

The 5 Domains of Best Pain Care · Objectives • Identify 5 key domains of best practice pain care...
107
The 5 Domains of Best Pain Care Catriona Buist, Psy.D. Oregon Health and Science University OHSU Assistant Professor in Anethesiology and Perioperative Medicine & Psychiatry Chair, Oregon Pain Management Commission Oregon Institute of Occupational Health Sciences, OHSU Pain at Work: How to Prevent, Recognize and Treat Wilsonville, OR May 31, 2018
Transcript of The 5 Domains of Best Pain Care · Objectives • Identify 5 key domains of best practice pain care...

The5DomainsofBestPainCare
CatrionaBuist,Psy.D.OregonHealthandScienceUniversity
OHSUAssistantProfessorinAnethesiology andPerioperativeMedicine&PsychiatryChair,OregonPainManagementCommission
OregonInstituteofOccupationalHealthSciences,OHSUPainatWork:HowtoPrevent,RecognizeandTreat
Wilsonville,ORMay31,2018

Disclosures
• Theauthorhasnothingtodisclose.
2

Objectives
• Identify5keydomainsofbestpracticepaincare
• Understandtheroleofshareddecisionmakinginimprovingtreatmentplanning
• Recognizefeaturesofcomplexpaininapatientpresentation
• IdentifyOregonresourcesforyouandyourpatientsandcolleagues
3

4ProvidenceHealthandServices copyright

Painalwaysresultsfrombodilydamage?
5


Biopsychosocial ModelBecausePainisComplex!
•Anxiety•Depression•PTSD•Catatrophizing•FearofMovement•Traumahistory

WhatAreWeOftenReallyMedicatingWithOpiates???

ToolsWeCouldUseMoreOftenforScreening
• BodyMap• BriefPainInventory(BPI)• PHQ-9(depression)• PHQ-4(depressionandanxiety)• PainAnxietySymptomScale(PASS)• PainCatastrophizingScale(PCS)• PTSDscreenforprimarycare(PC-PTSD-5)• AdverseChildhoodExperiences(traumahistory)• STOP-BANG(sleepapnea)• STarT BackTool(screenforbiopsychosocialissues)• PEG(pain,enjoymentinlife,generalactivity)



Centralsensitization=Awindupofthenervoussystemwhichbecomesregulatedinapersistentstateofhighreactivityandisassociatedwiththedevelopmentandmaintenanceofchronicpain


Our goal is to help people get their life back…
TheirShrinking World…

Redirectconversationsawayfromeliminatingpainandmovetowardsmanagingpainwithafocuson:
- Function- Qualityoflife- Livingameaningfullife

• Physicians• PhysicianAssistants• Nursing• Acupuncture• Psychologists• Physicaltherapists• Occupationaltherapists• Chiropracticphysicians• Naturopathicphysicians• Pharmacists• Dentists
RequiredPainManagementEducation
www.oregonpainmodule.org

PrioritizingCare:KeyDomains
Knowledgeofpain
Nutrition
Activity
Sleep
Mood
• KeyConcepts• Strategies• Resources• Connecting with
yourpatient

Wheretostartwithacomplexpresentation:shareddecisionmakinghelpspatientsengageandenhancesmotivationalinterviewingtowardspositivebehaviorchange.
AvailablebylinkhereandinResourcesectionandOPMCwebsite. Providence Toolkitisavailable
PainToolKit


20
MotivationalInterviewing
Skills
ExpressEmpathy
RollwithResistance
Developdiscrepancy
Supportself-efficacy
Avoidargumentation

21
TraumaInformedCare
Culturalcompetence
Familyempowerment
TraumaCompetenceSafety
Trustworthiness

22

23
PainEducationAsATreatmentInterventionDecreaseinpainrating(VanOosterwijcketal2011,Meeusetal,2010,Ryanetal,2010,Moseley,2002,2003,2004)
Decreaseinfearofre-injury(VanOosterwijcketal2011,Moseley,2002,2003)
Decreaseinpaincatastrophizing(Meeus etal,Moseley2004,Louw etal2011,ArchPhys MedReh Systematicreview)
Decreaseinutilizationofservicespostoperatively(Adriaan Louw,PhD,PT,etSPINEVolume39,#18)
Increaseinfunction(VanOosterwijcketal2011,Moseley,2002,2003,,Louw etal2011ArchPhys MedReh Systematicreview)
Increaseinmobility(MoseleyandHodges, Clin JPain. 2004 Louw etalPhysiotherapyJ,2011)
NoraStern,MSPTProvidenceHealthandServices copyright

OregonPainGuidanceMay17,2018 24

OregonPainGuidanceMay17,2018 25
https://www.youtube.com/watch?v=MqoS7RUrUqg

OregonPainGuidanceMay17,2018 26

OregonPainGuidanceMay17,2018 27

OregonPainGuidanceMay17,2018 28

OregonPainGuidanceMay17,2018 29NEVESTHATFIRETOGETHERWIRETOGETHER

30
ThreatValue
MorePain LessPain
Painresponsechangesbasedonthreatvalue

31
Clicktoaddtext
ProvidenceHealthandServicescopyright

Negativethoughtsaboutpaincanleadtomaladaptivecopingandincreasedsufferinganddisability
Thought:“IhaveDDD.”“Mybackiscrumbling”
Emotion:fear
Behavior:seekadditionalmedicaltreatment
Idea:changewordingfrom“DDD”to“normalagerelatedchanges.”

KnowledgeofPain:Strategies
Changelanguagetodecreaseunintentionalthreat
- "Sorebutsafe"- "Paindoesnotequalharm"- "Thereisalotthatyoucandotochangeyourpain"
Teachaboutpainincludingpainprocessingandneuroplasticity/reversibilityUsingwrittenmaterialandvideosPainknowledgeassessmenttools: click
here,orseeaddendumorOPMCwebsite

34

35
Translations:English,Spanish,Russian,Cantonese,Arabic,Somali,Vietnamese

KeyDomains:Sleep
Knowledgeofpain
Nutrition
Activity
Sleep
Mood
KEYDOMAINS

37

38

FromCBT-i:- Getoutofbedifcan’tsleep- Bedforsleepandpartnertime- Sleeprestrictiontobuildupsleeppressure- Scheduleworrytime- Createtimetounwindbeforesleep
Connectingwithpatient
40



43

44

45

AdaptedfromWenzel,Brown,Karlin 2011Ex.Ifbackpainisexperiencedstandingupfromachairapersonmayfeeldiscouragedandfrustrated(emotion)Andthink,“ifItrytodoanythingtodayI’mgoingtohurtmore(thought)whichmayleadtostayingintheirreclinerandavoidingmovingfortherestoftheday(behavior)
CBTforChronicPainTherapistManualfromVA

Anxiety&PTSD Thought:“Ifeeloverwhelmed.”“Ifeeloutofcontrol”“nobodyunderstandsorbelievesme.”
Emotion:fear,anxiety
Behavior:shutdown

Catastrophizing =magnifyingthenegativeandanticipatingtheworsecasescenarioThought:“mypainwillneverstop”or“nothingcanbedonetoimprovemypain.”“IfthispaincontinuesIwillendupinawheelchairlikemymother”
Emotion:feelhelplessandoverwhelmed,anxiety
Behavior:stopallactivity

Depressionornegativeaffect
Thought:“Ican’tdoanythingthatIenjoy”“LasttimeIwenttotheparkwithmykidsIhadaflareup”“IfeelguiltyIcan’ttakecareofmykids,spouse,contributetothefamilylikeIwantto.”
Emotion:depression,sadness
Behavior:withdrawalfromactivity

Lossofselfandidentity Thought:“I’vealwaysworkedsohardtobethebest______.WhoamInow?”“Ihavelostmyindependence.”
Emotion:shame,sadness,grief
Behavior:stopactivity,socializing,gettingdressed,doingthingsenjoydoing

Blackandwhitethinking
Thought:“IfIcan’t_____likeIdidbefore,Iamnotgoingtodoanythingatall.”
Emotion:anger,sadness
Behavior:stopallfunactivity

ShouldThought:“Ishould beabletodanceallnightlong,gotothemallalldaywithmyfriends,mowthelawn,fishwithmybuddiesprovideformyfamilylikeIuseto.”
Emotion:shame,guilt,sadness
Behavior:retreatintoself.Stopsocializingandgoingout

WhatHappensWhenStressContinuesPainbecomesthelionfollowingyouaround…
- Increasedpain- Depression- Moodswings- Celldeathinthe
hippocampus- Memorychanges- Poortissuehealing- Weightgain- Alteredimmunity
(FromExplainPain,2003)

Quietingstressresponsequietspain
54
PainStress
Response
QuietingStressResponse
Pain
Sleep
Anti-InflammatoryChemicals
ReleaseInflammatoryChemicals
Copyright(C)2016ProvidenceHealth&Services
Relatedproblems:• Poorsleep• Poordigestion• Healingdifficulties• Painandachinessallover

PhysiologicalQuietingVideo
Copyright(C)2016ProvidenceHealth&Services 55

Roleofthefamily&others?
Mayrequirehelpingthemunderstandpain
Settingboundaries
Gettingridoftoxicrelationships
Improvingcommunicationskills

“People don’t hurt if they
have something better to do.”
W. Fordyce, Ph.D
“Lowering yourstressresponsetopainwillreduceyourpain.Hereishow:
Thesamepartsofoursystemthatworkhardwhenwefeelstressalsoworkhardwhenwefeelpain.
That’sbecausebothfeelingsareparofourEmergencyResponseSystem.Whenourbrainsensedanger,itactivatesthissystem.Stressdoesn’tdirectlycarepain.Butstresscanmakepainworseanditcanmakepainlastlonger.”
58

59
Relaxationvideos:Bodyscan,progressivemusclerelaxationandbreathingEnglish,SpanishandRussian

60

HurtvsHarm&FearofMovement(kinesiophobia)
Thought:“painmeansIamhurtingmyself.”Emotion:fear(ofpain)Behavior:stopallactivity,guard,protect,holdbreath

62

OregonPainGuidanceMay17,2018 63

OregonPainGuidanceMay17,2018 64https://www.youtube.com/watch?v=hjenuiXDUZg

The Activity-Rest Cycle in Chronic Pain (Gil, Ross, & Keefe, 1988) in Psychological Approaches to Pain Management: A Practitioner’s Handbook. Edited by Robert J. Gatchel and Dennis C. Turk (1996)

ExpectFlareUpsandteachflareupmanagementstrategiestobuildself-efficacyandincreasesenseofcontrol

67

68
KnowledgeofPainandActivity:Resources
Activityvideosegmenttobeembeddedsoon

69

70

71

72

73

PainCareisEveryone’sJob
74
75
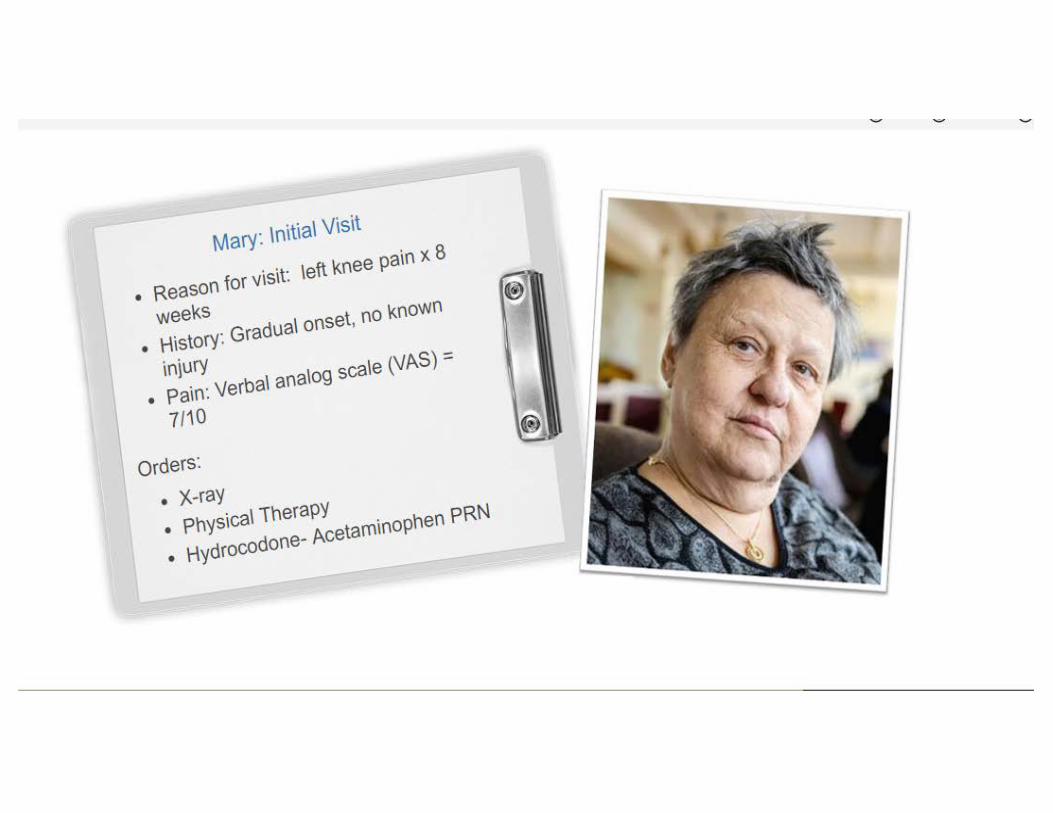
AddChristinahistoryhereandsolicitconversation• Identifyareasoffocus

76
• Firstslide:herfirstpresentation

77

78

79

80

81





88

Legislation established a Pain Task Force in 1997; followed by The Pain Management Program and Coordinator position in 1999; And, in 2001 the Pain Management Commission.
• 17 voting members, 2 legislative members
Oregon Pain Management Commission:
• MDs• PhysicianAssistant• Nurses• NursePractitioner• NaturopathicPhysician• ChiropracticPhysician• Acupuncturist• Pharmacist• Psychologist• Dentist
• AddictionCounseling• PhysicalTherapist• OccupationalTherapist• HealthCareConsumers• PatientAdvocates• PublicRepresentative• LegislativeMembers
-Senate-House

90Providenceoregon.org/paintoolkit
Newresourcesforclinicians

#PainMed2018 AAPM34thAnnualMeeting|April26-29,2018 91

LorimerMosely– ChronicPainTametheBeast5’utube
https://www.youtube.com/watch?v=XwBYkw-iZdQ

Understandingpainandwhattodoaboutitinlessthan5minutes- JointPainEducationProjectvideofromtheDepartmentofDefenseandVeteransHealthAdministrationtolearnmoreaboutchronicpainmanagement.
https://www.youtube.com/watch?v=cLWntMDgFcs
“UnderstandingPainandWhattodoAboutItinlessthan5Minutes”utube

ClassesonLivingWellwithChronicPainwww.healthoregon.org/livingwell
This2015bookisdesignedtohelpmanagepainsopeoplewithchronicpaincangetonwithlivingasatisfying,fulfillinglife,andincludestheMovingEasyProgram CD.ThisbookandCDarethecompanionresourcestotheChronicPainSelf-Managementworkshop.

SleepResources
1. Maintainaregularbedandwaketimeschedule,includingweekends2. Establisharegular,relaxingbedtimeroutine3. Workoutregularly(stopexercise3hoursbeforebed)4. Noelectronicsinbedroom- TV,phones5. NoexposuretoTVorcomputers2hourspriortobedtime6. Usebedroomonlyforsleepandpartnertime7. Finisheatingatleast2-3hoursbeforebed8. Refrainfromtakingnaps(notmorethan20’)9. Avoidcaffeineafternoon10. Avoidalcoholclosetobedtime
Resource:CBT-i Coach

HealthySleepResourcesfromKimberlyHutchison,MD,FAASMBooks
1. TheInsomniaAnswer:APersonalizedProgramforIdentifyingandOvercomingtheThreeTypesofInsomnia,byPaulGovinksyandArtSpielman.2. SayGoodnighttoInsomnia,byGreggJacobs.
Apps,Podcasts,orOnlineResources
1. InsightTimer(free)2. Noisli.com(varioussounds)3. SmilingMinds4. SimpleHabit5. RelaxandSleepWellbyGlennHarrold(free)6. Calm7. Headspace8. Sleep withMePodcast9. JeffBridgesSleepingTapes
CBTI
1. ClevelandClinicMindfulnessBasedInsomniaTherapy($40for6weekonlineprogram) http://www.clevelandclinicwellness.com/Programs/Pages/Sleep.aspx#pop2. OHSUIndividualCBTI(AmyKobus,PhD)or OHSUGroupCBTI(TeniDavoudian,PhD)3.SHUTi($149),CBTI-coach(free),NightOwl($10)
AlternativeTherapiesforAdults
1. EssentialOilSprays(lavenderisapopularscent)2. WorryStone(alsoknownaspalmstonesorthumbstones)aresmooth,polishedstoneswithathumb-sizedindentationinthecenter.Theyareusedbyholdingbetweentheindexfingerandthumbandrubbinggentlyforrelaxationoranxietyrelief.3. Acupuncture4. MassageTherapy

• CBTManualforChronicPainhttps://www.va.gov/PAINMANAGEMENT/docs/CBT-CP_Therapist_Manual.pdf
• BeverlyThornhasalowliteracymanualforchronicpain
CognitiveBehavioralTherapy(CBT)Resources

Acceptance & Commitment Therapy (ACT) resourcesSteven Hayes, 1994
https://contextualscience.org/act
https://www.actmindfully.com.au/
PortlandPsychotherapyClinichttp://portlandpsychotherapyclinic.com/resources/acceptance_and_commitment_therapy_exercises_and_audiofiles/
KevinVowelsACTmanualhttps://contextualscience.org/files/CP_Acceptance_Manual_09.2008.pdf

NeuroplasticityResources

MindfulnessandRelaxationResources

MotivationalInterviewingforHealthcareProfessionals-OnlineEducationCollegeofNursingattheUniversityofColoradohttp://www.ucdenver.edu/academics/colleges/nursing/programs-admissions/CE-PD/Pages/Motivational-Interviewing-for-Healthcare-Professionals.aspx
TheEfficacyofMotivationalInterviewinginAdultswithChronicPain:AMeta-AnalysisandSystematicReviewDionAlperstein&LouiseSharpeTheJournalofPain,Vol17,No4(April),2016:pp393-403.“MIsignificantlyincreasedadherencetochronicpaintreatmentintheshortterm…”
MotivationalInterviewingresources(MillerandRollnick,2009)

FreeVideoTrainingonDifficultConversationshttps://www.scopeofpain.com/
• SCOPEofPainisaseriesofcontinuingmedicaleducation/continuingnursingeducationactivitiesdesignedtohelpyousafelyandeffectivelymanagepatientswithchronicpain,whenappropriate,withopioidanalgesics.
• Trainer’stoolkit- 7videos:• Initiatingopioidtherapy,discussingsafetyandbenefit• Assessingandmanagingaberrantopioidtakingbehavior• Discussingdiscontinuationofopioidsduetolackofbenefitandexcessiverisk• Modifyingtreatmentplanofinheritedpatientonhighdoses• Assessingandmanagingillicitdruguseinpatientwithchronicopioidtherapy• AssessingandmanagingPDMPquestionableactivityinestablishedpatientandinanewpatient

ResourcesforUnderstandingtheIssuesRelatedtotheOpioidEpidemic&toHelpPatients
ChasingHeroin(Frontline&PBS)
http://www.pbs.org/wgbh/frontline/film/chasing-heroin/

FreePainCME
www.coperems.org
www.scopeofpain.com
www.pcsso.org www.pcssmat.org

March2016NationalPainStrategy- outlinesactionsforimprovingpaincareinAmerica toreducetheburdenandprevalenceofpainandtoimprovethetreatmentofpain(CourtesyofDr.SeanMacKey)

1 3
InitiativetoAddressOpioidsandDrugswithAddictive/AbusePotential
IMPROVEPATIENTCAREREDUCERISKSTOPATIENTSBY
MAKINGPHYSICALANDBEHAVIORALHEALTH
TREATMENTS SAFER,addressinghistoryoftrauma,and
providingnon-pharmacologicaltreatmentoptions
REDUCE PATIENTHARMSREDUCEHARMSANDSUPPORTRECOVERYFROMSUBSTANCEUSEDISORDERSbymakingSubstanceUseDisorder
treatmentmoreaccessibleandaffordable,andaddressingrecoveryasachronicdisease
IMPLEMENT POPULATION-BASED STRATEGIES
ProtectthecommunitybyREDUCINGTHENUMBEROF
PILLSINCIRCULATIONthroughimplementationofsafeprescribing,storage,and
disposalpractices
2
Aim:Reducedeaths,overdoses,andharmstoOregoniansfromopioidsandotherdrugswithaddictive/abusepotentialthroughpublichealthandhealthsystemsinterventions
EDUCATIONANDOUTREACH
DATATOINFORM,MONITOR,ANDEVALUATE

EvidenceBasedReportsSupportingMultidisciplinaryTreatmentforChronicPain
3/16CDC urgedhealthcareproviderstoturntonon-drugandnon-opioidpainkillersbeforeconsideringopioids
11/16AgencyforHealthcareResearchandQuality- 800pagereviewonchronicLBP-nonpharmacologicaltherapiesappeartobeeffectiveforimprovingpainorfunctionincludingexercise,yoga,taichi,psychologicaltherapies,multidisciplinaryrehabilitation,acupuncture,spinalmanipulation…
2/17AmericanCollegeofPhysicians adviseddoctorsandpatientstotrynon-drugtherapiessuchasexercise,acupuncture,taichi,yoga,chiropractorandavoidprescriptiondrugsorsurgicaloptionswhenpossible.Ifnon-drugtherapiesfail,recommendnonsteroidalanti-inflammatorydrugsasfirstlinetherapy,ortramadolorduloxetineassecondlinetherapy.
11/17InstituteforClinicalandEconomicReviewFinalReport– recommendsenhancedcoverageofcertainnon-drugmanagementoptionsforlowbackpainincludingacupuncture,CBT,MBSR,andyoga


















