
THE ARIAS STELLA REACTION
5
THE ARIAS STELLA REACTION BY DAVID CHARLES, M.B., M.R.C.O.G. Departments of Gynaecology and Pathology, University of Glasgow ARIAS STELLA (1954) described atypical endo- metrial changes in cases of uterine abortion, hydatidiform mole, chorionepithelioma, syn- cytial endometritis and one case of ectopic pregnancy. The atypical findings are noted in glands in the proliferative or secretory phase and consist of nuclear and cellular enlargement. The nuclei are hyperchromatic, often two to five times the normal size, sometimes lobulated, and tend to occupy the luininal portion of the cell. Mitoses are occasionally noted. The cytoplasm may be vacuolated and present a foamy appear- ance. In some glands intra-luminal tufts with loss of cellular boundaries can be observed. The changes are normally focal involving one or two cells in a group or in some cases the majority of cells in several glands. Confirmations of Arias Stella’s findings have appeared in the American literature (Pildes and Wheeler, 1957; Roach, Guderian and Brewer, 1960; Birch and Collins, 1961), but not from this country where the condition appears to be insufficiently known. It can be of value in diagnosis of several conditions where tropho- blast is present in the body. It is the purpose of this article to demonstrate the lesion and offer TABLE Histological Findings in Cuvettings Case Pregnancy Endometrial Pattern Decidua Suspected Arias Stella Reaction 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 .. .. .. .. .. .. .. .. .. .. .. .. .. .. .. .. .. .. .. .. .. .. .. .. .. .. .. .. .. .. .. .. .. .. .. .. .. .. .. .. .. .. .. *. .. .. .. .. .. .. .. .. .. .. .. .. .. .. ,. .. .. .. .. .. .. .. Yes No Yes Yes Yes Yes No Yes Yes Yes Yes No Yes No Yes Yes Yes Yes Yes Yes Yes Yes Secretory Secretory Mixed Proliferative Secretory Secretory Secretory Mixed lnsufficient for diagnosis Proliferative Mixed Secretory Pro1iferative Mixed Mixed lnsufficient for diagnosis Proliferative Secretory Secretory Mixed Proliferative Mixed - - - - Present Present Present Present - - Present - - - Present - - Present Present Present - - Present Present Present Present Present Piesent Present - - - Present Present Present Present - - - Present Present Present - - Total 22 18 Secretory 8 Present in 9 Present in 14 Mixed 7 Proliferative 5
-
Upload
david-charles -
Category
Documents
-
view
217 -
download
1
Transcript of THE ARIAS STELLA REACTION

THE ARIAS STELLA REACTION BY
DAVID CHARLES, M.B., M.R.C.O.G. Departments of Gynaecology and Pathology, University of Glasgow
ARIAS STELLA (1954) described atypical endo- metrial changes in cases of uterine abortion, hydatidiform mole, chorionepithelioma, syn- cytial endometritis and one case of ectopic pregnancy. The atypical findings are noted in glands in the proliferative or secretory phase and consist of nuclear and cellular enlargement. The nuclei are hyperchromatic, often two to five times the normal size, sometimes lobulated, and tend to occupy the luininal portion of the cell. Mitoses are occasionally noted. The cytoplasm may be vacuolated and present a foamy appear- ance. In some glands intra-luminal tufts with loss
of cellular boundaries can be observed. The changes are normally focal involving one or two cells in a group or in some cases the majority of cells in several glands.
Confirmations of Arias Stella’s findings have appeared in the American literature (Pildes and Wheeler, 1957; Roach, Guderian and Brewer, 1960; Birch and Collins, 1961), but not from this country where the condition appears to be insufficiently known. It can be of value in diagnosis of several conditions where tropho- blast is present in the body. It is the purpose of this article to demonstrate the lesion and offer
TABLE Histological Findings in Cuvettings
Case Pregnancy Endometrial Pattern Decidua Suspected Arias Stella
Reaction
1 2 3 4 5 6 7 8 9
10 1 1 12 1 3 14 15 16 17 18 19 20 21 22
..
..
. .
..
..
..
..
..
. .
..
. .
..
. .
. .
..
..
. .
. .
..
..
..
..
. .
..
. .
. .
. .
..
. .
. .
. .
..
..
. .
. .
. .
..
..
..
. .
..
. .
. . * .
..
..
. .
. .
. .
..
. .
. .
. .
. .
..
. .
. .
.. ,. . . .. . . .. . . . . ..
Yes No Yes Yes Yes Yes No Yes Yes Yes Yes No Yes No Yes Yes Yes Yes Yes Yes Yes Yes
Secretory Secretory
Mixed Proliferative
Secretory Secretory Secretory
Mixed lnsufficient for diagnosis
Proliferative Mixed
Secretory Pro1 iferat ive
Mixed Mixed
lnsufficient for diagnosis Proliferative
Secretory Secretory
Mixed Proliferative
Mixed
- -
- -
Present Present Present Present - -
Present - - -
Present - -
Present Present Present -
-
Present Present Present
Present Present Piesent Present
-
- -
Present Present
Present Present
-
- -
Present Present Present - -
Total 22 18 Secretory 8 Present in 9 Present in 14 Mixed 7 Proliferative 5

THE ARIAS STELLA REACTION
examples of its value in diagnosis. In addition an association with chorionepithelioma of extra- genital origin is recorded for the first time.
This report is based upon the histological study of twenty-two cases of tubal pregnancy where endometrial curettings were available, four cases of hydatidiform mole and two cases of chorionepithelioma. All available cases from the files of the Department of Pathology, Western Infirmary, Glasgow, for the period October, 1955 until October, 1961 are included.
1007
TUBAL PREGNANCY In the period of time covered by this review,
84 cases of tubal pregnancy were examined histologically, but endometrial curettings were obtained in only 22 cases (Table). These are the cases in which there was some doubt as regards the clinical diagnosis. It will be seen that the cellular atypia was noted in all 9 cases with decidua in the curettings and in 8 in which decidua was absent.
Four cases are of special interest as the diagnosis of ectopic pregnancy had not been seriously considered at the time of curettage and recognition of the Arias Stella reaction might have been of diagnostic value.
Case Histories Case 1. Mrs. F.McK., was admitted to hospital on
account of recurrent abdominal pain of three-weeks duration. The pain resembled renal colic and in view of a past history of a renal calculus she was investigated by the Urological Department but no renal lesion was discovered. However, as her last three periods had occurred at intervals of fourteen days a diagnostic curettage was performed and at the time of operation some thickening was noted in the right adnexal region. She was allowed home but was re-admitted two days later with a ruptured left tubal pregnancy. The curettings showed secretory phase endometrium but no decidua or chorionic tissue. In retrospective study the endometrial glands show marked cellular atypia of Arias Stella type (Fig. 1).
Case 2. Mrs. A.B., was admitted with a history of vaginal bleeding for five days and lower abdominal pain following 4 months amenorrhoea. Examination under anaesthesia revealed no significant abnormality.
Curettage produced hyperplastic tissue which on histological examination revealed secretory phase endo- metrium and decidua but no chorionic tissue. She remained in hospital on account of abdominal pain and eventually, in view of the histological report, a lapar- otomy was performed which revealed a left tubal pregnancy.
FIG. 1 Endometrium in the presence of a tubal pregnancy obtained from Case 1, showing intraluminal tufts with foamy vacuolated cytoplasm and nuclear hyper-
chromatism. Haematoxylin and Eosin x 215.
In retrospective study the endometrium was in the secretory phase with focal evidence of the Arias Stella reaction.
Case 3. Mrs. I.McA., was admitted to hospital on account of lower abdominal pain and irregular bleeding. The history suggested pelvic inflammatory disease following an abortion.
Examination under anaesthesia revealed a bulky uterus and no evidence of an adnexal mass. Curettage was per- formed and the histological findings revealed scant fragments of secretory endometrium with no evidence of decidua or chorionic tissue. The patient was discharged from hospital but returned four days later with a ruptured tubal pregnancy.
Again retrospective study reveals the Arias Stella Reaction in the endometrial glands (Fig. 2).
FIG. 2 Endometrium obtained from Case 3 showing focal enlargement of the gland cells with nuclear hypertrophy and hyperchromatism. Haematoxylin and Eosin x 84.

1008 JOURNAL OF OBSTETRICS AND GYNAECOLOGY
Case 4. Mrs. M.McG., was admitted on account of hypogastric discomfort and vaginal bleeding following 8-weeks amenorrhoea. No adnexal lesion was dis- covered on examination under anaesthesia. Endometrial tissue was obtained on curettage but no decidua or chorionic tissues. The histological picture of the endo- metrial tissue revealed a mixed proliferative secretory pattern.
She was allowed home but seven days later was admitted with a ruptured right tuba1 pregnancy.
In retrospect the secretory endometrial glands showed evidence of the Arias Stella Reaction (Fig. 3).
HYDATIDIFORM MOLE In 3 of the 4 cases the atypical endometrial
pattern was observed in the curettings following extrusion of the mole. In the fourth case the interval between curettage and evacuation of the mole was 28 days and no atypia was noted.
FIG. 4 Endometrial gland from the case of extragenital chorio- carcinoma (Case 5) which had been treated with methotrexate showing the Arias Stella reaction.
Haematoxylin and Eosin x 207.
CHORIONEPITHELIOMA The cellular atypia was noted in the endo-
Case 5. Mrs. M.C., was transferred from another hospital after examination of a right nephrectomy specimen had revealed choriocarcinoma. She was admitted originally with haematuria which was found to be due to a tumour of the right kidney. Chest X-ray revealed extensive metastatic deposits in both lungs. There was no history of anomalous uterine bleeding and a curettage revealed no uterine malignancy, although the cellular atypia was present in the endometrial glands.
She was treated by immunotherapy with her husband’s white cells (Jackson, Anderson and Gebbie, 1961) and
metrium in both cases.
FIG. 5 This is a further gland from the same uterus as Figure 4, illustrating the considerable variation in nuclear size.
Haematoxylin and Eosin x210.
received six courses of methotrexate therapy and radio- therapy to the lung metastases. Despite all measures her condition deteriorated and death occurred six months after the onset of her original symptom of haematuria. The final course of methotrexate was completed one week prior to death.
Necropsy showed the presence of widespread meta- stases in the lungs, small intestine, left kidney, brain, right femur and right second toe. The uterus, cervix, vagina, tubes and ovaries showed no evidence of disease. The endometrial glands showed the Arias Stella Reaction despite the methotrexate therapy (Figs. 4 and 5). FIG. 3
Endometrium obtained from Case 4 showing the atypical Case 6. Mrs. M.W., was admitted to hospital with a epithelial changes as described by Arias Stella. three-months history of post-coital bleeding and scant
Haematoxylin and Eosin X 131. periods for six months. The uterus was bulky and
THE ARIAS STELLA REACTION 1009
In animals where castration had been carried out combined oestrogen and progesterone resulted in endometrial aberrations and as a result he concluded that excessive pituitary gonadotrophin production accounted for these effects.
If Arias Stella’s conclusions from animal experimentation are correct the factors which influence the atypical reactions are hormonal. In ectopic pregnancy the disruption and resultant degeneration of villi could account for reduction of chorionic gonadotrophin and a consequent regression of the corpus luteum of pregnancy. A reduction in the oestrogen and progesterone levels would result in and promote progressive desquamation of the endometrium. This fact would also account for variations in the figures published for decidua in the endo- metrium in cases of tuba1 pregnancy (Romney et al., 1951; Pildes and Wheeler, 1957). In the 22 cases reported in the present series decidua was present in 9 and the Arias Stella reaction in 14 cases and in the latter cases the endo- metrium was either secretory or of a mixed secretory proliferative pattern. The Arias Stella lesion was not noted in a proliferative phase gland.
In cases of hydatidiform mole and chorio- carcinoma a greater amount of chorionic gonadotrophin is produced and in the cases presented marked endometrial aberrations are features worthy of consideration. The case that came to autopsy after methotrexate therapy had a florid endometrial atypia. Women with chorionepithelioma give a history of anomalous uterine bleeding as the primary lesion is usually located in the genital tract. The absence of pelvic signs or symptoms during the whole clinical course in this case signifies the prob- ability that the renal tumour was the primary site. The failure of methotrexate therapy also supports this conclusion, as Li et al. (1956) reported no success with this therapy in chorion- epithelioma in the male. The interesting fact that methotrexate did not modify the Arias Stella reaction in this case also indicates that the success of such therapy could be assessed by the presence or absence of cellular atypia. Curettage may, therefore, be an ancillary diagnostic and prognostic aid in the follow up of trophoblast tumours which might be especially helpful in
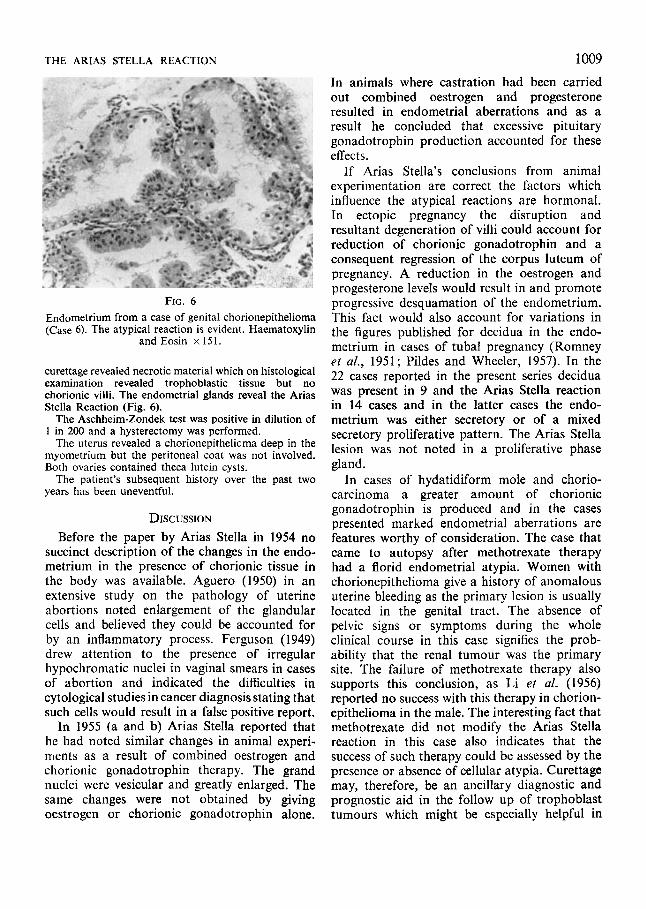
FIG. 6 Endometrium from a case of genital chorionepithelioma (Case 6) . The atypical reaction is evident. Haematoxylin
and Eosin x 151.
curettage revealed necrotic material which on histological examination revealed trophoblastic tissue but no chorionic villi. The endometrial glands reveal the Arias Stella Reaction (Fig. 6).
The Aschheim-Zondek test was positive in dilution of 1 in 200 and a hysterectomy was performed.
The uterus revealed a chorionepithelicma deep in the myometrium but the peritoneal coat was not involved. Both ovaries contained theca lutein cysts.
The patient’s subsequent history over the past two years has been uneventful.
DISCUSSION Before the paper by Arias Stella in 1954 no
succinct description of the changes in the endo- metrium in the presence of chorionic tissue in the body was available. Aguero (1950) in an extensive study on the pathology of uterine abortions noted enlargement of the glandular cells and believed they could be accounted for by an inflammatory process. Ferguson (1949) drew attention to the presence of irregular hypochromatic nuclei in vaginal smears in cases of abortion and indicated the difficulties in cytological studies in cancer diagnosis stating that such cells would result in a false positive report.
In 1955 (a and b) Arias Stella reported that he had noted similar changes in animal experi- ments as a result of combined oestrogen and chorionic gonadotrophin therapy. The grand nuclei were vesicular and greatly enlarged. The same changes were not obtained by giving oestrogen or chorionic gonadotrophin alone.

1010 the presence of false negative pregnancy tests such as are sometimes obtained in these cases (Thompson, Gross and Straus, 1951).
Most authors have pointed out that although these atypical changes mimic malignancy the process in fact is benign. In 1956 Truemner reported a radical hysterectomy performed on a woman aged 40 years on account of atypical cells in an endometrial biopsy which were reported as malignant. In the course of the operation an unruptured tubal pregnancy was discovered.
Roach, Guderian and Brewer (1960) found no resemblance to the cellular reaction of Arias Stella in 100 cases of endometrial carcinoma. The endometrial picture presenting in associ- ation with chorionic tissue in the body should offer no diagnostic difficulty when one can correlate the individual cells with the surrounding tissues.
JOURNAL OF OBSTETRICS AND GYNAECOLOGY
(2) It is a valuable diagnostic aid in unsus- pected cases of ectopic pregnancy when curet- tage has been performed for menorrhagia.
(3) In the follow up of trophoblastic tumours the presence of cellular atypia denotes activity and is not altered by methotrexate therapy as is illustrated by the case of extragenital chorion- epithelioma described.
SUMMARY
(1) The endometrial cellular atypia in associ- ation with tubal pregnancy, hydatidiform mole and chorionepithelioma (genital and extra- genital) is described.
REFERENCES Aguero, L. (1950): Cirug. Ginec. Urol., 1, 278. Arias Stella, J. (1954): A.M.A. Arch. Path., 58, 112. Arias Stella, J. (1955a): A.M.A. Arch. Path., 60,49. Arias Stella, J. (1955b): A.M.A. Arch. Path., 60, 59. Birch, H. W., and Collins, C. G. (1961): Amer. J . Obstet.
Ferguson, J. H. (1949): Cancer (Philad.), 2, 845. Jackson, J. M., Anderson, J. R. , and Gebbie, D. (1961):
Li, M. C., Hertz, R., and Spencer, D. B. (1956): Proc.
Pildes, R. B., and Wheeler, J . D. (1957): Amer. J . Obster.
Roach, W. R., Guderian, A. M., and Brewer, J. I. (1960):
Romney, S. L., Hertig, A. T., and Reid, D. E. (1951):
Thompson, R., Gross, S., and Straus, R. (1951): Amer.
Truemner, K. M. (1956): A.M.A. Arch. Path.. 61, 149.
Gynec., 81, 1198.
Brit. med. J. , 2, 1708.
SOC. exp. BioL., 93, 361.
Gynec., 13, 19.
Amer. J . Obstet. Gynec., 79,680.
Surg. Gynec. Obstet., 91, 605.
J. Obstet. Gynec., 61, 930.


















