
TEMS – pushing the limits - Pelican Courses · TART inferior to TEMS ... Rectoscope tube 12 or...
38
Transanal Excision SPECC Training day Stephan Korsgen Good Hope Hospital, Sutton Coldfield
Transcript of TEMS – pushing the limits - Pelican Courses · TART inferior to TEMS ... Rectoscope tube 12 or...

Transanal Excision SPECC Training day
Stephan Korsgen Good Hope Hospital, Sutton Coldfield
Scope of presentation
TART: Transanal excision (using retractors)
TEMS: Transanal endoscopic microsurgery
TEO: Transanal endoscopic operation
TAMIS: Transanal minimally invasive surgery

Which one to choose?
TART inferior to TEMS
TEO same principle as TEMS but not binocular vision and less stable platform
TAMIS early days, but seems to be less versatile and difficult to get stable platform

Scope of presentation
Know your audience

Scope of presentation
Basics of TEMS/TEO
Indications
Limitations
Complications
Case selection

TEMS -what is it?
Endoluminal rectal surgery
Rectoscope tube 12 or 20cm long, 40mm
Stereoscopic optics with magnification
Channels for CO2 insufflation, rectal pressure measurements, irrigation
3 ports for grasper, diathermy, suction
Specialised instrumentation

Gerhard Bueß (1948 -2010)
Developed in Cologne, West Germany 1980 – 1983
First NOTES (natural orifice transluminal endoscopic surgery), using a natural orifice to gain access to the gut i.e. rectum
Ignored outside Germany until early 1990’ies
Introduced at Good Hope Hospital by Arthur Allan in 1994



Indications and limitations
For excision of rectal tumours up to 18cm from anal verge
Allows full thickness excision and suturing
Adenoma even circumferential
Carcinoma
Carcinoid
GIST

Advantages
Excellent access and binocular view of whole rectum
Sphincters less compromised than using retractors
Constant gas insufflation stable platform
Ability to dissect and suture
Limitations
Anal stenosis
Narrow / rigid rectum
Fixed rectosigmoid jct
Lesion out of reach

TEM and rectal cancer
For cure: low risk T1 ca: G1/G2 SM1 ?SM2
For compromise: high risk T1/T2 with (chemo)radiation possibly cure
For palliation: T3 with (chemo)radiation
Unresolved:
?accurate preop staging
?when to add preop DXR/chemorad
Pathway
Referral > Assessment plus ERUS
Review of staging plus histology at MDT
If low risk / benign: TEMS
If high risk / not suitable; refer back
Review TEMS histology at MDT
If high risk, discuss standard surgery

Why local excision
It’s fun!
And it’s beautiful!

Complications/pitfalls
Bleeding
Perforation/dehiscence
Rectal stricture
Urinary retention
Impaired continence
Recurrence

How to refer
Via network proforma MDT coordinator
E-mail / fax / phone call
Letter in the post takes a long time!
Fax: 0121 4249548 (surgical secretaries)
E-mail: [email protected]
Mobile: 07801 654781
Try to see within the week
Problem patients a little local excision gone wrong

K.W. 42F
Soiling of mesorectum
Settled with i.v. antibiotics

M.S. 80y F
Faecal impaction in mesorectum (ypT3)
Patient died from sepsis

H.M. 80y M Soiling of mesorectum (ypT1)
Wound breakdown > fistula into seminal vesicle 2 months later
Settled with defunctioning colostomy
Videos

Gerhard Buess teaching video

Rectal cancer pT2
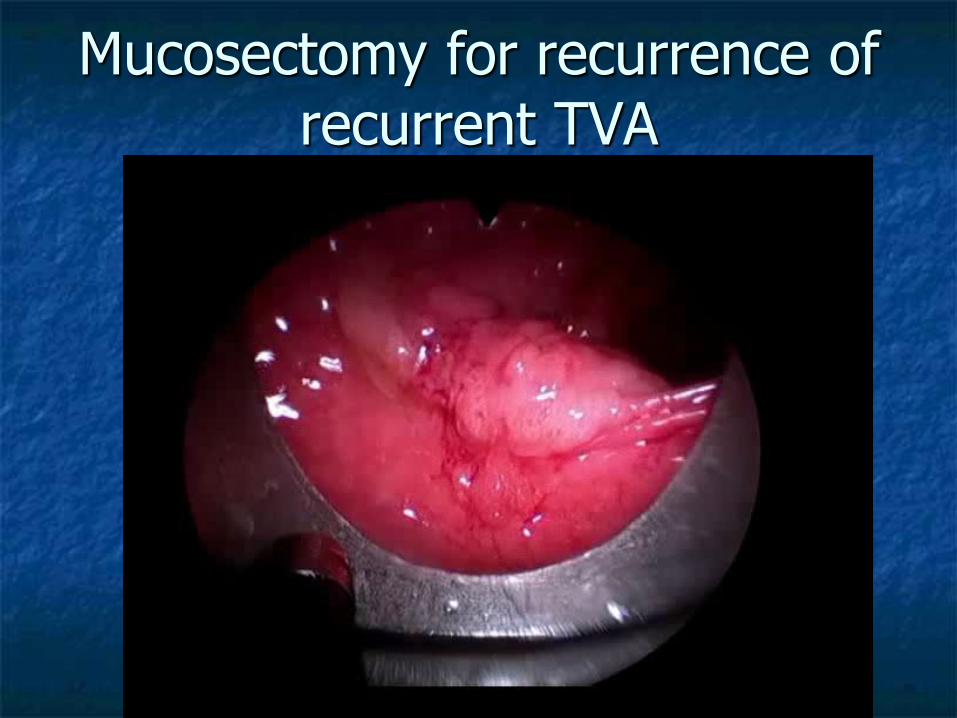
Mucosectomy for recurrence of recurrent TVA

pT1SM1
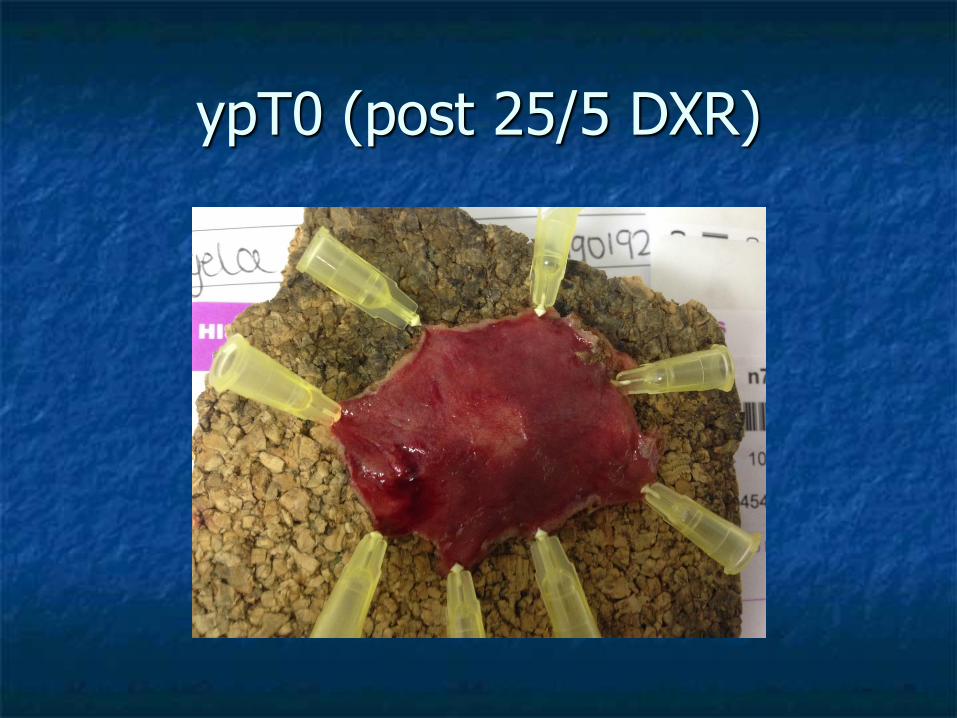
ypT0 (post 25/5 DXR)

yPt3

pT1SM2

TVA HGD

TVA LGD

Take care:
Start with small benign lesions
Can you close the defect if peritoneum is opened?
Can you safely perform further surgery if malignancy dictates so?

Rectal cancer treated with TEMS at GHH 1995 - 2012
154 patients (93 men):
91 without DXR
38 short course DXR
17 long course chemoradiation
8 post op DXR

No preop DXR (91)
59 pT1:
16 after prev. polyp cancer: no residual ca
33 favourable histology: no further treatment
2 local recurrences (11-51m); 1 salvage, 1 too frail
2 incompletely excised (too high): too frail for resection
8 poor prognostic features > radical resection: no recurrences, no mets

No preop DXR (91)
30 pT2:
18 radical surgery:
2 lung mets (2-18m) > 1 resected
12 too frail for radical surgery:
5 died unrelated (3-25m)
1 local recurrence (4m), 2 metastases (3-11m)> died
4 alive and well
2 pT3: radical surgery: alive and well
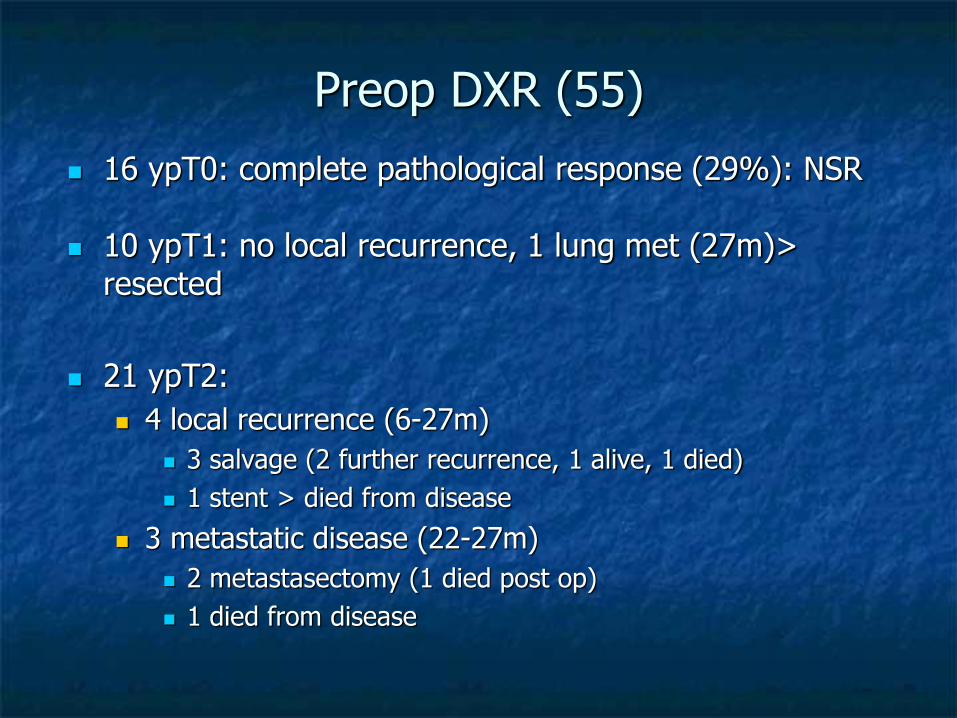
Preop DXR (55)
16 ypT0: complete pathological response (29%): NSR
10 ypT1: no local recurrence, 1 lung met (27m)> resected
21 ypT2:
4 local recurrence (6-27m)
3 salvage (2 further recurrence, 1 alive, 1 died)
1 stent > died from disease
3 metastatic disease (22-27m)
2 metastasectomy (1 died post op)
1 died from disease

Preop DXR (55)
8 ypT3:
2 radical surgery: one disease free, one died from metastatic disease (no LR)
1 died post op (day 11)
2 local recurrence (7-18m)> 1 salvage APR, 1 died
1 died metastatic disease (2m)
1 died unrelated (9m)
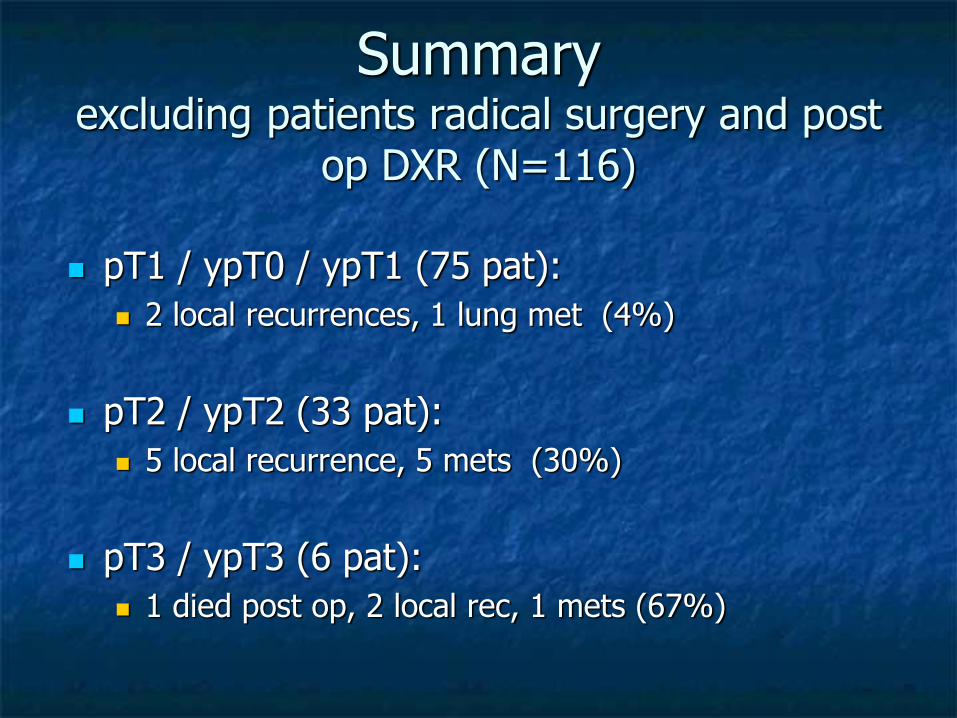
Summary excluding patients radical surgery and post
op DXR (N=116)
pT1 / ypT0 / ypT1 (75 pat):
2 local recurrences, 1 lung met (4%)
pT2 / ypT2 (33 pat):
5 local recurrence, 5 mets (30%)
pT3 / ypT3 (6 pat):
1 died post op, 2 local rec, 1 mets (67%)


















