
TERAPIJA PODHRANJENOSTI PRI PD - Slovensko … · •18-51% CAPD pacientov . ... • Nepro, Nepro...
38
TERAPIJA PODHRANJENOSTI PRI PD Bojan Knap Klinični oddelek za nefrologijo Univerzitetni Klinični center Ljubljana
Transcript of TERAPIJA PODHRANJENOSTI PRI PD - Slovensko … · •18-51% CAPD pacientov . ... • Nepro, Nepro...

TERAPIJA PODHRANJENOSTI
PRI PD
Bojan Knap
Klinični oddelek za nefrologijo
Univerzitetni Klinični center Ljubljana
Renal Patient Medical Challenges
bull Renal diet compliance
bull Anorexia (lack of appetite)
bull Nutritional status
bull Hyperglycemia diabetes
bull Cardiovascular risk
mortality
bull Hyperphosphetemia
bull Infection immune status
bull PEW ndash weight loss
anorexia inflammation etc
bull Multiple medications
bull Bone mineral disorders
bull Edema
bull Anemia
bull High potassium levels
bull Frequent hospitalizations
bull Life-style issues
bull Quality of life
bull Delaying CKD progression
bull Longevity of dialysis or
transplantation
RX
Cardiovascular and diabetic prescriptions may help
No proof of improved survival
Maintenance therapy
Catabolic
Long waiting time
Risky costly
Repeat kidney failure
Nutrition is the only low-cost effective available treatment
Transplant Dialysis Nutrition
3
Lakota in sitost
Realnost bolnika s KLB
Johansen K L JASN 2007181845-1854
Johansen K L JASN 2007181845-1854
Importance of physical activity
DEBELEJŠI DIALIZNI BOLNIKI
ŽIVIJO DLJE
DIALIZNI BOLNIKI Z ALBUMINI MANJ KOT 30GL
UMIRAJO PREJ
DIA
OMEJEN VNOS ZDRAVE HRANE
PRI KLB
Better nutritional status is associated with improved long
term survival in dialysis patients
Source Chan et al (2012) J Ren Nutr 2012 Nov22(6)547-57
LEDVIČNI BOLNIKI IMAJO SLAB APETIT
bull Izguba apetita in želje za hrano
bull Izguba vonja in okusa
bull Prezgodnja sitost
bull Motnje v delovanju hipotalamusa
bull Vpliv zvišane koncentracije citokinov
bull Omenjeno olajša nastanek kaheksije s
nezadostnim vnosom energije in
proteinov
DIETA LEDVIČNEGA BOLNIKA
Phosphorus balance
ŠTEVILNI VZROKI PODHRANJENOSTI PRI
LEDVIČNI BOLEZNI
bull Zmanjšan vnos hrane
bull Omejevalne diete proteini
bull Uremični toksini
bull Metabolna acidoza
bull Endokrini dejavniki
bull Gastrointestinalni dejavniki
bull MIA sindrom
UREMIČNI SINDROM
Vodi k podhranjenosti tudi zaradi
bull Insulinske rezistence
bull Motenega klirensa lipidov
bull Metabolične acidoze
bull Sekundarnega hiperparatireoidizma
uremične kostne bolezni
DEBELOST OGROŽA TUDI
LEDVIČNE BOLNIKE
bull METABOLIČNI SINDROM
bull SLADKORNA BOLEZEN II
bull MAŠČOBNE CELICE KOT ENDOKRINI ORGAN TUDI PRI KLB VPLIVAJO NA KVS
bull PROBLEM MOTENJ HRANJENJA IN MALNUTRICIJA Z OHRANJENO TELESNO MASO OB ZMANJŠANJU PUSTE TELESNE MASE
bull pomen določanja puste telesne mase z bioimpedanco
bull lean tissue index fat mass index
VLOGA LEPTINA PRI KAHEKSIJI KLB
bull Zvišan pri KLB
bull Deluje podobno kot citokinski receptorji
tipa IL6(vnetje)
bull Preko receptorjev za melanocortin v
hipotalamusu deluje na apetit in
metabolizem
bull Antagonisti MC-R4 receptorja nov
terapevtski obet
VELIK POMEN PREHRANSKE
DIAGNOSTIKE ZA DIALIZNE PACIENTE
bull Klinična presoja pacienta in kvalitete
življenja oziroma uspeha zdravljenja
bull Biokemijavrednosti albuminov
prealbumina in vnosa proteinov (35gl
300mgl 1gkgdan)
bull Nadzor telesna teža BMI SGA
BCM(bioimpedanca) serumski albumin
kreatinin
SUBJEKTIVNA GLOBALNA
NUTRICIJSKA OCENA-SGA
SGA ocena prehranjenosti zajema
bull anamnezo (o spremembi telesne teže o
vnosu hrane simptomih s strani GIT
funkcionalne zmogljivosti) in
bull telesni pregled (atrofija mišic zmanjšanje
podkožne maščobe in pojav oteklin)
bull zlati standard ocene bolnika(Keith
Nutrition in Clinical Practice 2008)
Malnutrition Inflammation Score
(MIS)
bullFully quantitative
bullUses the 7 original SGA components
bullAdds 3 new components
ndashBody mass index
ndashSerum albumin
ndashSerum total iron binding capacity
PEM - PROTEINSKO
ENERGETSKA MALNUTRICIJA
bull PEM je pogost v KLB
bull Je povezan s povečano obolevnostjo in
umrljivostjo
bull 40 PEM na začetku nadomestnega
zdravljenja KOL
bull 10-70 HD pacientov
bull 18-51 CAPD pacientov
Nutritional RecommendationsDialysisStage 5 CKD
KDOQI1 ESPEN2 EBPG3
EnergyCalories lt 60 years 35
kcalkgd
60 years or obese
30-35 kcalkgd
35 kcalkgd 30-40 kcalkgd
Protein 12 gkgd
50 HBV
12-14 gkg
IBWd
11 gkgd
Sodium ― 18-25 gd 2000-3000
mgd
Fluid ― 1000 mL + urine
volume
―
Potassium ― 2000-2500 mgd 1950-2730
mgd
Phosphorus 800-1000 mgd
lt 17 mgkg IBW or
SBWd
800-1000 mgd 800-1000 mgd
Calcium 2 gd ― 2000 mgd
1 NKF KDOQI Clinical practice guidelines for nutrition in chronic renal failure AJKD 2000 35S1-S140
2 Cano N et al Clin Nutr 2006 25295-310
3 Fouque D et al NDT 2007 22(suppl 2)ii45-ii87
Ocena prehranskih potreb
bull V akutni fazi 20-25 nebeljakovinskih kkalkgdan v anabolni fazi in podhranjeni 25 -30 kkalkgdan
bull Maščobe 03 gkg ttdan do 2 gkg ttdan (30 do 70)
bull Ogljikovi hidrati 2-5g kgdan (30 do 70)
bull Beljakovine povprečno 15 g kg tt dan (15 -20 )
bull Mikrohranila-dnevne priporočene potrebe individualno glede na obolenje
bull Opečenci več Cu Se in Zn
AA V PARENTERALNI PREHRANI
bull Povečana izguba AA
bull Neravnovesje med izgubo in porabo
bull Esencielne AA z dodatkom histidina ter arginina niso optimum
bull Nadomeščanje tirozina problem zaradi slabe topnostihellip
bull Acetil-tirozin je rešitev vendar ne pri KLB
bull Rešitev predstavlja dipeptid glicil-tirozin ki je dobro topen in idealno nadomešča večje potrebe po tirozinu pri KLB (AminoMel nephro)
PREHRANSKI DODATKI
Enteralni
bull Nepro Nepro HP Nepro LP Ensure Ensure Plus Advance Prosure Fresubinhellipenkrat na dan per os
bull Glutamin 5-10g na dan per os
bull Carenal 1 tableto po dializi
bull L-karnitin
Parenteralni
bull Aminomel Nephro aminokisline (500ml med HD)
bull Kabiven
bull Glamin 500ml
bull Dipeptiven 100ml
bull Soluvit N(vodotopni vitamini)
bull Vitalipid N(maščobotopni vitamini)
bull Addamel N(mikroelementi)
bull Omegaven (ribje oljehellip)
Component Renal Specific
ONS
Standard ONS
Protein Optimum Medium
Glycemic Index
(Carbohydrates) Low High
MUFA Omega-3
(FatsLipids) High Low
Electrolytes
Phosphorus
Potassium Sodium
Low High
Fluid volume Low High
Caloric density High Standard
Fiber High Low
Prebiotics scFOS Present None
CKD-specific vitamin
amp mineral profile Optimized None
Why Renal Specific ONS
Why Standard versus Renal Specific ONS
Nutrition Intervention in CKD Patients
bull Expert recommendations
KDOQI1 ESPEN2 EBPG3
Nutrition
Support
Individuals undergoing
maintenance dialysis
who are unable to
meet their protein and
energy requirements
with food intake for an
extended period of
time should receive
nutritional support
Special formula
products for HD
treatment can be
useful especially in
malnourished patients
who are not able to
increase their nutrient
intake
Oral nutritional
supplements should
be prescribed if
nutritional counseling
does not achieve an
increase in nutrient
intake to a level that
covers minimum
recommendations
Products
specifically
designed for
dialysis patients
should be
prescribed
1 NKF KDOQI Clinical practice guidelines for nutrition in chronic renal failure AJKD 2000 35S1-S140
2 Cano N et al Clin Nutr 2006 25295-310
3 Fouque D et al NDT 2007 22(suppl 2)ii45-ii87
Recomm-S
ESPEN KDOQI EBPG
Proteini (gkgdan) 12-14 10-12 11
Energija
(kCalkgdan)
35 lt60 g 35
gt60 g 30
30-35
gt50 intke lt1 gkgdan
Actual ntake 20-25 kCalkg 08-1 g proteinakg
Renal Specific Nutritional Therapy
Clinical studies have shown that renal-specific nutrition offers advantages over standard nutrition
bull Phosphorus levels were lower with the renal-specific nutrition than with the standard nutrition1
bull Less fluid and potassium in renal-specific nutrition offers advantages over standard nutrition2
1 Cockram DB et al J Ren Nutr 1998825-33
2 Williams RF Summers AM J Ren Nutr 200919183-188
PREHRANSKE ZAHTEVE DIALIZE
PRAKSA
ENERGIJA 35KCALKG TT NA DAN
PROTEINI 12GKG TT NA DAN
VNOS TEKOČINE 1000ML + IZLOČEN URIN
NATRIJ 2-3G NA DAN
KALIJ 2-3G NA DAN
FOSFOR 08-12GDAN
NKFKDOQI 2000 ADA 2002 WILKENS 2004
BIOIMPEDANCE PRINCIPLES
Phase angle
bull Phase angle is an indicator based on reactance and
resistance obtained from bioelectrical impedance
analysis (BIA)
bull PA depends on cell membrane integrity and on body cell
mass
bull Although its biological meaning is still not clear phase
angle appears to have an important prognostic role
bull Phase angle differs across categories of sex age BMI
and percentage fat bull Maria Cristina G Barbosa-Silva Aluiacutesio JD Barros Jack Wang Steven B Heymsfield and Richard
N Pierson Jr Am J Clin Nutr July 2005 vol 82 no 1 49-52
bull Satish Kumar1 Aswini Dutt1 Sandhya Hemraj2 Shankar Bhat1 and Bhat Manipadybhima Iran
J Basic Med Sci 2012 Nov-Dec 15(6) 1180ndash1184
PHASE ANGLE AND LEAN TISSUE
INDEX ARE SLIGHTLY HIGHER IN
HEMODIALYSIS THAN IN PERITONEAL
DIALYSIS GROUP OF PATIENTS
BKnap ZVeceric Haler JButurovic-Ponikvar
RPonikvar AF Bren
University Clinical Center Ljubljana
Department of Nephrology Slovenia
Ideal nutrition ndash CKD patients
bull Prevents musle loss
bull Prevent andor treat PEW
bull Correct metabolic derrangements
bull Decrease morbidity and mortlity
bull Improve QoL
bull Does not promote progression of CKD
bull Or ideally slow down progression of CKD
ZAKLJUČEK
bull Podhranjenost je pomembna in pogosto
ključna za preživetje
bull Sodobne metode detekcije in zdravljenja
podhranjenosti omogočajo zgodnejšo
nutricijsko intervencijo
bull Prehranski dodatki tako enteralni kot
parenteralni so pogosto nujna in včasih
edina možnost
Kaj je dobro vedetihelliphellip
bull LEDVIČNI BOLNIKI JEDO SLABO
bull V ZAČETNI FAZI KLB TERAPIJA Z OMEJEVANJEM VNOSA PROTEINOV LAHKO PRIPELJE DO MALNUTRICIJE IN KAHEKSIJE
bull POMEMBNA OCENA HRANJENOSTI IN PRAVOČASNA NUTRICIJSKA INTERVENCIJA V VSEH FAZAH KLB
bull USPEH ZDRAVLJENJA MALNUTRICIJE JE POVEZAN Z DOBRIM ZDRAVLJENJEM OSNOVNE LEDVIČNE BOLEZNI IN CELOSTNEGA ZDRAVLJENJA KLB
bull POLEG HRANE VELIKO PRISPEVAJO K KVALITETI ŽIVLJENJA TUDI PREHRANSKI DODATKI IN TELESNA VADBA
bull ANABOLNI AGENSI IN STIMULATORJI APETITA NA NIVOJU HIPOTALAMUSA SO OBET BLIŽNJE PRIHODNOSTI

Renal Patient Medical Challenges
bull Renal diet compliance
bull Anorexia (lack of appetite)
bull Nutritional status
bull Hyperglycemia diabetes
bull Cardiovascular risk
mortality
bull Hyperphosphetemia
bull Infection immune status
bull PEW ndash weight loss
anorexia inflammation etc
bull Multiple medications
bull Bone mineral disorders
bull Edema
bull Anemia
bull High potassium levels
bull Frequent hospitalizations
bull Life-style issues
bull Quality of life
bull Delaying CKD progression
bull Longevity of dialysis or
transplantation
RX
Cardiovascular and diabetic prescriptions may help
No proof of improved survival
Maintenance therapy
Catabolic
Long waiting time
Risky costly
Repeat kidney failure
Nutrition is the only low-cost effective available treatment
Transplant Dialysis Nutrition
3
Lakota in sitost
Realnost bolnika s KLB
Johansen K L JASN 2007181845-1854
Johansen K L JASN 2007181845-1854
Importance of physical activity
DEBELEJŠI DIALIZNI BOLNIKI
ŽIVIJO DLJE
DIALIZNI BOLNIKI Z ALBUMINI MANJ KOT 30GL
UMIRAJO PREJ
DIA
OMEJEN VNOS ZDRAVE HRANE
PRI KLB
Better nutritional status is associated with improved long
term survival in dialysis patients
Source Chan et al (2012) J Ren Nutr 2012 Nov22(6)547-57
LEDVIČNI BOLNIKI IMAJO SLAB APETIT
bull Izguba apetita in želje za hrano
bull Izguba vonja in okusa
bull Prezgodnja sitost
bull Motnje v delovanju hipotalamusa
bull Vpliv zvišane koncentracije citokinov
bull Omenjeno olajša nastanek kaheksije s
nezadostnim vnosom energije in
proteinov
DIETA LEDVIČNEGA BOLNIKA
Phosphorus balance
ŠTEVILNI VZROKI PODHRANJENOSTI PRI
LEDVIČNI BOLEZNI
bull Zmanjšan vnos hrane
bull Omejevalne diete proteini
bull Uremični toksini
bull Metabolna acidoza
bull Endokrini dejavniki
bull Gastrointestinalni dejavniki
bull MIA sindrom
UREMIČNI SINDROM
Vodi k podhranjenosti tudi zaradi
bull Insulinske rezistence
bull Motenega klirensa lipidov
bull Metabolične acidoze
bull Sekundarnega hiperparatireoidizma
uremične kostne bolezni
DEBELOST OGROŽA TUDI
LEDVIČNE BOLNIKE
bull METABOLIČNI SINDROM
bull SLADKORNA BOLEZEN II
bull MAŠČOBNE CELICE KOT ENDOKRINI ORGAN TUDI PRI KLB VPLIVAJO NA KVS
bull PROBLEM MOTENJ HRANJENJA IN MALNUTRICIJA Z OHRANJENO TELESNO MASO OB ZMANJŠANJU PUSTE TELESNE MASE
bull pomen določanja puste telesne mase z bioimpedanco
bull lean tissue index fat mass index
VLOGA LEPTINA PRI KAHEKSIJI KLB
bull Zvišan pri KLB
bull Deluje podobno kot citokinski receptorji
tipa IL6(vnetje)
bull Preko receptorjev za melanocortin v
hipotalamusu deluje na apetit in
metabolizem
bull Antagonisti MC-R4 receptorja nov
terapevtski obet
VELIK POMEN PREHRANSKE
DIAGNOSTIKE ZA DIALIZNE PACIENTE
bull Klinična presoja pacienta in kvalitete
življenja oziroma uspeha zdravljenja
bull Biokemijavrednosti albuminov
prealbumina in vnosa proteinov (35gl
300mgl 1gkgdan)
bull Nadzor telesna teža BMI SGA
BCM(bioimpedanca) serumski albumin
kreatinin
SUBJEKTIVNA GLOBALNA
NUTRICIJSKA OCENA-SGA
SGA ocena prehranjenosti zajema
bull anamnezo (o spremembi telesne teže o
vnosu hrane simptomih s strani GIT
funkcionalne zmogljivosti) in
bull telesni pregled (atrofija mišic zmanjšanje
podkožne maščobe in pojav oteklin)
bull zlati standard ocene bolnika(Keith
Nutrition in Clinical Practice 2008)
Malnutrition Inflammation Score
(MIS)
bullFully quantitative
bullUses the 7 original SGA components
bullAdds 3 new components
ndashBody mass index
ndashSerum albumin
ndashSerum total iron binding capacity
PEM - PROTEINSKO
ENERGETSKA MALNUTRICIJA
bull PEM je pogost v KLB
bull Je povezan s povečano obolevnostjo in
umrljivostjo
bull 40 PEM na začetku nadomestnega
zdravljenja KOL
bull 10-70 HD pacientov
bull 18-51 CAPD pacientov
Nutritional RecommendationsDialysisStage 5 CKD
KDOQI1 ESPEN2 EBPG3
EnergyCalories lt 60 years 35
kcalkgd
60 years or obese
30-35 kcalkgd
35 kcalkgd 30-40 kcalkgd
Protein 12 gkgd
50 HBV
12-14 gkg
IBWd
11 gkgd
Sodium ― 18-25 gd 2000-3000
mgd
Fluid ― 1000 mL + urine
volume
―
Potassium ― 2000-2500 mgd 1950-2730
mgd
Phosphorus 800-1000 mgd
lt 17 mgkg IBW or
SBWd
800-1000 mgd 800-1000 mgd
Calcium 2 gd ― 2000 mgd
1 NKF KDOQI Clinical practice guidelines for nutrition in chronic renal failure AJKD 2000 35S1-S140
2 Cano N et al Clin Nutr 2006 25295-310
3 Fouque D et al NDT 2007 22(suppl 2)ii45-ii87
Ocena prehranskih potreb
bull V akutni fazi 20-25 nebeljakovinskih kkalkgdan v anabolni fazi in podhranjeni 25 -30 kkalkgdan
bull Maščobe 03 gkg ttdan do 2 gkg ttdan (30 do 70)
bull Ogljikovi hidrati 2-5g kgdan (30 do 70)
bull Beljakovine povprečno 15 g kg tt dan (15 -20 )
bull Mikrohranila-dnevne priporočene potrebe individualno glede na obolenje
bull Opečenci več Cu Se in Zn
AA V PARENTERALNI PREHRANI
bull Povečana izguba AA
bull Neravnovesje med izgubo in porabo
bull Esencielne AA z dodatkom histidina ter arginina niso optimum
bull Nadomeščanje tirozina problem zaradi slabe topnostihellip
bull Acetil-tirozin je rešitev vendar ne pri KLB
bull Rešitev predstavlja dipeptid glicil-tirozin ki je dobro topen in idealno nadomešča večje potrebe po tirozinu pri KLB (AminoMel nephro)
PREHRANSKI DODATKI
Enteralni
bull Nepro Nepro HP Nepro LP Ensure Ensure Plus Advance Prosure Fresubinhellipenkrat na dan per os
bull Glutamin 5-10g na dan per os
bull Carenal 1 tableto po dializi
bull L-karnitin
Parenteralni
bull Aminomel Nephro aminokisline (500ml med HD)
bull Kabiven
bull Glamin 500ml
bull Dipeptiven 100ml
bull Soluvit N(vodotopni vitamini)
bull Vitalipid N(maščobotopni vitamini)
bull Addamel N(mikroelementi)
bull Omegaven (ribje oljehellip)
Component Renal Specific
ONS
Standard ONS
Protein Optimum Medium
Glycemic Index
(Carbohydrates) Low High
MUFA Omega-3
(FatsLipids) High Low
Electrolytes
Phosphorus
Potassium Sodium
Low High
Fluid volume Low High
Caloric density High Standard
Fiber High Low
Prebiotics scFOS Present None
CKD-specific vitamin
amp mineral profile Optimized None
Why Renal Specific ONS
Why Standard versus Renal Specific ONS
Nutrition Intervention in CKD Patients
bull Expert recommendations
KDOQI1 ESPEN2 EBPG3
Nutrition
Support
Individuals undergoing
maintenance dialysis
who are unable to
meet their protein and
energy requirements
with food intake for an
extended period of
time should receive
nutritional support
Special formula
products for HD
treatment can be
useful especially in
malnourished patients
who are not able to
increase their nutrient
intake
Oral nutritional
supplements should
be prescribed if
nutritional counseling
does not achieve an
increase in nutrient
intake to a level that
covers minimum
recommendations
Products
specifically
designed for
dialysis patients
should be
prescribed
1 NKF KDOQI Clinical practice guidelines for nutrition in chronic renal failure AJKD 2000 35S1-S140
2 Cano N et al Clin Nutr 2006 25295-310
3 Fouque D et al NDT 2007 22(suppl 2)ii45-ii87
Recomm-S
ESPEN KDOQI EBPG
Proteini (gkgdan) 12-14 10-12 11
Energija
(kCalkgdan)
35 lt60 g 35
gt60 g 30
30-35
gt50 intke lt1 gkgdan
Actual ntake 20-25 kCalkg 08-1 g proteinakg
Renal Specific Nutritional Therapy
Clinical studies have shown that renal-specific nutrition offers advantages over standard nutrition
bull Phosphorus levels were lower with the renal-specific nutrition than with the standard nutrition1
bull Less fluid and potassium in renal-specific nutrition offers advantages over standard nutrition2
1 Cockram DB et al J Ren Nutr 1998825-33
2 Williams RF Summers AM J Ren Nutr 200919183-188
PREHRANSKE ZAHTEVE DIALIZE
PRAKSA
ENERGIJA 35KCALKG TT NA DAN
PROTEINI 12GKG TT NA DAN
VNOS TEKOČINE 1000ML + IZLOČEN URIN
NATRIJ 2-3G NA DAN
KALIJ 2-3G NA DAN
FOSFOR 08-12GDAN
NKFKDOQI 2000 ADA 2002 WILKENS 2004
BIOIMPEDANCE PRINCIPLES
Phase angle
bull Phase angle is an indicator based on reactance and
resistance obtained from bioelectrical impedance
analysis (BIA)
bull PA depends on cell membrane integrity and on body cell
mass
bull Although its biological meaning is still not clear phase
angle appears to have an important prognostic role
bull Phase angle differs across categories of sex age BMI
and percentage fat bull Maria Cristina G Barbosa-Silva Aluiacutesio JD Barros Jack Wang Steven B Heymsfield and Richard
N Pierson Jr Am J Clin Nutr July 2005 vol 82 no 1 49-52
bull Satish Kumar1 Aswini Dutt1 Sandhya Hemraj2 Shankar Bhat1 and Bhat Manipadybhima Iran
J Basic Med Sci 2012 Nov-Dec 15(6) 1180ndash1184
PHASE ANGLE AND LEAN TISSUE
INDEX ARE SLIGHTLY HIGHER IN
HEMODIALYSIS THAN IN PERITONEAL
DIALYSIS GROUP OF PATIENTS
BKnap ZVeceric Haler JButurovic-Ponikvar
RPonikvar AF Bren
University Clinical Center Ljubljana
Department of Nephrology Slovenia
Ideal nutrition ndash CKD patients
bull Prevents musle loss
bull Prevent andor treat PEW
bull Correct metabolic derrangements
bull Decrease morbidity and mortlity
bull Improve QoL
bull Does not promote progression of CKD
bull Or ideally slow down progression of CKD
ZAKLJUČEK
bull Podhranjenost je pomembna in pogosto
ključna za preživetje
bull Sodobne metode detekcije in zdravljenja
podhranjenosti omogočajo zgodnejšo
nutricijsko intervencijo
bull Prehranski dodatki tako enteralni kot
parenteralni so pogosto nujna in včasih
edina možnost
Kaj je dobro vedetihelliphellip
bull LEDVIČNI BOLNIKI JEDO SLABO
bull V ZAČETNI FAZI KLB TERAPIJA Z OMEJEVANJEM VNOSA PROTEINOV LAHKO PRIPELJE DO MALNUTRICIJE IN KAHEKSIJE
bull POMEMBNA OCENA HRANJENOSTI IN PRAVOČASNA NUTRICIJSKA INTERVENCIJA V VSEH FAZAH KLB
bull USPEH ZDRAVLJENJA MALNUTRICIJE JE POVEZAN Z DOBRIM ZDRAVLJENJEM OSNOVNE LEDVIČNE BOLEZNI IN CELOSTNEGA ZDRAVLJENJA KLB
bull POLEG HRANE VELIKO PRISPEVAJO K KVALITETI ŽIVLJENJA TUDI PREHRANSKI DODATKI IN TELESNA VADBA
bull ANABOLNI AGENSI IN STIMULATORJI APETITA NA NIVOJU HIPOTALAMUSA SO OBET BLIŽNJE PRIHODNOSTI

RX
Cardiovascular and diabetic prescriptions may help
No proof of improved survival
Maintenance therapy
Catabolic
Long waiting time
Risky costly
Repeat kidney failure
Nutrition is the only low-cost effective available treatment
Transplant Dialysis Nutrition
3
Lakota in sitost
Realnost bolnika s KLB
Johansen K L JASN 2007181845-1854
Johansen K L JASN 2007181845-1854
Importance of physical activity
DEBELEJŠI DIALIZNI BOLNIKI
ŽIVIJO DLJE
DIALIZNI BOLNIKI Z ALBUMINI MANJ KOT 30GL
UMIRAJO PREJ
DIA
OMEJEN VNOS ZDRAVE HRANE
PRI KLB
Better nutritional status is associated with improved long
term survival in dialysis patients
Source Chan et al (2012) J Ren Nutr 2012 Nov22(6)547-57
LEDVIČNI BOLNIKI IMAJO SLAB APETIT
bull Izguba apetita in želje za hrano
bull Izguba vonja in okusa
bull Prezgodnja sitost
bull Motnje v delovanju hipotalamusa
bull Vpliv zvišane koncentracije citokinov
bull Omenjeno olajša nastanek kaheksije s
nezadostnim vnosom energije in
proteinov
DIETA LEDVIČNEGA BOLNIKA
Phosphorus balance
ŠTEVILNI VZROKI PODHRANJENOSTI PRI
LEDVIČNI BOLEZNI
bull Zmanjšan vnos hrane
bull Omejevalne diete proteini
bull Uremični toksini
bull Metabolna acidoza
bull Endokrini dejavniki
bull Gastrointestinalni dejavniki
bull MIA sindrom
UREMIČNI SINDROM
Vodi k podhranjenosti tudi zaradi
bull Insulinske rezistence
bull Motenega klirensa lipidov
bull Metabolične acidoze
bull Sekundarnega hiperparatireoidizma
uremične kostne bolezni
DEBELOST OGROŽA TUDI
LEDVIČNE BOLNIKE
bull METABOLIČNI SINDROM
bull SLADKORNA BOLEZEN II
bull MAŠČOBNE CELICE KOT ENDOKRINI ORGAN TUDI PRI KLB VPLIVAJO NA KVS
bull PROBLEM MOTENJ HRANJENJA IN MALNUTRICIJA Z OHRANJENO TELESNO MASO OB ZMANJŠANJU PUSTE TELESNE MASE
bull pomen določanja puste telesne mase z bioimpedanco
bull lean tissue index fat mass index
VLOGA LEPTINA PRI KAHEKSIJI KLB
bull Zvišan pri KLB
bull Deluje podobno kot citokinski receptorji
tipa IL6(vnetje)
bull Preko receptorjev za melanocortin v
hipotalamusu deluje na apetit in
metabolizem
bull Antagonisti MC-R4 receptorja nov
terapevtski obet
VELIK POMEN PREHRANSKE
DIAGNOSTIKE ZA DIALIZNE PACIENTE
bull Klinična presoja pacienta in kvalitete
življenja oziroma uspeha zdravljenja
bull Biokemijavrednosti albuminov
prealbumina in vnosa proteinov (35gl
300mgl 1gkgdan)
bull Nadzor telesna teža BMI SGA
BCM(bioimpedanca) serumski albumin
kreatinin
SUBJEKTIVNA GLOBALNA
NUTRICIJSKA OCENA-SGA
SGA ocena prehranjenosti zajema
bull anamnezo (o spremembi telesne teže o
vnosu hrane simptomih s strani GIT
funkcionalne zmogljivosti) in
bull telesni pregled (atrofija mišic zmanjšanje
podkožne maščobe in pojav oteklin)
bull zlati standard ocene bolnika(Keith
Nutrition in Clinical Practice 2008)
Malnutrition Inflammation Score
(MIS)
bullFully quantitative
bullUses the 7 original SGA components
bullAdds 3 new components
ndashBody mass index
ndashSerum albumin
ndashSerum total iron binding capacity
PEM - PROTEINSKO
ENERGETSKA MALNUTRICIJA
bull PEM je pogost v KLB
bull Je povezan s povečano obolevnostjo in
umrljivostjo
bull 40 PEM na začetku nadomestnega
zdravljenja KOL
bull 10-70 HD pacientov
bull 18-51 CAPD pacientov
Nutritional RecommendationsDialysisStage 5 CKD
KDOQI1 ESPEN2 EBPG3
EnergyCalories lt 60 years 35
kcalkgd
60 years or obese
30-35 kcalkgd
35 kcalkgd 30-40 kcalkgd
Protein 12 gkgd
50 HBV
12-14 gkg
IBWd
11 gkgd
Sodium ― 18-25 gd 2000-3000
mgd
Fluid ― 1000 mL + urine
volume
―
Potassium ― 2000-2500 mgd 1950-2730
mgd
Phosphorus 800-1000 mgd
lt 17 mgkg IBW or
SBWd
800-1000 mgd 800-1000 mgd
Calcium 2 gd ― 2000 mgd
1 NKF KDOQI Clinical practice guidelines for nutrition in chronic renal failure AJKD 2000 35S1-S140
2 Cano N et al Clin Nutr 2006 25295-310
3 Fouque D et al NDT 2007 22(suppl 2)ii45-ii87
Ocena prehranskih potreb
bull V akutni fazi 20-25 nebeljakovinskih kkalkgdan v anabolni fazi in podhranjeni 25 -30 kkalkgdan
bull Maščobe 03 gkg ttdan do 2 gkg ttdan (30 do 70)
bull Ogljikovi hidrati 2-5g kgdan (30 do 70)
bull Beljakovine povprečno 15 g kg tt dan (15 -20 )
bull Mikrohranila-dnevne priporočene potrebe individualno glede na obolenje
bull Opečenci več Cu Se in Zn
AA V PARENTERALNI PREHRANI
bull Povečana izguba AA
bull Neravnovesje med izgubo in porabo
bull Esencielne AA z dodatkom histidina ter arginina niso optimum
bull Nadomeščanje tirozina problem zaradi slabe topnostihellip
bull Acetil-tirozin je rešitev vendar ne pri KLB
bull Rešitev predstavlja dipeptid glicil-tirozin ki je dobro topen in idealno nadomešča večje potrebe po tirozinu pri KLB (AminoMel nephro)
PREHRANSKI DODATKI
Enteralni
bull Nepro Nepro HP Nepro LP Ensure Ensure Plus Advance Prosure Fresubinhellipenkrat na dan per os
bull Glutamin 5-10g na dan per os
bull Carenal 1 tableto po dializi
bull L-karnitin
Parenteralni
bull Aminomel Nephro aminokisline (500ml med HD)
bull Kabiven
bull Glamin 500ml
bull Dipeptiven 100ml
bull Soluvit N(vodotopni vitamini)
bull Vitalipid N(maščobotopni vitamini)
bull Addamel N(mikroelementi)
bull Omegaven (ribje oljehellip)
Component Renal Specific
ONS
Standard ONS
Protein Optimum Medium
Glycemic Index
(Carbohydrates) Low High
MUFA Omega-3
(FatsLipids) High Low
Electrolytes
Phosphorus
Potassium Sodium
Low High
Fluid volume Low High
Caloric density High Standard
Fiber High Low
Prebiotics scFOS Present None
CKD-specific vitamin
amp mineral profile Optimized None
Why Renal Specific ONS
Why Standard versus Renal Specific ONS
Nutrition Intervention in CKD Patients
bull Expert recommendations
KDOQI1 ESPEN2 EBPG3
Nutrition
Support
Individuals undergoing
maintenance dialysis
who are unable to
meet their protein and
energy requirements
with food intake for an
extended period of
time should receive
nutritional support
Special formula
products for HD
treatment can be
useful especially in
malnourished patients
who are not able to
increase their nutrient
intake
Oral nutritional
supplements should
be prescribed if
nutritional counseling
does not achieve an
increase in nutrient
intake to a level that
covers minimum
recommendations
Products
specifically
designed for
dialysis patients
should be
prescribed
1 NKF KDOQI Clinical practice guidelines for nutrition in chronic renal failure AJKD 2000 35S1-S140
2 Cano N et al Clin Nutr 2006 25295-310
3 Fouque D et al NDT 2007 22(suppl 2)ii45-ii87
Recomm-S
ESPEN KDOQI EBPG
Proteini (gkgdan) 12-14 10-12 11
Energija
(kCalkgdan)
35 lt60 g 35
gt60 g 30
30-35
gt50 intke lt1 gkgdan
Actual ntake 20-25 kCalkg 08-1 g proteinakg
Renal Specific Nutritional Therapy
Clinical studies have shown that renal-specific nutrition offers advantages over standard nutrition
bull Phosphorus levels were lower with the renal-specific nutrition than with the standard nutrition1
bull Less fluid and potassium in renal-specific nutrition offers advantages over standard nutrition2
1 Cockram DB et al J Ren Nutr 1998825-33
2 Williams RF Summers AM J Ren Nutr 200919183-188
PREHRANSKE ZAHTEVE DIALIZE
PRAKSA
ENERGIJA 35KCALKG TT NA DAN
PROTEINI 12GKG TT NA DAN
VNOS TEKOČINE 1000ML + IZLOČEN URIN
NATRIJ 2-3G NA DAN
KALIJ 2-3G NA DAN
FOSFOR 08-12GDAN
NKFKDOQI 2000 ADA 2002 WILKENS 2004
BIOIMPEDANCE PRINCIPLES
Phase angle
bull Phase angle is an indicator based on reactance and
resistance obtained from bioelectrical impedance
analysis (BIA)
bull PA depends on cell membrane integrity and on body cell
mass
bull Although its biological meaning is still not clear phase
angle appears to have an important prognostic role
bull Phase angle differs across categories of sex age BMI
and percentage fat bull Maria Cristina G Barbosa-Silva Aluiacutesio JD Barros Jack Wang Steven B Heymsfield and Richard
N Pierson Jr Am J Clin Nutr July 2005 vol 82 no 1 49-52
bull Satish Kumar1 Aswini Dutt1 Sandhya Hemraj2 Shankar Bhat1 and Bhat Manipadybhima Iran
J Basic Med Sci 2012 Nov-Dec 15(6) 1180ndash1184
PHASE ANGLE AND LEAN TISSUE
INDEX ARE SLIGHTLY HIGHER IN
HEMODIALYSIS THAN IN PERITONEAL
DIALYSIS GROUP OF PATIENTS
BKnap ZVeceric Haler JButurovic-Ponikvar
RPonikvar AF Bren
University Clinical Center Ljubljana
Department of Nephrology Slovenia
Ideal nutrition ndash CKD patients
bull Prevents musle loss
bull Prevent andor treat PEW
bull Correct metabolic derrangements
bull Decrease morbidity and mortlity
bull Improve QoL
bull Does not promote progression of CKD
bull Or ideally slow down progression of CKD
ZAKLJUČEK
bull Podhranjenost je pomembna in pogosto
ključna za preživetje
bull Sodobne metode detekcije in zdravljenja
podhranjenosti omogočajo zgodnejšo
nutricijsko intervencijo
bull Prehranski dodatki tako enteralni kot
parenteralni so pogosto nujna in včasih
edina možnost
Kaj je dobro vedetihelliphellip
bull LEDVIČNI BOLNIKI JEDO SLABO
bull V ZAČETNI FAZI KLB TERAPIJA Z OMEJEVANJEM VNOSA PROTEINOV LAHKO PRIPELJE DO MALNUTRICIJE IN KAHEKSIJE
bull POMEMBNA OCENA HRANJENOSTI IN PRAVOČASNA NUTRICIJSKA INTERVENCIJA V VSEH FAZAH KLB
bull USPEH ZDRAVLJENJA MALNUTRICIJE JE POVEZAN Z DOBRIM ZDRAVLJENJEM OSNOVNE LEDVIČNE BOLEZNI IN CELOSTNEGA ZDRAVLJENJA KLB
bull POLEG HRANE VELIKO PRISPEVAJO K KVALITETI ŽIVLJENJA TUDI PREHRANSKI DODATKI IN TELESNA VADBA
bull ANABOLNI AGENSI IN STIMULATORJI APETITA NA NIVOJU HIPOTALAMUSA SO OBET BLIŽNJE PRIHODNOSTI

Lakota in sitost
Realnost bolnika s KLB
Johansen K L JASN 2007181845-1854
Johansen K L JASN 2007181845-1854
Importance of physical activity
DEBELEJŠI DIALIZNI BOLNIKI
ŽIVIJO DLJE
DIALIZNI BOLNIKI Z ALBUMINI MANJ KOT 30GL
UMIRAJO PREJ
DIA
OMEJEN VNOS ZDRAVE HRANE
PRI KLB
Better nutritional status is associated with improved long
term survival in dialysis patients
Source Chan et al (2012) J Ren Nutr 2012 Nov22(6)547-57
LEDVIČNI BOLNIKI IMAJO SLAB APETIT
bull Izguba apetita in želje za hrano
bull Izguba vonja in okusa
bull Prezgodnja sitost
bull Motnje v delovanju hipotalamusa
bull Vpliv zvišane koncentracije citokinov
bull Omenjeno olajša nastanek kaheksije s
nezadostnim vnosom energije in
proteinov
DIETA LEDVIČNEGA BOLNIKA
Phosphorus balance
ŠTEVILNI VZROKI PODHRANJENOSTI PRI
LEDVIČNI BOLEZNI
bull Zmanjšan vnos hrane
bull Omejevalne diete proteini
bull Uremični toksini
bull Metabolna acidoza
bull Endokrini dejavniki
bull Gastrointestinalni dejavniki
bull MIA sindrom
UREMIČNI SINDROM
Vodi k podhranjenosti tudi zaradi
bull Insulinske rezistence
bull Motenega klirensa lipidov
bull Metabolične acidoze
bull Sekundarnega hiperparatireoidizma
uremične kostne bolezni
DEBELOST OGROŽA TUDI
LEDVIČNE BOLNIKE
bull METABOLIČNI SINDROM
bull SLADKORNA BOLEZEN II
bull MAŠČOBNE CELICE KOT ENDOKRINI ORGAN TUDI PRI KLB VPLIVAJO NA KVS
bull PROBLEM MOTENJ HRANJENJA IN MALNUTRICIJA Z OHRANJENO TELESNO MASO OB ZMANJŠANJU PUSTE TELESNE MASE
bull pomen določanja puste telesne mase z bioimpedanco
bull lean tissue index fat mass index
VLOGA LEPTINA PRI KAHEKSIJI KLB
bull Zvišan pri KLB
bull Deluje podobno kot citokinski receptorji
tipa IL6(vnetje)
bull Preko receptorjev za melanocortin v
hipotalamusu deluje na apetit in
metabolizem
bull Antagonisti MC-R4 receptorja nov
terapevtski obet
VELIK POMEN PREHRANSKE
DIAGNOSTIKE ZA DIALIZNE PACIENTE
bull Klinična presoja pacienta in kvalitete
življenja oziroma uspeha zdravljenja
bull Biokemijavrednosti albuminov
prealbumina in vnosa proteinov (35gl
300mgl 1gkgdan)
bull Nadzor telesna teža BMI SGA
BCM(bioimpedanca) serumski albumin
kreatinin
SUBJEKTIVNA GLOBALNA
NUTRICIJSKA OCENA-SGA
SGA ocena prehranjenosti zajema
bull anamnezo (o spremembi telesne teže o
vnosu hrane simptomih s strani GIT
funkcionalne zmogljivosti) in
bull telesni pregled (atrofija mišic zmanjšanje
podkožne maščobe in pojav oteklin)
bull zlati standard ocene bolnika(Keith
Nutrition in Clinical Practice 2008)
Malnutrition Inflammation Score
(MIS)
bullFully quantitative
bullUses the 7 original SGA components
bullAdds 3 new components
ndashBody mass index
ndashSerum albumin
ndashSerum total iron binding capacity
PEM - PROTEINSKO
ENERGETSKA MALNUTRICIJA
bull PEM je pogost v KLB
bull Je povezan s povečano obolevnostjo in
umrljivostjo
bull 40 PEM na začetku nadomestnega
zdravljenja KOL
bull 10-70 HD pacientov
bull 18-51 CAPD pacientov
Nutritional RecommendationsDialysisStage 5 CKD
KDOQI1 ESPEN2 EBPG3
EnergyCalories lt 60 years 35
kcalkgd
60 years or obese
30-35 kcalkgd
35 kcalkgd 30-40 kcalkgd
Protein 12 gkgd
50 HBV
12-14 gkg
IBWd
11 gkgd
Sodium ― 18-25 gd 2000-3000
mgd
Fluid ― 1000 mL + urine
volume
―
Potassium ― 2000-2500 mgd 1950-2730
mgd
Phosphorus 800-1000 mgd
lt 17 mgkg IBW or
SBWd
800-1000 mgd 800-1000 mgd
Calcium 2 gd ― 2000 mgd
1 NKF KDOQI Clinical practice guidelines for nutrition in chronic renal failure AJKD 2000 35S1-S140
2 Cano N et al Clin Nutr 2006 25295-310
3 Fouque D et al NDT 2007 22(suppl 2)ii45-ii87
Ocena prehranskih potreb
bull V akutni fazi 20-25 nebeljakovinskih kkalkgdan v anabolni fazi in podhranjeni 25 -30 kkalkgdan
bull Maščobe 03 gkg ttdan do 2 gkg ttdan (30 do 70)
bull Ogljikovi hidrati 2-5g kgdan (30 do 70)
bull Beljakovine povprečno 15 g kg tt dan (15 -20 )
bull Mikrohranila-dnevne priporočene potrebe individualno glede na obolenje
bull Opečenci več Cu Se in Zn
AA V PARENTERALNI PREHRANI
bull Povečana izguba AA
bull Neravnovesje med izgubo in porabo
bull Esencielne AA z dodatkom histidina ter arginina niso optimum
bull Nadomeščanje tirozina problem zaradi slabe topnostihellip
bull Acetil-tirozin je rešitev vendar ne pri KLB
bull Rešitev predstavlja dipeptid glicil-tirozin ki je dobro topen in idealno nadomešča večje potrebe po tirozinu pri KLB (AminoMel nephro)
PREHRANSKI DODATKI
Enteralni
bull Nepro Nepro HP Nepro LP Ensure Ensure Plus Advance Prosure Fresubinhellipenkrat na dan per os
bull Glutamin 5-10g na dan per os
bull Carenal 1 tableto po dializi
bull L-karnitin
Parenteralni
bull Aminomel Nephro aminokisline (500ml med HD)
bull Kabiven
bull Glamin 500ml
bull Dipeptiven 100ml
bull Soluvit N(vodotopni vitamini)
bull Vitalipid N(maščobotopni vitamini)
bull Addamel N(mikroelementi)
bull Omegaven (ribje oljehellip)
Component Renal Specific
ONS
Standard ONS
Protein Optimum Medium
Glycemic Index
(Carbohydrates) Low High
MUFA Omega-3
(FatsLipids) High Low
Electrolytes
Phosphorus
Potassium Sodium
Low High
Fluid volume Low High
Caloric density High Standard
Fiber High Low
Prebiotics scFOS Present None
CKD-specific vitamin
amp mineral profile Optimized None
Why Renal Specific ONS
Why Standard versus Renal Specific ONS
Nutrition Intervention in CKD Patients
bull Expert recommendations
KDOQI1 ESPEN2 EBPG3
Nutrition
Support
Individuals undergoing
maintenance dialysis
who are unable to
meet their protein and
energy requirements
with food intake for an
extended period of
time should receive
nutritional support
Special formula
products for HD
treatment can be
useful especially in
malnourished patients
who are not able to
increase their nutrient
intake
Oral nutritional
supplements should
be prescribed if
nutritional counseling
does not achieve an
increase in nutrient
intake to a level that
covers minimum
recommendations
Products
specifically
designed for
dialysis patients
should be
prescribed
1 NKF KDOQI Clinical practice guidelines for nutrition in chronic renal failure AJKD 2000 35S1-S140
2 Cano N et al Clin Nutr 2006 25295-310
3 Fouque D et al NDT 2007 22(suppl 2)ii45-ii87
Recomm-S
ESPEN KDOQI EBPG
Proteini (gkgdan) 12-14 10-12 11
Energija
(kCalkgdan)
35 lt60 g 35
gt60 g 30
30-35
gt50 intke lt1 gkgdan
Actual ntake 20-25 kCalkg 08-1 g proteinakg
Renal Specific Nutritional Therapy
Clinical studies have shown that renal-specific nutrition offers advantages over standard nutrition
bull Phosphorus levels were lower with the renal-specific nutrition than with the standard nutrition1
bull Less fluid and potassium in renal-specific nutrition offers advantages over standard nutrition2
1 Cockram DB et al J Ren Nutr 1998825-33
2 Williams RF Summers AM J Ren Nutr 200919183-188
PREHRANSKE ZAHTEVE DIALIZE
PRAKSA
ENERGIJA 35KCALKG TT NA DAN
PROTEINI 12GKG TT NA DAN
VNOS TEKOČINE 1000ML + IZLOČEN URIN
NATRIJ 2-3G NA DAN
KALIJ 2-3G NA DAN
FOSFOR 08-12GDAN
NKFKDOQI 2000 ADA 2002 WILKENS 2004
BIOIMPEDANCE PRINCIPLES
Phase angle
bull Phase angle is an indicator based on reactance and
resistance obtained from bioelectrical impedance
analysis (BIA)
bull PA depends on cell membrane integrity and on body cell
mass
bull Although its biological meaning is still not clear phase
angle appears to have an important prognostic role
bull Phase angle differs across categories of sex age BMI
and percentage fat bull Maria Cristina G Barbosa-Silva Aluiacutesio JD Barros Jack Wang Steven B Heymsfield and Richard
N Pierson Jr Am J Clin Nutr July 2005 vol 82 no 1 49-52
bull Satish Kumar1 Aswini Dutt1 Sandhya Hemraj2 Shankar Bhat1 and Bhat Manipadybhima Iran
J Basic Med Sci 2012 Nov-Dec 15(6) 1180ndash1184
PHASE ANGLE AND LEAN TISSUE
INDEX ARE SLIGHTLY HIGHER IN
HEMODIALYSIS THAN IN PERITONEAL
DIALYSIS GROUP OF PATIENTS
BKnap ZVeceric Haler JButurovic-Ponikvar
RPonikvar AF Bren
University Clinical Center Ljubljana
Department of Nephrology Slovenia
Ideal nutrition ndash CKD patients
bull Prevents musle loss
bull Prevent andor treat PEW
bull Correct metabolic derrangements
bull Decrease morbidity and mortlity
bull Improve QoL
bull Does not promote progression of CKD
bull Or ideally slow down progression of CKD
ZAKLJUČEK
bull Podhranjenost je pomembna in pogosto
ključna za preživetje
bull Sodobne metode detekcije in zdravljenja
podhranjenosti omogočajo zgodnejšo
nutricijsko intervencijo
bull Prehranski dodatki tako enteralni kot
parenteralni so pogosto nujna in včasih
edina možnost
Kaj je dobro vedetihelliphellip
bull LEDVIČNI BOLNIKI JEDO SLABO
bull V ZAČETNI FAZI KLB TERAPIJA Z OMEJEVANJEM VNOSA PROTEINOV LAHKO PRIPELJE DO MALNUTRICIJE IN KAHEKSIJE
bull POMEMBNA OCENA HRANJENOSTI IN PRAVOČASNA NUTRICIJSKA INTERVENCIJA V VSEH FAZAH KLB
bull USPEH ZDRAVLJENJA MALNUTRICIJE JE POVEZAN Z DOBRIM ZDRAVLJENJEM OSNOVNE LEDVIČNE BOLEZNI IN CELOSTNEGA ZDRAVLJENJA KLB
bull POLEG HRANE VELIKO PRISPEVAJO K KVALITETI ŽIVLJENJA TUDI PREHRANSKI DODATKI IN TELESNA VADBA
bull ANABOLNI AGENSI IN STIMULATORJI APETITA NA NIVOJU HIPOTALAMUSA SO OBET BLIŽNJE PRIHODNOSTI

Realnost bolnika s KLB
Johansen K L JASN 2007181845-1854
Johansen K L JASN 2007181845-1854
Importance of physical activity
DEBELEJŠI DIALIZNI BOLNIKI
ŽIVIJO DLJE
DIALIZNI BOLNIKI Z ALBUMINI MANJ KOT 30GL
UMIRAJO PREJ
DIA
OMEJEN VNOS ZDRAVE HRANE
PRI KLB
Better nutritional status is associated with improved long
term survival in dialysis patients
Source Chan et al (2012) J Ren Nutr 2012 Nov22(6)547-57
LEDVIČNI BOLNIKI IMAJO SLAB APETIT
bull Izguba apetita in želje za hrano
bull Izguba vonja in okusa
bull Prezgodnja sitost
bull Motnje v delovanju hipotalamusa
bull Vpliv zvišane koncentracije citokinov
bull Omenjeno olajša nastanek kaheksije s
nezadostnim vnosom energije in
proteinov
DIETA LEDVIČNEGA BOLNIKA
Phosphorus balance
ŠTEVILNI VZROKI PODHRANJENOSTI PRI
LEDVIČNI BOLEZNI
bull Zmanjšan vnos hrane
bull Omejevalne diete proteini
bull Uremični toksini
bull Metabolna acidoza
bull Endokrini dejavniki
bull Gastrointestinalni dejavniki
bull MIA sindrom
UREMIČNI SINDROM
Vodi k podhranjenosti tudi zaradi
bull Insulinske rezistence
bull Motenega klirensa lipidov
bull Metabolične acidoze
bull Sekundarnega hiperparatireoidizma
uremične kostne bolezni
DEBELOST OGROŽA TUDI
LEDVIČNE BOLNIKE
bull METABOLIČNI SINDROM
bull SLADKORNA BOLEZEN II
bull MAŠČOBNE CELICE KOT ENDOKRINI ORGAN TUDI PRI KLB VPLIVAJO NA KVS
bull PROBLEM MOTENJ HRANJENJA IN MALNUTRICIJA Z OHRANJENO TELESNO MASO OB ZMANJŠANJU PUSTE TELESNE MASE
bull pomen določanja puste telesne mase z bioimpedanco
bull lean tissue index fat mass index
VLOGA LEPTINA PRI KAHEKSIJI KLB
bull Zvišan pri KLB
bull Deluje podobno kot citokinski receptorji
tipa IL6(vnetje)
bull Preko receptorjev za melanocortin v
hipotalamusu deluje na apetit in
metabolizem
bull Antagonisti MC-R4 receptorja nov
terapevtski obet
VELIK POMEN PREHRANSKE
DIAGNOSTIKE ZA DIALIZNE PACIENTE
bull Klinična presoja pacienta in kvalitete
življenja oziroma uspeha zdravljenja
bull Biokemijavrednosti albuminov
prealbumina in vnosa proteinov (35gl
300mgl 1gkgdan)
bull Nadzor telesna teža BMI SGA
BCM(bioimpedanca) serumski albumin
kreatinin
SUBJEKTIVNA GLOBALNA
NUTRICIJSKA OCENA-SGA
SGA ocena prehranjenosti zajema
bull anamnezo (o spremembi telesne teže o
vnosu hrane simptomih s strani GIT
funkcionalne zmogljivosti) in
bull telesni pregled (atrofija mišic zmanjšanje
podkožne maščobe in pojav oteklin)
bull zlati standard ocene bolnika(Keith
Nutrition in Clinical Practice 2008)
Malnutrition Inflammation Score
(MIS)
bullFully quantitative
bullUses the 7 original SGA components
bullAdds 3 new components
ndashBody mass index
ndashSerum albumin
ndashSerum total iron binding capacity
PEM - PROTEINSKO
ENERGETSKA MALNUTRICIJA
bull PEM je pogost v KLB
bull Je povezan s povečano obolevnostjo in
umrljivostjo
bull 40 PEM na začetku nadomestnega
zdravljenja KOL
bull 10-70 HD pacientov
bull 18-51 CAPD pacientov
Nutritional RecommendationsDialysisStage 5 CKD
KDOQI1 ESPEN2 EBPG3
EnergyCalories lt 60 years 35
kcalkgd
60 years or obese
30-35 kcalkgd
35 kcalkgd 30-40 kcalkgd
Protein 12 gkgd
50 HBV
12-14 gkg
IBWd
11 gkgd
Sodium ― 18-25 gd 2000-3000
mgd
Fluid ― 1000 mL + urine
volume
―
Potassium ― 2000-2500 mgd 1950-2730
mgd
Phosphorus 800-1000 mgd
lt 17 mgkg IBW or
SBWd
800-1000 mgd 800-1000 mgd
Calcium 2 gd ― 2000 mgd
1 NKF KDOQI Clinical practice guidelines for nutrition in chronic renal failure AJKD 2000 35S1-S140
2 Cano N et al Clin Nutr 2006 25295-310
3 Fouque D et al NDT 2007 22(suppl 2)ii45-ii87
Ocena prehranskih potreb
bull V akutni fazi 20-25 nebeljakovinskih kkalkgdan v anabolni fazi in podhranjeni 25 -30 kkalkgdan
bull Maščobe 03 gkg ttdan do 2 gkg ttdan (30 do 70)
bull Ogljikovi hidrati 2-5g kgdan (30 do 70)
bull Beljakovine povprečno 15 g kg tt dan (15 -20 )
bull Mikrohranila-dnevne priporočene potrebe individualno glede na obolenje
bull Opečenci več Cu Se in Zn
AA V PARENTERALNI PREHRANI
bull Povečana izguba AA
bull Neravnovesje med izgubo in porabo
bull Esencielne AA z dodatkom histidina ter arginina niso optimum
bull Nadomeščanje tirozina problem zaradi slabe topnostihellip
bull Acetil-tirozin je rešitev vendar ne pri KLB
bull Rešitev predstavlja dipeptid glicil-tirozin ki je dobro topen in idealno nadomešča večje potrebe po tirozinu pri KLB (AminoMel nephro)
PREHRANSKI DODATKI
Enteralni
bull Nepro Nepro HP Nepro LP Ensure Ensure Plus Advance Prosure Fresubinhellipenkrat na dan per os
bull Glutamin 5-10g na dan per os
bull Carenal 1 tableto po dializi
bull L-karnitin
Parenteralni
bull Aminomel Nephro aminokisline (500ml med HD)
bull Kabiven
bull Glamin 500ml
bull Dipeptiven 100ml
bull Soluvit N(vodotopni vitamini)
bull Vitalipid N(maščobotopni vitamini)
bull Addamel N(mikroelementi)
bull Omegaven (ribje oljehellip)
Component Renal Specific
ONS
Standard ONS
Protein Optimum Medium
Glycemic Index
(Carbohydrates) Low High
MUFA Omega-3
(FatsLipids) High Low
Electrolytes
Phosphorus
Potassium Sodium
Low High
Fluid volume Low High
Caloric density High Standard
Fiber High Low
Prebiotics scFOS Present None
CKD-specific vitamin
amp mineral profile Optimized None
Why Renal Specific ONS
Why Standard versus Renal Specific ONS
Nutrition Intervention in CKD Patients
bull Expert recommendations
KDOQI1 ESPEN2 EBPG3
Nutrition
Support
Individuals undergoing
maintenance dialysis
who are unable to
meet their protein and
energy requirements
with food intake for an
extended period of
time should receive
nutritional support
Special formula
products for HD
treatment can be
useful especially in
malnourished patients
who are not able to
increase their nutrient
intake
Oral nutritional
supplements should
be prescribed if
nutritional counseling
does not achieve an
increase in nutrient
intake to a level that
covers minimum
recommendations
Products
specifically
designed for
dialysis patients
should be
prescribed
1 NKF KDOQI Clinical practice guidelines for nutrition in chronic renal failure AJKD 2000 35S1-S140
2 Cano N et al Clin Nutr 2006 25295-310
3 Fouque D et al NDT 2007 22(suppl 2)ii45-ii87
Recomm-S
ESPEN KDOQI EBPG
Proteini (gkgdan) 12-14 10-12 11
Energija
(kCalkgdan)
35 lt60 g 35
gt60 g 30
30-35
gt50 intke lt1 gkgdan
Actual ntake 20-25 kCalkg 08-1 g proteinakg
Renal Specific Nutritional Therapy
Clinical studies have shown that renal-specific nutrition offers advantages over standard nutrition
bull Phosphorus levels were lower with the renal-specific nutrition than with the standard nutrition1
bull Less fluid and potassium in renal-specific nutrition offers advantages over standard nutrition2
1 Cockram DB et al J Ren Nutr 1998825-33
2 Williams RF Summers AM J Ren Nutr 200919183-188
PREHRANSKE ZAHTEVE DIALIZE
PRAKSA
ENERGIJA 35KCALKG TT NA DAN
PROTEINI 12GKG TT NA DAN
VNOS TEKOČINE 1000ML + IZLOČEN URIN
NATRIJ 2-3G NA DAN
KALIJ 2-3G NA DAN
FOSFOR 08-12GDAN
NKFKDOQI 2000 ADA 2002 WILKENS 2004
BIOIMPEDANCE PRINCIPLES
Phase angle
bull Phase angle is an indicator based on reactance and
resistance obtained from bioelectrical impedance
analysis (BIA)
bull PA depends on cell membrane integrity and on body cell
mass
bull Although its biological meaning is still not clear phase
angle appears to have an important prognostic role
bull Phase angle differs across categories of sex age BMI
and percentage fat bull Maria Cristina G Barbosa-Silva Aluiacutesio JD Barros Jack Wang Steven B Heymsfield and Richard
N Pierson Jr Am J Clin Nutr July 2005 vol 82 no 1 49-52
bull Satish Kumar1 Aswini Dutt1 Sandhya Hemraj2 Shankar Bhat1 and Bhat Manipadybhima Iran
J Basic Med Sci 2012 Nov-Dec 15(6) 1180ndash1184
PHASE ANGLE AND LEAN TISSUE
INDEX ARE SLIGHTLY HIGHER IN
HEMODIALYSIS THAN IN PERITONEAL
DIALYSIS GROUP OF PATIENTS
BKnap ZVeceric Haler JButurovic-Ponikvar
RPonikvar AF Bren
University Clinical Center Ljubljana
Department of Nephrology Slovenia
Ideal nutrition ndash CKD patients
bull Prevents musle loss
bull Prevent andor treat PEW
bull Correct metabolic derrangements
bull Decrease morbidity and mortlity
bull Improve QoL
bull Does not promote progression of CKD
bull Or ideally slow down progression of CKD
ZAKLJUČEK
bull Podhranjenost je pomembna in pogosto
ključna za preživetje
bull Sodobne metode detekcije in zdravljenja
podhranjenosti omogočajo zgodnejšo
nutricijsko intervencijo
bull Prehranski dodatki tako enteralni kot
parenteralni so pogosto nujna in včasih
edina možnost
Kaj je dobro vedetihelliphellip
bull LEDVIČNI BOLNIKI JEDO SLABO
bull V ZAČETNI FAZI KLB TERAPIJA Z OMEJEVANJEM VNOSA PROTEINOV LAHKO PRIPELJE DO MALNUTRICIJE IN KAHEKSIJE
bull POMEMBNA OCENA HRANJENOSTI IN PRAVOČASNA NUTRICIJSKA INTERVENCIJA V VSEH FAZAH KLB
bull USPEH ZDRAVLJENJA MALNUTRICIJE JE POVEZAN Z DOBRIM ZDRAVLJENJEM OSNOVNE LEDVIČNE BOLEZNI IN CELOSTNEGA ZDRAVLJENJA KLB
bull POLEG HRANE VELIKO PRISPEVAJO K KVALITETI ŽIVLJENJA TUDI PREHRANSKI DODATKI IN TELESNA VADBA
bull ANABOLNI AGENSI IN STIMULATORJI APETITA NA NIVOJU HIPOTALAMUSA SO OBET BLIŽNJE PRIHODNOSTI

Johansen K L JASN 2007181845-1854
Johansen K L JASN 2007181845-1854
Importance of physical activity
DEBELEJŠI DIALIZNI BOLNIKI
ŽIVIJO DLJE
DIALIZNI BOLNIKI Z ALBUMINI MANJ KOT 30GL
UMIRAJO PREJ
DIA
OMEJEN VNOS ZDRAVE HRANE
PRI KLB
Better nutritional status is associated with improved long
term survival in dialysis patients
Source Chan et al (2012) J Ren Nutr 2012 Nov22(6)547-57
LEDVIČNI BOLNIKI IMAJO SLAB APETIT
bull Izguba apetita in želje za hrano
bull Izguba vonja in okusa
bull Prezgodnja sitost
bull Motnje v delovanju hipotalamusa
bull Vpliv zvišane koncentracije citokinov
bull Omenjeno olajša nastanek kaheksije s
nezadostnim vnosom energije in
proteinov
DIETA LEDVIČNEGA BOLNIKA
Phosphorus balance
ŠTEVILNI VZROKI PODHRANJENOSTI PRI
LEDVIČNI BOLEZNI
bull Zmanjšan vnos hrane
bull Omejevalne diete proteini
bull Uremični toksini
bull Metabolna acidoza
bull Endokrini dejavniki
bull Gastrointestinalni dejavniki
bull MIA sindrom
UREMIČNI SINDROM
Vodi k podhranjenosti tudi zaradi
bull Insulinske rezistence
bull Motenega klirensa lipidov
bull Metabolične acidoze
bull Sekundarnega hiperparatireoidizma
uremične kostne bolezni
DEBELOST OGROŽA TUDI
LEDVIČNE BOLNIKE
bull METABOLIČNI SINDROM
bull SLADKORNA BOLEZEN II
bull MAŠČOBNE CELICE KOT ENDOKRINI ORGAN TUDI PRI KLB VPLIVAJO NA KVS
bull PROBLEM MOTENJ HRANJENJA IN MALNUTRICIJA Z OHRANJENO TELESNO MASO OB ZMANJŠANJU PUSTE TELESNE MASE
bull pomen določanja puste telesne mase z bioimpedanco
bull lean tissue index fat mass index
VLOGA LEPTINA PRI KAHEKSIJI KLB
bull Zvišan pri KLB
bull Deluje podobno kot citokinski receptorji
tipa IL6(vnetje)
bull Preko receptorjev za melanocortin v
hipotalamusu deluje na apetit in
metabolizem
bull Antagonisti MC-R4 receptorja nov
terapevtski obet
VELIK POMEN PREHRANSKE
DIAGNOSTIKE ZA DIALIZNE PACIENTE
bull Klinična presoja pacienta in kvalitete
življenja oziroma uspeha zdravljenja
bull Biokemijavrednosti albuminov
prealbumina in vnosa proteinov (35gl
300mgl 1gkgdan)
bull Nadzor telesna teža BMI SGA
BCM(bioimpedanca) serumski albumin
kreatinin
SUBJEKTIVNA GLOBALNA
NUTRICIJSKA OCENA-SGA
SGA ocena prehranjenosti zajema
bull anamnezo (o spremembi telesne teže o
vnosu hrane simptomih s strani GIT
funkcionalne zmogljivosti) in
bull telesni pregled (atrofija mišic zmanjšanje
podkožne maščobe in pojav oteklin)
bull zlati standard ocene bolnika(Keith
Nutrition in Clinical Practice 2008)
Malnutrition Inflammation Score
(MIS)
bullFully quantitative
bullUses the 7 original SGA components
bullAdds 3 new components
ndashBody mass index
ndashSerum albumin
ndashSerum total iron binding capacity
PEM - PROTEINSKO
ENERGETSKA MALNUTRICIJA
bull PEM je pogost v KLB
bull Je povezan s povečano obolevnostjo in
umrljivostjo
bull 40 PEM na začetku nadomestnega
zdravljenja KOL
bull 10-70 HD pacientov
bull 18-51 CAPD pacientov
Nutritional RecommendationsDialysisStage 5 CKD
KDOQI1 ESPEN2 EBPG3
EnergyCalories lt 60 years 35
kcalkgd
60 years or obese
30-35 kcalkgd
35 kcalkgd 30-40 kcalkgd
Protein 12 gkgd
50 HBV
12-14 gkg
IBWd
11 gkgd
Sodium ― 18-25 gd 2000-3000
mgd
Fluid ― 1000 mL + urine
volume
―
Potassium ― 2000-2500 mgd 1950-2730
mgd
Phosphorus 800-1000 mgd
lt 17 mgkg IBW or
SBWd
800-1000 mgd 800-1000 mgd
Calcium 2 gd ― 2000 mgd
1 NKF KDOQI Clinical practice guidelines for nutrition in chronic renal failure AJKD 2000 35S1-S140
2 Cano N et al Clin Nutr 2006 25295-310
3 Fouque D et al NDT 2007 22(suppl 2)ii45-ii87
Ocena prehranskih potreb
bull V akutni fazi 20-25 nebeljakovinskih kkalkgdan v anabolni fazi in podhranjeni 25 -30 kkalkgdan
bull Maščobe 03 gkg ttdan do 2 gkg ttdan (30 do 70)
bull Ogljikovi hidrati 2-5g kgdan (30 do 70)
bull Beljakovine povprečno 15 g kg tt dan (15 -20 )
bull Mikrohranila-dnevne priporočene potrebe individualno glede na obolenje
bull Opečenci več Cu Se in Zn
AA V PARENTERALNI PREHRANI
bull Povečana izguba AA
bull Neravnovesje med izgubo in porabo
bull Esencielne AA z dodatkom histidina ter arginina niso optimum
bull Nadomeščanje tirozina problem zaradi slabe topnostihellip
bull Acetil-tirozin je rešitev vendar ne pri KLB
bull Rešitev predstavlja dipeptid glicil-tirozin ki je dobro topen in idealno nadomešča večje potrebe po tirozinu pri KLB (AminoMel nephro)
PREHRANSKI DODATKI
Enteralni
bull Nepro Nepro HP Nepro LP Ensure Ensure Plus Advance Prosure Fresubinhellipenkrat na dan per os
bull Glutamin 5-10g na dan per os
bull Carenal 1 tableto po dializi
bull L-karnitin
Parenteralni
bull Aminomel Nephro aminokisline (500ml med HD)
bull Kabiven
bull Glamin 500ml
bull Dipeptiven 100ml
bull Soluvit N(vodotopni vitamini)
bull Vitalipid N(maščobotopni vitamini)
bull Addamel N(mikroelementi)
bull Omegaven (ribje oljehellip)
Component Renal Specific
ONS
Standard ONS
Protein Optimum Medium
Glycemic Index
(Carbohydrates) Low High
MUFA Omega-3
(FatsLipids) High Low
Electrolytes
Phosphorus
Potassium Sodium
Low High
Fluid volume Low High
Caloric density High Standard
Fiber High Low
Prebiotics scFOS Present None
CKD-specific vitamin
amp mineral profile Optimized None
Why Renal Specific ONS
Why Standard versus Renal Specific ONS
Nutrition Intervention in CKD Patients
bull Expert recommendations
KDOQI1 ESPEN2 EBPG3
Nutrition
Support
Individuals undergoing
maintenance dialysis
who are unable to
meet their protein and
energy requirements
with food intake for an
extended period of
time should receive
nutritional support
Special formula
products for HD
treatment can be
useful especially in
malnourished patients
who are not able to
increase their nutrient
intake
Oral nutritional
supplements should
be prescribed if
nutritional counseling
does not achieve an
increase in nutrient
intake to a level that
covers minimum
recommendations
Products
specifically
designed for
dialysis patients
should be
prescribed
1 NKF KDOQI Clinical practice guidelines for nutrition in chronic renal failure AJKD 2000 35S1-S140
2 Cano N et al Clin Nutr 2006 25295-310
3 Fouque D et al NDT 2007 22(suppl 2)ii45-ii87
Recomm-S
ESPEN KDOQI EBPG
Proteini (gkgdan) 12-14 10-12 11
Energija
(kCalkgdan)
35 lt60 g 35
gt60 g 30
30-35
gt50 intke lt1 gkgdan
Actual ntake 20-25 kCalkg 08-1 g proteinakg
Renal Specific Nutritional Therapy
Clinical studies have shown that renal-specific nutrition offers advantages over standard nutrition
bull Phosphorus levels were lower with the renal-specific nutrition than with the standard nutrition1
bull Less fluid and potassium in renal-specific nutrition offers advantages over standard nutrition2
1 Cockram DB et al J Ren Nutr 1998825-33
2 Williams RF Summers AM J Ren Nutr 200919183-188
PREHRANSKE ZAHTEVE DIALIZE
PRAKSA
ENERGIJA 35KCALKG TT NA DAN
PROTEINI 12GKG TT NA DAN
VNOS TEKOČINE 1000ML + IZLOČEN URIN
NATRIJ 2-3G NA DAN
KALIJ 2-3G NA DAN
FOSFOR 08-12GDAN
NKFKDOQI 2000 ADA 2002 WILKENS 2004
BIOIMPEDANCE PRINCIPLES
Phase angle
bull Phase angle is an indicator based on reactance and
resistance obtained from bioelectrical impedance
analysis (BIA)
bull PA depends on cell membrane integrity and on body cell
mass
bull Although its biological meaning is still not clear phase
angle appears to have an important prognostic role
bull Phase angle differs across categories of sex age BMI
and percentage fat bull Maria Cristina G Barbosa-Silva Aluiacutesio JD Barros Jack Wang Steven B Heymsfield and Richard
N Pierson Jr Am J Clin Nutr July 2005 vol 82 no 1 49-52
bull Satish Kumar1 Aswini Dutt1 Sandhya Hemraj2 Shankar Bhat1 and Bhat Manipadybhima Iran
J Basic Med Sci 2012 Nov-Dec 15(6) 1180ndash1184
PHASE ANGLE AND LEAN TISSUE
INDEX ARE SLIGHTLY HIGHER IN
HEMODIALYSIS THAN IN PERITONEAL
DIALYSIS GROUP OF PATIENTS
BKnap ZVeceric Haler JButurovic-Ponikvar
RPonikvar AF Bren
University Clinical Center Ljubljana
Department of Nephrology Slovenia
Ideal nutrition ndash CKD patients
bull Prevents musle loss
bull Prevent andor treat PEW
bull Correct metabolic derrangements
bull Decrease morbidity and mortlity
bull Improve QoL
bull Does not promote progression of CKD
bull Or ideally slow down progression of CKD
ZAKLJUČEK
bull Podhranjenost je pomembna in pogosto
ključna za preživetje
bull Sodobne metode detekcije in zdravljenja
podhranjenosti omogočajo zgodnejšo
nutricijsko intervencijo
bull Prehranski dodatki tako enteralni kot
parenteralni so pogosto nujna in včasih
edina možnost
Kaj je dobro vedetihelliphellip
bull LEDVIČNI BOLNIKI JEDO SLABO
bull V ZAČETNI FAZI KLB TERAPIJA Z OMEJEVANJEM VNOSA PROTEINOV LAHKO PRIPELJE DO MALNUTRICIJE IN KAHEKSIJE
bull POMEMBNA OCENA HRANJENOSTI IN PRAVOČASNA NUTRICIJSKA INTERVENCIJA V VSEH FAZAH KLB
bull USPEH ZDRAVLJENJA MALNUTRICIJE JE POVEZAN Z DOBRIM ZDRAVLJENJEM OSNOVNE LEDVIČNE BOLEZNI IN CELOSTNEGA ZDRAVLJENJA KLB
bull POLEG HRANE VELIKO PRISPEVAJO K KVALITETI ŽIVLJENJA TUDI PREHRANSKI DODATKI IN TELESNA VADBA
bull ANABOLNI AGENSI IN STIMULATORJI APETITA NA NIVOJU HIPOTALAMUSA SO OBET BLIŽNJE PRIHODNOSTI

Johansen K L JASN 2007181845-1854
Importance of physical activity
DEBELEJŠI DIALIZNI BOLNIKI
ŽIVIJO DLJE
DIALIZNI BOLNIKI Z ALBUMINI MANJ KOT 30GL
UMIRAJO PREJ
DIA
OMEJEN VNOS ZDRAVE HRANE
PRI KLB
Better nutritional status is associated with improved long
term survival in dialysis patients
Source Chan et al (2012) J Ren Nutr 2012 Nov22(6)547-57
LEDVIČNI BOLNIKI IMAJO SLAB APETIT
bull Izguba apetita in želje za hrano
bull Izguba vonja in okusa
bull Prezgodnja sitost
bull Motnje v delovanju hipotalamusa
bull Vpliv zvišane koncentracije citokinov
bull Omenjeno olajša nastanek kaheksije s
nezadostnim vnosom energije in
proteinov
DIETA LEDVIČNEGA BOLNIKA
Phosphorus balance
ŠTEVILNI VZROKI PODHRANJENOSTI PRI
LEDVIČNI BOLEZNI
bull Zmanjšan vnos hrane
bull Omejevalne diete proteini
bull Uremični toksini
bull Metabolna acidoza
bull Endokrini dejavniki
bull Gastrointestinalni dejavniki
bull MIA sindrom
UREMIČNI SINDROM
Vodi k podhranjenosti tudi zaradi
bull Insulinske rezistence
bull Motenega klirensa lipidov
bull Metabolične acidoze
bull Sekundarnega hiperparatireoidizma
uremične kostne bolezni
DEBELOST OGROŽA TUDI
LEDVIČNE BOLNIKE
bull METABOLIČNI SINDROM
bull SLADKORNA BOLEZEN II
bull MAŠČOBNE CELICE KOT ENDOKRINI ORGAN TUDI PRI KLB VPLIVAJO NA KVS
bull PROBLEM MOTENJ HRANJENJA IN MALNUTRICIJA Z OHRANJENO TELESNO MASO OB ZMANJŠANJU PUSTE TELESNE MASE
bull pomen določanja puste telesne mase z bioimpedanco
bull lean tissue index fat mass index
VLOGA LEPTINA PRI KAHEKSIJI KLB
bull Zvišan pri KLB
bull Deluje podobno kot citokinski receptorji
tipa IL6(vnetje)
bull Preko receptorjev za melanocortin v
hipotalamusu deluje na apetit in
metabolizem
bull Antagonisti MC-R4 receptorja nov
terapevtski obet
VELIK POMEN PREHRANSKE
DIAGNOSTIKE ZA DIALIZNE PACIENTE
bull Klinična presoja pacienta in kvalitete
življenja oziroma uspeha zdravljenja
bull Biokemijavrednosti albuminov
prealbumina in vnosa proteinov (35gl
300mgl 1gkgdan)
bull Nadzor telesna teža BMI SGA
BCM(bioimpedanca) serumski albumin
kreatinin
SUBJEKTIVNA GLOBALNA
NUTRICIJSKA OCENA-SGA
SGA ocena prehranjenosti zajema
bull anamnezo (o spremembi telesne teže o
vnosu hrane simptomih s strani GIT
funkcionalne zmogljivosti) in
bull telesni pregled (atrofija mišic zmanjšanje
podkožne maščobe in pojav oteklin)
bull zlati standard ocene bolnika(Keith
Nutrition in Clinical Practice 2008)
Malnutrition Inflammation Score
(MIS)
bullFully quantitative
bullUses the 7 original SGA components
bullAdds 3 new components
ndashBody mass index
ndashSerum albumin
ndashSerum total iron binding capacity
PEM - PROTEINSKO
ENERGETSKA MALNUTRICIJA
bull PEM je pogost v KLB
bull Je povezan s povečano obolevnostjo in
umrljivostjo
bull 40 PEM na začetku nadomestnega
zdravljenja KOL
bull 10-70 HD pacientov
bull 18-51 CAPD pacientov
Nutritional RecommendationsDialysisStage 5 CKD
KDOQI1 ESPEN2 EBPG3
EnergyCalories lt 60 years 35
kcalkgd
60 years or obese
30-35 kcalkgd
35 kcalkgd 30-40 kcalkgd
Protein 12 gkgd
50 HBV
12-14 gkg
IBWd
11 gkgd
Sodium ― 18-25 gd 2000-3000
mgd
Fluid ― 1000 mL + urine
volume
―
Potassium ― 2000-2500 mgd 1950-2730
mgd
Phosphorus 800-1000 mgd
lt 17 mgkg IBW or
SBWd
800-1000 mgd 800-1000 mgd
Calcium 2 gd ― 2000 mgd
1 NKF KDOQI Clinical practice guidelines for nutrition in chronic renal failure AJKD 2000 35S1-S140
2 Cano N et al Clin Nutr 2006 25295-310
3 Fouque D et al NDT 2007 22(suppl 2)ii45-ii87
Ocena prehranskih potreb
bull V akutni fazi 20-25 nebeljakovinskih kkalkgdan v anabolni fazi in podhranjeni 25 -30 kkalkgdan
bull Maščobe 03 gkg ttdan do 2 gkg ttdan (30 do 70)
bull Ogljikovi hidrati 2-5g kgdan (30 do 70)
bull Beljakovine povprečno 15 g kg tt dan (15 -20 )
bull Mikrohranila-dnevne priporočene potrebe individualno glede na obolenje
bull Opečenci več Cu Se in Zn
AA V PARENTERALNI PREHRANI
bull Povečana izguba AA
bull Neravnovesje med izgubo in porabo
bull Esencielne AA z dodatkom histidina ter arginina niso optimum
bull Nadomeščanje tirozina problem zaradi slabe topnostihellip
bull Acetil-tirozin je rešitev vendar ne pri KLB
bull Rešitev predstavlja dipeptid glicil-tirozin ki je dobro topen in idealno nadomešča večje potrebe po tirozinu pri KLB (AminoMel nephro)
PREHRANSKI DODATKI
Enteralni
bull Nepro Nepro HP Nepro LP Ensure Ensure Plus Advance Prosure Fresubinhellipenkrat na dan per os
bull Glutamin 5-10g na dan per os
bull Carenal 1 tableto po dializi
bull L-karnitin
Parenteralni
bull Aminomel Nephro aminokisline (500ml med HD)
bull Kabiven
bull Glamin 500ml
bull Dipeptiven 100ml
bull Soluvit N(vodotopni vitamini)
bull Vitalipid N(maščobotopni vitamini)
bull Addamel N(mikroelementi)
bull Omegaven (ribje oljehellip)
Component Renal Specific
ONS
Standard ONS
Protein Optimum Medium
Glycemic Index
(Carbohydrates) Low High
MUFA Omega-3
(FatsLipids) High Low
Electrolytes
Phosphorus
Potassium Sodium
Low High
Fluid volume Low High
Caloric density High Standard
Fiber High Low
Prebiotics scFOS Present None
CKD-specific vitamin
amp mineral profile Optimized None
Why Renal Specific ONS
Why Standard versus Renal Specific ONS
Nutrition Intervention in CKD Patients
bull Expert recommendations
KDOQI1 ESPEN2 EBPG3
Nutrition
Support
Individuals undergoing
maintenance dialysis
who are unable to
meet their protein and
energy requirements
with food intake for an
extended period of
time should receive
nutritional support
Special formula
products for HD
treatment can be
useful especially in
malnourished patients
who are not able to
increase their nutrient
intake
Oral nutritional
supplements should
be prescribed if
nutritional counseling
does not achieve an
increase in nutrient
intake to a level that
covers minimum
recommendations
Products
specifically
designed for
dialysis patients
should be
prescribed
1 NKF KDOQI Clinical practice guidelines for nutrition in chronic renal failure AJKD 2000 35S1-S140
2 Cano N et al Clin Nutr 2006 25295-310
3 Fouque D et al NDT 2007 22(suppl 2)ii45-ii87
Recomm-S
ESPEN KDOQI EBPG
Proteini (gkgdan) 12-14 10-12 11
Energija
(kCalkgdan)
35 lt60 g 35
gt60 g 30
30-35
gt50 intke lt1 gkgdan
Actual ntake 20-25 kCalkg 08-1 g proteinakg
Renal Specific Nutritional Therapy
Clinical studies have shown that renal-specific nutrition offers advantages over standard nutrition
bull Phosphorus levels were lower with the renal-specific nutrition than with the standard nutrition1
bull Less fluid and potassium in renal-specific nutrition offers advantages over standard nutrition2
1 Cockram DB et al J Ren Nutr 1998825-33
2 Williams RF Summers AM J Ren Nutr 200919183-188
PREHRANSKE ZAHTEVE DIALIZE
PRAKSA
ENERGIJA 35KCALKG TT NA DAN
PROTEINI 12GKG TT NA DAN
VNOS TEKOČINE 1000ML + IZLOČEN URIN
NATRIJ 2-3G NA DAN
KALIJ 2-3G NA DAN
FOSFOR 08-12GDAN
NKFKDOQI 2000 ADA 2002 WILKENS 2004
BIOIMPEDANCE PRINCIPLES
Phase angle
bull Phase angle is an indicator based on reactance and
resistance obtained from bioelectrical impedance
analysis (BIA)
bull PA depends on cell membrane integrity and on body cell
mass
bull Although its biological meaning is still not clear phase
angle appears to have an important prognostic role
bull Phase angle differs across categories of sex age BMI
and percentage fat bull Maria Cristina G Barbosa-Silva Aluiacutesio JD Barros Jack Wang Steven B Heymsfield and Richard
N Pierson Jr Am J Clin Nutr July 2005 vol 82 no 1 49-52
bull Satish Kumar1 Aswini Dutt1 Sandhya Hemraj2 Shankar Bhat1 and Bhat Manipadybhima Iran
J Basic Med Sci 2012 Nov-Dec 15(6) 1180ndash1184
PHASE ANGLE AND LEAN TISSUE
INDEX ARE SLIGHTLY HIGHER IN
HEMODIALYSIS THAN IN PERITONEAL
DIALYSIS GROUP OF PATIENTS
BKnap ZVeceric Haler JButurovic-Ponikvar
RPonikvar AF Bren
University Clinical Center Ljubljana
Department of Nephrology Slovenia
Ideal nutrition ndash CKD patients
bull Prevents musle loss
bull Prevent andor treat PEW
bull Correct metabolic derrangements
bull Decrease morbidity and mortlity
bull Improve QoL
bull Does not promote progression of CKD
bull Or ideally slow down progression of CKD
ZAKLJUČEK
bull Podhranjenost je pomembna in pogosto
ključna za preživetje
bull Sodobne metode detekcije in zdravljenja
podhranjenosti omogočajo zgodnejšo
nutricijsko intervencijo
bull Prehranski dodatki tako enteralni kot
parenteralni so pogosto nujna in včasih
edina možnost
Kaj je dobro vedetihelliphellip
bull LEDVIČNI BOLNIKI JEDO SLABO
bull V ZAČETNI FAZI KLB TERAPIJA Z OMEJEVANJEM VNOSA PROTEINOV LAHKO PRIPELJE DO MALNUTRICIJE IN KAHEKSIJE
bull POMEMBNA OCENA HRANJENOSTI IN PRAVOČASNA NUTRICIJSKA INTERVENCIJA V VSEH FAZAH KLB
bull USPEH ZDRAVLJENJA MALNUTRICIJE JE POVEZAN Z DOBRIM ZDRAVLJENJEM OSNOVNE LEDVIČNE BOLEZNI IN CELOSTNEGA ZDRAVLJENJA KLB
bull POLEG HRANE VELIKO PRISPEVAJO K KVALITETI ŽIVLJENJA TUDI PREHRANSKI DODATKI IN TELESNA VADBA
bull ANABOLNI AGENSI IN STIMULATORJI APETITA NA NIVOJU HIPOTALAMUSA SO OBET BLIŽNJE PRIHODNOSTI

DEBELEJŠI DIALIZNI BOLNIKI
ŽIVIJO DLJE
DIALIZNI BOLNIKI Z ALBUMINI MANJ KOT 30GL
UMIRAJO PREJ
DIA
OMEJEN VNOS ZDRAVE HRANE
PRI KLB
Better nutritional status is associated with improved long
term survival in dialysis patients
Source Chan et al (2012) J Ren Nutr 2012 Nov22(6)547-57
LEDVIČNI BOLNIKI IMAJO SLAB APETIT
bull Izguba apetita in želje za hrano
bull Izguba vonja in okusa
bull Prezgodnja sitost
bull Motnje v delovanju hipotalamusa
bull Vpliv zvišane koncentracije citokinov
bull Omenjeno olajša nastanek kaheksije s
nezadostnim vnosom energije in
proteinov
DIETA LEDVIČNEGA BOLNIKA
Phosphorus balance
ŠTEVILNI VZROKI PODHRANJENOSTI PRI
LEDVIČNI BOLEZNI
bull Zmanjšan vnos hrane
bull Omejevalne diete proteini
bull Uremični toksini
bull Metabolna acidoza
bull Endokrini dejavniki
bull Gastrointestinalni dejavniki
bull MIA sindrom
UREMIČNI SINDROM
Vodi k podhranjenosti tudi zaradi
bull Insulinske rezistence
bull Motenega klirensa lipidov
bull Metabolične acidoze
bull Sekundarnega hiperparatireoidizma
uremične kostne bolezni
DEBELOST OGROŽA TUDI
LEDVIČNE BOLNIKE
bull METABOLIČNI SINDROM
bull SLADKORNA BOLEZEN II
bull MAŠČOBNE CELICE KOT ENDOKRINI ORGAN TUDI PRI KLB VPLIVAJO NA KVS
bull PROBLEM MOTENJ HRANJENJA IN MALNUTRICIJA Z OHRANJENO TELESNO MASO OB ZMANJŠANJU PUSTE TELESNE MASE
bull pomen določanja puste telesne mase z bioimpedanco
bull lean tissue index fat mass index
VLOGA LEPTINA PRI KAHEKSIJI KLB
bull Zvišan pri KLB
bull Deluje podobno kot citokinski receptorji
tipa IL6(vnetje)
bull Preko receptorjev za melanocortin v
hipotalamusu deluje na apetit in
metabolizem
bull Antagonisti MC-R4 receptorja nov
terapevtski obet
VELIK POMEN PREHRANSKE
DIAGNOSTIKE ZA DIALIZNE PACIENTE
bull Klinična presoja pacienta in kvalitete
življenja oziroma uspeha zdravljenja
bull Biokemijavrednosti albuminov
prealbumina in vnosa proteinov (35gl
300mgl 1gkgdan)
bull Nadzor telesna teža BMI SGA
BCM(bioimpedanca) serumski albumin
kreatinin
SUBJEKTIVNA GLOBALNA
NUTRICIJSKA OCENA-SGA
SGA ocena prehranjenosti zajema
bull anamnezo (o spremembi telesne teže o
vnosu hrane simptomih s strani GIT
funkcionalne zmogljivosti) in
bull telesni pregled (atrofija mišic zmanjšanje
podkožne maščobe in pojav oteklin)
bull zlati standard ocene bolnika(Keith
Nutrition in Clinical Practice 2008)
Malnutrition Inflammation Score
(MIS)
bullFully quantitative
bullUses the 7 original SGA components
bullAdds 3 new components
ndashBody mass index
ndashSerum albumin
ndashSerum total iron binding capacity
PEM - PROTEINSKO
ENERGETSKA MALNUTRICIJA
bull PEM je pogost v KLB
bull Je povezan s povečano obolevnostjo in
umrljivostjo
bull 40 PEM na začetku nadomestnega
zdravljenja KOL
bull 10-70 HD pacientov
bull 18-51 CAPD pacientov
Nutritional RecommendationsDialysisStage 5 CKD
KDOQI1 ESPEN2 EBPG3
EnergyCalories lt 60 years 35
kcalkgd
60 years or obese
30-35 kcalkgd
35 kcalkgd 30-40 kcalkgd
Protein 12 gkgd
50 HBV
12-14 gkg
IBWd
11 gkgd
Sodium ― 18-25 gd 2000-3000
mgd
Fluid ― 1000 mL + urine
volume
―
Potassium ― 2000-2500 mgd 1950-2730
mgd
Phosphorus 800-1000 mgd
lt 17 mgkg IBW or
SBWd
800-1000 mgd 800-1000 mgd
Calcium 2 gd ― 2000 mgd
1 NKF KDOQI Clinical practice guidelines for nutrition in chronic renal failure AJKD 2000 35S1-S140
2 Cano N et al Clin Nutr 2006 25295-310
3 Fouque D et al NDT 2007 22(suppl 2)ii45-ii87
Ocena prehranskih potreb
bull V akutni fazi 20-25 nebeljakovinskih kkalkgdan v anabolni fazi in podhranjeni 25 -30 kkalkgdan
bull Maščobe 03 gkg ttdan do 2 gkg ttdan (30 do 70)
bull Ogljikovi hidrati 2-5g kgdan (30 do 70)
bull Beljakovine povprečno 15 g kg tt dan (15 -20 )
bull Mikrohranila-dnevne priporočene potrebe individualno glede na obolenje
bull Opečenci več Cu Se in Zn
AA V PARENTERALNI PREHRANI
bull Povečana izguba AA
bull Neravnovesje med izgubo in porabo
bull Esencielne AA z dodatkom histidina ter arginina niso optimum
bull Nadomeščanje tirozina problem zaradi slabe topnostihellip
bull Acetil-tirozin je rešitev vendar ne pri KLB
bull Rešitev predstavlja dipeptid glicil-tirozin ki je dobro topen in idealno nadomešča večje potrebe po tirozinu pri KLB (AminoMel nephro)
PREHRANSKI DODATKI
Enteralni
bull Nepro Nepro HP Nepro LP Ensure Ensure Plus Advance Prosure Fresubinhellipenkrat na dan per os
bull Glutamin 5-10g na dan per os
bull Carenal 1 tableto po dializi
bull L-karnitin
Parenteralni
bull Aminomel Nephro aminokisline (500ml med HD)
bull Kabiven
bull Glamin 500ml
bull Dipeptiven 100ml
bull Soluvit N(vodotopni vitamini)
bull Vitalipid N(maščobotopni vitamini)
bull Addamel N(mikroelementi)
bull Omegaven (ribje oljehellip)
Component Renal Specific
ONS
Standard ONS
Protein Optimum Medium
Glycemic Index
(Carbohydrates) Low High
MUFA Omega-3
(FatsLipids) High Low
Electrolytes
Phosphorus
Potassium Sodium
Low High
Fluid volume Low High
Caloric density High Standard
Fiber High Low
Prebiotics scFOS Present None
CKD-specific vitamin
amp mineral profile Optimized None
Why Renal Specific ONS
Why Standard versus Renal Specific ONS
Nutrition Intervention in CKD Patients
bull Expert recommendations
KDOQI1 ESPEN2 EBPG3
Nutrition
Support
Individuals undergoing
maintenance dialysis
who are unable to
meet their protein and
energy requirements
with food intake for an
extended period of
time should receive
nutritional support
Special formula
products for HD
treatment can be
useful especially in
malnourished patients
who are not able to
increase their nutrient
intake
Oral nutritional
supplements should
be prescribed if
nutritional counseling
does not achieve an
increase in nutrient
intake to a level that
covers minimum
recommendations
Products
specifically
designed for
dialysis patients
should be
prescribed
1 NKF KDOQI Clinical practice guidelines for nutrition in chronic renal failure AJKD 2000 35S1-S140
2 Cano N et al Clin Nutr 2006 25295-310
3 Fouque D et al NDT 2007 22(suppl 2)ii45-ii87
Recomm-S
ESPEN KDOQI EBPG
Proteini (gkgdan) 12-14 10-12 11
Energija
(kCalkgdan)
35 lt60 g 35
gt60 g 30
30-35
gt50 intke lt1 gkgdan
Actual ntake 20-25 kCalkg 08-1 g proteinakg
Renal Specific Nutritional Therapy
Clinical studies have shown that renal-specific nutrition offers advantages over standard nutrition
bull Phosphorus levels were lower with the renal-specific nutrition than with the standard nutrition1
bull Less fluid and potassium in renal-specific nutrition offers advantages over standard nutrition2
1 Cockram DB et al J Ren Nutr 1998825-33
2 Williams RF Summers AM J Ren Nutr 200919183-188
PREHRANSKE ZAHTEVE DIALIZE
PRAKSA
ENERGIJA 35KCALKG TT NA DAN
PROTEINI 12GKG TT NA DAN
VNOS TEKOČINE 1000ML + IZLOČEN URIN
NATRIJ 2-3G NA DAN
KALIJ 2-3G NA DAN
FOSFOR 08-12GDAN
NKFKDOQI 2000 ADA 2002 WILKENS 2004
BIOIMPEDANCE PRINCIPLES
Phase angle
bull Phase angle is an indicator based on reactance and
resistance obtained from bioelectrical impedance
analysis (BIA)
bull PA depends on cell membrane integrity and on body cell
mass
bull Although its biological meaning is still not clear phase
angle appears to have an important prognostic role
bull Phase angle differs across categories of sex age BMI
and percentage fat bull Maria Cristina G Barbosa-Silva Aluiacutesio JD Barros Jack Wang Steven B Heymsfield and Richard
N Pierson Jr Am J Clin Nutr July 2005 vol 82 no 1 49-52
bull Satish Kumar1 Aswini Dutt1 Sandhya Hemraj2 Shankar Bhat1 and Bhat Manipadybhima Iran
J Basic Med Sci 2012 Nov-Dec 15(6) 1180ndash1184
PHASE ANGLE AND LEAN TISSUE
INDEX ARE SLIGHTLY HIGHER IN
HEMODIALYSIS THAN IN PERITONEAL
DIALYSIS GROUP OF PATIENTS
BKnap ZVeceric Haler JButurovic-Ponikvar
RPonikvar AF Bren
University Clinical Center Ljubljana
Department of Nephrology Slovenia
Ideal nutrition ndash CKD patients
bull Prevents musle loss
bull Prevent andor treat PEW
bull Correct metabolic derrangements
bull Decrease morbidity and mortlity
bull Improve QoL
bull Does not promote progression of CKD
bull Or ideally slow down progression of CKD
ZAKLJUČEK
bull Podhranjenost je pomembna in pogosto
ključna za preživetje
bull Sodobne metode detekcije in zdravljenja
podhranjenosti omogočajo zgodnejšo
nutricijsko intervencijo
bull Prehranski dodatki tako enteralni kot
parenteralni so pogosto nujna in včasih
edina možnost
Kaj je dobro vedetihelliphellip
bull LEDVIČNI BOLNIKI JEDO SLABO
bull V ZAČETNI FAZI KLB TERAPIJA Z OMEJEVANJEM VNOSA PROTEINOV LAHKO PRIPELJE DO MALNUTRICIJE IN KAHEKSIJE
bull POMEMBNA OCENA HRANJENOSTI IN PRAVOČASNA NUTRICIJSKA INTERVENCIJA V VSEH FAZAH KLB
bull USPEH ZDRAVLJENJA MALNUTRICIJE JE POVEZAN Z DOBRIM ZDRAVLJENJEM OSNOVNE LEDVIČNE BOLEZNI IN CELOSTNEGA ZDRAVLJENJA KLB
bull POLEG HRANE VELIKO PRISPEVAJO K KVALITETI ŽIVLJENJA TUDI PREHRANSKI DODATKI IN TELESNA VADBA
bull ANABOLNI AGENSI IN STIMULATORJI APETITA NA NIVOJU HIPOTALAMUSA SO OBET BLIŽNJE PRIHODNOSTI

DIALIZNI BOLNIKI Z ALBUMINI MANJ KOT 30GL
UMIRAJO PREJ
DIA
OMEJEN VNOS ZDRAVE HRANE
PRI KLB
Better nutritional status is associated with improved long
term survival in dialysis patients
Source Chan et al (2012) J Ren Nutr 2012 Nov22(6)547-57
LEDVIČNI BOLNIKI IMAJO SLAB APETIT
bull Izguba apetita in želje za hrano
bull Izguba vonja in okusa
bull Prezgodnja sitost
bull Motnje v delovanju hipotalamusa
bull Vpliv zvišane koncentracije citokinov
bull Omenjeno olajša nastanek kaheksije s
nezadostnim vnosom energije in
proteinov
DIETA LEDVIČNEGA BOLNIKA
Phosphorus balance
ŠTEVILNI VZROKI PODHRANJENOSTI PRI
LEDVIČNI BOLEZNI
bull Zmanjšan vnos hrane
bull Omejevalne diete proteini
bull Uremični toksini
bull Metabolna acidoza
bull Endokrini dejavniki
bull Gastrointestinalni dejavniki
bull MIA sindrom
UREMIČNI SINDROM
Vodi k podhranjenosti tudi zaradi
bull Insulinske rezistence
bull Motenega klirensa lipidov
bull Metabolične acidoze
bull Sekundarnega hiperparatireoidizma
uremične kostne bolezni
DEBELOST OGROŽA TUDI
LEDVIČNE BOLNIKE
bull METABOLIČNI SINDROM
bull SLADKORNA BOLEZEN II
bull MAŠČOBNE CELICE KOT ENDOKRINI ORGAN TUDI PRI KLB VPLIVAJO NA KVS
bull PROBLEM MOTENJ HRANJENJA IN MALNUTRICIJA Z OHRANJENO TELESNO MASO OB ZMANJŠANJU PUSTE TELESNE MASE
bull pomen določanja puste telesne mase z bioimpedanco
bull lean tissue index fat mass index
VLOGA LEPTINA PRI KAHEKSIJI KLB
bull Zvišan pri KLB
bull Deluje podobno kot citokinski receptorji
tipa IL6(vnetje)
bull Preko receptorjev za melanocortin v
hipotalamusu deluje na apetit in
metabolizem
bull Antagonisti MC-R4 receptorja nov
terapevtski obet
VELIK POMEN PREHRANSKE
DIAGNOSTIKE ZA DIALIZNE PACIENTE
bull Klinična presoja pacienta in kvalitete
življenja oziroma uspeha zdravljenja
bull Biokemijavrednosti albuminov
prealbumina in vnosa proteinov (35gl
300mgl 1gkgdan)
bull Nadzor telesna teža BMI SGA
BCM(bioimpedanca) serumski albumin
kreatinin
SUBJEKTIVNA GLOBALNA
NUTRICIJSKA OCENA-SGA
SGA ocena prehranjenosti zajema
bull anamnezo (o spremembi telesne teže o
vnosu hrane simptomih s strani GIT
funkcionalne zmogljivosti) in
bull telesni pregled (atrofija mišic zmanjšanje
podkožne maščobe in pojav oteklin)
bull zlati standard ocene bolnika(Keith
Nutrition in Clinical Practice 2008)
Malnutrition Inflammation Score
(MIS)
bullFully quantitative
bullUses the 7 original SGA components
bullAdds 3 new components
ndashBody mass index
ndashSerum albumin
ndashSerum total iron binding capacity
PEM - PROTEINSKO
ENERGETSKA MALNUTRICIJA
bull PEM je pogost v KLB
bull Je povezan s povečano obolevnostjo in
umrljivostjo
bull 40 PEM na začetku nadomestnega
zdravljenja KOL
bull 10-70 HD pacientov
bull 18-51 CAPD pacientov
Nutritional RecommendationsDialysisStage 5 CKD
KDOQI1 ESPEN2 EBPG3
EnergyCalories lt 60 years 35
kcalkgd
60 years or obese
30-35 kcalkgd
35 kcalkgd 30-40 kcalkgd
Protein 12 gkgd
50 HBV
12-14 gkg
IBWd
11 gkgd
Sodium ― 18-25 gd 2000-3000
mgd
Fluid ― 1000 mL + urine
volume
―
Potassium ― 2000-2500 mgd 1950-2730
mgd
Phosphorus 800-1000 mgd
lt 17 mgkg IBW or
SBWd
800-1000 mgd 800-1000 mgd
Calcium 2 gd ― 2000 mgd
1 NKF KDOQI Clinical practice guidelines for nutrition in chronic renal failure AJKD 2000 35S1-S140
2 Cano N et al Clin Nutr 2006 25295-310
3 Fouque D et al NDT 2007 22(suppl 2)ii45-ii87
Ocena prehranskih potreb
bull V akutni fazi 20-25 nebeljakovinskih kkalkgdan v anabolni fazi in podhranjeni 25 -30 kkalkgdan
bull Maščobe 03 gkg ttdan do 2 gkg ttdan (30 do 70)
bull Ogljikovi hidrati 2-5g kgdan (30 do 70)
bull Beljakovine povprečno 15 g kg tt dan (15 -20 )
bull Mikrohranila-dnevne priporočene potrebe individualno glede na obolenje
bull Opečenci več Cu Se in Zn
AA V PARENTERALNI PREHRANI
bull Povečana izguba AA
bull Neravnovesje med izgubo in porabo
bull Esencielne AA z dodatkom histidina ter arginina niso optimum
bull Nadomeščanje tirozina problem zaradi slabe topnostihellip
bull Acetil-tirozin je rešitev vendar ne pri KLB
bull Rešitev predstavlja dipeptid glicil-tirozin ki je dobro topen in idealno nadomešča večje potrebe po tirozinu pri KLB (AminoMel nephro)
PREHRANSKI DODATKI
Enteralni
bull Nepro Nepro HP Nepro LP Ensure Ensure Plus Advance Prosure Fresubinhellipenkrat na dan per os
bull Glutamin 5-10g na dan per os
bull Carenal 1 tableto po dializi
bull L-karnitin
Parenteralni
bull Aminomel Nephro aminokisline (500ml med HD)
bull Kabiven
bull Glamin 500ml
bull Dipeptiven 100ml
bull Soluvit N(vodotopni vitamini)
bull Vitalipid N(maščobotopni vitamini)
bull Addamel N(mikroelementi)
bull Omegaven (ribje oljehellip)
Component Renal Specific
ONS
Standard ONS
Protein Optimum Medium
Glycemic Index
(Carbohydrates) Low High
MUFA Omega-3
(FatsLipids) High Low
Electrolytes
Phosphorus
Potassium Sodium
Low High
Fluid volume Low High
Caloric density High Standard
Fiber High Low
Prebiotics scFOS Present None
CKD-specific vitamin
amp mineral profile Optimized None
Why Renal Specific ONS
Why Standard versus Renal Specific ONS
Nutrition Intervention in CKD Patients
bull Expert recommendations
KDOQI1 ESPEN2 EBPG3
Nutrition
Support
Individuals undergoing
maintenance dialysis
who are unable to
meet their protein and
energy requirements
with food intake for an
extended period of
time should receive
nutritional support
Special formula
products for HD
treatment can be
useful especially in
malnourished patients
who are not able to
increase their nutrient
intake
Oral nutritional
supplements should
be prescribed if
nutritional counseling
does not achieve an
increase in nutrient
intake to a level that
covers minimum
recommendations
Products
specifically
designed for
dialysis patients
should be
prescribed
1 NKF KDOQI Clinical practice guidelines for nutrition in chronic renal failure AJKD 2000 35S1-S140
2 Cano N et al Clin Nutr 2006 25295-310
3 Fouque D et al NDT 2007 22(suppl 2)ii45-ii87
Recomm-S
ESPEN KDOQI EBPG
Proteini (gkgdan) 12-14 10-12 11
Energija
(kCalkgdan)
35 lt60 g 35
gt60 g 30
30-35
gt50 intke lt1 gkgdan
Actual ntake 20-25 kCalkg 08-1 g proteinakg
Renal Specific Nutritional Therapy
Clinical studies have shown that renal-specific nutrition offers advantages over standard nutrition
bull Phosphorus levels were lower with the renal-specific nutrition than with the standard nutrition1
bull Less fluid and potassium in renal-specific nutrition offers advantages over standard nutrition2
1 Cockram DB et al J Ren Nutr 1998825-33
2 Williams RF Summers AM J Ren Nutr 200919183-188
PREHRANSKE ZAHTEVE DIALIZE
PRAKSA
ENERGIJA 35KCALKG TT NA DAN
PROTEINI 12GKG TT NA DAN
VNOS TEKOČINE 1000ML + IZLOČEN URIN
NATRIJ 2-3G NA DAN
KALIJ 2-3G NA DAN
FOSFOR 08-12GDAN
NKFKDOQI 2000 ADA 2002 WILKENS 2004
BIOIMPEDANCE PRINCIPLES
Phase angle
bull Phase angle is an indicator based on reactance and
resistance obtained from bioelectrical impedance
analysis (BIA)
bull PA depends on cell membrane integrity and on body cell
mass
bull Although its biological meaning is still not clear phase
angle appears to have an important prognostic role
bull Phase angle differs across categories of sex age BMI
and percentage fat bull Maria Cristina G Barbosa-Silva Aluiacutesio JD Barros Jack Wang Steven B Heymsfield and Richard
N Pierson Jr Am J Clin Nutr July 2005 vol 82 no 1 49-52
bull Satish Kumar1 Aswini Dutt1 Sandhya Hemraj2 Shankar Bhat1 and Bhat Manipadybhima Iran
J Basic Med Sci 2012 Nov-Dec 15(6) 1180ndash1184
PHASE ANGLE AND LEAN TISSUE
INDEX ARE SLIGHTLY HIGHER IN
HEMODIALYSIS THAN IN PERITONEAL
DIALYSIS GROUP OF PATIENTS
BKnap ZVeceric Haler JButurovic-Ponikvar
RPonikvar AF Bren
University Clinical Center Ljubljana
Department of Nephrology Slovenia
Ideal nutrition ndash CKD patients
bull Prevents musle loss
bull Prevent andor treat PEW
bull Correct metabolic derrangements
bull Decrease morbidity and mortlity
bull Improve QoL
bull Does not promote progression of CKD
bull Or ideally slow down progression of CKD
ZAKLJUČEK
bull Podhranjenost je pomembna in pogosto
ključna za preživetje
bull Sodobne metode detekcije in zdravljenja
podhranjenosti omogočajo zgodnejšo
nutricijsko intervencijo
bull Prehranski dodatki tako enteralni kot
parenteralni so pogosto nujna in včasih
edina možnost
Kaj je dobro vedetihelliphellip
bull LEDVIČNI BOLNIKI JEDO SLABO
bull V ZAČETNI FAZI KLB TERAPIJA Z OMEJEVANJEM VNOSA PROTEINOV LAHKO PRIPELJE DO MALNUTRICIJE IN KAHEKSIJE
bull POMEMBNA OCENA HRANJENOSTI IN PRAVOČASNA NUTRICIJSKA INTERVENCIJA V VSEH FAZAH KLB
bull USPEH ZDRAVLJENJA MALNUTRICIJE JE POVEZAN Z DOBRIM ZDRAVLJENJEM OSNOVNE LEDVIČNE BOLEZNI IN CELOSTNEGA ZDRAVLJENJA KLB
bull POLEG HRANE VELIKO PRISPEVAJO K KVALITETI ŽIVLJENJA TUDI PREHRANSKI DODATKI IN TELESNA VADBA
bull ANABOLNI AGENSI IN STIMULATORJI APETITA NA NIVOJU HIPOTALAMUSA SO OBET BLIŽNJE PRIHODNOSTI
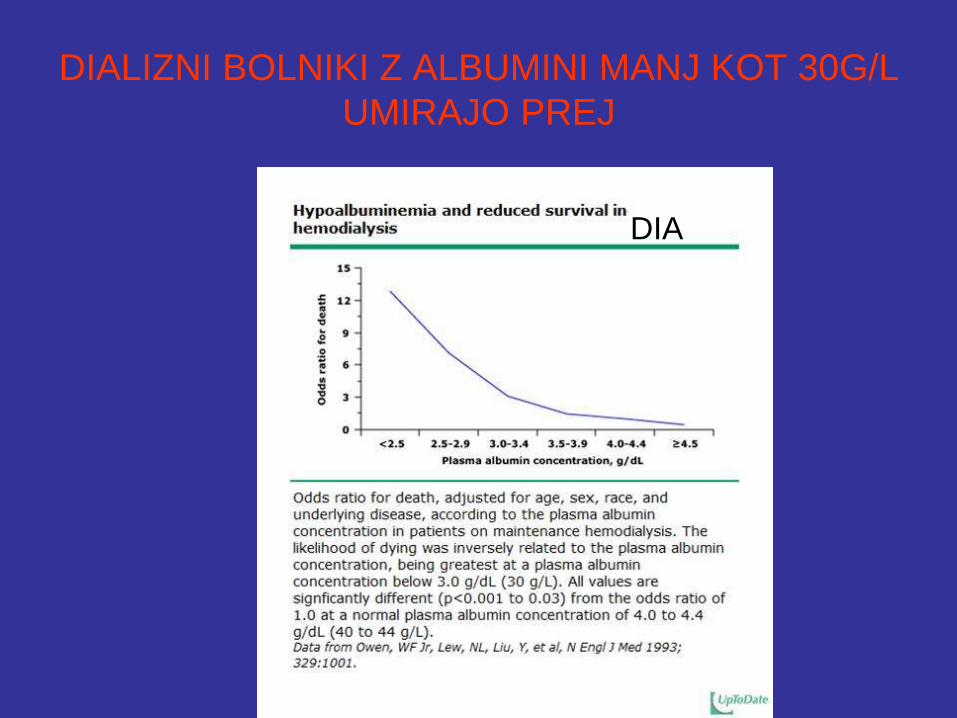
OMEJEN VNOS ZDRAVE HRANE
PRI KLB
Better nutritional status is associated with improved long
term survival in dialysis patients
Source Chan et al (2012) J Ren Nutr 2012 Nov22(6)547-57
LEDVIČNI BOLNIKI IMAJO SLAB APETIT
bull Izguba apetita in želje za hrano
bull Izguba vonja in okusa
bull Prezgodnja sitost
bull Motnje v delovanju hipotalamusa
bull Vpliv zvišane koncentracije citokinov
bull Omenjeno olajša nastanek kaheksije s
nezadostnim vnosom energije in
proteinov
DIETA LEDVIČNEGA BOLNIKA
Phosphorus balance
ŠTEVILNI VZROKI PODHRANJENOSTI PRI
LEDVIČNI BOLEZNI
bull Zmanjšan vnos hrane
bull Omejevalne diete proteini
bull Uremični toksini
bull Metabolna acidoza
bull Endokrini dejavniki
bull Gastrointestinalni dejavniki
bull MIA sindrom
UREMIČNI SINDROM
Vodi k podhranjenosti tudi zaradi
bull Insulinske rezistence
bull Motenega klirensa lipidov
bull Metabolične acidoze
bull Sekundarnega hiperparatireoidizma
uremične kostne bolezni
DEBELOST OGROŽA TUDI
LEDVIČNE BOLNIKE
bull METABOLIČNI SINDROM
bull SLADKORNA BOLEZEN II
bull MAŠČOBNE CELICE KOT ENDOKRINI ORGAN TUDI PRI KLB VPLIVAJO NA KVS
bull PROBLEM MOTENJ HRANJENJA IN MALNUTRICIJA Z OHRANJENO TELESNO MASO OB ZMANJŠANJU PUSTE TELESNE MASE
bull pomen določanja puste telesne mase z bioimpedanco
bull lean tissue index fat mass index
VLOGA LEPTINA PRI KAHEKSIJI KLB
bull Zvišan pri KLB
bull Deluje podobno kot citokinski receptorji
tipa IL6(vnetje)
bull Preko receptorjev za melanocortin v
hipotalamusu deluje na apetit in
metabolizem
bull Antagonisti MC-R4 receptorja nov
terapevtski obet
VELIK POMEN PREHRANSKE
DIAGNOSTIKE ZA DIALIZNE PACIENTE
bull Klinična presoja pacienta in kvalitete
življenja oziroma uspeha zdravljenja
bull Biokemijavrednosti albuminov
prealbumina in vnosa proteinov (35gl
300mgl 1gkgdan)
bull Nadzor telesna teža BMI SGA
BCM(bioimpedanca) serumski albumin
kreatinin
SUBJEKTIVNA GLOBALNA
NUTRICIJSKA OCENA-SGA
SGA ocena prehranjenosti zajema
bull anamnezo (o spremembi telesne teže o
vnosu hrane simptomih s strani GIT
funkcionalne zmogljivosti) in
bull telesni pregled (atrofija mišic zmanjšanje
podkožne maščobe in pojav oteklin)
bull zlati standard ocene bolnika(Keith
Nutrition in Clinical Practice 2008)
Malnutrition Inflammation Score
(MIS)
bullFully quantitative
bullUses the 7 original SGA components
bullAdds 3 new components
ndashBody mass index
ndashSerum albumin
ndashSerum total iron binding capacity
PEM - PROTEINSKO
ENERGETSKA MALNUTRICIJA
bull PEM je pogost v KLB
bull Je povezan s povečano obolevnostjo in
umrljivostjo
bull 40 PEM na začetku nadomestnega
zdravljenja KOL
bull 10-70 HD pacientov
bull 18-51 CAPD pacientov
Nutritional RecommendationsDialysisStage 5 CKD
KDOQI1 ESPEN2 EBPG3
EnergyCalories lt 60 years 35
kcalkgd
60 years or obese
30-35 kcalkgd
35 kcalkgd 30-40 kcalkgd
Protein 12 gkgd
50 HBV
12-14 gkg
IBWd
11 gkgd
Sodium ― 18-25 gd 2000-3000
mgd
Fluid ― 1000 mL + urine
volume
―
Potassium ― 2000-2500 mgd 1950-2730
mgd
Phosphorus 800-1000 mgd
lt 17 mgkg IBW or
SBWd
800-1000 mgd 800-1000 mgd
Calcium 2 gd ― 2000 mgd
1 NKF KDOQI Clinical practice guidelines for nutrition in chronic renal failure AJKD 2000 35S1-S140
2 Cano N et al Clin Nutr 2006 25295-310
3 Fouque D et al NDT 2007 22(suppl 2)ii45-ii87
Ocena prehranskih potreb
bull V akutni fazi 20-25 nebeljakovinskih kkalkgdan v anabolni fazi in podhranjeni 25 -30 kkalkgdan
bull Maščobe 03 gkg ttdan do 2 gkg ttdan (30 do 70)
bull Ogljikovi hidrati 2-5g kgdan (30 do 70)
bull Beljakovine povprečno 15 g kg tt dan (15 -20 )
bull Mikrohranila-dnevne priporočene potrebe individualno glede na obolenje
bull Opečenci več Cu Se in Zn
AA V PARENTERALNI PREHRANI
bull Povečana izguba AA
bull Neravnovesje med izgubo in porabo
bull Esencielne AA z dodatkom histidina ter arginina niso optimum
bull Nadomeščanje tirozina problem zaradi slabe topnostihellip
bull Acetil-tirozin je rešitev vendar ne pri KLB
bull Rešitev predstavlja dipeptid glicil-tirozin ki je dobro topen in idealno nadomešča večje potrebe po tirozinu pri KLB (AminoMel nephro)
PREHRANSKI DODATKI
Enteralni
bull Nepro Nepro HP Nepro LP Ensure Ensure Plus Advance Prosure Fresubinhellipenkrat na dan per os
bull Glutamin 5-10g na dan per os
bull Carenal 1 tableto po dializi
bull L-karnitin
Parenteralni
bull Aminomel Nephro aminokisline (500ml med HD)
bull Kabiven
bull Glamin 500ml
bull Dipeptiven 100ml
bull Soluvit N(vodotopni vitamini)
bull Vitalipid N(maščobotopni vitamini)
bull Addamel N(mikroelementi)
bull Omegaven (ribje oljehellip)
Component Renal Specific
ONS
Standard ONS
Protein Optimum Medium
Glycemic Index
(Carbohydrates) Low High
MUFA Omega-3
(FatsLipids) High Low
Electrolytes
Phosphorus
Potassium Sodium
Low High
Fluid volume Low High
Caloric density High Standard
Fiber High Low
Prebiotics scFOS Present None
CKD-specific vitamin
amp mineral profile Optimized None
Why Renal Specific ONS
Why Standard versus Renal Specific ONS
Nutrition Intervention in CKD Patients
bull Expert recommendations
KDOQI1 ESPEN2 EBPG3
Nutrition
Support
Individuals undergoing
maintenance dialysis
who are unable to
meet their protein and
energy requirements
with food intake for an
extended period of
time should receive
nutritional support
Special formula
products for HD
treatment can be
useful especially in
malnourished patients
who are not able to
increase their nutrient
intake
Oral nutritional
supplements should
be prescribed if
nutritional counseling
does not achieve an
increase in nutrient
intake to a level that
covers minimum
recommendations
Products
specifically
designed for
dialysis patients
should be
prescribed
1 NKF KDOQI Clinical practice guidelines for nutrition in chronic renal failure AJKD 2000 35S1-S140
2 Cano N et al Clin Nutr 2006 25295-310
3 Fouque D et al NDT 2007 22(suppl 2)ii45-ii87
Recomm-S
ESPEN KDOQI EBPG
Proteini (gkgdan) 12-14 10-12 11
Energija
(kCalkgdan)
35 lt60 g 35
gt60 g 30
30-35
gt50 intke lt1 gkgdan
Actual ntake 20-25 kCalkg 08-1 g proteinakg
Renal Specific Nutritional Therapy
Clinical studies have shown that renal-specific nutrition offers advantages over standard nutrition
bull Phosphorus levels were lower with the renal-specific nutrition than with the standard nutrition1
bull Less fluid and potassium in renal-specific nutrition offers advantages over standard nutrition2
1 Cockram DB et al J Ren Nutr 1998825-33
2 Williams RF Summers AM J Ren Nutr 200919183-188
PREHRANSKE ZAHTEVE DIALIZE
PRAKSA
ENERGIJA 35KCALKG TT NA DAN
PROTEINI 12GKG TT NA DAN
VNOS TEKOČINE 1000ML + IZLOČEN URIN
NATRIJ 2-3G NA DAN
KALIJ 2-3G NA DAN
FOSFOR 08-12GDAN
NKFKDOQI 2000 ADA 2002 WILKENS 2004
BIOIMPEDANCE PRINCIPLES
Phase angle
bull Phase angle is an indicator based on reactance and
resistance obtained from bioelectrical impedance
analysis (BIA)
bull PA depends on cell membrane integrity and on body cell
mass
bull Although its biological meaning is still not clear phase
angle appears to have an important prognostic role
bull Phase angle differs across categories of sex age BMI
and percentage fat bull Maria Cristina G Barbosa-Silva Aluiacutesio JD Barros Jack Wang Steven B Heymsfield and Richard
N Pierson Jr Am J Clin Nutr July 2005 vol 82 no 1 49-52
bull Satish Kumar1 Aswini Dutt1 Sandhya Hemraj2 Shankar Bhat1 and Bhat Manipadybhima Iran
J Basic Med Sci 2012 Nov-Dec 15(6) 1180ndash1184
PHASE ANGLE AND LEAN TISSUE
INDEX ARE SLIGHTLY HIGHER IN
HEMODIALYSIS THAN IN PERITONEAL
DIALYSIS GROUP OF PATIENTS
BKnap ZVeceric Haler JButurovic-Ponikvar
RPonikvar AF Bren
University Clinical Center Ljubljana
Department of Nephrology Slovenia
Ideal nutrition ndash CKD patients
bull Prevents musle loss
bull Prevent andor treat PEW
bull Correct metabolic derrangements
bull Decrease morbidity and mortlity
bull Improve QoL
bull Does not promote progression of CKD
bull Or ideally slow down progression of CKD
ZAKLJUČEK
bull Podhranjenost je pomembna in pogosto
ključna za preživetje
bull Sodobne metode detekcije in zdravljenja
podhranjenosti omogočajo zgodnejšo
nutricijsko intervencijo
bull Prehranski dodatki tako enteralni kot
parenteralni so pogosto nujna in včasih
edina možnost
Kaj je dobro vedetihelliphellip
bull LEDVIČNI BOLNIKI JEDO SLABO
bull V ZAČETNI FAZI KLB TERAPIJA Z OMEJEVANJEM VNOSA PROTEINOV LAHKO PRIPELJE DO MALNUTRICIJE IN KAHEKSIJE
bull POMEMBNA OCENA HRANJENOSTI IN PRAVOČASNA NUTRICIJSKA INTERVENCIJA V VSEH FAZAH KLB
bull USPEH ZDRAVLJENJA MALNUTRICIJE JE POVEZAN Z DOBRIM ZDRAVLJENJEM OSNOVNE LEDVIČNE BOLEZNI IN CELOSTNEGA ZDRAVLJENJA KLB
bull POLEG HRANE VELIKO PRISPEVAJO K KVALITETI ŽIVLJENJA TUDI PREHRANSKI DODATKI IN TELESNA VADBA
bull ANABOLNI AGENSI IN STIMULATORJI APETITA NA NIVOJU HIPOTALAMUSA SO OBET BLIŽNJE PRIHODNOSTI

Better nutritional status is associated with improved long
term survival in dialysis patients
Source Chan et al (2012) J Ren Nutr 2012 Nov22(6)547-57
LEDVIČNI BOLNIKI IMAJO SLAB APETIT
bull Izguba apetita in želje za hrano
bull Izguba vonja in okusa
bull Prezgodnja sitost
bull Motnje v delovanju hipotalamusa
bull Vpliv zvišane koncentracije citokinov
bull Omenjeno olajša nastanek kaheksije s
nezadostnim vnosom energije in
proteinov
DIETA LEDVIČNEGA BOLNIKA
Phosphorus balance
ŠTEVILNI VZROKI PODHRANJENOSTI PRI
LEDVIČNI BOLEZNI
bull Zmanjšan vnos hrane
bull Omejevalne diete proteini
bull Uremični toksini
bull Metabolna acidoza
bull Endokrini dejavniki
bull Gastrointestinalni dejavniki
bull MIA sindrom
UREMIČNI SINDROM
Vodi k podhranjenosti tudi zaradi
bull Insulinske rezistence
bull Motenega klirensa lipidov
bull Metabolične acidoze
bull Sekundarnega hiperparatireoidizma
uremične kostne bolezni
DEBELOST OGROŽA TUDI
LEDVIČNE BOLNIKE
bull METABOLIČNI SINDROM
bull SLADKORNA BOLEZEN II
bull MAŠČOBNE CELICE KOT ENDOKRINI ORGAN TUDI PRI KLB VPLIVAJO NA KVS
bull PROBLEM MOTENJ HRANJENJA IN MALNUTRICIJA Z OHRANJENO TELESNO MASO OB ZMANJŠANJU PUSTE TELESNE MASE
bull pomen določanja puste telesne mase z bioimpedanco
bull lean tissue index fat mass index
VLOGA LEPTINA PRI KAHEKSIJI KLB
bull Zvišan pri KLB
bull Deluje podobno kot citokinski receptorji
tipa IL6(vnetje)
bull Preko receptorjev za melanocortin v
hipotalamusu deluje na apetit in
metabolizem
bull Antagonisti MC-R4 receptorja nov
terapevtski obet
VELIK POMEN PREHRANSKE
DIAGNOSTIKE ZA DIALIZNE PACIENTE
bull Klinična presoja pacienta in kvalitete
življenja oziroma uspeha zdravljenja
bull Biokemijavrednosti albuminov
prealbumina in vnosa proteinov (35gl
300mgl 1gkgdan)
bull Nadzor telesna teža BMI SGA
BCM(bioimpedanca) serumski albumin
kreatinin
SUBJEKTIVNA GLOBALNA
NUTRICIJSKA OCENA-SGA
SGA ocena prehranjenosti zajema
bull anamnezo (o spremembi telesne teže o
vnosu hrane simptomih s strani GIT
funkcionalne zmogljivosti) in
bull telesni pregled (atrofija mišic zmanjšanje
podkožne maščobe in pojav oteklin)
bull zlati standard ocene bolnika(Keith
Nutrition in Clinical Practice 2008)
Malnutrition Inflammation Score
(MIS)
bullFully quantitative
bullUses the 7 original SGA components
bullAdds 3 new components
ndashBody mass index
ndashSerum albumin
ndashSerum total iron binding capacity
PEM - PROTEINSKO
ENERGETSKA MALNUTRICIJA
bull PEM je pogost v KLB
bull Je povezan s povečano obolevnostjo in
umrljivostjo
bull 40 PEM na začetku nadomestnega
zdravljenja KOL
bull 10-70 HD pacientov
bull 18-51 CAPD pacientov
Nutritional RecommendationsDialysisStage 5 CKD
KDOQI1 ESPEN2 EBPG3
EnergyCalories lt 60 years 35
kcalkgd
60 years or obese
30-35 kcalkgd
35 kcalkgd 30-40 kcalkgd
Protein 12 gkgd
50 HBV
12-14 gkg
IBWd
11 gkgd
Sodium ― 18-25 gd 2000-3000
mgd
Fluid ― 1000 mL + urine
volume
―
Potassium ― 2000-2500 mgd 1950-2730
mgd
Phosphorus 800-1000 mgd
lt 17 mgkg IBW or
SBWd
800-1000 mgd 800-1000 mgd
Calcium 2 gd ― 2000 mgd
1 NKF KDOQI Clinical practice guidelines for nutrition in chronic renal failure AJKD 2000 35S1-S140
2 Cano N et al Clin Nutr 2006 25295-310
3 Fouque D et al NDT 2007 22(suppl 2)ii45-ii87
Ocena prehranskih potreb
bull V akutni fazi 20-25 nebeljakovinskih kkalkgdan v anabolni fazi in podhranjeni 25 -30 kkalkgdan
bull Maščobe 03 gkg ttdan do 2 gkg ttdan (30 do 70)
bull Ogljikovi hidrati 2-5g kgdan (30 do 70)
bull Beljakovine povprečno 15 g kg tt dan (15 -20 )
bull Mikrohranila-dnevne priporočene potrebe individualno glede na obolenje
bull Opečenci več Cu Se in Zn
AA V PARENTERALNI PREHRANI
bull Povečana izguba AA
bull Neravnovesje med izgubo in porabo
bull Esencielne AA z dodatkom histidina ter arginina niso optimum
bull Nadomeščanje tirozina problem zaradi slabe topnostihellip
bull Acetil-tirozin je rešitev vendar ne pri KLB
bull Rešitev predstavlja dipeptid glicil-tirozin ki je dobro topen in idealno nadomešča večje potrebe po tirozinu pri KLB (AminoMel nephro)
PREHRANSKI DODATKI
Enteralni
bull Nepro Nepro HP Nepro LP Ensure Ensure Plus Advance Prosure Fresubinhellipenkrat na dan per os
bull Glutamin 5-10g na dan per os
bull Carenal 1 tableto po dializi
bull L-karnitin
Parenteralni
bull Aminomel Nephro aminokisline (500ml med HD)
bull Kabiven
bull Glamin 500ml
bull Dipeptiven 100ml
bull Soluvit N(vodotopni vitamini)
bull Vitalipid N(maščobotopni vitamini)
bull Addamel N(mikroelementi)
bull Omegaven (ribje oljehellip)
Component Renal Specific
ONS
Standard ONS
Protein Optimum Medium
Glycemic Index
(Carbohydrates) Low High
MUFA Omega-3
(FatsLipids) High Low
Electrolytes
Phosphorus
Potassium Sodium
Low High
Fluid volume Low High
Caloric density High Standard
Fiber High Low
Prebiotics scFOS Present None
CKD-specific vitamin
amp mineral profile Optimized None
Why Renal Specific ONS
Why Standard versus Renal Specific ONS
Nutrition Intervention in CKD Patients
bull Expert recommendations
KDOQI1 ESPEN2 EBPG3
Nutrition
Support
Individuals undergoing
maintenance dialysis
who are unable to
meet their protein and
energy requirements
with food intake for an
extended period of
time should receive
nutritional support
Special formula
products for HD
treatment can be
useful especially in
malnourished patients
who are not able to
increase their nutrient
intake
Oral nutritional
supplements should
be prescribed if
nutritional counseling
does not achieve an
increase in nutrient
intake to a level that
covers minimum
recommendations
Products
specifically
designed for
dialysis patients
should be
prescribed
1 NKF KDOQI Clinical practice guidelines for nutrition in chronic renal failure AJKD 2000 35S1-S140
2 Cano N et al Clin Nutr 2006 25295-310
3 Fouque D et al NDT 2007 22(suppl 2)ii45-ii87
Recomm-S
ESPEN KDOQI EBPG
Proteini (gkgdan) 12-14 10-12 11
Energija
(kCalkgdan)
35 lt60 g 35
gt60 g 30
30-35
gt50 intke lt1 gkgdan
Actual ntake 20-25 kCalkg 08-1 g proteinakg
Renal Specific Nutritional Therapy
Clinical studies have shown that renal-specific nutrition offers advantages over standard nutrition
bull Phosphorus levels were lower with the renal-specific nutrition than with the standard nutrition1
bull Less fluid and potassium in renal-specific nutrition offers advantages over standard nutrition2
1 Cockram DB et al J Ren Nutr 1998825-33
2 Williams RF Summers AM J Ren Nutr 200919183-188
PREHRANSKE ZAHTEVE DIALIZE
PRAKSA
ENERGIJA 35KCALKG TT NA DAN
PROTEINI 12GKG TT NA DAN
VNOS TEKOČINE 1000ML + IZLOČEN URIN
NATRIJ 2-3G NA DAN
KALIJ 2-3G NA DAN
FOSFOR 08-12GDAN
NKFKDOQI 2000 ADA 2002 WILKENS 2004
BIOIMPEDANCE PRINCIPLES
Phase angle
bull Phase angle is an indicator based on reactance and
resistance obtained from bioelectrical impedance
analysis (BIA)
bull PA depends on cell membrane integrity and on body cell
mass
bull Although its biological meaning is still not clear phase
angle appears to have an important prognostic role
bull Phase angle differs across categories of sex age BMI
and percentage fat bull Maria Cristina G Barbosa-Silva Aluiacutesio JD Barros Jack Wang Steven B Heymsfield and Richard
N Pierson Jr Am J Clin Nutr July 2005 vol 82 no 1 49-52
bull Satish Kumar1 Aswini Dutt1 Sandhya Hemraj2 Shankar Bhat1 and Bhat Manipadybhima Iran
J Basic Med Sci 2012 Nov-Dec 15(6) 1180ndash1184
PHASE ANGLE AND LEAN TISSUE
INDEX ARE SLIGHTLY HIGHER IN
HEMODIALYSIS THAN IN PERITONEAL
DIALYSIS GROUP OF PATIENTS
BKnap ZVeceric Haler JButurovic-Ponikvar
RPonikvar AF Bren
University Clinical Center Ljubljana
Department of Nephrology Slovenia
Ideal nutrition ndash CKD patients
bull Prevents musle loss
bull Prevent andor treat PEW
bull Correct metabolic derrangements
bull Decrease morbidity and mortlity
bull Improve QoL
bull Does not promote progression of CKD
bull Or ideally slow down progression of CKD
ZAKLJUČEK
bull Podhranjenost je pomembna in pogosto
ključna za preživetje
bull Sodobne metode detekcije in zdravljenja
podhranjenosti omogočajo zgodnejšo
nutricijsko intervencijo
bull Prehranski dodatki tako enteralni kot
parenteralni so pogosto nujna in včasih
edina možnost
Kaj je dobro vedetihelliphellip
bull LEDVIČNI BOLNIKI JEDO SLABO
bull V ZAČETNI FAZI KLB TERAPIJA Z OMEJEVANJEM VNOSA PROTEINOV LAHKO PRIPELJE DO MALNUTRICIJE IN KAHEKSIJE
bull POMEMBNA OCENA HRANJENOSTI IN PRAVOČASNA NUTRICIJSKA INTERVENCIJA V VSEH FAZAH KLB
bull USPEH ZDRAVLJENJA MALNUTRICIJE JE POVEZAN Z DOBRIM ZDRAVLJENJEM OSNOVNE LEDVIČNE BOLEZNI IN CELOSTNEGA ZDRAVLJENJA KLB
bull POLEG HRANE VELIKO PRISPEVAJO K KVALITETI ŽIVLJENJA TUDI PREHRANSKI DODATKI IN TELESNA VADBA
bull ANABOLNI AGENSI IN STIMULATORJI APETITA NA NIVOJU HIPOTALAMUSA SO OBET BLIŽNJE PRIHODNOSTI

LEDVIČNI BOLNIKI IMAJO SLAB APETIT
bull Izguba apetita in želje za hrano
bull Izguba vonja in okusa
bull Prezgodnja sitost
bull Motnje v delovanju hipotalamusa
bull Vpliv zvišane koncentracije citokinov
bull Omenjeno olajša nastanek kaheksije s
nezadostnim vnosom energije in
proteinov
DIETA LEDVIČNEGA BOLNIKA
Phosphorus balance
ŠTEVILNI VZROKI PODHRANJENOSTI PRI
LEDVIČNI BOLEZNI
bull Zmanjšan vnos hrane
bull Omejevalne diete proteini
bull Uremični toksini
bull Metabolna acidoza
bull Endokrini dejavniki
bull Gastrointestinalni dejavniki
bull MIA sindrom
UREMIČNI SINDROM
Vodi k podhranjenosti tudi zaradi
bull Insulinske rezistence
bull Motenega klirensa lipidov
bull Metabolične acidoze
bull Sekundarnega hiperparatireoidizma
uremične kostne bolezni
DEBELOST OGROŽA TUDI
LEDVIČNE BOLNIKE
bull METABOLIČNI SINDROM
bull SLADKORNA BOLEZEN II
bull MAŠČOBNE CELICE KOT ENDOKRINI ORGAN TUDI PRI KLB VPLIVAJO NA KVS
bull PROBLEM MOTENJ HRANJENJA IN MALNUTRICIJA Z OHRANJENO TELESNO MASO OB ZMANJŠANJU PUSTE TELESNE MASE
bull pomen določanja puste telesne mase z bioimpedanco
bull lean tissue index fat mass index
VLOGA LEPTINA PRI KAHEKSIJI KLB
bull Zvišan pri KLB
bull Deluje podobno kot citokinski receptorji
tipa IL6(vnetje)
bull Preko receptorjev za melanocortin v
hipotalamusu deluje na apetit in
metabolizem
bull Antagonisti MC-R4 receptorja nov
terapevtski obet
VELIK POMEN PREHRANSKE
DIAGNOSTIKE ZA DIALIZNE PACIENTE
bull Klinična presoja pacienta in kvalitete
življenja oziroma uspeha zdravljenja
bull Biokemijavrednosti albuminov
prealbumina in vnosa proteinov (35gl
300mgl 1gkgdan)
bull Nadzor telesna teža BMI SGA
BCM(bioimpedanca) serumski albumin
kreatinin
SUBJEKTIVNA GLOBALNA
NUTRICIJSKA OCENA-SGA
SGA ocena prehranjenosti zajema
bull anamnezo (o spremembi telesne teže o
vnosu hrane simptomih s strani GIT
funkcionalne zmogljivosti) in
bull telesni pregled (atrofija mišic zmanjšanje
podkožne maščobe in pojav oteklin)
bull zlati standard ocene bolnika(Keith
Nutrition in Clinical Practice 2008)
Malnutrition Inflammation Score
(MIS)
bullFully quantitative
bullUses the 7 original SGA components
bullAdds 3 new components
ndashBody mass index
ndashSerum albumin
ndashSerum total iron binding capacity
PEM - PROTEINSKO
ENERGETSKA MALNUTRICIJA
bull PEM je pogost v KLB
bull Je povezan s povečano obolevnostjo in
umrljivostjo
bull 40 PEM na začetku nadomestnega
zdravljenja KOL
bull 10-70 HD pacientov
bull 18-51 CAPD pacientov
Nutritional RecommendationsDialysisStage 5 CKD
KDOQI1 ESPEN2 EBPG3
EnergyCalories lt 60 years 35
kcalkgd
60 years or obese
30-35 kcalkgd
35 kcalkgd 30-40 kcalkgd
Protein 12 gkgd
50 HBV
12-14 gkg
IBWd
11 gkgd
Sodium ― 18-25 gd 2000-3000
mgd
Fluid ― 1000 mL + urine
volume
―
Potassium ― 2000-2500 mgd 1950-2730
mgd
Phosphorus 800-1000 mgd
lt 17 mgkg IBW or
SBWd
800-1000 mgd 800-1000 mgd
Calcium 2 gd ― 2000 mgd
1 NKF KDOQI Clinical practice guidelines for nutrition in chronic renal failure AJKD 2000 35S1-S140
2 Cano N et al Clin Nutr 2006 25295-310
3 Fouque D et al NDT 2007 22(suppl 2)ii45-ii87
Ocena prehranskih potreb
bull V akutni fazi 20-25 nebeljakovinskih kkalkgdan v anabolni fazi in podhranjeni 25 -30 kkalkgdan
bull Maščobe 03 gkg ttdan do 2 gkg ttdan (30 do 70)
bull Ogljikovi hidrati 2-5g kgdan (30 do 70)
bull Beljakovine povprečno 15 g kg tt dan (15 -20 )
bull Mikrohranila-dnevne priporočene potrebe individualno glede na obolenje
bull Opečenci več Cu Se in Zn
AA V PARENTERALNI PREHRANI
bull Povečana izguba AA
bull Neravnovesje med izgubo in porabo
bull Esencielne AA z dodatkom histidina ter arginina niso optimum
bull Nadomeščanje tirozina problem zaradi slabe topnostihellip
bull Acetil-tirozin je rešitev vendar ne pri KLB
bull Rešitev predstavlja dipeptid glicil-tirozin ki je dobro topen in idealno nadomešča večje potrebe po tirozinu pri KLB (AminoMel nephro)
PREHRANSKI DODATKI
Enteralni
bull Nepro Nepro HP Nepro LP Ensure Ensure Plus Advance Prosure Fresubinhellipenkrat na dan per os
bull Glutamin 5-10g na dan per os
bull Carenal 1 tableto po dializi
bull L-karnitin
Parenteralni
bull Aminomel Nephro aminokisline (500ml med HD)
bull Kabiven
bull Glamin 500ml
bull Dipeptiven 100ml
bull Soluvit N(vodotopni vitamini)
bull Vitalipid N(maščobotopni vitamini)
bull Addamel N(mikroelementi)
bull Omegaven (ribje oljehellip)
Component Renal Specific
ONS
Standard ONS
Protein Optimum Medium
Glycemic Index
(Carbohydrates) Low High
MUFA Omega-3
(FatsLipids) High Low
Electrolytes
Phosphorus
Potassium Sodium
Low High
Fluid volume Low High
Caloric density High Standard
Fiber High Low
Prebiotics scFOS Present None
CKD-specific vitamin
amp mineral profile Optimized None
Why Renal Specific ONS
Why Standard versus Renal Specific ONS
Nutrition Intervention in CKD Patients
bull Expert recommendations
KDOQI1 ESPEN2 EBPG3
Nutrition
Support
Individuals undergoing
maintenance dialysis
who are unable to
meet their protein and
energy requirements
with food intake for an
extended period of
time should receive
nutritional support
Special formula
products for HD
treatment can be
useful especially in
malnourished patients
who are not able to
increase their nutrient
intake
Oral nutritional
supplements should
be prescribed if
nutritional counseling
does not achieve an
increase in nutrient
intake to a level that
covers minimum
recommendations
Products
specifically
designed for
dialysis patients
should be
prescribed
1 NKF KDOQI Clinical practice guidelines for nutrition in chronic renal failure AJKD 2000 35S1-S140
2 Cano N et al Clin Nutr 2006 25295-310
3 Fouque D et al NDT 2007 22(suppl 2)ii45-ii87
Recomm-S
ESPEN KDOQI EBPG
Proteini (gkgdan) 12-14 10-12 11
Energija
(kCalkgdan)
35 lt60 g 35
gt60 g 30
30-35
gt50 intke lt1 gkgdan
Actual ntake 20-25 kCalkg 08-1 g proteinakg
Renal Specific Nutritional Therapy
Clinical studies have shown that renal-specific nutrition offers advantages over standard nutrition
bull Phosphorus levels were lower with the renal-specific nutrition than with the standard nutrition1
bull Less fluid and potassium in renal-specific nutrition offers advantages over standard nutrition2
1 Cockram DB et al J Ren Nutr 1998825-33
2 Williams RF Summers AM J Ren Nutr 200919183-188
PREHRANSKE ZAHTEVE DIALIZE
PRAKSA
ENERGIJA 35KCALKG TT NA DAN
PROTEINI 12GKG TT NA DAN
VNOS TEKOČINE 1000ML + IZLOČEN URIN
NATRIJ 2-3G NA DAN
KALIJ 2-3G NA DAN
FOSFOR 08-12GDAN
NKFKDOQI 2000 ADA 2002 WILKENS 2004
BIOIMPEDANCE PRINCIPLES
Phase angle
bull Phase angle is an indicator based on reactance and
resistance obtained from bioelectrical impedance
analysis (BIA)
bull PA depends on cell membrane integrity and on body cell
mass
bull Although its biological meaning is still not clear phase
angle appears to have an important prognostic role
bull Phase angle differs across categories of sex age BMI
and percentage fat bull Maria Cristina G Barbosa-Silva Aluiacutesio JD Barros Jack Wang Steven B Heymsfield and Richard
N Pierson Jr Am J Clin Nutr July 2005 vol 82 no 1 49-52
bull Satish Kumar1 Aswini Dutt1 Sandhya Hemraj2 Shankar Bhat1 and Bhat Manipadybhima Iran
J Basic Med Sci 2012 Nov-Dec 15(6) 1180ndash1184
PHASE ANGLE AND LEAN TISSUE
INDEX ARE SLIGHTLY HIGHER IN
HEMODIALYSIS THAN IN PERITONEAL
DIALYSIS GROUP OF PATIENTS
BKnap ZVeceric Haler JButurovic-Ponikvar
RPonikvar AF Bren
University Clinical Center Ljubljana
Department of Nephrology Slovenia
Ideal nutrition ndash CKD patients
bull Prevents musle loss
bull Prevent andor treat PEW
bull Correct metabolic derrangements
bull Decrease morbidity and mortlity
bull Improve QoL
bull Does not promote progression of CKD
bull Or ideally slow down progression of CKD
ZAKLJUČEK
bull Podhranjenost je pomembna in pogosto
ključna za preživetje
bull Sodobne metode detekcije in zdravljenja
podhranjenosti omogočajo zgodnejšo
nutricijsko intervencijo
bull Prehranski dodatki tako enteralni kot
parenteralni so pogosto nujna in včasih
edina možnost
Kaj je dobro vedetihelliphellip
bull LEDVIČNI BOLNIKI JEDO SLABO
bull V ZAČETNI FAZI KLB TERAPIJA Z OMEJEVANJEM VNOSA PROTEINOV LAHKO PRIPELJE DO MALNUTRICIJE IN KAHEKSIJE
bull POMEMBNA OCENA HRANJENOSTI IN PRAVOČASNA NUTRICIJSKA INTERVENCIJA V VSEH FAZAH KLB
bull USPEH ZDRAVLJENJA MALNUTRICIJE JE POVEZAN Z DOBRIM ZDRAVLJENJEM OSNOVNE LEDVIČNE BOLEZNI IN CELOSTNEGA ZDRAVLJENJA KLB
bull POLEG HRANE VELIKO PRISPEVAJO K KVALITETI ŽIVLJENJA TUDI PREHRANSKI DODATKI IN TELESNA VADBA
bull ANABOLNI AGENSI IN STIMULATORJI APETITA NA NIVOJU HIPOTALAMUSA SO OBET BLIŽNJE PRIHODNOSTI
DIETA LEDVIČNEGA BOLNIKA
Phosphorus balance
ŠTEVILNI VZROKI PODHRANJENOSTI PRI
LEDVIČNI BOLEZNI
bull Zmanjšan vnos hrane
bull Omejevalne diete proteini
bull Uremični toksini
bull Metabolna acidoza
bull Endokrini dejavniki
bull Gastrointestinalni dejavniki
bull MIA sindrom
UREMIČNI SINDROM
Vodi k podhranjenosti tudi zaradi
bull Insulinske rezistence
bull Motenega klirensa lipidov
bull Metabolične acidoze
bull Sekundarnega hiperparatireoidizma
uremične kostne bolezni
DEBELOST OGROŽA TUDI
LEDVIČNE BOLNIKE
bull METABOLIČNI SINDROM
bull SLADKORNA BOLEZEN II
bull MAŠČOBNE CELICE KOT ENDOKRINI ORGAN TUDI PRI KLB VPLIVAJO NA KVS
bull PROBLEM MOTENJ HRANJENJA IN MALNUTRICIJA Z OHRANJENO TELESNO MASO OB ZMANJŠANJU PUSTE TELESNE MASE
bull pomen določanja puste telesne mase z bioimpedanco
bull lean tissue index fat mass index
VLOGA LEPTINA PRI KAHEKSIJI KLB
bull Zvišan pri KLB
bull Deluje podobno kot citokinski receptorji
tipa IL6(vnetje)
bull Preko receptorjev za melanocortin v
hipotalamusu deluje na apetit in
metabolizem
bull Antagonisti MC-R4 receptorja nov
terapevtski obet
VELIK POMEN PREHRANSKE
DIAGNOSTIKE ZA DIALIZNE PACIENTE
bull Klinična presoja pacienta in kvalitete
življenja oziroma uspeha zdravljenja
bull Biokemijavrednosti albuminov
prealbumina in vnosa proteinov (35gl
300mgl 1gkgdan)
bull Nadzor telesna teža BMI SGA
BCM(bioimpedanca) serumski albumin
kreatinin
SUBJEKTIVNA GLOBALNA
NUTRICIJSKA OCENA-SGA
SGA ocena prehranjenosti zajema
bull anamnezo (o spremembi telesne teže o
vnosu hrane simptomih s strani GIT
funkcionalne zmogljivosti) in
bull telesni pregled (atrofija mišic zmanjšanje
podkožne maščobe in pojav oteklin)
bull zlati standard ocene bolnika(Keith
Nutrition in Clinical Practice 2008)
Malnutrition Inflammation Score
(MIS)
bullFully quantitative
bullUses the 7 original SGA components
bullAdds 3 new components
ndashBody mass index
ndashSerum albumin
ndashSerum total iron binding capacity
PEM - PROTEINSKO
ENERGETSKA MALNUTRICIJA
bull PEM je pogost v KLB
bull Je povezan s povečano obolevnostjo in
umrljivostjo
bull 40 PEM na začetku nadomestnega
zdravljenja KOL
bull 10-70 HD pacientov
bull 18-51 CAPD pacientov
Nutritional RecommendationsDialysisStage 5 CKD
KDOQI1 ESPEN2 EBPG3
EnergyCalories lt 60 years 35
kcalkgd
60 years or obese
30-35 kcalkgd
35 kcalkgd 30-40 kcalkgd
Protein 12 gkgd
50 HBV
12-14 gkg
IBWd
11 gkgd
Sodium ― 18-25 gd 2000-3000
mgd
Fluid ― 1000 mL + urine
volume
―
Potassium ― 2000-2500 mgd 1950-2730
mgd
Phosphorus 800-1000 mgd
lt 17 mgkg IBW or
SBWd
800-1000 mgd 800-1000 mgd
Calcium 2 gd ― 2000 mgd
1 NKF KDOQI Clinical practice guidelines for nutrition in chronic renal failure AJKD 2000 35S1-S140
2 Cano N et al Clin Nutr 2006 25295-310
3 Fouque D et al NDT 2007 22(suppl 2)ii45-ii87
Ocena prehranskih potreb
bull V akutni fazi 20-25 nebeljakovinskih kkalkgdan v anabolni fazi in podhranjeni 25 -30 kkalkgdan
bull Maščobe 03 gkg ttdan do 2 gkg ttdan (30 do 70)
bull Ogljikovi hidrati 2-5g kgdan (30 do 70)
bull Beljakovine povprečno 15 g kg tt dan (15 -20 )
bull Mikrohranila-dnevne priporočene potrebe individualno glede na obolenje
bull Opečenci več Cu Se in Zn
AA V PARENTERALNI PREHRANI
bull Povečana izguba AA
bull Neravnovesje med izgubo in porabo
bull Esencielne AA z dodatkom histidina ter arginina niso optimum
bull Nadomeščanje tirozina problem zaradi slabe topnostihellip
bull Acetil-tirozin je rešitev vendar ne pri KLB
bull Rešitev predstavlja dipeptid glicil-tirozin ki je dobro topen in idealno nadomešča večje potrebe po tirozinu pri KLB (AminoMel nephro)
PREHRANSKI DODATKI
Enteralni
bull Nepro Nepro HP Nepro LP Ensure Ensure Plus Advance Prosure Fresubinhellipenkrat na dan per os
bull Glutamin 5-10g na dan per os
bull Carenal 1 tableto po dializi
bull L-karnitin
Parenteralni
bull Aminomel Nephro aminokisline (500ml med HD)
bull Kabiven
bull Glamin 500ml
bull Dipeptiven 100ml
bull Soluvit N(vodotopni vitamini)
bull Vitalipid N(maščobotopni vitamini)
bull Addamel N(mikroelementi)
bull Omegaven (ribje oljehellip)
Component Renal Specific
ONS
Standard ONS
Protein Optimum Medium
Glycemic Index
(Carbohydrates) Low High
MUFA Omega-3
(FatsLipids) High Low
Electrolytes
Phosphorus
Potassium Sodium
Low High
Fluid volume Low High
Caloric density High Standard
Fiber High Low
Prebiotics scFOS Present None
CKD-specific vitamin
amp mineral profile Optimized None
Why Renal Specific ONS
Why Standard versus Renal Specific ONS
Nutrition Intervention in CKD Patients
bull Expert recommendations
KDOQI1 ESPEN2 EBPG3
Nutrition
Support
Individuals undergoing
maintenance dialysis
who are unable to
meet their protein and
energy requirements
with food intake for an
extended period of
time should receive
nutritional support
Special formula
products for HD
treatment can be
useful especially in
malnourished patients
who are not able to
increase their nutrient
intake
Oral nutritional
supplements should
be prescribed if
nutritional counseling
does not achieve an
increase in nutrient
intake to a level that
covers minimum
recommendations
Products
specifically
designed for
dialysis patients
should be
prescribed
1 NKF KDOQI Clinical practice guidelines for nutrition in chronic renal failure AJKD 2000 35S1-S140
2 Cano N et al Clin Nutr 2006 25295-310
3 Fouque D et al NDT 2007 22(suppl 2)ii45-ii87
Recomm-S
ESPEN KDOQI EBPG
Proteini (gkgdan) 12-14 10-12 11
Energija
(kCalkgdan)
35 lt60 g 35
gt60 g 30
30-35
gt50 intke lt1 gkgdan
Actual ntake 20-25 kCalkg 08-1 g proteinakg
Renal Specific Nutritional Therapy
Clinical studies have shown that renal-specific nutrition offers advantages over standard nutrition
bull Phosphorus levels were lower with the renal-specific nutrition than with the standard nutrition1
bull Less fluid and potassium in renal-specific nutrition offers advantages over standard nutrition2
1 Cockram DB et al J Ren Nutr 1998825-33
2 Williams RF Summers AM J Ren Nutr 200919183-188
PREHRANSKE ZAHTEVE DIALIZE
PRAKSA
ENERGIJA 35KCALKG TT NA DAN
PROTEINI 12GKG TT NA DAN
VNOS TEKOČINE 1000ML + IZLOČEN URIN
NATRIJ 2-3G NA DAN
KALIJ 2-3G NA DAN
FOSFOR 08-12GDAN
NKFKDOQI 2000 ADA 2002 WILKENS 2004
BIOIMPEDANCE PRINCIPLES
Phase angle
bull Phase angle is an indicator based on reactance and
resistance obtained from bioelectrical impedance
analysis (BIA)
bull PA depends on cell membrane integrity and on body cell
mass
bull Although its biological meaning is still not clear phase
angle appears to have an important prognostic role
bull Phase angle differs across categories of sex age BMI
and percentage fat bull Maria Cristina G Barbosa-Silva Aluiacutesio JD Barros Jack Wang Steven B Heymsfield and Richard
N Pierson Jr Am J Clin Nutr July 2005 vol 82 no 1 49-52
bull Satish Kumar1 Aswini Dutt1 Sandhya Hemraj2 Shankar Bhat1 and Bhat Manipadybhima Iran
J Basic Med Sci 2012 Nov-Dec 15(6) 1180ndash1184
PHASE ANGLE AND LEAN TISSUE
INDEX ARE SLIGHTLY HIGHER IN
HEMODIALYSIS THAN IN PERITONEAL
DIALYSIS GROUP OF PATIENTS
BKnap ZVeceric Haler JButurovic-Ponikvar
RPonikvar AF Bren
University Clinical Center Ljubljana
Department of Nephrology Slovenia
Ideal nutrition ndash CKD patients
bull Prevents musle loss
bull Prevent andor treat PEW
bull Correct metabolic derrangements
bull Decrease morbidity and mortlity
bull Improve QoL
bull Does not promote progression of CKD
bull Or ideally slow down progression of CKD
ZAKLJUČEK
bull Podhranjenost je pomembna in pogosto
ključna za preživetje
bull Sodobne metode detekcije in zdravljenja
podhranjenosti omogočajo zgodnejšo
nutricijsko intervencijo
bull Prehranski dodatki tako enteralni kot
parenteralni so pogosto nujna in včasih
edina možnost
Kaj je dobro vedetihelliphellip
bull LEDVIČNI BOLNIKI JEDO SLABO
bull V ZAČETNI FAZI KLB TERAPIJA Z OMEJEVANJEM VNOSA PROTEINOV LAHKO PRIPELJE DO MALNUTRICIJE IN KAHEKSIJE
bull POMEMBNA OCENA HRANJENOSTI IN PRAVOČASNA NUTRICIJSKA INTERVENCIJA V VSEH FAZAH KLB
bull USPEH ZDRAVLJENJA MALNUTRICIJE JE POVEZAN Z DOBRIM ZDRAVLJENJEM OSNOVNE LEDVIČNE BOLEZNI IN CELOSTNEGA ZDRAVLJENJA KLB
bull POLEG HRANE VELIKO PRISPEVAJO K KVALITETI ŽIVLJENJA TUDI PREHRANSKI DODATKI IN TELESNA VADBA
bull ANABOLNI AGENSI IN STIMULATORJI APETITA NA NIVOJU HIPOTALAMUSA SO OBET BLIŽNJE PRIHODNOSTI
Phosphorus balance
ŠTEVILNI VZROKI PODHRANJENOSTI PRI
LEDVIČNI BOLEZNI
bull Zmanjšan vnos hrane
bull Omejevalne diete proteini
bull Uremični toksini
bull Metabolna acidoza
bull Endokrini dejavniki
bull Gastrointestinalni dejavniki
bull MIA sindrom
UREMIČNI SINDROM
Vodi k podhranjenosti tudi zaradi
bull Insulinske rezistence
bull Motenega klirensa lipidov
bull Metabolične acidoze
bull Sekundarnega hiperparatireoidizma
uremične kostne bolezni
DEBELOST OGROŽA TUDI
LEDVIČNE BOLNIKE
bull METABOLIČNI SINDROM
bull SLADKORNA BOLEZEN II
bull MAŠČOBNE CELICE KOT ENDOKRINI ORGAN TUDI PRI KLB VPLIVAJO NA KVS
bull PROBLEM MOTENJ HRANJENJA IN MALNUTRICIJA Z OHRANJENO TELESNO MASO OB ZMANJŠANJU PUSTE TELESNE MASE
bull pomen določanja puste telesne mase z bioimpedanco
bull lean tissue index fat mass index
VLOGA LEPTINA PRI KAHEKSIJI KLB
bull Zvišan pri KLB
bull Deluje podobno kot citokinski receptorji
tipa IL6(vnetje)
bull Preko receptorjev za melanocortin v
hipotalamusu deluje na apetit in
metabolizem
bull Antagonisti MC-R4 receptorja nov
terapevtski obet
VELIK POMEN PREHRANSKE
DIAGNOSTIKE ZA DIALIZNE PACIENTE
bull Klinična presoja pacienta in kvalitete
življenja oziroma uspeha zdravljenja
bull Biokemijavrednosti albuminov
prealbumina in vnosa proteinov (35gl
300mgl 1gkgdan)
bull Nadzor telesna teža BMI SGA
BCM(bioimpedanca) serumski albumin
kreatinin
SUBJEKTIVNA GLOBALNA
NUTRICIJSKA OCENA-SGA
SGA ocena prehranjenosti zajema
bull anamnezo (o spremembi telesne teže o
vnosu hrane simptomih s strani GIT
funkcionalne zmogljivosti) in
bull telesni pregled (atrofija mišic zmanjšanje
podkožne maščobe in pojav oteklin)
bull zlati standard ocene bolnika(Keith
Nutrition in Clinical Practice 2008)
Malnutrition Inflammation Score
(MIS)
bullFully quantitative
bullUses the 7 original SGA components
bullAdds 3 new components
ndashBody mass index
ndashSerum albumin
ndashSerum total iron binding capacity
PEM - PROTEINSKO
ENERGETSKA MALNUTRICIJA
bull PEM je pogost v KLB
bull Je povezan s povečano obolevnostjo in
umrljivostjo
bull 40 PEM na začetku nadomestnega
zdravljenja KOL
bull 10-70 HD pacientov
bull 18-51 CAPD pacientov
Nutritional RecommendationsDialysisStage 5 CKD
KDOQI1 ESPEN2 EBPG3
EnergyCalories lt 60 years 35
kcalkgd
60 years or obese
30-35 kcalkgd
35 kcalkgd 30-40 kcalkgd
Protein 12 gkgd
50 HBV
12-14 gkg
IBWd
11 gkgd
Sodium ― 18-25 gd 2000-3000
mgd
Fluid ― 1000 mL + urine
volume
―
Potassium ― 2000-2500 mgd 1950-2730
mgd
Phosphorus 800-1000 mgd
lt 17 mgkg IBW or
SBWd
800-1000 mgd 800-1000 mgd
Calcium 2 gd ― 2000 mgd
1 NKF KDOQI Clinical practice guidelines for nutrition in chronic renal failure AJKD 2000 35S1-S140
2 Cano N et al Clin Nutr 2006 25295-310
3 Fouque D et al NDT 2007 22(suppl 2)ii45-ii87
Ocena prehranskih potreb
bull V akutni fazi 20-25 nebeljakovinskih kkalkgdan v anabolni fazi in podhranjeni 25 -30 kkalkgdan
bull Maščobe 03 gkg ttdan do 2 gkg ttdan (30 do 70)
bull Ogljikovi hidrati 2-5g kgdan (30 do 70)
bull Beljakovine povprečno 15 g kg tt dan (15 -20 )
bull Mikrohranila-dnevne priporočene potrebe individualno glede na obolenje
bull Opečenci več Cu Se in Zn
AA V PARENTERALNI PREHRANI
bull Povečana izguba AA
bull Neravnovesje med izgubo in porabo
bull Esencielne AA z dodatkom histidina ter arginina niso optimum
bull Nadomeščanje tirozina problem zaradi slabe topnostihellip
bull Acetil-tirozin je rešitev vendar ne pri KLB
bull Rešitev predstavlja dipeptid glicil-tirozin ki je dobro topen in idealno nadomešča večje potrebe po tirozinu pri KLB (AminoMel nephro)
PREHRANSKI DODATKI
Enteralni
bull Nepro Nepro HP Nepro LP Ensure Ensure Plus Advance Prosure Fresubinhellipenkrat na dan per os
bull Glutamin 5-10g na dan per os
bull Carenal 1 tableto po dializi
bull L-karnitin
Parenteralni
bull Aminomel Nephro aminokisline (500ml med HD)
bull Kabiven
bull Glamin 500ml
bull Dipeptiven 100ml
bull Soluvit N(vodotopni vitamini)
bull Vitalipid N(maščobotopni vitamini)
bull Addamel N(mikroelementi)
bull Omegaven (ribje oljehellip)
Component Renal Specific
ONS
Standard ONS
Protein Optimum Medium
Glycemic Index
(Carbohydrates) Low High
MUFA Omega-3
(FatsLipids) High Low
Electrolytes
Phosphorus
Potassium Sodium
Low High
Fluid volume Low High
Caloric density High Standard
Fiber High Low
Prebiotics scFOS Present None
CKD-specific vitamin
amp mineral profile Optimized None
Why Renal Specific ONS
Why Standard versus Renal Specific ONS
Nutrition Intervention in CKD Patients
bull Expert recommendations
KDOQI1 ESPEN2 EBPG3
Nutrition
Support
Individuals undergoing
maintenance dialysis
who are unable to
meet their protein and
energy requirements
with food intake for an
extended period of
time should receive
nutritional support
Special formula
products for HD
treatment can be
useful especially in
malnourished patients
who are not able to
increase their nutrient
intake
Oral nutritional
supplements should
be prescribed if
nutritional counseling
does not achieve an
increase in nutrient
intake to a level that
covers minimum
recommendations
Products
specifically
designed for
dialysis patients
should be
prescribed
1 NKF KDOQI Clinical practice guidelines for nutrition in chronic renal failure AJKD 2000 35S1-S140
2 Cano N et al Clin Nutr 2006 25295-310
3 Fouque D et al NDT 2007 22(suppl 2)ii45-ii87
Recomm-S
ESPEN KDOQI EBPG
Proteini (gkgdan) 12-14 10-12 11
Energija
(kCalkgdan)
35 lt60 g 35
gt60 g 30
30-35
gt50 intke lt1 gkgdan
Actual ntake 20-25 kCalkg 08-1 g proteinakg
Renal Specific Nutritional Therapy
Clinical studies have shown that renal-specific nutrition offers advantages over standard nutrition
bull Phosphorus levels were lower with the renal-specific nutrition than with the standard nutrition1
bull Less fluid and potassium in renal-specific nutrition offers advantages over standard nutrition2
1 Cockram DB et al J Ren Nutr 1998825-33
2 Williams RF Summers AM J Ren Nutr 200919183-188
PREHRANSKE ZAHTEVE DIALIZE
PRAKSA
ENERGIJA 35KCALKG TT NA DAN
PROTEINI 12GKG TT NA DAN
VNOS TEKOČINE 1000ML + IZLOČEN URIN
NATRIJ 2-3G NA DAN
KALIJ 2-3G NA DAN
FOSFOR 08-12GDAN
NKFKDOQI 2000 ADA 2002 WILKENS 2004
BIOIMPEDANCE PRINCIPLES
Phase angle
bull Phase angle is an indicator based on reactance and
resistance obtained from bioelectrical impedance
analysis (BIA)
bull PA depends on cell membrane integrity and on body cell
mass
bull Although its biological meaning is still not clear phase
angle appears to have an important prognostic role
bull Phase angle differs across categories of sex age BMI
and percentage fat bull Maria Cristina G Barbosa-Silva Aluiacutesio JD Barros Jack Wang Steven B Heymsfield and Richard
N Pierson Jr Am J Clin Nutr July 2005 vol 82 no 1 49-52
bull Satish Kumar1 Aswini Dutt1 Sandhya Hemraj2 Shankar Bhat1 and Bhat Manipadybhima Iran
J Basic Med Sci 2012 Nov-Dec 15(6) 1180ndash1184
PHASE ANGLE AND LEAN TISSUE
INDEX ARE SLIGHTLY HIGHER IN
HEMODIALYSIS THAN IN PERITONEAL
DIALYSIS GROUP OF PATIENTS
BKnap ZVeceric Haler JButurovic-Ponikvar
RPonikvar AF Bren
University Clinical Center Ljubljana
Department of Nephrology Slovenia
Ideal nutrition ndash CKD patients
bull Prevents musle loss
bull Prevent andor treat PEW
bull Correct metabolic derrangements
bull Decrease morbidity and mortlity
bull Improve QoL
bull Does not promote progression of CKD
bull Or ideally slow down progression of CKD
ZAKLJUČEK
bull Podhranjenost je pomembna in pogosto
ključna za preživetje
bull Sodobne metode detekcije in zdravljenja
podhranjenosti omogočajo zgodnejšo
nutricijsko intervencijo
bull Prehranski dodatki tako enteralni kot
parenteralni so pogosto nujna in včasih
edina možnost
Kaj je dobro vedetihelliphellip
bull LEDVIČNI BOLNIKI JEDO SLABO
bull V ZAČETNI FAZI KLB TERAPIJA Z OMEJEVANJEM VNOSA PROTEINOV LAHKO PRIPELJE DO MALNUTRICIJE IN KAHEKSIJE
bull POMEMBNA OCENA HRANJENOSTI IN PRAVOČASNA NUTRICIJSKA INTERVENCIJA V VSEH FAZAH KLB
bull USPEH ZDRAVLJENJA MALNUTRICIJE JE POVEZAN Z DOBRIM ZDRAVLJENJEM OSNOVNE LEDVIČNE BOLEZNI IN CELOSTNEGA ZDRAVLJENJA KLB
bull POLEG HRANE VELIKO PRISPEVAJO K KVALITETI ŽIVLJENJA TUDI PREHRANSKI DODATKI IN TELESNA VADBA
bull ANABOLNI AGENSI IN STIMULATORJI APETITA NA NIVOJU HIPOTALAMUSA SO OBET BLIŽNJE PRIHODNOSTI

ŠTEVILNI VZROKI PODHRANJENOSTI PRI
LEDVIČNI BOLEZNI
bull Zmanjšan vnos hrane
bull Omejevalne diete proteini
bull Uremični toksini
bull Metabolna acidoza
bull Endokrini dejavniki
bull Gastrointestinalni dejavniki
bull MIA sindrom
UREMIČNI SINDROM
Vodi k podhranjenosti tudi zaradi
bull Insulinske rezistence
bull Motenega klirensa lipidov
bull Metabolične acidoze
bull Sekundarnega hiperparatireoidizma
uremične kostne bolezni
DEBELOST OGROŽA TUDI
LEDVIČNE BOLNIKE
bull METABOLIČNI SINDROM
bull SLADKORNA BOLEZEN II
bull MAŠČOBNE CELICE KOT ENDOKRINI ORGAN TUDI PRI KLB VPLIVAJO NA KVS
bull PROBLEM MOTENJ HRANJENJA IN MALNUTRICIJA Z OHRANJENO TELESNO MASO OB ZMANJŠANJU PUSTE TELESNE MASE
bull pomen določanja puste telesne mase z bioimpedanco
bull lean tissue index fat mass index
VLOGA LEPTINA PRI KAHEKSIJI KLB
bull Zvišan pri KLB
bull Deluje podobno kot citokinski receptorji
tipa IL6(vnetje)
bull Preko receptorjev za melanocortin v
hipotalamusu deluje na apetit in
metabolizem
bull Antagonisti MC-R4 receptorja nov
terapevtski obet
VELIK POMEN PREHRANSKE
DIAGNOSTIKE ZA DIALIZNE PACIENTE
bull Klinična presoja pacienta in kvalitete
življenja oziroma uspeha zdravljenja
bull Biokemijavrednosti albuminov
prealbumina in vnosa proteinov (35gl
300mgl 1gkgdan)
bull Nadzor telesna teža BMI SGA
BCM(bioimpedanca) serumski albumin
kreatinin
SUBJEKTIVNA GLOBALNA
NUTRICIJSKA OCENA-SGA
SGA ocena prehranjenosti zajema
bull anamnezo (o spremembi telesne teže o
vnosu hrane simptomih s strani GIT
funkcionalne zmogljivosti) in
bull telesni pregled (atrofija mišic zmanjšanje
podkožne maščobe in pojav oteklin)
bull zlati standard ocene bolnika(Keith
Nutrition in Clinical Practice 2008)
Malnutrition Inflammation Score
(MIS)
bullFully quantitative
bullUses the 7 original SGA components
bullAdds 3 new components
ndashBody mass index
ndashSerum albumin
ndashSerum total iron binding capacity
PEM - PROTEINSKO
ENERGETSKA MALNUTRICIJA
bull PEM je pogost v KLB
bull Je povezan s povečano obolevnostjo in
umrljivostjo
bull 40 PEM na začetku nadomestnega
zdravljenja KOL
bull 10-70 HD pacientov
bull 18-51 CAPD pacientov
Nutritional RecommendationsDialysisStage 5 CKD
KDOQI1 ESPEN2 EBPG3
EnergyCalories lt 60 years 35
kcalkgd
60 years or obese
30-35 kcalkgd
35 kcalkgd 30-40 kcalkgd
Protein 12 gkgd
50 HBV
12-14 gkg
IBWd
11 gkgd
Sodium ― 18-25 gd 2000-3000
mgd
Fluid ― 1000 mL + urine
volume
―
Potassium ― 2000-2500 mgd 1950-2730
mgd
Phosphorus 800-1000 mgd
lt 17 mgkg IBW or
SBWd
800-1000 mgd 800-1000 mgd
Calcium 2 gd ― 2000 mgd
1 NKF KDOQI Clinical practice guidelines for nutrition in chronic renal failure AJKD 2000 35S1-S140
2 Cano N et al Clin Nutr 2006 25295-310
3 Fouque D et al NDT 2007 22(suppl 2)ii45-ii87
Ocena prehranskih potreb
bull V akutni fazi 20-25 nebeljakovinskih kkalkgdan v anabolni fazi in podhranjeni 25 -30 kkalkgdan
bull Maščobe 03 gkg ttdan do 2 gkg ttdan (30 do 70)
bull Ogljikovi hidrati 2-5g kgdan (30 do 70)
bull Beljakovine povprečno 15 g kg tt dan (15 -20 )
bull Mikrohranila-dnevne priporočene potrebe individualno glede na obolenje
bull Opečenci več Cu Se in Zn
AA V PARENTERALNI PREHRANI
bull Povečana izguba AA
bull Neravnovesje med izgubo in porabo
bull Esencielne AA z dodatkom histidina ter arginina niso optimum
bull Nadomeščanje tirozina problem zaradi slabe topnostihellip
bull Acetil-tirozin je rešitev vendar ne pri KLB
bull Rešitev predstavlja dipeptid glicil-tirozin ki je dobro topen in idealno nadomešča večje potrebe po tirozinu pri KLB (AminoMel nephro)
PREHRANSKI DODATKI
Enteralni
bull Nepro Nepro HP Nepro LP Ensure Ensure Plus Advance Prosure Fresubinhellipenkrat na dan per os
bull Glutamin 5-10g na dan per os
bull Carenal 1 tableto po dializi
bull L-karnitin
Parenteralni
bull Aminomel Nephro aminokisline (500ml med HD)
bull Kabiven
bull Glamin 500ml
bull Dipeptiven 100ml
bull Soluvit N(vodotopni vitamini)
bull Vitalipid N(maščobotopni vitamini)
bull Addamel N(mikroelementi)
bull Omegaven (ribje oljehellip)
Component Renal Specific
ONS
Standard ONS
Protein Optimum Medium
Glycemic Index
(Carbohydrates) Low High
MUFA Omega-3
(FatsLipids) High Low
Electrolytes
Phosphorus
Potassium Sodium
Low High
Fluid volume Low High
Caloric density High Standard
Fiber High Low
Prebiotics scFOS Present None
CKD-specific vitamin
amp mineral profile Optimized None
Why Renal Specific ONS
Why Standard versus Renal Specific ONS
Nutrition Intervention in CKD Patients
bull Expert recommendations
KDOQI1 ESPEN2 EBPG3
Nutrition
Support
Individuals undergoing
maintenance dialysis
who are unable to
meet their protein and
energy requirements
with food intake for an
extended period of
time should receive
nutritional support
Special formula
products for HD
treatment can be
useful especially in
malnourished patients
who are not able to
increase their nutrient
intake
Oral nutritional
supplements should
be prescribed if
nutritional counseling
does not achieve an
increase in nutrient
intake to a level that
covers minimum
recommendations
Products
specifically
designed for
dialysis patients
should be
prescribed
1 NKF KDOQI Clinical practice guidelines for nutrition in chronic renal failure AJKD 2000 35S1-S140
2 Cano N et al Clin Nutr 2006 25295-310
3 Fouque D et al NDT 2007 22(suppl 2)ii45-ii87
Recomm-S
ESPEN KDOQI EBPG
Proteini (gkgdan) 12-14 10-12 11
Energija
(kCalkgdan)
35 lt60 g 35
gt60 g 30
30-35
gt50 intke lt1 gkgdan
Actual ntake 20-25 kCalkg 08-1 g proteinakg
Renal Specific Nutritional Therapy
Clinical studies have shown that renal-specific nutrition offers advantages over standard nutrition
bull Phosphorus levels were lower with the renal-specific nutrition than with the standard nutrition1
bull Less fluid and potassium in renal-specific nutrition offers advantages over standard nutrition2
1 Cockram DB et al J Ren Nutr 1998825-33
2 Williams RF Summers AM J Ren Nutr 200919183-188
PREHRANSKE ZAHTEVE DIALIZE
PRAKSA
ENERGIJA 35KCALKG TT NA DAN
PROTEINI 12GKG TT NA DAN
VNOS TEKOČINE 1000ML + IZLOČEN URIN
NATRIJ 2-3G NA DAN
KALIJ 2-3G NA DAN
FOSFOR 08-12GDAN
NKFKDOQI 2000 ADA 2002 WILKENS 2004
BIOIMPEDANCE PRINCIPLES
Phase angle
bull Phase angle is an indicator based on reactance and
resistance obtained from bioelectrical impedance
analysis (BIA)
bull PA depends on cell membrane integrity and on body cell
mass
bull Although its biological meaning is still not clear phase
angle appears to have an important prognostic role
bull Phase angle differs across categories of sex age BMI
and percentage fat bull Maria Cristina G Barbosa-Silva Aluiacutesio JD Barros Jack Wang Steven B Heymsfield and Richard
N Pierson Jr Am J Clin Nutr July 2005 vol 82 no 1 49-52
bull Satish Kumar1 Aswini Dutt1 Sandhya Hemraj2 Shankar Bhat1 and Bhat Manipadybhima Iran
J Basic Med Sci 2012 Nov-Dec 15(6) 1180ndash1184
PHASE ANGLE AND LEAN TISSUE
INDEX ARE SLIGHTLY HIGHER IN
HEMODIALYSIS THAN IN PERITONEAL
DIALYSIS GROUP OF PATIENTS
BKnap ZVeceric Haler JButurovic-Ponikvar
RPonikvar AF Bren
University Clinical Center Ljubljana
Department of Nephrology Slovenia
Ideal nutrition ndash CKD patients
bull Prevents musle loss
bull Prevent andor treat PEW
bull Correct metabolic derrangements
bull Decrease morbidity and mortlity
bull Improve QoL
bull Does not promote progression of CKD
bull Or ideally slow down progression of CKD
ZAKLJUČEK
bull Podhranjenost je pomembna in pogosto
ključna za preživetje
bull Sodobne metode detekcije in zdravljenja
podhranjenosti omogočajo zgodnejšo
nutricijsko intervencijo
bull Prehranski dodatki tako enteralni kot
parenteralni so pogosto nujna in včasih
edina možnost
Kaj je dobro vedetihelliphellip
bull LEDVIČNI BOLNIKI JEDO SLABO
bull V ZAČETNI FAZI KLB TERAPIJA Z OMEJEVANJEM VNOSA PROTEINOV LAHKO PRIPELJE DO MALNUTRICIJE IN KAHEKSIJE
bull POMEMBNA OCENA HRANJENOSTI IN PRAVOČASNA NUTRICIJSKA INTERVENCIJA V VSEH FAZAH KLB
bull USPEH ZDRAVLJENJA MALNUTRICIJE JE POVEZAN Z DOBRIM ZDRAVLJENJEM OSNOVNE LEDVIČNE BOLEZNI IN CELOSTNEGA ZDRAVLJENJA KLB
bull POLEG HRANE VELIKO PRISPEVAJO K KVALITETI ŽIVLJENJA TUDI PREHRANSKI DODATKI IN TELESNA VADBA
bull ANABOLNI AGENSI IN STIMULATORJI APETITA NA NIVOJU HIPOTALAMUSA SO OBET BLIŽNJE PRIHODNOSTI

UREMIČNI SINDROM
Vodi k podhranjenosti tudi zaradi
bull Insulinske rezistence
bull Motenega klirensa lipidov
bull Metabolične acidoze
bull Sekundarnega hiperparatireoidizma
uremične kostne bolezni
DEBELOST OGROŽA TUDI
LEDVIČNE BOLNIKE
bull METABOLIČNI SINDROM
bull SLADKORNA BOLEZEN II
bull MAŠČOBNE CELICE KOT ENDOKRINI ORGAN TUDI PRI KLB VPLIVAJO NA KVS
bull PROBLEM MOTENJ HRANJENJA IN MALNUTRICIJA Z OHRANJENO TELESNO MASO OB ZMANJŠANJU PUSTE TELESNE MASE
bull pomen določanja puste telesne mase z bioimpedanco
bull lean tissue index fat mass index
VLOGA LEPTINA PRI KAHEKSIJI KLB
bull Zvišan pri KLB
bull Deluje podobno kot citokinski receptorji
tipa IL6(vnetje)
bull Preko receptorjev za melanocortin v
hipotalamusu deluje na apetit in
metabolizem
bull Antagonisti MC-R4 receptorja nov
terapevtski obet
VELIK POMEN PREHRANSKE
DIAGNOSTIKE ZA DIALIZNE PACIENTE
bull Klinična presoja pacienta in kvalitete
življenja oziroma uspeha zdravljenja
bull Biokemijavrednosti albuminov
prealbumina in vnosa proteinov (35gl
300mgl 1gkgdan)
bull Nadzor telesna teža BMI SGA
BCM(bioimpedanca) serumski albumin
kreatinin
SUBJEKTIVNA GLOBALNA
NUTRICIJSKA OCENA-SGA
SGA ocena prehranjenosti zajema
bull anamnezo (o spremembi telesne teže o
vnosu hrane simptomih s strani GIT
funkcionalne zmogljivosti) in
bull telesni pregled (atrofija mišic zmanjšanje
podkožne maščobe in pojav oteklin)
bull zlati standard ocene bolnika(Keith
Nutrition in Clinical Practice 2008)
Malnutrition Inflammation Score
(MIS)
bullFully quantitative
bullUses the 7 original SGA components
bullAdds 3 new components
ndashBody mass index
ndashSerum albumin
ndashSerum total iron binding capacity
PEM - PROTEINSKO
ENERGETSKA MALNUTRICIJA
bull PEM je pogost v KLB
bull Je povezan s povečano obolevnostjo in
umrljivostjo
bull 40 PEM na začetku nadomestnega
zdravljenja KOL
bull 10-70 HD pacientov
bull 18-51 CAPD pacientov
Nutritional RecommendationsDialysisStage 5 CKD
KDOQI1 ESPEN2 EBPG3
EnergyCalories lt 60 years 35
kcalkgd
60 years or obese
30-35 kcalkgd
35 kcalkgd 30-40 kcalkgd
Protein 12 gkgd
50 HBV
12-14 gkg
IBWd
11 gkgd
Sodium ― 18-25 gd 2000-3000
mgd
Fluid ― 1000 mL + urine
volume
―
Potassium ― 2000-2500 mgd 1950-2730
mgd
Phosphorus 800-1000 mgd
lt 17 mgkg IBW or
SBWd
800-1000 mgd 800-1000 mgd
Calcium 2 gd ― 2000 mgd
1 NKF KDOQI Clinical practice guidelines for nutrition in chronic renal failure AJKD 2000 35S1-S140
2 Cano N et al Clin Nutr 2006 25295-310
3 Fouque D et al NDT 2007 22(suppl 2)ii45-ii87
Ocena prehranskih potreb
bull V akutni fazi 20-25 nebeljakovinskih kkalkgdan v anabolni fazi in podhranjeni 25 -30 kkalkgdan
bull Maščobe 03 gkg ttdan do 2 gkg ttdan (30 do 70)
bull Ogljikovi hidrati 2-5g kgdan (30 do 70)
bull Beljakovine povprečno 15 g kg tt dan (15 -20 )
bull Mikrohranila-dnevne priporočene potrebe individualno glede na obolenje
bull Opečenci več Cu Se in Zn
AA V PARENTERALNI PREHRANI
bull Povečana izguba AA
bull Neravnovesje med izgubo in porabo
bull Esencielne AA z dodatkom histidina ter arginina niso optimum
bull Nadomeščanje tirozina problem zaradi slabe topnostihellip
bull Acetil-tirozin je rešitev vendar ne pri KLB
bull Rešitev predstavlja dipeptid glicil-tirozin ki je dobro topen in idealno nadomešča večje potrebe po tirozinu pri KLB (AminoMel nephro)
PREHRANSKI DODATKI
Enteralni
bull Nepro Nepro HP Nepro LP Ensure Ensure Plus Advance Prosure Fresubinhellipenkrat na dan per os
bull Glutamin 5-10g na dan per os
bull Carenal 1 tableto po dializi
bull L-karnitin
Parenteralni
bull Aminomel Nephro aminokisline (500ml med HD)
bull Kabiven
bull Glamin 500ml
bull Dipeptiven 100ml
bull Soluvit N(vodotopni vitamini)
bull Vitalipid N(maščobotopni vitamini)
bull Addamel N(mikroelementi)
bull Omegaven (ribje oljehellip)
Component Renal Specific
ONS
Standard ONS
Protein Optimum Medium
Glycemic Index
(Carbohydrates) Low High
MUFA Omega-3
(FatsLipids) High Low
Electrolytes
Phosphorus
Potassium Sodium
Low High
Fluid volume Low High
Caloric density High Standard
Fiber High Low
Prebiotics scFOS Present None
CKD-specific vitamin
amp mineral profile Optimized None
Why Renal Specific ONS
Why Standard versus Renal Specific ONS
Nutrition Intervention in CKD Patients
bull Expert recommendations
KDOQI1 ESPEN2 EBPG3
Nutrition
Support
Individuals undergoing
maintenance dialysis
who are unable to
meet their protein and
energy requirements
with food intake for an
extended period of
time should receive
nutritional support
Special formula
products for HD
treatment can be
useful especially in
malnourished patients
who are not able to
increase their nutrient
intake
Oral nutritional
supplements should
be prescribed if
nutritional counseling
does not achieve an
increase in nutrient
intake to a level that
covers minimum
recommendations
Products
specifically
designed for
dialysis patients
should be
prescribed
1 NKF KDOQI Clinical practice guidelines for nutrition in chronic renal failure AJKD 2000 35S1-S140
2 Cano N et al Clin Nutr 2006 25295-310
3 Fouque D et al NDT 2007 22(suppl 2)ii45-ii87
Recomm-S
ESPEN KDOQI EBPG
Proteini (gkgdan) 12-14 10-12 11
Energija
(kCalkgdan)
35 lt60 g 35
gt60 g 30
30-35
gt50 intke lt1 gkgdan
Actual ntake 20-25 kCalkg 08-1 g proteinakg
Renal Specific Nutritional Therapy
Clinical studies have shown that renal-specific nutrition offers advantages over standard nutrition
bull Phosphorus levels were lower with the renal-specific nutrition than with the standard nutrition1
bull Less fluid and potassium in renal-specific nutrition offers advantages over standard nutrition2
1 Cockram DB et al J Ren Nutr 1998825-33
2 Williams RF Summers AM J Ren Nutr 200919183-188
PREHRANSKE ZAHTEVE DIALIZE
PRAKSA
ENERGIJA 35KCALKG TT NA DAN
PROTEINI 12GKG TT NA DAN
VNOS TEKOČINE 1000ML + IZLOČEN URIN
NATRIJ 2-3G NA DAN
KALIJ 2-3G NA DAN
FOSFOR 08-12GDAN
NKFKDOQI 2000 ADA 2002 WILKENS 2004
BIOIMPEDANCE PRINCIPLES
Phase angle
bull Phase angle is an indicator based on reactance and
resistance obtained from bioelectrical impedance
analysis (BIA)
bull PA depends on cell membrane integrity and on body cell
mass
bull Although its biological meaning is still not clear phase
angle appears to have an important prognostic role
bull Phase angle differs across categories of sex age BMI
and percentage fat bull Maria Cristina G Barbosa-Silva Aluiacutesio JD Barros Jack Wang Steven B Heymsfield and Richard
N Pierson Jr Am J Clin Nutr July 2005 vol 82 no 1 49-52
bull Satish Kumar1 Aswini Dutt1 Sandhya Hemraj2 Shankar Bhat1 and Bhat Manipadybhima Iran
J Basic Med Sci 2012 Nov-Dec 15(6) 1180ndash1184
PHASE ANGLE AND LEAN TISSUE
INDEX ARE SLIGHTLY HIGHER IN
HEMODIALYSIS THAN IN PERITONEAL
DIALYSIS GROUP OF PATIENTS
BKnap ZVeceric Haler JButurovic-Ponikvar
RPonikvar AF Bren
University Clinical Center Ljubljana
Department of Nephrology Slovenia
Ideal nutrition ndash CKD patients
bull Prevents musle loss
bull Prevent andor treat PEW
bull Correct metabolic derrangements
bull Decrease morbidity and mortlity
bull Improve QoL
bull Does not promote progression of CKD
bull Or ideally slow down progression of CKD
ZAKLJUČEK
bull Podhranjenost je pomembna in pogosto
ključna za preživetje
bull Sodobne metode detekcije in zdravljenja
podhranjenosti omogočajo zgodnejšo
nutricijsko intervencijo
bull Prehranski dodatki tako enteralni kot
parenteralni so pogosto nujna in včasih
edina možnost
Kaj je dobro vedetihelliphellip
bull LEDVIČNI BOLNIKI JEDO SLABO
bull V ZAČETNI FAZI KLB TERAPIJA Z OMEJEVANJEM VNOSA PROTEINOV LAHKO PRIPELJE DO MALNUTRICIJE IN KAHEKSIJE
bull POMEMBNA OCENA HRANJENOSTI IN PRAVOČASNA NUTRICIJSKA INTERVENCIJA V VSEH FAZAH KLB
bull USPEH ZDRAVLJENJA MALNUTRICIJE JE POVEZAN Z DOBRIM ZDRAVLJENJEM OSNOVNE LEDVIČNE BOLEZNI IN CELOSTNEGA ZDRAVLJENJA KLB
bull POLEG HRANE VELIKO PRISPEVAJO K KVALITETI ŽIVLJENJA TUDI PREHRANSKI DODATKI IN TELESNA VADBA
bull ANABOLNI AGENSI IN STIMULATORJI APETITA NA NIVOJU HIPOTALAMUSA SO OBET BLIŽNJE PRIHODNOSTI

DEBELOST OGROŽA TUDI
LEDVIČNE BOLNIKE
bull METABOLIČNI SINDROM
bull SLADKORNA BOLEZEN II
bull MAŠČOBNE CELICE KOT ENDOKRINI ORGAN TUDI PRI KLB VPLIVAJO NA KVS
bull PROBLEM MOTENJ HRANJENJA IN MALNUTRICIJA Z OHRANJENO TELESNO MASO OB ZMANJŠANJU PUSTE TELESNE MASE
bull pomen določanja puste telesne mase z bioimpedanco
bull lean tissue index fat mass index
VLOGA LEPTINA PRI KAHEKSIJI KLB
bull Zvišan pri KLB
bull Deluje podobno kot citokinski receptorji
tipa IL6(vnetje)
bull Preko receptorjev za melanocortin v
hipotalamusu deluje na apetit in
metabolizem
bull Antagonisti MC-R4 receptorja nov
terapevtski obet
VELIK POMEN PREHRANSKE
DIAGNOSTIKE ZA DIALIZNE PACIENTE
bull Klinična presoja pacienta in kvalitete
življenja oziroma uspeha zdravljenja
bull Biokemijavrednosti albuminov
prealbumina in vnosa proteinov (35gl
300mgl 1gkgdan)
bull Nadzor telesna teža BMI SGA
BCM(bioimpedanca) serumski albumin
kreatinin
SUBJEKTIVNA GLOBALNA
NUTRICIJSKA OCENA-SGA
SGA ocena prehranjenosti zajema
bull anamnezo (o spremembi telesne teže o
vnosu hrane simptomih s strani GIT
funkcionalne zmogljivosti) in
bull telesni pregled (atrofija mišic zmanjšanje
podkožne maščobe in pojav oteklin)
bull zlati standard ocene bolnika(Keith
Nutrition in Clinical Practice 2008)
Malnutrition Inflammation Score
(MIS)
bullFully quantitative
bullUses the 7 original SGA components
bullAdds 3 new components
ndashBody mass index
ndashSerum albumin
ndashSerum total iron binding capacity
PEM - PROTEINSKO
ENERGETSKA MALNUTRICIJA
bull PEM je pogost v KLB
bull Je povezan s povečano obolevnostjo in
umrljivostjo
bull 40 PEM na začetku nadomestnega
zdravljenja KOL
bull 10-70 HD pacientov
bull 18-51 CAPD pacientov
Nutritional RecommendationsDialysisStage 5 CKD
KDOQI1 ESPEN2 EBPG3
EnergyCalories lt 60 years 35
kcalkgd
60 years or obese
30-35 kcalkgd
35 kcalkgd 30-40 kcalkgd
Protein 12 gkgd
50 HBV
12-14 gkg
IBWd
11 gkgd
Sodium ― 18-25 gd 2000-3000
mgd
Fluid ― 1000 mL + urine
volume
―
Potassium ― 2000-2500 mgd 1950-2730
mgd
Phosphorus 800-1000 mgd
lt 17 mgkg IBW or
SBWd
800-1000 mgd 800-1000 mgd
Calcium 2 gd ― 2000 mgd
1 NKF KDOQI Clinical practice guidelines for nutrition in chronic renal failure AJKD 2000 35S1-S140
2 Cano N et al Clin Nutr 2006 25295-310
3 Fouque D et al NDT 2007 22(suppl 2)ii45-ii87
Ocena prehranskih potreb
bull V akutni fazi 20-25 nebeljakovinskih kkalkgdan v anabolni fazi in podhranjeni 25 -30 kkalkgdan
bull Maščobe 03 gkg ttdan do 2 gkg ttdan (30 do 70)
bull Ogljikovi hidrati 2-5g kgdan (30 do 70)
bull Beljakovine povprečno 15 g kg tt dan (15 -20 )
bull Mikrohranila-dnevne priporočene potrebe individualno glede na obolenje
bull Opečenci več Cu Se in Zn
AA V PARENTERALNI PREHRANI
bull Povečana izguba AA
bull Neravnovesje med izgubo in porabo
bull Esencielne AA z dodatkom histidina ter arginina niso optimum
bull Nadomeščanje tirozina problem zaradi slabe topnostihellip
bull Acetil-tirozin je rešitev vendar ne pri KLB
bull Rešitev predstavlja dipeptid glicil-tirozin ki je dobro topen in idealno nadomešča večje potrebe po tirozinu pri KLB (AminoMel nephro)
PREHRANSKI DODATKI
Enteralni
bull Nepro Nepro HP Nepro LP Ensure Ensure Plus Advance Prosure Fresubinhellipenkrat na dan per os
bull Glutamin 5-10g na dan per os
bull Carenal 1 tableto po dializi
bull L-karnitin
Parenteralni
bull Aminomel Nephro aminokisline (500ml med HD)
bull Kabiven
bull Glamin 500ml
bull Dipeptiven 100ml
bull Soluvit N(vodotopni vitamini)
bull Vitalipid N(maščobotopni vitamini)
bull Addamel N(mikroelementi)
bull Omegaven (ribje oljehellip)
Component Renal Specific
ONS
Standard ONS
Protein Optimum Medium
Glycemic Index
(Carbohydrates) Low High
MUFA Omega-3
(FatsLipids) High Low
Electrolytes
Phosphorus
Potassium Sodium
Low High
Fluid volume Low High
Caloric density High Standard
Fiber High Low
Prebiotics scFOS Present None
CKD-specific vitamin
amp mineral profile Optimized None
Why Renal Specific ONS
Why Standard versus Renal Specific ONS
Nutrition Intervention in CKD Patients
bull Expert recommendations
KDOQI1 ESPEN2 EBPG3
Nutrition
Support
Individuals undergoing
maintenance dialysis
who are unable to
meet their protein and
energy requirements
with food intake for an
extended period of
time should receive
nutritional support
Special formula
products for HD
treatment can be
useful especially in
malnourished patients
who are not able to
increase their nutrient
intake
Oral nutritional
supplements should
be prescribed if
nutritional counseling
does not achieve an
increase in nutrient
intake to a level that
covers minimum
recommendations
Products
specifically
designed for
dialysis patients
should be
prescribed
1 NKF KDOQI Clinical practice guidelines for nutrition in chronic renal failure AJKD 2000 35S1-S140
2 Cano N et al Clin Nutr 2006 25295-310
3 Fouque D et al NDT 2007 22(suppl 2)ii45-ii87
Recomm-S
ESPEN KDOQI EBPG
Proteini (gkgdan) 12-14 10-12 11
Energija
(kCalkgdan)
35 lt60 g 35
gt60 g 30
30-35
gt50 intke lt1 gkgdan
Actual ntake 20-25 kCalkg 08-1 g proteinakg
Renal Specific Nutritional Therapy
Clinical studies have shown that renal-specific nutrition offers advantages over standard nutrition
bull Phosphorus levels were lower with the renal-specific nutrition than with the standard nutrition1
bull Less fluid and potassium in renal-specific nutrition offers advantages over standard nutrition2
1 Cockram DB et al J Ren Nutr 1998825-33
2 Williams RF Summers AM J Ren Nutr 200919183-188
PREHRANSKE ZAHTEVE DIALIZE
PRAKSA
ENERGIJA 35KCALKG TT NA DAN
PROTEINI 12GKG TT NA DAN
VNOS TEKOČINE 1000ML + IZLOČEN URIN
NATRIJ 2-3G NA DAN
KALIJ 2-3G NA DAN
FOSFOR 08-12GDAN
NKFKDOQI 2000 ADA 2002 WILKENS 2004
BIOIMPEDANCE PRINCIPLES
Phase angle
bull Phase angle is an indicator based on reactance and
resistance obtained from bioelectrical impedance
analysis (BIA)
bull PA depends on cell membrane integrity and on body cell
mass
bull Although its biological meaning is still not clear phase
angle appears to have an important prognostic role
bull Phase angle differs across categories of sex age BMI
and percentage fat bull Maria Cristina G Barbosa-Silva Aluiacutesio JD Barros Jack Wang Steven B Heymsfield and Richard
N Pierson Jr Am J Clin Nutr July 2005 vol 82 no 1 49-52
bull Satish Kumar1 Aswini Dutt1 Sandhya Hemraj2 Shankar Bhat1 and Bhat Manipadybhima Iran
J Basic Med Sci 2012 Nov-Dec 15(6) 1180ndash1184
PHASE ANGLE AND LEAN TISSUE
INDEX ARE SLIGHTLY HIGHER IN
HEMODIALYSIS THAN IN PERITONEAL
DIALYSIS GROUP OF PATIENTS
BKnap ZVeceric Haler JButurovic-Ponikvar
RPonikvar AF Bren
University Clinical Center Ljubljana
Department of Nephrology Slovenia
Ideal nutrition ndash CKD patients
bull Prevents musle loss
bull Prevent andor treat PEW
bull Correct metabolic derrangements
bull Decrease morbidity and mortlity
bull Improve QoL
bull Does not promote progression of CKD
bull Or ideally slow down progression of CKD
ZAKLJUČEK
bull Podhranjenost je pomembna in pogosto
ključna za preživetje
bull Sodobne metode detekcije in zdravljenja
podhranjenosti omogočajo zgodnejšo
nutricijsko intervencijo
bull Prehranski dodatki tako enteralni kot
parenteralni so pogosto nujna in včasih
edina možnost
Kaj je dobro vedetihelliphellip
bull LEDVIČNI BOLNIKI JEDO SLABO
bull V ZAČETNI FAZI KLB TERAPIJA Z OMEJEVANJEM VNOSA PROTEINOV LAHKO PRIPELJE DO MALNUTRICIJE IN KAHEKSIJE
bull POMEMBNA OCENA HRANJENOSTI IN PRAVOČASNA NUTRICIJSKA INTERVENCIJA V VSEH FAZAH KLB
bull USPEH ZDRAVLJENJA MALNUTRICIJE JE POVEZAN Z DOBRIM ZDRAVLJENJEM OSNOVNE LEDVIČNE BOLEZNI IN CELOSTNEGA ZDRAVLJENJA KLB
bull POLEG HRANE VELIKO PRISPEVAJO K KVALITETI ŽIVLJENJA TUDI PREHRANSKI DODATKI IN TELESNA VADBA
bull ANABOLNI AGENSI IN STIMULATORJI APETITA NA NIVOJU HIPOTALAMUSA SO OBET BLIŽNJE PRIHODNOSTI

VLOGA LEPTINA PRI KAHEKSIJI KLB
bull Zvišan pri KLB
bull Deluje podobno kot citokinski receptorji
tipa IL6(vnetje)
bull Preko receptorjev za melanocortin v
hipotalamusu deluje na apetit in
metabolizem
bull Antagonisti MC-R4 receptorja nov
terapevtski obet
VELIK POMEN PREHRANSKE
DIAGNOSTIKE ZA DIALIZNE PACIENTE
bull Klinična presoja pacienta in kvalitete
življenja oziroma uspeha zdravljenja
bull Biokemijavrednosti albuminov
prealbumina in vnosa proteinov (35gl
300mgl 1gkgdan)
bull Nadzor telesna teža BMI SGA
BCM(bioimpedanca) serumski albumin
kreatinin
SUBJEKTIVNA GLOBALNA
NUTRICIJSKA OCENA-SGA
SGA ocena prehranjenosti zajema
bull anamnezo (o spremembi telesne teže o
vnosu hrane simptomih s strani GIT
funkcionalne zmogljivosti) in
bull telesni pregled (atrofija mišic zmanjšanje
podkožne maščobe in pojav oteklin)
bull zlati standard ocene bolnika(Keith
Nutrition in Clinical Practice 2008)
Malnutrition Inflammation Score
(MIS)
bullFully quantitative
bullUses the 7 original SGA components
bullAdds 3 new components
ndashBody mass index
ndashSerum albumin
ndashSerum total iron binding capacity
PEM - PROTEINSKO
ENERGETSKA MALNUTRICIJA
bull PEM je pogost v KLB
bull Je povezan s povečano obolevnostjo in
umrljivostjo
bull 40 PEM na začetku nadomestnega
zdravljenja KOL
bull 10-70 HD pacientov
bull 18-51 CAPD pacientov
Nutritional RecommendationsDialysisStage 5 CKD
KDOQI1 ESPEN2 EBPG3
EnergyCalories lt 60 years 35
kcalkgd
60 years or obese
30-35 kcalkgd
35 kcalkgd 30-40 kcalkgd
Protein 12 gkgd
50 HBV
12-14 gkg
IBWd
11 gkgd
Sodium ― 18-25 gd 2000-3000
mgd
Fluid ― 1000 mL + urine
volume
―
Potassium ― 2000-2500 mgd 1950-2730
mgd
Phosphorus 800-1000 mgd
lt 17 mgkg IBW or
SBWd
800-1000 mgd 800-1000 mgd
Calcium 2 gd ― 2000 mgd
1 NKF KDOQI Clinical practice guidelines for nutrition in chronic renal failure AJKD 2000 35S1-S140
2 Cano N et al Clin Nutr 2006 25295-310
3 Fouque D et al NDT 2007 22(suppl 2)ii45-ii87
Ocena prehranskih potreb
bull V akutni fazi 20-25 nebeljakovinskih kkalkgdan v anabolni fazi in podhranjeni 25 -30 kkalkgdan
bull Maščobe 03 gkg ttdan do 2 gkg ttdan (30 do 70)
bull Ogljikovi hidrati 2-5g kgdan (30 do 70)
bull Beljakovine povprečno 15 g kg tt dan (15 -20 )
bull Mikrohranila-dnevne priporočene potrebe individualno glede na obolenje
bull Opečenci več Cu Se in Zn
AA V PARENTERALNI PREHRANI
bull Povečana izguba AA
bull Neravnovesje med izgubo in porabo
bull Esencielne AA z dodatkom histidina ter arginina niso optimum
bull Nadomeščanje tirozina problem zaradi slabe topnostihellip
bull Acetil-tirozin je rešitev vendar ne pri KLB
bull Rešitev predstavlja dipeptid glicil-tirozin ki je dobro topen in idealno nadomešča večje potrebe po tirozinu pri KLB (AminoMel nephro)
PREHRANSKI DODATKI
Enteralni
bull Nepro Nepro HP Nepro LP Ensure Ensure Plus Advance Prosure Fresubinhellipenkrat na dan per os
bull Glutamin 5-10g na dan per os
bull Carenal 1 tableto po dializi
bull L-karnitin
Parenteralni
bull Aminomel Nephro aminokisline (500ml med HD)
bull Kabiven
bull Glamin 500ml
bull Dipeptiven 100ml
bull Soluvit N(vodotopni vitamini)
bull Vitalipid N(maščobotopni vitamini)
bull Addamel N(mikroelementi)
bull Omegaven (ribje oljehellip)
Component Renal Specific
ONS
Standard ONS
Protein Optimum Medium
Glycemic Index
(Carbohydrates) Low High
MUFA Omega-3
(FatsLipids) High Low
Electrolytes
Phosphorus
Potassium Sodium
Low High
Fluid volume Low High
Caloric density High Standard
Fiber High Low
Prebiotics scFOS Present None
CKD-specific vitamin
amp mineral profile Optimized None
Why Renal Specific ONS
Why Standard versus Renal Specific ONS
Nutrition Intervention in CKD Patients
bull Expert recommendations
KDOQI1 ESPEN2 EBPG3
Nutrition
Support
Individuals undergoing
maintenance dialysis
who are unable to
meet their protein and
energy requirements
with food intake for an
extended period of
time should receive
nutritional support
Special formula
products for HD
treatment can be
useful especially in
malnourished patients
who are not able to
increase their nutrient
intake
Oral nutritional
supplements should
be prescribed if
nutritional counseling
does not achieve an
increase in nutrient
intake to a level that
covers minimum
recommendations
Products
specifically
designed for
dialysis patients
should be
prescribed
1 NKF KDOQI Clinical practice guidelines for nutrition in chronic renal failure AJKD 2000 35S1-S140
2 Cano N et al Clin Nutr 2006 25295-310
3 Fouque D et al NDT 2007 22(suppl 2)ii45-ii87
Recomm-S
ESPEN KDOQI EBPG
Proteini (gkgdan) 12-14 10-12 11
Energija
(kCalkgdan)
35 lt60 g 35
gt60 g 30
30-35
gt50 intke lt1 gkgdan
Actual ntake 20-25 kCalkg 08-1 g proteinakg
Renal Specific Nutritional Therapy
Clinical studies have shown that renal-specific nutrition offers advantages over standard nutrition
bull Phosphorus levels were lower with the renal-specific nutrition than with the standard nutrition1
bull Less fluid and potassium in renal-specific nutrition offers advantages over standard nutrition2
1 Cockram DB et al J Ren Nutr 1998825-33
2 Williams RF Summers AM J Ren Nutr 200919183-188
PREHRANSKE ZAHTEVE DIALIZE
PRAKSA
ENERGIJA 35KCALKG TT NA DAN
PROTEINI 12GKG TT NA DAN
VNOS TEKOČINE 1000ML + IZLOČEN URIN
NATRIJ 2-3G NA DAN
KALIJ 2-3G NA DAN
FOSFOR 08-12GDAN
NKFKDOQI 2000 ADA 2002 WILKENS 2004
BIOIMPEDANCE PRINCIPLES
Phase angle
bull Phase angle is an indicator based on reactance and
resistance obtained from bioelectrical impedance
analysis (BIA)
bull PA depends on cell membrane integrity and on body cell
mass
bull Although its biological meaning is still not clear phase
angle appears to have an important prognostic role
bull Phase angle differs across categories of sex age BMI
and percentage fat bull Maria Cristina G Barbosa-Silva Aluiacutesio JD Barros Jack Wang Steven B Heymsfield and Richard
N Pierson Jr Am J Clin Nutr July 2005 vol 82 no 1 49-52
bull Satish Kumar1 Aswini Dutt1 Sandhya Hemraj2 Shankar Bhat1 and Bhat Manipadybhima Iran
J Basic Med Sci 2012 Nov-Dec 15(6) 1180ndash1184
PHASE ANGLE AND LEAN TISSUE
INDEX ARE SLIGHTLY HIGHER IN
HEMODIALYSIS THAN IN PERITONEAL
DIALYSIS GROUP OF PATIENTS
BKnap ZVeceric Haler JButurovic-Ponikvar
RPonikvar AF Bren
University Clinical Center Ljubljana
Department of Nephrology Slovenia
Ideal nutrition ndash CKD patients
bull Prevents musle loss
bull Prevent andor treat PEW
bull Correct metabolic derrangements
bull Decrease morbidity and mortlity
bull Improve QoL
bull Does not promote progression of CKD
bull Or ideally slow down progression of CKD
ZAKLJUČEK
bull Podhranjenost je pomembna in pogosto
ključna za preživetje
bull Sodobne metode detekcije in zdravljenja
podhranjenosti omogočajo zgodnejšo
nutricijsko intervencijo
bull Prehranski dodatki tako enteralni kot
parenteralni so pogosto nujna in včasih
edina možnost
Kaj je dobro vedetihelliphellip
bull LEDVIČNI BOLNIKI JEDO SLABO
bull V ZAČETNI FAZI KLB TERAPIJA Z OMEJEVANJEM VNOSA PROTEINOV LAHKO PRIPELJE DO MALNUTRICIJE IN KAHEKSIJE
bull POMEMBNA OCENA HRANJENOSTI IN PRAVOČASNA NUTRICIJSKA INTERVENCIJA V VSEH FAZAH KLB
bull USPEH ZDRAVLJENJA MALNUTRICIJE JE POVEZAN Z DOBRIM ZDRAVLJENJEM OSNOVNE LEDVIČNE BOLEZNI IN CELOSTNEGA ZDRAVLJENJA KLB
bull POLEG HRANE VELIKO PRISPEVAJO K KVALITETI ŽIVLJENJA TUDI PREHRANSKI DODATKI IN TELESNA VADBA
bull ANABOLNI AGENSI IN STIMULATORJI APETITA NA NIVOJU HIPOTALAMUSA SO OBET BLIŽNJE PRIHODNOSTI

VELIK POMEN PREHRANSKE
DIAGNOSTIKE ZA DIALIZNE PACIENTE
bull Klinična presoja pacienta in kvalitete
življenja oziroma uspeha zdravljenja
bull Biokemijavrednosti albuminov
prealbumina in vnosa proteinov (35gl
300mgl 1gkgdan)
bull Nadzor telesna teža BMI SGA
BCM(bioimpedanca) serumski albumin
kreatinin
SUBJEKTIVNA GLOBALNA
NUTRICIJSKA OCENA-SGA
SGA ocena prehranjenosti zajema
bull anamnezo (o spremembi telesne teže o
vnosu hrane simptomih s strani GIT
funkcionalne zmogljivosti) in
bull telesni pregled (atrofija mišic zmanjšanje
podkožne maščobe in pojav oteklin)
bull zlati standard ocene bolnika(Keith
Nutrition in Clinical Practice 2008)
Malnutrition Inflammation Score
(MIS)
bullFully quantitative
bullUses the 7 original SGA components
bullAdds 3 new components
ndashBody mass index
ndashSerum albumin
ndashSerum total iron binding capacity
PEM - PROTEINSKO
ENERGETSKA MALNUTRICIJA
bull PEM je pogost v KLB
bull Je povezan s povečano obolevnostjo in
umrljivostjo
bull 40 PEM na začetku nadomestnega
zdravljenja KOL
bull 10-70 HD pacientov
bull 18-51 CAPD pacientov
Nutritional RecommendationsDialysisStage 5 CKD
KDOQI1 ESPEN2 EBPG3
EnergyCalories lt 60 years 35
kcalkgd
60 years or obese
30-35 kcalkgd
35 kcalkgd 30-40 kcalkgd
Protein 12 gkgd
50 HBV
12-14 gkg
IBWd
11 gkgd
Sodium ― 18-25 gd 2000-3000
mgd
Fluid ― 1000 mL + urine
volume
―
Potassium ― 2000-2500 mgd 1950-2730
mgd
Phosphorus 800-1000 mgd
lt 17 mgkg IBW or
SBWd
800-1000 mgd 800-1000 mgd
Calcium 2 gd ― 2000 mgd
1 NKF KDOQI Clinical practice guidelines for nutrition in chronic renal failure AJKD 2000 35S1-S140
2 Cano N et al Clin Nutr 2006 25295-310
3 Fouque D et al NDT 2007 22(suppl 2)ii45-ii87
Ocena prehranskih potreb
bull V akutni fazi 20-25 nebeljakovinskih kkalkgdan v anabolni fazi in podhranjeni 25 -30 kkalkgdan
bull Maščobe 03 gkg ttdan do 2 gkg ttdan (30 do 70)
bull Ogljikovi hidrati 2-5g kgdan (30 do 70)
bull Beljakovine povprečno 15 g kg tt dan (15 -20 )
bull Mikrohranila-dnevne priporočene potrebe individualno glede na obolenje
bull Opečenci več Cu Se in Zn
AA V PARENTERALNI PREHRANI
bull Povečana izguba AA
bull Neravnovesje med izgubo in porabo
bull Esencielne AA z dodatkom histidina ter arginina niso optimum
bull Nadomeščanje tirozina problem zaradi slabe topnostihellip
bull Acetil-tirozin je rešitev vendar ne pri KLB
bull Rešitev predstavlja dipeptid glicil-tirozin ki je dobro topen in idealno nadomešča večje potrebe po tirozinu pri KLB (AminoMel nephro)
PREHRANSKI DODATKI
Enteralni
bull Nepro Nepro HP Nepro LP Ensure Ensure Plus Advance Prosure Fresubinhellipenkrat na dan per os
bull Glutamin 5-10g na dan per os
bull Carenal 1 tableto po dializi
bull L-karnitin
Parenteralni
bull Aminomel Nephro aminokisline (500ml med HD)
bull Kabiven
bull Glamin 500ml
bull Dipeptiven 100ml
bull Soluvit N(vodotopni vitamini)
bull Vitalipid N(maščobotopni vitamini)
bull Addamel N(mikroelementi)
bull Omegaven (ribje oljehellip)
Component Renal Specific
ONS
Standard ONS
Protein Optimum Medium
Glycemic Index
(Carbohydrates) Low High
MUFA Omega-3
(FatsLipids) High Low
Electrolytes
Phosphorus
Potassium Sodium
Low High
Fluid volume Low High
Caloric density High Standard
Fiber High Low
Prebiotics scFOS Present None
CKD-specific vitamin
amp mineral profile Optimized None
Why Renal Specific ONS
Why Standard versus Renal Specific ONS
Nutrition Intervention in CKD Patients
bull Expert recommendations
KDOQI1 ESPEN2 EBPG3
Nutrition
Support
Individuals undergoing
maintenance dialysis
who are unable to
meet their protein and
energy requirements
with food intake for an
extended period of
time should receive
nutritional support
Special formula
products for HD
treatment can be
useful especially in
malnourished patients
who are not able to
increase their nutrient
intake
Oral nutritional
supplements should
be prescribed if
nutritional counseling
does not achieve an
increase in nutrient
intake to a level that
covers minimum
recommendations
Products
specifically
designed for
dialysis patients
should be
prescribed
1 NKF KDOQI Clinical practice guidelines for nutrition in chronic renal failure AJKD 2000 35S1-S140
2 Cano N et al Clin Nutr 2006 25295-310
3 Fouque D et al NDT 2007 22(suppl 2)ii45-ii87
Recomm-S
ESPEN KDOQI EBPG
Proteini (gkgdan) 12-14 10-12 11
Energija
(kCalkgdan)
35 lt60 g 35
gt60 g 30
30-35
gt50 intke lt1 gkgdan
Actual ntake 20-25 kCalkg 08-1 g proteinakg
Renal Specific Nutritional Therapy
Clinical studies have shown that renal-specific nutrition offers advantages over standard nutrition
bull Phosphorus levels were lower with the renal-specific nutrition than with the standard nutrition1
bull Less fluid and potassium in renal-specific nutrition offers advantages over standard nutrition2
1 Cockram DB et al J Ren Nutr 1998825-33
2 Williams RF Summers AM J Ren Nutr 200919183-188
PREHRANSKE ZAHTEVE DIALIZE
PRAKSA
ENERGIJA 35KCALKG TT NA DAN
PROTEINI 12GKG TT NA DAN
VNOS TEKOČINE 1000ML + IZLOČEN URIN
NATRIJ 2-3G NA DAN
KALIJ 2-3G NA DAN
FOSFOR 08-12GDAN
NKFKDOQI 2000 ADA 2002 WILKENS 2004
BIOIMPEDANCE PRINCIPLES
Phase angle
bull Phase angle is an indicator based on reactance and
resistance obtained from bioelectrical impedance
analysis (BIA)
bull PA depends on cell membrane integrity and on body cell
mass
bull Although its biological meaning is still not clear phase
angle appears to have an important prognostic role
bull Phase angle differs across categories of sex age BMI
and percentage fat bull Maria Cristina G Barbosa-Silva Aluiacutesio JD Barros Jack Wang Steven B Heymsfield and Richard
N Pierson Jr Am J Clin Nutr July 2005 vol 82 no 1 49-52
bull Satish Kumar1 Aswini Dutt1 Sandhya Hemraj2 Shankar Bhat1 and Bhat Manipadybhima Iran
J Basic Med Sci 2012 Nov-Dec 15(6) 1180ndash1184
PHASE ANGLE AND LEAN TISSUE
INDEX ARE SLIGHTLY HIGHER IN
HEMODIALYSIS THAN IN PERITONEAL
DIALYSIS GROUP OF PATIENTS
BKnap ZVeceric Haler JButurovic-Ponikvar
RPonikvar AF Bren
University Clinical Center Ljubljana
Department of Nephrology Slovenia
Ideal nutrition ndash CKD patients
bull Prevents musle loss
bull Prevent andor treat PEW
bull Correct metabolic derrangements
bull Decrease morbidity and mortlity
bull Improve QoL
bull Does not promote progression of CKD
bull Or ideally slow down progression of CKD
ZAKLJUČEK
bull Podhranjenost je pomembna in pogosto
ključna za preživetje
bull Sodobne metode detekcije in zdravljenja
podhranjenosti omogočajo zgodnejšo
nutricijsko intervencijo
bull Prehranski dodatki tako enteralni kot
parenteralni so pogosto nujna in včasih
edina možnost
Kaj je dobro vedetihelliphellip
bull LEDVIČNI BOLNIKI JEDO SLABO
bull V ZAČETNI FAZI KLB TERAPIJA Z OMEJEVANJEM VNOSA PROTEINOV LAHKO PRIPELJE DO MALNUTRICIJE IN KAHEKSIJE
bull POMEMBNA OCENA HRANJENOSTI IN PRAVOČASNA NUTRICIJSKA INTERVENCIJA V VSEH FAZAH KLB
bull USPEH ZDRAVLJENJA MALNUTRICIJE JE POVEZAN Z DOBRIM ZDRAVLJENJEM OSNOVNE LEDVIČNE BOLEZNI IN CELOSTNEGA ZDRAVLJENJA KLB
bull POLEG HRANE VELIKO PRISPEVAJO K KVALITETI ŽIVLJENJA TUDI PREHRANSKI DODATKI IN TELESNA VADBA
bull ANABOLNI AGENSI IN STIMULATORJI APETITA NA NIVOJU HIPOTALAMUSA SO OBET BLIŽNJE PRIHODNOSTI

SUBJEKTIVNA GLOBALNA
NUTRICIJSKA OCENA-SGA
SGA ocena prehranjenosti zajema
bull anamnezo (o spremembi telesne teže o
vnosu hrane simptomih s strani GIT
funkcionalne zmogljivosti) in
bull telesni pregled (atrofija mišic zmanjšanje
podkožne maščobe in pojav oteklin)
bull zlati standard ocene bolnika(Keith
Nutrition in Clinical Practice 2008)
Malnutrition Inflammation Score
(MIS)
bullFully quantitative
bullUses the 7 original SGA components
bullAdds 3 new components
ndashBody mass index
ndashSerum albumin
ndashSerum total iron binding capacity
PEM - PROTEINSKO
ENERGETSKA MALNUTRICIJA
bull PEM je pogost v KLB
bull Je povezan s povečano obolevnostjo in
umrljivostjo
bull 40 PEM na začetku nadomestnega
zdravljenja KOL
bull 10-70 HD pacientov
bull 18-51 CAPD pacientov
Nutritional RecommendationsDialysisStage 5 CKD
KDOQI1 ESPEN2 EBPG3
EnergyCalories lt 60 years 35
kcalkgd
60 years or obese
30-35 kcalkgd
35 kcalkgd 30-40 kcalkgd
Protein 12 gkgd
50 HBV
12-14 gkg
IBWd
11 gkgd
Sodium ― 18-25 gd 2000-3000
mgd
Fluid ― 1000 mL + urine
volume
―
Potassium ― 2000-2500 mgd 1950-2730
mgd
Phosphorus 800-1000 mgd
lt 17 mgkg IBW or
SBWd
800-1000 mgd 800-1000 mgd
Calcium 2 gd ― 2000 mgd
1 NKF KDOQI Clinical practice guidelines for nutrition in chronic renal failure AJKD 2000 35S1-S140
2 Cano N et al Clin Nutr 2006 25295-310
3 Fouque D et al NDT 2007 22(suppl 2)ii45-ii87
Ocena prehranskih potreb
bull V akutni fazi 20-25 nebeljakovinskih kkalkgdan v anabolni fazi in podhranjeni 25 -30 kkalkgdan
bull Maščobe 03 gkg ttdan do 2 gkg ttdan (30 do 70)
bull Ogljikovi hidrati 2-5g kgdan (30 do 70)
bull Beljakovine povprečno 15 g kg tt dan (15 -20 )
bull Mikrohranila-dnevne priporočene potrebe individualno glede na obolenje
bull Opečenci več Cu Se in Zn
AA V PARENTERALNI PREHRANI
bull Povečana izguba AA
bull Neravnovesje med izgubo in porabo
bull Esencielne AA z dodatkom histidina ter arginina niso optimum
bull Nadomeščanje tirozina problem zaradi slabe topnostihellip
bull Acetil-tirozin je rešitev vendar ne pri KLB
bull Rešitev predstavlja dipeptid glicil-tirozin ki je dobro topen in idealno nadomešča večje potrebe po tirozinu pri KLB (AminoMel nephro)
PREHRANSKI DODATKI
Enteralni
bull Nepro Nepro HP Nepro LP Ensure Ensure Plus Advance Prosure Fresubinhellipenkrat na dan per os
bull Glutamin 5-10g na dan per os
bull Carenal 1 tableto po dializi
bull L-karnitin
Parenteralni
bull Aminomel Nephro aminokisline (500ml med HD)
bull Kabiven
bull Glamin 500ml
bull Dipeptiven 100ml
bull Soluvit N(vodotopni vitamini)
bull Vitalipid N(maščobotopni vitamini)
bull Addamel N(mikroelementi)
bull Omegaven (ribje oljehellip)
Component Renal Specific
ONS
Standard ONS
Protein Optimum Medium
Glycemic Index
(Carbohydrates) Low High
MUFA Omega-3
(FatsLipids) High Low
Electrolytes
Phosphorus
Potassium Sodium
Low High
Fluid volume Low High
Caloric density High Standard
Fiber High Low
Prebiotics scFOS Present None
CKD-specific vitamin
amp mineral profile Optimized None
Why Renal Specific ONS
Why Standard versus Renal Specific ONS
Nutrition Intervention in CKD Patients
bull Expert recommendations
KDOQI1 ESPEN2 EBPG3
Nutrition
Support
Individuals undergoing
maintenance dialysis
who are unable to
meet their protein and
energy requirements
with food intake for an
extended period of
time should receive
nutritional support
Special formula
products for HD
treatment can be
useful especially in
malnourished patients
who are not able to
increase their nutrient
intake
Oral nutritional
supplements should
be prescribed if
nutritional counseling
does not achieve an
increase in nutrient
intake to a level that
covers minimum
recommendations
Products
specifically
designed for
dialysis patients
should be
prescribed
1 NKF KDOQI Clinical practice guidelines for nutrition in chronic renal failure AJKD 2000 35S1-S140
2 Cano N et al Clin Nutr 2006 25295-310
3 Fouque D et al NDT 2007 22(suppl 2)ii45-ii87
Recomm-S
ESPEN KDOQI EBPG
Proteini (gkgdan) 12-14 10-12 11
Energija
(kCalkgdan)
35 lt60 g 35
gt60 g 30
30-35
gt50 intke lt1 gkgdan
Actual ntake 20-25 kCalkg 08-1 g proteinakg
Renal Specific Nutritional Therapy
Clinical studies have shown that renal-specific nutrition offers advantages over standard nutrition
bull Phosphorus levels were lower with the renal-specific nutrition than with the standard nutrition1
bull Less fluid and potassium in renal-specific nutrition offers advantages over standard nutrition2
1 Cockram DB et al J Ren Nutr 1998825-33
2 Williams RF Summers AM J Ren Nutr 200919183-188
PREHRANSKE ZAHTEVE DIALIZE
PRAKSA
ENERGIJA 35KCALKG TT NA DAN
PROTEINI 12GKG TT NA DAN
VNOS TEKOČINE 1000ML + IZLOČEN URIN
NATRIJ 2-3G NA DAN
KALIJ 2-3G NA DAN
FOSFOR 08-12GDAN
NKFKDOQI 2000 ADA 2002 WILKENS 2004
BIOIMPEDANCE PRINCIPLES
Phase angle
bull Phase angle is an indicator based on reactance and
resistance obtained from bioelectrical impedance
analysis (BIA)
bull PA depends on cell membrane integrity and on body cell
mass
bull Although its biological meaning is still not clear phase
angle appears to have an important prognostic role
bull Phase angle differs across categories of sex age BMI
and percentage fat bull Maria Cristina G Barbosa-Silva Aluiacutesio JD Barros Jack Wang Steven B Heymsfield and Richard
N Pierson Jr Am J Clin Nutr July 2005 vol 82 no 1 49-52
bull Satish Kumar1 Aswini Dutt1 Sandhya Hemraj2 Shankar Bhat1 and Bhat Manipadybhima Iran
J Basic Med Sci 2012 Nov-Dec 15(6) 1180ndash1184
PHASE ANGLE AND LEAN TISSUE
INDEX ARE SLIGHTLY HIGHER IN
HEMODIALYSIS THAN IN PERITONEAL
DIALYSIS GROUP OF PATIENTS
BKnap ZVeceric Haler JButurovic-Ponikvar
RPonikvar AF Bren
University Clinical Center Ljubljana
Department of Nephrology Slovenia
Ideal nutrition ndash CKD patients
bull Prevents musle loss
bull Prevent andor treat PEW
bull Correct metabolic derrangements
bull Decrease morbidity and mortlity
bull Improve QoL
bull Does not promote progression of CKD
bull Or ideally slow down progression of CKD
ZAKLJUČEK
bull Podhranjenost je pomembna in pogosto
ključna za preživetje
bull Sodobne metode detekcije in zdravljenja
podhranjenosti omogočajo zgodnejšo
nutricijsko intervencijo
bull Prehranski dodatki tako enteralni kot
parenteralni so pogosto nujna in včasih
edina možnost
Kaj je dobro vedetihelliphellip
bull LEDVIČNI BOLNIKI JEDO SLABO
bull V ZAČETNI FAZI KLB TERAPIJA Z OMEJEVANJEM VNOSA PROTEINOV LAHKO PRIPELJE DO MALNUTRICIJE IN KAHEKSIJE
bull POMEMBNA OCENA HRANJENOSTI IN PRAVOČASNA NUTRICIJSKA INTERVENCIJA V VSEH FAZAH KLB
bull USPEH ZDRAVLJENJA MALNUTRICIJE JE POVEZAN Z DOBRIM ZDRAVLJENJEM OSNOVNE LEDVIČNE BOLEZNI IN CELOSTNEGA ZDRAVLJENJA KLB
bull POLEG HRANE VELIKO PRISPEVAJO K KVALITETI ŽIVLJENJA TUDI PREHRANSKI DODATKI IN TELESNA VADBA
bull ANABOLNI AGENSI IN STIMULATORJI APETITA NA NIVOJU HIPOTALAMUSA SO OBET BLIŽNJE PRIHODNOSTI
Malnutrition Inflammation Score
(MIS)
bullFully quantitative
bullUses the 7 original SGA components
bullAdds 3 new components
ndashBody mass index
ndashSerum albumin
ndashSerum total iron binding capacity
PEM - PROTEINSKO
ENERGETSKA MALNUTRICIJA
bull PEM je pogost v KLB
bull Je povezan s povečano obolevnostjo in
umrljivostjo
bull 40 PEM na začetku nadomestnega
zdravljenja KOL
bull 10-70 HD pacientov
bull 18-51 CAPD pacientov
Nutritional RecommendationsDialysisStage 5 CKD
KDOQI1 ESPEN2 EBPG3
EnergyCalories lt 60 years 35
kcalkgd
60 years or obese
30-35 kcalkgd
35 kcalkgd 30-40 kcalkgd
Protein 12 gkgd
50 HBV
12-14 gkg
IBWd
11 gkgd
Sodium ― 18-25 gd 2000-3000
mgd
Fluid ― 1000 mL + urine
volume
―
Potassium ― 2000-2500 mgd 1950-2730
mgd
Phosphorus 800-1000 mgd
lt 17 mgkg IBW or
SBWd
800-1000 mgd 800-1000 mgd
Calcium 2 gd ― 2000 mgd
1 NKF KDOQI Clinical practice guidelines for nutrition in chronic renal failure AJKD 2000 35S1-S140
2 Cano N et al Clin Nutr 2006 25295-310
3 Fouque D et al NDT 2007 22(suppl 2)ii45-ii87
Ocena prehranskih potreb
bull V akutni fazi 20-25 nebeljakovinskih kkalkgdan v anabolni fazi in podhranjeni 25 -30 kkalkgdan
bull Maščobe 03 gkg ttdan do 2 gkg ttdan (30 do 70)
bull Ogljikovi hidrati 2-5g kgdan (30 do 70)
bull Beljakovine povprečno 15 g kg tt dan (15 -20 )
bull Mikrohranila-dnevne priporočene potrebe individualno glede na obolenje
bull Opečenci več Cu Se in Zn
AA V PARENTERALNI PREHRANI
bull Povečana izguba AA
bull Neravnovesje med izgubo in porabo
bull Esencielne AA z dodatkom histidina ter arginina niso optimum
bull Nadomeščanje tirozina problem zaradi slabe topnostihellip
bull Acetil-tirozin je rešitev vendar ne pri KLB
bull Rešitev predstavlja dipeptid glicil-tirozin ki je dobro topen in idealno nadomešča večje potrebe po tirozinu pri KLB (AminoMel nephro)
PREHRANSKI DODATKI
Enteralni
bull Nepro Nepro HP Nepro LP Ensure Ensure Plus Advance Prosure Fresubinhellipenkrat na dan per os
bull Glutamin 5-10g na dan per os
bull Carenal 1 tableto po dializi
bull L-karnitin
Parenteralni
bull Aminomel Nephro aminokisline (500ml med HD)
bull Kabiven
bull Glamin 500ml
bull Dipeptiven 100ml
bull Soluvit N(vodotopni vitamini)
bull Vitalipid N(maščobotopni vitamini)
bull Addamel N(mikroelementi)
bull Omegaven (ribje oljehellip)
Component Renal Specific
ONS
Standard ONS
Protein Optimum Medium
Glycemic Index
(Carbohydrates) Low High
MUFA Omega-3
(FatsLipids) High Low
Electrolytes
Phosphorus
Potassium Sodium
Low High
Fluid volume Low High
Caloric density High Standard
Fiber High Low
Prebiotics scFOS Present None
CKD-specific vitamin
amp mineral profile Optimized None
Why Renal Specific ONS
Why Standard versus Renal Specific ONS
Nutrition Intervention in CKD Patients
bull Expert recommendations
KDOQI1 ESPEN2 EBPG3
Nutrition
Support
Individuals undergoing
maintenance dialysis
who are unable to
meet their protein and
energy requirements
with food intake for an
extended period of
time should receive
nutritional support
Special formula
products for HD
treatment can be
useful especially in
malnourished patients
who are not able to
increase their nutrient
intake
Oral nutritional
supplements should
be prescribed if
nutritional counseling
does not achieve an
increase in nutrient
intake to a level that
covers minimum
recommendations
Products
specifically
designed for
dialysis patients
should be
prescribed
1 NKF KDOQI Clinical practice guidelines for nutrition in chronic renal failure AJKD 2000 35S1-S140
2 Cano N et al Clin Nutr 2006 25295-310
3 Fouque D et al NDT 2007 22(suppl 2)ii45-ii87
Recomm-S
ESPEN KDOQI EBPG
Proteini (gkgdan) 12-14 10-12 11
Energija
(kCalkgdan)
35 lt60 g 35
gt60 g 30
30-35
gt50 intke lt1 gkgdan
Actual ntake 20-25 kCalkg 08-1 g proteinakg
Renal Specific Nutritional Therapy
Clinical studies have shown that renal-specific nutrition offers advantages over standard nutrition
bull Phosphorus levels were lower with the renal-specific nutrition than with the standard nutrition1
bull Less fluid and potassium in renal-specific nutrition offers advantages over standard nutrition2
1 Cockram DB et al J Ren Nutr 1998825-33
2 Williams RF Summers AM J Ren Nutr 200919183-188
PREHRANSKE ZAHTEVE DIALIZE
PRAKSA
ENERGIJA 35KCALKG TT NA DAN
PROTEINI 12GKG TT NA DAN
VNOS TEKOČINE 1000ML + IZLOČEN URIN
NATRIJ 2-3G NA DAN
KALIJ 2-3G NA DAN
FOSFOR 08-12GDAN
NKFKDOQI 2000 ADA 2002 WILKENS 2004
BIOIMPEDANCE PRINCIPLES
Phase angle
bull Phase angle is an indicator based on reactance and
resistance obtained from bioelectrical impedance
analysis (BIA)
bull PA depends on cell membrane integrity and on body cell
mass
bull Although its biological meaning is still not clear phase
angle appears to have an important prognostic role
bull Phase angle differs across categories of sex age BMI
and percentage fat bull Maria Cristina G Barbosa-Silva Aluiacutesio JD Barros Jack Wang Steven B Heymsfield and Richard
N Pierson Jr Am J Clin Nutr July 2005 vol 82 no 1 49-52
bull Satish Kumar1 Aswini Dutt1 Sandhya Hemraj2 Shankar Bhat1 and Bhat Manipadybhima Iran
J Basic Med Sci 2012 Nov-Dec 15(6) 1180ndash1184
PHASE ANGLE AND LEAN TISSUE
INDEX ARE SLIGHTLY HIGHER IN
HEMODIALYSIS THAN IN PERITONEAL
DIALYSIS GROUP OF PATIENTS
BKnap ZVeceric Haler JButurovic-Ponikvar
RPonikvar AF Bren
University Clinical Center Ljubljana
Department of Nephrology Slovenia
Ideal nutrition ndash CKD patients
bull Prevents musle loss
bull Prevent andor treat PEW
bull Correct metabolic derrangements
bull Decrease morbidity and mortlity
bull Improve QoL
bull Does not promote progression of CKD
bull Or ideally slow down progression of CKD
ZAKLJUČEK
bull Podhranjenost je pomembna in pogosto
ključna za preživetje
bull Sodobne metode detekcije in zdravljenja
podhranjenosti omogočajo zgodnejšo
nutricijsko intervencijo
bull Prehranski dodatki tako enteralni kot
parenteralni so pogosto nujna in včasih
edina možnost
Kaj je dobro vedetihelliphellip
bull LEDVIČNI BOLNIKI JEDO SLABO
bull V ZAČETNI FAZI KLB TERAPIJA Z OMEJEVANJEM VNOSA PROTEINOV LAHKO PRIPELJE DO MALNUTRICIJE IN KAHEKSIJE
bull POMEMBNA OCENA HRANJENOSTI IN PRAVOČASNA NUTRICIJSKA INTERVENCIJA V VSEH FAZAH KLB
bull USPEH ZDRAVLJENJA MALNUTRICIJE JE POVEZAN Z DOBRIM ZDRAVLJENJEM OSNOVNE LEDVIČNE BOLEZNI IN CELOSTNEGA ZDRAVLJENJA KLB
bull POLEG HRANE VELIKO PRISPEVAJO K KVALITETI ŽIVLJENJA TUDI PREHRANSKI DODATKI IN TELESNA VADBA
bull ANABOLNI AGENSI IN STIMULATORJI APETITA NA NIVOJU HIPOTALAMUSA SO OBET BLIŽNJE PRIHODNOSTI

PEM - PROTEINSKO
ENERGETSKA MALNUTRICIJA
bull PEM je pogost v KLB
bull Je povezan s povečano obolevnostjo in
umrljivostjo
bull 40 PEM na začetku nadomestnega
zdravljenja KOL
bull 10-70 HD pacientov
bull 18-51 CAPD pacientov
Nutritional RecommendationsDialysisStage 5 CKD
KDOQI1 ESPEN2 EBPG3
EnergyCalories lt 60 years 35
kcalkgd
60 years or obese
30-35 kcalkgd
35 kcalkgd 30-40 kcalkgd
Protein 12 gkgd
50 HBV
12-14 gkg
IBWd
11 gkgd
Sodium ― 18-25 gd 2000-3000
mgd
Fluid ― 1000 mL + urine
volume
―
Potassium ― 2000-2500 mgd 1950-2730
mgd
Phosphorus 800-1000 mgd
lt 17 mgkg IBW or
SBWd
800-1000 mgd 800-1000 mgd
Calcium 2 gd ― 2000 mgd
1 NKF KDOQI Clinical practice guidelines for nutrition in chronic renal failure AJKD 2000 35S1-S140
2 Cano N et al Clin Nutr 2006 25295-310
3 Fouque D et al NDT 2007 22(suppl 2)ii45-ii87
Ocena prehranskih potreb
bull V akutni fazi 20-25 nebeljakovinskih kkalkgdan v anabolni fazi in podhranjeni 25 -30 kkalkgdan
bull Maščobe 03 gkg ttdan do 2 gkg ttdan (30 do 70)
bull Ogljikovi hidrati 2-5g kgdan (30 do 70)
bull Beljakovine povprečno 15 g kg tt dan (15 -20 )
bull Mikrohranila-dnevne priporočene potrebe individualno glede na obolenje
bull Opečenci več Cu Se in Zn
AA V PARENTERALNI PREHRANI
bull Povečana izguba AA
bull Neravnovesje med izgubo in porabo
bull Esencielne AA z dodatkom histidina ter arginina niso optimum
bull Nadomeščanje tirozina problem zaradi slabe topnostihellip
bull Acetil-tirozin je rešitev vendar ne pri KLB
bull Rešitev predstavlja dipeptid glicil-tirozin ki je dobro topen in idealno nadomešča večje potrebe po tirozinu pri KLB (AminoMel nephro)
PREHRANSKI DODATKI
Enteralni
bull Nepro Nepro HP Nepro LP Ensure Ensure Plus Advance Prosure Fresubinhellipenkrat na dan per os
bull Glutamin 5-10g na dan per os
bull Carenal 1 tableto po dializi
bull L-karnitin
Parenteralni
bull Aminomel Nephro aminokisline (500ml med HD)
bull Kabiven
bull Glamin 500ml
bull Dipeptiven 100ml
bull Soluvit N(vodotopni vitamini)
bull Vitalipid N(maščobotopni vitamini)
bull Addamel N(mikroelementi)
bull Omegaven (ribje oljehellip)
Component Renal Specific
ONS
Standard ONS
Protein Optimum Medium
Glycemic Index
(Carbohydrates) Low High
MUFA Omega-3
(FatsLipids) High Low
Electrolytes
Phosphorus
Potassium Sodium
Low High
Fluid volume Low High
Caloric density High Standard
Fiber High Low
Prebiotics scFOS Present None
CKD-specific vitamin
amp mineral profile Optimized None
Why Renal Specific ONS
Why Standard versus Renal Specific ONS
Nutrition Intervention in CKD Patients
bull Expert recommendations
KDOQI1 ESPEN2 EBPG3
Nutrition
Support
Individuals undergoing
maintenance dialysis
who are unable to
meet their protein and
energy requirements
with food intake for an
extended period of
time should receive
nutritional support
Special formula
products for HD
treatment can be
useful especially in
malnourished patients
who are not able to
increase their nutrient
intake
Oral nutritional
supplements should
be prescribed if
nutritional counseling
does not achieve an
increase in nutrient
intake to a level that
covers minimum
recommendations
Products
specifically
designed for
dialysis patients
should be
prescribed
1 NKF KDOQI Clinical practice guidelines for nutrition in chronic renal failure AJKD 2000 35S1-S140
2 Cano N et al Clin Nutr 2006 25295-310
3 Fouque D et al NDT 2007 22(suppl 2)ii45-ii87
Recomm-S
ESPEN KDOQI EBPG
Proteini (gkgdan) 12-14 10-12 11
Energija
(kCalkgdan)
35 lt60 g 35
gt60 g 30
30-35
gt50 intke lt1 gkgdan
Actual ntake 20-25 kCalkg 08-1 g proteinakg
Renal Specific Nutritional Therapy
Clinical studies have shown that renal-specific nutrition offers advantages over standard nutrition
bull Phosphorus levels were lower with the renal-specific nutrition than with the standard nutrition1
bull Less fluid and potassium in renal-specific nutrition offers advantages over standard nutrition2
1 Cockram DB et al J Ren Nutr 1998825-33
2 Williams RF Summers AM J Ren Nutr 200919183-188
PREHRANSKE ZAHTEVE DIALIZE
PRAKSA
ENERGIJA 35KCALKG TT NA DAN
PROTEINI 12GKG TT NA DAN
VNOS TEKOČINE 1000ML + IZLOČEN URIN
NATRIJ 2-3G NA DAN
KALIJ 2-3G NA DAN
FOSFOR 08-12GDAN
NKFKDOQI 2000 ADA 2002 WILKENS 2004
BIOIMPEDANCE PRINCIPLES
Phase angle
bull Phase angle is an indicator based on reactance and
resistance obtained from bioelectrical impedance
analysis (BIA)
bull PA depends on cell membrane integrity and on body cell
mass
bull Although its biological meaning is still not clear phase
angle appears to have an important prognostic role
bull Phase angle differs across categories of sex age BMI
and percentage fat bull Maria Cristina G Barbosa-Silva Aluiacutesio JD Barros Jack Wang Steven B Heymsfield and Richard
N Pierson Jr Am J Clin Nutr July 2005 vol 82 no 1 49-52
bull Satish Kumar1 Aswini Dutt1 Sandhya Hemraj2 Shankar Bhat1 and Bhat Manipadybhima Iran
J Basic Med Sci 2012 Nov-Dec 15(6) 1180ndash1184
PHASE ANGLE AND LEAN TISSUE
INDEX ARE SLIGHTLY HIGHER IN
HEMODIALYSIS THAN IN PERITONEAL
DIALYSIS GROUP OF PATIENTS
BKnap ZVeceric Haler JButurovic-Ponikvar
RPonikvar AF Bren
University Clinical Center Ljubljana
Department of Nephrology Slovenia
Ideal nutrition ndash CKD patients
bull Prevents musle loss
bull Prevent andor treat PEW
bull Correct metabolic derrangements
bull Decrease morbidity and mortlity
bull Improve QoL
bull Does not promote progression of CKD
bull Or ideally slow down progression of CKD
ZAKLJUČEK
bull Podhranjenost je pomembna in pogosto
ključna za preživetje
bull Sodobne metode detekcije in zdravljenja
podhranjenosti omogočajo zgodnejšo
nutricijsko intervencijo
bull Prehranski dodatki tako enteralni kot
parenteralni so pogosto nujna in včasih
edina možnost
Kaj je dobro vedetihelliphellip
bull LEDVIČNI BOLNIKI JEDO SLABO
bull V ZAČETNI FAZI KLB TERAPIJA Z OMEJEVANJEM VNOSA PROTEINOV LAHKO PRIPELJE DO MALNUTRICIJE IN KAHEKSIJE
bull POMEMBNA OCENA HRANJENOSTI IN PRAVOČASNA NUTRICIJSKA INTERVENCIJA V VSEH FAZAH KLB
bull USPEH ZDRAVLJENJA MALNUTRICIJE JE POVEZAN Z DOBRIM ZDRAVLJENJEM OSNOVNE LEDVIČNE BOLEZNI IN CELOSTNEGA ZDRAVLJENJA KLB
bull POLEG HRANE VELIKO PRISPEVAJO K KVALITETI ŽIVLJENJA TUDI PREHRANSKI DODATKI IN TELESNA VADBA
bull ANABOLNI AGENSI IN STIMULATORJI APETITA NA NIVOJU HIPOTALAMUSA SO OBET BLIŽNJE PRIHODNOSTI
Nutritional RecommendationsDialysisStage 5 CKD
KDOQI1 ESPEN2 EBPG3
EnergyCalories lt 60 years 35
kcalkgd
60 years or obese
30-35 kcalkgd
35 kcalkgd 30-40 kcalkgd
Protein 12 gkgd
50 HBV
12-14 gkg
IBWd
11 gkgd
Sodium ― 18-25 gd 2000-3000
mgd
Fluid ― 1000 mL + urine
volume
―
Potassium ― 2000-2500 mgd 1950-2730
mgd
Phosphorus 800-1000 mgd
lt 17 mgkg IBW or
SBWd
800-1000 mgd 800-1000 mgd
Calcium 2 gd ― 2000 mgd
1 NKF KDOQI Clinical practice guidelines for nutrition in chronic renal failure AJKD 2000 35S1-S140
2 Cano N et al Clin Nutr 2006 25295-310
3 Fouque D et al NDT 2007 22(suppl 2)ii45-ii87
Ocena prehranskih potreb
bull V akutni fazi 20-25 nebeljakovinskih kkalkgdan v anabolni fazi in podhranjeni 25 -30 kkalkgdan
bull Maščobe 03 gkg ttdan do 2 gkg ttdan (30 do 70)
bull Ogljikovi hidrati 2-5g kgdan (30 do 70)
bull Beljakovine povprečno 15 g kg tt dan (15 -20 )
bull Mikrohranila-dnevne priporočene potrebe individualno glede na obolenje
bull Opečenci več Cu Se in Zn
AA V PARENTERALNI PREHRANI
bull Povečana izguba AA
bull Neravnovesje med izgubo in porabo
bull Esencielne AA z dodatkom histidina ter arginina niso optimum
bull Nadomeščanje tirozina problem zaradi slabe topnostihellip
bull Acetil-tirozin je rešitev vendar ne pri KLB
bull Rešitev predstavlja dipeptid glicil-tirozin ki je dobro topen in idealno nadomešča večje potrebe po tirozinu pri KLB (AminoMel nephro)
PREHRANSKI DODATKI
Enteralni
bull Nepro Nepro HP Nepro LP Ensure Ensure Plus Advance Prosure Fresubinhellipenkrat na dan per os
bull Glutamin 5-10g na dan per os
bull Carenal 1 tableto po dializi
bull L-karnitin
Parenteralni
bull Aminomel Nephro aminokisline (500ml med HD)
bull Kabiven
bull Glamin 500ml
bull Dipeptiven 100ml
bull Soluvit N(vodotopni vitamini)
bull Vitalipid N(maščobotopni vitamini)
bull Addamel N(mikroelementi)
bull Omegaven (ribje oljehellip)
Component Renal Specific
ONS
Standard ONS
Protein Optimum Medium
Glycemic Index
(Carbohydrates) Low High
MUFA Omega-3
(FatsLipids) High Low
Electrolytes
Phosphorus
Potassium Sodium
Low High
Fluid volume Low High
Caloric density High Standard
Fiber High Low
Prebiotics scFOS Present None
CKD-specific vitamin
amp mineral profile Optimized None
Why Renal Specific ONS
Why Standard versus Renal Specific ONS
Nutrition Intervention in CKD Patients
bull Expert recommendations
KDOQI1 ESPEN2 EBPG3
Nutrition
Support
Individuals undergoing
maintenance dialysis
who are unable to
meet their protein and
energy requirements
with food intake for an
extended period of
time should receive
nutritional support
Special formula
products for HD
treatment can be
useful especially in
malnourished patients
who are not able to
increase their nutrient
intake
Oral nutritional
supplements should
be prescribed if
nutritional counseling
does not achieve an
increase in nutrient
intake to a level that
covers minimum
recommendations
Products
specifically
designed for
dialysis patients
should be
prescribed
1 NKF KDOQI Clinical practice guidelines for nutrition in chronic renal failure AJKD 2000 35S1-S140
2 Cano N et al Clin Nutr 2006 25295-310
3 Fouque D et al NDT 2007 22(suppl 2)ii45-ii87
Recomm-S
ESPEN KDOQI EBPG
Proteini (gkgdan) 12-14 10-12 11
Energija
(kCalkgdan)
35 lt60 g 35
gt60 g 30
30-35
gt50 intke lt1 gkgdan
Actual ntake 20-25 kCalkg 08-1 g proteinakg
Renal Specific Nutritional Therapy
Clinical studies have shown that renal-specific nutrition offers advantages over standard nutrition
bull Phosphorus levels were lower with the renal-specific nutrition than with the standard nutrition1
bull Less fluid and potassium in renal-specific nutrition offers advantages over standard nutrition2
1 Cockram DB et al J Ren Nutr 1998825-33
2 Williams RF Summers AM J Ren Nutr 200919183-188
PREHRANSKE ZAHTEVE DIALIZE
PRAKSA
ENERGIJA 35KCALKG TT NA DAN
PROTEINI 12GKG TT NA DAN
VNOS TEKOČINE 1000ML + IZLOČEN URIN
NATRIJ 2-3G NA DAN
KALIJ 2-3G NA DAN
FOSFOR 08-12GDAN
NKFKDOQI 2000 ADA 2002 WILKENS 2004
BIOIMPEDANCE PRINCIPLES
Phase angle
bull Phase angle is an indicator based on reactance and
resistance obtained from bioelectrical impedance
analysis (BIA)
bull PA depends on cell membrane integrity and on body cell
mass
bull Although its biological meaning is still not clear phase
angle appears to have an important prognostic role
bull Phase angle differs across categories of sex age BMI
and percentage fat bull Maria Cristina G Barbosa-Silva Aluiacutesio JD Barros Jack Wang Steven B Heymsfield and Richard
N Pierson Jr Am J Clin Nutr July 2005 vol 82 no 1 49-52
bull Satish Kumar1 Aswini Dutt1 Sandhya Hemraj2 Shankar Bhat1 and Bhat Manipadybhima Iran
J Basic Med Sci 2012 Nov-Dec 15(6) 1180ndash1184
PHASE ANGLE AND LEAN TISSUE
INDEX ARE SLIGHTLY HIGHER IN
HEMODIALYSIS THAN IN PERITONEAL
DIALYSIS GROUP OF PATIENTS
BKnap ZVeceric Haler JButurovic-Ponikvar
RPonikvar AF Bren
University Clinical Center Ljubljana
Department of Nephrology Slovenia
Ideal nutrition ndash CKD patients
bull Prevents musle loss
bull Prevent andor treat PEW
bull Correct metabolic derrangements
bull Decrease morbidity and mortlity
bull Improve QoL
bull Does not promote progression of CKD
bull Or ideally slow down progression of CKD
ZAKLJUČEK
bull Podhranjenost je pomembna in pogosto
ključna za preživetje
bull Sodobne metode detekcije in zdravljenja
podhranjenosti omogočajo zgodnejšo
nutricijsko intervencijo
bull Prehranski dodatki tako enteralni kot
parenteralni so pogosto nujna in včasih
edina možnost
Kaj je dobro vedetihelliphellip
bull LEDVIČNI BOLNIKI JEDO SLABO
bull V ZAČETNI FAZI KLB TERAPIJA Z OMEJEVANJEM VNOSA PROTEINOV LAHKO PRIPELJE DO MALNUTRICIJE IN KAHEKSIJE
bull POMEMBNA OCENA HRANJENOSTI IN PRAVOČASNA NUTRICIJSKA INTERVENCIJA V VSEH FAZAH KLB
bull USPEH ZDRAVLJENJA MALNUTRICIJE JE POVEZAN Z DOBRIM ZDRAVLJENJEM OSNOVNE LEDVIČNE BOLEZNI IN CELOSTNEGA ZDRAVLJENJA KLB
bull POLEG HRANE VELIKO PRISPEVAJO K KVALITETI ŽIVLJENJA TUDI PREHRANSKI DODATKI IN TELESNA VADBA
bull ANABOLNI AGENSI IN STIMULATORJI APETITA NA NIVOJU HIPOTALAMUSA SO OBET BLIŽNJE PRIHODNOSTI

Ocena prehranskih potreb
bull V akutni fazi 20-25 nebeljakovinskih kkalkgdan v anabolni fazi in podhranjeni 25 -30 kkalkgdan
bull Maščobe 03 gkg ttdan do 2 gkg ttdan (30 do 70)
bull Ogljikovi hidrati 2-5g kgdan (30 do 70)
bull Beljakovine povprečno 15 g kg tt dan (15 -20 )
bull Mikrohranila-dnevne priporočene potrebe individualno glede na obolenje
bull Opečenci več Cu Se in Zn
AA V PARENTERALNI PREHRANI
bull Povečana izguba AA
bull Neravnovesje med izgubo in porabo
bull Esencielne AA z dodatkom histidina ter arginina niso optimum
bull Nadomeščanje tirozina problem zaradi slabe topnostihellip
bull Acetil-tirozin je rešitev vendar ne pri KLB
bull Rešitev predstavlja dipeptid glicil-tirozin ki je dobro topen in idealno nadomešča večje potrebe po tirozinu pri KLB (AminoMel nephro)
PREHRANSKI DODATKI
Enteralni
bull Nepro Nepro HP Nepro LP Ensure Ensure Plus Advance Prosure Fresubinhellipenkrat na dan per os
bull Glutamin 5-10g na dan per os
bull Carenal 1 tableto po dializi
bull L-karnitin
Parenteralni
bull Aminomel Nephro aminokisline (500ml med HD)
bull Kabiven
bull Glamin 500ml
bull Dipeptiven 100ml
bull Soluvit N(vodotopni vitamini)
bull Vitalipid N(maščobotopni vitamini)
bull Addamel N(mikroelementi)
bull Omegaven (ribje oljehellip)
Component Renal Specific
ONS
Standard ONS
Protein Optimum Medium
Glycemic Index
(Carbohydrates) Low High
MUFA Omega-3
(FatsLipids) High Low
Electrolytes
Phosphorus
Potassium Sodium
Low High
Fluid volume Low High
Caloric density High Standard
Fiber High Low
Prebiotics scFOS Present None
CKD-specific vitamin
amp mineral profile Optimized None
Why Renal Specific ONS
Why Standard versus Renal Specific ONS
Nutrition Intervention in CKD Patients
bull Expert recommendations
KDOQI1 ESPEN2 EBPG3
Nutrition
Support
Individuals undergoing
maintenance dialysis
who are unable to
meet their protein and
energy requirements
with food intake for an
extended period of
time should receive
nutritional support
Special formula
products for HD
treatment can be
useful especially in
malnourished patients
who are not able to
increase their nutrient
intake
Oral nutritional
supplements should
be prescribed if
nutritional counseling
does not achieve an
increase in nutrient
intake to a level that
covers minimum
recommendations
Products
specifically
designed for
dialysis patients
should be
prescribed
1 NKF KDOQI Clinical practice guidelines for nutrition in chronic renal failure AJKD 2000 35S1-S140
2 Cano N et al Clin Nutr 2006 25295-310
3 Fouque D et al NDT 2007 22(suppl 2)ii45-ii87
Recomm-S
ESPEN KDOQI EBPG
Proteini (gkgdan) 12-14 10-12 11
Energija
(kCalkgdan)
35 lt60 g 35
gt60 g 30
30-35
gt50 intke lt1 gkgdan
Actual ntake 20-25 kCalkg 08-1 g proteinakg
Renal Specific Nutritional Therapy
Clinical studies have shown that renal-specific nutrition offers advantages over standard nutrition
bull Phosphorus levels were lower with the renal-specific nutrition than with the standard nutrition1
bull Less fluid and potassium in renal-specific nutrition offers advantages over standard nutrition2
1 Cockram DB et al J Ren Nutr 1998825-33
2 Williams RF Summers AM J Ren Nutr 200919183-188
PREHRANSKE ZAHTEVE DIALIZE
PRAKSA
ENERGIJA 35KCALKG TT NA DAN
PROTEINI 12GKG TT NA DAN
VNOS TEKOČINE 1000ML + IZLOČEN URIN
NATRIJ 2-3G NA DAN
KALIJ 2-3G NA DAN
FOSFOR 08-12GDAN
NKFKDOQI 2000 ADA 2002 WILKENS 2004
BIOIMPEDANCE PRINCIPLES
Phase angle
bull Phase angle is an indicator based on reactance and
resistance obtained from bioelectrical impedance
analysis (BIA)
bull PA depends on cell membrane integrity and on body cell
mass
bull Although its biological meaning is still not clear phase
angle appears to have an important prognostic role
bull Phase angle differs across categories of sex age BMI
and percentage fat bull Maria Cristina G Barbosa-Silva Aluiacutesio JD Barros Jack Wang Steven B Heymsfield and Richard
N Pierson Jr Am J Clin Nutr July 2005 vol 82 no 1 49-52
bull Satish Kumar1 Aswini Dutt1 Sandhya Hemraj2 Shankar Bhat1 and Bhat Manipadybhima Iran
J Basic Med Sci 2012 Nov-Dec 15(6) 1180ndash1184
PHASE ANGLE AND LEAN TISSUE
INDEX ARE SLIGHTLY HIGHER IN
HEMODIALYSIS THAN IN PERITONEAL
DIALYSIS GROUP OF PATIENTS
BKnap ZVeceric Haler JButurovic-Ponikvar
RPonikvar AF Bren
University Clinical Center Ljubljana
Department of Nephrology Slovenia
Ideal nutrition ndash CKD patients
bull Prevents musle loss
bull Prevent andor treat PEW
bull Correct metabolic derrangements
bull Decrease morbidity and mortlity
bull Improve QoL
bull Does not promote progression of CKD
bull Or ideally slow down progression of CKD
ZAKLJUČEK
bull Podhranjenost je pomembna in pogosto
ključna za preživetje
bull Sodobne metode detekcije in zdravljenja
podhranjenosti omogočajo zgodnejšo
nutricijsko intervencijo
bull Prehranski dodatki tako enteralni kot
parenteralni so pogosto nujna in včasih
edina možnost
Kaj je dobro vedetihelliphellip
bull LEDVIČNI BOLNIKI JEDO SLABO
bull V ZAČETNI FAZI KLB TERAPIJA Z OMEJEVANJEM VNOSA PROTEINOV LAHKO PRIPELJE DO MALNUTRICIJE IN KAHEKSIJE
bull POMEMBNA OCENA HRANJENOSTI IN PRAVOČASNA NUTRICIJSKA INTERVENCIJA V VSEH FAZAH KLB
bull USPEH ZDRAVLJENJA MALNUTRICIJE JE POVEZAN Z DOBRIM ZDRAVLJENJEM OSNOVNE LEDVIČNE BOLEZNI IN CELOSTNEGA ZDRAVLJENJA KLB
bull POLEG HRANE VELIKO PRISPEVAJO K KVALITETI ŽIVLJENJA TUDI PREHRANSKI DODATKI IN TELESNA VADBA
bull ANABOLNI AGENSI IN STIMULATORJI APETITA NA NIVOJU HIPOTALAMUSA SO OBET BLIŽNJE PRIHODNOSTI
AA V PARENTERALNI PREHRANI
bull Povečana izguba AA
bull Neravnovesje med izgubo in porabo
bull Esencielne AA z dodatkom histidina ter arginina niso optimum
bull Nadomeščanje tirozina problem zaradi slabe topnostihellip
bull Acetil-tirozin je rešitev vendar ne pri KLB
bull Rešitev predstavlja dipeptid glicil-tirozin ki je dobro topen in idealno nadomešča večje potrebe po tirozinu pri KLB (AminoMel nephro)
PREHRANSKI DODATKI
Enteralni
bull Nepro Nepro HP Nepro LP Ensure Ensure Plus Advance Prosure Fresubinhellipenkrat na dan per os
bull Glutamin 5-10g na dan per os
bull Carenal 1 tableto po dializi
bull L-karnitin
Parenteralni
bull Aminomel Nephro aminokisline (500ml med HD)
bull Kabiven
bull Glamin 500ml
bull Dipeptiven 100ml
bull Soluvit N(vodotopni vitamini)
bull Vitalipid N(maščobotopni vitamini)
bull Addamel N(mikroelementi)
bull Omegaven (ribje oljehellip)
Component Renal Specific
ONS
Standard ONS
Protein Optimum Medium
Glycemic Index
(Carbohydrates) Low High
MUFA Omega-3
(FatsLipids) High Low
Electrolytes
Phosphorus
Potassium Sodium
Low High
Fluid volume Low High
Caloric density High Standard
Fiber High Low
Prebiotics scFOS Present None
CKD-specific vitamin
amp mineral profile Optimized None
Why Renal Specific ONS
Why Standard versus Renal Specific ONS
Nutrition Intervention in CKD Patients
bull Expert recommendations
KDOQI1 ESPEN2 EBPG3
Nutrition
Support
Individuals undergoing
maintenance dialysis
who are unable to
meet their protein and
energy requirements
with food intake for an
extended period of
time should receive
nutritional support
Special formula
products for HD
treatment can be
useful especially in
malnourished patients
who are not able to
increase their nutrient
intake
Oral nutritional
supplements should
be prescribed if
nutritional counseling
does not achieve an
increase in nutrient
intake to a level that
covers minimum
recommendations
Products
specifically
designed for
dialysis patients
should be
prescribed
1 NKF KDOQI Clinical practice guidelines for nutrition in chronic renal failure AJKD 2000 35S1-S140
2 Cano N et al Clin Nutr 2006 25295-310
3 Fouque D et al NDT 2007 22(suppl 2)ii45-ii87
Recomm-S
ESPEN KDOQI EBPG
Proteini (gkgdan) 12-14 10-12 11
Energija
(kCalkgdan)
35 lt60 g 35
gt60 g 30
30-35
gt50 intke lt1 gkgdan
Actual ntake 20-25 kCalkg 08-1 g proteinakg
Renal Specific Nutritional Therapy
Clinical studies have shown that renal-specific nutrition offers advantages over standard nutrition
bull Phosphorus levels were lower with the renal-specific nutrition than with the standard nutrition1
bull Less fluid and potassium in renal-specific nutrition offers advantages over standard nutrition2
1 Cockram DB et al J Ren Nutr 1998825-33
2 Williams RF Summers AM J Ren Nutr 200919183-188
PREHRANSKE ZAHTEVE DIALIZE
PRAKSA
ENERGIJA 35KCALKG TT NA DAN
PROTEINI 12GKG TT NA DAN
VNOS TEKOČINE 1000ML + IZLOČEN URIN
NATRIJ 2-3G NA DAN
KALIJ 2-3G NA DAN
FOSFOR 08-12GDAN
NKFKDOQI 2000 ADA 2002 WILKENS 2004
BIOIMPEDANCE PRINCIPLES
Phase angle
bull Phase angle is an indicator based on reactance and
resistance obtained from bioelectrical impedance
analysis (BIA)
bull PA depends on cell membrane integrity and on body cell
mass
bull Although its biological meaning is still not clear phase
angle appears to have an important prognostic role
bull Phase angle differs across categories of sex age BMI
and percentage fat bull Maria Cristina G Barbosa-Silva Aluiacutesio JD Barros Jack Wang Steven B Heymsfield and Richard
N Pierson Jr Am J Clin Nutr July 2005 vol 82 no 1 49-52
bull Satish Kumar1 Aswini Dutt1 Sandhya Hemraj2 Shankar Bhat1 and Bhat Manipadybhima Iran
J Basic Med Sci 2012 Nov-Dec 15(6) 1180ndash1184
PHASE ANGLE AND LEAN TISSUE
INDEX ARE SLIGHTLY HIGHER IN
HEMODIALYSIS THAN IN PERITONEAL
DIALYSIS GROUP OF PATIENTS
BKnap ZVeceric Haler JButurovic-Ponikvar
RPonikvar AF Bren
University Clinical Center Ljubljana
Department of Nephrology Slovenia
Ideal nutrition ndash CKD patients
bull Prevents musle loss
bull Prevent andor treat PEW
bull Correct metabolic derrangements
bull Decrease morbidity and mortlity
bull Improve QoL
bull Does not promote progression of CKD
bull Or ideally slow down progression of CKD
ZAKLJUČEK
bull Podhranjenost je pomembna in pogosto
ključna za preživetje
bull Sodobne metode detekcije in zdravljenja
podhranjenosti omogočajo zgodnejšo
nutricijsko intervencijo
bull Prehranski dodatki tako enteralni kot
parenteralni so pogosto nujna in včasih
edina možnost
Kaj je dobro vedetihelliphellip
bull LEDVIČNI BOLNIKI JEDO SLABO
bull V ZAČETNI FAZI KLB TERAPIJA Z OMEJEVANJEM VNOSA PROTEINOV LAHKO PRIPELJE DO MALNUTRICIJE IN KAHEKSIJE
bull POMEMBNA OCENA HRANJENOSTI IN PRAVOČASNA NUTRICIJSKA INTERVENCIJA V VSEH FAZAH KLB
bull USPEH ZDRAVLJENJA MALNUTRICIJE JE POVEZAN Z DOBRIM ZDRAVLJENJEM OSNOVNE LEDVIČNE BOLEZNI IN CELOSTNEGA ZDRAVLJENJA KLB
bull POLEG HRANE VELIKO PRISPEVAJO K KVALITETI ŽIVLJENJA TUDI PREHRANSKI DODATKI IN TELESNA VADBA
bull ANABOLNI AGENSI IN STIMULATORJI APETITA NA NIVOJU HIPOTALAMUSA SO OBET BLIŽNJE PRIHODNOSTI

PREHRANSKI DODATKI
Enteralni
bull Nepro Nepro HP Nepro LP Ensure Ensure Plus Advance Prosure Fresubinhellipenkrat na dan per os
bull Glutamin 5-10g na dan per os
bull Carenal 1 tableto po dializi
bull L-karnitin
Parenteralni
bull Aminomel Nephro aminokisline (500ml med HD)
bull Kabiven
bull Glamin 500ml
bull Dipeptiven 100ml
bull Soluvit N(vodotopni vitamini)
bull Vitalipid N(maščobotopni vitamini)
bull Addamel N(mikroelementi)
bull Omegaven (ribje oljehellip)
Component Renal Specific
ONS
Standard ONS
Protein Optimum Medium
Glycemic Index
(Carbohydrates) Low High
MUFA Omega-3
(FatsLipids) High Low
Electrolytes
Phosphorus
Potassium Sodium
Low High
Fluid volume Low High
Caloric density High Standard
Fiber High Low
Prebiotics scFOS Present None
CKD-specific vitamin
amp mineral profile Optimized None
Why Renal Specific ONS
Why Standard versus Renal Specific ONS
Nutrition Intervention in CKD Patients
bull Expert recommendations
KDOQI1 ESPEN2 EBPG3
Nutrition
Support
Individuals undergoing
maintenance dialysis
who are unable to
meet their protein and
energy requirements
with food intake for an
extended period of
time should receive
nutritional support
Special formula
products for HD
treatment can be
useful especially in
malnourished patients
who are not able to
increase their nutrient
intake
Oral nutritional
supplements should
be prescribed if
nutritional counseling
does not achieve an
increase in nutrient
intake to a level that
covers minimum
recommendations
Products
specifically
designed for
dialysis patients
should be
prescribed
1 NKF KDOQI Clinical practice guidelines for nutrition in chronic renal failure AJKD 2000 35S1-S140
2 Cano N et al Clin Nutr 2006 25295-310
3 Fouque D et al NDT 2007 22(suppl 2)ii45-ii87
Recomm-S
ESPEN KDOQI EBPG
Proteini (gkgdan) 12-14 10-12 11
Energija
(kCalkgdan)
35 lt60 g 35
gt60 g 30
30-35
gt50 intke lt1 gkgdan
Actual ntake 20-25 kCalkg 08-1 g proteinakg
Renal Specific Nutritional Therapy
Clinical studies have shown that renal-specific nutrition offers advantages over standard nutrition
bull Phosphorus levels were lower with the renal-specific nutrition than with the standard nutrition1
bull Less fluid and potassium in renal-specific nutrition offers advantages over standard nutrition2
1 Cockram DB et al J Ren Nutr 1998825-33
2 Williams RF Summers AM J Ren Nutr 200919183-188
PREHRANSKE ZAHTEVE DIALIZE
PRAKSA
ENERGIJA 35KCALKG TT NA DAN
PROTEINI 12GKG TT NA DAN
VNOS TEKOČINE 1000ML + IZLOČEN URIN
NATRIJ 2-3G NA DAN
KALIJ 2-3G NA DAN
FOSFOR 08-12GDAN
NKFKDOQI 2000 ADA 2002 WILKENS 2004
BIOIMPEDANCE PRINCIPLES
Phase angle
bull Phase angle is an indicator based on reactance and
resistance obtained from bioelectrical impedance
analysis (BIA)
bull PA depends on cell membrane integrity and on body cell
mass
bull Although its biological meaning is still not clear phase
angle appears to have an important prognostic role
bull Phase angle differs across categories of sex age BMI
and percentage fat bull Maria Cristina G Barbosa-Silva Aluiacutesio JD Barros Jack Wang Steven B Heymsfield and Richard
N Pierson Jr Am J Clin Nutr July 2005 vol 82 no 1 49-52
bull Satish Kumar1 Aswini Dutt1 Sandhya Hemraj2 Shankar Bhat1 and Bhat Manipadybhima Iran
J Basic Med Sci 2012 Nov-Dec 15(6) 1180ndash1184
PHASE ANGLE AND LEAN TISSUE
INDEX ARE SLIGHTLY HIGHER IN
HEMODIALYSIS THAN IN PERITONEAL
DIALYSIS GROUP OF PATIENTS
BKnap ZVeceric Haler JButurovic-Ponikvar
RPonikvar AF Bren
University Clinical Center Ljubljana
Department of Nephrology Slovenia
Ideal nutrition ndash CKD patients
bull Prevents musle loss
bull Prevent andor treat PEW
bull Correct metabolic derrangements
bull Decrease morbidity and mortlity
bull Improve QoL
bull Does not promote progression of CKD
bull Or ideally slow down progression of CKD
ZAKLJUČEK
bull Podhranjenost je pomembna in pogosto
ključna za preživetje
bull Sodobne metode detekcije in zdravljenja
podhranjenosti omogočajo zgodnejšo
nutricijsko intervencijo
bull Prehranski dodatki tako enteralni kot
parenteralni so pogosto nujna in včasih
edina možnost
Kaj je dobro vedetihelliphellip
bull LEDVIČNI BOLNIKI JEDO SLABO
bull V ZAČETNI FAZI KLB TERAPIJA Z OMEJEVANJEM VNOSA PROTEINOV LAHKO PRIPELJE DO MALNUTRICIJE IN KAHEKSIJE
bull POMEMBNA OCENA HRANJENOSTI IN PRAVOČASNA NUTRICIJSKA INTERVENCIJA V VSEH FAZAH KLB
bull USPEH ZDRAVLJENJA MALNUTRICIJE JE POVEZAN Z DOBRIM ZDRAVLJENJEM OSNOVNE LEDVIČNE BOLEZNI IN CELOSTNEGA ZDRAVLJENJA KLB
bull POLEG HRANE VELIKO PRISPEVAJO K KVALITETI ŽIVLJENJA TUDI PREHRANSKI DODATKI IN TELESNA VADBA
bull ANABOLNI AGENSI IN STIMULATORJI APETITA NA NIVOJU HIPOTALAMUSA SO OBET BLIŽNJE PRIHODNOSTI

Component Renal Specific
ONS
Standard ONS
Protein Optimum Medium
Glycemic Index
(Carbohydrates) Low High
MUFA Omega-3
(FatsLipids) High Low
Electrolytes
Phosphorus
Potassium Sodium
Low High
Fluid volume Low High
Caloric density High Standard
Fiber High Low
Prebiotics scFOS Present None
CKD-specific vitamin
amp mineral profile Optimized None
Why Renal Specific ONS
Why Standard versus Renal Specific ONS
Nutrition Intervention in CKD Patients
bull Expert recommendations
KDOQI1 ESPEN2 EBPG3
Nutrition
Support
Individuals undergoing
maintenance dialysis
who are unable to
meet their protein and
energy requirements
with food intake for an
extended period of
time should receive
nutritional support
Special formula
products for HD
treatment can be
useful especially in
malnourished patients
who are not able to
increase their nutrient
intake
Oral nutritional
supplements should
be prescribed if
nutritional counseling
does not achieve an
increase in nutrient
intake to a level that
covers minimum
recommendations
Products
specifically
designed for
dialysis patients
should be
prescribed
1 NKF KDOQI Clinical practice guidelines for nutrition in chronic renal failure AJKD 2000 35S1-S140
2 Cano N et al Clin Nutr 2006 25295-310
3 Fouque D et al NDT 2007 22(suppl 2)ii45-ii87
Recomm-S
ESPEN KDOQI EBPG
Proteini (gkgdan) 12-14 10-12 11
Energija
(kCalkgdan)
35 lt60 g 35
gt60 g 30
30-35
gt50 intke lt1 gkgdan
Actual ntake 20-25 kCalkg 08-1 g proteinakg
Renal Specific Nutritional Therapy
Clinical studies have shown that renal-specific nutrition offers advantages over standard nutrition
bull Phosphorus levels were lower with the renal-specific nutrition than with the standard nutrition1
bull Less fluid and potassium in renal-specific nutrition offers advantages over standard nutrition2
1 Cockram DB et al J Ren Nutr 1998825-33
2 Williams RF Summers AM J Ren Nutr 200919183-188
PREHRANSKE ZAHTEVE DIALIZE
PRAKSA
ENERGIJA 35KCALKG TT NA DAN
PROTEINI 12GKG TT NA DAN
VNOS TEKOČINE 1000ML + IZLOČEN URIN
NATRIJ 2-3G NA DAN
KALIJ 2-3G NA DAN
FOSFOR 08-12GDAN
NKFKDOQI 2000 ADA 2002 WILKENS 2004
BIOIMPEDANCE PRINCIPLES
Phase angle
bull Phase angle is an indicator based on reactance and
resistance obtained from bioelectrical impedance
analysis (BIA)
bull PA depends on cell membrane integrity and on body cell
mass
bull Although its biological meaning is still not clear phase
angle appears to have an important prognostic role
bull Phase angle differs across categories of sex age BMI
and percentage fat bull Maria Cristina G Barbosa-Silva Aluiacutesio JD Barros Jack Wang Steven B Heymsfield and Richard
N Pierson Jr Am J Clin Nutr July 2005 vol 82 no 1 49-52
bull Satish Kumar1 Aswini Dutt1 Sandhya Hemraj2 Shankar Bhat1 and Bhat Manipadybhima Iran
J Basic Med Sci 2012 Nov-Dec 15(6) 1180ndash1184
PHASE ANGLE AND LEAN TISSUE
INDEX ARE SLIGHTLY HIGHER IN
HEMODIALYSIS THAN IN PERITONEAL
DIALYSIS GROUP OF PATIENTS
BKnap ZVeceric Haler JButurovic-Ponikvar
RPonikvar AF Bren
University Clinical Center Ljubljana
Department of Nephrology Slovenia
Ideal nutrition ndash CKD patients
bull Prevents musle loss
bull Prevent andor treat PEW
bull Correct metabolic derrangements
bull Decrease morbidity and mortlity
bull Improve QoL
bull Does not promote progression of CKD
bull Or ideally slow down progression of CKD
ZAKLJUČEK
bull Podhranjenost je pomembna in pogosto
ključna za preživetje
bull Sodobne metode detekcije in zdravljenja
podhranjenosti omogočajo zgodnejšo
nutricijsko intervencijo
bull Prehranski dodatki tako enteralni kot
parenteralni so pogosto nujna in včasih
edina možnost
Kaj je dobro vedetihelliphellip
bull LEDVIČNI BOLNIKI JEDO SLABO
bull V ZAČETNI FAZI KLB TERAPIJA Z OMEJEVANJEM VNOSA PROTEINOV LAHKO PRIPELJE DO MALNUTRICIJE IN KAHEKSIJE
bull POMEMBNA OCENA HRANJENOSTI IN PRAVOČASNA NUTRICIJSKA INTERVENCIJA V VSEH FAZAH KLB
bull USPEH ZDRAVLJENJA MALNUTRICIJE JE POVEZAN Z DOBRIM ZDRAVLJENJEM OSNOVNE LEDVIČNE BOLEZNI IN CELOSTNEGA ZDRAVLJENJA KLB
bull POLEG HRANE VELIKO PRISPEVAJO K KVALITETI ŽIVLJENJA TUDI PREHRANSKI DODATKI IN TELESNA VADBA
bull ANABOLNI AGENSI IN STIMULATORJI APETITA NA NIVOJU HIPOTALAMUSA SO OBET BLIŽNJE PRIHODNOSTI
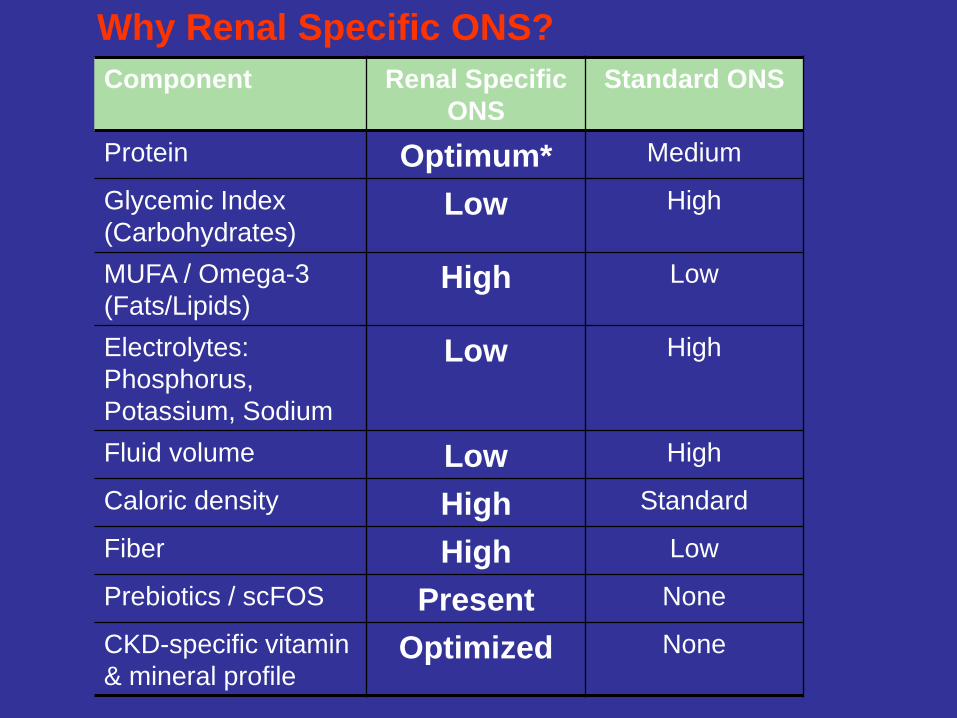
Why Standard versus Renal Specific ONS
Nutrition Intervention in CKD Patients
bull Expert recommendations
KDOQI1 ESPEN2 EBPG3
Nutrition
Support
Individuals undergoing
maintenance dialysis
who are unable to
meet their protein and
energy requirements
with food intake for an
extended period of
time should receive
nutritional support
Special formula
products for HD
treatment can be
useful especially in
malnourished patients
who are not able to
increase their nutrient
intake
Oral nutritional
supplements should
be prescribed if
nutritional counseling
does not achieve an
increase in nutrient
intake to a level that
covers minimum
recommendations
Products
specifically
designed for
dialysis patients
should be
prescribed
1 NKF KDOQI Clinical practice guidelines for nutrition in chronic renal failure AJKD 2000 35S1-S140
2 Cano N et al Clin Nutr 2006 25295-310
3 Fouque D et al NDT 2007 22(suppl 2)ii45-ii87
Recomm-S
ESPEN KDOQI EBPG
Proteini (gkgdan) 12-14 10-12 11
Energija
(kCalkgdan)
35 lt60 g 35
gt60 g 30
30-35
gt50 intke lt1 gkgdan
Actual ntake 20-25 kCalkg 08-1 g proteinakg
Renal Specific Nutritional Therapy
Clinical studies have shown that renal-specific nutrition offers advantages over standard nutrition
bull Phosphorus levels were lower with the renal-specific nutrition than with the standard nutrition1
bull Less fluid and potassium in renal-specific nutrition offers advantages over standard nutrition2
1 Cockram DB et al J Ren Nutr 1998825-33
2 Williams RF Summers AM J Ren Nutr 200919183-188
PREHRANSKE ZAHTEVE DIALIZE
PRAKSA
ENERGIJA 35KCALKG TT NA DAN
PROTEINI 12GKG TT NA DAN
VNOS TEKOČINE 1000ML + IZLOČEN URIN
NATRIJ 2-3G NA DAN
KALIJ 2-3G NA DAN
FOSFOR 08-12GDAN
NKFKDOQI 2000 ADA 2002 WILKENS 2004
BIOIMPEDANCE PRINCIPLES
Phase angle
bull Phase angle is an indicator based on reactance and
resistance obtained from bioelectrical impedance
analysis (BIA)
bull PA depends on cell membrane integrity and on body cell
mass
bull Although its biological meaning is still not clear phase
angle appears to have an important prognostic role
bull Phase angle differs across categories of sex age BMI
and percentage fat bull Maria Cristina G Barbosa-Silva Aluiacutesio JD Barros Jack Wang Steven B Heymsfield and Richard
N Pierson Jr Am J Clin Nutr July 2005 vol 82 no 1 49-52
bull Satish Kumar1 Aswini Dutt1 Sandhya Hemraj2 Shankar Bhat1 and Bhat Manipadybhima Iran
J Basic Med Sci 2012 Nov-Dec 15(6) 1180ndash1184
PHASE ANGLE AND LEAN TISSUE
INDEX ARE SLIGHTLY HIGHER IN
HEMODIALYSIS THAN IN PERITONEAL
DIALYSIS GROUP OF PATIENTS
BKnap ZVeceric Haler JButurovic-Ponikvar
RPonikvar AF Bren
University Clinical Center Ljubljana
Department of Nephrology Slovenia
Ideal nutrition ndash CKD patients
bull Prevents musle loss
bull Prevent andor treat PEW
bull Correct metabolic derrangements
bull Decrease morbidity and mortlity
bull Improve QoL
bull Does not promote progression of CKD
bull Or ideally slow down progression of CKD
ZAKLJUČEK
bull Podhranjenost je pomembna in pogosto
ključna za preživetje
bull Sodobne metode detekcije in zdravljenja
podhranjenosti omogočajo zgodnejšo
nutricijsko intervencijo
bull Prehranski dodatki tako enteralni kot
parenteralni so pogosto nujna in včasih
edina možnost
Kaj je dobro vedetihelliphellip
bull LEDVIČNI BOLNIKI JEDO SLABO
bull V ZAČETNI FAZI KLB TERAPIJA Z OMEJEVANJEM VNOSA PROTEINOV LAHKO PRIPELJE DO MALNUTRICIJE IN KAHEKSIJE
bull POMEMBNA OCENA HRANJENOSTI IN PRAVOČASNA NUTRICIJSKA INTERVENCIJA V VSEH FAZAH KLB
bull USPEH ZDRAVLJENJA MALNUTRICIJE JE POVEZAN Z DOBRIM ZDRAVLJENJEM OSNOVNE LEDVIČNE BOLEZNI IN CELOSTNEGA ZDRAVLJENJA KLB
bull POLEG HRANE VELIKO PRISPEVAJO K KVALITETI ŽIVLJENJA TUDI PREHRANSKI DODATKI IN TELESNA VADBA
bull ANABOLNI AGENSI IN STIMULATORJI APETITA NA NIVOJU HIPOTALAMUSA SO OBET BLIŽNJE PRIHODNOSTI

Recomm-S
ESPEN KDOQI EBPG
Proteini (gkgdan) 12-14 10-12 11
Energija
(kCalkgdan)
35 lt60 g 35
gt60 g 30
30-35
gt50 intke lt1 gkgdan
Actual ntake 20-25 kCalkg 08-1 g proteinakg
Renal Specific Nutritional Therapy
Clinical studies have shown that renal-specific nutrition offers advantages over standard nutrition
bull Phosphorus levels were lower with the renal-specific nutrition than with the standard nutrition1
bull Less fluid and potassium in renal-specific nutrition offers advantages over standard nutrition2
1 Cockram DB et al J Ren Nutr 1998825-33
2 Williams RF Summers AM J Ren Nutr 200919183-188
PREHRANSKE ZAHTEVE DIALIZE
PRAKSA
ENERGIJA 35KCALKG TT NA DAN
PROTEINI 12GKG TT NA DAN
VNOS TEKOČINE 1000ML + IZLOČEN URIN
NATRIJ 2-3G NA DAN
KALIJ 2-3G NA DAN
FOSFOR 08-12GDAN
NKFKDOQI 2000 ADA 2002 WILKENS 2004
BIOIMPEDANCE PRINCIPLES
Phase angle
bull Phase angle is an indicator based on reactance and
resistance obtained from bioelectrical impedance
analysis (BIA)
bull PA depends on cell membrane integrity and on body cell
mass
bull Although its biological meaning is still not clear phase
angle appears to have an important prognostic role
bull Phase angle differs across categories of sex age BMI
and percentage fat bull Maria Cristina G Barbosa-Silva Aluiacutesio JD Barros Jack Wang Steven B Heymsfield and Richard
N Pierson Jr Am J Clin Nutr July 2005 vol 82 no 1 49-52
bull Satish Kumar1 Aswini Dutt1 Sandhya Hemraj2 Shankar Bhat1 and Bhat Manipadybhima Iran
J Basic Med Sci 2012 Nov-Dec 15(6) 1180ndash1184
PHASE ANGLE AND LEAN TISSUE
INDEX ARE SLIGHTLY HIGHER IN
HEMODIALYSIS THAN IN PERITONEAL
DIALYSIS GROUP OF PATIENTS
BKnap ZVeceric Haler JButurovic-Ponikvar
RPonikvar AF Bren
University Clinical Center Ljubljana
Department of Nephrology Slovenia
Ideal nutrition ndash CKD patients
bull Prevents musle loss
bull Prevent andor treat PEW
bull Correct metabolic derrangements
bull Decrease morbidity and mortlity
bull Improve QoL
bull Does not promote progression of CKD
bull Or ideally slow down progression of CKD
ZAKLJUČEK
bull Podhranjenost je pomembna in pogosto
ključna za preživetje
bull Sodobne metode detekcije in zdravljenja
podhranjenosti omogočajo zgodnejšo
nutricijsko intervencijo
bull Prehranski dodatki tako enteralni kot
parenteralni so pogosto nujna in včasih
edina možnost
Kaj je dobro vedetihelliphellip
bull LEDVIČNI BOLNIKI JEDO SLABO
bull V ZAČETNI FAZI KLB TERAPIJA Z OMEJEVANJEM VNOSA PROTEINOV LAHKO PRIPELJE DO MALNUTRICIJE IN KAHEKSIJE
bull POMEMBNA OCENA HRANJENOSTI IN PRAVOČASNA NUTRICIJSKA INTERVENCIJA V VSEH FAZAH KLB
bull USPEH ZDRAVLJENJA MALNUTRICIJE JE POVEZAN Z DOBRIM ZDRAVLJENJEM OSNOVNE LEDVIČNE BOLEZNI IN CELOSTNEGA ZDRAVLJENJA KLB
bull POLEG HRANE VELIKO PRISPEVAJO K KVALITETI ŽIVLJENJA TUDI PREHRANSKI DODATKI IN TELESNA VADBA
bull ANABOLNI AGENSI IN STIMULATORJI APETITA NA NIVOJU HIPOTALAMUSA SO OBET BLIŽNJE PRIHODNOSTI

Renal Specific Nutritional Therapy
Clinical studies have shown that renal-specific nutrition offers advantages over standard nutrition
bull Phosphorus levels were lower with the renal-specific nutrition than with the standard nutrition1
bull Less fluid and potassium in renal-specific nutrition offers advantages over standard nutrition2
1 Cockram DB et al J Ren Nutr 1998825-33
2 Williams RF Summers AM J Ren Nutr 200919183-188
PREHRANSKE ZAHTEVE DIALIZE
PRAKSA
ENERGIJA 35KCALKG TT NA DAN
PROTEINI 12GKG TT NA DAN
VNOS TEKOČINE 1000ML + IZLOČEN URIN
NATRIJ 2-3G NA DAN
KALIJ 2-3G NA DAN
FOSFOR 08-12GDAN
NKFKDOQI 2000 ADA 2002 WILKENS 2004
BIOIMPEDANCE PRINCIPLES
Phase angle
bull Phase angle is an indicator based on reactance and
resistance obtained from bioelectrical impedance
analysis (BIA)
bull PA depends on cell membrane integrity and on body cell
mass
bull Although its biological meaning is still not clear phase
angle appears to have an important prognostic role
bull Phase angle differs across categories of sex age BMI
and percentage fat bull Maria Cristina G Barbosa-Silva Aluiacutesio JD Barros Jack Wang Steven B Heymsfield and Richard
N Pierson Jr Am J Clin Nutr July 2005 vol 82 no 1 49-52
bull Satish Kumar1 Aswini Dutt1 Sandhya Hemraj2 Shankar Bhat1 and Bhat Manipadybhima Iran
J Basic Med Sci 2012 Nov-Dec 15(6) 1180ndash1184
PHASE ANGLE AND LEAN TISSUE
INDEX ARE SLIGHTLY HIGHER IN
HEMODIALYSIS THAN IN PERITONEAL
DIALYSIS GROUP OF PATIENTS
BKnap ZVeceric Haler JButurovic-Ponikvar
RPonikvar AF Bren
University Clinical Center Ljubljana
Department of Nephrology Slovenia
Ideal nutrition ndash CKD patients
bull Prevents musle loss
bull Prevent andor treat PEW
bull Correct metabolic derrangements
bull Decrease morbidity and mortlity
bull Improve QoL
bull Does not promote progression of CKD
bull Or ideally slow down progression of CKD
ZAKLJUČEK
bull Podhranjenost je pomembna in pogosto
ključna za preživetje
bull Sodobne metode detekcije in zdravljenja
podhranjenosti omogočajo zgodnejšo
nutricijsko intervencijo
bull Prehranski dodatki tako enteralni kot
parenteralni so pogosto nujna in včasih
edina možnost
Kaj je dobro vedetihelliphellip
bull LEDVIČNI BOLNIKI JEDO SLABO
bull V ZAČETNI FAZI KLB TERAPIJA Z OMEJEVANJEM VNOSA PROTEINOV LAHKO PRIPELJE DO MALNUTRICIJE IN KAHEKSIJE
bull POMEMBNA OCENA HRANJENOSTI IN PRAVOČASNA NUTRICIJSKA INTERVENCIJA V VSEH FAZAH KLB
bull USPEH ZDRAVLJENJA MALNUTRICIJE JE POVEZAN Z DOBRIM ZDRAVLJENJEM OSNOVNE LEDVIČNE BOLEZNI IN CELOSTNEGA ZDRAVLJENJA KLB
bull POLEG HRANE VELIKO PRISPEVAJO K KVALITETI ŽIVLJENJA TUDI PREHRANSKI DODATKI IN TELESNA VADBA
bull ANABOLNI AGENSI IN STIMULATORJI APETITA NA NIVOJU HIPOTALAMUSA SO OBET BLIŽNJE PRIHODNOSTI

PREHRANSKE ZAHTEVE DIALIZE
PRAKSA
ENERGIJA 35KCALKG TT NA DAN
PROTEINI 12GKG TT NA DAN
VNOS TEKOČINE 1000ML + IZLOČEN URIN
NATRIJ 2-3G NA DAN
KALIJ 2-3G NA DAN
FOSFOR 08-12GDAN
NKFKDOQI 2000 ADA 2002 WILKENS 2004
BIOIMPEDANCE PRINCIPLES
Phase angle
bull Phase angle is an indicator based on reactance and
resistance obtained from bioelectrical impedance
analysis (BIA)
bull PA depends on cell membrane integrity and on body cell
mass
bull Although its biological meaning is still not clear phase
angle appears to have an important prognostic role
bull Phase angle differs across categories of sex age BMI
and percentage fat bull Maria Cristina G Barbosa-Silva Aluiacutesio JD Barros Jack Wang Steven B Heymsfield and Richard
N Pierson Jr Am J Clin Nutr July 2005 vol 82 no 1 49-52
bull Satish Kumar1 Aswini Dutt1 Sandhya Hemraj2 Shankar Bhat1 and Bhat Manipadybhima Iran
J Basic Med Sci 2012 Nov-Dec 15(6) 1180ndash1184
PHASE ANGLE AND LEAN TISSUE
INDEX ARE SLIGHTLY HIGHER IN
HEMODIALYSIS THAN IN PERITONEAL
DIALYSIS GROUP OF PATIENTS
BKnap ZVeceric Haler JButurovic-Ponikvar
RPonikvar AF Bren
University Clinical Center Ljubljana
Department of Nephrology Slovenia
Ideal nutrition ndash CKD patients
bull Prevents musle loss
bull Prevent andor treat PEW
bull Correct metabolic derrangements
bull Decrease morbidity and mortlity
bull Improve QoL
bull Does not promote progression of CKD
bull Or ideally slow down progression of CKD
ZAKLJUČEK
bull Podhranjenost je pomembna in pogosto
ključna za preživetje
bull Sodobne metode detekcije in zdravljenja
podhranjenosti omogočajo zgodnejšo
nutricijsko intervencijo
bull Prehranski dodatki tako enteralni kot
parenteralni so pogosto nujna in včasih
edina možnost
Kaj je dobro vedetihelliphellip
bull LEDVIČNI BOLNIKI JEDO SLABO
bull V ZAČETNI FAZI KLB TERAPIJA Z OMEJEVANJEM VNOSA PROTEINOV LAHKO PRIPELJE DO MALNUTRICIJE IN KAHEKSIJE
bull POMEMBNA OCENA HRANJENOSTI IN PRAVOČASNA NUTRICIJSKA INTERVENCIJA V VSEH FAZAH KLB
bull USPEH ZDRAVLJENJA MALNUTRICIJE JE POVEZAN Z DOBRIM ZDRAVLJENJEM OSNOVNE LEDVIČNE BOLEZNI IN CELOSTNEGA ZDRAVLJENJA KLB
bull POLEG HRANE VELIKO PRISPEVAJO K KVALITETI ŽIVLJENJA TUDI PREHRANSKI DODATKI IN TELESNA VADBA
bull ANABOLNI AGENSI IN STIMULATORJI APETITA NA NIVOJU HIPOTALAMUSA SO OBET BLIŽNJE PRIHODNOSTI
BIOIMPEDANCE PRINCIPLES
Phase angle
bull Phase angle is an indicator based on reactance and
resistance obtained from bioelectrical impedance
analysis (BIA)
bull PA depends on cell membrane integrity and on body cell
mass
bull Although its biological meaning is still not clear phase
angle appears to have an important prognostic role
bull Phase angle differs across categories of sex age BMI
and percentage fat bull Maria Cristina G Barbosa-Silva Aluiacutesio JD Barros Jack Wang Steven B Heymsfield and Richard
N Pierson Jr Am J Clin Nutr July 2005 vol 82 no 1 49-52
bull Satish Kumar1 Aswini Dutt1 Sandhya Hemraj2 Shankar Bhat1 and Bhat Manipadybhima Iran
J Basic Med Sci 2012 Nov-Dec 15(6) 1180ndash1184
PHASE ANGLE AND LEAN TISSUE
INDEX ARE SLIGHTLY HIGHER IN
HEMODIALYSIS THAN IN PERITONEAL
DIALYSIS GROUP OF PATIENTS
BKnap ZVeceric Haler JButurovic-Ponikvar
RPonikvar AF Bren
University Clinical Center Ljubljana
Department of Nephrology Slovenia
Ideal nutrition ndash CKD patients
bull Prevents musle loss
bull Prevent andor treat PEW
bull Correct metabolic derrangements
bull Decrease morbidity and mortlity
bull Improve QoL
bull Does not promote progression of CKD
bull Or ideally slow down progression of CKD
ZAKLJUČEK
bull Podhranjenost je pomembna in pogosto
ključna za preživetje
bull Sodobne metode detekcije in zdravljenja
podhranjenosti omogočajo zgodnejšo
nutricijsko intervencijo
bull Prehranski dodatki tako enteralni kot
parenteralni so pogosto nujna in včasih
edina možnost
Kaj je dobro vedetihelliphellip
bull LEDVIČNI BOLNIKI JEDO SLABO
bull V ZAČETNI FAZI KLB TERAPIJA Z OMEJEVANJEM VNOSA PROTEINOV LAHKO PRIPELJE DO MALNUTRICIJE IN KAHEKSIJE
bull POMEMBNA OCENA HRANJENOSTI IN PRAVOČASNA NUTRICIJSKA INTERVENCIJA V VSEH FAZAH KLB
bull USPEH ZDRAVLJENJA MALNUTRICIJE JE POVEZAN Z DOBRIM ZDRAVLJENJEM OSNOVNE LEDVIČNE BOLEZNI IN CELOSTNEGA ZDRAVLJENJA KLB
bull POLEG HRANE VELIKO PRISPEVAJO K KVALITETI ŽIVLJENJA TUDI PREHRANSKI DODATKI IN TELESNA VADBA
bull ANABOLNI AGENSI IN STIMULATORJI APETITA NA NIVOJU HIPOTALAMUSA SO OBET BLIŽNJE PRIHODNOSTI

Phase angle
bull Phase angle is an indicator based on reactance and
resistance obtained from bioelectrical impedance
analysis (BIA)
bull PA depends on cell membrane integrity and on body cell
mass
bull Although its biological meaning is still not clear phase
angle appears to have an important prognostic role
bull Phase angle differs across categories of sex age BMI
and percentage fat bull Maria Cristina G Barbosa-Silva Aluiacutesio JD Barros Jack Wang Steven B Heymsfield and Richard
N Pierson Jr Am J Clin Nutr July 2005 vol 82 no 1 49-52
bull Satish Kumar1 Aswini Dutt1 Sandhya Hemraj2 Shankar Bhat1 and Bhat Manipadybhima Iran
J Basic Med Sci 2012 Nov-Dec 15(6) 1180ndash1184
PHASE ANGLE AND LEAN TISSUE
INDEX ARE SLIGHTLY HIGHER IN
HEMODIALYSIS THAN IN PERITONEAL
DIALYSIS GROUP OF PATIENTS
BKnap ZVeceric Haler JButurovic-Ponikvar
RPonikvar AF Bren
University Clinical Center Ljubljana
Department of Nephrology Slovenia
Ideal nutrition ndash CKD patients
bull Prevents musle loss
bull Prevent andor treat PEW
bull Correct metabolic derrangements
bull Decrease morbidity and mortlity
bull Improve QoL
bull Does not promote progression of CKD
bull Or ideally slow down progression of CKD
ZAKLJUČEK
bull Podhranjenost je pomembna in pogosto
ključna za preživetje
bull Sodobne metode detekcije in zdravljenja
podhranjenosti omogočajo zgodnejšo
nutricijsko intervencijo
bull Prehranski dodatki tako enteralni kot
parenteralni so pogosto nujna in včasih
edina možnost
Kaj je dobro vedetihelliphellip
bull LEDVIČNI BOLNIKI JEDO SLABO
bull V ZAČETNI FAZI KLB TERAPIJA Z OMEJEVANJEM VNOSA PROTEINOV LAHKO PRIPELJE DO MALNUTRICIJE IN KAHEKSIJE
bull POMEMBNA OCENA HRANJENOSTI IN PRAVOČASNA NUTRICIJSKA INTERVENCIJA V VSEH FAZAH KLB
bull USPEH ZDRAVLJENJA MALNUTRICIJE JE POVEZAN Z DOBRIM ZDRAVLJENJEM OSNOVNE LEDVIČNE BOLEZNI IN CELOSTNEGA ZDRAVLJENJA KLB
bull POLEG HRANE VELIKO PRISPEVAJO K KVALITETI ŽIVLJENJA TUDI PREHRANSKI DODATKI IN TELESNA VADBA
bull ANABOLNI AGENSI IN STIMULATORJI APETITA NA NIVOJU HIPOTALAMUSA SO OBET BLIŽNJE PRIHODNOSTI

PHASE ANGLE AND LEAN TISSUE
INDEX ARE SLIGHTLY HIGHER IN
HEMODIALYSIS THAN IN PERITONEAL
DIALYSIS GROUP OF PATIENTS
BKnap ZVeceric Haler JButurovic-Ponikvar
RPonikvar AF Bren
University Clinical Center Ljubljana
Department of Nephrology Slovenia
Ideal nutrition ndash CKD patients
bull Prevents musle loss
bull Prevent andor treat PEW
bull Correct metabolic derrangements
bull Decrease morbidity and mortlity
bull Improve QoL
bull Does not promote progression of CKD
bull Or ideally slow down progression of CKD
ZAKLJUČEK
bull Podhranjenost je pomembna in pogosto
ključna za preživetje
bull Sodobne metode detekcije in zdravljenja
podhranjenosti omogočajo zgodnejšo
nutricijsko intervencijo
bull Prehranski dodatki tako enteralni kot
parenteralni so pogosto nujna in včasih
edina možnost
Kaj je dobro vedetihelliphellip
bull LEDVIČNI BOLNIKI JEDO SLABO
bull V ZAČETNI FAZI KLB TERAPIJA Z OMEJEVANJEM VNOSA PROTEINOV LAHKO PRIPELJE DO MALNUTRICIJE IN KAHEKSIJE
bull POMEMBNA OCENA HRANJENOSTI IN PRAVOČASNA NUTRICIJSKA INTERVENCIJA V VSEH FAZAH KLB
bull USPEH ZDRAVLJENJA MALNUTRICIJE JE POVEZAN Z DOBRIM ZDRAVLJENJEM OSNOVNE LEDVIČNE BOLEZNI IN CELOSTNEGA ZDRAVLJENJA KLB
bull POLEG HRANE VELIKO PRISPEVAJO K KVALITETI ŽIVLJENJA TUDI PREHRANSKI DODATKI IN TELESNA VADBA
bull ANABOLNI AGENSI IN STIMULATORJI APETITA NA NIVOJU HIPOTALAMUSA SO OBET BLIŽNJE PRIHODNOSTI
Ideal nutrition ndash CKD patients
bull Prevents musle loss
bull Prevent andor treat PEW
bull Correct metabolic derrangements
bull Decrease morbidity and mortlity
bull Improve QoL
bull Does not promote progression of CKD
bull Or ideally slow down progression of CKD
ZAKLJUČEK
bull Podhranjenost je pomembna in pogosto
ključna za preživetje
bull Sodobne metode detekcije in zdravljenja
podhranjenosti omogočajo zgodnejšo
nutricijsko intervencijo
bull Prehranski dodatki tako enteralni kot
parenteralni so pogosto nujna in včasih
edina možnost
Kaj je dobro vedetihelliphellip
bull LEDVIČNI BOLNIKI JEDO SLABO
bull V ZAČETNI FAZI KLB TERAPIJA Z OMEJEVANJEM VNOSA PROTEINOV LAHKO PRIPELJE DO MALNUTRICIJE IN KAHEKSIJE
bull POMEMBNA OCENA HRANJENOSTI IN PRAVOČASNA NUTRICIJSKA INTERVENCIJA V VSEH FAZAH KLB
bull USPEH ZDRAVLJENJA MALNUTRICIJE JE POVEZAN Z DOBRIM ZDRAVLJENJEM OSNOVNE LEDVIČNE BOLEZNI IN CELOSTNEGA ZDRAVLJENJA KLB
bull POLEG HRANE VELIKO PRISPEVAJO K KVALITETI ŽIVLJENJA TUDI PREHRANSKI DODATKI IN TELESNA VADBA
bull ANABOLNI AGENSI IN STIMULATORJI APETITA NA NIVOJU HIPOTALAMUSA SO OBET BLIŽNJE PRIHODNOSTI
ZAKLJUČEK
bull Podhranjenost je pomembna in pogosto
ključna za preživetje
bull Sodobne metode detekcije in zdravljenja
podhranjenosti omogočajo zgodnejšo
nutricijsko intervencijo
bull Prehranski dodatki tako enteralni kot
parenteralni so pogosto nujna in včasih
edina možnost
Kaj je dobro vedetihelliphellip
bull LEDVIČNI BOLNIKI JEDO SLABO
bull V ZAČETNI FAZI KLB TERAPIJA Z OMEJEVANJEM VNOSA PROTEINOV LAHKO PRIPELJE DO MALNUTRICIJE IN KAHEKSIJE
bull POMEMBNA OCENA HRANJENOSTI IN PRAVOČASNA NUTRICIJSKA INTERVENCIJA V VSEH FAZAH KLB
bull USPEH ZDRAVLJENJA MALNUTRICIJE JE POVEZAN Z DOBRIM ZDRAVLJENJEM OSNOVNE LEDVIČNE BOLEZNI IN CELOSTNEGA ZDRAVLJENJA KLB
bull POLEG HRANE VELIKO PRISPEVAJO K KVALITETI ŽIVLJENJA TUDI PREHRANSKI DODATKI IN TELESNA VADBA
bull ANABOLNI AGENSI IN STIMULATORJI APETITA NA NIVOJU HIPOTALAMUSA SO OBET BLIŽNJE PRIHODNOSTI

Kaj je dobro vedetihelliphellip
bull LEDVIČNI BOLNIKI JEDO SLABO
bull V ZAČETNI FAZI KLB TERAPIJA Z OMEJEVANJEM VNOSA PROTEINOV LAHKO PRIPELJE DO MALNUTRICIJE IN KAHEKSIJE
bull POMEMBNA OCENA HRANJENOSTI IN PRAVOČASNA NUTRICIJSKA INTERVENCIJA V VSEH FAZAH KLB
bull USPEH ZDRAVLJENJA MALNUTRICIJE JE POVEZAN Z DOBRIM ZDRAVLJENJEM OSNOVNE LEDVIČNE BOLEZNI IN CELOSTNEGA ZDRAVLJENJA KLB
bull POLEG HRANE VELIKO PRISPEVAJO K KVALITETI ŽIVLJENJA TUDI PREHRANSKI DODATKI IN TELESNA VADBA
bull ANABOLNI AGENSI IN STIMULATORJI APETITA NA NIVOJU HIPOTALAMUSA SO OBET BLIŽNJE PRIHODNOSTI


















