Testosterone – What to Measure & When...General Outline My Interest in Testosterone Measurements...
38
Godfrey C Moses, Godfrey C Moses, BSc BSc , , MSc MSc , PhD, FCACB , PhD, FCACB Laboratory Director/Discipline Leader Chemistry, Laboratory Director/Discipline Leader Chemistry, Gamma Gamma - - Dynacare Medical Laboratories, Dynacare Medical Laboratories, London, ON ( London, ON ( mosesg@gamma mosesg@gamma - - dynacare.com dynacare.com ) ) Testosterone – What to Measure & When
Transcript of Testosterone – What to Measure & When...General Outline My Interest in Testosterone Measurements...

Godfrey C Moses, Godfrey C Moses, BScBSc, , MScMSc, PhD, FCACB, PhD, FCACBLaboratory Director/Discipline Leader Chemistry,Laboratory Director/Discipline Leader Chemistry,
GammaGamma--Dynacare Medical Laboratories,Dynacare Medical Laboratories,London, ON (London, ON (mosesg@[email protected]))
Testosterone – What to Measure & When

General Outline
My Interest in Testosterone MeasurementsMy Interest in Testosterone MeasurementsBrief Review of Testosterone & Clinical Brief Review of Testosterone & Clinical SignificanceSignificanceSome Factors Affecting Interpretation of Some Factors Affecting Interpretation of Testosterone ResultsTestosterone ResultsTechnical Issues Associated with Total Technical Issues Associated with Total Testosterone Measurements Testosterone Measurements What & When to Measure What & When to Measure –– Recommendations Recommendations from 2 major studiesfrom 2 major studiesSummary & AcknowledgementsSummary & Acknowledgements

Background
Why no stated ageWhy no stated age--specific RIspecific RI’’s for Serum Free s for Serum Free TestoTestoin Women when most Labs & Textbooks did; plus such in Women when most Labs & Textbooks did; plus such RIRI’’s were vital in diagnosing & treating his patients?s were vital in diagnosing & treating his patients?
Why < 12 Why < 12 pmolpmol/L as RI for FT in women when a result /L as RI for FT in women when a result of 0 of 0 pmolpmol/L is pathological for all post/L is pathological for all post--pubertal ages?pubertal ages?
…….... comprehensive review of RIcomprehensive review of RI’’s Free & Total s Free & Total TestoTesto and participation in the OSCC Consensus and participation in the OSCC Consensus Conference on Functional Conference on Functional TestoTesto Measurements in Measurements in Males & Females.Males & Females.

What is testosterone & whymeasure it?C19 steroid C19 steroid

Multiple Forms……
Tissue form (Tissue form (DihydroDihydro--TestoTesto –– DHT)DHT)
Circulatory form (bound & unbound to proteins)Circulatory form (bound & unbound to proteins)
Major androgen; Stimulate spermatogenesisMajor androgen; Stimulate spermatogenesis
Synthesis & biochemical function Synthesis & biochemical function -- under under HypothalHypothal--Pit ControlPit Control

Clinical Significance
Increased in:Increased in:Precocious PubertyPrecocious PubertyAndrogen resistance Androgen resistance Ovarian cancerOvarian cancerCongenital Adrenal Hyperplasia Congenital Adrenal Hyperplasia Polycystic Ovary DiseasePolycystic Ovary DiseaseTesticular CancerTesticular Cancer
Decreased in:Decreased in:HypopituitarismHypopituitarismTesticular Failure Testicular Failure Delayed puberty Delayed puberty Chronic illness Chronic illness ProlactinomaProlactinoma

Delta 5 Pregnenolone is an Obligatory Intermediate in its Biosynthesis …..

What is the Current Status?
Routinely assayed in Serum or Plasma as..Routinely assayed in Serum or Plasma as..Total Testosterone (TT) Total Testosterone (TT) –– nmolnmol/L/LUnbound or Free Testosterone (FT) Unbound or Free Testosterone (FT) –– pmol/L(2pmol/L(2--3 % 3 % of TT)of TT)BioavailableBioavailable Testosterone (BAT) Testosterone (BAT) –– nmol/L(43% of nmol/L(43% of TT)TT)Free Androgen Index (FAI; TT/SHBG) Units: 1, 10, Free Androgen Index (FAI; TT/SHBG) Units: 1, 10, 100100SHBG SHBG –– nmol/L(55% of TT)nmol/L(55% of TT)DHT (Tissue Form) DHT (Tissue Form) –– Not Done RoutinelyNot Done Routinely

Factors Affecting Interpretation Factors Affecting Interpretation –– RIRI’’ss
Reviewed Published RIReviewed Published RI’’s for FT in Females s for FT in Females 11 major providers, US/Canada 11 major providers, US/Canada
7 Reference Labs7 Reference Labs1 Teaching Hospital Lab1 Teaching Hospital Lab2 Text Books2 Text Books1 Manufacturer Kit Insert 1 Manufacturer Kit Insert ––Analog Analog
5 state age5 state age--specific RIspecific RI’’s in adults onlys in adults only1 states RI in children age 1 1 states RI in children age 1 ––10 yrs (not10 yrs (not--age specific)age specific)Low end of RI ranged from 0.1 Low end of RI ranged from 0.1 –– 3.1 3.1 pmolpmol/L/L1 states low end RI as 1 states low end RI as ““less thanless than””
Ref: Moses, G.C (2001) Ref: Moses, G.C (2001) –– Unpublished DataUnpublished Data

RI - Quebec (Sherebrooke) Study
CHUS on Young Healthy Women (N=188, 18 CHUS on Young Healthy Women (N=188, 18 –– 40Y) 40Y) TestTest ULR ULR TTTT 2.54 2.54 nmolnmol/L (/L (cfcf 2.7 2.7 nmolnmol/L)/L)
BATBAT 0.90 0.90 nmolnmol/L (/L (cfcf 1.2 1.2 nmolnmol/L)/L)FT (Calc)FT (Calc) 43.4 43.4 pmolpmol/L (/L (cfcf 58.0 58.0 pmolpmol/L)/L)SHBGSHBG UTD (because study UTD (because study inclincl
women on the pill)women on the pill)Ref: Fink, G.D (2007) Ref: Fink, G.D (2007) –– Clin.Chem.2007; 53(6) Clin.Chem.2007; 53(6)

Actual Patient Results (LIS Data) show 6 % of Actual Patient Results (LIS Data) show 6 % of men & 17% of women had undetectable TT men & 17% of women had undetectable TT (<0.3nmol/L)(<0.3nmol/L)……
2 months period (N=5714)2 months period (N=5714)Males: 3286 Males: 3286 Females: 2438 Females: 2438
TTTT % % MalesMales FemalesFemales
<0.3 <0.3 nmolnmol/L/L 6.06.0 17.417.4<12.0 <12.0 nmolnmol/L/L 4.44.4 99.499.4>10.0 >10.0 nmolnmol/L/L 50.550.5 0.70.7<3.0 <3.0 nmolnmol/L/L 12.012.0 96.696.6
Ref: Moses, G.C (2004 Ref: Moses, G.C (2004 –– Unpublished Data)Unpublished Data)

Factors Affecting InterpretationFactors Affecting Interpretation…….. ..
Biological Variation

Factors Affecting InterpretationFactors Affecting Interpretation……. .
Biological Variation

Factors Affecting SHBG
Increased in Increased in Estrogen Treatment, Androgen and Growth Estrogen Treatment, Androgen and Growth Hormone deficiencies, Aging, Hormone deficiencies, Aging, ThyrotoxicosisThyrotoxicosis, , Alcoholic Cirrhosis and HepatitisAlcoholic Cirrhosis and Hepatitis
Decreased inDecreased inHyperinsulinemiaHyperinsulinemia, Obesity, , Obesity, AcromegalyAcromegaly, Androgen , Androgen Treatment, Hypothyroidism, Treatment, Hypothyroidism, NephroticNephrotic Syndrome, Syndrome, HypercortisolemiaHypercortisolemia, Familial Disorders, Familial Disorders

How is TT measured & what are some of the issues?
TT:TT: Immunoassays Immunoassays –– Direct & Indirect (Extraction); Direct & Indirect (Extraction); Direct Automated Preferred; Chromatography Direct Automated Preferred; Chromatography ––HPLC & GC Mass Spectrometry; Tedious/unsuited HPLC & GC Mass Spectrometry; Tedious/unsuited for routine usefor routine useFT:FT: Measured Measured -- Immunoassays Immunoassays –– RIA & RIA & AnaloqAnaloq; ; Equilibrium DialysisEquilibrium DialysisCalculated Calculated –– (1) {TT (1) {TT ––[[AlbT+SHBGTAlbT+SHBGT]}; (2) [BAT ]}; (2) [BAT –– AlbTAlbT]]BAT:BAT: Measured Measured -- Immunoassays Immunoassays –– RIA/AS RIA/AS pptpptCalculated Calculated –– (1) {FT +(1) {FT +AlbTAlbT}; (2) [TT }; (2) [TT –– SHBGT]SHBGT]
ED is gold standard but not suitable for routine useED is gold standard but not suitable for routine useAnaloqAnaloq--based FT has no added clinical information to measured based FT has no added clinical information to measured TT TT (Fritz, K. S. et al. (Fritz, K. S. et al. ClinClin ChemChem 2008; 54: 512 2008; 54: 512 –– 516)516)Majority of users in CAP Survey still use the analogMajority of users in CAP Survey still use the analog--based FTbased FT

Few Labs Perform SHBG & FAI
FAI (Free Androgen Index) & SHBG: FAI (Free Androgen Index) & SHBG: FAI = TT FAI = TT nmolnmol/L / SHBG /L / SHBG nmolnmol/L x 10, x100, x1000/L x 10, x100, x1000
Result is method dependentResult is method dependentSHBG SHBG –– immunoassay; manual; few automated assays immunoassay; manual; few automated assays exists but not available in most labsexists but not available in most labsCalculated FT, BAT & FAI must have accurate & Calculated FT, BAT & FAI must have accurate & precise SHBG assaysprecise SHBG assaysAS AS pptppt method of choice BAT but results can vary method of choice BAT but results can vary from lab to lab (technique)from lab to lab (technique)

Issues with assays for multiple components of Testo…
IAIA’’s: Perform differently in males and females s: Perform differently in males and females Cross reactivity with other steroids Cross reactivity with other steroids Lack Adequate Anal Lack Adequate Anal SensSens for use in kids, women & elderly menfor use in kids, women & elderly menwith diagnosed androgen deficiencywith diagnosed androgen deficiency
Others: Lack of evidenceOthers: Lack of evidence--based protocol for BAT based protocol for BAT AgeAge--associated discrepancy between associated discrepancy between mBATmBAT and and cBATcBAT in men; ain men; a
decrease in decrease in cBAT is aprrox. 2 x mBAT((DechaudDechaud, H. et al. , H. et al. ClinClin ChemChem 2007; 53(4): 723 2007; 53(4): 723 –– 728728). ).
When to do further workWhen to do further work--up? On females if TT by automated up? On females if TT by automated IAIA’’s >1.2nmol/s >1.2nmol/L, >3nmol/L or L, >3nmol/L or 5 5 nmolnmol/L? (> 3 /L? (> 3 nmolnmol/L most common); SHBG, extract in/L most common); SHBG, extract in--house and/or send out to another lab with different IA house and/or send out to another lab with different IA method or IDMS reference lab?method or IDMS reference lab?

IA’s for TT perform differently in men & women..Immunoassays Immunoassays vsvs GCGC--MSMS
Total Total TestoTesto; n=10 IA ; n=10 IA vsvs ID/GCMSID/GCMS7/10 had higher values than GCMS (up to 46% higher) 7/10 had higher values than GCMS (up to 46% higher) in Femalesin Females4/10 had lower values than GCMS (up to 46% lower in 4/10 had lower values than GCMS (up to 46% lower in MalesMalesMagnitude of Mean Differences (Bias) were also Magnitude of Mean Differences (Bias) were also different in males & femalesdifferent in males & females0/10 was sufficiently reliable for use in Children & 0/10 was sufficiently reliable for use in Children & womenwomen7/10 had r > 0.95 but only in men; r < 0.95 for females 7/10 had r > 0.95 but only in men; r < 0.95 for females in all 10.in all 10.
Ref. 1. Ref. 1. TaiebTaieb et al. et al. ClinClin. Chem. 2003; 49(8): 1381. Chem. 2003; 49(8): 1381--1391.1391.

IA’s for TT perform differently in men & women..Female TT GCMS Targeting Exercise. Sept 2002; N=218 Female TT GCMS Targeting Exercise. Sept 2002; N=218
labslabs
All had Slope > 1.00 relative to GCMS, except Bayer All had Slope > 1.00 relative to GCMS, except Bayer Centaur, Beckman Access and an inCentaur, Beckman Access and an in--house RIA house RIA extraction method.extraction method.75% had + bias in normal range & 50% had + bias at 75% had + bias in normal range & 50% had + bias at traditional ULNtraditional ULNBetween and within method variability was Between and within method variability was ““HugeHuge””
Ref. Jonathan Middle. UK NEQAS Ref. Jonathan Middle. UK NEQAS –– Steroid Hormone 2002 Annual ReviewSteroid Hormone 2002 Annual Review

Several Formulae for calculating FT & BAT are available, but need to keep in mind..
Calculations are based on binding constants at Calculations are based on binding constants at physiological protein concentrations physiological protein concentrations
Provide results in either SI or nonProvide results in either SI or non--SI units, expressed SI units, expressed as absolute values or percentages of TTas absolute values or percentages of TT
Calculation of BAT & FT in men: A Comparison of 5 Calculation of BAT & FT in men: A Comparison of 5 Published Algorithms (Published Algorithms (De De RondeRonde, W. et al. , W. et al. ClinClin ChemChem 2006; 2006; 52:17752:177--17841784))
The International Society for the Study of the Aging The International Society for the Study of the Aging Male (ISSAM) Website (Male (ISSAM) Website (www.issam.ch/freetesto.htmwww.issam.ch/freetesto.htm))
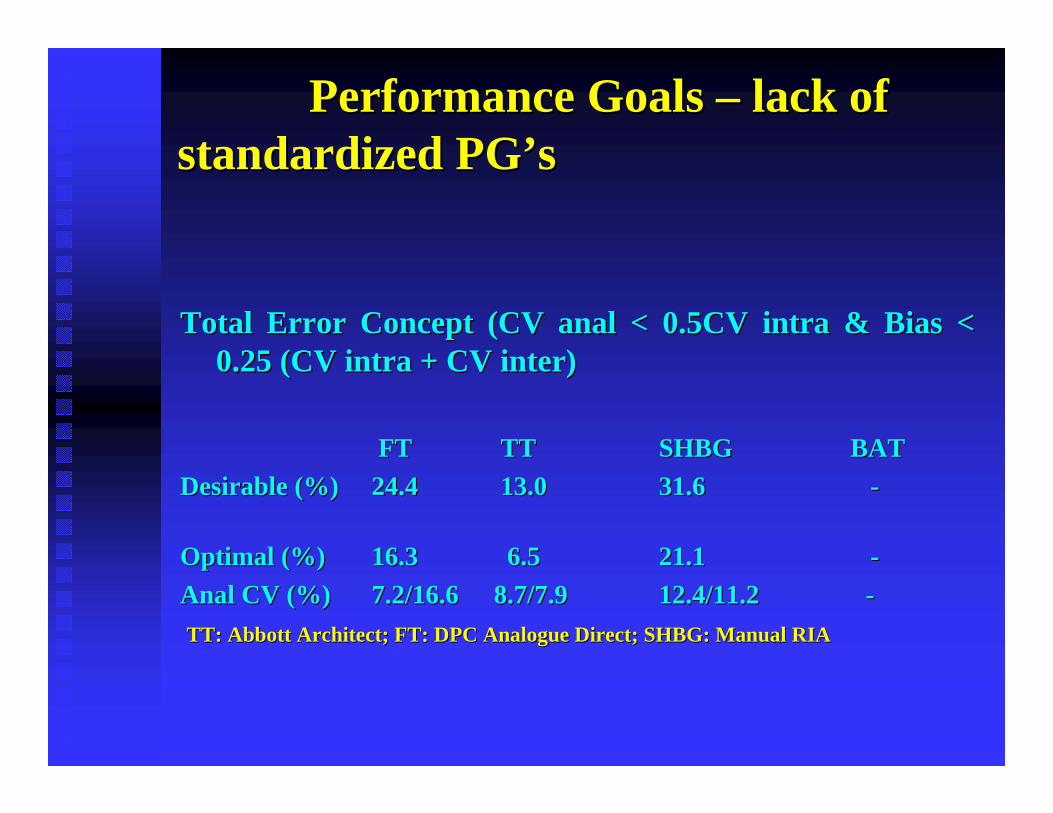
Performance GoalsPerformance Goals –– lack of lack of standardized PGstandardized PG’’ss
Total Error Concept (CV anal < 0.5CV intra & Bias < Total Error Concept (CV anal < 0.5CV intra & Bias < 0.25 (CV intra + CV inter) 0.25 (CV intra + CV inter)
FTFT TTTT SHBGSHBG BATBATDesirable (%)Desirable (%) 24.424.4 13.013.0 31.631.6 --
Optimal (%)Optimal (%) 16.316.3 6.56.5 21.121.1 --Anal CV (%)Anal CV (%) 7.2/16.67.2/16.6 8.7/7.98.7/7.9 12.4/11.2 12.4/11.2 --TT: Abbott Architect; FT: DPC Analogue Direct; SHBG: Manual RIATT: Abbott Architect; FT: DPC Analogue Direct; SHBG: Manual RIA

Reference Change Value (RCV,%) Utility…
FTFT TTTT SHBGSHBG BATBATL1 L1 L2L2 L1L1 L2L2 L1L1 L2L2 L1 L2L1 L2
95 % CL 52.795 % CL 52.7 45.745.7 34.334.3 32.832.8 48.048.0 32.632.6 -- --
99% CL 68.999% CL 68.9 42.642.6 44.844.8 42.842.8 62.762.7 59.759.7 -- --
[Anal & Intra[Anal & Intra--Individual Variation: {1.414 x Z x SQRT (CVIndividual Variation: {1.414 x Z x SQRT (CV22anal anal + CV + CV 22
intraintra)}] x100])}] x100]

There is not always Gold in the “Gold Standard” - Ref: Joint Committee for Traceability in Lab Medicine Database (www.bipm.org/jctlm)
IDMS Methods for Testosterone in Blood Serum.IDMS Methods for Testosterone in Blood Serum.Method 1Method 1 DGKC definitive method for serum TDGKC definitive method for serum TMethod descriptionMethod description ID/GC/MSID/GC/MSApplicable RangeApplicable Range 2 2 nmol/lnmol/l to 45 to 45 nmol/lnmol/lExpected Uncertainty (95% CL)Expected Uncertainty (95% CL) 1 % to 3 %1 % to 3 %Reference(s)Reference(s) SiekmannSiekmann et al., J. Steroid et al., J. Steroid BiochemBiochem., .,
1979, 11, 1171979, 11, 117--123123Method 2Method 2 Univ. of Ghent Univ. of Ghent RfRf. Meas. . Meas. ProcedProced. for T . for T
•• Method description Method description ID/GC/MSID/GC/MS•• Applicable RangeApplicable Range 0.05 0.05 nmol/lnmol/l to 70 to 70 nmol/lnmol/l
Expected Uncertainty (95% CL)Expected Uncertainty (95% CL) 1.5 % to 3 %1.5 % to 3 %Reference(s)Reference(s) Anal Chem., 199, 66, 4116Anal Chem., 199, 66, 4116--4141
EurEur. J. . J. ClinClin. Chem. . Chem. ClinClin. . BiochemBiochem., ., 1996, 34, 8531996, 34, 853--860860
LCLC--MS/MS MS/MS –– AACC: AACC: AbstrAbstr # 189. # 189. Anal Anal SensSens: 0.07 : 0.07 nmolnmol/L; AMR: 0 /L; AMR: 0 -- 129 129 nmolnmol

How is Clinical Applicability of GCHow is Clinical Applicability of GC-- & LC& LC--MS MS Techniques Assessed?Techniques Assessed?
Comparison with Direct Automated ImmunoassaysComparison with Direct Automated ImmunoassaysClinical Data (evidenceClinical Data (evidence--based medicine) Neededbased medicine) NeededVarying Analytical SensitivitiesVarying Analytical Sensitivities
Detection Limits 10 Immunoassay Systems (TT; Detection Limits 10 Immunoassay Systems (TT; nmolnmol/L)/L)Assay System Assay System Detection Limit Detection Limit
(manufacturer(manufacturer’’s claim)s claim)Abbott ArchitectAbbott Architect 0.280.28Bayer CentaurBayer Centaur 0.350.35Bayer Immuno1Bayer Immuno1 0.170.17BioBio--MerieuxMerieux ((VidasVidas)) 0.350.35ImmunliteImmunlite 2000(DPC)2000(DPC) 0.300.30VitrosVitros EciEci (OCD)(OCD) 0.030.03Perkin Elmer Perkin Elmer AutoDelphiaAutoDelphia 0.400.40Roche Roche ElecsysElecsys 20102010 0.0690.069Beckman (Beckman (ImmunoTechImmunoTech) ) 0.0860.086Dade Behring (PC)Dade Behring (PC) 0.140.14
Ref. 1. Ref. 1. TaiebTaieb et al. et al. ClinClin ChemChem 2003; 49(8): 13812003; 49(8): 1381–– 1391.1391.

What & When to Measure Testosterone & Which Method/Assay?

Ontario Community Labs Perform More Ontario Community Labs Perform More FT Than TT AnnuallyFT Than TT Annually……
Total Total FreeFree BATBAT SHBGSHBG
2003 2003 ––20042004Hospital LabsHospital Labs 2556525565 98699869 -- --Community labsCommunity labs 9568195681 100284100284 -- --
Lab Licensing Lab Licensing Testing Labs Data (Testing Labs Data (’’04)*04)*Hospital LabsHospital Labs 325**325** 12001200Community LabsCommunity Labs 1280012800 420420
*Data is annualized and do not include all provincial Labs; ** s*Data is annualized and do not include all provincial Labs; ** some ome regional hosp. labs do not perform Total T or BAT, while others regional hosp. labs do not perform Total T or BAT, while others are are looking at offering a calculated BAT in the nearlooking at offering a calculated BAT in the near future.future.

What is really driving the continued interest in Testing for Testosterone?
Need for prompt diagnosis and treatment of Need for prompt diagnosis and treatment of hypogonadismhypogonadism in elderly men in elderly men Testosterone (sex hormone) concentration Testosterone (sex hormone) concentration and selfand self--rated health & life satisfaction, rated health & life satisfaction, depression or dementia in the elderly depression or dementia in the elderly Improved Sex Drive/Sexual Performance in Men Improved Sex Drive/Sexual Performance in Men Increased Libido and Mood in womenIncreased Libido and Mood in women
Testosterone (sex hormone) influence on Testosterone (sex hormone) influence on pubertal growth pubertal growth

What is driving interest cont’d……Erectile Dysfunction (ED) Erectile Dysfunction (ED) -- Relatively Common; Relatively Common; Affects Men & Women (Affects Men & Women (Dean J. et al. Dean J. et al. IntInt J J ClinClin Practice. 2008; Practice. 2008; 62: 12762: 127--133 & Fisher W.A. et al. FEMALES Study 133 & Fisher W.A. et al. FEMALES Study –– Females Experience Females Experience of Menof Men’’s Attitudes to Life Events and Sexuality s Attitudes to Life Events and Sexuality –– J Sex Med. 2005; 2: 675J Sex Med. 2005; 2: 675--672) 672)
Evidence that testosterone treatment is beneficialEvidence that testosterone treatment is beneficialImproved/enhanced sexual function and moodImproved/enhanced sexual function and moodDecreased body fat massDecreased body fat massIncreased lean body massIncreased lean body massIncreased bone mineral densityIncreased bone mineral densityNormalized blood total & free testosterone in Normalized blood total & free testosterone in deficient subjectsdeficient subjects
Ref. Wang et al. J Ref. Wang et al. J ClinClin EndocrinolEndocrinol MetabMetab. 2004; 89:2085 . 2004; 89:2085 –– 2098 2098 & & SynderSynder et al. J et al. J ClinClin EndocrinolEndocrinol MetabMetab. 2000; 85:2670 . 2000; 85:2670 –– 2677) 2677)

What is driving interest cont’d……
T Replacement Therapy T Replacement Therapy In US # prescriptions for T replacement increased In US # prescriptions for T replacement increased by 1700% from 1994 by 1700% from 1994 –– 2003 2003 ((BhasinBhasin, S. et al. J , S. et al. J AndolAndol. 2003; 24: 299. 2003; 24: 299--311 .311 .…… recommendations for recommendations for monitoring & managing risks of prostate disease monitoring & managing risks of prostate disease during T replacement therapy in older men) during T replacement therapy in older men) ––FinasterideFinasteride TxTx for BPH (F is 5for BPH (F is 5--alpha alpha reductasereductaseinhibitor) inhibitor) –– effects on T replacement?effects on T replacement?
In Finland, nearly 100% increases in wholesale In Finland, nearly 100% increases in wholesale turnover for T between 1993 & 2004 (E472.9K to turnover for T between 1993 & 2004 (E472.9K to E913.4K) E913.4K)

Evidence for multiple health & functional Evidence for multiple health & functional benefits for testosterone supplementation, benefits for testosterone supplementation, particularly often sought by the elderly, real?particularly often sought by the elderly, real?
Finish StudyFinish StudyAssociations of Sex Hormone Concentrations with Health and Associations of Sex Hormone Concentrations with Health and Life Satisfaction in Elderly Men Life Satisfaction in Elderly Men ((EskelinenEskelinen, S. I. et al. , S. I. et al. EndocrEndocrPractPract. . 2007; 13(7): 7432007; 13(7): 743--749.749. Also on Also on www.medscape.com/viewarticle/572248)www.medscape.com/viewarticle/572248)19981998-- 1999, N = 517 elderly men (mean age, 73 years; range, 64 1999, N = 517 elderly men (mean age, 73 years; range, 64 to 97)to 97)Serum levels of TT, LH, follicleSerum levels of TT, LH, follicle--stimulating hormone (FSH), stimulating hormone (FSH), sex hormonesex hormone--binding globulin (SHBG), and binding globulin (SHBG), and estradiolestradiol (E(E22) were ) were determined by the determined by the AutoDelfiaAutoDelfia automatic immunoassay (Timeautomatic immunoassay (Time--resolved fluorescent immunoassay). resolved fluorescent immunoassay). NonNon--SHBGSHBG--bound T (bound T (cFTcFT/BAT) calculated as follows: %FT = /BAT) calculated as follows: %FT = 2.28 2.28 --1.38 1.38 ×× log(SHBG [nmol/L]/10)log(SHBG [nmol/L]/10)

Evidence of benefits Evidence of benefits ……. Finish Study Cont. Finish Study Cont’’dd
Serum FT (Serum FT (pmolpmol/L) = %FT /L) = %FT ×× TT (TT (nmolnmol/L) /L) ×× 10. The analytical 10. The analytical sensitivity of the TT assay was 0.3 sensitivity of the TT assay was 0.3 nmolnmol/L. Calibrated with IDMS /L. Calibrated with IDMS traceable standard. traceable standard. SelfSelf--rated Health, rated Health, Life Satisfaction, SelfLife Satisfaction, Self--Rating Depression & Rating Depression & Dementia (21 Q questionnaire)Dementia (21 Q questionnaire)ConclusionConclusion
Low serum T concentration was associated with diagnosed Low serum T concentration was associated with diagnosed depression.depression.SubclinicalSubclinical hypogonadismhypogonadism may be associated with diagnosed may be associated with diagnosed dementia. dementia. Older age and being overweight were predictors of poor health Older age and being overweight were predictors of poor health or occurrence of many symptoms among elderly men. or occurrence of many symptoms among elderly men.

What to Measure & When? OSCC ExpertsWhat to Measure & When? OSCC Experts
OSCC Consensus ConferenceOSCC Consensus ConferenceC. P. COLLIER, et al. C. P. COLLIER, et al. FuFunctional testosterone: Biochemical nctional testosterone: Biochemical assessment of assessment of hypogonadismhypogonadism in men in men –– Report from a Report from a multidisciplinary workshop hosted by the Ontario Society of multidisciplinary workshop hosted by the Ontario Society of Clinical Chemists. Clinical Chemists. The Aging Male 2008; 10(4): 211 The Aging Male 2008; 10(4): 211 –– 216216
Objectives: to establish the most reliable, costObjectives: to establish the most reliable, cost--effective effective approach to the biochemical assessment of approach to the biochemical assessment of hypogonadismhypogonadism in in men.men.
Who: Specialists across Canada in clinical biochemistry, Who: Specialists across Canada in clinical biochemistry, endocrinology, family medicine and urology (1endocrinology, family medicine and urology (1--day workshop)day workshop)

OSCC Experts OSCC Experts CCon’t
Method: Two key challenges Method: Two key challenges -- 1) Total testosterone (TT) 1) Total testosterone (TT) determinations are equivalent to determinations are equivalent to bioavailablebioavailable testosterone testosterone (BAT) or calculated BAT ((BAT) or calculated BAT (cBATcBAT) or free testosterone (FT) (by ) or free testosterone (FT) (by analogue radioimmunoassay or equilibrium dialysis) or analogue radioimmunoassay or equilibrium dialysis) or calculated FT (calculated FT (cFTcFT); 2) No good evidence that borderline low ); 2) No good evidence that borderline low testosterone concentrations in men should be treated. testosterone concentrations in men should be treated. Outcomes: Identify what agreement exists in Canada, what Outcomes: Identify what agreement exists in Canada, what issues were still controversial, and what research remains to beissues were still controversial, and what research remains to beaddressedaddressedConclusions. Total testosterone is a reliable marker for the Conclusions. Total testosterone is a reliable marker for the initial investigation of men presenting with symptoms of initial investigation of men presenting with symptoms of hypogonadismhypogonadism; ; cBATcBAT is a reasonable followis a reasonable follow--up test in patients up test in patients with equivocal biochemical or consistent symptomatic findings.with equivocal biochemical or consistent symptomatic findings.
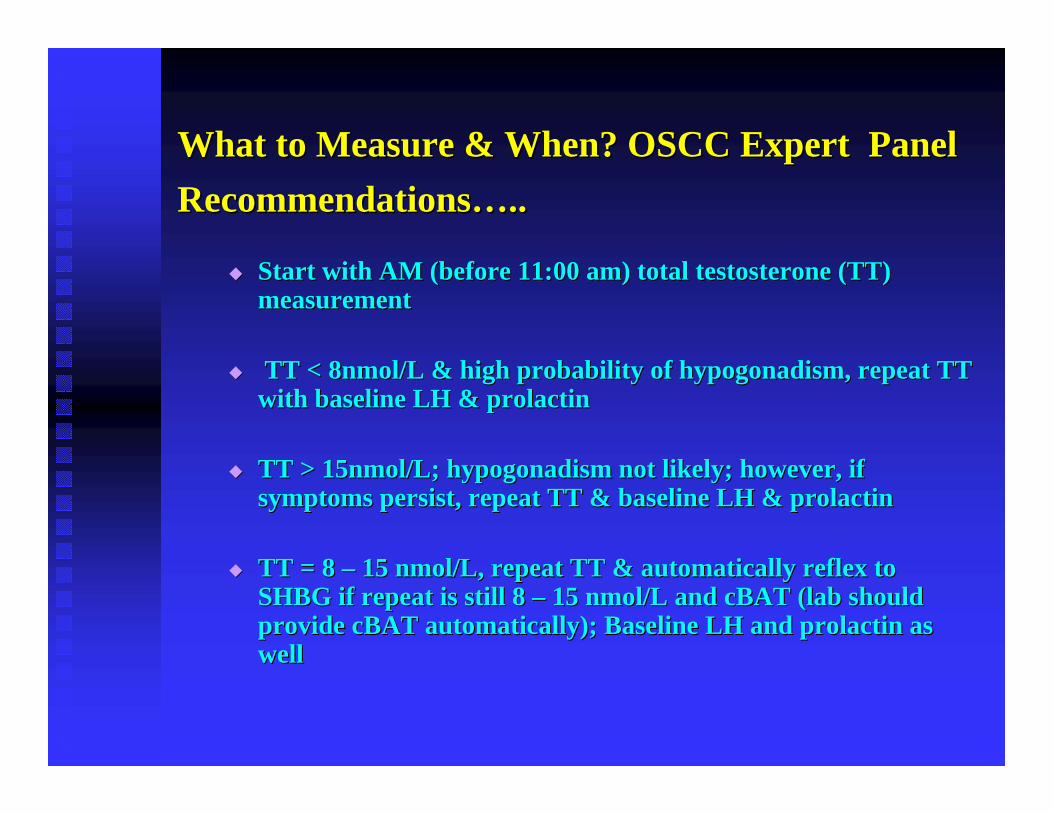
What to Measure & When? OSCC Expert Panel What to Measure & When? OSCC Expert Panel RecommendationsRecommendations…….. ..
Start with AM (before 11:00 am) total testosterone (TT) Start with AM (before 11:00 am) total testosterone (TT) measurementmeasurement
TT < 8nmol/L & high probability of TT < 8nmol/L & high probability of hypogonadismhypogonadism, repeat TT , repeat TT with baseline LH & with baseline LH & prolactinprolactin
TT > 15nmol/L; TT > 15nmol/L; hypogonadismhypogonadism not likely; however, if not likely; however, if symptoms persist, repeat TT & baseline LH & symptoms persist, repeat TT & baseline LH & prolactinprolactin
TT = 8 TT = 8 –– 15 15 nmolnmol/L, repeat TT & automatically reflex to /L, repeat TT & automatically reflex to SHBG if repeat is still 8 SHBG if repeat is still 8 –– 15 15 nmolnmol/L and /L and cBATcBAT (lab should (lab should provide provide cBATcBAT automatically); Baseline LH and automatically); Baseline LH and prolactinprolactin as as well well

OSCC Expert Panel Recommendations ContOSCC Expert Panel Recommendations Cont’’dd
Measured FT by analogue should Not be used in Measured FT by analogue should Not be used in diagnosis of diagnosis of hypogonadismhypogonadism; Should be replaced by ; Should be replaced by cBATcBAT using SHBG & TT (note: did not using SHBG & TT (note: did not favourfavourmBATmBAT))
Provincial governments should support the Provincial governments should support the development of IDMS reference testing laboratory development of IDMS reference testing laboratory to assure the accuracy and reliability of testosterone to assure the accuracy and reliability of testosterone assays.assays.
-- Large study in elderly men is needed to fully Large study in elderly men is needed to fully addressed challenge #2addressed challenge #2……

Summary: What to Measure & When…
Androgen excess in males & females, at any age Androgen excess in males & females, at any age -- TT TT by conventional IA by conventional IA In females, be mindful of falsely elevated results; In females, be mindful of falsely elevated results; Access to alternate direct auto IA, preAccess to alternate direct auto IA, pre--treatment treatment (extraction) with rerun, FAI/FT or BAT (extraction) with rerun, FAI/FT or BAT HypogonadalHypogonadal function in males function in males –– TT by conventional TT by conventional IA in most casesIA in most casesIf sex hormone binding globulin abnormality is If sex hormone binding globulin abnormality is suspected in suspected in hypogonadichypogonadic states, BAT and/or states, BAT and/or measured or calculated FT measured or calculated FT In preIn pre--pubertal children (males & females) and pubertal children (males & females) and normal females normal females –– TT by HPLC or Mass Spec; need to TT by HPLC or Mass Spec; need to established RIestablished RI’’ss
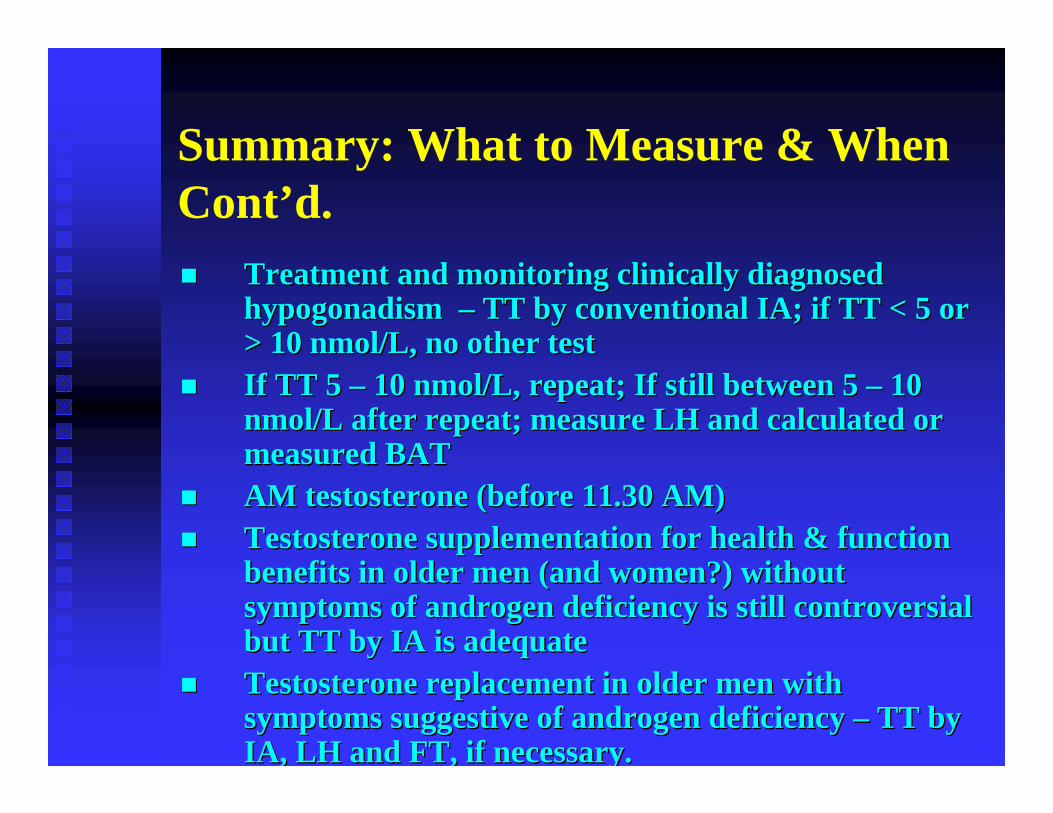
Summary: What to Measure & When Cont’d.
Treatment and monitoring clinically diagnosed Treatment and monitoring clinically diagnosed hypogonadismhypogonadism –– TT by conventional IA; if TT < 5 or TT by conventional IA; if TT < 5 or > 10 > 10 nmolnmol/L, no other test/L, no other testIf TT 5 If TT 5 –– 10 10 nmolnmol/L, repeat; If still between 5 /L, repeat; If still between 5 –– 10 10 nmolnmol/L after repeat; measure LH and calculated or /L after repeat; measure LH and calculated or measured BAT measured BAT AM testosterone (before 11.30 AM) AM testosterone (before 11.30 AM) Testosterone supplementation for health & function Testosterone supplementation for health & function benefits in older men (and women?) without benefits in older men (and women?) without symptoms of androgen deficiency is still controversial symptoms of androgen deficiency is still controversial but TT by IA is adequatebut TT by IA is adequateTestosterone replacement in older men with Testosterone replacement in older men with symptoms suggestive of androgen deficiency symptoms suggestive of androgen deficiency –– TT by TT by IA, LH and FT, if necessary.IA, LH and FT, if necessary.

AcknowledgementsAcknowledgements
Drs Chris Collier & Hilde Drs Chris Collier & Hilde VandenbergeVandenbergeTechnical and IT Staff at GDMLTechnical and IT Staff at GDMLOSCC Executive OSCC Executive Colleagues at CML & Colleagues at CML & LifeLabsLifeLabs