Texas' STAR+ Program: Managed Long Term Care Services and Supports
24
description
This session will feature three Medicaid state directors on the challenges and opportunities that Medicaid managed long-term care services and supports can provide. You will hear from states that have "gone there" and "done that," which will provide insights on lessons learned. >>Faculty: Justin Senior, Deputy Secretary, Division of Medicaid, Florida Agency for Health-Care Administration || Martha Roherty, Executive Director, National Association of States United for Aging and Disabilities || Marc Gold, Special Advisor for Policy and Promoting Independence, Texas Department of Aging and Disability Services
Transcript of Texas' STAR+ Program: Managed Long Term Care Services and Supports


Medicaid Managed Long Term Care Services and Supports: What Have We
Gotten Into?: Texas’ STAR+ Program
May 7, 2013 Charlotte, North Carolina
Marc Gold Texas Department of Aging and Disability Services

History and Goals 1995 - Legislative Direction to create STAR+. 1998 - Pilot in Houston as (b)(c) waivers. 2007; 2011; 2012 – Major expansions. 2011 - STAR+ became a 1115 waiver. 2013 - Significant changes being made after legislative session. Proposed statewide coverage replacing remaining fee-for-service program. Increased access to community services. Improved coordination between acute and LTSS. Reduction in NF admission rates. Overall improved efficiency of the acute and LTSS systems.

What is STAR+ Integrated delivery system for acute and long term services and supports to provide coordinated health care, acute, and LTSS. Waiver authority: 1115 (was a b/c until December 2011. Risk-based, capitated model. Includes dual eligibles (Medicare and Medicaid) Delivered through licensed managed care. organizations (at least two in each catchment area):
Medicaid beneficiaries receive both acute and LTSS through Medicaid MCO
Dual Eligible beneficiaries receive acute services through Medicare and Medicaid LTSS services through Medicaid MCO (Dual Eligible Project: 2015).

Who is qualifies for STAR+ Individuals with a physical disability or a mental health need and qualify at the SSI level of income. Individuals age 21 or older who receive Medicaid because they are in a social security exclusion program. Individuals who qualify for TX’ fee-for-service nursing facility waiver* -- will change. Individuals who are Dual eligible (55%). Children are voluntary (20%)*-- will change.

Who doesn’t qualify: May 2013 NF residents*- will change. STAR+ members who have been in a NF for more than
120 days*- will change. Residents of ICFs for individuals with intellectual and
developmental disabilities (IDD)*- eventually may change.
Individuals not eligible for full Medicaid. Individuals in IDD waivers*- eventually may change. Children in foster care.

Special Features Service coordination
Makes home visits; Develops individual plan of care for acute/LTSS; Authorizes LTSS; Arranges and coordinates acute services; Assists with Medicare physician.
Unlimited prescriptions (Duals receive drugs through Medicare Part D).
No limit on inpatient psychiatric services. Value-added services (dependent on each managed care
organization). Enrollment broker.

Services State Plan:
Acute – all state plan services primary preventive doctor hospital lab x-ray.
Attendant* and day activity and health services. Mental Health and Substance Abuse. *Consumer-directed Option

Services Waiver” services:
Respite* Nursing* Therapies* Adaptive aids Minor home modifications Adult Foster Care Services within assisted living Dental Emergency response Home delivered meals
*Consumer-directed Option

Cost Effectiveness Reduced costs in STAR+ compared to non-capitated
systems, savings as percentage reductions include:
22% for in-patient 15% for acute out-patient 10% for LTSS.

Capitated/Risk Model Four capitation rates dependent on:
if the individual is Medicaid only or dual eligible. eligible for lower-level State Plan programs or full
waiver services based on NF eligibility criteria. Rates are region specific. Rate structure will change in September 2014.
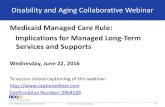
Rebate % of Revenues MCO Share State Share
0% to 3% 100% 0%
3% to 5% 80% 20%
5% to 7% 60% 40%
7% to 9% 40% 60%
9% to 12% 20% 80%
>12% 0% 100%
Capitated At-Risk Capitation Rate At-Risk methodology is dependent on the
outcome of pre-identified performance-based measures.
Uniform Managed Care Contract (UMCC) includes a provision which puts up to five percent of the MCO’s capitation at risk.
The objective is that all MCOs achieve performance levels that enable to receive the full at-risk amount.
HHSC identifies no more than 10 at-risk performance indicators for each MCO Program.

Quality Challenge Award HHSC reallocates any unearned funds from the
performance-based, at-risk portion of a MCO’s capitation rate to the MCO Program’s Quality Challenge Award.
HHSC determines the number of MCOs that will receive Quality Challenge Award funds annually based on the amount of the funds to be reallocated.
Separate Quality Challenge Award payments are made for each of the MCO programs.
HHSC works with the EQRO and the MCOs to identify the performance indicators for which their capitation will be placed at risk.

Quality Strategy Summarizes the history of Medicaid managed care in Texas
and the 1115 Medicaid Waiver Demonstration. Provides an overview of HHSC’s quality goals, objectives,
and strategy. Discusses the role of the EQRO in conducting quality
assessment and improvement of managed care. Describes how HHSC will assess MCO contractual
requirements and compliance. Describes how HHSC will attempt to improve the quality of
care delivered by the MCO. Highlights some of the ongoing initiatives aimed at
improving health care quality and/or services.

Statistics

Statistics
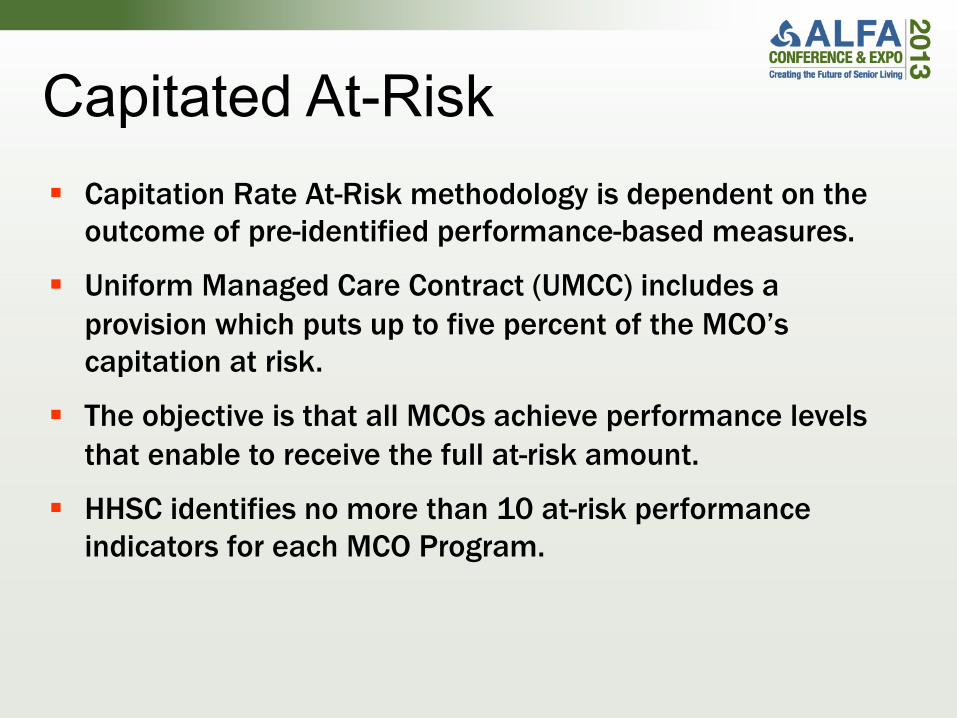
Source: August 2012 Capitation File
Statistics: August 2012

STAR+ Impact on Rebalancing LTSS Individuals at the SSI level receive waiver services as an
entitlement. Increased retention of individuals in community and
prevention of returning to an institutional setting.
Significant decrease on NF waiver “waiting lists”. Overall, more efficient system and easier access to
services.
Lessons Learned Greater outreach to consumers and providers. More extensive education for MCOs: TX was one of the
first states to implement managed LTSS and most MCOs (HMOs) did not have experience with LTSS.
Pilot continued in the one site too long. Enrollment broker tied to success of enrollment (80
percent). Creation of Regional Advisory Committees. Exclusion of NF from system. Better oversight of service coordination role.

Lessons Learned Greater oversight of quality measures: establishment of
“dashboard” measure.
Should have established IT systems to more easily separate acute from LTSS costs for purposes of reporting.

Future of STAR+/Managed Care Senate Bills 7 and 58 Full statewide coverage of STAR+ Inclusion of Nursing Facility: 9/2014 Inclusion of Medicaid behavioral health services Creation of a mandatory managed care program for
children at SSI level of income: STAR Kids Testing models for inclusion of individuals with intellectual
and developmental disabilities Inclusion of Community First Choice

Contact Information Marc S. Gold TX Department of Aging and Disability Services Special Advisor for Policy Office of the Commissioner 512.438.2260 [email protected] www.dads.state.tx.us/business/pi/index.html.

Contact Information Gary Jessee Health and Human Services Commission Deputy Director, Medicaid/CHIP Division 512.491.1379 [email protected] www.hhsc.state.tx.us/starplus/starplus.htm.