The Alarming Challenge! Staffing Single Room NICUs · PDF fileThe Alarming Challenge! Staffing...
15
The Alarming Challenge! Staffing Single Room NICUs and Alarm Burden Rebecca J. Vartanian MD Assistant Professor Division of Neonatal-Perinatal Medicine Department of Pediatrics and Communicable Diseases University of Michigan Ann Arbor, MI Rebecca Jane Vartanian MD is an Assistant Professor in the Division of Neonatal-Perinatal Medicine within the Department of Pediatrics and Communicable Diseases at the University of Michigan. She received her medical degree from Wayne State University School of Medicine and completed her Pediatrics and Neonatology training at the University of Michigan. Dr. Vartanian joined the faculty in 2010. Dr. Vartanian oversees and facilitates the quality improvement initiatives in the Newborn Intensive Care Unit, including multi-center collaborations within Vermont Oxford Network and the State of Michigan Quality Initiative. Her clinical interests include oxygen management in premature infants, optimization of neonatal nutrition, and the care of extremely low birth weight infants. Michelle Nemshak MSN, RNC-NIC Clinical Nurse Specialist Brandon Newborn ICU C.S. Mott Children’s Hospital University of Michigan Health System Ann Arbor, MI Michelle Nemshak MSN, RNC-NIC is a Clinical Nurse Specialist in the Brandon Newborn ICU at C.S. Mott Children’s Hospital, University of Michigan Health System. Ms. Nemshak received her BSN from Nazareth College in Kalamazoo, MI and MSN from the University of Michigan. Ms. Nemshak has held a variety of leadership roles within the NICU and spent three years as a clinical project manager for a replacement hospital project. Ms. Nemshak oversees the clinical nursing practice, education, and quality improvement for the Newborn ICU. Her professional interests include process improvement, family centered care and neuro-protective care. Annual Quality Congress Breakout Session, Saturday, October 3, 2015 The Alarming Challenge! Staffing Single Room NICUs and Alarm Burden Objective: Identify the use of real-time alarm data to guide staffing decisions in a single room NICU setting.
Transcript of The Alarming Challenge! Staffing Single Room NICUs · PDF fileThe Alarming Challenge! Staffing...

The Alarming Challenge! Staffing Single Room NICUs and Alarm Burden
Rebecca J. Vartanian MD Assistant Professor Division of Neonatal-Perinatal Medicine Department of Pediatrics and Communicable Diseases University of Michigan Ann Arbor, MI
Rebecca Jane Vartanian MD is an Assistant Professor in the Division of Neonatal-Perinatal Medicine within the Department of Pediatrics and Communicable Diseases at the University of Michigan. She received her medical degree from Wayne State University School of Medicine and completed her Pediatrics and Neonatology training at the University of Michigan. Dr. Vartanian joined the faculty in 2010. Dr. Vartanian oversees and facilitates the quality improvement initiatives in the Newborn Intensive Care Unit, including multi-center collaborations within Vermont Oxford Network and the State of Michigan Quality Initiative. Her clinical interests include oxygen management in premature infants, optimization of neonatal nutrition, and the care of extremely low birth weight infants.
Michelle Nemshak MSN, RNC-NIC Clinical Nurse Specialist Brandon Newborn ICU C.S. Mott Children’s Hospital University of Michigan Health System Ann Arbor, MI
Michelle Nemshak MSN, RNC-NIC is a Clinical Nurse Specialist in the Brandon Newborn ICU at C.S. Mott Children’s Hospital, University of Michigan Health System. Ms. Nemshak received her BSN from Nazareth College in Kalamazoo, MI and MSN from the University of Michigan. Ms. Nemshak has held a variety of leadership roles within the NICU and spent three years as a clinical project manager for a replacement hospital project. Ms. Nemshak oversees the clinical nursing practice, education, and quality improvement for the Newborn ICU. Her professional interests include process improvement, family centered care and neuro-protective care.
Annual Quality Congress Breakout Session, Saturday, October 3, 2015 The Alarming Challenge! Staffing Single Room NICUs and Alarm Burden Objective: Identify the use of real-time alarm data to guide staffing decisions in a single room NICU setting.
The Alarming Challenge! Staffing Single Room NICUs and Minimizing Alarm Burden
Michelle Nemshak MSN, RNC-NIC, CNS / Rebecca Vartanian MD
October 3, 2015 1
The Alarming Challenge! Staffing Single Room NICUs and Minimizing
Alarm Burden
Michelle Nemshak MSN, RNC‐NIC, CNS
Rebecca Vartanian MDUniversity of Michigan Health System
C.S. Mott Children’s Hospital
October 3, 2015
Disclosure
Ms. Nemshak and Dr. Vartanian do not have any financial arrangement or affiliations with a commercial entity.
We will not be discussing the unlabeled use of a commercial product in our presentation.
Why Our Session?
Context #1: TJC is Coming!
• The Joint Commission mandated National Patient Safety Goal (NPSG.06.01.01)– Phase I: (ends December 2015)
• Establish alarms as a hospital priority
• Identify the most important alarms to manage
– Phase II: (beginning in Jan 2016)• Develop and implement specific policies and procedures for alarm management
• Develop a mechanism to educate staff about the purpose and proper operation of alarm systems
Context #2: Confused about Where to Start
Context #3: Seeking Clarification

The Alarming Challenge! Staffing Single Room NICUs and Minimizing Alarm Burden
Michelle Nemshak MSN, RNC-NIC, CNS / Rebecca Vartanian MD
October 3, 2015 2
Any Others?
Objective
• Identify the use of real‐time alarm data to guide staffing decisions in a single room (or any) NICU setting
Today’s Road Trip
• Stop 1: Addressing Alarm Management
• Stop 2: How to identify and use pulse oximetry and/or alarm data to improve your alarm management
• Stop 3: Single‐center experience with specific focus on the single‐patient room
Definitions
• Alarm Fatigue
– Desensitization to audio and/or visual alarm signals resulting from excessive exposure (sensory overload).
• Alarm fatigue has been identified as a major health hazard in reported sentinel events that have resulted in major injury or death
Why does it happen?
• The majority of alarms (85‐99%) are false alarms (JCAHO 2013)
– A false alarm, also called a nuisance alarm, is the deceptive or erroneous report of an emergency, causing unnecessary panic and/or bringing resources (such as emergency services) to a place where they are not needed.
‐Wikipedia1
– More alarms = More false alarms
Our Story
Aim: To decrease the incidence of severe ROP (defined as >stage II ROP) in infants with birthweight <1500 grams from approximately 10% to 5% with a stretch goal of 3% by June 2013.
The Alarming Challenge! Staffing Single Room NICUs and Minimizing Alarm Burden
Michelle Nemshak MSN, RNC-NIC, CNS / Rebecca Vartanian MD
October 3, 2015 3
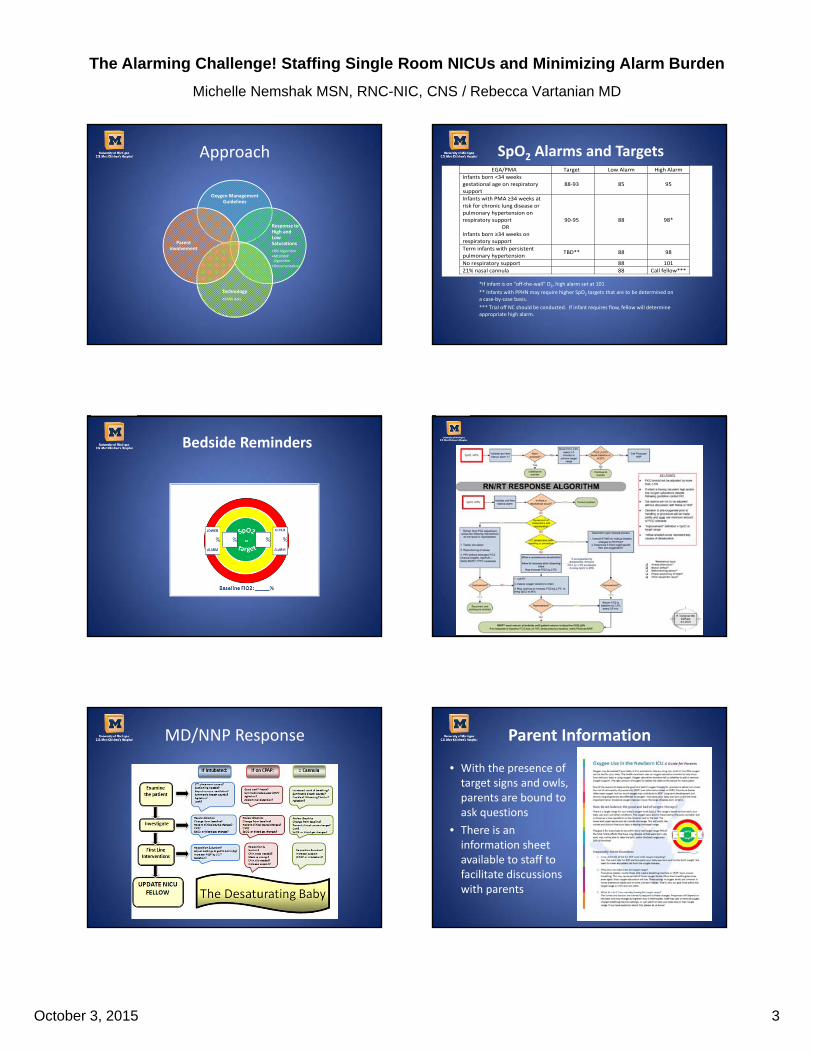
Approach
Oxygen Management Guidelines
Response to High and Low Saturations
•RN Algorithm
•MD/NNP Algorithm
•Documentation
Technology
•SANS data
Parent involvement
SpO2 Alarms and Targets
*If infant is on “off‐the‐wall” O2, high alarm set at 101
** Infants with PPHN may require higher SpO2 targets that are to be determined on a case‐by‐case basis.
*** Trial off NC should be conducted. If infant requires flow, fellow will determine appropriate high alarm.
EGA/PMA Target Low Alarm High Alarm
Infants born <34 weeks gestational age on respiratory support
88‐93 85 95
Infants with PMA ≥34 weeks at risk for chronic lung disease or pulmonary hypertension on respiratory support
OR Infants born ≥34 weeks on respiratory support
90‐95 88 98*
Term infants with persistent pulmonary hypertension
TBD** 88 98
No respiratory support 88 101
21% nasal cannula 88 Call fellow***
Bedside Reminders
MD/NNP Response Parent Information
• With the presence of target signs and owls, parents are bound to ask questions
• There is an information sheet available to staff to facilitate discussions with parents
The Alarming Challenge! Staffing Single Room NICUs and Minimizing Alarm Burden
Michelle Nemshak MSN, RNC-NIC, CNS / Rebecca Vartanian MD
October 3, 2015 4
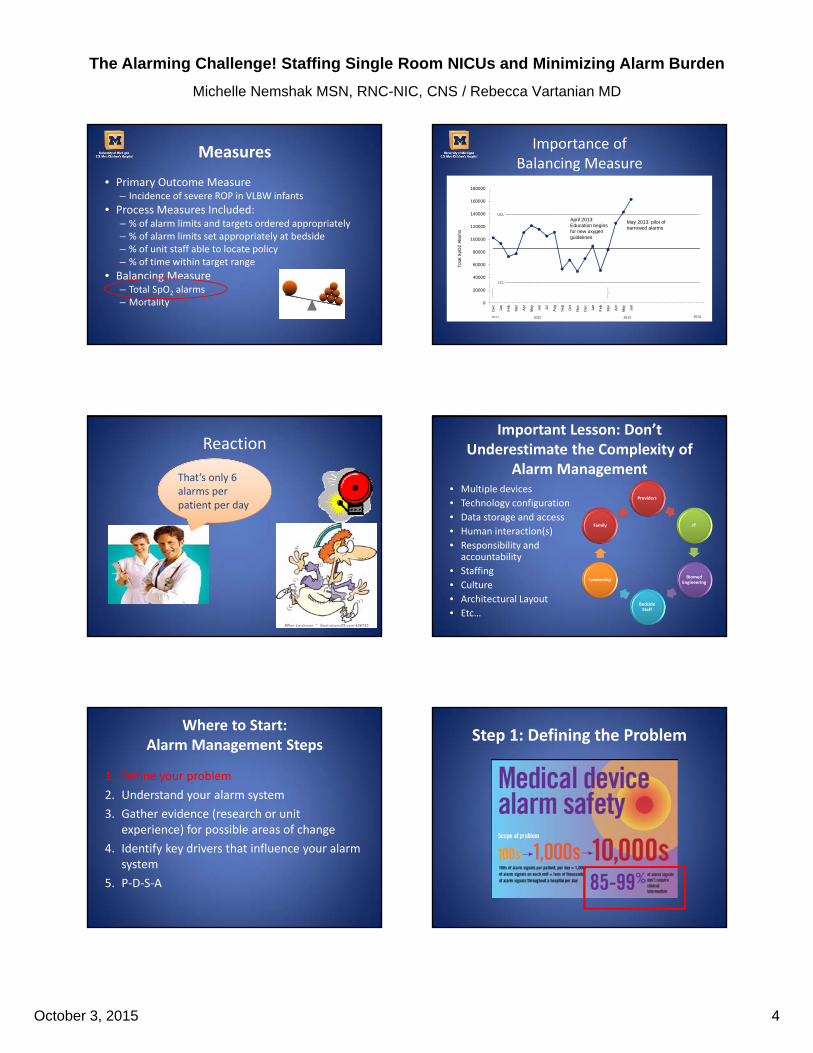
Measures
• Primary Outcome Measure– Incidence of severe ROP in VLBW infants
• Process Measures Included:– % of alarm limits and targets ordered appropriately– % of alarm limits set appropriately at bedside– % of unit staff able to locate policy– % of time within target range
• Balancing Measure– Total SpO2 alarms– Mortality
Importance of Balancing Measure
UCL
LCL
0
20000
40000
60000
80000
100000
120000
140000
160000
180000
De
c
Jan
Fe
b
Ma
r
Ap
r
Ma
y
Jun
Jul
Au
g
Se
p
Oct
No
v
De
c
Jan
Fe
b
Ma
r
Ap
r
Ma
y
Jun
Tot
al S
pO2
Ala
rms
2011 2012 2013 2014
April 2013: Education begins for new oxygenguidelines
May 2013: pilot of narrowed alarms
PRE‐IMPLEMENTATION PHASE
Reaction
That’s only 6 alarms per patient per day
Important Lesson: Don’t Underestimate the Complexity of
Alarm Management• Multiple devices
• Technology configuration
• Data storage and access
• Human interaction(s)
• Responsibility and accountability
• Staffing
• Culture
• Architectural Layout
• Etc…
Providers
IT
Biomed Engineering
Bedside Staff
Leadership
Family
Where to Start: Alarm Management Steps
1. Define your problem
2. Understand your alarm system
3. Gather evidence (research or unit experience) for possible areas of change
4. Identify key drivers that influence your alarm system
5. P‐D‐S‐A
Step 1: Defining the Problem

The Alarming Challenge! Staffing Single Room NICUs and Minimizing Alarm Burden
Michelle Nemshak MSN, RNC-NIC, CNS / Rebecca Vartanian MD
October 3, 2015 5
Defining the Problem Our Approach
Data!
– 10% of babies account for ~65‐75% of alarms
– Individual alarm counts range from 0400+
400 alarms per day
24 hours per day
1 alarm every 3.5 minutes
UCL
LCL
0
20000
40000
60000
80000
100000
120000
140000
160000
180000
Dec
Jan
Feb
Ma
r
Apr
Ma
y
Jun
Jul
Aug
Sep Oct
Nov
Dec
Jan
Feb
Ma
r
Apr
Ma
y
Jun
Tot
al S
pO
2 A
larm
s
2 2 2 2
PRE‐IMPLEMENTATION PHASE
Alarm Management Steps
1. Define your problem
2. Understand your alarm system
3. Gather evidence (research or unit experience) for possible areas of change
4. Develop a driver diagram to align concepts of change with your aim
5. P‐D‐S‐A
Step 2: Understand Your System
Simple SystemStep 1: Prepare
your tools
Response
Step 2: Draw your key system components
Simple System
How does that work?
How is the alarm set? How is it triggered
Step 3: Take it to the next level
Response

The Alarming Challenge! Staffing Single Room NICUs and Minimizing Alarm Burden
Michelle Nemshak MSN, RNC-NIC, CNS / Rebecca Vartanian MD
October 3, 2015 6
Exercise
• Exercise
– Diagram your alarm system
– Discuss with your team:
• What components do you need to know more about?
• Who else should be a part of your team?
• What are the opportunities for change?
“A bad system will beat a good person every time” ‐W. Edwards Deming
Brandon NICU System
Alarm Management Steps
1. Define your problem
2. Understand your alarm system
3. Gather evidence (research or unit experience) for possible areas of change
4. Develop a driver diagram to align concepts of change with your aim
5. P‐D‐S‐A
Step 3: Evidence
Now that you understand your alarm system components, review the evidence about what can be modified:
• Staffing
• Technology
• Provider Response
• Appropriate settings
NACNS Alarm Fatigue Task Force
Seek More Information
• Providers– How do you respond? What are your barriers?
• Biomedical Engineering (Clinical Engineering)– How does this work? Are there delays? What are the modifiable settings?
• Information Technologists– Where does the data go and how do I get it?
• Parents– What do you need to know?
Walk the Walk
• Identify your top “alarmers”– They are not all the same
• Observe work flow for areas to improve– Human response to alarms
– Waste
– Stress
– Potential harm
• Talk with families‐‐perceptions and worries
The Alarming Challenge! Staffing Single Room NICUs and Minimizing Alarm Burden
Michelle Nemshak MSN, RNC-NIC, CNS / Rebecca Vartanian MD
October 3, 2015 7
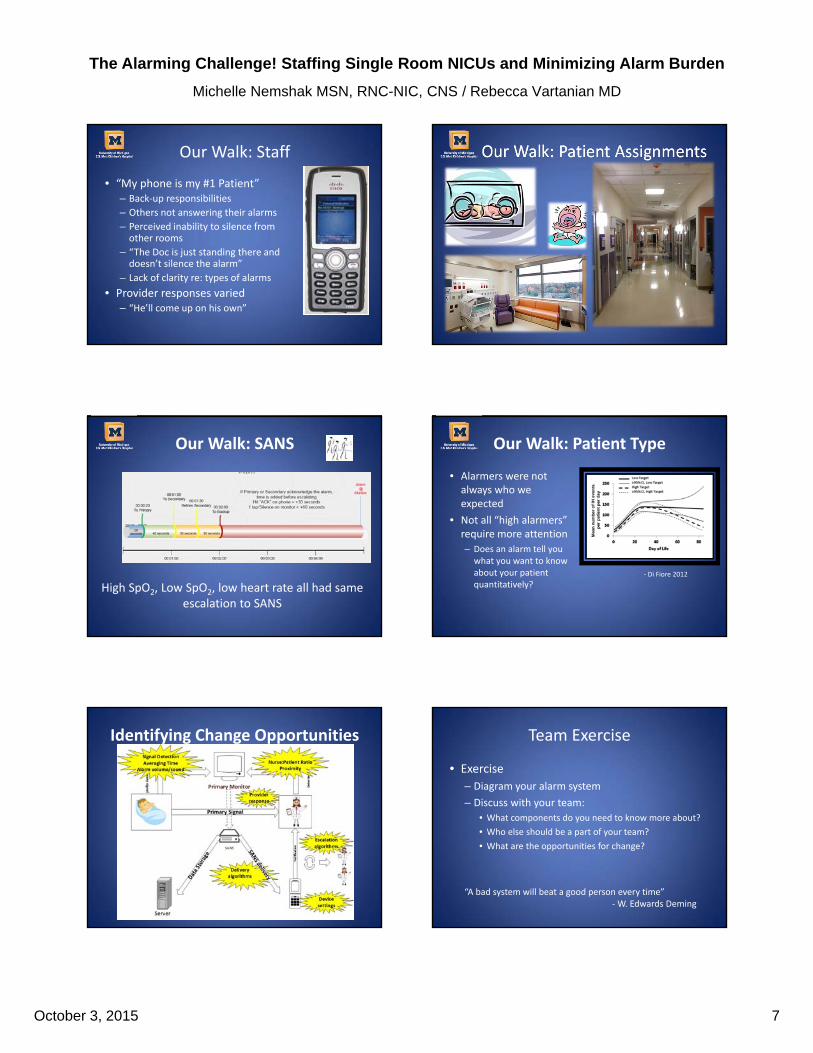
Our Walk: Staff
• “My phone is my #1 Patient”– Back‐up responsibilities
– Others not answering their alarms
– Perceived inability to silence from other rooms
– “The Doc is just standing there and doesn’t silence the alarm”
– Lack of clarity re: types of alarms
• Provider responses varied– “He’ll come up on his own”
Our Walk: Patient Assignments
Our Walk: SANS
High SpO2, Low SpO2, low heart rate all had same escalation to SANS
Our Walk: Patient Type
• Alarmers were not always who we expected
• Not all “high alarmers” require more attention
– Does an alarm tell you what you want to know about your patient quantitatively?
‐ Di Fiore 2012
Identifying Change Opportunities Team Exercise
• Exercise
– Diagram your alarm system
– Discuss with your team:
• What components do you need to know more about?
• Who else should be a part of your team?
• What are the opportunities for change?
“A bad system will beat a good person every time” ‐W. Edwards Deming
The Alarming Challenge! Staffing Single Room NICUs and Minimizing Alarm Burden
Michelle Nemshak MSN, RNC-NIC, CNS / Rebecca Vartanian MD
October 3, 2015 8
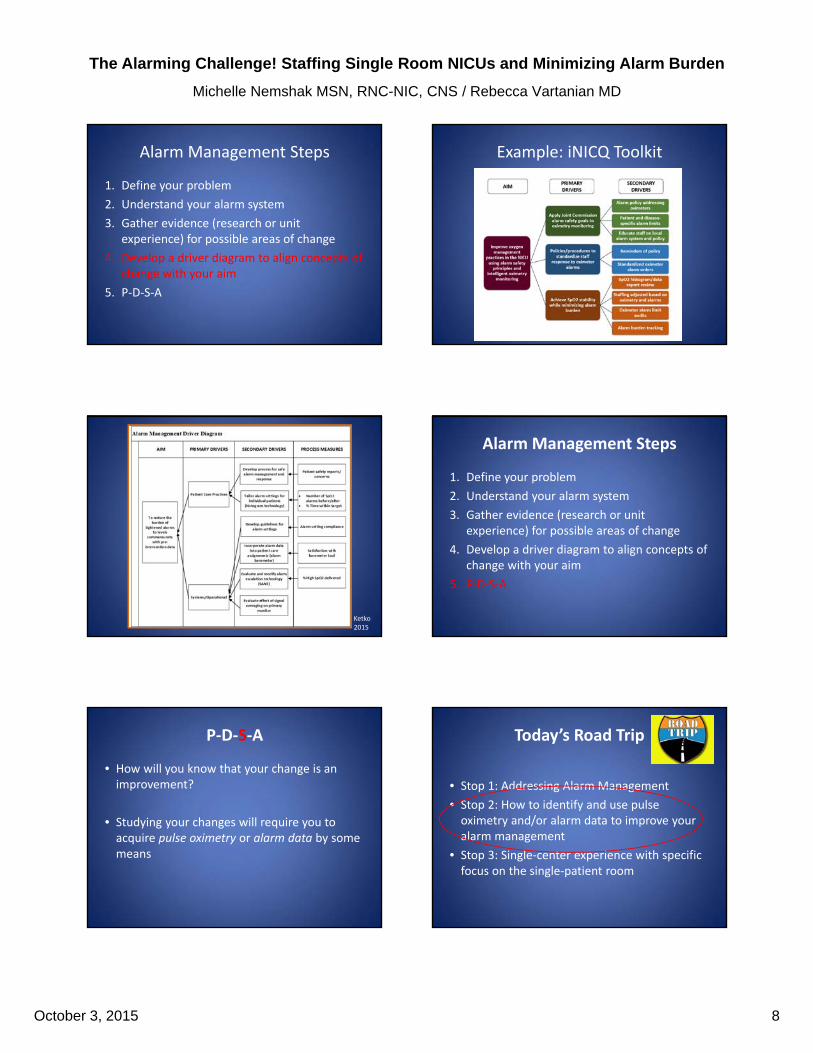
Alarm Management Steps
1. Define your problem
2. Understand your alarm system
3. Gather evidence (research or unit experience) for possible areas of change
4. Develop a driver diagram to align concepts of change with your aim
5. P‐D‐S‐A
Example: iNICQ Toolkit
Driver Diagram
Ketko 2015
Alarm Management Steps
1. Define your problem
2. Understand your alarm system
3. Gather evidence (research or unit experience) for possible areas of change
4. Develop a driver diagram to align concepts of change with your aim
5. P‐D‐S‐A
P‐D‐S‐A
• How will you know that your change is an improvement?
• Studying your changes will require you to acquire pulse oximetry or alarm data by some means
Today’s Road Trip
• Stop 1: Addressing Alarm Management
• Stop 2: How to identify and use pulse oximetry and/or alarm data to improve your alarm management
• Stop 3: Single‐center experience with specific focus on the single‐patient room

The Alarming Challenge! Staffing Single Room NICUs and Minimizing Alarm Burden
Michelle Nemshak MSN, RNC-NIC, CNS / Rebecca Vartanian MD
October 3, 2015 9
How to obtain and use pulse oximetry/alarm data
Steps
1. Identify potential data opportunities in your system
2. Explore the accessibility and ease of data extraction for given data opportunities
3. Prioritize data (biggest bang for the buck)
4. PDSA
Identifying Data Opportunities
Primary Monitor
Detection
ServerPrim
ary sign
al
SANS
Notification
What data can I pull from the
monitor?
How is this data stored? How do I access it?
What data do providers have?
Where does this signal go?
Is there data here?
How to obtain and use pulse oximetry/alarm data
Steps
1. Identify potential data opportunities in your system
2. Explore the accessibility and ease of data extraction for given data opportunities
3. Prioritize data (biggest bang for the buck)
4. PDSA
“Easiest” = Electronic Data
MiddlewareInput Output
Input
Input
Server
“Automated” Data
• To become fully automated, the information must still be retrieved and packaged for clinicians
• Information technologists/Clinical Engineering must:
– Incorporate data from separate systems
– Query servers and manipulate data
– Develop meaningful reports
Data Factors
• Data must have clinical value
• Data may still need interpretation
• Data may need context– How many alarms is too
many?
– How much time outside range is too much?
• Individuals may provide different data based on their own thresholds

The Alarming Challenge! Staffing Single Room NICUs and Minimizing Alarm Burden
Michelle Nemshak MSN, RNC-NIC, CNS / Rebecca Vartanian MD
October 3, 2015 10
What if we don’t have capability?
Look at Your Data Opportunities
Walk the walk:
• Quantitative:
– Bedside monitor
– Other? Audits, hand clickers, etc
• Qualitative:
– Staff
– Families
Bedside Monitor
• Most bedside monitors capture a certain number of alarms– Estimate of alarms/day from captured alarms
• 100 alarms in 24 hours
• 100 alarms in 6 hours
– SpO2 trends
• Incorporated histogram technology– Use baseline percentage outside alarm settings
– Time per day in alarm state or non‐target state
Qualitative Data
• It may not be 100% accurate, but people can provide you data
– Charge nurse could query staff
– Nurse driven reporting (e.g. notify charge RN if alarms > X)
– What could parents provide?
How to obtain and use pulse oximetry/alarm data
Steps
1. Identify potential data opportunities in your system
2. Explore the accessibility and ease of data extraction for given data opportunities
3. Prioritize data (biggest bang for the buck)
4. PDSA
Prioritize Data & PDSA
• Newer technology can provide volumes of data– Can be too much– Align what you want with processes– Look inside your institution at what other units have done
• If you will be relying on audits or other non‐automated reports:– Use your people wisely– Start with one measure and evaluate usefulness and ease of obtaining
• Try it (PDSA) and see what works!

The Alarming Challenge! Staffing Single Room NICUs and Minimizing Alarm Burden
Michelle Nemshak MSN, RNC-NIC, CNS / Rebecca Vartanian MD
October 3, 2015 11
Today’s Road Trip
• Stop 1: Addressing Alarm Management
• Stop 2: How to identify and use pulse oximetry and/or alarm data to improve your alarm management
• Stop 3: Single‐center experience with specific focus on the single‐patient room
Applying Data: Patient Care Assignments
Bringing it all TogetherUsing data to optimize patient care assignments
Patient care assignments
Staffing Optimizing Care at the Bedside
Data
Where is it? How do I use it?
Assignments
“A focus on staffing ‘numbers’ to the exclusion of other factors is unlikely to improve patient safety and may even be detrimental to it. . . Beyond the basic numbers of personnel present on units and their qualifications, the critical elements of experience and expertise of nurses in caring for particular populations and of team stability are surely important”
Source: The Joint Commission Journal on Quality and Patient Safety, Volume 33, Supplement 1, November 2007, pp. 30‐44(15)
Nursing Workload
• Nurses manage work at various levels– Unit– Job– Patient– Situational
• Evidence indicates nursing workload has an affect on nurse‐sensitive conditions (infection, pressure ulcer, pain, etc.)
• Influence on self– Stress, burnout– Work arounds– Errors Carayon & Gurses, (2008)
Nursing Care is Complex
• Competing tasks
• Physical demands
• Mental demands
– Family, patient acuity
• Trade‐off decisions
– Decisions made between different but interacting or conflicting goals
• Interruptions

The Alarming Challenge! Staffing Single Room NICUs and Minimizing Alarm Burden
Michelle Nemshak MSN, RNC-NIC, CNS / Rebecca Vartanian MD
October 3, 2015 12
Staffing Decisions
Nurse‐Patient Assignment
HPPD
Barometer
Geography
Acuity
Resources
“A focus on staffing numbers to the exclusion of other factors is unlikely
to improve patient safety …”
Making the Data Useful
“…if you have over 400 alarms two days in a row, something’s not right…action is needed”
Real Life Barometer Use• Charge RN’s emailed alarm barometer daily– Used to guide nursing assignments
– Goal: avoidance of two “Red Dots” together
– Discussed in shift huddle
• Daily Bed Management Meeting– Multidisciplinary group– Alarm barometer has permanent spot
Real Life Barometer Use
• Strengths– Actual versus estimated/perceived
– Aids in all staff knowing the “pain”
– Aids providers
• Limitations– Barometer is based on past 24 hours
– Does not capture if monitor is off or paused
Very
helpfu
l
Helpfu
l
Somew
hat hel
pful
Mak
es n
o diff
eren
ce0
10
20
30
40
50
Charge RN Responses Regarding Identifying Frequent Alarmers for RN Assignments
How helpful is the alarm barometer in directing RN assignments?
Pe
rce
nta
ge
of C
ha
rge
RN
s (n
=1
7)
Exercise
Take a few minutes to discuss how patient care assignments are determined in your unit. Map out the process that is used.
Using Data to Optimize Patient Care

The Alarming Challenge! Staffing Single Room NICUs and Minimizing Alarm Burden
Michelle Nemshak MSN, RNC-NIC, CNS / Rebecca Vartanian MD
October 3, 2015 13
Breaking it Down
Using data to optimize patient care assignments
Patient care assignments
Staffing Optimizing Care at the Bedside
Data
Where is it?How do I use it?
In Search of A New Tool
ALARM management
ALARM management
OXYGEN management
OXYGEN management
Histogram Technology Optimizing Care at the Bedside
• Data accessible to care providers level can:
– Decrease alarms
– Increase satisfaction with care provided
– Provide visual representation of patient status
• Histogram technology specifically
– Takes complex data interpretation and makes it easy to see/use
A Bedside RN’s Perspective
• “The trends tell you how you have to respond to adjusting oxygen/support”
• “Helps to find that baby’s ‘sweet spot’ “
• “I use it to help me determine if a baby is ready to wean yet or not”
“Finding this at the start of my shift was so frustrating I had to take a picture of it…this
was not okay”
Overall, We Like It
0%
10%
20%
30%
40%
50%
60%
Alarm frequency has improved I feel that alarm fatigue is beingaddressed
Histogram monitors have helpedwith oxygen targeting
Brandon NICU as a whole hasimproved our oxygen management
Strongly Agree Agree Neither Agree nor Disagree Disagree Strongly Disagree
The Alarming Challenge! Staffing Single Room NICUs and Minimizing Alarm Burden
Michelle Nemshak MSN, RNC-NIC, CNS / Rebecca Vartanian MD
October 3, 2015 14
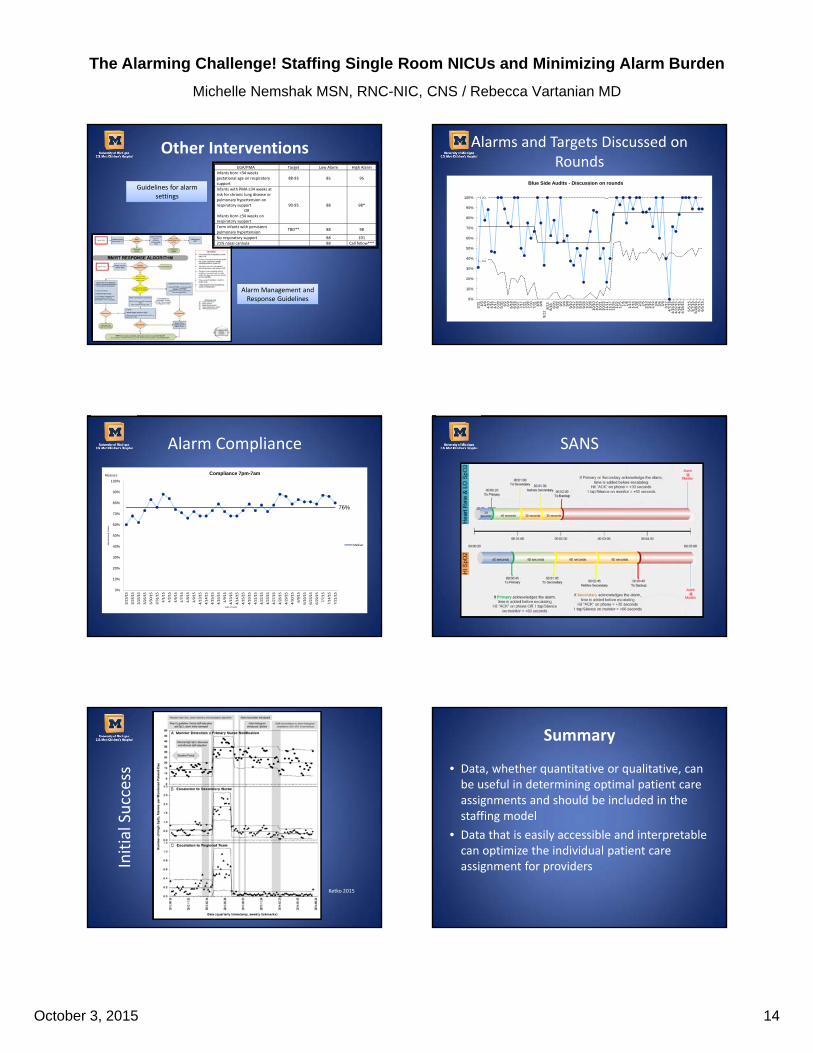
Other Interventions
Alarm Management and Response Guidelines
Guidelines for alarm settings
EGA/PMA Target Low Alarm High Alarm
Infants born <34 weeks gestational age on respiratory support
88‐93 85 95
Infants with PMA ≥34 weeks at risk for chronic lung disease or pulmonary hypertension on respiratory support
OR Infants born ≥34 weeks on respiratory support
90‐95 88 98*
Term infants with persistent pulmonary hypertension
TBD** 88 98
No respiratory support 88 101
21% nasal cannula 88 Call fellow***
EGA/PMA Target Low Alarm High Alarm
Infants born <34 weeks gestational age on respiratory support
88‐93 85 95
Infants with PMA ≥34 weeks at risk for chronic lung disease or pulmonary hypertension on respiratory support
OR Infants born ≥34 weeks on respiratory support
90‐95 88 98*
Term infants with persistent pulmonary hypertension
TBD** 88 98
No respiratory support 88 101
21% nasal cannula 88 Call fellow***
Alarms and Targets Discussed on Rounds
UCL
LCL
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
3/3
14
/34
/94
/10
4/1
64
/17
5/2
85
/30
6/2
6/9
6/1
86
/19
6/2
77
/17
7/2
17
/29
7/3
07
/31
8/5
8/8
8/1
28
/13
8/1
88
/20
8/2
29
/29
/49
/89
/10
9/1
29
/18
9/1
99
/23
10/
21
0/9
10/
10
10/
15
10/
21
10/
23
11/
11
11/
17
11/
24
12/
21
2/5
1/5
1/8
1/1
31
/16
1/2
82
/32
/52
/13
2/1
62
/19
3/4
3/6
3/9
3/1
24
/7/1
5…4
/15
/15
…4
/22
/15
…4
/24
/15
…4
/18
/15
…
5/5
/15…
5/7
/15…
5/2
8/1
5…
6/3
/15…
6/5
/15…
Blue Side Audits - Discussion on rounds
Alarm Compliance
76%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
3/2
3/1
5
3/2
4/1
5
3/2
5/1
5
3/2
6/1
5
3/3
0/1
5
3/3
1/1
5
4/1
/15
4/2
/15
4/6
/15
4/7
/15
4/8
/15
4/9
/15
4/1
3/1
5
4/1
4/1
5
4/1
5/1
5
4/1
6/1
5
4/9
/15
4/1
3/1
5
4/1
4/1
5
4/1
5/1
5
4/1
6/1
5
4/2
1/1
5
4/2
2/1
5
4/2
3/1
5
4/2
7/1
5
4/2
8/1
5
4/2
9/1
5
4/3
0/1
5
6/9
/15
6/1
6/1
5
6/2
3/1
5
6/2
9/1
5
7/7
/15
7/1
4/1
5
7/2
1/1
5
Ala
rms
Mat
ch O
rder
s
Date of Audit
Compliance 7pm-7am
Median
Measure
SANS
Initial Success
Ketko 2015
Summary
• Data, whether quantitative or qualitative, can be useful in determining optimal patient care assignments and should be included in the staffing model
• Data that is easily accessible and interpretable can optimize the individual patient care assignment for providers