TEST BOOK OF C&D
67
Book Inner Pages
-
Upload
smartfront -
Category
Documents
-
view
231 -
download
1
description
Uof T Book
Transcript of TEST BOOK OF C&D

Book Inner Pages

WelcomeGreetings from the Prime MinisterGreetings from the PremierGreeting from the MayorKeynote SpeakersMeeting ProgramMaps and FloorplansTaxis & Local Organizing Committee2013-14 Faculty2013-14 Affiliate Scientists2013-14 Residents2013-14 Clinical FellowsPerspective Pieces Notes
12
1819
2021
222356
0705
0403
02
jtam
Sticky Note
Restaurants are missing
jtam
Sticky Note
would like to change the color selection in person with you

It all started with Dr. Kenneth McKenzie in 1923, and
now the Division of Neurosurgery at the University
of Toronto is pleased to announce a celebration of
90 years of neurosurgery in Canada on October 6-8,
2013 at the Royal Conservatory’s Koerner Hall in
the new TELUS Centre for Performance and
Learning, located centrally at Bay and Bloor in
downtown Toronto.
We plan an event with a homecoming theme span-
ning three days with a welcome reception on the
evening of October 6, 2013, a gala dinner on October
7, and a two-day scientific symposium on October 7
and 8 covering the major disciplines in neurosurgery.
It will be directed towards neurosurgeons,
neuroscientists, nurses, current trainees and past
alumni from around the world. This function will give
us a chance to meet, get reacquainted, review our
progress and that of our alumni, and get an appraisal
of where we are going at the University Division and
at each of our four hospitals-the Hospital for Sick
Children, St. Michael’s Hospital, Sunnybrook Hospital
and Toronto Western Hospital.
Welcome
jtam
Sticky Note
Add updated Welcome, sent by email Sep 30th, 5:41 pm
jtam
Sticky Note
Please add a (page) 1 indicator somewhere on this page.
2
jtam
Sticky Note
Update with 3 letters and 3 photos, sent Sep 30th, 5:41 pm

3
4

KEYNOTE SPEAKER
Dr. Mitch Berger
Chair, Department of Neurological SurgeryUniversity of California, San Francisco
The Evolution of Low-Grade Gliomas: From Bench to Bedside
Dr. Max Findlay
University of AlbertaChair, Scientific Committee, Canadian Society of Neurosciences
History of Neurosurgery in Toronto
Dr. Andrew Jea
Director, Neurospine ProgramTexas Children’s Hospital
Advances (and Setbacks) in Pediatric Spine Surgery
Dr. John Kestle
Head, Department of SurgeryUniversity of British Columbia
We All Make Mistakes: Finding and Fixing Them
5
jtam
Sticky Note
Try original photo files, sent Sep 30th, 5:43 pm
jtam
Sticky Note
Add S: Keynote Speakers
jtam
Sticky Note
Dr. Mitch Berger Chair, Department of Neurological Surgery University of California, San Francisco Past President, American Association of Neurological Surgeons
KEYNOTE SPEAKER
Dr. Andres Lozano
Dan Family Chair in NeurosurgeryUniversity of Toronto
Overview of Neurosurgeryat the University of Toronto
Dr. Christopher Shaffrey
Director, Spine Division, Department of Neurosurgery, University of VirginiaTitle t.b.d.
Dr. Robert Spetzler
Chair, Division of Neurological Surgery Barrow Neurological Institute
Where is Cerebrovascular Surgery Going?
Dr. Douglas Kondziolka
Vice Chair, Clinical Research, NeurosurgeryNew York University
What Have I Learned That They Did Not Teach Me in Residency
6
jtam
Sticky Note
Neurosurgery at
jtam
Sticky Note
(Title:) Advances in Spinal Surgery
jtam
Sticky Note
Department of Neurosurgery, University of Virginia (one line)
jtam
Sticky Note
Move Surgery to end of line above

SUNDAY, OCTOBER 6, 2013 TELUS Centre for Performance and Learning Koerner Hall, 273 Bloor Street West Toronto, ON M5S 1W2
1600-1830 Registration
1830-2100 Welcome Reception
MONDAY,TOBER 7, 2013 TELUS Centre for Performance and Learning Koerner Hall, 273 Bloor Street West Toronto, ON M5S 1W20700-0800 Coffee and Registration
0800-1000 Scientific Session 1 – Welcome & History Chair: Dr. Andres Lozano, Toronto Western Hospital 0800-0820 Welcome and Opening Remarks
0820-0900 KEYNOTE SPEAKERS Max Findlay, University of Alberta History of Neurosurgery in Toronto
0900-1000 Andres Lozano, Toronto Western Hospital Overview of Neurosurgery at the University of Toronto
1000-1030 Coffee
1030-1245 Scientific Session 2 – Cerebrovascular Chairs: Dr. Loch Macdonald, St. Michael’s Hospital Dr. Michael Tymianski, Toronto Western Hospital
1030-1115 KEYNOTE SPEAKER Robert Spetzler, Barrow Neurological Institute Where is Cerebrovascular Surgery Going?
PROGRAME DETAILS
7
jtam
Sticky Note
no E: Program
jtam
Sticky Note
Use bold/italics from PDF version, as discussed Sep 30th
jtam
Sticky Note
typo: OCTOBER
jtam
Sticky Note
make blue and bold
jtam
Sticky Note
indent
jtam
Sticky Note
Add 3 new speakers from file sent Sep 30th, 5:41 pm
jtam
Sticky Note
ADD TALK: Nima Etminan, 1115-1125, from PDF program
jtam
Sticky Note
Move indent to left, and keep to 2 lines, as in PDF program
jtam
Sticky Note
Move indent to left, and keep to 2 lines, as in PDF program

PROGRAME DETAILS
1125-1135 Mel Boulton, Western University Five Years After…
1135-1145 Max Findlay, University of Alberta The evolution of carotid artery repair
1145-1155 Amir Dehdashti, Northshore LIJ University Hospital Surgery of posterior circulation aneurysms in the endovascularera
1155-1205 Leo da Costa, Sunnybrook Hospital Title t.b.d.
1205-1215 Loch Macdonald, St. Michael’s Hospital Vasospasm 25 years on: What Next?
1215-1225 Michael Tymianski, Toronto Western Hospital Title t.b.d.
1225-1245 Discussion
1300-1430 Lunch Attendees are responsible for own lunch on Monday, October 7th.
1430-1620 Scientific Session 3 – Functional Chair: Dr. Andres Lozano, Toronto Western Hospital
1430-1500 KEYNOTE SPEAKER Andres Lozano, Toronto Western Hospital Emerging indications in Functional neurosurgery
1500-1510 Mojgan Hodaie, Toronto Western Hospital What Can We Learn from Tractography?
1510-1520 Robert Gross, Emory University Advances in Epilepsy
1520-1530 Taufik Valiante, Toronto Western Hospital From neurons to networks: integration through oscillation within the human brain
8
jtam
Sticky Note
No E: Program
jtam
Sticky Note
space: endovascular era
jtam
Sticky Note
jtam
Sticky Note
Start titles new lines
jtam
Sticky Note
Title on new line
jtam
Sticky Note
title from PDF program
jtam
Sticky Note
title from PDF program
jtam
Sticky Note
Capitalize all major words in titles
jtam
Sticky Note
Capitalize all major words in titles
jtam
Sticky Note
Capitalize all major words in titles
jtam
Sticky Note
Capitalize all major words in titles

1530-1600 KEYNOTE SPEAKER Douglas Kondziolka, New York University What have I learned that they did not teach me in residency
1600-1620 Discussion
1620-1830 Free Time
1830-2200 GALA DINNER Liberty Grand Toronto, Centennial Room 25 British Columbia Road, Toronto, Ontario, Canada M6K 3C3
TUESDAY, OCTOBER 8, 2013 TELUS Centre for Performance and Learning Koerner Hall, 273 Bloor Street West Toronto, ON M5S 1W2
0700-0800 Coffee and registration
0800-0940 Scientific Session 4 – Spine Chair: Dr. Michael Fehlings Toronto Western Hospital
0800-0830 KEYNOTE SPEAKER Christopher Shaffrey, University of Virginia Title t.b.d.
0830-0840 Michael Fehlings, Toronto Western Hospital New Developments in the Pathophysiology and Treatment of Cervical Myelopathy 0840-0850 Eric Massicotte, Toronto Western Hospital Minimally Invasive Surgery for Spinal Metastases
0850-0900 Mohammed Shamji, Toronto Western Hospital Novel Insights into the Pathopysiology of Spinal Neuropathic Pain
PROGRAME DETAILS
9
jtam
Sticky Note
No E: Program
jtam
Sticky Note
Capitalize all major words in titles
jtam
Sticky Note
Advances in Spinal Surgery
jtam
Sticky Note
move to one line
jtam
Sticky Note
Move indent to left, and keep to 2 lines, as in PDF program
PROGRAME DETAILS
0900-0910 Arjun Sahgal, Sunnybrook Hospital Radiosurgery for Spinal Metastases
0910-0930 Discussion
0940-1010 Coffee
1010-1240 Scientific Session 5 – Neurooncology Chairs: Dr. Mark Bernstein, Toronto Western Hospital Dr. Todd Mainprize, Sunnybrook Hospital
1010-1040 KEYNOTE SPEAKER Mitch Berger, University of California, San Francisco The evolution of low grade gliomas: from bench to bedside
1040-1050 James Rutka, Hospital for Sick Children The establishment of the Arthur and Sonia Labatt Brain Tumour Research Centre at the University of Toronto
1050-1100 Sunit Das, St. Michael’s Hospital Epigenetic drivers of heterogeneity in glioblastoma
1100-1110 Fred Gentili, Toronto Western Hospital The Management of Craniopharyngioma: the role of endonasal endoscopic techniques
1110-1120 Gelareh Zadeh, Toronto Western Hospital Review of Brain Tumor Angiogenesis and Metabolism
1120-1130 Todd Mainprize, Sunnybrook Hospital MRI-guided Focused Ultrasound to open the Blood-Brain Barrier
1130-1140 Paul Kongkham, Toronto Western Hospital An epigenetic approach to understanding brain tumour pathogenesis
1140-1150 James Balogun, Fellow, Toronto Western Hospital Neuro-Oncology in Nigeria and how it can be helped by training abroad
10
jtam
Sticky Note
Indent
jtam
Sticky Note
Capital major words in title
jtam
Sticky Note
Capital major words in title
jtam
Sticky Note
Capital major words in title
jtam
Sticky Note
Capital major words in title
jtam
Sticky Note
Capital major words in title
jtam
Sticky Note
Capital major words in title
jtam
Sticky Note
change to: Hospital for Sick Children
1150-1200 Antonio Di Ieva, Fellow, St. Michael’s Hospital Fractal geometry of gliomas
1200-1220 Discussion
1300-1430 Lunch University of Toronto Hart House, The Great Hall 7 Hart House Circle, Toronto, ON M5S 3H3
1430-1615 Scientific Session 6 – Pediatrics Chair: Dr. James Drake, Hospital for Sick Children
1430-1510 E. Bruce Hendrick Visiting Professor John Kestle, University of British Columbia We All Make Mistakes: Finding and Fixing them
1510-1530 KEYNOTE SPEAKER Andrew Jea, Baylor College of Medicine Advances (and Setbacks) in Pediatric Spine Surgery
1530-1545 Peter Dirks, Hospital for Sick Children Brain Tumour Initiating Cells
1545-1600 Michael Taylor, Hospital for Sick Children Molecular Heterogeneity Through Space and Time Drives the Clinical Behaviour of Medulloblastoma
1600-1615 Pat McDonald, University of Manitoba Mentoring in Neurosurgery - It Doesn’t End with Residency
1615 Closing Remarks
PROGRAME DETAILS
11
jtam
Sticky Note
no E: Program
jtam
Sticky Note
capitalize major words in title
TELUS Centre for Performance and LearningKoerner Hall, 273 Bloor Street WestToronto, ON M5S 1W2
MAP1
12
jtam
Sticky Note
add telephone numbers
jtam
Sticky Note
Move Koerner Hall to 1st line, with a comma
jtam
Sticky Note
make font same as other Maps & Floorplans
jtam
Sticky Note
Put a space between Map and 1, for all maps and floorplans

FLOORPLAN1TELUS Centre for Performance and Learning Koerhner Hall
13
jtam
Sticky Note
add comma after Learning
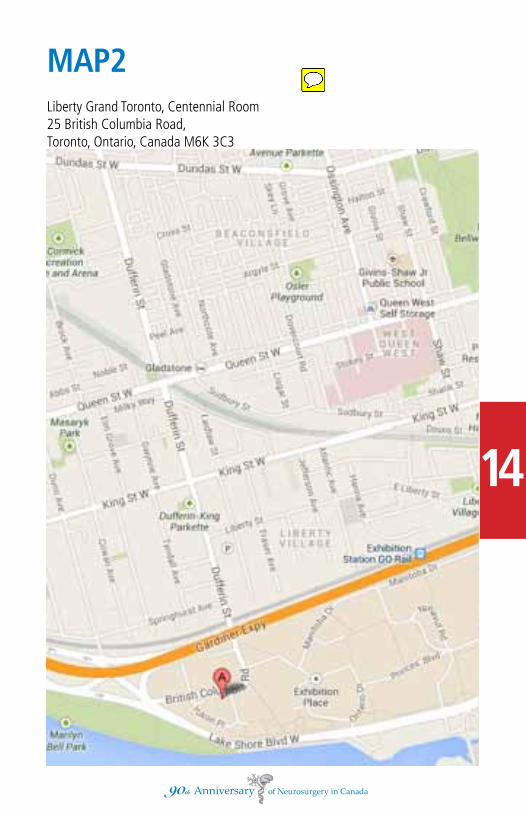
Liberty Grand Toronto, Centennial Room25 British Columbia Road, Toronto, Ontario, Canada M6K 3C3
MAP2
14
jtam
Sticky Note
add telephone numbers
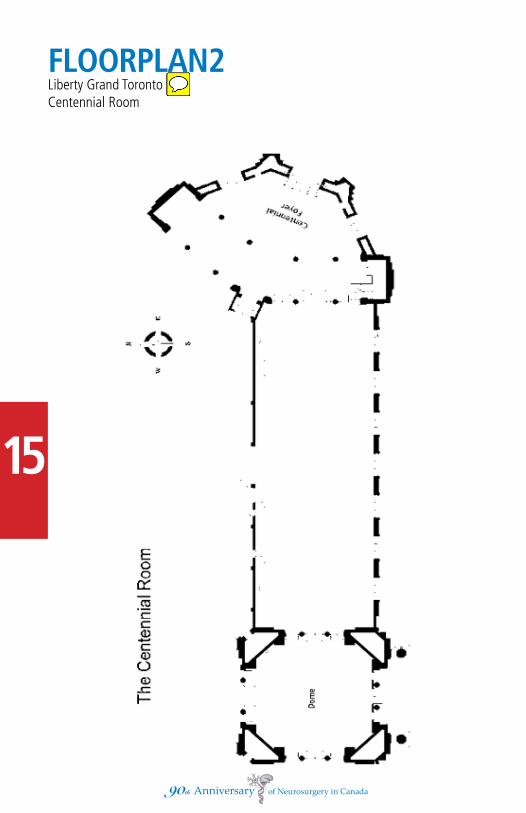
FLOORPLAN2Liberty Grand TorontoCentennial Room
15
jtam
Sticky Note
one line, with comma
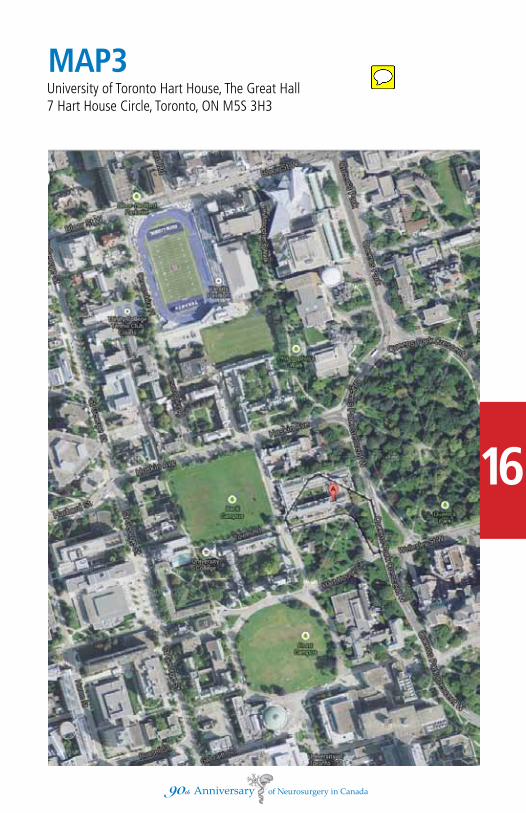
University of Toronto Hart House, The Great Hall7 Hart House Circle, Toronto, ON M5S 3H3
MAP3
16
jtam
Sticky Note
Add tel number
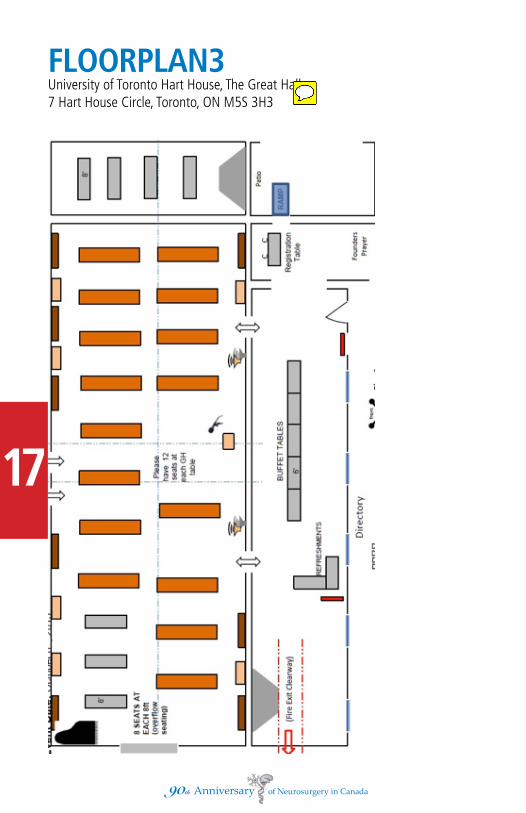
FLOORPLAN3University of Toronto Hart House, The Great Hall7 Hart House Circle, Toronto, ON M5S 3H3
17
jtam
Sticky Note
Remove 2nd line of address

Beck Taxi 416-751-5555
Co-Op Cabs 416-504-2667
Crown Taxi 416-240-0000
Diamond Taxicabs 416-366-6868
Maple Leaf Taxi 416 465-5555
Royal Taxi 416-777-9222
LOCAL ORGANIZING COMMITTEEDr. Andres Lozano (Chair) Dr. Loch MacdonaldDr. Mark Bernstein Dr. Todd MainprizeDr. James Drake Dr. Julian SpearsDr. Michael Fehlings
VOLUNTEERSSandi AmaralLauren BechardMary Ann BrowneErik FreisenDarina LandaKaren NgJoan RichardsonMadaline Perrino Shamim SumarMorgan Tilley
18
TAXI
jtam
Sticky Note
Taxis
jtam
Sticky Note
update as in file sent Sep 30th, 5:41 pm
jtam
Sticky Note
Remove Morgan Tilley

19
Neu
rosu
rgery
Facu
lty
20
Neu
rosu
rgery
Affi
late
Sci
en
tist
s

21
Neu
rosu
rgery
Resi
den
ts
22
Neu
rosu
rgery
Resi
den
ts

PERSPECTIVE PIECES
Dr. Ross Fleming 24
Dr. Alan Hudson 27
Dr. Bernard Schacter 28
Dr. Hart Schutz 29
Dr. Michael Schwartz 30
Dr. Ronald Tasker 32
Dr. William Tucker 38
Dr. Graham Vanderlinden 40
23
jtam
Sticky Note
Add Dr. Humphrey's here, and in his piece, add "Emeritus Professor, University of Toronto" under his name.
jtam
Sticky Note
Dr. R. Graham Vanderlinden
Dr. Ross Fleming
1.What got you interested in neurosurgery?
It began with the excellent, detailed and intensive undergraduate courses in basic sciences, neuroanatomy, neurophysiology, pathology and physiology, which occupied a much larger portion of the curriculum than today, and in clinical neurology and neurosurgery. (as a student I wrote a paper for the student medical journal on the unconscious patient)
The most important influence was my one month rotation as a ’junior intern’ on neurosurgery (probably similar to a clerkship elective today). The senior resident Dr. Eben Alexander provided outstanding mentorship, and both staff members, Dr. Kenneth Mackenzie and Dr. Harry Botterell provided very enthusiastic teaching and encouragement, took a personal interest in me, and gave me a considerable amount
2.Why did you choose to train in neurosurgery at the University of Toronto?
In 1947, Toronto was the only neurosurgical training program in Ontario. I believe that the only other program in Canada was McGill. The Toronto program had an excellent reputation thanks to Kenneth McKenzie, and become the hub from which neurosurgeons settled in various Canadian and American cities. At any rate, my roots and family were in Toronto, and Dr. Botterell (then Chief of Neurosurgery) encouraged me to enroll in the Toronto program.
3.What was the neurosurgery residency application and selection process for you?
There was no formal application or selection process. I believe that selection of candidates was done entirely by the Chairman of Neurosurgery (Dr. Botterell) together with the Chairman of Surgery (Dr. Janes) in consultation with other faculty members.
4.How did you come to work at the University of Toronto, Division of Neurosurgery as a faculty, and what was the hiring process?
By the time I had completed my training in 1956, neurosurgical programs had been established in more Canadian and American centres. 24
jtam
Sticky Note
Add "Emeritus Professor, University of Toronto" under his name.

I had four job offers, three Canadian and one American. However, I had recently married, and my wife did not want to move from Toronto or from her family. I had an excellent offer at the Toronto Western Hospital, which I happily accepted. .5.What have you seen as the most important advances between the time you were a resident and now?
1. The development of structured residency training programs with well de-signed, structured curriculum and rigorous evaluation, has been a huge advance. When I trained, there was no set curriculum, and much of the training was rather random and was based on the apprenticeship model. Didactic learning, apart from clinical teaching at the bedside or in the operating room, was from medi-cal journals, textbooks, rounds and an occasional conference. The chief resident was exposed to a huge and varied clinical volume 24/7, as he was not expected to take any time off, and usually lived in the hospital. Today’s residents enjoy a much more balanced life, although they lack the benefits of the hyper-intense exposure of the 1950’s.
2. Evidence-based medicine has been a very important advance. It was non-existent during my residency, and clinical decisions were all too often based on anecdotal evidence and personal preference.
3. Imaging techniques and the establishment of neuro radiology. When I was res-ident, diagnosis and localization relied heavily on clinical evaluation, supplement-ed by ventriculograms, pneumo-encephalograms, and arteriograms performed by direct carotid artery puncture by a resident. We have come a long way.
4. Sub-specialization within neurosurgery has been an important advance, and has encouraged greatly improved expertise in each sub-specialty, with establish-ment of a critical mass of clinicians and scientists to focus in each area.
5. Information technology. Medical literature was accessed by trips to libraries or bookstores. Research data were compiled manually, or sometimes by inserting a knitting needle through holes in punch cards. It is hard to believe that all medical records were on paper, hand written or typed, filed and retrieved by hand. A hospital-wide loud speaker system was used to ‘page’ hospital personnel and residents. Telephone communication depended entirely on switchboard operators.
6. Bioethics. Rarely mentioned and little understood when I was a resident, bioethical knowledge and consideration of ethical issues are now rightfully 25

7. Molecular biology. At the time of my residency, understanding of disease depended on gross and light microscopic pathology, test tube biochemistry and high school level Mendelian genetics. The huge field of molecular biology has grown exponentially and enormously increased our understanding of disease. 8.Technical developments in the operating room have been far too many to enumerate.
6.What was the most memorable event in your residency?
I’m thinking!!
7.What advice do you have for our residents and young faculty as they embark on their career as neurosurgeons?
I don’t like to give gratuitous advice. There are two practices that have always been fundamentally important to me:
• Always think creatively, look afresh at what you have always taken for granted. “Hang a question mark on the things you have normally taken for granted” (Bertrand Russell). If a patient or medical report provides a diagnosis, question it. Start by believing it to be incorrect, then take steps to prove it right or wrong. Always, always ask questions.
• “Listen to your patient, he/she is telling you the diagnosis” (Osler). It takes time and patience, but is absolutely fundamental to all clinical encounters. It is best to sit down beside the patient, even if briefly, and look at him/her and listen attentively, rather than standing, looking down and being perceived as being in a hurry. This maneuver will pay huge dividends to the outcome. Imaging and other diagnostic facilities are not a substitute for good conversations with patients and their families.
Dr. Ross Fleming
26

Dr. Alan Hudson1. I had completed my General Surgical Fellowship in England and applied from there for further General Surgical training in Toronto. To my great surprise, I received a telegram stating I had been accepted on Neurosurgical training pro-gram, to which I had not applied. 2. See 1. Had decided not to go back to South Africa, and Susan was Canadian, from Ontario. 3. See 1. No selection process, but I had my FRCS in Gen Surg., at age of 24. 4. I was first of “second stream” trainees i.e. I would not finish as senior resident at TGH. Bill Horsey, SiC of St Michaels, offered me job when I was senior resident at St Michaels. I was first hired in new plan i.e. my office in the hospital, not in a private building elsewhere. (1970). OHIP had just been introduced. I presume Horsey discussed this with Morley, but I did not. 5. Without question, CT and MRI. I trained without these tools. 6. (a) A man carried his young wife into emerge. Excruciating back pain. Diagno-sis was ruptured disc. I examined her and could not feel her femoral pulses. I listened to her heart and heard nothing abnormal. Turned her l side down and got her to exhale. Could just hear the mid diastolic rumble. Diagnosed mitral stenosis with saddle embolus. Vascular surgeons took out the embolus and she made full recovery. That was in 1963 and I can still remember what patient and husband looked like.- one of few occasions I thought I had actually made a dif-ference. (b) Opening the envelope at the end of the oral exams at the Western, and finding I had managed to bluff the examiners. 7. There is absolutely no substitute for experience. There are no short cuts. Work flat out for first five years of your faculty appointment, so your knowledge can mature to wisdom. As you love what you are doing, you should have a lot of fun. If you don’t love the opportunity, you are in the wrong job and should find something else to do.
- Dr. Alan Hudson
27
jtam
Sticky Note
Add "Emeritus Professor, University of Toronto" under his name. Add "Past Chair, Division of Neurosurgery, University of Toronto"
jtam
Sticky Note
MD, FRCSC, CM

Dr. Bernard Schacter1. What got you interested in neurosurgery?
I had exposure to a few neurosurgical cases and operations during my general surgery residency and this is what resulted in my interest in neurosurgery. The other part of that was that in those years there were no specific definitive diagnostic studies such as CT’s or MRFs and one had to arrive at the diagnoses with mainly clinical assessments and rather primitive ventriculograms, oil myelograms and direct puncture arteriograms which only provided a few films to review. This was more interesting and challenging than seeing a patient with an x-ray diagnosis made for you to treat.
2. Why did you choose to train in neurosurgery at the University ofToronto?
My neurosurgical training was in Brooklyn, New York under Dr. E. Jefferson Browder. Our affiliation was with the Downstate Medical College of New York.
3. What was the neurosurgery residency application and selection process for you?
I applied directly to Dr. Browder having almost completed a 4 year general surgical residency program. I was interviewed by Dr. Browder and following interview he said that I was accepted to start the program that July.
4. How did you come to work at the University ofToronto, Division ofNeurosurgery as a faculty and what was the hiring process?
Following my residency program I returned to the New Mount Sinai Hospital in Toronto and was working as a neurosurgeon at that hospital. I was invited to join the University ofToronto,Division of Neurosurgery by Dr. T.P. Morley once he became the Head of Division of Neurosurgery.
- Dr. Bernard Schacter
28
jtam
Sticky Note
Add "Emeritus Professor, University of Toronto" under his name.
Dr. Hart Schutz
The first question was what got me interested in neurosurgery and why did I chose to train in neurosurgery at the University of Toronto. My original interest was in orthopedic surgery but I was ‘forced’ to take neurosurgery and came under the influence of Dr. Lougheed. He was at the front of microvascular surgery at the time and neurosurgery seemed to be very exciting. Because of him (and Dr. Morley), I switched to neurosurgery.
My residency application and selection process was extremely simple and was accomplished with a stroke of a pen by Dr. Morley.
You also asked me why I came to work at the University of Toronto and the na-ture of the hiring process. In 1970, there was considerable expansion of both the East and the West of the City. Dr. Hudson went east and I went west. 1 covered Mississauga, Brampton and Oakville but brought all surgeries to the Toronto Western Hospital. That seemed to work until 1987. The Ministry of Health de-cided to initiate a Department of Neurosurgery at Trillium. At that time, I switched to Mississauga on a full-time basis.
You also asked what are the most important advances from the time I was a resi-dent to now. These advances would be (mainly) in the field of radiology. The MRJ scan, CT scan and interventional treatment of aneurysms are major advances. Other advances include electrophysiological monitoring during acoustic surgery. Of course, there are other important advances including much better anesthesia and improved surgery techniques.
What was my most memorable event in my residency? I can unequivocally say that my first solo clipping of an aneurysm which was a middle cerebral artery aneurysm (as a resident), was the most memorable event. The terror and excite-ment of the clipping is still a ‘stand out’ in my memory.
What advice would I give residents and young faculty as they embark ontheir career as neurosurgeons? I would strongly encourage them to develop and main-tain a level of critical thinking in everything they do. They should remain humble and they must realize they cannot cure everybody. To follow your patients foras long as possible is also a great educational experience.
- Dr. Hart Schutz
29
jtam
Sticky Note
MD, FRCSC, FACS
jtam
Sticky Note
Add "Neurosurgeon, Trillium Health Centre" under his name
Dr. Michael Schwartz
I was in medical school in the era before CT and MRI scanning, when investigation of nervous system disorders with imaging was invasive and when, of necessity, one usually made diagnoses at the bedside without recourse to lab tests. I thought it was exciting to look at, talk to, and instruct patients to do a few things and arrive at a diagnosis, or at least a short differential, with fair certainty after only a few minutes. Our bedside clinical group was very medically (as opposed to surgically) oriented. I believed, like my clinic mates, that surgeons were a bit like trained animals and had no particular interest in becoming a surgeon. In second or third year, we had Jack Silversides as our bedside clinician. As you know, he was a charismatic individual and we all admired his panache and the facility with which he could make sense of the patients’ signs and symptoms. In fact, 3 of 8 members of our group went on to do neurological specialties: Peter Carlen to do neurology and research, and Terry Picton to do neurophysiology and research, and I to do neurosurgery. In fourth year, when I was a clinical clerk on obstetrics and gynecology, I delivered babies in an operating room-like setting. It was the first time that I was doing the work and not assisting. It occurred to me that I had always used tools and enjoyed working in my father’s basement workshop, building and fixing things. It seemed logical: I liked clinical neurology, I liked surgery, I would do neurosurgery. At that point I had never actually worked on a neurosurgical service. In fourth year, I had one week at the General on Tom Morley’s service. Bill Lougheed and Ron Tasker were on staff. Jacques Francoeur was the resident. I thought neurosurgery was great. The next year during my rotating internship, which included a 2 month elective in medical neurology with Guy Courtois and André Barbeau, I applied to do my training in neurosurgery. A naïve way to decide, but it worked.
During my internship at the Hôtel-Dieu de Montréal, I decided to stay in Montreal and applied for the first year of surgical training at the Montreal General Hospital. I figured that I would then do neurosurgery at either McGill or the U of M. I had met Claude Bertrand during my intern year and found him very impres-sive. I was accepted, but about that time, there was a strike of Quebec radiolo-gists. There was little good will between the profession and the government. lt appeared that there would be work disruptions over the next several years that would interfere with my training, so I applied to Toronto.
To apply, I wrote letters to Tom Morley and to Bob Mustard, who was the director of the Gallie course, the postgraduate training course in surgery. Dr. Mustard had been one of my bedside clinical teachers and knew me.
30
jtam
Sticky Note
Add "Past Head, Division of Neurosurgery, Sunnybrook Hospital"
I recall getting some letters of reference from clinicians at the Hôtel-Dieu and I must have filled out some forms, but I never came for an interview.
During my training at U of T, I met Berney Schacter who was looking for a partner. Don Wilson, who was then the chairman of surgery, decided that I should be appointed to both the Mount Sinai and the Toronto General Hospital. And so I was. There was definitely no MOA or other formal requirement that I had to meet. After 4 years, I joined Charles Tator and Dave Rowed at Sunnybrook. For general neurosurgery, the most important advances have been cross-sectional imaging: CT and MRI scanning. These developments have made it possible to have non-invasive, detailed information prior to operating. Coupled with image-guidance systems, better imaging has made procedures shorter and safer. It has also made it clearer when not to operate. Postoperative imaging now offers a no-nonsense assessment of how the surgery really went. For example, there is no longer any doubt about how much of a tumor was removed or whether there is still a herniated disc fragment. One specialized aspect of neurosurgery that I consider important is radiosurgery which has evolved into a major modality in the treatment of arteriovenous malformations (AVMs) and small tumors. Deep AVMs may beaddressed with low morbidity and superficial AVMs may be treated in people who are unfit for or prefer not to have open surgery. Focused ultrasound is just coming on the scene and I predict that it will be useful for functional neurosurgery and possibly for opening the blood brain barrier in the treatment of tumors.
The most memorable event for me involves the advent of CT scanning. I was the senior resident at the Toronto General Hospital in 1974 when they acquired the first CT scanner in Toronto. I participated in the first operation on a person who was scanned and then operated. Prior to CT scanning you could see some brain tumors with low resolution nuclide scans, or after angiography if they were sufficiently vascular for the tumor vessels to show. If not, you had to imagine where the tumor was by seeing the displacement of nearby brain blood vessels. I recall that the patient had a butterfly glioma. The pixels in the early scans were as big as a checker board, but you could clearly see where the tumor was. I recall looking down between the cerebral hemispheres at operation and seeing the tumor. I knew at that moment that I was standing in a whole new era.
The first bit of advice is to look after your patients as carefully and thoughtfully as you can. Try to offer evidence-based management and if there is no evidence base, try to contribute new information. A dual career in basic science and clinical31
practice is unrealistic for almost all of us, but there is plenty of scope for care-ful evaluation of outcomes and critical scrutiny of your own work. Choose a “mini-career” within neurosurgery that particularly interests you and change your mini-career from time to time. Allow sufficient time for your family and outside activities and most of all, have fun.
- Dr. Michael Schwartz
Dr. Ronald TaskerRecollections of Neurosurgical Training in Toronto in the 1950s by R.R. Tasker
My paternal grandmother’s family, the Taylors, immigrated to a farm in Vaughan, north of Toronto, from Staffordshire in the UK in the 19th century but they moved to East York to take advantage of the water power for mills on the Don River. My father, who graduated from SPS in 1913 and worked as a fire protection engineer, whose mother was a Taylor, lived at 57 Duke Street in what was then York and every summer as a boy he went to the Don River area, stayed with the Taylors who lived on Beechwood Crescent on the brink ofthe Don Valley. When my parents married, they first lived inEast Yorkin alittle house on Peplar Avenue, later moving to Rivercourt Boulevard. My father then bought a larger piece of property at the corner of Don Mills Road and Broadview Avenue, currently O’Connor Drive and Broadview Avenue, where he built a larger house; I presume he had bought this property from his mother’s estate. He also inherited other real estate in the area from her and this is where I grew up. I could walk out the back door ofour house, down a trail to the Don River flats below and explore the DonValley on foot, a wonderful experience in those days before the Don Valley Parkway. As a result, I became infatuated with natural history and spent every spare moment exploring the Don Valley. I gather that my father in his day had had much the same experience and he showed me everything he could about the area. I attended East York Collegiate and really had no thought of ever entering Medicine. I was more interested in natural history. My mother, however, who was a legal secretary to a criminal lawyer felt strongly that I should enter medicine and as a compromise I went into Physiology and Biochemistry (P and Bclass of4T8 at Victoria College in Honour Science). While there, I met Dr. Bruce Falls, later vice-chair of Zoology, Dr. Jack Price,who later went to live in Trinidad 32
jtam
Sticky Note
Add "Emeritus Professor, University of Toronto" under his name.
jtam
Sticky Note
MD, MA, FRCSC, CM
33
and who worked at the Trinidad Virus Laboratory, Dr.John Speakman, later an ophthalmologist, and a number of others like the artist, Bob Bateman, all of whom greatly expanded my knowledge of and interest in biology. However, the chairman of Physiology was Dr. Charles Herbert Best, co-discoverer of insulin, who convinced me that, if I was interested in Physiology, it would be necessaryto go into medicine, which is, after all, applied Physiology; otherwise I could find a job only as a lab technician. I was familiar with Dr. Best as I saw him frequently on campus in the 1940’s resplendent in his Naval Captain’s uniform. This was wartime and he was supervising naval medical research. I entered P and B (Physiology Option) and was delighted to obtain a summer job in my first and second years in trout biology at the Ontario Fisheries Research Laboratory at Opeongo Lake in Algonquin Park run by Dr. Fred Fry which is known nowadays as the Harkness Laboratory. Fry was considered by Harold Atwood (subsequent Chairman of Physiology) who was the brother of Margaret Atwood, son of Dr. Karl Atwood, the Professor of Forest Entomology, to be the most significant Canadian biologist in those days. In my third year in Honour Science I was hired by the Ontario Department of Lands and Forests in limnology working in Northern Ontario. I found this very exciting because the country was so large, Ienjoyed northern Ontario more than Idid Algonquin Park, and I was on my own and able to travel widely in Ontario. Dr. Best convinced me that, if I was inter-ested in Physiology, I should enter Medicine.However, we could not afford the exorbitant East York Township taxes and university fees as well. I therefore had to depend on Greek and Latin scholarships, with Mathematics thrown, in to pay my way, working in the summer in the Banting and Best Department of Medical Research on the fifth floor ofthe Banting Institute under Dr. W. Stanley Hartroft on the effects ofcholine on intestinal fat absorption. Iwas swept offmy feet by the resulting associations with scientists and visitors at the Banting and Best. But I followed Dr. Best’s advice and entered Medicine (Class of 5T2) moving into the old interns’ residence onthe fourth floor of the College Street Wing of the Toronto General Hospital. Iwas 21-years-old. Among my first memories of this era was the sound ofthe Toronto City Hall Clock tolling endlessly through the night, never heard when I lived in East York. At first I thought that internal medicine run by such powerhouses as Dr. K.J.R. Wightnan and Ray Farquharson would be the best avenue to engage my interests in Physiology but soon changed my mind and switched to the postgraduate course in surgery. So many ofthe inpatients in internal medicine in those days died in hospital. Every fall, the medical wards would clear out the typhoid cases that had accumulated during the summer in readiness to replace them with patients with pneumococcal pneumonia. Effective treatment was too far in the future for such diseases as lymphoma, renal failure,and many other common medical conditions, and I came to the conclusion that neurosurgery was probably amore promising example of applied physiology
34
for me. I finally graduated from medicine in 1952 and received the FRCSC in neurosurgery and in general surgery in 1959 (as was the custom in those days) and joined the neurosurgery staff of the Toronto General Hospital. In myearly years on staff I would occasionally be called upon to help in the operating room at the Hospital for Sick Children. One day, a child developed cardiac arrest while being anaesthetized and I had nothing better to offer than to open the chest and massage the heart manually without benefit of gloves before the days of CPR. Another day, while making rounds on Ward C, the Cardiovascular Surgery Unit, at the Toronto General Hospital, a patient suddenly developed respiratory arrest and I had to carry out an emergency tracheotomy under local anesthetic using the ward’s emergency tracheotomy kit assisted by award nurse with a flashlight. But eventually I was finished, and sheepishly met with Dr. Botterell; I was too shy to ask for a job. In Toronto, I worked with Professor Dostrovsky and his staff in Neurophysiology whose contribution was inestimable. We would explore the appropriate part ofthe human brain prior to making astereotactic lesion or inserting a chronic stimulating electrode using serial micro stimulation or microelectrode recording. This would not only be necessary for the operation but also give us information concerning brain function.
I consulted Harry Botterell, chief of neurosurgery at the Toronto General Hospital. It was 1953 and UofT surgery was still recovering from the fact that so many of the staff had just returned from active service overseas. Ihad no military experi-ence except the East York Cadet Corps where I got on the rifle team, and joined the signal corps learning to use flags and Morse Code. He ran the Neurosurgi-cal Service like the army. Each member working in his particular assigned area would he expected to carry out clinical research and report it at national and international meetings publishing as the occasion offered. Harry was particularly interested in rehabilitation, particularly of the spinal cord-injured, starting with Lieutenant Counsell who had been wounded at Dieppe. He worked closely with Dr. Albin Jousse, physiatrist, starting what would become the Canadian Paraplegic Association. Thomas Paterson Morley who had served inthe RAF in India during the War was recruited from the UK through Harry’s friend Sir Geoffrey Jefferson. Dr. William Lougheed, who had already joined the Neurosur-gical Unit at the Toronto General Hospital, introduced hypothermia to facilitate the surgery for ruptured berry aneurysms after working with William Bigelow in cardiovascular surgery on Ward C TGH; his pet dog was called “Thermy” for hypothermia. Dr. Botterell understood my interest in neurosurgery as applied neurophysiology and arranged for me to pursue atravelling fellowship under Clinton Woolsey at the Laboratory of Neurophysiology in Madison, Wisconsin. Wisconsin, on the edge of the prairies, was a wonderful place for a Toronto naturalist to live for a year. Woolsey was famous for “figurine mapping” to
35
illustrate the physiological results of experiments on the cerebral cortex ofani-mals. Iworked with him and his staffhelping to study the organization ofthe cerebral cortex, in a number of species including red panda, chimpanzee and opossum; by mapping and comparing the motor results ofcerebrocortical mac-rostimulation. He would macro-stimulate at threshold and observe the motor responses. The latter would be plotted on a photograph ofthe cerebral cortex showing each response at the same site as that at which the stimulation was applied in the form ofa body outline with the responding area shaded in. The type of shading would indicate the threshold required to bring about aresponse and small symbols were used to indicate the type of response. Much ofthis work in the laboratory was done with macrostimulation of the exposed cerebral cortex recording and documenting the resulting motor effects. By comparing different species, the organization ofthe cortex could be better understood. Maps had always fascinated meand Woolsey convinced me that figurine mapping could also be used in man in stereotactic surgery and micro-electrode recording.The following year Botterell arranged asecond travelling fellowship in Europe for me where I visited neurosurgical centres that were doing stereotactic and functional (physiological) neurosurgery.
We began in London, England where we rented an apartment in Chelsea for six months so as to access the various London hospitals where neurosurgery was being done. Interest here, however, was greater in the surgery ofaneurysms and tumours than it was in stereotactic surgery. We went on to Paris where we stayed with friends and visited neurosurgical units who were carrying out stereotactic and functional neurosurgery such as those of Gerard Guiot and Jean Talairach. A significant problem while in Paris was to find aparking place each day close to the operating room on the Isle de la Cite in which these scientists worked. Guiot worked in the Hopital Foch in Suresnes. From Paris we went on to Freiburg where Traugott Riechert and Rolf Hassler were very active, to Stockholm to see Lars Leksell and to Barcelona with their odd operating room hours in the last days ofthe Franco Regime.The plan was that following the two travelling fellowships, Iwould return to Toronto to set up functional and stereotactic neurosurgery there. At the time I returned to Toronto in September 1961, the only functional neurosurgery being done in Toronto was open cordotomy, open proceduresfor tic douloureux, open lobotomy and the occasional pallidotomy to control Parkinsonian tremor. In Toronto, pallidotomies were done under local anesthesia through burr holes using surface-landmarks to start and then macrostimulation. One would avoid sites where the stimulation produced tetanization and seek those where it produced tremor arrest. A radiofrequency lesion would then be made. Harry’s plan was to have each staff person heavily involved in a particularproject and then present the results at national and international conferences
36
publishing the results project and then present the results at national and inter-national conferences publishing the results project and then present the results at national and international conferences publishing the results appropriately. However, Harry was well aware ofthe social necessities of the Neurosurgical Service. He considered it very important to have close associations between the various staff, an example ofwhich was the annual Christmas party held in “DOR”, the neurosurgical operating room; AOR and BOR were for General Surgery,COR Cardiovascular Surgery. The neurosurgical secretary, Annie Pyke, who suffered from fragilitas ossium saw to it that the department was run the way Harry and she wanted, using social techniques that kept people together. Hence the DOR Christmas party with the spectacular invitations constructed by Margot MacKay of the Art as applied to Medicine Department was held annually in the operat-ing room. Eventually the party conflicted with the need for OR space and could not be continued. Currently, prospective and actual neurosurgical house staffin Toronto must initially be involved in one or more demanding research projects before starting neurosurgery but in the 1950s the rules were not so strict. In the old days House staffwould be expected to make very careful rounds before the operating room opened at 8a.m. identifying and dealing with any gross prob-lems that arose. As far as the actual surgery went, depending on the difficulty of the case, the skill with no OHIP, the house staffwould position and prepare the patients, open certain cases and carry out various parts ofthe operations. When the day’s list was complete everybody would make rounds together.In emergency situations performed in the middle of the night or at other inopportune times the house staff might carry out more ofthe procedure if it was not too demanding,especially burr holes to look for hemorrhage.Potential psychosurgery patients were referred bythe psychiatrists at the Toronto Psychiatric Hospital for open lencotomy - two cases every Tuesday. The only stereotactic cases that were done were for Parkinsonian tremor under local anesthesia through burr holes using pneumoencephalograms for localization. Sites thought to lie in the globus pallidus were sought and macrostimulation carried out. Vigorous stimulation-induced tremor arrest was considered apositive indication for a radiofrequency lesion site. Sites where tetanization occurred were strictly avoided as one would expect. Botterell, Morley and Lougheed worked well together as ateam. Mackenzie, Canada’s first neurosurgeon, who had had to hold the unit together during the war when everybody else was overseas, was still working in the unit. Perhaps Botterell was atouch jealous of his seniority and I don’t think that he was close to Penfield. I remember Penfield’s flying visit to Toronto on one occasion to see one of Harry’s “private” cases when Harry was out of town for one or two days and the family called Penfield in. I continued to enjoy my hobbies. I had the satisfaction from my work in northern Ontario of seeing the Kesagami River/Lake Complex, where Iwas sent to do astream /lake

37
survey at the request of others who were interested in setting up acommercial fishery there, become aprovincial park. I think their request was denied after myreport was sent in. I developed a rather strange interest in acquiring land of natural history significance. I ended up with a piece of land in the Happy Valley Forest in King Township in Ontario, the finest piece of forest in the Toronto area on which we have given the Nature Conservatory of Canada, a Nature easement, another with 16,160 ft of shoreline on the south shore of Manitoulin Island which contains various rare wildflowers and which has been recognized as part of an “Important Bird Area.” We have turned over the largest part of this land to the Nature Conservancy of Canada. In the fall of 1961,1 joined the neurosurgical staff ofthe Toronto General Hospital, now the University Health Network I implemented Harry’s plan to initiate and develop stereotactic and functional neurosurgery at the Toronto General Hospital using the experience gained in Madison and Europe. Ienlisted the help of Professor Jonathan Dostrovsky, Dr. Leslie Organ, Dr. Peter Hawrylyshyn, and their staff in Neurophysiology at the University ofToronto, to set up computerized microelectrode figurine mapping of deep brain structures during certain neurosurgical procedures allowing study of the physiology ofthe area being operated upon at the same time as using the collected material for physiological localization for the surgery.
- Dr. Ronald Tasker
38
Dr. William Tucker
1. As a senior medical student, I enjoyed the precision of clinical diagnosis that was seen in neurology, and was thinking about a career in medical neurology.
Over the summer following 3rd year in medical school, I had a job at Princess Margaret Hospital, supported by the Ivan Smith Memorial Scholarship. I was mentored by Dr John Simpson, who did most of the neuro-oncology at PMH at the time, and I reviewed the PMH experience with craniopharyngiomas and pinealomas. Not surprisingly, I noted that the individuals making most of the decisions and actually treating these patients were neurosurgeons, not neurologists. Being by nature fairly aggressive, and interested in playing a useful active role in the care of patients, I was drawn to neurosurgery, which provided the intellectual stimulation of clinical neurology, along withe the opportunity to really alter the course of patients.
2. I was actually thinking about doing a year or two of general practice locum, likely in a smaller community, to hone my general medical skills and pay off a small student debt. However, while doing a stint on neurosurgery at Toronto Western Hospital during the rotating interneship, I told the senior resident, Hart Schutz, of my plan to eventually apply to train in neurosurgery. Hart told Ross Fleming, Head of the TWH division at the time, who stressed that the training was long, and should be started as soon as possible. Ross agreed to recommend me to Tom Morley, the Chair at the time, though applications and interviews were apparently finished already for that year. I felt that an opportunity like this might not be available when I was ready, so I accepted Ross Fleming’s offer of support, met with Tom Morley, and was accepted at once into the program.
3. This question has been answered with 2, above.
4. Alan Hudson and Bill Horsey were the only two neurosurgeons at St Michael’s Hospital as I approached the end of my training. Alan in particular was anxious to have another colleague, to permit more time for academic and life-style pursuits, and he asked me if I’d be interested. This was before I had worked at St Michael’s, so Alan must have been going on hearsay. As I was interested, Alan persuaded Bill Horsey, later, while I was senior resident in neurosurgery at St Michael’s, to hire me. As Bill was Chief Surgeon, and Chief of Neurosurgery at St Michael’s then, and also Chair of the Hospital’s Medical Advisory Board, this was seemingly readily arranged. As I was not willing to spend more than a year doing some basic research before beginning, there was some resistance from faculty
jtam
Sticky Note
Add in the questions from the 1st piece (Ross Fleming)
jtam
Sticky Note
Add "Emeritus Professor, University of Toronto" under his name.

39
at other sites in the University Division, but any obstacles were overcome, and the appointment proceeded.
5. The advent of CT and MRI scans have vastly improved the accuracy of diagnosis and the care of patients. Interventional approaches, especially to aneurysms, has also vastly improved care. Stereotaxic guidance, though probably overused, has certainly permitted more accurate procedures through smaller, precisely placed exposures. Spinal instrumentation has improved the efficacy of a range of spinal procedures. Perhaps the single biggest change has been the development of sub-specialty interests and practices in neurosurgery. This has increased academic productivity and almost certainly improved the quality of patient care.
6. I don’t have a ‘most memorable event’. There were numerous wonderful experiences. In general, I most appreciated the independence I was given, particularly as a senior resident, to operate without direct supervision. The present societal and legal atmosphere simply does not allow comparable opportunities today.
7. I am very concerned that we may be training too many neurosurgeons for the treatment resources available in Canada. I would encourage our residents and young faculty to develop sub-specialist interests, that will enhance their academic and clinical careers and help make them indispensable assets. I would also encourage our senior colleagues to reduce their clinical activity more willingly and earlier, to allow opportunities for the younger neurosugeons. That is in the best interest of the profession and society, in my view.
- Dr. William Tucker
40
Dr. Graham Vanderlinden
1.What got you interested in Neurosurgery?
obtained my M.D. degree from the University of Manitoba in 1957 and did the requisite rotating internship at the Winnipeg General Hospital. Dr. Dwight Parkinson was head of the Division of Neurosurgery and on the first day of the service, December 1, 1956 I was scheduled to be his only assistant at a craniotomy. Little did I realize at the time but this case was destined to make medical history. The patient had a ® Carotid-cavernous fistula and in an effort to relieve his symptoms, Dr. Parkinson had previously ligated both external carotid arteries and the right internal carotid in the neck. This operation was intended to clip the internal carotid artery intracranially and my job was to step on the Bovie pedal and provide as much assistance as my state of ignorance allowed. The tension in the O.R was palpable. DR. Parkinson had the reputation for being a meticulous, demanding, no- nonsense surgeon who was tyrannical in the OR and did not compromise his rigourous standards. His bearing was that of a drill sergeant with a straight back, a straight mouth and a military brush cut. His main hobby, however, was figure skating and through hard work and discipline he was excellent in the sport.
The operation went well apart from much bleeding. When the skull was exposed blood spurted out and arched onto the floor a couple of feet away. I was amazed and terrified but Dr. Parkinson must have controlled the blood bathe with bone wax and proceeded to put in the burr holes with a Hudson brace. The exposed dura resembled a basket of grapes for all the dural vessels were engorged like hemorrhoids. Finally the dura was opened and Dr. Parkinson began the careful dissection along the floor of the frontal fossa. I was unable to see anything but when he finally applied the clip he jumped up and down shouting “I did it, I did it, I did it”
The patient survived the surgery, the bruit and the exophthalmous subsided and it seemed as if the operation was successful for a couple of years. Unfortunately he was not cured and all the symptoms recurred. Dr. Parkinson faced this disappointment with determination and sought the answer in the anatomy lab where he dissected out 200 cavernous sinuses and discovered the area in thelateral wall of the sinus that could be safely opened and the fistula clipped directly. That safety zone became known as Parkinson’s triangle and about four years later he operated again under hypothermia and cardiac arrest and successfully cured the patient. The patient survived initially but died later from complications of the hypothermia.
jtam
Sticky Note
Dr. R. Graham Vanderlinden
jtam
Sticky Note
Neurosurgeon, Trillium Health Centre
41
Hugh Cameron was the second Neurosurgeon at the W.G.H. and his personality was the opposite to that of Dr. Parkinson. He was pleasant, easy going and af-fable but he wasn’t as deft and meticulous a surgeon either. A pretty 22 year old woman was referred to Dr. Cameron by an ophthalmologist because of papilledema. I can’t remember what studies were done but Dr. Cameron decided that she must have hydrocephalus and I helped him do a posterior fossa crani-otomy with the patient in the prone position. The cysterna magna seemed to be under pressure and when the arachnoid was opened the intracranial pressure was relieved. Dr. Cameron attempted to do a Torkildsen shunt but the technology was so crude that we only had a straight red rubber catheter with a wire stylet to insert into the ventricle. Dr. Cameron couldn’t get the stylet out and he asked me to try and I couldn’t retrieve it either. By this time he thought that the cysterna magna was really a congenital cyst and that by deflating the ‘cyst’ he had treated the cause of the raised intracranial pressure. He abandoned the idea of inserting a shunt idea, removed the catheter and we closed the wound. Later that evening I was talking to Dr. Parkinson about a new case he was sending in to the ‘Casualty’ for admission and he asked me about Dr. Cameron’s operation. I told him about the “diagnosis” and the failed shunt attempt. He asked me if it made sense to me and I said that it didn’t. He gave a little grunt and advised me to keep a close watch on the patient post-operatively. There was no intensive care unit in those days and the patient had been sent up to the ward from the post-anesthetic room. I checked on her several times throughout the evening until I left the hospital about mid-night. At seven a.m. I got an urgent page and ran across the street to the hospital and up to the patient’s room to find that the surgical and anesthetic residents were attempting to resuscitate her. It was too late. She had died by ‘coning’ and I realized that if we had been able to insert the shunt this outcome might have been avoided.I felt as if I had been this young woman’s executioner. I had to talk to her family who graciously consented to a post-mortem examination. Later in the autopsy room the answer was revealed--- she did have hydrocephalus that was caused by a small hemangiomablastoma in the midbrain that occluded the aqueduct. This is a very rare condition and the only treatment available would have been a successful Torkildsen shunt.
I went out to Biggar, SK. in July 1957 to do general practice in association with two other doctors who had also graduated from the U. of M.; Dr. Alan Hooge about 1937 and Dr. Laurie Dunbar in 1952. Biggar was Laurie’s home town and the Dunbar Srs and the Hooges were great friends so the practice essentially acted like a father and son clinic and I was the new guy on salary. They treated me well, however, but I had to build up my own practice and only cared for their patients when they were away or sick.
42
Dr. Hooge had been the only doctor in the district during W.W.II and therefore all + the community had been his patients at that time. Dr. Jerry Pinto was the fourth doctor in town and although he had also come from Winnipeg, Alan always referred to him as our opposition rather than colleague. I don’t know whether this attitude stemmed from the fact that Jerry was Jewish or whether it was Alan’s unsubstantiated belief that Jerry performed abortions. I never saw any evidence of the latter and was quite happy to care for Jerry’s patients when he was away and to assist him when he needed it. Indeed we became good friends and Nina and I found that we had more in common intellectually and socially with Jerry and Noma than with my partners in the Biggar Clinic.
One August day in 1958, two young farmers from the neighboring town of Per-due had spent the afternoon in the beer parlour ‘celebrating’ one of the lad’s im-pending nuptials. On the way home at high speed, the driver failed to negotiate a curve in the highway and the vehicle rolled into the ditch. The driver was lying on the ground unconscious whereas the passenger, the future groom, was lying on the nearby railway embankment about 20 meters away. He had been hurled out of the car and probably rolled across the flat ditch and up the embankment without having struck the telegraph lines at their foot. I was called to the scene and really didn’t know what to do.
People were stopping and gathering and expected me to take charge and do something. I took the driver’s blood pressure, examined him neurologically and as he was breathing on his own and didn’t show any lateralizing signs gave him an injection of Coramine, an obsolete drug that acted as a stimulant and would likely do no harm. By this time Schneider’s hearse-come-ambulance had arrived and we placed the patient onto a stretcher and gently into the ambulance. My attention then turned to the ‘groom’ who was groaning in pain, complaining of neck pain but moving all limbs. We put a collar on his neck and gently got him onto a stretcher and into the ambulance and both were rushed to St. Margaret’s Hospital in Biggar. X-Rays showed no apparent abnormalities. I called Dr. Joe Stratford, Neurosurgeon at the University Hospital, Saskatoon and he advised me to make certain that the airway was secure and that probably I could look after him in Biggar. I managed to insert a Guedel oropharyngeal tube into the uncon-scious patient and admitted him to the ward. About 0300hrs Sister Bezaire called me to report that the patient was becoming increasingly restless and slightly cyanotic. I went up to the hospital and he was gasping and struggling for air in spite of using oxygen. I wasn’t sufficiently confident of being able to intubate the patient but it was crucial for his survival to oxygenate his brain. I did a tracheostomy under local anesthetic and the sister’s assistance and as soon as the trachea was opened and he inhaled air his thrashing about settled and his

43
colour changed from blue to pink! I thought it best to transfer the patient to Saskatoon and Dr. Stratford’s care and we sent him off right away. We later learned that he had sustained a cerebral contusion with brain swelling but no intracerebral hematoma. After he was discharged home, the parents made a point of thanking me for Dr. Stratford had graciously assured them that I had saved their son’s life.
Meanwhile the groom was still in hospital complaining about his neck. We repeated the X-rays and the ‘bride’ happened to be our technician who was keenly interested in makmg sure that the films were the best possible but no fractures or dislocations appeared. On day three or four the groom announced that he had to go home and harvest his crop and threatened to sign himself out if I didn’t approve. I could find no reason to keep him in and off he went. Six weeks later he returned to the office and reported that his neck still hurt ‘like a son-of-a-bitch’ especially when he tried to turn it. There was still tenderness in the mid-line at the upper cervical region and limitation of cervical movement but no neurological signs. We X-rayed him again and finally a fracture of the odontoid was clearly seen with some movement on flexion and extension views indicating instability. I phoned Dr. Joe Stratford and he advised that I might try applying a cervical cast for three months but if the fracture didn’t unite the patient would need to have an atlanto-axial fusion.
For some strange reason the notion that my patient might have to undergo a C1/2 fusion filled me with dread and I resolved to attempt the conservative treatment. I had never applied a ‘spica’ cast before but I think I had seen one during my internship and I found an illustration in a text book. The cast consists of a plaster of Paris jacket with a heavy plaster extension posteriorly attached to a crown of plaster. Diagonal side attachments flowed from the crown against the cheeks and parallel to the sterno- mastoid muscle to be fixed to the jacket at the level of the sterno-clavicular joints. The ears were left open for hearing but the cast severely limited flexion, extension and rotation of the neck while allowing full movement of the mandible for chewing. The cast had to be in place for a full three months and needed to be re-enforced once or twice during that period.Our groom patiently endured this lengthy torture, however, and we were all very glad when the fracture had healed and the cast could be removed. Many years later I talked to Joe Stratford at a Canadian Neurosurgical meeting and he remarked that the cervical spica cast was abandoned because of its difficulty in application and the necessity for great endurance by the patient. I never again applied another cervical cast. By the time I was in Neurosurgical practice we either used skull tongs and a Stryker bed in the 1960’s and early 70’s and by the end of the 1970’s the halo-vest had become standard treatment for most cervical fracture-dislocations.
44
These Neurosurgical cases were all very challenging, interesting and memorable. They have stayed with me over the years and contributed substantially to my formative interest in Neurosurgery. The decision to train in the field, however, did not occur until November 1963.
2.Why did I choose to train in neurosurgery at the University of Toronto
Three years of General Practice in Biggar made me realize that I was fascinated by surgery and that I needed more training in a surgical specialty. I found that trauma was most challenging and a career as a “traumatologist” seemed very inviting. It also appeared that Orthopedics would provide an excellent base on which to launch such a career. The so-called Galley surgical training course at the University of Toronto was highly regarded in Winnipeg and therefore I decided to apply to that course. Dr. Elmer James was Head of Orthopedics at the Manitoba Clinic in Winnipeg but Biggar was also his “home town” and two of his married sisters still lived there. He was in the habit of visiting his sisters quite often and that is how he happened to be in Biggar in 1959. Millie James Gregory lived next door to us and both she and her husband were my patients. Her husband Lyle had undergone surgical repair of a right inguinal hernia twice by my colleague Dr. Alan Hooge and the hernia had recurred. The hernia became strangulated during Dr. James’s visit and Millie asked her brother to try to help Lyle as he was in great pain. Dr. James’s attempts failed to reduce the hernia so they called me over to their house. I gave Lyle an injection of Demerol which relieved his pain and I was easily able to reduce the hernia. I told the Gregorys that in my opinion we should refer him to a very able senior General Surgeon in Saskatoon for a definitive repair of his hernia and they agreed. Dr.James was pleased at the outcome of my management of his brother-in-law’s condition and when I confided in him my plan to apply for Orthopedics in Toronto, he asked me to contact him when we were in Winnipeg on our way east. I did so and consequently over lunch at the Manitoba Club he told me that if I completed orthopedic training and obtained a Fellowship degree they would offer me a position at the Manitoba Clinic and a staff appointment at the University of Manitoba. He promised to provide me a letter with this commitment to attach to my application to the Galley Course. We drove to Toronto where I met my mother’s first cousin, Dr. Ray Farquharson for lunch and he said he would be happy to provide me with a letter of recommendation of my character and he thought that as Professor of Medicine
45
such a recommendation would be very helpful to my being accepted in the surgical training program at the U. of T. I also had an interview with Dr. Paul McGoey who was the only staff orthopedist available that July. I subsequently learned that Dr. McGoey’s position on the staff of the Scarbough General Hospital meant that he was only peripherally involved in the academic training at the University but never the less I believe he supported me and I was accepted into the Orthopedic training program that began in July 1961.
The first year was spent doing research at the Banting Institute under the supervision of Dr. Ian McNab, an internationally known and respected Orthopedic surgeon. He was a man whose mind crackled with new and innovative ideas and whose wit and humour endeared him to patients and colleagues alike. Whenever he visited the lab, which was only once a month, he had several new plans and ideas and it was difficult if not impossible for me to implement them. By the end of the year we had worked on 13 different projects. This was not a satisfactory situation but made bearable by my collaboration with fellow researcher Dr. Marvin Tile ( later becoming Head of Orthopedics at Sunnybrook Hospital) who offered his support and friendship during a trying and frustrating time.
Dr. McNab was interested in utilizing plastics in orthopedic surgery in the hope that it would provide strength but yet could be moulded into special shapes and could also accept screws. He had employed a fascinating man named Col. Harry Pierce to act as a resource person in the lab. Harry knew something about plastics and had a friend in a plastics extrusion plant who could supply us with various plastic compositions. Although originating from the Eastern Townships of Quebec, Harry had been studying Psychology at the University of London when WWII broke out. He joined the Imperial Army and later wastransferred to the Canadian Armored Corps where he was involved in research and rapidly rose to the rank of Colonel at the age of 28. The war was the best time of his life but like many of his generation he was unable to settle into a successful peace-time life. He became an alcoholic which led to a divorce and estrangement from his son. By the time we met he had joined AA and was dry but the job was only temporary and I’m sure he felt financially insecure. His contract came to an end when I finished the research year in June 1962 and we kept in touch for a couple of years. Colonel Pierce was hired as bursar of one of the U.of Toronto colleges [Massey, I believe] and I think he had finally and happily come into his own in the academic setting charming each generation of students and reliving his days in London before the war.
The first day I met Dr. McNab he outlined his vision for plastics in surgery but firstly he thought it necessary to determine if the type of plastic he was
46
considering for implantation was oncogenic. How was I supposed to do that? What technique should be used? What animals, how many, where should the plastic be implanted, how long should the animals be kept and where were all questions that had to be addressed. As with all problems, I consulted the scientific literature and determined that the Worster strain of white rat was theclassical lab animal used to determine carcinogenicity of implants. I arranged an interview with the head of research at New Mount Sinai Hospital who gave me valuable advice. I met with the researchers at Princess Margaret Hospital and they agreed that I could perform the operations in their lab and they would maintain the rats for the two years necessary for the completion of the project. The experiment was designed to have three groups of rats: Group 1 was implanted with two one cm diameter discs of zirconium plastic subcutaneously on each side of the abdominal wall. Group 2 was implanted with a different type of plastic disc [perhaps it was polypropylene] with out zirconium. Group 3 was the control group for which we used glass cover slips [used in histology and pathology labs for the preparation of microscopic slides]. We also implanted match-stick sized plastics rods in the paraspinal muscles and stainless steel pins for the controls. There were 30 animals in each group. All the preliminary planning and the surgical implantations were completed by the end of August and the first tumours in the abdominal wall developed and were harvested in May 1963. It turned out that sarcomas occurred, in relationship to the membrane surrounding the plastic, in such a high proportion of animals (about 80% if I recall) that we had actually stumbled upon a method of producing tumours in the lab. There were few tumours in the paraspinal muscles but tumours did occur in the control group. The results of the experiment were presented at a meeting of the Canadian Orthopedic Society in Ottawa in October 1964. Dr. Harrington, an Orthopedist from Texas who had pioneered the technique of using steel rods to correct scoliosis, was an invited speaker also. He spoke to me after my presentation and told me that he had been thinking of using plastics in some of his cases but after hearing about our results he decided to abandon that idea.
Probably the most notorious experiment that was done during my research year was an attempt to reproduce whiplash cervical injuries in primates. Other centres had studied the effects of rear-end automobile collisions in monkeys using a hydraulic ram to strike the back seat of sitting animals but they required expensive equipment.
Dr. McNab had the idea of using gravity as the force to produce acceleration-deceleration injuries and obtained funding from the Ministry of Transport. When the Banting Institute was built in 1931 they constructed two elevator shafts but only installed one elevator. The vacant shaft extended from to to the fifth floor
47
and Dr. Mc Nab had previously arranged to have a steel frame set up at the bottom of the shaft and extended up about twenty feet. The mobile floor of the device could be raised to any height by a pulley system that was activated by a crank at the bottom. An Orthopaedic fellow had been assigned the job of devising some way to hold the monkeys that would ensure that only the head moved in flexion and extension and yet permitted survival of the fall down the shaft! He had been unable to solve this problem and therefore I was given the task. I recruited the assistance of a brilliant 4th year medical student who was very good at original concepts that I could put into practical use. Three problems occurred to us from the outset: (1) How to protect the animals from unwanted “side effects” (2) How to ensure that only flexion-extension cervical movements were produced and (3) How could the severity of injuries be increased without becoming lethal. It turned out that we only had 3 Rhesus monkeys and therefore we decided to fine tune the experiments using rabbits that were abundant and cheap.
We built a simple shallow cradle of wood, clamped it to the base plate and using foam rubber padding on the dorsal and ventral surfaces of the anaesthetized ani-mals tied them onto the cradle. The medical student (whose name escapes me) had the idea that if a metal helmet was fashioned with a rudder-like top sticking upwards akin to a Roman soldier’s helmet, the rudder could run along some type of track and thus eliminate rotational movements. This basic idea enabled me cut a “helmet”, with rudder, out of a tin can and taped it securely onto the animal’s head using facial side extensions. A wire coat hanger was bent double and curved upwards from an attachment on the bottom of the cradle. The rudder of the helmet slid along the guide that had been fashioned by the coat hanger and thus only flexion-extension movements of the cervical spine were possible. When two or three of the rabbits were tested they all died from the fact that they had sustained fracture-dislocations of the atlanto-axial joints. We realized that the maximum centre of movement in the cervical spine of a rabbit occurred at these upper levels when compared to the human level of Cervical 5/6 and the monkey level at C7/Thoracic 1.
The technique of the drops was finally ironed out and we tried our first monkey at a 10 foot drop. The animal survived with no obvious fractures or disabilities. A second monkey was dropped from 15 feet with no apparent disability. For the final drop we arranged to have the Toronto General Hospital photographer do a slow motion film of the procedure with special attention paid to the landing.Unfortunately, there was something wrong with the camera and although we were able to see the violent neck movement it was not as clear as we had hoped due to a “stuttering” effect from the faulty instrument.

48
McNab used the film anyway in several presentations and concocted a story that the photographer had been so freaked out by the experiment that he shook with fear and thus spoiled the film. People hearing his presentations were bemused by the story but we knew that it was a story to cover the real truth that the photographer was incompetent. Dr. McNab published our results as an abstract in The Journal of Bone and Joint Surgery J.B.J.S but I was disappointed that he never acknowledged my contribution to the important scientific knowledge our hard work had achieved. I vowed that I would always recognize the contributions of students and junior colleagues to any work that I published in the future.
The animals were ‘sacrificed’ (the euphemism of the day) or euthanized (the present euphemism) and the cervical spines dissected and preserved forhisto-pathological study. The histological slides showed that the least severe injury was a tearing of the anterior longitudinal ligament or even an avulsion of a small bit of bone from the inferior body of the vertebra above. The next degree of severity was a fracture through the vertebral body end plate of these immature animals and finally the most severe lesion was a subluxation of the vertebral bodies at the affected level. The pathology produced by these injuries was startling and demonstrated that whip lash was a real condition rather than an entity dreamed up by lawyers and denied by insurance companies and those specialists who ‘prostitute’ their opinions at the behest of the well paying insurers. The same Orthopedists, Neurologists, Neurosurgeons and Physiatrists are used by the insurance companies over and over to justify denying compensation benefits to plaintiffs whose lives have been wrecked by rear-end collisions.
3.What was the neurosurgery residency application and selection process for you?
The first clinical service of my Orthopedic training was six months of Neurosurgery at the Toronto Western Hospital beginning on January 1, 1963. I arrived at the hospital at 730 hours and reported to Dr. Andy Helmegyi, the out-going Surgical Senior assistant, whom I awakened in the Internes’ residence. He had been up through the night with a young man named Dieter Lees who had drunkenly crashed his car into a bridge abutment and had broken the windshield with his forehead. He was lying in the Emergency Department semi-conscious and waiting for Dr, J.F.Ross Fleming to come in and assess the patient. I had checked in with Ross a few days before to introduce myself and become familiarized with this new hospital where I would be spending the next six months. He had taken me on Rounds, showed me the patients on the various wards and summarized their medical histories.
49
I was thus somewhat prepared to work with this iconic character. At that time Ross was only 37 years old but his pre-mature balding made him appear older. He was perhaps 6 ft. 2 inches tall with a thin face, lithe frame with long limbs which reminded me of Ichabod Crane, Washington Irving’s famous character. He had boundless stamina and energy, with a keen intellect that lead to meticulous but slow work. Unfortunately, his underlying insecurities and lack of self confidence resulted in an obsessive-compulsive personality that attempted to control all situations especially in the operating room. When complications arose during surgery he became angry and demanding and more that one scrub nurse had fled from the O.R. in tears but had later received a bouquet of flowers froma contrite Dr.Fleming.
Ross was standing over the unfortunate Dieter in the Emergency Department when I arrived. The Glasgow Coma Scale had not yet been invented, or had not been in use beyond the Clyde, and all we could do in our assessments of the level of consciousness was to describe a patient’s reaction to a vocal or painful stimulus and label them as being conscious, stuporous or comatose. The G.C.S. was devised by Mr.Bryan Jannet and Mr. Graham Teasdale at the Glasgow Neurosurgical unit in the mid 1960s and was instantly realized as a major advance in head injury care and the standard of coma assessment the world over. I can’t remember Dieter’s level of consciousness but he was responding to painful stimulation, he was restless, there were lacerations of his forehead and compound comminuted fractures of the frontal bone that had been confirmed by X-rays. Ross pointed out that the bloody material he had wiped off the patient’s brow was brain tissue and therefore we would have to operate and repair the damage. The operating room was alerted, the patient was transported and anaesthetized and we began the surgery about 0900 hrs and finished about 4 hours later. Ross was in an expansive mood and he paid for our New Years turkey dinner in the hospital cafeteria. Thus began my first 6 months of clinical Neurosurgical training as well as a professional collaboration with Ross that extended over the next 24 years.
4.How did you come to work at the University of Toronto, Division of Neurosurgery as a faculty member and what was the hiring process ?
The Surgical staff at the Toronto Western Hospital was on the look-out for a replacement for Dr. William Keith who had founded the divisions of Neurosurgery at both the Toronto Western and Sick Children’s Hospitals in 1937. By 1963, Bill Keith was winding down his practice and indeed he had been suffering from a severe depression for several years prior to my arrival.
50
To-wards the end of my rotation both Bill and Ross told me that they considered that I would make a good Neurosurgeon if I switched from Orthopedics. I was flattered by this confidence and told them that I would think about their offer of a staff position at the Western but wanted to carry on with the next scheduled stint of a year’s rotating surgical training at “Sick Kids” before making up my mind. They agreed and thought it would be wise to assess my abilities at H.S.C. and have the in-put of Dr. Bruce Hendricks and Dr. Keith as well as the other surgeons there. I spent the months of September and October as a senior on the Neurosurgical service with Dr. Robert (Bob) Elgie as the resident. I still loved the Neurosurgical work but when November and December’s rotation in Orthopedics under Dr. Robert Salter came along I found that I hated the mechanical nature of the specialty. The contrast between Ortho and Neuro was like night and day and I therefore decided to switch after talking it over with my wife. I spoke to Bill Keith and told him of my decision and he immediately picked up the phone and called Dr. Fred Kergin, the Surgeon-in-chief and head of the Gallie training program. Dr. Kergin made an appointment for me to see him in his office in the Banting Institute. Kergin was a very strict disciplinarian and an autocrat with a penchant for insulting any trainee who had the temerity of having graduated from what he considered a second class Medical school such as the University of Manitoba. He said this to Hjalmer Johnson who graduated from U. of M. a year or two before me and was enrolled in the Gallie course to train in Urology at H.S.C. I was scared to death when I attended that meeting with Dr. Kergin but all he said was that it was too bad I had not made up my mind a couple of weeks sooner for they had already chosen the candidate (Skip Pearless) for the Neurosurgical program. They would have to make other arrangements for me. Little did I know that the other arrangements were to train with Dr. Charles Drake in London, Ontario.
5.What have you seen as the most important advances between the time you were a resident and now?
(A) The first advance was the establishment of magnification in surgery. Dr. Drake began to use Loupes in 1965 (when he was 45 years old and likely developing presbyopia) but of course the assistant had to operate with the naked eye. I clearly recall Charlie introducing me to Dr. Ted Kurze, then chairman of the Dept. of Neurosurgery, Los Angeles Medical Center and the University of Southern California who had first introduced the use of the binocular operating microscope to clinical Neurosurgery in 1957. By this time he had been using the microscope for 8 or 9 years and was much impressed by the results. He said that operating with 10 power magnification was like “the rapture of the deep” as a whole new world had opened up to him.
51
He urged Charlie to obtain an operating microscope as soon as possible. We got our first Zeiss microscope at the Toronto Western Hospital in 1968-69 and indeed it was thrilling to use. My most impressive insight was that when the eye saw and the brain perceived at the higher magnification, the motor control was likewise enhanced and much finer work was then possible and achieved. To-day it would be considered malpractice to attempt to clip an aneurysm or dissect a tumour off a cranial nerve using the naked eye alone.
(B) The second most important advance was the implementation of diagnostic imaging that has ballooned in significance to such a degree in the Neurosciences that departments of Radiology are now called departments of Diagnostic Imaging. When I was a resident at the Toronto General Hospital it fell to the neurological and neurosurgical seniors to carry out percutaneous carotid artery punctures and perform the angiograms in the O.R. where the radiologist or radiology technician operated the X-Ray machine and pulled out the X-ray films as they were being exposed. A generation prior to that, actual plates of radiosensitive silvered glass were used and some of the older radiologist (and therefore some of the inexperienced trainees) still referred to Roentgen images as “plates” much to the irritation of their more obsessive-compulsive colleagues. Percutaneous brachial artery injections were popularized by some radiologists and Dr. John Allcock in London, ON was so skilled that he routinely did percutaneous vertebral arteriograms! These techniques, however, were soon superceded by the femoral artery injections that were also favoured by cardiologists and have become the standard. Angiography was moved to the Departments of Radiology as new equipment required expansions of their facilities and the technological advances of intra-arterial catheters lead to the present growth of Therapeutic Neuroradiologists.
a. During my residency the diagnosis of intracranial lesions such as tumours, cysts, abscesses and hydrocephalus depended upon the clinical perspicacity of the neurosurgeon and the neurologist. Dr. Bill Keith worked closely with Dr. Jack Silversides at the Western Hospital and Dr. Stobo Prichard at H.S.C and relied heavily on their opinions. Pneumoencephalograms (PEG) were still being done and some Neurologists sadistically ordered them on their teen aged patients who persistently complained of headaches without any other neurological signs. They considered these young people as expressing behavioral or neurotic problems that should be gotten over with the experience of a “real “headache that a PEG would produce. These tests were referred to as “punitive air studies”.
b. Ventriculograms were done initially in the O.R. where a parietal-occipital burr hole was performed, a cannula was inserted into the lateral ventricle

52
and radio-opaque liquid injected while the patient was in a seated position with the head tilted forward. The patients were then taken to the Radiology Dept. where they were seated in a special chair or table that summer-saulted them around causing the “dye” to roll back across the top of the ventricle and through the Foramen of Munro and finally into the III rd and IV th ventricles. This study was indicated when an intracranial mass was obstructing the ventricular system and causing hydrocephalus and papilledema in which case a PEG was contraindicated.
c. Radio-isotopic studies were begun during my residency but the technology was very basic and the results imperfect when compared to later imaging techniques. The images obtained after running a Geiger counter over a patient’s head following the intravenous injection of an isotope were grainy as the pixels were relatively large but it gave us a much clearer idea as to the location of a mass lesion than did the neurological examination. I recall one patient at The Western with a very “hot” lesion in the left tempero-parietal area but a craniotomy showed only fattened gyri and the probing brain needle yielded only edematous brain matter. The craniotomy was closed and the patient treated with the steroid dexamethasone which controlled the edema for the next year. The patient underwent a second craniotomy by Dr. Fleming while I was on vacation the following summer and again nothing was found except edema. A few months later the patient died as we were unable to control the brain swelling. The family consented to an autopsy and this revealed that a 2 cm. metastatic tumour was present on the inferior surface of the brain against the tentorium and caused the edema to extend superiorly into the tempero-parietal lobe where it appeared in the nucleogram. The primary was a bronchogenic carcinoma that was only about 5mm. in diameter and almost missed by the pathologist. The case was also unusual in that there were no other metastases and the patient lasted about 2 years from the time of first diagnosis of the brain tumor. Unfortunately, his immune system was so compromised that he died of multiple abscesses and overwhelming infection.
d. Ultra sound was in its infancy during my training and was primarily used as a diagnostic tool in the E.R. to determine if there was a midline shift of the brain in a head injured patient. The presence of a shift suggested a mass on the opposite side of the brain whereas if there was no shift we felt relatively confident that the patient could be observed and monitored and not subjected to diagnostic burr holes as had been the practice at The Toronto General.
53
e. The first Computed Axial Tomograms (CAT scan) were invented in Britain and developed by the Electrical Music Institute (The Beetle’s recording company) in the late l960.s and were initially known as EMIs. I believe the first EMI machine in Canada was obtained by the Montreal Neurological Institute and I saw my first CAT image at a Canadian Neuroscience meeting in the early 1970s. Our first CT machine was installed at the Western about 1976 and it represented a great leap forward in diagnostics. About 5 years later our first Magnetic Resonance Imaging machine (MRI) was installed and they are now the standard of diagnosis. Fortunately the PEG, ventriculogram and myelogram have become obsolete and drifted into history.
6.What was the most memorable event in your residency?
There were so many memorable events that it is difficult to single out any one but two cases during my 18 months with Dr. Charlie Drake were very dramatic in their presentation and final result.
The first occurred in the fall of 1965 when I had been Dr. Drake’s resident for about 9 months. A mentally challenged young man, who came from a family that was similarly afflicted, presented in the Woodstock General Hospital E.R. with a history of progressively worsening headache, erythema and puffiness over the forehead, with two days of fever and obtunded level of consciousness. Skull X-rays revealed a “moth-eaten” appearance of the frontal bone and opacification of the frontal sinuses. I saw him in the E.R. of the Victoria Hospital and found that he was one of the sickest patients I had ever seen. The clinical diagnosis was apparent as he had developed a cerebral empyema secondary to osteomyelitis of the frontal bone caused by acute on chronic sinusitis. This condition was rare by the latter half of the 20th century for most people in Ontario would have consulted a physician and been treated long before the pathological process had developed to that extent. He was prepared for emergency surgery that consisted of turning a bifrontal craniotomy flap, leaving the bone out to be autoclaved (and later replaced). Purulent material was syringed from the epidural space; the dura was opened and also drained of pus. Drains from the sub-dural and epidural spaces were established to collect residual pus. I can’t remember the organism but it was likely a pneumococcal bacterium that was sensitive to antibiotics which we administered intravenously in high doses.
The patient was transferred to the isolation ward that consisted of about 6 beds located on the third floor of an older wing that could only be accessed by a very slow, creaky freight elevator although one could exit the unit by a back staircase.

54
The following morning the patient began to have generalized seizures and I was summoned from the second floor O.R. to administer intravenous diazepam which controlled the seizures temporarily while the phenytoin came up to therapeutic levels. Carbamazepine (Tegretal) was only available to research scientists then. Each time the seizures began, I was called out of the O.R. to administer the diazepam as the nurses said they were not allowed to give these drugs intravenously. I asked Pharmacy to mix up a 50cc syringe of Valium, inserted the needle into the I.V. tubing and asked the nurses to inject 2 ccs when ever the patient began to have a fit. No, they weren’t allowed to do that either. I talked to the anesthetic staff and they suggested using a machine available in their department whereby the 50 cc syringe could be clamped in and calibrated so that the press of a button turned on the machine and the proper dose of anti-seizure medication was automatically delivered intravenously. Now the nurses were allowed to press the button and effectively treat the seizure. The patient eventually made a full recovery but I was always convinced that if it wasn’t for a little ingenuity on the part of the medical staff the strictures that the heads of the nursing department placed on their members might have lead to the demise of this unfortunate young man. This is one example of how reactionary the senior nursing staff had become, much to the frustration of doctors and many of the young, bright nurses who eventually changed the culture of their profession. They gradually modernized and this lead to the development of Nurse Practitioners, Physician Assistants and the highly skilled workers in our Intensive Care Units.
The second memorable case occurred on June 18, 1966, the last Saturday night of my tour of duty at the Victoria Hospital in London, Ont. About 1730 hrs a five year old London girl named Suzie was playing alone in the family garage and although we didn’t know it at the time must have fallen and struck the right side of her head on some solid object. She was probably unconscious for a short period of time but regained consciousness and responded when her mother called her in for supper. The mother was puzzled by her daughter’s apparent listless and fussy approach to the meal for Suzie was always a lively, chatty child with a generous appetite especially after an afternoon’s play in the fresh air. Suzie complained that her head hurt and when she began to vomit her mother became concerned and called their Pediatrician. He knew the child and that the family didn’t call unless something significant was occurring. He advised them to take Suzie to the Emergency Department of Victoria Hospital and he would come down to see her there later. They arrived in the Emergency about 1915 hrs and were greeted by a waiting room full of sick, frustrated, impatient patients and their families.

55
One should avoid at all costs requiring emergency services in the first week after June 15th for that is the date when the teaching hospitals are restaffed by a new group of interns who have just finished their 4th year examinations and are inexperienced in the practical application of all that knowledge. At 2000 hrs the exhausted interns who had been working slowly and methodically all day came to the end of their shift leaving a back log of some twenty patients for the night shift. The night shift rotation was taken over by a pediatric senior who had just completed two years of research and his clinical skills were rather rusty. The head nurse was carrying out a triage when she finally came across Suzie and her par-ents. There was nothing the matter with her nursing skills nor with her intuition. She didn’t like the looks of the child who was pale, vomiting and complaining of headache when she wasn’t sleeping. She informed the new senior that he should see this patient immediately and knowing her competency he followed this advice. He really didn’t know what was going on with the child in view of the sketchy history and therefore sent her off to the Radiology Department for a skull X-Ray at 2020 hrs. This bought some time until the expected arrival of the Pedia-trician. The Pediatrician didn’t see anything on the poorly exposed X-rays and de-cided to take Suzie back for another film in the hope that something would ‘turn up’ or at least come to mind. About 2100 hrs, in the radiology department, Suzie stopped breathing and began to exhibit the cyanosis of apnea. She was dying.
That Saturday night I had been invited to Bob and Mary Barr’s home for dinner about 1900 hrs and Lorne Amacher (the level 3 neurosurgical senior) and his wife were expected to join us for a pleasant evening of fellowship and conversa-tion. The Barrs [Bob was training in Hematology at the Victoria Hospital while his brother Hugh was training as a Neurosurgeon at the Toronto General Hospital were sons of the illustrious Murray Barr of Barr-body fame and Professor of Neuro-anatomy at The University of Western Ontario] lived in one of the houses owned by The Victoria Hospital at the end of the street that bordered the hospi-tal. They were only half a block away so we were permitted to spend time there and still be on call. At 2100 hrs we had finished dinner and Bob and I were just settling down in the living room for a post prandial cigar when the phone rang for me. The hospital operator said there was an emergency call from the X-ray Department and that I better get over there quickly for it sounded like the ‘real deal’. I dropped the phone and ran down the front steps, nearly bowling over the Amachers on the way. There was a back door to the X-Ray suite about 50 yards away and I sprinted through and arrived at the scene in about 30 seconds.
56
Here was this still, little child with cyanotic lips lying like a ghost on a large gurney with a panicked pediatrician trying to compress her chest while the nurse and radiology technician looked on helplessly. A quick assessment revealed dilated pupils, apnea and no movement in response to pain. I said rather rashly and ominously, “She has gone! What the hell has happened here?” They gave me a quick summary of what little they knew and thought she must have suffered a head injury. I placed my hands on either side of her head and felt the scalp swelling on the right that likely indicated an underlying skull fracture. The stethoscope revealed a rapid but barely discernable heart beat. I gave her mouth-to- mouth respiration and she pinked up. There was a chance that she had sustained an epidural hematoma beneath the skull fracture and that prompt action might still save her. I inserted a pharyngeal airway and asked the pediatrician to pump oxygen via face mask, ordered the technician to call the OR that we were on our way and the nurse to summon the elevator while I pushed the stretcher down the hall running with the others trying to keep up. There was no time to talk to the parents who waited forlornly worrying about their precious daughter and quite ignorant of the flurry of activity her condition had inspired.
Fortunately the OR was quiet and the nursing team was sitting in their lounge enjoying the Saturday evening break. The team was one of our best and they had the OR ready and instrument bundles open in three minutes. I did a quick wash of my hands and Suzie’s scalp, donned a pair of gloves and without any anesthetic incised the scalp and put in a burr hole. The black, clotted epidural blood spurted out and a sense of relief and even elation came over us as the child began to move and breathe with the release of the intracranial pressure. Only then were we able to summon the on-call anesthetist, do a proper scrub, prep and drape while one of the nurses held Suzie down so she wouldn’t fall off the OR table. Once anaesthetized the burr hole was extended into a craniotomy and the entire clot removed, the craniotomy closed and a full head dressing applied as was the custom in those days. Suzie was taken to the Recovery Room and I could finally go down to the Emergency waiting room to speak to the parents who were much relieved to learn what had happened to their daughter. As usual I tempered my cautiously optimistic prognosis with the admonition that the final outcome was still unknown. In Neurosurgery it is wise to employ the adage that we hope for the best but have to be prepared for the worst.
The next morning, Sunday, I started my rounds in the recovery room where the nurses had been monitoring our patient all night without finding it necessary to call me. Suzie was lying in a crib with her eyes closed looking fragile and vulnerable with the large head dressing accentuating her tiny size.
57
I gave her a shake and called her name. Without opening her eyes she said rather irritatedly, “I want to see grandma”. It was a real thrill to realize that she was fine and everything would turn out alright. A magnificent way to complete a residency! There was no way, however, that such an accomplishment would go to my head for when I told Dr. Drake about the case next day his laconic comment was “you were lucky”.
7.What advice do you have for our residents and young faculty as they embark on their career as neurosurgeons?
1.Be honest!
2.Don’t be afraid to question orthodoxy.
3.Seek new ways to solve ongoing problems.
4.Strive to find better methods of doing surgical operations and procedures (Try to think out-side of the box).
5.Always consider the suggestions of colleagues, juniors and students.(Remember that many of them are smarter than you are)
6.Keep a record of your cases and periodically review your results.
-Dr. R. Graham Vanderlinden

58
Notes:
59
Notes:
60
Notes: