
Temporomandibular disorders among Sami women745766/FULLTEXT01.pdf · Temporomandibular disorders...
100
Temporomandibular disorders among Sami women Perspectives based on an epidemiological survey with mixed methods Christina Storm Mienna Department of Odontology Umeå 2014
Transcript of Temporomandibular disorders among Sami women745766/FULLTEXT01.pdf · Temporomandibular disorders...

Temporomandibular disorders among Sami women Perspectives based on an epidemiological survey with mixed methods
Christina Storm Mienna
Department of Odontology
Umeå 2014
Responsible publisher under Swedish law: the Dean of the Medical Faculty
This work is protected by the Swedish Copyright Legislation (Act 1960:729)
ISBN: 978-91-7601-121-8
ISSN: 0345-7532
©Christina Storm Mienna
Cover photo: Nieidabákti, photographed by Ingrid Storm
Cover pattern: Olav Svonni
Layout: Inhousebyrån, Hans Karlsson
Elektronisk version tillgänglig på http://umu.diva-portal.org/
Printed by: Print & Media
Umeå, Sweden 2014

To Alexander
“Just as the mountain spring flows, so is
life. It is like a river we cannot stop, but
can only try to accept.”
(Quotation from a 48-year-old woman)
”Precis som jokken rinner, så är vårt liv.
Det är liksom ett flöde som vi inte kan
stoppa, utan får försöka acceptera.”
(Citat från kvinna 48 år)

i
Table of Contents
Table of Contents i Abstract iii Abbreviations v Populärvetenskaplig sammanfattning på svenska vi Bealledieđalaš čoahkkáigeassu davvisámegillii viii Original papers x Preface xi Introduction 1
The Sami population 1 Temporomandibular disorders 3 Terminology 3 Classification 4 Etiology 5 Epidemiology 6 Gender differences 7 Co-morbidity 9 Consequences 9 Mixed methods 10 Rationale 12
Aims 13 Study population and methods 14
Study population 15 Methods 20 Questionnaire (Paper I and III) 20 Clinical examination (Paper II) 20 Statistical methods (Papers I-III) 23 Thematic interviews (Paper IV) 24
Results 27 Study population 27 Symptoms indicative of TMD 27 Headaches and neckshoulder pain 29 Disability related to symptoms indicative of TMD 29 Disability related to headaches and neckshoulder pain 30 Co-morbidities 31 Case–control study 32 Thematic interviews 35
Discussion 41 Main findings 41 Study population 41 Methodological considerations 43
ii
Ethical considerations 46 Temporomandibular disorders 49 Casecontrol study 54 Thematic interviews 56
Clinical implications and future perspectives 59 Summary of results 60 Conclusions and generated hypotheses 61 Acknowledgments 62 References 65 Appendix

iii
Abstract
Introduction The aim of the research project was to examine prevalence,
co-morbidity, and impact on daily life of pain and dysfunction in the
jawface, head, and neckshoulder regions among adult Sami women in
northern Sweden. The aim of the qualitative part of the study was to explore,
thoughts, experiences, and beliefs regarding temporomandibular disorders
(TMD) among Sami women with and without TMD, to gain insights into
their health care experiences.
Methods The research project used a mixed methods approach including
questionnaire analysis, a casecontrol study, and thematic interviews. The
study population (Papers I and III) included 487 women living in the Arctic
region of northern Sweden and enrolled in the register of the Swedish Sami
Parliament or registered as reindeer owners or reindeer herders in the
Swedish Board of Agriculture. Two years after the questionnaire study, 22
women (cases) with longstanding, intense, and frequent symptoms
indicative of TMD, together with 46 age-matched women (controls) without
any symptoms in the jaw–face region, underwent a clinical examination of
the function of the temporomandibular joint, jaw- and neck muscles,
mandibular mobility, and dental occlusion. The examiner was blind to the
women’s affiliation (Paper II). Thematic interviews with a strategic
subsample of 17 Sami women (Paper IV) were thereafter conducted and
analyzed with a grounded theory approach.
Results The prevalence of frequent symptoms indicative of TMD was 17%,
of headaches 19%, and of neckshoulder pain (NSP) 30%. Seventeen percent
reported that their TMD affected daily life. Duration of jaw pain,
troublesome impaired jaw opening, and neck pain, together with a low
education level, affected the statement of whether TMD influenced daily life
or not. Factors related to pain had the greatest influence when these Sami
women rated the related impairment. There was a statistically significant
relationship between TMD, frequent headaches, and frequent NSP (P
<0.0001). Longstanding, intense, and frequent symptoms indicative of TMD
remained essentially unchanged over the two-year follow-up period. Cases
reported impaired general health and awareness of clenching teeth
significantly more frequently than did controls. Variations in dental
occlusion did not distinguish cases from controls. In the qualitative part of
the project the core category, “Grin(d) and bear it,” summarizes the
participants’ various ways and stages of processing and handling the
interacting categories: (1) triggers, (2) strains, (3) distrust, and (4)
reconciliation with pain and/or difficulties in life. Perpetuating factors were

iv
described as mentalphysical strain and stress, and also a tooth clenching
behavior. Women without TMD expressed factors that helped them to
handle strains, reconcile, and stay healthy. They relied on helpful social
support.
Conclusion Disabling TMD, headaches, and NSP are common in Sami
women. Women with TMD commonly expressed that tooth clenching was a
familiar habit related to strains in life; they described an impaired general
state of health and distrust in the care providers’ competence and ability to
manage their problems. Women without TMD expressed confidence in their
self-efficacy and were generally less concerned with strains in their lives.
Rehabilitation strategies aiming at empowerment and improved self-efficacy
may be a successful approach in women with disabling TMD.
Keywords: epidemiology, gender, headache, indigenous, pain, qualitative, quality of life, temporomandibular disorders
v
Abbreviations
ADL activities of daily living
Ai anamnestic dysfunction index
BMI body mass index
CI confidence interval
Di clinical dysfunction index
GT grounded theory
NRS 11-point numerical rating scale
NSP neckshoulder pain
OHRQoL oral health-related quality of life
OR odds ratio
RDC/TMD Research Diagnostic Criteria for Temporomandibular
Disorders
SD standard deviation
TMD temporomandibular disorders
TMJ temporomandibular joint
vi
Populärvetenskaplig sammanfattning på svenska
(Popular science summary in Swedish)
Smärta och funktionsstörningar i käksystemet (eng. temporomandibular
disordersTMD) är vanligt förkommande i befolkningen, och ett
folkhälsoproblem associerat med ökad sjukfrånvaro, vårdkonsumtion och
inverkan på livskvalitet. Kvinnor är i majoritet bland de som drabbas av
långvariga besvär. Syftet med forskningsprojektet var att bland samiska
kvinnor, undersöka förekomst av smärta och funktionsstörningar i
käksystemet, dess samsjuklighet med huvudvärk och smärtor i
nacke/skuldror samt hur symtomen påverkade kvinnornas dagliga
aktiviteter. Studien avsåg även att utforska tankar, erfarenheter och
föreställningar om symtom i käkarna och få en inblick i kvinnornas
erfarenhet av vården av dessa tillstånd. Kvinnorna som inkluderas i studien
var folkbokförda i Kiruna eller Gällivare kommun och registrerade i 1997-års
sametingsröstlängd eller jordbrukverkets företagarregister över
renägare/renskötare. Data insamlades med hjälp av frågeformulär, klinisk
undersökning av käksystemet samt genom tematisk intervju. Totalt
besvarade 487 kvinnor mellan 21 och 70 år, enkäten som fokuserade på
förekomst av symtom från käkar, huvud, nacke/skuldror, hur ofta symtomen
förekom, under hur lång tid de haft dessa samt en skattning av symtomens
intensitet och påverkan på dagliga aktiviteter.
Frekvent (minst en gång i veckan) återkommande smärtor och
funktionsstörningar i käksystemet rapporterades av 17% av deltagarna i
enkätstudien, frekvent återkommande huvudvärk av 19% och smärta från
nacke/skuldror av 30%. Sjutton procent av samtliga kvinnor angav att
symtomen i käkarna påverkade deras dagliga liv negativt, och många av
kvinnorna hade symtom från samtliga undersökta områden, som tecken på
en samsjuklighet för tillstånden. Smärta från käkar hade störst betydelse när
kvinnorna skattade hur symtom från käkarna påverkade deras dagliga
aktiviteter, även nedsatt gapförmåga, smärta i nackregionen och låg
utbildningsnivå var av betydelse.
Alla kvinnor med långvarig, intensiv och frekvent smärta och
funktionsstörning i käksystemet erbjöds en klinisk undersökning 2 år efter
enkätstudien; 22 TMD kvinnor (fall) och 46 åldersmatchade kvinnor
(kontroller) utan några symtom från käkarna deltog. Undersökaren var
blindad dvs. visste inte vilka som var fall eller kontroller. Den kliniska
undersökningen omfattade käkled, käkmuskulatur, käkrörlighet och
bettförhållanden. Fall och kontroller hade likartade bettförhållanden. Fallen

vii
hade högre body mass index (BMI) än kontrollerna. Kvinnorna inom
fallgruppen rapporterade sämre allmän hälsa och högre medvetenhet om
tandpressningsovanor än kontrollerna.
Sjutton kvinnor från den kliniska undersökningen, varav tio kvinnor med
TMD, valdes ut till en tematisk intervju. Intervjuerna fokuserade på tre
teman, det samiska arvet, livserfarenheter, hälsa/ohälsa. Intervjuerna
analyserades med en kvalitativ metodik som kallas grounded theory.
Metoden syftar till att generera hypoteser. Analysen kom fram till
huvudkategorin ”Det är bara att bita ihop”, vilken sammanfattar deltagarnas
olika sätt och stadier av bearbetning och hantering av de samverkande
kategorierna: (1) utlösande faktorer, (2) belastning/spänningar (3)
misstro/misstrodd, och (4) förlikning med smärta och/eller svårigheter i
livet. Vidmakthållande faktorer beskrevs i termer av mentalfysisk
belastning, och stress, samt en vana av att hålla/bita ihop käken. Kvinnorna
utan TMD beskrev faktorer som hjälpte dem att hantera påfrestningar,
förlika sig med besvären, och hålla sig friska. De förlitade sig också på
omgivningens sociala stöd.
Sammanfattningsvis visar avhandlingen att smärta och funktionsstörningar i
käksystemet, huvudvärk och smärta från nacke/skuldror är vanligt
förekommande bland samiska kvinnor. Medvetenhet om tandpressning eller
att hålla ihop käkarna förknippades med belastningar/spänningar i livet,
nedsatt allmän hälsa och med symtom från käkarna. De som intervjuades
och hade symtom ifrån käkarna utryckte misstro mot vårdgivares kompetens
och möjligheter att behandla deras problem i käkarna. De kvinnor som inte
hade symtom uttryckte stark tilltro till sin egen förmåga att klara av
svårigheter och var i allmänhet mindre oroliga för påfrestningar i livet.
Behandlingsinsatser som inkluderar självbestämmande och att stärka
individens tilltro till sin egen förmåga kan vara viktiga delar för
framgångsrik behandling av kvinnor med handikappande smärtor och
käkfunktionsstörningar.

viii
Bealledieđalaš čoahkkáigeassu davvisámegillii
(abstract in North Sami)
Várka ja doaibmahehttejupmi geađaš-oalulvuogádagas (eaŋg. temporo-
mandibular disorders, TMD) lea olbmuid gaskkas dábálaš ja mielddisbuktá
váttuid álbmotdearvvašvuođa dillái ja dasa gullá bargosaji váilevaš
oassálastin, eanet dikšungeavaheapmi ja dat váikkuha olbmuid eallindillái.
Dutkanprošeavtta ulbmil leai sápmelaš nissonolbmuid gaskkas guorahallat
jus lea várka ja doaibmahehttejupmi geađaš-oalulvuogádagas, ja mo dat
doibmet ovttas iežá buohccivuođain dego oaivebákčasiin ja várkkain
niskkis/oalggis ja got dávdamearkkat váikkuhit nissoniid beaivválaš
doaimmaide. Dutkan galggai maiddái iskat jurdagiid, vásáhusaid ja
miellagovaid mat gullet dávdamearkkaide geađaš-oalulvuogádagas ja oažžut
gova nissoniid vásáhusain dikšuma hárrái dan dáfus. Nissonat geat ledje
mielde guorahallamis ledje Girona ja Jiellevári gielddaid álbmotlogus ja ledje
mielde sámedikki 1997 jagi jienastanlogus dahje eanandoallodoaimmahaga
boazodoallofitnodatlogus. Dieđut čohkkejuvvojedje jearahallanskovi bokte,
geađaš-oalulvuogádaga klinihkalaš iskama bokte ja temáhtalaš jearahallama
bokte. Oktiibuot vástidedje 487 nissona geat ledje gaskal 21 ja 70 jagi
boarrásat jearahallanskovi jearaldagaide, mas váldojearaldahkan ledje
dávdamearkkat geađaš-olloliin, oaivvis, niskkis/oalggis, man dávjá dovde
daid mearkkaid, ja man guhká dat ledje leamaš sis ja sin meroštallama
makkár váivvádusdássi leai ja mo dávdamearkkat váikkuhedje sin beaivválaš
doaimmaide.
Várka ja doaibmahehttejupmi mii dáhpáhuvai dávjá geađaš-oalulvuogádagas
(unnimusat oktii vahkus) leai 17 % sis geat oassálastet jearahallan-
guorahallamis. Dávjjes oaivebákčasa dieđihedje 19% ja várkka niskkis/
oalggis 30 %. Čiežanuppelohkái proseanta oppa nissonjoavkkus dieđihedje
ahte dávdamearkkat geađaš-oalulvuogádagas váikkuhedje sin beaivválaš
eallima negatiivvalaččat. Olu nissonat dieđihedje dávdamearkkaid juohke
guorahallojuvvon oasis, mii mearkkaša ahte buohccivuođat doibmet
oktasaččat. Várka olloliin leai deaŧaleamus go sii meroštallet mii dávda-
mearkkaid váikkuhii eanamusat sin beaivválaš doaimmaide, muhto
mearkkašupmi leai maiddái jus sis leai váilevaš njálmmi cakkastandássi,
várka niskkis/oalggis ja vuollegis oahpahusdássi. Visot nissonat geain leai
guhkálaš, garra ja dávjjes várka ja doaibmahehttejupmi geađaš-
oalulvuogádagas bovdejuvvojedje klinihkalaš guorahallamii 2 jagi maŋŋel
jearahallanguorahallama: 22 TMD nissona (ášši) ja 46 nissona geat ledje
seamma agis ja geain eai lean dávdamearkkat geađaš-oalulvuogádagas
(buohtastahtti) oassálaste.

ix
Guorahalli ieš leai diehtemeahttun goappá jovkui visses nisson gulai.
Klinihkalaš guorahallamii gulle geađaš-oalullađđasat, geađaš-oaluldeahkit,
geađaš-oalullihkadeapmi ja gáskinvejolašvuođat. Gáskinvejolašvuođat ledje
seammalágánat ášši- ja buohtastahtti-joavkkus. Nissoniin ášši-joavkkus leai
alit BMI (Body Mass Index) go buohtastahtti-joavkkus. Nissonat geat gulle
ášši-jovkui dieđihedje heajut almmolaš dearvvašvuođa ja alit diđolašvuođa
heajos bátnegaskindábiid birra go buohtastahtti-joavkku nissonat.
Čiežanuppelohkái nissona klinihkalaš guorahallamis, ja dan joavkkus logis
geas leai TMD, válljejuvvojedje njálmmálaš jearahallamii. Jearahallamiin
biddjojuvvui deaddu golmma fáddái, sápmelaš árbedillái, eallinvásáhusaide
ja (váilevaš) dearvvašvuhtii. Jearahallamat analyserejuvvojedje kvalitatiivva
vuogi mielde (mii gohčoduvvo eaŋgalasgillii Grounded theory), man vuogi
mielde sáhttá ráhkadit hypotesaid. Analiissa gávnnahii čuovvovaš
váldokategoriija “Ii leat iežá go doallat njálmmi čavga gitta (ja gierdat)”, mii
čoahkkáigeassá oasseváldiid sierralágán vugiid ja dásiid got meannudedje ja
gieđahalle oktiigullevaš kategoriijaid: (1) dili álggaheaddji (2) deaddu/
gealdagat (3) eahpeluohttámuš ja (4) várkka ja/dahje eallima váigatvuođaid
gierdan. Dili doalaheaddji fáktorat dieđihuvvojedje leat mentála-fysalaš
deaddu ja streassa, ja maiddái dáhpi gaskit/doallat njálmmi čavga gitta.
Nissoniin geain ii lean TMD dieđihedje fáktoriid mat veahkehit sin gierdat
váigatvuođaid, soabadit váivviin, ja bissut dearvvašin. Sii dorvvastedje
maiddái lagasolbmuid sosiála doarjagii.
Oppalaččat čájeha nákkosgirji ahte várka ja doaibmahehttejupmi geađaš-
oalulvuogádagas, oaivebávččas ja várka niskkis/oalggis lea dábálaš dilli
sápmelaš nissoniid gaskkas. Diđolašvuohta doallat bániid oktii dahje doallat
njálmmi čavga gitta mielddisbuvttii deattu/gealdagiid eallimii, váilevaš
almmolaš dearvvašvuođa ja dávdamearkkaid geađaš-oalulvuogádagas. Sii
guđet jearahallojuvvojedje ja geain ledje dávdamearkkat geađaš-
oalulvuogádagas dieđihedje eahpeluohttámuša sidjiide guđet doaimmahedje
dikšuma sin gelbbolašvuođa geažil ja eahpidedje maiddái sin vejolašvuođa
meannudit sin buohccedili. Nissonat geain eai lean dávdamearkkat
dieđihedje garra luohttámuša sin iežaset návccaide čoavdit sin iežaset
váttisvuođaid ja sis leai unnit ballu oažžut váttuid.
Dikšunstrategiijat mat siskkildit iešmearrideami ja mat nannejit oktonas
olbmo jáhku iežas návccaide sáhttet leat deaŧalaš oasit buori
buohccedikšumis nissoniidda geain leat várkkat mat hehttejit sin doaimmaid
ja váilevaš geađaš-oalulvuogádatdoaimmat.
Translation: Professor Mikael Svonni, UiT, The Arctic University of Norway

x
Original papers
This doctoral thesis is based on the following original papers, which will be
referred to in the text by their Roman numerals:
I. Storm C, Wänman A. Temporomandibular disorders, headaches and
neckshoulder pain among females in a Sami population. Acta Odontol
Scand 2006; 64: 319-325.
II. Storm C, Wänman A. A two-year follow-up study of temporomandibular
disorders in a female Sami population: validation of cases and controls as
predicted by questionnaire. Acta Odontol Scand 2007; 65: 341-347.
III. Mienna CS, Wänman A. Self-reported impact on daily life activities
related to temporomandibular disorders, headaches and neck-shoulder pain
among women in a Sami population living in northern Sweden. J Orofac
Pain 2012; 26: 215-224.
IV. Mienna CS, Johansson EE, Wänman A. “Grin(d) and bear it”- Narratives
from Sami women with and without temporomandibular disorders. A
qualitative study. J Orofac Pain & Headaches 2014; 28: 243-251.
The papers are reprinted with the kind permission of the publishers; Informa Healthcare, London (papers I and II), and Quintessence Publishing Company Inc, Chicago (papers III and IV).

xi
Preface
As I recall, it was a warm and sunny Easter day. I was resting on a reindeer
skin, in a snowdrift; a fire crackled, and my thoughts happened to be in the
deep woods surrounding Lake Inari in Finland. I had a break in the middle
of the 5th semester of my dental education, and my teacher in clinical oral
physiology had sent me off with a thesis, so I had “something to do during
the Easter holidays,” since the curriculum did not have any leisure, but “time
to read.” So far, it had been the most interesting course in the dental
program, and although I was still not sure about the choice of dental career,
this was while sitting on that reindeer skin that I decided to continue on with
the program. It was time to decide on a graduation project, and I believe the
teacher thought that the Helkimo study on Skolt and Inari Samis in Finland
would inspire me, since I was Sami myself. I had previously studied Sami
culture, history, and language at the University, and thought it might be a
suitable project, combining my choice of occupation with a project within a
Sami context. Easter was celebrated as usual, up in the mountains, at the
finest place I know, Rautasjaure, the birthplace of my grandparents and
ancestors. Like the Sami women who came to participate in my research, I
gather strength and energy in a place far away from modernity, such as
electricity, running water, and mobile phone coverage. Perhaps it is my Sami
heritage that raises my longing to be away from civilization at some point
every year, to find peace of mind.
Being able to finish this PhD has at times felt quite impossible, because of ill
health, which meant long periods of sick leave. Many times I have thought
that I wouldn’t manage to complete the project, but the work of this thesis
has often been a great way to dispel those thoughts, when life has been extra
tough. Illness sometimes leads to other perspectives, and I thought a lot
during those periods about how I wanted my career to develop. I decided to
study further to become a specialist in clinical oral physiology. Thus, any
interruption in the PhD program, I cannot ascribe to illness. There were also
positive events such as the three-year specialist training, and the biggest and
best event in my life, becoming a mother. I took as much maternal leave as I
possibly could.
My research started with questions about the prevalence of temporo-
mandibular disorders (TMD) in the Sami population, since the prevalence
was high in the Helkimo study compared to that of other populations.
Another perspective was related to the question why women dominate as
patients referred for treatment. Today, these patients constitute my everyday
life as a specialist. Combining the quantitative study with a qualitative
xii
approach made it possible to obtain a deeper knowledge of individuals’
experiences, in my wish to find reasons why women are more affected by
TMD than men. I believe that the answer is complex and may be found in the
biopsychosocial model. Our social context probably has a greater significance
for the way we handle things than we normally realize. Perspectives on a
condition may be widened when quantitative and qualitative research
methods are combined. In my opinion, one method is not better or worse
than the other; rather, they should be seen as complementary to each other,
and it has been educational to use both.
The cover photo is from my paradise, Rautasjaure, the mountain called
”nieidabákti” (girl mountain).
Morgonen därpå stack vi över sjön till Rimakalles sten, ett stort flyttblock,
som det inte var något annat märkvärdigt med än att jätten skulle ha
legat på den. Men vi kom rakt under Neitapaktes stup, och det var något
värt. Mästaren hade huggit hårt med mejseln däruppe; det var skarpa
drag och djupa fåror. Medan båten gled fram under stupet, undrade Lill,
varför dom kallat fjället just Neitapakte. Neita betydde ju flicka, men inte
var den där hemska bergväggen just flickaktigt. –Uppifrån fjället där vi
vaktar renarna, ser det ut på ett annat vis, svarade Lars Hova och
rodnade lätt. På vad vis då? Lars Hova hade svårt att komma fram med
svaret. Keinil log stilla, och när det äntligen blev klart, att fjällkonturen
däruppifrån påminde renskötarna om konturen av en flicka under
koltbarmen, då smittade unge Hovas rodnad av sig på den som frågade.
~ Ur boken Bortom fjällen av Ernst Manker, 1957
I hope you will enjoy this reading as much I have enjoyed writing it.
Umeå, September 2014
Christina Storm Mienna

INTRODUCTION
1
Introduction
The Sami population
The Samis are the Indigenous people in Sweden, Norway, Finland, and Kola
Peninsula in Russia. In 1977, the Swedish Parliament recognized the
indigenous status of the Sami. Since 2011 the Sami are recognized as a
people in the Swedish constitution. The Sami people have historically lived
in the region called Sápmi (Samiland), which overlaps the borders of four
nations (Figure 1).
Figure 1: Map of Sápmi. Reprinted and adjusted with permission from Nordiska museet, Stockholm.
Studies of genetic markers in the Sami people over four decades have shown
that they are genetically unique compared to other populations studied
(Beckman 1996). The relatively homogeneous genetic composition of the
Samis, combined with a shared cultural heritage, make them suitable for
studies related to development of diseases with a multifactorial background
(Johansson et al. 2005).
A detailed census of the Sami people has not taken place, as ethnic markers
are forbidden in national population registers, as regulated by Swedish laws.
It is estimated that there are about 85 000 Samis altogether, of whom
approximately 20 000 live in Sweden and of whom 2500 work full-time with
reindeer herding (Solbakk 2006). However, the Sami population in Sweden
may consist of as many as 40 00050 000 individuals, according to a
INTRODUCTION
2
constructed database on health and living conditions (Hassler et al. 2004a).
About 50% of the total Sami population in Sweden lives in the northernmost
county, Norrbotten (Sjölander 2011). For the Sami people, reindeer herding,
fishing, hunting, and handicrafts were historically traditional ways of life
(Solbakk 2006). Today most Sami participate as an integrated part in
various professions and economic activities in society. They have been
assimilated into a western lifestyle and thereby share the accompanying
diseases (Hassler et al. 2005).
Knowledge of the Sami health situation in Sweden is fairly limited, but
during the last decade several studies mainly based on data from national
registers, have been published. The Southern Lapland Research Department
in Vilhelmina has accounted for improvements in the knowledge of the Sami
people’s health situation in Sweden. Despite these efforts, Sweden is still far
behind Norway, where governmental resources have been allocated for
research on the health situation of their Indigenous people, the Samis. In
2007, the United Nations special rapporteur Paul Hunt (Hunt 2007)
recommended that the Swedish government support the establishment of a
Sami Health research centre, as in Norway; he also suggested that the
Swedish government should “consider establishing a body within the
Ministry of Health with national responsibility for oversight of Sami health”.
Hitherto, no such unit has been established in Sweden. During 2013
Västerbotten County Council applied to the Swedish government to start a
national Sami Healthcare center. If this becomes reality, related resources
may help to conduct further research on the Sami population’s health
conditions.
In general terms the health and living conditions of the Samis, in comparison
with other Indigenous peoples (Sjölander 2011), seem to be good and
essentially similar to that of the Swedish general population. Some
differences have nevertheless been observed. Cancer is the disease that has
been most thoroughly studied in the Sami population (Sjölander 2011). The
risk of developing and dying from cancer was lower among the Sami
compared to general populations in Norway, Sweden, and Finland. Plausible
explanations were lifestyle-related factors, including dietary components and
physical activity (Hassler et al. 2008a, Hassler et al. 2008b). Gender
differences in cardiovascular disease among the Sami have been reported.
Sami women showed an increased risk for mortality from subarachnoid
haemorrhage and ischemic heart diseases (Hassler et al. 2005). Among
women from reindeer-herding families, and for Sami men not involving in
reindeer herding, an increased risk of stroke has been reported. The
incidence of stroke was significantly increased for both Sami men and
women who had adopted a more westernized lifestyle (Sjölander et al.

INTRODUCTION
3
2008b). Sami women, particular those of reindeer-breeding families, were
more exposed than men to psychosocial risk factors, such as lower decision-
making latitude, social support, and intellectual discretion. Differences in
exposure to behavioral and biomedical risk factors can partly account for the
gender difference between Sami men and women (Edin-Liljegren et al.
2004). Musculoskeletal symptoms have been highly observed among both
men and women in reindeer-herding families. In men, the use of terrain
vehicles was the main cause (Daerga et al. 2004, Näyhä et al. 1991, Sjölander
et al. 2008a), with a higher risk for fatal accidents (Hassler et al. 2004b). In
women, on the other hand, the musculoskeletal symptoms seemed to be
related to psychosocial factors such as poor social support, high effort, low
reward, and high financial responsibilities.
Temporomandibular disorders
Terminology
The jaw system is essential for survival, and is involved in basic functions
such as mastication, biting, tasting, swallowing, respiration, and speech.
These functions engage the mandible, the teeth, the tongue, the cheeks, the
temporomandibular joint (TMJ), the skull, the upper part of the spinal
column, the jaw-and neck muscles, the salivary glands, the nervous system,
and blood supply. A disturbance in any of these parts may thus affect the
functions of the jaw system and the quality of life.
In 1934, an otolaryngologist, Dr. James Costen (Costen 1934), described
symptoms from around the ear and the temporomandibular joint, which he
attributed to the dental occlusion; the term Costen’s syndrome was coined.
Different ways to designate functional disturbances of the masticatory
system have since been advocated; temporomandibular joint dysfunction
syndrome, occlusomandibular disturbances, myoarthropathy of the
temporomandibular joint, myofascial pain dysfunction syndrome,
temporomandibular pain dysfunction syndrome, mandibular dysfunction,
internal derangements of the temporomandibular joint, and so on. The
different terms describe various views of the possible origin and main feature
of the condition; some focus on dysfunction and others emphasize pain.
These terms were in the 1980s included under the broader concept
craniomandibular disorders, and from the 1990s onwards the most
commonly used expression in the literature is temporomandibular disorders
(Okeson 2008).

INTRODUCTION
4
Temporomandibular disorders (TMD) is a collective term embracing a
cluster of related disorders in the masticatory system, with common
symptoms (Drangsholt and LeResche 1999) and clinical problems involving
muscles, the TMJ, the occlusion, the nervous system, and associated
structures (de Leeuw 2008). In 1983, the American Dental Association,
(Drangsholt and LeResche 1999) characterized TMD as a condition with pain
in the TMJ region and/or in the jaw muscles during function, limitation in
mandibular range of motion and/or TMJ sounds during jaw function. TMD
can be regarded as musculoskeletal disorders in the jawface region, since it
resembles other musculoskeletal disorders and chronic pain conditions.
Classification
Different systems have been advocated over the years to classify signs and
symptoms of TMD in attempts to systematically standardize definitions for
classifying or stating a diagnosis of TMD conditions (Fricton and Schiffman
1986, Lundeen et al. 1986, Dworkin and LeResche 1992,). In my doctoral
thesis two models for classification of TMD were used; the anamnestic (Ai)
and clinical dysfunction (Di) indices as devised by Helkimo (Helkimo 1974b)
and the Research Diagnostic Criteria for Temporomandibular Disorders
(RDC/TMD) (Dworkin and LeResche 1992). The anamnestic dysfunction
index was developed to classify reported symptoms in three grades based on
expected severity: Ai 0 = symptom-free, Ai I = mild symptoms (jaw tiredness
and TMJ sounds), and A II = severe symptoms (TMJ locking, difficulties in
opening wide and jaw pain). The clinical dysfunction index was based on the
outcome of a clinical examination that measures range of mandibular
movement, function of the temporomandibular joint, presence of pain on
movements of the mandible, presence of muscle pain, and/or
temporomandibular joint pain to palpation. Each variable examined is
scored on three levels of severity based on defined criteria: no signs of
dysfunction (0 points), mild signs of dysfunction (1 point), and severe signs
0f dysfunction (5 points). The sum of the scores can thus range from 0 to 25
points. The index is constructed as an ordinal scale in four grades of severity:
no signs of dysfunction (Di 0), mild signs of dysfunction (14 points, Di I),
moderate signs of dysfunction (59 points, Di II), and severe signs of
dysfunction (1025 points, Di III).
RDC/TMD was developed for clinical and epidemiological research purposes
to provide standardized diagnostic classifications of the most common TMD
conditions (Dworkin and LeResche 1992). Axis I is a non-hierarchical
diagnostic scheme, and a condition can be diagnosed into one of three main
groups: (1) muscle disorders (2) disc displacements, and (3) arthralgia,
arthritis, and arthrosis. The RDC/TMD Axis II classification system included

INTRODUCTION
5
pain-related disability and psychological status (Dworkin and LeResche
1992). The classification system has recently been revised to Diagnostic
Criteria of TMD (DC/TMD), aimed for clinical use (Schiffman et al. 2014).
Etiology
The etiology of TMD is complex and, multifactorial, and has been debated
over the years. One more recently advocated perspective is summarized in a
biopsychosocial model (Suvinen et al. 2005). Parker presented in 1990 a
dynamic model to depict the etiology. He proposed that there was a balance
in the masticatory system between destructive, overloading factors and
adaptive factors. Factors such as trauma, health/nutrition, the
musculoskeletal structure, coping strategies, and gender might increase or
decrease a patient’s adaptability. Life stressors, sleep disorders,
pain/depression, occlusion, and posture were proposed as predisposing
factors to dysfunction (Parker 1990).
Structural damage of the TMJ has also been proposed, because it changes
physical properties and may alter the ability to withstand loading forces
(Stegenga et al. 1991). In a similar perspective on the etiology of TMD, the
balance between load and capacity of the involved structures has been
advocated (Wänman and Agerberg 1991). Since no single factor has been
identified as a sufficient or necessary etiological factor, it may be more
relevant to describe them as contributing factors (De Boever and Carlsson
1994). These contributing factors have been classified as predisposing,
initiating, and perpetuating. Those that increase the risk of developing TMD
are regarded as predisposing factors, and it has been proposed that they be
subdivided into systemic (e.g. inflammatory or degenerative diseases);
psychological, such as personality, behavior, and mood disturbances; and
structural, such as different types of occlusal discrepancies and joint laxity.
Initiation factors are those that induce onset of TMD, and such proposed
factors are micro and macro trauma, and adverse or excessive loading of
joint structures, including parafunctions such as bruxism (De Boever and
Carlsson 1994). Factors that interfere with healing or enhance the
progression of TMD are referred to as perpetuating factors, which may be
divided into local (parafunctions and posture) and systemic such as
behavioral, social, emotional and cognitive factors (De Boever and Carlsson
1994, Okeson 2008). Occlusal factors, such as mandibular instability, and
cross bite have been reported as possible candidates in relation to
perpetuation of TMD (Kirveskari and Alanen 1984, De Boever et al. 2000,
Marklund and Wänman 2010a). Conflicting results exist regarding the
importance of dental occlusion in relation to the etiology of TMD. In a review
(Türp and Schindler 2012), bruxism, loss of posterior support, and unilateral

INTRODUCTION
6
posterior cross bite showed some possible relationship to TMD, but the
authors also pointed out that disturbances in the occlusion may be a
consequence of TMD and not its cause. In a recent study, the authors
concluded that malocclusion and loss of five or more posterior teeth did not
contribute to TMD (Sousa et al. 2014).
It is likely that many conditions can affect the function of the jaw system and
the individual response also depends on several factors that make research
in etiology both difficult and demanding.
Epidemiology
Epidemiological methods can be used to identify how common a condition is
in a population as well as its natural course if it is left untreated, and to
assess risk factors for onset and perpetuation. Cross-sectional studies based
on representative samples of a population are usually conducted to
determine the prevalence of the problem in focus. Prevalence is defined as
the number of persons with the condition at a specific time divided by the
total size of that population. Knowledge of the prevalence can help to
determine the magnitude of a health problem and its burden on the
individual and the society (Drangsholt and LeResche 1999).
Early clinical studies of TMD indicated that it is a common, heterogeneous
pain disorder, primarily afflicting women aged 2045 years (Helkimo 1976).
In 1972, the first epidemiological study of dysfunction of the masticatory
system was published (Helkimo et al. 1972). Helkimo performed a cross-
sectional study on 245 Skolt- and 76 Inari-Lapps in the north of Finland and
used the Ai and Di indices for descriptive purposes (Helkimo 1974b). He
observed that signs and symptoms of mandibular dysfunction were common
in this Sami population; 88% had one or more signs and 57% had symptoms
of mandibular dysfunction. He estimated that approximately 25% of this
population had need for treatment, since 22% had severe signs and 26% had
severe symptoms according to the indices (Helkimo 1974a). Despite a large
number of subsequent studies in different populations, none has since
reached the high prevalence found in Helkimo’s study on a Sami population
in Finland. Partly from this perspective it was interesting to conduct a new
study on a Sami population.
The prevalence of TMD signs and symptoms varies, depending on
methodology and population (Nydell et al. 1994). A review from 1984,
arrived at a median value of one out of three for TMD symptoms and two out
of three for TMD signs and found a large variation between different studies
(Carlsson 1984). The prevalence of TMD symptoms was 20% and 50% had

INTRODUCTION
7
TMD signs in a Dutch population (De Kanter et al. 1993). Salonen et al.
reported similar results based on a Swedish population (Salonen et al. 1990).
Jagger et al. reported a prevalence of TMD in an indigenous Ecuadorian
population similar to that of Scandinavian samples (Jagger et al. 2004). An
increase in prevalence of symptoms indicative of TMD during a 20-year
period has been observed (Anastassaki et al. 2012). It has been proposed that
psychosocial health determinants are involved in the observed time trend
(Anastassaki and Magnusson 2004). In a review of TMD pain, approximately
one out of three adults was predicted to develop TMD pain during their
lifetime (Drangsholt and LeResche 1999).
The prevalence of severe TMD symptoms is rare in young individuals
(Anastassaki et al. 2009), but increases during the adolescent period
(Nilsson et al. 2009). Longitudinal studies have shown that both signs and
symptoms of TMD fluctuate over time (Magnusson et al. 1985, Wänman
1987, Könönen and Nyström 1993, Marklund and Wänman 2010a). Several
population-based studies on TMD pain and headaches have observed a
declining prevalence with age (Salonen et al. 1990, Österberg and Carlsson
2007, Carlsson et al. 2014,), with older individuals reporting TMD symptoms
less often than younger ones. The reason behind this observation is not
known. In a sample of 90-year-olds, signs and symptoms of TMD were
predominately of mild character and infrequent, except for TMJ crepitation
(Tzakis et al. 1994). In a cross-sectional study including 70- and 80-year-
olds, 6-10%, reported some, and 1-2% rather great or severe problems of
TMD pain (Carlsson et al. 2014). TMD symptoms were also rarely reported
among another sample of 70-year-olds (Österberg and Carlsson 2007). In a
recent population-based study the prevalence of frequent symptoms
indicative of TMD peaked among 50-year-old women and then declined in
the more elderly women (Yekkalam and Wänman 2014a). Johansson et al.,
on the other hand, reported no differences in prevalence of TMD symptoms
between 50 and 60 years of age in a 10-year follow-up study (Johansson et
al. 2003).
Gender differences
It has generally been reported that women have more signs and symptoms of
TMD than men, but no major difference in the prevalence of mandibular
dysfunction was found between men and women in the Sami population in
northern Finland. Only a few symptoms differed in prevalence with gender,
with significantly higher prevalence of headache, NSP and feelings of fatigue
in the jaws in Sami women (Helkimo 1974c).

INTRODUCTION
8
Cross-sectional studies on samples from general populations have found
varying proportions of men and women relative to prevalence of TMD. One
reason may be related to inclusion criteria of symptomstheir frequency,
intensity, and duration. Among patients with TMD, women outnumber men,
with more women seeking treatment and being referred to consultants. For
referrals to specialist TMD clinics, commonly reported ratios of women-to-
men are 3:1, and the majority of patients are between 20 and 40 years of age
(Anastassaki and Magnusson 2004). In a sample drawn from the general
population, 50-year-old women reported significant higher prevalence of
symptoms indicative of TMD than men of the same age, no gender
differences were found in 65- to 75-year-olds (Yekkalam and Wänman
2014a). In a prospective study over approximately 10 years, women showed a
longer duration of TMD symptoms compared to men (Wänman 1996).
Different courses of TMD symptoms between men and women indicate that
women may be less likely to recover from these conditions, although
fluctuations of symptoms occurred among both men and women during the
observation period. Other differences in the TMD symptom’s quality, such as
its frequency, intensity, and effect on quality of life, may also be factors of
importance related to utilization of health care.
Sex-related differences have been observed in both clinical and
experimentally induced pain studies (Fillingim 2000). In a review, of gender
variations in pain experience (Unruh 1996), it was suggested that women are
more likely than men to experience a variety of recurrent pains. Women
report more severe pain levels, more frequent pain, and pain of longer
duration than men do. Women may also be at greater risk for pain-related
disability than men. Gender variation in coping strategies was also found. It
has been suggested that women develop coping strategies that include active
behavioral and cognitive coping, avoidance, emotion-focused coping, seeking
social support, relaxation, and distraction. Men instead seem to use
strategies including talking problems down, denial, looking on the bright
side of life, and tension-reducing activities such as alcohol consumption,
smoking, and drug abuse. Gender differences in brain chemistry,
metabolism, physical structures, and hormone variations may influence the
biological mechanisms of pain transmission, sensitivity, and perception.
Sociological and psychological factors, culture, and ethnicity may also
influence pain perception and behavior. Women with multiple
responsibilities such as childcare, household management, and full or part-
time employment may have more than one reason to apprehend pain as a
threatening condition. Men may perceive pain as being of limited
importance unless it interferes with their work. These factors may be
important in understanding pain and disability in a population, and since
there may be gender-related influences of TMD, it has been proposed that

INTRODUCTION
9
men and women should be studied separately in research of contributing
factors to TMD (Wänman 1996, Henrikson 1999,). Women and men may
also differ in their recovery from pain and may therefore require different
interventions (Unruh 1996).
Co-morbidity
Several studies have demonstrated co-morbidity between TMD, headaches,
NSP, and back pain. (Schokker et al. 1990, Ciancaglini and Radaelli 2001,
Visscher et al. 2001b, Rantala et al. 2003, Wiesinger et al. 2007,). Headache
is a common condition in the population and has been associated with signs
and symptoms of TMD (Wänman and Agerberg 1987, Cooper and Kleinberg
2009, Marklund et al. 2014,). Headaches are more commonly reported by
women than by men after childhood (Rasmussen et al. 1991). There is a
relationship between TMD and muscle tenderness. In an epidemiological
study of 35-year-olds the subjects were grouped according to patterns of
muscle pain to palpation. Those who had tender sites to palpation at both
neck and jaw muscles, together with those who showed a pattern of more
generalized hyperalgesia, had significantly higher prevalence of signs and
symptoms of TMD than other groups (Wänman 1995). In addition to the
relationship between pain in jaw and neck muscles, there is also a functional
relationship between these regions. Thus, during jaw function such as
opening and closing, an integrated pattern between the jaw and head
movements has been observed (Eriksson et al. 1998, Eriksson et al. 2000).
Individuals with symptoms of TMD have also in several studies reported
impaired general health status (Agerberg and Carlsson 1975, Johansson et al.
2004, Österberg and Carlsson 2007, Carlsson et al. 2014). Central and
peripheral sensitization mechanisms are involved in pain perception (Sarlani
et al. 2004) and may induce spread of pain to the jawface area from other
regions, such as back, chest, and stomach. (John et al. 2003). Stimulation of
either the trigeminal or the spinal area affects the other, as has been shown
in experimental pain studies (Hellström et al. 2000, Komiyama et al. 2005).
Taken together, these findings indicate that pain and dysfunction in the jaws,
head, neck, and shoulders may influence each other and/or share the same
contributing factors.
Consequences
It has been proposed that TMD pain is related to social factors such as
unemployment and decreased work effectiveness (Drangsholt and LeResche
1999), and that individuals with chronic TMD pain had burdens, for society
and the individual, similar to those of people with back pain, severe
headache, and chest and abdominal pain, including psychological distress

INTRODUCTION
10
and, economic costs for society and the patient (Drangsholt and LeResche
1999). Other studies have shown negative consequences for individuals, such
as having spent a lot of money for treatment, or lost their jobs, and even
their houses and belongings (Garro et al. 1994). The costs for society due to
TMD pain include costs of providing care and costs associated with work loss
and decreased productivity of work. In a study from Finland a sample, drawn
from keyboard operators in an industry with NSP, were randomly referred to
either a treatment or a non-treatment group. The treatment was directed
towards stabilization of the mandible, with selective tooth grinding, and in
some cases, bite-splints. Both groups averaged 33 days of sick leave the year
before the study started. One year after, the treatment group showed an
average reduction of 11 days, while the non-treatment group had a slight
increase of sick-leave days (Kirveskari and Alanen 1984). In a review
(Dahlström and Carlsson 2010) it was shown that oral health-related quality
of life (OHRQoL) was negatively affected among TMD patients. Studies on
TMD are from this point of view important for both the individuals and for
society.
Mixed methods
A combination of quantitative and qualitative methodology can give new
perspectives from both approaches. Epidemiological studies with a
quantitative approach can add knowledge about incidence, prevalence,
natural history of diseases, and determinants. To capture a deeper
understanding about experiences, attitudes, norms, knowledge, and
behavior, qualitative approaches are more suited. Qualitative studies are
rooted in traditions from the disciplines of anthropology, sociology, and
psychology (Polit and Beck 2006). One commonly used description of a
qualitative approach is “an inquiry process of understanding based on
distinct methodological traditions of inquiry that explores a social or
human problem. The researcher builds a complex, holistic picture, analyses
words, reports detailed views of informants and conducts the study in a
natural setting” (Creswell 1998). Three basic types of mixed method designs
are described: convergent, sequential, and embedded. These are termed
differently by different authors, but the main procedures are equivalent
(Creswell 2003, Klassen et al. 2012, Zhang and Creswell 2013). This thesis
has used a sequential design where collection and analysis of the quantitative
data was followed by the collection and analysis of the qualitative data, to
elaborate on and expand the findings of one method with another. There are
different tools for collecting qualitative information, such as in-depth
interviews, observations, and focus group discussions. In this thesis
interviews were used to collect qualitative data.

INTRODUCTION
11
Grounded theory
Grounded theory (GT), a common method mostly used for designing and
analyzing of qualitative data, was used in this thesis. The method was
developed in sociology during the late 1960s (Glaser and Strauss 1967), with
its theoretical roots in symbolic interactionism, a social psychological
perspective where the society is regarded as a sum of all ongoing interactions
and events, and a process that is constantly changing and not a permanent
structure. It is thus process-oriented, as reality is considered to be fluid and
constantly created and modified (Morse 1992). The goal in GT is to generate
comprehensive explanations of phenomena that are grounded in reality
(Polit and Beck 2006), to generate a theory that explains a pattern relevant
to the participants involved in the study. Key features of doing GT are an
emergent design and constant comparisons (Dahlgren et al. 2004).
Trustworthiness in qualitative research
The criteria of trustworthiness in qualitative and quantitative research
capture similarities between the traditions, but have different terms because
of differences in applications and interpretations, as indicated below.
Credibility refers to the ability to capture the multiple realities of those
under study. In quantitative research the related term is internal validity,
which refers to the ability to capture the truth value (have you measured
what you meant to measure?).
Transferability refers to whether the knowledge can be transferred to other
contexts. The knowledge gained from a developed theory should fit different
scenarios that may occur in larger populations. The term for the same issue
in quantitative research is external validity, or ability to generalize (how
applicable are the results to other contexts?).
Dependability refers to the ability of the researcher to account for constantly
changing conditions of the phenomenon under study, for the interaction
with the participants, and for the emergent designed process. The term in
quantitative research is reliability, and it refers to, whether the research
result can be replicated in the same context with the same sample.
Confirmability refers to neutrality of the data rather than neutrality of the
researcher. In qualitative research the interaction between the researcher
and the participant is important, and a basis for credibility. The related term
in qualitative research, objectivity, or neutrality refers to the ability to have

INTRODUCTION
12
distance from the observed phenomenon, to be objective and to not impose
any effect on the study related to personal interests.
GT criteria for trustworthiness are somewhat different (Glaser and Strauss
1967), and are termed fitness, workability, relevance, and modifiability,
meaning that a theory fits when the categories fit the data and a theory
works when it is able to explain what is happening in reality or at a
conceptual level. A theory has relevance when the core problem according to
the informant is interpreted in natural ways, as in GT. A theory can be
changed in response to a changing world; it is in that way modifiable
(Dahlgren et al. 2004).
Rationale
The high prevalence of TMD signs and symptoms, together with a
predominantly fluctuating pattern of the condition, has called into question
the validity of epidemiological findings. From the clinical perspective,
women outnumber men as patients for these disturbances; the reasons for
this globally found pattern are not completely understood. It is essential not
to rely solely on patient samples when examining the associated and
contributing factors of a certain disease, because various elements may
influence a patient’s decision to seek health care. Therefore, samples drawn
from the general population are needed, not only to determine the
prevalence or incidence of a certain condition in a population, but also to
explore possible co-morbidities and relationships. Since pain and
dysfunction in the jawface/headneck region may be related to gender, it
has been proposed that men and women should be studied separately in
research of etiology. Gender, biological and psychological factors, culture,
and ethnicity may also influence pain perception and behavior and are
important in the understanding of pain and disability in a population. A
qualitative approach can help to get deeper insight in individual’s
experiences and thoughts about having longstanding dysfunction and pain
symptoms.

AIMS
13
Aims
The overall objective of this thesis was to investigate prevalence of signs and
symptoms indicative of TMD and factors related to perpetuation of
dysfunction and pain in the jawface, head, neckshoulder region and its
impact on well-being in a defined population of Sami women. The aim was
also to gain deeper insight into experiences, attitudes, and beliefs among
women with longstanding TMD.
Specific aims:
Paper I:
- To study the prevalence, frequency, intensity, duration and co-morbidity of
symptoms indicative of TMD, headaches, and neck-shoulder pain in a
defined population of Sami women.
Paper II:
- To validate self-reported longstanding, intense, and frequent symptoms of
pain and dysfunction in the jaw-face region in relation to RDC/TMD
diagnosis and clinical signs of dysfunction at a two-year follow-up.
- To compare women with TMD (cases) to women without TMD (controls)
with regard to dental occlusion, general health, and awareness of oral
parafunctions.
Paper III:
- To examine the influence of frequency, intensity, and duration of TMD,
headaches, and neckshoulder pain on activities of daily living (ADL).
- To analyze symptoms indicative of TMD, headaches, and NSP in relation to
age.
Paper IV:
- To explore thoughts, experiences, and beliefs regarding TMD among Sami
women with and without TMD.
- To gain insight into Sami women’s health care experiences.
- To generate hypotheses regarding factors associated with longstanding
TMD.

STUDY POPULATION & METHODS
14
Study population and methods
This doctoral thesis is based on three sub-studies, published in four papers.
To achieve the overall aim of the study a mixed methods approach was used.
Two papers are cross-sectional epidemiological studies, based on the
subjects’ response to a questionnaire (Papers I and III). Paper II is a
prospective casecontrol study based on a sub-sample of the former
epidemiological sample including a blinded clinical examination. Paper IV is
based on a qualitative method with thematic interviews using a grounded
theory approach on a strategic selected sample drawn from the study of
Paper II (Table 1). A flowchart over the study populations is presented in
Figure 2.
Table 1. Brief presentation of the study population and methods used.
Paper I Paper II Paper III Paper IV
Study design Cross-sectional
observational study
2-year prospective,
age-matched,
case and control study
Cross-sectional
observational study
Qualitative study
Data collection Questionnaire
Questionnaire and
blinded clinical
examination
Questionnaire
Thematic
interviews,
audio-taped
Sample
characteristics
Sami women aged
2170 years
in Sweden (n = 487)
Sami women with
(n = 22) and without
(n = 46) longstanding
symptoms indicative
of TMD
Sami women aged
2170 years
in Sweden
(n = 487)
17 informants
drawn
strategically from
Paper II
Data analysis Binary logistic
regression
(MantelHaenszel
estimates of odds
ratio)
Chi-square test,
Fisher’s exact test,
t-test, Wilcoxon’s
signed matched test,
binary logistic
regression
Multiple logistic
regression,
chi-square test
Transcribed
textfiles,
analysis based on
grounded theory

STUDY POPULATION & METHODS
15
Figure 2: Flowchart over the study populations. NRS=11-point numerical rating scale,
NSP=neckshoulder pain, TMD=temporomandibular disorders, n.s=non significant.
Study population
Papers I and III
The inclusion criteria for the questionnaire study were women living in the
communities of Kiruna or Gällivare, in the county of Norrbotten, in the
Arctic region of Sweden. To be included they had to be registered in the
electoral register of the Swedish Sami Parliament for 1997, or in the register
of the Swedish Board of Agriculture as reindeer owners or reindeer herders.
In the electoral register from 1997, 5991 individuals were registered
compared to 8322 individuals in the register from 2013. The electoral
participation has decreased from 63% (1997) to 54% (2013).

STUDY POPULATION & METHODS
16
The Sami Parliament Act (SFS1992:1433, Sametingslagen), states the criteria
a person must meet to have the right to vote in the Sami Parliament of
Sweden:
any person who considers themselves to be Sami; and
uses or has used the Sami language at home, or
can show that one of his or her parents or grandparents uses or used the Sami language at home, or
has a parent who is or has been listed in the electoral register of the Sami Parliament
At the time of the data selection (year 2000) the women included in the
study were between 21 and 70 years of age. The Southern Lapland Research
Department in Vilhelmina assisted in defining and selecting the sample. A
total of 751 Sami women fulfilled the inclusion criteria and were sent a
questionnaire.
Respondents and dropouts
Altogether, 487 females (65%) responded and returned the questionnaire.
Their mean age was 40.2 years (SD 12.9). In total, nine questionnaires were
returned undelivered, one because the respondent had deceased, and a
further twelve were returned blank (Table 2).
Dropout analysis
Out of those individuals who did not participate, every third one in each 10-
year age-cluster, was selected for a dropout analysis. A total of 53 women
were contacted for an interview by telephone, of whom 30 women agreed to
answer a few selected questions from the questionnaire. The most common
reasons given for not participating were “out of principle” (38%) and “for no
particular reason” (25%). Other answers were that they “had no time to fill
out the questionnaire” (11%), did not consider themselves to be Sami (9%),
had been away from their home address (8%), felt the study was
discriminatory (4%), had no symptoms (4%) or were severely ill (2%).
The prevalence of symptoms of TMD among the drop-out sample was 33%
and two out of three reported NSP. No significant differences in prevalence
of the symptoms examined were found between the dropouts and the
participants (Table 2).
STUDY POPULATION & METHODS
17
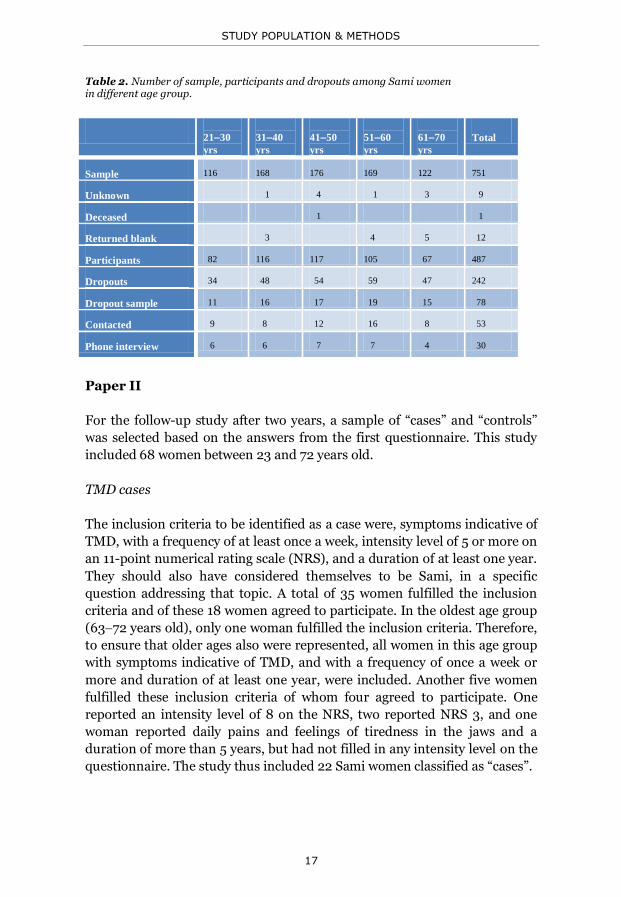
Table 2. Number of sample, participants and dropouts among Sami women in different age group.
2130
yrs
3140
yrs
4150
yrs
5160
yrs
6170
yrs
Total
Sample 116 168 176 169 122 751
Unknown 1 4 1 3 9
Deceased 1 1
Returned blank 3 4 5 12
Participants 82 116 117 105 67 487
Dropouts 34 48 54 59 47 242
Dropout sample 11 16 17 19 15 78
Contacted 9 8 12 16 8 53
Phone interview 6 6 7 7 4 30
Paper II
For the follow-up study after two years, a sample of “cases” and “controls”
was selected based on the answers from the first questionnaire. This study
included 68 women between 23 and 72 years old.
TMD cases
The inclusion criteria to be identified as a case were, symptoms indicative of
TMD, with a frequency of at least once a week, intensity level of 5 or more on
an 11-point numerical rating scale (NRS), and a duration of at least one year.
They should also have considered themselves to be Sami, in a specific
question addressing that topic. A total of 35 women fulfilled the inclusion
criteria and of these 18 women agreed to participate. In the oldest age group
(6372 years old), only one woman fulfilled the inclusion criteria. Therefore,
to ensure that older ages also were represented, all women in this age group
with symptoms indicative of TMD, and with a frequency of once a week or
more and duration of at least one year, were included. Another five women
fulfilled these inclusion criteria of whom four agreed to participate. One
reported an intensity level of 8 on the NRS, two reported NRS 3, and one
woman reported daily pains and feelings of tiredness in the jaws and a
duration of more than 5 years, but had not filled in any intensity level on the
questionnaire. The study thus included 22 Sami women classified as “cases”.

STUDY POPULATION & METHODS
18
Controls
The criteria to be included as a “control” were that they considered
themselves to be Sami, but did not report in the questionnaire any symptoms
indicative of TMD or pain in the neck- or shoulder region. In total, 127
women fulfilled these inclusion criteria. The women were stratified into five
age strata based on the base-line questionnaire (2130, 3140, 4150, 5160,
and 61-70 years old). The oldest age-group comprised 28 individuals of
whom 12 accepted participation, and the youngest age-groups comprised 16
individuals of whom four agreed to participate. In the other age-groups 16
women in each 10-year cluster were randomly selected. In total, 30 women
in this group agreed to participate. The control group thus comprised 46
women.
Dropouts
The non-participating cases included ten women who had moved from the
region, six women were not interested in participating, and one who was
severely ill. The drop-outs from controls included, from the oldest age
groups, seven women who did not want to be examined, four who could not
be reached or traced, three who had no possibility of travelling to the dental
clinic, one who had recently had a stroke with complications in locomotion,
and one who was away from home. In the youngest sample, seven could not
be reached or traced, and another five had moved. In the other age-groups
ten subjects could not be reached or traced, four did not want to participate,
two had moved, one could not travel to the clinic, and one had deceased.
Paper IV
For the qualitative thematic interview a purposive sample of informants with
severe TMD as well as a sample without TMD was selected. The selection of
informants was based on the answers in the two consecutive questionnaires
and the outcome of the clinical examination.
Informants with severe TMD had persistent, longstanding, frequently
occurring symptoms of TMD, with a reported intensity of 5 or more (NRS)
for at least one symptom and with clinical signs confirming a diagnosis of
TMD according to RDC/TMD. The other informants had no signs or
symptoms of TMD. The women were informed at the clinical examination
that they could be contacted again for an interview study. All of them agreed
to be contacted.
STUDY POPULATION & METHODS
19
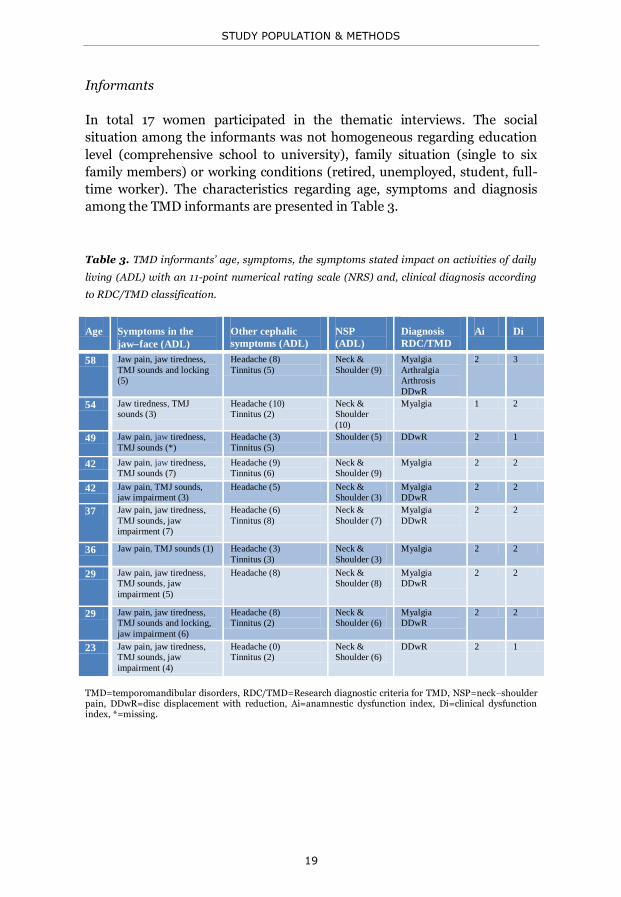
Informants
In total 17 women participated in the thematic interviews. The social
situation among the informants was not homogeneous regarding education
level (comprehensive school to university), family situation (single to six
family members) or working conditions (retired, unemployed, student, full-
time worker). The characteristics regarding age, symptoms and diagnosis
among the TMD informants are presented in Table 3.
Table 3. TMD informants’ age, symptoms, the symptoms stated impact on activities of daily
living (ADL) with an 11-point numerical rating scale (NRS) and, clinical diagnosis according
to RDC/TMD classification.
Age Symptoms in the
jawface (ADL)
Other cephalic
symptoms (ADL)
NSP
(ADL)
Diagnosis
RDC/TMD
Ai Di
58 Jaw pain, jaw tiredness,
TMJ sounds and locking
(5)
Headache (8)
Tinnitus (5)
Neck &
Shoulder (9)
Myalgia
Arthralgia
Arthrosis
DDwR
2 3
54 Jaw tiredness, TMJ
sounds (3)
Headache (10)
Tinnitus (2)
Neck &
Shoulder
(10)
Myalgia 1 2
49 Jaw pain, jaw tiredness,
TMJ sounds (*)
Headache (3)
Tinnitus (5)
Shoulder (5) DDwR 2 1
42 Jaw pain, jaw tiredness,
TMJ sounds (7)
Headache (9)
Tinnitus (6)
Neck &
Shoulder (9)
Myalgia 2 2
42 Jaw pain, TMJ sounds,
jaw impairment (3)
Headache (5) Neck &
Shoulder (3)
Myalgia
DDwR
2 2
37 Jaw pain, jaw tiredness,
TMJ sounds, jaw
impairment (7)
Headache (6)
Tinnitus (8)
Neck &
Shoulder (7)
Myalgia
DDwR
2 2
36 Jaw pain, TMJ sounds (1) Headache (3)
Tinnitus (3)
Neck &
Shoulder (3)
Myalgia 2 2
29 Jaw pain, jaw tiredness,
TMJ sounds, jaw
impairment (5)
Headache (8) Neck &
Shoulder (8)
Myalgia
DDwR
2 2
29 Jaw pain, jaw tiredness,
TMJ sounds and locking,
jaw impairment (6)
Headache (8)
Tinnitus (2)
Neck &
Shoulder (6)
Myalgia
DDwR
2 2
23 Jaw pain, jaw tiredness,
TMJ sounds, jaw
impairment (4)
Headache (0)
Tinnitus (2)
Neck &
Shoulder (6)
DDwR 2 1
TMD=temporomandibular disorders, RDC/TMD=Research diagnostic criteria for TMD, NSP=neckshoulder pain, DDwR=disc displacement with reduction, Ai=anamnestic dysfunction index, Di=clinical dysfunction index, *=missing.

STUDY POPULATION & METHODS
20
Methods
Questionnaire (Paper I and III)
A questionnaire concerning symptoms indicative of TMD, headaches, and
NSP was sent to each woman’s home address, together with information and
a pre-paid return envelope. The questionnaire focused on questions
regarding frequency, duration, and intensity of the symptoms, and their
impact on daily life (Appendix I). Seven weeks after the first letter had been
sent, a reminder, along with a questionnaire, was sent to those who had not
responded, and after a further four weeks a second reminder was sent out.
Frequency: Each question on symptoms had six possible response
alternatives describing frequency: Never; No, not now but had it previously;
Yes, at most once or twice a month; Yes, once a week; Yes, several times a
week; Yes, daily. “Frequent symptom” was defined as a reported frequency of
once a week or more.
Duration: To describe the duration, each symptom had four alternatives:
less than 1 month; 1 month to 1 year; 1 year to 5 years; more than 5 years.
“Longstanding symptom” was in this study defined as a reported duration of
one year or longer.
Intensity: The intensity of symptoms was measured on an 11-point
numerical rating scale (NRS).
Impact on activities on daily living (ADL): The impact of symptoms on ADL
was measured by NRS; scales addressed headaches and NSP, respectively,
and symptoms of TMD as a group.
Symptoms of pain and dysfunction in the jawface region were grouped in
accordance with the index Ai devised by Helkimo.
The questionnaire also included open-ended questions regarding health care
utilization, which are not included in the present thesis.
Clinical examination (Paper II)
A follow-up was conducted two years after the primary investigation. This
included the same questionnaire as previously used, with a few additional
questions and a clinical examination. Sixty-eight Sami women were invited
to the clinical examination free of charge at one of the dental clinics in
Karesuando, Kiruna, or Gällivare. Participants’ expenses for travel to and
STUDY POPULATION & METHODS
21
from the clinic were reimbursed. A standardized clinical examination was
performed by a specialist in TMD/orofacial pain who was blinded to the
participants’ affiliation as a case or a control. The examination included:
Dental occlusion: Number of teeth (032)
Overjet and overbite to the nearest mm
Contact pattern in centric relation (unilateral or bilateral)
Slide in centric in anteriorposterior, vertical, and lateral directions
to the nearest 0.5 mm
Tooth contact patterns at 3 mm and 9 mm lateral excursion of the
mandible (anterior guidance, cuspid guidance, group function,
balanced occlusion, laterotrusive side interference, mediotrusive
side interference)
Number of occluding pairs of teeth in intercuspal contact position
(ICP), at light and hard clenching effort
Supporting occlusal zones in accordance with Eichner (Eichner 1955,
Österberg and Landt 1976), without removable dentures
Presence of implant-supported fixed dental prosthesis
Degree of tooth wear Registered in accordance to Oilo (Oilo et al. 1987)
Mandibular mobility Unassisted maximal opening, protrusion, and laterotrusion
measured to the nearest millimeter with a ruler (Agerberg 1974)
TMJ signs TMJ sounds. Auscultation, without a stethoscope, for the presence of
TMJ sounds on opening and closing movements of the jaw. The
occurrence of sounds was classified as sharp clicking, dull clicking,
or crepitating.
TMJ tenderness. The TMJ was palpated laterally and posteriorly
through the auditory meatus. Pain was registered only if the
palpation elicited a palpebral reflex in the eye or a protective reflex
(withdrawal).
TMJ pain on unassisted jaw movements (opening wide,
laterotrusion, protrusion)
TMJ loading. The subject was asked to bite hard for 30 seconds on a
double wooden spatula (3 mm) placed on the region of the first
molars, each side separately. Elicited pain in the contralateral side of
the joint was registered as TMJ load pain.

STUDY POPULATION & METHODS
22
TMJ joint play. The examiner’s first finger on the right hand was
placed on the participants’ left molar region. While holding the
mandible, it was pulled forwards and backwards with the operator’s
third finger on the left hand placed over the left TMJ. The TMJ
movement was registered if restricted, painful, or both. The
procedure was repeated on the other side.
Muscle signs
Muscle tenderness. Presence of pain to palpation of muscle sites.
Pain was registered only if the palpation elicited a palpebral reflex in
the eye or a protective reflex (withdrawal). The following sites were
palpated: region of the lateral pterygoid muscles, medial pterygoid
muscles, anterior and posterior parts of temporal muscles, tendon of
the temporal muscles, superficial and deep parts of masseter
muscles, sternocleidomastoid muscles, trapezius muscles, neck
muscles in the region of linea nuchae and thumb muscles. If the
latter elicited a pain response, the muscles on the underside of the
forearms and the calf muscles were also palpated to measure signs of
a generalized pain response (hyperalgesia) to palpation.
Static loading of jaw muscles. The participant was asked to clench
her teeth hard in the intercuspal position for 30 seconds.
Development of feeling of tiredness/fatigue or pain in the head, face,
or jaws during clenching was registered.
Perception thresholds The perception over the areas innervated by the trigeminal nerve
was tested with von Frey filaments. The following areas were tested
on the right- and left-hand sides: the forehead, the infraorbital
region, the cheek, the mental region, and the temple.
Body Mass Index (BMI) Weight and height for calculating the BMI.
Some of the variables collected in the questionnaire and some of the
variables registered clinically were used to calculate the anamnestic
dysfunction index (Ai) and the clinical dysfunction index (Di), respectively
(Helkimo 1974b). A classification of each participant was also done in
accordance to RDC/TMD Axis I (Dworkin and LeResche 1992).

STUDY POPULATION & METHODS
23
Statistical methods (Papers I-III)
The questionnaire data were first transferred into a data-base (EpiInfo) and
then converted into SPSS ver. 12.0 (Paper I) ver. 14.0 (Paper II) ver. 17.0
(Paper III) for Windows. The level of statistical significance was set to a P-
value <0.05 (Papers IIII).
Paper I
Binary logistic regression by MantelHaenszel estimates of odds ratio (OR)
and 95% confidence interval (CI) were used.
Paper II
Comparisons between cases and controls with regard to categorical variables
were done using the chi-square test or Fisher’s exact test if the expected
counts were less than 5. Comparisons between groups with regard to
continuous variables were done using the t-test for independent samples.
Comparisons of registrations within cases and controls at the first and
second examination were done using Wilcoxon’s signed matched test.
Associations were assessed by means of ORs in unconditional logistic
regression models.
Paper III
Multiple logistic regression analysis was used to test the impact on daily life
with regard to frequency, intensity, and duration of TMD symptoms,
headaches, and NSP, together with age and education.
The dependent variable; answers on the ADL scale for TMD was
dichotomized into those who stated 0 and those who stated ≥1 for the
regression analysis. Answers on the ADL scale for headaches and neck or
shoulder pain were dichotomized, respectively, into those who stated <4 and
to those who stated ≥4, and used as dependent variable in the regression
analysis.
In the logistic regression model for ADL related to TMD, answers concerning
symptom frequency, intensity, and duration, and age and education were
used as independent variables, first, factor by factor, and then, all factors
that showed a statistically significant relationship to the dependent variable
in the univariate analysis were added into the model in a forward likelihood
ratio analysis. In the logistic regression model for ADL related to headaches
and neck and shoulder pain the same procedure was applied.

STUDY POPULATION & METHODS
24
Before the analysis, the independent variables were recoded as follows: The
frequency of symptoms was recoded as: 0 = No, never/No, not at present; 1
= Once or twice a month at most; and 2 = Once a week to daily. The duration
of each symptom was recoded as 0 = Never had symptoms, 1= <1 year, and 2
= ≥1 year. The intensity of each symptom was recoded as 0 (= 0 on NRS), 1
(= 1–4 on NRS) and 2 (≥5 on NRS). Education was dichotomized into those
who had studied nine years at most and those with longer education (senior
high school or university). Comparison between age groups for presence of
different symptoms in the jawface, head, and neckshoulder region was
done with a chi-square test. Ages were grouped in 10-year clusters (21–30,
31–40, 41–50, 51–60, and 61–70) for descriptive reasons.
Thematic interviews (Paper IV)
Data collection
The selected informants were phoned and an agreement on time and place
for the interview was decided. The women could choose to have the interview
at one of the public dental clinics after working hours or if they preferred, the
interview could be conducted at their home. All women gave their informed
consent and were assured anonymity and confidentiality. I conducted all the
interviews, using a thematic interview guide covering life history, the Sami
heritage, and health and illness experiences and beliefs. The guide was pre-
tested in pilot interviews before the study began. The interviews were tape-
recorded and took 4575 minutes. The interviews were fully transcribed
verbatim and then cross-checked with the tapes for accuracy. The text files
were transferred to a database, Open-Code (ver. 3.3), a computerized tool to
sort and classify the data.
Data analysis
The analysis was based on grounded theory. The first step in the analysis
process is to go through the text, line by line or sentence by sentence, and
write down codes, which are characteristics, and capture what is going on in
the data. The codes are initially close to the text and may be actual words
that the informants use. The next step is to decide which codes are
important, then cluster them together and transform them into categories
with different levels of abstraction. The categories derived must be relevant
and meaningful and describe the phenomenon under study. A category can
be described as a concept with which to organize reality. The codes and
categories are constantly compared with data collected earlier, so that
commonalities and variations can be determined. The data collection ends
when the findings are saturated, that is, the categories are solid and

STUDY POPULATION & METHODS
25
recognizable in all interviews. A major component in GT is the discovery of a
core category. The core category is a pattern of behavior that is relevant for
the study participants and related to the categories identified. The first
coding procedure was performed manually and separately by me and my two
supervisors, going through the texts and annotating the transcripts with
codes and tentative categories in. Numerous meetings followed, involving
comparisons of codes and evolving categories, putting new questions to data,
and formulating a core category and theoretical outlines. Discussions
continued until consensus on the categorizations was reached.

STUDY POPULATION & METHODS
26
Table 4. Example of the process of analysis: quotations, codes, subcategories, and categories
leading to the core category
Quotation
Codes
Sub -categories
Categories
Core Category
I was chewing a caramel and then
something happened here on the left
side, like it jumped out. I don’t know
what happened. And then it swelled up
and that's what I’ve had ever since
then. I think it began with this injury
with the caramel… that there was an
uneven stress and that it affects the
entire body.
Chewing
Something
happened
Don’t know what
Ever since
Impairment
Strain
Musculoskeletal
Problems
Biting
behavior
Inflicted
injury
Bodily strain
Triggers
Grin(d)
and bear
it
No, when I get stressed I bite. I bite
and become so focused on what I’m
doing so that I’m not aware of what
is happening around me. I’m
extremely focused on getting done
whatever is lying around waiting for
me. I bite down and become quiet,
until, until I have finished
doing most of the job.
Stress
Bite together
Focused
Awareness
Active
Bite together
Stress
Bite together
Strain
He [the dentist] examined every which
way. He turned and twisted and
checked everything and he didn’t find
anything wrong. He couldn’t figure
what I had. He was downright rude, I
think.
Examined from all
angles
Nothing wrong
Unfriendly
Blame on me
Ignorance
Mutual
mistrust
Distrust
Sure there are days when you don’t
feel so great, and then I usually think
that it’s just my imagination and then
you get a second wind. In some way
I’ve accepted that you aren’t always at
your best.
Bad days
Not feeling fit
It’s imagination
Come through
Accepted
Not always on top
Visions of
health
Acceptance
Reconciliation

RESULTS
27
Results
Study population
In total, 82% of the women identified themselves as Sami. Six percent stated that they were not quite sure of their affiliation to the Sami population. The majority (63%) of the latter group reported that their uncertainty was because they were not active in reindeer herding or did not speak the Sami language, but their basic family background was nevertheless Sami. Seven percent were married to a Sami. The remaining 30% gave no comments or commented that the question was irrelevant.
Twelve percent of the women did not consider themselves as Sami. The majority of these (53%) stated that their roots were Sami but that they were not living as a Sami or were not viewed as a Sami among other Samis or authorities. Twelve percent of these women were married to a Sami, 24% stated that they were not Sami, but most of them were reindeer owners, and 10% made no comments.
In the total study population of Sami women, 12% reported they were working actively with reindeer herding, and 63% were working outside their homes, twelve percent were retired or had a disability pension, ten percent were studying, and eight percent were unemployed.
The majority of the Sami women (86%) reported that their general state of health was good, whereas 13% reported that their health was not so good, and one percent that it was bad. Almost one of four reported that they had a disease that was under medical care, and 29% had medicine prescribed by physicians on a regular basis.
Symptoms indicative of TMD
The prevalence of ongoing symptoms indicative of TMD varied between 8%
and 32%, depending on the criteria used to determine frequency and
intensity. The prevalence of ongoing symptoms indicative of TMD was 32%,
of which approximately half (17%) were symptoms reported at a frequency of
at least once a week; this was reduced by half again (8%) when only those
were included who also stated that their symptoms intensity level was at 5 or
more on the NRS. When the criterion of impact on daily life, registering
more than one on the NRS was added in, the prevalence was further reduced
to 6% (Figure 3).
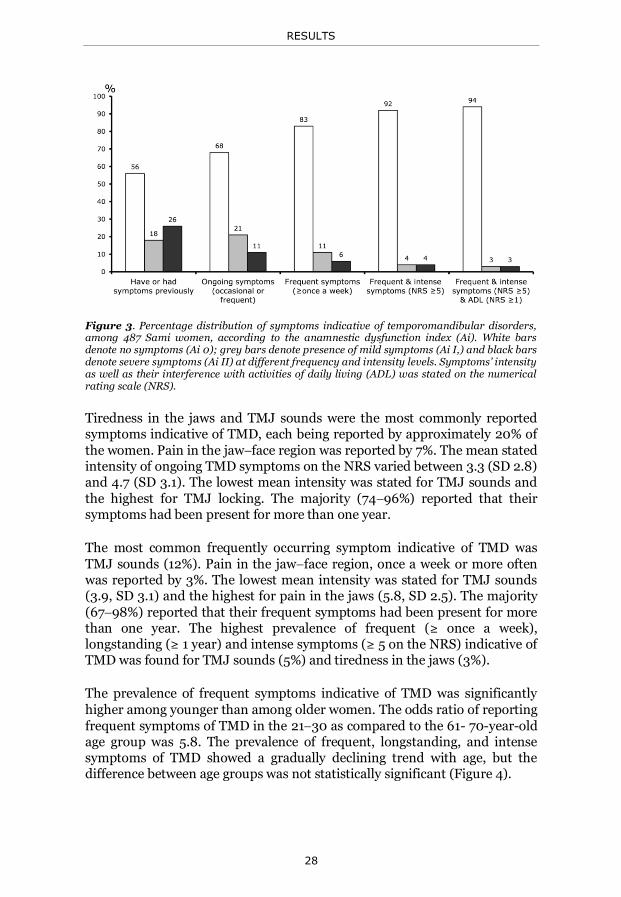
RESULTS
28
Figure 3. Percentage distribution of symptoms indicative of temporomandibular disorders, among 487 Sami women, according to the anamnestic dysfunction index (Ai). White bars denote no symptoms (Ai 0); grey bars denote presence of mild symptoms (Ai I,) and black bars denote severe symptoms (Ai II) at different frequency and intensity levels. Symptoms’ intensity as well as their interference with activities of daily living (ADL) was stated on the numerical rating scale (NRS).
Tiredness in the jaws and TMJ sounds were the most commonly reported symptoms indicative of TMD, each being reported by approximately 20% of the women. Pain in the jawface region was reported by 7%. The mean stated intensity of ongoing TMD symptoms on the NRS varied between 3.3 (SD 2.8) and 4.7 (SD 3.1). The lowest mean intensity was stated for TMJ sounds and the highest for TMJ locking. The majority (7496%) reported that their symptoms had been present for more than one year.
The most common frequently occurring symptom indicative of TMD was TMJ sounds (12%). Pain in the jawface region, once a week or more often was reported by 3%. The lowest mean intensity was stated for TMJ sounds (3.9, SD 3.1) and the highest for pain in the jaws (5.8, SD 2.5). The majority
(6798%) reported that their frequent symptoms had been present for more than one year. The highest prevalence of frequent (≥ once a week), longstanding (≥ 1 year) and intense symptoms (≥ 5 on the NRS) indicative of TMD was found for TMJ sounds (5%) and tiredness in the jaws (3%).
The prevalence of frequent symptoms indicative of TMD was significantly
higher among younger than among older women. The odds ratio of reporting frequent symptoms of TMD in the 2130 as compared to the 61- 70-year-old age group was 5.8. The prevalence of frequent, longstanding, and intense symptoms of TMD showed a gradually declining trend with age, but the difference between age groups was not statistically significant (Figure 4).

RESULTS
29
Headaches and neckshoulder pain
More than half of the Sami women reported headaches (61%) and NSP
(56%). When only frequently occurring symptoms were considered, the
prevalence of headaches was reduced to 19%, and of NSP to 30%. Eleven
percent reported frequent and intense headaches, and 21% frequent and
intense NSP. The mean stated intensity level was 6 for both frequent
headaches and frequent NSP. More than 80% reported that these symptoms
had been present for more than one year. The prevalence of longstanding,
intense headaches was significantly higher in the younger age groups than
among the older. The prevalence of frequent headaches showed a gradually
significantly declining trend with age. The pattern of frequent NSP showed a
gradual increase up to the age of 60, but the difference in relation to age
groups was significant only for longstanding, intense neck pain (Figure 4).
Figure 4. Percentage distribution of frequent (once a week or more often) and grievous symptoms of TMD, headache, and NSP, respectively, in five age groups of women in a Sami
population (2130 yr, n = 82; 3140 yr, n = 116; 4150 yr, n = 117; 5160 yr, n = 105; 61 70 yr, n = 67). Grievous denotes that symptoms occurred at least once a week, with a reported severity level of 5 or more on an 11-point numerical rating scale (NRS) and were of at least one-year’s duration.
Disability related to symptoms indicative of TMD
Of those 142 women with ongoing symptoms indicative of TMD and stating a
related impairment of their ADL on an NRS, 57% reported that the
symptoms affected their ADL to some degree and 19% stated a value of 5 or
higher on the NRS. When calculated based on the total sample of Sami
women, 6% thus reported a substantial effect on their ADL from symptoms
indicative of TMD. A total of 8% (n=39) reported longstanding, frequent,

RESULTS
30
intense symptoms indicative of TMD and of these, 77% (n=30) stated that
their symptoms interfered with daily life. All women who reported frequent
jaw pain stated their ADL was negatively affected. The majority of those who
reported no negative interference at all were those with frequent
longstanding TMJ sounds.
In the multivariate analysis including all independent variables that were
statistically significant for an effect on ADL related to TMD in univariate
analyses, low education level, reported intensity level of impaired jaw
opening, reported intensity level of neck pain, and duration of jaw pain
remained in the model as factors significantly related to the women’s
reported effect on ADL related to symptoms indicative of TMD (Figure 5).
Disability related to headaches and neckshoulder pain
Almost half of the study population reported that headaches (47%) or NSP
(48%) to some degree disturbed their daily activities. The interference was
scored 5 or higher among 23% for both headaches and NSP. Twenty-one
percent reported longstanding, frequent and intense pain in the neck and/or
shoulder region, and 97% of these women stated that the pain had a negative
impact on their ADL. Eleven percent reported longstanding, frequent, and
intense headaches, and all of these stated that their headaches negatively
affected daily life.
In the multivariate forward logistic regression model the stated intensity
level of headaches and frequency of tiredness in the jaws remained as factors
significantly related to the women’s statements of the effect of headaches on
ADL.
In the multivariate forward logistic regression model stated intensity level of
pain in the shoulders, stated intensity level of tiredness in the jaws, and
stated intensity level of neck pain were factors that significantly related to
the women’s statement of the effect of NSP on ADL (Figure 5).

RESULTS
31
Figure 5. The black pies show the percentage of those who reported that their symptoms to some degree disturbed their daily life activities. The bars show, respectively, the percentage distribution of the degree of interference with daily life stated on the NRS in relation to the symptoms. Black bars indicate cases and white bars indicate controls used as dependent variables in the regression analysis. Odds ratio (OR) and 95% confidence interval (CI) presented for the significant factors that remained explanatory in multiple logistic regression analysis.
Co-morbidities
A reported impaired general state of health was significantly related to
ongoing TMD symptoms (OR 2.1, 95% CI 1.23.5), ongoing frequent TMD
symptoms (OR 2.7, 95% CI 1.54.8), and longstanding, frequent, and intense
symptoms indicative of TMD (OR 2.8, 95% CI 1.36.0). Statistically significant associations between frequent symptoms indicative of TMD and frequent headaches, between frequent symptoms indicative of

RESULTS
32
TMD and frequent neckshoulder pain, and between frequent headaches and frequent neckshoulder pain were found. These associations were similar when the criteria of longstanding and intense were added. Approximately 50 % of those with frequent and more intense symptoms indicative of TMD as well as of those with frequent and more intense headaches also had frequent symptoms in the neck-shoulder region (Figure 6).
Figure 6: Relationship between women who reported longstanding, frequent symptoms
indicative of TMD, headaches and neckshoulder pain (NSP) with an intensity level of 5 to 10 on an 11-point numerical rating scale (NRS). Odds ratio (OR) and 95% confidence interval of the relationship between cases with the symptoms.
Case–control study
The mean age of the clinically examined study population was 48.7 years (SD
13.1). The positive predictive value of having signs and frequent symptoms
indicative of TMD was 0.82; the negative predictive value was 0.87 at the
two-year follow-up. An annual incidence rate of TMD was 6.5% among
controls. Cases had significantly higher odds ratios of reporting impaired
general health, taking prescribed medication, and being aware of tooth
clenching and tongue pressing than the controls. A diagnosis in accordance
with the RDC/TMD classification system was established in 59% of cases.
Symptomatic TMJ disc displacement was diagnosed in 46% of cases
compared to diagnosis in 7% of the controls (P < 0.001). Myofascial pain was
diagnosed in 40% of cases as compared to 2% of controls (P < 0.001).
Diagnoses of TMJ arthralgia and TMJ arthrosis were established in 5% and
9%, respectively, of cases, but in none of the controls; the difference between
cases and controls was not statistically significant. The distribution of
symptoms (Ai) and clinical signs (Di) of dysfunction is presented in Figure 7.
In total, 91% of cases had signs of dysfunction compared to 37% of controls.

RESULTS
33
Figure 7. Percentage distribution of frequent (≥ once a week) symptoms (A) and signs of TMD (B) among controls (white bars) and TMD cases (black bars) in Sami women. A. Ai 0 denotes no symptoms, Ai I denotes mild symptoms, and Ai II denotes severe symptoms of dysfunction. B. Di 0 denotes no signs, Di I denotes mild signs, Di II denotes moderate signs, and Di III denotes severe signs of dysfunction.
The following clinical observations were made among cases and controls:
Dental occlusion
Two subjects, one in each group, were edentulous. The mean number of teeth was 25.2 (SD 7.2) with no statistically
significant difference between cases and controls. No statistically significant difference was found between cases and
controls in classifications of morphologic occlusion (neutrocclusion 72%, distocclusion 27%, mesiocclusion 1.5%, deep bite 16%, open bite 3%, edge-to-edge bite 8%, cross bite 8%, and scissors bite 3%).
No statistically significant difference was found between cases and controls for contact patterns in centric relation (unilateral contact in 57%), or slide in centric or contact patterns in eccentric positions.
Cases had fewer contacting pair of teeth in centric occlusion (mean 8.2, SD 2.9) than controls (mean 9.8, SD 2.8) (P =0.034).
There was no significant difference between cases and controls in the distribution of supporting occlusal zones according to the Eichner index.
RESULTS
34
Degree of tooth wear Forty-three percent of the cases were registered with considerable
tooth wear and with obvious change of anatomical tooth form (Mike or Tango) compared to 36% of controls. No significant differences were found between cases and controls.
Mandibular mobility No statistically significant difference was found between cases and
controls for mandibular mobility. The mean maximal jaw opening capacity was 48.4 mm (SD 6.5), the mean laterotrusion to the right side was 9.1 mm (SD 2.5), the mean laterotrusion to the left side was 9.0 mm (SD 2.7), and the mean maximal protrusion was 8.7 mm (SD 2.2).
TMJ signs Temporomandibular joint sounds were registered in 50% of cases
and 9% of controls (P <0.001).
Tenderness to palpation over the TMJ (lateral and/or posterior) was registered in 4.5% of cases and 2.2% of controls, with no statistically significant difference between the two groups.
Pain was elicited from the TMJ region in 26% of the cases and in none of the controls (P =0.002).
Muscle signs Tenderness to palpation over jaw muscle sites was registered in
68% of cases and 20% of controls (P <0.001).
Forty-five percent of cases developed symptoms during a 30- second clenching task compared to 15% of controls (P =0.007).
Perception thresholds All those included in the study population had similar tactile
perception thresholds at all tested regions of the face, as determined with von Frey filaments.
BMI The cases had a statistically significantly (P =0.027) higher body
mass index (28.2) than did the controls (25.4).

RESULTS
35
Thematic interviews
The core category derived from the categories was “Grin(d) and bear it.” It
summarizes the informants’ various ways and stages of processing and
handling the interacting categories that emerged in the analysis: (1) triggers,
(2) strains, (3) distrust, and (4) reconciliation with pain and/or difficulties in
life (Figure 8).
Figure 8: Grounded theory model. The figure illustrates the interaction between triggering factors, perpetuating factors such as different stress and strain life situations, and curative circumstances. Distrust can be directed towards the caregiver; it can also mean a feeling of being mistrusted.
For women with TMD the core category described their awareness of regular
tooth-clenching behavior whenever they were in pain or stressed. Informants
without TMD used the same expression, but more as a metaphor for a
strategy for handling difficulties in life.
Women with TMD expressed both similar and divergent understandings and
experiences of related impairments. The women without TMD contributed
foremost with their thoughts regarding factors that helped them to handle
strains, reconcile, and stay healthy. Women with and without TMD seemed
to cope differently with life situations. The healthy women handled
difficulties in life by leaving bad experiences behind; they were looking
forward and striving to get on with life, despite any difficulties. To succeed in
this strategy, they relied heavily on support from family and friends. The
women with persistent symptoms of TMD described a life situation
characterized by a limited social network, loneliness, and a feeling of being
an outsider, off the labor market and also outside the health care service.
They did not know where to find help for their symptoms. They also
expressed feeling unsafe and uneasy. All informants expressed both negative
and positive experiences of the Sami heritage.
RESULTS
36
The following section presents the four categories that emerged from the
analysis.
Triggers
This category involves reflections and possible etiological explanations of
why and how pain symptoms in the jaws might evolve. These explanations
were varying; the onset was sometimes related to a sudden local injury, in
the orofacial area, in the neck, or elsewhere. Mostly, however, the jaw
dysfunction had evolved insidiously.
Co-morbidities were described between TMD symptoms and symptoms from
the neck and shoulder region. Diseases, such as sinusitis, muscle diseases,
rheumatic diseases, asthma, glaucoma, and hypertension were also reported.
“Well, I think that’s because of my muscular disease. Oh yes, there’s a
connection, all right. And that I tense up when get stressed, and then
my jaw gets tight.”
One woman related her jaw problem to an ankle fracture a long time ago,
which she believed had changed her body posture and thereby caused TMD.
“It has developed very gradually, but I believe a lot of the damage
happened that time in ´87 when I hurt myself—that I put on weight
and got this postural imbalance. I don’t know if that’s a part of it. That
my body has gone crooked.”
One woman related her problems to a virus infection in the 8th cranial
nerve. Another woman thought heredity might be a cause, as her mother had
arthritis and her father had rheumatic disease.
“So you wonder, is it something hereditary is it something in our genes
that caused it, or just what is it? Because the fact is that of the five of us
siblings, none of us is really healthy. Everyone has pain in some joint
or muscle.”
Some women with TMD linked their pain to dental treatments, such as a
tooth extraction or a dental prosthesis. One woman had to clench the jaws
together to keep her dentures in place. Bruxism, such as, tooth clenching and
tooth grinding, were common explanations suggested by the women with
TMD.

RESULTS
37
The women without TMD offered possible reasons for why they had
managed to avoid having TMD; for example they had few medical problems,
and no muscle tenderness or hereditary muscle problems. The impact of
financial or other personal problems on health was also mentioned:
“Maybe it’s because I'm not stressed. I don’t lie around, gnashing my
teeth.... I think you develop pain if you have this kind of stress, money
worries and one thing after the other. In the end it just gets to be too
much. I don’t have anything like that.”
They also more often described awareness of ergonomic relationships to
musculoskeletal disorders.
...and at work I think about lifting properly, so then it doesn’t happen,
either.
Physical activities during childhood, protecting them from pain and
dysfunction disorders were also considered.
“And it may also be because when we were little, we also had to work a
lot. Carry in wood and carry water and work hard outdoors…. That
you’ve really built up your muscles. That could be it. And we were
outdoors a lot and went skiing and sledding. We were active. Really
active. We were rarely indoors. I don’t know if it has to do with that.”
Strains
This category involves behaviors of biting/clenching/holding teeth together,
mental strain, bodily strain, and stress. A relationship between stressful
situations and tensions or pain in the body, foremost from the jaw-face,
head, and neck region, but also in other locations was described. The women
mentioned awareness of biting, clenching, or holding their teeth together in
specific life situations. Some reported these activities as a part of their
normal everyday behavior, a momentary event; others, as an ongoing habit:
“Yes, I’m always sitting around with my teeth clenched. You see, I
grind my teeth a lot, you know. I feel like I wake up with it. I can wake
up with the worst headache in the world, and my jaw is stiff. And it’s
because I’ve clenched my teeth, quite simply.”
“When I’m lying down reading, I lie there and clench my teeth. I sometimes notice then that my muscles are getting tired.”

RESULTS
38
Some women had common experiences of difficulties in early life and
recalled various stressful situations, for example early separations from their
parents, as they were sent to nomadic schools—special schools for Sami
children from the age of seven, and other traumatic events such as teasing
and harassment by other school children.
“When you got to school, you didn’t know anyone. There was one
person who became my guardian angel. When she graduated, you
could say that all hell broke loose. I was bullied then, and it wasn’t
much fun.”
Feelings of having been treated as outsiders by the majority group, and
experiences of marginalization of the Sami society under Swedish laws were
also expressed. Many had been forbidden to speak their mother tongue and
had therefore lost their Sami language, one important marker of ethnic
affiliation. Situations where they had to defend the Sami people and culture,
and sometimes had chosen to hide their Sami origin, were also described.
Distrust
This category involves feelings of mistrust and distrust regarding the
women’s contacts with medical and/or dental health services. They
expressed a belief that physicians and dentists suspected that their main
objective was to be on sick leave or to have other secondary gains. They
shared negative experiences of the general health services, and also
mentioned inaccessibility.
“And he asked if I wanted to go on sick leave. I got angry at him. I said
that I don’t run here because I want to go on sick leave; I come because
I want to get help. And, yes, we discussed it—in the end I felt that he
did not believe anything I said, so I walked away. I said that I have no
reason to be here if you don’t believe me, and so I left. Yeah, he was
really stupid, in my opinion.”
Some women expressed mistrust of the care providers’ competence and
ability to manage their problems:
“What kind of a doctor could there be who would understand this? I’ve
looked high and low.”
Mistrust towards treatment received was also described. Many reported that
they had tried oral splints or adjustments of the occlusion. Their common
RESULTS
39
experiences of these treatments were that they had no major effect on
symptoms.
“I've had oral splints. I've tried several of them, but I don’t know that
I’ve gotten any better.
A few women expressed passiveness regarding things they needed to manage, for example, physical activities, work ability, and household work. They seemed to be stuck within the pain condition, which was keeping them back from enacting changes in their lives.”
“I wish it would just disappear. That I could move my body more without feeling absolutely numb with pain. Do something at home without feeling sudden pain, like, “Oops, can’t do that now” … Yeah… If only I’d been spared that part, I could have gotten through anything.”
Reconciliation
This category describes the Sami women’s wish, intention, and strength to
“bear it” and move on with life, despite difficulties.
The women related to their Sami heritage with pride and appreciation for the
possibility of gaining health: a free, unrestricted, and sound life “up in the
mountains.” To be included and accepted in the Sami group was also of great
importance.
“Then I’ve like, I’ve like felt that when I’ve been having a really rough time, I’ve gone out into nature. Gotten connected—so I’ve meditated a great deal, gone to yoga class and stuff like that. And it’s a way for me to feel I can, you know, keep on going with this. That I need to get out into the wilderness, so my kids can say, “Mom, here’s a place where you can meditate.”
The women described different physical activities undertaken to improve
their well-being. The majority also utilized care from different professions,
such as physicians, physiotherapists, and dental surgeons, and also from
alternative medicine therapists, in their search for alleviation.
Self-treatments were a part of the women’s strategy to find their own way to
manage daily life. Over-the-counter medicine, stretching, and massage were
common examples mentioned.

RESULTS
40
“Yes, I often have a headache and feel stiff in the jaw. I try to sit down somewhere then and massage myself. And then I feel after a while it goes away and my muscles relax—and they’re always tense.”
“I try now—I take an analgesic and try to massage the back of my head a little. It usually helps. If my head and my jaw are really hurting I’ll take a warm shower, and that makes me feel better.”
Some women had reached a point of acceptance and tried to make the best of
their situation:
“In some way I’ve accepted that you aren’t always at your best. You
can’t always feel so great. It’s just sometimes like this.”
Social networks with others in the same situation were important for
managing their longstanding TMD problems.
“Then I meet up with my fibromyalgia buddies, and that’s so nice. Because we understand each other. They’re not any healthier than I am—some of them are actually worse off some days—and we cheer each other up and encourage each other.”
The healthy women seemed to handle difficulties in life by leaving bad
experiences behind, looking forward, and striving to get on with their lives,
despite difficulties. To succeed in this strategy they relied heavily on support
from family and friends. They tended to have a more conciliatory approach
to solving problems and handling shortcomings:
“I try to manage to get the (important) things done that I have to do.
In other words, I know that maybe I planned so I would have time to
do more, but then I don’t. It really doesn’t matter. If you don’t have
time, you don’t have time.”
Good health was mainly described and perceived by the women in terms of
ability to work and having energy left for leisure time.
“If you don’t have the strength for physical activities, you don’t have
good health and quality of life.”
Other important factors related to good health were feelings of safety,
freedom, good mental health, stable finances, and a healthy family.

DISCUSSION
41
Discussion
Main findings
Signs and symptoms indicative of temporomandibular disorders, headaches and neckshoulder pain, were common conditions in Sami women living in the Arctic region of Sweden. The prevalence of these conditions was essentially similar to those reported in other population studies on women. It should be emphasized that any reported prevalence of TMD symptoms strongly depends on the criteria used for frequency and intensity. There was a tendency of higher prevalence of headaches and TMD in the younger compared to the older Sami women. This finding is in line with studies on the general population in Västerbotten, Sweden (Yekkalam and Wänman 2014a), and in Jönköping, Sweden (Anastassaki and Magnusson 2004). The study also indicates that for quite a large part of the Sami women, the activities of daily living were negatively influenced by the frequency, intensity, and duration of pain in the jawface region together with impaired jaw opening and co-morbid symptoms of pain in the neck. The results are in agreement with those from a systematic review that demonstrated that OHRQoL of life was negatively affected among TMD patients (Dahlström and Carlsson 2010). Epidemiological studies have seldom found that variations in the dental occlusion have had a major impact on prevalence of TMD (Carlsson 2010, Türp and Schindler 2012). This study was no exception, since occlusion did not clearly distinguish whether a Sami woman was a TMD case or not, in the cross-sectional analysis. TMD cases reported impaired general state of health and awareness of parafunctions more frequently than controls.
In the qualitative part of the study the narratives from Sami women with more severe and longstanding symptoms of TMD relayed that they perceived that the jaw often felt strained. Although the informants (TMD cases) were strategically selected based on their TMD signs and symptoms all of these also had other symptoms such as headaches, NSP and tinnitus. The Sami women shared common thoughts and experiences about factors that might trigger and perpetuate TMD symptoms, headaches, and NSP. In the narratives they expressed distrust, one on hand, in the capabilities of the health care providers to handle symptoms of pain and dysfunction, but also reconciliation experiences, on the other, indicating that these women’s needs had not been met by the dental and health care system.
Study population
Epidemiology as a scientific method focuses on the incidence, prevalence and determinants of disease in human populations. Patterns of illness in the population are examined to try to gain knowledge about why certain

DISCUSSION
42
individuals develop a specific disease, whereas others do not (Greenberg et al. 2001).
The Sami population may from certain perspectives be viewed as a fairly homogenous group, with regard to ethnicity, culture, traditions, resources, language, geographic living area, and to some extent, also genetics. As such, they may help to add knowledge about development and determinants of specific diseases. The Sami society of today can be regarded as integrated into the Swedish society. According to the thesis by Andrea Amft from 2004, marriage within the Sami society is not longer a necessity. She also reported that Sami women traditionally take more responsibility than men for care of children and household chores, as in most other cultures. Responsibility for the products of the reindeer herding enterprise, such as food and materials for sewing clothes, has traditionally also been among the Sami women’s duties (Amft 2000). Only the oldest women in this population had experience of a more traditional, nomadic way of living.
The feeling of considering themselves included in the Sami society was addressed in one question. Despite the study population having been defined according to the Sami Parliament’s criteria, almost one out of five expressed doubts of being regarded as a Sami. This result may reflect that having heredity in the Sami culture is not enough, if they are not viewed as a Sami by other Samis or authorities. Identity is created through discourse, and not automatically transferred. Although a person is born Sami, but it is the person’s upbringing that determinates whether the person becomes a Sami. Sami women have to subordinate themselves to be a “genuine” Sami, and if a woman were to take a political stand as both a Sami and a woman, she might risk being defined as an outsider in relation to the ethnic group (Amft 2000). Some women in this study had difficulties in identifying themselves as Sami since their membership in the electoral register was related to matrimony. They were nevertheless a part of the Sami society and culture. Three percent of the women had a reindeer mark, were registered in the Swedish Board of Agriculture, and stated that they were not Sami. In our analyses, we did not find that there were any significant differences in the distribution of answers between those who were active in reindeer herding and not, and between those who stated that they were Sami and the rest of the sample. The study population included in this thesis may be considered as a fairly homogeneous sample in the sense that they are all women who share the Sami heritage and are living in the Swedish Arctic region.
The strategic choice to exclusively study women was based on the indications
that TMD symptoms, headaches, and neckshoulder pain are more common in women (Bovim et al. 1994, LeResche 1997a, Jensen 1999,), and that longstanding TMD pain and dysfunction are more commonly observed in women than in men (Wänman 1996, Kuttila et al. 1998, Rantala et al. 2003, Goncalves et al. 2010). Longitudinal studies of TMD have shown a fairly
DISCUSSION
43
consistent pattern of predominantly transient symptoms of pain and dysfunction with time (Könönen and Nyström 1993, Kitai et al. 1997, Magnusson et al. 2000, Nilsson et al. 2007). However, in a 10-year prospective study, women were at higher risk of reporting longstanding symptoms, even though significant fluctuations in TMD symptoms occurred over the period (Wänman 1996). There may be unknown factors involved in the maintenance of symptoms that relate to the female gender. Several hypotheses regarding this issue have been proposed, including psychosocial factors (LeResche 1997a, Dao and LeResche 2000, Rantala et al. 2003) and sex hormones (LeResche 1997b, Warren and Fried 2001, Cairns and Gazerani 2009, Cairns 2010). The role of genetic variation in relation to development of TMD is currently addressed in a large prospective research project-OPPERA (Smith et al. 2013). Several factors may thus be related to TMD pain, but no conclusive knowledge has yet been reached. These findings were also reasons for studying a fairly well-defined sample of Sami women from different perspectives. Since symptoms indicative of TMD, headaches, and NSP have fairly high prevalence, the size of the study population was considered acceptable. Dropouts complicate the assumptions and may jeopardize the study results. In the questionnaire study the dropout rate was approximately one out of three. Since the dropout analysis did not indicate any systematic errors related to presence of the symptoms in focus, the study results could be considered reliable. The risk of sampling error was small since all available individuals from the Sami register were included. The register on the other hand represents a clearly biased group in relation to the total Swedish population. The most common reason given for declining to participate was “on principle.” Discrimination was also mentioned as a reason. Stigmatization can occur among Indigenous Peoples, and discrimination of Samis is an ongoing debate (DO2008:1, DO2008:2, Ledman 2012a, Omma 2013).
Methodological considerations
Questionnaire
The balance between the number of questions included in a questionnaire and the expected number of participants willing to take the time to answers all the questions in population-based studies influenced the design of the questionnaire. It was structured around defined symptoms and their occurrence, intensity and duration. A question may address a condition’s occurrence on a lifetime, yearly, monthly, weekly, or daily basis. It is obvious that the outcome will be influenced by the wordings used. It has previously been reported that the reliability of answers to questions regarding symptoms of TMD increases when a frequency of once a week or more often is used as the time frame and probably also the “clinical relevance” increase when this time frame is used as an inclusion criterion (Nydell et al. 1994, Wahlund et al. 1998, List et al. 1999). In this study the questions were
DISCUSSION
44
constructed so the prevalence could be calculated for different time frames in order to compare the results with previous studies and to identify women with more frequent, intense, longstanding, and disabling symptoms for the subsequent thematic interviews.
To assess the intensity of symptoms as well as the impairment related to TMD symptoms, headaches, and neck-shoulder pain the NRS was used. Rating scales are commonly used to capture pain intensity and shown to have an acceptable reliability (List and Helkimo 1995, Conti et al. 2001, , Williamson and Hoggart 2005), as well as having the advantage of also being easy for participants to understand (Williams et al. 2000). Disadvantages of a rating scale are that the individual’s interpretation of the scale may differ, and thus, inter-individual comparisons are scarce. The scales can also be criticized for being one-dimensional. The validity of the NRS for capturing the severity of impact on daily life is not known. In the analysis of TMD the scale was dichotomized into those who stated no interference at all and the remaining women which we considered reasonable in relation to the analysis. The dependent variable was thus composed of an approximately equal number of those with and without impairment related to TMD symptoms. In the corresponding analyses of impairment related to headaches and NSP, the dichotomizing split was based on the distribution of the response, also creating an approximately equal numerical size in both groups. In the graded chronic pain scale (Von Korff et al. 1992) the pain score is dichotomized into the lower (<5) and higher (≥5) levels. The split in this sample may thus be interpreted as between those with a lower and a higher impairment related to headaches and neck‒shoulder pain,
respectively.
Different classification systems were used to cluster the women’s TMD‒related symptoms, using the RDC/TMD criteria to establish a
diagnosis (Dworkin and LeResche 1992), and the Ai and Di for severity of dysfunction. Both systems are well-established and internationally used classification systems. The Helkimo indices have been criticized (van der Weele and Dibbets 1987) and the RDC/TMD recently adjusted (Schiffman et al. 2014). The Ai captures presence of symptoms indicative of TMD. Based on the results from the present study, the index division in severity may be questioned. The severity of a condition is a subjective experience, and the subjects’ reports of symptoms’ intensity levels and their affect on daily life expressed on the NRS were similar for Ai 1 (mild symptoms) and Ai 2 (severe symptoms), as shown in figure 3. In support of the division used was the observation that most of those who reported no affect on daily life were those with TMJ sounds. The RDC/TMD diagnostic system may also be criticized, since it has its main focus on pain conditions, which is too limitative for the disorder. In this study population TMD pain had certainly affected the women’s ADL, but so had symptoms of dysfunction.

DISCUSSION
45
Case‒control study
The design of the case–control study was to compare individuals with symptoms indicative of TMD and those without symptoms, as identified by the questionnaire. The study has several strengths: cases and controls were selected from the same population, and thus had the same sex, ethnicity, and culture. Cases were identified based on severity of their symptoms and not on their status as consulting patients or as referrals. Twice as many controls as cases were included, and they were age-matched. The selection also focused on the extremes at each end of a normal distribution, with regard to severity of symptoms in the jaw–face region. The examiner (AW) was an experienced TMD specialist, and throughout the study was kept blinded to the women’s affiliation. Since two years passed between the first and second examinations, the identified cases really could be defined as severe cases with persistent TMD symptoms. Only those who subjectively considered themselves as Sami were included, because one of the themes of the subsequent, planned, thematic interview study was the life experience of being a Sami woman.
Because of relatively few cases twice as many controls were selected. Nothing, however, indicates that dropout was related to changes in TMD symptoms. The main reason for dropping out was that they could not be reached because they had moved away from the included municipalities. There were no statistically significant differences in answers to the first questionnaire between the participating women and those who were not accessible. Having a small number of participants increases the risk of making a type-2 error in data interpretation and accepting a null hypothesis, even though it is false. The distributions of most clinical variables examined in the cases and controls were, however, quite similar, so even a significant increase in the number of cases and controls would hardly have changed the interpretation of the results.
Interview study
The qualitative research approach was used to get insights into the women’s experiences and beliefs and to generate hypotheses of factors that might influence the development of longstanding TMD. The informants were strategically selected from the epidemiological sample, which may increase transferability. The selection of informants was based on their experience of having longstanding, severe TMD symptoms, or having no experience of TMD, and being approximately the same ages. The women who were included had consequently varying experiences relating to education level, family status, and working conditions, as a reflection of their different social living conditions. No Sami woman in the older ages was included, since there was no one available with severe symptoms. This finding is interesting by

DISCUSSION
46
itself and may warrant further qualitative studies addressing specifically women after retirement.
Grounded theory was chosen, as it is an established method used to explore complex phenomena and patient experiences in the health sector. The data collection ended when the categories were considered solid and recognizable in the interviews. To enhance credibility, triangulation, peer debriefing, and negative case analysis (Dahlgren et al. 2004) were used. The three of us researchers, separately performed the coding procedure, and meetings and discussions ensued until consensus had been reached. We all had different backgrounds, pre-understandings, experiences, and perspectives, which were considered an advantage, as it contributed to triangulation in the analysis procedure. I have, as a native Sami woman myself, an “insider perspective,” used as knowledge. The other two investigators provided the perspectives of a male dentist specialized in TMD (AW) and a female general practitioner (EEJ) with specific interest in chronic pain conditions. Preliminary findings were discussed with colleagues outside the process for inputs and comments, assigned to peer debriefing. Negative cases were included as references, not for direct comparisons, but to distinguish general life experiences among Sami women and those more specific to TMD cases.
Ethical considerations
The study was approved by the Regional Ethical Review Board at Umeå University, Sweden. As the ethical review in Sweden does not specifically consider Sami perspectives, I have chosen to relate to ethics more thoroughly than is required by Swedish law (SFS2003:460), as discussed by Ledman (Ledman 2012a). In practice, this implies that the study also has been carried out in contact with the Sami Parliament in Sweden. They approved the use of the electoral register and have also supported the study with grants. The results have been reported to the Sami Parliament for those papers they have supported. The results have also been reported in public, in conferences both within the field and also on a conference with Sami context. The study received attention in Sami media when it started, and my intention is also to report the final results in a more popular form. From these perspectives the research process has been transparent, and the Sami society has been given the opportunity to take part in this process. This approach is in line with what is recommended within international standards for indigenous research (Ledman 2012a, Smith 2012).
In studies of a specific group of people, as in this case, a specific gender and
an ethnic minority, stigmatization is a potential risk, as both the individual
and the group may believe they are being accused. The risk in this case was
considered low. As a native Sami, I might have increased the participants’
confidence. Even as an insider, one may have an outsider perspective (Åhren
2008). It is, however, more likely that the insider brings more familiarity

DISCUSSION
47
with the prevailing norms and values and can use this pre-understanding in
all phases of the research process. An example of being an insider for me was
that during the interviews an informant sometimes did not explain deeply
her experiences, instead commenting, “...but you know how it is‒you are a
Sami woman yourself.”
Epidemiological studies on the Sami population in Sweden were, at the
beginning of the year 2000 when this study was initiated, limited.
Knowledge about the health situation and living conditions has since
increased and is still increasing and required. In other countries with
Indigenous peoples, such as Canada, Australia, United States and New
Zealand, certain ethic guidelines for indigenous research have been
developed. These have been designed according to the Indigenous people’s
own values, standard, and requirements (Ledman 2012a). Such ethical
guidelines are not available in Sweden, but are warranted (Nilsson LM
2012). As the indigenous researcher Linda Tuhiwai Smith wrote in her book,
Decolonizing Methodologies, “research is probably one of the dirtiest words
in the indigenous world’s vocabulary” (Smith 2012). I also experienced some
skepticism, especially when the questionnaires were sent out. Some came
back with comments about the negative feeling of being selected through a
register. They mentioned the dark era in Swedish history with the race
biology studies, on the Sami people, who were considered a lower status race
during that time (Ledman 2012b, Lundmark 2007). The researcher may be
presumed to represent all the research that has conducted on the Sami
people, including research perceived as negative (Ledman 2012a). This is a
further aspect to have in mind when entering into a project with indigenous
themes.
Ethical risk is always to be considered in research of humans. The study was
conducted following the ethical principles for medical research involving
human subjects according to the World Medical Association Declaration of
Helsinki and the basic ethical principles in human research in accordance
with the International guidelines for ethical review of epidemiological
studies. The principle of respect for persons, meaning for their autonomy
and their capacity for self-determination has been relevant throughout the
study. The women decided by themselves to first participate in the
questionnaire. For the follow-up study they once again decided to
participate, and also for the subsequent interview. They were informed
during the follow-up (clinical examination) that they might be invited to an
interview. All of them gave their consent to be contacted by phoned and
asked for their agreement, and they could also choose to decline to
participate at that occasion. It has been my intention to give information as
much as possible about the study aims during the data collection process. I
DISCUSSION
48
believe that it was one of the reasons why all of them whom I met in clinical
settings agreed to be invited for an interview. All the participants were
informed orally and in writing about the aims. They were all assured
confidentiality and the opportunity to withdraw from the study anytime
without having to specify reasons for leaving. This promotes freedom of
choice. The study was thus conducted with respect for the right of informed
consent. A balance between benefit and harm must always be considered in
planning process of the research process. The benefit of this study was
considered at the individual level, that those with longstanding pain
symptoms could have the opportunity to obtain diagnosis, advice and
assistance. On group level possible factors of importance within the group
could be identified and lead to proposals for preventive measures. On
community level, knowledge of factors important for the development of
longstanding TMD is still lacking, and the study may generate increased
knowledge in this area. The principle of beneficence means that the expected
benefits of the research should be larger than the harms (non-maleficence).
In this study, a possible harm could be pain experienced by women during
the clinical examination. On the other hand, those participants also could get
some benefits in the form of advice for pain relief. In epidemiological
studies, particularly in clinical examinations, a sudden unexpected and
undesired diagnosis can be found. In this study, in the field of TMD,
however, no fatal diseases were expected. A benefit can instead be that the
participant was advised to contact her regular dentist or was referred to a
specialist in TMD, providing further assessments. The principle of justice has
been applied when it has been applicable. The women with pain might had
been more vulnerable than the women without pain; all were been treated
equally. Transportations costs were supported, so also those who had a
longer distance to the examination had the same chance to participate
without incurring any costs. There is also a potential risk of the participants
feeling subordinate to the researcher. It is my belief that as a native Sami
woman myself, I reduced that risk.
All data have been treated confidentially. Questionnaires and interviews
were done anonymously and stored, locked up, in a location separate from
the code keys. Even though the population was spread between two different
communities and areas within the communities (for example, Karesuando),
the Sami population have close internal contacts; many are even relatives.
No information regarding geographic area was presented, so it would not be
possible to identify specific individuals from the interviews. All quantitative
data were givens serial numbers, which were kept away from personal
identification data. The analyses were done at group level, and the
participants were remained anonymous throughout the analyses, with the
results being presented only at group levels.
DISCUSSION
49
Qualitative methodology is regarded as less threatening on an individual
level because of the close interactions between the researcher and the
informant. It has also been suggested that the methodology empowers
people through their active participation in the process (Dahlgren et al.
2004). In the qualitative study, the participants were informed that
researchers other than the interviewer were also going to work with the text
files. Confidentiality was assured. Private data such as name and so on were
kept away from the text files and would not be reported. The audio files were
coded and locked away. The key code linking personal identification to a
given code number was stored elsewhere. The ethical risks of being a
participant in an interview study may include the interviewer getting too
close to their life experiences, which may result in stress and fear about the
questions asked. This risk was considered as small, since the women were
informed about the topics in the beginning of the interview and told that
they could choose not to answer the questions if they felt that they did not
want to, without offering any explanations. The participants may also start to
reflect up on well-being and potential stress events, which may lead to
improved self-efficacy. It can be a benefit that someone takes time to listen
to their stories.
Temporomandibular disorders
Prevalence
The prevalence of symptoms indicative of TMD was lower among the Sami women than the prevalence observed in a Sami population examined in the early 1970s. These Skolt and Inari Lapps were at that time more or less uninfluenced by other cultures due to isolation and a high degree of marriage within their society. Their economical standard was low and living conditions simple. They also had a bad dental status but their general health was otherwise good (Helkimo 1974a). The prevalence among the Sami women in this study was close to a median value of symptoms based on several population based studies (Carlsson 1984, Salonen et al. 1990, De Kanter et al. 1993, Rantala et al. 2003,), which, on the other hand, were based on both men and women. In comparison to a survey in Västerbotten in 2002 (Yekkalam and Wänman 2014a) the prevalence of frequent symptoms, as well as the age distribution with higher prevalence in the younger as compared to the older women was similar, except that the peak of prevalence observed in the 50-year-old women in Västerbotten was not obvious in the Sami women. A similar age peak was reported based on a TMD patient sample (Manfredini et al. 2010a). The different prevalence figures related to symptoms indicative of TMD depending on the symptoms reported frequency, stated intensity, and interference with daily living may imply that for most individuals in the general population symptoms of TMD are of low

DISCUSSION
50
or inconsistent frequency, or low and manageable intensity. Most individuals thus seem to cope with these symptoms and do not demand treatment. The 6‒8% who reported more significant symptoms of TMD resembled estimated
treatment needs in the adult population (Agerberg and Carlsson 1975, Locker 1988, Alanen et al. 1997, Kuttila et al. 1998, Carlsson 1999). The results therefore add understanding to why previous fairly high prevalence figures reported in epidemiological studies never have been directly transformed into treatment. The demand for treatment is not based just on the bare presence of signs and symptoms indicative of TMD; the frequency, intensity, duration, and disability has a significant influence also (Macfarlane et al. 2003). These factors may not only increase the reliability but also the clinical relevance in studies of TMD. Prospective studies based on non‒patient samples have shown a fluctuating pattern of TMD symptoms
and that individuals with such mild, and inconsistent symptoms rarely develop more severe TMD (Könönen and Nyström 1993, Carlsson 1999, Magnusson et al. 2000). The most commonly reported symptoms indicative of TMD were feelings of tiredness in the jaws and TMJ sounds, in agreement with many previous studies (Helkimo et al. 1972, Carlsson 1984, Wänman 1987, Salonen et al. 1990, Nydell et al. 1994, Wänman 1996, Magnusson et al. 2000). Notable was that almost twice as many (6.1%) reported frequent, intense, and longstanding dysfunctional symptoms as reported frequent, intense, and longstanding pain (3.8%). Since there seem to have been a gradual shift in the professions’ view on TMD from dysfunction to pain, these opinions may need to be reconsidered.
Impact on daily life
Remarkably small differences in the distribution of the rated intensities between the different symptoms were observed. Feelings of tiredness in the jaws were rated as almost as intense/disturbing as pain in the jaws. The symptom that was given the lowest intensity level was TMJ sounds. Seventeen percent stated that their symptoms indicative of TMD to some degree interfered with activities of daily living of which presence of frequent, intensive jaw pain of long duration had the highest impact, together with impaired jaw opening. The results are in accord with previous studies showing that patients with myofascial pain, arthralgia, or disc displacement without reduction have reported a higher impairment than patients with disc displacement with reduction (John et al. 2007, Reissmann et al. 2007, Rener-Sitar et al. 2008, Barros Vde et al. 2009). The results from the present study also resemble a previously reported, epidemiological study, where 14% of those with facial pain and 48% of those with severe headaches reported that, at times, they were unable to carry on some activities because of the pain (Von Korff et al. 1988). In a review on TMD and its relation to oral health-related quality of life, non-painful conditions had less impact on
OHRQoL than painful conditions (Dahlström and Carlsson 2010). Among Sami women, TMJ sounds also dominated among those who stated no

DISCUSSION
51
disability related to the condition. The results indicate that most individuals, with non-painful joint sounds, adapt to the condition and thus are less disabled than they would be by painful conditions. Patients with myofascial pain more often used splints, consulted more physicians, and received more physiotherapy than patients with joint pathology (Schmitter et al. 2005). Sleep disturbances, impaired mood, and difficulties in chewing are other possible consequences of TMD pain (Murray et al. 1996). Even children with TMD symptoms report impaired quality of life, limited physical activities, and effects on their schoolwork and on activities with friends (Jedel et al. 2007). A higher absence from school and higher consumption of over-the-counter analgesics among adolescents with TMD pain were noted in a Swedish sample (Nilsson et al. 2009), as well as consequences for all aspects of their lives, even when the pain was absent the adolescents were constantly thinking of their pain (Nilsson et al. 2011). The incidence of pain in the jaw, TMJ and temple region seems to coincidence with the early teen-age period (Nilsson et al. 2007). With reference to the negative consequences for the quality of life (Dahlström and Carlsson 2010, John et al. 2007, Anderson et al. 2011) affected individuals should be identified in the dental health care systems as early as possible.
Influence of age
The lowest prevalence of the pain conditions examined was observed in the oldest age group. This is in agreement with previous studies in which older individuals reported TMD symptoms less often than younger ones (Schmidt-Kaunisaho et al. 1994, Österberg et al. 1992). For headaches as well, young and middle-aged groups reported the highest prevalence and thereafter prevalence declined with age (Anastassaki et al. 2012, Radtke and Neuhauser 2009, Yekkalam and Wänman 2014a). Frequent as well as grievous TMD symptoms and headaches declined with age, but not the related disability stated on the NRS. The prevalence pattern of these symptoms in relation to age was quite similar, which may indicate a shared etiology. The prevalence of headache and facial pain among women peaked in 25- to 44-year-olds and was observed to be at lowest among the 65-year olds and older ages (Von Korff et al. 1988). A trend of continuing decrease in prevalence of TMD related symptoms in elderly has also been observed (Carlsson et al. 2014); 80-year-olds reported lower prevalence of such symptoms than 70-year-olds. These observations of declining prevalence of pain conditions from approximately the age of 60 and onwards are interesting in relation to the understanding of the phenomenon pain. Changes in levels of sex hormones after menopause (Fillingim 2000, Cairns and Gazerani 2009), changed stress levels and related behavior have been offered as explanations (List et al. 2001) but there may be other reasons. Future studies specifically addressing elderly and their beliefs about why pain conditions may decrease with age might help to generate new hypotheses on the subject. It is not inconceivable that differences in lifestyle between elderly and younger

DISCUSSION
52
generations of Sami women may account for some of the differences in pain prevalence. During the 1930s to 1950s, physical activity was a more normal part of the Sami daily life, than it is today (Nilsson LM. et al. 2011). Also a sedentary life in front of a computer constitutes a part of a normal weekday among many of the younger generation, which may constitute a risk factor for increased symptoms in the neck and, shoulders and for TMD (Perri et al. 2008).
The causes of age-differences are complex and probably related to both external and internal factors. Previous studies have shown that older TMD patients reported a greater negative impact on quality of life (John et al. 2007, Rener-Sitar et al. 2008) which supports the finding that despite age being significantly and inversely related to prevalence of TMD symptoms the estimated impact on daily life was not.
Co-morbid conditions
In this study on Sami women, significant relationships were found between
symptoms in trigeminally and spinally innervated regions. Those included in
the interview also considered the symptoms in the jaw-, head-, and
neck/shoulder region as more or less unified. These observations confirms
the results from previous studies (Wänman and Agerberg 1987, Schokker et
al. 1990, Hasvold and Johnsen 1993, Ciancaglini and Radaelli 2001,
Magnusson et al. 2000, Visscher et al. 2001b, Rantala et al. 2003, Wiesinger
et al. 2007, Marklund et al. 2014) and indicates that these conditions are
influenced by the same contributing factors and/or mutually affected or
potentiated by each other. Co-morbidity between headaches and TMD pain
has been observed already from the teen-age period of life (Nilsson et al.
2013). The lowest common denominator of these associations may be tooth-
clenching habits, which beside the Sami women’s narratives also have been
identified as a risk factor associated with frequent headaches in a prospective
study (Marklund et al. 2014).
Headaches and NSP are common symptoms in the population (Bovim et al. 1994, Göbel et al. 1994, Unruh 1996, Côte et al. 1998, Scher et al. 1998, Rantala et al. 2003) and in accordance to the observations of the Sami women. Women report pain more frequently in these areas (Andersson et al. 1993, Bovim et al. 1994, Unruh 1996, Scher et al. 1998, Rantala et al. 2003), and they also report a higher degree of related disability than men do (Bovim et al. 1994, Unruh 1996, Webb et al. 2003, Unruh 2008). The prevalence of frequent headaches among the examined Sami women was close to figures previously presented in women (Agerberg and Bergenholtz 1989, Rasmussen et al. 1991, Boardman et al. 2003, Rantala et al. 2003, Yekkalam and Wänman 2014a). The approximately 40% reduction in prevalence of headache that occurred when moderate to severe intensity level was added

DISCUSSION
53
as criteria resemble results presented in a previous study (Boardman et al. 2003). The prevalence of frequent (weekly) neck pain was lower in the Sami women than among 3055 year old Finnish women (Rantala et al. 2003), but higher than reported for a general population sample in England (Webb et al. 2003), and close to the prevalence reported in a Norwegian survey (Hasvold and Johnsen 1993). In a Canadian sample, the 95% confidence interval for lifetime prevalence of neck pain, among both men and women, was found to be within 64%70% (Côte et al. 1998). This was only slightly higher than among the Sami women in this study. Differences in how questions are constructed probably account for some of the variations in prevalence between the studies. Using the same questions, the one-year period prevalence of troublesome neck pain among women reached 40% in a Norwegian (Bovim et al. 1994) as well as in an Italian sample (Ciancaglini and Radaelli 2001). In the former study the prevalence was halved when only longstanding and troublesome neck pain was included. A pattern similar to that of the present study. When the criterion frequent (weekly), intense (moderate or worse) neck pain of at least five year’s duration and with a significant effect on daily life was added in an analysis the 95% confidence interval for prevalence of neck pain among women was 2.2%5.4% (Webb et al. 2003), a figure significantly lower than in this sample.
Even in adolescents neck and back pain, have been significantly related to TMD pain (Nilsson et al. 2013). The severity of pain in the spinal region has been shown to affect the prevalence of TMD symptoms (both pain and dysfunction) in a mutual dose‒response like pattern (Wiesinger et al. 2009).
Reciprocity has also been found between the incidence of spinal pain and TMD signs in a prospective study on university students (Marklund et al. 2010b). Furthermore, it has been reported that patients with chronic craniomandibular pain often suffer from NSP and spinal pain (Visscher et al. 2001b). The exact causality of the observed co-morbidity is not known. The functional pattern shown between neck and jaw regions during rhythmical jaw movements indicates a synchronized motor control between the jaw and the upper spine (Eriksson et al. 1998, Eriksson et al. 2000), with activation of both jaw and neck muscles (Häggman-Henrikson et al. 2013). Stimulation of nociceptors in the temporomandibular joint area in cat activated the fusimotor-muscle spindle system of the dorsal neck muscles, suggesting that reflexes might be involved in the pathophysiological mechanisms responsible for the sensory‒motor disturbances in the neck region often found in
patients with temporomandibular disorders (Hellström et al. 2002). In healthy subjects the temporal coordination between the neck and the jaw system is high during normal jaw opening‒closing movements (Eriksson et
al. 2000, Zafar et al. 2000), but hampered in patients with a whiplash associated disorder (Häggman-Henrikson et al. 2002).

DISCUSSION
54
Chronic pain in the head and neckshoulder region has also been associated with mood disturbances and perceived impaired general state of health (Linton 2000, Croft et al. 2001, Rantala et al. 2003, Bingefors and Isacson 2004, Carroll et al. 2004).
The present study showed that the estimates on the ADL scale for TMD symptoms was influenced by the intensity of neck pain, the estimate on the ADL scale for headache was affected by the frequency and intensity of feelings of tiredness in the jaws and the estimate on the ADL scale for neck‒shoulder pain was influenced by the reported intensity of tiredness in
the jaws. The individual’s cognition of the symptoms’ interference with daily life (which may indicate a higher state of severity) seemed to share a pattern of mutual impact similar to that between trigeminal and spinal symptoms. The results support previous observations on a relationship between neck disability and jaw disability in a sample based on subjects who attended a TMD/orofacial pain clinic compared to healthy subjects (Olivo et al. 2010). This study in Sami women thus gives support to the observations that symptoms in trigeminal and spinal regions are closely interrelated.
Casecontrol study
The reasons why women outnumber men as TMD patients are still not fully understood. Women may pay more attention to their health, and may have more sensitive perceptions of the symptoms, feel higher levels of disability and impact on social life, and experience the symptoms for a longer duration and at higher intensity than men do. Factors related to sex or gender may predispose or increase the vulnerability of women to developing
longstanding pain and dysfunction, in general, as well as in the jawface region, which has powerful proprio- and nociception. Polymorphism of catecholamine-O-methyl transferase (Diatchenko et al. 2005) and serotonin (Ojima et al. 2007) as well as differences in the haplotypes of β receptors (Diatchenko et al. 2006) have been reported to be related to the development of TMD pain. This, together with the role of sex steroids and psychosocial factors, have formed the hypothesis of biopsychosocial mechanisms and increased vulnerability of certain individuals to developing pain and dysfunction in the jawface region (Diatchenko et al. 2006).
The significantly higher BMI of the cases may indicate that obesity is related to TMD in women. High levels of estrogen have been related both to higher BMI values (Olson et al. 2006) and to TMD pain (LeResche et al. 1997b). The link may thus relate to female hormones, physical activity levels, or both, and warrants more research. Factors that induce increased physical loading on the tissues involved may be individually significant and related to the individual’s reaction patterns and capacities (Wänman and Agerberg 1991). One major difference between cases and controls with regard to clinically registered variables was the pain

DISCUSSION
55
elicited when loading the muscles and the TMJ. One of the first studies to find differences between cases and controls with regard to submaximal clenching was that of Clark et al in 1984 (Clark et al. 1984). The finding of pain reactions on TMJ loading may indicate that the prevalence of arthralgia was higher than indicated by the RDC/TMD classification schema, in which tenderness to palpation over the joint area is an obligate criterion. The cases also presented a significantly higher proportion of pain reactions to palpation. These signs are often interpreted as indicating myofascial involvement, although recent research indicates that they may be inferred as indicating a reduced pain threshold to pressure (Svensson and Arendt-Nielson 2000). No major differences in the state of dental occlusion or variations in the specific examined occlusal factors were observed between cases and controls. The result thus support the opinion that factors in the dental occlusion do not have a predominate role in the perpetuation of musculoskeletal symptoms in the jawface region. The results are in line with the results of most previous epidemiological studies, which demonstrate that a similar variability of dental occlusal factors exists among subjects with and without TMD (Carlsson GE 2010). Contradictory results have also been presented. Artificial interferences were attached to the teeth in TMD patients previously treated with positive outcomes, and in controls. The study showed that the patients were more vulnerable to develop symptoms and more sensitive to the change than the controls (Le Bell et al. 2006). Some factors in the dental occlusion were identified as risk factors for incidence and persistence of TMD in a prospective study (Marklund and Wänman 2010a). The authors of the latter study expressed that a too simplistic view of the dental occlusion may be harmful to the individual patient with longstanding TMD signs and symptoms. Studies investigating causation should have a prospective design. Further, well controlled, and prospective studies in the future may help us to decide if the “occlusal door” should be ajar or closed.
Persistent pain in the jawface region may be caused by a focal neuropathic pain disorder (Clark 2006). Idiopathic pain conditions in the face are bothersome for the patient and difficult to manage. It has been hypothesized that neuropathic pain disorders may be related to changed perception of tactile stimulation (Jacobs et al. 2002). The tactile thresholds in the trigeminal innervated regions were thus tested with von Frey monofilaments. The cases and controls, however, responded uniformly to the tactile perception test. From my clinic experiences, patients with severe idiopathic facial pain conditions can present signs of both hypo-, and dysesthesia in the painful region of the face. One interpretation of the result may be that the population of approximately 500 included women was too small to capture such cases. The prevalence of these conditions may thus be counted per thousand.
Women with TMD considered their general health status as more impaired
than that of the controls which supplements and confirms the results of

DISCUSSION
56
previous studies (Agerberg and Carlsson 1975, Johansson et al. 2004, Yekkalam and Wänman 2014b). The significant and high likelihood of reporting impaired health among the cases was interesting, since the proportion of those under medical care due to disease did not differ significantly between cases and controls. This result should not be interpreted a direct correlation between the experience of symptoms in the jawface region and impaired general health. There may be several confounders of the results, such as co-morbid pain in other locations, with related sleep disturbances (Lobbezoo et al. 2004) and psychological distress (Visscher et al. 2001a).
Thematic interviews
Experiences of TMD
In the interview a choice was made to display a variety of beliefs towards and experiences of jaw, neck, and shoulder pains from the Sami women’s non-expert perspective. All informants with TMD also had neck and shoulder pains, headaches and tinnitus, and described, expressed, and regarded all these symptoms as a more or less unified condition. The pathophysiological background of such perception may be attributed to convergence of trigeminal and cervical nerves in the brainstem (Sessle et al. 1986, Piovesan et al. 2003). The women without TMD, headaches and NSP contributed with their thoughts regarding triggering factors, strains, distrust, and reconciliation. Most triggering factors were described in terms of inflicted injuries, but behavior, heredity, and life circumstances were all proposed and fit with the biopsychosocial model (Suvinen et al. 2005, Gatchel et al. 2007,). The model could therefore be used as a model for shared understanding in patient information and treatment sessions.
Proposed causes of TMD
A common statement among the participants with TMD symptoms was that
they were aware of clenching their teeth together. Bruxism (tooth clenching
and/or grinding) is one proposed etiological factor of TMD. The participants
comprehended that their biting behavior was a cause of their TMD problems.
Several studies have found relationships between reported bruxism and
TMD (Glaros and Burton 2004, Svensson et al. 2008). This relationship has,
however, been questioned with reference to the weakness in self-reported
bruxism and analyses mostly based on cross-sectional samples (Molina et al.
2000, van der Meulen et al. 2006). In a fairly recent systematic review on
bruxism and temporomandibular disorders (Manfredini and Lobbezoo
2010b), the authors concluded that self-reported bruxism was associated
with TMD pain, but that studies using more specific methods to diagnose
bruxism showed weaker association with TMD symptoms. The present study

DISCUSSION
57
gives support to the existence of a relationship between TMD and tooth
clenching habits, based on the participants’ narratives and experiences. A
habit of long-term, low-level clenching (holding teeth tightly together) might
thus be a significant factor in the development of longstanding TMD (Glaros
et al. 1998, Glaros and Williams 2012). In the case-control study, the cases
significantly more often reported awareness of tooth clenching habits than
the controls. Even a light clenching effort, referred to a tooth contact habit
with the maxillary and the mandibular teeth continuously in contact with
minimal force in a nonfunctional situation (Sato et al. 2006), may cause
strain of the TMJ and masticatory muscles. A habit of maintaining tooth
contact has been noted as a risk factor for development of myofascial pain
(Michelotti et al. 1997, Chen et al. 2007,). The strain may cause injury of
muscle fibers and reduce the blood supply to the muscle since perfusion is
impaired during clenching (Kim et al. 1999, Buzinelli and Berzin 2001,
Svensson et al. 2001, Nakamura et al. 2005). One of the most commonly
reported symptom in the questionnaire study, was feelings of tiredness in the
jaws which may be an effect of habitual nonfunctional tooth contact activity.
The results are thus in line with previously found associations between oral
parafunctions and TMD (Magnusson et al. 2000, Jacobs et al. 2002,
Johansson et al. 2004, Marklund and Wänman 2010a), indicating that these
jaw motor behavior patterns, especially tooth clenching and tongue pressing,
are significant in patients with TMD.
Distrust in healthcare
The Sami women shared experiences of distrust of both medical and dental health care services. Similar results were found in a qualitative study of chronic orofacial pain patients referred to a pain clinic (Wolf et al. 2006). The orofacial pain patients, however, expressed anger and frustration and regarded their pain as elusive. Such strong expressions were not used among these Sami women. This difference may be related to differences in the explicit dental health care situations and related expectations. Participants in the orofacial patient sample also expressed feelings of helplessness and a need to be taken care of (Wolf et al. 2006). The Sami women, on the other hand, indicated empowerment in their self-management and coping strategies, and gave examples of factors that provided them at least temporary pain relief. Both of these studies, however, indicate that the consultations are a critical event, which at least among those with longstanding pain has not favored recovery and rehabilitation. In an article by Eccleston and co-workers, responsibility, blame, and identity protection among pain patients and professionals were unfolded (Eccleston et al. 1997). The consequence of not being believed, and questioned, severely damages the trust between patient and caregiver. Such experiences may even prolong the pain and are less likely to motivate the patient to adherence to suggested

DISCUSSION
58
treatment strategies. The consultation event thus seems to be a potential area for development among physicians and dentists. The caregiver should pay attention to the patient’s own thoughts and beliefs, since this could be a good point of departure in the rehabilitation process.
Health aspects
Most participants shared thoughts regarding the healing and reconciliation processes. For these women, good health was equal to, and a prerequisite for, independence and freedom. The ability to work was thus an important keystone, together with the vision of physical fitness. Access to nature was also important. The participants reported various types of physical activities such as walking, running, skiing, and taking part in group training. Exercise is also recommended as an important part of rehabilitation in patients with chronic pain (SBU 2006). A study from the north of Norway showed that ethnic origin had an impact on the level of physical activity. Sami women were more active than the Norse women (Hermansen et al. 2002). The results indicated a common understanding of exercise being an important part of a coping strategy to stay healthy. All people are probably, at some point of their life, subjected to various strains, related to physical, psychological and/or social difficulties. The ways people succeed in facing these difficulties varies. Despite similar level of strains, some manage to stay healthy while others do not. Some of the results from the interviews can be viewed from a salutogenic perspective as proposed by Antonovski, (Antonovsky 2005). His model focuses on people’s resources and abilities to resist adversities, maintain health, and cope with negative stressors. An individual's capacity to handle stress and diseases depends on the extent to which life is experienced as meaningful, manageable and understandable all important keystones in the concept of sense of coherence. The Sami women, described difficulties, strains and life stressors, but some obviously remained healthy. The women without TMD described a social context in which they felt secure and presented various strategies to cope with strains. They described a strong social support, in accordance to the salutogenic model. It has been reported that a strong sense of coherence is associated with better health-related quality of life and self-efficacy as well as less catastrophizing thinking in patients with chronic pain (Chumbler et al. 2013). It was further concluded that sense of coherence may be an important factor for patients with chronic musculoskeletal pain. Efforts to strengthen empowerment and self-efficacy in individuals with pain and dysfunction in jaw, head, and neck, may be fruitful for both the individual and the society. I thus consider further studies with salutogenetic perspectives important, to gain increased knowledge in factors of importance for maintenance of the good health.

CLINICAL IMPLICATIONS & FUTURE PERSPECTIVES
59
Clinical implications and future perspectives
My vision of this research project was to follow a path of discovery from the
answers in a questionnaire down to the individual perspective among Sami
women. The gender perspective was chosen, since women outnumber men
as patients with TMD, and the Samis, since available surveys were limited
when the project started, and because they may be regarded as a fairly
homogenous population. The latter assumption may, however, be
questioned. In general terms, the observed prevalence of conditions examined was briefly in line with other population-based studies conducted during a fairly similar period, indicating that the findings are not specific to the Sami women, but may be considered valid for women in general. The results support previous studies on TMD and its dependence on age, affect on quality of life, relationship to other pain conditions, and awareness of oral parafunctions among the affected. From the narratives it was evident that many of the women with longstanding pain in the jaw‒face region had been treated with bite splints,
but they were not quite convinced about the effect. Splints are today advocated as a treatment of choice, and their positive effect has been shown in several studies (Swedish guidelines for dental health care in adults). There is, of course, no universal treatment effective for all individuals, and perhaps the selected women were those who did not respond to previous treatment strategies. Splints may be viewed as a fairly passive and conservative treatment approach. If the patient is not fully motivated, her compliance with the treatment may be hampered. From these perspectives an approach by dental health care providers that includes active listening, confirmation, motivation, and individually adjusted information is essential to build trust and reconciliation and improve adherence to treatment regimes. The management should be supportive and enhance the patient’s empowerment and self-efficacy to handle stress and strain and to take active part and responsibility in the rehabilitation process. An understanding of the patient’s social context and support should also be taken into consideration. A multidisciplinary approach is advocated for more severe cases, since the women with longstanding and more severe TMD also were affected by headaches, neck‒shoulder pain, and tinnitus. The remuneration system for
treatments of these patients in dental and medical care should, accordingly, for this group of patients be the same. Future studies should try to find answers to explain factors related to the observed decline of TMD symptoms and headaches with age. Rehabilitation in groups may be tested in patients with disabling TMD to elucidate whether that context can improve a sense of coherence, self-efficacy, and coping strategies for the benefit of the patient.

SUMMARY OF RESULTS
60
Summary of results
This investigation among Sami women in Arctic Sweden showed that
Symptoms indicative of temporomandibular disorders, headaches and neck‒shoulder pain were frequently reported and showed co-
morbidity in a cross-sectional analysis.
The most commonly reported symptoms indicative of temporomandibular disorders were feelings of tiredness of the jaws and temporomandibular joint sounds.
The prevalence of symptoms indicative of temporomandibular disorders and headaches diminished with age.
Symptoms indicative of temporomandibular disorders, headaches, and neck‒shoulder pain influenced daily life negatively. Seventeen
percent of the Sami women reported some disability related to their symptoms indicative of temporomandibular disorders.
Factors related to pain had the greatest influence when these Sami women rated the related impairment.
The individuals’ cognition of the symptoms’ interference with daily life showed a pattern of mutual influence between trigeminal and spinal areas.
Longstanding, severe, and frequent symptoms indicative of temporomandibular disorders remained essentially unchanged over a two-year follow-up period.
In the examined cases, a diagnosis according to the Research Diagnostic Criteria for Temporomandibular Disorders classification was established in 59%, and 91% had signs of dysfunction according to the clinical dysfunction index.
An impaired general state of health was commonly reported among women with temporomandibular disorders
The state of the dental occlusion was similar between the TMD cases and controls.
Women with TMD symptoms expressed awareness of habits of biting/holding teeth together, and a limited social support.

CONCLUSIONS & GENERATED HYPOTHESES
61
Conclusions and generated hypotheses
Women are commonly affected by symptoms in the jaw, head, and
neckshoulder region. Both pain and dysfunction symptoms in the temporomandibular region are related to disability and interference with daily life.
Sami women with longstanding TMD symptoms related their symptoms to fairly simple triggers and a more or less consistent jaw-clenching behavior, indicating that relieving such behaviors and related strains should be an essential element in treatment of patients with TMD.
Co-morbidity between symptoms in trigeminally and spinally innervated regions may affect both perpetuation of symptoms and related disability. This indicates that in management of patients with such symptoms, pain and dysfunction in both regions should be taken into consideration.
Women with TMD, associated headaches, and NSP may benefit from empowerment of their self-efficacy to handle stress and strain and also to take active part in their rehabilitation. An understanding of the patient’s social context and support may, in that coherence, be crucial to the outcome.
An approach by health care providers that includes active listening, confirmation, motivation, and individually adjusted information may help to build trust, reconciliation and improve adherence to treatment regimes. Group rehabilitation may also be tried in patients with disabling TMD to elucidate whether that context can improve a sense of coherence, self-efficacy, and coping strategies for the benefit of the individual patient.

ACKNOWLEDGMENTS
62
Acknowledgments
Completion of this thesis would not have been possible without support.
Many people have been involved, several of them throughout the long
journey, others for shorter periods of time—but with equally important
input. A collective “Thank you” to all of you who in one way or another have
helped, supported, and encouraged me during all these years. In particular, I
would like to thank the following:
Professor Anders Wänman, my main supervisor and mentor, for always
believing in me during this long research process. You have, with great
patience, never-ending support, and a big heart, throughout the years
encouraged me to finish this thesis, although at times it felt completely
impossible. Thanks for so generously sharing your enormous knowledge in
the field of clinical oral physiology, both in research and in the clinic. You
have inspired me since I was an undergraduate student, and especially
during my specialist training and PhD studies. Your door has always been
open, and you have given me your time whenever needed. I am so proud of
having been educated and clinically trained by you and to continue to be part
of your research team. I’ll always bring with me your wise advice; bib!
Professor emerita Eva E. Johansson, my co-supervisor, for giving me your
full support in the qualitative part of this project, despite the fact that you
came in late in the process. Your expertise has been tremendously valuable,
and your wisdom has inspired me during our work together.
Kerstin Hägg, my former co-supervisor, for valuable advice and comments
regarding my test interviews and the interview guide, when planning the
interview study.
Professor emeritus Per-Olof Eriksson, for valuable comments on the thesis,
and for nice conversations about Kiruna, over the years.
Dr. Susanna Marklund, Head of Specialisttandvården, for valuable
comments on the thesis, great encouragement in my research as well as in
my clinical work, and for sharing your excellent clinical expertise.
Ewa Lampa and Dr. Catharina Österlund, my specialist colleagues for good
company, many laughs, and pep talks, and for sharing your clinical skills.
Ewa, my roommate, it feels like Kiruna is just around the corner, and that
feels really good. Hoja!
ACKNOWLEDGMENTS
63
Dr. Birgitta Wiesinger, and Dr. Birgitta Häggman-Henrikson, for valuable
comments on this thesis, for good company, support and for sharing your
scientific knowledge.
Ann-Sofie Strandberg, Hjördis Olsson, and Lillemor Hägglund for
administrative support.
Colleagues and workmates at Specialisttandvården and at the Department of
Clinical Oral Physiology, for being supportive and for providing a good
working environment. Special thanks to my former boss, Eva Utterberg, who
always tried to do the best for me, trixing and fixing with schedules and so
on. Good luck with new challenges!
The Public Dental Health Service in Kiruna, Karesuando, and Gällivare, for
letting me carry out the clinical examinations there. Special thanks to Bitte
Lindgren, my former boss in Kiruna, for invaluable help when scheduling my
research time.
Lars Holmgren, Fredrik Wiklund and Hans Stenlund for statistical advice
and guidance.
Humbly, thank you to all the Sami women who participated in the study.
Without you this thesis would not have been possible. A special thank you to
the women in the interview study, who so openheartedly shared their life
experiences.
Professor Mikael Svonni, my uncle, for translation of the abstract into North
Sami, and for good dinner company when you were working in Umeå.
Marie Enoksson, at the Sami Parliament, for always, both at work and
privately, answering my questions about one thing or the other.
Anna-Lill Ledman and Charlotta Svonni, at the Centre for Sami Research, for
fruitful discussions about ethics in research involving Indigenous peoples.
Charlotta Svonni, my dear friend and cousin, for tremendous support, pep
talks, and fruitful discussions about everything in between heaven and earth.
And not forgetting all the excellent dinners, whenever needed, especially
when I was away from home during my specialist training. Lotta, I do not
think there is anyone outside the field of clinical oral physiology who knows
as much about TMD as you do, and I promise from now on, to be all ears
about the history of the nomadic school, until your defense of your own
thesis.

ACKNOWLEDGMENTS
64
Relatives and friends, thanks for just being there, keeping me in touch with
the world outside my project. Special thanks to Annika Josbrant and Annette
Svonni, my cousins (“big sisters”), for always having been around in my life,
with love and support.
My extended family, the Mienna family, for all the pleasant times together.
Next summer I promise to participate in more activities. Special thanks to
Máhtte for all “emergency” computer help.
My dear parents, Ingrid and Olav, for all your love and consideration.
Without you, neither my specialist nor my PhD studies would have been
possible. Thank you for all the support and help, for me and my family,
during all these years, with everything from household chores to carpentry
and childcare, and freezers full of meat, fish, and berries. Having moved to
Umeå certainly has some drawbacks!
Thorbjörn, my big brother, who has always taken care of your little sister.
Thanks for your thoughtfulness, your wisdom, your bravery, and your advice
in big and in small. Thanks to Jennifer, for friendship, and language advice.
Thanks to Molly Grace and Jackson, for hugs and laughs, although the hugs
are fewer the older you get. Love you all and miss you always. The USA is too
far away.
Alexander and Ole, the guys in my life, for your endless love and never-
ending support, and for putting things into perspective. Thank you, Ole, for
having taken so much responsibility at home, but from now on I will give you
more help. I promise both of you to be more present henceforward. Thanks
for giving me so much happiness and joy in life. Lucky me, for having you!
This work was financially supported by: Department of Odontology, Umeå
University; Västerbotten County Council; Norrbotten County Council; The
Sami Parliament in Sweden; Visare Norr/Northern County Councils; Göran
Gustafsson Foundation; Stiftelsen JC Kempes Memorial Fund and the
Swedish Dental Society.

REFERENCES
65
References
Agerberg, G. (1974) Maximal mandibular movements in young men and women. Sven Tandlak Tidskr, 67(2), pp. 81-100.
Agerberg, G. and Carlsson, G. E. (1975) Symptoms of functional disturbances of the masticatory system. A comparison of frequencies in a population sample and in a group of patients. Acta Odontol Scand, 33(4), pp. 183-90.
Agerberg, G. and Bergenholtz, A. (1989) Craniomandibular disorders in adult populations of West Bothnia, Sweden. Acta Odontol Scand, 47(3), pp. 129-40.
Alanen, P., Kuttila, M. and Le Bell, Y. (1997) Fluctuation of temporomandibular disorders in accordance with two classifications: the Helkimo dysfunction index and treatment need grouping. Acta Odontol Scand, 55(1), pp. 14-7.
Amft, A. (2000) Sápmi i förändringens tid-en studie av svenska samers levnadsvillkor under 1900-talet ur ett genus- och etnicitets perspektiv, Umeå: Thesis; Samiska studier, Umeå university.
Anastassaki, A. and Magnusson, T. (2004) Patients referred to a specialist clinic because of suspected temporomandibular disorders: a survey of 3194 patients in respect of diagnoses, treatments, and treatment outcome. Acta Odontol Scand, 62(4), pp. 183-92.
Anastassaki Köhler, A., Helkimo, A. N., Magnusson, T. and Hugoson, A. (2009) Prevalence of symptoms and signs indicative of temporomandibular disorders in children and adolescents. A cross-sectional epidemiological investigation covering two decades. Eur Arch Paediatr Dent, 10 Suppl 1, pp. 16-25.
Anastassaki Köhler, A., Hugoson, A. and Magnusson, T. (2012) Prevalence of symptoms indicative of temporomandibular disorders in adults: cross-sectional epidemiological investigations covering two decades. Acta Odontol Scand, 70(3), pp. 213-23.
Anderson, G. C., John, M. T., Ohrbach, R., Nixdorf, D. R., Schiffman, E. L., Truelove, E. S. and List, T. (2011) Influence of headache frequency on clinical signs and symptoms of TMD in subjects with temple headache and TMD pain. Pain, 152(4), pp. 765-71.

REFERENCES
66
Andersson, H. I., Ejlertsson, G., Leden, I. and Rosenberg, C. (1993) Chronic pain in a geographically defined general population: studies of differences in age, gender, social class, and pain localization. Clin J Pain, 9(3), pp. 174-82.
Antonovsky, A. (2005) Hälsans mysterium, Andra utgåvan, Stockholm: Natur och Kultur.
Ballegaard, V., Thede-Schmidt-Hansen, P., Svensson, P. and Jensen, R. (2008) Are headache and temporomandibular disorders related? A blinded study. Cephalalgia, 28(8), pp. 832-41.
Barros Vde, M., Seraidarian, P. I., Cortes, M. I. and de Paula, L. V. (2009) The impact of orofacial pain on the quality of life of patients with temporomandibular disorder. J Orofac Pain, 23(1), pp. 28-37.
Beckman, L. (1996) Samerna-en genetiskt unik urbefolkning: fyra decenniers genetiska studier av svenska samer-från blodgrupper till mitokondriellt DNA, Umeå: Thesis; Institutionen för medicinsk genetik, Umeå universitet. .
Bingefors, K. and Isacson, D. (2004) Epidemiology, co-morbidity, and impact on health-related quality of life of self-reported headache and musculoskeletal pain--a gender perspective. Eur J Pain, 8(5), pp. 435-50.
Boardman, H. F., Thomas, E., Croft, P. R. and Millson, D. S. (2003) Epidemiology of headache in an English district. Cephalalgia, 23(2), pp. 129-37.
Bovim, G., Schrader, H. and Sand, T. (1994) Neck pain in the general population. Spine, 19(12), pp. 1307-9.
Buzinelli, R. V. and Berzin, F. (2001) Electromyographic analysis of fatigue in temporalis and masseter muscles during continuous chewing. J Oral Rehabil, 28(12), pp. 1165-7.
Cairns, B. E. and Gazerani, P. (2009) Sex-related differences in pain. Maturitas, 63(4), pp. 292-6.
Cairns, B. E. (2010) Pathophysiology of TMD pain--basic mechanisms and
their implications for pharmacotherapy. J Oral Rehabil, 37(6), pp. 391-410.
Carlsson, G. E. (1984) Epidemiological studies of signs and symptoms of temporomandibular joint-pain-dysfunction. A literature review. Aust Prosthodont Soc Bull, 14, pp. 7-12.

REFERENCES
67
Carlsson, G. E. (1999) Epidemiology and treatment need for temporomandibular disorders. J Orofac Pain, 13(4), pp. 232-7.
Carlsson, G. E. (2010) Some dogmas related to prosthodontics, temporomandibular disorders and occlusion. Acta Odontol Scand, 68(6), pp. 313-22.
Carlsson, G. E., Ekbäck, G., Johansson, A., Ordell, S. and Unell, L. (2014) Is there a trend of decreasing prevalence of TMD-related symptoms with ageing among the elderly? Acta Odontol Scand, Epub; March 25, 2014. (doi:10.3109/00016357.2014.898787)
Carroll, L. J., Cassidy, J. D. and Côte, P. (2004) Depression as a risk factor for onset of an episode of troublesome neck and low back pain. Pain, 107(1-2), pp. 134-9.
Chen, C. Y., Palla, S., Erni, S., Sieber, M. and Gallo, L. M. (2007) Nonfunctional tooth contact in healthy controls and patients with myogenous facial pain. J Orofac Pain, 21(3), pp. 185-93.
Chumbler, N. R., Kroenke, K., Outcalt, S., Bair, M. J., Krebs, E., Wu, J. and Yu, Z. (2013) Association between sense of coherence and health-related quality of life among primary care patients with chronic musculoskeletal pain. Health Qual Life Outcomes, 11, pp. 216.
Ciancaglini, R. and Radaelli, G. (2001) The relationship between headache and symptoms of temporomandibular disorder in the general population. J Dent, 29(2), pp. 93-8.
Clark, G. T., Beemsterboer, P. L. and Jacobson, R. (1984) The effect of sustained submaximal clenching on maximum bite force in myofascial pain dysfunction patients. J Oral Rehabil, 11(4), pp. 387-91.
Clark, G. T. (2006) Persistent orodental pain, atypical odontalgia, and phantom tooth pain: when are they neuropathic disorders? J Calif Dent Assoc, 34(8), pp. 599-609.
Conti, P. C., de Azevedo, L. R., de Souza, N. V. and Ferreira, F. V. (2001) Pain measurement in TMD patients: evaluation of precision and sensitivity of different scales. J Oral Rehabil, 28(6), pp. 534-9.
Cooper, B. C. and Kleinberg, I. (2009) Relationship of temporomandibular disorders to muscle tension-type headaches and a neuromuscular orthosis approach to treatment. Cranio, 27(2), pp. 101-8.
REFERENCES
68
Costen JB. (1934) Syndrome of ear and sinus symptoms dependent upon
functions of the temporomandibular joint, Ann Otol Rhinol Laryngol 3: 1-4,
1934.
Côte, P., Cassidy, J. D. and Carroll, L. (1998) The Saskatchewan Health and Back Pain Survey. The prevalence of neck pain and related disability in Saskatchewan adults. Spine, 23(15), pp. 1689-98.
Creswell, J. W. (1998) Qualitative inquiry and research design: choosing among five traditions, London: SAGE.
Creswell, J. W. (2003) Research design: qualitative, quantitative, and mixed methods approaches, 2. ed., Thousand Oaks: Sage.
Croft, P. R., Lewis, M., Papageorgiou, A. C., Thomas, E., Jayson, M. I., Macfarlane, G. J. and Silman, A. J. (2001) Risk factors for neck pain: a longitudinal study in the general population. Pain, 93(3), pp. 317-25.
Daerga, L., Edin-Liljegren, A. and Sjölander, P. (2004) Work-related musculoskeletal pain among reindeer herding Sami in Sweden--a pilot study on causes and prevention. Int J Circumpolar Health, 63 Suppl 2, pp. 343-8.
Dahlgren, L., Emmelin, M., Winkvist, A. and Lindhgren, M. (2004) Qualitative methodology for international public health, Umeå: Epidemiology and Public Health Sciences, Department of Public Health and Clinical Medicine, Umeå University.
Dahlström, L. and Carlsson, G. E. (2010) Temporomandibular disorders and oral health-related quality of life. A systematic review. Acta Odontol Scand, 68(2), pp. 80-5.
Dao, T. T. and LeResche, L. (2000) Gender differences in pain. J Orofac Pain, 14(3), pp. 169-84; discussion 184-95.
De Boever, J. A. and Carlsson, G. E. (1994) Etiology and differential diagnosis. in Zarb, G. A., Carlsson, G. E., Sessle, B. J. and Mohl, N. D., (eds.) Temporomandibular joint and masticatory muscle disorders,Copenhagen: Munksgaard. pp. 171-207.
De Boever, J. A., Carlsson, G. E. and Klineberg, I. J. (2000) Need for occlusal therapy and prosthodontic treatment in the management of temporomandibular disorders. Part I. Occlusal interferences and occlusal adjustment. J Oral Rehabil, 27(5), pp. 367-79.

REFERENCES
69
De Kanter, R. J., Truin, G. J., Burgersdijk, R. C., Van 't Hof, M. A., Battistuzzi, P. G., Kalsbeek, H. and Käyser, A. F. (1993) Prevalence in the Dutch adult population and a meta-analysis of signs and symptoms of temporomandibular disorder. J Dent Res, 72(11), pp. 1509-18.
de Leeuw, R. (2008) Temporomandibular disorders. in de Leeuw, R., (ed.) Orofacial pain: Guidelines for assessment, diagnosis, and management,Hannover Park: Quintessence Publishing Co, Inc. pp. 129-204.
Diatchenko, L., Slade, G. D., Nackley, A. G., Bhalang, K., Sigurdsson, A., Belfer, I., Goldman, D., Xu, K., Shabalina, S. A., Shagin, D., Max, M. B., Makarov, S. S. and Maixner, W. (2005) Genetic basis for individual variations in pain perception and the development of a chronic pain condition. Hum Mol Genet, 14(1), pp. 135-43.
Diatchenko, L., Anderson, A. D., Slade, G. D., Fillingim, R. B., Shabalina, S. A., Higgins, T. J., Sama, S., Belfer, I., Goldman, D., Max, M. B., Weir, B. S. and Maixner, W. (2006) Three major haplotypes of the beta2 adrenergic receptor define psychological profile, blood pressure, and the risk for development of a common musculoskeletal pain disorder. Am J Med Genet B Neuropsychiatr Genet, 141b(5), pp. 449-62.
DO 2008:1. Pikkarainen, H., Brodin, B. (2008) Diskriminering av samer
samers rättigheter ur ett diskrimineringsperspektiv. DO:s rapportserie 2008:1., Ombudsmannen mot etnisk diskriminering (DO), Stockholm, ISBN 978-91-973654-4-4.
DO 2008:2. Pikkarainen, H., Brodin, B. (2008) Diskriminering av nationella minoriteter inom utbildningsväsendet. DO:s rapportserie 2008:2., Ombudsmannen mot etnisk diskriminering (DO), Stockholm, ISBN 978-91-973654-9-9.
Drangsholt, M. and LeResche, L. (1999) Temporomandibular Disorder Pain. in Crombie., I. K., (ed.) Epidemiology of Pain,Seattle: IASP press. pp. 203-233.
Dworkin, S. F. and LeResche, L. (1992) Research diagnostic criteria for temporomandibular disorders: review, criteria, examinations and specifications, critique. J Craniomandib Disord, 6(4), pp. 301-55.
Eccleston, C., Williams, A. C. and Rogers, W. S. (1997) Patients' and professionals' understandings of the causes of chronic pain: blame, responsibility and identity protection. Soc Sci Med, 45(5), pp. 699-709.
REFERENCES
70
Edin-Liljegren, A., Hassler, S., Sjölander, P. and Daerga, L. (2004) Risk factors for cardiovascular diseases among Swedish Sami-a controlled cohort study. Int J Circumpolar Health, 63 Suppl 2, pp. 292-7.
Eichner, K. (1955) Über eine Gruppeneinteilung des Lückengebisses für die Prothetik. Dtsche Zahnärztl Z, 10, pp. 1831-1834.
Eriksson, P. O., Zafar, H. and Nordh, E. (1998) Concomitant mandibular and head-neck movements during jaw opening-closing in man. J Oral Rehabil, 25(11), pp. 859-70.
Eriksson, P. O., Häggman-Henrikson, B., Nordh, E. and Zafar, H. (2000) Co-ordinated mandibular and head-neck movements during rhythmic jaw activities in man. J Dent Res, 79(6), pp. 1378-84.
Fillingim, R. B. (2000) Sex, gender, and pain: women and men really are different. Curr Rev Pain, 4(1), pp. 24-30.
Fricton, J. R. and Schiffman, E. L. (1986) Reliability of a craniomandibular index. J Dent Res, 65(11), pp. 1359-64.
Garro, L., Stephenson, K. and Good, B. (1994) Chronic illness of the temporomandibular joints as experienced by support-group members. J Gen Intern Med, 9(7), pp. 372-8.
Gatchel, R. J., Peng, Y. B., Peters, M. L., Fuchs, P. N. and Turk, D. C. (2007) The biopsychosocial approach to chronic pain: scientific advances and future directions. Psychol Bull, 133(4), pp. 581-624.
Glaros, A. G., Tabacchi, K. N. and Glass, E. G. (1998) Effect of parafunctional clenching on TMD pain. J Orofac Pain, 12(2), pp. 145-52.
Glaros, A. G. and Burton, E. (2004) Parafunctional clenching, pain, and effort in temporomandibular disorders. J Behav Med, 27(1), pp. 91-100.
Glaros, A. G. and Williams, K. (2012) Tooth contact versus clenching: oral parafunctions and facial pain. J Orofac Pain, 26(3), pp. 176-80.
Glaser, B. G. and Strauss, A. L. (1967) The discovery of grounded theory : strategies for qualitative research, Observations, Chicago,: Aldine.
Goncalves, D. A., Bigal, M. E., Jales, L. C., Camparis, C. M. and Speciali, J. G. (2010) Headache and symptoms of temporomandibular disorder: an epidemiological study. Headache, 50(2), pp. 231-41.
REFERENCES
71
Greenberg, R. S., Daniels, S. R., Flanders, W. D., Eley, J. W. and Boring, J. R. (2001) Medical Epidemiology, 3rd ed., USA: The McGraw-Hill Companies, Inc.
Göbel, H., Petersen-Braun, M. and Soyka, D. (1994) The epidemiology of headache in Germany: a nationwide survey of a representative sample on the basis of the headache classification of the International Headache Society. Cephalalgia, 14(2), pp. 97-106.
Hassler, S., Sjölander, P. and Ericsson, A. J. (2004a) Construction of a database on health and living conditions of the Swedish Sami population. Befolkning och bosättning i norr: Etnicitet, identitet och gränser i historiens sken., Miscellaneous publications no.1, pp. 107-124.
Hassler, S., Sjölander, P., Johansson, R., Grönberg, H. and Damber, L. (2004b) Fatal accidents and suicide among reindeer-herding Sami in Sweden. Int J Circumpolar Health, 63 Suppl 2, pp. 384-8.
Hassler, S., Johansson, R., Sjölander, P., Grönberg, H. and Damber, L. (2005) Causes of death in the Sami population of Sweden, 1961-2000. Int J Epidemiol, 34(3), pp. 623-9.
Hassler, S., Sjölander, P., Grönberg, H., Johansson, R. and Damber, L. (2008a) Cancer in the Sami population of Sweden in relation to lifestyle and genetic factors. Eur J Epidemiol, 23(4), pp. 273-80.
Hassler, S., Soininen, L., Sjölander, P. and Eero, P. (2008b) Cancer among the Sami-a review on the Norwegian, Swedish and Finnish Sami populations. Int J Circumpolar Health, 67(5), pp. 421-32.
Hasvold, T. and Johnsen, R. (1993) Headache and neck or shoulder pain--frequent and disabling complaints in the general population. Scand J Prim Health Care, 11(3), pp. 219-24.
Helkimo, M., Carlsson, G. E., Hedegård, B., Helkimo, E. and Lewin, T. (1972) Function and dysfunction of the masticatory system in Lapps in northern Finland. Preliminary report of an epidemiological investigation. Sven Tandlak Tidskr, 65(2), pp. 95-105.
Helkimo, M. (1974a) Studies on function and dysfunction of the masticatory system. I. An epidemiological investigation of symptoms of dysfunction in Lapps in the north of Finland. Proc Finn Dent Soc, 70(2), pp. 37-49.

REFERENCES
72
Helkimo, M. (1974b) Studies on function and dysfunction of the masticatory system. II. Index for anamnestic and clinical dysfunction and occlusal state. Sven Tandlak Tidskr, 67(2), pp. 101-21.
Helkimo, M. (1974c) Studies on function and dysfunction of the masticatory system. IV. Age and sex distribution of symptoms of dysfunction of the masticatory system in Lapps in the north of Finland. Acta Odontol Scand, 32(4), pp. 255-67.
Helkimo, M. (1976) Epidemiological surveys of dysfunction of the masticatory system. Oral Sci Rev, 7, pp. 54-69.
Hellström, F., Thunberg, J., Bergenheim, M., Sjölander, P., Pedersen, J. and Johansson, H. (2000) Elevated intramuscular concentration of bradykinin in jaw muscle increases the fusimotor drive to neck muscles in the cat. J Dent Res, 79(10), pp. 1815-22.
Hellström, F., Thunberg, J., Bergenheim, M., Sjölander, P., Djupsjöbacka, M. and Johansson, H. (2002) Increased intra-articular concentration of bradykinin in the temporomandibular joint changes the sensitivity of muscle spindles in dorsal neck muscles in the cat. Neurosci Res, 42(2), pp. 91-9.
Henrikson, T. (1999) Temporomandibular disorders and mandibular function in relation to Class II malocclusion and orthodontic treatment. A controlled, prospective and longitudinal study. Swed Dent J Suppl, 134, pp. 1-144.
Hermansen, R., Njolstad, I. and Fonnebo, V. (2002) Physical activity according to ethnic origin in Finnmark county, Norway. The Finnmark Study. Int J Circumpolar Health, 61(3), pp. 189-200.
Hunt, P. (2007) Report of the Special Rapporteur on the right of everyone to enjoyment of the highest attainable standard of physical and mental health. UN: Human rights council, A/HRC/4/28/add.2.
Häggman-Henrikson, B., Zafar, H. and Eriksson, P. O. (2002) Disturbed jaw behavior in whiplash-associated disorders during rhythmic jaw movements. J Dent Res, 81(11), pp. 747-51.
Häggman-Henrikson, B., Nordh, E. and Eriksson, P. O. (2013) Increased sternocleidomastoid, but not trapezius, muscle activity in response to increased chewing load. Eur J Oral Sci, 121(5), pp. 443-9.

REFERENCES
73
Jacobs, R., Wu, C. H., Goossens, K., Van Loven, K., Van Hees, J. and Van Steenberghe, D. (2002) Oral mucosal versus cutaneous sensory testing: a review of the literature. J Oral Rehabil, 29(10), pp. 923-50.
Jagger, R. G., Woolley, S. M. and Savio, L. (2004) Signs and symptoms of temporomandibular disorders in Ecuadorian Indians. J Oral Rehabil, 31(4), pp. 293-7.
Jedel, E., Carlsson, J. and Stener-Victorin, E. (2007) Health-related quality of life in child patients with temporomandibular disorder pain. Eur J Pain, 11(5), pp. 557-63.
Jensen, R. (1999) Pathophysiological mechanisms of tension-type headache: a review of epidemiological and experimental studies. Cephalalgia, 19(6), pp. 602-21.
Johansson, A., Unell, L., Carlsson, G., Söderfeldt, B. and Halling, A. (2003) Gender difference in symptoms related to temporomandibular disorders in a population of 50-year-old subjects. J Orofac Pain, 17(1), pp. 29-35.
Johansson, A., Unell, L., Carlsson, G., Söderfeldt, B., Halling, A. and Widar, F. (2004) Associations between social and general health factors and symptoms related to temporomandibular disorders and bruxism in a population of 50-year-old subjects. Acta Odontol Scand, 62(4), pp. 231-7.
Johansson, A., Vavruch-Nilsson, V., Edin-Liljegren, A., Sjölander, P. and Gyllensten, U. (2005) Linkage disequilibrium between microsatellite markers in the Swedish Sami relative to a worldwide selection of populations. Hum Genet, 116(1-2), pp. 105-13.
John, M. T., Miglioretti, D. L., LeResche, L., Von Korff, M. and Critchlow, C. W. (2003) Widespread pain as a risk factor for dysfunctional temporomandibular disorder pain. Pain, 102(3), pp. 257-63.
John, M. T., Reissmann, D. R., Schierz, O. and Wassell, R. W. (2007) Oral health-related quality of life in patients with temporomandibular disorders. J Orofac Pain, 21(1), pp. 46-54.
Kim, Y. J., Kuboki, T., Tsukiyama, Y., Koyano, K. and Clark, G. T. (1999) Haemodynamic changes in human masseter and temporalis muscles induced by different levels of isometric contraction. Arch Oral Biol, 44(8), pp. 641-50.

REFERENCES
74
Kirveskari, P. and Alanen, P. (1984) Effect of occlusal treatment on sick leaves in TMJ dysfunction patients with head and neck symptoms. Community Dent Oral Epidemiol, 12(2), pp. 78-81.
Kitai, N., Takada, K., Yasuda, Y., Verdonck, A. and Carels, C. (1997) Pain and other cardinal TMJ dysfunction symptoms: a longitudinal survey of Japanese female adolescents. J Oral Rehabil, 24(10), pp. 741-8.
Klassen, A. C., Creswell, J., Plano Clark, V. L., Smith, K. C. and Meissner, H. I. (2012) Best practices in mixed methods for quality of life research. Qual Life Res, 21(3), pp. 377-80.
Komiyama, O., Arai, M., Kawara, M., Kobayashi, K. and De Laat, A. (2005) Pain patterns and mandibular dysfunction following experimental trapezius muscle pain. J Orofac Pain, 19(2), pp. 119-26.
Kuttila, M., Niemi, P. M., Kuttila, S., Alanen, P. and Le Bell, Y. (1998) TMD treatment need in relation to age, gender, stress, and diagnostic subgroup. J Orofac Pain, 12(1), pp. 67-74.
Könönen, M. and Nyström, M. (1993) A longitudinal study of craniomandibular disorders in Finnish adolescents. J Orofac Pain, 7(4), pp. 329-36.
Le Bell, Y., Niemi, P. M., Jamsa, T., Kylmala, M. and Alanen, P. (2006) Subjective reactions to intervention with artificial interferences in subjects with and without a history of temporomandibular disorders. Acta Odontol Scand, 64(1), pp. 59-63.
Ledman, A. L. (2012a) Att representera och representeras: samiska kvinnor i svensk och samisk press 1966-2006, Skrifter från Centrum för samisk forskning,, Umeå: Thesis; Institutionen för idé- och samhällsstudier, Umeå universitet.
Ledman, A. L. (2012b) Att utmana koloniala strukturer -etik i samiskrelaterad forskning. BÅRJÅS, pp. 37-47.
LeResche, L. (1997a) Epidemiology of temporomandibular disorders: implications for the investigation of etiologic factors. Crit Rev Oral Biol Med, 8(3), pp. 291-305.
LeResche, L., Saunders, K., Von Korff, M. R., Barlow, W. and Dworkin, S. F. (1997b) Use of exogenous hormones and risk of temporomandibular disorder pain. Pain, 69(1-2), pp. 153-60.
REFERENCES
75
Linton, S. J. (2000) A review of psychological risk factors in back and neck pain. Spine (Phila Pa 1976), 25(9), pp. 1148-56.
List, T. and Helkimo, M. (1995) A scale for measuring the activities of daily living (ADL) of patients with craniomandibular disorders. Swed Dent J, 19(1-2), pp. 33-40.
List, T., Wahlund, K., Wenneberg, B. and Dworkin, S. F. (1999) TMD in children and adolescents: prevalence of pain, gender differences, and perceived treatment need. J Orofac Pain, 13(1), pp. 9-20.
List, T., Wahlund, K. and Larsson, B. (2001) Psychosocial functioning and dental factors in adolescents with temporomandibular disorders: a case-control study. J Orofac Pain, 15(3), pp. 218-27.
Lobbezoo, F., Visscher, C. M. and Naeije, M. (2004) Impaired health status, sleep disorders, and pain in the craniomandibular and cervical spinal regions. Eur J Pain, 8(1), pp. 23-30.
Locker, D. (1988) The symptom iceberg in dentistry. Treatment-seeking in relation to oral and facial pain. J Can Dent Assoc, 54(4), pp. 271-4.
Lundeen, T. F., Levitt, S. R. and McKinney, M. W. (1986) Discriminative ability of the TMJ scale: age and gender differences. J Prosthet Dent, 56(1), pp. 84-92.
Lundmark, L. (2007) Allt som kan mätas är inte vetenskap en populärhistorisk skrift om Rasbiologiska institutet, Stockholm: Forum för levande historia.
Macfarlane, T. V., Blinkhorn, A. S., Davies, R. M., Kincey, J. and Worthington, H. V. (2003) Factors associated with health care seeking behaviour for orofacial pain in the general population. Community Dent Health, 20(1), pp. 20-6.
Magnusson, T., Egermark-Eriksson, I. and Carlsson, G. E. (1985) Four-year longitudinal study of mandibular dysfunction in children. Community Dent Oral Epidemiol, 13(2), pp. 117-20.
Magnusson, T., Egermark, I. and Carlsson, G. E. (2000) A longitudinal epidemiologic study of signs and symptoms of temporomandibular disorders from 15 to 35 years of age. J Orofac Pain, 14(4), pp. 310-9.

REFERENCES
76
Manfredini, D., Piccotti, F., Ferronato, G. and Guarda-Nardini, L. (2010a) Age peaks of different RDC/TMD diagnoses in a patient population. J Dent, 38(5), pp. 392-9.
Manfredini, D. and Lobbezoo, F. (2010b). Relationship between bruxism and temporomandibular disorders: a systematic review of literature from 1998 to 2008. Oral Surg Oral Med Oral Pathol Oral Radiol Endod, 109(6), pp. e26-50 (doi: 10.1016/j.tripleo.2010.02.013).
Marklund, S. and Wänman, A. (2010a) Risk factors associated with incidence and persistence of signs and symptoms of temporomandibular disorders. Acta Odontol Scand, 68(5), pp. 289-99.
Marklund, S., Wiesinger, B. and Wänman, A. (2010b) Reciprocal influence on the incidence of symptoms in trigeminally and spinally innervated areas. Eur J Pain, 14(4), pp. 366-71.
Marklund, S., Häggman-Henrikson, B. and Wänman, A. (2014) Risk factors associated with incidence and persistence of frequent headaches. Acta Odontol Scand. Epub; April 7, 2014. (doi:10.3109/00016357.2014.906652)
Michelotti, A., Farella, M., Vollaro, S. and Martina, R. (1997) Mandibular rest position and electrical activity of the masticatory muscles. J Prosthet Dent, 78(1), pp. 48-53.
Molina, O. F., dos Santos Junior, J., Nelson, S. J. and Nowlin, T. (2000) Profile of TMD and Bruxer compared to TMD and nonbruxer patients regarding chief complaint, previous consultations, modes of therapy, and chronicity. Cranio, 18(3), pp. 205-19.
Morse, J. M. (1992) Qualitative health research, Newbury Park, Calif. ; London: Sage.
Murray, H., Locker, D., Mock, D. and Tenenbaum, H. C. (1996) Pain and the quality of life in patients referred to a craniofacial pain unit. J Orofac Pain, 10(4), pp. 316-23.
Nakamura, Y., Torisu, T., Noguchi, K. and Fujii, H. (2005) Changes in masseter muscle blood flow during voluntary isometric contraction in humans. J Oral Rehabil, 32(8), pp. 545-51.
Nilsson, I. M., List, T. and Drangsholt, M. (2007) Incidence and temporal patterns of temporomandibular disorder pain among Swedish adolescents. J Orofac Pain, 21(2), pp. 127-32.
REFERENCES
77
Nilsson, I. M., Drangsholt, M. and List, T. (2009) Impact of temporomandibular disorder pain in adolescents: differences by age and gender. J Orofac Pain, 23(2), pp. 115-22.
Nilsson, I. M., List, T. and Willman, A. (2011) Adolescents with temporomandibular disorder pain-the living with TMD pain phenomenon. J Orofac Pain, 25(2), pp. 107-16.
Nilsson, I. M., List, T. and Drangsholt, M. (2013) Headache and co-morbid pains associated with TMD pain in adolescents. J Dent Res, 92(9), pp. 802-7.
Nilsson, L. M., Dahlgren, L., Johansson, I., Brustad, M., Sjölander, P. and Van Guelpen, B. (2011) Diet and lifestyle of the Sami of southern Lapland in the 1930s--1950s and today. Int J Circumpolar Health, 70(3), pp. 301-18.
Nilsson, L. M. (2012) Sami lifestyle and health epidemiological studies from northern Sweden, Umeå: Thesis; Folkhälsa och klinisk medicin, näringsfroskning, Umeå university.
Nydell, A., Helkimo, M. and Koch, G. (1994) Craniomandibular disorders in childrena critical review of the literature. Swed Dent J, 18(5), pp. 191-205.
Näyhä, S., Videman, T., Laakso, M. and Hassi, J. (1991) Prevalence of low back pain and other musculoskeletal symptoms and their association with work in Finnish reindeer herders. Scand J Rheumatol, 20(6), pp. 406-13.
Oilo, G., Dahl, B. L., Hatle, G. and Gad, A. L. (1987) An index for evaluating wear of teeth. Acta Odontol Scand, 45(5), pp. 361-5.
Ojima, K., Watanabe, N., Narita, N. and Narita, M. (2007) Temporomandibular disorder is associated with a serotonin transporter gene polymorphism in the Japanese population. Biopsychosoc Med, 1, pp. 3.
Okeson, J. P. (2008) Etiology of functional disturbances in the masticatory system. in Okeson, J. P., (ed.) Management of Temporomandibular disorders and occlusion,St Louis, Missouri: Mosby. pp. 130-163.
Olivo, S. A., Fuentes, J., Major, P. W., Warren, S., Thie, N. M. and Magee, D. J. (2010) The association between neck disability and jaw disability. J Oral Rehabil, 37(9), pp. 670-9.

REFERENCES
78
Olson, M. B., Shaw, L. J., Kaizar, E. E., Kelsey, S. F., Bittner, V., Reis, S. E., Smith, K., Braunstein, G. D., Berga, S. L., Johnson, B. D. and Bairey Merz, C. N. (2006) Obesity distribution and reproductive hormone levels in women: a report from the NHLBI-sponsored WISE Study. J Womens Health (Larchmt), 15(7), pp. 836-42.
Omma, L. (2013) Ung same i Sverige : livsvillkor, självvärdering och hälsa, Umeå University medical dissertations,, Umeå: Clinical Sciences Psychiatry Umeå university.
Parker, M. W. (1990) A dynamic model of etiology in temporomandibular disorders. J Am Dent Assoc, 120(3), pp. 283-90.
Perri, R., Huta, V., Pinchuk, L., Pinchuk, C., Ostry, D. J. and Lund, J. P. (2008) Initial Investigation of the relation between extended computer use and temporomandibular joint disorders. J Can Dent Assoc, 74(7), pp. 643.
Piovesan, E. J., Kowacs, P. A. and Oshinsky, M. L. (2003) Convergence of cervical and trigeminal sensory afferents. Curr Pain Headache Rep, 7(5), pp. 377-83.
Polit, D. F. and Beck, C. T. (2006) Essentials of nursing research : methods, appraisal, and utilization, 6. ed., Philadelphia: Lippincott.
Radtke, A. and Neuhauser, H. (2009) Prevalence and burden of headache and migraine in Germany. Headache, 49(1), pp. 79-89.
Rantala, M. A., Ahlberg, J., Suvinen, T. I., Nissinen, M., Lindholm, H., Savolainen, A. and Kononen, M. (2003) Temporomandibular joint related painless symptoms, orofacial pain, neck pain, headache, and psychosocial factors among non-patients. Acta Odontol Scand, 61(4), pp. 217-22.
Rasmussen, B. K., Jensen, R., Schroll, M. and Olesen, J. (1991) Epidemiology of headache in a general population--a prevalence study. J Clin Epidemiol, 44(11), pp. 1147-57.
Reissmann, D. R., John, M. T., Schierz, O. and Wassell, R. W. (2007) Functional and psychosocial impact related to specific temporomandibular disorder diagnoses. J Dent, 35(8), pp. 643-50.
Rener-Sitar, K., Celebic, A., Stipetic, J., Marion, L., Petricevic, N. and Zaletel-Kragelj, L. (2008) Oral health related quality of life in Slovenian patients with craniomandibular disorders. Coll Antropol, 32(2), pp. 513-7.

REFERENCES
79
Salonen, L., Hellden, L. and Carlsson, G. E. (1990) Prevalence of signs and symptoms of dysfunction in the masticatory system: an epidemiologic study in an adult Swedish population. J Craniomandib Disord, 4(4), pp. 241-50.
Sarlani, E., Grace, E. G., Reynolds, M. A. and Greenspan, J. D. (2004) Evidence for up-regulated central nociceptive processing in patients with masticatory myofascial pain. J Orofac Pain, 18(1), pp. 41-55.
Sato, F., Kino, K., Sugisaki, M., Haketa, T., Amemori, Y., Ishikawa, T., Shibuya, T., Amagasa, T., Shibuya, T., Tanabe, H., Yoda, T., Sakamoto, I., Omura, K. and Miyaoka, H. (2006) Teeth contacting habit as a contributing factor to chronic pain in patients with temporomandibular disorders. J Med Dent Sci, 53(2), pp. 103-9.
SBU (2006) Methods for the treatment of croncic pain. A systematic literature review., SBU report no.177/1, Stockholm: Swedish Council and Technology Assessment in Healthcare (SBU).
Scher, A. I., Stewart, W. F., Liberman, J. and Lipton, R. B. (1998) Prevalence of frequent headache in a population sample. Headache, 38(7), pp. 497-506.
Schiffman, E., Ohrbach, R., Truelove, E., Look, J., Anderson, G., Goulet, J. P., List, T., Svensson, P., Gonzalez, Y., Lobbezoo, F., Michelotti, A., Brooks, S. L., Ceusters, W., Drangsholt, M., Ettlin, D., Gaul, C., Goldberg, L. J., Haythornthwaite, J. A., Hollender, L., Jensen, R., John, M. T., De Laat, A., de Leeuw, R., Maixner, W., van der Meulen, M., Murray, G. M., Nixdorf, D. R., Palla, S., Petersson, A., Pionchon, P., Smith, B., Visscher, C. M., Zakrzewska, J. and Dworkin, S. F. (2014) Diagnostic Criteria for Temporomandibular Disorders (DC/TMD) for Clinical and Research Applications: recommendations of the International RDC/TMD Consortium Network* and Orofacial Pain Special Interest Groupdagger. J Oral Facial Pain Headache, 28(1), pp. 6-27.
Schmidt-Kaunisaho, K., Hiltunen, K. and Ainamo, A. (1994) Prevalence of symptoms of craniomandibular disorders in a population of elderly inhabitants in Helsinki, Finland. Acta Odontol Scand, 52(3), pp. 135-9.
Schmitter, M., Kress, B., Ohlmann, B., Henningsen, P. and Rammelsberg, P. (2005) Psychosocial behaviour and health care utilization in patients suffering from temporomandibular disorders diagnosed on the basis of clinical findings and MRI examination. Eur J Pain, 9(3), pp. 243-50.
Schokker, R. P., Hansson, T. L. and Ansink, B. J. (1990) Craniomandibular disorders in patients with different types of headache. J Craniomandib Disord, 4(1), pp. 47-51.
REFERENCES
80
Sessle, B. J., Hu, J. W., Amano, N. and Zhong, G. (1986) Convergence of cutaneous, tooth pulp, visceral, neck and muscle afferents onto nociceptive and non-nociceptive neurones in trigeminal subnucleus caudalis (medullary dorsal horn) and its implications for referred pain. Pain, 27(2), pp. 219-35.
SFS 1992:1433. Sametingslagen. Svensk författningssamling. SFS, 1992:1433.
SFS 2003:460 Lag om etikprövning av forskning som avser människor. Svensk författningssamling. SFS, 2003:460.
Sjölander, P., Daerga, L., Edin-Liljegren, A. and Jacobsson, L. (2008a) Musculoskeletal symptoms and perceived work strain among reindeer herders in Sweden. Occup Med (Lond), 58(8), pp. 572-9.
Sjölander, P., Hassler, S. and Janlert, U. (2008b) Stroke and acute myocardial infarction in the Swedish Sami population: incidence and mortality in relation to income and level of education. Scand J Public Health, 36(1), pp. 84-91.
Sjölander, P. (2011) What is known about the health and living conditions of the indigenous people of northern Scandinavia, the Sami? Glob Health Action, 4.
Smith, L. T. (2012) Decolonizing methodologies: research and indigenous peoples, 2nd ed., London; New York: Zed Books.
Smith, S.B., Mir, E., Bair, E., Slade, G.D., Dubner, R., Fillingim, R.B., Greenspan, J.D., Ohrbach, R., Knott, C., Weir, B., Maixner, W., Diatchenko, L. (2013) Genetic variants associated with development of TMD and its intermediate phenotypes: the genetic architecture of TMD in the OPPERA prospective cohort study. J Pain: 14, T91-101.e101-103.
Solbakk, J. T. (2006) The Sámi people : a handbook, Ny omarb. uppl. ed., Karasjok: Davvi Girji.
Sousa, S. T., Mello, V. V., Magalhaes, B. G., Morais, M. P., Vasconcelos, M.
M., Junior, A. D. and Gomes, S. G. (2014) The role of occlusal factors on the
occurrence of temporomandibular disorders. Cranio. 2014 Jul
16:2151090314Y0000000015. [Epub ahead of print]
Stegenga, B., de Bont, L. G., Boering, G. and van Willigen, J. D. (1991) Tissue responses to degenerative changes in the temporomandibular joint: a review. J Oral Maxillofac Surg, 49(10), pp. 1079-88.

REFERENCES
81
Suvinen, T. I., Reade, P. C., Kemppainen, P., Könönen, M. and Dworkin, S. F. (2005) Review of aetiological concepts of temporomandibular pain disorders: towards a biopsychosocial model for integration of physical disorder factors with psychological and psychosocial illness impact factors. Eur J Pain, 9(6), pp. 613-33.
Svensson, P. and Arendt-Nielson, L. (2000) Clinical and experimental aspects of temporomandibular disorders. Curr Rev Pain, 4(2), pp. 158-65.
Svensson, P., Burgaard, A. and Schlosser, S. (2001) Fatigue and pain in human jaw muscles during a sustained, low-intensity clenching task. Arch Oral Biol, 46(8), pp. 773-7.
Svensson, P., Jadidi, F., Arima, T., Baad-Hansen, L. and Sessle, B. J. (2008) Relationships between craniofacial pain and bruxism. J Oral Rehabil, 35(7), pp. 524-47.
Türp, J. C. and Schindler, H. (2012) The dental occlusion as a suspected cause for TMDs: epidemiological and etiological considerations. J Oral Rehabil, 39(7), pp. 502-12.
Tzakis, M. G., Österberg, T. and Carlsson, G. E. (1994) A study of some masticatory functions in 90-year old subjects. Gerodontology, 11(1), pp. 25-9.
Unruh, A. M. (1996) Gender variations in clinical pain experience. Pain, 65(2-3), pp. 123-67.
Unruh, A. M. (2008) Pain in women. Pain Res Manag, 13(3), pp. 199-200.
van der Meulen, M. J., Lobbezoo, F., Aartman, I. H. and Naeije, M. (2006) Self-reported oral parafunctions and pain intensity in temporomandibular disorder patients. J Orofac Pain, 20(1), pp. 31-5.
van der Weele, L. T. and Dibbets, J. M. (1987) Helkimo's index: a scale or just a set of symptoms? J Oral Rehabil, 14(3), pp. 229-37.
Visscher, C. M., Lobbezoo, F., de Boer, W., van der Meulen, M. and Naeije, M. (2001a) Psychological distress in chronic craniomandibular and cervical spinal pain patients. Eur J Oral Sci, 109(3), pp. 165-71.
Visscher, C. M., Lobbezoo, F., de Boer, W., van der Zaag, J. and Naeije, M. (2001b) Prevalence of cervical spinal pain in craniomandibular pain patients. Eur J Oral Sci, 109(2), pp. 76-80.

REFERENCES
82
Von Korff, M., Dworkin, S. F., Le Resche, L. and Kruger, A. (1988) An epidemiologic comparison of pain complaints. Pain, 32(2), pp. 173-83.
Von Korff, M., Ormel, J., Keefe, F. J. and Dworkin, S. F. (1992) Grading the severity of chronic pain. Pain, 50(2), pp. 133-49.
Wahlund, K., List, T. and Dworkin, S. F. (1998) Temporomandibular disorders in children and adolescents: reliability of a questionnaire, clinical examination, and diagnosis. J Orofac Pain, 12(1), pp. 42-51.
Warren, M. P. and Fried, J. L. (2001) Temporomandibular disorders and hormones in women. Cells Tissues Organs, 169(3), pp. 187-92.
Webb, R., Brammah, T., Lunt, M., Urwin, M., Allison, T. and Symmons, D. (2003) Prevalence and predictors of intense, chronic, and disabling neck and back pain in the UK general population. Spine, 28(11), pp. 1195-202.
Wiesinger, B., Malker, H., Englund, E. and Wänman, A. (2007) Back pain in relation to musculoskeletal disorders in the jaw-face: a matched case-control study. Pain, 131(3), pp. 311-9.
Wiesinger, B., Malker, H., Englund, E. and Wänman, A. (2009) Does a dose-response relation exist between spinal pain and temporomandibular disorders? BMC Musculoskelet Disord, 10, pp. 28.
Williams, d. C. A. C., Davies, H. T. and Chadury, Y. (2000) Simple pain rating scales hide complex idiosyncratic meanings. Pain, 85(3), pp. 457-63.
Williamson, A. and Hoggart, B. (2005) Pain: a review of three commonly used pain rating scales. J Clin Nurs, 14(7), pp. 798-804.
Wolf, E., Birgerstam, P., Nilner, M. and Petersson, K. (2006) Patients' experiences of consultations for nonspecific chronic orofacial pain: A phenomenological study. J Orofac Pain, 20(3), pp. 226-33.
Wänman, A. (1987) Craniomandibular disorders in adolescents. A longitudinal study in an urban Swedish population. Swed Dent J Suppl, 44, pp. 1-61.
Wänman, A. and Agerberg, G. (1987) Recurrent headaches and craniomandibular disorders in adolescents: a longitudinal study. J Craniomandib Disord, 1(4), pp. 229-36.

REFERENCES
83
Wänman, A. and Agerberg, G. (1991) Etiology of craniomandibular disorders: evaluation of some occlusal and psychosocial factors in 19-year-olds. J Craniomandib Disord, 5(1), pp. 35-44.
Wänman, A. (1995) The relationship between muscle tenderness and craniomandibular disorders: a study of 35-year-olds from the general population. J Orofac Pain, 9(3), pp. 235-43.
Wänman, A. (1996) Longitudinal course of symptoms of craniomandibular disorders in men and women. A 10-year follow-up study of an epidemiologic sample. Acta Odontol Scand, 54(6), pp. 337-42.
Yekkalam, N. and Wänman, A. (2014a) Prevalence of signs and symptoms indicative of temporomandibular disorders and headaches in 35-, 50-, 65- and 75-year-olds living in Vasterbotten, Sweden. Acta Odontol Scand, 72(6), pp. 458-65.
Yekkalam N, Wänman A. (2014b) Associations between craniomandibular
disorders, sociodemographic factors and self-perceived general and oral
health in an adult population. Acta Odontol Scand, 72. [in press].
Zafar, H., Nordh, E. and Eriksson, P. O. (2000) Temporal coordination between mandibular and head-neck movements during jaw opening-closing tasks in man. Arch Oral Biol, 45(8), pp. 675-82.
Zhang, W. and Creswell, J. (2013) The use of "mixing" procedure of mixed methods in health services research. Med Care, 51(8), pp. e51-7.
Åhren, C. (2008) Är jag en riktig same? En etnologisk studie av unga samers identitetsarbete, Umeå: Institutionen för kultur-och medievetenskaper/Etnologi, Umeå universitet.
Österberg, T. and Landt, H. (1976) [Index for occlusal state for epidemiological studies and clinical use]. Tandläkartidningen, 68(21), pp. 1216-23.
Österberg, T., Carlsson, G. E., Wedel, A. and Johansson, U. (1992) A cross-sectional and longitudinal study of craniomandibular dysfunction in an elderly population. J Craniomandib Disord, 6(4), pp. 237-45.
Österberg, T. and Carlsson, G. E. (2007) Relationship between symptoms of temporomandibular disorders and dental status, general health and psychosomatic factors in two cohorts of 70-year-old subjects. Gerodontology, 24(3), pp. 129-35.



















