Technology Newborn Screening for Medium Chain Acyl~CoA ...€¦ · Newborn screening for certain...
73
Newborn Screening for Medium Chain Acyl~CoA Dehydrogenase Deficiency Using Tandem Mass Spectrometry: Clinical and Cost-effectiveness Technology Report Issue 62 March 2006
Transcript of Technology Newborn Screening for Medium Chain Acyl~CoA ...€¦ · Newborn screening for certain...

Newborn Screening for Medium Chain Acyl~CoA Dehydrogenase Deficiency Using Tandem Mass Spectrometry: Clinical and Cost-effectiveness
Technology Report
Issue 62 March 2006

Cite as: Tran K, Banerjee S, Li H, Noorani HZ, Mensinkai S, Dooley K. Newborn screening for medium chain acyl~CoA dehydrogenase deficiency using tandem mass spectrometry: clinical and cost-effectiveness [Technology report no 62]. Ottawa: Canadian Coordinating Office for Health Technology Assessment; 2006. This report and the French version entitled Le dépistage néonatal du déficit en acyl-coenzyme A déshydrogénase des acides gras à chaîne moyenne par le biais de la spectrométrie de masse en tandem : efficacité clinique et rapport coût-efficacité are available on CCOHTA’s web site. Production of this report is made possible by financial contributions from Health Canada and the governments of Alberta, British Columbia, Manitoba, New Brunswick, Newfoundland and Labrador, Northwest Territories, Nova Scotia, Nunavut, Ontario, Prince Edward Island, Québec, Saskatchewan, and Yukon. The Canadian Coordinating Office for Health Technology Assessment takes sole responsibility for the final form and content of this report. The views expressed herein do not necessarily represent the views of Health Canada or any provincial or territorial government. Reproduction of this document for non-commercial purposes is permitted provided appropriate credit is given to CCOHTA. CCOHTA is funded by Canadian federal, provincial and territorial governments. Legal Deposit - 2006 National Library of Canada ISBN: 1-897257-02-3 (print) ISBN: 1-897257-03-1 (online) PUBLICATIONS MAIL AGREEMENT NO. 40026386 RETURN UNDELIVERABLE CANADIAN ADDRESSES TO CANADIAN COORDINATING OFFICE FOR HEALTH TECHNOLOGY ASSESSMENT 600-865 CARLING AVENUE OTTAWA ON K1S 5S8
Publications can be requested from:
CCOHTA 600-865 Carling Avenue
Ottawa ON Canada K1S 5S8 Tel. (613) 226-2553 Fax. (613) 226-5392
Email: [email protected]
or download from CCOHTA’s web site: http://www.ccohta.ca

Canadian Coordinating Office for Health Technology Assessment
Newborn Screening for Medium Chain Acyl~CoA Dehydrogenase Deficiency Using Tandem Mass Spectrometry: Clinical and Cost-effectiveness
Khai Tran MSc PhD1
Srabani Banerjee MSc PhD1
Huimin Li MA1
Hussein Z. Noorani MSc1
Shaila Mensinkai MA MLIS1
Kent Dooley PhD FCACB2
March 2006
1 Canadian Coordinating Office for Health Technology Assessment (CCOHTA), Ottawa ON 2 Department of Pathology, Dalhousie University School of Medicine, Halifax NS

i
Reviewers These individuals kindly provided comments on this report.
External Reviewers Denis C. Lehotay, PhD DABCC FCACB FACB Adjunct Professor of Pathology University of Saskatchewan College of Medicine, Saskatoon SK Director, Metabolic Diseases Laboratory Consultant Biochemist, Provincial Laboratory Regina SK
Khalid Aziz, MA FRCPCH FRCPC Associate Professor Discipline of Pediatrics Faculty of Medicine Memorial University of Newfoundland St. John’s NL
Tim Caulfield, LLM BSc LLB Canada Research Chair in Health Law & Policy Research Director, Health Law Institute Professor, Faculty of Law, Faculty of Medicine & Dentistry University of Alberta Edmonton AB
Pranesh Chakraborty, BSc MD FRCPC (Medical Biochemistry and Pediatrics) FCCMG (Biochemical Genetics) Assistant Professor Departments of Pediatrics, and Pathology and Laboratory Medicine University of Ottawa Ottawa ON
CCOHTA Scientific Advisory Panel Reviewers Jeff Scott, MD Provincial Medical Officer of Health Province of Nova Scotia 1690 Hollis Street Halifax NS
David Hailey, MSC PhD GradRIC Professor University of Alberta Department of Public Health Sciences Faculty of Medicine and Oral Health Sciences 13-103 Clinical Sciences Bldg. Edmonton AB
Philip Jacobs, PhD Professor University of Alberta Department of Public Health Sciences Faculty of Medicine and Oral Health Sciences 13-103 Clinical Sciences Bldg. Edmonton AB
This report is a review of existing public literature, studies, materials and other information and documentation (collectively the “source documentation”) which are available to CCOHTA. The accuracy of the contents of the source documentation on which this report is based is not warranted, assured or represented in any way by CCOHTA and CCOHTA does not assume responsibility for the quality, propriety, inaccuracies or reasonableness of any statements, information or conclusions contained in the source documentation.

ii
CCOHTA takes sole responsibility for the final form and content of this report. The statements and conclusions in this report are those of CCOHTA and not of its Panel members or reviewers. Authorship All authors participated in the planning of the project, revision of the manuscript drafts, and addressing of the reviewers’ comments. These steps were coordinated by Khai Tran. Khai Tran was the project lead and lead author for the report. Khai Tran and Srabani Banerjee jointly drafted, reviewed, and revised all sections of the report. Kent Dooley provided clinical content expertise, cost data, the detailed information required for economic analysis and budget impact, and advice on the literature search. He also reviewed manuscript drafts. Huimin Li was lead author of the Economic Analysis section. Hussein Noorani was lead author of the Ethical and Psychosocial section. Shaila Mensinkai was responsible for the design and execution of the literature search strategies, for writing the methods section and associated appendix on literature searching, and for verifying and formatting the bibliographic references. For clinical studies, the screening, data extraction, and quality assessments were done by Khai Tran and Srabani Banerjee; for economic studies, by Huimin Li and Khai Tran; and for ethical and psychosocial studies, by Hussein Noorani and Khai Tran. Acknowledgements The authors are grateful to Mark Walker MD, the Ottawa Hospital and University of Ottawa; and Khalid Aziz, Memorial University of Newfoundland, for the revision of the economic model; and to Bruce Brady, CCOHTA, for advice during the economic analysis and budget impact development. Conflict of Interest No conflicts of interest were declared by the authors.

iii
REPORT IN BRIEF March 2006 Newborn Screening for Medium Chain Acyl~CoA Dehydrogenase Deficiency Using Tandem Mass Spectrometry: Clinical and Cost-effectiveness
Technology Tandem mass spectrometry (MS/MS)-based newborn screening for medium chain acyl~CoA dehydrogenase deficiency (MCADD).
Disease MCADD is an inherited metabolic disorder. In Canada, there are about 20 incident cases/year. Most MCADD patients are asymptomatic before an acute episode, which manifests with signs of encephalopathy, hypoglycemia, or sudden death. Of those who have an acute episode, almost one-quarter will die, and one-third of survivors will have irreversible neurological damage.
Issue Newborn screening for certain inborn errors of metabolism is standard across Canada, but screening for MCADD is not consistently practised. Thus, many cases of MCADD are diagnosed clinically, often during an acute episode. Because it is treatable if diagnosed early, there is a need to determine whether jurisdictional newborn screening programs should be expanded to include MCADD. Methods and Results A systematic review of the clinical and economic literature was performed. The clinical sensitivity and specificity of MS/MS-based screening for MCADD were very high.
The economic review and analysis showed that screening results in more quality-adjusted life-years (QALY), and lower morbidity and mortality compared with no screening. The economic review showed that screening is cost-effective compared to no screening if willingess to pay is $50,000 per QALY. The primary economic analysis using Canadian data showed that screening is cost-effective if willingness to pay is $20,000 per QALY.
Implications for Decision Making • Newborn screening of MCADD by MS/MS
identifies patients while they are asympto-matic. Without screening, diagnoses of MCADD are typically made at clinical presentation, often during an acute episode.
• MS/MS screening for MCADD has high clinical validity. The addition of MCADD to Canadian newborn screening programs would identify about 20 cases/year.
• MS/MS-based screening for MCADD consumes more resources but attains better health outcomes than no screening.
• Based on a primary economic analysis, screening is cost-effective if willingness to pay is $20,000 per QALY.
• Ethical and psychosocial issues, such as informed consent, false diagnosis, parental anxiety, privacy, and confidentiality, warrant consideration.
This summary is based on a comprehensive health technology assessment available from CCOHTA’s web site (www.ccohta.ca): Tran K, Banerjee S, Li H, Noorani HZ, Mensinkai S, Dooley K. Newborn screening for medium chain acyl~CoA dehydrogenase deficiency using tandem mass spectrometry: clinical and cost-effectiveness.
Canadian Coordinating Office for Health Technology Assessment (CCOHTA) 600-865 Carling Avenue, Ottawa ON Canada K1S 5S8 Tel: 613-226-2553 Fax: 613-226-5392 www.ccohta.ca
CCOHTA is an independent, not-for-profit organization that supports informed health care decision making by
providing unbiased, reliable information about health technologies.

iv
EXECUTIVE SUMMARY The Issue Medium chain acyl~CoA dehydrogenase deficiency (MCADD) is a rare metabolic disorder that can be treated, if diagnosed early. Screening for MCADD is not consistently practised across Canadian health jurisdictions. There is a need to determine whether jurisdictional screening programs should be expanded to include MCADD. Objective The aim of this report is to review the use of tandem mass spectrometry (MS/MS) in newborn screening for MCADD as opposed to clinical diagnosis. Clinical Review Methods: Multiple databases were searched to obtain literature. Results: After searching electronic databases from 1995 onwards, we identified 957 citations, of which 21 studies (15 full-length reports, 6 abstracts) of limited quality met our selection criteria. Most of the studies on MCADD screening by MS/MS addressed only the incidence data, which was high in Germany (1:9,773 to 1:15,625) and northern UK (1:12,600). The mean incidence was 1:16,667 (95% CI: 1:14,286 to 1:20,000). The clinical sensitivity and specificity were 100% and 99.99% respectively, and the positive and negative predictive values were 51% and 100% respectively, assuming a false negative rate to be zero. Nine studies conducted MCADD screening for up to eight years and reported 96% of patients as asymptomatic. Five of the nine studies had no clinical follow-up. Among patients who were detected by clinical diagnosis, 23% were asymptomatic, and 16% had died. Most patients detected by newborn screening were asymptomatic, while most who presented clinically had potentially irreversible damage. The percentage of fatal cases among those diagnosed clinically was significantly higher than that among those diagnosed by screening. Economic Review Methods: After searching electronic databases from 1995 onwards, we identified 289 citations, of which two studies met selection criteria. Quality was assessed via the BMJ 35-item checklist. Results:One study showed that screening yields an incremental cost-effectiveness ratio (ICER) of $41,862 per quality-adjusted life-year (QALY) over a lifetime. The other study showed that the ICER was $5,600 (95% CI: <$0 to $17,100) per QALY over the first 20 years of life, and $100 (95% CI: <$0 to $6,900) per QALY over a 70-year horizon. Both studies showed that MS/MS screening was cost-effective compared to no screening, if willingness to pay is $50,000 per QALY.

v
Economic Analysis Methods: A decision-tree model guided our analysis of cost-effectiveness, with pathways based on disease progression, the impact of screening on the health care system, and the availability of data. Results: In Canada, screening uses more resources, but results in lower morbidity and mortality than no screening. Under the base case analysis, the ICER was $2,514 per QALY. Under the best scenario, where both the incidence of MCADD and the positive predictive value of the test were higher than under the base case, the ICER was $928 per QALY. Under the worst scenario, where both the incidence of MCADD and the positive predictive value of the screening were lower than under base case conditions, the ICER was $11,456 per QALY. In the one-way sensitivity analysis, the ICER was most sensitive to varying screening cost, changing from dominant to $6,963 per QALY with a screening cost of $0.50 to $5.60. Similarly, the ICER values varied from dominant to <$11,000 per QALY in the two-way sensitivity analyses. The results indicate that screening is cost-effective based on the CE threshold of C$20,000 per QALY. Health Services Impact The estimated prevalence for MCADD in Canada is 1:16,000 or 20 cases among 330,000 newborns each year. The ratio of true to false positives would be 1:1.65. Based on the Nova Scotia experience (8,533 newborns per year), the screening program would cost $220,419 in the first year with a total cost of $270,438 over the first three years and $317,920 over five years. Ethical and Psychosocial Issues The screening of IEM in newborns raises concerns, including informed consent, false diagnosis, parental anxiety, privacy, and confidentiality. Parents need to be adequately informed about the screening tests and their associated risks, so that they have the option to refuse the tests. Positive screens need to be reported quickly for clinical reasons. Conclusion Despite limitations in the quality of the identified studies, the benefits of MS/MS screening for MCADD in newborns are greater than those of no screening. MCADD can be a fatal disease, but it is preventable if it is detected pre-symptomatically. There is limited evidence of clinical follow-up or of concomitant comparison of outcomes between newborn screening and clinical diagnosis. Our economic review and our primary economic analysis show that MS/MS-based screening for MCADD consumes more resources, but results in better health outcomes when compared to no screening. In both of the studies included in the economic review, screening was found to be cost-effective if willingness to pay is $50,000 per QALY. Our primary economic analysis, which was based on Canadian data so as to better reflect the Canadian setting, found screening to be cost-effective if willingness to pay is $20,000 per QALY. Not all parents may want their newborns screened for MCADD, but they should be informed about the risks and given the option to refuse.

vi
ABBREVIATIONS AC8 octanoylcarnitine AC10 decanoylcarnitine CBA cost-benefit analysis CEA cost-effectiveness analysis CH congenital hypothyroidism CI confidence interval CMA cost-minimization analysis CUA cost-utility analysis ICER incremental cost-effectiveness ratio IEM inborn errors of metabolism MCADD medium chain acyl~coenzyme A dehydrogenase deficiency MS/MS tandem mass spectrometry PKU phenylketonuria QALY quality-adjusted life-year

vii
GLOSSARY Clinical sensitivity: proportion of patients with disease who test positive. Clinical specificity: proportion of patients without disease who test negative. Compound heterozygote: MCADD individual who is heterozygous for two MCADD mutations, usually A985G mutation on one allele and different mutation on the other; differs from wild-type heterozygote, which is a carrier who is unaffected clinically. 95% confidence interval (CI) of the mean: one can be 95% sure that the calculated interval contains the population mean. 95% confidence interval (CI) of the difference between means: one can be 95% sure that the true difference between means lies within the interval; if the 95% CI for the difference between the means includes zero, the difference is not statistically significant. Cost-effectiveness threshold: Cost-effectiveness (CE) analysis is used to inform policy decision makers on the allocation of health care resources. Although it has met criticism, policy makers often apply the CE threshold to decision making. The threshold figure of US$50,000/QALY has been quoted since 1982. This number was originally based on the “dialysis standard” for patients with chronic renal failure. For the Canadian health care system, Laupacis et al.1 proposed a threshold range with lower and upper boundaries. Adoption of an intervention is strong if the CE ratio is <C$20,000/QALY, moderate if it is between C$20,000/QALY and C$100,000/QALY, and weak if it is >C$100,000/QALY. A comprehensive review on CE thresholds was recently published.2 Dominate: The new technology dominates the old technology when the cost per unit of effectiveness for the new technology is lower compared with that of the old technology. Incremental cost-effectiveness ratio (ICER): cost of an extra unit of effectiveness produced when the new technology is used over comparator; please refer to the Health Technology Assessment Handbook.3 Negative predictive value: probability that individuals with negative test results will not get the disorder. Patient years of follow-up: sum of individual units of time that persons in the study population have been followed. Positive predictive value: probability that individuals with positive test results will get the disorder. Quality-adjusted life-years (QALY): This result of a quality adjustment of each gained life-year from an intervention is a common measure of benefit that combines quantity and quality of life. It is calculated by estimating the total number of life-years gained from treatment and by

viii
weighting each year with a quality of life score (or utility) to reflect the quality of life in that year. Please refer to the Health Technology Assessment Handbook.3 Utility-weight: utility in a health state in the form of health-related quality of life during time considered; value can be between zero and one; value of zero stands for worst possible health state, where patient is dead; value of one indicates that the patient is in perfect health.

ix
TABLE OF CONTENTS EXECUTIVE SUMMARY ......................................................................................................... iv ABBREVIATIONS...................................................................................................................... vi 1 INTRODUCTION................................................................................................................. 1
1.1 Background..................................................................................................................... 1 1.2 Overview of the Technology .......................................................................................... 3
2 THE ISSUE............................................................................................................................ 4 3 OBJECTIVES ....................................................................................................................... 4 4 CLINICAL EFFECTIVENESS REVIEW......................................................................... 4
4.1 Methods........................................................................................................................... 4 4.1.1 Literature search strategy .................................................................................... 5 4.1.2 Selection criteria and method.............................................................................. 5 4.1.3 Data extraction strategy....................................................................................... 6 4.1.4 Strategy for quality assessment ........................................................................... 6 4.1.5 Data analysis methods ......................................................................................... 6
4.2 Results............................................................................................................................. 6 4.2.1 Quantity and quality of research available .......................................................... 6 4.2.2 Trial characteristics ............................................................................................. 8 4.2.3 Data analysis and synthesis ................................................................................. 8
4.3 Discussion..................................................................................................................... 19 5 ECONOMIC ANALYSIS .................................................................................................. 22
5.1 Review of Economic Evaluations................................................................................. 22 5.1.1 Methods............................................................................................................. 22 5.1.2 Results ............................................................................................................... 24 5.1.3 Discussion ......................................................................................................... 27
5.2 Primary Economic Analysis ......................................................................................... 27
5.2.1 Methods............................................................................................................. 27 5.2.2 Results ............................................................................................................... 32 5.2.3 Discussion ......................................................................................................... 38
6 HEALTH SERVICES IMPACT ....................................................................................... 41
6.1 Population Impact ......................................................................................................... 41 6.2 Budget Impact............................................................................................................... 42
6.2.1 Assumptions ...................................................................................................... 42 6.2.2 Methods............................................................................................................. 42 6.2.3 Results ............................................................................................................... 43 6.2.4 Discussion ......................................................................................................... 43
6.3 Planning, Implementation, and Legal or Regulatory Issues ......................................... 45

x
7 ETHICAL AND PSYCHOSOCIAL ISSUES................................................................... 46
7.1 Methods......................................................................................................................... 46 7.1.1 Literature search strategy .................................................................................. 46 7.1.2 Inclusion and exclusion criteria......................................................................... 46 7.1.3 Data extraction strategy..................................................................................... 46
7.2 Results and Discussion ................................................................................................. 47 7.2.1 Quality of research available............................................................................. 47 7.2.2 Trial characteristics ........................................................................................... 47 7.2.3 Data analysis and synthesis ............................................................................... 47
7.3 Summary ....................................................................................................................... 51 8 CONCLUSION ................................................................................................................... 52 9 REFERENCES.................................................................................................................... 53 APPENDICES - available from CCOHTA's web site www.ccohta.ca APPENDIX 1: Literature Search Strategy for Clinical Objectives APPENDIX 2: Literature Search Strategy for Economic Objectives APPENDIX 3: Literature Search Strategy for Psychosocial/Ethical Objectives APPENDIX 4: Clinical Data Extraction Form APPENDIX 5: Quality Assessment of Included Clinical Studies* APPENDIX 6: Equations for Calculation of 95% Confidence Interval APPENDIX 7: Characteristics of Included Clinical Studies APPENDIX 8: Inclusion and Exclusion Criteria of Clinical Studies APPENDIX 9: Protocol of Included Clinical Studies APPENDIX 10: Economic Data Extraction Form APPENDIX 11: Quality Assessment of Included Economic Studies APPENDIX 12: Probabilities of Different Health Outcomes Illustrated in Decision Tree APPENDIX 13: Cost-related Variables and Cost Parameters Used in Economic Model APPENDIX 14: Values of Parameters in Base Case Scenario APPENDIX 15: Protocol for Follow-up for Case Detected with MCADD* APPENDIX 16: Costs Incurred for Cases with Different Health Consequences in Model (Applicable to all Scenarios) APPENDIX 17: Values of Key Parameters Varied Under Three Scenarios APPENDIX 18: Estimated Values of Key Parameters (In Addition to those in Base Case Scenario) Used for Budget Analysis APPENDIX 19: Study and Patient Characteristics and Ethical or Psychosocial Considerations

1
1 INTRODUCTION
1.1 Background Inborn errors of metabolism (IEM) are rare disorders with a wide spectrum of clinical manifestations. The morbidity or mortality associated with some of these disorders can be prevented by early diagnosis and treatment. Many of these disorders fall into one of three biochemical categories – amino acid disorders, organic acid disorders, and fatty acid oxidation disorders. One of the fatty acid oxidation disorders, medium chain acyl~CoA dehydrogenase deficiency (MCADD), is an autosomal recessive inherited abnormality, and one of the most common metabolic defects of fatty acid ß-oxidation. The pathway of fatty acid ß-oxidation plays a crucial role in energy production during fasting or exercise.4 When energy is needed during those periods, fatty acids are released from adipose tissue into the circulation; taken up by the cells of the heart, muscle, and liver; and converted to acyl~CoA esters in the cytoplasm. The acyl~CoA esters traverse the mitochondria membrane as acylcarnitines and are reconverted into acyl~CoA in the mitochondria matrix. The first step of ß-oxidation is mediated by very long chain acyl~CoA dehydrogenase, medium chain acyl~CoA dehydrogenase, or short chain acyl~CoA dehydrogenase, depending on the acyl chain length (Figure 1). Incompletely oxidized acyl chain intermediates exit the cells, because of a defect in one of the enzymes, and accumulate in the plasma as acylcarnitines. MCADD is characterized by the increased plasma levels of octanoylcarnitine (AC8) or an increased ratio of AC8 to decanoylcarnitine (AC10). There is no correlation between mutation type and clinical phenotype. Although there are approximately 30 mutations found in the MCADD gene,5 >80% of clinically diagnosed patients are homozygous for A985G mutation, and 18% are compound heterozygous with the A985G mutation on one allele and another mutant allele.6 About half of those identified through screening programs of different populations are homozygous for the A985G mutation. A new mutation, 199T→C, which was not found in clinically diagnosed patients, but is present in a large proportion of the acylcarnitine-positive samples from newborn screening, also causes MCADD.7 It is unknown why this new mutation is not prevalent in children presenting symptomatically. Symptoms manifest most commonly in early childhood, with signs of acute encephalopathy and hypoglycemia that could link to sudden death. Most MCADD patients are asymptomatic before an acute episode. An acute episode usually occurs within the first two months of life; 19% to 25% will die; and one third of the survivors will have irreversible neurological damage and may require life-time hospital care. 6,8,9 Affected individuals are kept well by dietary management, or returned to stability by timely intervention. A preventive strategy, which is based on a high carbohydrate intake orally or intravenously during fasting or gastrointestinal infection, seems to be effective.8,10 Because newborn screening for MCADD is new, there are no long-term studies of the treatment outcomes of patients who are identified by newborn screening.

2
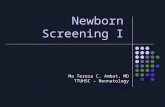
Figure 1: Simplified pathway of mitochondrial ß-oxidation
Adapted from Vianey-Liaud et al.11 Plasma free fatty acids enter the cells by simple diffusion. Fatty acyl~CoA esters are produced in the cells and converted to fatty acylcarnitine derivatives, which are transported through the mitochondial membranes by the enzyme carnitine palmitoyl transferase (CPT). Inside the mitochondria, fatty acyl~CoA are reformed and progressively catabolized to acetyl~CoA by ß-oxidation through a series of dehydrogenation reactions, yielding energy directly in the citric acid cycle or through ketogenesis. Three fatty acyl-CoA dehydrogenases have been identified: long chain acylCoA dehydrogenase (LCAD), medium chain acylCoA dehydrogenase (MCAD), short chain acylCoA dehydrogenase (SCAD). FAD=flavin adenine dinucleotide, ETF= electron transfer flavoprotein, ETF DH=electron transfer flavoprotein dehydrogenase. Patients who are diagnosed clinically with MCADD or as siblings of MCADD patients, have been shown to remain free from life-threatening episodes once diagnosed and monitored by a metabolic disease clinic.10 Because the common A985G mutation of MCADD originated in people of northern European descent, MCADD prevalence is higher in Germany, the UK, and English-speaking countries.12,13 About 35 to 70 newborns each year in the UK (prevalence of 1:20,000 to 1:9,091) have MCADD.14 In German states, including Lower Saxony (northern Germany), the incidence was found to be 1:9,773.15 Given that the Canadian birth rate in 2003-2004 was 10.4 per 1,000 or 330,803 births,16 Canada would expect to have about 20 cases of MCADD if the incidence is 1:16,000.
Acyl~CoA +
Carnitine
long chain Acyl~CoA+
Carnitine
medium chain Acyl~CoA
short chain Acyl~CoA
Acyl~CoA
FAD ETF ETF DH
FAD ETF ETF DH
FAD ETF ETF DH
LCAD
MCAD
SCAD
CPT
mitochondria cytoplasm

3
Epidemiological data, such as the incidence and prevalence of MCADD in different provinces in Canada, are unavailable, and may vary depending on the ethnic origin of the population. In Canada, newborn screening is not provided consistently across all jurisdictions. Researchers in the US, Germany, the UK, and Australia have advocated for newborn screening of MCADD by tandem mass spectrometry (MS/MS) to reduce morbidity and mortality. In the US, 40 states already do so, and in 31 of these states, MCADD screening is mandatory.17
1.2 Overview of the Technology The MS/MS method uses two mass spectrometers in sequence (tandem).18 The first spectrometer separates compounds by their molecular mass (precursor ions) from a nebulized and ionized blood spot extract. The separated molecular ions pass through a “collision cell,” where they are bombarded with a gas that generates fragments (product ions). These are then passed to a second spectrometer for an analysis of their masses. The results specify each molecule and quantitate the amount. Abnormal levels of the analytes of interest can be detected based on a pre-determined cut-off concentration. The application of MS/MS in the screening of different IEMs from one dried-blood spot has been reviewed.19 For MCADD, most laboratories extract the acylcarnitines from the blood samples and derivatize them into corresponding butyl ester forms before MS/MS analysis, while a small number of laboratories analyze acylcarnitines in an underivatized form. Care should be given to result interpretation, because it may affect the sensitivity of the test. MS/MS is the method of choice for detecting the increased levels of medium chain acylcarnitines in patients with MCADD. Alternative technologies include high performance liquid chromatography, gas chromatography, mass spectrometry, and DNA technology. These technologies are limited by their lack of robustness and high throughput, low rates of sensitivity and specificity, reduced cost-effectiveness, or unavailable automation. The screening of MCADD using MS/MS technology has high specificity, and sensitivity. The concentrations of AC8 decrease as time progresses after birth. This increases the false negative rate as a function of age. This should not be a problem as newborns are screened before 72 hours of age.20 Appropriate cut-off concentrations of AC8 must be predetermined to avoid excessive false positives. Newborn screening cutoffs for AC8 range from 0.3 µM to 1.5 µM, with most programs using a cutoff of 0.5 µM to 1.0 µM.20,21 Depending on the age and type of enzyme mutation, AC8 concentrations can be as low as 0.3 µM, which is below the cut-off values used in many laboratories. As a result, effective detection requires the determination of other identifiers including a relative molar ratio of AC8 to AC10.20 Positive results require additional testing. There is a risk of an initial positive becoming a false negative, if one relies on MS/MS testing on a repeat blood spot to confirm the screening result, because AC8 drops with age and may only be raised when the patient is stressed. As a result, positive cases should be followed up with molecular testing, fibroblast enzyme activity, or clinical evaluation with organic acid, acylglycine, and acylcarnitine analysis to confirm or rule out the diagnosis. According to the experience of the Nova Scotia Screening Program, this is

4
manageable, because the false positive rate with a cutoff of 0.7 µM should be <1:10,000 (KD, unpublished observations, 2005). MS/MS-based screening facilities can be established in hospital or public health laboratories. Private companies, such as Pediatrix, provide screening services in the US. Perkin Elmer does not directly provide screening, but supplies laboratories with equipment, software, and kits for screening. It is essential to have a follow-up infrastructure that involves the services of clinical geneticists, genetic counsellors (or metabolic clinicians), dietitians; and of a specialized metabolic clinic. These facilities are available in most provinces in Canada, mainly for PKU and CH. These may not be adequate for MCADD, or other fatty acid, organic acid, or amino acid diseases. 2 THE ISSUE MCADD is a rare metabolic disorder that can be treated if diagnosed early. Screening for MCADD is not consistently practised across Canadian health jurisdictions. There is a need to determine whether jurisdictional screening programs should be expanded to include MCADD. 3 OBJECTIVES The objective of this report is to review the potential application of MS/MS to detect MCADD in newborns, in the Canadian context of screening programs, taking into account the clinical, financial, ethical, and psychosocial issues. This report will assist policy makers and program managers in making informed decisions as whether MCADD should be included in the existing screening program. The questions that will be addressed by the report include: • What is the evidence of benefit, harm, and validity (sensitivity, specificity, and predictive
values) from MS/MS-based newborn screening of MCADD? • What are the clinical outcomes of patients with MCADD whose conditions were detected at
birth by MS/MS compared to those who were diagnosed later in childhood? • What is the cost-effectiveness of screening for MCADD using MS/MS? • What is the budget impact of screening for MCADD using MS/MS? • What are the ethical and psychosocial issues associated with newborn screening for MCADD
using MS/MS? 4 CLINICAL EFFECTIVENESS REVIEW
4.1 Methods A protocol for the review was written a priori and followed throughout the review process.

5
4.1.1 Literature search strategy
We obtained published literature by cross-searching MEDLINE®, BIOSIS Previews®, PASCAL, Social ScienceSearch®, PSYCInfo®, ERIC, and EMBASE® databases from 1995 onwards. A broad search strategy with appropriate descriptors and keywords was used. We also ran parallel searches on PubMed, CINAHL®, and Cochrane databases. Appendix 1 includes details of the literature search strategy. We established regular alerts on MEDLINE®, BIOSIS Previews®, and EMBASE® databases until March 2005, and updated searches on PubMed, CINAHL®, and Cochrane databases regularly. The last PubMed update was performed in August 2005. Grey literature was obtained by searching the web sites of regulatory agencies, health technology assessment and related agencies. Specialized databases such as the University of York NHS Centre for Reviews and Dissemination, and the Latin American and Caribbean Center on Health Sciences Information (LILACS) were also searched. We searched the Internet using search engines for web-based information.
4.1.2 Selection criteria and method
Inclusion criteria specified studies of newborn screening for MCADD using MS/MS, and those comparing outcomes of MS/MS-based screening and clinical diagnosis. We also included studies on outcomes of MCADD patients detected from clinical diagnosis only. a) Selection criteria • study design: cohort (prospective and retrospective) • population: newborns or children (unspecified age) • intervention: screening for MCADD using MS/MS • comparator: no screening (clinical diagnosis) • outcome: information on incidence, clinical validity, and genetics of MCADD detected by
MS/MS and clinical diagnosis were captured and compared; clinical outcomes such as disability and mortality that occurred after detection and during follow-up were also recorded; details of outcomes to be extracted are listed in Appendix 4.
Reviews, letters, comments, and secondary observations that were not primary studies were excluded. Validation studies on the efficacy of MS/MS technology were also excluded. b) Selection method Two reviewers (KT and SB) independently screened all citation titles and abstracts retrieved from the literature search, based on the selection criteria. The reviewers compared what each had included and excluded before ordering full texts. Differences were resolved by consensus. They then independently reviewed the full text articles, applied the selection criteria to these, and again compared which studies they had accepted. Duplicate publications of the same trial were excluded. All decisions about which studies to include were verified by the content expert author (KD).

6
4.1.3 Data extraction strategy
Data from selected studies were extracted independently by the same two reviewers using the data extraction form (Appendix 4). Discrepancies were resolved by discussion.
4.1.4 Strategy for quality assessment
Two reviewers (KT and SB) used a quality assessment tool known as QUADAS22 to assess the quality of studies of MS/MS-based screening for MCADD. It includes items that cover bias, variability, and reporting. The tool consists of 14 questions that can be answered as yes (Y), no (N), unclear (U), or not applicable (NA), with the help of the tool’s guidelines for scoring (Appendix 5). Quality assessment was not performed with studies retrieved in abstract forms.
4.1.5 Data analysis methods
The results of the MS/MS-based screening for MCADD included incidence, rate of detection, sensitivity, specificity, and predictive values. Markers for MCADD were AC8 levels and the ratio of AC8/AC10 in the plasma. The DNA analysis for the common A985G mutation determined the genotype (homozygosity or compound heterozygosity) whose percentage could be calculated. The data available for clinically diagnosed MCADD patients included rate of detection, numbers of symptomatic patients, asymptomatic patients, heterozygotes, and homozygotes; and outcomes such as hypoglycemia and lethargy, coma and encephalopathy, neurological impairment and developmental delay, full recovery, and death. The 95% CI for incidence and detection rate were calculated using the equations shown in Appendix 6. The weighted means and corresponding 95% confidence intervals (CI) were calculated for symptomatic patients, asymptomatic patients, homozygotes, heterozygotes, and several outcomes (e.g., death, neurological impairment, coma, hypoglycemia, and full recovery) using the equations listed in Appendix 6. To compare MCADD patients detected by MS/MS screening with those diagnosed clinically, the mean difference and corresponding 95% CI were calculated using the equations shown in Appendix 6.
4.2 Results 4.2.1 Quantity and quality of research available
The literature search yielded 957 publications, of which 48 potentially relevant clinical studies were identified. After reviewing the full text of retrieved reports, 21 studies were included for data extraction.6,7,15,20,23-39 Among the included studies, 15 are full-length6,7,15,20,23-27,29-31,37-39 and six are in abstract forms.28,32-36 Of the 27 excluded articles, seven were of general IEM without MCADD data or case studies,40-46 six were duplicates of included studies,10,47-51 six were on establishing the test criteria,52-57 and eight had an inappropriate study design.58-65 The selection of clinical studies is shown in Figure 2.

7
Figure 2: Selection of clinical evidence for review
We assessed the quality of 14 of the 21 included studies, using the QUADAS scale. The results are shown in Appendix 5 and summarized in Table 1. Of the remaining seven studies, six were reported in the abstract form28,32-36 and one, which was a retrospective evaluation of the outcomes of clinically diagnosed MCADD patients,6 was not subjected to quality assessment. Of the tool’s 14 questions, questions 5, 6, 11, and 12 are more specific for diagnostic testing, but not applicable to the current screening test. In 12 of 14 studies, the populations were from certain ethnic groups and not a mixed population. Most studies did not describe the selection criteria or the time period between the reference standard test and MS/MS screening. The reference standard (DNA analysis and fibroblast enzyme activity assay) is likely to correctly classify MCADD. In 11 out of 14 studies, the reference standard test used was independent of the MS/MS screening. Six studies described the MS/MS procedure for the analysis of acylcarnitine
957 citations identified from electronic search and screened
909 citations excluded
48 potentially relevant reports retrieved for further scrutiny
21 relevant reports describing 21 studies
27 reports excluded: • general IEM (n=7) • duplicate publications (n=6) • study on establishing test criteria (n=6) • inappropriate study design (n=8)

8
profiles in enough detail to permit replication. Most studies (10 out of 14) did not describe how they did their reference standard test. As the MS/MS screening was given before the reference standard test, they are independent of each other (question 10, score Y). None of the studies reported or explained uninterpretable or intermediate test results and withdrawals.
Bias-related items 3, 7, and 10 showed that most studies used an appropriate reference standard to correctly classify the target condition, although it was unclear about the time period between reference standard and screening test (item 4). Bias-related item 14 shows that all studies did not report withdrawals. Variablity-related items 1 and 2 dealing with the spectrum of patients and patient selection criteria were poorly scored in most studies. Reporting-related items 8, 9, and 13 were also scored negatively among included studies.
4.2.2 Trial characteristics
Of the 21 studies, four compared outcomes of patients identified by MS/MS screening and those of patients identified by clinical diagnosis,23,25,27,29 one studied the outcomes of MCADD patients after being diagnosed,6 and 16 presented the results of patients identified by MS/MS screening only7,15,20,24,26,28,30-39 (see Appendix 7 for the characteristics of included clinical studies). Most are prospective studies for MS/MS-based MCADD screening, except for the study by Pourfarzam et al.30 which used MS/MS to screen 100,600 newborn blood samples that had been collected in the past two and a half years. The screening results were compared with those obtained by clinical diagnosis during that period. There were two studies on outcomes of patients detected by clinical diagnosis.6,30 The study period varied from one to eight years for MS/MS-based screening, and one to 24 years for clinical diagnosis. The screening population of newborns ranged from 9,320 to 930,078. The sampling time also varied between studies, but usually was taken after the second or third day of life. Patients who were clinically diagnosed for MCADD were in their early childhood (two days to 10.5 years). The plasma AC8 cut-off levels indicated in 10 studies7,15,20,26,27,29-31,34,38 varied from 0.25µM to 1 µM. Three studies20,24,34 appeared to be funded by Neo Gen Screening, Inc. The inclusion criteria and the protocol of MS/MS screening of the included studies are shown in Appendices 6 and 7 respectively.
4.2.3 Data analysis and synthesis
a) Incidence, rate of detection, clinical validity and predictive values Table 2 summarizes the incidence of MCADD, rate of its detection, clinical validity, and predictive values of MS/MS-based newborn screening. Of those studies, five20,26,29-31 provided all listed information, while the others presented mainly the incidence of MCADD. The calculated MCADD incidence based on the detected cases and the study population varies from 1:68,560 to 1:8,930. The mean of the incidence is 1:16,667 (95% CI: 1:20,000; 1:14,286). The rate of detection of MCADD, expressed as cases per year, varies from 0.25 to 17 with a mean of 5.4 (95% CI: 4.3 to 6.4). The incidence and rate of detection were highest in two studies in Germany15,23 (1:9,773 to 1:15, 625 in Bavaria, Baden-Wurttemberg, and Lower Saxony).26

9
A high incidence was also found among newborns in the northern region of the UK (1:12,600).30 The incidence rate from one study in Argentina36was inconclusive, because of its relatively small population (9,320 newborns). Exclusion of this study does not affect the overall mean incidence (not shown). In the US, particularly for newborn populations in Pennsylvania, Massachusetts, and North Carolina, the incidence varies from 1:8,930 to 1:28,571 with a mean of 1:18,695. Four studies from Australia reported the incidence of MCADD at 1:21,294,25 1:22,971,29 1:47,500,32 and 1:68,560.38 As there was no long-term follow-up, it would be impossible to accurately determine the number of false negatives. Available data from five studies20,26,29-31 showed that the means for clinical sensitivity and specificity were 100% and 99.99% respectively, and the means for positive and negative predictive values were 51% and 100% respectively, assuming that the false negatives were zero. b) Acylcarnitine profile and DNA analysis for common A985G mutation of MCADD
patients identified by MS/MS screening The plasma AC8 levels, the ratios of AC8/AC10, and the percentage of A985G mutation in individuals (homozygotes and compound heterozygotes) identified by MS/MS screening are listed in Table 3. Of 10 studies,7,15,20,24,28,29,31,33,34,39 six7,15,28,29,31,34 reported plasma AC8 levels, and five 7,15,28,29,34 reported the ratio of AC8/AC10 from MCADD homozygotes and compound heterozygotes. The mean plasma AC8 levels of the homozygotes and compound heterozygotes were 6 μmol/L (95% CI: 0.9 to 11.6) and 4 μmol/L (95% CI: 0.4 to 7.2) respectively. The mean difference of plasma AC8 levels was 2 μmol/L (95% CI: -3.3 to 7.3), which is not statistically significant. The mean of AC8/AC10 ratios of the homozygotes and compound heterozygotes were 11 (95% CI: 7.8 to 14.4) and five (95% CI: 3.0 to 6.9) respectively. The mean difference of AC8/AC10 ratios was six (95% CI: 3.0 to 9.0), which is statistically significant. Among the MCADD patients detected by MS/MS-based screening, a mean of 54% (95% CI: 46 to 61) are homozygous, and a mean of 34% (95% CI: 28 to 41) are compound heterozygous for A985G mutation. This is in contrast to clinical diagnosed patients, who were mostly (>80%) homozygous. c) Outcomes of MCADD patients detected by MS/MS-based screening Outcomes of MCADD patients detected by MS/MS were classified as asymptomatic, symptomatic, and dead (Table 4). Of nine studies, five7,23,25,28,29 had no follow-up period, and two27,39 did not clearly mention follow-up details. The outcomes were mostly reported during the screening period, which varied from one to eight years. Two studies followed patients who tested positive for MCADD through screening. The study by Schulze et al.26 reported its follow-up period as 20 months (mean), while the study by McCandless et al.34 reported its follow-up period as 36.5 patient years.

10
Table 1: Quality assessment performed for 14 studies using QUADAS tool
Number of Studies for which Response was Question Yes (Y)
No (N)
Unclear (U)
Not Applicable (NA)
1. Was the spectrum of patients representative of the patients who will receive the test in practice?
2 1 11 0
2. Were selection criteria clearly described? 2 12 0 0 3. Is the reference standard likely to correctly classify the target condition?
11 1 2 0
4. Is the time period between reference standard and index test short enough to be reasonably sure that the target condition did not change between the two tests?
0 0 13 1
5. Did the whole sample or a random selection of the sample, receive verification using a reference standard of diagnosis?
0 0 0 14
6. Did patients receive the same reference standard regardless of the index test result?
0 0 0 14
7. Was the reference standard independent of the index test (i.e. the index test did not form part of the reference standard)?
11 0 3 0
8. Was the execution of the index test described in sufficient detail to permit replication of the test?
6 8 0 0
9. Was the execution of the reference standard described in sufficient detail to permit its replication?
3 10 1 0
10. Were the index test results interpreted without knowledge of the results of reference standard?
14 0 0 0
11. Were the reference standard results interpreted without the knowledge of the results of the index test?
0 0 1 13
12. Were the same clinical data available when test results were interpreted as would be available when the test is used in practice?
0 0 0 14
13. Were uninterpretable/ intermediate test results reported? 0 14 0 0 14. Were withdrawals from the study explained? 0 14 0 0
Wording of 14 questions taken directly from QUADAS. 22

11
Table 2: Incidence, rate of detection, sensitivity, specificity and predictive values of MS/MS screening
Incidence Positive Negative Predictive Value
(%) Author
(country) Population Number
of Cases Per
100,000
Rate of Detection
(cases/year) True False True False
Sensitivity (%)
Specificity (%)
Positive Negative
Hoffmann (Germany)23
382,247 29 1:13,000 8 14.5
Marsden (US)24
~200,000 7 1:28,571 4 2.8
Wilcken (Australia)25
362,000 17 1:21,294 5 4.3
Schulze (Germany)26
250,000 16 1:15,625 6 4.6 16 46 249,938 0 100 99.98 25.81 100
Shigematsu (Japan)27
102,200 2 1:51,100 2 0.46
*McCandless (US)28
557,720 41 1:13,603 7
Carpenter (Australia)29
275,653 12 1:22,971 4 3 12 11 275,630 0 100 99.99 52.2 100
Pourfarzam (UK)30
100,600 8 1:12,600 8 3.2 8 6 100,586 0 100 99.99 57 100
Andresen (US)7
930,078 62 1:15,001 7 7.8
Zytkovicz (US)31
184,000 10 1: 18,400 5 5 10 42 183,973 0 100 99.98 19 100
*Wilcken (Australia)32
190,000 4 1:47,500 2 2
*Marsden (US)33
108,000 4 1:27,000 4 4
*McCandless (US)34
327,031 24 1:13,629 7 8
*Rosher (Germany)35
166,000 13 1:12,769 8 4.3
Sander (Germany)15
283,408 29 1:9,773 10 17

12
Incidence Positive Negative Predictive Value (%)
Author (country)
Population Number of Cases
Per 100,000
Rate of Detection
(cases/year) True False True False
Sensitivity (%)
Specificity (%)
Positive Negative
*Abdenur (Argentina)36
9320 1 1:9,320 11 0.25
Naylor, 1999 (US)37
601,440 39 1:15,422 6 5.9
Wiley (Australia)38
137,120 2 1:68,560 1 2
Chace (US)20 283,803 16 1: 17,706 6 3.8 16 0 283,783 0 100 100 100 100 Ziadeh (US)39
80,371 9 1:8,930 11 9
Mean (CI, 95%)
1:16,667 (1:20,000; 1:14,286)
6 [5, 7]
5.4 (4.3, 6.4)
100 99.99 51 (11; 91)
100
* indicates abstracts

13
Table 3: Results of MS/MS analysis of acylcarnitine profile and DNA analysis for common A985G mutation
AC8 (µM) AC8/AC10 Ratio Percent of Cases Author
(country) Homozygous Compound Heterozygous Homozygous Compound Heterozygous
Homozygous Compound Heterozygous
Marsden (US) 24 43 (3/7) 57 (4/7) *McCandless (US) 28
3.91 (CI, 95%: 3.24 to 4.59)
1.86 (CI, 95%: 0.83 to 2.89) 10.2 (CI, 95%: 9.2 to 11.2)
6.0 (CI, 95%: 3.3-7.9)
71 (30/41) 25 (10/41)
Carpenter (Aurtralia)29
Screening: 5.6 (range 2.6 to 8.4) Follow-up: 9.6 (range 8.0 to 24.6)
Screening: 7.5 (range 1.1 to 24.6) Follow-up: 2.1 (range 0.7 to 3.8)
9.6 5.3 33 (4/12) 67 (8/12)
Andresen (US)7 >2 0.5 to 2.0 >4 2 to 4 63 (39/62) 34 (21/62) Zytkovicz (US)31 13.8 (range 9 to
22) 2.6 (range 1.9 to 3.2) 40 (4/10) 60 (6/10)
*Marsden (US)33 25 (1/4) 75 (3/4) *McCandless (US) 34
3.64 1.18 14.2 3.2 70 (14/20) 30 (6/20)
Sander (Germany)15
4.15 (mean of 15 patients)
5.86 (of one patient) 10.4 5.3 52 (15/29) 3.4 (1/29)
Chace (US)20 56 (9/16) 44 (7/16) Ziadeh (US)39 44 (4/9) 56 (5/9) Mean (CI, 95%) 6 (0.9, 11.6) 4 (0.4, 7.2) 11 (7.8, 14.4) 5 (3.0, 6.9) 54 (46, 61) 34 (28, 41)
*indicates abstract; AC8=octanoylcarnitine; AC10=decanoylcarnotine; compound heterozygous=heterozygous for two MCADD mutations.

14
Only the study by Schulze et al.26 reported that MCADD patients began their treatments between the ages of seven and 65 days. Five7,26,27,34,39 out of nine studies described the treatment in general as avoidance of fasting, low fat and high carbohydrate diets, and supplementation with carnitine. Glucose infusion was given to patients having clinical episodes, poor oral intake, or viral illness. Most MCADD patients identified by MS/MS-based screening were asymptomatic. The mean percent of patients with or without symptoms after detection by screening was 4% (95% CI: 1 to 9) and 96% (95% CI: 92 to 98) respectively. The mean percent of patients who died during or after positive detection by screening was 2% (95% CI: 1 to 6). Symptoms in MCADD patients included hypoglycemia and vomiting.27,28 Some asymptomatic patients were admitted to hospital for intravenous glucose infusion because of inadequate intake of fluids.34 The patients who died were usually those first detected at the start of screening as a result of complications associated with MCADD or with intercurrent illness.7 The actual number of fatal cases after screening should be lower than 2%.39 d) Results of studies comparing outcomes between MCADD patients detected by
MS/MS-based screening and those detected by clinical diagnosis Four studies23,25,27,29 compared outcomes between MCADD patients detected by MS/MS-based screening and those detected by clinical diagnosis (Table 5). Patients diagnosed through screening were observed from two to four years, while those diagnosed clinically were observed from two to 24 years. The mean rate of detection for MS/MS screening is 5.4 cases/year (95% CI: 4.3 to 6.4), while that of clinical diagnosis is 3.8 cases/year (95% CI: 1.6 to 6.0). The mean (individual values) of MCADD incidence obtained from MS/MS screening is 1:27,091 (1:13,000; 1:21,294; 1:51,100; 1:22,971) and from clinical diagnosis is 1:68,109 (1:44,000; 1:92,217). The study by Carpenter et al.29 compared DNA analysis between MCADD patients detected by MS/MS screening and clinical diagnosis. Among patients who were detected by clinical diagnosis, 85% were homozygotes for the A985G mutation, compared to 33% of those detected by MS/MS screening. In contrast, more compound heterozygous patients were found by MS/MS screening (67%) than by clinical diagnosis (15%). The study of Hoffmann et al.23 showed that patients identified by MS/MS were asymptomatic, while 68% (13/19) of patients diagnosed clinically had symptoms, leading to hypoglycemic seizure (1/19, 5%), developmental delay (3/19, 16%), and death (2/19, 10%). The other symptoms such as hepatitis and anemia might not be causally related with MCADD.

15
Table 4: Outcomes of MCADD patients detected by MS/MS-based screening
Outcomes Author (cuntry) Follow-up Period Age at Start of
Treatment Method of Treatment % of Asymptomatic
(na/n) % of Symptomatic
(ns/n) % Died (nd/n)
Hoffmann (Germany)23
No follow-up NA NA 100 (29/29) 0 (0/29) 0 (0/29)
Wilcken (Australia)25
No follow-up NA NA 88 (15/17) 12 (2/17) 6 (1/17)
Schulze (Germany)26
Mean=20 months, after detection by screening
range 7 to 65 days
Avoidance of fasting and supplementation with L-carnitine
100 (16/16) 0 (0/16) 0 (0/16)
Shigematsu (Japan)27
NM NM Low-fat formula and L-carnitine supplement
50 (1/2) 50 (1/2) with hypoglycemia
0 (0/2)
*McCandless (US)28
No follow-up NA NA 98 (40/41) 100 (10/10) heterozygotes
2 (1/41) 3 (1/30) homozygotes with hypoglycemia several heterozygotes with vomiting
0 (0/41)
Carpenter (Aurtralia)29
No follow-up NA NA 92 (11/12) 8 (1/12)
0 (0/12)
Andresen (US)7 No follow-up After identification of MCADD
On breast milk or regular formula, with no fat restriction during first year of life; prolonged fasting; most received oral carnitine in varied doses; some had glucose infusion when having episodes or poor oral intake or viral illness
97 (60/62) No deaths, related symptoms, or serious and permanent sequelae identified after implementation of treatment
3 (2/62) as result of complications associated with MCADD; those were first detected at start of screening

16
Outcomes Author (cuntry) Follow-up Period Age at Start of
Treatment Method of Treatment % of Asymptomatic
(na/n) % of Symptomatic
(ns/n) % Died (nd/n)
*McCandless (US)34
36.5 patient years NM On L-carnitine treatment and breast milk or regular infant formula with no fat restriction in first year of life; avoid prolonged fasting and monitor blood glucose using glucometers when concerned about child’s oral intake or clinical status
100 (24/24) 8% (2/24) during follow-up period, 2 patients have been admitted total of 4 times for intravenous glucose infusion due to inadequate intake of fluids
0 (0/24) No significant hypoglycemia, no seizures, no developmentally abnormal
0 (0/24)
Ziadeh (US)39 NM NM Low fat, high carbohydrate diet; parents are provided with genetic counselling and prenatal diagnosis
78 (7/9) 22 (2/9) ;2 died suddenly; one was homozygous for G985A mutation, entered a metabolic crisis after immunization; other was compound heterozygous, died during intercurrent illness
Mean (CI, 95%)
96 (92, 98) 4 (1, 9) 2 (1, 6)
* indicates abstracts; NA=not applicable; NM=not mentioned; n=number of cases detected; na=number of cases with no symptoms; ns=number of cases with symptoms; nd=number of patients who died.

17
Table 5: Results of studies involving MS/MS-based screening and clinical diagnosis
Author (Country) Outcomes MS/MS Clinical Diagnosis Period of study (years) 2 2 Cases detected (n) 29 19 Rate of detection (case/year) 14.5 9.5 Incidence 1:13,000 1:44,000
Hoffmann (Germany)23
% of symptomatic (ns/n) 0 (0/29) 68 (13/19) leading to hypoglycemic seizures (1), developmental delay (3), death (2)
Period of study (years) 4 24 Cases detected (n) 17 23 Rate of detection (cases/year) 4.25 0.96
Wilcken (Australia)25
Incidence 1:21,294 1:92,217 Period of study (years) 4.3 2 Cases detected (n) 2 1 Rate of detection (cases/year) 0.46 0.5
Shigematsu (Japan)27
Incidence 1:51,100 ND Period of study (years) 4 13.5 Cases detected (n) 12 13 Rate of detection (cases/year) 3 0.96 Incidence 1:22,971 ND % of homozygosity for A985G mutation
33 85
% of heterozygosity for A985G mutation
67 15
Carpenter (Australia)29
% of symptomatic (ns/n) 8 (1/12) ; one heterozygote with hypoglycemia
8 (1/13) ; one homozygote with hypoglycemia, coma and encephalopathy on day 2
ND=not determined; n=number of cases detected; ns=number of cases with symptoms e) Outcomes of patients detected by clinical diagnosis Our literature search from 1995 onwards identified two studies,6,30which examined only the outcomes of patients who were clinically diagnosed. As a result, the study of Wilson et al.,10 which reported the same cohort as that of Pollitt et al.6 was excluded. The results are presented in Table 6. The mean percent of homozygosity and heterozygosity for A985G mutation in clinically diagnosed patients and the corresponding 95% CI are 81% (95% CI: 70 to 89) and 19% (95% CI: 11 to 30) respectively. Most patients presented with symptoms [76% (95% CI: 64 to 85)], which included hypoglycemia and lethargy [59% (95% CI: 46 to 70)], coma and encephalopathy [37% (95% CI: 26 to 50)] and neurological impairment and developmental delay [10% (95% CI: 4 to 20)]. The mean percent of fatal cases was 16% (95% CI: 8 to 26).

18
Table 6: Results of studies of MCADD patients after being diagnosed clinically
Author (country) Clinical Status Pourfarzam (UK)30 Pollitt (UK)6
Mean (CI, 95%)
Cases 8 patients 62 (family history, n=13; symptomatic, n=46, 10 of whom died; other reasons, n=3)
NA
% of homozygosity for A985G mutation
87.5 80 81 (70, 89)
% of heterozygosity for A985G mutation
12.5 20 19 (11, 30)
Follow-up period None (retrospective) None % of asymptomatic 12.5 (1/8) 24 (15/62) 23 (14, 35) % of symptomatic 87.5 (7/8) 74 (46/62) 76 (64, 85) % of full recovery from attack NR 48 (30/62) NA % of hypoglycemia and lethargy 50 (4/8, at age 6 months to 3 years) 60 (37/62) 59 (46, 70) % of coma and encephalopathy 38 (3/8 at age 2 to 3 years) 37 (23/62) 37 (26, 50) % of neurological impairment and developmental delay
13 (1/8, learning difficulties, no episodes of encephalopathy)
10 (6/62) 10 (4, 20)
% died 13 (1/8 died of gastroenteritis at age 17 months)
16 (10/62) 16 (8, 26)
NA=not applicable; NR=not reported. f) Mean differences in outcomes of MCADD patients detected by MS/MS-based
screening and those who were clinically diagnosed Table 7 compares outcomes between studies of MS/MS screening alone (from Tables 2, 3, 4) and those of clinical diagnosis alone (Table 6). The rate of detection for MS/MS was taken from Table 2, while that of clinical diagnosis was from Table 5. As shown in Table 7, the difference in the rate of detection of MCADD from MS/MS screening and from clinical diagnosis was 1.6 cases/year (95% CI: −4.1 to 7.3) and is not statistically significant (i.e., the corresponding 95% CI for the difference between the means includes zero). On the other hand, the differences in the percent of homozygosity and heterozygosity for A985G mutation, the percent of fatal cases, and the percent of patients who present with or without symptoms are statistically significant. Proportions of homozygotes and heterozygotes found in MCADD patients detected by MS/MS screening were 54% (95%CI: 47 to 61) and 34% (95% CI: 28 to 41) respectively, whereas the corresponding proportions in MCADD patients detected by clinical diagnosis were 81% (95% CI: 70 to 89) and 19% (95% CI: 11 to 30) respectively. Almost all (96%) MCADD patients detected by MS/MS screening were asymptomatic, while most (76%) of those detected by clinical diagnosis were symptomatic. Significantly fewer fatal cases were seen by MS/MS screening than by clinical diagnosis, with a mean difference of -13 (95% CI: -25 to -5).

19
Table 7: Outcomes of MCADD patients detected by MS/MS-based screening versus after being clinically diagnosed
MS/MS* Clinical Diagnosis† Outcomes
Mean (CI, 95%) Mean Difference
(CI, 95%) Rate of detection (cases/year) 5.4 (4.3, 6.4) 3.8 (1.6, 6) 1.6 (−4.1, 7.3) % of homozygosity for A985G mutation 54 (47, 61) 81 (70, 89) −28 (−38, −14) % of heterozygosity for A985G mutation 34 (28, 41) 19 (11, 30) 15 (2, 26) % of asymptomatic 96 (92, 98) 23 (14, 35) 73 (60, 82) % of symptomatic 4 (1, 9) 76 (64, 85) −72 (−82, −59) % died 2 (1, 6) 16 (8, 26) −13 (−25, −5)
*data from Tables 2 to 4; †data from Table 6. See Appendix 7 for calculation of 95% confidence interval (CI, 95%) of mean and of difference between means.
4.3 Discussion The quality of most of the identified studies is limited, according to the QUADAS tool (Appendix 5). Some populations were specific ethnic groups, which calls into question the external validity of the results, because most did not describe their selection criteria. There was also no description of the period between getting positive results from MS/MS screening and getting a confirmatory test, which is usually DNA analysis or fibroblast enzyme activity assay. This would not be a major point of concern, because a preventive treatment would immediately begin once the positive screening results are repeated (experience from the Nova Scotia program). The confirmatory test is independent of the screening test and is likely to correctly classify the disorder. In most cases, the methods of screening, either by MS/MS or confirmatory tests, were not described in enough detail to permit replication. None of the included studies reported uninterpretable or intermediate test results, or withdrawals from the studies. Of 21 studies, 15 prospectively used MS/MS to screen for MCADD. With the exception of the studies by Schulze et al.26 and that of McCandless et al.,34 most did not follow up on patients who tested positive. The studies usually only reported the symptoms, including hypoglycemia and vomiting, or death, observed within the study period, which varied from one to eight years. Efforts were made to identify and exclude duplicate studies in which the same population was used more than once, although there is some uncertainty in this respect among the included studies. The incidence and rate of detection for MCADD varied between studies depending on the study population. For instance, the incidence was high (1:9,773 to 1:15, 625) in some regions of Germany such as Bavaria, Baden-Wurttemberg, and Lower Saxony,15,26,35 and in the northern region of the UK (1:12,600).30 Studies on the Australian populations reported incidences from 1:21,294 to 1:68,560, and one study on the Japanese population reported an incidence of 1:51,100. Similarly, studies in the US reported different incidences that varied from 1:8,930 to 1:28,571. The estimated incidence expressed as weighted mean was 1:16,667 (95% CI: 14,286 to 1:20,000). It would be reasonable to assume that the incidence for MCADD in Canada, with its

20
multicultural population, would be close to 1:16,000. With this incidence rate, approximately 20 cases would be expected in Canada, given a population of 330,803 newborns in 2003-2004.66 Because MCADD is a fatal disease yet is treatable if detected early, the plasma AC8 cut-off level was set low (from 0.25 µM to 1 µM), which allowed detection of both compound heterozygotes [mean for AC8 was 4 (95% CI: 0.4 to 7.2)] and homozygotes [mean for AC8 was 6 (95% CI: 0.9 to 11.6)]. With this setting and with the assumption of no false negatives, the results of five studies showed that the clinical sensitivity and specificity of the screening test was 100% and 99.99% respectively (Table 2). 20,26,29-31 As there was no long-term follow-up, it is uncertain whether the MS/MS screening caught every case (i.e., all false negatives over the long term). For those studies using AC8 cutoffs at 1 µM, which is higher than the lower limits of the 95% CIs of mean AC8 of both homozygotes and compound heterozygotes, there exists a chance of having false negatives. Four of the five studies showed that of those who tested positive, the percentage of true positives (i.e., positive predictive values, which determine the chance that a patient has the disease if the test is positive) varied between 19% and 57%.26,29-31 One study20 showed that all those who tested positive were true positives. The false positive error rate varied between 0% and 0.02%. Unlike false negatives, some false positives in a screening test are tolerable, because they can be eliminated by subsequent confirmatory tests, although with extra cost and at the expense of parental stress. Laboratory confirmation tests include a urine organic acid profile, DNA technology, and fibroblast enzyme assay.12 The literature review indicates that most studies did not describe their reference standards. For a national screening initiative, it is important to reach an agreement among jurisdictions on which reference standard is the best indicator for MCADD confirmation. The numbers of false positives and the positive predictive values can vary with a small change in specificity.67 Table 8 shows the range of positive predictive values for MCADD detected by MS/MS-based screening in the Canadian newborn population of 330,803 for 2003-2004, assuming a sensitivity of 100%, an incidence of 1:16000, and specificity varying between 99% and 99.995%. With a specificity of 99.995%, one would expect to find a positive test result in 37 newborns; of which 17 would be false positives (i.e., would not have MCADD). The false positive rate would be about 1:19,500. With a specificity of 99% (a drop of 0.995%), 3,328 newborns would test positive; of which 3,308 cases would be false positives. The false positive rate then would now be 1:100. The positive predictive value drops from 54% to 0.6% with a change of specificity from 99.995% to 99%. Thus, consideration should be given not only to the sensitivity, but also to the specificity of the screening test. The optimal specificity should be determined by the setting of the AC8 cut-off levels to efficiently include all true positives and not too many false positives.

21
Table 8: Prediction of positive predictive values of the MS/MS screening for the Canadian newborn population in 2003-2004
Given 330,803 births in 2003-2004, 100% sensitivity and 99.99% specificity, and incidence=1:16,000
With MCADD Without MCADD Total Positive test (A) 20 (D) 33 (G) 53 Negative test (B) 0 (E) 330,750 (H) 330,750
Total (C) 20 (F) 330,783 (I) 330,803 With 100% sensitivity, but specificity varies between 99.995% and 99.00%
Specificity (%) A D G Positive Predictive Value (%)
99.995 20 17 37 54 99.99 20 33 53 38 99.95 20 165 185 11 99.90 20 331 351 5.7 99.00 20 3,308 3,328 0.6
A=true positive; B=false negative; D=false positive; G=A+D; E=true negative. There is limited evidence on the outcomes of MCADD patients whose conditions were detected at birth by MS/MS, compared to those who were later diagnosed in childhood. From 1995 to 2005, there are four studies comparing the outcomes of patients identified by MS/MS screening and those identified by clinical diagnosis (Table 5),23,25,27,29 and two that solely reported the outcomes of patients found from clinical diagnosis (Table 6).6,30 The rates of detection and incidence for MCADD seem to be higher in MS/MS screening than those in clinical diagnosis (Table 5).23,25,27 Data compiled from studies of MS/MS screening (Table 2) and studies of clinical diagnosis (Table 5) showed no statistically significant difference (Table 7), though the precision remains to be determined. Hoffmann et al.23 showed that all of the cases detected by MS/MS screening were asymptomatic, while 68% of those identified clinically were symptomatic, associated with hypoglycemia, seizures, developmental delay, and death. There was no follow-up process to determine if the asymptomatic cases from MS/MS screening would become symptomatic over time. There is a significant difference in mortality rate between MS/MS screening {2% (95% CI, 1 to 6)] and clinical diagnosis [16% (95% CI, 8 to 26)] (Table 7). Previous published data from Iafolla et al.8 and Touma and Charpentier68 respectively estimated 19% and 25% of MCADD patients died before diagnosis was made. The method of preventive treatment includes avoidance of fasting, and supplementation with glucose and L-carnitine when necessary, though the effectiveness of the treatment has not been empirically verified by published randomized controlled trials. In a follow-up study by Wilson et al.,10 41 patients who were clinically diagnosed and then treated, subsequently had reduced symptoms and adverse effects, implying that the treatment had worked. Most of the cases detected clinically were homozygous for the common A985G mutation, and their symptoms would readily show because of the reduced levels of the MCADD enzyme activity.29 There is no clear correlation between mutation genotype and clinical phenotype.5 Screening detects more compound heterozygotes than clinical diagnosis, and it is unclear why clinical diagnosis detects more homozygotes than newborn screening. One explanation is that only a subset of MCADD patients is detected clinically; many die in early childhood without a diagnosis of MCADD

22
having been made. It is also possible that newborn screening detects all biochemical deficient patients, whereas retrospective clinical diagnosis may detect only those with classical symptoms. MCADD individuals are detected by the raised plasma AC8 level, which is an indication of the impairment of fatty acid metabolism. Environmental factors such as exposure to metabolic stress (starvation or viral infection) and other genetic factors seem to be the most important determinants for affected individuals to become symptomatic. Overall, within the study periods, there were statistically significant differences in the percentages of A985G homozygotes, compound heterozygotes, symptomatic, asymptomatic, and fatal cases among the MCADD cases identified by MS/MS screening compared to those identified by clinical diagnosis (Table 7). 5 ECONOMIC ANALYSIS
5.1 Review of Economic Evaluations 5.1.1 Methods
a) Literature search strategy We cross-searched MEDLINE®, BIOSIS Previews®, PASCAL, and EMBASE® databases on the DIALOG® system from 1995 onwards, using appropriate descriptors and keywords. The search was broadened from the clinical search to include descriptors for “Inborn Errors of Metabolism.” An economic filter was used to restrict results to relevant economic records. We also ran a parallel search on PubMed, CINAHL®, and Cochrane databases. Please refer to Appendix 2 for the literature search strategy. We established regular database alerts on MEDLINE®, BIOSIS Previews®, and EMBASE® databases until March 2005 and updated searches on PubMed, CINAHL®, and Cochrane databases regularly. The last PubMed update was performed in August 2005. A search was run and updated on HEED: Health Economic Evaluations Database using a broad search strategy. We obtained cost information for the economic model by contacting experts and searching the Canadian Institute for Health Information (CIHI) and the Ontario Case Costing Initiative (OCCI) web sites. Grey literature was obtained by searching the web sites of regulatory agencies, and health technology assessment and related agencies. We also searched specialized databases such as the University of York NHS Centre for Reviews and Dissemination and the Latin American and Caribbean Center on Health Sciences Information (LILACS). We used search engines to find web-based information on the Internet.

23
b) Selection criteria Studies containing economic evaluations were included only if they satisfied all the following criteria: • study design: full economic evaluation, such as cost minimization analysis, cost-effectiveness
analysis, cost utility analysis, or cost benefit analysis • population: infants or children with MCADD • intervention: screening by MS/MS • comparator: because MS/MS is technology of choice for MCADD screening and no
alternative method has been used, comparator in this study is “no screening” for MCADD • primary outcome: reported as aggregated estimate of cost-effectiveness or disaggregated
estimate of incremental cost or effectiveness from no intervention to adopting intervention. c) Data extraction strategy Two reviewers (HL and KT) independently screened all abstracts released from the literature search, according to the selection criteria. After comparing results, full-text articles were ordered and the same criteria were applied again to judge their relevance. A study was included for review only if both reviewers answered yes for all criteria. Consensus was required. The same two reviewers independently extracted data using a structured data extraction form (Appendix 10), covering key aspects such as study design, methods, and results. Any disagreement on the content extracted was resolved by discussion. d) Strategy for quality assessment The British Medical Journal (BMJ) 35-item checklist was used to assess the quality of studies included for review. This checklist was initially designed as a guideline for authors and peer reviewers of economic submissions to the BMJ.69 It is a commonly used tool for the quality assessment of economic evaluations. The checklist consists of three parts: study design (seven items), data collection (14 items), analysis and interpretation of results (14 items). For each item, there are four possible answers: “yes,” “no,” “can’t say,” and “not applicable.” Details of the checklist and results of our assessment are listed in Appendix 11. e) Data analysis methods Study characteristics appear in Table 9 and results appear in Table 10. A synopsis of each study’s findings is also presented.

24
Table 9: Study characteristics of included economic studies
Author Intervention Versus
Comparator
Method (Study Design, Perspective,
Time Horizon)
Geographic Location
Data Source
Insinga70 MCADD neonatal screening versus no screening
Model-based study, societal perspective, lifetime analysis horizon
Wisconsin, US Published literature and Wisconsin State Laboratory of Hygiene cost accounting system
Venditti71 MCADD neonatal screening versus no screening
Model-based study, societal perspective, 20 and 70 years analysis horizons
Pennsylvania, Ohio, New Jersey, Illinois, Florida, and North Carolina, US
Wisconsin screening program, Children’s Hospital of Philadelphia, chart review of 32-patient cohort, interview, published reports
5.1.2 Results
a) Literature search The flow chart in Figure 3 demonstrates how studies for review were identified, and either included or excluded. Of 289 abstracts available from the literature search, we ordered full-length articles of 29 studies that met the inclusion criteria. Two articles could not be obtained in their entirety, either because they were unpublished conference posters, or because the author did not respond. Of the 27 we retrieved, two were identified as economic evidence for review. Of the 25 excluded studies, 19 were excluded because of inappropriate study type (e.g., clinical efficacy, health policy analysis, review of clinical and economic evidence), and six because of inappropriate study population (e.g., PKU+CH+MCADD, all IEM). b) Quality assessment As shown in Appendix 11, the qualities of the two reviewed studies were acceptable and similar. In terms of study design in the BMJ checklist, both satisfied all seven items. For data collection, most items were addressed, but both studies failed to report productivity chances, discuss their relevance, and separately state quantities of resources, unit costs, and price data. The details of the models used were not demonstrated sufficiently. These weaknesses compromise the transparency of the two studies and limit the application of their results. For the analysis and interpretation of results, most items were addressed, but not the justification for the choice of rate. Nor were the details of statistical tests and confidence intervals given for stochastic data. Furthermore, the study by Insinga et al.70 did not state the value range of variables used in one-way sensitivity analysis and did not report incremental results. c) Results The study characteristics of the two included studies are listed in Table 9. Both were American, with a societal perspective, and using the primary and secondary data. Their model structures were different. The study by Insinga et al.70 was based on five health consequences: asymptomatic, acute complications only, mild neurological impairment, severe neurological impairment, and death. Venditti et al.71 categorized patients on the basis of their diagnosis, without considering the status of their health. In addition, the type of cost used by Insinga et al.70 does not appear to reflect a societal perspective, as indicated in the study by Venditti et al.71

25
Figure 3: Selection of economic evidence for review
Study results are shown in Table 10, including baseline and sensitivity analysis findings. Insinga et al.70 reported an incremental cost-effectiveness ratio (ICER) of US$41,862 per quality-adjusted life year (QALY), meaning an additional QALY gained by screening would cost the health care system an extra US$41,862 for a cohort of 100,000 babies. Life expectancy was assumed to be 65 years. In the study by Venditti et al.71 the ICER was approximately US$5,600 per QALY over 20 years and US$100 per QALY over a 70-year horizon. It was suggested that the marked decline in the latter is largely due to a reduction of clinical sequelae over the extended 50 years. Both studies undertook a sensitivity analysis to explore the robustness of their model. Insinga et al.70 performed a threshold analysis on four variables: effectiveness of early diagnosis and treatment, incremental cost of MS/MS screening test, screening test sensitivity, and MCADD incidence. The base case results were found to be most sensitive to variations in these parameters. For the $50,000 per QALY threshold to be crossed (i.e., for the ICER of “screening” versus “no screening” to be more than $50,000 per QALY), the study found that the effectiveness of early diagnosis and treatment needs to be <36%; the incremental testing cost to the existing newborn screening program must be >$13.05 per infant; the test sensitivity must be <28%; and incidence of disease must be <1.4:100,000. These values are all beyond their realistic ranges. Hence, alteration of variables within their ranges will not affect the cost-effectiveness of MCADD newborn screening, as indicated in the base case result.
289 citations identified from electronic search and screened
260 citations excluded
29 potentially relevant reports retrieved for further scrutiny
2 relevant reports describing 2 studies
27 reports excluded: inappropriate study design (n=19) inappropriate study population (n=6) no full text papers (n=2)

26
Table 10: Results of included economic studies
Author (country)
Currency Year
Baseline Result Sensitivity Analysis Result Conclusion
Insinga (US)70 US dollars 2001
ICER: $41,862 per QALY (over lifetime horizon)
Base case results most sensitive to variations in screening test costs, sensitivity, underlying MCADD incidence, and effectiveness of early diagnosis and treatment
In Wisconsin, MS/MS screening for MCADD alone seems to be cost effective; future analyses should examine cost- effectiveness of alternative follow-up and treatment regimens for MCADD and other panel disorders
Venditti (US)71 US dollars 2001
ICER: $11,000 per life-year saved (over 20 years horizon); $300 per life-year saved (over 70 years horizon); $5,600 per QALY (over 20 years horizon); $100 per QALY (over 70 years horizon)
Generally, potential threshold ($50,000 per QALY) was not exceeded when model inputs were varied across plausible ranges
Simulation modelling indicates newborn screening for MCADD reduces morbidity and mortality at incremental cost below range for accepted health care interventions; at 70-year horizon, model predicts that almost all additional costs of screening would be offset by avoided sequels
Venditti et al.71did more comprehensive sensitivity analyses, including one-way sensitivity analysis, threshold analysis, two-way sensitivity analysis, and probabilistic sensitivity analysis. With a one-way sensitivity analysis for the 20-year horizon, the base case results were not sensitive and remained <$10,000 per QALY over wide ranges of most variables, including MCADD prevalence, sensitivity, specificity, mortality risks, and discount rate. Next, similar to the study by Insinga et al.,70 the threshold analysis showed that the ICER only exceeded $50,000 per QALY if the utility weight for the screened MCADD was at <0.76, if the asymptomatic rate was >76%, or if the screening test cost was >$14.90. Moreover, two-way sensitivity analysis (prevalence versus cost of screening; sensitivity versus specificity) was also conducted. Over the 70-year horizon, the ICER never exceeded the threshold when MCADD prevalence was between 1:10,000 and 1:20,000 and screening cost per infant was <$20. For the 20-year horizon, the threshold was exceeded when the cost of screening exceeded $11.20 and the prevalence was at 1:20,000. For both time horizons, the ICER was more sensitive with screening cost when the prevalence was at 1:50,000. In addition, the two-way analysis evaluating sensitivity and specificity showed that the ICER for the 20-year horizon reached $50,000 per QALY when sensitivity and specificity of the test decreased to 0.975 and 0.995 respectively. Finally, the probabilistic sensitivity analysis estimated the ICER to be $5,600 (95% CI: <$0 to $17,100) per QALY over the 20-year horizon, and $100 (95% CI: <$0 to $6,900) per QALY over the 70-year horizon, compared with no screening. When expressed as per life-year saved, the ICER was $11,000 (95% CI: <$0 to $33,800) for the 20-year horizon, and $300 (95% CI: <$0 to $13,000) for the 70-year horizon.

27
5.1.3 Discussion
Overall, the two studies reached the same conclusion: MCADD screening by MS/MS seemed to be cost-effective compared to no screening. It was based on the assumption that a health care program should be encouraged if its ICER is below the cost-effectiveness (CE) threshold of US$50,000 per QALY. In the Canadian health care system, Laupacis et al.1 proposed a threshold range with lower and upper boundaries. Adoption of an intervention is strong if the CE ratio is C$20,000/QALY or lower, moderate if it is between C$20,000/QALY and C$100,000/QALY, and weak if it exceeds C$100,000/QALY. A comprehensive review on CE thresholds has been published.2 The difference in the ICER value between the two studies is due to many factors, including the structure of their models, parameter values, analysis horizon, and the jurisdiction where the study occurred. Both studies have strengths and limitations. a) Strengths First, both studies used QALY to measure the effectiveness of health care alternatives. Second, both studies used a lifetime study horizon, which is closer to a real-life situation than a short-term horizon analysis. Third, both studies considered the additional post-screening costs of health care that would be part of the total cost of newborn screening. b) Limitations First, though a societal perspective was indicated in their economic analysis, neither study included the QALY of patients’ family members (e.g., parents) from either a screening or no-screening scenario. The QALY was calculated using secondary sources rather than primary data. The second limitation is the lack of transparency in how data were collected. Neither study reported on resources used or unit costs.
5.2 Primary Economic Analysis Given the limitations in the existing economic evaluations, and the absence of an economic analysis in the Canadian context, a primary economic analysis was warranted. Data from this report’s clinical review and from relevant Canadian sources were used to answer the question: is it cost-effective to screen MCADD by MS/MS in Canada?
5.2.1 Methods
a) Overview A model-based cost-effectiveness analysis that compared the effectiveness and cost between “screening” and “no screening” was performed (Figure 4). Results are reported in the forms of incremental cost, incremental effectiveness, and incremental cost-effectiveness ratio, where applicable.

28
Figure 4: Decision tree: “Screening” and “No Screening”

29
The main features of the economic evaluation are population, intervention, comparator, study perspective, time horizon, health outcomes, resource use, discounting and handling of uncertainty: • Of two similar hypothetical cohorts of newborns in Canada, one undergoes screening and the
other does not. • The value of a screening program depends not only on detecting MCADD cases, but also on
the quality of health care provided after screening to prevent adverse outcomes. Hence, this economic analysis includes follow-up and other necessary health care.
• Three provinces in Canada screen for MCADD using MS/MS technology. Therefore, the comparator chosen in our study is no screening. To ensure comparability between the two, health care costs associated with no screening were also considered.
• Our analysis is based on the direct medical costs borne by the public health care payer. Because of the unavailability of indirect medical costs, a societal analysis was impossible.
• We tried to capture all MCADD-related costs and outcomes over the life of the cohort to reflect the true economic impact of MCADD newborn screening. The specific lifetime is decided by the current Canadian life expectancy.
• Acute episodes from MCADD cases were seen as short-term outcomes, while long-term outcomes included the risk of mild to severe neurological impairment and death, and the chance of being asymptomatic or recovering from an acute episode (Appendix 12).
• From the perspective of the public health care payer, the resources considered in this study are those consumed in the newborn screening stage, the acute clinical episode stage, and the long-term irreversible outcome stage (Appendix 13). We used only direct medical costs in our analysis.
• During the newborn screening stage, resources included screening test, follow-up, post-screening clinical visit, diagnosis, post-diagnosis visit, and routine medical visit.
• During the acute clinical episode stage, resources included transportation of the patient, physician service, diagnostic tests, intensive care unit, and post-intensive care unit hospitalization. All episodes are assumed to have occurred within the first year of life and warranted hospitalization.
• During the long-term irreversible outcome stage, resources included long-term health care for patients with irreversible outcomes (i.e., asymptomatic, acute complications only, mild or severe neurological impairment). Because of time constraints, it was assumed that mild neurological impairment does not incur extra direct medical costs, whereas severe neurological impairment requires routine medical examinations, clinical visits, and special education.
• Both costs and health outcomes are discounted by an annual rate of 3% to reflect that they are worth less in the future. The values of costs and health outcomes that occurs in t years are reduced, as they are multiplied with the factor 1/(1+r)t, where r is the chosen discount rate.
• The handling of uncertainty is done by best and worst scenario analysis, and one-way and two-way sensitivity analyses. The necessary evidence for sensitivity analysis is taken from this report’s clinical review, estimations, published literature, and personal communications with experts.

30
b) Model structure A decision-tree analytical model was constructed, based on what is known about the natural progression of MCADD, the impact of newborn screening on the health care system, and the availability of relevant data (Figure 4). Probable pathways and consequences are shown. For each patient group with different health consequences, the cost and effectiveness are estimated separately. Then, by multiplying them with relevant probability and summing up the results, the total cost and effectiveness for screening versus no screening could be estimated. In the model, there are 16 pathways for screening and six for no screening. The pathways under screening are distinguished from each other by the results (positive or negative), MCADD status (true or false positive), the time of acute episode (early or late) and the long-term health consequences (asymptomatic, acute complications only, mild or severe neurological impairment, death). The pathways under no screening differ from each other only in terms of MCADD status (with or without) and long-term health consequences. The key model parameters and inputs are: • accuracy of screening: sensitivity, specificity, positive predictive value and negative
predictive value (Appendix 14) • health outcome risks under screening and no screening: probabilities of the patient
experiencing an acute episode, recovering from acute episode, having neurological impairment, and dying from episode (Appendix 12).
The economic results are presented in terms of: • expected costs of screening versus no screening • expected effectiveness of screening versus no screening, which is measured by number of
QALY increased, life-years increased, number of cases detected pre-symptomatically, number of hospitalization avoided, number of morbidity and mortality cases reduced
• incremental cost-effectiveness ratio of screening over no screening. c) Parameter values and assumptions The values of parameters and assumptions for the base case scenario are shown in Appendix 14 (see Appendix 12 for the probabilities of different adverse health outcomes). These are point estimates. Clinical data are based on the results of this report’s clinical review, while cost-related data were obtained from the Nova Scotia screening program. A sensitivity analysis was performed to explore the impact of varying key parameter values on the economics of screening. Calculations of the values of some cost-related parameters are detailed in Appendix 13. Those parameters have the same values under screening as under no screening. For example, the health care costs associated with acute clinical episodes presumably stayed the same, regardless of whether MCADD was detected before symptoms appeared. The follow-up protocol for monitoring the health status of MCADD patients was obtained from the Nova Scotia Newborn Screening Service in Halifax (KD, unpublished observations, 2005). The number and duration of visits with health professionals are listed in Appendix 15. The information was used to estimate the costs for post-screening clinical visits, post-diagnosis clinical visits, and lifetime routine clinical visits. Life-time costs per case were attributed to

31
different health consequences, as shown in the decision tree model and listed in Appendix 16. d) Sensitivity analysis To test the robustness of the base-case findings, best and worst scenarios were determined, and one-way and two-way sensitivity analyses were performed (Appendix 17): Best scenario • The incidence of MCADD is as high as 1:14,286 (clinical review, Table 2) and positive
predictive value correspondingly rises to 41% (estimated, formula shown in footnotes of Appendix 14).
• The probability of being asymptomatic is 98% for screening and 14% for no screening (clinical review, Table 7).
• The probability of death associated with MCADD is 1% for screening and 26% for no screening (clinical review, Table 7).
• The probability of cases with acute complication is justified to 1% for screening and 50% for no screening.
Worst scenario (data sources are the same as those for best scenario) The following parameters had their values in favour of no screening: • The incidence of MCADD is as low as 1:20,000, and the positive predictive value
correspondingly is 33%. • The probability of being asymptomatic is 92% for screening, and 35% for no screening. • The probability of death associated with MCADD is 6% for screening, and 8% for no
screening. • The probability of cases with acute complication only is justified to 2% for screening and
47.5% for no screening. One-way sensitivity analysis One-way sensitivity analysis is performed by varying the value of the following six parameters to demonstrate the impact of their variation, within plausible ranges, on base-case findings (data references are shown in Appendix 14): • specificity of screening for MCADD, from 99.95% to 99.995% • MCADD incidence (among newborns), from 1:20,000 to 1:14,286 • screening cost, from C$0.50 to C$5.60 per case • cost associated with routine health care monitoring (management cost), from $1,500 to
$4,000 per MCADD case. • cost associated with acute episode, from $10,000 to $20,000 per case per episode • direct medical cost associated with severe neurological impairment, from $100,000 to
$250,000 per case over a life-time
Two-way sensitivity analysis This test explores how the cost-effectiveness of screening is affected by varying two parameters simultaneously. According to the findings in one-way sensitivity analysis, selected parameters had a marked impact on the ICER. The two pairs of parameters chosen are: • screening cost and specificity • screening cost and cost associated with an acute episode.

32
5.2.2 Results
a) Base case From the perspective of public health care payer, the results under a baseline scenario were expressed as the expected costs of screening and no screening, the expected effectiveness of screening and no screening, and the incremental cost-effectiveness ratio of screening over no screening (Table 11). Expected costs Under the screening scenario, the total cost was $934,922.97 for one cohort of 330,803 newborns over a 77-year horizon. The major cost was the cost of screening (84.92%). Other costs were for following up patients who tested positive for MCADD but who were asymptomatic (5.35%); following up babies who had false-positive screening results (5.36%); providing care for patients with acute episodes (3.09%); and providing long-term care for patients with severe neurological impairment (1.27%). Under the no-screening scenario, the total cost was $450,520.55 for one cohort (same population as above) over a 77-year horizon. The costs were for providing care for patients with acute episodes (56.52%), and providing long-term care for patients with severe neurological impairment (43.48%). Expected effectiveness Given a hypothetical cohort of 330,803 newborns in Canada and other assumptions, the number of MCADD cases is approximately 20. Under a screening scenario, 18.48 cases were detected pre-symptomatically. Early detection reduces adverse health outcomes with the result that the number of acute episodes was estimated to be 1.75; morbidity due to MCADD was 0.12 (0.06 for mild neurological impairment, 0.06 for severe neurological impairment); and death due to MCADD was 0.64. In terms of QALY, screening results in 21,932,152.77 for the cohort or 66.30 per case. Under a no-screening scenario, there were 15.28 acute episodes, 2.00 morbidities, and 3.18 mortalities due to MCADD. The QALY was 21,931,971.53 for the cohort or 66.30 per case. Incremental results The incremental results represent the difference in the cost of resources consumed, and the difference in health outcomes of the hypothetical cohort when there is screening and when there is no screening (Table 11).

33
Table 11: Estimated costs and health outcomes under base case scenario
Screening No Screening Resource Unit Cost (C$) Utilization Total cost
(C$) Utilization Total cost
(C$)
Incremental Results
Screening 2.40 330,803.00 793,927.20 0 0 793,927.20 Follow-up • type A* 2,764.00 18.10 50,028.40 0 0 50,028.40 • type B† 35.00 0.26 9.10 0 0 9.10 • type C‡ 795 0.38 302.10 0 0 302.10 • type D** 1,515.00 33.08 50,116.20 0 0 50,116.20
Acute episode 16,450.00 1.75 28,787.50 15.48 254,646.00 −225,858.50 Long-term care for severe neurological impairment
195,874.55 0.06 11,752.47 1.00 195,874.55 −184,122.08
Others (for investigation of death)
1,000.00 0 0 3.18 3,180.00 −3,180.00
Total 934,922.97 450,520.55 484,402.42 Health outcome Healthy babies 330,783 330,783 0 MCADD cases 20 20 0 Total life years 25,471,781.36 25,471,574.36 207.00 Average life year per case
77.00 77.00
QALY 21,932,152.77 21,931,971.53 181.24 QALY per case 66.30 66.30 Cases detected pre-symptomatically
18.48 0 18.48
Hospitalization 1.75 15.28 −13.73 Morbidity 0.12 2 −1.88 • mild
neurological impairment
0.06
1 −0.94
• severe neurological impairment
0.06
1 −0.94
Death 0.64 3.18 −2.54 * including cost of follow-up, post-screening visit, diagnosis, post-diagnosis visit, and routine health care for monitoring health status of cases with MCADD; used for patients whose MCADD is asymptomatic but detected (In our model, it includes patients at ending nodes 1, 2, 3, 5 to 8) † including cost of follow-up, used for patients who die from an early acute episode and their conditions are subsequently reported; in our model, it includes patients at ending node 4 ‡ including all costs in type A but excluding routine health care for monitoring cases; used for patients who die from acute episode due to MCADD, but their conditions were detected, in the model, refers to the patient group at ending node 9 ** including cost for following up, post-screening visit and diagnosis, used for patients whose screening results are false positive, in the model, refers to patient group at ending node 10.

34
In terms of resources consumed, the incremental results were positive for the cost of screening and the cost of follow-up, which were absent in the no-screening group. Conversely, they were negative for the cost associated with an acute episode, the cost associated with long-term care for severe neurological impairment, and the cost for investigation of death. Screening consumed more resources for screening and follow-up, but less resources in treating adverse events resulting from clinical events. The total amount of resources consumed in screening was two times that of no screening. In terms of health outcomes gained, the incremental results for total life-years (207.00) and QALY (181.24) were positive, while those associated with morbidity and mortality were negative. This indicates that screening achieves better health outcomes than no screening. Overall, screening consumed more resources, but resulted in better health outcomes than no screening. In terms of incremental cost per QALY gained, the base case ICER was $2,514.02, which is below the threshold of C$20,000 proposed by Laupacis et al.1 and suggests that the intervention is cost-effective. The ICERs expressed under different health outcomes are listed in Table 13. b) Sensitivity analysis Best and worst scenarios Both best and worst scenarios showed that screening consumed more resources than no screening, but with the advantage of better health outcomes (Table 12). In terms of incremental cost, it was $389,117.88 in the best scenario and $596,075.26 in the worst for cost of screening over no screening. For an incremental QALY of screening over no screening, it was 378.46 in the best scenario and 52.33 in the worst. The ICERs, if expressed as incremental cost per QALY gained, were $928.11 and $11,456.10 for best and worst scenarios respectively. Both are below the C$20,000 threshold, indicating that screening is cost-effective in both scenarios. The ICERs expressed under different health outcomes are listed in Table 13. One-way sensitivity analysis After sequentially varying the values of the six parameters outlined earlier, the ICER for each case was calculated and expressed as incremental cost per QALY gained by screening over no screening. The ICER had different degrees of sensitivity depending on the parameters tested (Table 14). For instance, the ICER is more sensitive to changes in screening cost and specificity than of other parameters. With the screening cost ranging from $0.50 to $5.60, the ICER values were from dominant (<0) to 6,963.40. Increasing the specificity of the screening test from 99.95% to 99.995% decreased the ICER values from $3,094.66 to $2077.96. The ICER decreased with increased specificity, incidence rate, cost associated with acute episode, and cost associated with severe neurological impairment. Conversely, the ICER increased with increased screening cost and management cost. Within the plausible ranges of the parameters that we tested, all ICER values were below the C$20,000 threshold.

35
Table 12: Estimated cost and health outcome results under best and worst scenarios
Best Scenario Worst Scenario Screening No Screening Incremental
Results Screening No Screening Incremental
Results Resource (C$) Screening stage 793,927.20 793,927.20 793,927.20 793,927.20 Follow-up 109,893.44 109,893.4 90,840.85 90,840.85 Acute episode 26,320.00 327,519.50 −301,199.50 34,216.00 176,837.50 −142,621.50 Long-term care for severe neurological impairment
13,711.22 227,214.48 −213,503.26 9,989.60 154,740.89 −144,751.29
Others 6,020.00 −6,020.00 1,320.00 −1,320.00 Total 94,3851.86 55,473.98 389,117.88 928,973.65 332,898.39 596,075.26 Health outcome Healthy babies 330,780 330,780 330,786 330,786 MCADD cases 23 23 17 17 Total life-years 25,471,790.02 25,471,353.52 436.50 25,471,741.23 25,471,719.686 21.55 Average life-year per case 77 77.00 0 77.00 77.00 0 QALY 21,932,153.00 21,931,774.54 378.46 21,932,159.26 21,932,106.931 52.33 QALY per case 66.30 66.30 0 66 66.30 0 Cases detected pre-symptomatically
21.78 0 21.78 14.77 0 14.77
Hospitalization 1.60 19.91 −18.31 2.08 10.75 −8.67 Morbidity 0.14 2.32 −2.18 0.1 1.58 −1.48 • mild neurological impairment 0.07 1.16 −1.09 0.05 0.79 −0.74 • severe neurological impairment 0.07 1.16 −1.09 0.05 0.79 −0.74
Death 0.52 6.02 −5.50 1.16 1.32 −0.16

36
Table 13: ICER in three scenarios
ICER (C$ per Effectiveness) Effectiveness Base Best Worst
Life-year gained 2,201.09 804.69 27,821.43 QALY gained 2,514.02 928.11 11,456.10 Case detected pre-symptomatically 24,654.44 16,127.30 40,590.55 Hospitalization due to acute episode avoided 33,183.83 19,183.65 69,149.08 Morbidity avoided 242,347.89 161,125.09 40,5082.76 Mild neurological impairment avoided 480,733.16 323,315.28 816,058.01 Severe neurological impairment avoided 480,733.16 323,315.28 816,058.01 Death avoided 179,337.25 63,669.03 3,625,461.73
Two-way sensitivity analysis The ICER was estimated as a function of specificity and cost of screening (Table 15). At a screening cost of $0.50, the ICER showed that screening was dominant (<0) when specificity was between 99.9635% and 99.995%. The remaining ICER values were positive, ranging from $5 to $7,873 per QALY. The second results of the two-way sensitivity analysis are shown in Table 16, where the ICER was estimated as a function of cost associated with acute episode and cost of screening. At a screening cost of $0.50, the ICER showed that screening was dominant (<0) with respect to all the values of cost associated with an acute episode within the tested range. When the screening cost was at $1.01, screening dominated no screening with a range of cost associated with an acute episode of $19,000 to $20,000. The remaining ICER values were positive, ranging from $23 to $7,363 per QALY. The results of two-way sensitivity analyses showed that screening for MCADD consumes more resources (in most cases), but obtains higher QALY compared with no screening. When the ICER was estimated as a function of specificity and screening cost, it ranged from −$756 to $7,875 per QALY. When ICER was estimated as a function of cost associated with acute episode and screening cost, it ranged from −$860 to $7,363 per QALY. Thus, screening remains cost-effective under a two-way sensitivity analysis. c) Summary of results In base case and sensitivity analyses, the screening for MCADD results in a higher consumption of resources compared with no screening. In terms of health outcomes, screening results in more life-years and QALY, and lower morbidity and mortality compared with no screening. All ICER values, expressed as an incremental cost per QALY gained, are below the Laupacis CE threshold of C$20,000.

37
Table 14: One-way sensitivity analysis
Parameters ICER* Parameters ICER* Specificity Incidence 0.9995 3,094.66 1:20,000 2,951.99 0.999545 2,992.99 1:19,231 2,776.36 0.99959 2,891.32 1:18,519 2,613.74 0.999635 2,789.65 1:17,857 2,462.73 0.99968 2,687.98 1:17,241 2,322.14 0.999725 2,586.31 1:16,667 2,190.93 0.99977 2,484.64 1:16,129 2,068.17 0.999815 2,382.97 1:15,625 1,953.09 0.99986 2,281.30 1:15,152 1,844.99 0.999905 2,179.63 1:14,706 1,743.24 0.99995 2,077.96 1:14.286 1,647.31 Screening cost (C$) Management cost (C$) 0.5 (Dominated) 1,500 2,150.30 1.01 117.88 1,750 2,171.96 1.52 878.50 2,000 2,193.61 2.03 1,639.11 2,250 2,215.27 2.54 2,399.72 2,500 2,236.92 3.05 3,160.33 2,750 2,258.58 3.56 3,920.95 3,000 2,280.23 4.07 4,681.56 3,250 2,301.89 4.58 5,442.17 3,500 2,323.54 5.09 6,202.78 3,750 2,345.20 5.6 6,963.40 4,000 2,366.85 Cost associated with acute episode (C$)
Cost associated with severe neurological impairment (C$)
10,000 2,584.56 100,000 2,600.59 11,000 2,523.53 115,000 2,536.49 12,000 2,462.50 130,000 2,472.40 13,000 2,401.47 145,000 2,408.31 14,000 2,340.44 160,000 2,344.21 15,000 2,279.42 175,000 2,280.12 16,000 2,218.39 190,000 2,216.03 17,000 2,157.36 205,000 2,151.94 18,000 2,096.33 220,000 2,087.84 19,000 2,035.30 235,000 2,023.75 20,000 1,974.28 250,000 1,959.66
* ICER=incremental cost-effectiveness ratio where effectiveness was measured as QALY.

38
Table 15: Two-way sensitivity analysis – screening cost versus specificity
ICER* Screening Cost (C$)
Specificity
0.5 1.01 1.52 2.03 2.54 3.05 3.56 4.07 4.58 5.09 5.60 0.9995 261 1,022 1,784 2,545 3,306 4,067 4,828 5,590 6,351 7,112 7,873 0.999545 159 921 1,682 2,443 3,204 3,965 4,727 5,488 6,249 7,010 7,771 0.99959 58 819 1,580 2,341 3,102 3,864 4,625 5,386 6,147 6,908 7,670 0.999635 −44 717 1,478 2,240 3,001 3,762 4,523 5,284 6,046 6,807 7,568 0.99968 −146 615 1,377 2,138 2,899 3,660 4,421 5,183 5,944 6,705 7,466 0.999725 −248 514 1,275 2,036 2,797 3,558 4,320 5,081 5,842 6,603 7,364 0.99977 −349 412 1,173 1,934 2,695 3,457 4,218 4,979 5,740 6,501 7,263 0.999815 −451 310 1,071 1,833 2,594 3,355 4,116 4,877 5,639 6,400 7,161 0.99986 −553 208 970 1,731 2,492 3,253 4,014 4,776 5,537 6,298 7,059 0.999905 −655 107 868 1,629 2,390 3,151 3,913 4,674 5,435 6,196 6,957 0.99995 −756 5 766 1,527 2,289 3,050 3,811 4,572 5,333 6,094 6,856
Table 16: Two-way sensitivity analysis – screening cost versus cost
associated with acute episode (C_acute)
ICER* Screening Cost (C$)
C_acute
0.5 1.01 1.52 2.03 2.54 3.05 3.56 4.07 4.58 5.09 5.60 10,000 −249 512 1,273 2,034 2,795 3,557 4,318 5,079 5,840 6,601 7,363 11,000 −310 451 1,212 1,973 2,734 3,496 4,257 5,018 5,779 6,540 7,302 12,000 −371 390 1,151 1,912 2,673 3,435 4,196 4,957 5,718 6,479 7,241 13,000 −433 329 1,090 1,851 2,612 3,373 4,135 4,896 5,657 6,418 7,179 14,000 −494 268 1,029 1,790 2,551 3,312 4,074 4,835 5,596 6,357 7,118 15,000 −555 207 968 1,729 2,490 3,251 4,013 4,774 5,535 6,296 7,057 16,000 −616 145 907 1,668 2,429 3,190 3,951 4,713 5,474 6,235 6,996 17,000 −677 84 846 1,607 2,368 3,129 3,890 4,652 5,413 6,174 6,935 18,000 −738 23 785 1,546 2,307 3,068 3,829 4,590 5,352 6,113 6,874 19,000 −799 -38 723 1,485 2,246 3,007 3,768 4,529 5,291 6,052 6,813 20,000 −860 -99 662 1,424 2,185 2,946 3,707 4,468 5,230 5,991 6,752
* ICER = incremental cost-effectiveness ratio where effectiveness was measured as QALY.
5.2.3 Discussion
The economic implication of newborn screening for MCADD in Canada was evaluated by performing a cost-effectiveness analysis using a decision-tree analytical model. From the perspective of a public health care payer, the resources used and the health outcomes associated with screening and without screening were estimated and compared. The analysis horizon was a cohort-based lifetime. Evidence on the effectiveness of screening was based on the results of this report’s clinical review, published literature, and personal communications. Uncertainty was tested by best and worst scenario analyses, and one-way and two-way sensitivity analyses.

39
In the base case scenario, the cost-effectiveness of screening is sensitive to six parameters: specificity of MS/MS in the screening of MCADD, incidence of MCADD, screening cost, cost associated with an acute episode due to MCADD, cost associated with long-term health care for severe neurological impairment, and cost of routine health care for MCADD patients. The values of these parameters could be influenced by multiple factors. For instance, the specificity of MS/MS could be affected by the cut-off value of detected metabolites, the level of experience of the technologist, or the time of blood sample collection. The range of specificity in this study was obtained from the results of this report’s clinical review, so that some external validity is ensured. In the absence of epidemiological data for Canada, this report’s clinical review provided the estimated range of incidence for the economic analysis undertaken. Though its mean value may not accurately reflect the number in Canada, it covers both extreme values. With Canada’s multicultural population, the incidence of MCADD is assumed to fall within the tested range, which was shown in the one-way sensitivity analysis. The cost of MS/MS-based screening in this study is for MCADD alone. If the screening is used to detect multiple IEM simultaneously, then it is expected that the cost would be shared by the additional disorders. In this study, the screening cost per case was set at C$2.40 under the base case scenario where the estimated ICER was C$2514.02. Even if the screening cost rose to C$5.60 per case, the ICER values still remained below C$10,000, which is lower than the threshold of C$20,000. The range of screening costs tested in our study needs to be verified and adjusted for each province. We estimated the cost associated with severe neurological impairment in this study, by basing it on the results of a US study.72 The US study examined the costs associated with developmental delay, cerebral palsy, hearing loss, and vision impairment. Although these are the best available data, the Canadian situation may not be reflected because of differences in health care systems (Canadian versus US) and of measurements (severe neurological impairment versus developmental delay). Because screening for MCADD had been implemented in only three Canadian provinces as of April 2005, there is no agreed-upon screening protocol or guidelines. For this study, the costs associated with the screening procedure were based on the protocol obtained from the Nova Scotia screening program. Given the health care payer’s perspective in Canada, the costs should fall within an acceptable range for all jurisdictions, though adjustments may be required, because of the different provincial health care systems. In the base-case analysis, the ICER of this study (C$2,514.02 per QALY) is lower than that of the study by Insinga et al.70 (US$41,862, approximately C$58,607 per QALY). This is probably due to the differences in some key parameter values, such as MS/MS sensitivity (90% in the Insinga et al.’s study; and 100% in this study) and specificity (99.9% in Insinga et al.’s study; and 99.99% in this study), effectiveness of screening to reduce adverse outcomes (in the study of Insinga, 60% mortality was reduced because of screening; in this study, it was approximated to

40
be 80%), cost of screening (US$3.99 per sample estimated in the study of Insinga et al.; C$2.40 per sample in this study) and QALY weight assigned to severe neurological impairment status (0.06 in the study of Insinga et al.; 0.38 in this study). Comparing this study with that of Venditti et al.,71 is also inappropriate because of the principal differences in the model structures, data sources and health care systems. The largest discrepancy between this study and that of Venditti et al. is that the QALY weight assigned in the latter was based on the detection or diagnosis of MCADD, while in this study, it was based on the long-term health outcome of MCADD patients. Compared to the two reviewed studies, this study is likely to better reflect the economic implications of screening for MCADD in the Canadian context, but several potential limitations are noteworthy. Some uncertainty may still exist for the tested parameters, although we analyzed the extremes (best and worst scenarios). Most data were obtained from a provincial laboratory of Nova Scotia and these may vary between provinces. Direct evidence for the long-term health outcomes of MCADD patients is unavailable. As with the study by Insinga et al.70 this study estimates the QALY based on the values in three US studies,73-75 none of which had MCADD patients. They measured quality of life of healthy populations, low-birth-weight infants, and patients with Alzheimer’s disease respectively. Another potential limitation to this study is the economic model used. Although it provides a picture of the impact of a screening program on the health care system and shows the impact of certain factors on the screening program, it was built on the basis of assumptions that need more supporting evidence. In particular, the model did not consider the repetition of acute episodes, the cost difference of acute episodes occurring at different times, and changing health outcomes. Another issue is the practical aspect of having MS/MS-based screening to detect other IEM, particularly PKU, once the system is set up for MCADD. This study does not examine how the economic implication of MCADD screening would change in this scenario. More study is warranted to determine how the MS/MS-based screening of multiple IEM would affect capital costs, resource consumption, and health consequences. Despite different objectives, three recent HTA reports76-78 unanimously found that PKU fulfilled all the screening criteria and agreed on the expansion of the UK newborn screening programs to include MCADD. The report of Seymour et al.76 suggested that glutaric aciduria type 1 (GA1, incidence 1:40,000) and MCADD (incidence 1:8000 to 1:15,000) be added to the screening program, where MS/MS technology can be used to screen for these diseases including PKU. The report suggested that a further study with more than one million infants is needed to validate the utility of this technology in the screening of these diseases. The report of Pollitt et al.77 reviewed newborn screening in the UK, and analyzed the costs and benefits of introducing MS/MS into the screening program. It was found that screening for PKU and hypothyroidism has met the criteria and is cost-effective; parents support the process despite the anxiety generated from screening; and MS/MS technology can be introduced into the screening program, but should be limited to defined diseases for which there are satisfactory confirmatory tests. The report of Pandor et al.78 evaluated the clinical and cost-effectiveness of MS/MS-based screening for IEMs in UK. Of

41
many IEMs, the report determined that MCADD can be readily detected by MS/MS. Robust clinical evidence was limited for many IEMs that can be detected by MS/MS. Economic modelling suggests that using MS/MS to screen PKU and MCADD is economically attractive. 6 HEALTH SERVICES IMPACT 6.1 Population Impact Epidemiological data for MCADD in Canada are unavailable. It is possible to estimate the prevalence of the disorder in Canada, knowing that in different populations of northern Europe and in the US, it varies between 1:9,000 and 1:30,000. Given that Canada has a multicultural population, the estimated prevalence for MCADD would be 1:16,000. If all provinces and territories participate in screening for MCADD, approximately 330,000 babies born each year would be screened. Among these, about 20 cases would have MCADD. With the sensitivity and specificity of MS/MS being 100% and 99.99% respectively, the technology would detect 53 positive cases, of which 33 would be false positives. Currently, MS/MS is the favoured technology for the screening of MCADD. Other technologies are more difficult to automate and are no less expensive (Dr. Denis Lehotay, University of Saskatchewan, Saskatoon: personal communication, 2005 Jan 26). The number of births and estimated MCADD cases for the 2003-2004 newborn populations of provinces and territories are listed in Table 17.
Table 17: Number of births and estimated MCADD cases among Canadian provinces and territories in 2003-2004
Population Birth Rate per 1,000
Population Number of
Births Estimated
MCADD Cases* Canada 31,807,981 10.4 330,803 20.68 Newfoundland and Labrador
517,386 8.8 4,553 0.28
Prince Edward Island 138,021 9.6 1,325 0.08 Nova Scotia 937,692 9.1 8,533 0.53 New Brunswick 752,935 9.2 6,927 0.43 Quebec 7,524,343 9.9 74,491 4.66 Ontario 12,351,442 10.4 128,455 8.03 Manitoba 1,161,333 12.0 13,936 0.87 Saskatchewan 996,102 11.8 11,754 0.73 Alberta 3,174,146 12.3 39,042 2.44 British Columbia 4,170,729 9.6 40,039 2.50 Yukon 30,870 11.5 355 0.02 Northwest Territories 42,400 15.0 636 0.04 Nunavut 29,341 25.8 757 0.05
Source: Statistics Canada16 *Assuming an incidence of 1:16,000.

42
6.2 Budget Impact A budget impact analysis differs from the earlier primary economic study in that its purpose is to discuss the affordability of introducing one intervention to the health care system. On the basis of a primary economic study, whether an intervention is cost-effective and whether it is worth implementing can be determined yet its potential budget impact would remain unclear. So, a simple budget impact analysis was conducted with limited data to provide a basic idea about how much MCADD screening by MS/MS will eventually cost the health care system.
6.2.1 Assumptions
The impact of MCADD screening with MS/MS on health care budgets was predicted using limited data, mostly from the Nova Scotia program. The prediction was based on the assumptions (listed in Appendix 18). • The study perspective was that of a public health care payer. • The analysis horizon was five years. • The study population included Nova Scotia newborns (n=8,533) during five years. • The MS/MS screening sensitivity and specificity were the same as those in the base case
scenario of our primary economic analysis. • The health outcomes of the cohort were estimated in a similar fashion as in our primary
economic analysis. The values of the relevant parameters used are the same as those in the base case scenario.
• MS/MS acquisition and set-up costs are allocated to the first year of setting up the MCADD screening program.
• The additional fixed costs for MS/MS included associated personnel salaries and the annual maintenance fee. The additional costs of insurance for equipment and capital costs for facility space were not considered.
• The additional variable costs for MS/MS refer to the isotopic labelling material expenditure and the cost saving of PKU screening.
• The economic burden due to severe neurological impairment is considered yearly. • Follow-up, post-screen consulting and confirmation tests are applicable in all cases with
positive screening results. • Post-confirmation-test consulting and routine health care are applicable in all true cases of
MCADD.
6.2.2 Methods
The budget analysis was performed in the following steps: • This report’s economic model was used to examine the use of resources. • A model for budget impact analysis was built using Microsoft Excel software, where the
predicted resource utilization was input, and cost was calculated and grouped into two categories: health care and MS/MS-related expenditures. Health care costs include screening tests, follow-up, post-screening consulting, routine monitoring of detected cases, care provided to patients with acute episodes and severe neurological impairment, and investigation of death. The MS/MS-related expenditure consists of acquisition cost, yearly

43
fixed cost (i.e., personnel salary, maintenance cost) and yearly variable cost (i.e., isotopic labelling material and cost saving per case in PKU screening).
• Health care costs and MS/MS-related costs for five newborn cohorts over a five-year horizon, according to the applicable year, were estimated separately.
• Corresponding costs incurred by cohort(s) of a particular year within the five-year period were summed and tabulated for the values of screening and no screening and their differences.
• Both three-year and five-year budget impacts were determined.
6.2.3 Results
Details and a summary of results are shown in Tables 18 and 19. The values are in Canadian dollars. • With screening, the predicted yearly budget is $220,419 for the first year, and $25,335,
$24,684, $24,050, and $23,432 for subsequent years. • With no screening, the predicted yearly budget due to MCADD is about $25,506 for the first
year and $24,925, $24,356, $23,799, and $23,254 for subsequent years. • The differences between screening and no screening for years 1 to 5 yield $194,913, $410,
$328, $251, and $178. For a five-year horizon, a budget of $317,921 is predicted for screening, and $121,841 for no screening. The budget difference is $196,080.
6.2.4 Discussion
With the screening scenario, a considerable proportion (90.74%) of the first-year budget is spent on acquiring MS/MS equipment (Appendix 18). This explains the bigger budget. The cost of screening in the following years declines, and costs are largely associated with MS/MS-related expenditure. The average lifetime of the machine (10 years) should be considered in short-term budgets. For those provinces that have MS/MS in place for other purposes, the technology could be extended for the use of MCADD screening with a significant reduction in costs. With the no-screening scenario, the budget is mainly spent on providing health care for acute episodes and severe neurological impairment. It remains relatively stable over the years, largely because the cost of health care for acute episodes is assumed to be similar for each newborn cohort. With screening, these costs could be prevented. The budget difference between screening and no screening is relatively unchanged for both three- and five-year horizons, because the main expenditures occur within the first year of the budget. One limitation of this budget analysis is that the values of key parameters were not verified by formal survey, because it was beyond the scope of this report. For instance, the cost of a more sophisticated MS/MS machine (the API 4000™ LC/MS/MS) is higher than the $200,000 used for the API 2000™ LC/MS/MS model in the current budget analysis. Conversely, the price of the predecessor may also be depreciated with the evolving technology. Thus, attention should be given to the type of equipment used in the budget analysis, because it has an impact on the budget. Attention should also be given to the requirement of having a back-up or partner machine in another jurisdiction in case the principal one breaks down. The operational cost, including salary, is the second most important cost worth mentioning. In the current analysis,

44
data obtained from the Nova Scotia screening program might be inapplicable to other jurisdictions, given the possible differences in salaries and proportion of time that staff spends on screening for MCADD. The degree of cost saving with PKU screening by MS/MS depends on the technology used. Some could be expensive while others are not.
Table 18: Estimation of cost of screening and no screening for each cohort* during five-year period (C$)
Year 1 2 3 4 5
Cohort 1 Screening
Health care cost 2,547.89 170.50 87.53 84.98 82.51 MS/MS related cost 217,871.20 Total 220,419.10 170.50 87.53 84.98 82.51
No screening Health care cost 25,506.15 161.78 157.07 152.49 148.05
Cohort 2 Screening
Health care cost 2,473.69 165.53 84.98 82.51 MS/MS related cost 22,690.45 Total 25,164.13 165.53 84.98 82.51
No screening Health care cost 24,763.26 157.07 152.50 148.05
Cohort 3 Screening
Health care cost 2,401.64 160.71 82.51 MS/MS related cost 22,029.56 Total 24,431.20 160.71 82.51
No screening Health care cost 24,042.00 152.50 148.05
Cohort 4 Screening
Health care cost 2,331.69 156.03 MS/MS related cost 21,387.92 Total 23,719.61 156.03
No screening Health care cost 23,341.74 148.05
Cohort 5 Screening
Health care cost 2,263.77 MS/MS related cost 20,764.97 Total 23,028.75
No screening Health care cost 22,661.89
*a cohort of 8,533 newborns and assumed to be unchanged for each year; discounting rate:3%.

45
Table 19: Budget impact analysis results* (C$)
Screening No Screening Difference Year 1 220,419.10 25,506.15 194,912.90 Year 2 25,334.63 24,925.04 409.59 Year 3 24,684.26 24,356.13 328.12 Year 4 24,050.28 23,799.23 251.05 Year 5 23,432.29 23,254.10 178.19 3-year budget 270,437.90 74,787.32 195,650.60 5-year budget 317,920.50 121,840.60 196,079.90
*a cohort of 8,533 newborns and assumed to be unchanged for each year.
Limitations that are due to our assumptions about disease prognosis and parameter values from our economic analysis might be carried over and limit our budget analysis. Other limitations include the lack of sensitivity analysis, the complete allocation of acquisition cost to the first year budget, and the potential irrelevance of the current budget in terms of cost-saving. A careful interpretation should be done for the differences in QALY between screening and no screening of a small cohort over a short period.
6.3 Planning, Implementation, and Legal or Regulatory Issues
In terms of planning issues, there is no impact on waiting lists and little impact on individual family physicians. As with other IEM, adding MCADD into the current screening program would require follow-up, which involves the services of metabolic geneticists, metabolic laboratories, genetic counsellors, dietitians, and a specialized metabolic clinic. Most jurisdictions have such an infrastructure in place or available. The cost analysis shows a shift away from intensive care and emergency medicine to genetics and therapeutic nutrition and drug costs (carnitine), because patients who would have had severe symptoms or would have died are surviving. Screening for MCADD has no impact on other newborn screening. For instance, specimen collection, timing, and reporting constraints are less than or equal to those for existing newborn screening tests. Adding a screening program for MCADD is not required under the Canada Health Act or by human rights laws. As MCADD screening becomes the standard of care in the US or in certain provinces, liability issues could be generated for provinces that do not offer it.

46
7 ETHICAL AND PSYCHOSOCIAL ISSUES
7.1 Methods 7.1.1 Literature search strategy
We cross-searched MEDLINE®, BIOSIS Previews®, PASCAL, Social ScienceSearch®, PSYCInfo®, ERIC, and EMBASE® databases on the DIALOG® system from 1995 onwards, using appropriate descriptors and keywords. The search was broadened from the clinical search to include descriptors for “inborn errors of metabolism” (IEM). Using appropriate descriptors and keywords, we restricted results to the psychosocial and ethical aspects of newborn screening (Appendix 3). We ran parallel searches on PubMed, CINAHL®, and Cochrane databases. Regular database alerts were established on MEDLINE®, BIOSIS Previews®, and EMBASE® databases until March 2005. Searches on PubMed, CINAHL®, and Cochrane databases were updated at regularly. The last PubMed update was performed in August 2005. We obtained grey literature by searching the web sites of regulatory agencies, and health technology assessment and related agencies. Specialized databases such as the University of York NHS Centre for Reviews and Dissemination, and the Latin American and Caribbean Center on Health Sciences Information (LILACS) were also searched. The Internet was searched using search engines for web-based information.
7.1.2 Inclusion and exclusion criteria
Inclusion criteria specified studies that addressed the ethical and psychosocial issues pertaining to screening newborns using MS/MS. Given the likelihood of finding a few studies, we did not restrict our search to MCADD alone, but were open to relevant studies on all IEM. The approach taken was to restrict the analysis to published references, and limit the analysis to concepts and issues based on the results of the literature search. Ethical and psychosocial issues require a “big picture” approach, which includes the involvement of stakeholders, including discussions with the respective newborn screening advisory committees in the Canadian jurisdictions. The latter was not undertaken in this report, because of time and scope constraints.
7.1.3 Data extraction strategy
Two reviewers (HN and KT) reviewed the reports that were identified during the searches for relevance on the basis of title (and abstract where available). If relevant, or in the case of doubt, full-text articles were obtained and reviewed according to the selection criteria. They also scanned the reference lists of relevant reports for further documents. Differences were resolved by consensus. The same reviewers independently extracted data (Appendix 19) using a structured data extraction form covering aspects such as study characteristics, family characteristics, and outcome measures. Any disagreement on the content was resolved by discussion.

47
7.2 Results and Discussion 7.2.1 Quality of research available
During the literature search strategy, we found 504 citations, with 68 potential reports identified for further scrutiny. This resulted in 27 relevant reports, of which 21 were excluded (reviews, primary studies on ethical or psychosocial aspects of other genetic conditions), leaving six primary articles that were used for the analysis of ethical and psychosocial issues (Figure 5).
7.2.2 Trial characteristics
We selected six articles reporting on three primary studies.10,24,79-82 The study by Waisbren et al. on the New England Consortium of Metabolic Programs was reported in three articles,24,79,80 with the most comprehensive report on outcomes in children and parental stress published in 2003.79 Liebl et al. presented the results of the expanded newborn screening program in Bavaria in two reports: one on informed consent issues,81 and the other on the quality assurance procedure to track recalls for testing.82 The study by Wilson et al., which was undertaken in the UK, primarily reported on the outcomes among MCADD patients after the diagnosis had been established, and included a discussion about the psychosocial impact on affected families.10 The three primary studies reported limited data on the ethical or psychosocial impact of MS/MS screening. The study by Wilson et al. 10 reported on MCADD, while the other two studies reported on multiple conditions.79,81 The study by Waisbren et al. compared the results of MS/MS screening with those of clinical identification.79 An overview of the studies objectives is shown in Table 20, and details about the family characteristics can be found in Appendix 19.
Table 20: Study objectives of selected studies for ethical and psychosocial issues
Author, Country Objective(s) of study Liebl, Germany81 To find out whether high compliance with expanded MS-MS-based screening program
can be achieved despite move to written parental consent Waisbren, US79
To compare newborn identification by expanded screening with clinical identification of biochemical genetic disorders and to assess the impact on families of a false-positive screening result compared with a normal result in expanded newborn screening program
Wilson, UK10 To investigate outcome of MCADD after diagnosis has been established
7.2.3 Data analysis and synthesis
For details about our findings on ethical and psychosocial issues from the selected studies, please refer to Appendix 19. Ethical issues The issue of informed consent for MS/MS screening is complicated, partly because uniformly effective therapies have not been developed for all the conditions this technology can detect and because it may detect previously unrecognized metabolites or conditions.83 The capability of MS/MS to provide profiles of metabolites makes it simple to incrementally add other conditions

48
Figure 5: Selection of ethical and psychosocial evidence for review to a newborn screening program. This may tempt some jurisdictions to expand their screening repertoire beyond that which would be supported by accepted population screening guidelines.84 The MS/MS technology does not stand alone and should be used in the context of a follow-up structure.84 The debate on the approach taken to parental consent pertain to established newborn screening tests such as tests for phenylketonuria (PKU) and congential hypothyroidism (CH) and is unaffected by the addition of MCADD screening.85 Given that the current debate exists, a discussion of the issue of consent for newborn screening is included for completeness. A multidisciplinary working group was convened to explore the social, ethical, and legal issues regarding MS/MS screening with the objective of building a theoretical framework. This workshop was held in association with the Garrod Society Annual Symposium on May 28, 2005 at the Children’s Hospital of Eastern Ontario in Ottawa. 86 Also noteworthy is the availability of general literature on the consent issues associated with genetic screening programs that fall
68 potentially relevant reports retrieved for further scrutiny
42 reports excluded: ethical or psychosocial implications not the primary focus
27 reports included for selection
504 citations identified from literature search
Six articles reporting on three primary studies
21 reports excluded from analysis: • 18 reviews • 3 primary studies on cystic fibrosis
One report identified from other sources

49
outside the scope of this review.87-89 The ethical principle of autonomy means respecting the right to self-determination and protecting those with diminished autonomy.90 Informed consent requires two components: information and explicit consent.91 There are at least two models to consider, each resulting in different practical implications (in terms of cost and time). • Information may be provided without explicit consent procedures. Different strategies for
providing information may be used in different situations. • Opt-in and opt-out models of explicit consent respect the principle of autonomy, and the
general public is informed of the model chosen. One approach would be to choose the opt-out model in situations that are not controversial, such as newborn screening for PKU and CH, and reserve the opt-in model for cases that are more controversial.
The current approach to screening newborns leans towards the first model, which is to perform routine screening tests on newborns without explicit parental consent.85 In some jurisdictions, authority for newborn screening is by hospital regulations and specifically identifies those disorders to be screened, for example PKU and CH. Some jurisdictions allow for parental refusal (opt-out model). Many jurisdictions provide information about newborn screening to parents even in the absence of their explicit consent.85 Metabolic screening programs are increasingly confronted with a series of ethical questions. Which conditions should be targeted and included in comprehensive screening programs? Is explicit parental consent required before conducting screening tests91,92 for conditions that are not, or are only marginally, amenable to treatment? Which genetic or metabolic tests should parents be able to request? With further advances in technology, the number of conditions that could be included in newborn screening programs is anticipated to expand over the next decade. As more genes are implicated in disease, the desire by health professionals to test for more conditions is likely to grow. The problem of justification will intensify with advances in screening techniques that make it easier to test for more conditions. It is logistically difficult to require explicit consent for some conditions and not for others. This represents another argument for not casually adopting tests into a newborn screening program. The number of different conditions included in screening programs differs between jurisdictions in Canada and elsewhere.76-78 Parents should be informed about what tests are available, and the risks of those tests, and given the option to refuse the tests. One major concern with requiring explicit consent is the possibility that many parents would refuse to give it and their infants would not be tested. However, in their study, Liebl et al. found that despite a written consent requirement for MS/MS screening, refusal was uncommon when parents were given good information.81 The explicit consent process will also increase parents’ knowledge about newborn screening. Their increased knowledge may relieve the anxiety associated with false-positive results.79 More research is needed to examine the issue of parental consent and the limits to parental refusal through an analysis of the relevant Canadian law and legislation.

50
Psychosocial issues Any consideration of the benefits and risks of screening must include the psychosocial dimensions, and the clinical and economic outcomes. Much of the concern over psychological adversity has been based on experience with other genetic conditions such as cystic fibrosis and sickle cell disease.93-98 Early detection of a genetic condition such as MCADD in a newborn infant, through MS/MS screening, is likely to be a shock and an emotionally traumatic experience for parents, for whom there may have been no warning signs.78 Conversely, as demonstrated by the findings from Waisbren et al.79 and others,77,97 early diagnosis of a problem may be helpful for parents, allowing them to prepare emotionally and practically for the development of the disease in the child. The psychosocial benefit of early diagnosis reported through screening is reduction of the anxiety often experienced by families as they endure tests, clinic visits or hospitalizations with little idea of what is wrong with their child or what the future will hold in terms of morbidity and mortality.96 It has been reported that diagnostic distress, although considerable, is no more extreme after a newborn diagnosis than after a later clinical one, nor is the parent-child relationship more negatively affected.79,97 Newborn screening can help parents avoid the stresses of diagnostic delay and have the psychological benefit of involvement in prophylactic treatment.97 Another psychosocial benefit for parents is knowing their own genetic status.96 Understanding this information through genetic counselling provides for informed reproduction.96 The MS/MS technology does not stand alone and should be used in the context of a follow-up structure. The evidence that families are emotionally distressed when they first hear of an abnormal screening result is not surprising. The findings reported by Waisbern et al.,79 Wilson et al., 10 and others,97 raise three issues. First, policy-makers need to address the question of specificity in providing this service, to ensure that parental distress is minimized. Second, families must be given enough information, to provide informed consent. Finally, health professionals need to be aware that some families may continue to worry and will require ongoing support. There are psychosocial concerns associated with positive and negative test results for MCADD screening and newborn screening. Health professionals should be aware of the emotional and psychological impact on parents and other family members of symptomatic or postmortem diagnosis with risk of psychological sequelae in the context of the possibility of screening. Some parents whose child tests positive may treat the child as though he or she is ill even before symptoms develop, and become overprotective (vulnerable child syndrome).99 On the other hand, unaffected family members have been reported to experience survivor guilt over their “escape” from a genetic disease.96 Confirmation of screening results by DNA mutation analysis may also lead to the identification of mispaternity, or to stigmatization of the parents or the child.96 With other diseases of genetic origin such as cystic fibrosis, the misconception that the heterozygote child is at risk of developing the disorder has sometimes led to difficulties with health or life insurance, and employment discrimination.95,96 This form of discrimination is unlikely to occur with MCADD, given the availability of a preventive treatment regimen.

51
A false diagnosis of newborns can create anxiety and psychosocial problems for parents. Although newborn screening tests are designed to detect infants with metabolic illnesses, certain tests may also identify carriers or individuals with variants who may be clinically asymptomatic. For example, 15% to 35% of infants with MCADD will never experience any ill effects and there is no way of predicting which children these will be.77 The potential consequences of diagnosis for this asymptomatic group include anxiety about the risk of hypoglycemia during early childhood and adverse effects of clinically unwarranted treatment. In rare cases, parents may be wrongly reassured after a false-negative test, as a result of insensitivity of the test, human error in laboratory procedures, record-keeping, or communication.96 Several authors have noted that an undue delay in receiving confirmatory test results is an important factor in increasing family stress.77,97 Time delays that prolong uncertainty for parents may have different implications for affected and carrier families confirmed by DNA mutation analysis. In the former situation, time delays could compromise early treatment, and in the latter, they could prolong the period during which parents are worrying that their infant might be affected.97 In the case of MS/MS screening for MCADD, false-positive test results are treated as positives until proven to be false, due to the benign nature of the treatment. The relationship between the amount and type of information provided to parents and their anxiety has been noted in several reports. As demonstrated by the findings of Waisbren et al.,79 many parents may have difficulty understanding the variety of diseases tested for and the screening process involved. Parental anxiety and dissatisfaction with the screening process have been found to be lower in those who feel they have received adequate referral and information.78 Therefore, as part of the informed consent process, information about why a blood sample is being taken, what type of disorders are being tested for, and what the results will mean for the child (and the family) should be provided to parents in a timely fashion. Information about false-positive (potentially the cause of distress as shown by Waisbren et al.79 and false-negative test results should be provided to reduce the fears and anxiety that these results can create for parents.
7.3 Summary Newborn screening raises many of the same ethical and psychosocial concerns that other genetic testing has raised, including those of informed consent, false diagnosis, and privacy and confidentiality of test results from third parties. Genetic and metabolic screening programs have been confronted with a series of ethical questions. Which conditions should be targeted in the tests included in comprehensive screening programs? Which genetic or metabolic tests should parents be able to request? Is explicit parental consent required before conducting screening tests? Parents need to be informed about the screening tests being conducted and the attendant risks of those tests, and given the option to refuse the tests. Information regarding why a blood sample is being taken, what type of conditions are being tested for, and what the results will mean for the child and the family should be provided to parents. Any delay in reporting a correct diagnosis, either positive or negative, should be kept to a minimum.

52
In general, MCADD testing has minimal effect on the ethical and psychosocial context of newborn screening. To a greater extent than seen with PKU or CH, some children identified with MCADD will not experience the manifestations of the disease. Confirmation of the disease, in the subset of compound heterozygotes, may take longer than for PKU and CH. MS/MS screening makes it simple to incrementally add conditions other than MCADD to the screening program. 8 CONCLUSION The benefits of MS/MS-based screening are clear: the vast majority of patients whose MCADD was detected by newborn screening were asymptomatic, whereas most of those who presented clinically had suffered potentially irreversible damage. The percentage of fatal cases among those diagnosed clinically was significantly higher than that among those diagnosed by MS/MS-based screening. There is, however, limited evidence of clinical follow-up or of contemporaneous comparison of outcomes between newborn screening and clinical diagnosis. Given the high clinical validity (sensitivity and specificity) of MS/MS-based screening, and the estimated incidence of MCADD (pooled from different studies involving populations of differing ethnic composition), it is likely that about 20 cases of MCADD would be detected in Canada annually. This assumes that 330,000 infants are born in Canada per year. Left untreated, MCADD can be fatal, but it is preventable with simple treatment if detected pre-symptomatically. Our review of two existing economic evaluations and our primary economic analysis both show that MS/MS-based screening for MCADD is cost-effective; while screening does consume more resources than not screening, it results in lower morbidity and lower mortality. In the review of two existing economic evaluations, the ICER values fell below the commonly applied threshold of US$50,000 per QALY.2 In the case of our primary economic analysis, which was based on data from relevant Canadian sources, ICER values fell below the CE threshold of C$20,000 per QALY proposed by Laupacis et al.1 Nevertheless, further studies on the long-term health consequences of MCADD, health improvements due to early detection, and health-related quality of life among MCADD patients are still needed, particularly in the Canadian context, so as to provide for improved economic analyses. Jurisdictions contemplating the introduction of MS/MS-based MCADD newborn screening should pay special attention to data about MCADD incidence, cost of acute episode, MS/MS acquisition cost, MS/MS specificity, per sample screening cost, cost of follow-up management, salary for personnel involved in screening program, and current PKU screening cost. The newborn screening of IEM raises ethical and psychosocial concerns including informed consent, false diagnosis, parental anxiety, and privacy and confidentiality of test results from third parties. Parents need to be adequately informed about screening tests conducted by MS/MS and their associated risks, and given the option to explicitly refuse the tests. Positive screens need to be reported quickly for clinical reasons.

53
9 REFERENCES
1. Laupacis A, Feeny D, Detsky AS, Tugwell PX. How attractive does a new technology have to be to warrant adoption and utilization? Tentative guidelines for using clinical and economic evaluations. CMAJ 1992;146(4):473-81.
2. Eichler HG, Kong SX, Gerth WC, Mavros P, Jonsson B. Use of cost-effectiveness analysis in health-care resource allocation decision-making: how are cost-effectiveness thresholds expected to emerge? Value Health 2004;7(5):518-28.
3. Kristensen FB, Horder M, Poulsen PB. Health technology assessment handbook. Copenhagen, Denmark: National Board of Health; 2001. Available: http://www.dihta.dk.
4. Roe C, Coates P. Acyl-coA dehydrogenase deficiencies. In: Scriver C, Beaudet A, Sly W, Valle D, editors. The metabolic basis of inherited disease. New York: McGraw Hill; 1989. p.889-914.
5. Andresen BS, Bross P, Udvari S, Kirk J, Gray G, Kmoch S, et al. The molecular basis of medium-chain acyl-CoA dehydrogenase (MCAD) deficiency in compound heterozygous patients: is there correlation between genotype and phenotype? Hum Mol Genet 1997;6(5):695-707. Available: http://hmg.oxfordjournals.org/cgi/reprint/6/5/695 (accessed 2005 Jul 28).
6. Pollitt RJ, Leonard JV. Prospective surveillance study of medium chain acyl-CoA dehydrogenase deficiency in the UK. Arch Dis Child 1998;79(2):116-9. Available: http://adc.bmjjournals.com/cgi/reprint/79/2/116 (accessed 2004 Nov 8).
7. Andresen BS, Dobrowolski SF, O'Reilly L, Muenzer J, McCandless SE, Frazier DM, et al. Medium-chain acyl-CoA dehydrogenase (MCAD) mutations identified by MS/MS-based prospective screening of newborns differ from those observed in patients with clinical symptoms: identification and characterization of a new, prevalent mutation that results in mild MCAD deficiency. Am J Hum Genet 2001;68(6):1408-18.
8. Iafolla AK, Thompson RJ, Roe CR. Medium-chain acyl-coenzyme A dehydrogenase deficiency: clinical course in 120 affected children. J Pediatr 1994;124(3):409-15.
9. Wilcken B, Hammond J, Silink M. Morbidity and mortality in medium chain acyl coenzyme A dehydrogenase deficiency. Arch Dis Child 1994;70(5):410-2.
10. Wilson CJ, Champion MP, Collins JE, Clayton PT, Leonard JV. Outcome of medium chain acyl-CoA dehydrogenase deficiency after diagnosis. Arch Dis Child 1999;80(5):459-62. Available: http://adc.bmjjournals.com/cgi/reprint/80/5/459 (accessed 2004 Sep 29).
11. Vianey-Liaud C, Divry P, Gregersen N, Mathieu M. The inborn errors of mitochondrial fatty acid oxidation. J Inherited Metab Dis 1987;10 Suppl 1:159-200.
12. Wang SS, Fernhoff PM, Hannon WH, Khoury MJ. Medium chain acyl-CoA dehydrogenase deficiency: human genome epidemiology review. Genet Med 1999;1(7):332-9.
13. Liebl B, Nennstiel-Ratzel U, Roscher A, Von Kries R. Data required for the evaluation of newborn screening programmes. Eur J Pediatr 2003;162 Suppl 1:S57-S61.
14. Seddon HR, Gray G, Pollitt RJ, Iitia A, Green A. Population screening for the common G985 mutation causing medium-chain acyl-CoA dehydrogenase deficiency with Eu-labeled oligonucleotides and the DELFIA system. Clin Chem 1997;43(3):436-42.

54
15. Sander S, Janzen N, Janetzky B, Scholl S, Steuerwald U, Schäfer J, et al. Neonatal screening for medium chain acyl-CoA deficiency: high incidence in Lower Saxony (northern Germany). Eur J Pediatr 2001;160(5):318-9.
16. Births and birth rate, by provinces and territories. Ottawa: Statistics Canada; 2005. Available: http://www.statcan.ca/english/Pgdb/demo04b.htm (accessed 2005 May 4).
17. National Newborn Screening and Genetics Resource Center. National newborn screening status report:U.S. national screening status report - updated 4/27/05. Austin (TX): The Center; 2005. Available: http://genes-r-us.uthscsa.edu/nbsdisorders.pdf (accessed 2005 May 3).
18. Fearing MK, Levy HL. Expanded newborn screening using tandem mass spectrometry. Adv Pediatr 2003;50:81-111.
19. Chace DH, Kalas TA, Naylor EW. The application of tandem mass spectrometry to neonatal screening for inherited disorders of intermediary metabolism. Annu Rev Genomics Hum Genet 2002;3:17-45.
20. Chace DH, Hillman SL, Van Hove JL, Naylor EW. Rapid diagnosis of MCAD deficiency: quantitatively analysis of octanoylcarnitine and other acylcarnitines in newborn blood spots by tandem mass spectrometry. Clin Chem 1997;43(11):2106-13. Available: http://www.clinchem.org/cgi/reprint/43/11/2106 (accessed 2004 Nov 8).
21. Van Hove JL, Zhang W, Kahler SG, Roe CR, Chen YT, Terada N, et al. Medium-chain acyl-CoA dehydrogenase (MCAD) deficiency: diagnosis by acylcarnitine analysis in blood. Am J Hum Genet 1993;52(5):958-66.
22. Whiting P, Rutjes AW, Reitsma JB, Bossuyt PM, Kleijnen J. The development of QUADAS: a tool for the quality assessment of studies of diagnostic accuracy included in systematic reviews. BMC Med Res Methodol 2003;3(1):25.
23. Hoffmann GF, Von Kries R, Klose D, Lindner M, Schulze A, Muntau AC, et al. Frequencies of inherited organic acidurias and disorders of mitochondrial fatty acid transport and oxidation in Germany. Eur J Pediatr 2004;163(2):76-80.
24. Marsden D. Expanded newborn screening by tandem mass spectrometry: the Massachusetts and New England experience. Southeast Asian J Trop Med Public Health 2003;34 Suppl 3:111-4.
25. Wilcken B, Wiley V, Hammond J, Carpenter K. Screening newborns for inborn errors of metabolism by tandem mass spectrometry. N Engl J Med 2003;348(23):2304-12.
26. Schulze A, Lindner M, Kohlmüller D, Olgemöller K, Mayatepek E, Hoffmann GF. Expanded newborn screening for inborn errors of metabolism by electrospray ionization-tandem mass spectrometry: results, outcome, and implications. Pediatrics 2003;111(6 Pt 1):1399-406.
27. Shigematsu Y, Hirano S, Hata I, Tanaka Y, Sudo M, Sakura N, et al. Newborn mass screening and selective screening using electrospray tandem mass spectrometry in Japan. J Chromatogr B Analyt Technol Biomed Life Sci 2002;776(1):39-48.
28. McCandless SE, Millington D, Andresen BS, Gregersen N, Muenzer J, Frazier DM. Clinical findings in MCAD patients heterozygous for the common mutation identified by MS/MS newborn screening [abstract]. Am J Hum Genet 2002;71(4 Suppl):419. Available: http://www.ashg.org/genetics/abstracts/abs02/f1456.htm (accessed 2004 Nov 8).

55
29. Carpenter K, Wiley V, Sim KG, Heath D, Wilcken B. Evaluation of newborn screening for medium chain acyl-CoA dehydrogenase deficiency in 275 000 babies. Arch Dis Child Fetal Neonatal Ed 2001;85(2):F105-F109.
30. Pourfarzam M, Morris A, Appleton M, Craft A, Bartlett K. Neonatal screening for medium-chain acyl-CoA dehydrogenase deficiency. Lancet 2001;358(9287):1063-4.
31. Zytkovicz TH, Fitzgerald EF, Marsden D, Larson CA, Shih VE, Johnson DM, et al. Tandem mass spectrometric analysis for amino, organic, and fatty acid disorders in newborn dried blood spots: a two-year summary from the New England Newborn Screening Program. Clin Chem 2001;47(11):1945-55.
32. Wilcken B, Wiley V, Carpenter K. Two years of routine newborn screening by tandem mass spectrometry (MSMS) in New South Wales, Australia [abstract]. J Inherited Metab Dis 2000;23 Suppl 1:4.
33. Marsden D, Zytkovicz T, Larson C, Shih V, Grady G. Prevalence of fatty acid oxidation disorders and organic acidemias in New England newborns screened by tandem mass spectrometry [abstract]. J Inherited Metab Dis 2000;23 Suppl 1:15.
34. McCandless SE, Muenzer J, Chaing SH, Weavil SD, Moore EG, Frazier DM. Tandem mass spectrometry newborn screening for medium-chain acyl-CoA dehydrogenase deficiency in North Carolina [abstract]. Am J Hum Genet 2000;67(4 Suppl 2):10.
35. Roscher A, Liebl B, Fingerhut R, Olgemöller B. Prospective study of MS-MS newborn screening in Bavaria, Germany. Interim results [abstract]. J Inherited Metab Dis 2000;23 Suppl 1:4.
36. Abdenur JE, Chamoles NA, Schenone A, Guinle A, Fusta M, Gaggioli D. Supplemental newborn screening of amino acids (AA) and acylcarnitines (AC) by electrospray tandem mass spectrometry (ESI- MS/MS): experience in Argentina [abstract]. J Inherited Metab Dis 2000;23 Suppl 1:13.
37. Naylor EW, Chace DH. Automated tandem mass spectrometry for mass newborn screening for disorders in fatty acid, organic acid, and amino acid metabolism. J Child Neurol 1999;14 Suppl 1:S4-S8.
38. Wiley V, Carpenter K, Wilcken B. Newborn screening with tandem mass spectrometry: 12 months' experience in NSW Australia. Acta Paediatr Suppl 1999;88(432):48-51.
39. Ziadeh R, Hoffman EP, Finegold DN, Hoop RC, Brackett JC, Strauss AW, et al. Medium chain acyl-CoA dehydrogenase deficiency in Pennsylvania: neonatal screening shows high incidence and unexpected mutation frequencies. Pediatr Res 1995;37(5):675-8.
40. Beatty S, Chace D, Naylor E. The population disease frequency of disorders of fatty, organic, and amino acid metabolism in over 1.2 million infants screened by tandem mass spectrometry [abstract]. Genet Med 2002;4(3):176.
41. Yoon H-R, Lee KR, Kim H, Kang S, Ha Y, Lee DH. Tandem mass spectrometric analysis for disorders in amino, organic and fatty acid metabolism: two year experience in South Korea. Southeast Asian J Trop Med Public Health 2003;34 Suppl 3:115-20.
42. Yoon HR, Lee DH, Lee KR, Kang SW, Cho KH. Screening of newborns and high risk infants for inherited metabolic diseases by tandem mass spectrometry in South Korea: 2 years of experience [abstract]. J Inherited Metab Dis 2003;26 Suppl 2:16.
43. McCandless SE, Davis EB, Frazier DM, Muenzer J. Linking infant death records to tandem mass spectrometry (MS/MS) newborn screen results in North Carolina [abstract]. Am J Hum Genet 2001;69(4 Suppl):210. Available: http://www.ashg.org/genetics/ashg01/f175.htm (accessed 2004 Nov 8).

56
44. Shigematsu Y, Fujisawa K, Hata I, Mayumi M, Tanaka Y, Sudo M. Newborn screening by tandem mass spectrometry: results of pilot study and retrospective analysis in Japan [abstract]. J Inherited Metab Dis 2000;23 Suppl 1:6.
45. Wasant P, Naylor EW, Liammongkolkul S. Detection of inherited metabolic disorders via tandem mass spectrometry in Thai infants. Southeast Asian J Trop Med Public Health 1999;30 Suppl 2:154-9.
46. Wilcken B, Wiley V, Sherry G, Carpenter K. Using tandem mass spectrometry in a routine newborn screening laboratory in Australia [abstract]. J Inherited Metab Dis 1998;21 Suppl 2:139.
47. Shigematsu Y, Hirano S, Hata I, Tanaka Y, Sudo M, Sakura N, et al. Target disorders in newborn screening by tandem mass spectrometry in Japan [abstract]. J Inherited Metab Dis 2003;26 Suppl 2:12.
48. Klose DA, Kölker S, Heinrich B, Prietsch V, Mayatepek E, Von Kries R, et al. Incidence and short-term outcome of children with symptomatic presentation of organic acid and fatty acid oxidation disorders in Germany. Pediatrics 2002;110(6):1204-11. Available: http://pediatrics.aappublications.org/cgi/reprint/110/6/1204 (accessed 2004 Nov 8).
49. Wilcken B, Wiley V, Hammond J, Carpenter K. Newborn screening by tandem mass spectrometry (MS/MS) compared with clinical diagnosis in a defined population [abstract]. J Inherited Metab Dis 2002;25 Suppl 1:1.
50. Sander J, Janzen N, Sander S, Melchiors U, Steuerwald U. Tandemmassenspektrometrie: Beitrag zum Neugeborenenscreening auf angeborene Störungen des Stoffwechsels [Neonatal screening for inborn errors of metabolism using tandem mass spectrometry]. Monatsschr Kinderheilkd 2000;148(8):771-7.
51. Muenzer J, Frazier DM, Weavil SD, Millington DS, Moore EG, Burton SW, et al. Incidence of metabolic disorders detected by newborn screening in North Carolina using tandem mass spectrometry [abstract]. Am J Hum Genet 2000;67(4 Suppl 2):36. Available: http://genetics.faseb.org/genetics/ashg00/f127.htm (accessed 2004 Nov 8).
52. la Marca G, Malvagia S, Donati MA, Morrone A, Pasquini E, Zammarchi E. Rapid diagnosis of medium chain Acyl Co-A dehydrogenase (MCAD) deficiency in a newborn by liquid chromatography/tandem mass spectrometry. Rapid Commun Mass Spectrom 2003;17(23):2688-92.
53. Lin WD, Wu JY, Lai CC, Tsai FJ, Tsai CH, Lin SP, et al. A pilot study of neonatal screening by electrospray ionization tandem mass spectrometry in Taiwan. Acta Paediatr Taiwan 2001;42(4):224-30.
54. Rashed MS, Rahbeeni Z, Ozand PT. Application of electrospray tandem mass spectrometry to neonatal screening. Semin Perinatol 1999;23(2):183-93.
55. Simonsen H, Jensen UG, Brandt NJ, Christensen E, Skovby F, Nørgaard-Pedersen B. Design of a pilot study to evaluate tandem mass spectrometry for neonatal screening. Southeast Asian J Trop Med Public Health 1999;30 Suppl 2:166-9.
56. Clayton PT, Doig M, Ghafari S, Meaney C, Taylor C, Leonard JV, et al. Screening for medium chain acyl-CoA dehydrogenase deficiency using electrospray ionisation tandem mass spectrometry. Arch Dis Child 1998;79(2):109-15. Available: http://adc.bmjjournals.com/cgi/reprint/79/2/109 (accessed 2004 Nov 8).
57. Rashed MS, Bucknall MP, Little D, Awad A, Jacob M, Alamoudi M, et al. Screening blood spots for inborn errors of metabolism by electrospray tandem mass spectrometry with a microplate batch process and a computer algorithm for automated flagging of abnormal profiles. Clin Chem 1997;43(7):1129-41. Available: http://www.clinchem.org/cgi/reprint/43/7/1129.

57
58. Lehotay DC, LePage J, Thompson JR, Rockman-Greenberg C. Blood acylcarnitine levels in normal newborns and heterozygotes for medium-chain acyl-CoA dehydrogenase deficiency: A relationship between genotype and biochemical phenotype? J Inherited Metab Dis 2004;27(1):81-8.
59. Alluri VN, Mulvihill JJ. Medium chain acyl coenzyme A dehydrogenase (MCAD) deficiency: the case for screening all newborns. J Okla State Med Assoc 2002;95(5):326-8.
60. Andresen B, Dobrowolski SF, O'Reilly L, Knudsen I, Banas R, Chace D, et al. The spectrum of MCAD mutations observed in newborns with diagnostic acyl-carnitines identified by prospective MSMS screening of blood spots differs from that in affected patients [abstract]. Eur J Hum Genet 2000;8 Suppl 1:146.
61. Andresen BS, Dobrowolski SF, O'Reilly L, Engel P, Knudsen I, Banas R, et al. The mutational spectrum in the MCAD gene of newborns identified by prospective tandem MS screening for "diagnostic" acyl-carnitines in blood spots differs from that observed in clinically affected patients [abstract]. J Inherited Metab Dis 2000;23 Suppl 1:12.
62. Kozàk L, Hrabincovà E, Rudolfoà J, Vràbelovà S, Freiberger T. Screening of the most common medium-chain acyl CoA dehydrogenase (MCAD) deficiency mutation (K329E) in the Czech newborn population. Southeast Asian J Trop Med Public Health 1999;30 Suppl 2:49-50.
63. Wasant P, Svasti J, Srisomsap C, Liammongkolkul S, Naylor EW, Matsumoto I. Inherited metabolic disorders in Thailand--Siriraj experience. Southeast Asian J Trop Med Public Health 1999;30 Suppl 2:124-37.
64. Conne B, Zufferey R, Belin D. The A985G mutation in the medium-chain acyl-CoA dehydrogenase gene: high prevalence in the Swiss population resident in Geneva. J Inherited Metab Dis 1995;18(5):577-83.
65. Szalai C, Czinner A, Révai K, Nagy I. [Newborn screening for medium chain acyl-CoA dehydrogenase deficiency in Hungary]. Orv Hetil 1995;136(30):1595-8.
66. Components of population growth, by provinces and territories. Ottawa: Statistics Canada; 2005. Available: http://www.statcan.ca/english/Pgdb/demo33a.htm (accessed 2005 May 4).
67. Dezateux C. Newborn screening for medium chain acyl-CoA dehydrogenase deficiency: evaluating the effects on outcome. Eur J Pediatr 2003;162 Suppl 1:S25-S28.
68. Touma EH, Charpentier C. Medium chain acyl-CoA dehydrogenase deficiency. Arch Dis Child 1992;67(1):142-5.
69. Drummond MF, Jefferson TO, BMJ Economic Evaluation Working Party. Guidelines for authors and peer reviewers of economic submissions to the BMJ. BMJ 1996;313(7052):275-83. Available: http://www.bmj.com/cgi/content/full/313/7052/275.
70. Insinga RP, Laessig RH, Hoffman GL. Newborn screening with tandem mass spectrometry: examining its cost-effectiveness in the Wisconsin Newborn Screening Panel [erratum published J Pediatr 2003 142(1):56]. J Pediatr 2002;141(4):524-31.
71. Venditti LN, Venditti CP, Berry GT, Kaplan PB, Kaye EM, Glick H, et al. Newborn screening by tandem mass spectrometry for medium-chain Acyl-CoA dehydrogenase deficiency: a cost-effectiveness analysis. Pediatrics 2003;112(5):1005-15.
72. Center for Disease Control. Mental retardation following diagnosis of a metabolic disorder in children aged 3-10 years -- metropolitan Atlanta, Georgia, 1991-1994. MMWR Morb Mortal Wkly Rep 1999;48(17):353-6. Available: http://www.cdc.gov/mmwr/preview/mmwrhtml/mm4817a3.htm (accessed 2005 Jan 31).

58
73. Neumann PJ, Sandberg EA, Araki SS, Kuntz KM, Feeny D, Weinstein MC. A comparison of HUI2 and HUI3 utility scores in Alzheimer's disease. Med Decis Making 2000;20(4):413-22.
74. Erickson P, Wilson R, Shannon L. Years of healthy life. Statistical Notes 1995;(7):1-16. Available: http://www.cdc.gov/nchs/data/statnt/statnt07.pdf.
75. Saigal S, Feeny D, Rosenbaum P, Furlong W, Burrows E, Stoskopf B. Self-perceived health status and health-related quality of life of extremely low-birth-weight infants at adolescence. JAMA 1996;276(6):453-9.
76. Seymour CA, Thomason MJ, Chalmers RA, Addison GM, Bain MD, Cockburn F, et al. Newborn screening for inborn errors of metabolism: a systematic review. Health Technol Assess 1997;1(11):1-95. Available: http://www.ncchta.org/fullmono/mon111.pdf (accessed 2004 Nov 12).
77. Pollitt RJ, Green A, McCabe CJ, Booth A, Cooper NJ, Leonard JV, et al. Neonatal screening for inborn errors of metabolism: cost, yield and outcome. Health Technol Assess 1997;1(7):1-202. Available: http://www.ncchta.org/fullmono/mon107.pdf (accessed 2004 Nov 10).
78. Pandor A, Eastham J, Beverley C, Chilcott J, Paisley S. Clinical effectiveness and cost-effectiveness of neonatal screening for inborn errors of metabolism using tandem mass spectrometry: a systematic review. Health Technol Assess 2004;8(12):1-134. Available: http://www.ncchta.org/fullmono/mon812.pdf (accessed 2004 Nov 12).
79. Waisbren SE, Albers S, Amato S, Ampola M, Brewster TG, Demmer L, et al. Effect of expanded newborn screening for biochemical genetic disorders on child outcomes and parental stress. JAMA 2003;290(19):2564-72.
80. Albers S, Waisbren SE, Ampola MG, Brewster TG, Burke LW, Demmer LA, et al. New England Consortium: a model for medical evaluation of expanded newborn screening with tandem mass spectrometry. J Inherited Metab Dis 2001;24(2):303-4.
81. Liebl B, Nennstiel-Ratzel U, Von Kries R, Fingerhut R, Olgemöller B, Zapf A, et al. Very high compliance in an expanded MS-MS-based newborn screening program despite written parental consent. Prev Med 2002;34(2):127-31.
82. Liebl B, Nennstiel-Ratzel U, Von Kries R, Fingerhut R, Olgemöller B, Zapf A, et al. Expanded newborn screening in Bavaria: tracking to achieve requested repeat testing. Prev Med 2002;34(2):132-7.
83. American College of Medical Genetics/American Society of Human Genetics Test and Technology Transfer Committee Working Group. Tandem mass spectrometry in newborn screening. Genet Med 2000;2(4):267-9.
84. Goel V. Appraising organised screening programmes for testing for genetic susceptibility to cancer. BMJ 2001;322(7295):1174-8.
85. Wildeman S, Downie J. Genetic and metabolic screening of newborns: Must health care providers seek explicit parental consent? Health Law J 2001;9:61-111.
86. Plant M, Avard D. Policy issues regarding newborn screening and tandem mass spectrometry [workshop]. Garrod Society Annual Symposium; 2005 May 28; Ottawa.
87. Caulfield T, Upshur RE, Daar A. DNA databanks and consent: a suggested policy option involving an authorization model. BMC Med 2003;4:E1.

59
88. Burgess MM, Laberge CM, Knoppers BM. Bioethics for clinicians: 14. Ethics and genetics in medicine. CMAJ 1998;158(10):1309-13.
89. Khoury MJ, McCabe LL, McCabe ER. Population screening in the age of genomic medicine. N Engl J Med 2003;348(1):50-8.
90. Beauchamp TL, Childress JF, editors. Principles of biomedical ethics. 5th. New York: Oxford University Press; 2004.
91. Hermerén G. Neonatal screening: ethical aspects. Acta Paediatr Suppl 1999;88(432):99-103.
92. Dhanda RK, Reilly PR. Legal and ethical issues of newborn screening. Pediatr Ann 2003;32(8):540-6.
93. Mérelle ME, Huisman J, Alderden-Van der Vecht A, Taat F, Bezemer D, Griffioen RW, et al. Early versus late diagnosis: psychological impact on parents of children with cystic fibrosis. Pediatrics 2003;111(2):346-50. Available: http://pediatrics.aappublications.org/cgi/reprint/111/2/346 (accessed 2004 Nov 12).
94. Parsons EP, Clarke AJ, Bradley DM. Implications of carrier identification in newborn screening for cystic fibrosis. Arch Dis Child Fetal Neonatal Ed 2003;88(6):F467-F471.
95. Farrell MH, Certain LK, Farrell PM. Genetic counseling and risk communication services of newborn screening programs. Arch Pediatr Adolesc Med 2001;155(2):120-6.
96. Farrell MH, Farrell PM. Newborn screening for cystic fibrosis: ensuring more good than harm. J Pediatr 2003;143(6):707-12. Available: http://www2.us.elsevierhealth.com/scripts/om.dll/serve?action=get-media&id=as0022347603005948&trueID=pdf_s0022347603005948&location=jpd031436&type=pdf&name=x.pdf (accessed 2004 Nov 12).
97. Parsons EP, Bradley DM. Psychosocial issues in newborn screening for cystic fibrosis. Paediatr Respir Rev 2003;4(4):285-92.
98. Oliver S, Dezateux C, Kavanagh J, Lempert T, Stewart R. Disclosing to parents newborn carrier status identified by routine blood spot screening. In: The Cochrane Database of Systematic Reviews. Issue 4; 2004.
99. Campbell E, Ross LF. Parental attitudes regarding newborn screening of PKU and DMD. Am J Med Genet 2003;120A(2):209-14.
100. Fleiss JL, Levin BA, Paik MC. Statistical methods for rates and proportions. 3rd ed. Hoboken (NJ): John Wiley and Sons; 2003.
101. Altman DG, Machin D, Bryant TN, Gardner MJ, editors. Statistics with confidence: confidence intervals and statistical guidelines. 2nd ed. London: BMJ Books; 2000.
102. Economic costs associated with mental retardation, cerebral palsy, hearing loss, and vision impairment --- United States, 2003. MMWR Morb Mortal Wkly Rep 2004;53(3):57-9. Available: http://www.cdc.gov/mmwr/preview/mmwrhtml/mm5303a4.htm (accessed 2005 May 4).
103. Financial market year average of exchange rates. Ottawa: Bank of Canada; 2003. Available: http://www.bankofcanada.ca/pdf/nraa03.pdf (accessed 2005 May 4).

APPENDICES
Available from CCOHTA's web site www.ccohta.ca