Thank you Honor and Privilege Speaker Everybody has a vision for something. You have a vision for...
137
-
Upload
philippa-dickerson -
Category
Documents
-
view
213 -
download
0
Transcript of Thank you Honor and Privilege Speaker Everybody has a vision for something. You have a vision for...



Thank you
Honor and Privilege
Speaker



Everybody has a vision for something.
You have a vision for something.

I also have a vision on medical education.
Dr. Rodolfo Dimayuga has a vision on medical education.

Vision
for a
More Effective Medical Curriculum
in the Philippines
Rodolfo C. Dimayuga, MD
Reynaldo O. Joson, MD, MHPEd, MHA, MS Surg

Lecture Outline
• What is a vision?• What is my vision on the medical
curriculum in the Philippines?• What led to my vision?• What have I done to attain my vision?• What obstacles have I encountered in
trying to attain my vision?• What remains to be done to attain my
vision on medical education?

What is a vision?

DREAM
= GOOD DREAM
= A DREAM FOR THE BETTERMENT OF SOMETHING

What is my vision on the medical curriculum
in the Philippines?

Vision
for a
More Effective Medical Curriculum
in the Philippines
Reynaldo O. Joson, MD, MHPEd, MHA, MS Surg

What led to my vision on
medical education?

VISION
Two triggers:
1. The experience itself , that is, being exposed to the situation
2. Desiring for something better, that is, after discovering some dissatisfaction with the situation

What brought about my Personal Vision/Aspirations for a More Effective Medical Curriculum in the Philippines?
1st trigger for a vision - the experience itself, that is, being exposed to the situation
medical curriculum in the Philippines

What brought about my Personal Vision/Aspirations for a More Effective Medical Curriculum in the Philippines?
1st trigger - experience and exposure to the medical curriculum in the Philippine
Length of Exposure -
30 YEARS (1970-2000)Trainor/FacultyMedical Schools and Teaching Hospitals
INS AND OUTS / IMPACT OF CURRICULUM IN THE PHILIPPINES

What brought about my Personal Vision/Aspirations for a More Effective Medical Curriculum in the Philippines?
2nd trigger for a vision - desiring for something better after discovering some dissatisfaction with the
situation
3 situations - to take a close look at medical curriculumto target it as a root cause for all the problems we
are having in the medical professiontherefore, to aspire for its change or improvement

What brought about my Personal Vision/Aspirations for a More Effective Medical Curriculum in the Philippines?
2nd trigger for a vision - desiring for something better after discovering some dissatisfaction with the situation
1st situation:
1982 to 1993, as a surgical educator of residents in the Philippine General Hospital, Ospital ng Maynila, Zamboanga City Medical Center, Tondo Medical Center, and other residents throughout the country,

What brought about my Personal Vision/Aspirations for a More Effective Medical Curriculum in the Philippines?
2nd trigger for a vision - desiring for something better after discovering some dissatisfaction with the situation
1982 to 1993, as an educator of surgical residents
I discovered a lot of “ill-habits, attitude and practices” in medical reasoning, decision-making and continuing education whose root could be traced to the earlier part of
residency training and even as far back as the medical school years.

What brought about my Personal Vision/Aspirations for a More Effective Medical Curriculum in the Philippines?
2nd trigger for a vision - desiring for something better after discovering some dissatisfaction with the situation
After more than 10 years of perseverently teaching surgical residents, I got burnt out and decided that I should target root cause, which I considered to be the medical curriculum at the medical school level.

What brought about my Personal Vision/Aspirations for a More Effective Medical Curriculum in the Philippines?
2nd trigger for a vision - desiring for something better after discovering some dissatisfaction with the situation
Thus, in 1994, when I had the opportunity to design the curriculum for a new medical school, I did not hesitate to accept the challenge.

What brought about my Personal Vision/Aspirations for a More Effective Medical Curriculum in the Philippines?
2nd trigger for a vision - desiring for something better after discovering some dissatisfaction with the situation
I helped design the innovative medical curriculum of Zamboanga Medical School Foundation.
This curriculum was later adopted by Southwestern University College of Medicine in 1995 and Bicol Christian College of Medicine, also in the same year.

What brought about my Personal Vision/Aspirations for a More Effective Medical Curriculum in the Philippines?
2nd trigger for a vision - desiring for something better after discovering some dissatisfaction with the situation
2nd situation:
From 1989 to present, as a hospital administrator of Manila Doctors Hospital in my capacity as an assistant medical director and chairperson of quality assurance program,

What brought about my Personal Vision/Aspirations for a More Effective Medical Curriculum in the Philippines?
2nd trigger for a vision - desiring for something better after discovering some dissatisfaction with the situation
I discovered a lot of “ill-habits, attitude and practices”, not to say, incompetences, not only in medical reasoning and decision-making among consultant staff but also in their way of managing a hospital unit or department assigned to them and in their participation in hospital operation.

What brought about my Personal Vision/Aspirations for a More Effective Medical Curriculum in the Philippines?
2nd trigger for a vision - desiring for something better after discovering some dissatisfaction with the situation
Again, I attributed the root cause to be at the medical school years level.

What brought about my Personal Vision/Aspirations for a More Effective Medical Curriculum in the Philippines?
2nd trigger for a vision - desiring for something better after discovering some dissatisfaction with the situation
Concerning the undesirable attitudes, habits, and practices of consultants in hospital management aspect,
I attributed the root cause to be due to the lack, if not absence of management course and training of physician to be co-players, managers and administrators of health institutions.

What brought about my Personal Vision/Aspirations for a More Effective Medical Curriculum in the Philippines?
2nd trigger for a vision - desiring for something better after discovering some dissatisfaction with the situation
There are only a few medical schools in the country that incorporate management course in their curricula.
If only physician-managerial skills can be developed in medical schools, hospitals will be easier to manage.

What brought about my Personal Vision/Aspirations for a More Effective Medical Curriculum in the Philippines?
2nd trigger for a vision - desiring for something better after discovering some dissatisfaction with the situation
3rd situation:
In my 20 years of practice, I have experienced a lot of irrational, ineffective, inefficient, and inhumane practices by my colleagues, which include not only co-physicians and co-specialists, but also co-teachers in the medical academe.

What brought about my Personal Vision/Aspirations for a More Effective Medical Curriculum in the Philippines?
2nd trigger for a vision - desiring for something better after discovering some dissatisfaction with the situation
3rd situation:
I have witnessed a lot of flaws in the diagnostic and treatment processes which would end-up in unnecessary mortality and morbidity, unnecessary expenses in laboratory workups and treatment, unnecessary hospitalizations, unnecessary anxiety on the part of the patients and relatives, etc.

What brought about my Personal Vision/Aspirations for a More Effective Medical Curriculum in the Philippines?
2nd trigger for a vision - desiring for something better after discovering some dissatisfaction with the situation
3rd situation:
Again, I attributed the root cause to be at the medical school level of training.

What brought about my Personal Vision/Aspirations for a More Effective Medical Curriculum in the Philippines?
2nd trigger for a vision - desiring for something better after discovering some dissatisfaction with the
situation
3 situations - to take a close look at medical curriculumto target it as a root cause for all the problems we
are having in the medical professiontherefore, to aspire for its change or improvement

What brought about my Personal Vision/Aspirations for a More Effective Medical Curriculum in the Philippines?
2nd trigger for a vision - desiring for something better after discovering some dissatisfaction with the situation
Areas of Dissatisfaction
1. Present medical schools and their curricula have NO documented direct and significant impact on the health development in the country.

What brought about my Personal Vision/Aspirations for a More Effective Medical Curriculum in the Philippines?
2nd trigger for a vision - desiring for something better after discovering some dissatisfaction with the situation
Areas of Dissatisfaction
2. A lot of things in the present medical curricula are not relevant.
3. Present medical curricula are NOT student-friendly.

1. Present medical schools and their curricula have NO documented direct and significant impact on the health development in the country.
1a. Present medical schools are contented merely with graduates passing the board.
1b. Present medical schools consider that with production of board-certified physicians
and with the latter practicing in the country, they have already contributed to the health
development in the country.

1. Present medical schools and their curricula have NO documented direct and significant impact on the health development in the country.
1c. Present medical schools consider incorporating a community immersion subject a way of
contributing to the health development in the country.
1d. Present medical schools do not work closely with the Department of Health which is the main agency in charge of health development in the country. They should incorporate the health programs of DOH into their curricula.

My vision and aspiration:
Medical schools and their curricula should have documented direct
and significant impact on the health development in the
country.

My vision and aspiration:
They should go beyond producing board-passers, community
immersion, and should work closely with DOH by incorporating the latter programs in their curricula.

In the curriculum which I designed,
1. DOH health programs are incorporated and implemented in the community
immersion.
2. as part of requirements for graduation, students with the help of faculty
should solve (at least attempt) one health problem in their assigned community formally documented through an action research.
With the above 2 strategies, at the end of the day, medical school can say that with its
medical curricula, it has contributed to the health development in the country.

2. A lot of things in the present medical curricula are not relevant.
2a. Students are taught things that are uncommon and rare in the
country with the same emphasis as common medical conditions.
Example: Crohns’s disease, ulcerative colitis, rare hereditary and newborn diseases, etc.

2. A lot of things in the present medical curricula are not relevant.
2b. Students are taught things which are NOT used in clinical practice.
Example: Students are taught traditional medical recording which is NOT done by certified physicians.

2. A lot of things in the present medical curricula are not relevant.
2b. Students are taught things which are NOT used in clinical practice.
Another example:
We often heard medical teachers saying:
“You have to do this while you are still students. Once you are a consultant or an expert like me, you don’t have to do it anymore.”

2. A lot of things in the present medical curricula are not relevant.
2c. Students are NOT taught effective “study methods” of certified
physicians, which is in the form of problem-based learning.
Practically, all certified physicians after graduating from medical schools learn medicine using the problem-based learning method. Yet, this is not being taught to the medical students until recently when slowly a number of schools have adopted PBL as a learning method.

My vision and aspirations:
Medical curricula should be relevant.
In the curriculum I designed, students are taught
1. common things found in the country2. processes and procedures used in
clinical practice 3. problem-based learning method

3. Present medical curricula are NOT student-friendly.
3a. There is NO standardization of “processes”.
3b. There is NO coordination among various disciplines.

3a. There is NO standardization of “processes.”
There are as many philosophies of medical management as there are medical
teachers.
As many approaches in medical management as there are medical
teachers.
As many diagnostic approaches as there are medical teachers.
As many treatment approaches as there are medical teachers.

3a. There is NO standardization of “processes.”
There are as many prescribed study methods for students as there are medical teachers.
There are as many biases that the students will have to contend with as there are medical teachers.

3a. There is NO standardization of “processes.”
The end result of this lack of standardization is that the students are confused andto survive, they just try to please their master-medical teachers from whom they will get their passing grades.

3a. There is NO standardization of “processes.”
Another end result of this lack of standardization is that thestudents expend too much energy and become exhausted
which is UNNECESSARY because there is A way to reduce and prevent it.
In other words, the present medical curricula in the country are NOT student-friendly.

3b. There is NO coordination among various disciplines or specialties.
Each specialist faculty wants the students to learn his/her
discipline.
There are overlaps among disciplines.
Furthermore, there are conflicts among disciplines, the conflicts consisting of different philosophy and approaches.
As I said earlier, there are as many philosophy and approaches as there are medical teachers.

3b. There is NO coordination among various disciplines or specialties.
The end result of this lack of coordination and
integration among various disciplines is again,
CONFUSION and EXHAUSTION on the part of the students.
In other words, NOT STUDENT-FRIENDLY.

My vision and aspirations:
Medical curricula should be student-friendly to be more effective, efficient, and humane.
In the curriculum I designed, there is/are
1. Standardization of management of a patient process
2. Standardization of managerial process 3. Frameworks (being used all
throughout)4. Standardization of learning method –
PBL5. Integration/coordination among
various disciplines

Thus far here in my talk,
I have told you the two triggers that led me to a vision/aspirations for a more effective medical curriculum in the Philippines:
•30-years of exposure to the situation •discovery of dissatisfaction with the present
medical curricula.
I have also partly described to you my vision and what I have done to pursue it.

What have I done to attain my vision
on medical education?

I started formally and systematically pursuing my vision for a more effective medical curriculum in the Philippines
in 1994
when I was given the opportunity.
That opportunity came to me by chance,by serenpidity.

Thank you
Dr. Fortunato (Khryss) Cristobal
Dean
Zamboanga Medical School Foundation, Inc.

To attain my vision on medical education -
1. I designed what I think will be a more effective medical curriculum than the traditional one.
2. I tried to develop it by formulating the frameworks and templates, writing some of the course packs, teaching the faculty, reaching out to the students, monitoring for flaws and improvement and lastly, revising it as necessary so that it will be what I envision it to be.
3. Helped medical schools who want to use my medical curriculum model.

RJoson’s
Medical Curriculum Model

RJoson’sMedical Curriculum Model
A comprehensivevertically integrated curriculum

community-oriented-based learningcompetency-based learningproblem-based learningdistance learning
vertically individual health management learning
community health management learningintegrated
biophysical issues learningcurriculum psychosocial issues learning
bioethical issues learningmedicolegal issues learningresearch issues learning
basic medical sciencesclinical medical sciences

RJoson’sMedical Curriculum Model
The Blueprint
Places of learning Course content
Teaching-learning strategiesEvaluation methods

RJoson’s Medical Curriculum ModelThe Blueprint
Places of learning
Features:• Community-based learning design of the
curriculum• Step-ladder design being advocated by DOH• Incorporation of distance education or
learning in the community

RJoson’s Medical Curriculum Model
Places of learning
YrSem
I1st
I2nd
II1st
II2nd
III1st
III2nd
IV1st
IV2nd
Mo.
1 CM CM CM CM CM H H AC2 CM CM CM CM CM H EL AC3 CM CM CM CM CM H EL AC4 AC AC AC AC AC AC AC AC5 AC AC6 AC AC

RJoson’s Medical Curriculum ModelThe Blueprint
Course Content
Features:
1. The modular design – MD-competency-based and problem-based courses
2. The use of DOH-priority health problems early on the curriculum, in the 2nd semester of Year Level I – Trauma, Infection-Infestation, and Maternal and Child-Health Problems (this goes for relevance and indigeniously Filipino model)

RJoson’s Medical Curriculum ModelThe Blueprint
Course Content
Features:
3. The use of an initial overview, followed by frameworks and concepts, progressing to foundation, development, and ending in mastery.
3.1 The design of Orientation and Introduction3.2 The overall overview-framework-foundation-
development-mastery design

RJoson’s Medical Curriculum Model
Yr Sem Phase Courses CommunityImmersion
I 1st Orientation /Introduction
Orientation to Schooland Community;Physician-to-bePlanning;Management inMedicine; How toStudy (PBL)

Orientation and IntroductionGeneral Objectives
• Orient
• Motivate
• Give an overview
• Build a framework
• Lay down foundation to facilitate learning to become a physician

Orientation and IntroductionConcept Map
Orientation Training
SchoolFramework Foundation
How to Study
CompetenciesExpected
Development*
Mastery*

RJoson’s Medical Curriculum Model
Yr Sem Phase Courses CommunityImmersion
I 1st Competenciesof an MD
Health Management Ind’l Health Mgt Family Health Mgt Com’ty Health MgtMgt of a Patient Screening for health problem Solution of a health problemMD-Teacher-learnerMD-ResearcherMD-AdministratorEmergency Medicine

RJoson’s Medical Curriculum Model
Yr Sem Phase Courses CommunityImmersion
I 1st CommunityHealthManagementI
CommunityDiagnosis4-yearComprensiveCommunityHealth Plan

RJoson’s Medical Curriculum Model
Yr Sem Phase Courses CommunityImmersion
I 2nd DOH PriorityHealthProblems
TraumaMaternal and Child HealthCancer

RJoson’s Medical Curriculum Model
Yr Sem Phase Courses Community Immersion
I 2nd CommunityHealthManagementII
Action Research Proposalfor an Identified HealthProblem in the Communityusing Primary Health CareApproach

RJoson’s Medical Curriculum Model
Yr Sem Phase Courses CommunityImmersion
II 1st –2nd
Organ/SystemProblems
Cardiovascular;Pulmonary;Abdominal; Nervous;Mind; EENT

RJoson’s Medical Curriculum Model
Yr Sem Phase Courses CommunityImmersion
II 1st –2nd
CommunityHealthManagementIII and IV
Implementationof ActionResearchProposalAnd CommunityHealth Plan

RJoson’s Medical Curriculum Model
Yr Sem Phase Courses CommunityImmersion
III 1st Organ/SystemProblems
Renal; Skin and SoftTissues; Bone andJoint; Hematologic /Immunologic;Sexuality

RJoson’s Medical Curriculum Model
Yr Sem Phase Courses CommunityImmersion
III 1st CommunityHealthManagementV
Implementationof ActionResearchProposalAnd CommunityHealth Plan

RJoson’s Medical Curriculum Model
Yr Sem Phase Courses CommunityImmersion
III 2nd HospitalImmersion
Pediatrics; InternalMedicine; Surgery;Obstetrics-Gynecology

RJoson’s Medical Curriculum Model
Yr Sem Phase Courses CommunityImmersion
III 2nd CommunityHealthManagementVI
Implementationof ActionResearchProposalAnd CommunityHealth Plan

RJoson’s Medical Curriculum Model
Yr Sem Phase Courses CommunityImmersion
IV 1st –2nd
Elective Hospital rotation;specialty rotation;others

RJoson’s Medical Curriculum Model
Yr Sem Phase Courses CommunityImmersion
IV 1st -2nd
CommunityHealthManagementVII
Implementationof ActionResearchProposalAnd CommunityHealth Plan

RJoson’s Medical Curriculum ModelThe Blueprint
Course Content
Features:
1. The modular design – MD-competency-based and problem-based courses
2. The use of DOH-priority health problems early on the curriculum, in the 2nd semester of Year Level I – Trauma, Infection-Infestation, and Maternal and Child-Health Problems (this goes for relevance and indigeniously Filipino model)

RJoson’s Medical Curriculum ModelThe Blueprint
Course Content
Features:
3. The use of an initial overview, followed by frameworks and concepts, progressing to foundation, development, and ending in mastery.
3.1 The design of Orientation and Introduction3.2 The overall overview-framework-foundation-
development-mastery design

A COMPETENT PHYSICIAN IN THE COMMUNITYEffective, Efficient, Humane
Orientation and Introduction
Management
How to Study
Health Management
Concept of Health and Disease
Community Health Mgt
Individual Health Mgt
Family Health Mgt
Other MD CompetenciesMD-Researcher
MD-Teacher-LearnerMD-Manager
OthersManagementof a Patient
Emergency Medicine

RJoson’s Medical Curriculum ModelThe Blueprint
Learning Strategies/Approaches/Activities/Resources
ACTIVE LEARNING ACTIVITIES
SELF-DIRECTED LEARNING ACTIVITIES
PROBLEM-BASED LEARNING METHOD

RJoson’s Medical Curriculum ModelThe Blueprint
Learning Strategies/Approaches/Activities/Resources
•Community-based learning
•Competency-based learning
•Problem-based learning

RJoson’s Medical Curriculum ModelThe Blueprint
Learning Strategies/Approaches/Activities/Resources
•Group discussions
•Lecturettes
•Independent studies

RJoson’s Medical Curriculum ModelThe Blueprint
Learning Strategies/Approaches/Activities/Resources
•Demonstration and return demonstration
•Simulated learning
•Actual/direct patient contact/learning
•Actual/direct community contact/learning

RJoson’s Medical Curriculum ModelThe Blueprint
Learning Strategies/Approaches/Activities/Resources
•Tasks/projects
•Hand-outs
•Self-instructional programs

RJoson’s Medical Curriculum ModelThe Blueprint
Learning Strategies/Approaches/Activities/Resources
ACTIVE LEARNING ACTIVITIES
SELF-DIRECTED LEARNING ACTIVITIES
PROBLEM-BASED LEARNING METHOD

RJoson’s Medical Curriculum ModelThe Blueprint
Assessment Methods
•Practical examinations
•Oral Examinations
•Written Examinations
•Outcome of tasks/projects

RJoson’s Medical Curriculum ModelThe Blueprint
Evaluation Tools - Expected Terminal Competencies
Specific Requirements for Graduation
•Completion of and satisfactory verbal and written presentation of an action-research project on a selected community health problem
(Evaluation tool for the community health problem solver competency that is expected of the graduates)

RJoson’s Medical Curriculum ModelThe Blueprint
Evaluation Parameters - Expected Terminal Competencies
Specific Requirements for Graduation
•Completion of and satisfactory verbal and written Case Presentation and Management of at least 27 different clinical cases corresponding to the problem-courses
(Evaluation tool for the physician-clinician competency that is expected of the graduates)

RJoson’s Medical Curriculum ModelThe Blueprint
Evaluation Tools - Expected Terminal Competencies
Specific Requirements for Graduation
•Passing of all the problem-courses
•Passing of a year-end comprehensive examination
(Evaluation tools for the physician-clinician and potential Philippine Medical Board Examination passer competences expected of the graduates)

RJoson’sMedical Curriculum Model
Use of Frameworks and Templates

RJoson’sMedical Curriculum Model
Use of Frameworks and Templates
To make the curriculum
not only faculty- and student-friendly but also
to promote efficiency and mastery of the processes used in the practice and
teaching of medicine

RJoson’sMedical Curriculum Model
Samples of Frameworks and Templates
• Management Process • Management of a Patient Process • Problem-based Learning Format • Templates for discussion of biological foundation
and basis on clinical management• Templates for Course Pack Writing and
Development • Action-research format for the community health
problem solving project• Templates for end-of-course symposia

Management Process
• Situational analysis - problem-identification
• Planning
• Implementation
• Evaluation
• Improvement

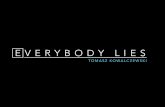
Management of a Patient Process
Patient
Interview (Symptoms)
MD
GOALHealth Problem Resolution
Physical Exam (Signs)
Clinical Diagnostic Process
Pattern Recognition
Prevalence
Clinical Diagnosis Advice

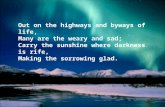
Management of a Patient Process
Patient
MD
GOALHealth Problem Resolution
Paraclinical Diagnostic Process
Indication (Certainty Deg/Mgt Plan)
Selection (Benefit/Risk/Cost/Avail)
Clinical Diagnosis Advice
Interpretation (Clinical Correlation)
Pretreatment DiagnosisAdvice
Clinical Diagnostic Process

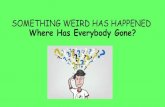
Management of a Patient Process
Patient
MD
GOALHealth Problem Resolution
Paraclinical Diagnostic Process
Specific Objective of Treatment
Selection (Benefit/Risk/Cost/Avail)
Clinical Diagnosis Advice
Mgt Outcome Evaluation
Pretreatment Diagnosis Advice
Treatment
Health Maintenance Advice
Clinical Diagnostic Process

Problem-based Learning in Medicine
Learningthe science and art
of medicine in the
functional or clinical context

PBL in Medicine in Small GroupFormat
Session I (2 hours)
1. Facilitator presents a problem (simulated or actual).
2. Students attempt to understand and solve the problem throughbrainstorming, discussion, and consensus.
They learn from each other as well as discover learning issues(later converted to students' learning objectives).

PBL in Medicine in Small GroupFormat
Session I (2 hours)
3.Students decide on a learning plan with or without the help of the facilitator.
The learning plan contain the following:Learning objectives
How to attain the learning objectivesMethods
Reading - what and which books, journalsAsking - who, where, whenDoing - what, where, when
Individual work or division of laborHow to assess attainment of learning objectivesTimetable
PBL in Medicine in Small GroupFormat
Session I (2 hours)
Independent Study (based on timetable in the learning plan)Students implement learning plan.
Session II (2 hours)

PBL in Medicine in Small GroupFormat
Session II (2 hours)
1.Students report and discuss the learning gained during the independent study in trying to understand and solve the initial problem.
2.Student may be given another problem to apply what they have just learned for reinforcement purposes.

THE TRAUMA
HEALTH PROBLEM
AN INSTRUCTIONAL PROGRAM FOR PRIMARY HEALTH CARE PHYSICIANS
DESIGNED FOR:
PROBLEM-BASED LEARNINGCOMPETENCY-BASED LEARNING
IN- AND OFF- CAMPUS LEARNING
Author:Reynaldo O. Joson, MD, MHPEd, MS Surg
1999

THE TRAUMA
HEALTH PROBLEM
Content
Title Goals and Strategies
Content .................................................................................A
About the Author ............................................................... B
Preface.................................................................................. C
The Course Pack - Content and How to Use ................... D

THE TRAUMA
HEALTH PROBLEM
Content ...Folder 1: Instructional Design............................................ I
Folder 2: Hypothetical and Actual Patient Management. II
Folder 3: Problem-based Learning Issues - Form ....….. III
Folder 4: Learning Objectives ...........................…..……. IV
General Learning Objectives ...................… IVAClinical Competencies ..............................… IVBBiological Foundation and Basis of Clinical
Management ……............................ IVC

THE TRAUMA
HEALTH PROBLEM
Content ...
Folder 5: Learning Resource Materials and References .V
List of Recommended References ............VA
Learning Resource Materials
Folder 6: Evaluation ....................................................… VI

THE TRAUMA
HEALTH PROBLEM
Content …Folder 7: Details and Format .......................….........… VII
Guidelines and FormatOverview and Personal Perspective .… VIICPublic Health Education ..........……… VIIDCommunity Health Management .....… VIIECase Presentation and Discussion ....…VIIFHypothetical Patient Management .......VIIG

THE TRAUMA
HEALTH PROBLEM
Content …Folder 7: Details and Format .....................…….........… VII
Guidelines and Format Psychosocial Issues ..............................VIIH
Bioethical Issues ..................................VII-IMedicolegal Issues ...............................VIIJResearch Issues ..............................…..VIIKGlossary ...............................................VIILSelf-Evaluation ....................................VIIMPresentation in a Symposium ............ VIIN

Module Making in
Medicine
Dear Module Maker or Student:
Thank you for your interest in making MODULES IN MEDICINE.
A TEMPLATE or SAMPLE is provided to make your task easy.

Module Making in
Medicine
1. Just change the name of the HEALTH PROBLEM.
Examples of health problems: HEADACHE, BURNS, DYSPNEA, PALLOR, DYSURIA, etc.

Module Making in
Medicine
2. Practically, what you are going to SUPPLY for the completion of a MODULE are just the following:
1. Patient simulations or hypothetical patients 2. Clinical abstracts 3. Specific clinical competencies 4. Biological foundation of clinical management 5. Evaluation

Module Making in
Medicine
I shall guide and help you as you go along.
When you make the MODULES IN MEDICINE, have in mind the contribution you will be giving to the development of effective, efficient, and humane physicians and in turn, to the health development of the country.
Thank you for joining hands with me in such an endeavor.
Reynaldo O. Joson, MD, MHA, MHPEd

What is the result or outcome
of all these things that I presented to you

What is the result or outcome
of all these things
that I presented to you
SATISFIED SO FAR!
BUT STILL A LOT TO DO !

What is the result or outcome
of all these things
that I presented to you
SATISFIED …...
CONTRIBUTION TO
HEALTH DEVELOPMENT

Community Health ManagementAction Research Outputs
• Reducing the Incidence of Diarrheal Diseases in Barangay Bantonan, Camalig, Albay, Through a 4-year Community Participated Intervention Program Using a Primary Health Care Approach (With Pictorial)

Community Health ManagementAction Research Outputs
• Reducing the Incidence Rate of Intestinal Parasitism Among Children 1 to 14 Years Old From 90% To 50 % by the year 2000 in Barangay Taladong, Camalig, Albay Using a Primary Health Care Approach

Community Health ManagementAction Research Outputs
• Reducing the Prevalence Rate of Underweight (2nd and 3rd Degree) Children (0 -5 Years Old) in Barangay Bariw, Camalig, Albay Using a Primary Health Care Strategy

What is the result or outcome
of all these things
that I presented to you
SATISFIED …...
BOARD PASSING

What is the result or outcome
of all these things
that I presented to you
SATISFIED …...
BETTER LEARNING

What is the result or outcome
of all these things
that I presented to you
SATISFIED …...
BETTER retention of learning
easy recall
development of skills
problem-solving, critical thinking, communication, interpersonal, cooperative learning, and self-directed learning

What is the result or outcome
of all these things
that I presented to you
SATISFIED SO FAR!
Repeat: Task is NOT yet completely done.There are STILL A LOT to accomplish.

What obstacles have I encountered
in trying to attain my vision on
medical education?

Obstacles Expected
•SCHOOL ADMINISTRATION
•FACULTY

Obstacles Expected
•SCHOOL ADMINISTRATION
NOT AN OBSTACLE AFTERALL!

Obstacles Expected
•FACULTY
BIGGEST AND HARDEST OBSTACLE!

Obstacles Expected
FACULTY
BIGGEST AND HARDEST OBSTACLE!
•CULTURE of traditional medical curriculum + BIASES + HABITS
•LACK OF TRAINING IN ANDRAGOGY
•LACK OF GENUINE DEDICATION TO TEACHING

What remains to be done to attain my vision
on medical education?

What remains to be done?
I will continue to develop the medical curriculum which I havevdesigned.
I will continue toStrengthen the frameworks and templates;Write course packs;Teach faculty – to produce more masters in medical
education with genuine dedication in teaching;Reach out to students to make the curriculum
student-friendly

What remains to be done?
I will document the impact of my curriculum model –
whether it is really more effective than the traditional ones and other innovative curricula;
whether it has better impact on the health development in the country;
whether it has more relevance to the health problems in the country; and lastly,
whether it is more student-friendly.

What remains to be done?
End-point -
At least five medical schools in the country,
spread out in Luzon, the Visayas, and Mindanao,
institutionalizing my medical curriculum model.
With your help,
with the help of Dr. Rodolfo Dimayuga who I am sure is listening to me and is pleased to hear our shared vision,
and with the help of Almighty God,
I am confident that I will be able to attain my dream.

I like to say thank you once again for the honor and privilege to be your speaker this afternoon.
I hope you enjoyed my talk.
I hope also that somehow I have inspired all of you to join Dr. Dimayuga and myself in contributing to a more effective medical curriculum in the Philippines.

Thank You and
Good Day