
Telemedicine in Europearmtelemed.org/resources/35-eu-ehealth-ceec2004.pdf · Telemedicine work in...
183
PETR NOVOTNY European Commission, DG Information Society, eHealth Unit E-HEALTH IN CENTRAL AND EAST EUROPEAN COUNTRIES with focus on Czech Republic, Hungary, Poland and Slovenia Brussels 29.2.2004
Transcript of Telemedicine in Europearmtelemed.org/resources/35-eu-ehealth-ceec2004.pdf · Telemedicine work in...
PETR NOVOTNY European Commission, DG Information Society, eHealth Unit
E-HEALTH IN CENTRAL AND EAST EUROPEAN COUNTRIES with focus on Czech Republic, Hungary, Poland and Slovenia
Brussels 29.2.2004
2
PREFACE AND THANKS...............................................................................................................................................................................................4 EXECUTIVE SUMMARY ...............................................................................................................................................................................................5 1. TELEMEDICINE IN EUROPE ...................................................................................................................................................................................12
1.1 Situation in EU 15........................................................................................................................................................................................12 1.1.1 Longer-term trends........................................................................................................................................................................12 1.1.2 The European healthcare ICT market...........................................................................................................................................12
1.2 Situation in Central and Eastern Europe ....................................................................................................................................................13 1.2.1 Introduction to Central and Eastern Europe (CEE)......................................................................................................................13 1.2.2 Demographic Data ........................................................................................................................................................................13 1.2.3 Health Indicators ...........................................................................................................................................................................14 1.2.4 Telemedicine Implementation ......................................................................................................................................................14 1.2.5 Economic and Information Technologies (IT) indicators ............................................................................................................15 1.2.5.1 GDP – Gross Domestic Product ................................................................................................................................................15 1.2.5.2 IT penetration.............................................................................................................................................................................15 1.2.6 IT Spending...................................................................................................................................................................................17 1.2.6.1 Investment in IT (excluding telecommunications) compared to GDP......................................................................................17 1.2.6.2 ICT market shares in 2002 (Relative IT market size) ...............................................................................................................18
1.3 Online Search for health information Europe .............................................................................................................................................18 2. COUNTRY PROFILES..............................................................................................................................................................................................19
2.1 Czech Republic.............................................................................................................................................................................................19 2.1.1 Government Action Plans (AP) ....................................................................................................................................................19 2.1.2. List of National Information Society Related Websites..............................................................................................................19 2.1.3 Ministry of Health.........................................................................................................................................................................20 2.1.4 The use of the Internet in Czech Health Institutions in 2002.......................................................................................................20 2.1.5 Survey of the Information Systems (IS) in the Czech Hospitals 2003.........................................................................................20 2.1.6 Telemedicina.CZ - Telemedicine Projects in Czech Republic.....................................................................................................21 2.1.7 ROSCH Foundation ......................................................................................................................................................................22 2.1.8 IZIP – Internet Medical Database.................................................................................................................................................22 2.1.9 MEDTEL & NetC@rd..................................................................................................................................................................23 2.1.11 Czech Society of Nuclear Medicine ...........................................................................................................................................23 2.1.12 PET center in Nemocnice Na Homolce hospital ........................................................................................................................24 2.1.13 IKEM CZ – Institute for clinical and experimental medicine....................................................................................................24 2.1.14 Euromise .....................................................................................................................................................................................24 2.1.15 Branch Contact Organization - Healthcare (BCO).....................................................................................................................25 2.1.16 Coordination Center for Departmental Medical Information Systems ......................................................................................26 2.1.17 National Health Registers ...........................................................................................................................................................26 2.1.18 Central registry of R&D projects................................................................................................................................................27
2.2 Hungary........................................................................................................................................................................................................28 2.2.1 Ministry of Health.........................................................................................................................................................................28 2.2.2 Ministry of Informatics and Communication ...............................................................................................................................28 2.2.3 List of National Information Society Related Websites...............................................................................................................28 2.2.5 National Institute and Library for Health Information .................................................................................................................29 2.2.6 GYOGYINFOK – Center for Healthcare Information.................................................................................................................29 2.2.7 Hungarian Office for Research and development ........................................................................................................................29 2.2.8 Institute of Experimental Medicine ..............................................................................................................................................29 2.2.9 OTKA – National Research Institute............................................................................................................................................30 2.2.10 Computer and Automation Research Institute, Hungarian Academy of Sciences ....................................................................30 2.2.11 PROREC.HU & WIDENET.......................................................................................................................................................30 2.2.12 PRIMACOM...............................................................................................................................................................................30 2.2.13 RETRANSPLAT ........................................................................................................................................................................30 2.2.14 MiM – Medical Info Media ........................................................................................................................................................31 2.2.15 VARIMED ..................................................................................................................................................................................31 2.2.16 List of Contacts ...........................................................................................................................................................................31
2.3 Poland ..........................................................................................................................................................................................................32 2.3.1 Ministry of Health.........................................................................................................................................................................32 2.3.2 List of National Information Society Related Websites...............................................................................................................32 2.3.3 ePolska (ePoland)..........................................................................................................................................................................32 2.3.4 National Health Care Programme.................................................................................................................................................33 2.3.5 Registry of Medical Services ........................................................................................................................................................33 2.3.6 National Pharmaceutical Portal ....................................................................................................................................................34 2.3.7 Informatization of hospitals in the Malopolskie province, 2002 .................................................................................................34 2.3.8 Telemedicine at University Hospital in Krakow ..........................................................................................................................34 2.3.9 Telemedicine in Poland.................................................................................................................................................................34 2.3.10 Research and Development Units...............................................................................................................................................35 2.3.11 The Role and Advantages of Using the Tele-ECG System in Daily Medical Practice - Telemedicine Project .......................35 2.3.12 Tele-ekg - CARDIAC MONITORING SYSTEM .....................................................................................................................36 2.3.13 Telewelfare.com..........................................................................................................................................................................36 2.3.14 PIONIER.....................................................................................................................................................................................37 2.3.15 Krakow Center of Telemedicine.................................................................................................................................................38 2.3.16 PRO-ACCESS ............................................................................................................................................................................40 2.3.17 The University Hospital in Krakow............................................................................................................................................42
3
2.3.18 Telemed.......................................................................................................................................................................................43 2.3.19 E-rejestracja ................................................................................................................................................................................43 2.3.20 List of Contacts ...........................................................................................................................................................................44
2.4 Slovenia ........................................................................................................................................................................................................45 2.4.1 Government’s Action Plans ..........................................................................................................................................................45 2.4.2 Ministry of Information ................................................................................................................................................................45 2.4.3 Ministry of Health.........................................................................................................................................................................46 2.4.5 List of Other National Information Society Related Websites.....................................................................................................46 2.4.6 Institute of Public Health ..............................................................................................................................................................46 2.4.7 Institute of Biomedical Informatics ..............................................................................................................................................46 2.4.8 Slovene Medical Informatics Association....................................................................................................................................47 2.4.9 SIZN - Nursing Informatics Interest Group .................................................................................................................................47 2.4.10 Telemedicine in Slovenia report .................................................................................................................................................47 2.4.11 Telemedicine Projects .................................................................................................................................................................48 2.4.11.1 Transtelephonic transmission of ECG.....................................................................................................................................48 2.4.12 InfoNet – Healthcare Information Systems Company ...............................................................................................................50 2.4.13 Nova Vizia (New Vision) ...........................................................................................................................................................53 2.4.14 List of Contacts ...........................................................................................................................................................................53
Annex I................................................................................................................................................................................................................54 Telemedicine Implementation in CEE region – Brief Overview..........................................................................................................54 Plans and organisations for Telemedicine implementation in CEE......................................................................................................57
SIBIS report (abstract) .................................................................................................................................................................................59 Annex III .............................................................................................................................................................................................................62
The use of the Internet in the Czech health institutions in 2002 .................................................................................................................62 Annex IV .............................................................................................................................................................................................................65
Survey of the Information Systems (IS) in the Czech hospitals 2003.........................................................................................................65 Annex V...............................................................................................................................................................................................................73
Telemedicina.CZ - Telemedicine Projects in Czech Republic..............................................................................................................73 Annex VI .............................................................................................................................................................................................................77
IZIP – Internet Medical Database, Czech Republic ....................................................................................................................................77 Annex VII............................................................................................................................................................................................................80
MEDTEL & NetC@rd, Czech Republic .....................................................................................................................................................80 Annex VIII...........................................................................................................................................................................................................82
National Health Registers, Czech Republic.................................................................................................................................................82 Annex IX .............................................................................................................................................................................................................87
E-HEALTH CARE IN HUNGARY, REPORT NO. 1..........................................................................................................................................................87 Annex X...............................................................................................................................................................................................................89
EHEALTH CARE IN HUNGARY, REPORT NO. 2 ...........................................................................................................................................................89 Annex XI ...........................................................................................................................................................................................................131
Department Of Informatics, National Institute And Library For Health Information, Hungary ..............................................................131 Annex XII..........................................................................................................................................................................................................134
Regional and International Integrated Telemedicine Network for Organ Transplant, Hungary ..............................................................134 Annex XIII.........................................................................................................................................................................................................135
Health care on-line – abstract from ePolska Action Plan, Poland.............................................................................................................135 Annex XIV.........................................................................................................................................................................................................138
Informatization of hospitals in the Malopolskie province, Poland ...........................................................................................................138 Annex XV ..........................................................................................................................................................................................................148
Telemedicine at University of Krakow hospital, Poland...........................................................................................................................148 Annex XVI.........................................................................................................................................................................................................150
Telemedicine in Poland..............................................................................................................................................................................150 Annex XVII .......................................................................................................................................................................................................156
Research and Development Units, Poland.................................................................................................................................................156 Annex XVIII ......................................................................................................................................................................................................159
Tele-ekg - CARDIAC MONITORING SYSTEM, Poland.......................................................................................................................159 Annex XIX.........................................................................................................................................................................................................163
Telemedicine in Slovenia – MESS report..................................................................................................................................................163 Annex XX ..........................................................................................................................................................................................................167
Telemedicine in Slovenia...........................................................................................................................................................................167 Annex XXI.........................................................................................................................................................................................................180
Health Insurance Card Project – Health Insurance Institute, Slovenia .....................................................................................................180 Annex XXII .......................................................................................................................................................................................................182
InfoNet – healthcare information systems company, Slovenia .................................................................................................................182
4
Preface and Thanks This report was done during my stage with eHealth Unit of Directorate General (DG) Information Society at European Commission from October 2003 to February 2004. It was done in order to compliment my previous experience in the telecommunication sector and to broaden my views in one of the leading industries of the near future that will be very dependent on information and communication technologies. The aim of this report is to give an overview about countries’ basic indicators, governments’ action plans for eHealth, and provides a collection of different telemedicine projects and studies that have been conducted in Central and Eastern Europe. The focus is on the following 4 countries: Czech Republic, Hungary, Poland and Slovenia. Telemedicine work in these four countries is presented in separate chapters. The overview is divided into short introduction on EU 15 eHealth market situation, general information about Central and Eastern Europe (CEE) and more detailed description of above mentioned four countries. The latter consists of presentation of official policy of each country, and eHealth and telemedicine projects/ pilots in the various medical fields where telemedicine is already of increasing importance. The projects and studies presented here do by no means cover the whole area of what is currently going on in the field of telemedicine. They represent a selection made by the author based mainly on the availability of the information on the Internet and response to the queries done by the author. Many more articles would also have been suitable for presentation, but due to the limited amount of space and time for collection as well as due to the lack of information in English on Internet, this was not possible. The sources from which the articles were obtained were the Internet and the contributions from public and private institutions.
I would like to thank the following people for helping me during creation of this report: Within the European Commission, eHealth unit: - Ilias Iakovidis (advisor) - Jean-Claude Healy - Silas Olsson - Andreas Lymberis - Octavian Purcarea - Sigurd von Ingersleben - Benedicte Vasseur-Tries - Jacqueline Teller Within the accessing countries - Jiri Valek the Czech Republic - Jana Zvarova the Czech Republic - Sandor G. Vari Hungary - Tamas Gergely Hungary - Pal Simon Hungary - Mariusz Duplaga Poland - Witold Poniklo Poland - Bostjan Bercic Slovenia - Livia Tusar Slovenia Petr Novotny
5
Executive Summary Objective: The main focus of the report is to describe current situation on eHealth and telemedicine (these two (2) terms will be used interchangeably) in Central and Eastern European Countries, namely Cyprus, the Czech Rep., Hungary, Poland, Romania, Slovakia and Slovenia. Methods: Information was collected primarily from available internet websites as well as by contacting relevant experts by e-mail and phone. Information was translated, analysed and classified in several categories and tables. The main report (53 pages) includes European Information Technologies market overview, Central and East European (CEE) countries basic indicators and separate chapters on eHealth situation and more detailed collection of pilots in 4 countries: Czech Republic, Hungary, Poland and Slovenia. The supporting materials such as complete surveys reports, detailed articles mentioned in the report, contributions from the other authors and other material are contained in the Annexes (130 pages). Findings: There are many pilots, especially in Central European Countries, that are mostly local in nature and often without any government or Health Authority commitment. All of the countries studied have eHealth action plans that often stems in different ministries than Ministry of Health. In some cases, such as the Czech Republic, Poland, and Slovenia, the competency and sometimes co-funding lies within Ministry of Health. Majority of the development and set up of pilots have been financed from private sources, but without follow up. The pilots are predominantly telemedicine services such as teleconsultation. Slovenia has made significant progress in deployment of electronic health record and health cards and has the only “viable” eHealth service that the author found in his research. Several countries are following that example of insurance based health data system. Also, the region of Krakow (Malopolskie) has made significant progress in planning and deploying eHealth systems and services. The findings of author lead to one major conclusion: creation of favourable environment for all the players (ministries, users, industries and social insurance players) to have common understanding and objectives through open dialog and optimising of resources. The national and regional plans should draw from the experiences and best practices that were developed elsewhere and that were supported by the EU research and development programmes in eHealth. More extended summary of the report follows: Telemedicine Today’s worldwide aging of the population is a direct consequence of the ongoing global fertility transition (decline) and of mortality decline at older ages, population aging is expected to be among the most prominent global demographic trends of the 21st century. Population aging is progressing rapidly in many industrialized countries, but those developing countries whose fertility declines began relatively early also are experiencing rapid increases in their proportion of elderly people. This pattern is expected to continue over the next few decades, eventually affecting the entire world. Population aging has many important socio-economic and health consequences, including the increase in the old-age dependency ratio. It presents challenges for public health (concerns over possible bankruptcy of Medicare and related programs) as well as for economic development (shrinking and aging of labour force, possible bankruptcy of social security systems). [1] The challenge for the health sector is to improve the standard of living through increased technology utilization reducing the costs of healthcare. It is clear that such technologies are changing the face of healthcare. For example, the Internet already offers society the opportunity to become better informed on health issues. This could eventually result in major changes in the relationship between doctor and patient. The UK Foresight Programme provides one vision of this future: By 2020 […] the first point of contact with health care will be through a ‘virtual’ cyber-physician (CP). Accessed through a TV screen, the CP system will replace other forms of triage such as the telephone and give access to information about professionals, hospitals and other aspects of health care. (OST, 2001, p. 18)
6
Changing patterns of information sharing and patient/doctor relationships will bring some fundamental changes to health organizations and the working relationships of health personnel. For instance, ICT systems are set to revolutionize information sharing between health professionals, e.g. through the development of seamless electronic patient records. It is widely anticipated that clinicians will have access to information and decision support at the point of care. This could occur by using a computer screen in offices and surgeries, or through a personal digital assistant (PDA) or mobile phone on wards and in other circumstances, including emergencies. Of course, changes in information-sharing patterns will bring different security concerns onto the health agenda. The security of health information is likely to be provided by a range of procedures and technologies, such as smart cards or biological identifiers. Telematics is the use of ICT to solve any type of problem remotely. Telemedicine is the application of telematics to facilitate healthcare delivery, and is defined by the EU Telemedicine Project as ‘the investigation, monitoring and management of patients, using systems which allow ready access to expert advice and to patient information, no matter where the patient or relevant information is located’. The major benefits of telemedicine applications are the improvements in the speed and cost of health services as well as an expected increase in the quality of patient care. Despite the high initial costs of investing in hardware and software, this should ensure considerable savings in the long term. [2] Central and East European Countries This report is primarily dealing with Central and East European countries and the telemedicine situation including Government’s Action Plans for eHealth, telemedicine pilots and projects that are planned for the near future or that has already taken place on national or regional level. It also contains surveys concerning IT state and plans in the hospitals of the respective countries. The countries covered in the report are Cyprus, Czech Republic, Hungary, Poland, Romania, Slovakia and Slovenia with special focus on Czech Republic, Hungary, Poland and Slovenia. The total population of these countries is 89.5 M people with Poland being the most (38.5 M) and Cyprus the least (745 K) populated. The projected population in 2030 is 86.5 M people. The number of the people with the age structure 65 years and older is on average 13% of the population at the moment. This number is expected to increase. Life expectancy is 74 years on average with Cyprus (77.27 years) having the longest and Romania (70.62 years) having the shortest life expectancy. The average health expenditure in region is around 6% of GDP with Slovenia having the highest (8.2 %) and Romania the lowest (3.9%) expenditure. The Czech Republic claims to have 0.4% investments into health informatics as part of the total health expenditures (7.24% of GDP). The total GDP of the selected countries is almost 937 billion USD. This figure can be compared to the GDP produced by Spain in 2002 (850.7 billion USD). The leading GDP in the region has Poland (368.1 billion USD). The purchasing power per capita is on average 13800 USD but there are big differences in the region. The highest figure is showed by Slovenia (18000 USD) and the lowest by Romania (7400 USD). Regarding IT penetration although, on average, 77% of households in the candidate countries now have a fixed telephone service as compared to 86% in the EU-15, the penetration rates for fixed telephone services in some countries hide large differences in penetration between urban and rural areas. From the observation that mobile penetration is starting to overtake fixed penetration in some Candidate Countries (CCs) and considering that technological innovations in mobile transmission (2.5 G and onwards) allow mobile networks to become Internet delivery platforms, it follows that these mobile networks have the potential to become the main Internet and voice delivery platform in the CCs, at least in those areas with poor fixed terrestrial infrastructure. (IPTS, No.77 – JRC – Seville, September 2003) At the end of 2001, 11% of the population in the Central and Eastern Europe (CEE) accessed the Internet an average of once a month, compared with 39% for West Europe as a whole (EITO, 2002). The low PC and Internet
7
penetration in general, particularly at home, limited by the access charges and high cost of PCs, the low level of fixed-line penetration, and low penetration of alternative access technologies, may represent a potential bottleneck for short to medium term Internet development in the region. (IPTS, No.77 – JRC – Seville, September 2003) As far as IT spending number of the countries still invest about 2% of GDP annually into IT, which suggests that it still will take couple of years for the region to reach IT penetration and spending levels of current EU15 states. The highest IT spending is reported in the Czech Republic (4%) and the lowest in Romania (1.5%). Per capita spending is reported highest in Slovenia (257 EUR) and lowest in Romania (30 EUR). Across the CEE region there are key differences in terms of current ICT market development, demand for specific technologies and the growth potential of individual country markets. The largest ICT spending has been reported in Poland (15.049 M EUR) and the Polish market represents 37.6 % of all region. The average ICT spending for the region is 4 M EUR. A survey carried out in 2002 shows that nearly 30% of Internet users in CEE reported online search for health-related information during 12 months period. Compare to EU15 (36,4%) it’s quite a satisfactory number but still low compare to U.S. (58.3%). Unfortunately the survey doesn’t contain success rate of searching for CEE countries. The success ration in the other countries was about 80 %. Czech Republic In the Czech Republic Ministry of Informatics (www.uvis.cz) is in charge of development of national action plan for information society. The projects dealing with health (Zdravotnictvi online) are in the competency of Ministry of Health (www.mzcr.cz) and are set for 2001 – 2005 with the total budget around 9700 EUR. The use of the Internet in the health institutions survey that was conducted in 2002 by the Institute of health information and statistics showed the following results: • 51.5% of the institutions responded to the survey • 86.3% of the institutions that have responded and have access to the Internet use it for gaining of the
information – mostly legislative and then pharmaceutical information respectively. • 74% use it for communication with insurance companies and then other administration respectively. • 99% have access only from health institution, 38% only from home, 23% from the institution and home The survey hasn’t given any result about how many institutions are connected to the Internet, it only shows the purpose of using of the Internet. Another survey conducted by Ministry of Health shows the state of hospital information systems (HIS) in the Czech hospitals in 2003. The return rate of the sent questionnaires was 24% and it revealed the following results: • 70% of the institutions that have responded have complete or at least half-way to complete HIS. • Only 3% of the institutions with complete HIS consider change of the system. • 17% of the institutions with incomplete HIS are satisfied, 40% look for change. • 61% of the institutions with incomplete HIS consider lack of finances as main barrier for completion. • Czech doctors show preference for future implementation of PACS-type solutions but very low interest in
management support systems and public solutions. • The IT personnel in Czech hospitals are without any influence on management decisions. There are few telemedicine projects already working in Czech hospitals. A good start for the overview is a portal www.telemedicina.cz with list of project and pilots already running or planned in Czech hospitals. Some of the projects done are Interventional teleradilogy, Acute neurotraumatology, Telepathology, etc. The platform was until recently supported by Czech Telecom. Another two big projects that are done in cooperation with VZP – the biggest health insurance company in the Czech Republic are IZIP – medical record online and NetC@rd - EHR. Most of the telemedicina.cz projects where possible due to the sponsorships and donations of private organizations such as Czech Telecom that unfortunately stopped recently its support and at present most of the planned projects are on hold. In the case of VZP the project results are available only to the patience covered by this insurance company.
8
In the future is will be necessary that these projects are done with support of entity such as Ministry of Health is we want to avoid failures of the projects due to the withdrawal of private sponsors that currently they are dependant on. Or that they are only available to the patience covered by sponsoring insurance company. There are also many institutes dealing with telemedicine. They are for example: - Czech Society of Nuclear Medicine - IKEM CZ – Institute for Clinical and Experimental Medicine - Euromise – Education and Research in Medical Informatics - Branch Contact Organization in Healthcare - or Coordination Center for Departmental Medical Information Systems Hungary In Hungary Ministry of Informatics and Communication (www.ihm.hu) is in charge of eHungary, an action plan for information society for the years 2004 – 2006. eHealth is one of the sectoral responsibilities for the AP. A survey made in 2001 by GKI Economic Research Inc. (http://www.gki.hu) has revealed that while all of the Hungarian outpatient centres possess and operate computer systems, only three-quarter of them is able to systematically lead the medical history of the patients by a suitable software system. A survey conducted in 2001 by GKI Economic Research Inc., Westel Mobile Communication Inc. and Sun Microsystems Hungary Ltd. on hospitals, outpatient stations, general practitioners and other health care institutions has revealed the following facts: • 9/10 of hospitals and 1/3 of outpatient stations had an Internet access. • Electronic communication between different institutions is rather an exception • Internet is used mainly for searching for professional information, developing contact with Hungarian or foreign
clinics and scientific centers and libraries. • ¼ of GPs are able to access the Internet from work • 4% of GPs have their own website to spread medical information and consultancy According to the survey the development of Internet access and webpage creation among general practitioners has a very positive tendency. It was expected to double in 2003. Local outpatient centres with Internet access are searching for the following information: • social security rules • laws, decrees and other regulations • professional articles • description of drugs Moreover, local outpatient centres with Internet access regularly make electronic contacts with the Ministry for Health, the Social Security Fund, other hospitals and laboratories. There are no local outpatient centres, which operate a service empowering patients to check in via Internet for a medical examination. Another survey shows that 64% of the IT assets owned by the healthcare institutions (incl. software/hardware) are more than 3 years old. This ratio is 66% for PCs and terminals, 67% for software, and 52% for mainframes, network and accessories. There is a wide selection of Government sponsored tenders in order to disseminate digitally based devices, methods and activities in the field of e-Health care. For example there are regularly repeated Government tenders with the aim of providing direct support for doctors, nurses, social care workers and others in the form of granting for them PCs, Internet access or ISDN connection cheaply or for free. In some case the co-financing of the tenders by private companies is available.
9
A way for overview about telemedicine projects in Hungary is a health care portal Varimed (www.varimed.hu). It lists the projects especially from international cooperation such as PROREC.HU & Widenet, Primacom or Retransplant. E-health care is also promoted by various professional organizations such as: - Hungarian Foundation for Medical Informatics - Hungarian Society for Medical Informatics - GYOGYINFOK – Center for Healthcare information of MoH - National Institute and library for Health Information - Institute of Experimental Medicine Poland In Poland Ministry of Scientific Research and Informatization technology (www.kbn.gov.pl) is in charge of development of national action plan for information society. The document ePoland for 2001 - 2006 follows the approach of eEurope+ and contains specific tasks for Health care on-line projects such as Creation of a uniform electronic data base on medical establishments and facilities available via the Internet, Creation of database on patients covered by health insurance, etc. The positive message is that MoH (www.mz.gov.pl) is usually the source of financing for these projects. The survey about Informatization of hospitals in Malopolskie province in 2002 with 98% questionnaire return showed the following results: • All hospitals have IT personnel. 47% are permanent employees, the rest are contractors, external firms or mix of
the two • 18% have complete network, 56% have at least half-way to completion network, 8% have absence of network! • 18% states full or near the integration of the software. The rest are long way from software integration. • 61% is declaring 3 years to be horizon for planned informatization. • 45% of hospitals plan to spend max. 65.000 EUR on IS building. Another 45% plans to spend funds beginning
from 100.000 EUR, which is more realistic. There is a range of telemedicine projects already implemented in Poland as they can be seen for example in Telewelfare.com (telezdrowie.pl), portal offering interactive service for diagnosis and rehabilitation of senses responsible for communication. Krakow Center for Telemedicine is also a center for telemedicine projects mainly focused on teleconsultation, telemonitoring and tele-education. Other examples can be also tele-ecg project that has been running in Poland from mid. 90s or project called Improvement of Care Delivery for Severe Asthma Patients co-financed by MoH and Ministry of Scientific Research and Informatiozation Technology www.astma.web.pl. Slovenia In Slovenia Ministry of Information (http://www2.gov.si/mid/mideng.nsf) is in charge of development of national plan for information society. Health is 1 of 12 e-services for citizens and 1 of 15 areas of Action Plan up to 2004. Responsibility for health area projects is in domain of Ministry of Health (http://www2.gov.si/mz/mz-splet.nsf). Ministry of Information runs Slovenian eGovernment portal since 2001. It provides range of e-services & government information for citizens, businesses and civil servants. Ministry of Health is responsible for National Health Sector Management Project and others like e-Waiting lists and E- SPP projects which the Health Sector Management Project initiated. Report of Ministry of education, science and sport (http://www.mszs.si/eng/) includes some interesting data regarding budgets allocated for research in Slovenia. Slovenia has investments in healthcare 8.6% of GDP = 1.877.3 M EUR. The proposed Slovenian direct investment in healthcare informatics (MoH) for 2004 is 4.3 M EUR. As far as telemedicine Slovenia is very successful with the implementation of EHR when all Slovenian residents have this card for at least one year. HIC includes basic information on the health of the particular person. The project was done in cooperation with ZZZS – Institute of Health Insurance in Slovenia. Other telemedicine projects
10
implemented in Slovenia are - just to name few – for example transtelephonic transmission of ECG used regularly by health institutions, PRIMACOM as international project, RETRANSPLANT or WIDENET. There are also many institutes dealing with telemedicine. They are for example: - Health Informatics Standards Board - Health Informatics Council - Centre for Health Informatics - Institute of Biomedical Informatics - Slovene Medical Informatics Association - or Nursing Informatics Interest Group SIZN Conclusion eHealth Activity • There is need for eHealth, mostly personal endeavours, lot of interest Lack of Health Authority commitment and leadership • Most of the contries have some sort of eHealth action plan but it often stems from other ministries than Ministry
of Health (MoH). Although it is sometimes co-funded by MoH and/or the responsibility rests with MoH. • There is certainly telemedicine activity in the CEE region. Most of the projects are introduced by doctors or
businesses but they are rarely supported by official government sources. The result is that they are rather individualistic not systematic projects.
• Doctors in the countries of focus were not aware of any national eHealth plans. This means that Ministries of Health in the surveyed countries should improve their communication to the medical staff.
National versus Regional Pilots and Implementation • In the large countries regional differences in the level of telemedicine can be expected (Poland) while in the
small countries the activities can be easier implemented nationally (Slovenia). • Without a favourable environment of cooperation between state and private sector the projects will be rather
standalone than national. Funding and sustainability • Majority of the projects has been financed from private sources, which carries the danger of sudden termination
of partner from the projects (Czech Telecom) and causing the projects to be on hold before another strategic partner is found. MoH should play more active role in the promotion granting and implementation of telemedicine projects to avoid this danger in the future.
Challenges • To find a solution by defining common goals and cooperation between state and private sectors. This is
important for the systematic approach to eHealth and it will be important especially in the larger countries. • To help to improve the communication to the doctors and to increase the number of professionals involved and
interested in the matter through these partnerships. Trends for the near future • Governments will be forced to adopt certain eHealth strategies accompanied by concrete actions if they want to
keep up with the future demands on health care and reduce increasing costs in the long run. • State sector will need to cooperate with private sector for implementation of successful nationwide projects. • The growth of the nationwide initiatives will enable use of electronic health record (EHR). • In case there is a 1 health insurance institute in the country than the projects as Electronic Health Card (EHR) is
done to cover the whole population (Slovenia). In case there are more than 1 health insurance providers then it is done to cover primarily the insured persons of the sponsoring insurance company (Czech Republic).
11
• Hospitals are going to be more interconnected for running the telemedicine solutions using ISDN connection in short/medium timeframe and broadband connection, as it becomes available and financially feasible.
• All hospitals are going to have access to the Internet using dial-up or fixed connection. • Medical professionals will continue to use Internet for searching for information concerning their field of
specification. They will use the Internet as a main instrument for correspondence. • As the number of the households connected to the Internet grows, the number of the websites/portals dedicated
to patients with certain decease (for ex. diabetes) will grow as well. It will also increase online communication between doctors and patients - email exchange, on-line booking systems.
Solutions
Addressing common challenges • Health authorities leadership • Creation of favourable environment for all players to have common understanding and objectives • Interoperability of health information systems • Constant enhancing of the information and communication technologies infrastructure • Leveraging investments Accelerating beneficial implementation • Information to citizens and authorities for health education and disease prevention • Integrated health information networks
Facilitating synergies and monitoring • Disseminating best practices • Benchmarking • International cooperation
Source: [1] http://longevity-science.org/Population_Aging.htm;
[2] http://www.emcc.eurofound.eu.int/publications/2003/sf_hss_1.pdf
12
1. Telemedicine in Europe 1.1 Situation in EU 15
1.1.1 Longer-term trends Population ageing is consistent across the globe. At the start of the twenty-first century, the world population included about 600 million people aged 65 and older (10% of the world population), triple the number recorded 50 years earlier (or 8% of the world population in 1950). By mid-century, there will be some 2 billion older persons (21%), once again a tripling of this age group in a span of 50 years. An ageing population has considerable implications and expected impacts on a wide variety of socio-economic factors and processes, such as economic growth, capital markets, pension systems, but also on technical progress and innovations, education and human capital, family and household structures - and last, but not least, on the health and social care system. It implies that the prevalence of chronic diseases will grow and the numbers of disabled persons rise. Evidence of age-related rationing of health interventions has been documented in some countries in the European Region. [1] For example Liz Lloyd discusses the nature of health and social care interventions in the care of older people dying in Britain. [2] The health sector is today already one of the leading sectors of all industrialized societies. It is to be expected that health in a wider, holistic sense - by encompassing wellness, personal development, environmental protection, biotechnology and the like - will further develop into the new leading industry of the 21st century. Source: [1] ICT&e-Business in the Health and Social Services Sector, the European e-Business Market Watch, sector report No.7 II/January 2003 [2] LLOYD, L. (2000). Dying in old age: promoting well-being at the end of life. Mortality, 5, 171 – 188.
1.1.2 The European healthcare ICT market It was estimated that the European Healthcare Information Society Technology (HIST) market amounted to approximately 11 billion Euro in 2001, which would account for less than 2% of the total western European ICT market of about 643 billion Euro p.a. Considering the economic relevance of the health sector for the EU with total expenditure of more than 8% of GDP, this HIST market value is very low and amounts to about 1.6% of the overall EU healthcare market estimated at 700 billion Euro for 2001. In the hospital sector, for example, the level of total annual IT investment is estimated at only 1.2% of all expenditures as compared to 2.5% in the USA and up to 10% (for ICT) and more in other information-intensive sectors such as financial services. Also for the USA, it is estimated that “with a 50% penetration, Healthcare has the lowest penetration of Internet business solutions,” but at the same time it is assessed that this sector may have the greatest upside with regards to cost savings in the future. Considering the relevance of the health sector for economic activity and employment, this state of affairs may be surprising. But when reflecting on the earlier discussions, a variety of factors come to mind which help to explain this situation: the wide variety and complexity of national healthcare systems, the varying and shifting public/private mix of delivery and financing, the size structure of the establishments, the complexity of communications relationships, the wide variety of business partners and the particular type of customers. All of these and additional factors render an analysis of the sector particularly challenging, and the dearth of detailed information and hard facts on ICT and e-business applications in this sector confirms this. Source: ICT&e-Business in the Health and Social Services Sector, the European e-Business Market Watch, sector report No.7 II/January 2003
13
1.2 Situation in Central and Eastern Europe
1.2.1 Introduction to Central and Eastern Europe (CEE) From early nineties, Central and Eastern Europe countries (CEEC) have undertaken considerable efforts to include themselves in the main activities related to research and development in health telematics in Europe. Countries of this region demonstrate diversified environment of economy transformation and healthcare system status. The process of market economy development brings essential risks to the healthcare system performance. What is also important, healthcare is particularly sensitive domain of social expectations. It seems that efforts of developing e-health environment in CEEC may be substantially accelerated by the co-operation with partners in current member states of European Union. [1] The use of e-health solutions may bring increased benefits for candidate countries with transforming economies. The reforms in healthcare systems are usually considerably delayed when compared to mainstream of changes taking place in these countries. The funds spent for healthcare are limited and the expectations of the society in this area are still growing. The implementation of telemedical applications may result in augmented effects in terms of quality of care and access of the patients to advanced diagnostic and therapeutic procedures. Source: [1] Mariusz Duplaga, Technologies to Central and Eastern European Countries, E-He@lth in Common Europe, Pro Access 2003
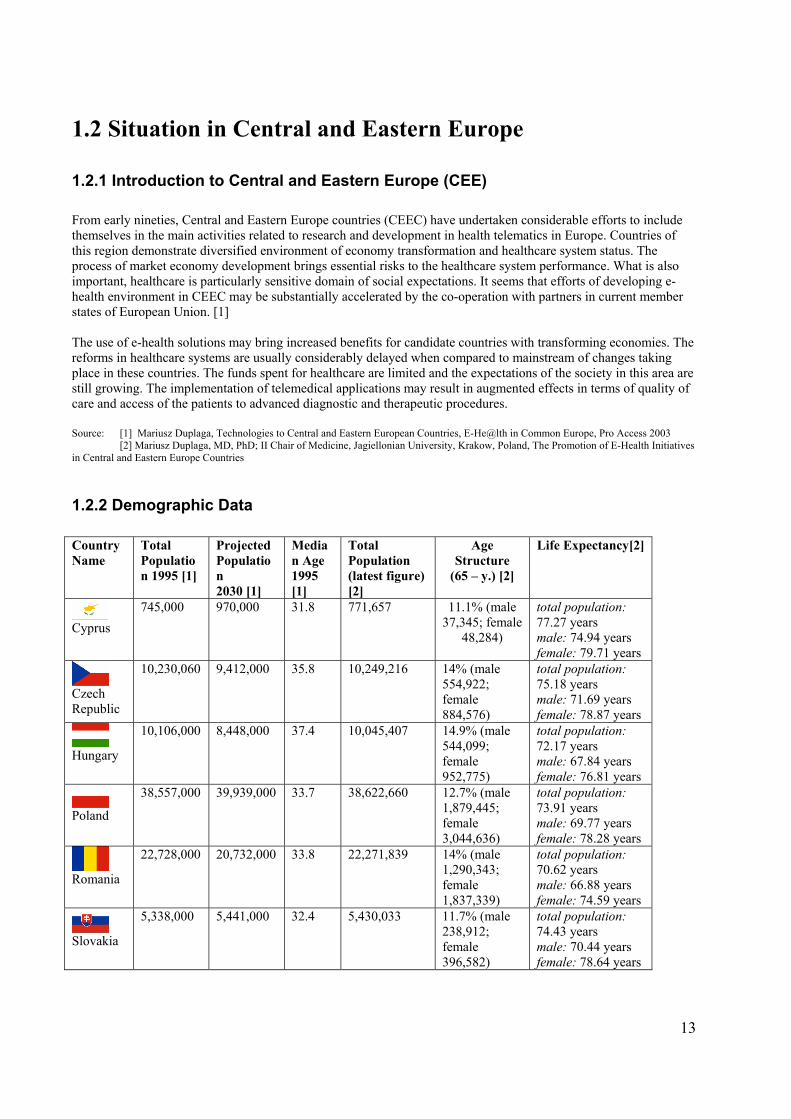
[2] Mariusz Duplaga, MD, PhD; II Chair of Medicine, Jagiellonian University, Krakow, Poland, The Promotion of E-Health Initiatives in Central and Eastern Europe Countries 1.2.2 Demographic Data Country Name
Total Population 1995 [1]
Projected Population 2030 [1]
Median Age 1995 [1]
Total Population (latest figure) [2]
Age Structure
(65 – y.) [2]
Life Expectancy[2]
Cyprus
745,000 970,000 31.8 771,657 11.1% (male 37,345; female
48,284)
total population: 77.27 years male: 74.94 years female: 79.71 years
Czech Republic
10,230,060 9,412,000
35.8 10,249,216 14% (male 554,922; female 884,576)
total population: 75.18 years male: 71.69 years female: 78.87 years
Hungary
10,106,000 8,448,000 37.4 10,045,407 14.9% (male 544,099; female 952,775)
total population: 72.17 years male: 67.84 years female: 76.81 years
Poland
38,557,000 39,939,000 33.7 38,622,660 12.7% (male 1,879,445; female 3,044,636)
total population: 73.91 years male: 69.77 years female: 78.28 years
Romania
22,728,000 20,732,000 33.8 22,271,839 14% (male 1,290,343; female 1,837,339)
total population: 70.62 years male: 66.88 years female: 74.59 years
Slovakia
5,338,000 5,441,000 32.4 5,430,033 11.7% (male 238,912; female 396,582)
total population: 74.43 years male: 70.44 years female: 78.64 years
14
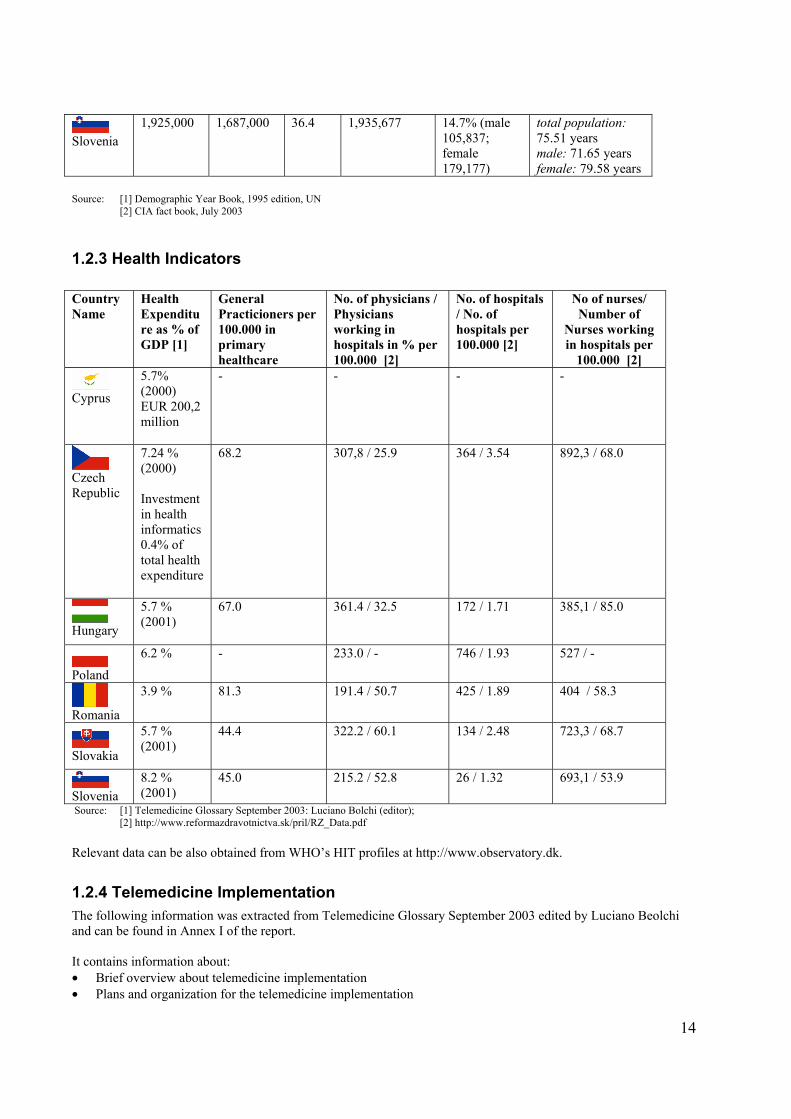
Slovenia
1,925,000 1,687,000 36.4 1,935,677 14.7% (male 105,837; female 179,177)
total population: 75.51 years male: 71.65 years female: 79.58 years
Source: [1] Demographic Year Book, 1995 edition, UN
[2] CIA fact book, July 2003
1.2.3 Health Indicators Country Name
Health Expenditure as % of GDP [1]
General Practicioners per 100.000 in primary healthcare
No. of physicians / Physicians working in hospitals in % per 100.000 [2]
No. of hospitals / No. of hospitals per 100.000 [2]
No of nurses/ Number of
Nurses working in hospitals per
100.000 [2]
Cyprus
5.7% (2000) EUR 200,2 million
- - - -
Czech Republic
7.24 % (2000) Investment in health informatics 0.4% of total health expenditure
68.2 307,8 / 25.9 364 / 3.54 892,3 / 68.0
Hungary
5.7 % (2001)
67.0 361.4 / 32.5 172 / 1.71 385,1 / 85.0
Poland
6.2 %
- 233.0 / - 746 / 1.93 527 / -
Romania
3.9 %
81.3 191.4 / 50.7 425 / 1.89 404 / 58.3
Slovakia
5.7 % (2001)
44.4 322.2 / 60.1 134 / 2.48 723,3 / 68.7
Slovenia
8.2 % (2001)
45.0 215.2 / 52.8 26 / 1.32 693,1 / 53.9
Source: [1] Telemedicine Glossary September 2003: Luciano Bolchi (editor); [2] http://www.reformazdravotnictva.sk/pril/RZ_Data.pdf
Relevant data can be also obtained from WHO’s HIT profiles at http://www.observatory.dk.
1.2.4 Telemedicine Implementation The following information was extracted from Telemedicine Glossary September 2003 edited by Luciano Beolchi and can be found in Annex I of the report. It contains information about: • Brief overview about telemedicine implementation • Plans and organization for the telemedicine implementation
15
in Cyprus, Czech Republic, Hungary, Poland, Romania, Slovakia and Slovenia. 1.2.5 Economic and Information Technologies (IT) indicators
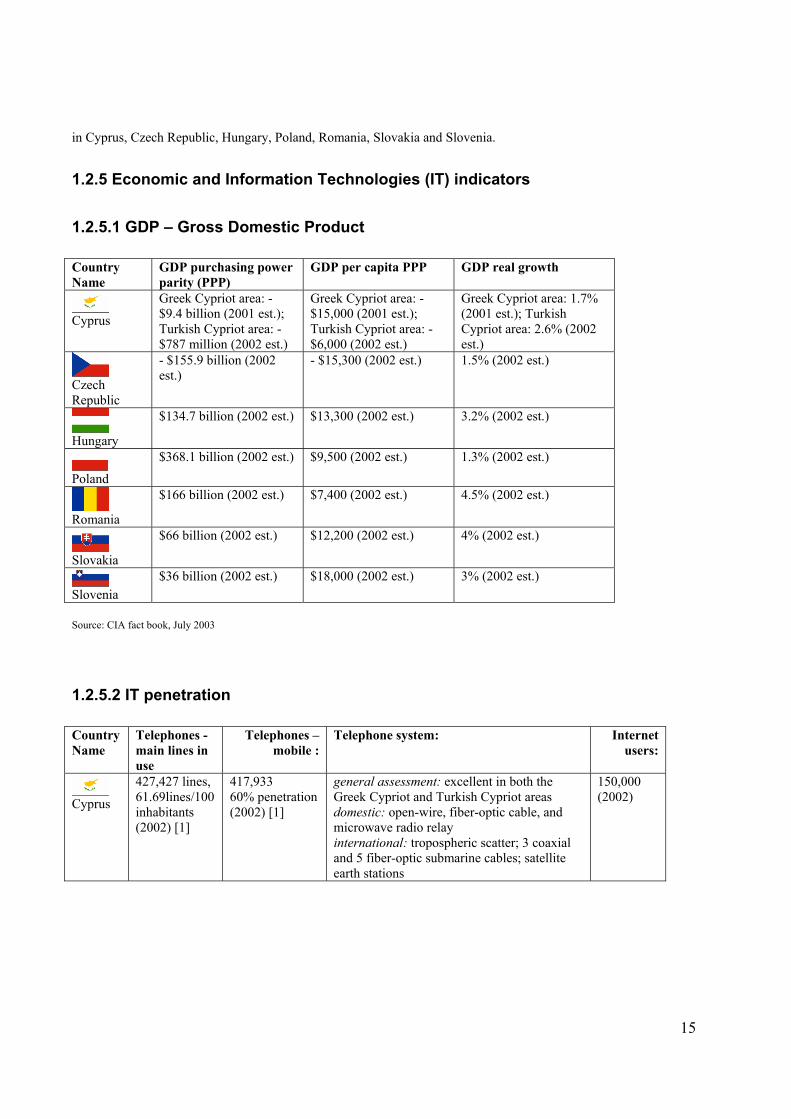
1.2.5.1 GDP – Gross Domestic Product Country Name
GDP purchasing power parity (PPP)
GDP per capita PPP GDP real growth
Cyprus
Greek Cypriot area: - $9.4 billion (2001 est.); Turkish Cypriot area: - $787 million (2002 est.)
Greek Cypriot area: - $15,000 (2001 est.); Turkish Cypriot area: - $6,000 (2002 est.)
Greek Cypriot area: 1.7% (2001 est.); Turkish Cypriot area: 2.6% (2002 est.)
Czech Republic
- $155.9 billion (2002 est.)
- $15,300 (2002 est.) 1.5% (2002 est.)
Hungary
$134.7 billion (2002 est.) $13,300 (2002 est.) 3.2% (2002 est.)
Poland
$368.1 billion (2002 est.) $9,500 (2002 est.) 1.3% (2002 est.)
Romania
$166 billion (2002 est.) $7,400 (2002 est.) 4.5% (2002 est.)
Slovakia
$66 billion (2002 est.) $12,200 (2002 est.) 4% (2002 est.)
Slovenia
$36 billion (2002 est.) $18,000 (2002 est.) 3% (2002 est.)
Source: CIA fact book, July 2003
1.2.5.2 IT penetration Country Name
Telephones - main lines in use
Telephones – mobile :
Telephone system: Internet users:
Cyprus
427,427 lines, 61.69lines/100 inhabitants (2002) [1]
417,933 60% penetration (2002) [1]
general assessment: excellent in both the Greek Cypriot and Turkish Cypriot areas domestic: open-wire, fiber-optic cable, and microwave radio relay international: tropospheric scatter; 3 coaxial and 5 fiber-optic submarine cables; satellite earth stations
150,000 (2002)
16
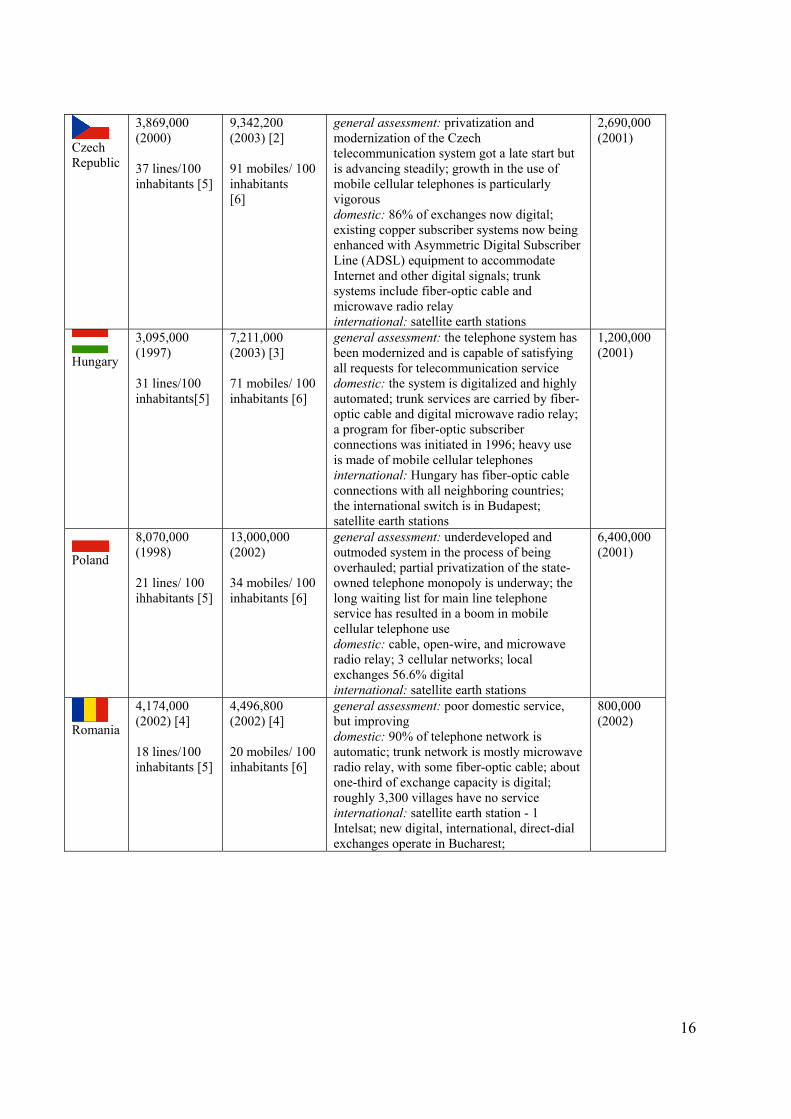
Czech Republic
3,869,000 (2000) 37 lines/100 inhabitants [5]
9,342,200 (2003) [2] 91 mobiles/ 100 inhabitants [6]
general assessment: privatization and modernization of the Czech telecommunication system got a late start but is advancing steadily; growth in the use of mobile cellular telephones is particularly vigorous domestic: 86% of exchanges now digital; existing copper subscriber systems now being enhanced with Asymmetric Digital Subscriber Line (ADSL) equipment to accommodate Internet and other digital signals; trunk systems include fiber-optic cable and microwave radio relay international: satellite earth stations
2,690,000 (2001)
Hungary
3,095,000 (1997) 31 lines/100 inhabitants[5]
7,211,000 (2003) [3] 71 mobiles/ 100 inhabitants [6]
general assessment: the telephone system has been modernized and is capable of satisfying all requests for telecommunication service domestic: the system is digitalized and highly automated; trunk services are carried by fiber-optic cable and digital microwave radio relay; a program for fiber-optic subscriber connections was initiated in 1996; heavy use is made of mobile cellular telephones international: Hungary has fiber-optic cable connections with all neighboring countries; the international switch is in Budapest; satellite earth stations
1,200,000 (2001)
Poland
8,070,000 (1998) 21 lines/ 100 ihhabitants [5]
13,000,000 (2002) 34 mobiles/ 100 inhabitants [6]
general assessment: underdeveloped and outmoded system in the process of being overhauled; partial privatization of the state-owned telephone monopoly is underway; the long waiting list for main line telephone service has resulted in a boom in mobile cellular telephone use domestic: cable, open-wire, and microwave radio relay; 3 cellular networks; local exchanges 56.6% digital international: satellite earth stations
6,400,000 (2001)
Romania
4,174,000 (2002) [4] 18 lines/100 inhabitants [5]
4,496,800 (2002) [4] 20 mobiles/ 100 inhabitants [6]
general assessment: poor domestic service, but improving domestic: 90% of telephone network is automatic; trunk network is mostly microwave radio relay, with some fiber-optic cable; about one-third of exchange capacity is digital; roughly 3,300 villages have no service international: satellite earth station - 1 Intelsat; new digital, international, direct-dial exchanges operate in Bucharest;
800,000 (2002)
17
Slovakia
1,934,558 (1998) 36 lines/ 100 inhabitants [5]
3,100,000 (2003) 58 mobiles/ 100 inhabitants [6]
general assessment: a modernization and privatization program is increasing accessibility to telephone service, reducing the waiting time for new subscribers, and generally improving service quality domestic: predominantly an analog system that is now receiving digital equipment and is being enlarged with fiber-optic cable, especially in the larger cities; mobile cellular capability has been added international: three international exchanges (one in Bratislava and two in Banska Bystrica) are available
700,000 (2000)
Slovenia
722,000 (1997) 38 lines/ 100 inhabitants [5]
1,650,000 (2002) 86 mobiles/ 100 inhabitants [6]
domestic: 100% digital (2000) 600,000 (2001)
Source: CIA fact book, July 2003,
[1] Cyta Annual Report 2002, www.cyta.com.cy, [2] www.eurotel.cz, www.t-mobile.cz, www.ceskymobil.cz, [3] http://www.templetonthorp.com/en/news349, [4] http://www.alcatel.com/newslink/0302/pdf/latitude.pdf [5] Formula: IT penetration.Telephones-main lines in use/Demographic Data.Total population [6] Formula: IT penetration.Telephones-mobile/Demographic Data.Telephones-mobile
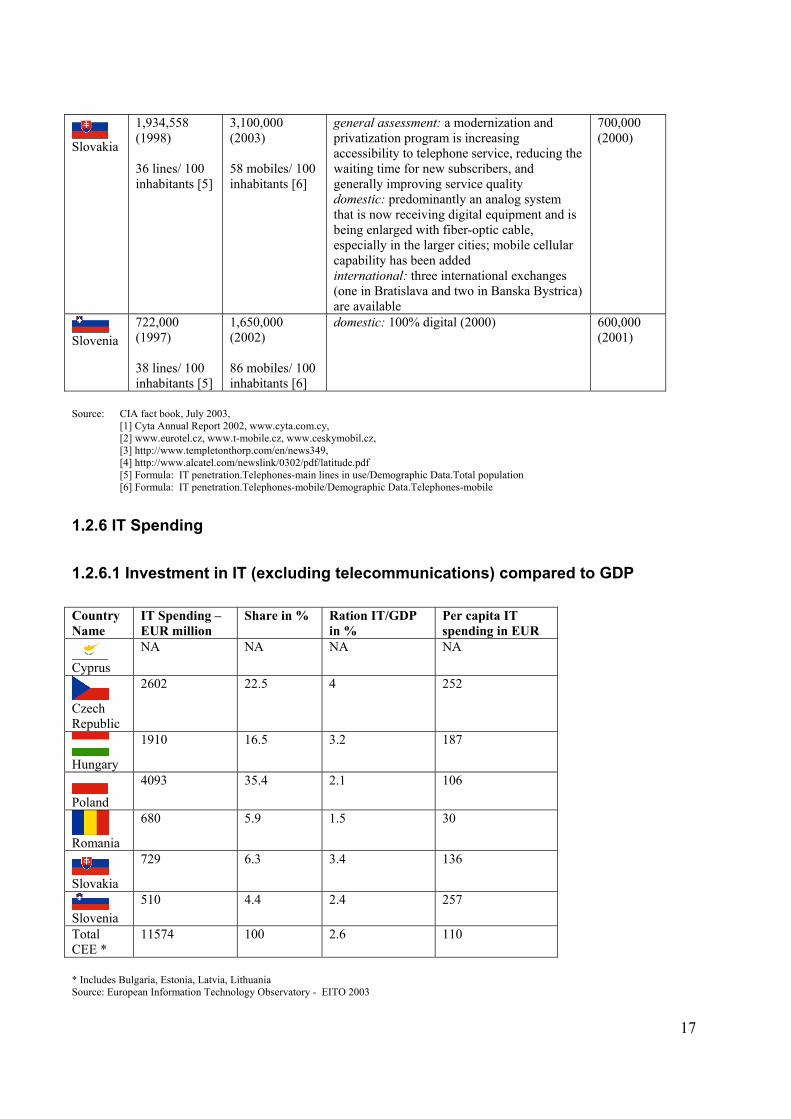
1.2.6 IT Spending
1.2.6.1 Investment in IT (excluding telecommunications) compared to GDP Country Name
IT Spending – EUR million
Share in % Ration IT/GDP in %
Per capita IT spending in EUR
Cyprus
NA NA NA NA
Czech Republic
2602 22.5 4 252
Hungary
1910 16.5 3.2 187
Poland
4093 35.4 2.1 106
Romania
680 5.9 1.5 30
Slovakia
729 6.3 3.4 136
Slovenia
510 4.4 2.4 257
Total CEE *
11574 100 2.6 110
* Includes Bulgaria, Estonia, Latvia, Lithuania Source: European Information Technology Observatory - EITO 2003
18
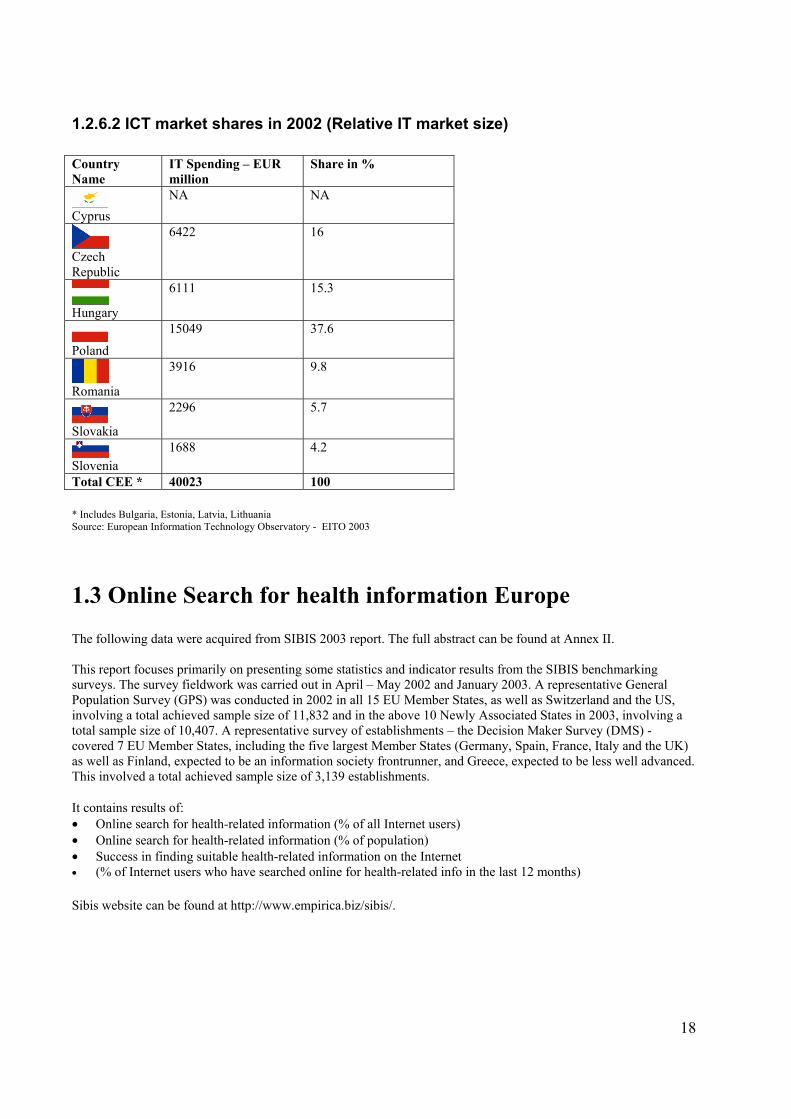
1.2.6.2 ICT market shares in 2002 (Relative IT market size) Country Name
IT Spending – EUR million
Share in %
Cyprus
NA NA
Czech Republic
6422 16
Hungary
6111 15.3
Poland
15049 37.6
Romania
3916 9.8
Slovakia
2296 5.7
Slovenia
1688 4.2
Total CEE * 40023 100 * Includes Bulgaria, Estonia, Latvia, Lithuania Source: European Information Technology Observatory - EITO 2003
1.3 Online Search for health information Europe The following data were acquired from SIBIS 2003 report. The full abstract can be found at Annex II. This report focuses primarily on presenting some statistics and indicator results from the SIBIS benchmarking surveys. The survey fieldwork was carried out in April – May 2002 and January 2003. A representative General Population Survey (GPS) was conducted in 2002 in all 15 EU Member States, as well as Switzerland and the US, involving a total achieved sample size of 11,832 and in the above 10 Newly Associated States in 2003, involving a total sample size of 10,407. A representative survey of establishments – the Decision Maker Survey (DMS) - covered 7 EU Member States, including the five largest Member States (Germany, Spain, France, Italy and the UK) as well as Finland, expected to be an information society frontrunner, and Greece, expected to be less well advanced. This involved a total achieved sample size of 3,139 establishments. It contains results of: • Online search for health-related information (% of all Internet users) • Online search for health-related information (% of population) • Success in finding suitable health-related information on the Internet • (% of Internet users who have searched online for health-related info in the last 12 months) Sibis website can be found at http://www.empirica.biz/sibis/.
19
2. Country Profiles
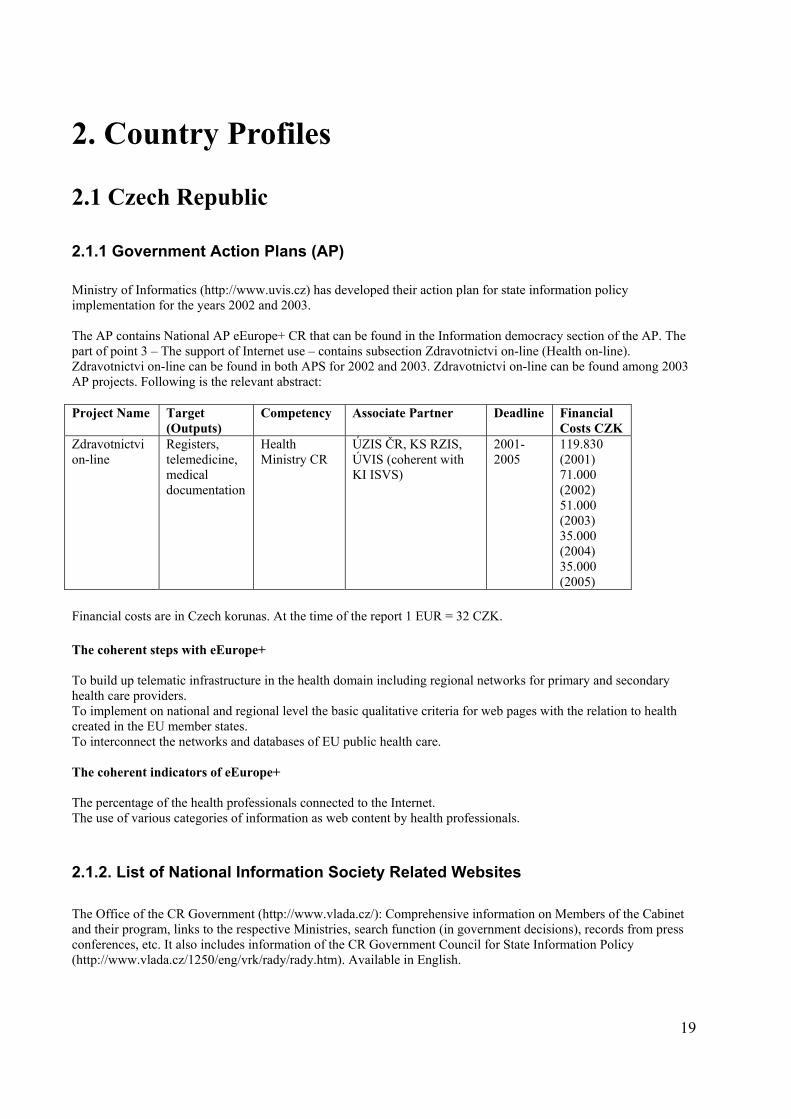
2.1 Czech Republic 2.1.1 Government Action Plans (AP) Ministry of Informatics (http://www.uvis.cz) has developed their action plan for state information policy implementation for the years 2002 and 2003. The AP contains National AP eEurope+ CR that can be found in the Information democracy section of the AP. The part of point 3 – The support of Internet use – contains subsection Zdravotnictvi on-line (Health on-line). Zdravotnictvi on-line can be found in both APS for 2002 and 2003. Zdravotnictvi on-line can be found among 2003 AP projects. Following is the relevant abstract: Project Name Target
(Outputs) Competency Associate Partner Deadline Financial
Costs CZK Zdravotnictvi on-line
Registers, telemedicine, medical documentation
Health Ministry CR
ÚZIS ČR, KS RZIS, ÚVIS (coherent with KI ISVS)
2001-2005
119.830 (2001) 71.000 (2002) 51.000 (2003) 35.000 (2004) 35.000 (2005)
Financial costs are in Czech korunas. At the time of the report 1 EUR = 32 CZK. The coherent steps with eEurope+ To build up telematic infrastructure in the health domain including regional networks for primary and secondary health care providers. To implement on national and regional level the basic qualitative criteria for web pages with the relation to health created in the EU member states. To interconnect the networks and databases of EU public health care. The coherent indicators of eEurope+ The percentage of the health professionals connected to the Internet. The use of various categories of information as web content by health professionals.
2.1.2. List of National Information Society Related Websites
The Office of the CR Government (http://www.vlada.cz/): Comprehensive information on Members of the Cabinet and their program, links to the respective Ministries, search function (in government decisions), records from press conferences, etc. It also includes information of the CR Government Council for State Information Policy (http://www.vlada.cz/1250/eng/vrk/rady/rady.htm). Available in English.
20
The Office for Public Information Systems (http://www.uvis.cz/): New website, currently under preparation. Access to basic documents related to State Information Policy, standards, and information from abroad, links to information resources. Available in English. Czech Forum for Information Society (http://www.info-forum.cz/indexe.html): The Forum is intended as a public dialogue on information society issues. Available in English. Czech Telecommunication Office (http://www.ctu.cz/index_a.htm): Site presents the origins of the Czech Telecommunication Office, its mission and activities. List of legal acts and implementing provisions. International activities. Available in English. Central website address (http://www.centralni-adresa.cz/cadr/index.htm): The official information system on public procurement and auctions. Link to the Public Administration portal (Prototype version) which is to become an integrated site to get information and/or use the services of public administration bodies. Available only in Czech. Source: eEurope+ 2003, Action Plan, June 2001 http://www.kbn.gov.pl/cele/eeurope/eeurope.pdf
2.1.3 Ministry of Health The official Ministry’s web site can be found at www.mzcr.cz. The specialized section for Health informatics can be found at http://www.mzcr.cz/kat/8 (Czech version only). 2.1.4 The use of the Internet in Czech Health Institutions in 2002 The following data were acquired from the information bulletin no. 13 from 3.4.2003 of UZIS CR (Institute of health information and statistics CR). For the complete information see Annex III of the report. The report consists of the data concerning: • The purpose of communication over the Internet. • The purpose of acquiring information over the Internet. • The use of the Internet in pharmacies and at GP office in 2002 • The use of the Internet for gaining the Information 2.1.5 Survey of the Information Systems (IS) in the Czech Hospitals 2003 The survey was conducted by Ministry of Health CR and IPVZ (Institute of postgraduate education in health), Prague. For the complete report please go to Annex IV of the report. The following data come from Anketa informatiku ceskych nemocnic, vysledky jaro 2003 (Survey of IT personnel in Czech hospitals, results spring 2003), edited June – August 2003, MuDr. Miroslav Seiner, IPVZ Prague. Note: HIS = Hospital information system The report consists of the data concerning: • Return of the sent our questionnaires • Types and size of the health institutions • State and perspective of building IS
• Current state of building of integrated HIS in the health institution • Satisfaction with complete HIS • Satisfaction with unfinished HIS • The reasons for not implementing HIS
• The opinions about the perspective of the various types of applications • Interest in further IS
21
• HIS personnel • Position of head of IT dept. • Status of the position • Education level of heads of IT dept.
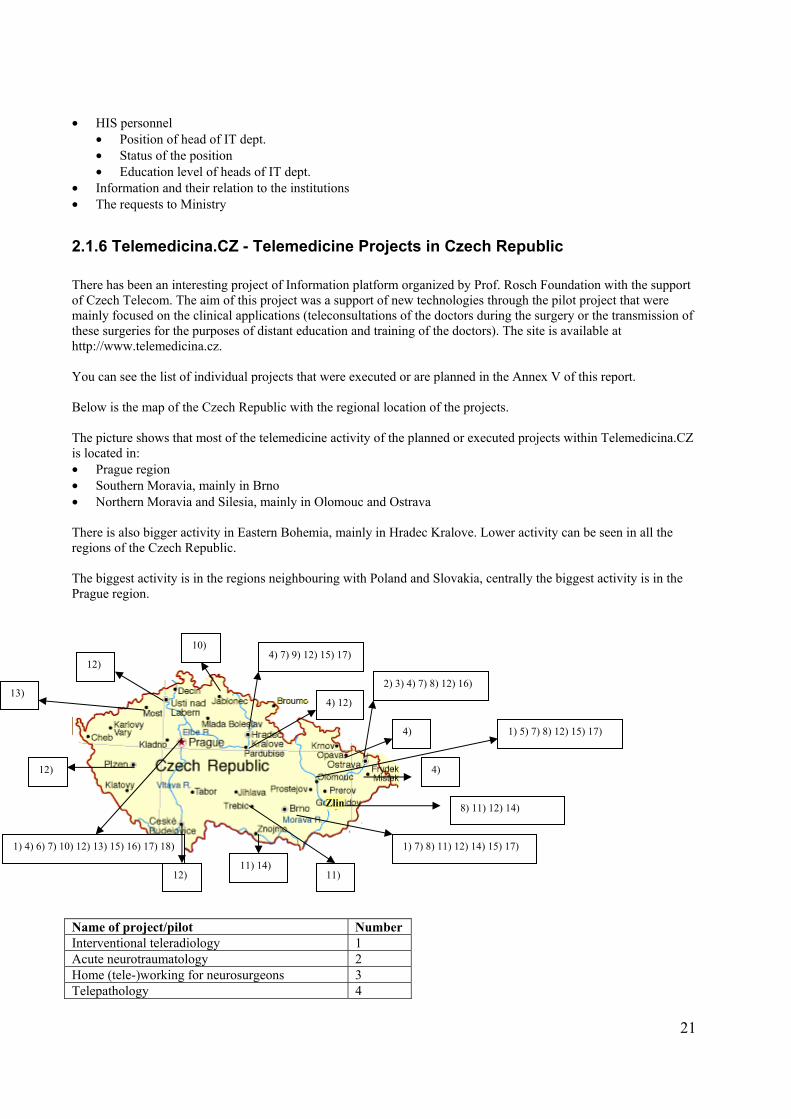
• Information and their relation to the institutions • The requests to Ministry 2.1.6 Telemedicina.CZ - Telemedicine Projects in Czech Republic There has been an interesting project of Information platform organized by Prof. Rosch Foundation with the support of Czech Telecom. The aim of this project was a support of new technologies through the pilot project that were mainly focused on the clinical applications (teleconsultations of the doctors during the surgery or the transmission of these surgeries for the purposes of distant education and training of the doctors). The site is available at http://www.telemedicina.cz. You can see the list of individual projects that were executed or are planned in the Annex V of this report. Below is the map of the Czech Republic with the regional location of the projects. The picture shows that most of the telemedicine activity of the planned or executed projects within Telemedicina.CZ is located in: • Prague region • Southern Moravia, mainly in Brno • Northern Moravia and Silesia, mainly in Olomouc and Ostrava There is also bigger activity in Eastern Bohemia, mainly in Hradec Kralove. Lower activity can be seen in all the regions of the Czech Republic. The biggest activity is in the regions neighbouring with Poland and Slovakia, centrally the biggest activity is in the Prague region.
Name of project/pilot Number Interventional teleradiology 1 Acute neurotraumatology 2 Home (tele-)working for neurosurgeons 3 Telepathology 4
1) 7) 8) 11) 12) 14) 15) 17) 1) 4) 6) 7) 10) 12) 13) 15) 16) 17) 18)
Zlin 8) 11) 12) 14)
1) 5) 7) 8) 12) 15) 17)
2) 3) 4) 7) 8) 12) 16)
4)
11) 14) 12) 11)
12)
4) 7) 9) 12) 15) 17)
4) 12)
10)
12)
13)
4)
22
Interconnection of the Olomouc country hospitals 5 Telecardiology 6 Telehematology 7 Teleortography 8 Teleconsultations and treatment of acute myocardial infarction
9
Teleconsultation of laparoscopic executions 10 Interconnection of Brno region hospitals 11 Teletraumatology 12 Teleconsultation in the area of pediatric auxomology and syndromology
13
Interconnection of Injury hospital Brno with cooperating hospitals
14
Teleendoscopy 15 Teledermatology 16 Telearthroscopy 17 Telebronchoscopy 18
2.1.7 ROSCH Foundation Recent Activities Since established in 1998, the Foundation and its partners have participated in the following activities:
• Five point-to-point tele-video medical specialty conferences between Prague and Portland, Oregon. • Two multi-point televideo medical conferences between Prague, Graz and Portland, Oregon, USA. • Regular multi-point televideo conferencing and teleconsutation services between a constellation of five
Czech hospitals in Prague, Hradec Kralove, Olomouc and Brno. • Technical planning and performance of more than 20 hours of transmission of live cases and multi-point
panel discussion to the 6th and 7th International Workshop in interventional radiology. • Live case transmission with demonstration of new minimal invasive procedures to five international
meetings in Europe and Asia. • Performance of a three-hour tele-meeting on advances in minimal invasive treatment with physicians in
Japan. • Teleconsultation in neurosurgery between 10 hospitals in Northern Moravia for facilitating diagnosis of
head and spine trauma injury management. • Home working via PCs and ISDN services for neurosurgeons at the Ostrava Hospital in the Czech
Republic. • Telepathology consultation at 6 Czech hospitals. • Telecardiology at several Czech hospitals with successful transmission of echocardiographic studies and
teleconsultations. 2.1.8 IZIP – Internet Medical Database For the full text please go to Annex VI of this document. You can find complete info about the project at the project website: http://www.izip.cz. The abbreviation IZIP in Czech language means Internet Access to Patient's Medical Information. The objective and substance of the IZIP project is to place the medical database of the insured patient into the public information network - the Internet.
23
The database consists of selected parts of medical documentation written into IZIP by the attending physicians. Both the doctor and the patient may at any time use a computer with internet access to view the results of clinical examinations, laboratory tests and X-ray pictures as well as a list of prescribed and used medicaments. The IZIP project is executed by a private company IZIP Ltd., Prague, with the support of General Health Insurance Fund of the Czech Republic (VZP CR) and other partners such as IBM, Czech Telecom, Eurotel, Komercni banka and others. The application solution, software and implementation are supplied by IBM, and the Czech Telecom and Eurotel look after the data transfer. Initiators Initiators of the projects were Pavel Hronek otorhinolaryngologist, Milan Cabrnoch pediatrician and Miroslav Ouzky rehab doctor. Demo version Available at http://www.izip.cz/demo/ 2.1.9 MEDTEL & NetC@rd For the full text concerning MEDTEL and NetC@rd project, please go to Annex VII of this document. You can find complete info about the project at the project website: http://www.medtel.cz/index_e.php. MEDTEL, o.p.s. is a non-profit organization. MEDTEL is a member of EHTEL. NetC@rd project Czech Republic prepares countrywide introduction of new health insurance cards for the ensured persons of VZP (70% of population) at the middle of 2004. The card reverse will have European health insurance card (EHIC) format and CR will be one of the first countries where EHIC will be implemented. Goal of the pilot project The goal is to securely identify the insured person and to create the pre-requisite for the automated authorization of the transactions. Costs related to the Czech part: 310,000,- EUR 2.1.10 MeDiMed – Regional Centre for Archiving and Interhospital Exchange of Medical Multimedia Data The website can be found at http://www.mou.cz and http://www.muni.cz. The goal of the project is to create shared outsourced medical multimedia data archiving and communication center which can serve as a “Trustworthy Neutral Exchange Point” for all participants of this project. More can be found at http://www.ten.cz/doc/2003/zprava/medimed.html (Czech only). 2.1.11 Czech Society of Nuclear Medicine The website of the Society can be found at http://www.csnm.cz/. PACS = Picture Archive and Communication System
24
PET = Position Emission Tomography The website describes telemedicine, PACS and PET systems in particular with the links to the PET center in Prague at Nemocnice Na Homolce hospital: http://www.homolka.cz/nm/. However in the time of writing this document there has been a second PET center opened in Brno at Masaryk Oncology Institute hospital: http://www.moi.cz/. The web site also contains various statistics for Czech Republic nuclear medicine data.
2.1.12 PET center in Nemocnice Na Homolce hospital For the information about position emission tomography (PET) center, go to the official website: http://www.homolka.cz/nm/index-e.html. PET Center Prague is located in a separate building within the complex of Na Homolce Hospital. The Department of Nuclear Medicine is located on the first floor of PET Center Prague. It is equipped with dedicated PET camera CTI/Siemens ECAT EXACT and with Siemens SPECT camera (E.CAM).
2.1.13 IKEM CZ – Institute for clinical and experimental medicine You can find out more about IKEM at http://www.ikem.cz IKEM hosts CZI MEDICON®, Healthcare Informatics Center for the development and operation of application and communication environment of the healthcare data network in the Czech Republic. It is a valuable resource for public, health outcome researchers, and academicians both in and outside of the Czech Republic. OVID System Ovid Web Gateway is an instrument for searching and working with bibliographical and full text information from the area of biomedicine. It is accessible to all employees of the member institutions of the consortium on the address: http://gateway.ovid.com/autologin.html Data Network of Health Department (dSRZ) medicon.cz DSRZ is multifunctional network of selected health institutions that are the base for future infrastructure of National Health Informational System (NZIS) and serve for informational and communicational needs of health department with country coverage, especially in the area of selected Informational System of NZIS framework DSRZ is realized on the base of TCP/IP protocol using the public network infrastructure of TCP/IP EUnet on top of which is built non-public network infrastructure of VPNs with the use of encrypted IP/IP tunnels. The traffic is separate from public Internet, at the same time there is a possibility to access Internet from the individual virtual private network (VPN). DSRZ is defined as a framework of mutually separated but interconnected independent VPNs of health sector with variable but controlled level of required level of security. This network infrastructure will enable other controlled, reliable and secure interconnection on other non-public and public networks, including the relationship on informational system of chip cards.
2.1.14 Euromise Euromise represents Education and Research in Medical Informatics and it can be found at http://www.euromise.cz and http://www.euromise2004.org. The European Center for Medical Informatics, Statistics and Epidemiology of Charles University and Academy of Sciences (EuroMISE Center) was set up in 1994.
25
Development of interdisciplinary postgraduate and lifelong education, mostly of university teachers, has been the main goal of the European project “Teaching Methodology for Heath Care” under the TEMPUS program and development of interdisciplinary research has started with the cooperation on the project “Managing Uncertainty in Medicine - MUM“ under the program COPERNICUS. The main targets of EuroMISE Center are: • To create an European teaching network for higher education in medical informatics, statistics and
epidemiology; • To organize and initiate graduate and postgraduate education on international level. • To start international research and development programs in the interdisciplinary field of medical informatics,
statistics and epidemiology; to cooperate closely with the healthcare resort. • Further development of the EuroMISE Center of Charles University and Academy of Sciences is based on close
cooperation with European universities, research and health organizations and on recommendations of the international committee.
Research Research activities of theEuroMISE Center are focused on the development of interdisciplinary research. It concentrates on methods of statistical data analyses, methods for extracting relevant information for decision making and managing uncertainty, methods for decision support, study of risk factors of diseases, mathematical methods in genetics and epidemiology. The research cooperation of the EuroMISE Center with other academic and health institutions is stimulated by Czech grant agencies (Grant Agency of the Czech Republic, Grant Agency of Charles University, Grant Agency of Ministry of Health of the Czech Republic) and by European projects MUM (COPERNICUS) and I4C - TRIPLEC (4th Framework Programme). Some research results are applied by programme prototypes, for example E. T. (quick processing of data from epidemiological studies), CORE (reduction and constitution of data) and HYPERTENZE (optimization of decision support in therapy of arterial hypertension). The results are published in both Czech and international journals. The EuroMISE Centre is also involved in editorial boards of journals (International Journal of Medical Informatics, Physician and Technology) and in scientific societies (IMIA, EFMI, Czech Medical Society of J. E. Purkyne, Society for cybernetics and Informatics of the Academy of Sciences of the Czech Republic). 2.1.15 Branch Contact Organization - Healthcare (BCO) Oborová kontaktní organizace - zdravotnictví (OKO) - Branch Contact Organization – Healthcare (BCO) in English. The web site can be found at http://www.oko-zdravotnictvi.cz. • Helps to involve Czech health care research subjects into the network of European institutions using shared
activities and programmes, especially with focus on the 5th Framework Programme of Research and Technological Development of EU (and prospectively on the 6th of Framework Programme),
• Is a small organization based on the common project of the Czech Medical Association J. E. Purkyne and the consulting of the Econsult and the financing with the grant support of the programme EUPRO by the Czech Ministry of Education,
• Reports the information about the programmes from the sphere of the international cooperation in the research and development at the health services of the Czech Ministry of Education,
• Is situated close to the secretariat of the Czech Medical Association in the Medical House in Prague (addr. Praha 2, Sokolská 31),
• Supports communication, coordination a cooperation among interested parties in the Czech Republic, especially healthcare researchers, small and medium-sized enterprises aimed on the health services and related partners in European Union,
• Organizes special informative events, looks for suitable partners for international projects of healthcare research and development,
• Assists and consults relevant project proposals, • Creates thematic database for healthcare research and innovation on Internet, • Opens up the Czech medical research and development on the Internet.
26
• Branch Contact Organization for healthcare closely collaborates with Technological Center of Academy of Science – the National Contact Organization for the 5th Framework Programme of EU, with related National Contact Point as well as with other regional and branch contact organizations.
2.1.16 Coordination Center for Departmental Medical Information Systems Koordinacni stredisko pro resortni zdravotnicke informacni systemy (KSRZIS) was established by the Ministry of Health as of December 1, 2000 as a contributive organization. The web site can be found at http://www.ksrzis.cz/. The main task of the Coordination Center is to perform managing, developing, coordination and publishing activity in medical informatics in connection with setup and operation of selected information systems with departmental force in the following areas:
national health registers other information systems of medical department.
Other tasks of the Center are in particular the following:
1. organization of direct operation and delegated administration of appointed departmental medical information systems,
2. organization and unification of information and communication technologies for operation of appointed medical information systems, particularly departmental data networks, system and application software, data interface, standards of medical informatics, and systems of electronic identification etc.,
3. Performance of data analysis according to health department requests.
The subject of activity of the Center is development, operation, and administration of data networks of the health department. The Center also fulfils tasks at development, operation and data processing in the following areas:
National register of cardiovascular interventions,
National register of patients after organ transplants,
National list of candidates for organ transplants including databases,
National register of deceased donors of organs including databases,
Other national medical registers appointed by the Health Ministry, Other information systems in the health department.
2.1.17 National Health Registers Following is the list of the national health registers. You can find complete details about the registers at http://www.ksrzis.cz/ (Czech version only) or in Annex VIII of this report. • IS TRANICON • National cardiosurgery registry (NKCHR) • National oncology registry (NOR) • National registry of vascular surgery • National registry of arthal replacements • Ophthalmology registry (OFR) • Nosocomial Infection registry (RNI)
27
2.1.18 Central registry of R&D projects The search in Central registry of R&D projects shows only 1 telemedicine project funded by Ministry of Health. The CEP web site is at http://www.vlada.cz/1250/rvv/cep/index_cep.html. Name: High-speed transmissions and archivation of digital medical images. Description: The project is of interdisciplinary character and deals with introducing the functional system of transmission and archiving image medicinal data into clinical practice and teaching the students and its effects on rationalization and economization of working. Another of the principal tasks is securing immediate availability of the data about patients for an attending physician and the possibility of immediate remote consultations of cases with colleagues. 2.1.19 List of Contacts Organization Name Contact Details Department of Informatics of Ministry of Health
Mr. Pribik – director Tel.: +420224972397
Department of Informatics of Ministry of Health
Mr. Cizek – deputy Tel.: +420224972774
Telemedicina.cz Ing. Jiri Valek tel./fax: 222318305, e-mail: [email protected]
ROSCH foundation Radek Svarz, Project Development Manager
e-mail: [email protected], [email protected] Phone: +420 2 4143 1122
MeDiMed Michal Javornik [email protected] IZIP e-mail: [email protected]
tel.: 00420 224 212 200 MEDTEL, o.p.s. tf: 233 376 194
e-mail: [email protected] PET centre – Na Homolce hospital
Otakar Belohlavek Tel.: +(420) 25727 2165
IKEM Head of Information and communication department Ing. Vladimír ROUS
tel: 261 364 201 email: [email protected]
Euromise Jana Zvárová head of the department
+420 266 053 097 [email protected]
Coordination Center for Departmental Medical IS
tel.: +420 2 6136 4045 e-mail: [email protected]
28
2.2 Hungary
2.2.1 Ministry of Health The official website of the Ministry is at http://www.eszcsm.hu/eszcsm/eszcsm_angol.main.page. Health Portal Ministry of Health also hosts a health portal at: http://www.eszcsm.hu/eszcsm/agazati_angol.main.page. At the moment the information is available only in Hungarian.
2.2.2 Ministry of Informatics and Communication The official website of the Ministry is at http://www.ihm.hu. eHungary eHungary is an action plan (AP) for information society for the years 2004 – 2006. eHealth is one of the sectoral responsibilities for the AP. Unfortunately it doesn’t contain any concrete projects mentioned in the text. More info can be found at http://www.ihm.hu/English/_20030211_5.html.
2.2.3 List of National Information Society Related Websites The Government of the Hungarian Republic (http://www.meh.hu/). Ministry of Informatics and Communication (http://www.ihm.hu/). 2.2.4 eHealth in Hungary There are 2 reports describing telemedicine situation in Hungary. The 1st report was written by Peter Futo and it’s part of SIBIS+Project WP4, Policy Issues document published 29. January 2003 in Budapest. This report gives overview about eHealth situation. The 2nd report was written by Sandor G. Vari, Tamas Gergely and Pal Simon and contains several articles giving more detailed information about the topic. This report is quite large in volume and it contains 30 pages. It contains articles about: - Historical review - Major milestones of Information Society Technologies (IST) development and implementation - The current situation of health informatics in Hungary - Implementation and use of the IST by hospitals/doctors today - Review of the National and EU RTD activities and implementations - IST strategies and action plan for eHealth in Hungary - and General comments regarding eHealth in Hungary You can find the 1st report in Annex IX and 2nd report in Annex X of this report.
29
2.2.5 National Institute and Library for Health Information Founded with the purpose to provide the Hungarian medical community with the latest achievement of foreign medical sciences. Its function is to provide information and literature to healthcare institutes, the community at large, and experts working in the healthcare profession. The official website of the Institute can be found at: http://www.medinfo.hu/index_en.html. The large abstract about the Institute can be found at Annex XI at the end of this report. The abstract contains info about: • Health communication • Healthline • National Library of Health Sciences • Proprietary databases • Other services • Other tasks 2.2.6 GYOGYINFOK – Center for Healthcare Information Gyogyinfok is the Center for Healthcare Information of the Ministry of Health, Social and Family Affairs. The Center’s website can be found at http://www.gyogyinfok.hu/angol.htm. Scope of activities: An organizational-methodological and research institution of the Ministry of Health, Social and Family Affairs in the field of health informatics with national responsibilities. Projects Programs (only in Hungarian) DRGs Version 4.3; DRGs Version 4.1; DRGs Version 4.0 DRGs Version 3.0; DRGs Version 3.1; DRGs Version 3.2 Outpatient unit's activity (TETELES Version 7.3) Dental program for data gathering at patient encounter level (TETFOG Version 2.82) 2.2.7 Hungarian Office for Research and development HunOR was established in 1999 by a national consortium of organizations responsible for science, research and development in Hungary in order to facilitate successful participation of Hungary in the Framework Programmes. The official website with information can be found at http://www.hunoriroda.hu/english.htm. 2.2.8 Institute of Experimental Medicine The Institute of Experimental Medicine of the Hungarian Academy of Sciences in Budapest is the only research institute in Hungary dedicated exclusively to medical research. The Institute’s website can be found at http://www.koki.hu/.
30
2.2.9 OTKA – National Research Institute Provides independent and extensive support to scientific research and to the research infrastructure and gives assistance for young researchers and to promote the achievement of scientific achievements of international standards. The website can be found at http://www.otka.hu.
2.2.10 Computer and Automation Research Institute, Hungarian Academy of Sciences The website of the Institute can be found at http://www.sztaki.hu. The list of the projects can be found at http://www.sztaki.hu/sztaki/projects/.
2.2.11 PROREC.HU & WIDENET The Hungarian PROREC Center is a separate project of the Computer and Automation Research Institute of the Hungarian Academy of Sciences. The main goal of PROREC is to promote and co-ordinate the European wide convergence towards comprehensive, communicable and secure Electronic Healthcare Records (EHCR). The full information can be found at http://www.sztaki.hu/projects/prorec-hu/Htmleng/prorec-hu.html.
2.2.12 PRIMACOM
The official website can be found at http://www.primacom.dk. The INCO-COPERNICUS project PRIMACOM (PRIMAry Care Physician’s COMmunication Network) demonstrates how such communication can be established in regions in Hungary and Slovenia. PRIMACOM is building on European messaging standards for EDI (Electronic Data Interchange) with practical experience from the Danish MedCom project. PRIMACOM is building on European messaging standards for EDI (Electronic Data Interchange) with practical experience from the Danish MedCom project and already commercialised in Slovenia and Hungary. The pilot site in Hungary includes a hospital and primary care center. A Hungarian software provider and a consultant are involved.
2.2.13 RETRANSPLAT The website can be found at: http://retransplant.vitamib.com/. The full abstract can be found in Annex XII of the report. Regional and International Integrated Telemedicine Network for Organ Transplant
31
The RETRANSPLANT project aims to facilitate the development of Telematics tools for dialysis and organ transplant centers, organizations coordinating recipient-donor selection, and other health care facilities for transplant services in the Central Eastern European Countries (CEE).
2.2.14 MiM – Medical Info Media
Health communication and information system provides information resources to the medical community by the one hand, and the consumers who search recovery, and rehabilitation by the other hand. The system enlists healthcare professionals, provides contact details and presentation of businesses, organizations and institutions related to health care in general. The website can be found at http://www.mimnet.hu/0200_eng/. 2.2.15 VARIMED Health Portal with the links to Hungarian telemedicine projects. The website can be found at http://www.varimed.hu/. 2.2.16 List of Contacts Organization Name Contact details Prorec.HU & Widenet György Szántó [email protected]
Tel: (+36 1) 209 5270 Primacom Attila Simay
Family Doctors Association of Miskolc
e-mail: [email protected] Phone: +36 46 320 335
Primacom Geza Nagy Semmelwis Hospital Dept. of Anesth. & CCU
e-mail: [email protected]
Primacom László Szerényi Praxis Medical System
Phone: +36 30 584 612 e-mail: [email protected]
Varimed Dr. Sandor G. Vari Phone:(818) 904-1954 (USA) Mobile: (818) 398-2642 (USA) Phone:36-1 487-0430 (Hungary) e-mail : [email protected]
32
2.3 Poland 2.3.1 Ministry of Health The official Ministry’s web site can be found at http://www.mz.gov.pl. The contact list of the Ministry can be found at http://www.mz.gov.pl/wwwmz/index?mr=m01411&ms=&ml=en&mi=141&mx=0&ma=656. 2.3.2 List of National Information Society Related Websites The website of the Polish Forum for Information Society (http://www.kbn.gov.pl/cele/index.html), the advisory body to the Council of Ministers, presents the basic Polish documents related to the Information Society development in Poland as well as the activities of the Forum. The Information Society website maintained by the State Committee for Scientific Research (KBN) (http://www.kbn.gov.pl/gsi/index_eng.html) presents the strategy "Aims and Directions of the Information Society Development in Poland" adopted by the Council of Ministers in 2000, other documents related to the Information Society development in Poland, links to the websites of European Information Society (documents, programmes, etc.) and provides information on the IST programme. Some essays and interviews could also be found. The website of the Ministry of Posts and Telecommunications (http://www.ml.gov.pl/english/documents/index.html) presents the list of ministerial licenses, regulations and documents; among them the latest "ePoland - The Strategy of an Information Society Development in Poland for 2001-2006". The Polish Information Processing Society website (http://www.pti.org.pl/english/index.html) provides information on the Society activities. It also presents some useful links to the Polish, foreign and international organizations active in IT related issues and provides information on the European Computer Driving License. The Interkl@sa programme website (http://www.interklasa.pl/portal/index/strony) presents the wide range of initiatives related to the education aspects of Information Society. It gives an overview of the actions undertaken, links to some educational web sites and many institutions active in this field. Source: eEurope+ 2003, Action Plan, June 2001 http://www.kbn.gov.pl/cele/eeurope/eeurope.pdf 2.3.3 ePolska (ePoland) On 11 September, 2001 the Council of Ministers adopted the document "ePoland – Action Plan on the Information Society Development in Poland for the years 2001 – 2006", which follows the approach of the "eEurope+" action plan and has to be updated annually. [1] Following is the part of the extract from ePolska AP that is focused on Health Care on-line. You can see the full abstract concerning eHealth in Annex XIII or the full report at http://www.kbn.gov.pl/cele/epolska/epoland.html. Specific tasks [2]
No Task Implementing / co-ordinating agencies Source of financing
Term of implementation
Creation of a uniform electronic data base on medical establishments and facilities, available via
CSIOZ
(Health Care
MoH (Ministry of Health) budget end of 2001
33
the Internet Information Systems Center)
Creation of an electronic data base on doctors, with the location, medical specialty, surgery hours, available in each medical facility
Supreme Chamber of Medical Practitioners
MoH and Supreme Chamber of Medical Practitioners budgets
end of 2002
Creation of a data base on patients covered by health insurance Agency appointed
by MoH
MoH and/or Sickness Fund (Kasa Chorych) budget
end of 2003
Development and implementation of an electronic system which supports reporting and presentation of information on health care
CSIOZ source of financing under agreements
after consultations
Determination and co-ordination of standards of electronic data interchange in medicine CSIOZ CSIOZ budget after
consultations
Establishment of the legal framework allowing payments for medical services to made over telematics networks
MoH MoH, voivods and Sickness Funds budgets
end of 2001
Preparation of a plan for the implementation of telemedicine
Agency appointed by MoH
source of financing under agreements
after consultations
Development and implementation of pilot distance training programmes CSIOZ CSIOZ budget after
consultations
Drawing up of legal and technical assumptions for the system of verification and authentication of information on medical products and services CSIOZ CSIOZ budget After
consultations
Source: [1] eEurope+ Progress Report, Ljubjana 3-4.5.2002, http://www.kbn.gov.pl/cele/ljubljana/index.html [2] ePolska Action Plan, http://www.kbn.gov.pl/cele/epolska/epoland.html 2.3.4 National Health Care Programme The National Health Care Programme (NHCP) as it exists now doesn’t contain any notion of telemedicine. The current NHCP sets objectives and guiding principles of the public health policy in Poland by the year 2005. The full version of NHCP can be viewed at http://www.medstat.waw.pl/nhp/index.html – English version residing on Department of Medical Statistics server (www.medstat.waw.pl) 2.3.5 Registry of Medical Services The following information was given by Katarzyna Owie¿awska [[email protected]] from ASM - Centrum Badan i Analiz Rynku Sp.z.o.o. ,SIBIS – national contact.
34
The construction of the integrated system of the Ministry of Health includes a currently realised set of projects, under the name “Register of Medical Services”. This is the biggest IT investment in the Polish history. The “RMS” project involves plans of issuing Health Insurance Cards for the entire society. The register of Health Care Institutes is being developed, and the Register of Pharmacies is being prepared for implementation. Common access to medical information will increase the participation of patients in the process of treatment. They will have the possibility to find information e.g. about the location of a selected health-care institution, the specialisation of a chosen doctor, the medical services offered etc.
2.3.6 National Pharmaceutical Portal National Pharmaceutical Portal can be found at http://www.pharmacy.pl/fwp/fwp.htm. It contains several search engines to search in address or drug databases, it contains calendar with local or national health events and it also contains legal matters, information about pharmaceutical magazines, pharmaceutical organizations and other pharmaceutical data. Unfortunately the whole project is in Polish only. 2.3.7 Informatization of hospitals in the Malopolskie province, 2002 The following are data describing IT in terms of hardware (in this case hospital's IT network), software (related to medical and administrative activities) and degree of it's integration in the Malopolskie province hospital. Malopolskie province is situated in the southeast of Poland with the capital city Crakow. For the complete report please go to Annex XIV of the report. The report contains the data about: • Types of IT personnel in hospitals • Information network coverage in hospitals • Range and level of the software integration used in hospitals • Planned time of introducing full integration • Forecasted costs for full informatization
2.3.8 Telemedicine at University Hospital in Krakow The following article was written by Witold Poniklo from Academic Computer Center CYFRONET of the University of Science and Technology in Cracow. For the complete article please go to Annex XV of the report. This memo consists of two parts – one describing University Hospital in Krakow achievements and second, pointing at the potential telemedicine system’s users. 2.3.9 Telemedicine in Poland Extensive report written by Mariusz Duplaga from CYFRONET can be found at Annex XVI of the report. The report contains information about: • National action plan • Barriers to successful implementation of telemedicine • Telemedicine technologies used by hospitals/doctors
35
• Status of HER • eHealth initiatives/pilots in Poland 2.3.10 Research and Development Units Following is the list of the R&D institutes in Poland. As an example I chose Instytut Fizjologii i Patologii Sluchu with their example of the successful project they participated in. The complete list of R&D Units can be seen in Annex XVII of this report. Instytut Fizjologii i Patologii Słuchu ul. Pstrowskiego 1 01-943 Warszawa tel. (022) 835-66-70 fax (022) 835-52-14 [email protected] Internet page: www.ifps.org.pl The Institute has organized and is the coordinator of the Program of Care over the Hearing-Impaired in Poland (1997). The general aim of that Program is to establish a uniform, complex system of care for all the hearing impaired providing more effective services for the deaf and hard of hearing, meeting the needs in diagnostics, treatment and rehabilitation, education and social welfare One of the first is the program of universal hearing screening "Słyszę..." (I can hear...) created to identify hearing impairments in children and teenagers (age 6-19 years) as early as possible and to provide immediate proper treatment and rehabilitation. In the next, original tools, diagnostic and rehabilitation systems, the latest achievements in informatics technology have been used to fight hearing impairments, tinnitus, speech and vision disorders. The prepared multimedia tools ("Mówię..." - I can speak...; "Tinnitus"; "Widzę..." - I can see...) solve many technical problems in audiological, phoniatric and speech and language pathology diagnostics and rehabilitation in a very economical way which makes it possible to be introduced on a mass scale. The institute has also recently been producing set of diagnostic and educational programs on CDs. The programs are aimed at persons interested in rehabilitation of hearing impairments and communication disorders. 2.3.11 The Role and Advantages of Using the Tele-ECG System in Daily Medical Practice - Telemedicine Project Telecardiology has played a very important role in the first Polish activities in the field of telemedicine. Morbidity from heart diseases in Poland is very high and the statistics show that they cause more than 50% of all deaths from cardiovascular diseases. In Poland the system of transtelephonic ECG has been developed since 1996. The system provides a nation-wide 24 hours a day the transtelephonic ECG support for patients under the supervision of on-call cardiologists. It enables efficient remote monitoring of patients with some cardiac problems (arrhythmia, atrial fibrillation, chest pain) and it seems to be easy and cost-effective. Within the system the patient is being equipped in the small mobile transmitter which enables transmission of the ECG signal to the cardiologic monitor center. In the center the signal after transforming by the use of PC computer into the ECG graph can be easily interpreted by the specialist on duty. In the same time the system allows for teleconversation with the patient to collect all necessary medical data and give the patient the professional advice. After each contact the medical record of the patient is updated. There are several telesystems of cardiologic survey currently run in Poland: ‘Kardiofon’, ‘Tele-Kardio-Med’, ‘Cardiotel’ and others. ‘Kardiofon’, based in Warsaw, is the biggest one; it employs some 20 experienced cardiologists and intensive care specialist. The system has involved 2.000 individual patients and over 12.000 patients from family doctors practices. The database contains over 22.500 records sent entirely by phone. During 5
36
years of research study showed the high compliance between preliminary diagnosis made on the base of tele-ECG transmission and the final hospital diagnosis. There were distinguished 3 main groups of interventions within the ‘Kardiofon’ system: 1. Typical cardiac problems (chest pain, arrhythmia, hypertension) verified by tele-ECG records – 40% of cases. 2. Check examinations (after therapeutic interventions, patients with implanted pacemakers, on the request of family physicians) – 32% of cases. 3. Interventions on initiative of the patients with non-specific ailments (weakness, fatigue, anxiety) and with no changes in the ECG record – 28% of cases. Among cardiac problems heart rate disturbances was the most common (56% of events); the heart ischemia appeared in 26% of events, hypertension problems in 13% of events and the heart failure in 5% events. The tele-ECG system proved to be most effective in diagnosing patients with acute heart ischemia and paroxysmal atrial fibrillation (PAF). In 1998 within tele-ECG system the research program of monitoring patients with PAF was implemented. It turned out owing to medical interventions of cardiologists working in the system, in 80% cases return to the sinus rhythm was obtained and patients didn’t need further hospital treatment. The program enabled the reduction of hospitalization rate from 5% of interventions in 1998 to 2% in 2000. The tele-ECG survey showed its high usefulness in diagnosing and monitoring patients with cardiac problems. The system is available for anyone who wants to closely monitor the condition of heart, whether he already need extra support or just wants to take a more active role in his health care. It is also expected that telecardiology services can eliminate unnecessary patient’s transport to the secondary care centers, reduce hospitalization rates and associated costs. Source: Maria Bujnowska–Fedak, Violetta Tobijasiewicz, Wojciech Drewniak, Dariusz Wojciechowski, Andrzej Steciwko, PRO-ACCESS, July 2003, http://www.pro-access.org 2.3.12 Tele-ekg - CARDIAC MONITORING SYSTEM The system is developed by PRO-PLUS company. The main goal is to develop system enabling distant ECG monitoring of patients by specialist doctors. The company’s website can be found at http://www.pro-plus.pl. The example of the system and description of the software can be found at Annex XVIII of this report. The complete list of the product can be found at the company’s website.
2.3.13 Telewelfare.com
Telemedical portal offering an interactive service for diagnosis and rehabilitation of the senses responsible for communication. The diagnosis and rehabilitation systems were conceived and prepared at the Sound & Vision Engineering Department of the Technical University of Gdansk (http://www.akustyka.com) and the Institute of Physiology and Pathology of Hearing in Warsaw (http://www.ifps.org.pl/). They are international patents pending in all international patent treaty countries. The applications are located in the common portal http://www.telewelfare.com . I can hear… Programme of Care for People with Hearing Impairment in Poland. It is a multimedia system of testing patients’ hearing.
37
The system "I CAN HEAR..." is a multimedia computer programme. The role of the "I CAN HEAR..." system is mainly to test the hearing mainly in children and youth. The tests use automatic questionnaire analysis, audiometric tone test procedure and testing speech intelligibility in noise. Tinnitus Diagnostic tests and information for tinnitus and hyperacusis sufferers. The "Tinnitus" site provides diagnostic tests and information for tinnitus and hyperacusis sufferers. It is designed for children, youth and adults. "Tinnitus" has examples of sound files for comparing the sounds with those heard by tinnitus sufferers. The site gives you an opportunity to listen to examples of background sounds used in tinnitus therapy. I can speak Universal System for Testing and Rehabilitation of Speech. The "I CAN SPEAK" site presents concepts and results of computer tools applied in phoniatry and speech therapy. I can see Universal System for Diagnosing Visual Impairments. I CAN SEE is a multimedia computer programme. It is designed for testing vision in adults, children and youth. The vision testing on this website consists of automatic survey analysis, and tests that check your colour vision, binocular vision and contrast discrimination. The idea of the system is to carry out vision screening tests, mainly in children and youth. The system also presents ample information about eye care, how vision problems originate and what methods are used by ophthalmologists to diagnose and rehabilitate disorders.
2.3.14 PIONIER
The initiative of academic environment to develop backbone network in Poland. All the relevant information can be found on the website: http://www.pionier.gov.pl. International Cooperation Stimulating International Scientific Cooperation POLAND'S PARTICIPATION IN GRID PROJECTS (5TH FP)
• CrossGrid (coordinated by CYFRONET) www.crossgrid.org • Eurogrid, iGrid (ICM) www.eurogrid.org • GridLab (coordinated by PSNC) www.gridlab.org
European Grid Projects funding sum - 35 mln Euro Poland participates in projects worth 15 mln Euro Stimulating International Scientific Cooperation POLAND'S PARTICIPATION IN NETWORK PROJECTS (5th FP)
• ATRIUM (PSNC) world.alcatel.be/atrium/index.htm • LION (UMM) • 6Net (PSNC) • 6Vinit (UMM)
38
SGIgrid High Performance Computing and Visualization with the SGI Grid for Virtual Laboratory Applications The SGIgrid project aims to design and implement:
• state-of-the-art, broadband services for remote access to expensive laboratory equipment • backup computational center • remote data-visualization service
These services will be based on the national HPC infrastructure and advanced visualization. The SGIgrid project will provide users of Polish HPC centers with high, aggregated computational power, bring savings due to better utilization of software licenses and also bring other immeasurable savings since the infrastructure will be used to build a backup computational center for IMiGW which is covered by the System of Country Monitoring and Protection. Important dates Start date: Dec 1, 2002 Ending date: Oct 31, 2004 (for research and development works) Ending date: Nov 30, 2005 (for implementation) The web presentation can be found at http://www.wcss.wroc.pl/pb/sgigrid/en/index.php List of project partners can be found at: http://www.wcss.wroc.pl/pb/sgigrid/en/partners.php Extended list of contact details can be found at http://www.wcss.wroc.pl/pb/sgigrid/en/contact.php 2.3.15 Krakow Center of Telemedicine The presentation of the centre can be found on the website: http://www.telemedycyna.krakow.pl/. All the information is in Polish only. The Krakow Telemedicine Center was established in Poland in the year 2000, as a consortium of leading institutions in the field of informatics and telecommunication from the AGH University of Science and Technology and medical centers associated with Collegium Medicum at Jagiellonian University. [1] The consortium of institution and organizations representing medical and technical environment: Jagiellonian University Medical College II Dept. of Medicine Dept. of Cardiac Surgery John Paul II Hospital AGH Science and Technology University Dept. Computer Science Dept. Telecommunication Academic Computer Center Cyfronet AGH Krakow Center of Telemedicine is part of PRO-ACCESS Project. The PRO-ACCESS project was initiated in the late phase of 5th Framework Programme as supporting action. It focused on the transfer of current concepts in health telematics to countries remaining in the preaccession phase. The process of dissemination of up-to-date approaches to e-health environment development is carried out by the Krakow Center of Telemedicine and is supported by leading health telematics centres in Europe. To accelerate the dissemination activities the network of co-operating centres in CEEC was established. [2] The main objective of the centre is to development of the regional health information network in Malopolska voivodship. The aim of the centre has been
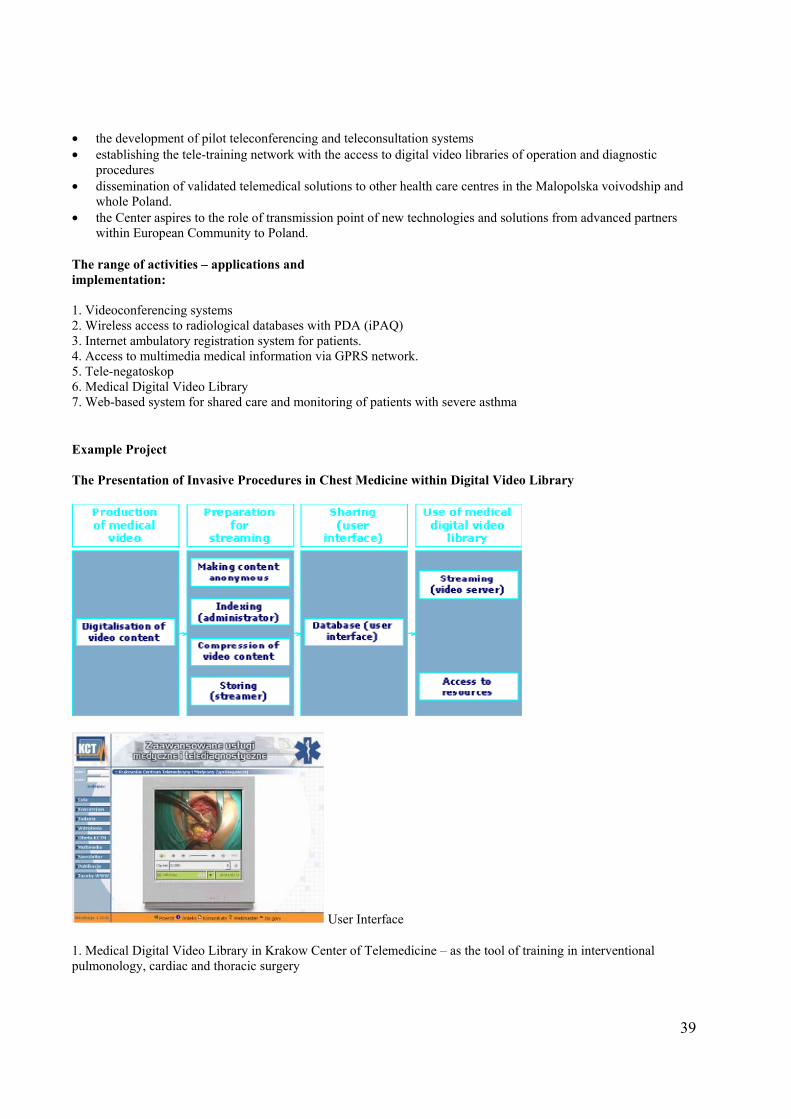
39
• the development of pilot teleconferencing and teleconsultation systems • establishing the tele-training network with the access to digital video libraries of operation and diagnostic
procedures • dissemination of validated telemedical solutions to other health care centres in the Malopolska voivodship and
whole Poland. • the Center aspires to the role of transmission point of new technologies and solutions from advanced partners
within European Community to Poland. The range of activities – applications and implementation: 1. Videoconferencing systems 2. Wireless access to radiological databases with PDA (iPAQ) 3. Internet ambulatory registration system for patients. 4. Access to multimedia medical information via GPRS network. 5. Tele-negatoskop 6. Medical Digital Video Library 7. Web-based system for shared care and monitoring of patients with severe asthma Example Project The Presentation of Invasive Procedures in Chest Medicine within Digital Video Library
User Interface 1. Medical Digital Video Library in Krakow Center of Telemedicine – as the tool of training in interventional pulmonology, cardiac and thoracic surgery
40
2. Access to digital video resources – increased motivation for peripheral centres to join teleconsultation scenarios. 3. The double use of established links: - For teleconsultation services - Access to MDVL Source: http://www.americantelemed.org/news/2003_presentations/M3b2.Duplaga.htm Example Project The Severe Asthma Patient Monitoring System - Joint initiative of Polish Ministry and National Scientific Committee, scheduled for 2002- 2003 - The network of reference centres - System of monitoring for patients - Patients access to the system: PC with Internet connection, mobile phones - Shared care (reference centre, local hospital, primary care shared care physician, other health professionals) - Disease course trends tracing - Alarm messages sent as emails and SMS to health professionals Objectives - Diminishing the rates of hospitalizations and emergency calls - Improving quality of life of patients - Harmonized co-operation between health care professionals - Lowering expenditures for care of this group of asthma patients [3] Conferences In June 2003, the 1st Conference "E-Health in Common Europe" was held in Krakow as part of the PRO-ACCESS project. The Organizing Committee is proceeding with preparations for the 2nd edition of this conference, which will take place on March 11-12, 2004. The details of the conference can be found at: http://www.pro-access.org/conference2/. Source: [1] Krakow center of telemedicine – developing the platform for regional telemedical networks, Krzystof Zielinski, E-he@lth in Common Europe, PRO-ACCESS 2003;
[2] The need for transfer of up-to-date e-health concepts and technologies to Central and Eastern Europe countries, Mariusz Duplaga, E-He@lth in Common Europe, PRO-ACCESS 2003
[3] http://www.univ-lille2.fr/cerim/colloques/e-sante/pdf/MDuplaga_Lille_24012002.pdf
2.3.16 PRO-ACCESS The following are the abstracts from PRO-ACCESS project papers. The details can be found at http://www.pro-access.org. Home Tele-Monitoring of Arterial Hypertension in Family Medicine Arterial hypertension (AH) and all its sequels are one of the most serious threats to human health and life. AH affects about 41% of the middle-aged population in Poland. Only 6% of people with AH have their disease adequately controlled, 40% just know about it, 27% know without taking any therapeutics, and 27% are treated ineffectively. Family doctors have a crucial role to play in the early detection of AH in their patients. They should also start treatment as early as possible and recommend the necessary lifestyle changes.
41
Home telecare exemplifies the application of telemedicine in primary care/family practice, including remote diagnosis and treatment, compliance monitoring, and tele-monitoring of vital signs. The experience gained from different trials and studies shows that ambulatory blood pressure (BP) monitoring and self BP measurements at home share similar advantages and can be successfully applied to the management of AH. Few randomized-controlled trials, however, have been carried out to determine the efficacy of telemedicine in reducing BP. We identified several recent studies on home tele-monitoring of BP and AH to present the specific telemedicine systems used for this approach, with its advantages and disadvantages. The aim of our project on Home tele-monitoring of hypertension in family medicine is the assessment of the diagnostic and tele-monitoring value of home BP measurement (in the newly diagnosed patients with AH). This randomized-controlled trial will be carried out in three family medicine settings. The patients will be recruited by their doctors and divided into two groups: (1) conventionally managed in family practice, (2) making daily BP measurements in their homes and transferring the results to the practice by phone. Office BP measurements will be compared with those taken in the patient’s home. The assessment will also include: patient compliance, quality of life, and cost-effectiveness of this approach. [1] A Telemedicine Support for Diabetes Management – The Pilot Project Effective control of diabetes is known to delay or prevent the progress of this disease. Despite enormous efforts to change the delivery of diabetes care, the outcome has not been satisfactory. However, telecommunication can improve the quality of diabetes care by altering the caring environment and care delivery process. In telecare applications the role of the patients become central, since they are actively involved in the process of managing care and treatments and they are responsible for collecting some measurements and related information. The aim of this project is to develop, demonstrate and evaluate a telemedicine system for diabetic patients’ management. The system is designed to improve the daily care and intensive management of diabetic patients through telemonitoring and telecare services. The paper presents architecture of the system, the technical solutions adopted and the methodologies on which it is based. The system is composed of two modules — a Patient Unit and a Medical Unit connected by the telecommunication network. The Patient Unit and the Medical Unit are able to communicate both over the Internet and the public switched telephone network. Using the system the patient is allowed to automatically down load his monitoring data from the blood glucose-monitoring device and to send them to the personal computer of his family physician. Both units, in an integrated approach, offer tools to doctors and patients for data collection, data analysis and decision support and enable them to send massages and/or therapeutic advice to the patients. The system will be evaluated for usability, telemedical protocols, metabolic controls and quality of life. This pilot study demonstrates the feasibility of the telediabetology supportive system in daily routine use and its potential benefits for diabetes care: improving the availability of information necessary in treatment decisions, showing the better, more precise metabolic control of patients. The study offers new physician-patient communication tools. It helps patients with management in the daily care of diabetes and increases patients’ independence without decreasing the essential continual support and supervision from the doctor. Moreover this telematic system seems to be not expensive and simple in use. [2] TEKOMED – Mobile Teleconsultation System In clinical practice essential quick consultation of patient's data with reference centre could be necessary to undertake the decision regarding further diagnostic or treatment. Simultaneously, it could be useful to enable medical consultation by the local expert who is actually outside his medical center. Such a system was created in the National Institute of Cardiology. It makes possible to access the clinical data – ECG, Holter ECG and coronary angiography. In the short time also the Echo study could be presented by the system. The access to the TEKOMED system is via Internet. It was also tested that sufficiently effective is also GPRS link by the mobile phone. In this way TEKOMED system enables to view all of the stored medical data in every place and any time. It is possible to be installed in any hospital over the Poland and other countries. TEKOMED gives the unique chance of the professional consultation for the patients’ medical data at the National Institute of Cardiology. TEKOMED makes possible the
42
transfer of requested clinical data by cellular phone. The transmission of the one sequence of the coronary angiography lasts about 1 minute. In the future, the development of the new cellular phone technology based on UMTS will shorten the transfer to maximum 15 seconds. [3] You can see the presentation of TEKOMED at http://box.ikard.waw.pl/tekomed/. TELEDICOM — Environment for Collaborative Medical Consultations The environment called TeleDICOM supporting remote collaborative consultations in medicine. The notion of collaborative work although well known in distributed systems area is unfortunately still hardly present in medical applications. Being able to process only local data or at most cooperate with databases they lack interactivity with other users. The functionality of TeleDICOM will be presented. The main usage scenario will allow a doctor from a local hospital to consult patient examinations in form of various digital documents with specialists from a clinic hospital. Supplemented with videoconferencing tools the whole environment will significantly improve access to highly qualified medical professionals for peripheral medical centres. The application seems to be very helpful also in the area of teaching medicine students which could either passively participate in real consultations or take active part in teaching sessions arranged specially for them. The system will use mainly DICOM images, which have high diagnostic quality and are generated by most modern medical equipment. The overall architecture of the system will be presented. The system is being developed using state-of-the-art distributed systems technologies. The data security, efficiency of network communication and userfriendliness of the application have been kept in mind. The idea of the application has been one of the laureates of a project “Internet w szkołach” organized by Polish President. TeleDICOM is being developed in Institute of Computer Science of AGH, which is an active member of Krakow Center for Telemedicine and Preventive Medicine. [4] The complete report can be found at: http://www.pro-access.org/ConfMan/SUBMISSIONS/ 93-Czekierda.doc 2.3.17 The University Hospital in Krakow The University Hospital in Krakow is one of the biggest hospitals in Poland, with over 200 years of history of operation. The Hospital consists of 32 Departments and 60 Outpatient Clinics covering practically all medical specialties. There are above 42 000 hospital's admissions every year and about 300 000 medical consultations at different Departments. The Hospital serves as a referral center for population of about 6 million from Southeast part of Poland. Number of hospital's employees is equal to 4 200 persons. The Hospital staff is involved not only into regular medical activities, but also into research, education and different medical projects. An international cooperation plays an important role at the Hospital's strategy of development. The University Hospital is considered as an institution, which effectively utilizes modern medical technologies and is well equipped with modern, sophisticated medical equipment for diagnosis - such as 3 CT's, MRI, Gamma Camera, CathLab's - and treatment. Also IT technologies play an important role at the Hospital's operation. Additionally, the Hospital's staff is developing different IT projects - including telemedicine - which would make the medical and administrative data flow and data processing easier. The web presentation can be found at http://www.su.krakow.pl/english/index.html. Source: [1] Andrzej Staniszewski and Jadwiga Staniszewska, PRO-ACCESS, July 2003, http://www.pro-access.org;
[2] Maria Bujnowska-Fedak, Edward Puchała, Andrzej Steciwko, PRO-ACCESS, July 2003, http://www.pro-access.org; [3] Rafał Baranowski, Adam Koprowski, PRO-ACCESS, July 2003, http://www.pro-access.org
[4] Jacek Cala, Łukasz Czekierda, PRO-ACCESS, July 2003, http://www.pro-access.org
43
2.3.18 Telemed TELEMED Ltd. has been formed to perform research, system development and integration, and services involving interactive videoconferencing systems, telecommunications systems, audio and video processing, information systems, and Internet, with the main focus on the following applications: • telemedicine • distance education and training • distance work and control • distance promotion-information-marketing
We also offer technical, medical, and scientific consulting services. Major activities of TELEMED Ltd. are directed towards the development and support of telemedicine. We organize videoconferencing and Internet based sessions for telemedicine both within Poland, and between Poland and North America. On the request of the medical and academic institutions as well as of privately owned medical clinics and federally sponsored hospitals, we provide and secure all the necessary information technologies, audio and video coders, diagnostic devices, and secure and reliable communications systems in order to support the medical care at a distance. We assure an excellent voice and video quality, and secure, reliable two-way communications between various centers in Poland, USA, and Canada. Two ways, interactive audiovisual sessions enable the medical doctors and experts on both sides, not only for joint professional meetings, education courses, seminars, conferences and scientific symposia, but also for medical consultations, exchange of opinions, joint decision making in the critical situations, and assisting "on-line" in the difficult medical procedures and operations.
2.3.19 E-rejestracja
eRejestracja – online patient registration system eRejestracja is a sample of online patient registration system developed by private company in Poland. The company website can be found at http://e-rejestracja.pl/. eRejestracja is a web-based service enabling patients to register online for medical check-ups or other medical services. The system is addressed to all kinds of medical institutions, both public and private. So far, online appointments in Poland have only been available to individual clinics or hospitals, usually private, via those institutions' websites. At our website (www.erejestracja.pl) patients have at their disposal various search engines, allowing users to narrow down their search using multiple criteria, e.g. type of medical service or location (voivodship, town, district, etc). Once the patients have found the service of their choice (e.g. a dentist located next to their office), they can make an online appointment. eRejestracja may be integrated with internal systems used in hospitals or clinics. Currently we are working on the implementation of such integrated systems in major medical institutions. Our future projects include appointments through sms (gsm-based short messaging system), a service which we shall introduce as one of the first in the world. eRejestracja is also developing a system allowing for secure data transfer between co-operating medical institutions. Our project is in accordance with the principles of the Electronic Health Record, as well as binding regulations on personal data protection (i.e. our integration solutions are founded on XML-based data exchange). Our project is in accordance with the requirements of the Wrota Polski (Gate of Poland), e-government policy. Source: Marcin Straburzyński MD, director of E-rejestracja
44
2.3.20 List of Contacts Organization Name Contact details National contact point
PYTKO, Anna (Ms.) LifeSciHealth NCP
URL: http://www.npk.gov.pl Tel: +48-22-8262502 Email: [email protected]
SIBIS national contact
ASM - Centrum Badan i Analiz Rynku Sp.z.o.o. Elzbieta Syrda
Email: [email protected] Tel ++48.24.3557715
SIBIS national contact
ASM - Centrum Badan i Analiz Rynku Sp.z.o.o. Maria Goreczna
Email: [email protected] Tel ++48.24.3557715
Ministry of Science and Informatics
Ms. Elzbieta Piechna Email: [email protected]
Krakow Center of Telemedicine
Mariusz Duplaga, MD, PhD Jagiellonian University Medical College
Email: [email protected]
The University Hospital in Krakow
Witold Poniklo Modernization and development of the hospital
Tel: +48(012)4247073 [email protected]
TELEMED Phone: (+48 22) 872-16-44 Fax: (+48 22) 872-32-74 e-mail: [email protected]
45
2.4 Slovenia 2.4.1 Government’s Action Plans In Slovenia, the commitment to the development of the Information Society was clearly expressed in January 2001 when the Ministry for Information Society was established. The ministry operates in close co-operation with the Government Office for Informatics and with other ministries and government offices. On a general policy level, the ministry contributed to the creation of the Slovene National Development Plan for the period 2001-2006. In spring 2002, the ministry prepared the National Programme Republic of Slovenia in Information Society as a policy document for Public Administration, Economy and Civil Society. Source: eEurope+ Progress Report, Ljubjana 3-4.5.2002, http://www.kbn.gov.pl/cele/ljubljana/index.html
2.4.2 Ministry of Information The website can be found at http://www2.gov.si/mid/mideng.nsf. The Ministry of Information Society holds the political responsibility for the information society, including e-government. However, at an operational level, the Government Centre for Informatics (GCI) is the body in charge of developing the country’s e-government infrastructure, and to support, control and coordinate government departments’ ICT projects. Slovenian eGovernment portal The portal has been launch in March 2001. It provides access to a range of e-services and government information for citizens, businesses and civil servants. The web site of the portal can be found at http://e-uprava.gov.si/e-uprava/en/portal.euprava and http://e-gov.gov.si/e-uprava/english/index.jsp (English version). Government Centre for Informatics The website can be found at http://www.gov.si/cvi/eng/ Action Plan eGovernment up to 2004 Health is one of 12 e-services for citizens - Services connected with health service (interactive counseling on available services in hospitals and interactive ordering for medical treatment). And also one of the 15 areas of Action Plan. Area Subareas & E-Services Actor Deadline Project G2C Health
Waiting periods MH 2004 Waiting Periods
Organization of working hours Organization of Working Hours
Development of a management system for health care
MH 2004 e-SPP
Definition of PIN immediately after birth in a maternity hospital
MH, IPH, GCI, MIA
Definition of PIN Immediately after Birth in a Maternity Hospital
46
G2B Health
Development of a management system for health care
MH 2004 e-SPP
Source: http://e-gov.gov.si/e-uprava/english/docs/akcijski_nacrt_e-uprave_do_leta_2004_1_3.doc
2.4.3 Ministry of Health The website of the Ministry can be found at http://www2.gov.si/mz/mz-splet.nsf. Ministry of Health’s National Health Sector Management Project The main project goal is to secure long-term stability of the system and to found its managing on provable and verifiable data focused on the patient. In Phase I, by the end of 2003, we aim to establish conditions required for the national scale implementation, which is the subject of Phase II, to follow up to 2006, provided that the Phase I outcome is successful. The budget for the project is 13,8 M EURO in the period 2001-2003 (phase 1) and 16,2 M EURO in 2004-2006 (phase 2). Complete description of the projects with the costs, names of the people involved can be found at http://www2.gov.si/mz/hsmp/hsmpeng.nsf. 2.4.4. Ministry of Education, Science and Sport The website of the Ministry can be found at http://www.mszs.si/eng/. The extensive report was prepared by the Ministry and can be found in Annex XVIX of the report. 2.4.5 List of Other National Information Society Related Websites Government (http://www.gov.si/). Society Informatika (http://www.drustvo-informatika.si): Translations of key information society documents; European driving license (ECDL) contact point 2.4.6 Institute of Public Health The web presentation of the Institute can be found at http://www.gov.si/ivz. The institute performs Health Research as one of the fields of work – collecting, organizing and analyzing the health-related data.
2.4.7 Institute of Biomedical Informatics The website of the Institute can be found at http://www.mf.uni-lj.si/ibmi-english/raziskovanje/index.html. Projects 1. Informatics Intelligent information storage and retrieval of Slovene and English medical documents on Internet (Subproject of INCO-Copernicus Project: 960154, CRII)
47
Digital library of Slovenian medical documents Evaluation of research in the field of biomedicine in Slovenia 2. Statistics Theoretical (project: Regression Models in Survival Analysis) Applied (IAEA project: Pain Relief In-Patients with Bone Metastases)
2.4.8 Slovene Medical Informatics Association The website of the Association can be found at http://www.simia.org/. The Association is sponsored by: • ZZZS - The Institute of Health Insurance of Slovenia (http://www.zzzs.si) • Nova Vizia d.o.o. Zalec – Health Informatics company (http://www.vizija.si/) • Infonet d.o.o. Kranj – Health Informatics company (http://www.infonet.si/) Projects PROREC.SI Electronic Health Record (EHR) For details see also Annex XX of the report.
2.4.9 SIZN - Nursing Informatics Interest Group The website of the Group can be found at http://www.kclj.si/sizn/. The work program includes: • Collaboration In International And National Projects • Informatics Meetings Provide • Advising And Issuing Expert Opinions • Collaboration By Related International Associations • Collaboration On Support At Base Of Research And Applicative Projects • Publishing • Annual Plan And Work Report The complete work program of the Group can be found at http://www.kclj.si/sizn/work_program.htm.
2.4.10 Telemedicine in Slovenia report Extensive report written by Bostjan Bercic from INFONET can be found at Annex XX of the report. The report contains information about: • Historical review and major milestones in IST development and implementation 1993 – 2003 • Review of the National and EU RTD activities and implementations • Barriers to successful implementation of telemedicine • Telemedicine technologies used by hospitals/doctors • PROREC Slovenia • Status of HER
48
• Expenditure of IT in Slovene hospitals • The most important eHealth initiatives/pilots in Slovenia 2.4.11 Telemedicine Projects
2.4.11.1 Transtelephonic transmission of ECG The transtelephonic transmission of electrocardiograms (ECGs) was introduced in Slovenia in 1996 and has been used regularly since September 1997 by health institutions and patients with cardiovascular diseases. Portable 12-channel ECG equipment weighing less than 200 g is generally used. The diagnostic centre is located in the intensive-care unit at the University Medical Center Ljubljana. In the first 12 months of regular operation we received 463 calls, 213 of which were diagnostic. The most common reasons for calling were: ischaemic chest pain, atypical chest pain, palpitations and dyspnoea. The most common diagnoses made on the basis of history and the ECG were: acute myocardial infarction, angina pectoris, paroxysmal tachycardias and atypical chest pain. In 40% of cases the cardiologist's advice sufficed; 38% of patients were referred to the emergency room, 29% immediately and 9% only if a suggested therapy did not prove successful; and in 21% of cases new medication or a change of dosage of current medication was suggested. Transtelephonic ECG transmission enables direct communication between general practitioner or patient and cardiologist. With its use, time from onset of symptoms to initiation of treatment is shortened, which reduces disability and mortality due to cardiovascular diseases and improves cost-benefit. Author. Source: Journal of telemedicine and telecare {J-Telemed-Telecare} 2000, VOL: 6 (4), P: 205-8, ISSN: 1357-633X., http://www.sgmi-ssim.ch/medline/IM_00041.htm
2.4.11.2 Second Opinion
The complete information can be found at http://www.maat.si/so.htm. Second Opinion Slovenia operates under the professional guidance and supervision of the largest health care center in Slovenia, the Clinical Center in Ljubljana. The project is called Second Opinion and with it, a second opinion of top specialists is attainable to patients from all over the world. The Project uses the latest achievements of telemedicine.
2.4.11.3 Health Insurance Card Project – Health Insurance Institute
The full details of the Health Card Project are available at http://www.zzzs.si/kzz/ang/ic_indx2.htm. You can also see Annexes XX and XXI of this report for more details. In the first phase of the Slovenian project, the Institute is introducing a card serving administrative purposes (implementation of rights derived from compulsory and voluntary health insurance), supporting the procedures regarding the selection of a personal physician, and carrying an elementary form digital prescription. The health insurance card is the only document applicable in the implementation of the compulsory and voluntary health insurance rights in Slovenia. A person is to present the card when visiting at the doctor's and at all other occasions of implementing the rights deriving from health insurance.
49
2.4.11.4 PRIMACOM
In 1997 the project PRIMACOM1 was launched, within INCO COPERNICUS Programme. The aim of the project was to supply health care professionals with systems and infrastructure for enhancement of communication between primary and secondary care – so-called Regional Health Care Networks or Community Health Information Networks. The main task of the project was to establish and evaluate pilots in two Eastern European countries, Slovenia and Hungary. The pilots upgraded the infrastructure and established direct communication between hospitals and Primary Care General Practitioners in Primary Health Care Centres. In the second phase of the project the software was adjusted to use European communication standards (EDIFACT) and electronic mailboxes were established (source: HSMP – Project Implementation Plan). Source: http://www2.gov.si/mz/hsmp/hsmpeng.nsf/V/KC3155D1785DE23AFC1256B49002B4B9A/$file/Annex-03_99-11-09.doc Implementation of PRIMACOM The following is the extract from e-mail correspondence from Mr. Bostjan Bercic. In Slovenia the system (i.e. the network and tools for message exchange) was implemented (like it was planned and like budget allowed) only in three pilot sites in a small region of Gorenjska. The system was being used in daily work for a few months and discontinued after that. One problem was the small number of pilot sites (one hospital and only about 6-8 GPs involved), as it was very inconvenient for the hospital to have 2 systems: to send electronic discharge letters to only a few GPs, and for the majority of others doing it still manually, e.g. on paper. In other words, the system was not practical, because it was not implemented generally, i.e. for all GPs and hospitals in the region. The other problem was the legislation. There was no official approval for electronic documents (e.g. signature) at that time. Now, when the digital signature infrastructure is in place and officially approved for the whole country, we have set a new project under the umbrella of PROREC Slovenia, using all the knowledge and experience from PRIMACOM, as well as the same principles. Only the technology is more modern, for example: using Internet technologies instead of X.400, XML instead of EDIFACT, etc. In comparison with PRIMACOM there are also many more technology providers involved as before. 2.4.11.5 Security and Protection of the Data in the Slovenian Government including at the Health Care Sector Project supported by Government of the Republic of Slovenia – Center for Informatics Data security has been increasingly dealt with at various professional meetings and congress on informatics in Slovenia and worldwide. Recently, a number of specialization workshops have been held with the aim of setting up an effective system of data security. In the field of data security the following points need to be emphasized:
(1) Data security is an integral part of planning, creating and managing the health care information systems at all levels; also both in public health institutions and in private practice.
(2) In addition to strictly medical information, a broad spectrum of personal, business and other databases, which in the modern information society are closely interlinked, also need special protection.
(3) Current information systems make use of various media, including classical as well as computer-assisted ones. Since in Slovenia, medical information systems are still in the phase of development, a comprehensive and legally regulated system of security should be established in order to prevent possible errors, abuse and organization inconsistencies.
(4) All those concerned with the acquisition and protection of medical data, i.e. both clerical, nursing and doctor staff, should be given adequate education, either through regular or periodical
50
trainingcourses,but first of all, they should be encouraged to apply the principles of data security to their everyday work.
The purpose of this project is to stress some legal and ethical aspects of data protection, as well as the importance of safe guarding the information privacy of each individual by taking into account the requirements of the profession and the legal system and international standards and recommendations, especially WHO and European Communities. The Ministry of Health of the Republic of Slovenia and Institute of Public Health of the Republic of Slovenia has prepared a draft of the new Health Care Record law that is now in parliamentary procedure, which deals with the content and forms as a legally valid documents, regardless of electronic media, it also validates the electronic signature and the extent of documents prescribed in health care. A group of experts in the field of Health Informatics and experts from all Health Care levels have prepared a document: »Principles and Guidelines for the Data Privacy and Security of Health Information Systems«. The proposed project has the potential to supply the necessary platforms for the Health Sector Management Project. Source: http://www2.gov.si/mz/hsmp/hsmpeng.nsf/V/KC3155D1785DE23AFC1256B49002B4B9A/$file/Annex-03_99-11-09.doc 2.4.12 InfoNet – Healthcare Information Systems Company The complete presentation of the company with the product range can be found at http://www.infonet.si. INFONET was founded in 1991 as an information engineering company. The main thrust of the company is the integration of our work, which is building and launching information systems in the health care and pharmaceutical sectors. The development and implementation covers three basic fields:
• hospital information systems • pharmacy information systems • information systems for Primary Health Care and GPs
You can also see more details in Annex XXII of this report. Activities in Information Environment for Healthcare a) Institute for Health Protection Ljubljana - at http://www.gov.si/ivz • Preparation Of Proposal For Uniform Definitions For The Field Of Hospital And Non-Hospital Activities In the working group that was appointed by the Minister of Health and is managed by Dr. Tit Albreht we prepare the uniform definitions for the basic conceptions which are used in the accounting/reimbursement system for obligatory and for additional voluntary health insurance, as well as in healthcare statistics. • Health Statistics We co-operate in work groups for optimum network performance, data collection, processing and transfer in inpatient and outpatient statistics. We were initiators of its updating and we are satisfied that both fields have been facing vital changes in the year 1997. • Data Collection, Aggregation And Analysis At Sick-Leave We have developed the software used by regional and republic Institute for Health Protection for collection, aggregation and analysis of data of sick leave. • Perinatal Information System On the basis of requirements, connected with modernisation of in-patient statistics, we developed the software application PerIS, which is used in Slovenian hospitals as information support to perinatal information system. The software is developed on Windows platform and is one of the most contemporary application programs in the Slovenian health care. • Standardisation And Classification Of Health Care Information System We have co-operated in PROJECT GROUP for definition of information needs on national level - Ministry of Health Care and Institute for Health Protection. In the continuation of the project we were included in: sub-project for definition of data protection starting points sub-project for minimum data collection verification
51
b) Institute for Health Insurance of Slovenia (IHIS) – at http://www.zzzs.si Health Insurance Card We were involved in two project groups for the project Health Insurance Card that started at the end of 1995 and is now in the phase of finalisation. We co-operated in all the phases of the project execution as the largest software house providing support to the healthcare providers information systems:
• In the definition of required changes and the completion of software applications for healthcare providers. • In the definition of requirements for electronic data interchange between healthcare providers and IHIS. • During the pilot project in Posavje region we worked out all the required and needed program application
changes, as well as made the whole implementation in General hospital and in Pharmacy of Brezice. The pilot project was a success!
• In the phase of national wide deployment we adopted all the remaining applications, which now allow for and confirm to all the business rules and logistics of the Health insurance card system. We have trained over 5000 users (i.e. healthcare actors) and set up over 1800 card readers all over Slovenia.
Electronic Data Interchange On our initiative and together with IHIS we started a joint project in 1993, in which we involved ourselves already in the very phase of requirements' definition. Additionally, we initiated a pilot project with the Railway Health Center Ljubljana. Successfully executed pilot projects accelerated the introduction of Electronic Data Interchange (EDI) among our business partners (e.g. healthcare providers) and IHIS. Presently, EDI for reimbursement purposes is being 100% used in all public healthcare institutions, as well as in two thirds of private ones. Elaboration of Software for Accounting and Invoicing Ihis We were the selected software providers for IHIS at the beginning of 1993. We prepared all installation procedures, developed all the required documentation and trained the users for the first software for accounting and invoicing IHIS. Around 3000 medical workers in Slovenia got introduced to the information technology, by using the software applications, for the first time. c) Institute Josef Stefan, Ljubljana - http://www.ijs.si/ijs.html Lab for Artificial Intelligence Cooperation at the execution of the EXPERT SYSTEMS project, supporting the THERAPEUTIC ACTIVITIES IN HEALTH CARE. Within the frame of this project we have developed software product PTAH, which is an aid to doctors for preventing and for monitoring the phenomenon of hospital infect, as well as for decision making in writing prescriptions for appropriate therapy. The project was co-financed by the Ministry of Science and Technology. International Projects in Medical Informatics a) PRIMACOM – http://www.primacom.dk Cooperation in the project PRIMACOM, a part of EU project CoCo-INCO COPERNICUS, which is a strategic project in the Telematics Application for Health program (HC1008). In a public-private partnership, two regions in Hungary and Slovenia have established Regional Health Care Network for exchange of routine messages between healthcare professionals. b) Information System for Treating the Patient at his Home The project was being run together with Faculty of Organisational Sciences Kranj and Faculty for medical personnel Ljubljana. The software for supporting the work of home nursing was included into Information system of Primary Healthcare and was developed by considering all international standards in this field, which arise within the project TELENURSE. c) Hansa East
52
The HANSA projects aim to promote the new technology and its standardised approaches through demonstrations and dissemination activities. This project demonstrates that employment of a middleware based open architecture yields reduction of working effort needed for interworking of existing systems capable to share ands exchange data. Meanwhile this architecture has already been adopted as a European standard, i.e. CEN TC 251 ENV 12967-1 ``Healthcare Information Systems Architecture (HISA – Standard) The overall objectives of HANSA EAST project were to transfer these distributed software technologies for open health, healthcare, hospital, and insurance systems and adopted European standards to the CEE/NIS countries: to the Health IT Authorities, and to Health IT providers for business development in order to create a local software industry for the health sector. HANSA EAST consisted of three different countries, complemented by a Concerted Action directed at the other countries, i.e. Albania, Bulgaria, Czech Republic, Estonia, Latvia, Lithuania, Slovak Republic and Slovenia. d) RETRANSPLANT (Regional and International Integrated Telemedicine Network for Medical Assistance in End Stage Diseases and Organ Transplant - HC-4028) RETRANSPLANT will implement a regional network to link different national organ transplant systems, to give on-line access to European transplant coordinators, donor centers, diagnostic specialists, to increase Europe-wide the effectiveness of organ transplant services. RETRANSPLANT is stimulating partnerships between those who are involved in research, development and implementation of information technologies, and user organizations of the different tools of the Health Telematics. RETRANSPLANT consortium believes that the health care of tomorrow needs to go to patients where they live, instead of patients going to the health care systems. Such a system will save money and lives. e) Leonardo da Vinci – PROPRACTITION The main and novel component of PROPRACTITION system is a new distributed architecture, comprised by a collaborative toolkit to add audio conferencing, telepointing, window sharing, user's co-ordination and application synchronisation facilities, either to existing or new medical diagnosis applications. In comparison with existing products, mainly based on centralised architectures, our distributed toolkit is specially designed for telemedicine applications: to allow different levels of sharing between participants, to improve user feedback in highly interactive user interfaces, and to optimise the required communication bandwidth in order to implement a telemedicine application on almost any telecommunication network. This system will be applied to build a co-operative medical education application, in which two doctors, located in different hospitals, need to achieve a co-operative diagnosis on cardio-vascular diseases. f) WIDENET WIDENET's mission is to promote the adoption and extended use of Standardised Electronic Health Care Records and the required infrastructure. The project aims to provide a sound and effective instrument for promoting and attaining such requirements. The plan is to form a European Institute for Healthcare Records and Management that will represent the permanent network of National Centres and provide quality and affordable added value services to the European market. Doing this fulfils calls from the European Parliament, the Council of Ministers, the Commission, and the Council of Europe. There is also an important goal dealing with the collaboration with strategic bodies (CEN, ISO, EC IST programme, EHTEL, WHO and national/international initiatives) to ensure that the ``European convergence" is appropriately conducted according to their guidance and standards. g) PHARE (SL-9803.02.0001.03) - Further Alignment of Slovene Statistical Methodology with EC Requirements The overall objective of the project is the creation of a methodological, technical and operational basis and the achievement of comprehensive competencies (on the side of IDP, statisticians and users) which will guarantee the sustainability of the project outcome from all the sub-components and the further re-usability of the obtained results within the statistical production and dissemination process.
53
2.4.13 Nova Vizia (New Vision) The company’s website can be found at http://www.nova.vizija.si/images/English/mi/default.htm. Health Informatics Products SOVA Computer aided medical information systems ZUBSTAT Outpatient healthcare statistics ICD International code of diseases EMERGENCY Data processing in emergency medical activity PP-NMP Learning and testing First Aid and Emergency Rescue SIMKPR Cardiopulmonary Resuscitation Simulator HEALTHCARE INSURRANCE CARD The HIC contractor for the pilot project of Posavje region 2.4.14 List of Contacts Organization Name Contact details Ministry of Education, Science and Sport
TUSAR, Livija (Dr) National contact Point
Tel: +386-1-4784681 Email: [email protected]
Government of the Republic of Slovenia Center for Informatics
Telephone: +386 (0)1 478 8600
Center for Health and health Research
Tit Albreht Tel: +38612441406 Email: [email protected]
Slovene Medical Informatics Association
SIZN – Nursing Informatics Interest Group
Vesna Prijatelj Email : [email protected]
IN Center for Intensive Internal Medicine, University Medical Center Ljubljana, Slovenia
AU Gorjup-V, Jazbec-A, Gersak-B. Transtelephonic transmission of ECG
Email: [email protected].
Second Opinion tel.: +386 1 437 74 64 Email: [email protected]
ZZZS (Health insurance card institute)
Phone: +386 13077324
Primacom Miran Rems General Hospital Jesenice
Phone: +386 64 868 0 Email: [email protected]
Primacom Janko Kersnik Family Doctors Association of Kranjska Gora
Phone: +386 64 881 426 Email: [email protected]
Primacom, INFONET Bostjan Bercic Phone: +386 64 331 131 Email: [email protected]
InfoNet Mrs. Smiljana V. Slavec General manager
Email: [email protected] Tel. +386 42 800 900
Nova Vizia Jozica Leskovsek [email protected] +386 (0)3 712 18 00
54
Annex I Telemedicine Implementation in CEE region – Brief Overview Country Name
Cyprus Legislation
Plan to introduce an effective National health Insurance Scheme.
Telemedicine implementation
RTD funded projects European funded: Ambulance – http://ambulance.cpr.it Emergency-112 http://www.biomed.ntua.gr/emergency112 HEALTHNET http://www.cs.ucy.ac.cy/healthnet MEDICATE http://www.medicate-online.org TELEPLAN and VIRTUOSO– teleconsultation National funded: EROS – evaluation of risk of stroke by telemedicine TELEGYN – diagnostic telepathology network DITIS – home healthcare of cancer patients Implemented services: The Cyprus Institute of Neurology and Genetics, the Paraskevaidion Surgery and Kidney Transplant Center, the Bank of Cyprus Oncology Center, the Makarios Hospital, and the Cyprus Society of Medical Informatics carry out these activities: In August 1998, a new video conferencing system was installed at the Paraskevaidion Surgical and Kidney Transplant Center in Cyprus. The system allows Orthopedic doctors in Cyprus to efficiently communicate with their assess difficult cases of children with orthopedic problems examined in Cyprus. The Clinic of Oncology Radiation Therapy and Radiation Diagnostics of the Bank of Cyprus Oncology Center is participating in the EU projects TELEPLAN and VIRTUOSO Bank of Cyprus Oncology Center: http://www.bococ.org.cy/
Country Name
Czech Republic Legislation
Laws of: - personal data security - electronic signature - health documentation, national health information system, and management of national health registers
Telemedicine implementation
www.telemedicina.cz – information platform for telecare projects National Research programs www.gacr.cz , www.ikem.cz , www.euromise.cz , www.cls.cz , www.cski.cz , www.crs.cz , www.ksrzis.cz Ongoing Initiatives: At present time the pilot project called Ophthalmologic Register is carried out. The project is equipped with the image database system for storage of eye ground images of patients with danger of eyesight or life loss. Web technology is used for data transmission through Internet with connection not only to the database in ophthalmic out-patient departments but also to highly specialized workstations with image analysis, it is used also for diagnostic evaluation and for setting of the operating term in case of need. In the metropolitan network of the city Brno the image archive system PACS, which enables to evaluate findings from 8 healthy instruments (e.g. CT) placed in 5 big hospitals is used. The system is very operable with the central database placed in the Masaryk Oncological Institute. EHTEL Virtual Demonstrator: Municipal Hospital Litomerice, Czech Republic In this demonstration site is implemented health card system bounded with the Hospital Information System (HIS). http://www.ehtel.org/SHWebClass.ASP?WCI=ShowDoc&DocID=1221&LangID=1
Country Name
55
Hungary Legislation
Projects of: - document management system - digital map database - government portal - electronic signature
Telemedicine implementation
There has been a fax-ECG communication system in the country operating as a pilot project for several years and transtelephonic ECG (“beeper”) placed by the patient can also be found. Small teleradiology R&D projects were done in the area of tele-traumatology, and tele-consultation through web is available in limited areas. A significant financing reform initiative, resembling HMOs were supported with electronic consulting in the Veresegyhaza Health Mission Project. Further info: www.eum.hu – ministry of health www.oep.hu – national health insurance www.gyogyinfok.hu – healthcare info www.medinfo.hu – community health information portal www.vitalitas.hu – health portal www.hazipatika.hu – health portal www.informed.hu - InforMed is a commercial Hungarian language Health & Medicine site www.mok.hu Medical chamber www.antszfov.hu National Public Health and Medical Offices Service Cooperation on Bepro, Gaster 2, ITNict, Prorec-Hungary, Retransplant, Samta
Country Name
Poland Legislation
Electronic signature
Telemedicine implementation
www.npk.gov.pl/prog_tem_2 The educational services using Internet are accessible in several sites, e.g. medical technology – https://medtech.eti.pg.gda.pl. There are several interesting medical Internet services available, as: Allergy – http://www.alergen.info.pl Cardiology – http://www.sccs.zabrze.pl/telekardio/informacje.html (ECG via phone); http://www.ptkardio.pl; http://www.nadcisnienie.med.pl Diabetes – http://www.cukrzyca.pl/index.html Testing of hearing and vision – I Can Hear; I Can Speak, Tinnitus, I Can See http://www.telezdrowie.pl; http://www.telezdrowie.pl/indexen.html To show the importance of such services it is worth to know that for example the number of patients using cardiology consultation via phone exceeded 20.000. Every year the Medical Internet Conference is organized where one may find what is going on in this technology – http://www.ptkardio.pl/IV-KONF. One of the main institutions supporting the medical Internet is the Stefan Batory Found – http://www.batory.org.pl/pl/data, where several initiatives already were financed pushing the development of IT technology in medicine.
Country Name
Romania Legislation
The Health insurance law, still needs to be adapted Legal and ethic matters concerning telemedicine have been discussed. Legislative initiatives are present but yet not discussed nor approved by the parliament.
Telemedicine implementation
www.kappa.ro EU project funds (TelenurseID ENTITY, PROPRACTITION) Public funding comes from Phare/World bank RTD funded projects: The Black Sea Tele-Diab: it is a multidisciplinary joint research project within the healthcare information. It has been funded by EU as part of the INCO/COPERNICUS program to support Research and Technical Development in CCE/NIS. The aim is to develop standardised software for the collection, storage, architecture based on the Good European Health Record which was developed within the Advanced Informatics in Medicine Program
56
www.telemed.ro/web_bstd/Trio_new.htm TeleNURSE ID ENTITY: The main objective of the project is to strengthen and enlarge the European consensus on the use of the International Classification of Nursing Practices as a standard computerised nursing language http://atlas.ici.ro/ehto/TELENURSE CDI – Interdisciplinary Dialog Center: The project is a feasibility study for an interdisciplinary centre for the Medical Informatics domain aiming to support the heath system, which now, in Romania, is passing through major changes, by improving the communication between human factors from health care, education, research and industry www.cdi.pub.ro MGT – Medical Guideline Technology: Representing, Interpreting and Sharing Cost-effective Standards Ongoing Initiatives Through a World Bank project for rehabilitation of the health sector, the Health Management Information System has been designed and implemented in 1999, linking in a public health network all the district health authorities (NT and Unix servers, X25 communication standard, dial-up connections of district public health authorities and the Computing Center of the Ministry of Health). In this system, resources are managed through SAP R/3h; patients’ management in hospitals and dispensaries is achieved trough the CHU-Grenoble software. At the level of the MoH several software products are used as DSS or documents management (COMSHARE, TeamLinks). In a pilot district the HEMATOS software is used in blood centers. Other pilot applications are in the field of emergency services (dispatcher for ambulances, radio links between regions and in-regions). Several pilot applications have been developed in the frame of projects funded by the National agency for Science, Technology and Innovation, the National Council for Academic Research, the Romanian Academy or by EU R&D programs covering the following issues: image processing and transfer, smart cards (diabetes, cardiology, neurology), information desks, calling centers, promotion of the ICNP for structuring nursing data, citizens education for health. Several web sites have been designed: http://atlas.ici.ro/ehto, www.ross.ro/EuroMed, http://atlas.ici.ro/ehto/sanatate . There are also some telemedicine applications encapsulated in long distance learning projects. A private company providing internet services has started in 1999 a tele-diagnostic program (www.kappa.ro) in collaboration with hospitals in USA and UK; they also have patient discussion lists and educational web pages. The MoH is in the process of evaluating a DRG pilot study. There are also other punctual projects. For example, smart cards applications are designed in the framework of the scientific and cultural co-operation agreement between Italy and Romania and the dispatcher system for emergency calls has been developed with Swiss governmental help.
Country Name
Slovakia Legislation
Electronic signature
Telemedicine implementation
In order to assist health-care reform in eastern Slovakia, a partnership was established with health-care institutions in Rhode Island. The aim of the partnership was to improve maternal and child health in Slovakia. Thirty-seven telemedicine sessions were conducted via a satellite link. A number of workshops, case studies, demonstrations and interactive discussions took place between various health-care professionals. The use of telemedicine accelerated the adoption of new procedures in Slovakia. (http://www.sgmi-ssim.ch/medline/IM_00035.htm) Project Nove Zamky – AITKEN Neurosurgery department in Nove Zamky is using image transfer of computer tomography through Internet for the consultations of the patients with serious head injuries with the professionals in Aitken Neurosurgery Center in New York
Country Name
Slovenia Legislation
Electronic signature
Telemedicine
Smart Cards: http://www.zzzs.si/kzz/ang/enghtml/systemhtm/document.htm
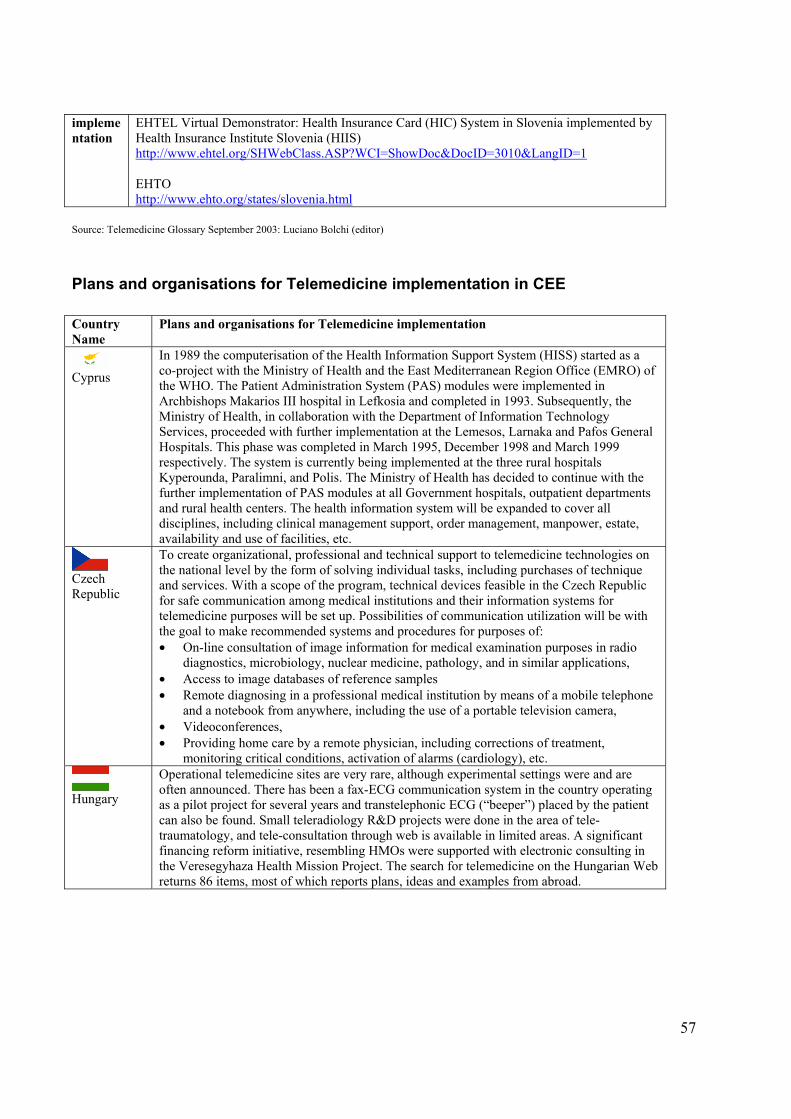
57
implementation
EHTEL Virtual Demonstrator: Health Insurance Card (HIC) System in Slovenia implemented by Health Insurance Institute Slovenia (HIIS) http://www.ehtel.org/SHWebClass.ASP?WCI=ShowDoc&DocID=3010&LangID=1 EHTO http://www.ehto.org/states/slovenia.html
Source: Telemedicine Glossary September 2003: Luciano Bolchi (editor)
Plans and organisations for Telemedicine implementation in CEE Country Name
Plans and organisations for Telemedicine implementation
Cyprus
In 1989 the computerisation of the Health Information Support System (HISS) started as a co-project with the Ministry of Health and the East Mediterranean Region Office (EMRO) of the WHO. The Patient Administration System (PAS) modules were implemented in Archbishops Makarios III hospital in Lefkosia and completed in 1993. Subsequently, the Ministry of Health, in collaboration with the Department of Information Technology Services, proceeded with further implementation at the Lemesos, Larnaka and Pafos General Hospitals. This phase was completed in March 1995, December 1998 and March 1999 respectively. The system is currently being implemented at the three rural hospitals Kyperounda, Paralimni, and Polis. The Ministry of Health has decided to continue with the further implementation of PAS modules at all Government hospitals, outpatient departments and rural health centers. The health information system will be expanded to cover all disciplines, including clinical management support, order management, manpower, estate, availability and use of facilities, etc.
Czech Republic
To create organizational, professional and technical support to telemedicine technologies on the national level by the form of solving individual tasks, including purchases of technique and services. With a scope of the program, technical devices feasible in the Czech Republic for safe communication among medical institutions and their information systems for telemedicine purposes will be set up. Possibilities of communication utilization will be with the goal to make recommended systems and procedures for purposes of: • On-line consultation of image information for medical examination purposes in radio
diagnostics, microbiology, nuclear medicine, pathology, and in similar applications, • Access to image databases of reference samples • Remote diagnosing in a professional medical institution by means of a mobile telephone
and a notebook from anywhere, including the use of a portable television camera, • Videoconferences, • Providing home care by a remote physician, including corrections of treatment,
monitoring critical conditions, activation of alarms (cardiology), etc.
Hungary
Operational telemedicine sites are very rare, although experimental settings were and are often announced. There has been a fax-ECG communication system in the country operating as a pilot project for several years and transtelephonic ECG (“beeper”) placed by the patient can also be found. Small teleradiology R&D projects were done in the area of tele-traumatology, and tele-consultation through web is available in limited areas. A significant financing reform initiative, resembling HMOs were supported with electronic consulting in the Veresegyhaza Health Mission Project. The search for telemedicine on the Hungarian Web returns 86 items, most of which reports plans, ideas and examples from abroad.
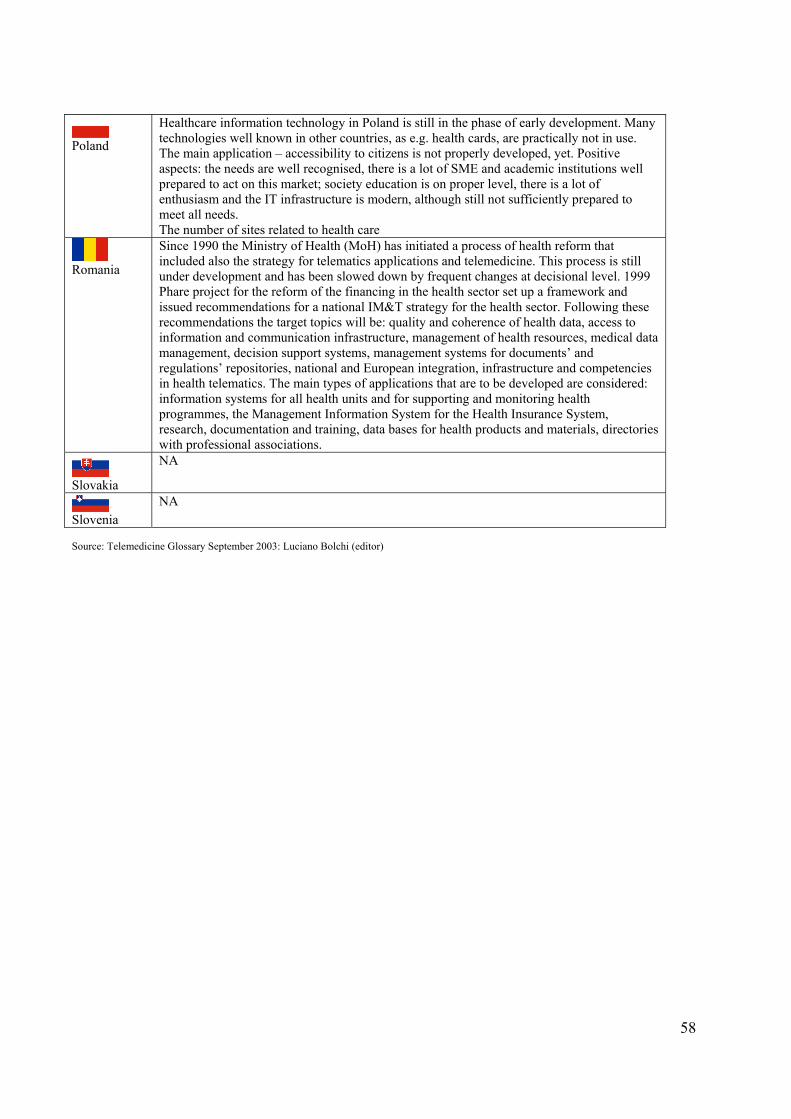
58
Poland
Healthcare information technology in Poland is still in the phase of early development. Many technologies well known in other countries, as e.g. health cards, are practically not in use. The main application – accessibility to citizens is not properly developed, yet. Positive aspects: the needs are well recognised, there is a lot of SME and academic institutions well prepared to act on this market; society education is on proper level, there is a lot of enthusiasm and the IT infrastructure is modern, although still not sufficiently prepared to meet all needs. The number of sites related to health care
Romania
Since 1990 the Ministry of Health (MoH) has initiated a process of health reform that included also the strategy for telematics applications and telemedicine. This process is still under development and has been slowed down by frequent changes at decisional level. 1999 Phare project for the reform of the financing in the health sector set up a framework and issued recommendations for a national IM&T strategy for the health sector. Following these recommendations the target topics will be: quality and coherence of health data, access to information and communication infrastructure, management of health resources, medical data management, decision support systems, management systems for documents’ and regulations’ repositories, national and European integration, infrastructure and competencies in health telematics. The main types of applications that are to be developed are considered: information systems for all health units and for supporting and monitoring health programmes, the Management Information System for the Health Insurance System, research, documentation and training, data bases for health products and materials, directories with professional associations.
Slovakia
NA
Slovenia
NA
Source: Telemedicine Glossary September 2003: Luciano Bolchi (editor)
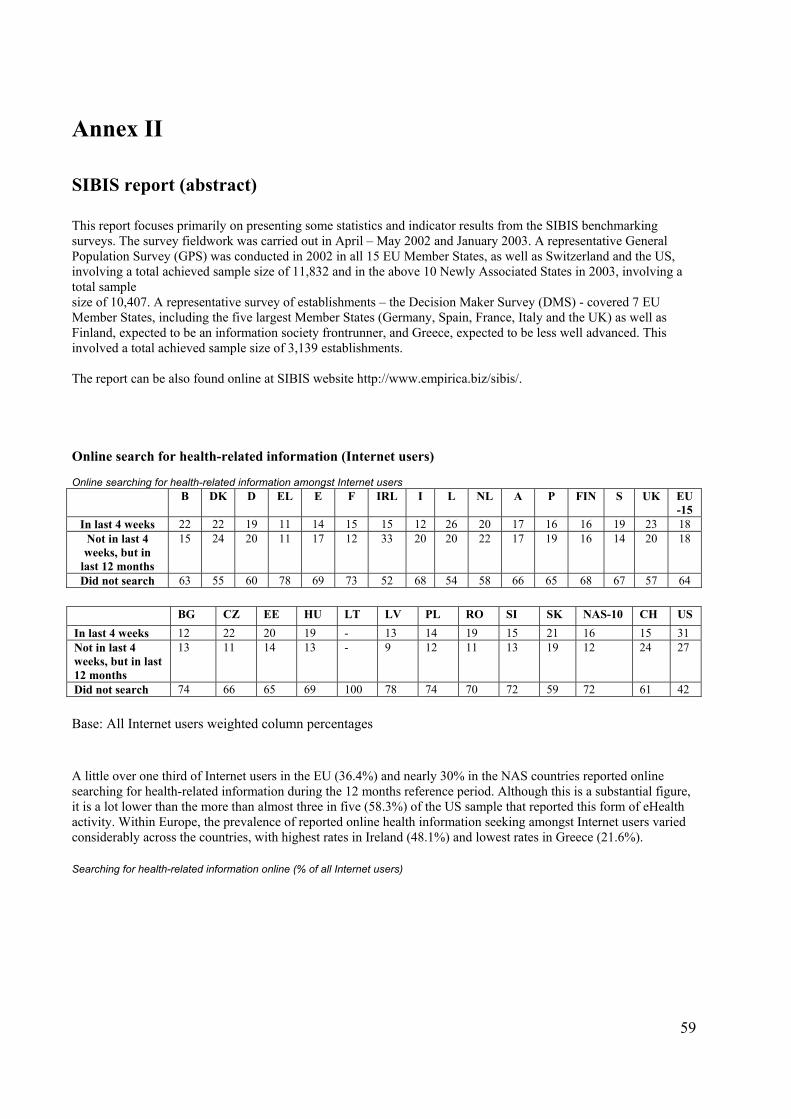
59
Annex II SIBIS report (abstract) This report focuses primarily on presenting some statistics and indicator results from the SIBIS benchmarking surveys. The survey fieldwork was carried out in April – May 2002 and January 2003. A representative General Population Survey (GPS) was conducted in 2002 in all 15 EU Member States, as well as Switzerland and the US, involving a total achieved sample size of 11,832 and in the above 10 Newly Associated States in 2003, involving a total sample size of 10,407. A representative survey of establishments – the Decision Maker Survey (DMS) - covered 7 EU Member States, including the five largest Member States (Germany, Spain, France, Italy and the UK) as well as Finland, expected to be an information society frontrunner, and Greece, expected to be less well advanced. This involved a total achieved sample size of 3,139 establishments. The report can be also found online at SIBIS website http://www.empirica.biz/sibis/. Online search for health-related information (Internet users) Online searching for health-related information amongst Internet users
B DK D EL E F IRL I L NL A P FIN S UK EU-15
In last 4 weeks 22 22 19 11 14 15 15 12 26 20 17 16 16 19 23 18 Not in last 4 weeks, but in
last 12 months
15 24 20 11 17 12 33 20 20 22 17 19 16 14 20 18
Did not search 63 55 60 78 69 73 52 68 54 58 66 65 68 67 57 64 BG CZ EE HU LT LV PL RO SI SK NAS-10 CH US In last 4 weeks 12 22 20 19 - 13 14 19 15 21 16 15 31 Not in last 4 weeks, but in last 12 months
13 11 14 13 - 9 12 11 13 19 12 24 27
Did not search 74 66 65 69 100 78 74 70 72 59 72 61 42 Base: All Internet users weighted column percentages A little over one third of Internet users in the EU (36.4%) and nearly 30% in the NAS countries reported online searching for health-related information during the 12 months reference period. Although this is a substantial figure, it is a lot lower than the more than almost three in five (58.3%) of the US sample that reported this form of eHealth activity. Within Europe, the prevalence of reported online health information seeking amongst Internet users varied considerably across the countries, with highest rates in Ireland (48.1%) and lowest rates in Greece (21.6%). Searching for health-related information online (% of all Internet users)
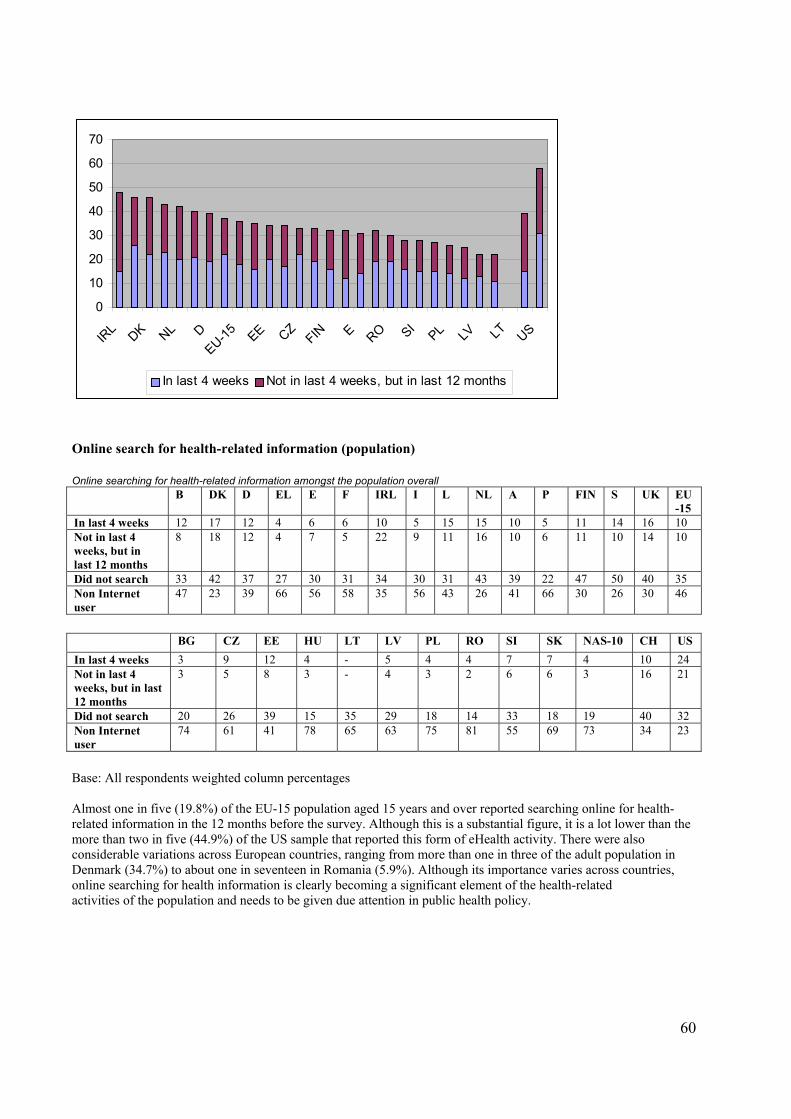
60
Online search for health-related information (population) Online searching for health-related information amongst the population overall B DK D EL E F IRL I L NL A P FIN S UK EU
-15 In last 4 weeks 12 17 12 4 6 6 10 5 15 15 10 5 11 14 16 10 Not in last 4 weeks, but in last 12 months
8 18 12 4 7 5 22 9 11 16 10 6 11 10 14 10
Did not search 33 42 37 27 30 31 34 30 31 43 39 22 47 50 40 35 Non Internet user
47 23 39 66 56 58 35 56 43 26 41 66 30 26 30 46
BG CZ EE HU LT LV PL RO SI SK NAS-10 CH US In last 4 weeks 3 9 12 4 - 5 4 4 7 7 4 10 24 Not in last 4 weeks, but in last 12 months
3 5 8 3 - 4 3 2 6 6 3 16 21
Did not search 20 26 39 15 35 29 18 14 33 18 19 40 32 Non Internet user
74 61 41 78 65 63 75 81 55 69 73 34 23
Base: All respondents weighted column percentages Almost one in five (19.8%) of the EU-15 population aged 15 years and over reported searching online for health-related information in the 12 months before the survey. Although this is a substantial figure, it is a lot lower than the more than two in five (44.9%) of the US sample that reported this form of eHealth activity. There were also considerable variations across European countries, ranging from more than one in three of the adult population in Denmark (34.7%) to about one in seventeen in Romania (5.9%). Although its importance varies across countries, online searching for health information is clearly becoming a significant element of the health-related activities of the population and needs to be given due attention in public health policy.
0
10
20
30
40
50
60
70
IRL DK NL D
EU-15 EE CZFIN E RO SI
PL LV LT US
In last 4 weeks Not in last 4 weeks, but in last 12 months
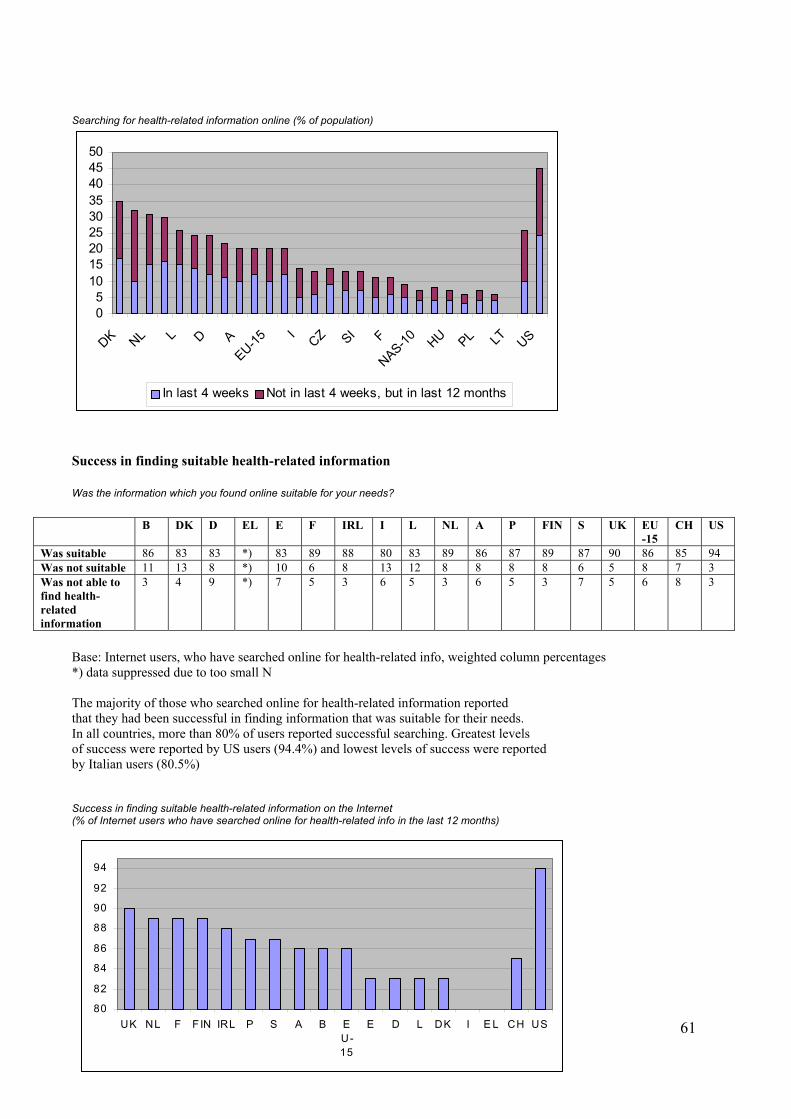
61
Searching for health-related information online (% of population)
Success in finding suitable health-related information Was the information which you found online suitable for your needs?
B DK D EL E F IRL I L NL A P FIN S UK EU-15
CH US
Was suitable 86 83 83 *) 83 89 88 80 83 89 86 87 89 87 90 86 85 94 Was not suitable 11 13 8 *) 10 6 8 13 12 8 8 8 8 6 5 8 7 3 Was not able to find health-related information
3 4 9 *) 7 5 3 6 5 3 6 5 3 7 5 6 8 3
Base: Internet users, who have searched online for health-related info, weighted column percentages *) data suppressed due to too small N The majority of those who searched online for health-related information reported that they had been successful in finding information that was suitable for their needs. In all countries, more than 80% of users reported successful searching. Greatest levels of success were reported by US users (94.4%) and lowest levels of success were reported by Italian users (80.5%) Success in finding suitable health-related information on the Internet (% of Internet users who have searched online for health-related info in the last 12 months)
05
101520253035404550
DK NL L D AEU-15
ICZ SI F
NAS-10 HU PL LT US
In last 4 weeks Not in last 4 weeks, but in last 12 months
80
82
84
86
88
90
92
94
UK NL F FIN IRL P S A B EU-15
E D L DK I E L CH US
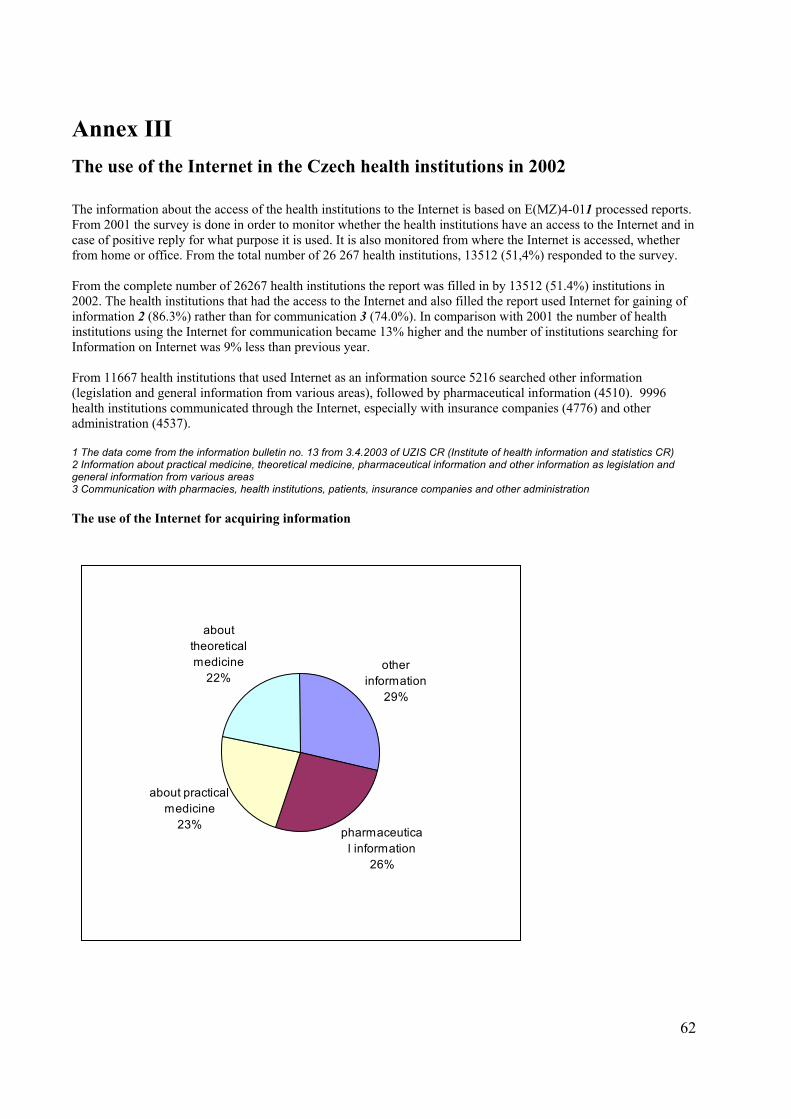
62
Annex III The use of the Internet in the Czech health institutions in 2002 The information about the access of the health institutions to the Internet is based on E(MZ)4-011 processed reports. From 2001 the survey is done in order to monitor whether the health institutions have an access to the Internet and in case of positive reply for what purpose it is used. It is also monitored from where the Internet is accessed, whether from home or office. From the total number of 26 267 health institutions, 13512 (51,4%) responded to the survey. From the complete number of 26267 health institutions the report was filled in by 13512 (51.4%) institutions in 2002. The health institutions that had the access to the Internet and also filled the report used Internet for gaining of information 2 (86.3%) rather than for communication 3 (74.0%). In comparison with 2001 the number of health institutions using the Internet for communication became 13% higher and the number of institutions searching for Information on Internet was 9% less than previous year. From 11667 health institutions that used Internet as an information source 5216 searched other information (legislation and general information from various areas), followed by pharmaceutical information (4510). 9996 health institutions communicated through the Internet, especially with insurance companies (4776) and other administration (4537). 1 The data come from the information bulletin no. 13 from 3.4.2003 of UZIS CR (Institute of health information and statistics CR) 2 Information about practical medicine, theoretical medicine, pharmaceutical information and other information as legislation and general information from various areas 3 Communication with pharmacies, health institutions, patients, insurance companies and other administration The use of the Internet for acquiring information
other information
29%
pharmaceutical information
26%
about practical medicine
23%
about theoretical medicine
22%
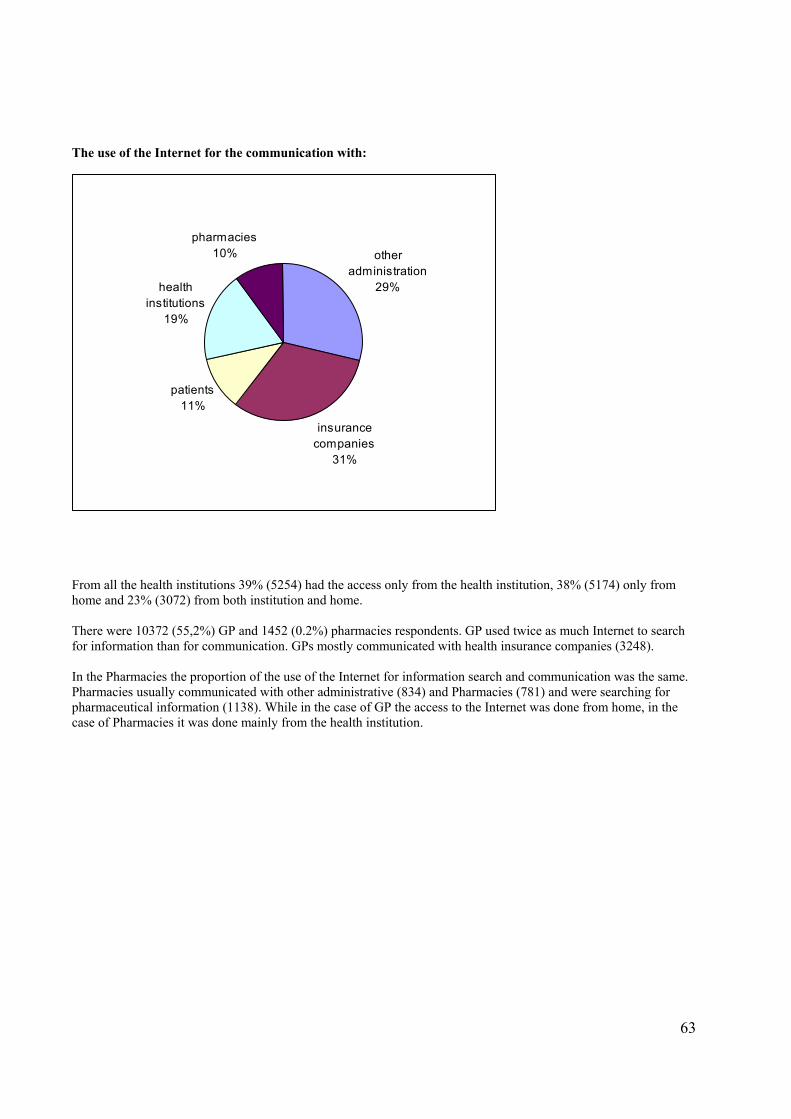
63
The use of the Internet for the communication with:
From all the health institutions 39% (5254) had the access only from the health institution, 38% (5174) only from home and 23% (3072) from both institution and home. There were 10372 (55,2%) GP and 1452 (0.2%) pharmacies respondents. GP used twice as much Internet to search for information than for communication. GPs mostly communicated with health insurance companies (3248). In the Pharmacies the proportion of the use of the Internet for information search and communication was the same. Pharmacies usually communicated with other administrative (834) and Pharmacies (781) and were searching for pharmaceutical information (1138). While in the case of GP the access to the Internet was done from home, in the case of Pharmacies it was done mainly from the health institution.
other administration
29%
insurance companies
31%
patients11%
health institutions
19%
pharmacies10%
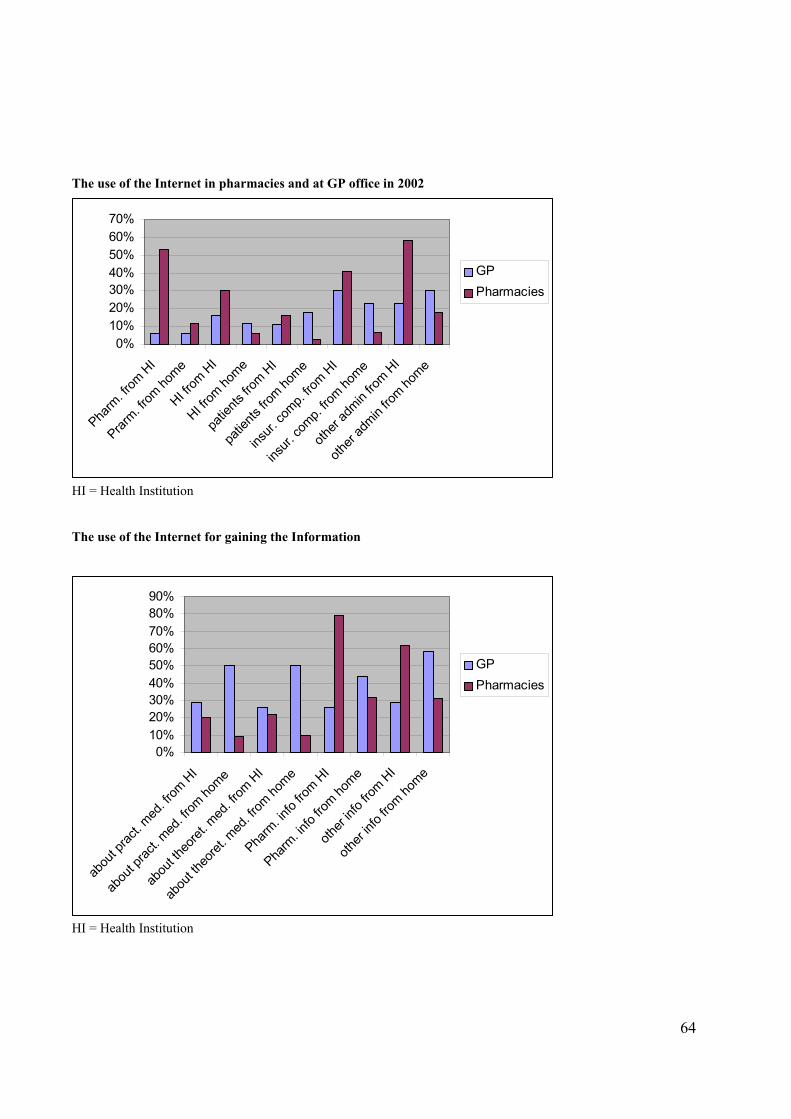
64
The use of the Internet in pharmacies and at GP office in 2002
HI = Health Institution The use of the Internet for gaining the Information
HI = Health Institution
0%10%20%30%40%50%60%70%80%90%
abou
t prac
t. med
. from
HI
abou
t prac
t. med
. from
home
abou
t theo
ret. m
ed. fr
om H
I
abou
t theo
ret. m
ed. fr
om ho
me
Pharm
. info
from H
I
Pharm
. info
from ho
me
other
info f
rom H
I
other
info f
rom ho
me
GPPharmacies
0%10%20%30%40%50%60%70%
Pharm
. from
HI
Prarm. fr
om ho
me
HI from
HI
HI from
home
patie
nts fro
m HI
patie
nts fro
m home
insur.
comp.
from H
I
insur.
comp.
from ho
me
other
admin
from H
I
other
admin
from ho
me
GPPharmacies
65
Annex IV
Survey of the Information Systems (IS) in the Czech hospitals 2003
The survey was conducted by Ministry of Health CR and IPVZ (Institute of postgraduate education in health), Prague. Acronyms used CLS JEP Ceska lekarska spolecnost Jana Evangelisty Purkyne IPVZ Institut postgradualniho vzdelavani ve zdravotnictvi, Praha IS Information System HIS Hospital information system About the Survey Motive of the Survey The motive for conducting this survey was the preparation of the health information systems courses that are for many years provided by department of clinical biology at IPVZ Prague. The attendees of the course pointed the fact that the data about HIS market that are used at the course are coming from the companies and these information is not adequately balanced by the data coming from hospitals. That’s why the professional guarantors agreed with the Department of Informatics of Ministry of Health to conduct this pilot survey. The data acquired are so far the biggest survey about the state of health informatics, that was every done in the Czech Republic, although the original purpose was to only improve the data used at the above mentioned course and the authors fully acknowledge the limitations that these data have. Purpose of the Survey 1. To acquire the basic overview about the building of HIS in Czech bed health institutions and about the state of market in this area 2. To confirm the usability of this method to regularly monitor the state of the market 3. To improve the documents for the attendees of the HIS course at IPVZ 4. To gain the impulses for the activity of Department of Informatics of Ministry of Health and Czech society of Health Informatics and scientific information at CLS JEP The Execution of the Survey 1. Written enquiry was sent to the addresses of Health Institutions with beds. The addresses came from the database of Ministry of Health CR and were addressed to the Head of Informatics Department with the request to voluntarily answer the questions. The data protection was guaranteed. (Jan – March 03) 2. The returned questionnaires were preliminarily evaluated and the conclusion was reported at IPVZ course. (April 03) 3. The survey was processed in detail for this evaluation (June – Aug. 03) 4. The survey has been made public – sent to the responders and posted on the Ministry of Health web site. (Sept 03) 5. Supposed error correction and release of the new version (Oct. 03) 6. Dissemination of the results at the seminars and literature (Oct. 03 – Jan. 04) The Results General questions Respondents, Return, Respondents’ Data
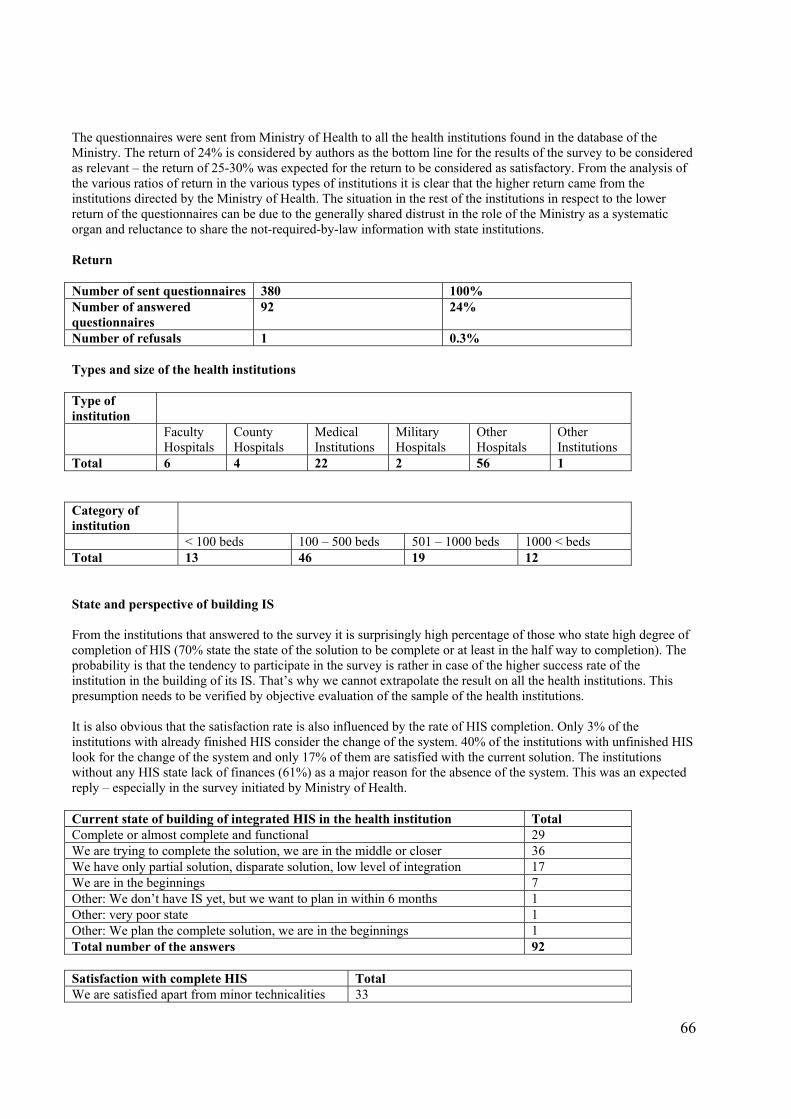
66
The questionnaires were sent from Ministry of Health to all the health institutions found in the database of the Ministry. The return of 24% is considered by authors as the bottom line for the results of the survey to be considered as relevant – the return of 25-30% was expected for the return to be considered as satisfactory. From the analysis of the various ratios of return in the various types of institutions it is clear that the higher return came from the institutions directed by the Ministry of Health. The situation in the rest of the institutions in respect to the lower return of the questionnaires can be due to the generally shared distrust in the role of the Ministry as a systematic organ and reluctance to share the not-required-by-law information with state institutions. Return Number of sent questionnaires 380 100% Number of answered questionnaires
92 24%
Number of refusals 1 0.3% Types and size of the health institutions Type of institution
Faculty Hospitals
County Hospitals
Medical Institutions
Military Hospitals
Other Hospitals
Other Institutions
Total 6 4 22 2 56 1 Category of institution
< 100 beds 100 – 500 beds 501 – 1000 beds 1000 < beds Total 13 46 19 12 State and perspective of building IS From the institutions that answered to the survey it is surprisingly high percentage of those who state high degree of completion of HIS (70% state the state of the solution to be complete or at least in the half way to completion). The probability is that the tendency to participate in the survey is rather in case of the higher success rate of the institution in the building of its IS. That’s why we cannot extrapolate the result on all the health institutions. This presumption needs to be verified by objective evaluation of the sample of the health institutions. It is also obvious that the satisfaction rate is also influenced by the rate of HIS completion. Only 3% of the institutions with already finished HIS consider the change of the system. 40% of the institutions with unfinished HIS look for the change of the system and only 17% of them are satisfied with the current solution. The institutions without any HIS state lack of finances (61%) as a major reason for the absence of the system. This was an expected reply – especially in the survey initiated by Ministry of Health. Current state of building of integrated HIS in the health institution Total Complete or almost complete and functional 29 We are trying to complete the solution, we are in the middle or closer 36 We have only partial solution, disparate solution, low level of integration 17 We are in the beginnings 7 Other: We don’t have IS yet, but we want to plan in within 6 months 1 Other: very poor state 1 Other: We plan the complete solution, we are in the beginnings 1 Total number of the answers 92 Satisfaction with complete HIS Total We are satisfied apart from minor technicalities 33
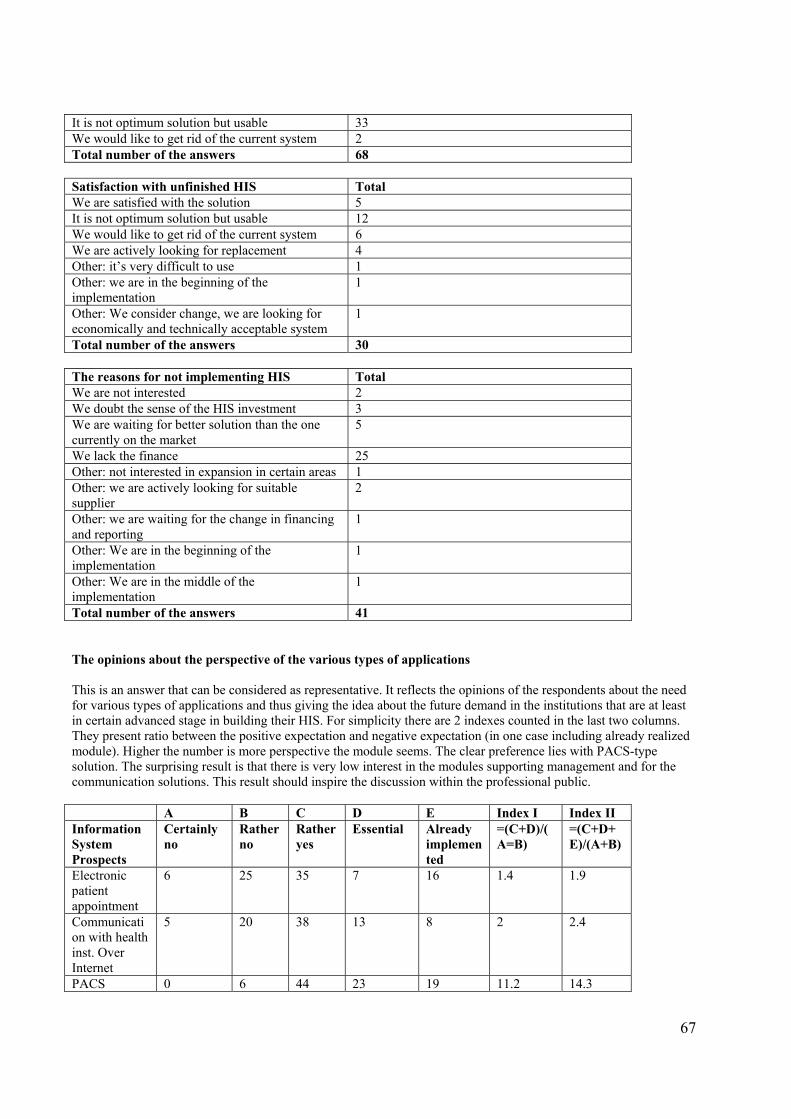
67
It is not optimum solution but usable 33 We would like to get rid of the current system 2 Total number of the answers 68 Satisfaction with unfinished HIS Total We are satisfied with the solution 5 It is not optimum solution but usable 12 We would like to get rid of the current system 6 We are actively looking for replacement 4 Other: it’s very difficult to use 1 Other: we are in the beginning of the implementation
1
Other: We consider change, we are looking for economically and technically acceptable system
1
Total number of the answers 30 The reasons for not implementing HIS Total We are not interested 2 We doubt the sense of the HIS investment 3 We are waiting for better solution than the one currently on the market
5
We lack the finance 25 Other: not interested in expansion in certain areas 1 Other: we are actively looking for suitable supplier
2
Other: we are waiting for the change in financing and reporting
1
Other: We are in the beginning of the implementation
1
Other: We are in the middle of the implementation
1
Total number of the answers 41 The opinions about the perspective of the various types of applications This is an answer that can be considered as representative. It reflects the opinions of the respondents about the need for various types of applications and thus giving the idea about the future demand in the institutions that are at least in certain advanced stage in building their HIS. For simplicity there are 2 indexes counted in the last two columns. They present ratio between the positive expectation and negative expectation (in one case including already realized module). Higher the number is more perspective the module seems. The clear preference lies with PACS-type solution. The surprising result is that there is very low interest in the modules supporting management and for the communication solutions. This result should inspire the discussion within the professional public. A B C D E Index I Index II Information System Prospects
Certainly no
Rather no
Rather yes
Essential Already implemented
=(C+D)/(A=B)
=(C+D+E)/(A+B)
Electronic patient appointment
6 25 35 7 16 1.4 1.9
Communication with health inst. Over Internet
5 20 38 13 8 2 2.4
PACS 0 6 44 23 19 11.2 14.3
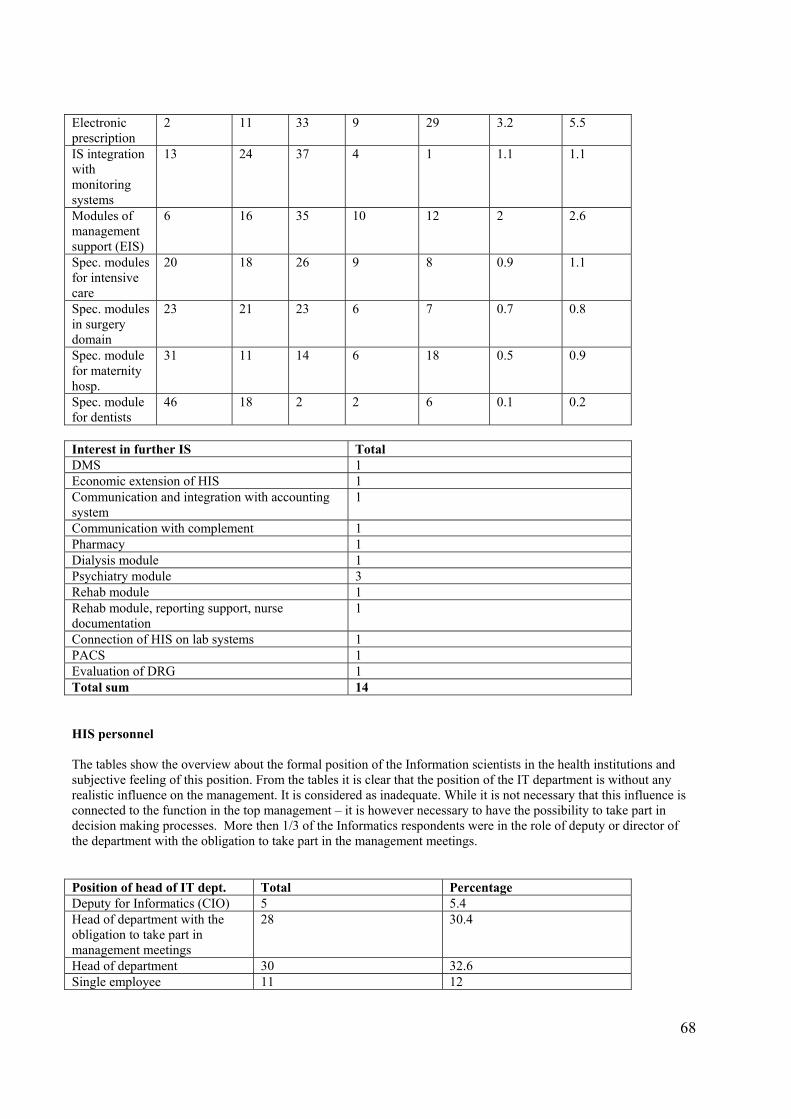
68
Electronic prescription
2 11 33 9 29 3.2 5.5
IS integration with monitoring systems
13 24 37 4 1 1.1 1.1
Modules of management support (EIS)
6 16 35 10 12 2 2.6
Spec. modules for intensive care
20 18 26 9 8 0.9 1.1
Spec. modules in surgery domain
23 21 23 6 7 0.7 0.8
Spec. module for maternity hosp.
31 11 14 6 18 0.5 0.9
Spec. module for dentists
46 18 2 2 6 0.1 0.2
Interest in further IS Total DMS 1 Economic extension of HIS 1 Communication and integration with accounting system
1
Communication with complement 1 Pharmacy 1 Dialysis module 1 Psychiatry module 3 Rehab module 1 Rehab module, reporting support, nurse documentation
1
Connection of HIS on lab systems 1 PACS 1 Evaluation of DRG 1 Total sum 14 HIS personnel The tables show the overview about the formal position of the Information scientists in the health institutions and subjective feeling of this position. From the tables it is clear that the position of the IT department is without any realistic influence on the management. It is considered as inadequate. While it is not necessary that this influence is connected to the function in the top management – it is however necessary to have the possibility to take part in decision making processes. More then 1/3 of the Informatics respondents were in the role of deputy or director of the department with the obligation to take part in the management meetings. Position of head of IT dept. Total Percentage Deputy for Informatics (CIO) 5 5.4 Head of department with the obligation to take part in management meetings
28 30.4
Head of department 30 32.6 Single employee 11 12
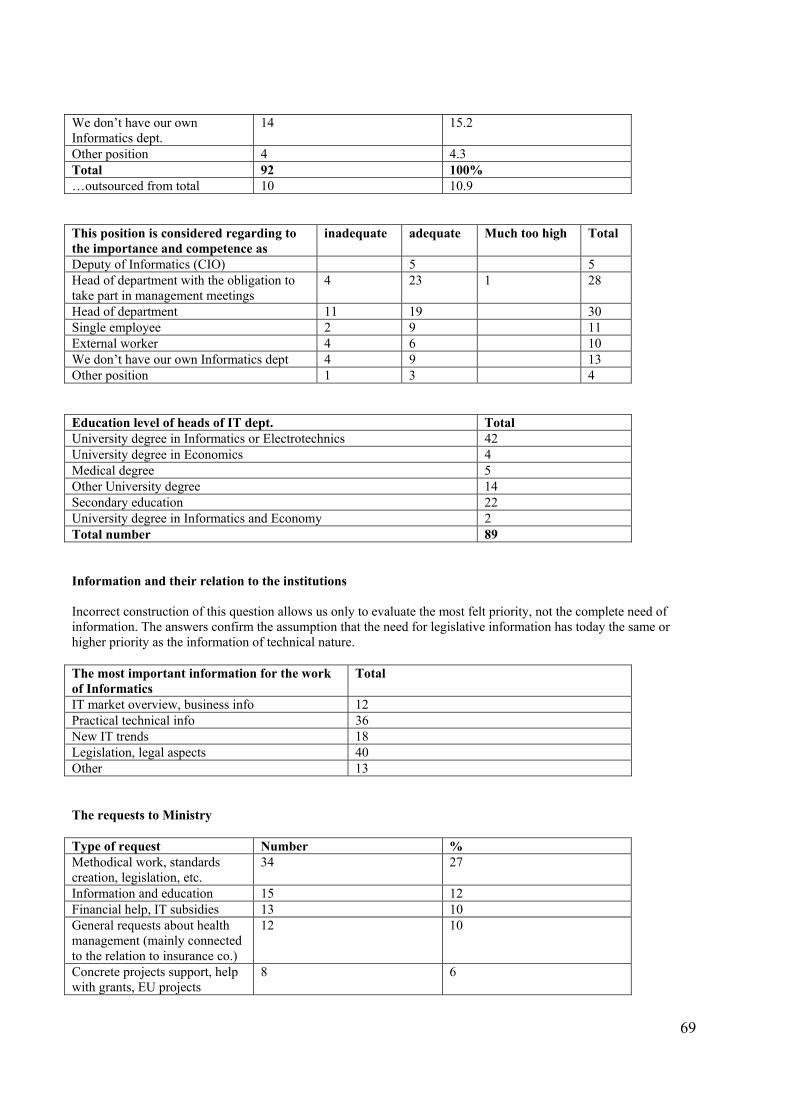
69
We don’t have our own Informatics dept.
14 15.2
Other position 4 4.3 Total 92 100% …outsourced from total 10 10.9 This position is considered regarding to the importance and competence as
inadequate adequate Much too high Total
Deputy of Informatics (CIO) 5 5 Head of department with the obligation to take part in management meetings
4 23 1 28
Head of department 11 19 30 Single employee 2 9 11 External worker 4 6 10 We don’t have our own Informatics dept 4 9 13 Other position 1 3 4 Education level of heads of IT dept. Total University degree in Informatics or Electrotechnics 42 University degree in Economics 4 Medical degree 5 Other University degree 14 Secondary education 22 University degree in Informatics and Economy 2 Total number 89 Information and their relation to the institutions Incorrect construction of this question allows us only to evaluate the most felt priority, not the complete need of information. The answers confirm the assumption that the need for legislative information has today the same or higher priority as the information of technical nature. The most important information for the work of Informatics
Total
IT market overview, business info 12 Practical technical info 36 New IT trends 18 Legislation, legal aspects 40 Other 13 The requests to Ministry Type of request Number % Methodical work, standards creation, legislation, etc.
34 27
Information and education 15 12 Financial help, IT subsidies 13 10 General requests about health management (mainly connected to the relation to insurance co.)
12 10
Concrete projects support, help with grants, EU projects
8 6
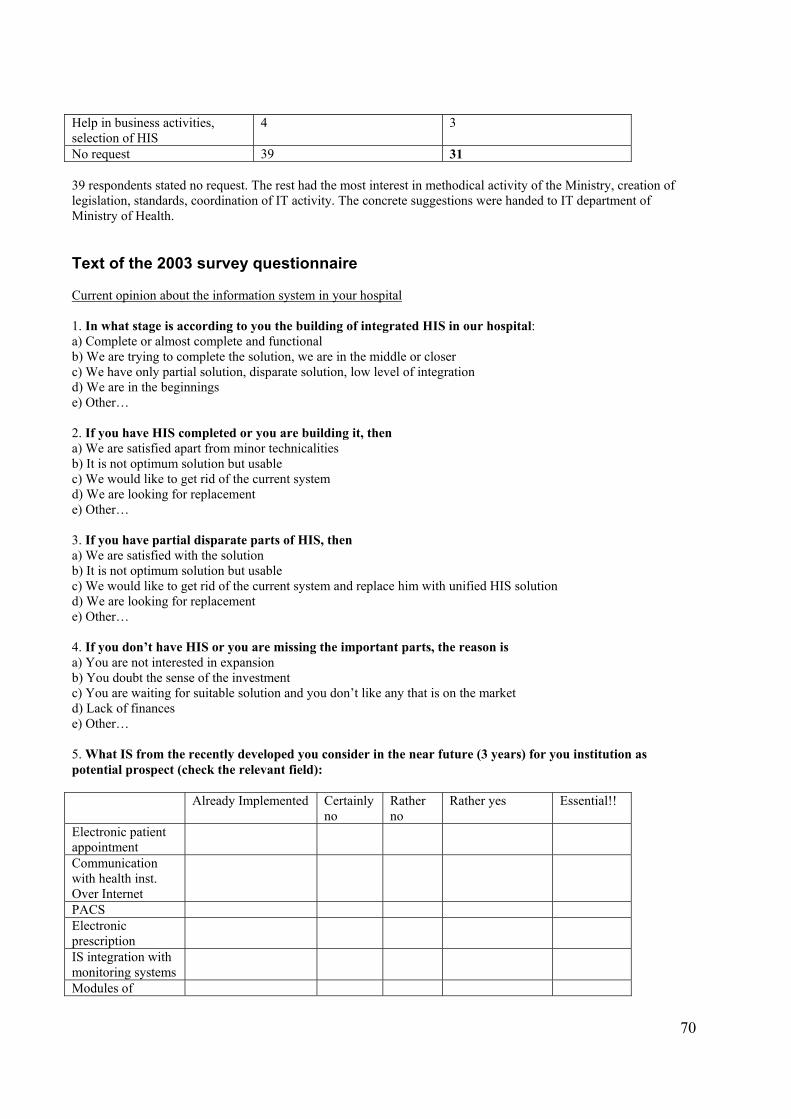
70
Help in business activities, selection of HIS
4 3
No request 39 31 39 respondents stated no request. The rest had the most interest in methodical activity of the Ministry, creation of legislation, standards, coordination of IT activity. The concrete suggestions were handed to IT department of Ministry of Health. Text of the 2003 survey questionnaire Current opinion about the information system in your hospital 1. In what stage is according to you the building of integrated HIS in our hospital: a) Complete or almost complete and functional b) We are trying to complete the solution, we are in the middle or closer c) We have only partial solution, disparate solution, low level of integration d) We are in the beginnings e) Other… 2. If you have HIS completed or you are building it, then a) We are satisfied apart from minor technicalities b) It is not optimum solution but usable c) We would like to get rid of the current system d) We are looking for replacement e) Other… 3. If you have partial disparate parts of HIS, then a) We are satisfied with the solution b) It is not optimum solution but usable c) We would like to get rid of the current system and replace him with unified HIS solution d) We are looking for replacement e) Other… 4. If you don’t have HIS or you are missing the important parts, the reason is a) You are not interested in expansion b) You doubt the sense of the investment c) You are waiting for suitable solution and you don’t like any that is on the market d) Lack of finances e) Other… 5. What IS from the recently developed you consider in the near future (3 years) for you institution as potential prospect (check the relevant field): Already Implemented Certainly
no Rather no
Rather yes Essential!!
Electronic patient appointment
Communication with health inst. Over Internet
PACS Electronic prescription
IS integration with monitoring systems
Modules of
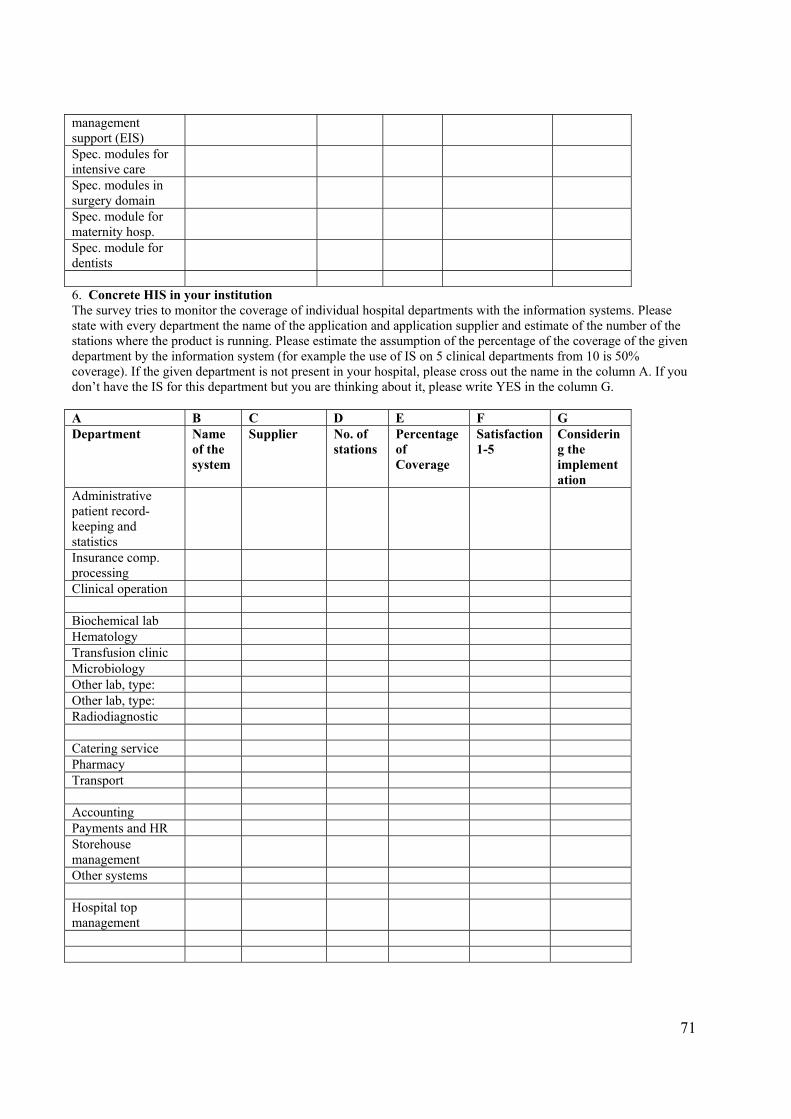
71
management support (EIS) Spec. modules for intensive care
Spec. modules in surgery domain
Spec. module for maternity hosp.
Spec. module for dentists
6. Concrete HIS in your institution The survey tries to monitor the coverage of individual hospital departments with the information systems. Please state with every department the name of the application and application supplier and estimate of the number of the stations where the product is running. Please estimate the assumption of the percentage of the coverage of the given department by the information system (for example the use of IS on 5 clinical departments from 10 is 50% coverage). If the given department is not present in your hospital, please cross out the name in the column A. If you don’t have the IS for this department but you are thinking about it, please write YES in the column G. A B C D E F G Department Name
of the system
Supplier No. of stations
Percentage of Coverage
Satisfaction1-5
Considering the implementation
Administrative patient record-keeping and statistics
Insurance comp. processing
Clinical operation Biochemical lab Hematology Transfusion clinic Microbiology Other lab, type: Other lab, type: Radiodiagnostic Catering service Pharmacy Transport Accounting Payments and HR Storehouse management
Other systems Hospital top management
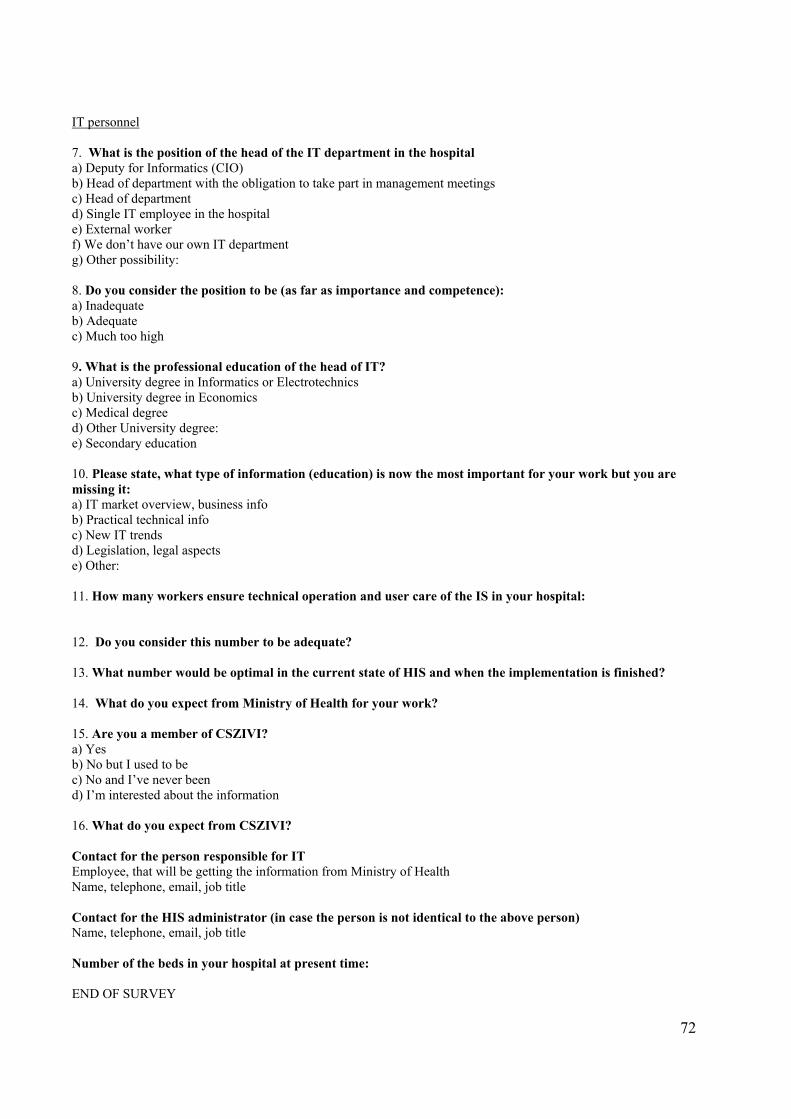
72
IT personnel 7. What is the position of the head of the IT department in the hospital a) Deputy for Informatics (CIO) b) Head of department with the obligation to take part in management meetings c) Head of department d) Single IT employee in the hospital e) External worker f) We don’t have our own IT department g) Other possibility: 8. Do you consider the position to be (as far as importance and competence): a) Inadequate b) Adequate c) Much too high 9. What is the professional education of the head of IT? a) University degree in Informatics or Electrotechnics b) University degree in Economics c) Medical degree d) Other University degree: e) Secondary education 10. Please state, what type of information (education) is now the most important for your work but you are missing it: a) IT market overview, business info b) Practical technical info c) New IT trends d) Legislation, legal aspects e) Other: 11. How many workers ensure technical operation and user care of the IS in your hospital: 12. Do you consider this number to be adequate? 13. What number would be optimal in the current state of HIS and when the implementation is finished? 14. What do you expect from Ministry of Health for your work? 15. Are you a member of CSZIVI? a) Yes b) No but I used to be c) No and I’ve never been d) I’m interested about the information 16. What do you expect from CSZIVI? Contact for the person responsible for IT Employee, that will be getting the information from Ministry of Health Name, telephone, email, job title Contact for the HIS administrator (in case the person is not identical to the above person) Name, telephone, email, job title Number of the beds in your hospital at present time: END OF SURVEY
73
Annex V Telemedicina.CZ - Telemedicine Projects in Czech Republic There has been an interesting project of Information platform organized by Prof. Rosch Foundation with the support of Czech Telecom. The aim of this project was a support of new technologies through the pilot project that were mainly focused on the clinical applications (teleconsultations of the doctors during the surgery or the transmission of these surgeries for the purposes of distant education and training of the doctors). The site is available at http://www.telemedicina.cz. FH = Faculty Hospital CT = Computer Tomography A) Main projects Interventional teleradiology Time Frame: 1998 – 2000 Description: Interconnection of radiological workplaces IKEM Praha, FH Hradec Kralove, FH Olomouc and FH Brno-Bohunice on the base of euroISDN services for the provision videoconferencing (pool of 6 B channels of 3 basic euroISDN2 terminals with 384 kb/s) and videoconferencing terminal Polyspan http://www.polyspan.com/ps/xx/en/products/video/video_medium.html, http://www.polyspan.com/ps/xx/en/downloads/products/video/128&512_data_sheet.Pdf . The purpose is to videoconference the surgery with mini-invasive method of interventional radiology for the purposes of teleconsultation during the surgery or to use it for distant teaching/training of the radiologists. http://www.telemedicina.cz/intervencni_teleradiologie.htm Acute Neurotraumatology Interconnection of Ostrava region hospitals for acute nerotramatological consultations Time frame: 2000 – 2001 Description: Interconnection of neurochirurgical workplaces of Ostrava region hospitals (FH with policlinic Ostrava – Poruba, State Salesian hospital in Opava, Hospital Havirov, Hospital Karvina 4, Hospital Karvina 6, Hospital Krnov, Municipal hospital Ostrava, Hospital Frydek-Mistek, Vitkovice hospital of blessed Maria Antonina, Hospital Trinec-Sosna, Hospital Novy Jicin) on the base of euroISDN services for transmission of CT images. http://www.telemedicina.cz/akutni_neurotraumatologie.htm Home (tele-) working for neurosurgeons Time Frame: 2001 Description: Interconnection of neurosurgeons from home to euroISDN2 terminals on the PC of neurosurgery clinic of FH with polyclinic of Ostrava – Poruba for the execution of consultancy services from the homes of neurosurgeons, enabling the possibility of teleconsultation of health documentation (CT images, etc.). The purchase of PC was supported by AutoContCZ a.s. Communication processes are supported by software pcAnywhere B) Other projects The following projects don’t have their own web presence or they are in the discussion phase. Telepathology Telepathology – 1st phase (2001)
74
Initiator of the project was MUDr. Jana Dvorackova ([email protected]) from Cytological and bioptical laboratory in Ostrava. The purpose of the project was to provide financially accessible instrument of static telepathology with the use of web. The following pathological workplaces are involved in the project: FH with P Ostrava, FH Hradec Kralove, Hospital Pardubice, VFH in Prague, State Salesian hospital in Opava, Hospital Frydek-Mistek, BioLab Praha, Pathology Litomysl, LF University of Palacky and Cytological and bioptical laboratories Ostrava. Pathologists had 2 web applications at their disposal: www.telepathology.cz created by Olympus C&S (www.olympus.cz) and www.telepatologie.cz created by Optoteam (www.optoteam.cz) and the possibility of using euroISDN2 or LAN network in the respective hospitals. The results of the project were not completely unambiguous because the given method of static telepathology requires the specific access of the user and doesn’t provide sufficient amount of information needed for reliable diagnosis, especially with more complicated cases. Because of this reason the 2nd phase of the project hasn’t started where 12 health subjects were supposed to be involved and further considerations in this direction are in cooperation with System602 (www.system602.cz). They are oriented on enforcing the methods of dynamic telepathology that enables pathologists in the real time to share bigger amounts of image information. Conclusion: The static and quasidynamic web applications are freely available on the web for the pathologists connected to the Internet. Interconnection of the Olomouc county hospitals with euroISDN service (2002-2003) The Interconnection of the Olomouc county hospitals (OL) based on euroISDN service (2002-2003) The initiators of the project were MUDr. Michal Filip from Neurosurgery clinic FH with polyclinic Ostrava and MUDr. Martin Gabrys ([email protected]) from Neurosurgery clinic FH Olomouc. The purpose of this project was to use the experience from the realization of this application in Osrava region and its adoption for fast and reliable CT images transfers for the needs of acute neurotraumatological consultations of head and spine injuries among the country hospitals and FH Olomouc. Apart from this solution there is also available the web version of the image transfer that is preferred by some users. The involved subjects are: FH Olomouc, Military hospital Olomouc, Hospital with policlinic Prerov, Hospital Sumperk, Hospital Bruntal, Country hospital Vsetin and Municipal hospital Valaske Mezirici. Additionally Hospital Prostejov became involved, where CT is run by the company ProMedica, sro. Conclusion: The project was finished 04/03 and the solution is available for the users. Telecardiology – 1st phase (2003) The initiator of the project is MUDr. Jiri Krupicka ([email protected]) from Cardiocenter FH KV Prague. The purpose of the project is to provide the transfer of echocardiographical images based on euroISDN and their teleconsultation among 3 workplaces of FH KV Prague: Cardiocentrum, ARO and Cardiosurgery. In case of positive results of the pilot project, the 2nd phase will be enlarged to other cooperating hospitals in the Central Bohemian region. IKEM Prague is also interested in the solution. According to the e-mail correspondence with MUDr. Jiri Kupicka the project hasn't started yet as of November 2003 due to the lack of financing. Telehemathology – 1st phase (2002 – 2003) Initiator of the project is prof. MUDr. Miroslav Penka, CSc. ([email protected]), chief of OKH FH Brno. The purpose of the project is to use the experience from static telepathology and provide the means for static telehemathology using the web instrument (http://www.telehematologie.cz) and to ensure the available instruments of dynamic telehemathology using the euroISDN services. The hematological workplaces involved in the project will be: FH Brno, Infantile hospital FH Brno, P&R Lab, sro Novy Jicin, MFH (VFN) in Prague, Municipal hospital Ostrava and FH Olomouc. In 03/03 web application www.telehematologie.cz was put up. It serves all hematologists as a instrument for consultations and demonstrations of their cases analogically. The same way the www.telepatologie.cz is at disposal for pathologists. Teleortography – 1st phase (2002 – 2003)
75
Initiator of the project is MUDr. Vilem Bruk ([email protected]), deputy of the chief of cardiosurgery department of FH Olomouc. The purpose of the project is to use the experience from the project “Interconnection of the Ostrava region hospitals” for the transfer and teleconsultation of orthographic images with the use of euroISDN. The hospitals involved in the project are: FH Olomouc, Vitkovice hospital of Blessed Marie Antonina, FH of St. Anna in Brno, FH Brno, Bata’s hospital Zlin and Municipal hospital Ostrava. Teleconsultation and treatment of acute myocardial infarction – 1st phase (2003) The project initiator is MUDr. Jan Hartman ([email protected]), GP from Rtyne in Podkrkonosi with catheterization unit of Cardiocenter FH Hradec Kralove on the base of fixed and mobile telecommunication network provided by Cesky Telecom as and EuroTel sro. Technically and operationally the teleconsultations will be tested by GP with the nearest Cardiocenter. The purpose is to increase the number of the patients with acute myocardial infarction treated with the help of direct PTCA. This application will enable the cooperation on the decision process (direct PTCA or classic approach) directly with the cardiologist from PTCA center. The patients from the distant regions would benefit most from the success and wider use of this application. (2nd phase) Teleconsultation of laparoscopic executions – 1st phase (2003) Initiator of the project is MUDr. Michael Vrany ([email protected]), head surgeon of Surgery department of Jablonec nad Nisou hospital (http://www.nemjbc.cz ). The purpose of the project is to connect Surgery department of Jablonec nad Nisou Hospital with Urological clinic of MFH (VFN) in Prague (http://www.vfn.cz) with the use of videoconferencing connection based on euroISDN service with the possibility of image and voice transfer to the lecture hall for the needs of education of medics and doctors. The solution could be also used for sharing the videoconferencing device and its accessories for other telemedicine applications inside of MFH (VFN). Interconnection of Brno region hospitals (2003) The initiators of the project are MUDr. Michal Filip from Neurosurgery clinic FNsP Ostrava and doc. MUDr. Vladimir Smrcka, CSc. ([email protected]), the chief of Neurosurgery clinic FH Brno. The project is in the set-up phase and will take the experience from the similar projects realized in the Ostrava and Olomouc region. It is assumed that the following hospitals will participate: FH Brno, Hospital Breclav, Country hospital with policlinic Znojmo, Hospital of TGM Hodonin, Country hospital Kyjov, Country hospital Nove Mesto na Morave, Hospital in Kromeriz, Hospital in Trebic, Hospital Havlickuv Brod, Hospital Boskovice IN, as, Hospital Blansko, Hospital Jihlava and Bata’s hospital Zlin. Teletraumatology – 1st phase (2003) Initiator of the project is doc. MUDr. Leopold Pleva, CSc. ([email protected]), chief of Traumatological center FHwP Ostrava (http://www.fnspo.cz/kliniky/tra/index.html) and member of the committee of Czech society for injury surgery (http://www.csuch.cz). The project is in the set-up phase and should solve the interconnection of 13 traumacenters in Czech Republic (FHwP Ostrava, FH in Plzen, HwP Ceske Budejovice, Mararyk’s HwP in Usti nad Labem, HwP Liberec, Country HwP Pardubice, FH Hradec Kralove, Injury hospital Brno, Bata’s hospital Zlin, FH Olomouc, FH Motol Praha, FH Kralovske Vinohrady Prague and Central military hospital Prague) with the use of videoconferencing interconnection based on euroISDN. Teleconsultation in the area of pediatric auxomology and syndromology (being discussed) The project is base on euroISDN services. The initiator of the project is Dr. Jan Vejvalka ([email protected]). In the 1st phase the following subjects should be involved: FH Motol (http://www.fnmotol.cz), Hospital Havlickuv Brod, Hospital Ceska Lipa, Hospital Litomerice and Hospital Most. Interconnection of Injury hospital Brno with cooperationg hospitals (being discussed) The project is based on euroISDN service with the use of videoconferencing communication. The initiator of the project is doc. MUDr. Peter Wendsche, CSc. ([email protected]), chief of spinal unit UN Brno
76
(http://www.unbr.cz). The purpose of the project is to provide teleconsultation activity of UN Brno in the area of injury surgery in the 1st phase with Bata’s hospital Zlin, Country HwP Znojmo and Hospital Havlickuv Brod. According to the e-mail correspondence with MUDr. Jiri Kupicka the project hasn't started yet as of November 2003 due to the lack of financing and interest of hospital management. Teleendoscopy (being discussed) Teleendoscopy – teleconsultation of endoscopic executions based on euroISDN services and videoconference transfers. The following subjects are preliminary interested: FH Hradec Kralove, IKEM Praha, FH Olomouc and FH Brno. Teledermatology (being discussed) Teledermatology – teleconsultation of dermatological findings with the help of dermatoscop and transfer of digital images with the use of web application or direct PC connection of dermatologists based on euroISDN service. The preliminary interest is by FH Motol and FHwP Ostrava. Telearthroscopy (being discussed) Teleartroscopy – teleconsultation of artroscopic executions at ortopedic surgery executions based on euroISDN services and videoconferencing transfer. Preliminarily are interested FH Motol, FH Hradec Kralove, FH Olomouc and FH Brno. Telebronchoscopy (being discussed) Telebronchoscopy – teleconsultation of bronchoscopic executions based on euroISDN services and videoconferencing transfers. Preliminarily is interested. Pneumological clinic Prague 6 - Veleslavin
77
Annex VI
IZIP – Internet Medical Database, Czech Republic The following text is extracted from the English version of the IZIP web site: www.izip.cz. The abbreviation IZIP in Czech language means Internet Access to Patient's Medical Information. As you already suspect, the objective and substance of the IZIP project is to place the medical database of the insured patient into the public information network - the Internet. The database consists of selected parts of medical documentation written into IZIP by the attending physicians. Both the doctor and the patient may at any time use a computer with internet access to view the results of clinical examinations, laboratory tests and X-ray pictures as well as a list of prescribed and used medicaments. Users may insert a record into IZIP within a few tens of seconds. However, it saves hours of phone calls needed for seeking information from traditional filing cabinets. Only the patient has access to data for reading in IZIP. However, he/she can designate which other persons will have the right to view his/her data. Therefore, every medical facility, which has the patient's consent, may share the records describing the provided care. The patient thus becomes an active element of health care while at the same time saving money in the public medical insurance system. The IZIP project has been devised by doctors for doctors. In line with the worldwide trend the team of authors has materialized their belief that when a patient comes to a medical office the doctor should have a source of up-to-date and reliable information about the provided health care. The IZIP project complies with the Act of the Czech Republic no. 101/2000 about personal data security. It corresponds to the objectives of national health care and information technology policies. The IZIP project is executed by a private company IZIP Ltd., Prague, with the support of General Health Insurance Fund of the Czech Republic (VZP CR) and other partners such as IBM, Czech Telecom, Eurotel, Komercni banka and others. The application solution, software and implementation are supplied by IBM, and the Czech Telecom and Eurotel look after the data transfer. Why Use IZIP The quality of health care attracts much interest from patients as well as doctors and medical insurance companies and it can be assessed from several perspectives. The creators of the IZIP project claim that one factor for the assessment of the quality of health care is the fact whether the insured patient and his physician have reliable and up-to-date information on the provided health care. A well-informed patient is able to make better decisions, cooperates better and gains a better understanding of the technical and possibly even financial limitations of the proposed procedures. In accordance with the act on personal data security, the only person with the authority to decide, who may view his medical data, is the patient himself. If the patient extends these rights to his physicians, laboratories, pharmacies etc. he may thus create his own "virtual hospital" within which he and all his future doctors have access to his complete medical history. After entering the access password, the IZIP provides systematically ordered information about the performed examinations, their results and the advancement of the therapy. The project opens new communication pathways between doctors. While at the present time doctors often have only inadequate information about the health care provided by other medical workers, the IZIP system may enable them to access the results of clinical examinations as well as laboratory and other tests in real time. A greater set of such information contributes to better decisions made by the physician concerning the diagnosis and the therapy. The exploitation of the IZIP system improves the quality of health care since a physician, who has been authorized by his patient to access the patient's IZIP, will assess the situation more easily and virtually resume where the previous doctors have stopped. The physician receives all necessary information on time right when he is with the patient. The Internet record is highly efficient especially for patients who suffer from chronic illnesses and who frequently undergo various examinations and tests. Information from the IZIP system enables the patient and his physician to anticipate unnecessary repetition of procedures which often present a risk to the patient's health. Moreover, the interception of unnecessary repeated jobs
78
leads to important savings in the public medical system while maintaining the quality of the provided care. The IZIP project enhances the efficiency of public medical insurance tools. The IZIP project supports a chip card system and the usage of electronic signatures. IZIP uses the most advanced information security methods for safeguarding the data against loss, misuse or damage. Information security in the system is higher that the current security of medical data in medical and other facilities. How does IZIP work IZIP is an Internet medical file with selected information about the patient's health. IZIP therefore does not replace the entire medical documentation in medical facilities (hospitals), however it presents a valuable selection constructed upon the patient's wish. In order to record data into IZIP, the physician uses his ambulatory software in his office. The interface to the IZIP system is developed either by medical software producers or the physician may use a special "button" in the ledge on the screen constructed to mediate writing into IZIP from the ambulatory site. Specialists may write into IZIP through an interface which allows for data transmission from emergency rooms, laboratories, complementary services and pharmacies. Records in the IZIP system contain: - Anamnesis Results of examinations performed by General Practitioner or Specialist, in chronological order - Results of laboratory tests and examinations - List of prescribed and issued medicaments - X-ray and sonograph pictures - Reports from hospitalisation, vaccination history etc. In emergency situations when the patient is e.g. unconscious, the IZIP system offers the so-called "Emergency Access" to the system. The first-aid physician receives a special access code which allows him to find the IZIP record even without the patient's consent using the patients personal identification number. A thorough record is kept on the access and is followed by a revision of the justification of such access. In terms of the information security of the medical records, IZIP draws on the most advanced tools for the protection of sensitive medical data against loss or misuse. This implies that the security of data in Internet medical files is higher than the security of information in common filing cabinets in medical offices and is on the same level as the security of electronic bank accounts. All data is located on secured servers that are subject to constant surveillance. The only staff members who can access the demarcated database areas are database administrators with authorization and special training. In addition to the access code, each patient may set up a second password, i.e. personal password, when entering the IZIP system on the internet. All information is therefore protected using two passwords and a limit on the number of access attempts. Consequently, as a result of this principle the only way the system may fail is when the user himself discloses both passwords. All patients are alerted of this risk. The Authority for Personal Data Security, which has been continuously consulted with respect to the technical and legal matters of medical records in IZIP, has granted consent with the operation of the IZIP project. The IZIP project is open to the expert community as well as the public. This fact has led to the establishment of the IZIP Project Council with its members being representatives of individual project partners, medical facilities and organizations, and the representatives of public administration, patients and the public. The members of the Council receive detailed information about the project and they act as natural contact persons between the project and the organizations which they represent. Experience with the pilot and testing operation During the pilot phase in the period January to July 2002 the project has registered approximately 10 000 clients in 4 regions of the Czech Republic. Partner companies IBM, Czech Telecom and Eurotel have supplied information technology equipment to registered doctors who did not have the sufficient apparatus. The pilot phase has revealed that 62 % of doctors use a computer for their work. 29 % of doctors have Internet access and 60 % doctors are interested in the IZIP project. A flexible team and a marketing strategy have been set up for the testing phase over the whole territory of the Czech Republic with the objective of extending the project to 50 000 clients by the beginning of the year 2003. After this date the IZIP project should start operating under regular mode.
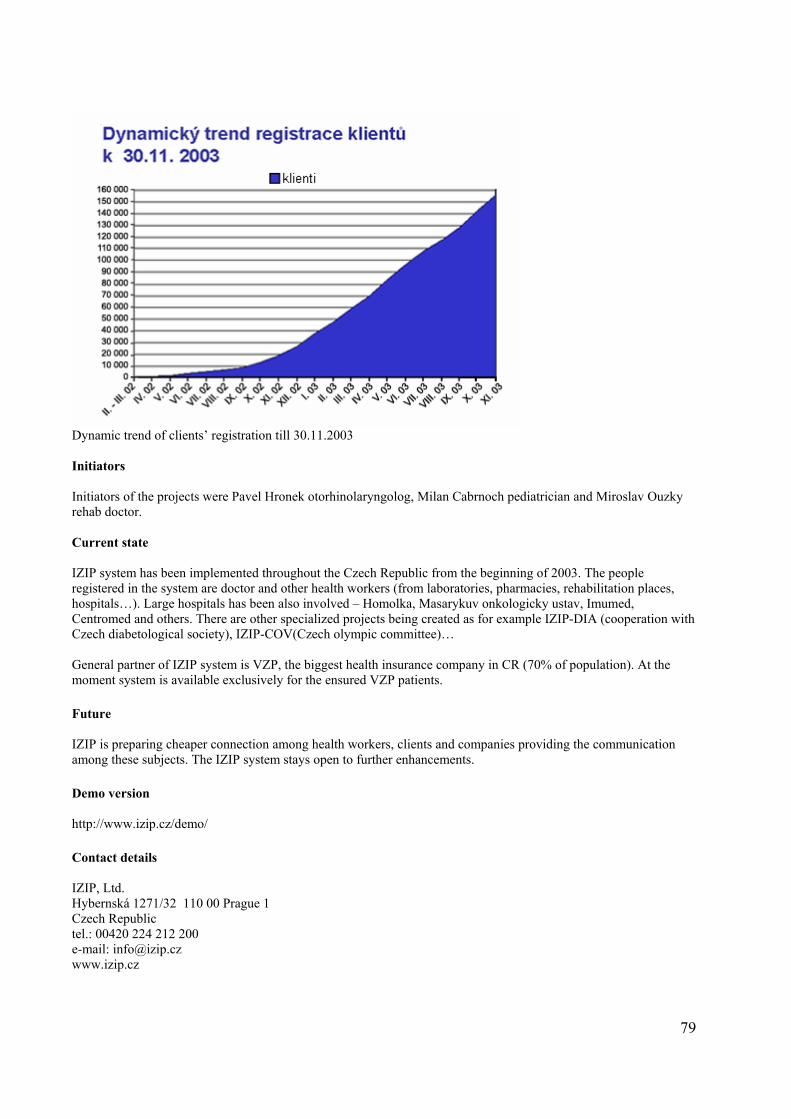
79
Dynamic trend of clients’ registration till 30.11.2003 Initiators Initiators of the projects were Pavel Hronek otorhinolaryngolog, Milan Cabrnoch pediatrician and Miroslav Ouzky rehab doctor. Current state IZIP system has been implemented throughout the Czech Republic from the beginning of 2003. The people registered in the system are doctor and other health workers (from laboratories, pharmacies, rehabilitation places, hospitals…). Large hospitals has been also involved – Homolka, Masarykuv onkologicky ustav, Imumed, Centromed and others. There are other specialized projects being created as for example IZIP-DIA (cooperation with Czech diabetological society), IZIP-COV(Czech olympic committee)… General partner of IZIP system is VZP, the biggest health insurance company in CR (70% of population). At the moment system is available exclusively for the ensured VZP patients. Future IZIP is preparing cheaper connection among health workers, clients and companies providing the communication among these subjects. The IZIP system stays open to further enhancements. Demo version http://www.izip.cz/demo/ Contact details IZIP, Ltd. Hybernská 1271/32 110 00 Prague 1 Czech Republic tel.: 00420 224 212 200 e-mail: [email protected] www.izip.cz
80
Annex VII
MEDTEL & NetC@rd, Czech Republic MEDTEL, o.p.s. is a non-profit organization that was founded with the purpose to become pernament democratic and neutral forum where the various participants (authorities in healthcare, healthcare providers, health insurance companies, patients and citizens associations, interest groups, business companies) could meet and together form the constructive approaches profitable to everyone. MEDTEL is a member of EHTEL. MEDTEL is open to everyone who is interested in taking part in activities in the area of health informatics and telematics with compliance with the status of MEDTEL. Contact details: MEDTEL, o.p.s. Veletrzni 67, 170 00 Praha 7 tf: 233 376 194 fax: 233 379 192 e-mail: [email protected] MUDr. Mgr. Petr Struk - [email protected] Ing. Jiri Ochozka - [email protected] Ing. Tomas Trpisovsky - [email protected] NetC@rd project Czech Republic prepares countrywide introduction of new health insurance cards for the ensured persons of VZP (70% of population) at the middle of 2004. The card reverse will have European health onsurance card (EHIC) format and CR will be one of the first countries where EHIC will be implemented. Goal of the pilot project To verify transborder application of EHIC and eventually citizen health card containing the data about health insurance issued in the EU countries in the conditions of the Czech Republic. The goal is to securely identify the insured person and to create the pre-requisite for the automated authorization of the transactions. The verification will be done in two ways. A. Acceptation of the EU citizens cards in CR The selected health institutions in the tourist-attractive locations will be able to identified EHIC enabled cards. These institutions will be equipped by the multifunctional terminal or by a card reader and SW enabling them to read and verify the cards’ data. B. Acceptation of Czech card (EI VZP) abroad in the EU countries VZP ensured patients will be equipped with new health card with EHIC format and they will be able to present this card when requesting healthcare in EU states. Hot line and/or Internet service will be available for the foreign partners. The scope and structure of the pilot project Pilot place: Prague Participants: VZP Selected health care providers in Prague
81
Subject of the pilot project: • The EU citizens will be able to identify themselves with the EHIC card (in various versions) at the selected
health institutions in Prague. This way of identification will be accepted and billing of the patient will be done based on this procedure.
• Vseobecna zdravotni pojistovna (VZP) is getting ready to issue a new health card in 2004. This card will comply with EU requirements: plastic card with EHIC design on one side. The subject of the pilot project will be preparation and realization of informational, organizational and technical background for issuing, distribution and administration of these cards, verification of the acceptation these cards abroad and related functions of billing and compensation for the provided health care.
The use of the card, the acceptation of the card by health personnel, treatment of the card holder and the way of use and processing of the data acquired from the card will be a subject of the evaluation as a part of the pilot project. Participants in CR
Prime contracter: MEDTEL, o.p.s. Member of consortium: VZP ČR Supporter: Ministerstvo zdravotnictví ČR (Ministry of Health)
CMÚ – Centrum mezistátních úhrad Costs related to the Czech part
310,000,- EUR
82
Annex VIII National Health Registers, Czech Republic IS TRANICON IS TRANICON gathers data to:
Waiting lists for kidney transplantation, combined transplantation of kidney and pancreas, liver, heart and lungs
Register of dead organ donors Register of patients after the transplantation has been done
IS TRANICON is used for selection of the most suitable recipients there organs. KSRZIS is responsible for technical part of the system. It ensures technical management, maintenance and support 24/7/365. IKEM CZ is responsible for the correctness of the data contained in IS TRANICON and for effective, correct and competent handling with these data. Transplantcenters in CR connected to IS TRANICON:
TC Institutu klinické a experimentální medicíny v Praze, TC Fakultní nemocnice v Brně, TC Fakultní nemocnice v Hradci Králové, TC Fakultní nemocnice Praha – Motol, TC Fakultní nemocnice v Olomouci,
National cardiosurgery registry (NKCHR) It came into existence because of the need of all the involved cardiosurgery workplaces to gain the information about the number of heart surgeries in the individual centers. Later it was expanded with the evaluation of the quality of the surgeries incl. Mortality rate, time for hospitalization and stratification of the risk factors. The purpose of NKCHR is:
• To monitor the development, causes and consequences of the serious cardiovascular diseases and states of
determination, monitoring and evaluation of the national quality coefficients, results of doctors’ and nurses’ cardiovascular care
• Determination of qualitative accreditative coefficients based on scientific ground • To provide individual prognostic information for each cardiosurgery intervention, needed for the clinical
decision processes of the doctors • Evaluation of the needs and state of cardiosurgery interventions as far as quality, effectiveness, results and
expenses • Identification of inadequate, potentially unsuitable interventions and therapeutic methods that don’t
accomplish the expected results
National cardiosurgery registry is a part of National medical information system (NZIS). Administrator is Ustav zdravotnickych informaci a statistiky CR (Health Information and Statistics Authority CR) It guarantees the methodological and structural unity of the registry.
83
Registry manager is KSRZIS that is responsible for smooth operation of the registry, state of the database, data control, technical security and data security. It also provides the information technology (HW, SW, communications), authentication and authorization. National oncology registry (NOR) National oncology registry of Czech Republic (NOR) is whole-area population registry run by Ustav zdravotnickych informaci and statistiky CR (UZIS CR) from 1976. NOR is integral part of complex oncological care. The NOR’s task is to register oncological affection, that means to gather data, their verification, storage, protection and processing. NOR offers complete data for statistical summaries on national and international level, further for epidemiological studies and medical research. The NOR’s data servers also as a support for early diagnose and cure of new growths and pretumor states, for monitoring trends and their occurrences, causal factors and social consequences. National oncological registry is part of National medical informational system (NZIS). The Administrator of NOR is UZIS CR. It guarantees the methodological and structural unity of the registry. Registry manager on country level is Koordinacni stredisko rezortnich zdravotnickych informacnich systemu (KSRZIS) that is responsible for smooth operation of the registry, technical security and data security. It also provides the information technology (HW, SW, communications), authentication and authorization. Registry managers on subcountry levels are NOR workplaces with determined area of responsibility, with obligation of maximum documentation of all – new and old – oncological disorders. National registry of vascular surgery From 1988 based on the decision of Committee of Cardiovascular section CS surg. Society (from 2001 Cardiovascular society) the vascular surgeries were monitored in CR vascular registry. In the National registry of vascular surgery (NRCCH), that maintains the continuity with vascular registry from previous years, the numbers of vascular surgeries and interventions in CR are being observed, including risk factors. The types of operations, meaning vascular reconstruction and specialized vascular operations, the frequency of complications, incl. Amputations and deaths, time and date of operations till patient release are being observed. NRCCH is helping the evaluation of the quality of treatment, sick rate in regions, monitoring the accessibility of professional care for vascular patients in the regions. It is a foundation for improving care for vascular patients in CR with direct economical impact. It also serves to Ministry of Health and professional society for necessary organizational measures. NRCCH is a part of National medical information system
National cardiosurgery registry is a part of National medical information system (NZIS). Administrator is Ustav zdravotnickych informaci a statistiky CR (Health Information and Statistics Authority CR) It guarantees the methodological and structural unity of the registry.
Registry manager is KSRZIS that is responsible for smooth operation of the registry, state of the database, data control, technical security and data security. It also provides the information technology (HW, SW, communications), authentication and authorization. National registry of arterial replacements National registry of arterial replacements (NRKN) is whole-area register focused for acquirement and gathering of information about the performed surgeries with the use of artificial joint replacement. This registry is a new element in the documentation, monitoring and overview in such focused orthopedic care and it is its indivisible part. The task of NRKN is the registration of the data about the patients with surgery with utilization of endoprothesis and specific information specifying this treatment. NRKN provides summarized data for statistical overviews for the national and international comparisons, for epidemiological studies and medical research. Registry provides also the information about the attributes of the used implantation materials, mainly from the point of their durability and costs for these
84
materials. The summarized data are the base for creation, realization and evaluation of preventive medical programs and for estimation of necessary financial costs for provision of complex orthopedic care. Anonymous individual data can be provided for epidemiological studies and medical research only in compliance with valid laws and with agreement of NRKN council. NRKN is part of National medical informational system (NZIS). National cardiosurgery registry is a part of National medical information system (NZIS). Administrator is Ustav zdravotnickych informaci a statistiky CR (Health Information and Statistics Authority CR) It guarantees the methodological and structural unity of the registry.
Registry manager is KSRZIS that is responsible for smooth operation of the registry, state of the database, data control, technical security and data security. It also provides the information technology (HW, SW, communications), authentication and authorization. Ophthalmology registry (OFR) Ophthalmology registry (OFR) is one of the pilot projects of telemedine in CR. OFR is image archiving system that solves the support of medical consultancy and decision process for treatment of serious eye diseases that require professional consultancy or manipulation at superkonsiliary ophthalmologic workplace. By using it one can achieve effective way to evaluate findings and ordering patients, which enables decreasing the danger of delays of ocular and/or life threatening stages. The purpose is to improve the communication between the ocular clinics of the faculty hospitals, ocular wards at hospitals and ambulatory specialists. Ophthalmologic Society of CLS JEP is the professional sponsor of the project. Nosocomial Infection registry (RNI) Nosocomial Infection registry (RNI) was establish by Ministry of Health CR for the purpose of using unified information instrument for monitoring and evaluation of clinical cases of nosocomial infection in CR. 1. Purpose and justification of the registry The creation of the RNI was initiated for the purpose of installing the method for measuring and monitoring of the quality and effectiveness of the care inside the individual institutions with the goal of finding important standards of conditions of precaution, providing and financing the care about the states complicated by nosocomial infection (NI) With the help of IT it is possible to effectively gather necessary data from microbiological laboratories and other information sources in the data center and to provide the base for needed analysis and also maximally shorten the time from the first detection of the concrete problem till the time of specific intervention. Local data gained, evaluated and interpreted according to the standard methodologies (management of quality) can be used as an indicator of the quality of care for comparison of incidence and level of the control of NI among the institutions. The results of surveillance in the central RNI acquired for the specific and mutually comparable groups of patients with comparable level of risk are priceless source of information for hospital management and public health administrators. In the stage of registry set-up there was unique interest indicated for its creation from the side of interested professional societies, health installations and public health institutions. The purpose of RNI is: • Registration of clinical cases of NI according to the standard definitions and criterions, optimization of
procedures and methods of collection • Registration and evaluation of clinical data for the purposes of standard local surveillance of NI. The results are
to be used at the same time locally (effective control of NI in given institution) and centrally (formulation of methodological processes, optimization of directives)
• Quality care management – creation and maintenance of statistically representative data base for calculation of key indicators of quality and effectiveness of care and states of potentially and realistically complicated NI
• Application of methods DST (Decision Supporting Tools) in this area • Location, implementation and optimization of economical aspects of NI and antibiotic resistance (incl. System
of covering the care at states of complicated NI)
85
Executive bodies of RNI and their competencies
RNI Administrator RNI Administrator is department of health care of Ministry of Health Czech Republic (OZP MZ CR). The Administrator determines access rights to the registry. RNI Operator Countrywide registry operator is KSRZIS – Coordination department for departmental medical information systems, which is responsible for smooth operation of the registry, state of the database, data control, technical security of the data. It provides information technologies (HW, SW, communications), authentication and authorization. RNI council RNI council is advisory body and professional guarantee of RNI. The members of RNI council are nominated and withdrawn by the RNI Administrator – OZP MZ CR. The members of RNI are usually representatives of OZP MZ CR, KSRZIS and representatives of professional microbiological companies. The RNI is headed by elected chairman, vice-chairman and executive secretary. The RNI Council • Suggests the access rights and user roles to the Administrator • Suggests conceptual and content changes • Suggests the methodology and control relationships in the registry • Is involved in increasing the level of quality of each data in the database registry (by direct validation or
specifying the methodology explanation) • Suggest the aggregated output forms of presentation of the data from the registry for the professional society
and civilians • Controls the performance of the Administrator and Operator RIP – registry of Intensive care Registry of intensive care (RIP) was established by Ministry of Health Czech Republic for the purpose of using the unified information instrument for monitoring and evaluation of the intensive care in CR. The purpose and justification of the registry Intensive care registry was drawn up as an instrument of information support for introducing quality and effectiveness standards of the intensive care system in CR. Its origin was initiated for the purpose of creation and optimization of the system of acquisition, monitoring and evaluation of the given clinical, demographic and economic data as a necessary pre-requisite for standards definition for provision and financing of this type of medical treatment. The parties interested in creation of this registry were mainly the medical institutions of government, professional societies (Czech society of anesthesiology, resuscitation and intensive medicine), health insurance companies and it is assumed that the newly created regional centers will be also interested. The creation of this registry is a reaction of Czech Republic to the intensive medicine initiative of EC within EU. The purpose RIP is: • Registration of clinical cases of intensive care according to the standard definitions and criteria, optimization of
the methods of acquisition • Design of implementation and optimization of the structure of the monitored parameters, method of measuring
and evaluation the quality of intensive care and their reconciliation with European standards • Evaluation of the results of the system of intensive care, incl. The survival of patients and provision of these
data for the following domains
86
• Assessment of the input and output conditions for indication and termination of intensive care in various clinical states.
• Creation and maintenance of statistically representative data bases for : • Calculation of key indicators for quality and effectiveness of care • Application of DST methods in intensive care (mortality prediction, SMR etc.) • Accreditation, education and research in the area of intensive care • Location, implementation and optimization of economic aspects of intensive care Executive bodies of RIP and their competencies RIP Administrator RIP Administrator is department of health care of Ministry of Health Czech Republic (OZP MZ CR). The Administrator determines access rights to the registry. RIP Operator Countrywide registry operator is KSRZIS – Coordination department for departmental medical information systems, which is responsible for smooth operation of the registry, state of the database, data control, technical security of the data. It provides information technologies (HW, SW, communications), authentication and authorization. RIP Council RIP council is advisory body and professional guarantee of RIP. The members of RIP council are nominated and withdrawn by the RIP Administrator – OZP MZ CR. The members of RNI are usually representatives of OZP MZ CR, KSRZIS and representatives of professional companies. The RIP council is headed by elected chairman, vice-chairman and elective secretary. The RIP council: • Suggests the access rights and user roles to the Administrator • Suggests conceptual and content changes • Suggests the methodology and control relationships in the registry • Is involved in increasing the level of quality of each data in the database registry (by direct validation or
specifying the methodology explanation) • Suggest the aggregated output forms of presentation of the data from the registry for the professional society and
civilians • Controls the performance of the Administrator and Operator
87
Annex IX
e-Health care in Hungary, report no. 1 Hungarian health care is a traditionally under-financed public system. The financial reform of the social security system and a deep organizational reform of the institutions of health care are on the agenda of all consecutive governments of Hungary since the political changes of 1989. The ongoing activity and the development of its institutions - hospitals, outpatient stations and general practitioners - are jointly financed by the Social Security Fund, local governments, and projects of the central Government and directly by the public. Hungarian general practitioners (house doctors or "haziorvosok") operate their praxis in an entrepreneurial legal framework, whereby the income stems from the Social Security Fund and is approximately proportional with the number of patients who have chosen the general practitioner. This choice is free by legislation. As preceding strategy documents, the National Development Plan of 2002 (NFT) also stresses the importance of the modernization of electronic health care. It states that the efficient operation of the health care system requires the use of opportunities provided by information systems. Currently there is no systematic connection between the service providers, data is missing and incompatible. There is a need of an integrated sectoral system, in terms of communication, guidelines, protocols, central case studies and registration. The Plan attaches substantial resources to the development of electronic health care in Hungary. The development of the computer systems of hospitals and outpatient stations ("rendelointezetek") has begun in the 70s by a series of weakly co-ordinate local developments. Today many health care institutions, e.g. hospitals and clinics possess an isolated, but integrated information processing system. The offer is wide, since within the Hungarian software producing and informatics system integrating sector a wide range of providers of health care application systems has evolved. The core of these systems is the database consisting of the files of the patients. Some of these systems are run by the Informatics Departments of these institutions, other systems are outsourced, i.e. they have been developed and maintained by subcontractor companies. Outpatient health centres run by local governments have only recently introduced integrated software systems. But in many such institutions the files of the individual dispatched patients still have to be carried by nurses to the special departments. It is to be noted that hospitals, clinics and outpatient stations have to cope with a continuous shortage of nurse manpower - due to chronic underpayment of medical personnel. A survey made in 2001 by GKI Economic Research Inc. (http://www.gki.hu) has revealed that while all of the Hungarian outpatient centres possess and operate computer systems, only three-quarter of them is able to systematically lead the medical history of the patients by a suitable software system. Additionally - although the pace of technical development of Hungarian health care institutions is slow - since the 70s a growing number and an ever wider selection of specific medical devices is connected to a digital computer. This background is important for the interpretation of the appearance and usage of the Internet in Hungarian health care institutions. A survey conducted in 2001 by GKI Economic Research Inc., Westel Mobile Communication Inc. and Sun Microsystems Hungary Ltd. on hospitals, outpatient stations, general practitioners and other health care institutions has revealed the following facts. The survey has revealed that in September 2002 nine-tenth of hospitals and one-third of outpatient stations had an Internet access. Electronic communication between different institutions - e.g. between the laboratory attached to an outpatient station and a general practitioner - is rather an exception as a rule. Employees of hospitals and outpatient centres mainly use the Internet for searching for professional information, developing contacts with Hungarian and foreign clinics and scientific centres and libraries.
88
About one-quarter of the general practitioners are able to access the Internet from their cabinet, and some 4 per cent of the general practitioners operate their own website. General practitioners operating their own websites use this facility to spread medical information and consultancy. According to the survey the development of Internet access and webpage creation among general practitioners has a very positive tendency: in 2003 the respective indicators are expected to be doubled. For this professional segment the quickly provided patient-specific information offered by local outpatient centres is very important. Such information can help to formulate much needed early diagnoses. Local outpatient centres with Internet access are searching for the following information: • social security rules • laws, decrees and other regulations • professional articles • description of drugs Moreover, local outpatient centres with Internet access regularly make electronic contacts with the Ministry for Health, the Social Security Fund, other hospitals and laboratories. There are no local outpatient centres, which operate a service empowering patients to check in via Internet for a medical examination. There are many Internet based medical applications and contents available, some of them run by private firms, others by education institutes or benevolent organizations. In particular, a wide selection of medical journals, consultancy websites, product related sites with more or less open and covert advertisement purposes, and special, illness-related applications (e.g. high blood pressure related sites) are available in Hungarian language. These webpages compared to similar international sites are less interactive but they still represent a promising segment of the local Internet market. It is noteworthy that the possibility of online purchase of any type of medical drug is still missing. There is a wide selection of Government sponsored tenders in order to disseminate digitally based devices, methods and activities in the field of e-Health care. • There are regularly repeated Government tenders with the aim of providing direct support for doctors,
nurses, social care workers and others in the form of granting for them PCs, Internet access or ISDN connection cheaply or for free. In some case the co-financing of the tenders by private companies is available.
• A tender issued by the Ministry of Children, Youth and Sports in 2002 invites applicants to participate in the activity of e-health information dissemination. Applicants are invited to create web pages in the campaign aimed at drug prevention.
E-health care is also promoted by various professional organizations such as the Hungarian Foundation for Medical Informatics and the Hungarian Society for Medical Informatics.
89
Annex X
eHealth care in Hungary, report no. 2
Development and Implementation of Information Society Technologies and Activities in Hungary from 1996-2003 Sandor G. Vari1, Tamas Gergely2, Pal Simon3 1Sandor G. Vari M.D., VARIMED Ltd., Budapest, Hungary e-mail: [email protected] 2Prof. Dr. Tamas Gergely, Applied Logic Laboratory, Budapest, Hungary e-mail: [email protected] 3Dr. Pal Simon MD Ph. Sc., Senior expert in health informatics Templar Partnership Company, Budapest, Hungary, Adviser on Information Strategy in Ministry of Informatics and Communication, Hungary e-mail: [email protected] Historical review and major milestones in the progress of IST development and implementation in Hungary from 1996-2003 with the assistance of the European Commission Directorate General Information Society Technologies eHealth Unit
1. Introduction (Sandor G. Vari, Pal Simon)
Computers like the X-ray and stethoscope can be seen as clinical tools that provide physicians with improved expertise in solving patient management problems. As tools they enable us to extend our clinical information base, and they also provide facilities that improve the delivery of the health care we provide. Automation (computerisation) in the health domain will cause the computer to become a more integral part of health care management and delivery in 21st century. To understand how the computer assists those who deliver and manage health care, it is important to be aware of its functional capabilities and how we can use them in medical practice. The rapid technological advances in computers over the last two decades have had both beneficial and counterproductive effects on the implementation of effective computer applications in the delivery of health care in Hungary. The major controversial issue in the health care sector that, the rapid technological advances, which have produced a quantum leap in our ability to store and process information, have tended to make us overlook the need for effective computer programs which will meet the needs of patient care. As the 21st century began, those delivering health care (eg, physicians, nurses, pharmacists, administrators) need to become more involved in directing the effective implementation of computer applications that will provide the tools for improved information management, knowledge processing, and ultimately better patient care. Increasing use of the Internet by consumers in Hungary in general is being reflected in greater reliance on this medium for health information and health care. Patients are consulting the Web for medical information and resources from databases that are generally accessible to the public as well as physicians. In addition, interactions between physicians and patients via e-mail present an opportunity for greater efficiency in medical practice at this moment rarely used in Hungary. Though physicians have been somewhat reluctant to embrace this modality, it offers significant opportunities for enhancing patient care without undue liability. The general public also questions confidentiality and security of medical information. The number of health-related Web sites on the Internet is increasing in Hungary. Incorporating these sites into clinical decision support systems and other health care applications can significantly enhance the educational and instructional value of such systems.
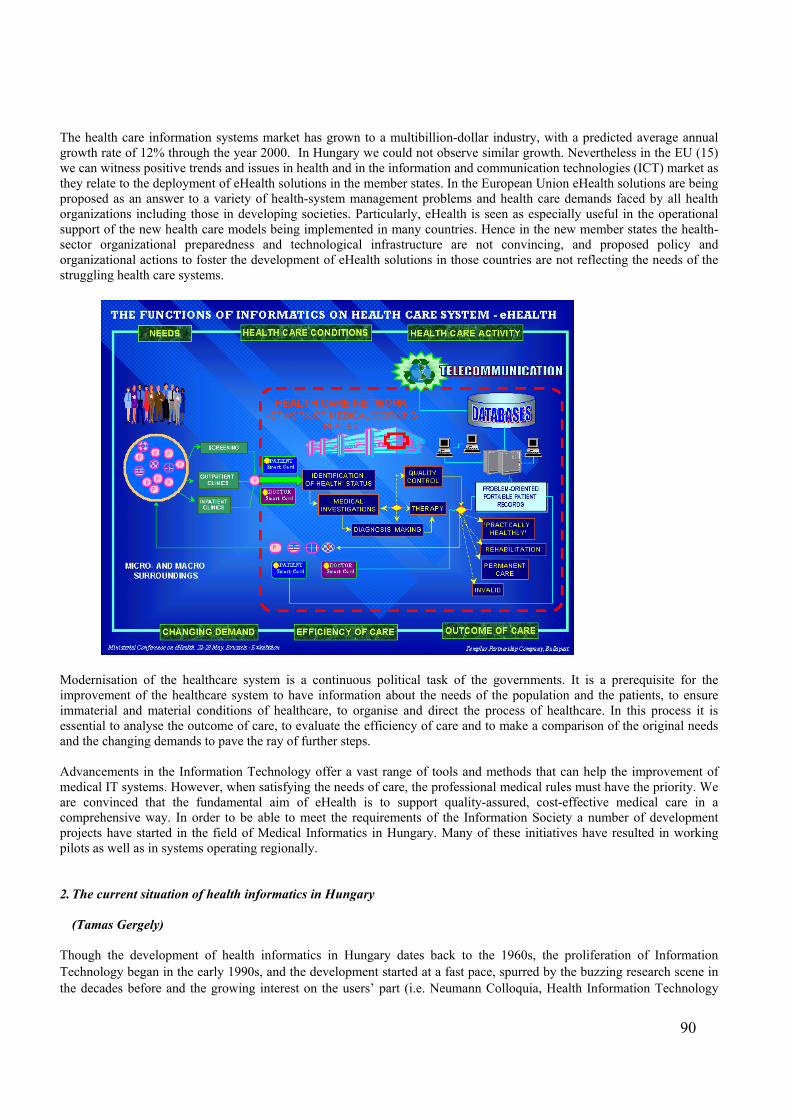
90
The health care information systems market has grown to a multibillion-dollar industry, with a predicted average annual growth rate of 12% through the year 2000. In Hungary we could not observe similar growth. Nevertheless in the EU (15) we can witness positive trends and issues in health and in the information and communication technologies (ICT) market as they relate to the deployment of eHealth solutions in the member states. In the European Union eHealth solutions are being proposed as an answer to a variety of health-system management problems and health care demands faced by all health organizations including those in developing societies. Particularly, eHealth is seen as especially useful in the operational support of the new health care models being implemented in many countries. Hence in the new member states the health-sector organizational preparedness and technological infrastructure are not convincing, and proposed policy and organizational actions to foster the development of eHealth solutions in those countries are not reflecting the needs of the struggling health care systems.
Modernisation of the healthcare system is a continuous political task of the governments. It is a prerequisite for the improvement of the healthcare system to have information about the needs of the population and the patients, to ensure immaterial and material conditions of healthcare, to organise and direct the process of healthcare. In this process it is essential to analyse the outcome of care, to evaluate the efficiency of care and to make a comparison of the original needs and the changing demands to pave the ray of further steps. Advancements in the Information Technology offer a vast range of tools and methods that can help the improvement of medical IT systems. However, when satisfying the needs of care, the professional medical rules must have the priority. We are convinced that the fundamental aim of eHealth is to support quality-assured, cost-effective medical care in a comprehensive way. In order to be able to meet the requirements of the Information Society a number of development projects have started in the field of Medical Informatics in Hungary. Many of these initiatives have resulted in working pilots as well as in systems operating regionally. 2. The current situation of health informatics in Hungary
(Tamas Gergely) Though the development of health informatics in Hungary dates back to the 1960s, the proliferation of Information Technology began in the early 1990s, and the development started at a fast pace, spurred by the buzzing research scene in the decades before and the growing interest on the users’ part (i.e. Neumann Colloquia, Health Information Technology
91
Travelling Seminars), and the funding reform. As a result, databases were developed and have been operating to grant a complete coverage of events at hospitals and then of all specialist care events. The standard report layout – which was top-of-the-range at the time – enabled the customised development of systems for hospitals and clinics to address the local needs and possibilities without disrupting the uniform reporting system. Obviously, the fulfilment of local needs led to a mixed result, and the ad hoc nature of funding brought about a lot of heterogeneous environments. Therefore, the existing systems – though operational on their own with varying levels of quality – cannot fulfil the requirements set for a nationwide information system. They typically operate with an administrative focus (i.e. the data is stored in alphanumeric files that are not very convenient for further processing) and have limited degrees of integration (with mediocre communications at the inter-departmental level and only minimum communications with financial and management systems). The National Health Insurance Fund Administration (NHIFA) possesses an information system and the IT devices that enable it to meet its current mandatory tasks; it also has the staff to operate them – yet the situation cannot be regarded as satisfactory. It cannot, because a great part of its currently used IT systems was designed to deliver individual functions and operate in an island mode as demanded by the situation at hand. Data communication between various levels of service (primary health care, outpatient specialist services, inpatient care) is not reliable, in fact, rather uncertain and cumbersome; and the systems are both difficult and expensive to update. Meeting the challenges posed by technological advancement is significantly hindered by the absence of tangible and intangible resources, as well as the limited nature of development. This is one of the reasons why the development projects launched end up on their own. The last major investment project also supported by the state in the health sector took place in 1997-99 (World Bank Project for Hospital Management Information Support System). Since then the individual hospitals have spent varying amounts toward IT projects. The functionality of a great part of the existing systems is not fully utilised. It should also be noted that the sector did not promote the roll-out of the health information systems implemented in the framework of IT R&D programmes. The systems installed in the past five years or so have practically used the same technology, whilst Information Technology has registered ever-faster advancements in the same period. All in all, we may say that the rate of technology development decreased relative to past levels, and that this setback has resulted in existing systems that look as though they predate the ‘Internet Boom’ – but in practice, they do not even fully utilise the capabilities of that legacy technology. The network connectivity of healthcare institutions (i.e. Internet access, secure communication network) is far from the desirable level. International statistics suggest that the web pages offering health-related information rank among the hottest sites. However, there are few websites in Hungary to offer high quality but easy-to-understand information with certified content to patients – despite the fact that there are thousands of websites addressing health issues.
Specifics regarding the current situation
The prevailing attitude does not regard information and knowledge as an asset, and does not consider Information Technology as a production tool.
The information deficit of the public, the profession and decision-makers compromises the quality of decisions regarding the health status, social position of individuals and the public at large, and leads to less substantiated decisions concerning the care provision systems:
The patients or customers often do not know where to go with their complaints, and have no information about the quality and availability of services.
Healthcare staff does not have electronic access to leading international knowledge bases. Instead, they are to remain up-to-date in medicine using outdated course books, guidelines published on paper, dozens of scientific periodicals, and the often distorted information received from pharmaceutical sales agents; there are hardly any decision support systems at the office.
The prerequisites for sectarian policy decisions to be scientifically substantiated and based on credible data are scarcely available.
The tools are mostly obsolete and the systems only offer limited interconnectivity, because of the deficiencies in technical and organisational conditions, and co-operation.
The Internet penetration is low, and access to the websites that would satisfy the information needs of the public and the requirements of professionals is both costly and limited.
The application of Hungarian IT research and development results is unresolved. The promotion and management of implementing up-to-date technologies in the sector in a co-ordinated fashion is
unresolved.
92
The sector’s information management situation
The information regarding health with the different players at various levels is currently amassed in an island mode, with very little of that information gets processed. The vast majority of the information gets deposited – some in data banks but most in archives – in a form that does not support post-processing. Utilising the sector’s information assets requires knowledge management, whose implementation is only at an embryonic stage in the sector. In order to organise and implement forms of care around the needy – as such care is likely to play an ever increasing role in the health organisations of the future – it is necessary to grasp the health status of an ill person in a complex way, and to tailor therapy and other services to the individual’s needs. The foregoing requires the efficient implementation of the data-information-knowledge flow, where adequate IT support is essential. It is clear from the assessment above that the elimination of pitfalls in this field requires more than Information Technology or reorganisation in the sector – in fact, it is only possible through concerted action by the relevant Ministries.
3. Implementation and use of the IST by hospitals/doctors today
(Tamas Gergely) Legal environment of e-Health sector There is a complex legal environment regulating the handling of health data, an environment in which direct and indirect legislation may apply at various levels in combination. The following is a description of the key elements in this environment, followed by a list of highlighted areas where progress seems important. The level of direct acts includes: • Act LXIII of 1992 on the protection of personal data and the publicity of data of public interest, and • Act XLVII of 1997 on the handling and protection of health data and related personal data. Mandatory data reporting – indirectly involving the handling of data and the applicable provisions – is regulated by:
• National Statistical Data Collection Program (NSDCP), • the Health Act, • the Statistics Act, • the applicable funding regulations, • the annual NHIFA budget, • the acts and regulations prescribing data collection and storage regarding the operation and tasks of National Public
Health and Medical Officer’s Service (NPHMOS), • other regulations (such as Ministry of Health Decree 24 of 1999 (VII. 6.) on the reporting procedures for certain
timorous diseases) Act XXXV of 2001 on electronic signatures must also be mentioned as an indirect piece of legislation whose implications for this field are not quite clear today.
It is generally true for the legislative situation that this issue is regulated – very appropriately – independently from the technology that is used to handle the data. In other words, the provisions do not vary depending on whether paper or an electronic data carrier is used. However, the legislation does not adequately reflect the attitude change necessitated by the propagation of electronic data management. This mainly manifests itself in focussing data protection on the physical storage of data, though the ‘place of data’ or ‘making copies’ are neither decisive concepts in digital data management, nor can they be interpreted well (e.g. simply displaying the data on a screen requires the making of a copy). The physical location of data must be replaced by access authorisation. This would also resolve a current issue, i.e. physicians currently violate the law by taking home the data in their own memory from the hospital.
It is not a technological but another attitude-related issue that the current legislation does little to define the mandatory minimum content of basic documentation – it just prescribes the data items to report. Due to the lack of clarity regarding basic documentation, some reporting requirements may occasionally contradict each-other. The imprecise regulation of basic documentation makes it to hard to improve the quality of data any further.
93
It is important to clarify the notion of use linked to a purpose, because the current definitions cannot be interpreted strictly for IT systems. For instance, it is impossible to decide what data is necessary and what is not necessary to achieve the goal of a consult.
The use of Social Insurance Numbers is regulated by specific rules under taxative legislation with reference to purpose, and the rules need to be amended all the time. Currently, it is a difficult issue to link updated demographic databases with the Social Insurance Numbers for applications like the TB screening system. The recording of deaths in the National Cancer Register is another unresolved issue. By virtue of Ministry of Health Decree 24 of 1999, the Central Statistical Office (CSO) should report deaths, but the CSO does not have the Social Insurance Numbers and cannot release any information about private persons.
A more reasonable specification should be provided regarding the mandatory data preservation period. The current provision does not specify the minimum retention period, but it prescribes that patient charts and discharge summaries must be preserved for exactly 30 and 50 years, respectively, which is practically unfeasible.
The data collection practices of certain professions and national institutions must be mapped and harmonised with the regulations – much as those practices are useful from a professional point of view, they are legally unresolved.
For reasons that have to do with history, the data content (lists, codes, code systems, classifications, nomenclatures, etc.) of the annexes to the acts, regulations, and rules is inconsistent, and does not allow for the development of a uniform data model to support the regulations electronically, i.e. the eGovernment initiative.
The Information and Communication Technology environment of the Health sector
A few features of healthcare and IT in Hungary • poor process control
• attempts to implement electronic patient records
• development driven by reporting requirements set by the authorities
• low integration levels
• development projects in island mode
• absence of knowledge-based systems
• absence of care management systems
• insufficient resources for ongoing development, innovation, regulation and funding
The development and current situation of health information in Hungary are determined by the reporting of funding data to the National Health Insurance Fund Administration in an electronic form. Although that defined the health-related data content concerning the different forms of care (MBDS2) and established the national code system, the information system thus developed is inappropriate as yet for the sufficiently detailed and true-to-life representation and storage of the medial content collected about the patients, due to the substantial simplification measures used at present. Due to the above reasons, the data structure of many patient administration systems hardly provide any more than what is mandatory under law, and the funding-centred changes in the central code systems have a major impact on the medical content of patient records, occasionally causing major distortions and generally truncating the medical content.
It is also typical of the sector that the documentation of patient care events is supported by separate subsystems. As a consequence, application integration is patchy, often even the traditionally stand-alone diagnostic systems are not integrated yet (general chemistry and microbiology laboratories). The medical functions and data content missing from the basic systems are mostly covered by stand-alone applications.
The same applies to support systems – such as the pharmacy module or financial management module. There is no computer support for nursing care activities either. The actual costs of care cannot be allocated to the individual cases and the expenditures of the care provider do not combine automatically to make up a patient bill including all cost elements.
The result of the above is that the information generated at various levels cannot encompass the full spectrum of care. For many systems, even the aggregation of available data into management information that goes beyond a case mix analysis and other listing functions represents a problem.
2 Minimum Basic Data Set
94
Development projects typically do not implement the desired platform-independent and vendor-independent solutions. Co-operation with the industry is hindered by the absence of mutually accepted standards, and the ongoing dynamic changes in the legal environment. Consequently, product upgrades are not seamless, which may give rise to disputes. It is partly due to this that healthcare institutions are exposed to the suppliers who offer ‘integrated solutions’.
National projects were launched in the past to remedy the typical situation outlined above, such as the Hospital Management Information Support System (HMISS) funded by the World Bank, which entered the implementation stage in 1998. The projects covered 15% of inpatient care – based on the number of hospital beds – opened the markets to complex IT systems, and contributed to the enhancement of the know-how of IT experts and users. However, the application of results has been limited by the absence of central resources for further development – in terms of the internal integration of the systems implemented, and the connectivity of additional sites.
Electronic communication between healthcare providers remains unresolved, which currently disables the implementation of a uniform ePatient Records System. The importance of regulation is highlighted by the fact that the implementation of the uniform ePatient Records System is hindered by the absence of an approved standard to ensure vendor-independent data communications between the middleware of the local systems.
The only example of uniform nationwide electronic communications is the healthcare providers’ data reporting system to the commissioners, a system that has been in operation for nearly a decade. However, neither the content nor the implementation of this system supports medical purposes.
Local development projects have been implemented over the past few years, achieving significant progress in the interconnection of various levels of care (e.g. hospitals and family practitioners) and in horizontal co-operation (e.g. patient administration within a group of hospitals) – and might even serve as a starting point for a solution that covers the whole sector. However, the systemic application of local development results would require nationwide co-ordination. This could ensure that the standards selected, naturalised, utilised, and co-ordinated with the knowledge representation models (e.g. with medical ontology dictionaries) developed simultaneously, to support the development of uniform nationwide recommendations.
The hardware infrastructure shows a lot of heterogeneity. Nearly two thirds (64%) of the IT assets owned by the healthcare institutions (including hardware and software) are more than three years old. This ratio is 66% for PCs and terminals, 67% for software, and 52% for mainframes, networks and accessories. Needless to say, the launching of a development programme would mean that two thirds of the ICT tools should be replaced, due to obsolescence.3
There are some institutions where the penetration of workstations is significant even by international standards. But replacement due to depreciation is a problem for the majority of even those sites. The intranet is generally limited to just one site, and upgrades represent a problem in this field. Network interconnectivity is not generally unavailable (Internet, extranet) even within an institution with multiple sites. The majority of the systems with Internet access use data communications solutions that do not ensure adequate privacy. For the above reasons, the Internet penetration of the health sector is low, so users do not have sufficient access to the information, education, and Information Technology opportunities offered by the new medium.
Health and healthcare on the Internet
The number of Hungarian websites related to health status and healthcare has grown very rapidly in recent years. The first web pages providing content services and pursuing portal ambitions have emerged and are apparently developing. However, their numbers and importance, as well as the volume of content, are less than desirable. There is a major backlog in services with ‘HON’ (Health on the Net’) certification, an international voluntary certification system designed to guarantee the reliability of the information made available through the websites. At the same time, there are many websites purporting to be scientific but actually featuring ‘parascientific’ or fake information.
Institutions handling healthcare information
The Centre for Healthcare Information — GYÓGYINFOK of Ministry of health, Social and family Affairs (MoHSFA) was established as a stand-alone budgetary organisation in 1974. It is the basic organisation, methodology and scientific research institute of the Ministry of Health in health information and economics. Its fundamental tasks also include data acquisition and processing on behalf of the Health Insurance system. Its role in developing and operating the funding system for healthcare organisations is governed by regulations (government and ministerial regulations).
3 Source: ‘The IT tools with an investment cost of above 50,000 HUF gross in the possession of the healthcare institutions
(reporting to the Institute for Medical and Hospital Engineering)’, 2001
95
The National Institute and Library for Health Information (MEDINFO) evolved out of an institution that had served as a national medical library earlier on. It started to focus on IT when the computer-based literature research systems emerged. Currently, its key task is to provide complex information about the Hungarian healthcare system, including traditional library information services, international health statistics, a knowledge centre function for the sector, the development of a Health Data Warehouse, and the implementation of authentic public electronic registers. Its organisational structure keeps changing as its tasks change. In that context, its IT unit has become stronger.
The National Health Insurance Fund Administration (NHIFA) is a central public administration organisation reporting to the Government. It has a nationwide mandate, and manages the Health Insurance Fund as the central organisation responsible for social insurance. NHIFA is a fully empowered budgetary organisation in the social insurance field with its own budget. It was established by the Government acting on authorisation by Parliament on 12th June 1993. The Health Insurance Fund, i.e. the central organisation in charge of health insurance, is supervised by the Government through the Minister of Health Social and Family Affairs. NHIFA is responsible for maximising the health gain of insured people and for managing health hazards by delivering and commissioning services that allow for the maintenance, restoration and improvement of health, for the compensation of wages lost temporarily or permanently, and for promoting return to work. NHIFA – as the managing body of the Health Insurance Fund – operates the health insurance system by fulfilling the fund management tasks, and actively participates in the maintenance of the contribution system, eligibility rules, and the services of the healthcare system. NHIFA and its administrative organisation, as well as service providers, collect and register the following data:
• Administrative certification of the Social Insurance Numbers, issuance of Social Insurance Cards, and the related registration tasks.
• NHIFA signs and registers the funding contracts regarding the healthcare services as specified by law. • NHIFA adjudicates books and registers cash health benefits.
Healthcare providers, retail pharmacies and medical device distributors maintain the registers prescribed for funding and accounting purposes regarding the patients treated, the services delivered, and medication provided. They report data under their funding contracts to NHIFA regarding the healthcare services that serve as the basis for reimbursement.
So NHIFA processes, adjudicates and analyses growing volumes of data that is also becoming more and more important. There have been efforts for years to implement electronic data communications between the networks of NHIFA, healthcare provider and pharmacies. The development of communications between the funding organisation and service providers is a common interest whose realisation requires central co-ordination.
Scientific organisations of health informatics
One of the scientific organisations in Hungary’s health informatics field, the Biomedical Section of the John von Neumann Computer Society, was established in 1968. This was among the first forums established in Europe. The international professional community recognised the achievements of Hungarian researchers at an early stage, which is one of the reasons why the Section became a member of the international organisation (International Medical Informatics Association, IMIA) and the European organisation in this field (European Federation for Medical Informatics, EFMI). The other scientific forum in Hungary, the Hungarian Medical Informatics Association, was established in the early 90s, and has assumed a major role in the modernisation of the IT field. The two associations have held their annual conferences in turns since the 80s, with 100-150 participants. These events have become the scientific forums of the health informatics field in a narrow sense (Neumann Colloquia and HMIA Travelling Seminars). In addition to those organisations, training and valuable workshops take place in some universities. There are also some technical and scientific associations dealing with borderline domains (e.g. MATE Medical Engineering Department). Unfortunately, however, the values of scientific and training organisations do not receive recognition, one reason for which is the absence of a policy concept.
3. Review of the National and EU RTD activities and implementations
(Simon Pal, Sandor G. Vari) The purposeful research and development activities on health (medical) informatics started more intensive in the middle of the nineties in Hungary. The first episode of RTD on the territory of information and communication technology (ICT) was
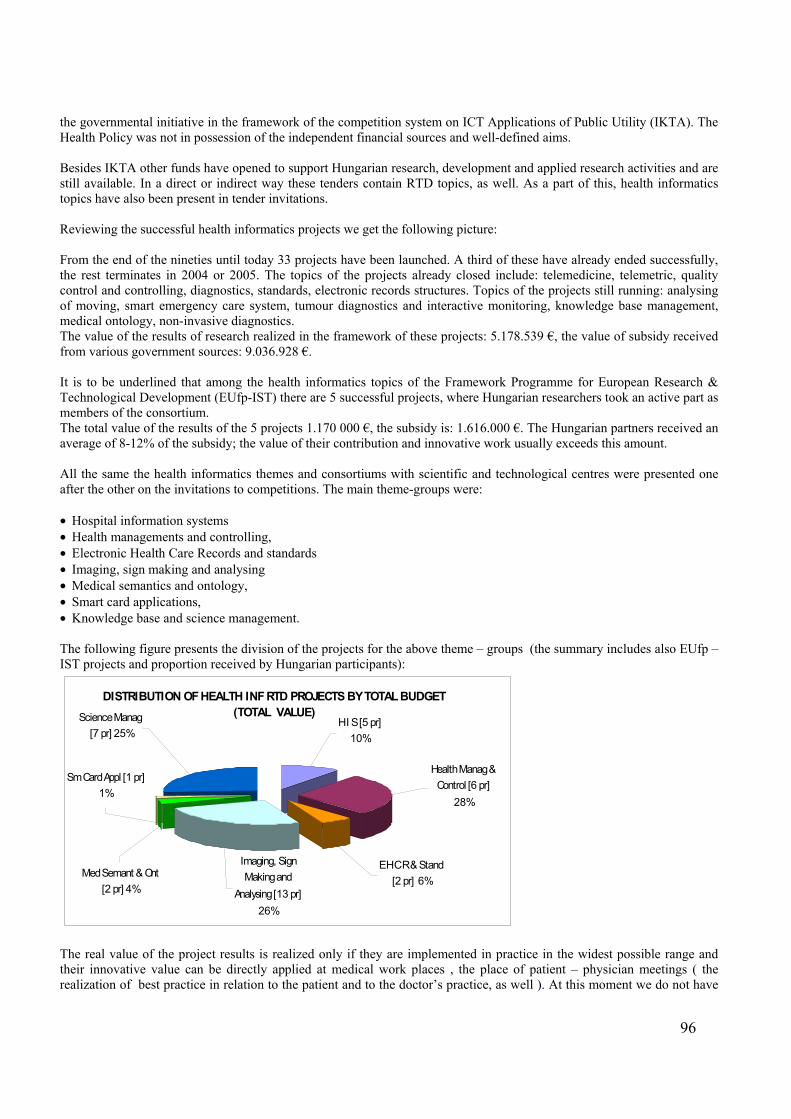
96
the governmental initiative in the framework of the competition system on ICT Applications of Public Utility (IKTA). The Health Policy was not in possession of the independent financial sources and well-defined aims. Besides IKTA other funds have opened to support Hungarian research, development and applied research activities and are still available. In a direct or indirect way these tenders contain RTD topics, as well. As a part of this, health informatics topics have also been present in tender invitations. Reviewing the successful health informatics projects we get the following picture: From the end of the nineties until today 33 projects have been launched. A third of these have already ended successfully, the rest terminates in 2004 or 2005. The topics of the projects already closed include: telemedicine, telemetric, quality control and controlling, diagnostics, standards, electronic records structures. Topics of the projects still running: analysing of moving, smart emergency care system, tumour diagnostics and interactive monitoring, knowledge base management, medical ontology, non-invasive diagnostics. The value of the results of research realized in the framework of these projects: 5.178.539 €, the value of subsidy received from various government sources: 9.036.928 €. It is to be underlined that among the health informatics topics of the Framework Programme for European Research & Technological Development (EUfp-IST) there are 5 successful projects, where Hungarian researchers took an active part as members of the consortium. The total value of the results of the 5 projects 1.170 000 €, the subsidy is: 1.616.000 €. The Hungarian partners received an average of 8-12% of the subsidy; the value of their contribution and innovative work usually exceeds this amount. All the same the health informatics themes and consortiums with scientific and technological centres were presented one after the other on the invitations to competitions. The main theme-groups were: • Hospital information systems • Health managements and controlling, • Electronic Health Care Records and standards • Imaging, sign making and analysing • Medical semantics and ontology, • Smart card applications, • Knowledge base and science management. The following figure presents the division of the projects for the above theme – groups (the summary includes also EUfp – IST projects and proportion received by Hungarian participants):
DISTRIBUTION OF HEALTH INF RTD PROJECTS BY TOTAL BUDGET (TOTAL VALUE)
Imaging, Sign Making and
Analysing [13 pr]26%
Med Semant & Ont [2 pr] 4%
Sm Card Appl [1 pr]1%
Science Manag [7 pr] 25%
H I S [5 pr] 10%
Health Manag & Control [6 pr]
28%
E H C R & Stand [2 pr] 6%
The real value of the project results is realized only if they are implemented in practice in the widest possible range and their innovative value can be directly applied at medical work places , the place of patient – physician meetings ( the realization of best practice in relation to the patient and to the doctor’s practice, as well ). At this moment we do not have
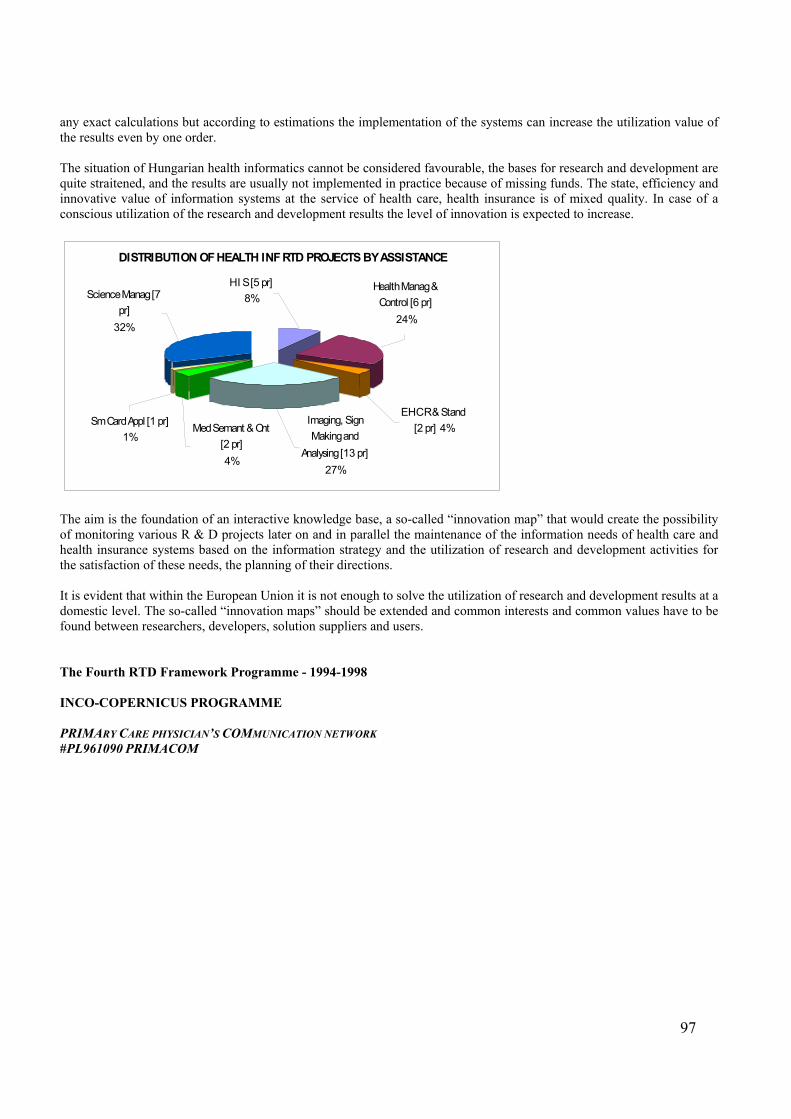
97
any exact calculations but according to estimations the implementation of the systems can increase the utilization value of the results even by one order. The situation of Hungarian health informatics cannot be considered favourable, the bases for research and development are quite straitened, and the results are usually not implemented in practice because of missing funds. The state, efficiency and innovative value of information systems at the service of health care, health insurance is of mixed quality. In case of a conscious utilization of the research and development results the level of innovation is expected to increase.
DISTRIBUTION OF HEALTH INF RTD PROJECTS BY ASSISTANCE
Health Manag & Control [6 pr]
24%
H I S [5 pr] 8%
E H C R & Stand [2 pr] 4%
Imaging, Sign Making and
Analysing [13 pr]27%
Med Semant & Ont [2 pr]4%
Sm Card Appl [1 pr]1%
Science Manag [7 pr]
32%
The aim is the foundation of an interactive knowledge base, a so-called “innovation map” that would create the possibility of monitoring various R & D projects later on and in parallel the maintenance of the information needs of health care and health insurance systems based on the information strategy and the utilization of research and development activities for the satisfaction of these needs, the planning of their directions. It is evident that within the European Union it is not enough to solve the utilization of research and development results at a domestic level. The so-called “innovation maps” should be extended and common interests and common values have to be found between researchers, developers, solution suppliers and users. The Fourth RTD Framework Programme - 1994-1998 INCO-COPERNICUS PROGRAMME PRIMARY CARE PHYSICIAN’S COMMUNICATION NETWORK #PL961090 PRIMACOM
98
In a public-private partnership, two regions in Hungary and Slovenia have established Regional Health Care Network for exchange of routine messages between professionals. Discharge letters are now daily exchanged between Hospitals and General Practitioner. PRIMACOM have used European standards, developed by CEN TC 251, for exchange of medical data and experience by implementing Regional Health Care Networks from Denmark and Italy. PRIMACOM has paved the way for establishing Regional and National Health Care Networks in Hungary and Slovenia.
Setting the Scene
On average, each hour of consultation with a general practitioner (GP) results in more than one message to another part of the health care sector. This generates a large flow of routine messages, such as prescriptions, referrals, examination requests, discharge letters and laboratory results. The accurate, fast and safe communication of information has, therefore become decisive to the cost, quality and patient service of the entire health service. Until now, there has been very little attention paid to the development of systems, which support the sharing of information between members of the multi-disciplinary team in health care.
Approach The aims of the PRIMACOM project have been to establish Regional Health Care Networks in Hungary and Slovenia based on European standards and experiences from the European Communities. From the beginning of the project it has been planned to implement one standard for electronic exchange of discharge letters between Hospitals and General Practitioners clinic. Later on it is easy to expand with new messages for exchange of laboratory request and reports, referrals, prescriptions, reimbursement claims and many more. Results and Achievements
These goals were achieved by providing the necessary tools and applications (handbook, implementation guidelines, trainingguidelines, expertise), establishing links between software companies in Denmark, Italy, Hungary and Slovenia establishing electronic links between health care professionals, and using structured messages communication to ensure re-use of data in different systems building on European
standards and existing infrastructure and systems in the regions
Conclusions and Plans for the Future PRIMACOM provided valuable experience for all participants in the project. Health care professionals came in contact with health care delivery of the future, in which communication will be an integral part of the care process. They became more prepared to, and are now better able to see, the possibilities of the future. The experiences and expertise needed for the development of regional health care network has been carefully documented. PRIMACOM has documented that once a technical solution has been developed it is possible to transfer the knowledge across borders and promote establishment of regional and national health care networks.
99
The positive experiences from everyone involved in PRIMACOM will be certainly be disseminated to others. The technical and standardisation work achieved in PRIMACOM will make it easier for software industries to adopt information exchange, and adapt these in other regions. Finally, it cannot be stressed sufficiently that all these results are valuable irrespective of the technology used. All standardisation and consensus activities, and all experiences gained will remain valid whether EDIFACT, HL7, XML, or any technology emerging in the future, is used.
Contact Details
Project Name: PRIMACOM – Primary Care Physician’s Communication Network Research Area: Telematics Applications for Health – INCO COPERNICUS Timescale: 01.12.97 - 30.11.99 Budget: Overall cost: ECU 436.366 European Commission contribution: ECU 300.000 Keywords: Healthcare, communications, integration, standardisation, Regional Health Care Networks. Key Project Participants: Danish Centre for Health Telematics, County of Funen (DK) Ramboll (DK) TSD-Projects (IT) VARIMED (HU) FADAM (HU) FAGOR (SI) Project Co-ordinator: Morten Bruun-Rasmussen Tel:+45 66 13 30 66 Fax:+45 66 13 50 66 E-mail: [email protected] Project URL:http://www.primacom.dk INTERactive HistoPATHology Consultation Network #PL 96 1121 INTERPATH SHORT DESCRIPTION The INTERPATH project enabled Hungarian and Russian pathologists and surgeons to perform site experimental casting of histological and cytological multimedia documents between hospitals and university institutes of pathology. INTERPATH promoted the use of telemedicine over Central and Eastern Europe and facilitated dissemination of spectral images that can’t be generated only in a few places. This could be a model for further development of a regional and nation wide telepathology network joining to European network. SETTING THE SCENE A considerable number of studies have been made on diagnosis and prognosis reproducibility in histopathology with respect to WHO classifications. In the overall medical strategy, improvement in the quality and reproducibility of microscopic examinations is of continuous concern. It has come to the point where pathologists are eager to accessing the imaging microscopy, remote control of a microscope, as well as image transmission via ISDN lines. The purpose of the INTERPATH project was thus to demonstrate the use of ISDN network for local and international transmission of both high-resolution digital images (pathology) and teleconsultation in real-time.

100
Pathology is one of the most demanding computer areas of medicine and, as a result, diagnostic histo-pathologists have often been at the cutting edge of computer literacy. The majority of laboratories use HIS to issue and store pathology reports. Many of these systems provide the diagnostician with the ability to retrieve reports and cases using a code-based system such as SNOMED, but more advanced computer facilities that might assist the pathologist in the diagnosis or interpretation of a case are often lacking. In recent years, advances in computer technology have begun to have a much wider impact on the practice of medicine and newer technologies are beginning to find their way into the reporting area. The INTERPATH project covers some of the recent and emerging advances in IT that have the potential to revolutionize the practice of diagnostic histopathology and which were partially developed in the European Telematics for Healthcare project called EUROPATH, (HC 1038). Owing to INTERPATH, the ntechnology has been transferred into the participating Central and Eastern European Countries (CEEC). Diagnostic support systems aim to help reaching a diagnosis and yet none have been incorporated in widespread routine practice. During the project partners were considering where the impact of information technology and imaging spectroscopy in the future could be useful ? Perhaps the most obvious answer is that for the majority of pathologists, most diagnoses are straightforward and can be reached without requiring any computer-based support system. The benefit of IT for most pathologists thus come from enhancements to the reporting process; improving efficiency and accuracy and accessing an expert at a distance for difficult or rare cases. It must be ensured that there is good standard coding of the diagnosis, and that any new information available on the clinical condition of a particular patient it is made available to the pathologist. Additionally, imaging spectroscopy has the potential to greatly enhance practice, but at present the few available systems require prolonged training for both users and computers and spectral images must be combined with good conventional images. However, it is clear that as a new diagnostic method like multispectral imaging is introduced, pathologists will move even further away from the simple recognition of morphological patterns, which are inevitably subjective, although they have been the gold-standard for several centuries in the daily practice. Until we reach the stage of purely molecular diagnosis, seeking expert opinion through telepathology and multispectral imaging systems is likely to be of more value, than lengthy automated decision support. APPROACH During the 3rd and 4th Framework programme, the IMPACT and the EUROPATH projects have developed a telepathology system using the commercially available Integrated Services Digital Network (ISDN). The main software and hardware elements of INTERPATH systems were from EUROPATH project and it included: Axioplan 2 workstations, a SAMBA software for simultaneous transfer of image, voice and data, and a data bank for storage of patients' data and microscopic images. The pathology multimedia workstations were then interconnected in Hungary to develop a pathology consultation network, HugaroPath including : the 1st Institute of Pathology and Experimental Cancer Research, the 2nd Institute of Pathology, the Transplant and Surgery Clinic of Budapest, the Szent Györgyi Albert Medical University, Institute of Pathology of Szeged, and the Central Hospital Ministry of Interior in Budapest. The following step was to use of telecommunication via ISDN line and satellite in order to transmit pathology information from Medical University of Semmelweis in Budapest, to pathologists and clinicians at Institute Albert Bonniot, Faculté de Medicine, Grenoble and to the Moscow State University. Pathologists and surgeons examined the validity and accuracy of telepathology services in the histological diagnosis of biopsy specimens from transplanted kidney and liver using traditional imaging techniques. Then, given the assistance of Laser and Medical Technology Institute in Berlin, the spectral imaging techniques were implemented and tested. ACHIEVEMENTS During this project, the use of medical multimedia image transmission in pathology and telepathology was applied mainly;
To enable rapid diagnosis of kidney and liver biopsies during organ transplant using spectroscopic imaging method integrated into a multimedia imaging microscope.
To establish on-line and off-line consultation with experts of Joseph Fourier University Grenoble, Albert Bonniot
Institute and Moscow State University, Department of Pathology, on difficult and rare cases of histopathology and cytopathology.
THE INTERPATH consortium developed the first international telepathology consultation system in the Central and Eastern European Countries (CEEC) and in the new independent States (NIS). This project included imaging microscope, imaging spectroscopy and communication networks. Laser und Medizin-Technologie GmbH, Berlin
101
(LMTB) has developed the spectroscopic imaging system. The imaging and spectroscopic imaging systems evaluated with reference to conventional practice. Tele-consultation and peer discussions were performed in difficult domains of diagnostic activities of organ transplantation for optimal use of expertise from LMTB, SOTE, Albert Bonniot Institute, Joseph Fourier University Grenoble and Moscow State University. This telepathology project was successfully established with the assistance of the EUROPATH project : “European Pathology Assisted by Telematics for Health”, (HC 1038) driven by the Comission of the European Union (DG XIII) in the 4th framework Programme : Telematics for Health Care. The INTERPATH consortium developed telepathology network which can be combined with spectroscopic imaging and successfully used for expert consultation of intra-operative frozen sections, panel discussions of difficult carcinoma cases, and in assistance to organ transplantation. Contact Details Project name: INTERPATH INTERactive HistoPATHology Consultation Network Reasearch Area : Tele-consultation for health professionals and health organizations. Timescale : 01/01/98 – 30/06/2000 Budget: Overall cost: 360 725 Euro EU Commission contribution: 246 000 Euro Keywords : Telepathology – Spectral Imaging Remote Consultation – Diagnostic pathology Key project participants : Laser und Medicine Technologie GmbH (DE) VARIMED Ltd., (HU) Université Joseph Fourier (FR) Semmelweiss Medical University (HU) TriTech GmbH (DE) Moscow State University (RU) Contact Person: Pr. Gerhard MULLER Tel: +49 30 844 9230 Fax:+ 49 30 844 9239 E-mail: [email protected] REgional and International Integrated Telemedicine Network for Medical Assistance in End Stage Diseases and Organ TRANSPLANT Project. www.varimed.hu HC 4028 RETRANSPLANT
SUMMARY
The RETRANSPLANT project aimed to develop and install telematics tools to bridge the various and geographically dispersed institutions playing a role in the complex process of organ collection from a donor and transplantation into one or several recipients. The generic model used was kidney transplantation and the information and communication technologies developed so far networked dialysis centers, organ transplant surgery clinics, tissue typing laboratories, organizations coordinating recipient to
102
donor selection, and other health care facilities for organ transplant services in the Central and Eastern European Countries. SETTING THE SCENE
Organ transplant is an increasingly successful and viable treatment for patients suffering from chronic end stage diseases and from irreversible failure of organs such as kidney, liver and heart. It offers new life to thousands of people in Europe. In response to the steeply rising demand for transplantation, both the number of transplant centers and the number of patients on waiting lists have grown rapidly. Graft rejection is still a major problem in kidney, liver, and heart transplantation. The financial cost of organ transplant made it imperative to develop health telematics tools for the patient selection and matching and early identification and treatment of graft rejection. The fast and efficient communication between the many medical actors is both a paradigm and a challenge for health telematics.
In Europe, as a rule, donor organs are matched to recipients by national or multinational organ-sharing organizations. For example, EUROTRANSPLANT, serves medical institutions in Germany, Austria, and the Benelux states, HUNGARO-TRANSPLANT in Hungary, and SLOVENJA-TRANSPLANT in Slovenia. There is an increasing demand to improve the operational effectiveness and inter-operability of these entities at both the national and international levels having in mind the on-going integration of European countries. APPROACH The starting point is the implementation of a networked electronic patient database playing a pivotal role to combine information from transplant waiting list, donor-recipient immuno-logical typing, organ allocation, and patient selection in the Czech and Slovak Republics, Lithuania, Hungary, Slovenia, and Poland. Such networked facilities for the final Recipient to Donor Selection is required for an optimal use of available organs and tissues over Western and Central Europe so that any potential donor in any country might become matched against a recipient anywhere and vice versa. Kidney transplantation was selected as a generic model since it is the most frequently transplanted organ and follows well established guidelines. Recipients are well identified in Dialysis centers and the whole health telematics process could start with The DialysisCard and TransplantCard to be seen as an electronic identification support with additional data storage and management tools for dialysis and transplantation candidates at least in Hungary and Slovenia. The adopted communication model thus allows different types of PC-based workstations in several points of care to exchange data with these active memory Smart Cards that are a secure and updated channel to relevant medical information. RESULTS AND ACHIEVEMENTS The most complex aspect was the development and installation of an Electronic Medical Record system at the organ transplant centers in Hungary (Budapest, Szeged), and Slovenia (Ljubljana) that can be accessed through the web and that compiles all clinical records including diagnostic codes (ICPC/ICD10), drugs, procedures, investigations, laboratory tests, etc. in the working language. To ensure standardized and consistent information that must be mobilized and checked in a very short time, the indexing had to be updated centrally and on a regular basis to ease and secure the data exchange and consultation about the patients from one health care facility to another. The major integrated achievement of the project was to create a continuum between the patients and health professionals SmartCard, the Electronic Patient Record shared through Internet and a Transplant Information Portal including several web-based services that are actually used by the concerned healthcare actors. CONCLUSIONS AND PLANS FOR THE FUTURE With respect to the Health Telematics Application of the 4th Framework Programme, the RETRANSPLANT portal and connected resources can serve as a very concrete and realistic basis for any further step toward actual use of ICT in any medical activity requiring multiple access over regional, national and international networks. The take-up of the technology by the medical actors will be strengthen in the framework of the BePrO take-up action supported by the EU Commission. The Transplant Information Portal is on the way to be distributed to any potential users. The major advantage is that, owing to the open-source technology used and the low cost for implementation, the translation into any regional language and the implementation in any hospital environment are easy, feasible and of obvious cost benefit to the patients and the health professionals. Nevertheless, it remains questionable, whether the business model could prove its strength within the fast evolving picture of medical informatics that is slowly abandoned by the large companies in Europe as a consequence of the inability of European institutions to establish a clear health strategy and policy.
103
CONTACT DETAILS Project Name: RETRANSPLANT, Regional and International Integrated Telemedicine Network for Medical Assistance in End Stage Disease and Organ Transplant Project. Research Area: Healthcare – Organ Transplant – Medical Information Portal Timescale: 01.10..98 - 31.03.91 Budget: Overall cost: 2185 k € E C contribution: 1530 k € Keywords: Healthcare – Organ Transplant – Medical Information Portal Key Project Participants: Universite Joseph Fourier (F) VARIMED (HU) Laser und Medizin Tech. GmbH (D) EUROTRANSPLANT (HU) Inst Immunology, Bratislava(SK) TELES AG (D) HUNGAROTRANSPLANT(HU) SLOVENJA-TRANSPLANT(SJ) FORTH (GR) BULL SA (F) BULL Hungary (HU) North Eastern Health Board (IE) VITAMIB sarl (F) Project Co-ordinator: Prof. Gérard Brugal, University Joseph Fourier Grenoble 1 38706 La Tronche Cedex, France Tel: +33 4 76 54 94 01 Fax: +33 4 76 54 95 49 E-mail: [email protected] Project General Manager, Dr. Sandor Vari VARIMED Ltd 1124 Budapest, Hungry Tel: +36 1 487 0430 Fax: +36 1 487 0430 E-mail: [email protected] The Fifth Framework Programme (1998-2002) Enabling Best Practices for Oncology BePrO N° 25252

104
Summary The BEPRO project aimed to provide reference cancer centers with resources to extend the pilot use of results from previous European projects in Information Technologies for Health. They deployed IT applications, integrated them into their routine environment, and received appropriate training. The resulting best practice was demonstrated in use.
PROBLEM The multiplicity of developments and fast evolution of the Internet technology play against the smooth integration of health telematics into medical practice thus providing arguments to support waiting attitudes and conservatism. The decision to use ICT tools is finally made by medical actors who do not have the time and evidences for fast integration of fully digital support systems for prevention, detection, diagnosis, treatment and follow up of patients. How the use of information and communication technologies impact the best medical practice is still a challenge and a prerequisite for cost-benefit analysis with regard to social and medical interests.
AIM The BEPRO project demonstrated best practice in action enabled by the use of innovative ICT applications in Oncology. Five influential centres, each at the heart of a Regional, National or European network of cancer specialists experimented these ICT applications for sake of integration in their respective working environments. Co-operative services allowed sharing experience and reaching consensus at inter-application and trans-national levels. Results disseminated to the relevant medical community and submitted, whenever applicable, to standardization bodies.
TECHNICAL APPROACH The project dealt with data exchange procedures based on XML and DTD kept at the most generic and re-usability levels dealing with state-of-the-art data exchange technologies independently of the medical applications. BEPRO followed 3 successive phases to reach its main objectives. A SETUP PHASE reviewed the environment and networks with respect to industrial standards. A MEDICAL EVALUATION PHASE monitored the medical use of ICT tools in close collaboration with the industrial partners and concentrated on the medical and organisational impact of the selected applications. A CONSOLIDATION PHASE assessed the extent of the use of ICT tools impact medical practices.
RESULTS The BEPRO project ended with 4 medical reference platforms in FRANCE, UNITED KINGDOM, HOLLAND and HUNGARY each at the heart of a professional network where the information and communication technologies for health had been integrated in routine work. It carried out in a way consistent with European safe and secure integration of medical best practices in several respects: reference diagnostic, consensus on electronic forms and remote data entry to report to epidemiological centers and clinical trials coordinators, guidelines and continuous medical education. Co-ordinator: Université Joseph Fourier, Grenoble I - France Samba Technologies SARL SAMBA - France Institut Gustave Roussy - France InferMed Limited INFERMED - United Kingdom Medizinische Einrichtungen der Universität Essen - Germany VARIMED LTD - Hungary VITAMIB SARL VITAMIB - France Het Nederlands Kanker Instituut - Holland Maxim VOF - Holland Medical Research Council MRC United Kingdom
105
Project contract number: IST-2000-25252 Project start date: 01-Jan-2001 Project duration: 18 months
ProRec
The main goal of the European ProRec initiative (Promote Records) is to promote and co-ordinate the European wide convergence towards comprehensive, communicable and secure Electronic Healthcare Records (EHCR). This is achieved by co-ordinating and supporting the European Commission's Telematics Applications for Health projects and other initiatives in the area of EHCRs, both nationally and internationally. The primary objective of this initiative is that within a reasonable timescale a EHCR is installed in all Member States such that healthcare data originating from various sources are communicable and understandable. ProRec's mission is realised by undertaking monitoring, assessment and dissemination activities. Better collaboration between the different healthcare providers is critical for achieving the level of quality and continuity that European citizens increasingly expect. Efficient exchange of information is the key element for managing resources, evaluating quality, and raising cost-effectiveness. I t is commonly recognised that IT is essential to providing such data, and the use of standards-based record elements is crucial for interoperation. In order to support this process, ProRec centres have been established in different European countries, These centres leverage the EHCR activities across Europe and help to co-ordinate the convergence between the countries. The Hungarian ProRec centre has been set up in order to act as a link between the European ProRec initiative and the domestic healthcare actors. One of the key issues has been to reach and connect all potential players involved in the field of application of electronic healthcare records, and to concentrate efforts on the co-ordination of Hungarian EHCR related activities, This work has been carried out in further cooperation with other (national) ProRec centres, within the PROREC and WIDENET projects, i.e. the frame of the 4th and 5th RTD Framework Programs of the EU. The ProRec objectives are fully in line with those declared and supported preferences of the Hungarian government, The coincidence of the goals of the general national healthcare policy and the ProRec mission was also expressed through a valuable grant received from the National Committee for Technological Development that helped the operation of the Hungarian ProRec centre. The core task of the Hungarian ProRec centre is to collect and make publicly available information about different IT products and developments in this area, as well as to raise the awareness of the developers of the individual domestic healthcare telematics applications so that these systems become interoperable both inside Hungary and between the country and the EU. The system vendors and the users of medical information systems in their everyday work shall use the information disseminated by the Hungarian ProRec centre. The acquired knowledge must help the responsible management in making proper strategic decisions. The measures also consist of building independent criteria and offering services for evaluating IT solutions, and a degree of accreditation of health telematics services and products.
FOR MORE FIFTH FRAMEWORK PROGRAMME (1998-2002) PROPOSALS AND PROJECTS PLEASE REVIEW THE APPENDIX SECTION OF OUR PAPER
106
4. IST strategies and action plan for eHealth in Hungary 4
(Tamas Gergely)
• The Hungarian Government approved the Minister’s report on restructuring healthcare and the related implementation schedule. The key targets of the Government programme are as follows:
• Improve quality of life through health promotion. • Enhance the equity of the healthcare system by reducing regional inequalities and by eliminating roadblocks to
access (i.e. in care, and in financial, social and mental terms). • Make professional standards of care consistent, enhanced and accountable through quality management;
disseminate technologies; • Improve the efficiency of the care provision system and individual service providers (by improving allocation
efficiency and technical efficiency in parallel) and to that end, design, implement and organise regional care based on the principle of progressive care.
• Restructure the care provision system to make it ‘patient friendly’, i.e. improve the conditions of care, grant patients more choice, and make patients more informed.
The key tools to implement the above targets include:
2. Implement the public health programme approved by Parliament.
3. The consolidation and development programme linked to the regional restructuring of the healthcare system.
This programme package implements a development environment in a complex way, by creating regional planning for care, development policy, and the related institutional system. This development environment ensures balanced access to healthcare, uniform technical standards, including the replacement of obsolete key equipment (for ambulance and emergency services, diagnostics and oncological therapy) and the installation of such equipment where necessary. The programme integrates various funds, including EU funds, national development funds, ministerial development funds, municipal funds, and private investment for public purposes (Public Private Partnership programmes).
The integration of the health care provision systems, and ensuring co-operation between organisations and funding arrangements are key tasks in restructuring the care provision system.
1. The Human Resources programme group includes improved recognition for staff in the sector (thereby reducing the attractiveness of job-shifting), the simplification of professional training, and support for IT-based distance learning in ongoing continued training.
2. The financing reform is aimed at reinforcing the current public funding system and improving its efficiency. In order to enhance the equity of the system, we wish to promote private funding arrangements. The Government expects this initiative to help reduce gratuities and distribute the public burden more equally.
3. Information and Communication Technology (ICT) development. The key targets of ICT development are to propagate the application of knowledge-based solutions in therapy and in strategic planning at the Government and regional levels, to improve the efficiency and quality of healthcare, and to promote uniform healthcare services. Other directions for action include improving the level of information available to patients and the healthy public, the application of ICT solutions in health improvement and patient information.
4.
Domestic Trends Health monitoring 4 Source: Care and Social Sector Information Strategy, Ministry of Health, Social and Family Affairs
107
The collection, processing and publication of data regarding the health status of the public or the key health factors – jointly referred to as health monitoring – is an important support tool for health policy making in most developed states. The collection of health information and operational data regarding the care delivery system in Hungary falls within the competence of several organisations. The key organisation in charge is the Central Statistical Office. Analysis regarding the care delivery system is undertaken by the organisation supervised by the Ministry of Health, including NPHMOS, Centre for Healthcare Information (GYÓGYINFOK) and National Institute and Library for Health Information (MEDINFO). The analysis performed by NHIFA is also becoming more and more important. The health monitoring and reporting system in Hungary is predominantly about mandatory statistical data collection – prescribed by the Act and Statistics and the National Statistical Data Collection Program – i.e. quantitative information about various forms of care and – with a few exceptions – paper-based publication mostly in statistical tables. In recent years – to satisfy modern requirements, i.e. a growing demand for prevalence data regarding chronic incommunicable diseases and their key factors – many new initiatives have emerged in the health monitoring field. Examples include the National Population Health Survey (OLEF2000) and the Program of Morbidity Data Collection in Family Practice (PMDCFP). Regular health surveys and data collection based on the ongoing verified reports by certain family practitioners are not part of the domestic health monitoring and reporting system as yet. One of the key developments in recent years in health monitoring has been the development of partnership between the institutions. This is evidenced by the Forum for Health Statistics – held twice to date – and co-operation of NPHMOS and CSO in order to improve the quality of mortality statistics, and the co-operation between NPHMOS and DE OEC School of Public Health in PMDCFP. By now most players have realised that an efficient health monitoring and reporting system can only be based on institutional co-operation with a division of tasks and collaboration. In addition to the development of partnership, the key directions of development include the implementation and ongoing improvement of the domestic health indicator system, in line with international requirements; and in that context, a rethinking of data collection, with special regard to whether it is necessary and credible; the extension of analysis capacity; publication of data, information and know-how; the development of communication methods, their adaptation to the needs and absorption capacity of the target audience, as well as the development of electronic knowledge bases. The international benchmarking and analysis of the correlations between healthcare and economy are enabled by the National Health Account project, a CSO programme based on a set of indicators used by OECD. In line with the ‘tools and purposes’ stated in the Hungarian Information Society Strategy (HISS) and the societal tasks regarding the implementation of eHealth, the following targets have been set for the sector:
4.1 To produce health information and knowledge
• Equal opportunities in access to information i.e. ensure balanced access to information and knowledge.
• Produce professional information and knowledge of public interest regarding health, and healthcare services.
• Develop electronic content services and make them available to the professional target audience.
• Deliver information services to the public over the Internet and through call centres.
• Develop the information content of the virtual health marketplace.
4.2 To provide the resources
Information and Communication Technology environment
Laying the foundations for eHealth by providing the infrastructure, standards and tools:
• Build the infrastructure that serves as the foundation of eAdministration.
• Expand the scope of basic registers and authentic records – and electronize those registers.
• Develop the glossary of terms and term management technology, as well as standards for the sector.
• Develop and naturalise standards for eApplication.
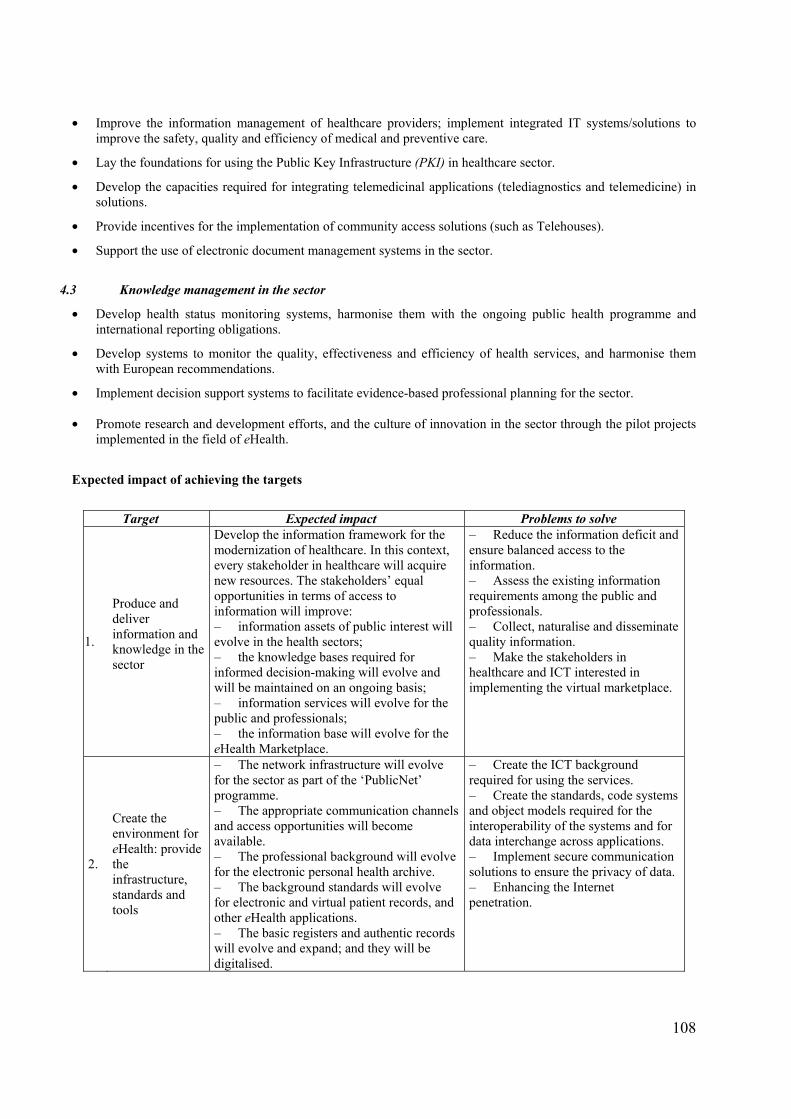
108
• Improve the information management of healthcare providers; implement integrated IT systems/solutions to improve the safety, quality and efficiency of medical and preventive care.
• Lay the foundations for using the Public Key Infrastructure (PKI) in healthcare sector.
• Develop the capacities required for integrating telemedicinal applications (telediagnostics and telemedicine) in solutions.
• Provide incentives for the implementation of community access solutions (such as Telehouses).
• Support the use of electronic document management systems in the sector.
4.3 Knowledge management in the sector
• Develop health status monitoring systems, harmonise them with the ongoing public health programme and international reporting obligations.
• Develop systems to monitor the quality, effectiveness and efficiency of health services, and harmonise them with European recommendations.
• Implement decision support systems to facilitate evidence-based professional planning for the sector.
• Promote research and development efforts, and the culture of innovation in the sector through the pilot projects implemented in the field of eHealth.
Expected impact of achieving the targets
Target Expected impact Problems to solve
1.
Produce and deliver information and knowledge in the sector
Develop the information framework for the modernization of healthcare. In this context, every stakeholder in healthcare will acquire new resources. The stakeholders’ equal opportunities in terms of access to information will improve: – information assets of public interest will evolve in the health sectors; – the knowledge bases required for informed decision-making will evolve and will be maintained on an ongoing basis; – information services will evolve for the public and professionals; – the information base will evolve for the eHealth Marketplace.
– Reduce the information deficit and ensure balanced access to the information. – Assess the existing information requirements among the public and professionals. – Collect, naturalise and disseminate quality information. – Make the stakeholders in healthcare and ICT interested in implementing the virtual marketplace.
2.
Create the environment for eHealth: provide the infrastructure, standards and tools
– The network infrastructure will evolve for the sector as part of the ‘PublicNet’ programme. – The appropriate communication channels and access opportunities will become available. – The professional background will evolve for the electronic personal health archive. – The background standards will evolve for electronic and virtual patient records, and other eHealth applications. – The basic registers and authentic records will evolve and expand; and they will be digitalised.
– Create the ICT background required for using the services. – Create the standards, code systems and object models required for the interoperability of the systems and for data interchange across applications. – Implement secure communication solutions to ensure the privacy of data. – Enhancing the Internet penetration.
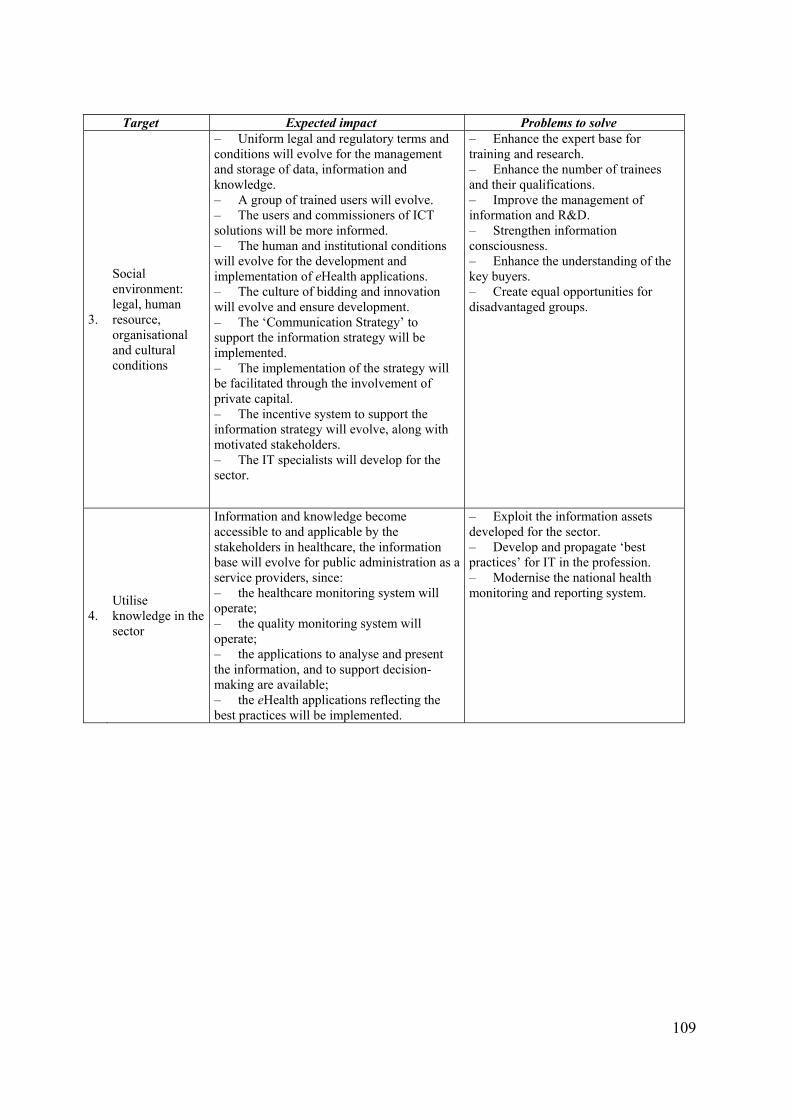
109
Target Expected impact Problems to solve
3.
Social environment: legal, human resource, organisational and cultural conditions
– Uniform legal and regulatory terms and conditions will evolve for the management and storage of data, information and knowledge. – A group of trained users will evolve. – The users and commissioners of ICT solutions will be more informed. – The human and institutional conditions will evolve for the development and implementation of eHealth applications. – The culture of bidding and innovation will evolve and ensure development. – The ‘Communication Strategy’ to support the information strategy will be implemented. – The implementation of the strategy will be facilitated through the involvement of private capital. – The incentive system to support the information strategy will evolve, along with motivated stakeholders. – The IT specialists will develop for the sector.
– Enhance the expert base for training and research. – Enhance the number of trainees and their qualifications. – Improve the management of information and R&D. – Strengthen information consciousness. – Enhance the understanding of the key buyers. – Create equal opportunities for disadvantaged groups.
4. Utilise knowledge in the sector
Information and knowledge become accessible to and applicable by the stakeholders in healthcare, the information base will evolve for public administration as a service providers, since: – the healthcare monitoring system will operate; – the quality monitoring system will operate; – the applications to analyse and present the information, and to support decision-making are available; – the eHealth applications reflecting the best practices will be implemented.
– Exploit the information assets developed for the sector. – Develop and propagate ‘best practices’ for IT in the profession. – Modernise the national health monitoring and reporting system.
110
5. What general comments therefore can be made regarding eHealth in Hungary? (Sandor G. Vari)
Linking different record systems to each other sometimes raises criticism (primary –secondary care), in particular in cases, which may involve personal/patient records. The systems are in place designed to fulfill the requirements of the National Health Insurance Fund Administration (NHIFA). The main feature of these systems (Primary Care, HIS) to able to deal with the diagnostic (ICD 10) and intervention (WHO) codes on a way the health care facilities able to report the most cost effective coding for reimbursement. The database for patient records, which will provide medical information and history on the patient from cradle-to-grave, is less important and very heterogeneous. Hence electronic medical records need to be stored in standard format not only translatable departments and health care facilities, but also universally comprehendible by any practitioner who must use the information system. Today there exist many different types of medical records within the clinical environments to cover specific areas of care and treatment. The patient is normally connected to numerous monitoring and therapeutic devices. Thus there can be difficulty in gathering data from these diverse sources to enable the most effective clinical decisions to be made. There is need to secure standards and qualities and for appropriate steps, nationally and internationally, to be taken in the search for solutions. Also, lack of guidance from central authorities has in many instances led to a mish-mash of non-compatible computer-based patient record systems in the Primary Care in Hungary. Such circumstances have caused problems to arise in the smooth processing of patients between health service units, even within the same health authority (or equivalent). For the civil community, one can envision an eventual central, cradle-to-grave, medical information management system containing records on each citizen of the country, for every country in the world, with appropriate security and control measures instituted according to local laws and regulations is a dream in this day. There are certainly important ethical concerns in relation to composition of health records and access to the same. In spite of the many positive aspects of devolution / decentralization, there is a need for central coordination based on the National eHealth Strategy. This observation may also have some bearing internationally with the high volume of people travelling across national boarders in the European Union and sometimes needing emergency health treatment outside of their respective countries. In these cases, quick and efficient transfer, electronically, of medical records may be essential for achieving delivery of good quality acute care.
Most relevant changes are needed in Hungary to implement nationwide eHealth access eHealth is the use of modern telecommunications and information technologies for the provision of clinical care to individuals at a distance, and transmission of information to provide that care. eHealth can be used for collaborative arrangements for the real-time management, decision making, and remote monitoring of patients.. The use of telecommunications and information technologies in providing health services is determined. eHealth is described as combination of topics from the fields of medicine, telecommunication, and computer technologies. The medical systems infrastructure consisting of the equipment and processes used to acquire and present clinical information and to store and retrieve data are explained in details. The challenges existing in eHealth development in the European Union in different countries differ by technological, political, and professional barriers. Nevertheless in the progress of the integration of health care services the eHealth solutions are crucial and will play a pivotal role in the future. Integrated Health Care System Information and communications technology (ICT) is increasingly being used in management of illnesses to facilitate shared services (virtual health networks and electronic health records), knowledge management (care rules and protocols, scheduling, information directories), as well as consumer-based health education and evidence-based clinical protocols. The integration of health care services with the use of eHealth solutions holds for both clinicians and health care leaders the real possibility of stimulating fresh insights and approaches to health and medical care-both its provision and its organization. Clinicians and leaders of health care organizations must understand the complexity of the integration process. They have to consider difficult challenges in both patient and organizational management. Nevertheless there are some basic eHealth solutions

111
they can use in this extraordinarily complicated task of jointly creating integrated health care systems. In Hungary we shall implement an eHealth application tightly integrated with electronic medical record system that provides physicians and patients with a convenient, continuously available communication channel to the health care system. Physicians and patients can view summary data from medical record, including the results of diagnostic tests, and request medical advice, prescription renewals, appointments, or updates to their demographic information. Online tools for physicians and patients, when integrated with an electronic medical record, can provide better access to health information, improve patient satisfaction, and improve operational efficiency.
Computer-based medical records The main application in Hungary is computer-based medical records (Primary Care and HIS), nevertheless very few computer-based patient records that are able to axchange data with other record systems and facilitating clinical decision-making. These records may be linked to knowledge-oriented systems that may contribute to quality control of clinical processes. Such a decision support has been demonstrated to improve outcomes.
Computer-based population or community health records Computer-based population or community health records do not exist at this moment in Hungary, however these systems are particularly valuable in public health where one is trying to trace different types of health hazards, linked either to medical, environmental or social agents. Disease management Disease management has been described as a comprehensive, integrated approach to care and reimbursement based on the natural course of a disease. It requires a management approach, which brings together research evidence, best practice and inter-professional and inter-agency working. Starting with the ideal of continuity of care for individual patients, it implies structured co-ordination of care over time and across primary, secondary and tertiary settings. The appeal of disease management is that it promises reduced costs, combined with increased quality of care and patient satisfaction. But the concept is open to different definitions and interpretations and its effectiveness in the Hungarian healthcare is untested. Decision Support With rapid changes taking place in the practice and delivery of health care, decision support systems have assumed an increasingly important role. More and more health care institutions are deploying data warehouse applications as decision support tools for strategic decision-making. By making the right information available at the right time to the right decision-makers in the right manner, data warehouses empower employees to become knowledge workers with the ability to make the right decisions and solve problems, creating strategic leverage for the organization. Nevertheless the web based decision support systems linked to Hospital Information System (HIS) are not used in the daily practice in Hungary. While search engines exist for finding sites and criteria are available for assessing site quality, few tools are available for managing Web-based health care information. Management of Web-based information is particularly challenging because the information is continually changing and new resources are continually being added.
Nursing and Home Care Since 90% of people's health needs require nursing, not medical care, it is important those nurses be appointed to management positions and participate in national health services, that research on nursing education includes primary health care. The new member states, with all their differences, face strikingly similar problems in administration and nursing administration in particular: emphasis on hospitals top-down hierarchies undeveloped human resources lack of high performance systems lack of infrastructures for health service delivery ineffective rural-urban links
Now the focus in Hungary is on the appropriate use of resources, cooperation between public and private sectors, and sustainability. It is important to emphasize developmental process rather than targets, and to work at the local level. Home health care is an expanding area within the health care system. The idea of moving

112
parts of the health care process from expensive specialized hospital care to primary health care and home health care might be attractive in a cost perspective is a very important issue in the Hungarian health care system. Common applications of ICT include home monitoring of vital signs for patients with chronic disease, as well as replacing home visits by nurses in person with telemedicine videophone consultations. A patient-managed Home Telecare System with integrated clinical signs monitoring, automated scheduling and medication reminders, as well as access to health education and daily logs, is presented as an example of ICT use for chronic disease self-management does not exist in Hungary. A clinical case study demonstrates how early identification of adverse trends in clinical signs recorded in the home can either avoid hospital readmission or reduce the length of hospital stay.
ePharmacy Pharmacy is one of the key health care professions that must adopt Information and communications technology (ICT). A stepwise structure for pharmacy informatics has to be proposed in Hungary; it should consists of establishing a relationship with the patient, establishing a database, listing and ranking problems, choosing among alternatives, and planning and monitoring. Pharmacists will need to use ICT to enhance their worth on the health care team and to improve patient care. It includes determining the consequences of less than optimal drug therapy, improving drug therapy, and reengineering pharmacy departments and services across all patients care settings to deliver optimal pharmacotherapy. Prevention and reduction of adverse drug events, disease state management, and other methods to improve quality of care are of major importance.
Patient self-management Self-management is an essential but frequently neglected component of chronic illness management that is challenging to implement. Available effectiveness data regarding self-management interventions tend to be from stand-alone programs rather than from efforts to integrate self-management into routine medical care in Hungary. We have to make tremendous efforts to integrate self-management support into broader health care systems change to improve the quality of patient care in the chronic illness. Available data suggest that teams from a variety of health care organizations made improvements in support provided for self-management. Improvements were found for both diabetes and heart failure, suggesting that this improvement process may be broadly applicable. Evidence based health care management. The health care providers must introduce a new approach for health care management called Evidence Based Management. This approach promises to improve the practice of health care management, at the same time as it may stimulate research on the organization and management of health care. Evidence Based Management means that health care managers should learn to search for and critically appraise evidence from management research as a basis for their practice. This will require some new managerial skills that should be included in the education and training of health care managers. It will also require a new orientation for research on health care management. There will be a demand for more applied research, and also for research with a more positivist orientation. Health care management must plan and implement data warehousing strategy using a best practice approach. Through the power of data warehousing, health care management can negotiate better managed care contracts based on the ability to provide accurate data on case mix and resource utilization. Management can also save millions of dollars through the implementation of clinical pathways in better resource utilization and changing physician behaviour to best practices based on evidence-based medicine. Modelling-based health care management ought to become just as popular as evidence based medicine. Making managerial decisions based on evidence by modelling efforts is certainly could be one of the major steps forward. Examples can be given of many successful applications in different areas of decision-making:
• disease process modelling • screening and prevention policy development • resource allocation • waiting lists and waiting times • patient scheduling

113
Also examples shell be given which would have benefited by prior modelling, for example adverse effects of health care system reform decisions in Hungary. The advantage of mapping modelling applications in this way is that we are able to position contributions within a reference framework with a focus on processes, with the patient process at the top. The acceptance of process-orientation as a basis for modelling has consequences for the way models are developed. Close cooperation between modeler and manager and a profound insight into the dynamics of the modelling area concerned are important requirements for developing successful models. eHealth ethics The Internet is changing how people receive health information and health care. All who use the Internet for health-related purposes must join together to create an environment of trusted relationships to assure high quality information and services; protect privacy; and enhance the value of the Internet for both consumers and providers of health information, products, and services. The next step has to be in Hungary the implementation of the "e-Health Code of Ethics" that is to ensure that all people in the country can confidently, and without risk, realize the full benefits of the Internet to improve their health. The National e-Health Code of Ethic should reflect the results of the "eHealth Ethics Summit," which convened in Washington DC on 31 January 2000 - 2 February 2000. The Summit was organized by the Internet Healthcare Coalition and hosted by the World Health Organisation/Pan-American Health Organisation (WHO/PAHO), and attended by a panel of about 50 invited experts from all over the world. It sets forth guiding principles under five main headings: candor and trustworthiness; quality; informed consent, privacy, and confidentiality; best commercial practices; and best practices for provision of health care on the Internet by health care professionals.
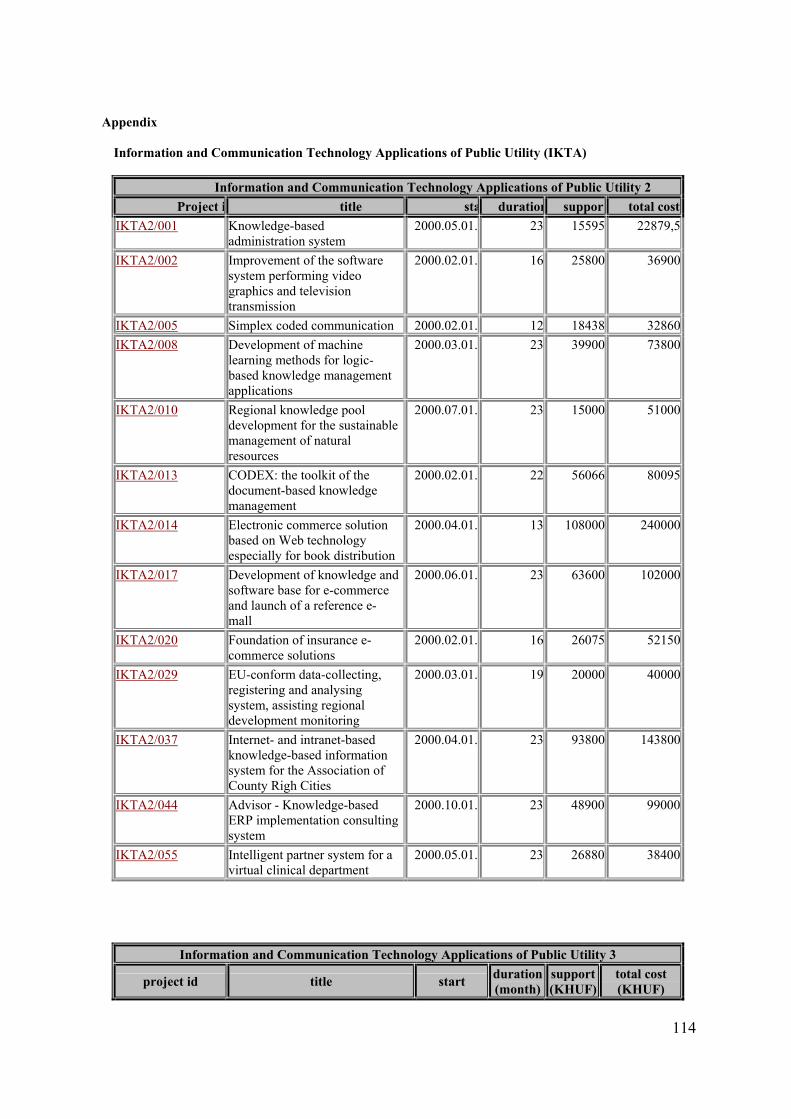
114
Appendix Information and Communication Technology Applications of Public Utility (IKTA)
Information and Communication Technology Applications of Public Utility 2 Project i title sta duration support total cost
IKTA2/001 Knowledge-based administration system
2000.05.01. 23 15595 22879,5
IKTA2/002 Improvement of the software system performing video graphics and television transmission
2000.02.01. 16 25800 36900
IKTA2/005 Simplex coded communication 2000.02.01. 12 18438 32860IKTA2/008 Development of machine
learning methods for logic-based knowledge management applications
2000.03.01. 23 39900 73800
IKTA2/010 Regional knowledge pool development for the sustainable management of natural resources
2000.07.01. 23 15000 51000
IKTA2/013 CODEX: the toolkit of the document-based knowledge management
2000.02.01. 22 56066 80095
IKTA2/014 Electronic commerce solution based on Web technology especially for book distribution
2000.04.01. 13 108000 240000
IKTA2/017 Development of knowledge and software base for e-commerce and launch of a reference e-mall
2000.06.01. 23 63600 102000
IKTA2/020 Foundation of insurance e-commerce solutions
2000.02.01. 16 26075 52150
IKTA2/029 EU-conform data-collecting, registering and analysing system, assisting regional development monitoring
2000.03.01. 19 20000 40000
IKTA2/037 Internet- and intranet-based knowledge-based information system for the Association of County Righ Cities
2000.04.01. 23 93800 143800
IKTA2/044 Advisor - Knowledge-based ERP implementation consulting system
2000.10.01. 23 48900 99000
IKTA2/055 Intelligent partner system for a virtual clinical department
2000.05.01. 23 26880 38400
Information and Communication Technology Applications of Public Utility 3
project id title start duration (month)
support (KHUF)
total cost (KHUF)
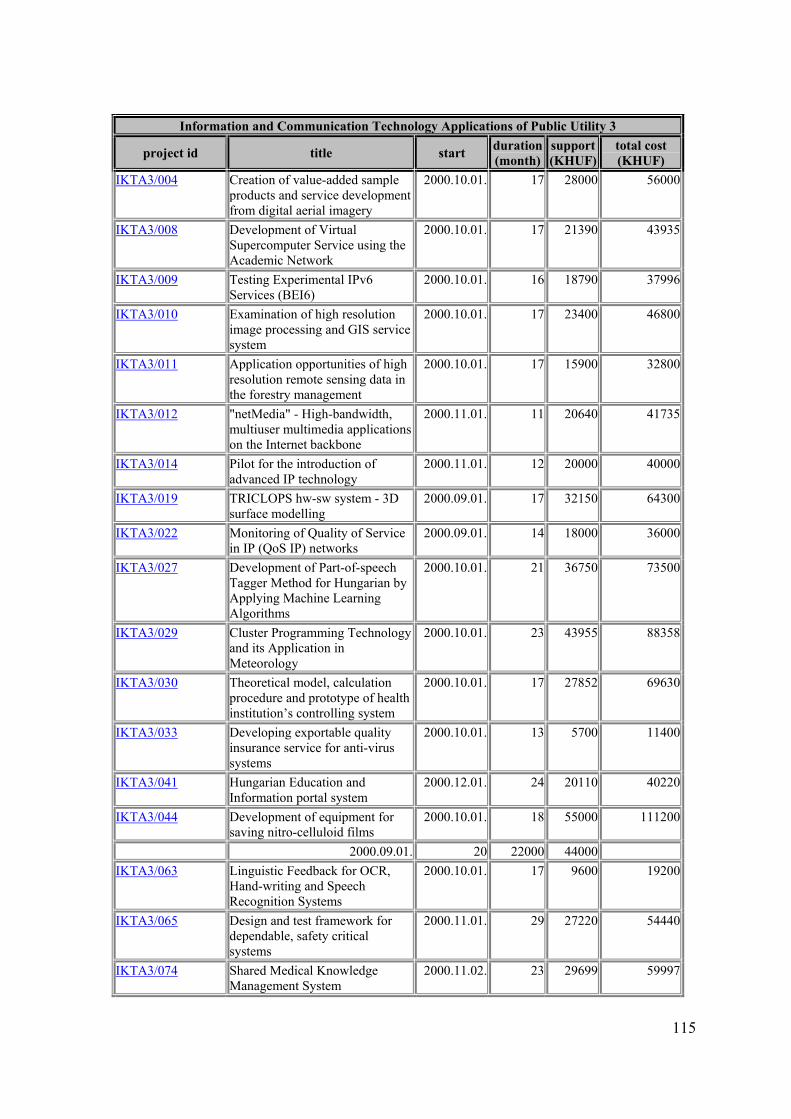
115
Information and Communication Technology Applications of Public Utility 3
project id title start duration (month)
support (KHUF)
total cost (KHUF)
IKTA3/004 Creation of value-added sample products and service development from digital aerial imagery
2000.10.01. 17 28000 56000
IKTA3/008 Development of Virtual Supercomputer Service using the Academic Network
2000.10.01. 17 21390 43935
IKTA3/009 Testing Experimental IPv6 Services (BEI6)
2000.10.01. 16 18790 37996
IKTA3/010 Examination of high resolution image processing and GIS service system
2000.10.01. 17 23400 46800
IKTA3/011 Application opportunities of high resolution remote sensing data in the forestry management
2000.10.01. 17 15900 32800
IKTA3/012 "netMedia" - High-bandwidth, multiuser multimedia applications on the Internet backbone
2000.11.01. 11 20640 41735
IKTA3/014 Pilot for the introduction of advanced IP technology
2000.11.01. 12 20000 40000
IKTA3/019 TRICLOPS hw-sw system - 3D surface modelling
2000.09.01. 17 32150 64300
IKTA3/022 Monitoring of Quality of Service in IP (QoS IP) networks
2000.09.01. 14 18000 36000
IKTA3/027 Development of Part-of-speech Tagger Method for Hungarian by Applying Machine Learning Algorithms
2000.10.01. 21 36750 73500
IKTA3/029 Cluster Programming Technology and its Application in Meteorology
2000.10.01. 23 43955 88358
IKTA3/030 Theoretical model, calculation procedure and prototype of health institution’s controlling system
2000.10.01. 17 27852 69630
IKTA3/033 Developing exportable quality insurance service for anti-virus systems
2000.10.01. 13 5700 11400
IKTA3/041 Hungarian Education and Information portal system
2000.12.01. 24 20110 40220
IKTA3/044 Development of equipment for saving nitro-celluloid films
2000.10.01. 18 55000 111200
2000.09.01. 20 22000 44000 IKTA3/063 Linguistic Feedback for OCR,
Hand-writing and Speech Recognition Systems
2000.10.01. 17 9600 19200
IKTA3/065 Design and test framework for dependable, safety critical systems
2000.11.01. 29 27220 54440
IKTA3/074 Shared Medical Knowledge Management System
2000.11.02. 23 29699 59997
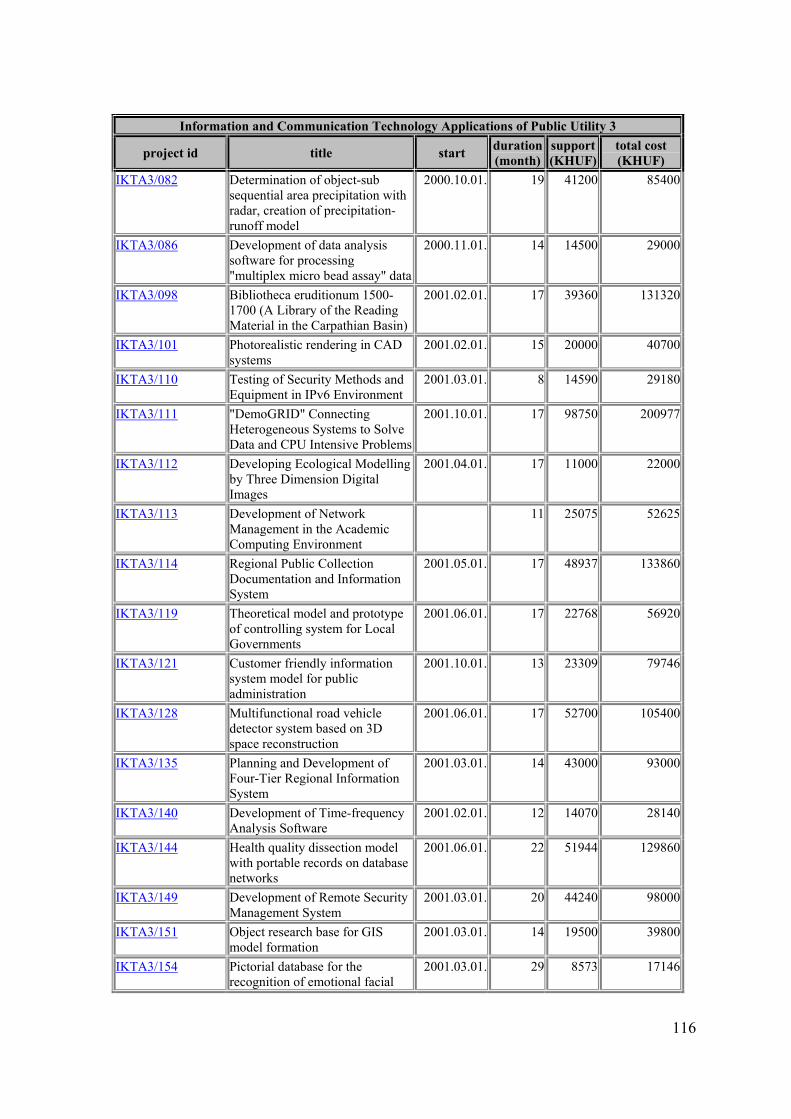
116
Information and Communication Technology Applications of Public Utility 3
project id title start duration (month)
support (KHUF)
total cost (KHUF)
IKTA3/082 Determination of object-sub sequential area precipitation with radar, creation of precipitation-runoff model
2000.10.01. 19 41200 85400
IKTA3/086 Development of data analysis software for processing "multiplex micro bead assay" data
2000.11.01. 14 14500 29000
IKTA3/098 Bibliotheca eruditionum 1500-1700 (A Library of the Reading Material in the Carpathian Basin)
2001.02.01. 17 39360 131320
IKTA3/101 Photorealistic rendering in CAD systems
2001.02.01. 15 20000 40700
IKTA3/110 Testing of Security Methods and Equipment in IPv6 Environment
2001.03.01. 8 14590 29180
IKTA3/111 "DemoGRID" Connecting Heterogeneous Systems to Solve Data and CPU Intensive Problems
2001.10.01. 17 98750 200977
IKTA3/112 Developing Ecological Modelling by Three Dimension Digital Images
2001.04.01. 17 11000 22000
IKTA3/113 Development of Network Management in the Academic Computing Environment
11 25075 52625
IKTA3/114 Regional Public Collection Documentation and Information System
2001.05.01. 17 48937 133860
IKTA3/119 Theoretical model and prototype of controlling system for Local Governments
2001.06.01. 17 22768 56920
IKTA3/121 Customer friendly information system model for public administration
2001.10.01. 13 23309 79746
IKTA3/128 Multifunctional road vehicle detector system based on 3D space reconstruction
2001.06.01. 17 52700 105400
IKTA3/135 Planning and Development of Four-Tier Regional Information System
2001.03.01. 14 43000 93000
IKTA3/140 Development of Time-frequency Analysis Software
2001.02.01. 12 14070 28140
IKTA3/144 Health quality dissection model with portable records on database networks
2001.06.01. 22 51944 129860
IKTA3/149 Development of Remote Security Management System
2001.03.01. 20 44240 98000
IKTA3/151 Object research base for GIS model formation
2001.03.01. 14 19500 39800
IKTA3/154 Pictorial database for the recognition of emotional facial
2001.03.01. 29 8573 17146
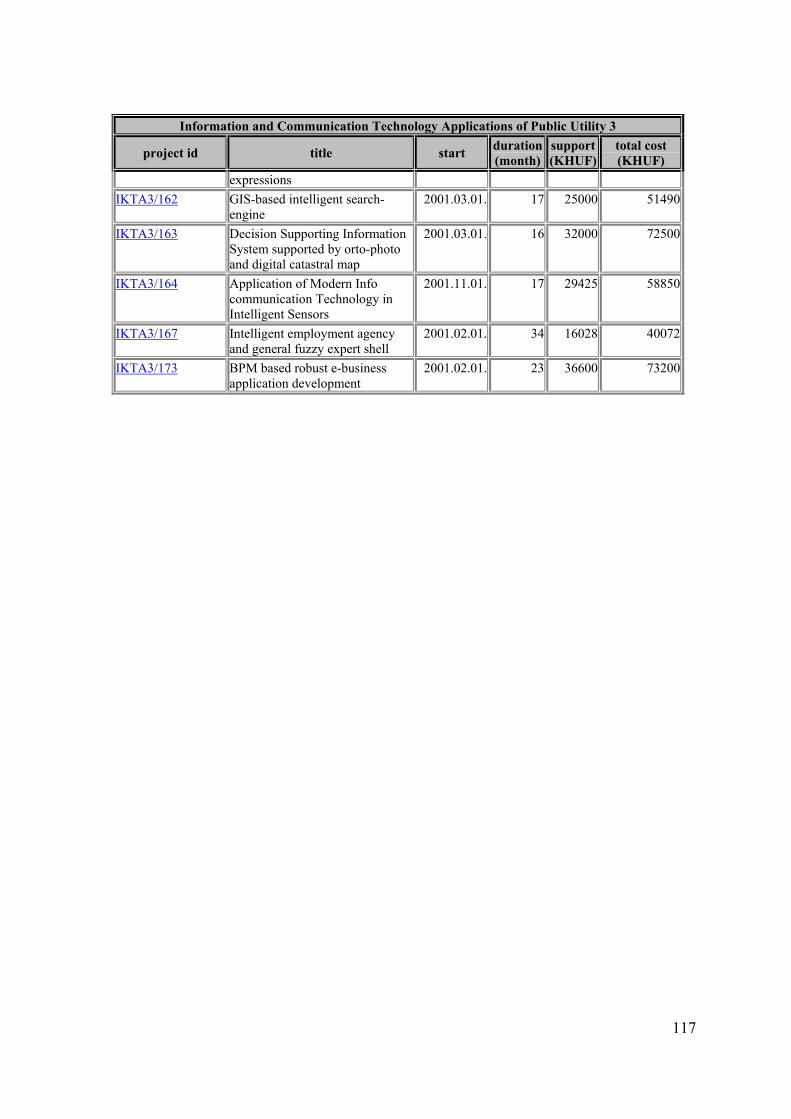
117
Information and Communication Technology Applications of Public Utility 3
project id title start duration (month)
support (KHUF)
total cost (KHUF)
expressions IKTA3/162 GIS-based intelligent search-
engine 2001.03.01. 17 25000 51490
IKTA3/163 Decision Supporting Information System supported by orto-photo and digital catastral map
2001.03.01. 16 32000 72500
IKTA3/164 Application of Modern Info communication Technology in Intelligent Sensors
2001.11.01. 17 29425 58850
IKTA3/167 Intelligent employment agency and general fuzzy expert shell
2001.02.01. 34 16028 40072
IKTA3/173 BPM based robust e-business application development
2001.02.01. 23 36600 73200
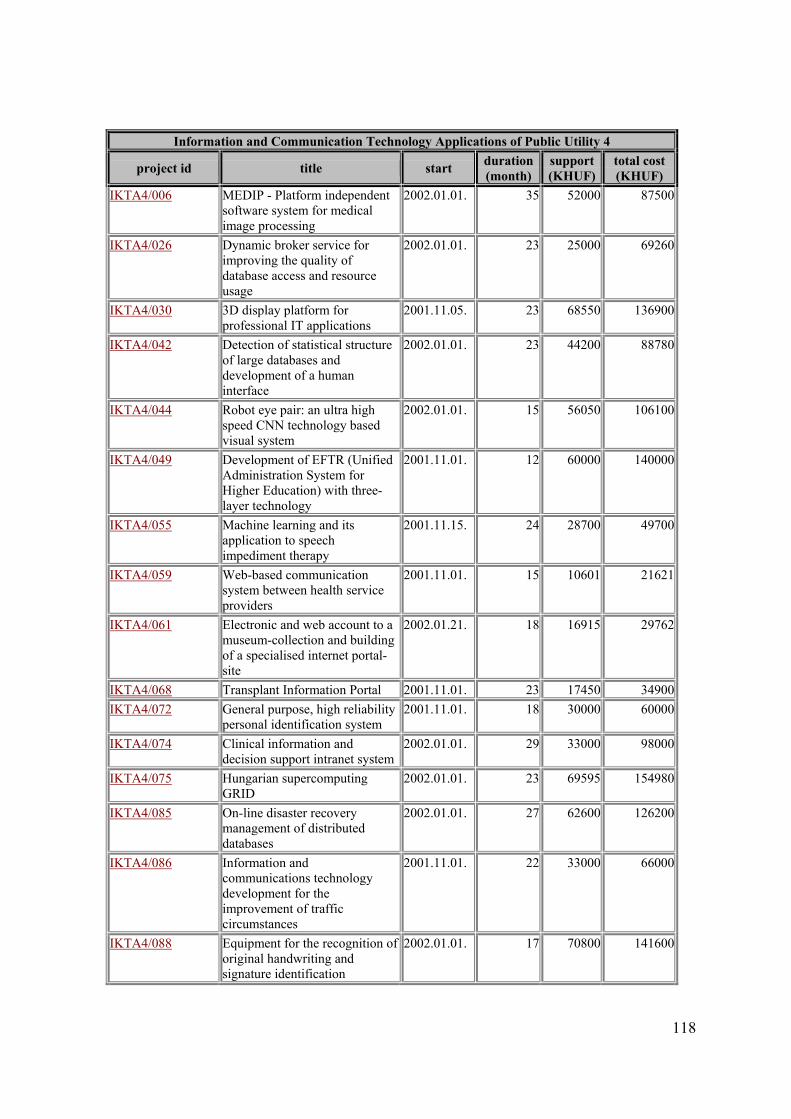
118
Information and Communication Technology Applications of Public Utility 4
project id title start duration (month)
support (KHUF)
total cost (KHUF)
IKTA4/006 MEDIP - Platform independent software system for medical image processing
2002.01.01. 35 52000 87500
IKTA4/026 Dynamic broker service for improving the quality of database access and resource usage
2002.01.01. 23 25000 69260
IKTA4/030 3D display platform for professional IT applications
2001.11.05. 23 68550 136900
IKTA4/042 Detection of statistical structure of large databases and development of a human interface
2002.01.01. 23 44200 88780
IKTA4/044 Robot eye pair: an ultra high speed CNN technology based visual system
2002.01.01. 15 56050 106100
IKTA4/049 Development of EFTR (Unified Administration System for Higher Education) with three-layer technology
2001.11.01. 12 60000 140000
IKTA4/055 Machine learning and its application to speech impediment therapy
2001.11.15. 24 28700 49700
IKTA4/059 Web-based communication system between health service providers
2001.11.01. 15 10601 21621
IKTA4/061 Electronic and web account to a museum-collection and building of a specialised internet portal-site
2002.01.21. 18 16915 29762
IKTA4/068 Transplant Information Portal 2001.11.01. 23 17450 34900IKTA4/072 General purpose, high reliability
personal identification system 2001.11.01. 18 30000 60000
IKTA4/074 Clinical information and decision support intranet system
2002.01.01. 29 33000 98000
IKTA4/075 Hungarian supercomputing GRID
2002.01.01. 23 69595 154980
IKTA4/085 On-line disaster recovery management of distributed databases
2002.01.01. 27 62600 126200
IKTA4/086 Information and communications technology development for the improvement of traffic circumstances
2001.11.01. 22 33000 66000
IKTA4/088 Equipment for the recognition of original handwriting and signature identification
2002.01.01. 17 70800 141600
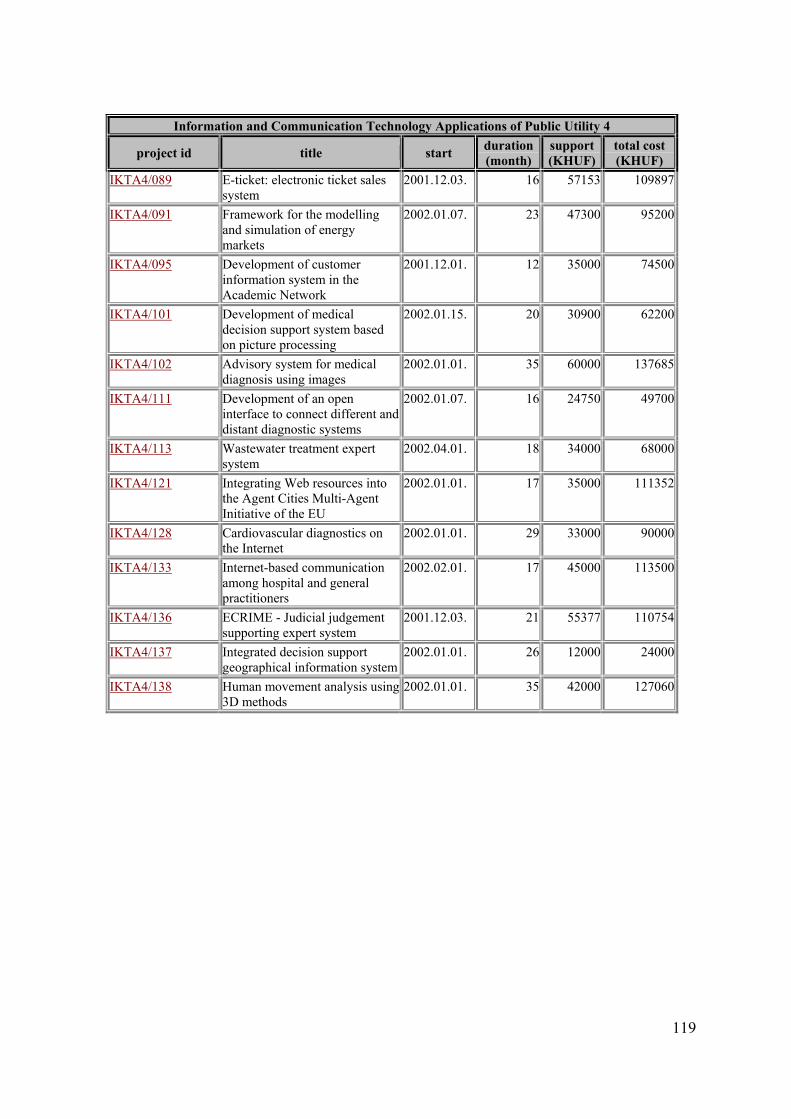
119
Information and Communication Technology Applications of Public Utility 4
project id title start duration (month)
support (KHUF)
total cost (KHUF)
IKTA4/089 E-ticket: electronic ticket sales system
2001.12.03. 16 57153 109897
IKTA4/091 Framework for the modelling and simulation of energy markets
2002.01.07. 23 47300 95200
IKTA4/095 Development of customer information system in the Academic Network
2001.12.01. 12 35000 74500
IKTA4/101 Development of medical decision support system based on picture processing
2002.01.15. 20 30900 62200
IKTA4/102 Advisory system for medical diagnosis using images
2002.01.01. 35 60000 137685
IKTA4/111 Development of an open interface to connect different and distant diagnostic systems
2002.01.07. 16 24750 49700
IKTA4/113 Wastewater treatment expert system
2002.04.01. 18 34000 68000
IKTA4/121 Integrating Web resources into the Agent Cities Multi-Agent Initiative of the EU
2002.01.01. 17 35000 111352
IKTA4/128 Cardiovascular diagnostics on the Internet
2002.01.01. 29 33000 90000
IKTA4/133 Internet-based communication among hospital and general practitioners
2002.02.01. 17 45000 113500
IKTA4/136 ECRIME - Judicial judgement supporting expert system
2001.12.03. 21 55377 110754
IKTA4/137 Integrated decision support geographical information system
2002.01.01. 26 12000 24000
IKTA4/138 Human movement analysis using 3D methods
2002.01.01. 35 42000 127060
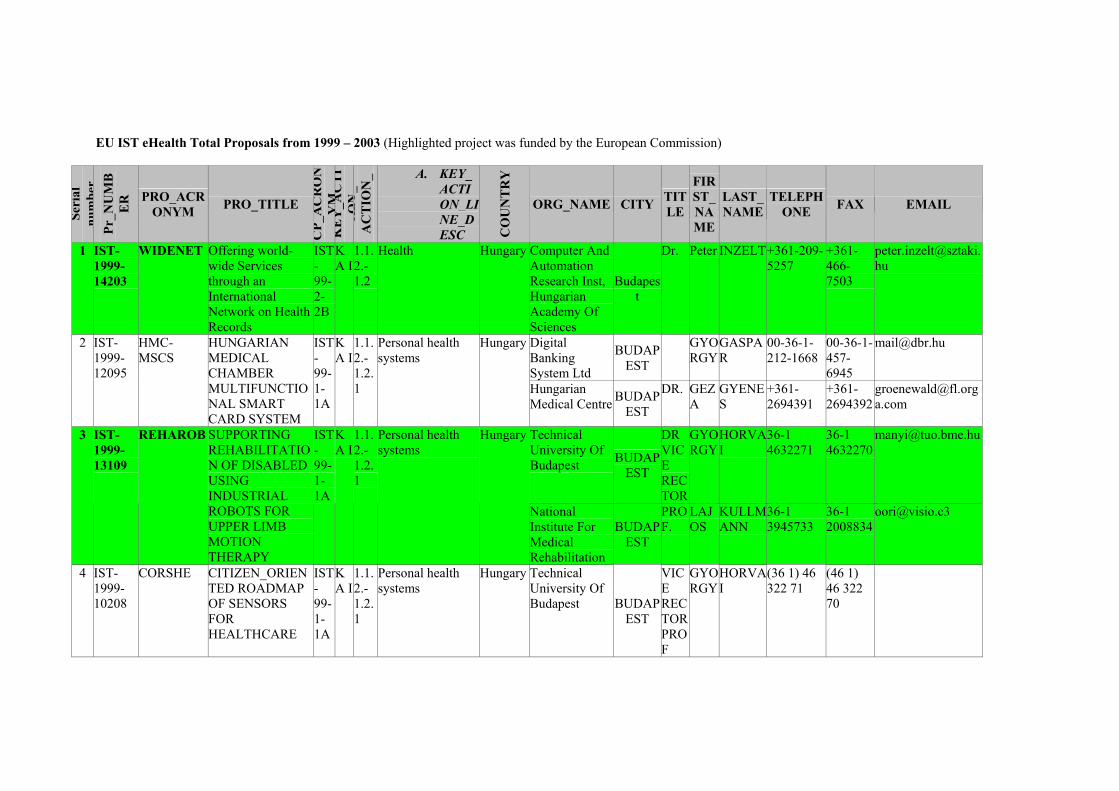
EU IST eHealth Total Proposals from 1999 – 2003 (Highlighted project was funded by the European Commission)
Seri
al
num
ber
Pr_N
UM
BE
R PRO_ACR
ONYM PRO_TITLE
CP_
AC
RO
NY
MK
EY
_AC
TI
ON
KE
Y_
A
CT
ION
_L
INE
A. KEY_ACTION_LINE_DESC C
OU
NT
RY
ORG_NAME CITY TITLE
FIRST_NAME
LAST_ NAME
TELEPHONE FAX EMAIL
1 IST-1999-14203
WIDENET Offering world-wide Services through an International Network on Health Records
IST-99-2-2B
KA I
1.1.2.-1.2
Health Hungary Computer And Automation Research Inst, Hungarian Academy Of Sciences
Budapest
Dr. Peter INZELT+361-209-5257
+361-466-7503
Digital Banking System Ltd
BUDAPEST
GYORGY
GASPAR
00-36-1-212-1668
00-36-1-457-6945
[email protected] 2 IST-1999-12095
HMC-MSCS
HUNGARIAN MEDICAL CHAMBER MULTIFUNCTIONAL SMART CARD SYSTEM
IST-99-1-1A
KA I
1.1.2.-1.2.1
Personal health systems
Hungary
Hungarian Medical Centre BUDAP
EST
DR. GEZA
GYENES
+361-2694391
+361-2694392
Technical University Of Budapest BUDAP
EST
DR VICE RECTOR
GYORGY
HORVAI
36-1 4632271
36-1 4632270
[email protected] IST-1999-13109
REHAROB SUPPORTING REHABILITATION OF DISABLED USING INDUSTRIAL ROBOTS FOR UPPER LIMB MOTION THERAPY
IST-99-1-1A
KA I
1.1.2.-1.2.1
Personal health systems
Hungary
National Institute For Medical Rehabilitation
BUDAPEST
PROF.
LAJOS
KULLMANN
36-1 3945733
36-1 2008834
4 IST-1999-10208
CORSHE CITIZEN_ORIENTED ROADMAP OF SENSORS FOR HEALTHCARE
IST-99-1-1A
KA I
1.1.2.-1.2.1
Personal health systems
Hungary Technical University Of Budapest BUDAP
EST
VICE RECTOR PROF
GYORGY
HORVAI
(36 1) 46 322 71
(46 1) 46 322 70
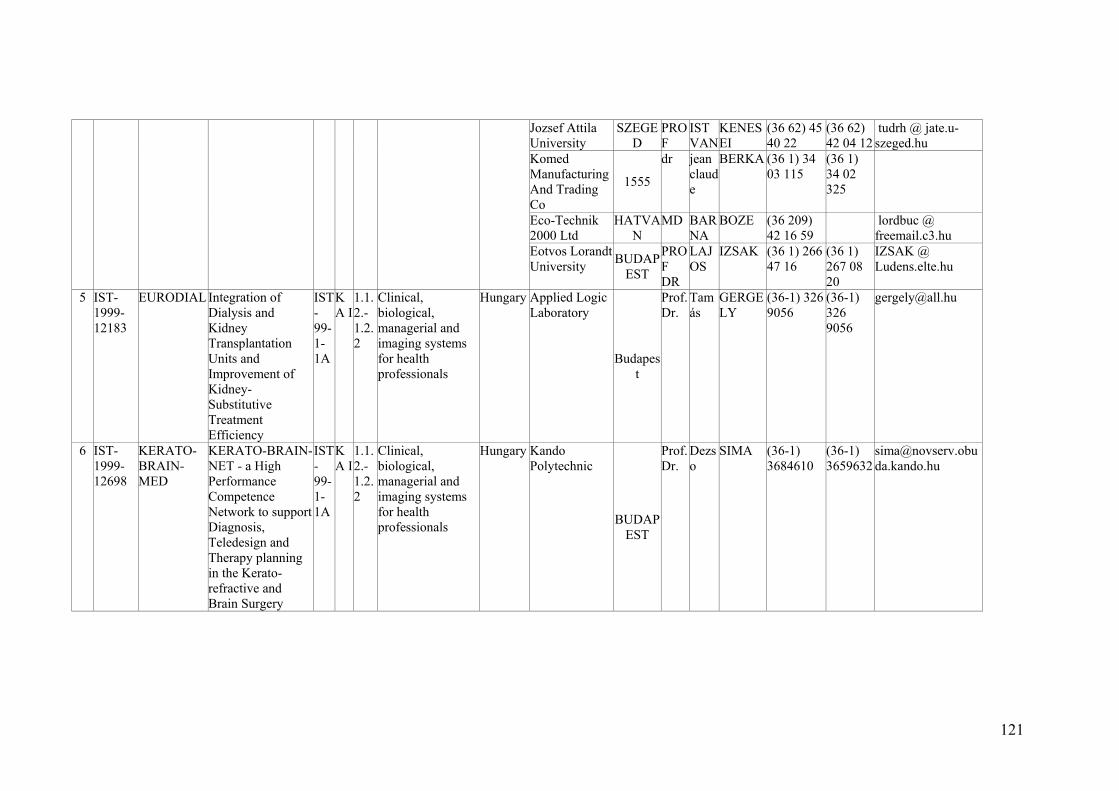
121
Jozsef Attila University
SZEGED
PROF
ISTVAN
KENESEI
(36 62) 45 40 22
(36 62) 42 04 12
tudrh @ jate.u-szeged.hu
Komed Manufacturing And Trading Co
1555
dr jean claude
BERKA (36 1) 34 03 115
(36 1) 34 02 325
Eco-Technik 2000 Ltd
HATVAN
MD BARNA
BOZE (36 209) 42 16 59
lordbuc @ freemail.c3.hu
Eotvos Lorandt University BUDAP
EST
PROF DR
LAJOS
IZSAK (36 1) 266 47 16
(36 1) 267 08 20
IZSAK @ Ludens.elte.hu
5 IST-1999-12183
EURODIAL Integration of Dialysis and Kidney Transplantation Units and Improvement of Kidney-Substitutive Treatment Efficiency
IST-99-1-1A
KA I
1.1.2.-1.2.2
Clinical, biological, managerial and imaging systems for health professionals
Hungary Applied Logic Laboratory
Budapest
Prof. Dr.
Tamás
GERGELY
(36-1) 326 9056
(36-1) 326 9056
6 IST-1999-12698
KERATO-BRAIN-MED
KERATO-BRAIN-NET - a High Performance Competence Network to support Diagnosis, Teledesign and Therapy planning in the Kerato- refractive and Brain Surgery
IST-99-1-1A
KA I
1.1.2.-1.2.2
Clinical, biological, managerial and imaging systems for health professionals
Hungary Kando Polytechnic
BUDAPEST
Prof. Dr.
Dezso
SIMA (36-1) 3684610
(36-1) 3659632
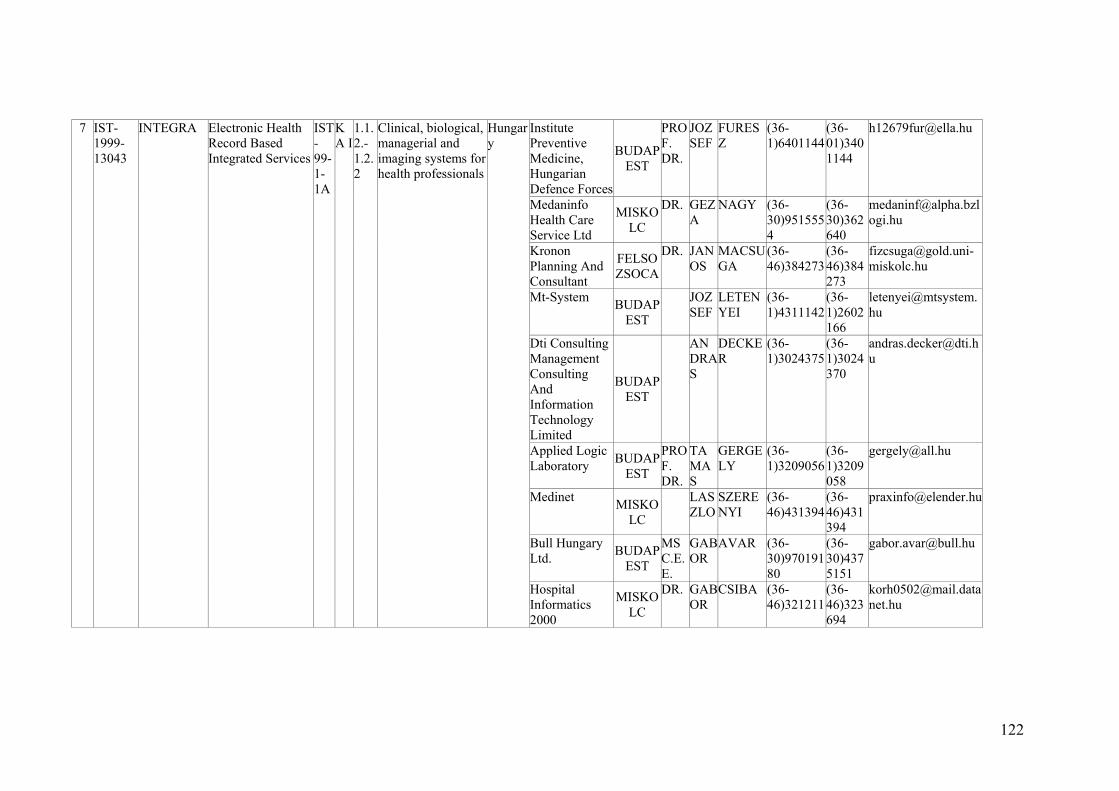
122
Institute Preventive Medicine, Hungarian Defence Forces
BUDAPEST
PROF. DR.
JOZSEF
FURESZ
(36-1)6401144
(36-01)3401144
Medaninfo Health Care Service Ltd
MISKOLC
DR. GEZA
NAGY (36-30)9515554
(36-30)362640
Kronon Planning And Consultant
FELSOZSOCA
DR. JANOS
MACSUGA
(36-46)384273
(36-46)384273
Mt-System BUDAPEST
JOZSEF
LETENYEI
(36-1)4311142
(36-1)2602166
Dti Consulting Management Consulting And Information Technology Limited
BUDAPEST
ANDRAS
DECKER
(36-1)3024375
(36-1)3024370
Applied Logic Laboratory BUDAP
EST
PROF. DR.
TAMAS
GERGELY
(36-1)3209056
(36-1)3209058
Medinet MISKOLC
LASZLO
SZERENYI
(36-46)431394
(36-46)431394
Bull Hungary Ltd. BUDAP
EST
MSC.E.E.
GABOR
AVAR (36-30)97019180
(36-30)4375151
7 IST-1999-13043
INTEGRA Electronic Health Record Based Integrated Services
IST-99-1-1A
KA I
1.1.2.-1.2.2
Clinical, biological, managerial and imaging systems for health professionals
Hungary
Hospital Informatics 2000
MISKOLC
DR. GABOR
CSIBA (36-46)321211
(36-46)323694
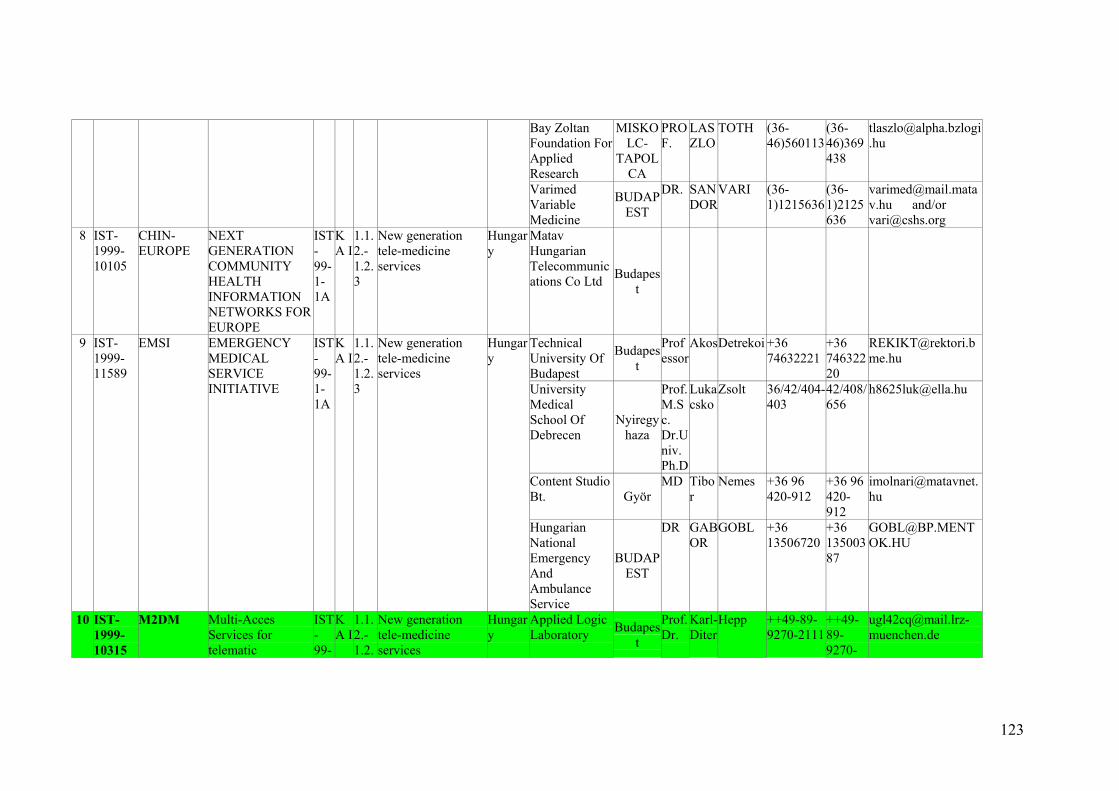
123
Bay Zoltan Foundation For Applied Research
MISKOLC-
TAPOLCA
PROF.
LASZLO
TOTH (36-46)560113
(36-46)369438
Varimed Variable Medicine
BUDAPEST
DR. SANDOR
VARI (36-1)1215636
(36-1)2125636
[email protected] and/or [email protected]
8 IST-1999-10105
CHIN-EUROPE
NEXT GENERATION COMMUNITY HEALTH INFORMATION NETWORKS FOR EUROPE
IST-99-1-1A
KA I
1.1.2.-1.2.3
New generation tele-medicine services
Hungary
Matav Hungarian Telecommunications Co Ltd Budapes
t
Technical University Of Budapest
Budapest
Professor
AkosDetrekoi +36 74632221
+36 74632220
University Medical School Of Debrecen
Nyiregyhaza
Prof. M.Sc. Dr.Univ. Ph.D
Lukacsko
Zsolt 36/42/404-403
42/408/656
Content Studio Bt. Györ
MD Tibor
Nemes +36 96 420-912
+36 96 420-912
9 IST-1999-11589
EMSI EMERGENCY MEDICAL SERVICE INITIATIVE
IST-99-1-1A
KA I
1.1.2.-1.2.3
New generation tele-medicine services
Hungary
Hungarian National Emergency And Ambulance Service
BUDAPEST
DR GABOR
GOBL +36 13506720
+36 13500387
10 IST-1999-10315
M2DM Multi-Acces Services for telematic
IST-99-
KA I
1.1.2.-1.2.
New generation tele-medicine services
Hungary
Applied Logic Laboratory Budapes
t
Prof. Dr.
Karl-Diter
Hepp ++49-89-9270-2111
++49-89-9270-
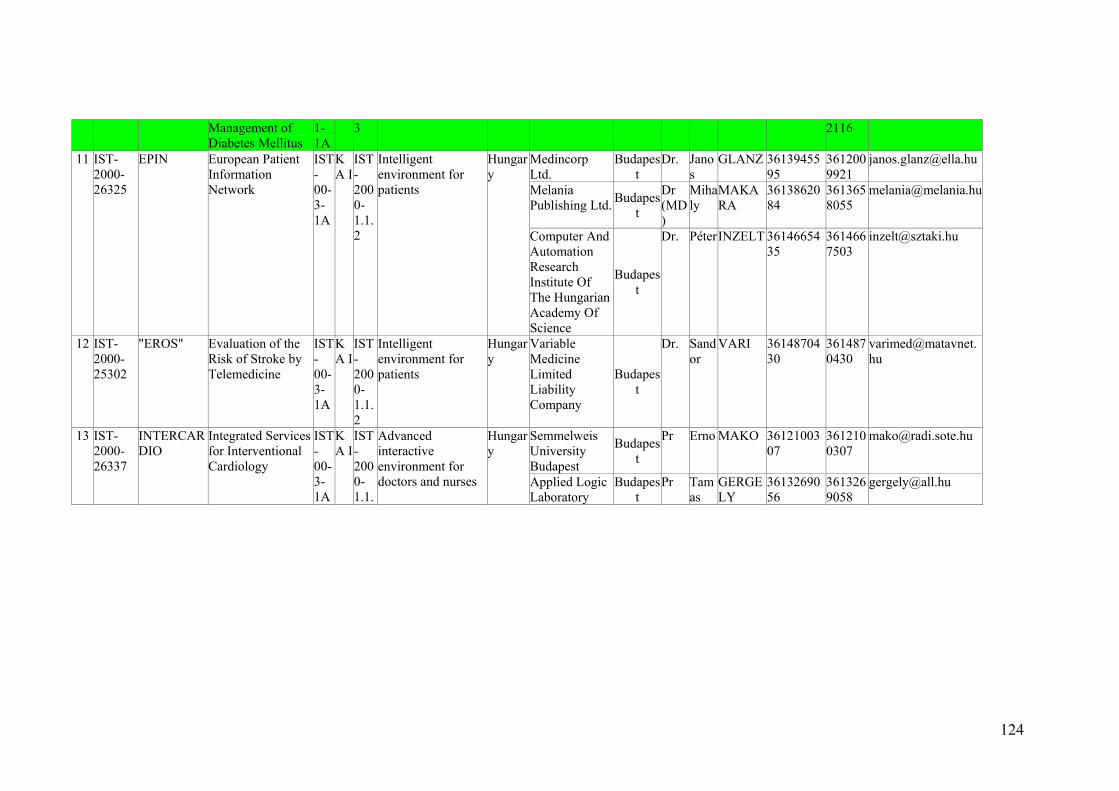
124
Management of Diabetes Mellitus
1-1A
3 2116
Medincorp Ltd.
Budapest
Dr. Janos
GLANZ 3613945595
3612009921
Melania Publishing Ltd. Budapes
t
Dr (MD)
Mihaly
MAKARA
3613862084
3613658055
11 IST-2000-26325
EPIN European Patient Information Network
IST-00-3-1A
KA I
IST-2000-1.1.2
Intelligent environment for patients
Hungary
Computer And Automation Research Institute Of The Hungarian Academy Of Science
Budapest
Dr. PéterINZELT 3614665435
3614667503
12 IST-2000-25302
"EROS" Evaluation of the Risk of Stroke by Telemedicine
IST-00-3-1A
KA I
IST-2000-1.1.2
Intelligent environment for patients
Hungary
Variable Medicine Limited Liability Company
Budapest
Dr. Sandor
VARI 3614870430
3614870430
Semmelweis University Budapest
Budapest
Pr Erno MAKO 3612100307
3612100307
[email protected] 13 IST-2000-26337
INTERCARDIO
Integrated Services for Interventional Cardiology
IST-00-3-1A
KA I
IST-2000-1.1.
Advanced interactive environment for doctors and nurses
Hungary
Applied Logic Laboratory
Budapest
Pr Tamas
GERGELY
3613269056
3613269058
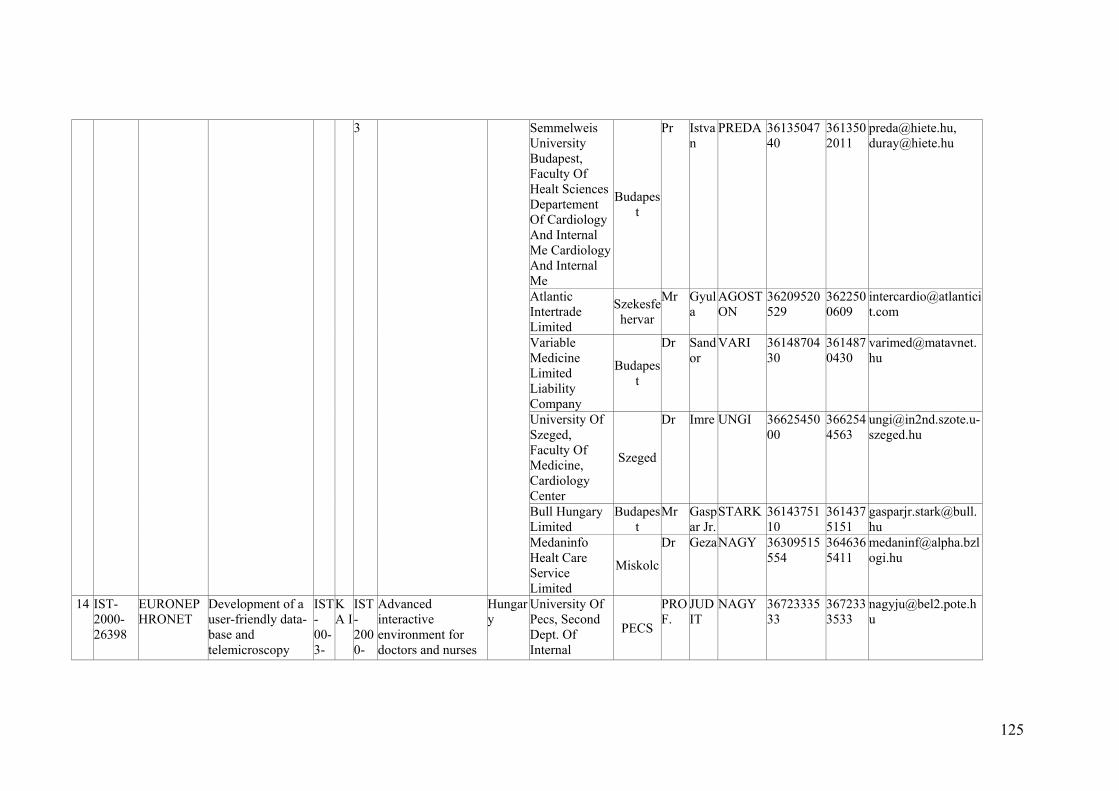
125
Semmelweis University Budapest, Faculty Of Healt Sciences Departement Of Cardiology And Internal Me Cardiology And Internal Me
Budapest
Pr Istvan
PREDA 3613504740
3613502011
[email protected], [email protected]
Atlantic Intertrade Limited
Szekesfehervar
Mr Gyula
AGOSTON
36209520529
3622500609
Variable Medicine Limited Liability Company
Budapest
Dr Sandor
VARI 3614870430
3614870430
University Of Szeged, Faculty Of Medicine, Cardiology Center
Szeged
Dr Imre UNGI 3662545000
3662544563
Bull Hungary Limited
Budapest
Mr Gaspar Jr.
STARK 3614375110
3614375151
3
Medaninfo Healt Care Service Limited
Miskolc
Dr GezaNAGY 36309515554
3646365411
14 IST-2000-26398
EURONEPHRONET
Development of a user-friendly data-base and telemicroscopy
IST-00-3-
KA I
IST-2000-
Advanced interactive environment for doctors and nurses
Hungary
University Of Pecs, Second Dept. Of Internal
PECS
PROF.
JUDIT
NAGY 3672333533
3672333533
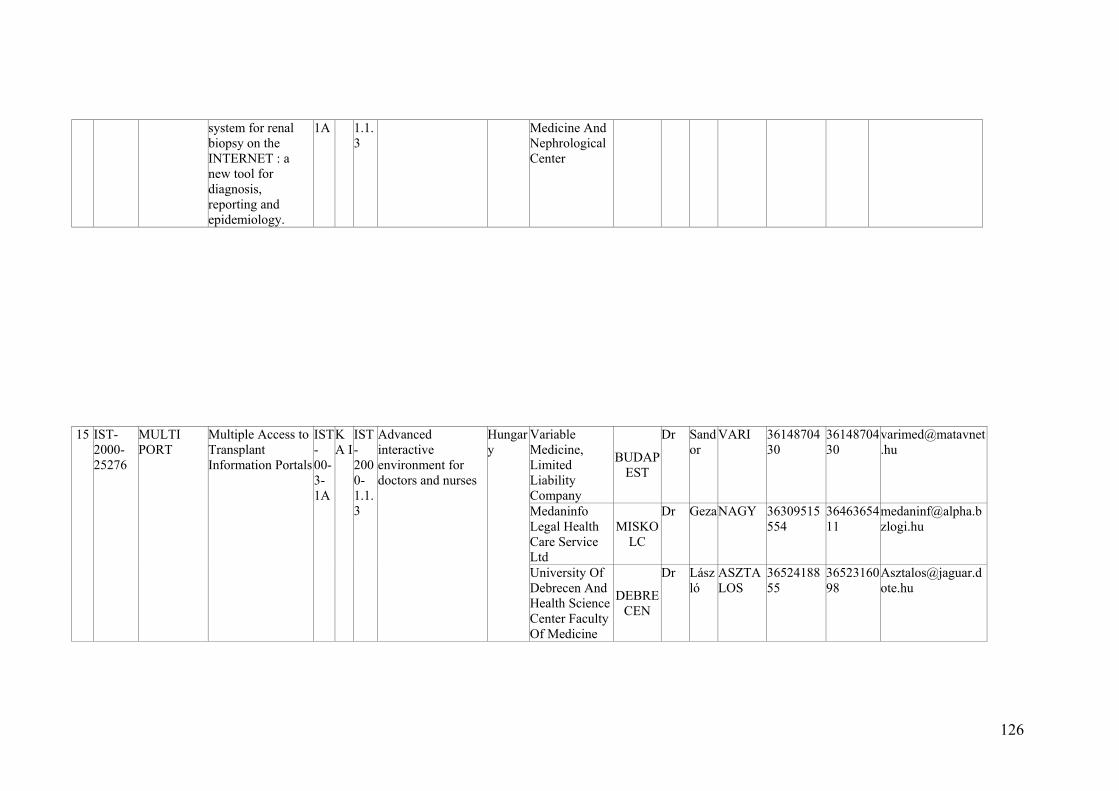
126
system for renal biopsy on the INTERNET : a new tool for diagnosis, reporting and epidemiology.
1A 1.1.3
Medicine And Nephrological Center
Variable Medicine, Limited Liability Company
BUDAPEST
Dr Sandor
VARI 3614870430
3614870430
Medaninfo Legal Health Care Service Ltd
MISKOLC
Dr GezaNAGY 36309515554
3646365411
15 IST-2000-25276
MULTI PORT
Multiple Access to Transplant Information Portals
IST-00-3-1A
KA I
IST-2000-1.1.3
Advanced interactive environment for doctors and nurses
Hungary
University Of Debrecen And Health Science Center Faculty Of Medicine
DEBRECEN
Dr László
ASZTALOS
3652418855
3652316098
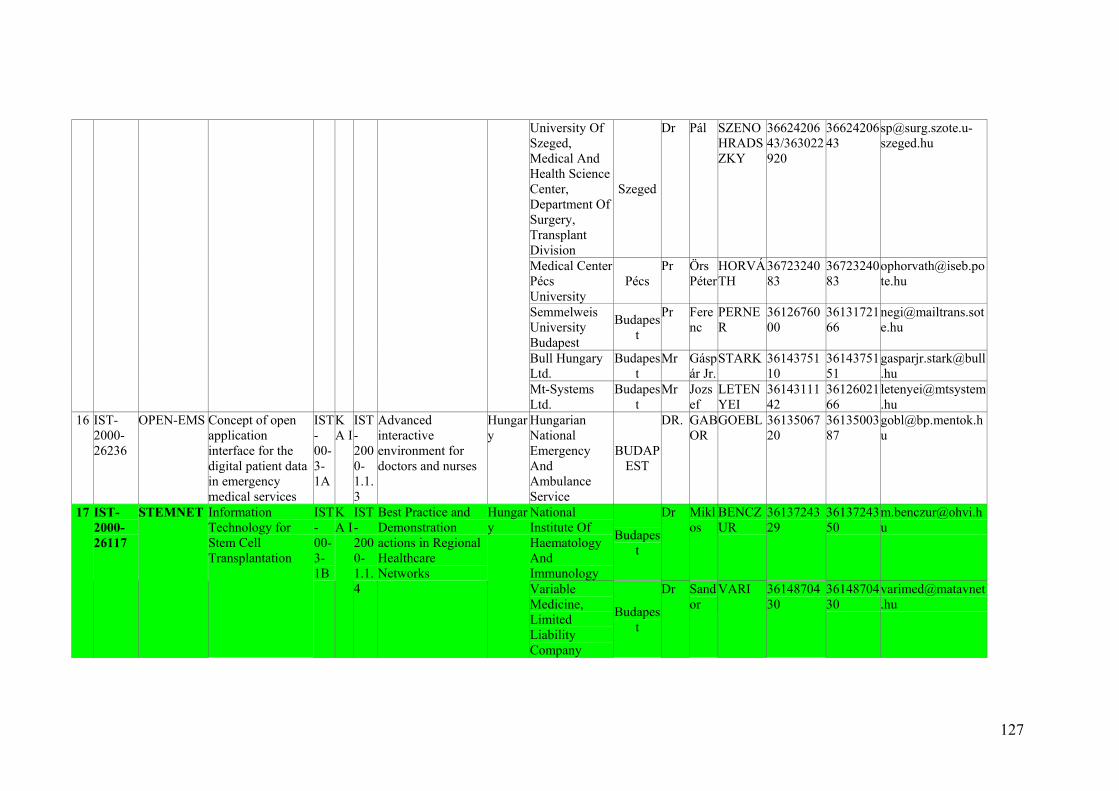
127
University Of Szeged, Medical And Health Science Center, Department Of Surgery, Transplant Division
Szeged
Dr Pál SZENOHRADSZKY
3662420643/363022920
3662420643
Medical Center Pécs University
Pécs Pr Örs
PéterHORVÁTH
3672324083
3672324083
Semmelweis University Budapest
Budapest
Pr Ferenc
PERNER
3612676000
3613172166
Bull Hungary Ltd.
Budapest
Mr Gáspár Jr.
STARK 3614375110
3614375151
Mt-Systems Ltd.
Budapest
Mr Jozsef
LETENYEI
3614311142
3612602166
16 IST-2000-26236
OPEN-EMS Concept of open application interface for the digital patient data in emergency medical services
IST-00-3-1A
KA I
IST-2000-1.1.3
Advanced interactive environment for doctors and nurses
Hungary
Hungarian National Emergency And Ambulance Service
BUDAPEST
DR. GABOR
GOEBL 3613506720
3613500387
National Institute Of Haematology And Immunology
Budapest
Dr Miklos
BENCZUR
3613724329
3613724350
17 IST-2000-26117
STEMNET Information Technology for Stem Cell Transplantation
IST-00-3-1B
KA I
IST-2000-1.1.4
Best Practice and Demonstration actions in Regional Healthcare Networks
Hungary
Variable Medicine, Limited Liability Company
Budapest
Dr Sandor
VARI 3614870430
3614870430
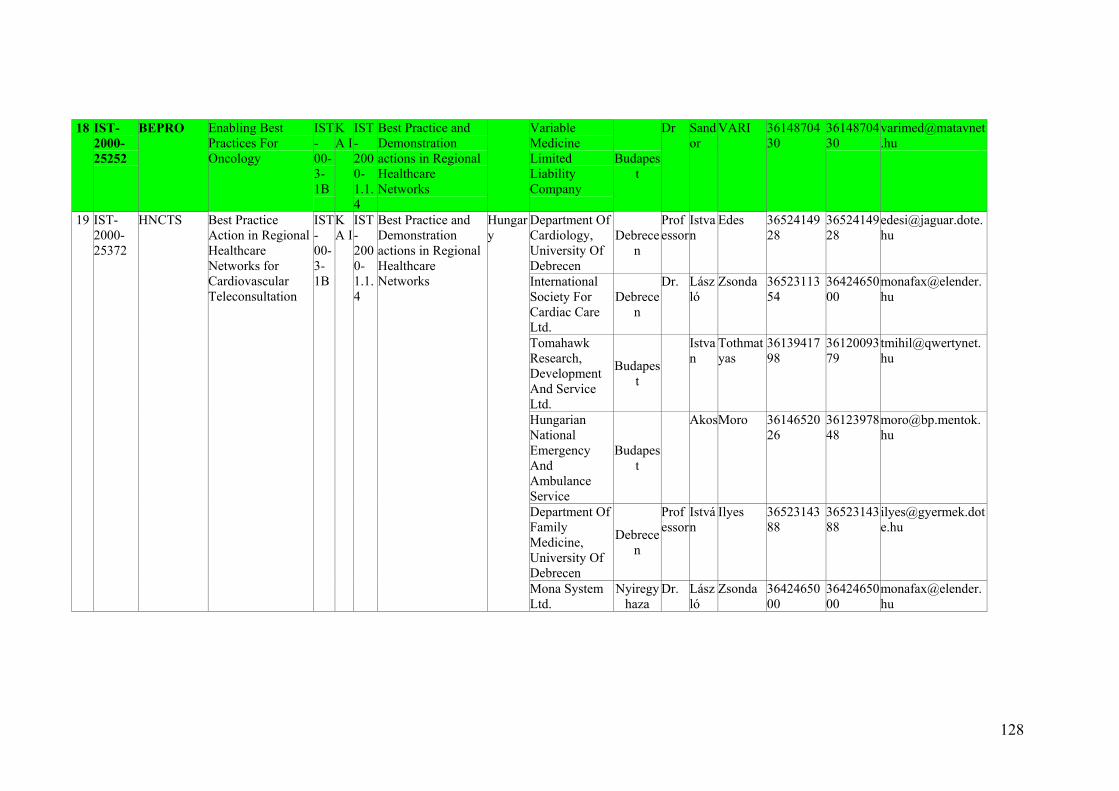
128
18 IST-2000-25252
BEPRO Enabling Best Practices For Oncology
IST-00-3-1B
KA I
IST-2000-1.1.4
Best Practice and Demonstration actions in Regional Healthcare Networks
Variable Medicine Limited Liability Company
Budapest
Dr Sandor
VARI 3614870430
3614870430
Department Of Cardiology, University Of Debrecen
Debrecen
Professor
Istvan
Edes 3652414928
3652414928
International Society For Cardiac Care Ltd.
Debrecen
Dr. László
Zsonda 3652311354
3642465000
Tomahawk Research, Development And Service Ltd.
Budapest
Istvan
Tothmatyas
3613941798
3612009379
Hungarian National Emergency And Ambulance Service
Budapest
AkosMoro 3614652026
3612397848
Department Of Family Medicine, University Of Debrecen
Debrecen
Professor
István
Ilyes 3652314388
3652314388
19 IST-2000-25372
HNCTS Best Practice Action in Regional Healthcare Networks for Cardiovascular Teleconsultation
IST-00-3-1B
KA I
IST-2000-1.1.4
Best Practice and Demonstration actions in Regional Healthcare Networks
Hungary
Mona System Ltd.
Nyiregyhaza
Dr. László
Zsonda 3642465000
3642465000
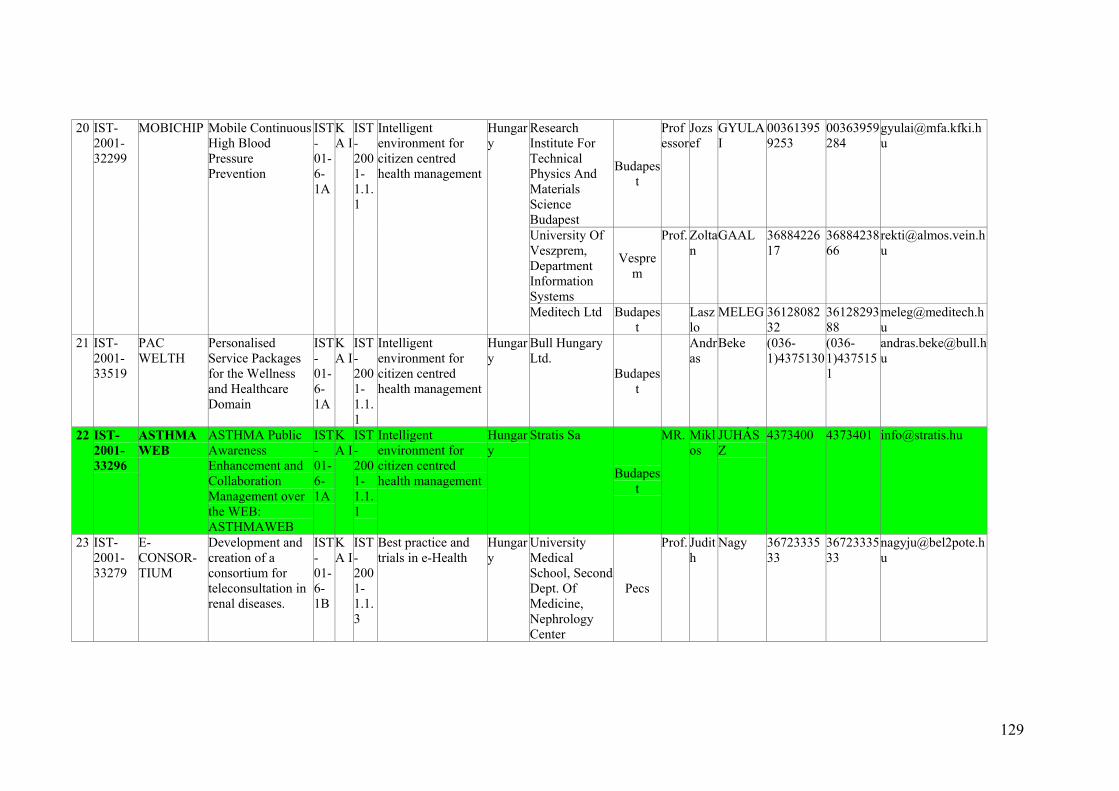
129
Research Institute For Technical Physics And Materials Science Budapest
Budapest
Professor
Jozsef
GYULAI
003613959253
00363959284
University Of Veszprem, Department Information Systems
Vesprem
Prof. Zoltan
GAAL 3688422617
3688423866
20 IST-2001-32299
MOBICHIP Mobile Continuous High Blood Pressure Prevention
IST-01-6-1A
KA I
IST-2001-1.1.1
Intelligent environment for citizen centred health management
Hungary
Meditech Ltd Budapest
Laszlo
MELEG 3612808232
3612829388
21 IST-2001-33519
PAC WELTH
Personalised Service Packages for the Wellness and Healthcare Domain
IST-01-6-1A
KA I
IST-2001-1.1.1
Intelligent environment for citizen centred health management
Hungary
Bull Hungary Ltd.
Budapest
Andras
Beke (036-1)4375130
(036-1)4375151
22 IST-2001-33296
ASTHMA WEB
ASTHMA Public Awareness Enhancement and Collaboration Management over the WEB: ASTHMAWEB
IST-01-6-1A
KA I
IST-2001-1.1.1
Intelligent environment for citizen centred health management
Hungary
Stratis Sa
Budapest
MR. Miklos
JUHÁSZ
4373400 4373401 [email protected]
23 IST-2001-33279
E-CONSOR-TIUM
Development and creation of a consortium for teleconsultation in renal diseases.
IST-01-6-1B
KA I
IST-2001-1.1.3
Best practice and trials in e-Health
Hungary
University Medical School, Second Dept. Of Medicine, Nephrology Center
Pecs
Prof. Judith
Nagy 3672333533
3672333533
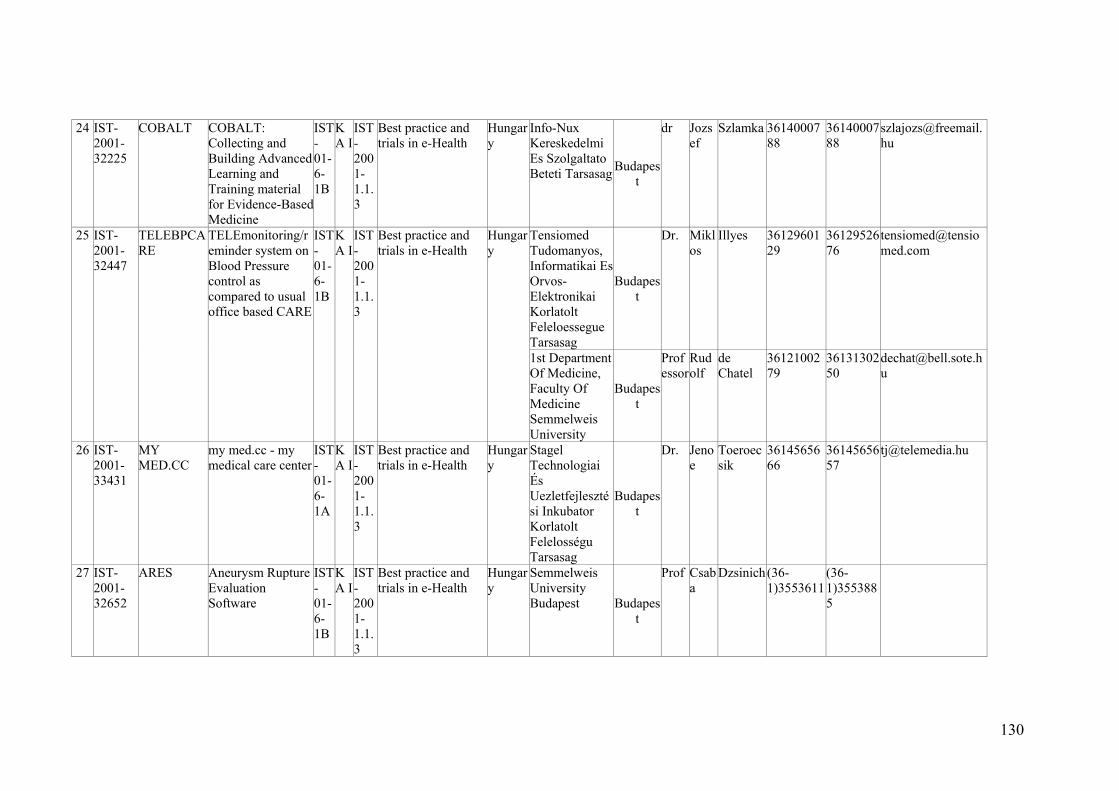
130
24 IST-2001-32225
COBALT COBALT: Collecting and Building Advanced Learning and Training material for Evidence-Based Medicine
IST-01-6-1B
KA I
IST-2001-1.1.3
Best practice and trials in e-Health
Hungary
Info-Nux Kereskedelmi Es Szolgaltato Beteti Tarsasag Budapes
t
dr Jozsef
Szlamka 3614000788
3614000788
Tensiomed Tudomanyos, Informatikai Es Orvos- Elektronikai Korlatolt Feleloessegue Tarsasag
Budapest
Dr. Miklos
Illyes 3612960129
3612952676
25 IST-2001-32447
TELEBPCARE
TELEmonitoring/reminder system on Blood Pressure control as compared to usual office based CARE
IST-01-6-1B
KA I
IST-2001-1.1.3
Best practice and trials in e-Health
Hungary
1st Department Of Medicine, Faculty Of Medicine Semmelweis University
Budapest
Professor
Rudolf
de Chatel
3612100279
3613130250
26 IST-2001-33431
MY MED.CC
my med.cc - my medical care center
IST-01-6-1A
KA I
IST-2001-1.1.3
Best practice and trials in e-Health
Hungary
Stagel Technologiai És Uezletfejlesztési Inkubator Korlatolt Felelosségu Tarsasag
Budapest
Dr. Jenoe
Toeroecsik
3614565666
3614565657
27 IST-2001-32652
ARES Aneurysm Rupture Evaluation Software
IST-01-6-1B
KA I
IST-2001-1.1.3
Best practice and trials in e-Health
Hungary
Semmelweis University Budapest Budapes
t
Prof Csaba
Dzsinich(36-1)3553611
(36-1)3553885
Annex XI
Department Of Informatics, National Institute And Library For Health Information, Hungary The Medical Documentation Centre, established in 1949 by the Hungarian Academy of Sciences, was founded with the purpose to provide the Hungarian medical community with the latest achievement of foreign medical sciences. In 1957 the institute – called the National Documentation Institute and Library of Medicine – functioned as a background institution of the Ministry of Health; since 1960 it operated as a national medical and health reference library and as the centre of the Hungarian network of medical libraries. Today the National Institute and Library for Health Information is sponsored by the Ministry of Health and is the professional information centre of the healthcare field in Hungary. Its function is to provide information and literature to healthcare institutes, the community at large, and experts working in the healthcare profession. Health communication The Ministry of Health formulated its national health promotion strategy in 1999. An essential element of this strategy was the decision to create a communication centre and network that covers the entire country and ties together the whole of Hungarian health communication. Central to health communication activities at MEDINFO will be the development of the structure and content of an Internet-based network and the operation of a user-friendly system. This will be closely connected with the preparation of publications that supplement Internet services and with the organisation of professional conferences that allow personal exchange of information. An additional goal is to establish co-operation with the health communication media market, both in the visual and the printed media. Healthline The services of MEDINFO - as a mediator of healthcare and health promotion information - is called Healthline. Healthline is a comprehensive health information service provided to a wide spectrum of users and is built upon 3 pillars: Internet access Professional publications Professional forums, conferences Some of the services already available on the Internet European Union news Health informatics newsletter Health promotion information Primary care information service Online library catalogue Hungarian Medical Bibliography Community health information database Career information for medical school graduates Journal for nurses Library information services Computerised literature searches Reference services Interlibrary lending Preparation of studies on the healthcare system of countries around the world National documentation centre and deposit library of the European Regional Office of the World Health Organisation Co-operation with the UK Cochrane Centre Marketing activities MEDINFO engages also in marketing activities: Translation and interpretation service
132
Publishing and editing activities Market surveys PR programs Organisation of meetings and conferences National Library of Health Sciences The National Institute and Library for Health Information (MEDINFO) operates a special library providing nationwide services to doctors, nurses, Ministry of Health staff, healthcare managers and other health workers. The library also fulfils the information needs of professionals working in educational and healthcare institutes, as well as users of community health information. The library has a full range of collection of Hungarian publications on medical science and related fields, social and family affairs, health promotion and health communication. Selected publications from the foreign literature in the above fields are also available. Proprietary databases The Magyar Orvosi Bibliográfia (Hungarian Medical Bibliography) provides complete coverage of the Hungarian medial literature. The Hungarian Medical Bibliography contains reference and bibliographical information of selected journal articles in the Hungarian medial literature in the English language.. Community Health Information is a database of articles, health care services and news from the lay media. The Clinical Practice Guidelines bibliography is a database of diagnostic and therapeutic procedures and recommendations. We also have access to international literature databases: Medline, Embase, HealthStar, Justis, OECD etc . Other services Our library is a national documentation centre and deposit library of the European Regional Office of the World Health Organisation. We collect and organise information on the healthcare systems and social policies of the countries around the world. We maintain a central catalogue of foreign books, annals, serial publications, congress publications and computerised databases available in all health and medical libraries in Hungary. Library use The library is open without restriction to any Hungarian and foreign citizen over 16 and can be used in person, on the telephone/fax or via e-mail. The reading room is available for using the international and Hungarian pe riodicals and monographs on the premises. Journals, materials from the reference collection and CD-ROM databases can be used only in the reading room. Photocopies of documents can be obtained upon request. Books and videotapes can be borrowed for a period of four weeks, 4 items taken at a time. It is permitted to renew material once for another four weeks provided there is no claim for the publications by other patrons. Renewals can be done in person, over the telephone or fax. Requests for interlibrary loans are filled from the collection of our library and the associated libraries. We undertake the borrowing of foreign books or articles from international journals through the British Library. Informatics Department The basic task of the Informatics Department is to fulfil Medinfo's information technology needs, to strengthen the institute's informatic autonomy and competence, and to build appropriate partnership with outside health care and IT institutes. These activities are performed in concert with the other departments and divisions. Other tasks

133
Implementation of the objectives of Health Communication Division as defined in the Division's strategy Performance of OLIB webmaster tasks for the National Library of Health Sciences Co-operation with the Publishing and Service Division in the electronic publication of Medinfo's marketing tasks Performance of software and hardware monitoring for the Finances Department Other activities covering the whole institute: Publishing Medinfo products on the Internet and providing the technological background for the edition of the web portal called Healthline Maintenance of PCs, peripherals and application software IT development, preparation of informatics procurement, supervision of its implementation The objective of the Department is to initiate and maintain professional partnerships with Sectoral and intersectoral partners: participation in laying the foundation for the health communication of the institute Partners in the private sector: laying the professional foundation for building partnership of the institute, supervision of co-operation

134
Annex XII
Regional and International Integrated Telemedicine Network for Organ Transplant, Hungary Abstract:
A substantial proportion of future medical practice will depend greatly on improved collaboration between the providers throughout the healthcare sector, and effective sharing of data and expertise by different healthcare professionals. In organ transplant it is a rule, donor organs are matched to recipients via national or multinational organ-sharing organizations. Only through close co-operation between transplant surgeons, immunologist, nephrologist, pathologist, radiologist and other physicians could increase the efficiency of organ transplant. Information technology (IT) became an inevitable and inherent part of transplantation medicine. RETRANSPLANT project interfaces and integrates information technologies (IT) from the European Union Fourth Framework projects to support the development of regional organ transplant information networks in Central Europe.
The RETRANSPLANT project aims to facilitate the development of Telematics tools for dialysis and organ transplant centers, organisations coordinating recipient-donor selection, and other health care facilities for transplant services in the Central Eastern European Countries (CEEC). In Europe, as a rule, donor organs are matched to recipients by national or multinational organ-sharing organizations. EUROTRANSPLANT, for example, serves medical institutions in Germany, Austria, and the Benelux states, HUNGARO-TRANSPLANT in Hungary, and SLOVENJA-TRANSPLANT in Slovenia. During the project lifetime the RETRANSPLANT consortium will carry out the following outcome: First the partners will implement an electronic patient database for transplant waiting list, donor-recipient matching, organ allocation, and patient selection in the Czech Republic, Lithuania, Hungary, Slovak Republic, Slovenia, and Poland. Recipient - the Donor Selection (RDS) network will help an optimal use of available donor organs and tissues. It is obvious that such activity is useful for both parties i. e. the EU and CEEC. Any potential donor in the CEEC countries might become matched for a EU patient and vice versa. The DialysisCard and TransplantCard have to be seen as an identification card, additional data storage and management tool for dialysis and transplant patient in Hungary and Slovenia. The communication model allows for different types of workstations for the different environments to communicate with these active memory Smart Cards. Implementation of an Electronic Medical Record (EMR) system at the organ transplant centres in Hungary (Budapest, Szeged), and Slovenia (Ljubljana) comprises all clinical records. The EMR contains standardised codes and information about diagnoses (ICPC/ICD10), drugs, procedures, investigations, laboratory tests. etc. To ensure standardised and identical information, it is recommended that these indexes are updated centrally. This makes it easier to transfer information about the patients from one health care facility to another.

135
Annex XIII
Health care on-line – abstract from ePolska Action Plan, Poland Assumptions Modern medicine, which intensively exploits growing information resources, faces a necessity of using processing and data transmission technologies. The technological progress has enabled distance diagnostic examinations and consultations. The best known examples are the possibility of distance heart examination (EKG, assessment of heart stimulators implanted). Already commonplace, the endoscope operation technique, during which visual control of the course of an operation is possible simply on a monitor screen, is a certain forerunner of that type of treatment – “virtual” procedures. Thus, an area called telemedicine* has emerged, which is a blessing especially for people who are not self-dependant and who cannot leave their homes on their own. As a result of the technological progress, some activities associated with the treatment process, hitherto reserved for doctors and specialist laboratories, will be so automated and simplified that it will be possible for patients to carry them out on their own, and a doctor will only be a teleconsultant overseeing the course of treatment. Another process which will raise a conscious participation of patients in treatment-related decisions will be universal access to medical information. Thanks to the existence of data bases with medical information in the Internet, the patient will be able at any time to obtain such information (e.g., the location and speciality of a doctor, medical services on offer, surgery hours, etc.). Therefore, the existing traditional paternalistic doctor – patient relation, which has been predominant until now, will be a more symmetric relation in the future. The globalisation of medical tasks, and free and increasingly faster flow of information within medicine itself, as well as owing to economic processes taking place outside medicine, will result in the standardisation of treatment. It will have an impact both on the improvement of medical services quality and the possibility of reducing health services costs. An enormous progress in health care and treatment, with the simultaneous lengthening of human life and ageing populations, inevitably leads to an increase in spending on health care. Thus, there is double challenge: to improve the quality and accessibility of health care for citizens, while constraining overall costs. These challenges will be impossible to meet without the deployment and widespread use of fully integrated, interoperable and modernised health systems. The dissemination of software supporting hospital and health care management in the macro scale, facilitating data collection and analysis (results of examinations, diagnosis, etc) or supporting the work of individual surgeries, would enhance effectiveness of health care. The effectiveness of health care exploiting digital technology capabilities will be conditional, to a great extent, upon co-ordination activities of the Health Care Information Systems Centre, established by the Minister of Health in September 2000. In accordance with principal tasks provided for in its charter, the Centre’s activities are focused on: establishing standards in the area of health care information systems, which incorporate European Union regulations and solutions, preparing and expressing opinion on legal acts which govern the functioning of health care in the process of its “going digital”, monitoring material and human resources, as well as the degree of accessibility to medical services, preparing projects relating to the development and enhancement of the medical services registration system,
136
co-ordinating the operation of the RUM *(Medical Services Register), informing, educating and putting out publications relating to the tasks performed. Alongside the Health Care Information Systems Centre, a data base on medical establishments and facilities was created. An essential change is a new, i.e., electronic form of the register of health care establishments and the use of identification codes. The register of health care establishments, and in the future ambulance fleets, individual medical practices and pharmacies, will become a universal source of knowledge on the functioning of the sector and a starting point for any analyses and projections. The combination of modern information and communication technologies with medicine will facilitate contact of the patient with the doctor, and will be instrumental in fast interchange of information between medical facilities and personnel, what will undoubtedly improve the quality of patients’ lives and efficiency of health care services. Objectives To prepare the society to consciously use information on health care and health prevention based on modern IT tools, To develop consumer information (for patients) as regards health care using IT tools, To use IT tools to promote healthy lifestyles and health education, To reduce costs of specialist medical care and enhance the medical care level by implementing telemedicine tools, in particular, outside large metropolitan areas, To ensure protection of patients’ personal data in electronic systems of medical data storage and exchange.. Planned actions Determination of standards for information collection and interchange, as well as data analysis in health care,
Creation of a uniform electronic data base on medical establishments and facilities, also incorporating the scope of services provided by them, available via the Internet,
Creation of a data base on medical emergency services units, available via the Internet,
Preparation of data bases containing information on persons covered by health insurance,
Creation of a patient data base,
Introduction of an electronic patient card,
Development and implementation of an electronic system which supports reporting and presentation of information on health care,
Establishment of the legal framework allowing payments for medical services to made over telematics networks,
Development of a plan for the application of telemedicine in health care,
Implementation of a pilot programme for the application of telemedicine in supporting treatment processes,
Launch of telediagnosis, teleconsultations, emergency teleservice, teleteaching, teleoperation,
Implementation of pilot programmes of health care personnel distance training,
Conduct of surveys on the impact of information and communication technologies on human psyche,
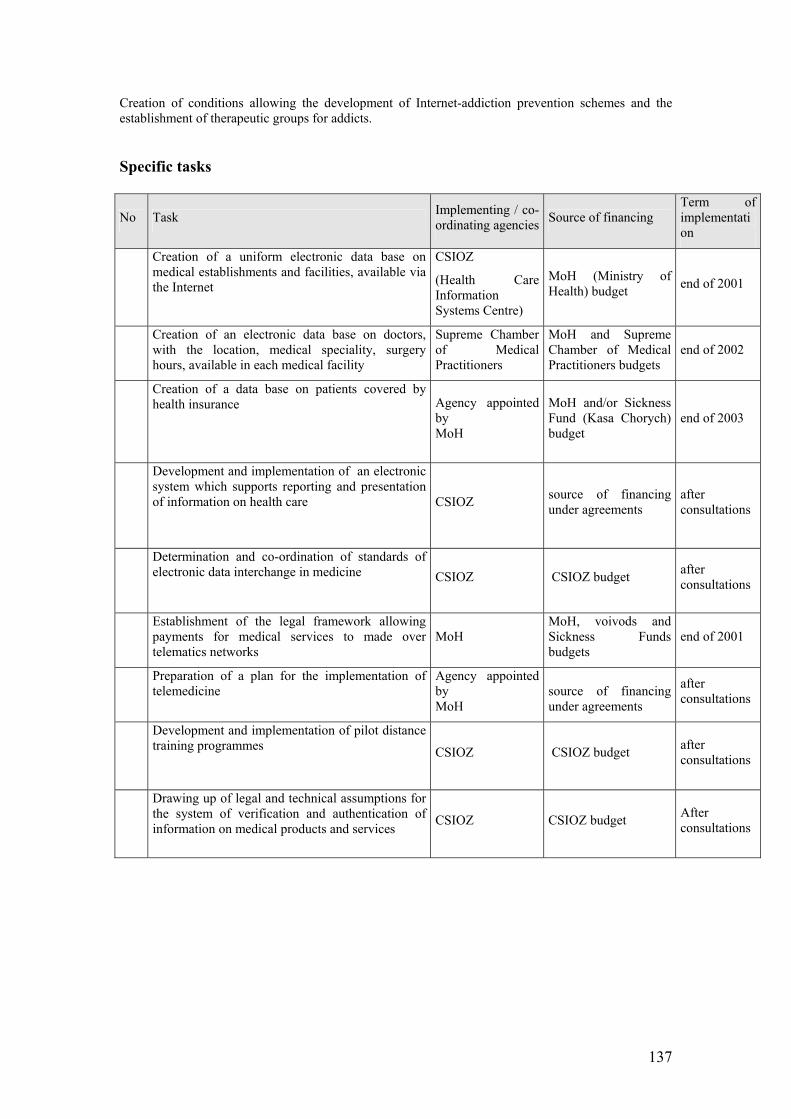
137
Creation of conditions allowing the development of Internet-addiction prevention schemes and the establishment of therapeutic groups for addicts.
Specific tasks
No Task Implementing / co-ordinating agencies Source of financing
Term of implementation
Creation of a uniform electronic data base on medical establishments and facilities, available via the Internet
CSIOZ
(Health Care Information Systems Centre)
MoH (Ministry of Health) budget end of 2001
Creation of an electronic data base on doctors, with the location, medical speciality, surgery hours, available in each medical facility
Supreme Chamber of Medical Practitioners
MoH and Supreme Chamber of Medical Practitioners budgets
end of 2002
Creation of a data base on patients covered by health insurance Agency appointed
by MoH
MoH and/or Sickness Fund (Kasa Chorych) budget
end of 2003
Development and implementation of an electronic system which supports reporting and presentation of information on health care
CSIOZ source of financing under agreements
after consultations
Determination and co-ordination of standards of electronic data interchange in medicine CSIOZ CSIOZ budget after
consultations
Establishment of the legal framework allowing payments for medical services to made over telematics networks
MoH MoH, voivods and Sickness Funds budgets
end of 2001
Preparation of a plan for the implementation of telemedicine
Agency appointed by MoH
source of financing under agreements
after consultations
Development and implementation of pilot distance training programmes CSIOZ CSIOZ budget after
consultations
Drawing up of legal and technical assumptions for the system of verification and authentication of information on medical products and services CSIOZ CSIOZ budget After
consultations
138
Annex XIV
Informatization of hospitals in the Malopolskie province, Poland The following are data describing IT in terms of hardware (in this case hospital's IT network), software (related to medical and administrative activities) and degree of it's integration in the Malopolskie province hospital. Malopolskie province is situated in the south-east of Poland with the capital city Crakow. Summary of the survey Final report: 1. Comparison of the results gained from the survey 2. Recapitulation 3. Enclosure – detailed comparison of the hospitals Part I – Comparison of the results of the survey In the 2nd half of 2002, from the initiative of Departament Polityki Społecznej Urzędu Marszałkowskiego Województwa Małopolskiego (Department of Social affairs of Malopolskie province) the research has been carried out to establish the level of IT in the Malopolskie hospitals. The collected data of the research are available in the Conclusion part of the report. The questionnaire with 5 questions has been sent to 50 hospitals. 49 hospitals have sent their reply. The following conclusions are with the level of reference (100%) to the 49 hospitals that accepted the survey. 1. Types of IT personnel in hospitals IT has been acknowledged as an important area for the function of the hospital in all surveyed units. All the institutions have at their disposal IT personnel. In some they are employed as contractors in others they are part of permanent staff. Hospitals also use the services of external IT companies. The following table and diagram show the differences in the way the IT personnel is employed in the hospitals. Type of employment Number of hospitals IT contractor 5 IT employee 23 IT employee and external firm 15 External firm 6
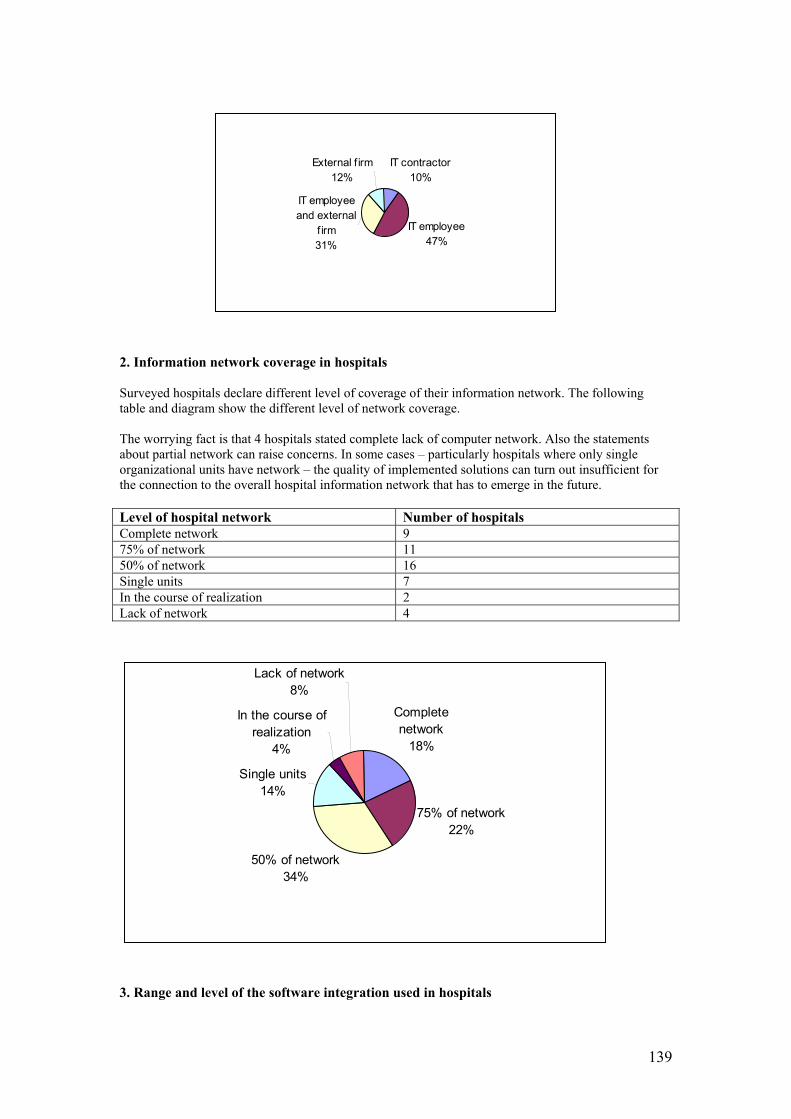
139
2. Information network coverage in hospitals Surveyed hospitals declare different level of coverage of their information network. The following table and diagram show the different level of network coverage. The worrying fact is that 4 hospitals stated complete lack of computer network. Also the statements about partial network can raise concerns. In some cases – particularly hospitals where only single organizational units have network – the quality of implemented solutions can turn out insufficient for the connection to the overall hospital information network that has to emerge in the future. Level of hospital network Number of hospitals Complete network 9 75% of network 11 50% of network 16 Single units 7 In the course of realization 2 Lack of network 4
3. Range and level of the software integration used in hospitals
IT contractor10%
IT employee47%
IT employee and external
f irm31%
External f irm12%
Complete network
18%
75% of network22%
50% of network34%
Single units14%
In the course of realization
4%
Lack of network8%
140
The full informatization of the hospital means the hospitals are fully equipped with complete IT network and have implemented the relevant software for the needs of medical staff and for administrative purposes. Both of the parts must be integrated. Certain level of hospital IT level has been demanded by institutions such as Zakład Ubezpieczeń Społecznych (Social insurance office) – program « Platnik » and Kasa Chorych (Health insurance office) – program « Start ». The below surveyed hospitals are ordered depending on a level of their software integration. Small number of hospitals (3) state the full integration of the software. 6 hospitals stated to be close to integrate medical and administrative parts. The rest of hospitals (40 institutions) are still a long way from integration. Lack of integration of the medical and admin parts can mean further requirements to implement additional software enabling the communication between the modules. The remaining hospitals didn’t have – at the time of the survey – software enabling the use of integrated computerized information system. Apart from this only 2 institutions stated work to be directed to the system implementation. The findings have shown that implementation of the medical software is regularly harder then of the administration. The fundamental element is the level of cooperation and acceptation of the software by medical staff. Reimbursement of the medical services by payer (Health Insurance Company) based on medical performances that is planned for the year 2004 has a consequence that there will be a need for integrated information hospital system for effective payment management. By not complying with this condition hospitals are risking big complications that are proportional to the size of the unit and the range of provided services. It is good to pay attention that among the number of hospitals (9 units) that are stating the ownership of full computerized network there are 3 hospitals having full software integration a 6 hospitals near the integration. Software and level of integration Number of hospitals Full integration 3 Close integration of medical and administrative software
6
Medical and administrative software is not integrated
19
Administrative software and incomplete stage of medical software
3
Administrative software. Medical software being implemented
1
Administrative software 5 Incomplete medical and administrative software 7 Partially administrative software 3 Single programs 1 In the course of realization 1
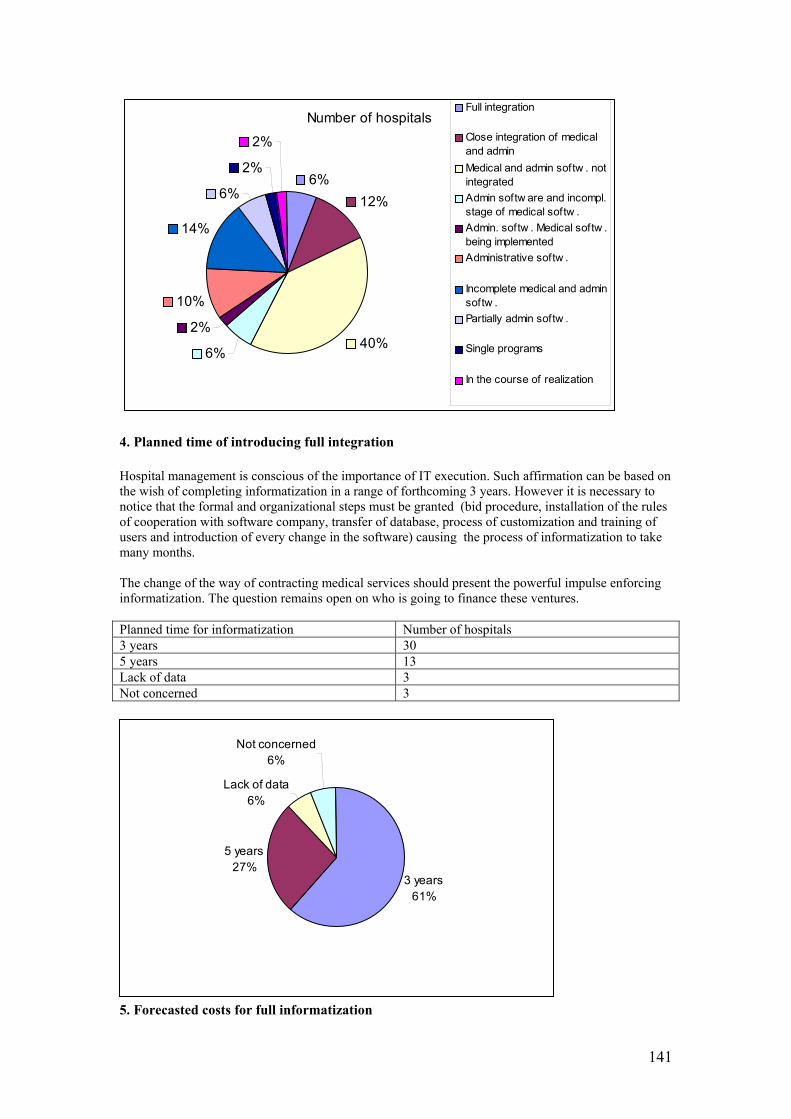
141
4. Planned time of introducing full integration Hospital management is conscious of the importance of IT execution. Such affirmation can be based on the wish of completing informatization in a range of forthcoming 3 years. However it is necessary to notice that the formal and organizational steps must be granted (bid procedure, installation of the rules of cooperation with software company, transfer of database, process of customization and training of users and introduction of every change in the software) causing the process of informatization to take many months. The change of the way of contracting medical services should present the powerful impulse enforcing informatization. The question remains open on who is going to finance these ventures. Planned time for informatization Number of hospitals 3 years 30 5 years 13 Lack of data 3 Not concerned 3
5. Forecasted costs for full informatization
Number of hospitals
6%12%
40%6%
2%
10%
14%
6%
2%
2%
Full integration
Close integration of medicaland adminMedical and admin softw . notintegratedAdmin softw are and incompl.stage of medical softw .Admin. softw . Medical softw .being implementedAdministrative softw .
Incomplete medical and adminsoftw .Partially admin softw .
Single programs
In the course of realization
3 years61%
5 years27%
Lack of data6%
Not concerned6%
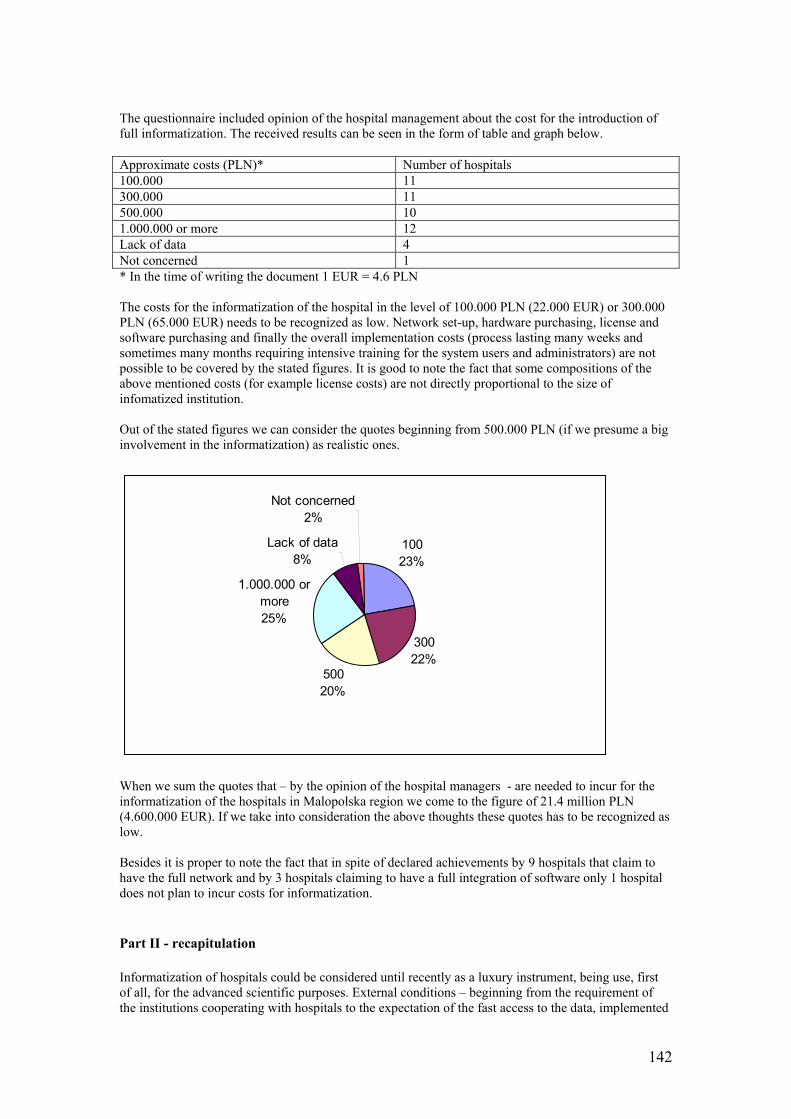
142
The questionnaire included opinion of the hospital management about the cost for the introduction of full informatization. The received results can be seen in the form of table and graph below. Approximate costs (PLN)* Number of hospitals 100.000 11 300.000 11 500.000 10 1.000.000 or more 12 Lack of data 4 Not concerned 1 * In the time of writing the document 1 EUR = 4.6 PLN The costs for the informatization of the hospital in the level of 100.000 PLN (22.000 EUR) or 300.000 PLN (65.000 EUR) needs to be recognized as low. Network set-up, hardware purchasing, license and software purchasing and finally the overall implementation costs (process lasting many weeks and sometimes many months requiring intensive training for the system users and administrators) are not possible to be covered by the stated figures. It is good to note the fact that some compositions of the above mentioned costs (for example license costs) are not directly proportional to the size of infomatized institution. Out of the stated figures we can consider the quotes beginning from 500.000 PLN (if we presume a big involvement in the informatization) as realistic ones.
When we sum the quotes that – by the opinion of the hospital managers - are needed to incur for the informatization of the hospitals in Malopolska region we come to the figure of 21.4 million PLN (4.600.000 EUR). If we take into consideration the above thoughts these quotes has to be recognized as low. Besides it is proper to note the fact that in spite of declared achievements by 9 hospitals that claim to have the full network and by 3 hospitals claiming to have a full integration of software only 1 hospital does not plan to incur costs for informatization. Part II - recapitulation Informatization of hospitals could be considered until recently as a luxury instrument, being use, first of all, for the advanced scientific purposes. External conditions – beginning from the requirement of the institutions cooperating with hospitals to the expectation of the fast access to the data, implemented
10023%
30022%
50020%
1.000.000 or more25%
Lack of data 8%
Not concerned2%
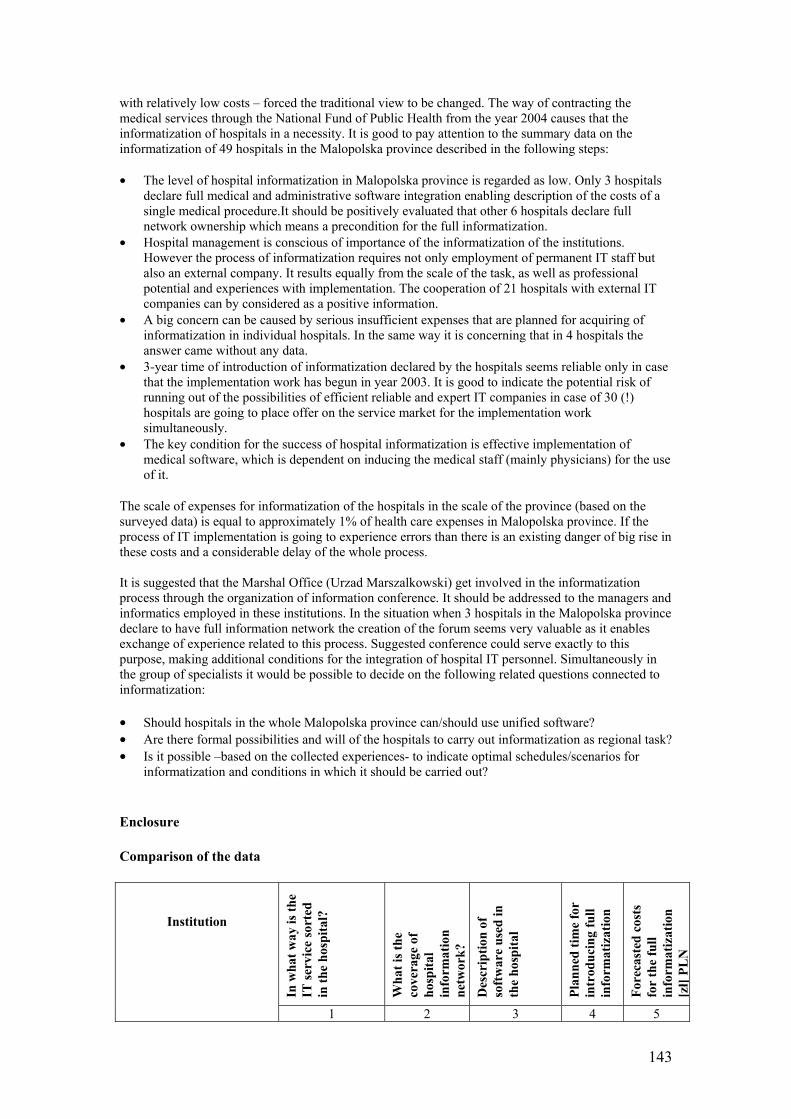
143
with relatively low costs – forced the traditional view to be changed. The way of contracting the medical services through the National Fund of Public Health from the year 2004 causes that the informatization of hospitals in a necessity. It is good to pay attention to the summary data on the informatization of 49 hospitals in the Malopolska province described in the following steps: • The level of hospital informatization in Malopolska province is regarded as low. Only 3 hospitals
declare full medical and administrative software integration enabling description of the costs of a single medical procedure.It should be positively evaluated that other 6 hospitals declare full network ownership which means a precondition for the full informatization.
• Hospital management is conscious of importance of the informatization of the institutions. However the process of informatization requires not only employment of permanent IT staff but also an external company. It results equally from the scale of the task, as well as professional potential and experiences with implementation. The cooperation of 21 hospitals with external IT companies can by considered as a positive information.
• A big concern can be caused by serious insufficient expenses that are planned for acquiring of informatization in individual hospitals. In the same way it is concerning that in 4 hospitals the answer came without any data.
• 3-year time of introduction of informatization declared by the hospitals seems reliable only in case that the implementation work has begun in year 2003. It is good to indicate the potential risk of running out of the possibilities of efficient reliable and expert IT companies in case of 30 (!) hospitals are going to place offer on the service market for the implementation work simultaneously.
• The key condition for the success of hospital informatization is effective implementation of medical software, which is dependent on inducing the medical staff (mainly physicians) for the use of it.
The scale of expenses for informatization of the hospitals in the scale of the province (based on the surveyed data) is equal to approximately 1% of health care expenses in Malopolska province. If the process of IT implementation is going to experience errors than there is an existing danger of big rise in these costs and a considerable delay of the whole process. It is suggested that the Marshal Office (Urzad Marszalkowski) get involved in the informatization process through the organization of information conference. It should be addressed to the managers and informatics employed in these institutions. In the situation when 3 hospitals in the Malopolska province declare to have full information network the creation of the forum seems very valuable as it enables exchange of experience related to this process. Suggested conference could serve exactly to this purpose, making additional conditions for the integration of hospital IT personnel. Simultaneously in the group of specialists it would be possible to decide on the following related questions connected to informatization: • Should hospitals in the whole Malopolska province can/should use unified software? • Are there formal possibilities and will of the hospitals to carry out informatization as regional task? • Is it possible –based on the collected experiences- to indicate optimal schedules/scenarios for
informatization and conditions in which it should be carried out? Enclosure Comparison of the data
Institution In
wha
t way
is th
e IT
serv
ice
sort
ed
in th
e ho
spita
l?
Wha
t is t
he
cove
rage
of
hosp
ital
info
rmat
ion
netw
ork?
Des
crip
tion
of
soft
war
e us
ed in
th
e ho
spita
l
Plan
ned
time
for
intr
oduc
ing
full
info
rmat
izat
ion
Fore
cast
ed c
osts
fo
r th
e fu
ll in
form
atiz
atio
n [zł]
PLN
1 2 3 4 5
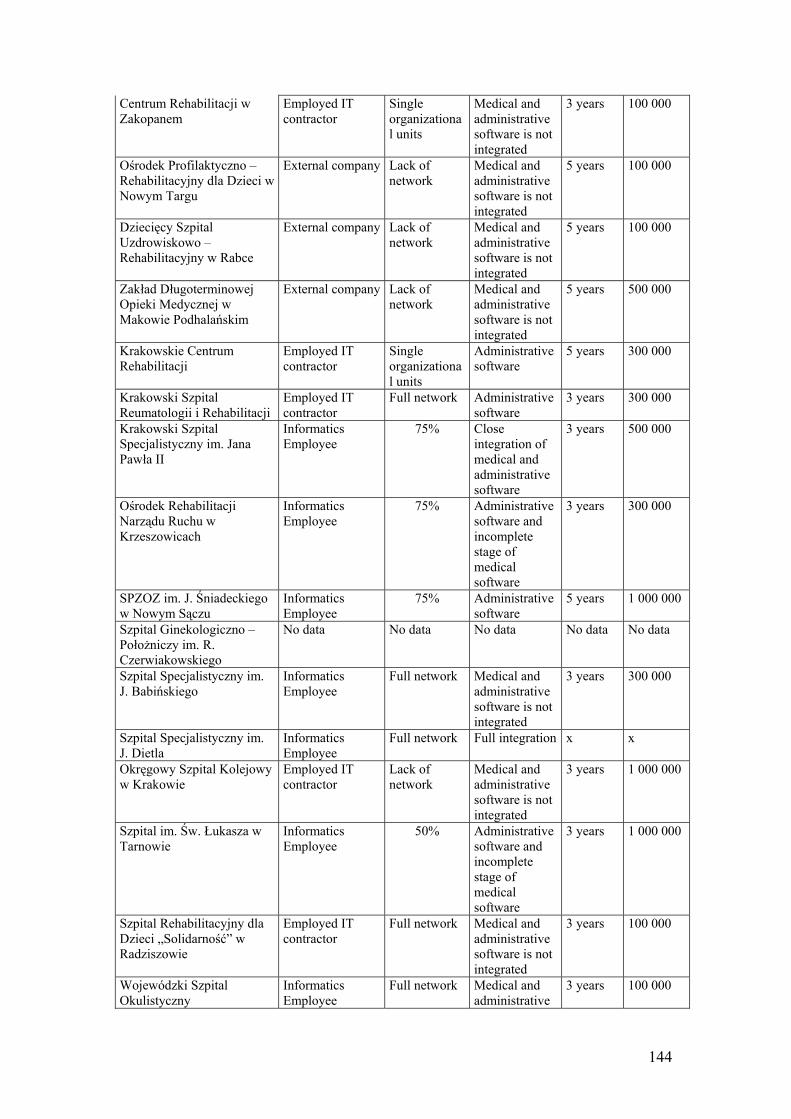
144
Centrum Rehabilitacji w Zakopanem
Employed IT contractor
Single organizational units
Medical and administrative software is not integrated
3 years 100 000
Ośrodek Profilaktyczno – Rehabilitacyjny dla Dzieci w Nowym Targu
External company Lack of network
Medical and administrative software is not integrated
5 years 100 000
Dziecięcy Szpital Uzdrowiskowo – Rehabilitacyjny w Rabce
External company Lack of network
Medical and administrative software is not integrated
5 years 100 000
Zakład Długoterminowej Opieki Medycznej w Makowie Podhalańskim
External company Lack of network
Medical and administrative software is not integrated
5 years 500 000
Krakowskie Centrum Rehabilitacji
Employed IT contractor
Single organizational units
Administrative software
5 years 300 000
Krakowski Szpital Reumatologii i Rehabilitacji
Employed IT contractor
Full network Administrative software
3 years 300 000
Krakowski Szpital Specjalistyczny im. Jana Pawła II
Informatics Employee
75% Close integration of medical and administrative software
3 years 500 000
Ośrodek Rehabilitacji Narządu Ruchu w Krzeszowicach
Informatics Employee
75% Administrative software and incomplete stage of medical software
3 years 300 000
SPZOZ im. J. Śniadeckiego w Nowym Sączu
Informatics Employee
75% Administrative software
5 years 1 000 000
Szpital Ginekologiczno – Położniczy im. R. Czerwiakowskiego
No data No data No data No data No data
Szpital Specjalistyczny im. J. Babińskiego
Informatics Employee
Full network Medical and administrative software is not integrated
3 years 300 000
Szpital Specjalistyczny im. J. Dietla
Informatics Employee
Full network Full integration x x
Okręgowy Szpital Kolejowy w Krakowie
Employed IT contractor
Lack of network
Medical and administrative software is not integrated
3 years 1 000 000
Szpital im. Św. Łukasza w Tarnowie
Informatics Employee
50% Administrative software and incomplete stage of medical software
3 years 1 000 000
Szpital Rehabilitacyjny dla Dzieci „Solidarność” w Radziszowie
Employed IT contractor
Full network Medical and administrative software is not integrated
3 years 100 000
Wojewódzki Szpital Okulistyczny
Informatics Employee
Full network Medical and administrative
3 years 100 000
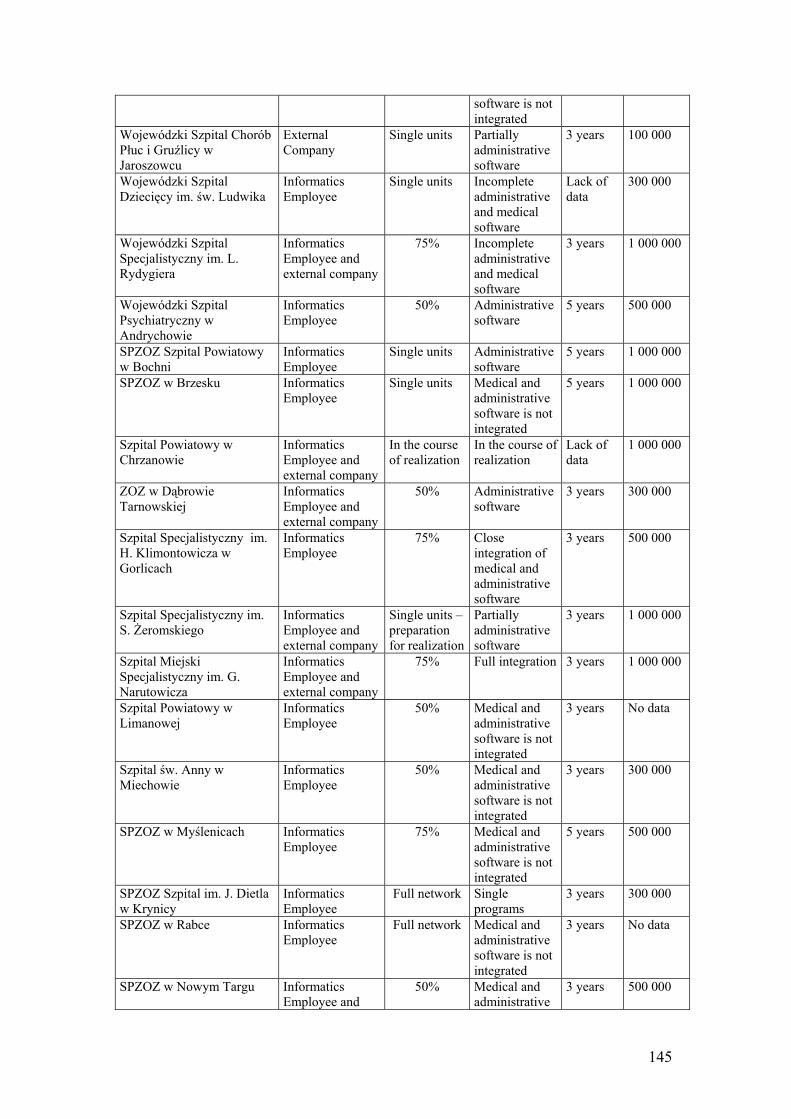
145
software is not integrated
Wojewódzki Szpital Chorób Płuc i Gruźlicy w Jaroszowcu
External Company
Single units Partially administrative software
3 years 100 000
Wojewódzki Szpital Dziecięcy im. św. Ludwika
Informatics Employee
Single units Incomplete administrative and medical software
Lack of data
300 000
Wojewódzki Szpital Specjalistyczny im. L. Rydygiera
Informatics Employee and external company
75% Incomplete administrative and medical software
3 years 1 000 000
Wojewódzki Szpital Psychiatryczny w Andrychowie
Informatics Employee
50% Administrative software
5 years 500 000
SPZOZ Szpital Powiatowy w Bochni
Informatics Employee
Single units Administrative software
5 years 1 000 000
SPZOZ w Brzesku Informatics Employee
Single units Medical and administrative software is not integrated
5 years 1 000 000
Szpital Powiatowy w Chrzanowie
Informatics Employee and external company
In the course of realization
In the course of realization
Lack of data
1 000 000
ZOZ w Dąbrowie Tarnowskiej
Informatics Employee and external company
50% Administrative software
3 years 300 000
Szpital Specjalistyczny im. H. Klimontowicza w Gorlicach
Informatics Employee
75% Close integration of medical and administrative software
3 years 500 000
Szpital Specjalistyczny im. S. Żeromskiego
Informatics Employee and external company
Single units – preparation for realization
Partially administrative software
3 years 1 000 000
Szpital Miejski Specjalistyczny im. G. Narutowicza
Informatics Employee and external company
75% Full integration 3 years 1 000 000
Szpital Powiatowy w Limanowej
Informatics Employee
50% Medical and administrative software is not integrated
3 years No data
Szpital św. Anny w Miechowie
Informatics Employee
50% Medical and administrative software is not integrated
3 years 300 000
SPZOZ w Myślenicach Informatics Employee
75% Medical and administrative software is not integrated
5 years 500 000
SPZOZ Szpital im. J. Dietla w Krynicy
Informatics Employee
Full network Single programs
3 years 300 000
SPZOZ w Rabce Informatics Employee
Full network Medical and administrative software is not integrated
3 years No data
SPZOZ w Nowym Targu Informatics Employee and
50% Medical and administrative
3 years 500 000
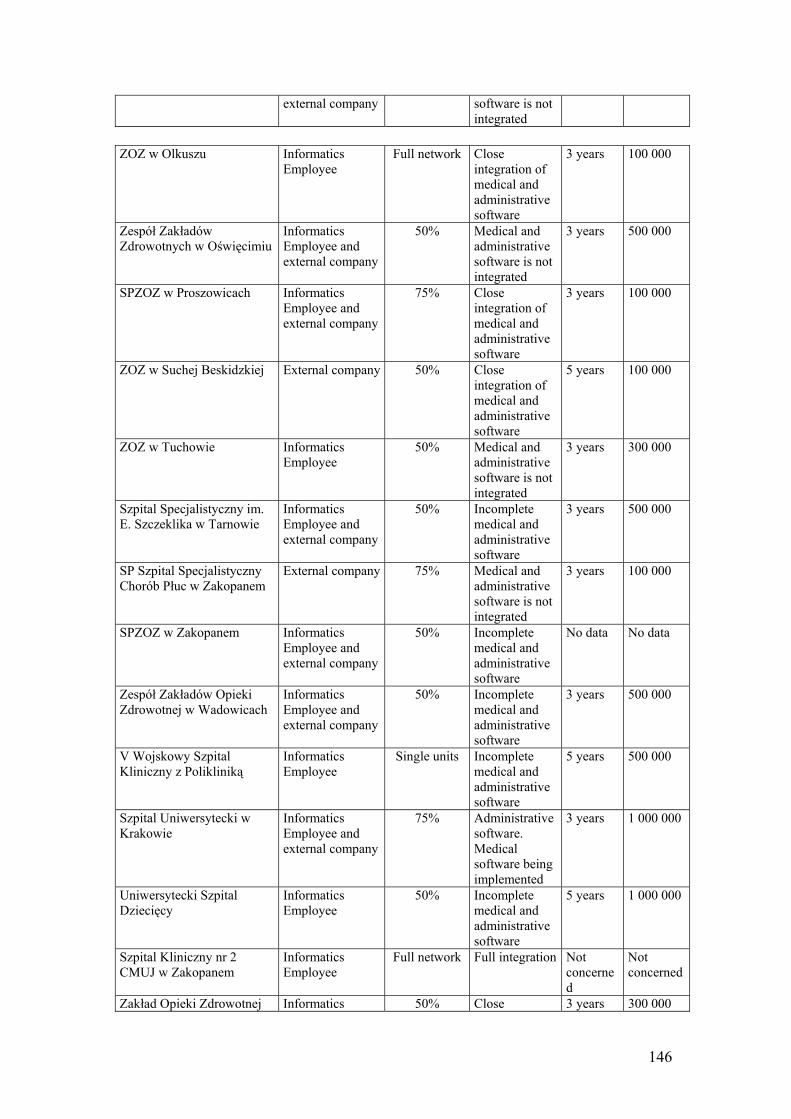
146
external company software is not integrated
ZOZ w Olkuszu Informatics
Employee Full network Close
integration of medical and administrative software
3 years 100 000
Zespół Zakładów Zdrowotnych w Oświęcimiu
Informatics Employee and external company
50% Medical and administrative software is not integrated
3 years 500 000
SPZOZ w Proszowicach Informatics Employee and external company
75% Close integration of medical and administrative software
3 years 100 000
ZOZ w Suchej Beskidzkiej External company 50% Close integration of medical and administrative software
5 years 100 000
ZOZ w Tuchowie Informatics Employee
50% Medical and administrative software is not integrated
3 years 300 000
Szpital Specjalistyczny im. E. Szczeklika w Tarnowie
Informatics Employee and external company
50% Incomplete medical and administrative software
3 years 500 000
SP Szpital Specjalistyczny Chorób Płuc w Zakopanem
External company 75% Medical and administrative software is not integrated
3 years 100 000
SPZOZ w Zakopanem Informatics Employee and external company
50% Incomplete medical and administrative software
No data No data
Zespół Zakładów Opieki Zdrowotnej w Wadowicach
Informatics Employee and external company
50% Incomplete medical and administrative software
3 years 500 000
V Wojskowy Szpital Kliniczny z Polikliniką
Informatics Employee
Single units Incomplete medical and administrative software
5 years 500 000
Szpital Uniwersytecki w Krakowie
Informatics Employee and external company
75% Administrative software. Medical software being implemented
3 years 1 000 000
Uniwersytecki Szpital Dziecięcy
Informatics Employee
50% Incomplete medical and administrative software
5 years 1 000 000
Szpital Kliniczny nr 2 CMUJ w Zakopanem
Informatics Employee
Full network Full integration Not concerned
Not concerned
Zakład Opieki Zdrowotnej Informatics 50% Close 3 years 300 000
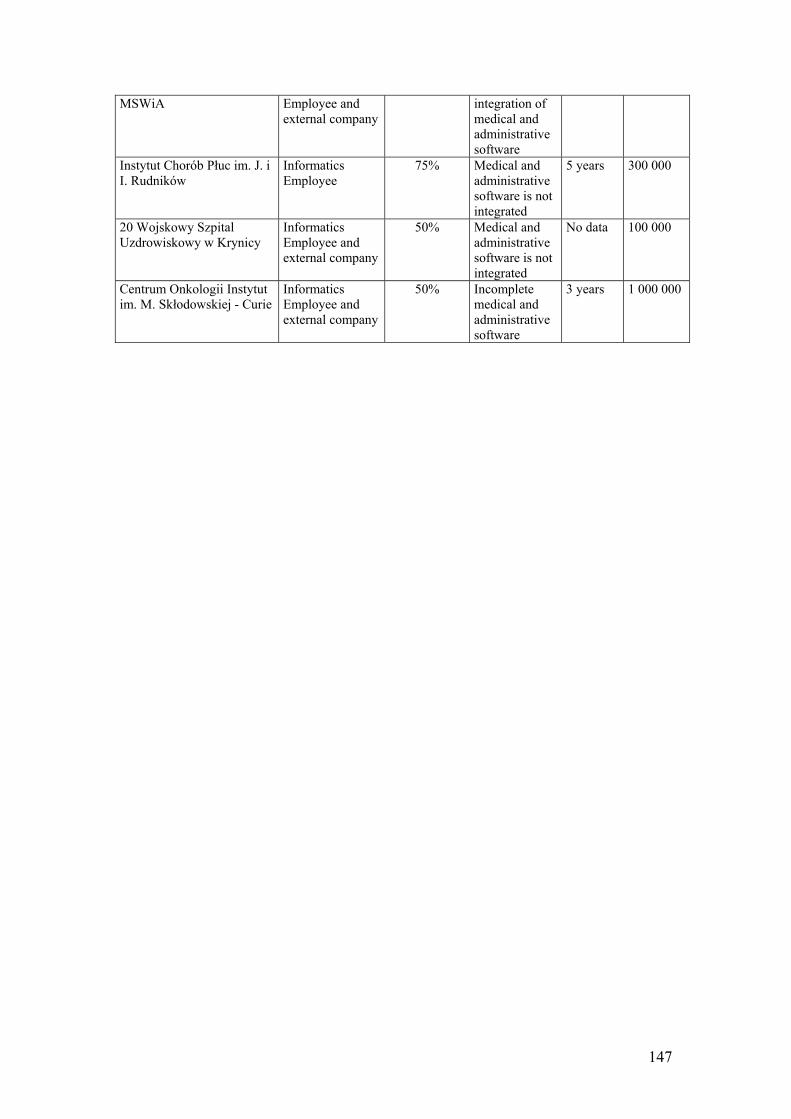
147
MSWiA Employee and external company
integration of medical and administrative software
Instytut Chorób Płuc im. J. i I. Rudników
Informatics Employee
75% Medical and administrative software is not integrated
5 years 300 000
20 Wojskowy Szpital Uzdrowiskowy w Krynicy
Informatics Employee and external company
50% Medical and administrative software is not integrated
No data 100 000
Centrum Onkologii Instytut im. M. Skłodowskiej - Curie
Informatics Employee and external company
50% Incomplete medical and administrative software
3 years 1 000 000
148
Annex XV Telemedicine at University of Krakow hospital, Poland The following article was written by Witold Poniklo from Academic Computer Centre CYFRONET of the University of Science and Technology in Cracow. I. University Hospital in Krakow (www.su.krakow.pl) The University Hospital (UH) in Krakow (Poland), has been interested in telemedicine for a long time. Since the Hospital should be considered as a referral medical center for Southeast part of Poland, telemedicine is as a natural way for providing medical consultations to local hospitals. To the date, 3 major telemedicine projects have been implemented:
1. TV transmission (analog signal) of surgeries. After a cycle of trials, at the Surgical Department UH a surgery consulted by specialist from Vienna has been performed. The Surgical Department of UH is equipped in a close circuit television system, which allows for such transmission as well as for internal monitoring of OR’s activities. This is mainly educational project, which is (technically) equal to a videoconference (via ISDN or IP). The UH owns all the equipment necessary to perform such transmissions.
2. Transmission of dynamic pictures of coronarography examinations.
Department of Cardiology at the UH cooperates with hospitals in Kielce (1 hospital) and Tarnów (2 hospitals) in the field of invasive cardiology. Coronarography examinations which are performed at the above mentioned hospitals could be consulted 24 hours a day by a specialist from UH. The system utilizes:
hardware (servers, routers, firewalls) own by UH. Each project participant has got
installed a dedicated set of hardware. telecommunication network. Connections to Kielce and Tarnów are done by: a
fiberoptic cable, radio-bridge connection, regular telecommunication cables, local Internet provider and (back-up) regular telephone lines (ISDN). Considering the transmission speed – critical in the case of dynamic pictures – the necessary network capacity must be at least 512kB/s, with recommended value equal to 1MB/s. Transmission costs are carried by local hospitals.
software. The network utilizes AcomWeb – software made by Siemens. AcomWeb utilizes DICOM3 radiological pictures transmission standard. A consultant from Krakow has access to the medical data gathered in the server at one of the local hospitals. These data are transmitted to Krakow, but not copied - staying at the place of their origin (generation). AcomWeb allows a consultant for all the data processing which could be done on the local operators console (zooming, geometrical measuring, viewing speed changes etc.). The software is owned by Siemens Medical Solutions Poland. Data (pictures) gathered during examination could be transmitted to the consultation network “on line” (hospital in Tarnow has installed an additional module to its angiography unit) or with an insignificant delay (data from the angiography unit are recorded on a CD, which is next manually moved to the system server – Kielce).
The project should be considered as an activity in the final stage of medical/technical trials. In fact, currently, there are monthly about 100 consultations (about 30 per local hospital). Based on the telemedicine system success, UH plans its further development. There are negotiations in this subject with hospitals in Rzeszow, Nowy Targ and Przemysl.

149
Additionally, The Cardiosurgical Hospital in Krakow – which has been trying implementation of its own telemedicine system – is negotiating implementation of UH telemedicine model. The telemedicine system operation requires also implementation of logistic solutions chain – the consultant must be informed (by SMS) that consultation data await him/her at the server. After consultation, certified e-mail message is send to the local hospital. All the logistic activities are a part of the telemedicine system network and all of them are stored at the server memory.
3. Emergency ECG data transmission.
Department of Cardiology UH has got installed a telemedicine system which allows for ECG curve consultation. 6 ambulances (which are dedicated for cardiological cases) in Krakow are equipped with defibrillator with diagnostic ECG (12 leads) module. An ambulance physician, could consult cardiac diagnosis with a specialist at UH. Defibrillator contains of a dedicated module (hardware) and software with are designed for ECG curve transmission by a GSM mobile phone (HSCSD). A single ECG curve is transmitted from an ambulance to UH in less than 1 minute. Transmission is activated by a single button. The data (message) are received at the Cardiology Department at UH and audio signal informs about it a consultant. The ECG curve is displayed on the consultant’s computer screen. Consultation is held by a mobile phone. Main purposes of the system are as follows:
to provide a diagnostic support a physician at an ambulance; to decide about the way of emergency treatment (selection of anticoagulants); to prepare the angiography room staff for an intervention before patient’s admission.
Currently, Krakow’s area is covered by the system. It is planned to extend it to the Krakow’s region (voivodship).
Additionally, UH IT staff has performed a pilot study of telemedicine system for CT and MRI pictures consultations (connections to: Sucha Beskidzka, Jaslo). This project is especially important for emergency neurological patients, who may have an examination at one of local hospital (transportation is avoided). Neurosurgical Department at UH is capable to consult all the necessary cases. UH IT staff works also on implementation of CT, MRI pictures transmission inside the UH (the Hospital is located in scattered buildings). II. Other telemedicine centers Despite vast interest of physicians in telemedicine, there is practically not successful implementations of such a system in Poland. It is worth to notice the following project/institutions: The Cardiosurgical Hospital in Krakow (Szpital Specjalistyczny im. Jana Pawla II w Krakowie) was trying to develop its own telemedicine system. As it is mentioned above, it is very likely that they will adapt UH telemedicine system (interventional cardiology, cardiosurgery). Krakow’s Telemedicine Center (Krakowskie Centrum Telemedyczne). This is a research institution. They were trying to implement their own software for medical images transmissions. Currently – due to my knowledge – they are focused on a telemedicine theory. Hospital in Przasnysz sends to Warsaw, to a commercial medical institution Centrum Medyczne ENEL-MED the following pictures: CT, MRI, ultrasound (http://www.mp.pl/kurier/show.php?aid=15236) for consultations.

150
Annex XVI
Telemedicine in Poland 1. Is there any formally written Action plan for eHealth in Poland? If yes, who are the people involved from the side of government? What are the areas/projects supported? What is the timeframe? How much financial resources are dedicated to eHealth in these plans? There is no formal Action Plan for e-Health available in Poland. The only document which addresses e-health area on national scale is ePoland. Its chapter Health online is devoted to the area of Internet applications in healthcare. However, its more like the list of expectations without realistic plan of development. Poland started radical changes in economy in the beginning of 1990s. Even though the changes in economy were quickly implemented, consecutive governments were afraid of changes in the healthcare system. The reforms in healthcare lagged off behind the main changes in economy in Poland. The first reform of health systems undertaken by post-solidarity government team resulted in establishment of Health Insurance Funds assigned territorially to main administrative units. . The system was not perfect but after first three years, the healthcare providers adjusted to the new requirements and situation in healthcare seemed to be stabilised. With new governmental team based on political coalition representing opposite political option, the concept of the National Health Fund was developed to substitute Health Insurance Funds. The new reform was introduced in the hurry and it became clear in the beginning of the 2004, that National Health Fund is not able to assure smooth access to healthcare services for Polish population. The prospects for the improvement of the status of Polish hospitals and other medical institutions remain also vague. Unsuccessful reform of healthcare system and general shortage of the resources for medical services add to poor financial situation of healthcare institutions in Poland. This in turn, translates into relatively insignificant interest in investments in telemedicine and related technologies. Furthermore, the main problem is still the poor access to sophisticated medical equipment. Healthcare providers seem do not see opportunities in the telemedicine and related applications as the salaries of medical professional remain low and the expenditures for the computer equipment and telecommunication fares prevail considerably above the expenses for workforce. Additional factors shaping unfavourable environment for e-heath development are: - low penetration of the Internet (the estimations from 2001-2002 say that only 10% of households have got the access to the Internet) - the political scene is changing radically with every new governmental team; so quickly that no coherent e-health action plan is expected - the essential problems with financing the traditional medical services results in relatively small interest in widespread use of new technologies. In summary, even if consecutive governmental teams declare high interests in Information Society development in Poland, only few actions are made to support it. The community of medical professionals are generally positive about the use of information technologies in practice. The same trends may be observed among the patients, but only few of them have got access to Internet. The position of the National Health Fund about e-Health has not been defined yet. Conclusions: 1. The action plan focused on e-Health is needed urgently in Poland to indicate priority areas for development. 2. The awareness of the opportunities related to e-health should be developed in National Health Fund environment and related organizations. 3. The pilot implementations should be spread in the cooperation with medical professional organizations and local authorities.
151
4. The best practices should be disseminated in target groups (politicians, local authorities, health professionals) on great scale. The education on e-health and medical informatics should be carried out systematically on various levels of education. 2. What are the most significant barriers to successful implementation of telemedicine in Poland? Barriers: - poor financial standing of the healthcare providers institutions, e.g. hospitals - unsuccessful reforms of healthcare system - high costs of IT infrastructure development in relation to the payment for medical personnel - lack of formal regulations of telecare and telemedicine services - undefined reimbursement issues for telemedical services – not official policy expressed so far neither by Health Insurance Funds previously nor National Health Fund currently 3. What are the telemedicine technologies used by hospitals/doctors today and what they are likely to adopt in next 3 years? Telecommunication infrastructure ISDN connections are available on nearly whole area of Poland. The service is offered mainly by Telekomunikacja Polska S.A., but also by other telecommunication providers aspiring for the market like Netia S.A. or Dialog S.A. The access to broadband fiberoptic connections is generally possible in main metropolitan areas due to the infrastructure developed by academic computer centre. Relatively good broadband connections is available in university hospital and some hospitals in greater cities. Peripheral hospitals, outside main voivodship centre must rely mainly on the ISDN connection, if they are going to develop telemedical communications. Most healthcare providers, both individual and institutional maintain some forms of access to Internet, generally through POTS with modem or fixed connections (ISDN, SDI, cable TV networks or radiolinks). The rates for band use are generally perceived as limiting for standard use, also in relation to telemedical interactions. Medical community and Internet Medical professionals, mainly physician, use the Internet access for browsing general content portals and portal targeting specifically this group of users. The communication between physician relies mainly on the traditional papers correspondence. The process of shaping the information infrastructure in healthcare providers in Poland was accompanied by the growing competition in the market of health-related portals. The dotcom rush that occurred in the USA and other markets influenced also considerably the trend for e-health initiatives in Poland. The pressure in the market resulted in the development of new Internet portals addressed to health professionals or to patients and citizens. Most of these initiatives relied on the provision of the content and business model based on attracting commercial partners interested in the advertisements targeted on the specific users. The competition between portals focused on health professionals as the main users appeared to be really intensive. Finally, after the dotcom bubble evaporated, only several Internet portal for physician survived in Poland. The main portal focused on health professionals include following websites: www.mediclub.pl, www.esculap.pl, www.mp.pl, www.clinika.pl , www.lekarze.com. Consumer e-health The access of general population to Internet is remains limited. The estimations indicate that only 10-15% of household have got the access to Internet. The number of users accessing Internet randomly (several times a month) is greater, but usually these are not regular episodes.
152
There is quite developed offer of Internet portals focused on delivery of health-related contents to general population. Their main revenue is based on the web-based advertisements. There are also some type of educational course offered. The portals addressed to patients are maintained by patients associations, non-profit organizations or industrial organizations, e.g. pharmaceutical companies interested in the promotion of specific products. One should remember that direct medication advertisement addressed to patients and all citizens is not allowed in Poland. So, pharmaceutical companies must avoid direct naming of the medications supplied by them to the market. Keeping the patients aware of available therapeutic options is one of possible solutions. Another of course, is developing advertising policies aimed on health professionals, mainly physician. Portal addressed to the patients could be classified into two groups: portals offering health-related contents, rarely services, aimed on health-related topics in general and websites focused on specific problems, e.g. addressed to patients with diabetes, arterial hypertension or sclerosis multiplex. Some of the websites offers additional benefits – some forms of teleconsultations or telemonitoring of patient’s health status. Websites focused on specific disorders deliver current information, educational contents, some type on-line advice and calculators for patients with one disease, e.g. arterial hypertension, diabetes (www.cukrzyca.pl, www.nadcisnienie.pl). Some medical centres and specialised Internet-based enterprises offer the on-line booking service of medical services (www.przychodnia.pl). The examples of general health-related portal addressed to all citizens encompass websites: - general health-related portal: www.mediweb.pl, zdrowie.medicentrum.pl, www.dbajozdrowie.pl - pharmaceutical-medical portal for patients www.pfm.pl - family health www.poradnikmedyczny.pl - information about healthcare providers according to location and speciality www.medycy.com.pl 4. What is the current status with EHR? Do you believe it’s likely to be adopted by health sector in next 3 years? The market of EHR software for individual healthcare providers and medical practices was developing according to client’s needs. There are many potential products offered by great IT companies and numerous SMEs. The electronic communication between software used in physicians’ officies and hospitals does not exist. The World Bank Project conducted from early 90ies by Polish Ministry of Health through its specialised Agency for Foreign Projects resulted in the purchases of Admission-Discharge-Transfer and Pharmacy modules to most of hospitals with at least 200 beds. The bid for the delivery of the information system was divided into 2 phases. In the first phase, every hospital participating in the Project was supposed to look into general proposals of solutions prepared by 6 consortia. The first phase resulted in choice of the 3 providers offering the best products from the view of the hospital. Then classic bid for proposal between 3 providers was conducted and the best proposal was chosen. The providers offering their products are enlisted below:. Consortium Software package AMIS, APEXIM MISS ALMA, ComArch Eskulap Computerland Zdrowie (SQLab, ComputerLand, PIK)
InfoMedica
Optimus OPTIMed RADCOMP Hipokrates The further development of information infrastructure, with specific aim of building comprehensive electronic healthcare record system was to be undertaken by every hospital. However, progress of this process is seriously hampered by the shortage of funds occurring in most Polish hospitals (see barriers discussed in point 2).
153
5. What is the expenditure for information technologies in Polish hospitals in general today? It is really difficult to estimate. The poor financial status of hospitals results on modest investment in information technologies. Most hospitals use information systems for running administrations and financial departments. The World Bank Project enabled the purchases of ADT and Pharmacy modules for hospitals with above 200 beds in Poland. Some hospitals follow the track and try develop other parts of the Hospital Information Systems, however the financial difficulties hamper the development of comprehensive Electronic Patient Record. 6. Would you please quickly mention the most important eHealth initiatives/pilots in Poland and the appropriate contact points or background documents/websites.
B. TELEZDROWIE. Telemedical diagnostic and rehabilitation systems. The project maintained by: Prof. Andrzej Czyżewski, Sound & Vision Engineering Department of the Technical University of Gdansk, Gdansk, Poland, http://sound.eti.pg.gda.pl/STAFF/acz.html Prof. Henryk Skarżyński, Insitute of Physiology and Pathology of Hearing, Warsaw, Poland http://www.ifps.org.pl Portal established in years 1999-2001 enabling access to diagnostic and rehabilitation tools for the area of impairments of human senses. The tools and solutions available on this website enable for quick on-line examination of the vision, hearing as well as screening for tinnitus and speech disorders. The tool “I can hear” is based on automatic questionnaire analysis, audiometric tone test procedure and testing speech intelligibility in noise. The tool “I can see” was prepared for the screening tests of vision. Two other tools enable also on-line screeining for tinnitus and speech problems. Portal is available under the address: www.telezdrowie.pl. Krakow Centre of Telemedicine (established as Centre of Excellence) Coordinator: Prof. Krzysztof Zieliński, Academic Computer Centre CYFRONET , UMM Science and Technology University, Krakow, Poland The Krakow Centre of Telemedicine was initially formed within the SCITECH II project. The Centre was established in the results of the agreement between several partners representing medical and technical university environments in Krakow. The main objectives of the centre include the development and implementation of the teleconsultation scenarios conducted with diversified information infrastructure, the application of wireless solution for access to medical databases and telemonitoring of the patients as well as building the medical digital video library supporting tele-education and training of health professionals in invasive procedures. Contact details: Prof. Krzysztof Zieliński, Institute of Computer Science, UMM Science and Technology University, Al.Mickiewicza 30, 30-059 Krakow, Poland off.ph.: +48 12 6173966, fax: +48 12 6339406, e-mail: [email protected] Mariusz Duplaga, MD, PhD, Department of Medicine, Jagiellonian University Medical College, Skawinska Str. 8, 31-066 Krakow, Poland off.ph.: +48 12 4305339, fax: +48 12 4305115, e-mail: [email protected], Project: Improvement of Care Delivery for Severe Asthma Patients Coordinator: Prof. Andrzej Szczeklik, Department of Medicine, Jagiellonian University Medical College, Krakow, Poland Project co-financed by Polish Ministry of Health and Polish Ministry of Scientific Research and Information Technology, carried out in years 2001-2003. It resulted in the establishment of the web-based system focused on the concept of sharing of asthma-related medical information of severe asthma patients among health professional as well as the support for patients empowerment and

154
telemonitoring. The system is available on the page www.astma.med.pl for registered users only including health professionals and patients. The initiative is based on the activities performed in 6 referential centres delivering care to population of asthma patients. Authorized health professionals taking care of their patients may access the electronic patient documentation online and browse the results of self-observations and self-measurements performed by patients on regular basis. Diversified access interfaces were offered to users, particularly patients involved in self-monitoring activities, like Internet browser, mobile phones with WAP protocol or SMS. The activities of the project were extended due to support from Ministry of Health for next years. Contact details: Mariusz Duplaga, Department of Medicine, Jagiellonian University Medical College, Skawinska Str. 8, 31-066 Krakow, Poland off.ph.: +48 12 4305339, fax: +48 12 4305115, e-mail: [email protected], National Register of Healthcare Providers. Centre for Information Systems in Healthcare, Ministry of Health, Warsaw, Poland http://www.csioz.gov.pl/ Centre for Information Systems in Healthcare prepared the register of healthcare providers including information about address, medical infrastructure, organisational structure, scope of specialities and health professionals employment in medical facilities. The register was designed as the tool improving the availability of healthcare information for administration supervision. It includes the solutions enhancing the monitoring of changes occurring in structure of healthcare organizations and institutions. Database of healthcare providers quicken also the process of proposal verification to National Health Fund during contracting healthcare services. Contact details: Centre for Information Systems in Healthcare Al. Jerozolimskie 155, 02-326 Warszawa, Poland ph.: . +48 22 8242727, fax: +48 22 824-27-37, e-mail: [email protected]
155
References • Central Statistical Office. Concise Statistical Yearbook of Poland. 2001
[http://www.stat.gov.pl] • Central Statistical Office. Demographic yearbook 2000. Warsaw 2000. • eEurope+. A co-operative effort to implement the Information Society in Europe. June 2001
[http://www.kbn.gov.pl/cele/ppt.html/01.ppt] • ePolska – Plan działań na rzecz rozwoju społeczeństwa informacyjnego w Polsce na lata
2001-2006. (Action plan for development of information society in Poland in years 2001-2006). [http://www.kbn.gov.pl/cele/ppt.html/02.ppt]
• European Communities and World Health Organization. Highlights on Health in Poland. Copenhagen, December 2001 [http://www.euro.who.int/countryinformation]
• European Survey of Information Society. Extension to Central and Eastern European Countries and Mediterranean Area. 2000 [http://www.ispo.cec.be/esis/]
• Filipiak J., Goliński J., Zacher L.W. Aims and directions of the information society development in Poland. State Committee for Scientific Research and Ministry of Posts and Telecommunication, November 28th, 2000 [http://www.kbn.gov.pl/en/cele_en.html]
• Government Population Council. Demographic Status of Poland. Sytuacja demograficzna Polski raport 1999-2000. Warsaw 2000
• IDG Poland.: ComputerWorld. The Annual Report 2002. June 2003 • Ministry of Health. National Health Programme 1996-2005. Intersectoral Task-Force for the
National Health Programme Coordination. Ministry of Health. Warsaw 2000 • Polish Ministry of Economy ePolska (ePoland) The Action Plan for the Information Society
Development in Poland for the years 2001-2006. • Rychlewski J., Węglarz J., Starzak S., Stroiński M., Nakonieczny M., Lesynga B., Noga M.,
Niezgódka M., Sąsiedzki P, Żenkiewicz J.: PIONIER: Polski Internet Optyczny – Zaawansowane Aplikacje, Usługi i Technologie dla Społeczeństwa Informacyjnego. (PIONIER: Polish Optical Internet – Advanced Applications, Services and Technologies for Information Society). September 2000 [http://www.kbn.gov.pl/analizy/ pionier/new/index.html]
• WHO Regional Office for Europe (European Observatory on Health Care Systems). Health care systems in transition. Poland. Copenhagen 1999.
WHO Regional Office For Europe. Health for all Database. January 2001 [http://www.euro.who.int./hfadb]
156
Annex XVII Research and Development Units, Poland Instytut Fizjologii i Patologii Słuchu ul. Pstrowskiego 1 01-943 Warszawa tel. (022) 835-66-70 fax (022) 835-52-14 [email protected] Internet page: www.ifps.org.pl Instytut Gruźlicy i Chorób Płuc ul. Płocka 26 01-138 Warszawa tel. (022) 691-21-28 fax (022) 691-24-53 [email protected] Internet page: www.igichp.edu.pl The person responsible for teleconsultations and telepathology is prof. dr hab. med. Janina Słodkowska, tel. 43 12 256 faks 43 12 452 e-mail: [email protected] Instytut Hematologii i Transfuzjologii ul. Chocimska 5 00-957 Warszawa tel. (022) 849-85-07 fax (022) 748-89-70 [email protected] Instytut Kardiologii im. Prymasa Tysiąclecia Stefana Kardynała Wyszyńskiego ul. Alpejska 42 04-628 Warszawa tel. (022) 815-25-24 fax (022)815-25-24 [email protected] Internet page: www.ikard.waw.pl Instytut Leków patrz: Narodowy Instytut Zdrowia Publicznego Instytut Matki i Dziecka ul. Kasprzaka 17a 01-211 Warszawa tel. (022) 632-68-58 fax (022) 632-68-58 [email protected] Internet page: www.imid.med.pl Instytut Medycyny Morskiej i Tropikalnej ul. Powstania Styczniowego 9b 81-519 Gdynia tel. (058) 622-33-54 fax (058) 622-33-54
157
[email protected] Internet page: www.immt.gdynia.pl Instytut Medycyny Wsi im. Witolda Chodźki ul. Jaczewskiego 2 20-950 Lublin tel. (081) 747-80-27 fax (081) 747-86-46 [email protected] Internet page: www.imw.lublin.pl Instytut Medycyny Pracy im. prof. dr Jerzego Nofera ul. Św. Teresy 8 90-950 Łódź tel. (042) 631-45-02 fax (042) 656-83-31 [email protected] Internet page: www.imp.lodz.pl Instytut Medycyny Pracy i Zdrowia Środowiskowego ul. Kościelna 13 41-200 Sosnowiec tel. (032) 266-06-40 fax (032) 266-11-24 [email protected] Internet page: www.imp.sosnowiec.pl Centrum Onkologii - Instytut im. Marii Skłodowskiej-Curie ul. W.K.Roentgena 5 02-781 Warszawa tel. (022) 644-02-00 fax (022) 644-02-08 [email protected] Internet page: www.coi.waw.pl Instytut Psychiatrii i Neurologii ul. Sobieskiego 1/9 02-957 Warszawa tel. (022) 842-68-02 fax (022) 642-53-75 [email protected] Internet page: www.ipin.edu.pl Instytut Reumatologiczny ul. Spartańska 1 02-637 Warszawa tel. (022) 844-95-22 fax (022) 844-95-22 [email protected] Instytut Żywności i Żywienia im. prof. dr med. Aleksandra Szczygła ul.Powsińska 61/63 02-903 Warszawa tel. (022) 842-21-71 fax (022) 842-11-03 [email protected] strona główna: www.izz.waw.pl Państwowy Zakład Higieny IN-B
158
ul. Chocimska 24 00-791 Warszawa tel. (022) 849-76-12 fax (022) 849-74-84 [email protected] Internet page: www.izz.waw.pl Pomnik-Centrum Zdrowia Dziecka Al. Dzieci Polskich 20 04-736 Warszawa tel. (022) 815-40-40 fax (022) 815-40-15 [email protected] Internet page: www.czd.waw.pl Centrum Zdrowia Matki Polki ul. Rzgowska 281/289 93-338 Łódź tel. (042) 645-11-14 fax (042)646-66-53 [email protected] Internet page: www.iczmp.edu.pl Centralny Ośrodek Techniki Medycznej ul. Boduena 4 00-950 Warszawa tel. (022) 827-82-51 fax (022) 827-87-91 [email protected] Internet page: www.cotm.pl Centralne Laboratorium Surowic i Szczepionek patrz: Narodowy Instytut Zdrowia Publicznego Narodowy Instytut Zdrowia Publicznego powstał 1 października 2002 r. z połączenia: Instytutu Leków oraz Centralnego Laboratorium Surowic i Szczepionek ul. Chełmska 30/34 00-725 Warszawa tel. (022) 851-43-69; (022) 841-29-40 fax (022) 841-06-52 [email protected] Internet page: www.nizp.edu.pl
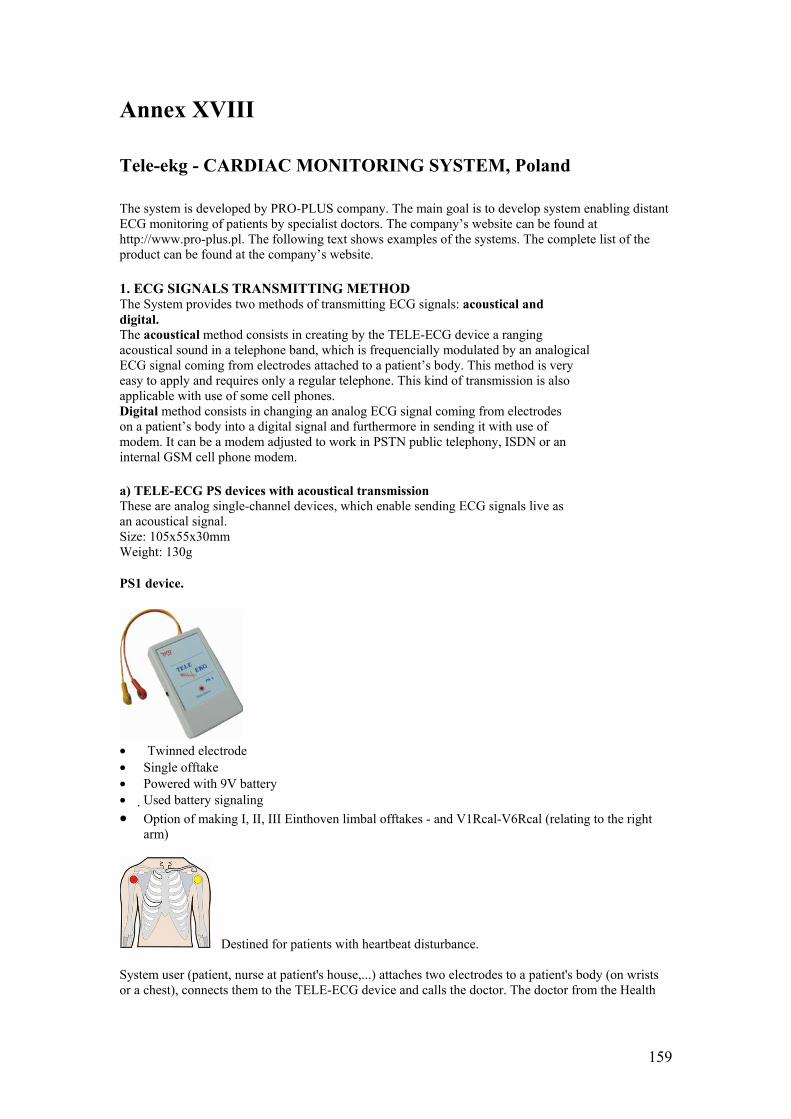
159
Annex XVIII
Tele-ekg - CARDIAC MONITORING SYSTEM, Poland The system is developed by PRO-PLUS company. The main goal is to develop system enabling distant ECG monitoring of patients by specialist doctors. The company’s website can be found at http://www.pro-plus.pl. The following text shows examples of the systems. The complete list of the product can be found at the company’s website. 1. ECG SIGNALS TRANSMITTING METHOD The System provides two methods of transmitting ECG signals: acoustical and digital. The acoustical method consists in creating by the TELE-ECG device a ranging acoustical sound in a telephone band, which is frequencially modulated by an analogical ECG signal coming from electrodes attached to a patient’s body. This method is very easy to apply and requires only a regular telephone. This kind of transmission is also applicable with use of some cell phones. Digital method consists in changing an analog ECG signal coming from electrodes on a patient’s body into a digital signal and furthermore in sending it with use of modem. It can be a modem adjusted to work in PSTN public telephony, ISDN or an internal GSM cell phone modem. a) TELE-ECG PS devices with acoustical transmission These are analog single-channel devices, which enable sending ECG signals live as an acoustical signal. Size: 105x55x30mm Weight: 130g PS1 device.
• Twinned electrode • Single offtake • Powered with 9V battery • Used battery signaling • Option of making I, II, III Einthoven limbal offtakes - and V1Rcal-V6Rcal (relating to the right
arm)
Destined for patients with heartbeat disturbance. System user (patient, nurse at patient's house,...) attaches two electrodes to a patient's body (on wrists or a chest), connects them to the TELE-ECG device and calls the doctor. The doctor from the Health
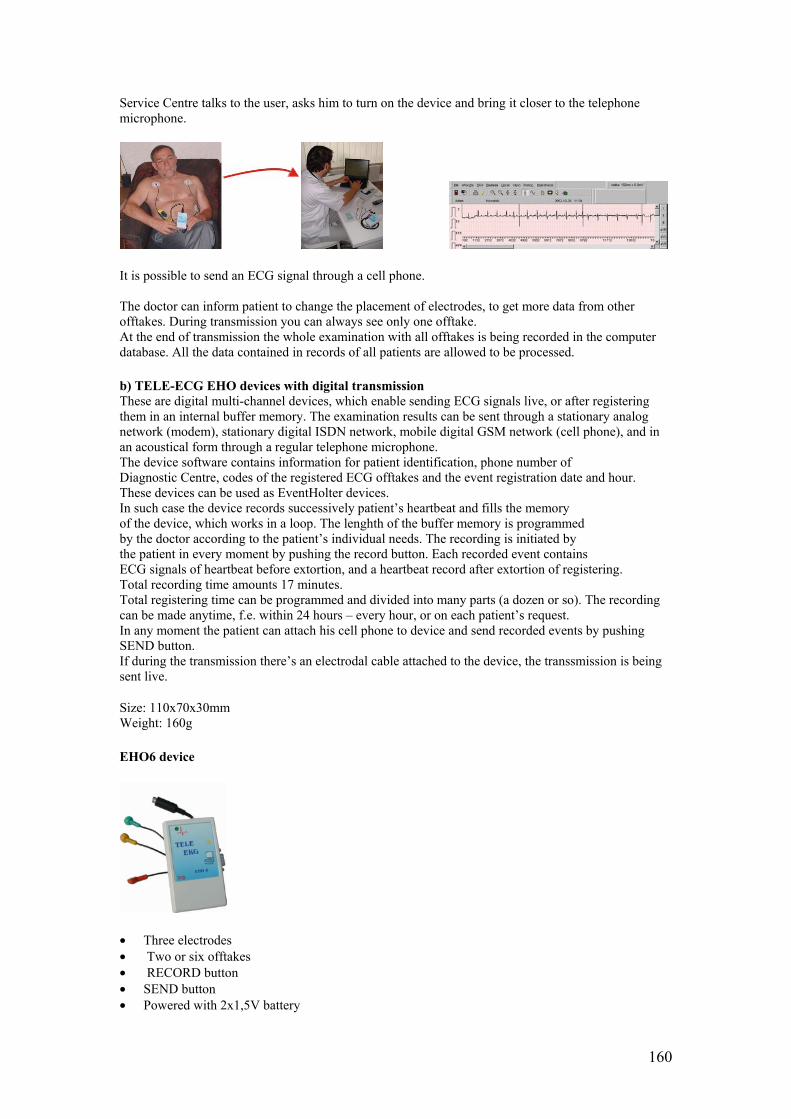
160
Service Centre talks to the user, asks him to turn on the device and bring it closer to the telephone microphone.
It is possible to send an ECG signal through a cell phone. The doctor can inform patient to change the placement of electrodes, to get more data from other offtakes. During transmission you can always see only one offtake. At the end of transmission the whole examination with all offtakes is being recorded in the computer database. All the data contained in records of all patients are allowed to be processed. b) TELE-ECG EHO devices with digital transmission These are digital multi-channel devices, which enable sending ECG signals live, or after registering them in an internal buffer memory. The examination results can be sent through a stationary analog network (modem), stationary digital ISDN network, mobile digital GSM network (cell phone), and in an acoustical form through a regular telephone microphone. The device software contains information for patient identification, phone number of Diagnostic Centre, codes of the registered ECG offtakes and the event registration date and hour. These devices can be used as EventHolter devices. In such case the device records successively patient’s heartbeat and fills the memory of the device, which works in a loop. The lenghth of the buffer memory is programmed by the doctor according to the patient’s individual needs. The recording is initiated by the patient in every moment by pushing the record button. Each recorded event contains ECG signals of heartbeat before extortion, and a heartbeat record after extortion of registering. Total recording time amounts 17 minutes. Total registering time can be programmed and divided into many parts (a dozen or so). The recording can be made anytime, f.e. within 24 hours – every hour, or on each patient’s request. In any moment the patient can attach his cell phone to device and send recorded events by pushing SEND button. If during the transmission there’s an electrodal cable attached to the device, the transsmission is being sent live. Size: 110x70x30mm Weight: 160g EHO6 device
• Three electrodes • Two or six offtakes • RECORD button • SEND button • Powered with 2x1,5V battery
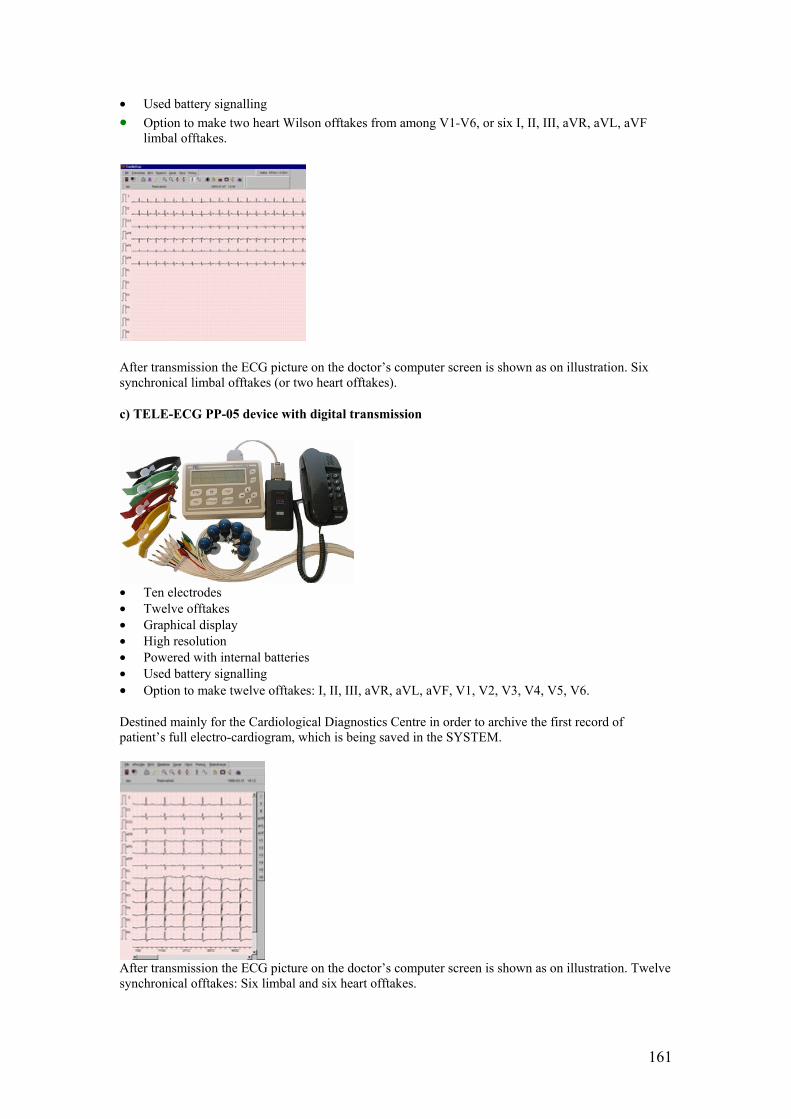
161
• Used battery signalling • Option to make two heart Wilson offtakes from among V1-V6, or six I, II, III, aVR, aVL, aVF
limbal offtakes.
After transmission the ECG picture on the doctor’s computer screen is shown as on illustration. Six synchronical limbal offtakes (or two heart offtakes). c) TELE-ECG PP-05 device with digital transmission
• Ten electrodes • Twelve offtakes • Graphical display • High resolution • Powered with internal batteries • Used battery signalling • Option to make twelve offtakes: I, II, III, aVR, aVL, aVF, V1, V2, V3, V4, V5, V6. Destined mainly for the Cardiological Diagnostics Centre in order to archive the first record of patient’s full electro-cardiogram, which is being saved in the SYSTEM.
After transmission the ECG picture on the doctor’s computer screen is shown as on illustration. Twelve synchronical offtakes: Six limbal and six heart offtakes.
162
2. CardioScp® SOFTWARE a) Software for Medical center The software installation can be performed by any PC user. Computer requirements: PC with WINDOWS’9x operation system Clock speed - minimum 160MHz HDD-20GB; FDD-1,44 RAM-64MB Internal modem PS mouse Two free RS232 COM ports Monitor 17“ Ink printer On the Installation Disc there’s a Manual and video presentation of the basic system working in a Medical Clinic, where the TELE-ECG system users are the patients of this and other clinics, which finish work at certain hours. CardioScp® software enables: • Receiving ECG examinations transmitted acoustically and digitally with an option of direct
telephone contact between SYSTEM user and doctor. • Automatical method of receiving ECG examination records – no service required. • ECG records archiving in database. • Keeping the patient’s records containing illness history and treatment methods. • Comparing the received ECG pictures with records in database. • Printing electro-cardiograms with use of any printer and paper. • In network version - cooperation between many receiving stations. CardioScp® software installed f.e. on the personal doctor ‘s computer (Local Diagnostic Centre) enables almost immediately initiation of cardiological monitoring with use of TELE-ECG PS devices with acoustic transmission. As the number of patients and assortment demand grows, f.e. for EHO (event-holter) devices, no computer modifications are necessary. In case when the number of patients embraced with service will grow considerably (over 2-3 thousands), it is advisable to connect the second computer (receiving station) or to connect to a Local Centre’s database via Internet. In last case the online connection is necessary. In the Local Centre, beside the server database software, there’s the same CardioScp® software at use. b) CardioScp_e-mail® software for patients using Internet For the Internet users (patients, working places, schools, etc.) there’s a CardioScp_e-mail® software created. It allows receiving transmission directly with use of transmitting cable from any TELE-ECG PS or EHO device to the user’s computer and next sending the record via e-mail to the Centre. After the Centre estimation – the description is sent back via e-mail to the user. The gathered ECG records in the user’s computer can be printed as in the Diagnostic Centre. c) Software main utilizing features CardioCsp® software offers many functions, which make diagnosis much easier for the doctor. They are (among the other things): an option magnify on the ECG fragments, scaling characteristic fragments, filtering network disturbances, printing in various formats etc.
163
Annex XIX
Telemedicine in Slovenia – MESS report Questions: 1. Is there any formaly written Action plan for eHealth in Slovenia? If yes, who are the people involved from the side of government? What are the areas/projects supported? What is the timeframe? How much financial resources are dedicated to eHealth in these plans? 6. Would you please quickly mention the most important eHealth initiatives/pilots in Slovenia and the appropriate contact points or background documents/websites.. MESS Ministry of Education, Science and Sport Trg OF 13, SI-1000 Ljubljana, Slovenia Phone: +386 1 478 46 00, fax: +386 1 478 47 19 The Ministry of Education, Science and Sport in Slovenia is responsible for the preparation of legislation, policy, funding of science activities on the basis of calls published in Slovenian Official Gazette and monitoring of the implementation of research activities. The calls for instruments, 5-years research programmes, Basic and Applied research projects, Targeted research programmes, Young researchers programme, Research infrastructure, International co-operation, are published in Slovenian Official Gazette where the details and forms for proposals are explained. Together with Slovenian participants could apply also partners from abroad but for the implementation of projects they should used their own budget. Foreign experts are also invited in the evaluation procedure of proposals. The Republic of Slovenia allocates 1,51 % of GDP for science and technology. In Year 2002 the budget of MESS amount was 129 Mio. EUR. In Slovenia no special programme for eHealth exists at the moment but the research programmes and projects are spread between two scientific fields: Engineering Sciences and Medical Sciences. The other fields are Natural Sciences, Biotechnical/Agricultural Sciences, Social Sciences and Humanities. •5-years research programmes: 3 (some of their activities) of 334 programmes in the field Engineering (2) and Medical Sciences (1). Head of the research group Research Institution Title
Budget in 2002 (EUR)
The field of Science
Dr. Nada Lavrač
Jozef Stefan Institute
Intelligent data analysis, computer logic and linguistics 154.753
Engineering Sciences
Dr. Janez Stare
University of Ljubljana, Faculty of Medicine
Biometrical, scientometrical and scientific computer data treatment and information in medicine 97.494
Medical Sciences
Dr. Ivan Bratko
University of Ljubljana, Faculty of Computer and Artificial intelligence 60.232
Engineering Sciences
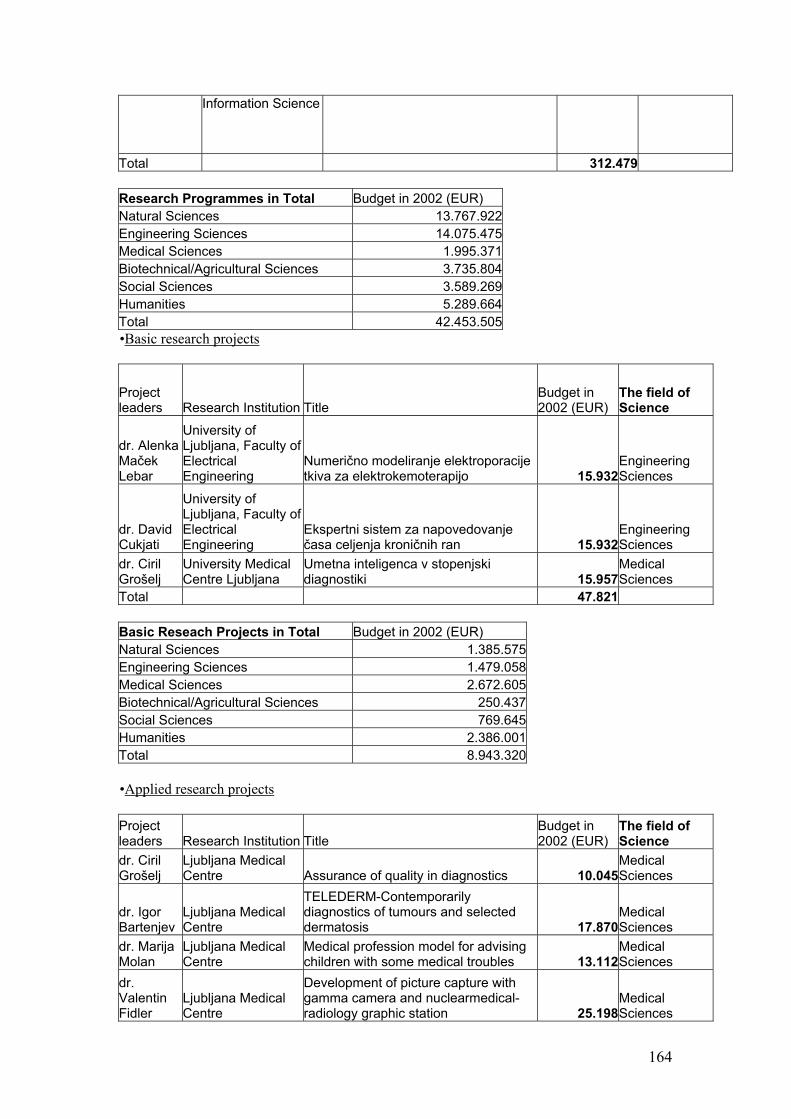
164
Information Science
Total 312.479 Research Programmes in Total Budget in 2002 (EUR) Natural Sciences 13.767.922Engineering Sciences 14.075.475Medical Sciences 1.995.371Biotechnical/Agricultural Sciences 3.735.804Social Sciences 3.589.269Humanities 5.289.664Total 42.453.505•Basic research projects
Project leaders Research Institution Title
Budget in 2002 (EUR)
The field of Science
dr. Alenka Maček Lebar
University of Ljubljana, Faculty of Electrical Engineering
Numerično modeliranje elektroporacije tkiva za elektrokemoterapijo 15.932
Engineering Sciences
dr. David Cukjati
University of Ljubljana, Faculty of Electrical Engineering
Ekspertni sistem za napovedovanje časa celjenja kroničnih ran 15.932
Engineering Sciences
dr. Ciril Grošelj
University Medical Centre Ljubljana
Umetna inteligenca v stopenjski diagnostiki 15.957
Medical Sciences
Total 47.821 Basic Reseach Projects in Total Budget in 2002 (EUR) Natural Sciences 1.385.575Engineering Sciences 1.479.058Medical Sciences 2.672.605Biotechnical/Agricultural Sciences 250.437Social Sciences 769.645Humanities 2.386.001Total 8.943.320 •Applied research projects Project leaders Research Institution Title
Budget in 2002 (EUR)
The field of Science
dr. Ciril Grošelj
Ljubljana Medical Centre Assurance of quality in diagnostics 10.045
Medical Sciences
dr. Igor Bartenjev
Ljubljana Medical Centre
TELEDERM-Contemporarily diagnostics of tumours and selected dermatosis 17.870
Medical Sciences
dr. Marija Molan
Ljubljana Medical Centre
Medical profession model for advising children with some medical troubles 13.112
Medical Sciences
dr. Valentin Fidler
Ljubljana Medical Centre
Development of picture capture with gamma camera and nuclearmedical-radiology graphic station 25.198
Medical Sciences
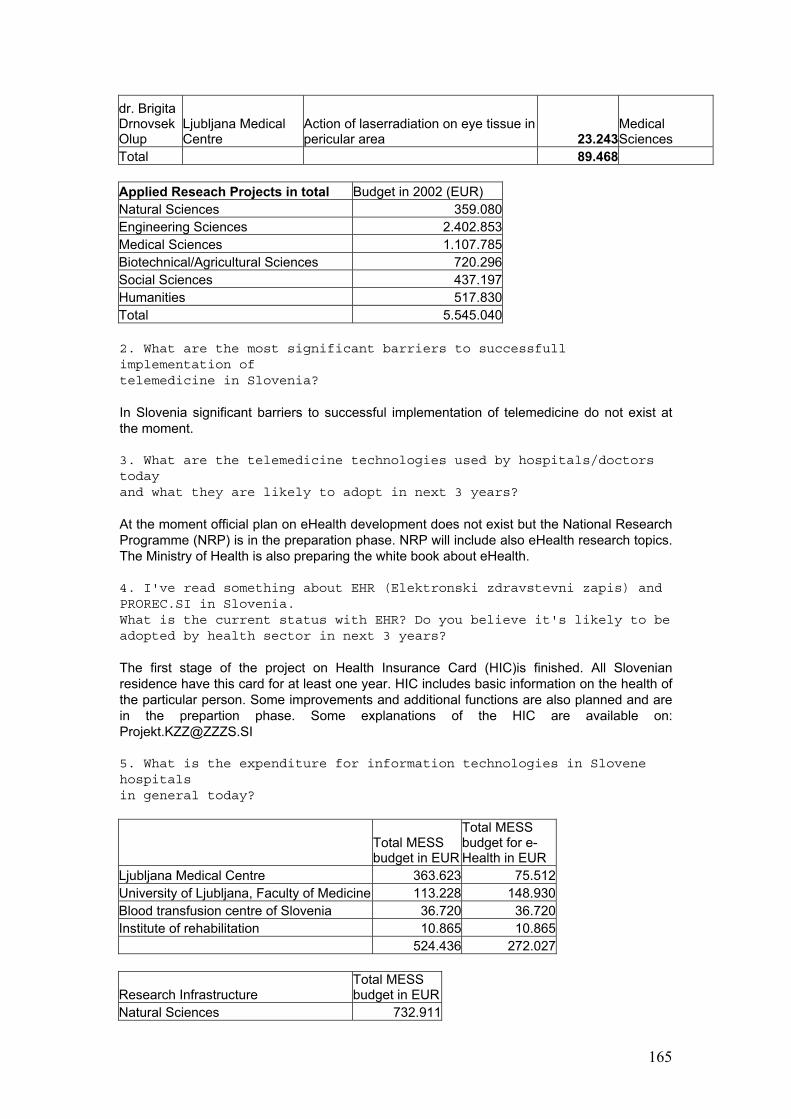
165
dr. Brigita Drnovsek Olup
Ljubljana Medical Centre
Action of laserradiation on eye tissue in pericular area 23.243
Medical Sciences
Total 89.468 Applied Reseach Projects in total Budget in 2002 (EUR) Natural Sciences 359.080Engineering Sciences 2.402.853Medical Sciences 1.107.785Biotechnical/Agricultural Sciences 720.296Social Sciences 437.197Humanities 517.830Total 5.545.040 2. What are the most significant barriers to successfull implementation of telemedicine in Slovenia? In Slovenia significant barriers to successful implementation of telemedicine do not exist at the moment. 3. What are the telemedicine technologies used by hospitals/doctors today and what they are likely to adopt in next 3 years? At the moment official plan on eHealth development does not exist but the National Research Programme (NRP) is in the preparation phase. NRP will include also eHealth research topics. The Ministry of Health is also preparing the white book about eHealth. 4. I've read something about EHR (Elektronski zdravstevni zapis) and PROREC.SI in Slovenia. What is the current status with EHR? Do you believe it's likely to be adopted by health sector in next 3 years? The first stage of the project on Health Insurance Card (HIC)is finished. All Slovenian residence have this card for at least one year. HIC includes basic information on the health of the particular person. Some improvements and additional functions are also planned and are in the prepartion phase. Some explanations of the HIC are available on: [email protected] 5. What is the expenditure for information technologies in Slovene hospitals in general today?
Total MESS budget in EUR
Total MESS budget for e-Health in EUR
Ljubljana Medical Centre 363.623 75.512University of Ljubljana, Faculty of Medicine 113.228 148.930Blood transfusion centre of Slovenia 36.720 36.720Institute of rehabilitation 10.865 10.865 524.436 272.027
Research Infrastructure Total MESS budget in EUR
Natural Sciences 732.911
166
Engineering Sciences 232.569Medical Sciences 524.436Biotechnical/Agricultural Sciences 371.682Social Sciences 176.227Humanities 83.131Total 2.120.955 The total budget of Slovenian hospitals on information technologies is not available only the MESS budget on information technologies needed for the implementation of the research work.
167
Annex XX
Telemedicine in Slovenia Introduction Historical review and major milestones in the progress of IST development and implementation in Slovenia from 1993-2003 A major step in the development of Medical Informatics in Slovenia was made at the beginning of 1993, when the Institute of Health Insurance of the Republic of Slovenia bought 2750 IBM personal computers and distributed them to public health institutions, as well as to the first private ones. In addition to hardware, health care institutions received a computer program for accounting and invoicing the health care services (reimbursement), free of charge. During the following months, over 5000 users were trained to work with computers, mainly administrative staff and nurses. Among the projects that followed, the following are worth to mention:
• Health Insurance Registry
• National Health Insurance Card (http://www.zzzs.si/kzz/ang/hic_indx.htm)
• Electronic Data Interchange (EDI) Project
• The Elements of Uniformity in Hospital and Outpatient Health Care Statistics at the national level
• Institute for Health Protection Project
• HANSA EAST - EU-HANSA
• TELENURSE
• PRIMACOM
• RETRANSPLANT
• PROPRACTITION
• WIDENET
• Health Sector Management Project (HSMP)
List of selected research projects (national and EU) with a brief indication of the overall goals.
Name of the PI, Title, ID No: Dates of Project (Entire Period of Support)
Smiljana V. Slavec, WIDENET, Promotion of the adoption and extended use of standardized Electronic Health Care Records and the required infrastructure, IST-1999-14203
12/2000 – 12/2003
Bostjan Bercic, “RETRANSPLANT” (Regional and International Integrated Telemedicine Network for Medical Assistance in End Stage Diseases and Organ Transplant), 5FP HC4028 – IN4028
10/1998 – 03/2001
168
Bostjan Bercic PROPRACTITION, Co-operative medical education toolkit Leonardo da Vinci programme, Contract # HU/99/1/083138/PI/III.3.a/CONT, Id No: 83138
07/1999 – 07/2001
Bostjan Bercic, “HANSA East” - Healthcare Advanced Networked Systems Architecture for the Countries of Central and Eastern Europe and New Independent States (CEN TC 251 ENV 12967-1 “Healthcare Information Systems Architecture - HISA Standard), HC1019, INCO COPERNICUS Project No. 96-0096
04/1997 – 10/1999
Bostjan Bercic, “PRIMACOM”- PRIMAry Care physician’s COMunication Network, (Regional Health Care Network for exchange of routine messages between healthcare professionals), 4FP CoCo-INCO COPERNICUS, HC1008, PL961090
04/1997 – 10/1999
Smiljana V. Slavec, Health Insurance (Chip) Card Project, Introduction and deployment of Health Insurance (Chip) Card in Slovenia. National project
10/1995 – 06/2000
Smiljana V. Slavec “TELENURSE”- Information System For Treating The Patient At His Home International (EU) Project
1997 - 1999
Smiljana V. Slavec “EXPERT SYSTEM for THERAPEUTIC ACTIVITIES IN HEALTH CARE” National project
1997 - 1999
Smiljana V. Slavec, “Electronic Data Interchange (EDI) Project”, Introduction and implementation of Electronic Data Interchange (EDI) between healthcare providers and IHIS in Slovenia. Messages: INVOIC, MEDREP, MEDREQ, MEDDIS. National project
12/1995 – 12/1999
Smiljana V. Slavec, Perinatal Information System, (Modernization of in-patient statistics), National project
1997 - 2003
Review of the National and EU RTD activities and implementations
Assignment Name: Health Insurance Registry
Start Date (Month/Year): 10/1993
Completion Date (Month/Year): 7/1996
Narrative Description of Project: The National Health Insurance System was re-established in Slovenia in 1992. The previous System based on Independent Regional Health financing Organizations. With re-establishment of National Health Insurance the newly established Health Insurance Institute of Slovenia was faced with decentralized Insured Persons Registries and applications on various platforms. In order to reorganize and integrate databases well defined business model was provided by the Health Insurance Institute Management. Main project goals were: Health Insurance Institute of Slovenia Information and data model development, Centralize ten regional databases/applications into integrated Health Insurance Information System, Develop a secure, stable and state-of-the-art Client/Server application, Central Database Server and
Private Wide Area Network Establishment, Develop and Maintain Internal Information Standards
169
Assignment Name: National Health Insurance Card
Start Date (Month/Year): 9/1995
Completion Date (Month/Year): 10/2000
Narrative Description of Project: The Project was started in order to achieve: to improve the quality of services and treatment of insured person, within HIIS and by health care service providers; to simplify and improve communications between HIIS, the physicians and health care institutions; to reduce the volume of (unnecessary) procedures involved in implementing the insured person's rights; to improve security of personal data within information systems; to reduce administrative chores and thereby, to increase efficiency of operation of HIIS and of the health care service; with reasonable financial investment, to secure long-term economic benefits at the national economy level. The health insurance card is the only document applicable in the implementation of the compulsory and voluntary health insurance rights in Slovenia. This electronic document on a smart card was issued to all persons dully covered by the compulsory health insurance in Slovenia, i.e. to the entire population of close to 2 million. A person is to present the card when visiting at the doctor's and at all other occasions of implementing the rights deriving from health insurance. The health insurance validity is updated by the card holder, through 275 self-service terminals nationwide. The updating of insurance validity also updates card data from the central databases. The card is a means of easy and direct transfer of data between the insured persons, Health Insurance Institute of Slovenia and the health care organizations. Data electronically recorded in the card are accessible for reading only to authorized health professional card holders. Procedures associated with the card are fast and ensure high service quality and data security. The card system is aligned with the Slovenian health care and health insurance sector conditions and regulations and it duly observes international recommendations and standards. A detailed project description can be found at http://www.zzzs.si/kzz/ang/hic_indx.htm
Assignment Name: Electronic Data Interchange (EDI) Project
Start Date (Month/Year): 12/93
Completion Date (Month/Year): 12/99
Narrative Description of Project: Introduction and implementation of Electronic Data Interchange (EDI) between healthcare providers and Health Insurance Institute of Slovenia in Slovenia. Messages: INVOIC, MEDREP, MEDREQ, MEDDIS. On Infonet’s initiative and together with Health Insurance Institute of Slovenia we started a joint project in 1993, in which we involved ourselves already in the very phase of requirements’ definition. Additionally, we initiated a pilot project with the Railway Health Center Ljubljana. Successfully executed pilot projects accelerated the introduction of Electronic Data Interchange (EDI) among our business partners (e.g. healthcare providers) and Health Insurance Institute of Slovenia. Presently, EDI for reimbursement purposes is being 100% used in all public healthcare institutions, as well as in two thirds of private ones.
170
Assignment Name: The Elements of Uniformity in Hospital and Outpatient Health Care Statistics at the national level
Start Date (Month/Year): 10/99
Completion Date (Month/Year): 07/2001
Narrative Description of Project: The preparation of the uniform definitions for the basic conceptions that are used in the accounting/reimbursement system for obligatory and for additional voluntary health insurance, as well as in healthcare statistics.
Assignment Name: Institute for Health Protection Project
Start Date (Month/Year): 10/95
Completion Date (Month/Year): 06/00
Narrative Description of Project: - Health statistics - Data Collection, Aggregation and Analysis of Sick-leave - Perinatal Information System Health statistics We co-operated in work groups for optimum network performance, data collection, processing and transfer in inpatient and outpatient statistics. Data Collection, Aggregation and Analysis of Sick-leave We have developed the software used by regional and republic Institute for Health Protection for collection, aggregation and analysis of data of sick-leave. Perinatal Information System On the basis of requirements, connected with modernization of in-patient statistics, we developed the software application PerIS, which is used in Slovenian hospitals as information support to Perinatal information system. The software is developed on Windows platform and is one of the most contemporary application programs in the Slovenian health care.
Assignment Name: HANSA EAST - EU-HANSA (Project Nr. HC1019)
Start Date (Month/Year): 01/98
Completion Date (Month/Year): 06/99
Narrative Description of Project: The HANSA projects aimed to promote the new technology and its standardized approaches through demonstrations and dissemination activities. This project demonstrated that employment of a middleware based open architecture yields reduction of working effort needed for interworking of existing systems capable to share ands exchange data. Meanwhile this architecture has already been adopted as a European standard, i.e. CEN TC 251 ENV 12967-1 “Healthcare Information Systems Architecture (HISA – Standard) The overall objectives of HANSA EAST project were to transfer the distributed software technologies for
171
open health, healthcare, hospital, and insurance systems and adopted European standards to the CEE/NIS countries: to the Health IT Authorities, and to Health IT providers for business development in order to create a local software industry for the health sector. HANSA EAST consisted of three different countries, complemented by a Concerted Action directed at the other countries, i.e. Albania, Bulgaria, Czech Republic, Estonia, Latvia, Lithuania, Slovak Republic and Slovenia. Through a series of RTD-projects, initiated from 1987 onwards and co-funded and supported by the CEU DGIII ESPRIT the basic distributed software technologies were available for open healthcare and hospital information systems based on European standards (i.e. HISA). EU-HANSA (Project Nr. HC1019) demonstrated and promoted these in 20 hospitals in 9 EU Member States. HANSA EAST applied, and evolved from results obtained through previous RTD (in HANSA WEST) and industrial activities: Architectural specification for open, modular healthcare and hospital information systems, offering interoperability of their constituent parts, stability of evolvement to future completion, and flexibility to replace or add modules in accordance with needs; Middleware of common services, i.e. the Distributed Health Environment (DHE), conformant to the HISA standard CEN/TC251 ENV 12967-1, already developed and demonstrated in the life scenarios in 10 EU-Member States, as a suitable platform for the integration of existing systems as well as for the implementation of new solutions; Methodological and technical experience gained by the organisations that particiapted in HANSA WEST. Description of Services Training in the DHE middleware, Installation of DHE middleware and migration of existing ‘legacy’ systems to an open,modular architecture, including training of local technical staff and technical support; Study with regard to the feasibility of the transfer of technology. Demonstrations to health IT authorities, health IT users and health IT suppliers, representing the CCE/NIS, and explanation of the benefits of the new technology. Health IT Strategy: identification, verification and publication of strategies to improve healthcare and to support healthcare reforms in CCE/NIS by the application of distributed software technologies for open HIS. Dissemination of Information: transfer of technology, promotion, documentation and dissemination of information about the application of distributed software technologies for open HISs in CCE/NIS. Market Creation, Implementation and Exploitation: collaborative action with and technical support to health IT authorities (for policy and setting the standards) and to health IT users (for practical implementation) in order to create growth markets of health IT in CCE/NIS; Identification of CCE/NIS health IT industries that are interested to invest, to adopt distributed software technologies for open HISs, and to collaborate and to transfer to these industries the new technology and support them with regard to business development to ensure successful exploitation; Creation of business opportunities in CCE/NIS to Western health IT industries and consultancies. Establishment of an international West-East network of excellence, including follow-up.
Assignment Name: INCO-COPERNICUS – PRIMACOM (PRIMAry Care physician’s COMunication Network) - PL961090
Start Date (Month/Year): 04/97
Completion Date (Month/Year): 10/99
Narrative Description of Project: In a public-private partnership, two regions in Hungary and Slovenia have established Regional Health Care Network for exchange of routine messages between healthcare professionals. Discharge letters are now daily
172
exchanged between Hospitals and General Practitioner. PRIMACOM have used European standards, developed by CEN TC 251, for exchange of medical data and experience by implementing Regional Health Care Networks from Denmark and Italy. PRIMACOM has paved the way for establishing Regional and National Health Care Networks in Slovenia and Hungary. PRIMACOM has supplied health care professionals with systems and infrastructure for enhancement of communication between primary and secondary healthcare. In Slovenia the role was to provide and implement the IT for the pilot regions, i.e. Hospital Information System , Primary Healthcare IS, integration with EDIFACT converter and mailer, as well as the establishment of a national Mail-box Server, connections to the virtual private healthcare network, and education and training of the end-users (i.e. doctors and nurses). Project PRIMACOM has provided standard for the discharge letter and demonstrated the use of best practice.
Assignment Name: RETRANSPLANT (REgional and International Integrated Telemedicine Network for Medical Assistance in End Stage Diseases and Organ TRANSPLANT Project) - HC4028 – IN4028
Start Date (Month/Year): 10/98
Completion Date (Month/Year): 03/01
Narrative Description of Project: The RETRANSPLANT project aimed to develop and install Telematics tools to bridge the various and geographically dispersed institutions playing a role in the complex process of organ collection from a donor and transplantation into one or several recipients. The generic model used was kidney transplantation and the information and communication technologies developed so far networked dialysis centers, organ transplant surgery clinics, tissue typing laboratories, organizations coordinating recipient to donor selection, and other health care facilities for organ transplant services in the Central and Eastern European Countries. RETRANSPLANT implemented a regional network to link different national organ transplant systems, to give on-line access to European transplant coordinators, donor centers, diagnostic specialists, to increase Europe-wide the effectiveness of organ transplant services. In the project we aimed to facilitate and realize introduction of information technology in the national (virtual private) network. We are sharing internationally developed IT tools, and provide support to establish networks in European countries and regions, as well as educate the end users for the use of information technology. Use of IT in everyday healthcare resulted in significant improvements in the care process and outcomes. We build the transplantation system on existing conventional clinical informatics systems by providing clinicians with network and multimedia health record-based decision support in Transplantology. We were involved in the following Work Packages (WP) and their corresponding deliverables: WP1 – Technology Implementation Objectives: To implement a generally applicable system for the communication between heterogeneous relational database systems. Flexibility, safety, security, confidentiality performance and cost effectiveness are key issues of its design. Deliverables: TI 1 Implementation of Local Area Networks in CEEC. Tool TI 2 Electronic medical record (EMR) at the tissue typing and Specification, Report Dialysis centers. TI 3 Implementation of the Multimedia Systems (PC/ISDN) Tool, Report in Ljubljana. TI 4 MEDANINFO Critical Care System in Ljubljana. Tool, Report TI 5 Implementation of Multimedia Imaging Systems. Specification, Report WP2 - Active Memory Card Objectives:
173
To register the patients on dialysis converted to an electronic patient database on chip card. Dialysis and Transplant Card enables an open architecture, which means it can easily be integrated into existing information systems and networking environments. Deliverables: AMC – Implementation of Dialysis and Transplant Card in Tool, Report Budapest and Ljubljana WP3 – Electronic Medical record Objectives: To implement a program where all clinical records can be registered. The program must contain standardized codes and information about diagnoses (ICPC/ICD10), drugs, procedures, investigations, laboratory tests etc. To ensure standardized and identical information, it is recommended that these indexes updated centrally. This makes it easier to transfer information about the patients from one health care facility to another. Deliverables: EMR1 Implementation and adaptation of the Electronic Tool, Specification Medical Record (EMR) in Ljubljana EMR2 Validation of EMR in and Ljubljana. Report WP4 – Recipient – Donor Selection Objectives: The electronic patient database (transplant waiting list, donor-recipient matching, organ allocation, patient selection) will help an optimal use of available donor organs and tissues in Czech, Slovak Republic, Hungary, Slovenia, Poland, Lithuania. Deliverables: RDS4 On line Access to HLA laboratories in CEEC Tool RDS5 ICD support. Specification, Report WP5 – Multimedia Medical System Objectives: The ISDN/PC-integrated Multimedia Medical System (MMS) provides integrated network of complementary services, i.e. Teleradiology, Telepathology, Telematics for anaesthesia, for organ transplant at Budapest and Szeged in Hungary and at Ljubljana in Slovenia. Deliverables: MMS Integration of Electronic Medical Systems including Tool, specification Active memory card, electronic patient record, Report Multimedia patient record in Budapest, Szeged and Ljubljana. WP6 – Regional Transplant Network Objectives: Fifteen medical units of the Central and Eastern European Countries participate in the project. The quality of the integration with existing devices (PC, Images, EMG, ECG) and basic functions of the RTPN System will be evaluated for quality assurance. Deliverables: RTPN1 – Integration of MMS, including Telepathology, Teleradiology Among Budapest, Szeged and Ljubljana Tools, Report RTPN2 – Interconnect Recipient - Donor Selection system and the Transplant Centers In CEEC Tools, Report RTPN3 – Validation of MMS among Budapest, Szeged and Ljubljana, Including EMR, Telepathology, Teleradiology Report WP7 – International Transplant Network Objectives: Interconnect and integrate the national networks and link to an existing international service result in to an International Transplant Network (ITPN).
174
Deliverables: ITPN1 - Interconnect the national RTPN and validate Prototype, Report the International Transplant Network. ITPN2 – Demonstration to the authorities and the public. Specification, Report WP8 – Integration of Transplant Networks on the European Level Objectives: The integration of networks: tissue typing and patient selection and matching laboratories, national transplant organisations, transplant clinics and the connected institutes will be achieved in the framework of the ACTION cluster of projects WP9 – Transplant Information Portal Objectives: The infrastructure for the deployment of TPweb (servers, routers, physical network, etc.) has been prepared. An English version of the TPweb would be implemented in Slovenia. Infonet provided the necessary technical support
Assignment Name: Health Sector Management Project (HSMP)
Start Date (Month/Year): 11/2000
Completion Date (Month/Year): Ongoing
Narrative Description of Project: The Health Sector Management Project (HSMP) has as its the primary objective “to secure the long term stability of the (health) system and to found its managing on provable and verifiable data focused on the patient”. The Project is formally an initiative of the Slovenia Ministry of Health and is funded by the Ministry. The Ministry has entered into a loan agreement with the World Bank for access to capital funds to complete the Project. The Project loan agreement became effective in November 2000 and the Project Office was formally established in April 2001. Major stakeholders working closely in concert with the Ministry include the Health Insurance Institute of Slovenia, the Public Health Institute, the Medical Chamber of Slovenia, the University Medical Center Ljubljana and the General Hospitals of Maribor and Jesenice. Additional stakeholders include professional organizations in the health sector, primary care centers and other hospitals. The Project has four primary components: C1: Health Policy Support C2: Health Information Systems Standards Formulation C3: Testing and Implementing Solutions in Pilot Organizations and Establishing a National Health Information Clearing House C4: Project Management Description of some Services: New Health Financing Development and Introduction Health Informatics Institute Scope and Functionality Definitions Validation of the common HISA model according to the national requirements To define Standard Interface for data exchange for NHICH network Organization and implementation of training and hands-on Documenting the modeling in Common Concept Library
175
Barriers to successful implementation of telemedicine Although no significant barriers to successful implementation of telemedicine exist at the moment in Slovenia, there are perhaps some obstacles that are slightly holding back its development. Some of them might be:
- Not enough awareness of its benefits from the user (e.g. doctors’) side
- Still not enough support from the Government side?
- Organisational issues: who is responsible for what; the lack of good project management (institutions)
Telemedicine technologies used by hospitals/doctors Applied research projects Project leaders Research Institution Title
Budget in 2002 (EUR)
The field of Science
dr. Ciril Grošelj
Ljubljana Medical Centre Assurance of quality in diagnostics 10.045Medical Sciences
dr. Igor Bartenjev
Ljubljana Medical Centre
TELEDERM-Contemporarily diagnostics of tumours and selected dermatosis 17.870Medical Sciences
dr. Marija Molan
Ljubljana Medical Centre
Medical profession model for advising children with some medical troubles 13.112Medical Sciences
dr. Valentin Fidler
Ljubljana Medical Centre
Development of picture capture with gamma camera and nuclearmedical-radiology graphic station 25.198Medical Sciences
dr. Brigita Drnovsek Olup
Ljubljana Medical Centre
Action of laserradiation on eye tissue in pericular area 23.243Medical Sciences
PROREC Slovenia Design and setting up of the National Centre (for Health Informatics) Several activities were taken in the first half of 2001: • Setting up a Widenet-SLO project team - staffing • Presentations for the Slovenian Medical Informatics Society members • Settling some financial and organisational issues at the national level • Two presentations have been made for the state Minister of Health and his Secretaries. The
Minister has promised his full support for the proposed Widenet activities. • Discussions and analyses have been initiated regarding the national Widenet centre and it’s statute
on the basis of the Belgium’s statute. • Prorec.SI statute drafted • Internet prorec-si.org domain acquired • An extensive draft version of the document ‘Promotion activities plan for the Widenet-Slo’ has
been prepared.
176
A promotional workshop organised for the potential Widenet project team members. Widenet-SLO project organisation structure and staffing have been set up. Promotional “white-paper” drafted. Widening and consolidating the network The following activities where taken in years 2001 and 2002: - Workshop on different aspects and possibilities of EPR data exchange in Slovenia - Co-organisers of the SMIS's conference Telecommunications in Healthcare; - Workshop and assessment of EPR and Health Risk Factors - Co-operation with the Slovenian national Health Sector Management Project (HSMP), dealing
with healthcare data modelling and Clearinghouse activities - Taking an active part in the Slovenian info-conference (INFOS), health informatics session - Widenet activities and meetings held during the MEDINFO 2001 conference, London - Prorec.Si Web page redesigned; - Participation in the Widenet web-site testing - Presentation and meetings of the 4 major Slovenian healthcare software providers consortium
organised. Planned activities for joined EHR activities. - Several meetings held managing PROREC.SI issues: project team, legal issues… - Participating at the EuroRec 2001 and a Widenet Consortium meeting, Nov.2001, Aix enP, France - SMIS's part of the deliverable 4.2 Strategies and Promotional Plans for National Markets prepared
and delivered, Jan 2002 - An International Prorec.Si EHCR event organised and held at Bled; jan-apr2002; - Prorec.SI legally established; a very successful kick-off event held. Prorec.SI – first projects started in 2003 A feasibility and technical study has been started regarding the lab results and discharge letter HL7/XML implementation. International experiences have been studied and compared. The first technical documentation was presented on a workshop for major Slovenian software providers. In the first quarter of 2004 the pilot project will be executed and evaluated. Members of the Slovenian Widenet project team have taken an active position in the:
• Preparation of a proposal for the national informatics and standardisation body • Restructuring governing bodies of the Prorec.SI • Advising in several local IT tenders regarding EHR issues.
Conclusion As a result of the Widenet project, a national Prorec centre (Prorec.SI) was established. Beside organisational and financial issues, the first project has already started. Status of EHR About 70% of all Slovenian hospitals are using an IT solution (e.g. Hospital Information System) developed in compliance with HISA pre-standard. This seems a good foundation for the development of a adequate EHR system, which would be based on the emerging European EHR standards, and implemented when they are available. The same fact is valid for around 60% of Primary Healthcare providers. Expenditure for IT in Slovene hospitals
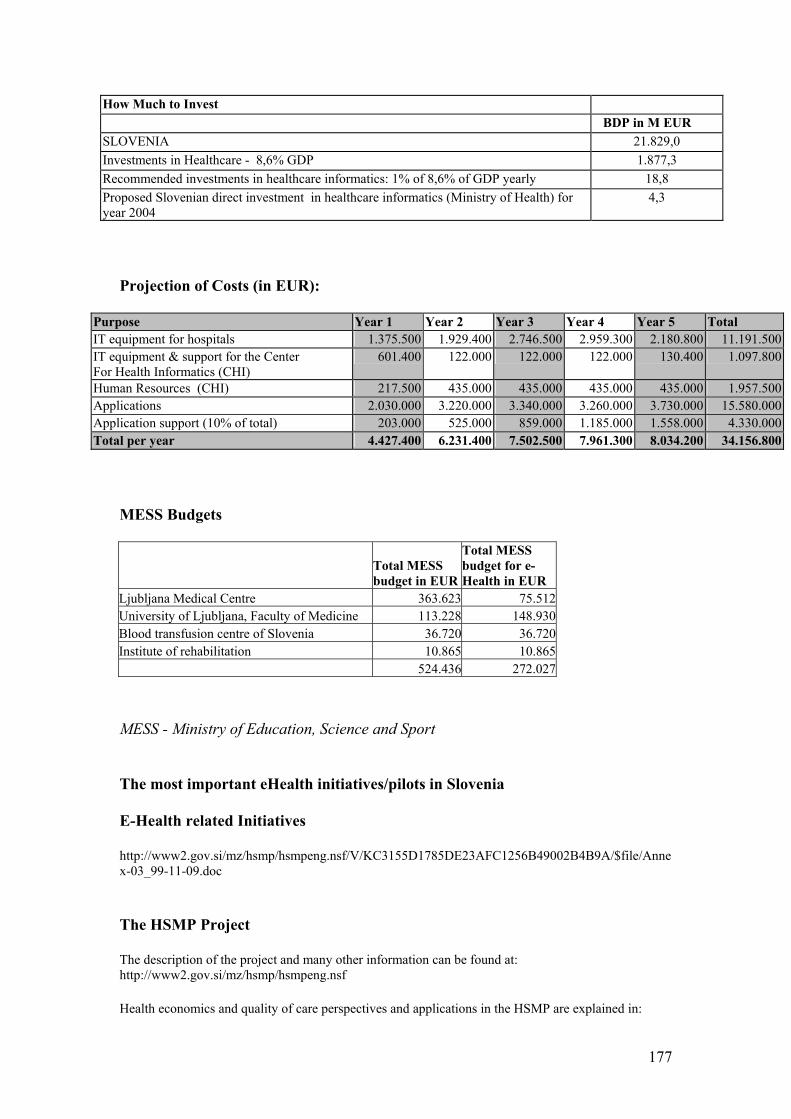
177
How Much to Invest BDP in M EUR SLOVENIA 21.829,0 Investments in Healthcare - 8,6% GDP 1.877,3 Recommended investments in healthcare informatics: 1% of 8,6% of GDP yearly 18,8 Proposed Slovenian direct investment in healthcare informatics (Ministry of Health) for year 2004
4,3
Projection of Costs (in EUR):
Purpose Year 1 Year 2 Year 3 Year 4 Year 5 Total IT equipment for hospitals 1.375.500 1.929.400 2.746.500 2.959.300 2.180.800 11.191.500IT equipment & support for the Center For Health Informatics (CHI)
601.400 122.000 122.000 122.000 130.400 1.097.800
Human Resources (CHI) 217.500 435.000 435.000 435.000 435.000 1.957.500Applications 2.030.000 3.220.000 3.340.000 3.260.000 3.730.000 15.580.000Application support (10% of total) 203.000 525.000 859.000 1.185.000 1.558.000 4.330.000Total per year 4.427.400 6.231.400 7.502.500 7.961.300 8.034.200 34.156.800
MESS Budgets
Total MESS budget in EUR
Total MESS budget for e-Health in EUR
Ljubljana Medical Centre 363.623 75.512University of Ljubljana, Faculty of Medicine 113.228 148.930Blood transfusion centre of Slovenia 36.720 36.720Institute of rehabilitation 10.865 10.865 524.436 272.027
MESS - Ministry of Education, Science and Sport The most important eHealth initiatives/pilots in Slovenia E-Health related Initiatives http://www2.gov.si/mz/hsmp/hsmpeng.nsf/V/KC3155D1785DE23AFC1256B49002B4B9A/$file/Annex-03_99-11-09.doc The HSMP Project The description of the project and many other information can be found at: http://www2.gov.si/mz/hsmp/hsmpeng.nsf Health economics and quality of care perspectives and applications in the HSMP are explained in:
178
http://vestnik.szd.si/st2-12ang/st2-12ang-757-759.htm Other task to be carried out before the end of HSMP project (and accepted and confirmed by the Ministry of Health) are also the following: Information Support to the System of Financing based on DRGs • All Slovenian hospitals were successfully connected to secure computer network “owned” by
Governmental Centre for Informatics.
• Hospitals have already adopted/updated their IT solutions to support the DGR system, and have already sent the data for the first 3-monthly period
• The data is being collected and processed on the national level. The responsible organisation is the National Institute for Health Protection/Public Health. Technical support is provided by Governmental Centre for Informatics.
Setting up the new bodies/entities to be responsible for health informatics on strategic and operational level Health Informatics Standards Board It should be noted that the Board is one of three key components of the national health informatics capability (the other components being the Health Informatics Council and the Centre for Health Informatics). The scope of the Board is informatics standards which are required and undertaken at the national level – i.e. those standards which are in common to all entities, agencies and institutions within the health system. The Board will engage in the identification of both standards (mandatory) and guidelines (optional but desirable). It will focus on the identification of standards and guidelines which promote and enable effective and efficient health information sharing. In most instances, this focus will result in standards and guidelines in the areas of data (e.g. data definitions, coding schemes), technology (e.g. data communications) and security (e.g. encryption). The Board will support and enable the achievement of Slovenian health sector goals by improving the quality, value, availability and accessibility of health information and provide proactive leadership in the cost effective use of informatics at the national level. Health Informatics Council The scope of the Council is informatics activities which are required and undertaken at the national level – i.e. those activities which are in common to all entities, agencies and institutions within the health system. The Council is accountable for all informatics activity required and undertaken in support of, and to enable, national level health system objectives. The Council reports, through the State Secretary, to the Minister of Health. The mandate of the Council is to support and enable the achievement of Slovenian health sector goals by improving the quality, value, availability and accessibility of health information and provide proactive leadership in the cost effective use of informatics at the national level of the Slovenian health sector Centre for Health Informatics The Centre itself is a professional agency operating on behalf of the overall health system (not just public health) but which is organisationally housed within the structure of the National Public Health Institute. As such, the Centre takes direction, for different aspects of its activities, from both the national health system and from the National Public Health Institute. The scope of the Centre is informatics activities which are required and undertaken at the national level – i.e. those activities which are in common to all entities, agencies and institutions within the health system. The mandate of the Centre is to support and enable the achievement of Slovenian health sector goals by improving the quality, value, availability and accessibility of health information and provide proactive leadership in the cost effective use of informatics at the national level of the Slovenian health sector.
179
Additional initiatives • National Healthcare Portal
• IT support for standardization with data dictionary
• Applications on the national level
• Support for Clinical Pathways
• Electronic Health Record • Data Interchange – Referrals, results, • Telemedicine • Computer at bed side
• DRG Support • e-DRG (already running) • DRG Grouper (already running)
Support for the DRG coding
180
Annex XXI Health Insurance Card Project – Health Insurance Institute, Slovenia In September 1995, the Health Insurance Institute of Slovenia, in conformity with the European and global development trends, and with its own business goals, defined the plan of substituting the health care identification booklet for a modern, computer-readable document - health insurance card. The health insurance card is an electronic tool of communication between the insured person, physician, health care center, hospital, health insurance provider, and pharmacy. The card transmits the key and stable data that are required in the implementation of health insurance. Ever since its foundation, the Institute has been systematically modernizing and promoting efficiency of operations in cooperation with its partners in the health care system, through an adequate information system and continuous upgrading of the system with state-of-the-art information technology. These efforts are also incorporated into the objectives, which served as the basis in the conception of the health insurance card project:
1. To improve the quality of services and of treating of insured persons both at the Institute and by other health care service providers.
2. To simplify and improve communication between the Institute, the physicians and health care institutions.
3. To cut down the number of various (unnecessary) procedures now required when the insured person implements their rights.
4. To improve the security of personal data within the information processing systems 5. To reduce the extent of administrative tasks and thereby achieve a higher efficiency of
operations at the Institute and within the health care service. 6. With reasonable financial investment, to provide long-term economic benefits at the
level of the national economy. In the first phase of the Slovenian project, the Institute is introducing a card serving administrative purposes (implementation of rights derived from compulsory and voluntary health insurance), supporting the procedures regarding the selection of a personal physician, and carrying an elementary form digital prescription. These functions involve legally incontestable identification details and their application for administrative purposes, the field where relatively modest organizational effort and costs promise to be repaid in clear and tangible benefits, due to a widespread use of the card. The card is designed to comply with the legal regulations and with the relevant Slovenian and international standards in force. The card is in accordance with the level of development of the information technology infrastructure in the Slovenian health care and health insurance networks. And its design also accommodates future expansion of the data set. Health Card The health insurance card is the only document applicable in the implementation of the compulsory and voluntary health insurance rights in Slovenia. This electronic document was issued to all persons dully covered by the compulsory health insurance in Slovenia, i.e. to the entire population of close to 2 million. A person is to present the card when visiting at the doctor's and at all other occasions of implementing the rights deriving from health insurance. The health insurance validity is updated by the card holder, through the self-service terminals. The updating of insurance validity also updates card data from the central databases. The card is a means of easy and direct transfer of data between the insured persons, the insurance company and the health care organizations. Data electronically recorded in the card are accessible for reading only to authorized health professional card holders. Procedures associated with the card are fast and ensure high service quality and data security. The card system is aligned with the Slovenian health care and health insurance sector conditions and regulations. Furthermore, it duly observes international recommendations and standards. Similar card
181
infrastructure is introduced in other European countries, in the framework of their efforts to create applicability of such electronic documents across national borders.
182
Annex XXII InfoNet – healthcare information systems company, Slovenia INFONET was founded in 1991 as an information engineering company. The company founders were three mathematicians that have been dealing with computer science in various environments for more than 10 years, and have resulted in a coordinated team with many experiences. The main thrust of the company is the integration of our work, which is building and launching information systems in the health care and pharmaceutical sectors. The development and implementation covers three basic fields:
• hospital information systems • pharmacy information systems • information systems for Primary Health Care and GPs
A major step in the development of Medical Informatics in Slovenia was made at the beginning of 1993, when the Institute of Health Insurance of the Republic of Slovenia bought 2750 IBM personal computers and distributed them to public health institutions, as well as to the first private ones. In addition to hardware, health care institutions received a computer program for accounting and invoicing the health care services (reimbursement), free of charge. The program was developed entirely by INFONET. During the following months, over 5000 users were trained to work with computers, mainly administrative staff and nurses. In the years when we were building information systems in the health care we have:
• Implemented into our systems all requirements of our legislation. • Tried to understand specific problems of medical information science and we learned to solve
them • Very well recognised the way of thinking and particularities of medical staff, and learned to
listen to them and comply with their requirements. • Assumed the role of advisers for the field of information systems at majority of our partners,
as well as for the organisation changes. • Joined with important companies from the computer science field in Slovenia, which grants us
and our business partners the latest technology and quality information service. • Included in our projects a lot of experiences and knowledge acquired on international
congresses and at various other forms of international co-operation with several partners from abroad.
Through our contracts in the medical professions, we are generally able to anticipate changes related to the legislature and are therefore able to provide application modifications and updates so as to avoid potential delays to our customers business processing. INFONET is assisted by medical specialists from different fields. Within the team there are in addition specialists for the different platforms and for the different applications. These professionals are also responsible for maintenance related to law, as well as for programming modifications and enhancements. In 1995 INFONET's development migrated to Graphical User Interface (GUI), to Client/Server model and to object oriented technologies, encapsulating OO paradigm in all areas of software development: from project planning, analysis, design, prototyping and data modelling to actual programming and testing. The original programme name was InfoMed (INFOrmatics in MEDicine), which has been lately renamed to InfoMed21 and complemented with E-Med21. The development and implementation still covers three basic fields: Hospital Information Systems, Information Systems for Primary Health Care, Pharmacy Information Systems. We are committed to the latest standards in distributed relational databases and object oriented development, as well as relying on the healthcare application standards such as HISA (CEN-TC251), ECHRA, HL7, CORBA and XML. Following the latest trends in object oriented design, distributed relational databases, and using the latest generation of object oriented programming languages and tools, we are able to offer the products

183
that conform to required standards and meet the immediate needs and that are adaptable to the future evolution. The use of this technology resulted in three different, extensive software applications (Multimedia Electronic Patient Record & Management System for Hospitals - BIRPIS21, Information System for Primary Healthcare (ISOZ21) and Healthcare Decision Support System. Furthermore, within the frame of E-Med programme, Internet and intranet (i.e. Web, Java and XML) solutions are being developed to remotely support information exchange between medical specialists, patient data inquiry, creation and examination of Medical Knowledge-bases and other general medical and administration information retrieval, using the latest IT, and based on intelligent interfaces and mobile multimedia. In April 2000 INFONET received an ISO 9001 Certificate for Quality System on ``Development and implementation of IS, consultations in the field of IS, integration, technical support and maintenance of IS". Infonet now has 27 employees, with expertise in mathematics and computer science, many of them being young engineers with a lot of knowledge, and fresh, original ideas. The company's turnover has increased steadily since it was established in 1991, particularly since four years ago. In 1999, consolidated net revenues were over 1.5 million USD.
• Activities in Information Environment for Healthcare • International Projects in Medical Informatics • References and Products - The InfoMed System • Name and Contact Details


















