthroughverbalself-regulation,acriticaldevelopmentalachievement.Anexampleofthisabilityiswhenapreschoolerisabletotellsomeoneheisangryinsteadofshowingaggressiontowardsapeerorobject.
Betweentheagesof5and7,childrenundergoamajordevelopmental
APPENDIX THREE
Descriptions of Recommended Early Intervention Programmes

Page 157
transformationthatgenerallyincludesincreasesincognitiveprocessingskills,aswellaschangesinbrainsizeandfunction.Thistransitionandtheaccompanyingalterationsallowchildrentoundertakemajorchangesinresponsibilities,independence,andsocialroles.
Duringtheelementaryschoolyears,furtherdevelopmentalintegrationsoccurbetweenaffect,behavior,andcognition/language.Thisintegrationisofcrucialimportanceinachievingsociallycompetentactionandhealthypeerrelations.Forexample,intheearlyelementaryyearswhenachildhasbeenrebuffedwhenattemptingtoenteragamewithpeers,shemightwalkaway,calmdown,assesshowbothsheandtheotherkidsfeel,andthinkofanotherstrategytoenterthegame,orthinkofsomethingelsetodoorsomeoneelsewithwhomshecanplay.
Althoughresearchhasdemonstratedthelinkagebetweendeficitsinemotionaldevelopmentandpsychopathology,surprisinglylittleattentionhasbeenpaidtothecrucialroleofemotionaldevelopmentinmodelsofpreventiveintervention.Takingthisfactorintoaccount,thePATHSCurriculummodelsynthesizesthedomainsofself-control,emotionalawarenessandunderstanding,andsocialproblem-solvingtoincreasesocialandemotionalcompetence.
Table 1 ABCDModel(Affective-Behavioral-Cognitive-Developmental)
StagesofDevelopmentalIntegration
1.Infancy(Birthto18months)
Emotion=CommunicationArousalandDesire=Behavior
2.Toddlerhood(18monthsto36months)
LanguageSupplementsEmotion=CommunicationVeryInitialDevelopmentofEmotionalLabelingArousalandDesire=Behavior
3.PreschoolYears(3to6years)
LanguageDevelopsPowerfulRoleinCommunicationChildcanRecognize/LabelBasicEmotionsArousalandDesire>SymbolicMediation>BehaviorDevelopmentofRole-takingAbilitiesBeginningofReflectiveSocialPlanningProblem-Solving(GenerationofAlternativePlansforBehavior)
4.SchoolYears(6to12-13years)
ThinkinginLanguagehasbecomeHabitualIncreasingAbilitytoReflectonandPlanSequencesofActionDevelopingAbilitytoConsiderMultipleConsequencesofActionIncreasingAbilitytoTakeMultiplePerspectivesonaSituation
5.Adolescence UtilizeLanguageintheServiceofHypotheticalThoughtAbilitytoSimultaneouslyConsiderMultiplePerspectives

Page 158
TheEco-BehavioralSystemsModelThesecondconceptualmodelincorporatesaneco-behavioralsystemsorientationandexamineslearningprimarilyatthelevelofsystemschange.School-basedprogramsthatfocusindependentlyonthechildorenvironmentarenotaseffectiveasthosethatsimultaneouslyeducatethechildandinstillpositivechangesintheenvironment.Trainingprogramsmayappropriatelybeconsideredperson-centeredwhenskillsaretaughtintheabsenceofcreatingenvironmentalsupportsforcontinuedskillapplicationindailyinteractions.Incontrast,ecologicallyorientedprogramsemphasizenotonlytheteachingofskills,butalsothecreationofmeaningfulreal-lifeopportunitiestouseskillsandtheestablishmentofstructurestoprovidereinforcementforeffectiveskillapplication.Thus,althoughacentralgoalofPATHSistopromotethedevelopmentalskillsofeachchildbyprovidinglearningthatintegratesaffect,cognition,andbehavior,acriticalingredientforsuccessisthedevelopmentofahealthyclassroomandschoolenvironment.
Fromthisperspective,thesuccessofskillstrainingprogramsmaydependlargelyontheirattentiontoencouragingandsupportingsocializationpatternsandsupportsintheinterventionsetting.Forexample,ecologicallyorientedproblem-solvingprogramstrytointroduceacommonsocialinformationprocessingframeworkthatchildrenandteacherscanusetocommunicatemoreeffectivelyaboutproblemsituations.Inotherwords,theytrytochangenotonlythechild’sbehavior,butalsotheteacher’sbehavior,therelationshipbetweentheteacherandchild,andclassroomandschool-levelresourcesandprocedurestosupportadaptiveproblem-solvingefforts,assumingthattheinteractionsaredysfunctionalorineffective.
Thegeneralizationprocedures,extensiveteachertraining,andfocusonsomelevelofparentparticipationusedinPATHShavethegoalofcombiningclassroominstructionwitheffortstocreateenvironmentalsupportandreinforcementfrompeers,familymembers,schoolpersonnelhealthprofessionals,andotherconcernedcommunitymembers.Further,trainingemphasizesthemannerinwhichtheteacherusesthecurriculummodelandgeneralizestheskillstobuildahealthyclassroomatmosphere(i.e.,onethatsupportsthechildren’suseandinternalizationofthematerialtheyhavebeentaught).
NeurobiologyandBrainStructuralization/OrganizationWhendesigningPATHS,wepaidspecialattentiontodevelopmentalmodelsofbrainorganization.Twoofthemostrelevantconceptsweincorporatedinvolve“vertical”controland“horizontal”communication(Kusché,1984).
“Vertical”controlreferstohigher-orderprocessingandregulationofemotionandactionsbythefrontallobesoverthelimbicsystemandsensory-motorareas.Whenadultsfirstexperienceemotionalinformation,itisrapidlyperceivedandprocessed
APPENDIX THREE
Descriptions of Recommended Early Intervention Programmes

Page 159
inthelimbicsysteminthemiddlepartofthebrain.Thisinitialinformationisthentransmittedtothefrontallobesintheneocortexforfurtherprocessingandinterpretation,and,subsequently,thefrontallobescantransmitmessagesbacktothelimbicsystemtomodifyemotionsignalsandtothesensory-motorcortextoinfluencepotentialactions.
Forexample,ifyousawacarcomingtowardsyouandyoustartledandjumpedtothesideoftheroad,allofthisrapidprocessingwouldhaveoccurredprimarilyinthelimbicsystemwithoutanytrueconsciousawarenessonyourpart.Afterwards,however,youwouldtakeinandprocessfurtherinformationatacorticallevel(e.g.,thethought,“Thatcaralmosthitme!”;thecolorofthecar;thelicenseplatenumber,etc.).Inadditiontotheinitialfear,youwouldprobablystarttofeelangry,aswellasrelieved,andyoumightdecidetoreporttheincidenttothepolice.
Rapidprimaryprocessingissometimescrucialforsurvival,asinthiscase,butsecondaryprocessinginthefrontalcortexisimportantbecauseitallowsustointegratedatainvolvingemotionswithknowledge-basedinformation,which,inturn,assistswithmakingappropriateplansforfurtheraction.
Earlyindevelopment(i.e.,bythetimeoftoddlerhood),therearefewinterconnectionsbetweenthelimbicsystemandthefrontallobes;thus,duringthe“terrible-twos,”childrenfrequentlyhit,bite,orkick“automatically”whentheyfeelangry.Aschildrenmature,however,increasingneuronalinterconnectionsevolvebetweenthefrontallobesandthelimbicsystem.Thisisespeciallyimportantwithregardtothedevelopmentofselfcontrol,becausethefrontalcortexbecomesincreasinglyabletoregulateimpulsesfromthelimbicareasandmodifypotentialactions.Betweentheagesof5and7,amajorshiftoccursinwhichnetworksinthefrontalareasachievesignificantdominancewithregardtoexertingemotionalself-regulationandbehavioralself-control.
However,thesedevelopmentalmilestonesdonotautomaticallyunfold,butratherareheavilyinfluencedbyenvironmentalinputthroughoutearlychildhood.Moreover,ifthesenetworksdonotdevelopinanoptimalmanner,childrenwillnothavetheneuronalstructurenecessarytocontroltheiractionsinresponsetostrongemotionalsignals.
Thus,inordertopromotethedevelopmentofexecutiveorverticalcontrolwithPATHS,weteachchildrentopracticeconsciousstrategiesforself-control,includingself-talk(i.e.,verbalmediationandtheControlSignalsPoster).Foryoungerchildrenandthosewitheitherdelayedlanguageordifficultiesinbehavioralandemotionalcontrol,weutilizethe“TurtleTechnique,”whichincludesamotor-inhibitingresponseinadditiontoself-talk.

Page 160
“Horizontal”communicationreferstoaphenomenonthatresultsfromtheasymmetryofinformationprocessinginthetwohalvesoftheneocortex(theoutermostandevolutionarilynewerpartofthebrain).
Thelefthemisphereisresponsibleforprocessingreceptiveandexpressivelanguageaswellasexpressingpositiveaffect.TherighthemisphereisspecializedforprocessingbothcomfortableanduncomfortablereceptiveaffectanduncomfortableexpressiveaffectinthemajorityofEnglish-speakingadults,theonlyculturalgrouponwhichresearchisavailable(Bryden&Ley,1983).
Nonlinguisticinformation(suchasemotionalsignals)isoftenprocessedwithoutawareness(preconsciousprocessing)unlessweverbally“think”aboutit.Toverballylabelouremotionalexperiences,andthusbecomeconsciouslyawareofthem,thisinformationmustbetransmittedtothelefthemisphere.However,theleftandrighthemispherescancommunicatewithoneanotheronlyviathecorpuscallosum,a“bridge”thathorizontallyconnectsthetwosidesofthebrain.Therefore,inordertobetrulyawareofouremotionalexperiences,wemustutilizeboththerightandlefthemispheres.Thelanguageareasontheleftsideofthebraincanalsomodifyandinfluenceaffectiveprocessingintheright(Davidson,1998;Sutton&Davidson,1997).
Aninterestingsituationoccursif,forsomereason,emotioninformationdoesnotreachthelefthemisphere(e.g.,anadequateneuralnetworkhasneverdevelopedorinterconnectionsareblockedfromintercommunication).Whenthisoccurs,anindividualwillexperienceemotion,butwillnotbeawareofhavingdoneso.Thus,otherpeoplecanbeawareofhowthepersonfeels(i.e.,byobservingfacialcues),buttheindividualwillnotbeawareofhavingexperiencedthefeelings.Afrequentillustrationofthisphenomenonoccurswhenateacherobservesachildwhoisclearlyfeelingangry,butthatchildtrulyhasnoconsciousawarenessofsuchanemotion(“Iamnotangry;Ifeelfine”).
Developmentofthecorpuscallosumisrelativelyslow,sothatitisonlywithmaturationthatoptimumhemisphericcommunicationispossible.Aswithverticalneuralnetworks,thewayinwhichinterhemisphericcommunicationoccursdependsheavilyonenvironmentalinputduringdevelopment.
Basedonthistheoryof“horizontal”communicationandcontrol,wehypothesizedthatverbalidentificationandlabeling,especiallyofuncomfortablefeelings,wouldpowerfullyassistwithmanagingthesefeelings,controllingbehavior,andimprovinghemisphericintegration.Thus,westresstheuseofFeelingFacecardsthatincludeboththefacialdrawingofeachaffect(recognitionofwhichismediatedbytherighthemisphere)anditsprintedlabel(whichismediatedbytheleft).In
APPENDIX THREE
Descriptions of Recommended Early Intervention Programmes

Page 161
addition,wealsoutilizeacolor-codeddifferentiationofcomfortable(yellow)versusuncomfortable(blue)feelings.Inaddition,encouragingchildrentotalkaboutemotionalexperiences(bothatthetimetheyareoccurringandinrecollection)furtherstrengthensneuralintegration.
Insummary,ourknowledgeoftheneurobiologicaldevelopmentofthebrainwasheavilyinfluentialinthedevelopmentofPATHS.Researchstronglysuggeststhatlearningexperiencesinthecontextofmeaningfulrelationshipsduringchildhoodinfluencethedevelopmentofneuralnetworksbetweendifferentareasofthebrain,whichinturnaffectself-controlandemotionalawareness.Thus,weincorporatedstrategiesinPATHStooptimizethenatureandqualityofteacher-childandpeer-peerinteractionsthatarelikelytoimpactbraindevelopmentaswellaslearning(Greenberg&Snell,1997).Optimumdevelopmentofboth“vertical”and“horizontal”communicationandcontrolduringchildhoodshouldpromotebetteradaptationinbothcurrentandlaterlife.
PsychodynamicEducationTheapplicationofpsychoanalytictheorytotheeducationofchildrenhasonlyrecentlyreceivedsignificantattention.Psychodynamiceducationisintendedtoenhancedevelopmentalgrowth,promotementalhealth,andpreventemotionaldistress,butitisnottreatment.Inthisregard,teachersarenottherapistsandarenotexpectedtoactassuch.However,teachersarepowerfulrolemodels(individualswithwhomchildrencanidentifyinapositivemanner),andtheinformationtheyimpartisoftengiventhestatusofabsolutetruth(i.e.,omniscience),especiallyduringtheelementaryschool-ageyears.Whenteachersexpressaninterestinchildren’sfeelingsandemotionalexperiencesorshowrespectforchildren’sopinions,theirstudentsareimpactedinaprofoundmanner.Astheteacher-studentrelationshipsgrowincreasinglymorepositiveandenriched,learningisenhanced.
Psychodynamiceducationisderivedfromadevelopmentaltheoryandaimstocoordinatesocial,emotional,andcognitivegrowth.Teachersareencouragedtoutilizeactualclassroomexperiencesandusechildren’screative,imaginalprocesses.Studentscanthendevelopahealthysenseofself-esteemfromobservingthepositivereactionsofotherstowardsthem,notbecausetheyhavebeenencouragedtoparrotsimplisticaffirmations.Further,teachersplayacrucialrolebyprovidingclarificationsandexplanationsofemotionsandsituations.Animportantwayinwhichpsychodynamiceducationdiffersfromothermodelsisitsemphasisoninternalization,theprocessofhealthydevelopmentofconscience,or“takingownership”andself-responsibilityforone’sactions.
Bypromotingthedevelopmentofinternalself-controlandself-motivationalongwithhealthystandardsforbehavior,childrendevelopanoptimalsenseofautonomy

Page 162
anddecision-makingwhilealsoconsideringtheneedsandfeelingsofothers.Forexample,studentscontemplateanddiscusstheconsequencesofhavinggoodvs.badmannersandevaluatewhygoodmannersareimportant(e.g.,thewayweactaffectshowotherpeoplefeel),ratherthansimplybeingtaughtalistofgoodmannersthattheyaresupposedtouse.Inthisway,thechildrencometo“own”theconceptsasbelongingtothemselves(i.e.,theyinternalizethem);asaresult,theyvoluntarilychoosetousegoodmannersbecausetheybelieveitistherightthingtodo.
Insummary,someofthelong-rangegoalsofpsychodynamiceducationareforeachchildtodevelopakindbutfairsenseofprosocialbehavioralcontrol,positivesenseofself,respectforselfandothers,healthyinternalmotivation,curiosityandloveforlearning,andsoonthatoperateindependentlyoftheexternalenvironment.Thesefactorsenhancedevelopmentalgrowth,improveschoolfunctioning,andoptimizementalhealth,whilepreventingantisocialtendencies,violentbehavior,andsubstanceabuse.
PsychologicalIssuesRelatedtotheCrucialRoleofEmotionalAwarenessResearchsuggeststhataschildrendevelopmorecomplexandaccurateplansandstrategiesregardingemotions,theseplanshaveamajorinfluenceontheirsocialbehavior.Forexample,theabilitytothinkthroughproblemsituationsandtoanticipatetheiroccurrenceiscriticalforsociallycompetentbehavior.However,these“cold”cognitiveprocessesareunlikelytobeeffectivelyutilizedinrealworldconditions(e.g.,whenbeingteased)unlessthechildcanbothaccuratelyprocesstheemotionalcontentofthesituationandeffectivelyregulatehisorheremotionalarousalsothatheandshecanthinkthroughtheproblem.
Similarly,ifchildrenmisidentifytheirownfeelingsorthoseofothers,theyarelikelytogeneratemaladaptivesolutionstoaproblem,regardlessoftheirintellectualcapacities.Inadditiontothesetypesofchallenges,thechild’smotivationtodiscussthesefeelingsandproblem-solveininterpersonalcontextswillalsobegreatlyimpactedbythemodelingandreinforcementofadultsandpeers.
Emotionalawarenessandunderstandingareimplicitinmanymodelsthathavebeendevelopedtopromotesocialcompetence,buthaverarelybeenacentralfocus,eventhoughnumerousstudieshaveassessedsocialproblem-solvingabilityasbothamediatorandoutcomeofintervention.Recently,emotionalcompetencehasbeensubsumedunderanew,morepopularterm,emotionalintelligence(Goleman,1995;Mayer&Salovey,1997),definedastheabilitytorecognizeemotionalresponsesinoneself,otherpeople,andsituations,andusethisknowledgeineffectiveways(e.g.,inmanagingone’sownemotionalresponses,motivatingoneself,andhandlingrelationshipseffectively).“Self-awareness—recognizingafeelingasithappens—isthekeystoneofemotional
APPENDIX THREE
Descriptions of Recommended Early Intervention Programmes

Page 163
intelligence….[T]heabilitytomonitorfeelingsfrommomenttomomentis[also]crucialtopsychologicalinsightandself-understanding.Aninabilitytonoticeourtruefeelingsleavesusattheirmercy.Peoplewithgreatercertaintyabouttheirfeelingsarebetterpilotsoftheirlives”(Goleman,1995,p.43).Thus,ithasbeenproposedthatemotionalintelligencemaybemoreimportantthancognitiveintelligenceinachievingsuccessandhappinessinlife.
Assuch,acentralfocusofPATHSisencouragingchildrentodiscussfeelings,experiences,opinions,andneedsthatarepersonallymeaningful,andmakingthemfeellistenedto,supported,andrespectedbybothteachersandpeers.Asaresult,theinternalizationoffeelingvalued,caredfor,appreciated,andpartofasocialgroupisfacilitated,which,inturn,motivateschildrentovalue,carefor,andappreciatethemselves,theirenvironment,theirsocialgroups,otherpeople,andtheirworld.
Thisfocuscannotbeemphasizedenough.Althoughallchildrenneedtofeellistenedtoorrespectedbyothers,especiallyadults,manychildrendonothaveanadultrolemodelwhowillsupporttheminthismanner;hence,theydonotlearntorespectthemselvesorothers.Theseaspectsofsocializationmustbetaughttochildren,andtobecometrulysocialized,childrenmustinternalizeandembracethemastheirown,hopefullypriortoreachingadolescence.Itisimportanttorecognize,however,thatthiscannotbeforceduponchildren,butratherisbestachievedthroughnurturanceandrespect.
BriefDescriptionofInterventionThePATHSCurriculumconsistsofanInstructionalManual,sixvolumesoflessons,pictures,photographs,posters,FeelingFaces,andadditionalmaterials.PATHSisdividedintothreemajorunits:(1)theReadinessandSelf-ControlUnit,12lessonsthatfocusonreadinessskillsanddevelopmentofbasicself-control;(2)theFeelingsandRelationshipsUnit,56lessonsthatfocusonteachingemotionalandinterpersonalunderstanding(i.e.,EmotionalIntelligence);and(3)theInterpersonalCognitiveProblem-SolvingUnit,33lessonsthatcoverelevenstepsforformalinterpersonalproblem-solving.TwofurtherareasoffocusinPATHSinvolvebuildingpositiveself-esteemandimprovingpeercommunications/relations.Ratherthanhavingseparateunitsonthesetopics,relevantlessonsareinterspersedthroughouttheotherthreeunits.ThereisalsoaSupplementaryUnitcontaining30lessonswhichreviewandextendPATHSconceptsthatarecoveredinthemajorthreeunits.ThePATHSunitscoverfiveconceptualdomains:
1. self-control,2. emotionalunderstanding,3. positiveselfesteem,

Page 164
4. relationships,and5. interpersonalproblemsolvingskills.
Eachofthesedomainshasavarietyofsub-goals,dependingontheparticulardevelopmentallevelandneedsofthechildrenreceivinginstruction.
PATHSisanexpansiveandflexibleprogramthatallowsimplementationofthe131lessonsovera5yearperiod,butitshouldbenotedthatanyparticularlessonisnotnecessarilyequivalenttoonesession;indeed,dependingontheneedsofanyspecificclassroom,onePATHSlessoncanrunfromonetofiveormorePATHSsessions.Picturesandphotographsareincludedforallofthelessons,withsmallergraphicsprovidedinthemarginsofthescriptstomakethecurriculummoreuser-friendly.MostofthematerialsthatareneededareincludedinThePATHSCurriculumkit,butsupplementarymaterialscancertainlybeaddedasdesired.
AseparatevolumeisalsoincludedwithPATHStoserveasanInstructionalManualforteachers.Toencouragegeneralizationtothehomeenvironment,parentlettersandinformationareprovidedperiodicallyinthecurricularlessonsandcanbesenthomebytheteachersasdesired.“Homeactivityassignments”(separateversionsforyoungerandolderstudents)arealsoincludedforchildrentodoathome(e.g.,Askyourmomordadorotheradultaboutatimewhentheyfeltproud)tofurtherinvolveparents(pleaseseeAppendicesEandF).
EvidenceofProgramEffectivenessThreecontrolledstudieswithrandomizedcontrolvs.experimentalgroups(usingoneyearofPATHSimplementationwithpre,post,andfollow-updata)havebeenconductedbythepresentauthors.Thesehaveincludedthreedifferentpopulationsincludingdeaf/hearingimpaired,regulareducation,andspecialeducation-classifiedchildren.
TherobustRCTevaluationofthePATHSprogrammeinCraigavon/Lurganshouldreportin2012.
IncreasingProtectiveFactorsInallthreeclinicaltrials,comparedtomatchedcontrolchildren,theuseofthePATHSCurriculumhassignificantlyincreasedthechildren’sabilityto:■ Recognizeandunderstandemotions■ Understandsocialproblems■ Developeffectivealternativesolutions■ Decreasethepercentageofaggressive/violentsolutions
APPENDIX THREE
Descriptions of Recommended Early Intervention Programmes

Page 165
Inallthreegroupsofchildren,teachersreportsignificantimprovementsinchildren’sprosocialbehaviorinthefollowingdomains:
■ Self-control■ Emotionalunderstanding■ Abilitytotoleratefrustration■ Useofeffectiveconflict-resolutionstrategies
CognitivetestingindicatesthatPATHSleadstoimprovementsinthefollowingskills:
■ Abilitytoplanaheadtosolvecomplextaskswithnormalandspecialneedschildren(WISC-RBlockDesignandAnalogiesoftheTestofCognitiveAbilities;nottestedintheDeaf/Hearing-Impairedgroup)
■ Cognitiveflexibilityandlowimpulsivitywithnon-verbaltasks(CodingfromtheWISC-R)
■ Improvedreadingachievementforyoungdeafchildren
ReducingMaladaptiveOutcomesTeachersreportthefollowingreductionsinbehavioraldifficultiesatone-yearpostintervention:
■ Decreasedinternalizingsymptoms(sadness,anxiety,andwithdrawal)inspecialneedsclassrooms
■ Decreasedexternalizingsymptoms(aggressiveanddisruptivebehavior)inspecialeducationclassrooms
Students(inregularandspecialneedsclasses)self-reportthefollowingreductionsinbehavioraldifficultiesatone-yearpostintervention:
■ Decreasedsymptomsofsadnessanddepression(ChildDepressionInventory)■ Decreasedreportofconductproblems
InitialFindingfromtheNationalFastTrackDemonstrationProgramTheFT/PATHSCurriculum(arevisedversionofPATHSwhichmaintainsthecriticalcomponentsoftheoriginalcurriculum)isthecentraluniversalpreventioncomponentoftheFastTrackProgram.FastTrackisacomprehensiveprogramwhosegoalsincludethepreventionofaggressionanddelinquencyandthepromotionofsocialandacademiccompetence.TheFastTrackPrograminvolvesalongitudinaldesignandisconductedinfourAmericanlocations(Seattle,Nashville,Durham,andruralPennsylvania).Findingsattheendoffirstgrade(afteroneyearofimplementation)indicatethatinschoolsinwhichPATHSis

Page 166
operating,thereisimprovedsocialadaptation(ascomparedtomatchedcontrolschools)asindexedbymorepositivereportsofthefollowingdimensions:
■ Lowerpeeraggressionscoresbasedonpeerratings(Sociometrics)■ Lowerteacherratingsofdisruptivebehavior(Teacherreport)■ Improvedclassroomatmosphere(assessedbyIndependentObservers)
Theinformationforthisfactsheetwasexcerptedfrom:
Greenberg,M.T.,Kusché,C.&Mihalic,S.F.(1998).BlueprintsforViolencePrevention,BookTen:PromotingAlternativeThinkingStrategies(PATHS).Boulder,CO:CenterfortheStudyandPreventionofViolence.
APPENDIX THREE
Descriptions of Recommended Early Intervention Programmes

Page 167
INCREDIBLEYEARSSERIES(IYS)
ProgramSummaryTheIncredibleYearsSeriesisasetofthreecomprehensive,multi-faceted,anddevelopmentally-basedcurriculumsforparents,teachersandchildrendesignedtopromoteemotionalandsocialcompetenceandtoprevent,reduce,andtreatbehaviorandemotionproblemsinyoungchildren.
ProgramTargetsChildren,agestwototen,atriskforand/orpresentingwithconductproblems(definedashighratesofaggression,defiance,oppositionalandimpulsivebehaviors).Theprogramshavebeenevaluatedas“selected”preventionprogramsforpromotingthesocialadjustmentofhighriskchildreninpreschool(HeadStart)andelementarygrades(uptogradethree)andas“indicated”interventionsforchildrenexhibitingtheearlyonsetofconductproblems.
ProgramContentThisseriesofprogramsaddressesmultipleriskfactorsacrosssettingsknowntoberelatedtothedevelopmentofConductDisordersinchildren.Inallthreetrainingprograms,trainedfacilitatorsusevideotapescenestoencouragegroupdiscussion,problem-solving,andsharingofideas.TheBASICparentseriesis“core”andanecessarycomponentofthepreventionprogramdelivery.Theotherparenttraining,teacher,andchildcomponentsarestronglyrecommendedwithparticularpopulationsthataredetailedinthisdocument.
IncredibleYearsTrainingforParentsTheIncredibleYearsparentingseriesincludesthreeprogramstargetingparentsofhigh-riskchildrenand/orthosedisplayingbehaviorproblems.TheBASICprogramemphasizesparentingskillsknowntopromotechildren’ssocialcompetenceandreducebehaviorproblemssuchas:howtoplaywithchildren,helpingchildrenlearn,effectivepraiseanduseofincentives,effectivelimit-settingandstrategiestohandlemisbehavior.TheADVANCEprogramemphasizesparentinterpersonalskillssuchas:effectivecommunicationskills,angermanagement,problem-solvingbetweenadults,andwaystogiveandgetsupport.TheSUPPORTINGYOURCHILD’SEDUCATIONprogram(knownasSCHOOL)emphasizesparentingapproachesdesignedtopromotechildren’sacademicskillssuchas:readingskills,parentalinvolvementinsettinguppredictablehomeworkroutines,andbuildingcollaborativerelationshipswithteachers.
IncredibleYearsTrainingforTeachersThisseriesemphasizeseffectiveclassroommanagementskillssuchas:theeffectiveuseofteacherattention,praiseandencouragement,useofincentivesfordifficult

Page 168
behaviorproblems,proactiveteachingstrategies,howtomanageinappropriateclassroombehaviors,theimportanceofbuildingpositiverelationshipswithstudents,andhowtoteachempathy,socialskillsandproblem-solvingintheclassroom.
IncredibleYearsTrainingforChildrenTheDinosaurCurriculumemphasizestrainingchildreninskillssuchasemotionalliteracy,empathyorperspectivetaking,friendshipskills,angermanagement,interpersonalproblem-solving,schoolrulesandhowtobesuccessfulatschool.Thetreatmentversionisdesignedforuseasa“pullout”treatmentprogramforsmallgroupsofchildrenexhibitingconductproblems.Thepreventionversionisdeliveredtotheentireclassroombyregularteachers,twotothreetimesaweek.
ProgramOutcomesMultiplerandomizedcontrolgroupevaluationsoftheparentingseriesindicatesignificant:
■ Increasesinparentpositiveaffectsuchaspraiseandreduceduseofcriticismandnegativecommands.
■ Increasesinparentuseofeffectivelimit-settingbyreplacingspankingandharshdisciplinewithnon-violentdisciplinetechniquesandincreasedmonitoringofchildren.
■ Reductionsinparentaldepressionandincreasesinparentalself-confidence.■ Increasesinpositivefamilycommunicationandproblem-solving.■ Reducedconductproblemsinchildren’sinteractionswithparentsand
increasesintheirpositiveaffectandcompliancetoparentalcommands.
Multiplerandomizedcontrolgroupevaluationsoftheteachertrainingseriesindicatesignificant:
■ Increasesinteacheruseofpraiseandencouragementandreduceduseofcriticismandharshdiscipline.
■ Increasesinchildren’spositiveaffectandcooperationwithteachers,positiveinteractionswithpeers,schoolreadinessandengagementwithschoolactivities.
■ Reductionsinpeeraggressionintheclassroom.
Multiplerandomizedcontrolgroupevaluationsofthechildtrainingseriesindicatesignificant:
■ Increasesinchildren’sappropriatecognitiveproblem-solvingstrategiesandmoreprosocialconflictmanagementstrategieswithpeers.
APPENDIX THREE
Descriptions of Recommended Early Intervention Programmes

Page 169
■ Reductionsinconductproblemsathomeandschool.
IndependentreplicationsinEngland,Wales,Norway,Canada,andtheUSconfirmthesefindings.
ProgramCostsThecostsofcurriculummaterials,includingvideoorDVDs,comprehensivemanuals,booksandotherteachingaidsfortheParentTrainingProgramare$1,300fortheBASICprogram,$775fortheADVANCEprogram,$1250fortheSCHOOLprogram;$1,250fortheTeacherTrainingProgram;and$1250fortheChildTrainingProgram.Discountsareavailableforpurchasesofmorethanonesetofanyprogram.Trainingandtechnicalassistancecostsarechargedbasedonadailyfee.
ProgramBackgroundThemissionoftheIncredibleYearsTrainingSeriesistopromotepositive,effective,andresearch-basedparentingandteachingpracticesandstrategieswhichstrengthenyoungchildren’ssocialcompetenceandproblem-solvingstrategiesandreduceaggressionathomeandatschool.Therearethreetypesofinterlockingtrainingcurriculums,whicharetargetedatparents,teachersandchildren(agestwotoeightyears).Initially,inthe1980’s,theBASICparentprogramwasevaluatedandfoundtobeverysuccessfulinpromotingpositiveandlastingimprovementsinparent-childinteractionsandinreducingchildren’sbehaviorproblemsathomeforatleasttwo-thirdsofchildren.However,afollow-upevaluationthreeyearslaterindicatedthatapproximatelyone-thirdofthechildrenwerestillhavingconsiderabledifficultiesatschoolandwithpeergroups.Improvementsathomedidnotnecessarilygeneralizetoschoolsettingsortopeerinteractionsforsomechildren.Inparticular,stressfulfamilysituations(e.g.,maritaldistressandpoverty)wererelatedtopooreroutcomes.Asaresultofthesefindings,twonewcomponentsweredeveloped:(1)theADVANCEparentprogramfocusingoncommunication,angermanagementandproblem-solvingskillsand,(2)thechildprogram(DinaDinosaurCurriculum)designedtotrainchildreninsocialskills,problem-solvingstrategiesandemotionallanguage.Evaluationofthesecomponentsindicatedthattheprogramsenhancedeffectsintermsofpeerrelationships,socialproblem-solvingandmaritalcollaboration.However,itwasstillevidentthataportionofthechildrenandtheirfamilieswerehavingdifficultiesmanagingtheschoolexperienceandworkingsuccessfullywithteachers.Inparticular,about40percentofthechildrenwerefoundtobeco-morbidforotherproblemssuchasAttentionDeficitHyperactivityDisorder,aswellaslanguageandlearningdelays.Theseproblemscreatedparticulardifficultiesforthechildrenintheclassroom,withteachersandwithpeers.Moreover,parentsofthesechildrenwerehavingdifficultyknowinghowtosuccessfullycollaboratewithteachersin

Page 170
planningfortheiracademicandsocialneeds.Consequently,forthepastsixyears,ateachertrainingcurriculumhasbeendevelopedandevaluatedforuseinteachingpositiveclassroommanagementskillsandpromotingsocial,emotionalandacademiccompetenciesintheclassroom.Inconjunctionwiththisprogram,theSupportingYouthChild’sEducation(SCHOOL)programforparentswasdevelopedtohelpparentslearnhowtofosteracademiccompetenceathome(e.g.,readingskillsandstudyhabits)andhavesuccessfulconferenceswithteachersatschool.Recentevaluationsoftheseprogramsindicatedsignificanteffectsindecreasingclassroomaggressionandincreasingacademiccompetence.
Thesecurriculumsmaybeusedinschools(e.g.,HeadStart,daycare,andkindergartenthroughgradethree)asearlypreventionprogramsforhigh-riskchildrenandtheirfamiliesandaredesignedtobuildprotectivefactors(e.g.,angermanagement,empathyskills,positivedisciplineandhome-schoolcollaboration)andreduceriskfactors(e.g.,earlysignsofaggressionandpeerrejection)thatresearchhasshowntoberelatedtolaterviolence.Additionally,thesecurriculumsmaybeusedinmentalhealthcentersastreatmentprogramsforchildrendiagnosedwithearly-onsetOppositionalDefiantDisorder(ODD)orConductDisorder(CD)andAttentionDeficitHyperactivityDisorder(ADHD).Thelongrangegoalofthesepreventionprogramsistoenhanceyoungchildren’ssocial,emotional,andacademicdevelopment,aswellaspreventandreduceconductproblemsinordertodecreaseviolence,drugabuse,anddelinquencyinlateryears.
ConductProblemsinYoungChildrenTheincidenceofaggressioninchildrenisescalating—andatyoungerages.Studiesindicatethatanywherefrom7to20percentofpre-schoolandearlyschoolagechildrenmeetthediagnosticcriteriaforOppositionalDefiantDisorder(ODD)andConductDisorder(CD).Theseratesareevenhigherforlow-incomefamilies.ResearchonthetreatmentandpreventionofConductDisordershasbeenidentifiedasoneofthenation’shighestpriorities.Thisagendaisvitallyimportantbecausethewidespreadoccurrenceofdelinquencyandescalatingviolenceinadolescenceresultinahighcosttosociety.“Earlyonset”ODD/CD(intheformofhighratesofoppositionaldefiance,aggressiveandnoncompliantbehaviors)isastabletraitovertimeformanypreschoolchildrenandappearstobethemostimportantbehavioralriskfactorforantisocialbehaviorforboysandgirlsinadolescence.Suchbehaviorhasrepeatedlybeenfoundtopredictthedevelopmentofdrugabuseinadolescence,aswellasotherproblems,includingjuveniledelinquency,depression,violentbehavior,andschooldropout.
Theoriesregardingthecausesofchildconductproblemsincludechildbiologicalanddevelopmentalriskfactors(e.g.,attentiondeficitdisorders,learningdisabilities,andlanguagedelays);familyfactors(e.g.,maritalconflict,depression,
APPENDIX THREE
Descriptions of Recommended Early Intervention Programmes

Page 171
drugabuse,andcriminalbehavior);ineffectiveparenting(e.g.,harshdisciplineandlowparentalinvolvementinschoolactivities);schoolriskfactors(e.g.,teachers’useofpoorclassroommanagementstrategies,classroomlevelofaggression,largeclasssizesandlowteacherinvolvementwithparents);andpeerandcommunityriskfactors(e.g.,povertyandgangs).
SinceConductDisorderbecomesincreasinglyresistanttochangeovertime,interventionthatbeginsintheearlyschoolyearsisclearlyastrategicwaytopreventorreduceaggressivebehaviorproblemsbeforethey“ripple”toresultinwell-establishednegativereputations,academicfailure,andescalatingviolenceinadolescence.Recentprojectionssuggestthatapproximately70percentofthechildrenwhoneedservicesforconductproblems—inparticular,youngchildren—donotreceivethem.Andveryfewofthosewhodoreceiveinterventioneverreceiveaninterventionwhichhasbeen“empiricallyvalidated.”
HighlightsoftheIncredibleYearsParent,TeacherandChildTrainingSeries
■ Comprehensive(includesintegratedtrainingforparents,teachersandchildren)
■ Proactive,collaborativeapproachbuiltonthe“strengthmodel”■ Flexibleindeliveryusingsequencedmodules(26topicsintotal)■ Culturallysensitive(availableinSpanish,Britishdialect,andNorwegian,as
wellasmulti-ethnicvideotapeactorsandpuppets)■ Appropriateforpreventionprogramsforhigh-riskchildren,aswellasfor
treatmentofchildrenwithconductproblems■ Userfriendly—usesacombinationofbooks,videotapes,extensivefacilitator
manuals,andhomeandschoolactivities■ Developmentallyappropriateforyoungchildren—includespuppets,gamesand
activities■ Providesextensiveprogramsupportfortrainingfacilitators,schoolpersonnel,
andorganizations,includinggroupfacilitatortraining■ Providescertificationforfacilitatorstoassurequalityimplementation■ Evidence-basedandreplicatedbyindependentresearchers
TheoreticalRationale/ConceptualFrameworkThetheoreticalrationaleforthethreecurriculumsforparents,teachers,andchildrenisdescribedbelow.
TheoreticalRationale/ConceptualFrameworkfortheIncredibleYearsParentTrainingSeriesParentinginteractionsareclearlythemostwellresearchedandmostimportantproximalcauseofthedevelopmentofconductproblemsinyoungchildren.

Page 172
Parentingpracticesassociatedwiththedevelopmentofconductproblemsincludepermissive,inconsistent,irritable,andharshdisciplineandlowmonitoring.DishionandLoeber(1985)andothershavefoundthatparentalmonitoringanddisciplinearelowforadolescentsubstanceabusers;moreover,theseparentalconstructsatagetenpredictedlaterantisocialbehavioranddrugabuse.ThemostinfluentialdevelopmentalmodelfordescribingthefamilydynamicsthatunderlieearlyantisocialbehaviorisPatterson’ssociallearningtheoryregardingthe“coerciveprocess”(Pattersonetal.,1992),apatternwherebychildrenlearntoescapeoravoidparentalcriticismbyescalatingtheirnegativebehaviors.This,inturn,leadstoincreasinglyaversiveparentinteractionsandescalatingdysregulationonthepartofthechild.Thesenegativeparentresponsesdirectlymodelandreinforcethechild’sdeviantbehaviors.
Inadditiontosociallearningtheory,attachmenttheory(Bowlby,1980)andnewmethodsofmeasuringattachmentbeyondthetoddlerhoodperiodhaveemphasizedtheimportanceoftheaffectivenatureoftheparent-childrelationship.Considerableevidenceindicatesthatawarm,positivebondbetweenparentandchildleadstomorepositivecommunicationandpositiveparentingstrategiesandamoresociallycompetentchild,whereashighlevelsofparentalnegativeaffectandhostilityisdisruptivetochildren’sabilitytoregulatetheiremotionalresponsesandmanageconflictappropriately.Forexample,researchhasshownthattherelationshipbetweenharshdisciplineandexternalizingproblemsoccursonlyamongchildreninhomesinwhichawarmchild-parentrelationshipislacking(Deater-Deckard,Dodge,Bates,&Pettit,1996).Likewise,inarecentreviewofresearchonriskandresilience,DollandLyon(1998)concludethatawarmrelationshipwithatleastonecaregiverisastrongprotectivefactoragainstthenegativeinfluencesoffamilydysfunction.Thisfindingissupportedbyresultsofalargenationalstudyofadolescentdevelopmentthatshowedthatyouthwhoreportpositiverelationshipsandbondingwiththeirfamiliesandschoolsengageinlessriskyandfewerantisocialbehaviors(Resnicketal.,1997).
Otherfamilyfactors,suchasdepression,maritalconflict,andhighnegativelifestress,havebeenshowntodisruptparentingskillsandcontributetoparentalhighnegativeaffect,inconsistentparenting,lowmonitoring,emotionalunavailabilityandinsecureattachmentstatus.Familyandparentingriskfactorresearchsuggeststheneedtotrainparentsineffectivechildmanagementskillsandassistthemincopingwithotherfamilystressors.
TheoreticalRationale/ConceptualFrameworkfortheIncredibleYearsTeacherTrainingSeriesOncechildrenwithbehaviorproblemsenterschool,negativeacademicandsocialexperiencesmakekeycontributionstothefurtherdevelopmentofconduct
APPENDIX THREE
Descriptions of Recommended Early Intervention Programmes

Page 173
problems.Aggressive,disruptivechildrenquicklybecomesociallyexcluded,leadingtofeweropportunitiestointeractsociallyandlearnappropriatefriendshipskills.Overtime,peersbecomemistrustfulandrespondtoaggressivechildreninwaysthatincreasethelikelihoodofreactiveaggression.Evidencesuggeststhatpeerrejectioneventuallyleadstothesechildren’sassociationwithdeviantpeers.Oncechildrenhaveformeddeviantpeergroups,theriskfordrugabuseandantisocialbehaviorisevenhigher.
Furthermore,Rutterandcolleagues(1976)findthatteacherbehaviorsandschoolcharacteristicssuchaslowemphasisofteachersonacademicwork,lowratesofpraise,littleemphasisonindividualresponsibility,andhighstudent-teacherratioarerelatedtoclassroomaggressivebehaviors,delinquency,andpooracademicperformance.High-riskchildrenareoftenclusteredinclassroomswithahighdensityofotherhigh-riskstudents,thuspresentingtheteacherwithadditionalmanagementchallenges.Rejectingandnon-supportiveresponsesfromteachersfurtherexacerbatetheproblemsofaggressivechildren.Suchchildrenoftendeveloppoorrelationshipswithteachersandreceivelesssupport,nurturing,andinstructionandmorecriticismintheclassroom.Someevidencesuggeststhatteachersretaliateinamannersimilartoparentsandpeers.WalkerandBuckley(Walker,1995;Walker&Buckley,1973)reportthatantisocialchildrenarelesslikelytoreceiveencouragementfromteachersforappropriatebehaviorandmorelikelytobepunishedfornegativebehaviorthanwell-behavedchildren.Aggressivechildrenarealsofrequentlyexpelledfromclassrooms.Inourownclinicstudieswithconductproblemchildrenagedthreetosevenyears,over50percenthadbeenaskedtoleavethreeormoreschoolsbysecondgrade.Thelackofteachersupportandexclusionfromtheclassroomexacerbatesnotonlythesechildren’ssocialproblems,butalsotheiracademicdifficulties,andalsocontributestothelikelihoodofschooldropout.Finally,recentresearchhasshownthatpoorlymanagedclassroomshavehigherlevelsofclassroomaggressionandrejectionthat,inturn,influencethecontinuingescalationofindividualchildbehaviorproblems.Aspiralingpatternofchildnegativebehaviorandteacherreactivitycanultimatelyleadtoparentdemoralization,withdrawalandalackofconnectionandconsistencybetweenthesocializationactivitiesoftheschoolandhome.Whilemostteacherswanttobeactivepartnersinfacilitatingthebondingprocesswithparents,manylacktheconfidence,skills,ortrainingtoworkcollaborativelywithfamilies.Teachereducationprogramsalsodevotescantattentiontobuildingrelationshipsandpartnershipswithparentsorimplementingsocialandemotionalliteracycurriculums.
Thisliteraturesuggeststhatapreventivemodelneedstopromotehealthybondsor“supportivenetworks”betweenteachersandparentsandchildrenandteachers.Strongfamily-schoolnetworksbenefitchildrenduetoparents’

Page 174
increasedexpectations,interestin,andsupportfortheirchild’ssocialandacademicperformance,andcreateaconsistentsocializationprocessacrosshomeandschoolsettings.Thenegativecycledescribedabovecanbepreventedwhenteachersdevelopnurturingrelationshipswithstudents,establishclearclassroomrulesaboutbullying,preventsocialisolationbypeers,andofferacurriculumwhichincludestrainingstudentsinemotionalliteracy,socialskills,andconflictmanagement.Considerableresearchhasdemonstratedthateffectiveclassroommanagementcanreducedisruptivebehaviorandenhancesocialandacademicachievement.Well-trainedteacherscanhelpaggressive,disruptive,anduncooperativechildrendeveloptheappropriatesocialbehaviorthatisaprerequisitefortheirsuccessinschool.Teacherbehaviorsassociatedwithimprovedclassroombehaviorincludethefollowing:highlevelsofpraiseandsocialreinforcement;proactivestrategiessuchaspreparingchildrenfortransitionsandsettingclear,predictableclassroomrules;effectiveuseofshort,clearcommands,warnings,reminders,anddistractions;tangiblereinforcementsystemsforappropriatesocialbehavior;team-basedrewards;mildbutconsistentresponsecostsforaggressiveordisruptivebehaviorincludingTimeOutandlossofprivileges;anddirectinstructioninappropriatesocialandclassroombehavior,problem-solvingandself-managementskills.
TheoreticalRationale/ConceptualFrameworkfortheIncredibleYearsChildTrainingSeriesMoffit(Moffitt,1993;Moffitt&Lynam,1994)andothershavearguedthatsomeabnormalaspectofthechild’sinternalorganizationatthephysiological,neurological,and/orneuropsychologicallevel(whichmaybegeneticallytransmitted)islinkedtothedevelopmentofConductDisorders,particularlyfor“lifecoursepersisters”(i.e.,thosewithachronichistoryofearlybehavioralproblems).
Childrenwithconductproblemshavebeenreportedtohavecertaintemperamentalcharacteristicssuchasinattentiveness,impulsivity,andHyperactivityAttentionDeficitDisorder.Researchersconcernedwiththebiologicalaspectsofthedevelopmentofconductproblemshaveinvestigatedvariablessuchasneurotransmitters,autonomicarousalsystem,skinconductanceandhormonalinfluences,andsomefindingssuggestthatsuchchildrenmayhavelowautonomicreactivity(i.e.,lowphysiologicalresponsetostimuli).OtherchildfactorshavealsobeenimplicatedinchildConductDisorder.Forexample,deficitsinsocial-cognitiveskillscontributetopooremotionalregulationandaggressivepeerinteractions.ResearchhasshownthatchildrenwithODD/CDmaydefineproblemsinhostileways,searchforfewercueswhendetermininganother’sintentionsandfocusmoreonaggressivecues.ChildrenwithODD/CDmayalsodistortsocialcuesduringpeerinteractions,generatefeweralternativesolutionstosocialproblems,and
APPENDIX THREE
Descriptions of Recommended Early Intervention Programmes

Page 175
anticipatefewerconsequencesforaggression.Thechild’sperceptionofhostileintentinothersmayencouragethechildtoreactaggressively.Researchrevealsthataggressivebehaviorinchildreniscorrelatedwithlowempathyacrossawideagerangewhichmaycontributetoalackofsocialcompetencyandantisocialbehavior.Additionally,studiesindicatethatchildrenwithconductproblemshavesignificantdelaysintheirpeerplayskills;inparticular,difficultywithreciprocalplay,cooperativeskills,turntaking,waiting,andgivingsuggestions.
Finally,reading,learningandlanguagedelaysarealsoimplicatedinchildrenwithconductproblems,particularlyfor“earlylifecoursepersisters”(Moffitt&Lynam,1994).Forthesechildren,lowacademicachievementoftenmanifestsitselfduringtheelementarygradesandcontinuesthroughhighschool.Pooracademicachievementalsopredictsadolescentdrugabuseinbothcross-sectional(Jessor,1987;Newcomer,Maddahian,&Bentler,1986)andlongitudinalsamples(Smith&Fogg,1978).TherelationshipbetweenacademicperformanceandCDisbi-directional.Academicdifficultiesmaycausedisengagement,increasedfrustration,andlowerself-esteem,whichcontributetothechild’sbehaviorproblems.Atthesametime,noncompliance,aggression,elevatedactivitylevels,andpoorattentionlimitachild’sabilitytobeengagedinlearningandachieveacademically.Thus,acycleiscreatedinwhichoneproblemexacerbatestheother.ThiscombinationofacademicdelaysandconductproblemsappearstocontributetothedevelopmentofmoresevereCDandschoolfailure.
Thedataconcerningthepossiblebiological,socio-cognitiveandacademicordevelopmentaldeficitsinchildrenwithconductproblemssuggesttheneedforparentandteachertrainingprogramswhichhelpthemunderstandchildren’sbiologicaldeficits(theirunresponsivenesstoaversivestimuliandheightenedinterestinnovelty)andsupporttheiruseofeffectiveparentingandteachingapproachessothattheycancontinuetobepositiveandprovideconsistentresponses.Thedataregardingautonomicunderarousaltheorysuggeststhatthesechildrenmayrequireoverteaching(i.e.,repeatedlearningtrials)inordertolearntoinhibitundesirablebehaviorsandmanageemotion.Parentsandteacherswillneedtouseconsistent,clear,specificlimit-settingthatutilizessimplelanguageandconcretecuesandreminders.Additionally,thisinformationsuggeststheneedtodirectlyintervenewithchildrenandfocusonsociallearningneedssuchasproblem-solving,perspectivetaking,andplayskillsaswellasliteracyandspecialacademicneeds.
BriefDescriptionofInterventionTheIncredibleYearsSeriesisacomprehensiveprogramforparents,teachers,andchildrenwiththegoalofpreventing,reducing,andtreatingbehavioralandemotionalproblemsinchildrenagestwotoeight.Thecoreoftheprogram

Page 176
istheBASICparenttrainingcomponentwhichemphasizesparentingskillssuchasplayingwithchildren;helpingchildrenlearn;usingeffectivepraise,incentives,andlimit-setting;andhandlingmisbehavior.AdditionalparenttrainingcomponentsincludeanADVANCEserieswhichemphasizesparentinterpersonalskillssuchaseffectivecommunication,angermanagement,problem-solvingbetweenadults,andwaystogiveandgetsupport,andaSCHOOLserieswhichfocusesonparentingapproachesdesignedtopromotechildren’sacademicskills.
Tofacilitategeneralizationfromhometotheschoolenvironment,atrainingseriesforteachersprovidingeffectiveclassroommanagementskillswasaddedtotheIncredibleYearsSeries.Thelastadditionwasthetrainingseriesforchildren(DinaDinosaurCurriculum),a“pullout”treatmentprogramforsmallgroupsofchildrenexhibitingconductproblems.Thiscurriculumemphasizesemotionalliteracy,empathyandperspectivetaking,friendshipdevelopment,angermanagement,interpersonalproblem-solving,followingschoolrules,andschoolsuccess.
TheBASICcomponent,whichisthecoreprogram,MUSTbeimplemented,andothercomponentsmaybeaddedaccordingtotheparticularfamilyandchildriskfactors.Abriefdescriptionoftheparent,teacher,andchildprogramsisprovidedbelow.
ParentTrainingProgramsBASIC.TheBASICparenttrainingprogramisguidedbythecognitivesociallearningandattachmentrelationshiptheoriesdescribedabove.Itisa12to14weekprogramforparentsinvolvingfacilitator-ledgroupdiscussionsof250videovignettes.Theprogramteachesparentschild-directedinteractiveplay,empathy,andreinforcementskills,whichhelpparentsachievearealistic,develop-mentallyappropriateunderstandingoftheirchildrenandtheirtemperamentsinordertofosterattachmentandnurturingrelationships.Thelatterhalfoftheprogramfocusesonnonviolentdisciplinetechniques,including“TimeOut”and“Ignore,”logicalandnaturalconsequences,andproblem-solvingstrategies.Finally,theprogramteachesparentsappropriatemonitoringstrategiesandhowtorespondtochildreninclear,predictableways.Theschool-ageversionoftheBASICparenttrainingseries(developedwithamoreculturallydiversepopulation)isdesignedforusewithparentsofchildrenuptoageeight(gradethree).
SCHOOL.TheSupportingYourChild’sEducation(SCHOOL)programwasdesignedtoteachparentstostrengthentheirchild’sreadingandacademicreadinessandpromotestrongconnectionsbetweenhomeandschoolbydevelopingpartnershipswithteachers.
APPENDIX THREE
Descriptions of Recommended Early Intervention Programmes

Page 177
ADVANCE.TheADVANCEparenttrainingprogramisalsoguidedbycognitivesociallearningtheoryandutilizeseffectiveaspectsofmaritalanddepressiontherapy(Jacobson,Schmaling,&Holtzworth-Monroe,1987).Thisprogramisa10to12weeksupplementtotheBASICprogramandaddressesotherfamilyriskfactorssuchasdepression,maritaldiscord,poorcopingskills,andlackofsupport.Theprogramcontentincludesteachingcognitiveself-controlstrategies,problem-solving,communicationskillsandwaystogiveandgetsupport.Figure1.ParentingPyramid
Allofthetrainingprogramsutilizeacollaborativetrainingprocessofgroupdiscussionguidedbytrainedfacilitators,andprogrammaterialsincludevideotapes,detailedmanualsforfacilitators,parentbooksandaudiotapes,andhomeactivitiesandrefrigeratornotes.
Problem Solving
CooperationSelf Esteem
Attachment
Social Skills
Thinking Skills
Motivation
Responsibility
PrediciabilityObedience
Ann
oyin
gB
ehav
iour
sA
ggre
ssio
n
BENEFITS FOR CHILDPARENT SKILLS & STRATEGIES
Praise
EncouragementRewards
Celebrations
Clear Limits
Household Rules
Consistent Follow-Through
Ignore
Distract
Redirect
Con
sequen
ces
Talking
Listen
ing
Problem
Solvin
g
Play
Atten
tion
and
Involvem
ent
Em
path
y

Page 178
TeacherTrainingProgramTheteachertrainingprogramincludesasix-day(or42-hour)workshopforteachers,schoolcounselors,andpsychologiststhatinvolvesgroup-basedtrainingtotargeteffectiveclassroommanagementstrategiesfordealingwithmisbehavior;promotingpositiverelationshipswithdifficultstudents;strengtheningsocialskillsintheclassroom,playground,bus,andlunchroom;andteachers’collaborativeprocessandpositivecommunicationwithparents(e.g.,theimportanceofpositivehomephonecalls,regularmeetingswithparents,homevisits,andsuccessfulparentconferences).Forindicatedchildren(i.e.,childrenwithConductDisorder),teachers,parents,andgroupfacilitatorswilljointlydevelop“transitionplans”thatdetailclassroomstrategiesthataresuccessfulwitheachindividualchild;goalsachievedandremaining;characteristics,interests,andmotivatorsforthechild;andpreferredmethodsofcontactingparents.Thisinformationispassedontothefollowingyear’steachers.Figure2.PyramidforBuildingRelationships
Respect
Enjoyment
LoveAcceptanceEmpathy
Coo
pera
tion
& P
artn
ersh
ip
BENEFIT FOR OTHER PERSONSELF
Involvement
& Time
with Another
Playing &
Having Fun
Listening
Taking Other’s
Prespective
Family
Meetings
Understanding
Generating
solutions
Evaluating
consequences
New solutions
Gettin
g
Support
Self
Care
Postive
Self-T
alk
Person
alS
elf-C
ontrol
Speaking Up
Politeness
APPENDIX THREE
Descriptions of Recommended Early Intervention Programmes

Page 179
Additionally,teacherslearnhowtopreventpeerrejectionbyteachingtheaggressivechildappropriateproblem-solvingstrategiesandhelpinghis/herpeersrespondappropriatelytoaggression.Teachersareencouragedtobesensitivetoindividualdevelopmentaldifferences(i.e.,variationinattentionspanandactivitylevel)andbiologicaldeficitsinchildren(e.g.,unresponsivenesstoaversivestimuli,heightenedinterestinnovelty),aswellashowtorespondtothesedifferencesinpositive,acceptingandconsistentways.Physicalaggressioninunstructuredsettings(e.g.,playground)istargetedforclosemonitoring,instructionandincentiveprograms.Figure3.TeachingPyramid
ChildTrainingProgram(DinosaurCurriculum)DinaDinosaur’sSocialSkillsandProblem-SolvingCurriculumwasguidedbychildriskfactorresearchandaimstoenhancechildren’sappropriateclassroombehaviors(e.g.,quiethandupandlisteningtoteacher),promotesocialskillsand
Problem Solving
CooperationSelf Esteem
Social Skills
Thinking Skills
Motivation
Responsibility
PrediciabilityObedience
Dis
rupt
ive
Beh
avio
urs
BENEFITS FOR CHILDTEACHER SKILLS & STRATEGIES
Praise
Encouragement
Incentives
Celebrations
Clear Limits
Classroom Structures
Non Verbal Cues
Positive Verbal Redirect
Distractions
Re-engagement Strategies
Con
sequen
ces
Talking
Listen
ing
Problem
Solvin
g
Play
Atten
tion
and
Involvem
ent
Em
path
y
Non-DisruptiveBehaviours
Reminder of
Expected Behaviour
Warning of
Consequence

Page 180
positivepeerinteractions(e.g.,waiting,takingturns,askingtoenteragroupandcomplimenting,etc.),helpchildrendevelopappropriateconflictmanagementstrategies,andreduceconductproblems.Inaddition,theprogramteacheschildrenwaystointegrateintotheclassroomanddeveloppositivefriendships.Thecurriculumisusedasa“pullout”programfortreatingsmallgroupsoffivetosixchildrenwithconductproblems.Thesesmallgroupsessionscanbeofferedtwiceaweekforanhouroronceaweekfortwohours(see“FutureDirections”forhowprogramisusedasaclassroom-basedcurriculum).Finally,thechildprogramisorganizedtodovetailtheparentandteachertrainingprograms.
SummaryEachofthethreetypesoftrainingprogramsdescribedabovetargetsdifferentantecedentsofConductDisorderinthehome,classroom,andschoolsetting,aswellasintheindividualchildandhis/herpeergroup.Eachofthethreesetsofcurriculumshasbeendesignedtobepractical,“userfriendly,”andimplementedbytrainedfacilitatorsincludingschoolpersonnel.Initially,thesefacilitatorswillreceiveextensive,group-basedtrainingtoconducttheclassroomandparentinterventions.Additionally,self-administeredmanualshavebeendevelopedfortheteacherandparenttrainingprogramssothatparticipantscanmake-upmissedsessionsinacost-effectivemanner.
Eachofthethreeinterventionsincludesa500pagemanualoutliningcontent;groupfacilitatorscripts(includingquestionsforgroupdiscussions);homeworkorclassroomactivities;refrigeratorandblackboardnotesoutliningkeypoints;videos;andbooksforchildren,parents,andteachers.
Trainedgroupfacilitatorsusethevideotapedvignettestofacilitatediscussion,problem-solving,andsharingofideasamongteachers.Groupfacilitatorshelpparticipantsdiscussimportantprinciplesandpracticenewskillsthroughrole-playingandclassroomassignments.
EvidenceofProgramEffectiveness
IncredibleYearsParentTrainingStudieswithChildrenDiagnosedwithOppositionalDefiantDisorderand/orConductDisorderOverthepast20years,theBASICprogramhasbeenevaluatedextensivelyasatreatmentprograminaseriesofsixrandomizedstudieswithmorethan800childrenreferredtotheprogramforconductproblems.ThesestudieshaveshownthattheBASICprogramresultsinsignificantlyimprovedparentalattitudesandparent-childinteraction,areductioninparents’useofviolentformsofdiscipline,andreducedchildconductproblems.Effectshavebeensustaineduptothreeyearsafterintervention(Webster-Stratton,1990b).
APPENDIX THREE
Descriptions of Recommended Early Intervention Programmes

Page 181
TheADVANCEprogramhasbeenshowninarandomizedstudytobeahighlyeffectivetreatmentforpromotingparents’useofeffectiveproblem-solvingandcommunicationskills,reducingmaternaldepression,andincreasingchildren’ssocialandproblem-solvingskills.TheseeffectswereobtainedoverandabovethesignificantchangesobtainedintheBASICprogram(Webster-Stratton,1994).LaterstudiescombiningBASICandADVANCEreplicatedthesefindingsandhaveshowneffectslastinguptoone4year(Webster-Stratton&Hammond,1997).Usershavebeenhighlysatisfiedwithbothprograms,andthedrop-outrateshavebeenlowregardlessofsocioeconomicstatus.
IncredibleYearsParentTrainingStudieswithHigh-riskFamiliesTheBASICprogramwasalsoevaluatedasaselectivepreventionprogramintworandomizedtrialswithover500HeadStartfamiliesrepresentingamulti-ethnic(50percentminority)populationlivinginpovertysituations.Inthefirststudy,resultsindicatedthattheparentingskillsofHeadStartparentswhoreceivedtrainingandthesocialcompetenceoftheirchildrensignificantlyimprovedcomparedwiththecontrolgroupfamilies.Thisdatasupportedthehypothesisthatstrengtheningparentingcompetenceandincreasingtheparentalinvolvementofhigh-riskwelfaremothersinchildren’sschool-relatedactivitieshelpstopreventchildren’sconductproblemsandpromotesocialcompetence(Webster-Stratton,1998b;Webster-Stratton&Reid,1999a).Mostoftheseimprovementsweremaintainedoneyearlater.ThesecondstudyreplicatedthefindingsofthefirststudywithHeadStartparentsandalsoevaluatedaddingasecondyearboosterparentinterventionutilizingabbreviatedcomponentsoftheADVANCEandSCHOOLprograms(Webster-Stratton,Reid&Hammond,inpress).Two-yearfollow-upresultsofthisstudyarecurrentlybeingconducted.
Thesefindingshavebeenindependentlyreplicatedinthreeotherstudieswithfamiliesofchildrenwithconductproblems(Scott,1999;Taylor,Schmidt,Pepler,&Hodgins,1998;Miller,Kamboukos,Klein,&Coard,1999)andinthreepreventiontrialsinlowincomechildcarecenterswithprimarilyAfricanAmericanfamiliesinChicago(Gross,Fogg,&Tucker,1995;Gross,Fogg,Webster-Stratton,&Grady,1999),withSpanish-speakingHeadStartfamiliesinNewYork(Miller&Rojas-Flores,1999),andwithamulti-ethnicgroupofHeadStartparentsinMassachusetts(Arnoldetal.,inprogress).
IncredibleYearsTeacherTrainingStudiesTheteachertrainingprogramwasfirstevaluatedinarandomizedtrialwith133childrendiagnosedwithconductproblems,andanalysescomparedchildtrainingandparenttrainingwithandwithoutteachertraining.Post-treatmentclassroomobservationsofteacherbehaviorconsistentlyfavoredconditionsinwhichteachersreceivedtraining.Trainedteacherswerelesscriticalandlessharshthancontrol

Page 182
teachers.Trainedteachersusedmorepraiseandweremorenurturing,lessinconsistent,andreportedmoreconfidenceinteachingthancontrolteachers.Resultsalsoindicatedthatinclassroomswhereteachersweretrained,childrenwereobservedtobesignificantlylessaggressivewithpeersandweremorecooperativewithteachersthanchildreninuntrainedteacherclassrooms.Trainedteachersalsoreportedthatchildrenhadincreasedacademiccompetencecomparedtochildrenincontrolclassrooms(Webster-Stratton&Reid,1999).Nearlyidenticalfindingsemergedinarandomizedtrialwith272HeadStartchildrenwhereinteachersandparentsreceivedthetrainingprogramsandwerecomparedwiththosereceivingregularHeadStartservices.Additionally,inclassroomswhereteachersreceivedtraining,childrenwereobservedtohavehigherschoolreadinessscores(engagementandon-taskbehavior)andincreasedpro-socialbehaviors,aswellassignificantlyreducedpeeraggression.Teachers’reportsofparentbondingandinvolvementinschool,aswellaschildren’ssocialcompetence,werealsosignificantlyhigherfortrainedteachersthanforuntrainedteachers.
ThesefindingshavebeenindependentlyreplicatedbyArnold(inprogress)inarandomizedstudyinvolvingeightdaycarecenters(12interventionand8controlclassrooms).Resultsindicatedthatteachersintheinterventionclassroomsreportedusingmoreeffectiveteachingstrategiesandlesslaxdisciplinethanteachersincontrolclassrooms.Moreover,interventionteachersreportedfeweraggressivebehaviorsthandidteachersincontrolclassrooms.
IncredibleYearsChildTrainingStudies—DinaDinosaurCurriculumTheDinaDinosaurCurriculumforchildrenwasevaluatedintworandomizedtrialswithconduct-disorderedchildrenagesfourtoeight.Thefirstofthesestudiesshowedthatthe20to22weekchildtrainingprogramresultedinsignificantimprovementsinobservationsofpeerinteractions.ChildrenwhohadreceivedtheDinosaurCurriculumweresignificantlymorepositiveintheirsocialskillsandconflictmanagementstrategiesthanchildrenwhoseparentsreceivedparenttrainingonlyorservedasuntreatedcontrols.Resultsshowedthatthecombinedparentandchildtrainingwasmoreeffectivethanparenttrainingaloneandthatbothweresuperiortothecontrolgroup.Oneyearlater,thecombinedparentandchildinterventionshowedthemostsustainedeffects.
Inthesecondstudy,theeffectsofthe20to22weekchildtrainingprogramwerereplicatedintermsofimprovedpeerconflictmanagementskillsincomparisontochildrenwhoonlyreceivedparenttraining(Webster-Stratton&Reid,1999).Whenchildtrainingwascombinedwithteachertraining,therewereimprovedreductionsinaggressivebehaviorintheclassroom.
APPENDIX THREE
Descriptions of Recommended Early Intervention Programmes

Page 183
SummaryofResultsTheIncredibleYearstrainingprogramshavebeenshowntoaffectthefollowingriskandprotectivefactors:
Parents■ Increasedpositiveandnurturingparentingstyle■ Decreasedharsh,inconsistentandunnecessarydiscipline■ Increasedpraiseandeffectivediscipline■ Decreasedparentalstressanddepression■ Increasedpositiveparentcommandsandproblem-solving■ Increasedparentbondingandinvolvementwithteachers
Teachers■ Increasedproactiveandpositiveclassroommanagementskills■ Decreasedharshandcriticalclassroommanagementstyle■ Increasedpositiveclassroomatmosphere■ Increasedbondingwithparents
Child■ Increasedpositiveconflictmanagementskillsandsocialskillswithpeers■ Decreasednegativebehaviorsandnoncompliancewithparentsathome■ Increasedsocialcompetenceatschool■ Decreasedpeeraggressionanddisruptivebehaviorsintheclassroom■ Increasedacademicengagement,schoolreadinessandcooperationwith
teachers
Thesefindingshavebeenreflectedinteacherandparentratings,childtestingandinterviewing,independentobservationsinthehomeandatschool,andlaboratoryobservationsofpeerinteractionsandinteractionswithparents.
Thisinformationwasexcerptedfrom:
Webster-Stratton,C.,Mihalic,S.,Fagan,A.,Arnold,D.,Taylor,T.,&Tingley,C.(2001).BlueprintsforViolencePrevention,BookEleven:TheIncredibleYears:Parent,TeacherAndChildTrainingSeries.Boulder,CO:CenterfortheStudyandPreventionofViolence.

Page 184
TRIPLEP-POSITIVEPARENTINGPROGRAM
ProgramOverviewTheTripleP(PositiveParentingProgram)isacomprehensive,community-widesystemofparentingandfamilysupport.Thefiveinterventionlevelsweredesignedtoenhanceparentalcompetenceandpreventoralterdysfunctionalparentingpractices,therebyreducinganimportantsetoffamilyriskfactorsbothforchildmaltreatmentandforchildren’sbehavioralandemotionalproblems.Atthepopulationlevel,theexistingworkforcecrossingseveraldisciplinesandsettings(suchasfamilyandsocialsupportservices,preschoolandchildcaresettings,elementaryschoolsandothercommunityentitieswithdirectcontactwithfamilies)istrainedtodelivertheTriplePsystemofinterventions.Thisworkforceisthenresponsiblefordeliveringtheprogramtoparents.
ProgramTargetsThecommunity-wideversionofTriplePtargetsparentswithchildrenyoungerthaneightyearsofage,andtheinterventionisdeliveredcommunity-widethroughmultipleproviders.
ProgramContentThemultilevelsystemincludesfiveinterventionlevelsofincreasingintensityandnarrowingpopulationreach:
Universal Triple P (Level 1)usesmediaandinformationalstrategiesthat:■ destigmatizeparentingandfamilysupport■ makeeffectiveparentingstrategiesavailabletoallparents■ facilitatehelpseekingandself-regulation
Selected Triple P (Level 2)normalizesparentinginterventionsthrough:■ briefandflexibleconsultationwithindividualparents■ parentingseminarswithlargegroupsofparents
Primary Care Triple P (Level 3)managesdiscretechildbehaviorproblemsthrough:■ fourbriefconsultationsthatincorporateactiveskillstraining■ selectiveuseofparentingtipsheetsoncommonproblemsofyoungchildren■ generalizationenhancementstrategiestoapplyskillstootherareas
Standard and Group Triple P (Level 4) benefitsindicatedpopulationsofchildrenwithdetectableproblemsby:■ teachingparentsavarietyofchildmanagementskills■ combiningprovisionofinformationwithactiveskillstrainingandsupport
APPENDIX THREE
Descriptions of Recommended Early Intervention Programmes

Page 185
■ teachingparentstoapplyskillstoabroadrangeoftargetbehaviorsinnumeroussettings
Enhanced Triple P (Level 5)isdirectedatfamilieswithadditionalriskfactorsandincludes:■ optionalmodulesonpartnercommunication,moodmanagementandparent
copingskills■ additionalpracticesessionsaddressingparent-childissues
ProgramOutcomesComparedtocontrolcounties,positiveeffectsintheTriplePSystemcountieswereseenforratesof:■ substantiatedchildmaltreatment■ childout-of-homeplacements■ hospitalizationsoremergency-roomvisitsforchildmaltreatmentinjuries
NoteOnlyTripleP,whenimplementedasatotalsysteminacommunity,isbeingcertifiedbyBlueprints.EvaluationsofindividuallevelsofTriplePimplementedalone,suchastheLevel4Standard,Group,orSelf-Directedformats,havenotmetBlueprintscriteria.
ReferencesPrinz,R.J.,Sanders,M.R.,Shapiro,C.J.,Whitaker,D.J.,andLutzker,J.R.(2009).Population-BasedPreventionofChildMaltreatment:TheU.S.TriplePSystemPopulationTrial.PreventionScience,10,1-12.

Page 186
Parent-ChildHome
TheProgramModelTheimportanceofParent-ChildinteractionAllchildren’sfirstyearsshouldbefilledwithverbalstimulationtobuildlanguageandliteracyskills.Eachdayshouldbefullofdiscoveryandofferopportunitiestogainnewskillsandlearnnewconcepts.Fosteringverbalinteractionbetweenparentsandtheiryoungchildrenisacriticalcomponentofhealthyandsuccessfuldevelopment(Bruner,1964and1966;Vygotsky1962).Theimportanceofthisinteractionhasbeenfurthervalidatedbythebrainandlanguagedevelopmentresearch(Hart&Risley).FormativeresearchonTheParent-ChildHomeProgram’s1965pilotproject(thenTheMother-ChildHomeProgram)affirmedthatthiscriticalparent-childinteractioncouldbestrengthenedbymodelingreading,play,andconversationforparentsandchildrenintheirownhomes(LevensteinandSunley1968).
Schoolreadiness:BridgingthepreparationgapAcrossthecountry,millionsofchildrenbeginkindergartenunprepared.Theyare“leftbehind”asearlyasthefirstdayofschool.Thesechildrenhavenotadequatelyexperiencedqualityverbalinteractionorbooks.Theyhavenotbeenexposedtoplayandinteractiveexperiencesthatencourageproblem-solvingandappropriatesocial-emotionaldevelopment.Theydonothavethelanguageskillstheyneedtosuccessfullyinteractwiththeirteachersandtheirclassmates.Theymaynotbeabletocontroltheirbehaviorsoremotionsaswellasotherstudents.Theymayhaveheardmorediscouragementsthanencouragements.Withouttheskillstheyneedtosuccessfullyadjusttotheclassroom,theybegintheiracademiccareersbehindtheirpeers.Manyofthesechildrenwillnevercatchup.
TheParent-ChildHomeProgrambridgesthis“preparationgap”byhelpingfamilieschallengedbypoverty,limitededucation,languageandliteracybarriers,andotherobstaclestoschoolsuccesspreparetheirchildrentoenterschoolreadytobeintheclassroom.
Theapproach:Modelingvs.teachingTheParent-ChildHomeProgramutilizesanon-directive,non-didacticapproach,modelingbehaviorsforparentsthatenhancechildren’sdevelopmentratherthanteachingbehaviors.HomeVisitorshelpparentsrealizetheirroleastheirchildren’sfirstandmostimportantteacher,generatingenthusiasmforlearningandverbalinteractionthroughtheuseofengagingbooksandstimulatingtoys.Parentsarenevergivenhomeworkorassignmentstocompletebutareencouragedtocontinuequalityplayandreadingbetweenvisitswiththebooksandtoystheyreceive
APPENDIX THREE
Descriptions of Recommended Early Intervention Programmes

Page 187
eachweek.The“lighttouch”employedbyParent-ChildHomeProgramHomeVisitorsisnon-intimidatingandempowersparents,allowingthemtopreparetheirchildrenforschoolsuccess,andtakeprideintheircommitmentto,andimpacton,theirchild’seducation.EveryParent-ChildHomeProgramlocalsiteadherestoacarefullydevelopedandwell-testedmodeltoensurehighqualityservicesandconsistentresults:
Site Structure: ■ EachsiteisrunbyaSiteCoordinatorhiredbythelocalpartneragencyand
trainedbyTheParent-ChildHomeProgram’sNationalCenter.■ TheSiteCoordinatorsarethenpreparedtorecruitandtraintheirlocalHome
Visitors.■ Traininginmulticulturalawarenessandtheethicsofhomevisitingare
importantcomponentsoftheParent-ChildHomeProgram’strainingcurriculumforSiteCoordinatorsandHomeVisitors.Respectandunderstandingarecriticalforsuccessfulhomevisitingrelationships.
■ Familiesparticipateinthetwo-yearprogramwhentheirchildrenaretwo-andthree-years-old,completingtheProgramastheyturnfourandtransitionintopre-kindergartenorHeadStart.Achildcan,however,entertheProgramasyoungas16monthsandsomesitesservefamilieswithchildrenupthroughfour-years-oldiftherearenootherpre-schoolservicesavailableinthecommunity.
Home Visit Structure: ■ AHomeVisitorismatchedwiththefamilyandvisitsthemforhalf-an-hour,
twice-a-weekonaschedulethatisconvenientforthefamily.■ Onthefirstvisitofeachweek,theHomeVisitorbringsacarefully-selected
bookoreducationaltoy,thecurricularmaterialfortheweek,whichisagifttothefamily.
■ Inthetwice-weeklyhomesessionswiththeparent(orotherprimarycaregiver)andthechild,theHomeVisitormodelsverbalinteraction,reading,andplayactivities,demonstratinghowtousethebooksandtoystobuildlanguageandemergentliteracyskillsandpromoteschoolreadiness.
■ OverthecourseofthetwoyearsintheProgram,familiesacquirealibraryofchildren’sbooksandalargecollectionofeducationalandstimulatingtoys.
■ EachProgramYearorCycleconsistsofaminimumof23weeksofhomevisitsor46homevisits.
TheParent-ChildHomeProgrammodeldoesallowforsomemodifications,iftheydonotaffectthevalidityofthemodelandareapprovedinadvancebytheNationalCenter,inordertoappropriatelyservefamiliesindiversecommunitiesandawiderangeofcircumstances.

Page 188
ReadingRecovery
ReadingRecoveryisaschool-based,short-terminterventiondesignedforchildrenagedbetweenfiveandsix,whoarethelowestliteracyachieversaftertheirfirstyearofschool.Thesechildrenareoftennotabletoreadthesimplestofbooksorevenwritetheirownnamebeforetheintervention.
Theinterventioninvolvesintensiveone-to-onelessonsfor30minutesadaywithatrainedReadingRecoveryteacher,foranaverageof20weeks(abouttwoterms).Theprogrammeisdifferentforeverychild,assessingwhatthechildknowsandwhathe/sheneedstolearnnext.Thefocusofeachlessonistocomprehendmessagesinreadingandconstructmessagesinwriting;learninghowtoattendtodetailwithoutlosingfocusonmeaning.
Childrencompletetheinterventionwhenanindependentobserverjudgesthemasabletoreadandwritewithouthelp,withintheappropriatebandfortheirage.Onaverage,childrenwhohavecompletedhavegonefromtextlevel0toalevel17;thesearebookswithelaboratedepisodesandevents,extendeddescriptions,someliterarylanguage,fullpagesofprint,moreunusualandchallengingvocabularyandlesssupportfromillustrations.Progresscontinuesaftertheintervention,withchildrenmakingonaverageonemonth’sgainwitheachmonththatpasses.
Childrenwhodonotmakethesegainsarereferredbacktotheschoolforlong-termsupport(oneinfive).Howevertheytoomakeconsiderableimprovements,makingoneyear’sgaininsixmonths,andonaveragegoingfromatextlevel0toalevel9;thesearesimplestorybookswithsomerepetitionofphrasepatterns,ideasandvocabulary,severallinesoftextandaround20-40wordsperpage.
ReadingRecoveryisthefoundationinterventionforEveryChildaReader(ECaR).
HistoryReadingRecoverywasfoundedinNewZealandbyMarieClay,basedonherextensiveresearchintoearlyliteracydifficulties
■ In1987MarievisitedCambridgeUniversity,whereshespokeofthedevelopmentofReadingRecoveryinNewZealand.InspiredbyMarie’svisitJeanPrance,anexperiencedprimaryheadteacherandteachereducator,wenttotheUniversityofAucklandtotrainasthefirstUKReadingRecoverytutor(nowknownasteacherleader)
■ In1990thefirstReadingRecoveryteachersweretrainedinSurrey,byJeanPranceandanexperiencedNewZealandtutor,forSurreyEducationAuthority
APPENDIX THREE
Descriptions of Recommended Early Intervention Programmes

Page 189
■ In1991theInstituteofEducation(IOE)invitedMarietoreturntotheUKwithasmallgroupofNewZealandcolleaguestosetupatutorprofessionaldevelopmentprogramme.SeventutorscompletedthetrainingforlocalauthoritiesinLondonandtheSouthEast
■ In1992thegovernmentcarriedoutathreeyearpilotfundedbyGrantsforEducationSupportandTraining.MariereturnedtotheUKforthefirstyeartosetuptwoparalleltutortrainingcourses,onebasedattheIOEandasecondinSheffield,and24tutorsweretrainedinthefirstyearforlocalauthoritiesacrossEngland.JeanPranceandJuliaDouetilweretrainedasthefirsttrainersfortheUK
■ Bythemid1990sReadingRecoveryhadspreadacrossEnglandandextendedtoschoolsinJersey,Scotland,Wales,NorthernIrelandandtheRepublicofIreland
■ In1995,afterthethreeyearpilotwascomplete,ReadingRecoverybecamelocallyfundedwithgovernmentsupportfornationalcoordinationinEngland
■ ThefirsttutorsforNorthernIrelandweretrainedin1993,forScotlandin1998,andforIrelandandWalesin1999
■ In2003auniversityprofessorfromCopenhagentrainedasaReadingRecoverytrainerattheInstituteofEducationandbeganaredevelopmentofReadingRecoveryintoDanishforimplementationinDenmark
■ InMay2005ReadingRecoverywasincludedintheDEIS(DeliveringEqualityofOpportunityinSchools)ActionPlanfortheRepublicofIreland,withfundingtargetedtochildrenindisadvantagedschools
■ Inearly2005theEuropeanCentreforReadingRecoveryworkedwithcolleaguesfromKPMGFoundationtodevelopEveryChildaReader(ECaR)asanextensionofReadingRecovery
■ InSeptember2005athree-yearECaRpilot,withReadingRecoveryatitscore,wasfundedbyacollectiveofcharitableorganisationsledbyKPMGFoundationandtheDepartmentforChildren,SchoolsandFamilies(DCSF)
■ In2008-11thesuccessoftheECaRpilotledtotheprogrammebeinggovernmentfundedinathree-yearrolloutacrossEngland
In2011governmentfundingforECaRwasplacedintoDedicatedSchoolsGrantforthefullthreeyearsofthe2011-14ComprehensiveSpendingReview,withtheintentiontoshifttheECaRstrategytoamarket-ledmodelProgramDescriptionReadingRecovery®isashort-termtutoringinterventionintendedtoservethelowest-achieving(bottom20%)first-gradestudents.ThegoalsofReadingRecovery®aretopromoteliteracyskills,reducethenumberoffirst-gradestudentswhoarestrugglingtoread,andpreventlong-termreadingdifficulties.ReadingRecovery®supplementsclassroomteachingwithone-to-onetutoringsessions,

Page 190
generallyconductedaspull-outsessionsduringtheschoolday.Tutoring,whichisconductedbytrainedReadingRecovery®teachers,takesplacedailyfor30minutesover12–20weeks.
ResearchFourstudiesofReadingRecovery®meetWhatWorksClearinghouse(WWC)evidencestandards,andonestudymeetsWWCevidencestandardswithreservations.Thefivestudiesincludedapproximately700first-gradestudentsinmorethan46schoolsacrosstheUnitedStates.3
Basedonthesefivestudies,theWWCconsiderstheextentofevidenceforReadingRecovery®tobemediumtolargeforalphabetics,smallforfluencyandcomprehension,andmediumtolargeforgeneralreadingachievement.Effectiveness
ReadingRecovery®wasfoundtohavepositiveeffectsonalphabeticsandgeneralreadingachievementandpotentiallypositiveeffectsonfluencyandcomprehension.
APPENDIX THREE
Descriptions of Recommended Early Intervention Programmes

Page 191
Parent–ChildInteractionTherapy(PCIT)
WhatisPCIT?Parent-ChildInteractionTherapy(PCIT)isanempirically-supportedtreatmentforconduct-disorderedyoungchildrenthatplacesemphasisonimprovingthequalityoftheparent-childrelationshipandchangingparent-childinteractionpatterns.InPCIT,parentsaretaughtspecificskillstoestablishanurturingandsecurerelationshipwiththeirchildwhileincreasingtheirchild’sprosocialbehavioranddecreasingnegativebehavior.Thistreatmentfocusesontwobasicinteractions:ChildDirectedInteraction(CDI)issimilartoplaytherapyinthatparentsengagetheirchildinaplaysituationwiththegoalofstrengtheningtheparent-childrelationship;ParentDirectedInteraction(PDI)resemblesclinicalbehaviortherapyinthatparentslearntousespecificbehaviormanagementtechniquesastheyplaywiththeirchild.
Parent–childinteractiontherapy(PCIT)isaformofpsychotherapydevelopedbySheilaEybergforchildrenages2–7andtheircaregivers.Itusesauniquecombinationofbehavioraltherapy,playtherapy,andparenttrainingtoteachmoreeffectivedisciplinetechniquesandimprovetheparent–childrelationship.PCITevolvedfromConnieHanf’stwo-stageoperantmodelofparenting.
StagesofPCITAlthoughPCITisdividedintotwostages,relationshipdevelopment(child-directedinteraction)anddisciplinetraining(parent-directedinteraction),therearealsothreedistinctassessmentperiods(pre-treatment,mid-treatment,post-treatment).
Child-directedinteractionThechild-directedinteractionportionofPCITaimstodevelopalovingandnurturingbondbetweentheparentandchildthroughaformofplaytherapy.Parentsaretaughtalistof“dos”and“don’ts”tousewhileinteractingwiththeirchild.TheywillusetheseskillsduringadailyplayperiodcalledSpecialTime.
DRIP/PRIDEskillsParentsaretaughtanacronymofskillstouseduringSpecialTimewiththeirchildren.Althoughtheacronymvariesfromtherapisttotherapist,itisgenerallyeither“DRIP”or“PRIDE.”DRIPstandsforthefollowing:
D–DescribeR–ReflectI–ImitateP–Praise

Page 192
Likewise,PRIDEstandsforthefollowing:
P–PraiseR–ReflectI–ImitateD–DescribeE–Enthusiasm
MostPCITtherapistscurrentlyusePRIDEbecauseDRIPisawkwardandthe“E”supportsthevalueandimportanceofparentalpositiveaffectiveengagementinparent–childinteractions.
Theseacronymsareremindersthatparentsshoulddescribetheactionsoftheirchild,reflectuponwhattheirchildsays,imitatetheplayoftheirchild,praisetheirchild’spositiveactions,andremainenthusiasticthroughoutSpecialTime.
Parent-directedinteractionTheparent-directedinteractionportionofPCITaimstoteachtheparentmoreeffectivemeansofdiscipliningtheirchildthroughaformofplaytherapyandbehavioraltherapy.Itcanbeusedwithmaltreatedchildren.
UsedPCIThasbeenusedwithabusivefamilies.PCIThasbeenusedwithoppositionalchildren.Parent–childinteractiontherapyisamodelthathasdemonstratedsuccesswithchildrenwithoppositionaldefiantdisorderthathasrecentlybeenappliedtochildrenwithautism.Currently,alotofresearchhasbeendoneonhowPCITcanbeusedtokeepdifficultparentingpopulationsintreatment.ResearchshowsthatskillslearnedinPCITtrainingsessionsgeneralizetothehome.
EfficacyPCIToutcomeresearchhasdemonstratedstatisticallyandclinicallysignificantimprovementsintheconduct-disorderedbehaviorofpreschoolagechildren:Aftertreatment,children’sbehavioriswithinthenormalrange.StudieshavedocumentedthesuperiorityofPCITtowaitlistcontrolsandtoparentgroupdidactictraining.Inadditiontosignificantchangesonparentratingsandobservationalmeasuresofchildren’sbehaviorproblems,outcomestudieshavedemonstratedimportantchangesintheinteractionalstyleofthefathersandmothersinplaysituationswiththechild.Parentsshowincreasesinreflectivelistening,physicalproximity,andprosocialverbalization,anddecreasesinsarcasmandcriticismofthechildaftercompletionofPCIT.Outcomestudieshavealsodemonstratedsignificantchangesonparents’self-reportmeasuresofpsychopathology,personaldistress,andparentinglocusofcontrol.Measuresof
APPENDIX THREE
Descriptions of Recommended Early Intervention Programmes

Page 193
consumersatisfactioninallstudieshaveshownthatparentsarehighlysatisfiedwiththeprocessandoutcomeoftreatmentatitscompletion.
CosteffectivenessParent–childinteractiontherapyhasbeenfoundtobeacosteffectiveapproach.Thewaythatcosteffectivenesswasmeasuredwasbycomparingratiooftreatmentcoststobehaviorgains,asmeasuredbyclinicallysignificantimprovementontheCBCL(reductionrangingfrom17–61%).
ForasummaryofPCITandinformationaboutthefutureresearchdirectionsofPCITsee:
Zisser,A.,&Eyberg,S.M.(2010).Treatingoppositionalbehaviorinchildrenusingparent-childinteractiontherapy.InA.E.Kazdin&J.R.Weisz(Eds.)Evidence-basedpsychotherapiesforchildrenandadolescents(2nded.,pp.179-193).NewYork:Guilford.

Page 194
FathersReadingEveryDay(FRED)
FathersReadingEveryDay(FRED)isanaward-winningUSfamilyliteracyprogrammeheldatlibraries,earlyyearscentres,nurseries,primaryschools,churchesetc.
Fathersreceiveapackcontainingareadinglog,tipsforreadingaloudandrecommendedbooklists.Duringfourweeksthedadsdocumenttimespentreadingtotheirchildrenandthenumberofbooksread.Collaboratingwithapubliclibraryencouragesfatherstosignup,familiarizesthemwiththelibrary,andprovidesaccesstofreebookstouseintheprogramme,aswellasbooksinlanguagesotherthanEnglish.
Morethan7,000fathershaveparticipatedsofarandstatisticallysignificantincreasespre/postinterventionincludetimespentreadingtochildren,numberofbooksread,levelofinvolvementinchildren’seducation,amountandqualityoftimespentwithchildren,andlevelofsatisfactionwiththefather-childrelationship.Thepercentageoffathersreadingtotheirchildrenthreeormoretimesperweekincreasedfrom53%to80%.
Over6,000fathersandchildrenfrom77TexasCountieshaveparticipatedintheFREDprogramsince2002.Outcomesfromtheprogramareverypositive.Participantswhocompletedtheprogramaveragedapproximately9hoursofreadingtimewiththeirchildrenandreadnearly40booksoverthecourseofthefour-weekprogram.
Resultsfromarecentevaluationstudyof300participantsdemonstratedsignificantimprovementsinmanyareas,includingtheamountoftimefathersspentreadingtotheirchildren,numberofbooksreadduringatypicalweek,levelofinvolvementintheirchildren’seducation,amountandqualityoftimespentwiththeirchildren,andlevelofsatisfactionwiththefather-childrelationship.Therewasalsoasignificantincreasefrompretopostinthenumberoffathersobtainingalibrarycard.OthersignificantfindingsfromFREDparticipantsinclude:
■ 61.4%reportedthatFRED“IncreasedthetimeIspentwithmychild.”■ 58.7%reportedthatFRED“ImprovedthequalityofthetimeIspendwithmy
child.”■ 57.2%reportedthatFRED“Helpedmebecomemoreinvolvedinmychild’s
education.”■ 66.2%reportedthatFRED“Increasedmysatisfactionlevelasaparent.”■ 70.3%reportedthatFRED“Improvedmyrelationshipwithmychild.”
APPENDIX THREE
Descriptions of Recommended Early Intervention Programmes

Page 195
Inopen-endedresponses,manyfathersindicatedthattheynotedimprovementsintheirchild’svocabulary,readingability,andinterestinbooksasaresultofparticipatinginFRED.Somefathersevennoticedimprovementsintheirownliteracyskills.

Page 196
TimetoRead
TimetoReadisapairedreadingprogrammeengagingbusinessvolunteersonaone-to-onebasiswithKeyStagetwochildrentodevelopthemsociallyandemotionallyaswellasenhancingtheirliteracyskills.Theprogrammewasestablishedin1999andwasinitiallychampionedbyNorthernIrelandElectricity.theprogrammewasevaluatedbyQueensUniversityusingarandomcontrolgroupdemonstratingitseffectiveness.
TimetoReadisoneofthreeTimeto…programmesdevelopedbyBusinessintheCommunity,inpartnershipwiththelocalEducationandLibraryBoards,tohelpimproveliteracy,numeracyandcomputingskillsinlocalprimaryschools.Theotherprogrammesare:Time2CountandTimetoCompute,the‘Timeto’CompaniessupporttheirstafftovolunteeranhourperweektoworkalongsideKeyStageTwochildren(eight—tenyearolds).
Currently48ofNorthernIreland’sleadingcompaniesparticipateonthe‘Timeto’programmesworkingin63schoolsacrossNorthernIreland,includingOldWarrenandKillowenPrimarySchools.
Suggestedbenefitstothecompanyinclude:■ developsstaffconfidence■ self-esteemandcommunicationskills■ motivatesstaffandenhancesteamwork■ raisesprofileinthelocalcommunity■ buildspartnershipswithlocalschools
Suggestedbenefitstotheschoolsinclude:■ providesaninsightintothebusinessworld■ motivatesanddevelopschildrenacademicallyandsocially■ introduceschildrentoapositiverolemodelfromtheworldofwork■ enableschildrentoworkonaone-to-onebasisimprovingcommunicationskills
Time2Count(notyetrobustlyevaluated)alsofocusesonchildreninPrimary5—Primary7.Theaimofthisprogrammeistomotivatechildrentoenjoymathsandtorecogniseitasaneverydayactivity.Volunteersplaymathbasedgameswiththechildrentoconsolidatemathslearningintheclassroom.NorthernBankleadthisnumeracyprogramme.
TimetoCompute(notyetrobustlyevaluated)hasbeendevelopedtohelpbridgethedigitaldivideinlocalprimaryschools.Businessvolunteersworkonaone-to-oneprogrammewithchildrenaged8-10helpingthemtobecomeliterateinInformation
APPENDIX THREE
Descriptions of Recommended Early Intervention Programmes

Page 197
andCommunicationsTechnology(ICT).HPhavesupportedtheTimetoComputeprogrammefromitslaunch.
TheCommitmentCompaniesinvolvedagreetoreleasestaffforonehouraweektovolunteerinalocalschool.Initialcommitmentisforoneyearwiththeoptionofextendingandmanyofourvolunteersarenowintheirfifthandsixthyear.CompaniesinvolvedinTimetoReadandTimetoCountalsoagreetocontributefinanciallytohelpprovideresourcesfortheschool(eitherbooksormathsmaterials).

Page 198
APPENDIX FOUR
Early Intervention Sites in the UK and Ireland
Nottingham
youngballymun
WestTallaghtCDI

Page 199
NottinghamEarlyIntervention
TheEarlyInterventionProjectsAnumberofinnovativedeliveryprojectshavebeentrialledaspartofthebroaderEarlyInterventionProgramme.Theprojectsincludednewworkandlearningfromexistingwork,andhavefocusedontacklingintergenerationalcyclesofdeprivationandcomplexproblemswithinNottingham,drivingtheProgramme’svision.
TheprojectsweredevelopedbythesixThemePartnershipsofOneNottingham,requiringjoined-upworkingtotacklecross-cuttingissues.
■ CrimeandDrugsPartnership• DrugAwareAward• StrongerFamiliesProject• AdultOffendingTeamFamilyInterventionProject
■ Children’sPartnership• DevelopingNaturalLearning• RaisingAspirations UsingCustomerInsighttoEnableEffectiveEngagement PuttingFamiliesattheCentre 11-16LifeSkills iRise FamilyWelfare-ReducingPersistentAbsence
■ HealthandWellbeingPartnership• FamilyNursePartnership• ActiveFamilies
■ NeighbourhoodPartnership• SanctuaryInitiative
TheseprojectsconcludedinMarch2011,withlearningfromthemostsuccessfulelementseitherbeingsustainedthroughmainstreamsystemsorbeingfurtherdevelopedandtested.Thiswillenablethedevelopmentofmorerobustevidenceoftheimpactofthesemodels.
Elementsofthefollowingprojectsarecontinuing:
■ StrongerFamiliesProject■ RaisingAspirations■ 11-16LifeSkills

Page 200
■ DrugAwareAward■ FamilyNursePartnership■ ThebroaderFamilyInterventionProject■ ActiveFamilies■ SanctuaryInitiative
Moreinformationwillbeavailablesoonontheseapproachesgoingforward.
CRIMEANDDRUGSPARTNERSHIP
DRUGAWAREAWARDSettingarobuststandardofexcellenceindrugseducationandpolicywithinschoolsandthecommunity.ProvidinganidentifiablebrandthatcanbeusedtodriveforwardthestandardofdrugsandalcoholeducationinNottinghamCityto:
■ EncourageschoolstoreachaboveandbeyondtheHealthySchoolsstandard■ Raisetheprofileofdrugseducationforpupils,parentsandthecommunity■ Ensureeffectivescreeningofdruguseandrisksofdruguse■ Ensureeffectivetargetedinterventionsforthosepupilsassessedas‘atrisk’
throughimprovedreferralpathwaystospecialistservicesandthroughembeddingtargetedinterventionswithinaschoolsettingwithappropriatelytrainedstaff
■ Helpparentstobemorefullyengaged(inbothpolicysettinganddrugseducation)
■ Increasepartnershipworkingwiththeschoolcommunity,NeighbourhoodBeatTeamandTradingStandards
■ InvolvepupilsintheCity-widedrugseducationpolicysetting■ Increasetheskillbaseofkeystaffwithinschools
STRONGERFAMILIESPROJECTStrongerFamilies,deliveredbyWomen’sAid,offersa12-weekprogrammeoffocusedgrouptherapeuticsessionsformothersandchildren(aged4-16)whohavebeenaffectedbydomesticabuse,oncetheperpetratorhasnowleftthefamilyhome.
Mothersandchildrenpartakeinseparategroupsessionswhichrunconcurrently.Thesessionsprovidebothmotherandchildwithasafespaceandtheopportunitytodisclose,processandunderstandtheabusethattheyhaveexperiencedorwitnessed.Mothersaresupportedtobetterunderstandtheirchild’sbehaviour,relatingtotheabuse.
APPENDIX FOUR
Early Intervention Sites in the UK and Ireland

Page 201
Theprojectaimstostoptheintergenerationalimpactofdomesticabusebysupportingfamiliestorecoverfromtheabuseanddecreasethelikelihoodofrepeatincidents.
FromAugust2009toDecember2010,therehavebeentwodomesticviolencerelatedrepeatincidentswithinthefirst26families(7.7%)whohavecompletedtheprogramme;significantlylowerthanthenationaldomesticviolencerepeatincidentrateof44%.
Schoolshavereportedimprovementsinthebehaviour,confidenceandinteractionsofyoungpeopleintheprogramme.Therehasbeenincreasedschoolattendanceofchildrenwherethishadpreviouslybeenaproblem.
ADULTOFFENDINGTEAMFAMILYINTERVENTIONPROJECTReducingtheriskofoffendingandentryintothecriminaljusticesystembychildreninthefamiliesofadultoffenders,particularlypersistentandprolificoffenders.Theprojectprovidesstabilityofaccommodation,supporttoreducesubstancemisuse,helptoobtaintrainingandemploymentforrelevantfamilymembersandtoincreasetheacademicsuccessofchildreninthefamily.Theprojectworksholisticallyandintensivelywiththefamiliesofadultoffenderswhoareeitherthemselvesparentsorareoldersiblingslivingwithinorimpactinguponanexistingfamilyunitinordertobreakthecycleofintergenerationaloffendingandreducethecriminalinfluencethatadultoffendershaveuponthechildrenwithwhomtheyhavecontact.Intensivesupportofatleastsixmonthsisprovidedtothefamiliesusing,whereappropriate,a‘coercive’modelofengagement.
Children’sPartnership
DEVELOPINGNATURALLEARNINGTriallingtheForestSchoolsapproachwithsixschoolsintheCity,encouragingchildrentoexploretheirlocalenvironmentanddevelopreasoningskills,analyserisksandpredicttheconsequencesoftheiractions.Theseven-weekoutdoorlearningprogrammepromotesteamwork,listeningskills,risktaking,tooluse,safetyawareness,cooperationandindependence.
Theactivitiescreateopportunitiesforemotional,socialandbehaviouraldevelopment,improvingoutcomesthroughimprovingbehaviourandhigherlevelthinkingskills.Theprojectaimstoembedthelearninginschoolsandprovideopportunitiesforstaffwithintheschooltosharelearningandbestpracticewithotherschoolsandcolleagues.

Page 202
Childrenhavereportedthattheprojectincreasedtheirconfidence,socialskillsandtheirabilitytomakebetterdecisionsandhashelpedthemtolearnwhichrisksarewisetotake.Parentsandteachershavealsogivenpositivefeedbackandtherehavebeennoexclusionsinthesegroupssincetheprojectstarted.
RAISINGASPIRATIONSDevelopingandtriallinganaspirations-raisingtoolkit,whichincludesauniqueaspirationsassessmenttool,apackageofinterventionsdesignedtoraiseaspirationandaprocessfordevelopinganaspirationsfocus.AspirationDevelopmentOfficersaredeliveringinterventionsinschoolsandresearchingandplanningfutureinterventions.
Theassessmenttoolisthefirstprimary-ageappropriate,aspirationassessmenttoolnationally.Itallowsschoolstotakeanearlyinterventionapproachtounderachievementandnegativebehaviours.Childrencannowbeidentifiedasbeing‘atrisk’ofmakingnegativedecisionsasaresultoflowlevelsofaspiration.Previouslytherehasbeennoassessmentmechanism.
Earlyindicatorsofimpactfromtheinterventionsbeingtrialledarealreadybeingreportedbyteachers,includingsignificantimprovementsintheconfidence,attitude,behaviourandengagementofpupilsinthecohortwhohadbeenidentifiedashavingverylowlevelsofconfidenceandaspirationatthestartoftheproject.
Theprojectisalsoshowingpositiveimpactonattendanceandattainmentofthosepupilsinvolvedintheproject.Twoschoolshavealreadyreportedthatthecohortreceivingaspiration-raisingsupport,performedwellaboveexpectationintheirSATs,withtwootherschoolsreportingresults10%higherthanpredictionsandinoneschoolanumberofindividualpupilshavemadeup13sub-levelsofprogress,comparedtothepredictedsix.
ItisplannedthatthetoolkitwillbeusedacrossthewiderChildren’sWorkforce.
USINGCUSTOMERINSIGHTTOENABLEEFFECTIVEENGAGEMENTWITHCHILDRENANDTHEIRPARENTSResearchhasbeenundertakenusingExperian’sCustomerInsightdatabase,whichprovidestheunderstandingofneedwithinNottinghamCitythatisrequiredtodelivertherightservicestotherightchildren,youngpeopleandfamilies,throughtherightfacilityattherighttime.Theinformationisbeingusedtoreengineerservicessothatserviceprovisionmeetsneedthrough:
■ Understandinglevelsofneedforserviceswithineachlocality
APPENDIX FOUR
Early Intervention Sites in the UK and Ireland

Page 203
■ Understandingthechildrenandfamilieswhouseandneedservices,withservicesbeingdeliveredinthemostappropriate,accessibleandeffectiveway
■ Communicationwiththetargetgroupsbeingundertakeninthemosteffectiveway
Effectivelyunderstandingneedwithinlocalitieswillenablecomparisonofserviceprovision,serviceuptakeandneedandthereforeidentificationofefficiencyofservices.Thiswillenablethetargetingofworkatindividualsorfamilieswhoareverylikelytohavedifficultiesorimpairedoutcomeswithouteffectivesupportorintervention.
Furtherdetailoncustomerinsightcanbefoundathttp://www.nottinghaminsight.org.uk/
PUTTINGFAMILIESATTHECENTRE(PARTOFTHECOLLABORATIONFORLEADERSHIPINAPPLIEDHEALTHRESEARCHANDCARE,NOTTINGHAMSHIRE,DERBYSHIREANDLINCOLNSHIRESTRAND[CLAHRCNDL])AnationalNHSandUniversityofNottinghamcollaboration.NottinghamisapartnerintheNDLstrandoftheCLAHRC.Thefocusoftheprojectistranslatingcurrentacademicresearcharoundmentalhealthservicesandchildrenandyoungpeopleintoworkingpracticethroughtwo‘DiffusionFellows’,actingaschangeagentsacrosstheCity.Theworkisexploringtheimpactofuncoveringparentalmentalhealthneedsinordertobettermeettheneedsofthechildandislookingintotheorganisationalbarrierstoajoined-upmodelofadultandchildmentalhealthprovisionintheCity.Proposalstotrialajoined-up,familyfocusedmodelarebeingdeveloped.
11-16LIFESKILLSThe11-16LifeSkillscurriculumprogrammeisdesignedtosupportthedevelopmentoftheskillsandknowledgeneededforyoungpeopletomakethebestlifedecisions,increaseconfidencelevelsandraiseaspirations.
Therearecurrentlyjustunder3000youngpeopleaccessingtheprogrammewithinsixsettings.Atrainingprogrammeandtoolkitforschoolstodelivertheprogrammeisbeingdeveloped,withtheaimofrollingitouttoallsecondarysettingsintheCityearlyin2011.
ThetoolkitwillincludeanumberofPlanningFrameworkmodelsandthenewSEAC(SocialEmotionalAspectsofChange)resourcematerials,whichisbasedonSEAL(SocialEmotionalaspectsofLearning,usedinallprimaryschools)focusingonchangingnegativebehaviours.

Page 204
TheNationalFoundationforEducationalResearch(NFER)haveconductedanindependentevaluationoftheproject;theinitialconsultationanddesignprocess,whichinvolved550studentsand218staff,wascitedasexcellentpractice.Theconsultationfoundthatstudentsfeelthatthereisaneedformorecoverageofmentalhealthissues,financialcapability,sexualrelationships,parentinganddemocracy.
Sofar,thefollowingimprovedoutcomesforchildrenandyoungpeoplehavebeendemonstrated;
■ Improvedconfidencetodiscusssensitivetopicswithteachersandformulateandexpressopinions
■ Improvedskilldevelopment,knowledgeandunderstandingoftopicareas■ Studentsreportedthattheyfeltbetterinformedandequippedtomake
decisionsaboutsexandrelationshipsandriskawareness■ Studentshaveimprovedawarenessofhowtoseekhelp,forexample,howto
accesssupportfromtheschoolnurseaboutcontraceptionandSTIs.
Staffhavealsoreportedanincreasedconfidenceinteachingsensitivetopics.
IRISEiRiseworkswithagroupofchildrenandyoungpeopleinKeyStages2-4(ages8-16)inNottinghamCityschools,whoareinthecareoftheLocalAuthority.Theprojectaimsistoincreasetheyoungpeople’sattainmentandaspirationanddeveloptheirsocialandemotionalresilience.Thiswillbeachievedthroughindividuallearningsupport,motivationalpersonaldevelopmentprogrammesfocusingongoalsettingandselfesteemandaspiration-raisingeventstoinformyoungpeopleaboutpost-16educationalopportunities.
ApositivepsychologydevelopmentprogrammehasbeendeliveredtoanumberofyoungpeopleinthecareoftheLocalAuthority.Participantshavereportedthatthecourseisusefulforanumberofareasoftheirlife;mostly‘takingcareofmyself’,‘takinganactivepartinFurtherEducation(FE)’andpersonalgoalsetting-94%saythattheywouldrecommendit.
PartnershipshavebeendevelopedwithAimingHigher,NewCollegeNottinghamandNottinghamCityCouncilSportandLeisureServicestodeliveraspiration-raisingeducationalopportunitiesawarenessevents.Allyoungpeopleinvolvedintheprojecthavereportedthattheseeventshavemadethemawareoftheopportunitiesavailabletothemandthattheyarenowplanningtoaccesspost-16education.
APPENDIX FOUR
Early Intervention Sites in the UK and Ireland

Page 205
FAMILYWELFARE-REDUCINGPERSISTENTABSENCEImprovingtheuseofresourcestotacklethecausesofabsenceinschools.Theprojectfocusesontheearlystageinthecycleofabsence,particularlyinprimaryschoolsandYearsSevenandEightofsecondaryschools,aswellasfocusingonfamilieswithyoungchildrenwhohavepoorattendingoldersiblings,inordertobreaktheintergenerationalcycleofnon-attendance.
Asignificantdecreaseinpersistentabsencehasbeendemonstrated.AcrossthesixschoolsspecificallytargetedbytheDepartmentforEducation,betweenSeptember2009andMarch2010,therewasadecreaseof133casesofpersistentabsence;areductionof26%.Summerterm2009statisticsshowareductionof23.5%acrossallSecondaryschoolsandAcademies,and44.9%acrossPrimaryschools.
IndicatorsalsoshowthatpersistentabsenceistackledandresolvedmorequicklywiththeuseoftheLeadProfessionalbudget,astheamountofchildrenoryoungpeoplewhoarepersistentlyabsentformorethanonetermhasshownadecreasingtrendsincethestartoftheproject,from46%inAutumn2008/09to23%inAutumn2009/10.
HEALTHANDWELLBEINGPARTNERSHIPFAMILYNURSEPARTNERSHIPProvidingsupporttofirst-timepregnantteenagersandtheirpartner,inordertopositivelyimpactontheirparentingskillsandoutcomesforthemandtheirchild.
Theprogrammehasdemonstratedimprovedmentalhealthandparentingskills,increasedbreastfeedingandimmunisationtake-upratesandreducedsmokingrates.
AnecdotalevidenceindicatesthatissuesareidentifiedatanearlierstageandthereforeSocialCaresupportismoreeffective.
Nottinghamispartofaninternationaltrialofamodelfordeliverytogroups(currentlyone-to-one)andislookingintothecostandimpactofthis.
Theprojectreceivedadditionalfundingtoexploreengagementoffathersintheirchild’slife.Findingsarenowreadyfordissemination,withkeymessagesincludingthatsomemendonotengagewiththeservicebecausetheybelieveittobejustformothers;howeverthedepthoftherelationshipthenursedevelopswiththefatheriscrucialinachievingsuccessfuloutcomesforthechild.

Page 206
ACTIVEFAMILIESIncreasingopportunitiesforfamiliestoengageinphysicalactivity,regularlytogether.Aimingtohalttheriseinobesityandreducehealthinequalitiesandcardiovasculardisease.AvarietyofphysicalactivityandsportsessionsareprovidedeachweekataselectionofleisurecentresacrosstheCity.
310families(1073individuals)haveengagedintheprojectsincethelaunchinMay2009.12%ofthesefamilieshavealreadystartedtoshowcontinuedengagement(5sessionsormoreattended).63%ofthoseengagedarefromareaswithlowlevelsofphysicalactivityandhighlevelsofchildobesityanddeprivation.
Theprojectalsoactsasauniquereferralpathwayforchildhoodobesitybetweentheagesoftwoandfour,andalsoapathwayfromtheGo4It!project.
NEIGHBOURHOODPARTNERSHIPTHESANCTUARYINITIATIVEProvidingadditionalsecuritytothehomesofsurvivorsofdomesticabuse,oncetheperpetratorhasbeenremoved,andapackageoffloatingsupport,includinghomevisits,foruptosixmonths.Theprojectenablesfamiliestostayintheirownhomeandsocialnetworkandthechildrentostayintheircurrentschool.
Evidenceofimpactisdemonstratedbythereducedrateofrepeatdomesticviolenceincidentswithinthecohort(30%),muchlowerthanthenationalrepeatincidentrateofdomesticviolence(44%).Therehasalsobeenareducedprevalenceofhomelessnessapplicationsduetodomesticviolence(NottinghamCityHousingAid)-thishasgonefrombeingthethirdmostprevalentreasonin2006/07tothefifthin2008/09.
APPENDIX THREE
Early Intervention Sites in the UK and Ireland

Page 207
youngballymun
youngballymunisoneofthreeprojectsestablishedthroughthePreventionandEarlyInterventionProgramme,jointlysupportedandresourcedbytheOfficeoftheMinisterforChildrenandYouthAffairsintheRepublicofIrelandandtheAtlanticPhilanthropies.
ThePreventionandEarlyInterventionProgrammeforChildrenwasestablishedbyGovernmentinFebruary2006tosupportandpromotebetteroutcomesforchildreninareasdesignatedasdisadvantaged,throughmoreinnovation,effectiveplanning,integrationanddeliveryofservices.
TheProgrammetargetsthreegeographicareasinwhichthereisevidenceoftheneedforearlyintervention-Ballymun,TallaghtWestandDarndale.Thepurposeoftheprogrammeistosupportthedevelopment,implementationandevaluationofstrategiesforchildrenatlocalleveldrawnupbythestatutory,voluntaryandcommunityagenciesoperatingintheareasconcerned.TheProgrammeprovidesfortheintroductionandevaluationofarangeofintegratedinterventionsforchildrenandtheirfamiliesandtestiftheymakeapositivedifferencetochildren.
Thefocusoftheprogrammeisonsupportinginterventionswhichfitwithnationalpolicyobjectivesandhavebeendevelopedinconjunctionwiththelocalcommunity.Learningandevaluationareimportantcomponentsoftheprogrammeandindividualservices,areaprojectsandtheoverallprogrammewillbesubjecttoongoingandrobustreviewandevaluation.
TheOMCYAhaspartneredwiththeAtlanticPhilanthropiesinfundingthisprogrammeandatotalfundofupto€36,000,000isavailableacrossthethreeprojects.GovernmentandtheAtlanticPhilanthropieswillprovide€18millioneachinfunding.
youngballymun,theChildhoodDevelopmentInitiative,TallaghtandPreparingforLifeNorthsidePartnershiptogetheraretheprojectsthatmakeupthePreventionandEarlyInterventionProgramme.ResearchandplanningonpreventionandearlyinterventionmeasuressponsoredbyAtlanticPhilanthropies,hadbeenundertakenintheseareasandtheywereconsideredtobeinanexcellentpositiontotestnewmodelsofservicedelivery.Ifthesemodelsprovesuccessful,theresultsoftheseprojectsmayprovidethebasisforenhancedresourceallocationprocessesandpolicychanges.

Page 208
TheoverallprogrammeisbeingmanagedbytheOfficeoftheMinsterforChildrenandYouthAffairsonbehalfoftheGovernment.Approvalhasbeengiventofundallthreeprojects2007-2011/12.
WestTallaghtChildDevelopmentInitiative
IntroductionTheChildhoodDevelopmentInitiative(CDI)beganasaplanninginitiativein2003tosupportbetteroutcomesforchildreninTallaghtWest.Aconsortiumof23membersrepresentingcommunityleaders,residentsandprofessionalslivingandworkinginTallaghtWestdevelopedtheoutcomes-focused10-yearstrategy‘APlaceforChildren’.Basedonthislong-termstrategy,adetailedimplementationwasagreedfor2007-2011,againstwhichamajorinvestmentof€15millioneurowasmade,co-fundedbytheDepartmentofChildrenandYouthAffairs,throughthePreventionandEarlyInterventionFund,andTheAtlanticPhilanthropies.
MissionThemissionofWestTallaghtCDIis“WewholiveandworkinTallaghtWesthavehighexpectationsforallchildrenlivinginourcommunities.Wewantourchildrentolovewhotheyareandtobecherishedirrespectiveofsocialbackground,culturaldifferencesandcountryoforigin.Weseeeverychildandeveryfamilybeingprovidedwithsupport,opportunitiesandchoicestomeettheseexpectations.Weseethewholecommunityowningresponsibilityforthequality,beautyandsafetyofthelocalenvironment.Weseechildrenencouragedandcherishedbythewholecommunity.”
QualityServices,BetterOutcomesWorkbooktheCDIhaverecentlypublished‘QualityServices,BetterOutcomes’whichprovidesapracticalresourceforfrontlinestaff,servicemanagersandorganisationsthatarecurrentlyimplementingorintendtoimplement,evidence-basedprogrammesandservicesforchildrenand/ortheirfamilies,drawingonresearchexamplesofbestpractice.
TheCDIProgrammes■ EarlyYearsService■ DoodleDenProgramme■ Mate-TricksProgramme(hasnowbeenstoppedfollowingpoorevaluation
results)■ HealthySchoolsProgramme■ CommunitySafetyInitiative■ QualityEnhancementProgramme■ SafeandHealthyPlace
APPENDIX THREE
Early Intervention Sites in the UK and Ireland

Page 209
■ RestorativePractice■ RestorativePracticeSchedule2011■ CommunityCoachingProgrammeTheirfivemainprogrammesaresubjecttoRCTevaluationsandshouldbeavailableshortly.
GovernanceTheWestTallaghtCDIgovernancestructuresincludethefollowing:■ CDIBoard■ CDIImplementationSupportGroup■ ExpertAdvisoryCommittee■ FinanceandRiskSubCommittee■ ExecutiveSubCommittee■ CommunitySafetyInitiativeSteeringCommittee■ HealthySchoolsSteeringCommittee■ SafeandHealthyPlaceSteeringCommittee■ RestorativePracticeManagmentCommittee

Page 210

Page 211

Page 212

Page 213

Forfurtherinformationoradditionalcopies
Please contact:
TheResurgamTrustSuite31stFloorLaganviewEnterpriseCentre69DrumbegDriveLirburnBT281NY
Tel:02892670755Fax:02892670755
Email:[email protected]