
Technical Strategy for MCHs3.amazonaws.com/zanran_storage/erc.msh.org/ContentPages/1703247… ·...
92
Family Planning and Health Systems Unit Technical Strategy for MCH (For a more complete document, please refer to the MCH Technical Strategy submitted to USAID on August 17, 2004) Deliverable No. 7C June 30, 2004 This report was made possible through support provided by the U.S. Agency for International Development, under the terms of Contract No. 492-C-00-03-00024-00. The opinions expressed herein are those of the author(s) and do not necessarily reflect the views of the U.S. Agency for International Development.
Transcript of Technical Strategy for MCHs3.amazonaws.com/zanran_storage/erc.msh.org/ContentPages/1703247… ·...

Family Planning and Health Systems Unit
Technical Strategy for MCH (For a more complete document, please refer to the MCH Technical Strategy
submitted to USAID on August 17, 2004)
Deliverable No. 7C
June 30, 2004
This report was made possible through support provided by the U.S. Agency for International Development, under the terms of Contract No. 492-C-00-03-00024-00. The opinions expressed herein are those of the author(s) and do not necessarily reflect the views of the U.S. Agency for International Development.

Maternal and Child Health Component Strategy 2004-2006
LEAD for Health Project
June 2004

TABLE OF CONTENTS Introduction
1
MCH Situation, Services, Programs in the Philippines
1
Maternal Health Situation
1
Maternal Care Practices
3
Child Health Situation
5
Childcare and Health-seeking Behavior
8
Maternal and Child Health Services and Programs
9
Child Health Services and Programs
15
Summary of Current Issues, Needs and Challenges in Maternal and Child Health
24
Maternal Care
24
Child Care
28
LEAD MCH Project Framework
32
Model Areas For Implementation
42
Summary of Interventions
43
Monitoring and Evaluation
45
Implementation Arrangement
46
LEAD for Health Project Organization
48
Timetable
49
List of Tables / Figures / Annexes
84
Acronyms
86
Acknowledgement
88

1
LEAD for Health Maternal and Child Health Component Strategy 2004-2006
Introduction The LEAD for Health project already identified Vitamin A supplementation as a major MCH strategy but did not specify the other MCH interventions that would be crucial to attain its mortality and morbidity reduction objectives. In order to specifically identify the suitable MCH interventions, interview, ocular visits and focus group discussions were conducted among various groups within the maternal and child health sector and the target communities and beneficiaries. Urban, rural and tribal communities were included. Perceptions by national, regional and LGU health staff, community health workers and community residents on the current health problems and program developments as well as their insights on successes and failures were gathered from selected areas with varying levels of performance: high, medium and low performing areas. MCH Situation, Services and Programs in the Philippines Maternal Health Situation Maternal Mortality Ratio Complications of pregnancy and childbirth are the leading causes of death among women of reproductive age in many developing countries like the Philippines. It is estimated that one woman for every 110 will die from pregnancy-related complications in Asia. The observation that less than 1 percent of these deaths occur in developed countries indicate that many of these deaths are avoidable. The Philippine National Demographic Health Survey in 1998 (NDHS 1998) detected the national maternal mortality ratio (MMR) – measured in terms of number of maternal deaths per 100,000 live births - to be 172, around 1,400 maternal deaths every year. These deaths comprise about 14% of deaths among Filipina women of reproductive age (15-49 years old). There is a slow but steady decline over the years, figure 1. This current level in the Philippines, however, is still higher than the ratio in the East Asia/ Pacific Region of 140 deaths per 100,000 live births. A developing country like Sri Lanka, with an MMR of 60, has demonstrated that the MMR could still be reduced much further despite some limitations in resources. Especially since the death of a mother also frequently results in the death or illness of her children, improvement of maternal health should be among the top priorities of all developing nations. The latest figures (1995) issued in the 2002 Statistical Yearbook of the National Statistics and Coordination Board show that eight regions (ARMM, Region X, Region IX, CAR, Region II, Region VIII, Region XII, and Region VI) had MMRs higher than the national ratio of 180 deaths per 100,000 live births, table 1. These regional variations could reflect the differences in terms of physical characteristics, resources allocation, culture and

2
educational level, among others, in different parts of the country. For instance, in CAR, some traditional tribal women could still deliver babies by themselves or prefer to be assisted only by their husbands. The relatively better MMR in NCR and Region 4 could reflect the relatively better access to maternity services in these areas. No data was available for CARAGA. Causes of Maternal Death It is globally recognized that the causes of maternal deaths are often multifactorial and involve complex interactions of several medical, obstetric, health service and social factors. (Carroli et al, Pediatric and Perinatal Epidemiology, 2001). Hemorrhage or severe bleeding, infection (including HIV), obstructed labor, hypertensive diseases of pregnancy (HDP) and unsafe abortion together account for at least two-thirds of all maternal deaths, figure 2. The 1998 NDHS reflected this worldwide observation. The most common obstetrical complication in the Philippines was prolonged labor (17%), followed by excessive bleeding at 7%. The 1998 Philippine Health Statistics report of the DOH lists the causes of maternal death as follows, figure 3. Maternal and neonatal morbidity Globally, it is been estimated that over 300 million women in developing countries currently suffer from short- or long-term illness related to pregnancy and childbirth. The short-term illnesses related to pregnancy include anemia, genitourinary tract infection, hypertension, and malnutrition, among others. Many women, especially in the rural communities, are already undernourished before pregnancy. During pregnancy, they may not reduce their work burden or raise their caloric intake. Non-life-threatening infections in the genitourinary tract also occur, but reliable data on these illnesses are not available. FNRI surveys indicate that maternal undernutrition level in terms of the proportion of women underweight for their height was 14.7% in 1998, a decline from 21.7% in 1993. The same survey listed the chronic energy deficiency (CED) among lactating women at 13,4% in 1998, an increase from 10.9% in 1993. The 1993 Safe Motherhood Survey (SMS 1993) found an induced abortion prevalence rate of 7%, 80% of which were among married women in their 3rd pregnancy. The 2003 Philippine Progress Report on the Millennium Development Goals (MDG), however, estimated that 400,000 abortions occurred annually in the world, and that 17% of these were among unmarried teenagers. Data indicating the reliable numbers of women mothers and neonates who suffer complications and survived are not readily available.

3
The long-term complications include uterine prolapse, fistulae along the birth canal, incontinence, pain during intercourse, nerve damage, pelvic inflammatory disease and infertility. It is estimated that about 2 million women are currently living with obstetric fistulae and that 50,000 to 100,000 new cases occur each year. Women who develop fistulae have been found to become social outcasts, rejected by their husbands and families. In the Philippines, long-term renal complications deserve further investigation in terms of its correlation with undetected urinary infections and obstetric complications. HIV/AIDS surveillance data of the Philippine Department of Health (DOH) listed a cumulative total of 1,947 persons with HIV/AIDS in the country from 1994 – Oct 2003, 256 of whom had already died. Of this, 29 (1.5%) were children who had been infected by their mothers. The adult (15-49 yrs) HIV prevalence rate in 2001 was <0.1%, placing the country among those with the lowest HIV infection rates. Many of these cases had been infected abroad. Tuberculosis (TB) was reported in 1996 to have a mortality rate of 37.7 per 100,000 population and a smear positive prevalence of 3.1 per 1,000 population, or about 250,000 cases identified and currently undergoing treatment. Using 2003 data from 8 regions, there was a 2.3:1 male to female ratio among the smear positive cases. Less than 1% were children younger than 14 years old, while 8.3% were elderly (above 65 years old). The bulk of the cases (about 64%) were between 25-54 years old. Considering a detection rate of only about 50%, there was still about the same number of undetected, and thus untreated, cases in the population. The ongoing TB-DOTS campaign had a treatment success rate of 87%. Malaria mortality rate was detected at 0.8 deaths per 100,000 population in 1996, with a morbidity rate of about 59 cases per 100,000 population. Dengue, hookworm and schistosomiasis were highly endemic in many places in the country. The dengue incidence rate was 32 per 100,000 population, schistosomiasis prevalence rate 4.5%, and soil transmitted helminthiases including hookworm prevalence rate was 57%. The case fatality rate from dengue was 2%. Low birth weight is currently reported at 13.6% of live births in 2000 (FHSIS). It was detected at 16.6% in the 1998 NDHS. Maternal Care Practices There are many Filipino practices and cultural taboos that surround pregnancy and childbirth, some helpful, others harmless, but those of real concern are the ones that cause harm and must therefore be changed. There are more than 85 different tribal groups in the country, and cultural variation among the sub-cultures is wide. To change these harmful yet culturally ingrained, age old practices is a real challenge to health workers. To complicate matters, the health workers and educators themselves subscribe to some of these practices. Indeed, only a deliberate, clear, consistent, sustained and comprehensive communication plan that starts from early childhood and goes through to late adulthood

4
or even, perhaps to the elderly period, and involving all sectors of society, especially the educators and health workers, might truly change deep-seated cultural beliefs. The first step, however, is always to sort out these various practices at the community and family levels. Traditional birth attendants (“hilots”) Even though professional midwifery was most probably introduced more than 200 years ago, many Filipino women, both rural and urban, still prefer to be delivered by the traditional birth attendants or hilots. Hilots not only provide the basic maternity services, they also do household chores like cooking or washing during the postnatal period. Hilots continue to be the main source of advice on almost everything in maternal care – from the foods pregnant women should eat or avoid, to what actions and rituals are appropriate to ensure a safe birth. Home deliveries Childbirth has traditionally been a family affair and occurs at home, surrounded by the woman’s husband, relatives, loved ones and inquisitive neighbors. Whether the home is in the mountain or in the urban slum, it is still the most comfortable place for a parturient. The hospital is a place regarded with fear. It is perceived as a place where women die. To tell a woman she has to go to the hospital to complete her delivery is like giving her a death sentence, thus she will do everything, and allow everything to be done to her, to make sure she completes her birth at home. Other family and community practices in maternal care Pregnancy is regarded as a critical period in life. It is believed that evil spirits are lurking around, waiting to eat the fetus in the womb, especially during the early weeks of pregnancy, that is the reason why women who just recently miss their period tried to keep her pregnancy a secret until it is well established in her womb. This is also probably one of the reasons why it difficult to get the women to consult early for prenatal care. Foods are also strongly believed to affect the fetus in the womb, which is generally correct. However, instead of eating better food because it will improve the baby’s health, this belief translates as avoiding certain foods, such as beans or eggs, which are actually nutritious. Foods are also believed to affect the child’s personality or physical attributes, so that dark-colored foods are avoided because this will make the child dark-skinned. Some hilots also advice pregnant women not too eat too much during pregnancy to avoid large a baby that could make delivery difficult. This is also partly true, but the advice translates as too little nutrition for the pregnancy woman. There is no good traditional gauge on what is adequate, what is inadequate and what is too much. Uterine massage is also a common practice, usually done by TBAs at about the second trimester on the belief that this improves maternal circulation and fetal development. If

5
massage is light, this may not be harmful, but some techniques may be too strong for the developing fetus. Many women and their families are still not aware of many of the danger signs of pregnancy and childbirth. They and their families need to be educated on these especially on the appropriate action to prevent deaths and severe complications. Traditionally through immediate breastfeeding after delivery, many women naturally practiced what is now called the Lactational amenorrhea (LAM) family planning method. With the decline in breastfeeding, this practice has to be reintroduced. There are traditional family planning methods but most of these are herbs or massage believed to abort the fetus. Modern family planning methods are just beginning to be understood. Many fears still surround their side effects. Availability of good quality FP counseling and FP services will hasten the acceptance of the modern FP methods. The notion that birth spacing can help improve maternal health is still not widely recognized. Health education on the benefits of FP on maternal health will also facilitate the acceptance of family planning. Child Health Situation Infant and Under-Five Mortality Figure 4 shows a slow decline of infant mortality rate (IMR) by 15 percent over the 15-year period from 1988-2002: from 34 per one thousand live births in 1993 (NDHS 1988-1992) to 29 in 2003 NDHS (1998-2002). The goal of reducing IMR to 36 by 2003 seems to have already been achieved, but when compared to other Asian countries, the IMR in the Philippines is still higher compared with Singapore, Malaysia and Thailand. The under-five mortality rate declined by twenty six percent over the same 15-year period: from 54 per thousand live births in 1993 to 40 per thousand in 2003 (figure 4). More than 50% of infant deaths occur during the neonatal period (1996 HIS – 52%). Although infant and under-five mortality rates are declining over the 15-year period from 1988-2002, regional disparities are still noted (1998 NDHS), figures 5 and 6. Infant mortality is highest in Eastern Visayas region at 61 per thousand live births, followed by ARMM and CARAGA at fifty-five and fifty-three. These rates are higher compared to the national figure of thirty-six, by 67% for Eastern Visayas, 53% for ARMM and 47% for CARAGA. ARMM has the highest under-five mortality rate (98 per thousand live births) and this is higher by 78% compared to the national average of 54.9. Consistently the same regions Eastern Visayas (85.6) and CARAGA (82.5) ranked next to ARMM with rates higher than the national by 56% and 50% respectively.

6
Causes of Infant and Under-five Mortality The leading causes of deaths among infants are respiratory conditions of fetus and newborns, pneumonia, congenital anomalies, birth injuries and difficult labor, diarrheal diseases, septicemia, meningitis, other respiratory diseases, avitaminoses and other nutritional deficiencies, and measles. The observation that more than 50% of infant deaths occur during the neonatal period implies poor maternal health, inadequate prenatal and natal care, inappropriate management of complications during pregnancy and delivery, poor hygiene during delivery and poor newborn care during the critical hours at birth.
Forty six percent of the under-five deaths are due to pneumonia, diarrhea, measles, malaria, dengue hemorrhagic fever and malnutrition (1994 DOH-HIS report). The relatively higher infant and under-five mortality rates in ARMM could be due to poor access to health services. Only 42 % of the women in ARMM had prenatal care by doctors / nurses and midwives compared to the national average of 86%. Six out of ten women in ARMM did not get tetanus toxoid vaccination. Child health services coverage in ARMM is also poor: as much as 34% of 13-24 months old children surveyed had never received any of the infant vaccinations while the national average was at only 8%; Vitamin A supplementation in ARMM was only 31%, the national coverage was 71%.
Infant and under-five mortality rates are strongly influenced by socio-economic factors such as place of residence, education of mothers, health practices as well as access to health services. In 1998 NDHS, under-five year old children in the rural areas have higher risk of dying than those in the urban areas. This is due to variations in accessibility and availability of quality health services. Mortality rates of infants and under-five children of mothers with no education or less educated are much higher compared to those whose mothers are in high school of college. This supports the study of Costelo who concluded that there is an inverse relationship between maternal education and infant mortality. In addition, children whose mothers have no antenatal or delivery care have much higher mortality rates during infancy or early childhood than those whose mothers had both antenatal and natal care.
The same 1998 NDHS report shows certain demographic characteristics affecting infant and under-five mortality rates, table 2. Infant deaths, especially during the neonatal period, and under-five deaths are higher among mothers below twenty years old and above forty years old, and among mothers with less than two years birth interval. Small and very small size babies at birth have less chances of survival during the neonatal, infancy and under-five years period.

7
Child Morbidity Nutritional Status Of Children Malnutrition has been a persistent problem in the Philippines. The 1998 Fifth National Nutrition Survey conducted by the Food and Nutrition Research Institute showed that sixty eight percent of children 0-5 years old are normal in weight- for-age using the NCHS/ WHO standards. On the other hand, thirty two percent of the same age is underweight and thirty four percent are stunted. Compared with the 2001 FNRI survey findings, there is a reduction of 1.4 and 2.6 percentage points in underweight (30.6%) and stunting (31.4%) respectively. Based on NSO estimated population of 2001, it is estimated that about 3.67 million children are underweight and 3.76 million are stunted. Figure 7 shows the trend of underweight and stunting over a decade from 1998-1990 to 2001 with a reduction of 3.9 and 8.5 percentage points respectively. Figure 8 shows that the highest percentage of underweight children is at the age of one and two years. This could be explained by the poor breastfeeding and feeding practices especially during weaning period. During these years, children are vulnerable to infectious diseases as shown by the ten leading causes of infant deaths that include pneumonia, diarrhea, measles and malnutrition and dengue hemorrhagic fever in some areas of the country. Almost thirteen percent of the newborns are underweight. This is influenced by maternal health and anemia of pregnant women. . Micronutrient deficiencies The 1998 FNRI survey revealed that the prevalence of IDD in the Philippines is mild based on a median urinary iodine excretion (UIE) level of 71.0 ug /L. Only 34.7 per cent of the 6-12 years old children have UIE values equal to or greater than 100 ug/L or no iodine deficiency; 29.6 per cent have values or UIE of 50-99ug/L or have mild iodine deficiency; 23.5 per cent have UIE values 20- below 50ug/L or moderate deficiency; and 12.3 per cent of children have severe iodine deficiency as their UIE values are lower or equal to 20ug/L. Seven regions, namely: Bicol, Western Visayas, Northern Mindanao, Southern Mindanao, Central Mindanao, CARAGA and CAR have higher percentage of children with severe iodine deficiency than national average. Forty-six provinces and three cities have a higher percentage of children who are moderately and severely iodine deficient than the national average of 35.8 per cent. Studies have shown that about 13.5 IQ points are irreversibly lost among iodine deficient children.
Vitamin A Deficiency is considered endemic in the Philippines. FNRI report of the 1998 National Nutrition Survey in the Philippines showed that Vitamin A Deficiency remains a public health problem. The VAD prevalence among 6 months to under- five children is 8.2%, which is slightly lower, compared to the 1993 survey data of 10.4%. The prevalence rate of deficient to low plasma retinol among the same age group is 38%, which is higher compared to the 1993 data of 35.3%. VAD prevalence among 6 months

8
to 5 years old children is a public health problem in all 16 regions of the country, which ranged from 25.9% in Ilocos region to 54.6% in Western Mindanao region. Same FNRI report shows that iron deficiency anemia is still prevalent among under-five year children. Three out of ten children has iron deficiency anemia. Regional disparities are noted. Regions I, II, III, V, VI, VIII, IX, X, XII and ARMM have higher IDA compared to the national average of 31.8%. The prevalence of IDA is observed to be declining as the child grows older (figure 9). The prevalence rate is highest among infants six months to one year at 56.6% and it is lowest among five-year-old children at 18.2%. This implies the influence of maternal health to child’s health as shown by iron deficiency anemia of pregnant women and lactating women at 50.7% and 45.7% respectively. Figure 9 shows the declining trend of IDA, as child grows older. Childcare and health-seeking behavior Breastfeeding and complementary feeding practices The Department of Health promoted three breastfeeding practices, which are early initiation within an hour after delivery, exclusive breastfeeding up to six months and extended breastfeeding up to two years. The 1998 NDHS report shows that early initiation of breastfeeding within an hour after birth occurred in 41% of newborns while 79% occurred within 24 hours. Twelve percent of children born five years before the survey were never breastfeed. The 2002 MCHS report revealed that the reasons for not breastfeeding were insufficient milk (33%), nipple/ breast problem (20%), mother working (16%), child refused (11%) and mother ill or weak (%).
The mean duration of exclusive breastfeeding in the Philippines is very short for only a month and half. Figure 10 shows decreasing trend of exclusive breastfeeding practices among under-six months old infants from 1998 to 2003 NDHS. The decreased by age group in months ranged from 4-5 percentage points. The improvement of exclusive breastfeeding practices in 1998 compared to the 1993 survey is mainly due to the successful implementation of the Mother Baby Friendly Hospital Initiatives and the monitoring of the compliance to the Milk Code by the Department of Health. In 1999 to present, turnover of national program managers and lack of evidence of monitoring of the Milk Code compliance have affected breastfeeding practices except in regions where coordinators are strong advocates of breastfeeding. The mean duration of breastfeeding is thirteen months and children in the rural areas are breastfed longer by ten months that those in the urban areas. Children whose mothers have no or little education are breastfeed three times longer than those whose mothers have college education. During focus group discussions of Badjao mothers in Cebu City and Muslim mothers in Tokawal, Alabel, Sarangani responded that they have no choice except to breastfeed since they cannot afford to buy milk formula. This is of course an incorrect reason. Mothers whose deliveries are attended by traditional midwives breastfed longer than those mothers whose deliveries are assisted by medically trained personnel.

9
The duration of postpartum amenorrhea is affected by both the duration and frequency of breastfeeding. LAM can be promoted by promoting exclusive breastfeeding up to six months. Complementary feeding starts very early in the Philippines as shown by the 1998 NDHS report that less than two months old babies are given complementary food. The same report shows that among the 7- 9 months old infants, 1.3% was still given breastmilk only, 66% were given grain, flour and eggs while 55% were given meat / fish, and 35% were given tubers. Focus group discussions of mothers in selected barangays of Muntinlupa, Cebu City, Minglanilla, Cebu and T’boli, South Cotabato revealed that most of them gave only rice porridge and vegetable soup during weaning period at 6-7 months. Health seeking behavior The 2003 NDHS report shows that only 46.3% of children under-five years old with symptoms of acute respiratory infection- cough and rapid breathing sought treatment from any health facility or provider. Forty four percent of children with cough and rapid breathing were treated with antibiotics while 49% were given cough syrup. Cough syrup is no longer necessary in the treatment of acute respiratory infections. On the other hand, only thirty two percent of children with diarrhea is brought to health facility and about 59% of diarrheal cases is given ORS / recommended home fluids and increased fluids. All children with cough and rapid breathing need treatment and most diarrheal cases can be managed at home with increased fluids and continue feeding. Figure 11 shows the diarrhea case management of families based on the Oral Rehydration Therapy protocol, which is increased fluids, continue feeding and fast referral of diarrheal patients. The graph still shows poor family practices of home management of diarrhea. ORT can reduce half of the deaths due to dehydration. Maternal and Child Health Services and Programs Maternal Health Services The differences in MMRs between the developed and the developing world could be traced to wide differences in maternity services. While the coverage of antenatal care, skilled attendance at delivery and postpartum care are all above 90% in developed countries, the coverage of these services are less than 65% in developing countries, figure 12. The latest DOH reports (FHSIS 2000) confirm the low coverage levels of maternal health services, table 3. Only 64.8% of pregnant women had 3 or more prenatal visits and 62.5% received tetanus toxoid vaccination during these visits. The coverage of postpartum women visited at least once is 74.6%. Of 1.7 million deliveries reported in the Philippines in 2000, 40.7% were delivered by professional midwives, 26.8% by physicians and 1.5% by nurses, table 4. More than 500,000 deliveries (or 30.5%) were still attended by

10
traditional birth attendants. Most of the reported births were normal, spontaneous vaginal deliveries (99.5%) and almost 70% of these occurred at home, table 5. The 2003 NDHS, on the other hand, shows that coverage for antenatal care varies significantly by region, urban-rural residence, age, birth order and educational level. ANC coverage is lower among women in rural areas, women age 35 and older, those in the higher order births, and women with less or no education. ARMM had the lowest coverage (50%). All the other regions have at least 77% ANC coverage. The survey also shows that the percentage of births delivered in a health facility increased over the past decade from 28% in 1993 to 34% in 1998 to 38% in 2003. Delivery in a health facility was less in rural areas (22%) than in urban areas (54%). In ARMM, Zamboanga and MIMAROPA, less than 20% of births occurred in a health facility. Mother’s education was a strong factor in the place of delivery. 69% of educated women (college or higher) delivered in health facilities while only 4% of the less educated women delivered in a health facility. The percentage of births attended by a health professional increased from 53% in 1993 to 56% in 1998 and to 60% in 2003. The percentage in urban areas (79%) was about twice that in rural areas (41%). Regional differentials are also wide with ARMM consistently having the lowest (22%) and the National Capital Region, the highest at 88%. Except for the provinces targeted for WHSMP2, there is limited information on the allocation of health resources and maternal services such as referral facilities for surgical obstetrics and emergency care that could be matched with the maternal and perinatal mortality and morbidity indicators in the areas. Maternal Care Programs Promoting maternal health would entail a multidisciplinary approach. The barriers to women’s health include economic, legal, social and cultural obstacles. The Safe Motherhood initiative summarizes key programmatic priorities into 10 action messages, annex A. The international community has committed to the development of clear and comprehensive national strategies to “ensure universal access to all individuals and couples of appropriate ages throughout their life cycle to a full range of high quality, affordable sexual and reproductive health services, which includes family planning, through the primary health care system as soon as possible, and no later than the year 2015, with particular attention to maternal and emergency obstetric care, particularly in underserved areas”. They community agreed “to establish or strengthen integrated safe motherhood programs, within the context of primary health care, with goals and targets to reduce maternal mortality and morbidity by one half of 1990 levels by the year 2000, and by a further one half by 2015”, to include services such as:
• Education on safe motherhood • Promotion of maternal nutrition • Provision of micronutrient supplementation and tetanus toxoid, where appropriate • Prenatal care and counseling

11
• Adequate delivery assistance, in all cases by a skilled person, without excessive recourse to caesarean sections
• Care for obstetric emergencies, including referral for pregnancy, childbirth, and abortion complications
• Postnatal care • Abortion-related care, including compassionate counseling and reliable
information for women who have unwanted pregnancies, humane counseling and treatment for women who have had recourse to abortion and sage abortion where not against the law
• Family planning counseling, information and services, and promotion of longer intervals between births
• Neonatal care, including exclusive breastfeeding for six months The initiatives current focus on efforts to improve the quality of maternal health services and access to these services, especially access to skilled attendance at birth. Access to skilled “attendance” is very much differentiated from mere access to a skilled “birth attendant”. Access to skilled attendance means access to a skilled health provider within a supportive environment that includes adequate supplies, equipment, infrastructure, an efficient and effective system of communication and referral/ transport, partnership among skilled attendants and emergency obstetric care. In October 1999, the interagency committee on Safe Motherhood launched a multi-step strategy to assess the importance and potential impact of skilled care during childbirth as a means of reducing maternal mortality, with the key components of gathering epidemiological evidence, continuing consultations and analysis of these data, and wide dissemination of information in order to assist the countries in developing their national plans of action. They are also monitoring the achievements of developing countries in terms of increasing coverage and reduction in maternal mortality. The outputs of these efforts are now being felt. At the technical level, WHO has released several studies evaluating the real benefits of antenatal care (ANC) and has proposed a new ANC model. Table 6 summarizes the antenatal interventions currently known to be effective. The new WHO ANC model focuses on appropriate actions to assess and manage specific problems and conditions during pregnancy rather than on risk scoring. Using the new WHO ANC model, the health provider classifies the mother during the first visit as either suitable to follow the basic ANC component or someone needing higher level of care. This assessment is reviewed at each subsequent visit. Appropriate referral to higher-level services and back referral to basic services is also included in the new model. The forms and activity checklist at each visit is attached as annex B. As much as 15% of deliveries are expected develop obstetrical emergencies even though the pregnancies did not seem to be complicated during antenatal. Thus, aside from good quality antenatal care with high ANC coverage (which is estimated to prevent 26% of maternal deaths), clean and safe natal with active management of the third stage of labor through timely and appropriate emergency care will also be necessary to prevent maternal

12
and fetal deaths. Emergency obstetric care is estimated to prevent 48% of maternal deaths. Emergency services are classified as basic or comprehensive services. Basic emergency obstetric care (BEmOC), in addition to the capability to handle normal spontaneous vaginal deliveries and provide routine newborn care, includes the ability to recognize, stabilize and manage the majority of obstetric complications that arise and threaten the life of the mother and her unborn child and do procedures that can be performed on site such as assisted vaginal delivery, manual removal of the placenta, evacuation of an incomplete miscarriage and basic neonatal resuscitation, annex C. Comprehensive emergency obstetric care (CEmOC), in addition to BEmOC, includes the ability to perform surgical obstetric care in an operating room, administer blood transfusion, and provide intensive neonatal care, annex D. To ensure timely emergency obstetric services, efforts to reduce the factors that cause delayed referral are also emphasized. About 3 major causes of delays in referral have been focused on:
1. Delay in recognizing the danger signs and decision to seek emergency care 2. Delay in the woman’s arrival to the emergency care facility 3. Delay in her treatment at the health facility
To reduce the delay in recognizing the danger signs of obstetric complications and in deciding to seek emergency care, efforts are geared towards training of traditional birth attendants and the women and their relatives. UNICEF’s East Asia and Pacific Regional Office Strategy Paper on the Reduction of Maternal Deaths in East Asia and the Pacific (draft) noted the need to promote facility-based deliveries – whether these are complicated or not - in countries and areas with adequate number of skilled birth attendants and adequate health facilities. To reduce delays in bringing the woman to the health facility, maternity waiting homes have been established where the women nearing their term could stay for a few weeks before and after delivery. To avoid delays in treatment when the woman has arrived in the health facility, efforts to improve standards and quality of services at the emergency health facilities are also being emphasized. Postpartum services are also important to prevent, detect and manage postpartum problems. Preparation for childcare and delivery of family planning services are essential at this stage. Detection and treatment of genitourinary infections and injury could prevent long-term morbidities and conditions. In many instances, the women need to be rehabilitated nutritionally, physically and emotionally. Maternal and neonatal mortality and morbidity reviews are also being conducted to monitor the improvements in the services.

13
Policies, training content and methods and systems of planning, allocation of resources and program and information management, among others, need to be reviewed, updated and widely disseminated to create the supportive environment very much needed to achieve the overall impact that will improve maternal health. National efforts have closely followed international initiatives. WHO has listed the following as the ten most important achievements of the Philippine Maternal Health program:
• Establishment and/ or upgrade of maternity waiting homes, birthing homes and lying-in centers in 25 provinces through the Women’s Health and Safe Motherhood Project Phase 1, with national guidelines on maternity waiting homes and birthing homes
• Training of first level referral physicians in emergency obstetric care • Distribution of clean-and-safe delivery kits • Advocacy on clean and safe delivery, with the 2nd week of May declared as
national Safe Motherhood Week • Inclusion of non-hospital, low-risk pregnancy in the maternity package of the
Philippine national health insurance • Training and promotion on the use of the Partograph for facility and non-facility
deliveries and its inclusion in the nursing and midwifery curricula • Formulation of Sentrong Sigla service quality standards for Safe Motherhood • Introduction and pilot-testing at the community level of the manual on “Essential
Care Practice Guide” • Development of training guidelines for the manual “Managing Complications in
Pregnancy and Childbirth: A Guide for Midwives and Doctors” and training of obstetrician trainers at the regional level
• Development and pilot-testing of a Mother-Baby Book, an integration of the Home-Based Mother’s Record and the Growth Monitoring Chart
In collaboration with WHO and the Asian Development Bank and other partners, a Philippine National Safe Motherhood Action Plan was formulated for 2001 - 2005. Its goal is to ensure that mothers and infants survive pregnancy and delivery. The objectives are to:
1. To reduce maternal mortality ratio to 86 deaths per 100,000 live births by 2004 2. To reduce the proportion of newborns with low birth weight to 12% of live births
by 2004 3. To reduce neonatal mortality rate to 3 per 1,000 live births (baseline 7.8 per 1,000
live births, 1994 Phil Health Statistics) The strategies listed are:
1. Mobilize and empower families and communities to recognize pregnancy complications and prevent maternal deaths
2. Improve first level referral capacities 3. Ensure adequate number of skilled attendants at delivery at all levels 4. Improve access to quality health and nutrition services

14
5. Focus on health promotion, education and advocacy 6. Establish linkages and develop collaboration with local governments, NGOs,
other government organizations and the media 7. Map health facilities and conduct inventory of personnel down to the barangay
level 8. Adopt a reproductive health approach with emphasis on family planning 9. Conduct rapid assessment of maternal mortality and morbidity 10. Conduct operational research on the use of the Partograph
The activities include policy development, advocacy and consultation to raise political commitment, maternal mortality audits, upgrading of health facilities, training and development of courses and modules, pilot studies, monitoring and evaluation, research, and IEC activities. The second Women’s Health and Safe Motherhood Project (WHSMP2) has been proposed to follow through the initiatives in maternal care. The new project incorporates the new directions and technical guidelines of the international inter-agency committee on Safe Motherhood. Focusing initially on two provinces and one city (Sorsogon, Surigao del Sur and Iloilo City), and later on 3 additional provinces (Eastern Samar, Mt. Province and Agusan del Norte), the project has the following development objectives:
1. To increase the access of disadvantaged women of reproductive age to acceptable, high quality and cost-effective reproductive health services and to enable them to safely attain their desired spacing and number of children
2. To assist in the development and implementation of sustainable systems within the framework of the Health Sector Reform Agenda for financing and delivery of reproductive health services
The project strategies are specified for target sectors and programs articulated as sets of interventions and support systems and specific actions. Service packages are also defined for maternal and newborn care, family planning, HIV/STI prevention and control, and adolescent reproductive health. The project implementation mechanism emphasizes the organization of functional teams at various levels:
1. The Women’s Health Team (WHT) at the BHS/ health center and community level composed of the rural health midwife, the traditional birth attendant (TBA) and the barangay health worker (BHW). This team is expected to act together to identify the pregnant women early during their pregnancy, provide ANC, advocate for a facility delivery, provide the Mother-Baby Book, counsel on a birth plan that includes provisions for emergencies such as transport, financial arrangements, recruitment of blood donors, or arrangement into a maternity waiting home. The team will also provide counseling on family planning, STIs, and newborn and childcare such as breastfeeding, nutrition, hygiene and immunization, among others. The same team will provide routine postpartum check-up. The TBAs will be encouraged to just assist in deliveries and other

15
maternal health services. The WHT will be linked to a physician for referral of complications.
2. The BEmOC Team or the Basic Emergency Obstetric Care Team at the rural
health unit or the district hospital, in addition to the capability to assist in normal spontaneous vaginal deliveries and provide newborn care, will be able diagnose and manage referrals for complications. This team will have parenteral antibiotics, oxytocics and anti-convulsants. The team should also be able to do assisted vaginal deliveries and manual removal of the placenta and other retained products. This team should also be able to diagnose and treat STIs and fetal complications and do newborn screening. This level will have to meet quality standards of care under Sentrong Sigla and would be using the partograph. Physical examination for anemia, diagnosis and management of infections and emotional problems will also be provided at this level.
3. The CEmOC Team or the Comprehensive Emergency Obstetric Care Team
at the district, provincial or regional hospitals and medical centers with operating rooms, and composed of an OB/ Gyne specialist or a General Practitioner with OB training, anesthesiologist or GP with anesthesiology training, operating room nurses or surgical midwife, and medical technologist, would be capable of surgical obstetrical procedures such as caesarean deliveries. Blood and other supplies should be sufficient at this level. The CEmOC team will also have the capability to provide Neonatal intensive care.
All the teams will be able to provide supplemental micronutrients such as iron and vitamin A, tetanus toxoid and infant vaccinations, anti-TB treatment. At the supporting levels, the causes for the 3 delays to maternal care will be reduced through various approaches that include training, advocacy and health education, among others, at various levels. The main project inputs will be include service delivery infrastructure (civil works and machineries/ equipment including waste management), LGU capability building, seed funding for supplies and services, project management, behavior change and communication, social assessment, blood supply, human resource development and monitoring and evaluation. Child Health Services and Programs Expanded Programme on Immunization (EPI) Expanded Programme on Immunization Disease Reduction Initiatives. The Philippines as one of the countries in the Western Pacific Region was declared polio free in October 2000. The country is now on the sustenance phase of polio eradication until global certification in 2005 wherein Polio coverage should be maintained at 80% per barangay and strengthen AFP surveillance system.

16
Philippine Measles Elimination Campaign ( PMEC) has four strategies: 1) Catch Up mass vaccination of children 9 months to less than 15 years old; 2) Keep Up strategy which is improving progressively routine vaccination coverage; 3) Follow-up mass vaccination of children 9 months to 59 months every 4-5 years; and 4) strengthened laboratory based measles surveillance. PMEC was launched through the Measles Catch Up campaign in September 1998 with twenty six million children 9 months to less than fifteen years old vaccinated against measles. Laboratory based measles surveillance was initiated in the same year and expanded to the whole country the following year. Follow Up campaign was done in February 2004 with measles vaccination coverage of 94% or 17.2 million children 9 months to less than eight years old. The Department of Health validated the reported coverage through a rapid coverage survey and result was 96% of targeted children were vaccinated. This could be probably due to the overestimation of eligible population in the rural areas.
The Department of Health in collaboration with WHO / UNICEF / POGS / PPS and others formulated a maternal and neonatal tetanus elimination program. It aims to eliminate neonatal tetanus by end of 2008. To date, the DOH is on the validation process of identifying high risk areas for tetanus neonatorum. The high risk areas will conduct mass tetanus toxoid immunization for women of reproductive age group 15-49 years old.
Status of Fully Immunized Children. Figure 13 shows a slight decreased in the percentage of fully immunized children from 62% in 1993 to 60% in 2003 but decrease is higher in 1998 at 65% to 60% in 2003. This could be explained that in 1999- 2002 there was irregular and inadequate vaccine supply as a result of DOH procurement problems coupled with global shortage of vaccine supplies. Republic Act No. 8980 of The ECCD Act/Law provides that the Department of Health will provide 100% of the vaccine requirement for EPI. This will ensure that adequate vaccines will be made available to all LGUs in the country for EPI. Children completely immunized is at 70% which is higher compared to the FIC status of 60% which means that 10% of children were given the complete antigen after 12 months of age. Access to the immunization services is high in the three National Demographic Health Survey of 1993,1998 and 2003 as there were 91% of 12-23 months old children who received BCG, which is the first antigen. It was noted in the report that there was less access to immunization in ARMM ( 71%) and Zamboanga Peninsula ( 76%). Access to immunization services was very high in NCR, Ilocos Region, MIMAROPA, Bicol and CARAGA at 94%. Measles coverage is 80% and this is the last antigen given to children 9- 11 months old children so the drop out rate was at 12%. Focused group discussion / interviews of City Health Officer / technical staff / RHU personnel / BHWs / BNS and mothers in Cebu City and Minglanilla, Cebu revealed that they consider EPI as the best and effective intervention. It is because parents demand services from health facilities
The 1998 NDHS report shows a relationship between mothers’ education and complete immunization of their children. Children whose mothers’ education are college or higher are most likely to get complete immunization than mothers with no education or had

17
elementary education. This is shown in Figure 14. In addition, full immunization has a direct relationship with the education of mothers since the drop out of mothers with college or higher education was only 8% compared to the 14% among children whose mothers have elementary education. Micronutrient Supplementation
Vitamin A supplementation – NDHS 2003 - 76% of 6-59 months old children received vitamin A in six months preceding the survey. Children in urban areas (80%) are likely to receive the supplements as compared to those children in the rural areas (70%). Regional disparities are noted where NCR, Central Luzon and Calabarzon have more than 80% of children receiving the supplements ARMM, Bicol and Zamboanga Peninsula have below 65% of children who received Vitamin A.
A 2003 HKI Survey report on vitamin A coverage of regions I, II, V, VIII, IX, X, XI, XII, and ARMM shows that the Vitamin A coverage is 92.1% among children 12-59 months. Table 7 shows that among 40 MOST / USAID/ HKI assisted provinces, 78% or 31 have a coverage of 90% and above. Among the 21 cities, only 57% or 12 cities had 90% and above coverage for Vitamin A among 15-59 months old children.
There is a strong relationship between mothers’ education and Vitamin A supplementation. Eighty five percent of children whose mothers with college or higher education received Vitamin A while only 37% of children whose mothers have no education received Vitamin A, figure 15. Iron Supplementation. The DOH Guidelines on Micronutrient Supplementation require iron supplementation for low birth weight babies to start at two months up to six months; for 6-11 months old children for three months; and for anemic and underweight 1-5 years old children iron supplementation is daily for three months or 30 mgs once a week for six months. The 2002 MCHS report shows that about 73 percent of children 6 months to 59 months were given iron drops or syrup. Children in the urban areas are more likely to get the iron supplements than those in the rural areas. The report does not specify if these children had completed the iron dosage required. Efforts are geared towards the implementation of the Food Fortification Act that mandates the fortification of rice and flour with iron. Universal Salt Iodization. The Philippine Government enacted ASIN Law in 1995 to virtually eliminate the prevalence iodine deficiency disorders. The 1998 FNRI-DOST survey results revealed a wide gap between awareness at 67.3 per cent and iodized salt utilization at 24.8 per cent. The most common reasons for non-use of iodized salt was its non-availability (45%) and unaffordability of the product (23%). The 1999 MICS report shows that only 22.4 per cent of households use iodized salt for the whole country. In 2001, HKI Post Garantisadong Pambata (Preschoolers’ Week) coverage survey revealed a proportion of 27.5 per cent of households use iodized salt in nine regions. The same report revealed that Nueva Viscaya was the first province to achieve USI at 91 per cent. The HKI 2003 survey report of 9 regions is very promising since the proportion of

18
households using iodized salt ranges from 48.5% in ARMM to 94.65% in region II. Figure 16 shows the marked increase of the proportion of households using iodized salt in 2003 compared to 2001. There are four regions- I, XI, VIII and XII that achieved universal salt iodization. Despite the mark increased in household using iodized salt, ARMM is still below fifty percent – 49%. Since the enactment of the ASIN Law, progress in USI was very slow up to 2001. In 2003, there was a marked increase in households using iodized salt. This is attributed to the increased availability and affordability of iodized salt not only in the markets but also in sari-sari stores, figure 16. This is a result of the DOH leadership to consider USI as one of the top priorities starting in 2002. Patak sa Asin was launched in October 2002. This is a quarterly monitoring of salt at the warehouses of salt producers / importers, markets and sari-sari stores. CHD directors are actively involved after the DOH secretary met all of them and discuss action steps to accelerate USI. Food Fortification. The implementation of the Philippine Food Fortification Act of 2000 or Republic Act 8976 has been accelerated through the assistance of the MOST – Micronutrient Project of USAID. A National Advocacy Plan for Food Fortification and Supplementation has been developed which will complement the food fortification communication plan that is scheduled to be implemented in November 2004. A memorandum of agreement has been signed recently between the Department of Health and Department of Agriculture to further strengthen the rice fortification in 2004. Integrated Management of Childhood Illnesses In developing countries, seven out of ten childhood deaths can be attributed to five main causes or often a combination of pneumonia, diarrhea, malaria, measles and malnutrition. In the Philippines, HIS report in 1996 reveals that five out of ten deaths among under-five were due to pneumonia, diarrhea, malaria, measles, dengue hemorrhagic fever and malnutrition. This data could be underestimated as this is based on reports of health centers since deaths are registered by place of occurrence. Most sick children present signs and symptoms related to more than one or more of these illnesses. Therefore, an integrated approach to managing sick children is indicated to address more effectively the combination of factors that threaten child health and consequently their growth and development. The 1993 World Bank Development Report, Investing in Health, ranked IMCI as one of the ten most cost effective interventions with the potential to have the greatest impact on the global burden of disease in low and middle-income countries. Integrated Management of Childhood Illness, developed by WHO / UNICEF is a strategy to reduce death and frequency and severity of illness and disability in children and to contribute to improved growth and development. It includes a range of interventions that includes curative care of improved case management of childhood illness and preventive aspects of nutrition, immunization, vitamin A supplementation, disease prevention and health promotion. IMCI has three components: 1) improvement in the case management of skills of health staff; 2) improvement in the health system required for effective management of

19
childhood illness; and 3) improvements in the family and community practices. The first two components focused in improving the quality of child health services at the health facility while the third component addresses preventive and caring practices of families and communities.
The DOH Child Survival Program – USAID assisted project developed in 1989- 1991 a manual on integrating services for mothers and children. IMCI is one of the strategies to operationalize the framework which does not only treat a sick child but broaden its approach to consider and respond to different factors contributing to his / her illness. The family and community component stresses not only preventive and home case management of the child but also maternal health and home environment that will promote conditions of giving the child the opportunity to survive, grow and develop to the fullest potential.
IMCI Introduction Phase. In June 1995, The Philippine Department of Health had an initial discussion on IMCI as a component of the Early Child Development Project, an ADB- WB project. In early 1996, DOH taskforce composed of the different program managers and technical staff of the concerned offices with the Philippine Pediatric Society and the Research Institute of Tropical Medicine started to adapt the IMCI generic guidelines of WHO / UNICEF. Adaptation was a long process since two major changes had to be made: 1) malaria situation of the country does not warrant inclusion of high malaria risk, presence of P. falcifarum / vivax and policy of blood smears for diagnosis at RHU level; and 2) inclusion of Dengue Hemorrhagic Fever as this is a social concern and increased trend was noted. The IMCI model course was conducted in 14-25 July 1997 to develop a pool of trainers and to pretest the modules. This course was participated by 7 national DOH program managers, 5 pediatrician from ATUs / DTUs, 4 from regional offices of IX and XI, 1 WHO and 1 UNICEF. After the course modules were finalized and printed and IMCI was piloted in Zamboanga Norte and Sarangani in 1997.
IMCI Expansion. DOH / WHO / UNICEF review report in May 1998 recommended its expansion. The expansion was approved as long as the academe will conduct the 11- day IMCI basic course. DOH conducted a consultative workshop with selected medical / nursing/ midwifery institutions to mobilize these institutions to conduct IMCI training. Unfortunately, the academe was not ready to conduct the training since the number of days required for them to be trainers is 17 days then for every training that they conduct will mean absence for 10 school days and nobody will pay for their salaries. Therefore, it was agreed that regional offices of IX and XI would conduct the training of facilitators for other regions. Component I: Improving case management skills of frontline health workers on IMCI. Training capability of CHDs and selected provinces and cities. All CHDs have training capability for IMCI except IV-A and IV-B. UNICEF provided funds to DOH for training of IMCI facilitators for all CHDs except Ilocos and Central Luzon regions and twenty CPC V provinces and five cities in 1999 and 2000. UNICEF provided training equipment to 14 selected hospitals designated by DOH as IMCI training sites. In October 2000, HKI
20
/ USAID project conducted training on the 11 day basic course and facilitators’ training for Region 1, III, X and XI and project areas.
Training of frontline health workers. The main training methodology is an 11-day course that consists of sixty nine hours for classroom teaching and thirty two hours for clinical practice in hospitals and health centers. Training of frontline health workers were supported by projects namely the UNICEF assisted - Fifth Country Programme for Children, World Bank assisted Early Child Development Project and the HKI/USAID project. Mati City of Davao Oriental is the only reported LGU who provided funds for IMCI training. There is a limited number of health facilities providing IMCI services due to the high initial investment required for training for the IMCI basic course.
ENRICH – a USAID assisted project has an IMCI training component in selected areas of ARMM. UNICEF and ECD continue to support component I.
IMCI On the Job training is an alternative methodology for IMCI training of frontline health workers. It was piloted in Sarangani province in the municipalities of Kiamba and Malapatan. The methodology was reviewed by DOH / WHO / UNICEF / HKI / CRS and guidelines were formulated for adoption. Guidelines include a 10 day modular training for three weeks at the main health center or district hospital with a suitable training area and 3 days clinical sessions in DOH accredited IMCI training hospitals; 1 facilitator per 2-3 participants; participant handles a minimum of 20 cases; course director should come from the province and all other requirements of the 11 day course are followed. Advantages of this methodology based on Sarangani experience are; least cost at P7,000 per participant compared to the 11 day basic course of P20,000; participants are in their own municipalities; facilitators are immediate supervisors of the participants so it will assure follow-up of participants after one month and three months and thereafter to reinforce skills of midwives. On the other hand, the disadvantages are quality assurance, changes in the scheduled 10 days due to interference of local activities and lack of IMCI cases in less populated municipalities. Most of the MHOs in Sultan Kudarat preferred to be trained on this methodology as they do not want to be out of the province for two weeks. IMCI Pre-service training. As a long-term interventions, the DOH with WHO and UNICEF had a meeting with the major stakeholders for the IMCI integration into the nursing and midwifery curricula. As a result of the meeting, an organized IMCI Pre-service Task Force was organized which is composed of the Department of Health, Professional Regulation Commission- Board of Nursing and Midwifery, Association of Deans of Philippine Colleges of Nursing, Association of Philippine Schools of Midwifery, Commission of Higher Education, WHO and UNICEF. In 2002, DOH through UNICEF assistance, conducted two batches of 11-day IMCI course for the academe. The participants are from 8 Centers of Excellence of Nursing and Midwifery Schools based on the accreditation of the Commission on Higher Education and the Association of Deans of the Philippine Colleges of Nursing and Midwifery Association. The capability building is to prepare them in modeling the IMCI Curricula integrated in the nursing and midwifery. The trained 36 participants started the implementation of the

21
integrated curricula during the second school semester of 2002-2003. Modeling of the integrated curricula is on going and review is planned for this year. On the other hand, discussions and meetings are going on for the integration of IMCI into the medical curricula. A survey of 22 medical schools all over the country shows that only 33% or 13 have fully or partially integrated IMCI into their curricula. Reasons cited include lack of IMCI trained faculty members, limited information of IMCI in the hospitals, perception of some faculty that IMCI is for community implementation, lack of opportunity to integrate in tertiary hospitals, inadequacy of strategies for integration and lack of funds. HKI and DOH conducted an assessment of the IMCI strategy implementation in selected project provinces of Regions I, III, X and XI. The study concluded that IMCI trained workers adopted the IMCI strategies but there were deficiencies in the assessment, classification and treatment of childhood illnesses. Almost 90 percent of children’s illnesses were not properly treated due to incorrect assessment and classification. This could be a problem in the quality of training, limited follow-up of trained personnel (only 55% were followed-up after training) and lack of supervisory skills and supervision by MHO / PHN. IMCI trainees are expected to be followed up one and four months after training. HKI- IMCI Monitoring report showed that trained midwives have a sense of empowerment in their ability to assess and manage a sick child and most of them use the standard approaches although a few did not practice due to large volume of patients and lack of confidence in the use of IMCI and clients were satisfied since their children are assess thoroughly. MICS / IMCI rider in Sarangani in 2000 revealed that almost all mothers were satisfied with the child health services in health facilities. To date, Sarangani province is the only province of the country where 95% of health personnel are trained on IMCI and 80% of health facilities are providing IMCI services. This is because Sarangani was the pilot province for IMCI and this is a UNICEF assisted LGU.
Component II: Improvement of health systems Improvement of health systems include drug availability, IMCI planning and management, organization of work at health facility, supervision, referral, health information systems and health sector reform. In the Philippines, the Department of Health with the assistance of WHO / UNICEF / HKI at the national level focused on setting up of standards and guidelines by developing a Manual of Operations. The manual is now edited to make it user friendly at all levels from policy to implementers. In HKI-USAID assisted and UNICEF project areas, at LGU level, IMCI has improved drug availability, strengthened supervision and referral system and improved work organization health facility. HKI has developed and pre-tested a training module for IMCI monitoring and supervision. Based on the HKI monitoring report, most of the health facilities monitored have clinic space and equipment although infant weighing scales, pediatric arm cuff and sterilizer were not available; most had cotrimoxazole, amoxycillin and paracetamol but did not have iron supplements, low dose of Vitamin A and anti-malaria drugs.

22
Component III: Improvement of family and community practices. This component works with families and communities to improve their ability to improve health of children and prevent health problems, to care for sick and well children and to decide when to avail of health services. One of the principles of the IMCI family and community component is built on existing community health activities. In the Philippines, it evolved from the child growth project of HKI /UNICEF / AusAID in 1995. The project addressed the malnutrition problem by regular growth monitoring, Vitamin A supplementation and improving breastfeeding, complementary feeding and feeding practices through training of rural health midwives and community volunteers on counseling, establishment of weighing posts and conduct of caregivers’ class. In 1997, in respond to the demand of mothers and recommendation of the project, the strategy was enhanced by expanding the health practices to maternal care, psychosocial care of children and environmental sanitation. The weighing posts are now called health and nutrition posts to indicate a comprehensive health care services for mothers and children. In 1998, the enhanced child growth strategy was modeled in Zamboanga Sur. The Fifth Country Programme for Children 1999-2003 – UNICEF assisted project expanded the strategy in CPC V areas. RHU personnel, BHWs and mother volunteers were trained on ECG Counseling on the 12 family practices. ECG Counseling Cards were provided to trained personnel to serve as IEC tools for counseling caregivers. Rapid appraisal in 2000 in Sarangani province revealed significant difference in health practices of those communities with health and nutrition posts compared to those without posts. Focus group discussions of mothers done by DOH during the CPC V midterm review in selected areas have also revealed among others improved nutritional status of children, higher Vitamin A supplementation, high utilization of iodized salt, high percentage of prenatal with 3 or more prenatal visits, high percentage of households with sanitary toilets, high exclusive breastfeeding infants, all mothers participate in community activities and all children were weighed monthly. In 2001, HKI in coordination with DOH and UNICEF, the ECG Counseling Cards was improved to include the fast referral of sick children and home case management. These cards, the Integrated Counseling for MCH, are tools utilize in the promotion of 14 family practices. This IMCI family and community component are adopted in project areas of UNICEF / ECD / HKI-USAID.
In the province of Sultan Kudarat, health and nutrition posts are utilized for Reproductive Health services while in some of the posts of Sarangani, follow-up of pill acceptors and TB cases is integrated into the health and nutrition activities. In Agusan Sur, some health and nutrition posts are utilized also for other purok activities. Caregiver functional literacy is a strategy of teaching caregivers how to read, write, compute simple arithmetic and learn about maternal and child health. The Department of Education and Department of Health with the assistance of UNICEF under the Fourth Country Programme for Children developed a facilitators’ guide and learners’ guide as IEC tools for the strategy. In CPC V, the content and methodology has been enhanced. Evaluation of CFL in Mountain Province and Bukidnon revealed that CFL had developed
23
their skills in reading, writing and numeracy and their self-esteem is enhanced. It is a powerful strategy to foster assertiveness of women in marginalized communities, in their health caring and seeking behavior, accessibility to IEC materials and health services through acquisition of skills in reading, writing and simple arithmetic. After interviews and focus group discussions among T’bolis and Muslim women, Undersecretary Milagros Fernandez of DOH mobilized projects, regional directors, provincial and city health officers of Mindanao to adopt the Enhanced Child Growth and caregiver functional literacy strategies. The 2000 Sarangani Multiple Cluster Survey (MICS) IMCI rider detected improved case management skills of frontline health workers as perceived by 86% of mothers surveyed. A 2003 desk review of IMCI implementation in Sarangani Province noted the following:
• 85-90% of caregivers interviewed can recall correctly home treatment and instructions given to them
• Reduced 2003 under-five deaths due to pneumonia, measles, diarrhea, malnutrition and malaria
• Reduced proportion of under-five deaths to total deaths • Improved nutritional status based on the result of 2003 Operation Timbang
(81% of under-six years old children had normal weight for age (International standards) compared with 68% in 2000)
• Improved health systems, specifically increased drug availability, referrals, service and organizational systems, and monitoring and supervision
The same review noted improved key family practices through training of community volunteers on integrated MCH counseling and increased access to health by establishment of health and nutrition posts in hard to reach areas, and among marginalized communities. The HKI / USAID IMCI project reports recommended the expansion of IMCI Early Childhood Care and Development The Act Promulgating a Comprehensive Policy and National System Law for Early Development or otherwise known as The ECCD Law was enacted in December 2000. The National ECCD System aims to enhance the physical, social, cognitive, psychological, spiritual and language development of young children. President Gloria Macapagal-Arroyo issued Executive Order No. 286 on 23 February, 2004, directing national government agencies and other concerned agencies to actively support and implement programs on the “Bright Child”. The Bright Child is the brand that will refer to the package of interventions on food and nutrition, health, early education, and psychosocial programs for young children that are expected to result in their optimum growth and development. Drafts have been developed focused on children 3-year and above. These drafts need enhancement to include the ECCD component for the unborn and the under-3 years old. Figure 19 illustrates strategies for child care.

24
Summary of Current Issues, Needs and Challenges in Maternal and Child Health Maternal Care In addition to data collection and analysis, interviews and focus group discussions with key informants at various levels of the DOH, the LGU and partner agencies were conducted to determine the needs, challenges and suitable interventions perceived by these groups. Visits to ongoing projects, especially those deemed to be most successful were also done in regions with varying levels of overall program performance. FGDs were also conducted among community leaders, BHWs and parents. Urban, rural and tribal communities were included. Experiences and insights on successes and failures at all levels were also gathered. Based on all these methods, the following are current major challenges and needs in maternal care: Policies, standards and guidelines Since the devolution of health services in 1993, there have been many problems in maintaining functional links that allow the smooth flow and feedback on policies, standards and guidelines among the various health offices and organizations of the DOH central office and local government units. Various reasons are listed in the 2004 MSH project completion report of the Integrated Family Planning and Maternal Health Program (IFP-MHP). This problem is most important to the maternal care since many of the innovations and new directions have only recently been formulated globally. National systems for in-depth policy analysis, testing and discussion have not been optimum. National strategies and action plans have not been widely disseminated or are not yet clearly understood. Orchestration and leadership at the national and regional levels need stronger support and assistance. Difficult policy issues such as the phase out or changing of the roles of TBAs need more thorough study and field testing to be resolved successfully. Training of TBAs started in the Philippines in the early 1950s and was mainly on improving the sterility of TBA-managed births. TBA training was supported and sustained over the years primarily by UNICEF. TBA training, however, had varied results. On one hand, TBA training helped reduce neonatal tetanus, but on the other hand, TBA training also provided prestige and acceptability to hilots, making it more difficult to impose strict licensing of midwifery practice. Some TBA training of Barangay Health Workers (BHWs) even make hilots out of otherwise non-birth attendant BHWs. TBA training gave them courage to handle deliveries. Even the issue of whether TBAs should be registered or not is controversial to this day. Will registration of hilots mean licensing them? But if they are not registered, there is no way of tracing accountability for some of the results of mismanaged deliveries, hilots looking no different from a kindly neighbor just trying to assist in an emergency.

25
Another angle to the issue of TBAs is that new hilots emerge among midwifery students who fail to pass their midwifery board exams. Is this not unfair for the women who deserve to be protected from quackery? Criticisms that the standards of some midwifery schools are so poor continue to persist. It is common knowledge that some of these schools are “diploma mills”, meaning they churn out diplomas for a fee to students who did not really complete the required number of deliveries. The issue becomes even more complicated when the question is asked: Who is truly the better skilled attendant – the hilot who spent on the job learning doing actual deliveries or the licensed midwife who just bought her diploma and license and thus does not have enough actual skill? Many midwives end up as orderlies in hospitals, cleaning and disinfecting the premises and instruments or molding cotton balls. Some end up as chambermaids, caregivers or domestics abroad. This happens in spite of the lack of professional midwives in rural or far-flung areas, areas serviced by TBAs. While the consensus at the technical level is to promote delivery by professional midwives, the actual community situation is that women, including urban women, still strongly prefer their local hilots because they feel more comfortable with them. Professional midwives are generally perceived to be culturally different, snobbish and expensive, even though in some areas the TBAs are really more expensive. TBAs provide “tender-loving care” that may include cooking and laundry. Besides, payment to the hilot can be delayed or given in installments. Hilots are also much more accessible to the women, since they live practically next door, while many midwives are no longer required to live in their areas of assignment by their local officials. It is also expected that policies and guidelines may need to consider the regional differences in terms of health facilities, terrain, culture, education and economics. The other important policy issue concerns home deliveries. There is also a need to more thoroughly study the decision – and the timing – to promote facility deliveries rather than home deliveries. Should this be applied in all areas or in selected areas only where there are adequate skilled attendants and health facilities? Home delivery is so culturally ingrained nationwide, even in urban communities. The current statistics show that about 70% of normal deliveries occur at home and less than 4% may occur in the health centers, table 5. The hospitals are expected to handle complicated births, would the push for facility-based deliveries put a strain on the budget and resources of the existing hospital facilities? The additional demand on hospital resources should be quantified and prepared for. Before a major push towards this direction, how should the health centers prepare for these deliveries? Lying-ins are very good alternatives, are there enough? Where should additional facilities be established? How much will this cost? While the WHSMP2 is initiating innovations in 6 areas in the country, what will happen in the rest of the provinces and cities? How will the small-scale initiatives be disseminated and sustained? How strong are the national, regional and LGU Safe Motherhood Committees? How much technical and managerial inputs are needed to firmly make these committees truly functional?

26
Recommended Action: Conduct more thorough study and testing of maternal care policies and guidelines especially in terms of TBAs and place of deliveries in order to ensure successfully policy and standards formulation and implementation. Support institutionalization of Safe Motherhood Committees at the national, regional and LGU levels to ensure smoother flow and continuing feedback and improvement of maternal care policies, standards and guidelines. Delivery of and access to quality, integrated maternal health services The quick assessment conducted in the formulation of this strategy shows there are major needs and gaps in the availability of state of the art midwifery and maternity services and facilities in almost all most communities. While systematic needs assessment will be done in the WHSMP2 project areas, there seems to be no such activity on a nationwide scale. There is clearly a need to take stock and continually promote the quality and improve the availability and access to the essential maternal health services in many parts in the country. The overwhelming LGU response to the Sentrong Sigla quality assurance initiatives validates that this approach is highly effective. If maintained within sustainable parameters, Sentrong Sigla quality improvement activities will considerably improve the availability and quality of maternal care services. Defining the desired quality of maternal services not only at the health center level but also at the lying in or referral facility levels through Sentrong Sigla will speed up the understanding and institutionalization of the quality targets. Technical assistance and inputs will then be consolidated towards the clearer and unified quality targets. All partners and stakeholders will speak the same language. Standards that require integration of services, for instance between maternal care and family planning such as the promotion of LAM and more consistent and in-depth FP counseling for high risk women, will have to be developed to ensure that these services do integrate. Resource sharing among various partners will be easier and will more likely lead to desired impact. It is inspiring to note that many LGUs are very much active in self-improvement. Many local executives now recognize health as an important component of their function. With stronger and clearer standards, the LGUs can be independent yet stay within the desirable technical boundaries, avoiding waste of meager resources on ineffective, sometimes even more expensive, initiatives. The LGUs especially need better skilled technical and managerial staff.

27
Recommended Action: Assist and facilitate the formulation, field-testing and continuing improvement of Sentrong Sigla quality standards in maternal health services not only at the health center level but also at the lying-in and district hospital levels. Provide technical assistance and other support to ensure that the LGUs commit to and are able to meet the SS quality standards. Improvement of support and program management systems In addition to improving policies, guidelines and quality standards of services, there is need to ensure that support systems and organizational arrangements allow continuing communication, coordination and synergy among various stakeholders in health service delivery. “One script” or cross-functional teams have been promoted by the DOH, Their institutionalization and their effective use of tools such as systems modeling in planning and coordinating their action still need much improvement. Such efforts should be encouraged and supported. Better data collection, analysis and completion of the feedback-action loop at the LGU level will contribute a lot to the continuing allocation and re-allocation of appropriate resources to solve problems and relieve bottlenecks. Maternal and neonatal death reviews as well as monitoring and feedback on selected process indicators will ensure a healthy data-based, responsive management of the maternal care programs. At the LGU level, it was noted that while they are able to produce Field Health Services Information reports, there was really a lack of accurate information on actual coverage of their services in their communities, especially in urban areas. Since the reports cover only services rendered in the health facilities, the health staff do not really know how many have really been reached, and how many and where are the groups that are really at risk. Health status reports, for instance on the level of undernutrition, are heavily dependent on outside sources such as FNRI surveys. LGUs should be able to develop information systems that will provide them with a better perspective of the actual needs of their population and targets. The community-based management information system (CBMIS) developed in the IFP-MHP project will still be very relevant to the LGUs, especially if the information includes additional maternal care-specific data, such as maternal and neonatal outcomes, morbidities and causes of these. Community development The initiatives to improve the supply side of the health service delivery system will not function optimally if the target beneficiaries do not understand the motives and arrangements. Better utilization of health services, commitment to personal and family responsibilities in health care, and sharing of community resources all have to be ensured through community development and community participation activities. Much of these will involve health education, communication and primary health care projects and

28
interventions. The BHWs should be sustained and their capability improved in terms of maternal and neonatal care. Desirable behaviors that promote better synergy between the health staff and the community leaders, could be disseminated, promoted and eventually instituted through interventions already proven to be effective such as functional literacy classes, role-modeling and community support groups, and empowerment of women in decision-making. Appropriate mix of communication interventions will be needed to effect behavioral changes. Monitoring of these changes is also crucial to the success of this effort. Recommended action: Define desirable behavior in maternal care targeted at individuals, families and community leaders and influentials and develop communication interventions with varying levels to promote behavioral change. The stages of change and communication approaches can follow the guidelines such as those used by the Linkages project, annex E. Develop and test a system of monitoring and quantifying behavioral changes and a system of feedback to formulate communication strategies and approaches. Assist in the training and strengthening of BHWs in terms of their role in maternal health service provision and health education, information and communication. Child Care
• Infant mortality rate and under-five mortality rates declined in fifteen year period and achievement of reduction goals of government has been surpassed ahead of time but still these are higher compared than rates of other Asian countries. Regional and provincial disparities are noted.
• Infants and children in rural areas have higher risk of dying than children in urban
areas. Infant and under-five mortality rates are high among children whose mothers have no education, no antenatal and natal care, age of mothers below 20 and 40 and above, and short birth intervals.
• Slow progress in the reduction of malnutrition problems and micronutrient
deficiencies among under-five year old children remain a challenge in the country. The highest percentage of underweight occurred at the age one and two.
*Reduce malnutrition by improving maternal health and provide a package of interventions focus on the first two years of life to include early initiation, exclusive breast feeding up to six months and extended up to 2 years, appropriate complementary feeding after six months of age, growth monitoring, micronutrient
supplementation and IMCI.

29
• Improving health caring and seeking behavior has not been significantly noted at national level but rapid assessment of community based interventions among indigenous and hard to reach communities revealed significant improvement. Home case management of diarrhea with increased fluids; continue feeding and fast referral is not significantly improved in ten-year period. In addition, health seeking behavior or fast referral for cough with rapid breathing has not gain progress. * Adopt the Integrated Counseling for FP- MCH and the functional literacy strategies among the uneducated / less educated, indigenous people / marginalized communities.
• Early initiation, exclusive and extended breastfeeding practices have not
improved when Mother Baby Friendly Initiative and monitoring compliance of the Milk Code were not considered priority strategies.
* DOH and LGUs will have to strengthen the MBFHI and the Milk Code Monitoring. Community support groups for breastfeeding should be in place.
• The Philippines has been certified as Polio Free and Measles Elimination
strategies are on track. Sustenance of high routine fully immunized children and the strengthened EPI Surveillance system are the focused of EPI Disease Reduction Initiatives. EPI is considered by many stakeholders including mothers as the best and effective intervention for health of children.
* DOH National and CHDs need to conduct regular program reviews with PHOs / CHOs.
• Percentage of fully immunized children decreased in 2003 NDHS due to
problems of inadequate and irregular supply of EPI vaccines due to DOH procurement problems coupled with global shortage of vaccines. ECCD Law provides assurance of 100% vaccine supply from DOH.
* DOH will continue to provide vaccines and Vitamin A capsules as stipulated by the IRR of the ECCD Act.
• Vitamin A supplementation coverage in most of the surveyed provinces is high at
more than 90%. This is because of the important role of the community volunteers. In addition, it is integrated into the Preschoolers’ Week or the Garantisadong Pambata in April and October or any national campaign of each year.
* Vitamin A should continue to be integrated in the Pre-schoolers’ Week. Validation survey will also be conducted every after GP week.

30
• Education of mothers influenced immunization status and Vitamin A supplementation of children. Children whose mothers are not educated or less educated are less likely to be fully immunized or to receive Vitamin A supplements.
* Uneducated and less educated mothers or caregivers will be one of the priority target population in community-based interventions.
• Salt iodization has gained progress towards universal salt iodization as shown by
the marked increased of households using iodized salt in 2003 compared to that of 2001.
* DOH leadership and LGUs will sustain the gains of USI and make sure that all families have access and afford iodized salt.
• IMCI, as one of the most cost effective interventions to reduce morbidity and
mortality among under-five children has been modeled and expanded nationwide. The three IMCI components have been implemented in limited areas of the country specifically in project areas.
* DOH and LGUs need to mobilize resources for nationwide expansion.
• IMCI On the Job training can be a good alternative for the 11 day basic course as
this is cheaper and done at the main health center level for 10 days in three weeks followed by three days at a designated IMCI training hospital, without sacrificing the quality as long as s provincial facilitator monitors the conduct of said training.
* LGUs can adopt this IMCI option for training of frontline workers.
• The Enhanced Child Growth and the Caregiver Functional Literacy strategies are
community-based interventions that are considered as effective in promoting health caring and seeking behaviors of families. The former is addressed to families at large but the later is focused to illiterate caregivers and parents.
* DOH / LGUs will have to adopt these community based strategies to ensure improvement of health caring and seeking behaviors.
Lessons learned from IMCI – based on HKI reports and CPC V UNICEF Midterm Review report
• IMCI Capability building of frontline workers ensured the institutionalization of the strategy. Support of international agencies and local government units promote the sustenance of the intervention.

31
• The follow-up after training strengthens skills in IMCI of trained health workers but there is a need to conduct it regularly. MHOs / PHNs need to be train as IMCI supervisors for midwives.
• Advocacy activities encouraged local leaders and stakeholders to support IMCI
especially the procurement of drugs and medicine and establishment of health and nutrition posts.
• Clients are satisfied with the IMCI approach even in barangay health stations as
their children are thoroughly assessed.
• Enhanced Child Growth is a perfect example of community empowerment since it operates through organized community efforts. It instills sense of responsibility and feeling of ownership. It promotes improvement in health caring and seeking behavior of families with less access to health services and among marginalized communities.
• Caregivers’ Functional Literacy was shown as a powerful strategy to foster
assertiveness of women in marginalized communities, in their health caring and seeking behavior, accessibility to IEC campaign materials, and to the services of health facilities through their acquisition of skills on reading, writing and computing simple arithmetic.
Lessons learned from focus group discussions and interviews of major stakeholders:
• EPI is considered both by health workers and mothers as the most successful intervention for children. Mothers demand immunization services for their children.
• In urban areas, clarification of roles of health personnel is important in deciding if
there is a need for midwives to be trained on IMCI. In Muntinlupa, midwives do not assess nor manage a patient but assist doctors in recording and information education activities. Therefore, midwives should be train on family and community component of IMCI rather than on the 11 day IMCI basic course.
• Advocacy activities to LGUs on health interventions facilitate support. Multi-
sectoral networking mobilized more resources for health program.
• Periodic monitoring and review of programs by major stakeholders improves performance and sustain good working relationship of health sector despite a devolved set-up.
• Barangay health workers who belong to their own tribe are effective in educating
their own people in improving their health and health of their children.

32
• Health and nutrition posts have improved access to health services and improved health caring and seeking behavior.
• Mothers who are acceptors of modern methods of family planning are mostly
those who are graduates of the caregiver functional literacy classes. Satisfied family planning acceptors especially tribal leaders have a strong influence on couples’ acceptance of the modern methods despite that their culture does not allow limiting or spacing number of children.
• CBMIS is a good tool of monitoring unmet needs of mothers and children. It
improves program performance as priority families are identified and regular visits by community health volunteers build trust and respect.
LEAD MCH Project Framework The MCH component of the LEAD for Health project will answer those specific MCH problems, needs and challenges that will affect the LEAD for Health deliverables in Family Planning, TB and HIV prevention and control, and Vitamin A supplementation. The MCH component will facilitate the attainment of these deliverables by supporting existing initiatives, policies and program directions of the DOH, LGUs and other partners in health. Although the resources in the other MCH activities need not be large, the proper selection of crucial interventions will still lead to significant and substantial results in the health situation of mothers and children. Many of the proposed interventions take into consideration the demands and suggestions expressed by DOH top and middle management, specifically Undersecretary Milagros Fernandez and Dir. Myrna Cabotaje, and by the DOH Regional and LGU staff in the areas visited. Community needs were also highlighted especially those detected in ARMM and other parts of Mindanao. The MCH component will ensure synergism with the other LEAD components through interventions that will likewise strengthen LGU support for the above-stated deliverables and improve national health policies that will facilitate the delivery of quality FP services of the LGU by promoting integration between FP and MCH. Interventions that promote MCH-FP integration include, among others:
1. Consistency and cohesiveness of MCH-FP policies, quality standards, guidelines, regulations, basic communication messages and management and information systems, at all levels: national, regional and LGU level
2. Clarification of specific areas of MCH-FP integration through more specific and
updated protocols, training modules and community communication materials such as: • TBA and BHW role in FP

33
• FP, HIV and TB prevention / control actions in the LEAD functional literacy module, IMCI case management flow chart, and ECCD songs and games, and other technical manuals and modules
• Antenatal FP packages and messages that will facilitate FP method decision at antenatal, so that FP services can be provided immediately, without delay, soon after delivery, before the woman gets pregnant again
• Child care packages and messages that will alert the health providers and BHWs to intensify FP counseling for parents of children with malnutrition, poor development and frequent illnesses, and those not fully reached by basic services such as immunization and vitamin A supplementation
3. Follow through at the community level to sustain behavior changes in MCH
caring and health-seeking behavior that will facilitate wide access of quality MCH-FP services
Goals The goals of this strategic plan are:
1. To contribute to the improvement of maternal health 2. To contribute to the reduction of the rates of fetal and neonatal mortality and
morbidity 3. To contribute to the reduction of rates of infant and under-five mortality and
malnutrition Objectives The following objectives will be pursued by this strategic plan:
1. To strengthen local government in the provision and management of quality maternal and child health services: Practical DOH policy options on the role of traditional birth attendants (TBAs) and on facility-based births / deliveries well articulated by mid-2005 50% of health centers, lying-ins and municipal/district hospitals in participating LGUs are certified as Sentrong Sigla for Level 2 MCH standards by mid-2006
80% participating LGUs with protocols to integrate FP into MCH services by mid-2006
70% of health facilities of participating municipalities providing IMCI services by EO 2006
90% of children 6 to 59 months old received Vitamin A capsules every 6 months by EO 2006

34
2. To improve health-caring and health-seeking behaviors of families, especially
those with uneducated and less educated parents, indigenous and disadvantaged families and those with least access to maternal and child health services:
80% of participating LGUs have functional models of integrated FP-MCH services at the community level delivered by TBAs, BHWs and other community health providers
50% of participating LGUs have implemented integrated, comprehensive problem and action-oriented health education and community-level communication activities on MCH-FP by mid-2006 50% of participating LGUs have systems in place to monitor selected MCH-FP behavior indicators by mid-2005 and trends monitored annually until EO 2006
70% of indigenous and marginalized communities or communities in hard to reach areas of participating LGUs have functional health and nutrition posts (HNPs) by EO 2006 50% of illiterate caregivers and TBAs completed LEAD functional literacy (FL) classes by EO 2006
Strategies and Activities To achieve the above-stated goals and objectives, the following shall be the strategies in the MCH component:
1. Policy support and standard setting at national and local levels 2. Expansion of access to quality integrated MCH-FP services 3. Stimulation of appropriate health-caring and health-seeking behavior of families
Figure 17 outlines these strategies and activities. Policy support and standard setting Changing role of the TBA While it may seem easy to make the technical decision to phase out or change the role of the TBA as one who will just assist the midwife in deliveries rather than do actual deliveries, such a policy still has to take into consideration the reality that TBAs are part of the Philippine culture. Any change in their role has to be carefully studied to ensure that the change will be an improvement over the current situation. If TBAs are phased out abruptly through legal means, and yet professional midwives continue to refuse to serve

35
in far-flung areas, or live with the people, access to midwifery services may even be reduced. The better way is to develop carefully thought out phasing in of new roles for the TBAs. These new roles should be in harmony with the increasing role of professional midwives and the supporting role of Barangay Health workers. There will be better chance of success in this role change if TBAs could be strengthened in other roles such as family planning, antenatal care, emergency referral and childcare. There is a need to test several role models for the TBA at the community level, with the LGUs. This will greatly influence this DOH policy articulation since Policy recommendations will come from actual experience, not hypothetical suggestions. Facility-based deliveries While it has been suggested in global strategic plans that facility-based births are safer, Filipino women are still very much used to home deliveries regardless of the location of their homes, urban or rural, island or mountain top. Only less than 4% deliver in health centers. The challenge of providing emergency obstetric care in all islands and municipalities, given the meager resources, is overwhelming. The women have to understand the urgency of delivering in more accessible health facilities. However, facility deliveries necessitate adequacy of skilled birth attendants in an adequately equipped health facility. Phasing out of home deliveries should involve phasing in of other resources that will absorb increased demand for facility deliveries, such as establishment of lying- in in health centers or other municipal facilities. Which LGUs in the country are already equipped to promote facility births? Of those not yet prepared for facility births, can they afford to establish strategically located lying ins? It is possible that the LGUs themselves can adequately respond to these problems if they are involved in formulating the solutions. There is a need to assist LGUs to sort out their allocations and priorities to come up with the best options to achieve optimum maternal and neonatal care. There is also a need to assist the LGU define essential local policies to sustain the enforcement of previous DOH policies such as requiring midwives to reside in their places of assignment.
Enhancement of MCH Level 2 Sentrong Sigla certification standards Sentrong Sigla (SS) Level 1certification has proven to be an important tool to improve the quality of care at the LGU level. Recognition and awards, when kept at sustainable levels, will continue to be a potent force that will drive up continuing quality improvement. DOH continues to pursue the second and third levels of SS certification. There is a need to continue partnership with DOH, especially since standards should be regarded as dynamic, needing continuing upgrade, synthesis and simplification. The qualities of an Integrated MCH-FP should be reflected in these standards so that the LGU can reap the recognition for such efforts. Enhanced Level 2 MCH standards for maternal care will eventually include other facilities such as lying ins and LGU hospitals. Since PHIC has been an active partner in the development of SS standards, PhilHealth requirements for basic health professionals will also be included in these standards. The PHIC benchbook will also be an important input in this activity.

36
Compliance with existing policies and regulations and development of other policies The ECCD law (RA 8980 s 2002) mandates that the DOH ensure nationwide availability of vaccines and vitamin A for the children. The budget for vaccines and vitamin A capsules are already in the DOH budget, and there should be no obstacles to the full compliance with the law. Political commitment to support existing MCH-FP policies are also lacking at the LGU level. Advocacy will be needed to mobilize existing multi-sectoral organizations at the local level to ensure political support. Local committees such as the local nutrition councils, local health boards, local councils for the protection of children and local development committees can be tapped to lobby to the Sanggunians for more adequate budget in MCH services and programs. Safe Motherhood committees have to be established within these existing networks. These local multi-sectoral committees will also generate resources from barangay funds, congressional funds, NGO or religious organizations, academe, Sanggunian ang Kabataan, among others. There is a need to assist the DOH and the LGUs in identifying blocks in its systems, at the national and regional levels, to facilitate full compliance with such policies and regulations. Advocacy is also needed to include in LGU performance benchmarks the requirement for functional ECCD committees and LCPCs, and the provision of funds for MCH activities such as IMCI training, drugs and supplies and logistics for maternal care services. There are many other policies, standards and guidelines in MCH that will need adequate study, analysis and testing to help guide DOH towards the right policy decisions and actions. Family Planning can still be better integrated into many national MCH policies and programs. There is a need to assist DOH and the LGUs in identifying blocks in its systems, at the national, regional levels to facilitate full compliance with such policies and regulations. Advocacy will facilitate the inclusion of FP in the Integrated Counseling MCH modules and the issuance of an administrative order (AO) to operationalize this integration. Increased access to quality integrated MCH-FP services Systems improvement towards integrated MCH-FP services In order to improve the management and coordination of all MCH initiatives, there is a need to improve LGU management and coordination systems by providing technical assistance at various levels.
1. To ensure that the LGUs meet and sustain the SS MCH Level 2 certification standards
2. To form and organize multi-sectoral MCH cross-functional groups (eg. “one
script” teams), especially those where LGU involvement is needed. The assistance
37
will include the development of tools for multi-sector coordination such as the use of systems models in planning and management, and other useful approaches that could be used by cross-functional program management teams
3. To develop a system of monitoring and feedback-action loops at the LGU level
When DOH completes it Level 2 SS MCH standards that include integrated MCH-FP protocols, the LGU will need assistance to meet these standards. There is a need to assist the DOH ensure that the LGUs are able to meet these SS standards by providing technical assistance in systems improvements and improving access to these services. Access will also be increased if the LGUs are able to meet these standards of care in their areas of responsibility. TA is needed to better link the LGUs to the referral hospitals, and for the referral hospitals to better integrate MCH-FP such as improved protocols that will trigger the hospital staff to provide BTL counseling for high risk mothers and post abortion women, preferably providing the FP services before the clients are discharged. Since there is a general lack of health resources at the national and regional levels, there is a need to assist the LGUs in better planning and budgeting as well as in more careful managing and monitoring of its finances in MCH. Advocacy to LGUs is necessary so that they truly recognize and accept the priorities that women and mothers deserve. The secret of the success of many management and support systems is a good internal system of communication, feedback and problem solving. Such systems need not be complicated or sophisticated in order to work adequately. Tried and tested methods using instruments already developed in previous projects such as the CBMIS, the logistics management systems and various planning and management tools including the innovations of the “One script” program using systems models will carry the work into higher levels and better chances of success. The MCH-FP sections of these tools will be improved and updated, in conjunction with the overall effort to improve the information resource center of the LGUs. There is also a need to assist the LGUs improve their individual, family and community health education and staff supervision techniques. Childcare Package In addition to vitamin A supplementation, the LEAD Childcare Package shall include expansion of IMCI. Universal Vitamin A Supplementation Vitamin A supplementation is recognized as a highly effective intervention to reduce child mortality by 25-34%. Based on 2003 Vitamin A coverage report of MOST/USAID/HKI assisted provinces and city, high coverage is noted but there is a

38
need to ensure that this is maintained at a high level. LEAD will negotiate with LGUs that have more than 90% coverage to maintain its high coverage, and with LGUs with less than 90% coverage to raise their coverage to 90%. Vitamin A supplementation will continue to be delivered during regular MCH services such as routine measles vaccination, growth monitoring activities, and national campaigns such as Garantisadong Pambata. Vitamin A supplements shall also be given to high-risk children, such as those with measles, severe pneumonia, malnutrition, diarrhea and other chronic or persistent infections. Low dose vitamin A supplements can also be provided to mothers at antenatal visits. Higher dose vitamin A (200,000 iu) can also be given to postpartum women during the first postpartum visit. Food fortification can also be given additional support, such as fortification of rice, sugar or flour. IEC activities for vitamin A will be integrated in all childcare and maternal care client interaction services, outreach projects and campaigns. LEAD will coordinate regularly with the DOH national and CHDs for timely availability, adequacy and distribution of Vitamin A capsules to provinces and cities. In addition, LEAD will also periodically coordinate with DOH for inclusion of Vitamin A coverage in their regular monitoring and MCH program reviews. LEAD will provide technical assistance and grants to identified LGUs with low coverage in coordination with CHDs / other projects such as, but not limited to, CPC V / VI and ENRICH. Adoption/ Expansion of IMCI in participating LGUs Based on the IMCI Experience in Sarangani, which reported good outcome in the improvement of case management skills of health workers, improvement in health systems and key family practices and improvement of health of children, there is a need to expand IMCI. Participating LGUs that have already initiated IMCI will expand their package to include all the other IMCI components - I, II and III, see pages 20-23. LGUs that have not yet initiated IMCI can begin with the family and community component to improve health- caring and health - seeking practices. To improve the case management skills of frontline health workers, LGUs can select between 2 approaches: (a) the 11-days continuous live-in course, or (b) the staggered 10-days (over 4 weeks) course that includes on-the-job outpatient practice. In both courses, the commitment of IMCI provincial coordinators and health center facilitators especially the MHO and PHN to strictly adhere to the training guidelines drafted by DOH / WHO / HKI / UNICEF will be essential.

39
There is a need to improve the IMCI protocol that explores the needs of the mother, especially in family planning; and the action planning/ re-entry planning portion at the end of the course. There is also a need to improve the follow-up activities to include home visits and discussion of actual cases in the community while the children are undergoing treatment. There is also a need to the strengths and weaknesses of the IMCI referral system so that this can be improved. There is also the need to assist the LGU improve its logistics and procurement of essential IMCI drugs and supplies to reduce the LGU dependence on DOH and donor supplies in accordance with overall effort to improve LGU logistics systems. Other activities will include improvement of the IMCI monitoring / supervisory checklist and integration of this checklist in the LGU monitoring system. There is a need to conduct orientation of Service Implementation Organizations (SIOs) and CHDs on IMCI supervision and monitoring. SIOs and CHDs will conduct training of MHOs / PHNs on IMCI monitoring and supervision to ensure follow up of trained personnel one month and after four months after training and regular supervision on IMCI implementation. Grant funds is needed for IMCI training, equipment and supplies. Stimulation of appropriate health –caring and health seeking-behavior of families Enhanced functional literacy courses UNICEF successfully developed and implemented a Female Functional Literacy (FFL) component in its Fifth Country Programme for Children (CPC V). However, due to limited resources, these were done only in selected areas of CPC V provinces / cities. In order to build on these efforts, improvements will be needed to put greater weight on the sections on FP, HIV and TB in the functional literacy (FL) Facilitators’ Guide and Learners’ Primer. This will be called the Enhanced Functional Literacy modules. This enhanced module will target not only females but also couples to facilitate decision-making in FP even as the couple learns basic reading, writing and arithmetic. There is also a need to provide technical assistance to LGUs in identifying, mapping and mobilizing priority groups for FL such as TBAs, indigenous peoples, uneducated/ less educated couples, and families in marginalized communities and hard to reach areas. Grants will be needed for training of trainers, midwives and community volunteers. Likewise, funds are necessary for the printing of facilitators’ guides and learners’ primers. Barangay multi- sectoral committees for MCH-FP One of the lessons learned from CPC V is that involvement of multi-sectoral councils in the overall management of community activities can generate more funds and help expand the models to other communities. By this time, there are already functional structures at the municipal, barangay, and purok levels that can be utilized for community mobilization and community participation. At the municipal level, there are local health boards or municipal nutrition committees, municipal councils for the

40
protection of children or the ECCD committees. At the barangay level, there are functional nutrition committees, and barangay councils for the protection of children. Most of the barangays also have purok organizations. The social mobilization and community participation guidelines will be developed. These guidelines will be provided to participating LGUs. Support for the activities of these multi-sectoral councils will be needed. Expansion or establishment of health and nutrition posts (HNPs) UNICEF CPC V was able to reach previously unreached barangays by establishing health and nutrition posts (HNPs) especially in barangays with no barangay health stations (BHS). This served not only as child weighing posts or places where MCH services are provided, but also as first aid posts, a place for FP acceptor and TB patient follow-up and for BHW meetings, and a general health service post for mobile health center staff such as the physician, midwife or dentist. The approach was very much appreciated by barangay leaders and community residents. There is a need to advocate to LGUs to establish more HNPs in un-served/ underserved barangays. Other activities will include orientation, assessment, planning and monitoring. There is a need to provide technical assistance in developing a checklist for a functional HNP that will integrate FP / TB indicators. The checklist developed by CPC V- UNICEF assisted project will be improved and expanded to accommodate the components of LEAD.
Participating LGUs will mobilize and assist communities to establish HNPs in target communities. Grants for equipment and IEC materials for the HNPs will also be needed. HNPs are managed by the community and supported by local multi-sectoral structures. These posts will be set up in areas with less access to health services, in indigenous communities and among marginalized communities. LGU and communities should ensure that health and nutrition posts are functional by making sure that the following criteria are followed: daily operations (for at least five days) manned by trained BHWs / BNS or parent volunteers; updated cluster spot map; updated database of newborns, malnourished children, pregnant and lactating women, couples of reproductive age group, FP users; available selected medical supplies / IEC materials / equipment / drugs; linkage with the nearest BHS and regular supervision of RHM; integrated MCH-FP and TB prevention and control services, among others. Community communication and participation in integrated MCH-FP The community is an essential partner in development. Good quality services will remain unused or irresponsibly used if target clients are ill informed or remain fearful or distrustful of the government health delivery system. This is most felt in maternal care. While it is indeed convenient to deliver at home, all pregnancies need to be connected to the formal health care system to ensure safety. The spirit of health volunteerism and primary health care is strong, yet there are still gaps in BHW selection, training and

41
upgrade. Politics has influenced BHW activities and priorities. BHW role in FP and MCH will also need clarification and promotion. Although the Integrated Counseling cards for MCH caregivers have been developed by HKI-USAID, this was only used in their project areas. Adult education techniques are not yet fully utilized for community development. Inappropriate lectures and guidelines only confuse local leaders and volunteers. There is still much room for better methods of communicating the desirable behaviors and in simplifying and integrating key MCH-FP behavioral messages. There is a need to assist LGUs conduct baseline studies on MCH-FP practices. Based on this and the IMCI family and community component, all participating LGUs will formulate their family and community communication and action plans to change family behavior in MCH. There is also a need to assist LGUs define and promote suitable and desirable individual, family and community behaviors and practices by providing assistance for community communication activities and campaigns. Assistance to develop and produce FL materials and counseling cards will also be needed. Various IEC materials need to be developed, especially those utilizing home visits as an approach to reinforce messages over and over, especially those that are difficult to understand or are intended to change traditional behaviors, for instance, on maternal nutrition and infant and young child feeding. Functional literacy materials will target TBAs, many of whom are illiterate, especially articulating the TBA role in family planning and integrated MCH-FP services. Training and recruitment of additional BHWs will be encouraged especially in indigenous communities, in Mindanao, not only among Muslim communities but among the other tribal groups such as the T’bolis, the Mansakas, Manobos and Mandayas, among others. The integration of FP into MCH will be incorporated in the counseling cards and will be called Integrated MCH-FP Counseling cards to be used by the literate BHWs and family caregivers. The protocol / guideline for community communication and social mobilization, especially of indigenous peoples, will be developed to serve as reference for LGUs and other partners working in marginalized communities. There is a need to synchronize and synergize these strategies and activities with all the various components of other projects including WHSMP2 in the areas where these projects are present. This strategy assumes that other agencies and units primarily concerned will provide these inputs with maternal care programs such as the DOH, the WHSMP2 project and other partners. There will be a need to actively assist in mobilizing LGU resources for upgrading or establishing maternal health facilities, such as lying-ins or maternity waiting homes in appropriate locations, whenever necessary.

42
Community level data and information It was noted during the visits, that only health center data, such as patients seen in the health facility, are available in the health facilities, especially in large urban areas in NCR. Community level data, such as true status of program coverage or behavior such as exclusive breastfeeding at 6 months old, or surveillance of diseases, are essential for better programming and planning of inputs. Quick validation methods, such as the WHO 30-cluster survey or the coverage validation used in the recently concluded Philippine Measles Elimination Follow-up Campaign will be useful for the LGUs, especially in urban areas. Analysis and utilization of CBMIS will also be part of this activity, which will synergize with the overall effort of to build on the previous experiences with community-based data systems. There is a need to provide technical assistance and grants for improvements in community level information system. Model Areas for implementation In conjunction with the functional literacy courses, community models of MCH –FP integration will be designed with the LGU to build on existing efforts, with the involvement of BHWs and other community leaders and volunteers. Monitoring, mapping and feedback of behavioral changes will be included. Mindanao, as a priority area, especially in areas where similar projects have already been initiated and the health providers are already trained and knowledgeable will be an active area for expansion of integrated MCH-FP services, strengthening of TBA role in FP, and expansion of the IMCI components I and II, among others. For instance, Region XI and XII have been UNICEF testing areas for functional literacy courses and CBMIS. Sarangani province already has trained staff in IMCI and community volunteers sustain CBMIS. Thus, all that is needed is to add the missing components of the intervention or strengthen the LGU where they are weak. Community behavioral modification can be intensified based on baseline behavior mapping. Local NGOs already working in the communities can facilitate the generation of faster results with relatively modest resource inputs. The community-based interventions, such as the family and community component of IMCI and functional literacy, will be implemented in selected target communities of participating LGUs. The rest of other strategies will be implemented in all participating LGUs. It should be emphasized that in all of these, the LGU will maintain the real power, decision-making and strength. Grants for model building, including for other LGU initiatives such as family cooperatives and local health financing schemes that will fill in gaps that are not provided by PHIC, for instance, support for transportation to referral facility.

43
Summary of interventions These strategies and activities can be synthesized using the following illustration below. In maternal care, the integration of MCH and FP will include definition of the standards of integration through the Sentrong Sigla. While initial MCH/FP level 2 standards have already been proposed at the program managers’ level, there is ongoing refinement and finalization before approval. Even when the level 2 standards are approved, there will have to be continuing review and refinement as new trends and insights are gained using the standards. In the previous MSH project IFP-MHP, MSH brought in technical consultants to support DOH efforts in SS.
Synthesis of LEAD inputs in MCH
Health delivery system Community
Integrated MCH-FP TBAs IMCI BHW, BNS & family caregivers
Systems improvements in MCH/FP will also converge towards the integrated MCH-FP standards. Activities will consist mainly of assisting the LGU internalize the drive towards continuing quality improvement. Established lying-ins and referral hospitals will be part of an integrated procedural protocol. The search for the appropriate and technically acceptable role for the TBA will also proceed according to the integrated MCH-FP concept so that the TBAs perform roles consistent with the integrated concept. In childcare, IMCI also embodies the integration concept. It includes a range of interventions that includes curative care of improved case management of childhood illness and preventive aspects of nutrition, immunization, vitamin A supplementation, disease prevention and health promotion. It links also to fortification, maternal care, TB control and FP services. IMCI does this through the protocols on health education and home treatment.

44
In the community level, TBAs are the main focus of change in terms of reducing their role in actually handling complicated deliveries (replacing this with their timely referral of such complications to emergency facilities), and in terms of enhancing their role in providing antenatal care, FP advice and services, and childcare. BHWs and selected caregivers in the family (mothers or siblings, etc) will be the focus of change in terms of their enhanced role in providing counseling to improve specific health-caring and health-seeking behavior, eg. when to bring the child to the health facility based on danger signals. The following table summarizes the LEAD for Health’s inputs:
Summary of LEAD for Health project inputs
The Problem What LEAD for Health will do Expected Results
1) While many LGUs have achieved high levels of coverage during the Vitamin A supplementation campaigns, the giving of Vitamin A supplements to sick children remains a problem. There are also some LGUs where the coverage of Vitamin A supplementation is less than optimal.
LEAD for Health will work with LGU partners to improve health worker practices in giving Vitamin A to sick children during clinic consultations. The project will also assist LGUs improve campaign-based Vitamin A supplementation activities through mobilization of volunteers and greater community participation.
• Increase coverage
of Vitamin A supplementation both during campaigns and during clinic consultations of sick children.
2) While many health care providers have been trained on IMCI case management, the health-seeking behavior of the community is still a problem and compliance to IMCI messages to improve house-based care by mothers and caregivers is still low.
In areas where health staff have been trained on IMCI, LEAD for Health will organize training courses (based on existing manuals) for BHWs who will teach women and caregivers to improve health-seeking behavior and improve compliance to key IMCI messages and recommended practices including family planning
• Early treatment of
sick children (reduce mortality and morbidity)
• Improved breastfeeding practices (including LAM)
• Increase FP acceptors
3) Many deliveries are attended by hilots or traditional birth attendants and these often lead to complications, even maternal deaths. There is no clear policy to deal with this issue other than promoting facility-based maternity services.
LEAD for Health will help organize a partnering of services between professional health workers and TBAs and use the PhilHealth maternity package, with Sentrong Sigla, as the entry point and incentive. The interventions will include FP
• Improved maternal
care • More FP clients • More sustainable
program

45
Antenatal, maternity and post-natal services by TBAs also provide opportunities to introduce FP counseling and information.
counseling and information as part of the safe maternity package.
4) In many parts of Mindanao where large indigenous populations exist (T Boli, Bilaans, Manobos, Timawas, Tausags, etc) literacy classes for women are organized by the DOH, UNICEF, other donors. Currently such literacy classes do not contain FP and TB as part of the core messages.
In areas where there is a continued and sustained effort to organize functional literacy classes for women, LEAD for Health will collaborate in developing training materials/messages for FP and TB control
• More FP acceptors • Better awareness of
TB symptoms
Monitoring and Evaluation Monitoring and evaluation will be part of the overall monitoring and evaluation system of the LEAD for Health project. Monitoring and evaluation will involve regular collection and analysis of input, process and impact indicators at various levels. The final indicators to be selected will be agreed upon by the LGUs and the project. Based on the basic systems model, figure 18, the following indicators are proposed for maternal care: Input indicators
• Policy studies conducted • Training modules and courses developed and implemented (eg. for capability
building in SS quality improvement) • Short-term consultants provided
Process indicators
• Increasing number of facilities SS certified for MCH standards • Increasing access to skilled attendance at birth • Systems introduced and institutionalized (UN process indicators could also be
included if relevant to the system introduced, annex F) • Verbal autopsies conducted indicating reduction in the 3 delays of maternal care • Improvements in quality and access to quality services using self-reporting by
women of the outcome and use of maternal health services Impact indicators

46
• Decline in mortality and morbidity rates (based on baselines and using CBMIS- generated information)
• Changes in behavior of individuals, families or communities, see list of desirable behavior, annex G.
Using the systems model, figure 18, other input, process or outcome indicators may also be considered. Some groups have used program indices, morbidity surveys, unmet needs indices (for FP, routine obstetric care, utilization, coverage, access, and quality of care), among others. The Futures Group completed in 2000 a project that measured the Maternal and Neonatal Program Effort Index (MNPI), which was funded by US Agency for International Development (USAID). This study used 81 individual aspects of maternal and neonatal health services, drawn from 13 categories:
• Health center capacity • District hospital capacity • Access to services • Antenatal care • Delivery care • Newborn care • Family planning services at health centers • Family planning services at district hospitals • Policies towards safe pregnancy and delivery • Adequacy of resources • Health promotion • Staff training • Monitoring and research
Forty-nine developing countries were assessed by about 10-25 experts in each country. In this study, the Philippines obtained an overall rating of 56, placing the Philippines 27th among 49 countries. Some of these indicators can be used in this strategic plan. Table 8 lists the recommended benchmarks for childcare. Implementation arrangements The MCH component of the LEAD for Health Project will be implemented through a synchronized mechanism with the other program components like TB-DOTS and FP, that is, through the LEAD pool of stakeholders that includes the LGUs, DOH, PHOs, DILG, PhilHealth, USAID, other donor and cooperating agencies, private individuals/ groups/ organizations/ agencies, the community, and MSH and its partner agencies. Among these stakeholders, DOH shall continue to take the lead in the implementation of the project across various levels – from the national down to the local level.

47
MSH as the prime contractor shall orient identified stakeholders in the different regions on the LEAD for Health Project and conduct consultation meetings with them. Roles and responsibilities of the different stakeholders shall be elicited and steps identified on how to proceed with the implementation of the project. LEAD for Health Project will continuously consult major stakeholders starting with an objective process in selecting LGUs to be enrolled on a given set of demographic, technical, and governance criteria. The LGUs shall be assisted in conducting an assessment of their local health situation in the areas of governance, health facilities, and LGU and community profile. After the in-depth assessment, the LGUs will be guided in planning their actions. Throughout the planning process, the LGUs will identify their needs, the available LGU resources, and the technical and financial assistance needed to address them. Through the leadership of the DOH and in partnership with the LGUs, provision of technical assistance and mobilization of other resources shall be initiated by the identified stakeholders in the respective localities to supplement and complement the identified available resources at the LGU level with the aim of improving the local provision of integrated MCH-FP services. DOH shall take the lead in the implementation of the project across various levels – from the national down to the local level. The DOH shall set policies and guidelines in the implementation of integrated MCH-FP throughout the country. Through their regional offices (CHDs), the DOH shall also provide logistics assistance (drugs and other supplies) to LGUs, provide technical and financial (whenever available) assistance, and conduct regular monitoring and evaluation. The DOH Representatives assigned to the LGUs shall serve as the project point persons at the local level. Collaborative arrangements will be initiated and maintained by the DOH regional offices with other stakeholders in trying to meet the identified needs of the LGUs. The PHO shall supplement and complement the role of the CHDs with respect to leadership, logistics, technical and financial (whenever available) assistance, and monitoring and evaluation. The DILG will assist LGUs in the governance aspects of health service delivery while PhilHealth will assist LGUs benefit from its health packages through facility accreditation and health provider accreditation. Under the leadership of the DOH, other stakeholders at the local level shall also serve as partners in the mobilization of technical and material resources for the successful local implementation of integrated MCH-FP. MSH will also provide essential inputs (technical and financial) to the project, whenever necessary, and assume the role of a catalyst to hasten the process. Through it all, the purpose of the partnerships is to tap other local resources (both technical and material) and mobilize them to support the integrated MCH-FP initiatives at the LGU level. By doing so, the project hopes to ensure sustainability of initiatives because 1) partnerships are DOH and LGU-initiated, 2) existing and available support and resources at the local level are tapped and mobilized, and 3) MSH will only serve as a catalyst, thus, success and continuity of program initiatives are not heavily dependent on external assistance.

48
LEAD for Health Project Organization The project’s staffing structure is designed to be responsive to the implementation requirements of the integrated MCH-FP strategy. It is headed by a Chief of Party and consists of three implementing units, namely, the LGU Unit, the Family Planning and Health Systems Unit, and the Policy Unit, and three support units, which are the Project Performance Monitoring Unit, the LGU Performance-Based Grants and Contracting Unit, and the Finance/Administrative Unit. The LEAD for Health Project will mobilize its key-implementing units to ensure that all elements of the integrated MCH-FP strategy are successfully implemented. The Family Planning and Health Systems Unit (FPHSU) will spearhead the development and adoption of the necessary tools that will enable LGUs to improve not only program management performance but also, monitoring and supervision. It will also design tools that will help LGUs conduct an in-depth assessment of their current health status, particularly as it pertains to integrated MCH-FP, to be able to establish baseline data on program clients and major areas affecting integrated MCH-FP efforts in their respective localities. The Policy Unit will initiate the assessment of the existing policy environment that largely affects the provision of quality and sustainable integrated MCH-FP services. It will ensure that policies supportive of the thrusts of the national program are in place and are actually being implemented for a more efficient financing and delivery of quality integrated MCH-FP services. Meanwhile, the LGU Unit will lead the project’s advocacy initiatives in this area primarily through its field coordinators and local advocacy groups that will be tapped for the purpose. The Project will mobilize Service Implementation Organizations (SIOs) in working with the LGUs, particularly in the provision of technical assistance. The SIOs will take an active role in assisting LGUs to identify their needs and to mobilize resources to respond to these needs. In this regard, the SIOs will be oriented on the key technical issues and project approaches to ensure that the project’s ground support have a clear grasp and understanding of the project’s priorities. The Project’s LGU Unit field staff will be monitoring performance and will continuously identify needs and possible type and sources of assistance.

49
Timetable The MCH component of the LEAD for Health Project will follow, as much as possible, the timetable of similar program components like TB-DOTS, FP and HIV/AIDS, as follows:
Activities Target dates Orientation and organization of pool of stakeholders June 2004 (already
conducted) Assessment of local situation with LGUs (health status, program status, facilities, resources, community profiles)
July 2004
Action planning with LGUs (specific targets, commitments)
August 2004
Development of tools (training modules, protocols, including monitoring indicators and proposals for LGU grants)
Sept-Dec 2004
Provision of technical and financial assistance for implementation
Sept 2004 – June 2006
Monitoring, supervision and consultation (continuing) Sept 2004 – Sept 2006 Evaluation Oct – Dec 2006

50
TABLES
Table 1: Maternal Mortality Ratio by Region, Philippines, 1990-1995
Region 1990 1991 1992 1993 1994 1995
NCR 170 160 150 139 129 119 CAR 222 216 210 204 199 193 I Ilocos Region 196 189 182 175 168 161 II Cagayan Valley 219 214 208 202 196 191 III Central Luzon 190 186 182 178 175 171 IV Southern Tagalog 165 160 155 149 144 139 V Bicol Region 180 175 169 164 158 166 VI Western Visayas 202 199 195 191 188 184 VII Central Visayas 184 179 174 168 163 158 VIII Eastern Visayas 226 219 211 204 197 190 IX Western Mindanao 218 214 211 207 204 200 X Northern Mindanao 239 236 234 231 228 225 XI Southern Mindanao 172 170 168 165 163 160 XII Central Mindanao 197 195 193 191 189 187 ARMM 377 365 354 343 332 320
Philippines 209 203 197 191 186 180 No data was available for CARAGA.

51
Table 2: Infant and Under-five Mortality Differentials by Socio-economic/ demographic Factors 1998, NDHS Socio-economic Factors Infant Mortality Rate Under-five Mortality Rate Residence: Rural 30.9 45.8 Urban 40.2 62.5 Education No education 78.5 135.7 Elementary education 45.1 73 High School 31.4 45.7 College or higher 23.4 28.3 Medical Maternity Care No antenatal / natal care 76.8 110.6 Either antenatal/natal 36.5 48.7 Both antenatal / natal care 22.5 30 Sex of child Male 39.4 59.4 Female 32.3 50.2 Age of mother at birth < 20 years 41.4 59.7 20-29 33.3 50.8 30-39 37.6 60 40-49 52 67.2 Previous birth interval < 2 years 46.1 73.2 2-3 years 28.2 49.4 4 years + 37.5 48.3 Size at birth Small or very small 48.6 61.9 Average or larger 28.6 40.8

52
Table 3 PRENATAL AND POSTNATAL CARE BY REGION , PHILIPPINES FHSIS 2000
ELIG. POP. PREGNANT
WOMEN PREGNANT
WOMEN ELIG. POP. POSTPARTUM
REGION WITH 3 OR MORE GIVEN TT2 PLUS WITH AT
LEAST
PRENATAL
VISITS 1 PP VISIT NCR* 364,108 58.5 61.4 312,092 76.2 CAR 49,125 60.1 48.6 42,107 72.8 Region 1 145,134 73.8 61.6 124,401 75.1 Region 2 97,972 76.1 71.4 83,976 76.0 Region 3 269,407 75.2 60.2 230,921 77.6 Region 4 396,362 69.2 65.4 339,739 83.2 Region 5 166,428 61.6 52.2 142,652 67.0 Region 6 221,503 54.2 49.9 189,860 63.4 Region 7 194,047 59.3 62.5 166,326 85.4 Region 8 131,118 64.5 59.8 112,387 75.3 Region 9 110,387 68.4 60.2 94,618 67.1 Region 10 97,124 65.9 60.1 83,249 70.1 Region 11 183,330 63.7 84.8 157,140 63.6 Region 12 93,141 56.5 70.3 79,835 75.4 ARMM 76,543 72.2 73.4 65,608 81.1 CARAGA 76,453 59.0 57.0 65,531 66.5 PHILIPPINES 2,672,185 64.8 62.5 2,290,444 74.6 * includes Batanes

53
TABLE 4: LIVEBIRTHS BY ATTENDANCE BY REGION PHILIPPINES 2000 FHSIS REPORT
REGION TOTAL PHYSICIAN NURSE MIDWIFE TRAINED
HILOT UNTRAINED
HILOT OTHERS DELIVERIES
NCR* 234,804 51.4 2.3 34.1 9.7 2.4 0.1 CAR 31,094 41.9 3.2 30.2 16.3 3.2 5.2 Region 1 86,513 27 0.9 59.9 11.0 0.6 0.6 Region 2 61,548 13.6 1.3 59.0 22.2 3.2 0.7 Region 3 171,476 32.6 2.3 52.0 10.7 1.3 0.1 Region 4 271,451 25.2 1.0 42.1 26.4 4.9 0.4 Region 5 109,969 12.9 0.9 33.0 47.1 5.8 0.3 Region 6 129,404 28.5 1.4 28.5 36.7 4.6 0.4 Region 7 13,468 23.7 0.9 51.4 21.6 1.4 0.3 Region 8 91,759 19.4 1.1 41.4 34.3 3.4 0.3 Region 9 64,809 16.4 3.6 41.9 32.3 5.4 0.3 Region 10 62,321 21.6 0.6 28.0 47.1 2.4 0.3 Region 11 108,675 21.6 0.9 28.2 40.3 7.4 1.6 Region 12 53,520 16.8 1.1 34.5 37.7 9.3 0.6 ARMM 52,600 2.9 1.3 49.0 35.7 10.4 0.8 CARAGA 41,555 15.4 0.5 33.9 48.1 1.8 0.3 PHILIPPINES 1,704,966 26.8 1.5 40.7 26.6 3.9 0.5

54
TABLE 5 :
DELIVERIES BY TYPE AND PLACE BY REGION
Philippines, 2000 FHSIS Report
REGION NUMBER TOTAL NORMAL SPONTANEOUS VAGINAL DELIVERY OTHER TYPES
OF NUMBER OF
LIVEBIRTHS DELIVERIES HOME HOSPITAL OTHERS TOTAL HOME HOSPITAL OTHERS TOTAL
% % % % % % % %
NCR* 234,804 234,804 33.4 52.3 14.3 100.0 0 0 0 0
CAR 31,094 31,094 55.7 44.0 0.3 100.0 0 0 0 0
Region 1 86,516 86,513 78.0 21.0 1.0 99.7 37.5 62.5 0.0 0.3
Region 2 61,548 61,548 85.3 13.6 1.2 99.5 23.7 29.5 46.8 0.5
Region 3 171,476 171,476 65.9 32.5 1.6 97.7 82.5 16.2 1.2 2.3
Region 4 271,451 271,451 71.1 25.9 3.0 100.0 0 0 0 0
Region 5 109,969 109,969 85.8 13.7 0.5 99.3 29.3 68.8 1.8 0.7
Region 6 129,404 129,404 66.2 30.6 3.3 99.0 36.9 45.6 17.5 1.0
Region 7 133,468 133,468 74.0 25.0 1.0 99.3 80.0 19.9 0.1 0.7
Region 8 91,759 91,759 77.4 19.4 3.2 100.0 0 0 0 0
Region 9 64,813 64,809 81.2 17.4 1.4 100.0 0 0 0 0
Region 10 62,321 62,321 no rep no rep no rep no rep no rep no rep no rep no rep
Region 11 108,675 108,675 69.1 29.5 1.4 100.0 0 0 0 0
Region 12 53,520 53,520 82.2 16.8 1.0 99.2 4.8 66.1 29.1 0.8
ARMM 52,542 52,600 94.0 5.1 0.9 100.0 0 0 0 0
CARAGA 41,927 41,555 82.9 16.5 0.6 100.0 0 0 0 0
PHILIPPINES 1,705,287 1,704,966 68.6 27.8 3.6 99.5 61.5 31.6 7.0 0.5

55
Table 6: Antenatal interventions known to be effective Condition / stage Test / treatment Effect
Reduced number of antenatal care visits Delivering antenatal care visits Prevention of anemia Detection and investigation of anemia Treatment of iron- deficiency anemia Detection and investigation of HDP Treatment of severe pre-eclampsia Treatment of eclampsia Prevention of obstructed labor Screening for infection Prevention of infection
Reductions to 4-5 antenatal visits, including proven effective interventions Midwife/general practitioner managed care compared with obstetrician / gynecologist-led shared care Routine supplementation with iron and folate during pregnancy Malaria chemoprophylaxis Copper sulphate densitometry test Colorimetric tests Coulter counter Blood film microscopy Oral iron and folate Intramuscular and intravenous iron Packed cell transfusion Measurement of blood pressure with sphygmomanometer using fifth Korotkoff sound Urinalysis of clean catch urine Transfer to first referral level for expert care Supportive first aid maintaining airway and preventing injury fruing fit Magnesium sulphate (IM or IV) Recognition and speedy transfer to fully equipped facility Expedited delivery External cephalic version at term Serological screening and treatment for syphilis Microbiological screening for gonorrhea Screening for bacteriuria with quantitative culture of urine Tetanus immunization in pregnancy and/or women of childbearing age Induction of labor in uncomplicated prelabor rupture of membranes
Similar maternal results Similar clinical effectiveness Reduces or prevents fall in hemoglobin. Reduces percentage of anemic women. Reduces percentage of women who become anemic Detects hemoglobin level below chosen cutoff point Estimates hemoglobin concentration Diagnosis of type of anemia Diagnosis of type of anemia and of malaria Can raise Hb by 0.4-0.7 g/dL per week Can raise Hb at same rate as oral. Avoids problems of compliance but need IM or IV equipment and trained staff. Danger of anaphylaxis. Raises Hb immediately. Hazards of blood transfusion-infection (HIV-hepatitis) and fluid overload. Need for equipment and trained staff. Detects hypertension Detects proteinuria. Indicative of pre-eclampsia in presence of hypertension. Control of disease. Reduces case fatality Reduces case fatality Reduces recurrent convulsions and maternal mortality Reduces case fatality Only definite treatment Reduces caesarean section at term Detects asymptomatic disease. Coupled with effective treatment, contact tracing and follow-up, reduces fetal loss and maternal and infant morbidity Detects asymptomatic disease. Coupled with effective treatment, contact tracing and follow-up, reduces fetal loss and maternal and infant morbidity Detects asymptomatic disease. Coupled with effective treatment prevents pyelonephritis and preterm delivery / low birthweight Prevents maternal and neonatal tetanus Prevents maternal infection
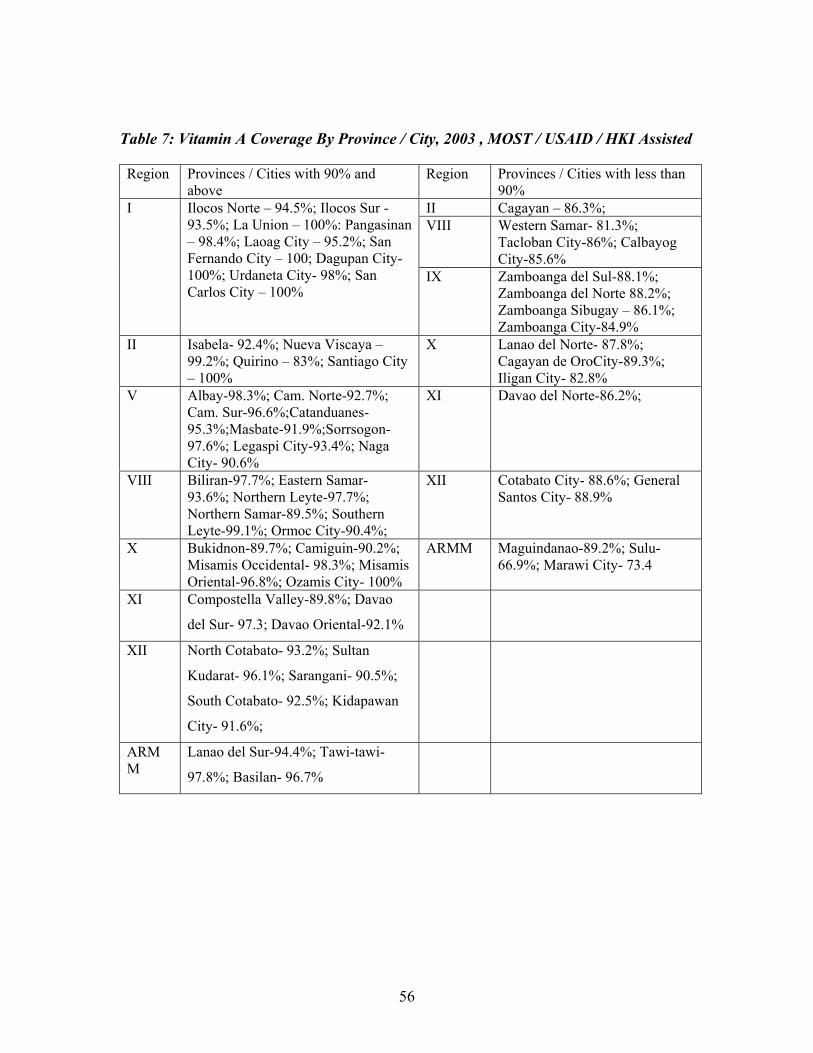
56
Table 7: Vitamin A Coverage By Province / City, 2003 , MOST / USAID / HKI Assisted
Region Provinces / Cities with 90% and above
Region Provinces / Cities with less than 90%
II Cagayan – 86.3%; VIII Western Samar- 81.3%;
Tacloban City-86%; Calbayog City-85.6%
I Ilocos Norte – 94.5%; Ilocos Sur - 93.5%; La Union – 100%: Pangasinan – 98.4%; Laoag City – 95.2%; San Fernando City – 100; Dagupan City- 100%; Urdaneta City- 98%; San Carlos City – 100%
IX Zamboanga del Sul-88.1%; Zamboanga del Norte 88.2%; Zamboanga Sibugay – 86.1%; Zamboanga City-84.9%
II Isabela- 92.4%; Nueva Viscaya – 99.2%; Quirino – 83%; Santiago City – 100%
X Lanao del Norte- 87.8%; Cagayan de OroCity-89.3%; Iligan City- 82.8%
V Albay-98.3%; Cam. Norte-92.7%; Cam. Sur-96.6%;Catanduanes-95.3%;Masbate-91.9%;Sorrsogon-97.6%; Legaspi City-93.4%; Naga City- 90.6%
XI Davao del Norte-86.2%;
VIII Biliran-97.7%; Eastern Samar- 93.6%; Northern Leyte-97.7%; Northern Samar-89.5%; Southern Leyte-99.1%; Ormoc City-90.4%;
XII Cotabato City- 88.6%; General Santos City- 88.9%
X Bukidnon-89.7%; Camiguin-90.2%; Misamis Occidental- 98.3%; Misamis Oriental-96.8%; Ozamis City- 100%
ARMM Maguindanao-89.2%; Sulu-66.9%; Marawi City- 73.4
XI Compostella Valley-89.8%; Davao
del Sur- 97.3; Davao Oriental-92.1%
XII North Cotabato- 93.2%; Sultan
Kudarat- 96.1%; Sarangani- 90.5%;
South Cotabato- 92.5%; Kidapawan
City- 91.6%;
ARMM
Lanao del Sur-94.4%; Tawi-tawi-
97.8%; Basilan- 96.7%

57
Table 8: Proposed Benchmarks for Childcare
Strategy I: Policy Support /Standard setting LGU Performance Benchmarks for Grants • SB Resolution of existing Structure as management / resource generation body • Approved additional budget for child health from GAD budget LEAD Performance Benchmarks • DOH allocate funds for EPI vaccines / Vit. A • AO for Integration of FP into MCH Counseling • LEAD Functional Literacy modules • LEAD Guide for Social Mobilization / Community Participation for rural poor / indigenous / hard to reach communities Strategy II: Increase Access to quality Child Health Services LGU Performance Benchmarks for Grants • 90% Vit. A coverage • Increase number of IMCI trained personnel • Adequate IMCI drugs for trained personnel • Supervisory visits conducted LEAD Performance Benchmark • CHD / LEAD conducted IMCI orientation for LGUs • LGU grants for IMCI training / equipment provided • IMCI Modules provided to LGUs Strategy III: Strengthen LGU/ Communities’ capacity to improve caring and seeking behaviors of families LGU Performance Benchmarks for Grants • SB and ABC resolution to adopt and expand CBI • HNP established in hard to reach communities, among indigenous communities, rural- poor communities and Muslim communities • LEAD FL classes conducted for the target communities • Trained rural health midwives and BHWs / BNS on Integrated Counseling on FP-MCH and LEAD functional literacy LEAD Performance Benchmarks • Performance grants provided for equipment / IEC materials for HNP • Printed Integrated Counseling for FP-MCH and LEAD functional literacy modules

58
Figure 1: Maternal mortality ratio, Philippines, 1990-98
0
50
100
150
200
250
1988 1990 1992 1994 1996 1998 2000
Year
Rat
e pe
r 100
.000
live
bi
rths

59
Figure 2:
Causes of Maternal Death, global data
severe bleeding24%
Infection 15%
unsafe abortion13%
eclampsia12%
obstructed labor8%
other direct causes
8%
indirect causes20%
* other direct causes include ectopic pregnancy, embolism, anesthesia-related complications ** indirect causes include: anemia, malaria, health disease, HIV/AIDS
Source: “Maternal Health Around the World” poster, World Health Organization and World Bank, 1997

60
Figure 3: Main Causes of Maternal Death, Philippines, 1998
Eclampsia27%
Hemorrhage26%
Pregnancy with abortive outcome
9%
Other complications of
pregnancy38%
Source: Philippine Health Statistics 1998, Department of Health, Philippines

61
Figure 4 :Trends in Infant and Under-five Mortality Rates, Phillipines, 1988-2002
34 3529
5448
40
0
10
20
30
40
50
60
1993( 1988-1992)
1998(1993-1997)
2003(1998-2002
Year of Survey
Rat
e pe
r one
thou
sand
live
bi
rths
Infant Mortality Rate
Under-five MortalityRate
Source: NDHS –1993,1998,2003
FIGURE 5: INFANT MORTALITY RATE BY REGION, 1998 NDHS
23.6
42.7 41.5
37.1
28.7
35.3
31.4
2623.6
60.8
44.6
41 40.9
48.4
55.153.2
0
10
20
30
40
50
60
70
NCRCAR I II III IV V VI
VIIVIII IX X XI
XII
ARMM
CARAGA
REGION
RA
TE P
ER 1
,000
IMR

62
FIGURE 6: UNDER-FIVE MORTALITY RATE BY REGION, 1998 NDHS
38.6
52.4 51.3 52.6
39.4
53.2 52.5
41.638.4
85.6
74.9
64.861.2
75.9
97.6
82.5
0
20
40
60
80
100
120
NCRCAR I II III IV V VI
VIIVIII IX X XI
XII
ARMM
CARAGA
REGION
RA
TE P
ER 1
,000
UFMR
Figure 7: Trend in the Prevalence of Malnutrition Among 0-5 years old children
31.43434.534.3
36.839.9
34.5 3429.9
30.63230.8
05
1015202530354045
1989-90 1992 1993 1996 1998 2001
Year
Perc
ent
UnderweightStunted
Source: DOST-FNRI National Nutrition Updates, 2001

63
Source: Philippine Nutrition, Facts and Figure, NNS 1998, FNRI - DOST
Figure 9: Prevalence of Iron Deficiency Anemia Among Under Five Children By Age
31.8
18.22023.4
36.9
53.256.6
0
10
20
30
40
50
60
6mos -11mos
1 year 2 year 3 year 4 year 5 year 6 mos- 5yr
Age of Children
perc
ent
Source: Philippine Nutrition, Facts and Figure, NNS 1998, FNRI – DOST
Figure 8: Percentage Distribution of Underweight Childrenby Single Age Group from 0-5 years
Philippines, 1998
12.9
38.6 37.234.1 34.6 32.6 32.0
6.0
11.0
16.0
21.0
26.0
31.0
36.0
41.0
0 1 2 3 4 5 0-5
Age (in years)
Perc
enta
ge

64
Source: NDHS reports of 1995,1998,2003
Figure11: DIARRHEA CASE MANAGEMENT 1998 NDHS, PHILIPPINES
51.758.343.9
010203040506070
Brought to health fac. Increased fluids Continue feeding
ORAL REHYDRATION THERAPY
PER
CEN
T
42.7
57.7
52.5
26.440.1
35.4
13.2
2016.1 1.8% 2.3% 1.4
0
10
20
30
40
50
60
70
80
90
100
<2 mos. 2-3 mos. 4-5 mos. 6-7 mos.
Figure10: EXCLUSIVE BREASTFEEDING STATUS - By Age in MonthsPhilippines - NDHS 1993/1998/ 2003
1993 1998 2003

65
Figure 12
Global Data: Coverage of Maternal Health Services
97% 99%90%
65%
53%
30%
0%
20%
40%
60%
80%
100%
120%
antenatal care skilled attendance atdelivery
postpartum care
developed countries developing countries
Source: “Coverage of Maternal Care: A Listing of Available Information, Fourth Edition”, World Health Organization, 1997

66
Figure 14: Complete Immunization Status of Children According To Mothers' Education, Philippines, NDHS 2003
67.4 69 83
44
0
20
40
60
80
100
No Education Elem. High School College or Higher
Mothers' Education
Percent
61.9
6560
71.5
72.8
70
8.7 7.9 70
10
20
30
40
50
60
70
80
90
100
FIC Complete None
Figure 13: IMMUNIZATION STATUS - FULLY IMMUNIZED 12-23 months old children
1993/1998,2003 NDHS, Philippines
1993 1998 2003

67
36.967.4
77.785.3
0
20
40
60
80
100
Percent
NoEducation
Elem. HighSchool
College orHigher
Mothers' Education
Figure 15: Vitamin A Supplementation According To Mothers' Education,
Philippines, NDHS 2003
Figure 16: Iodized Salt Use Proportion By Region, Year 2001,2002,2003
25.525.531.323.123.921.9
52.2
26.5 25.5
63.751.951.9
35.547.2
31
81.983.2
48.5
85.679.479.4
60.6
92.4
73.8
94.693.5
0
20
40
60
80
100
I II V VIII IX X XI XII ARMM
Region
Perc
ent
200120022003
Source: USAID-HKI REPORT

68
Figure 17: MATERNAL AND CHILD HEALTH COMPONENT STRATEGIC FRAMEWORK GOAL OBJECTIVES STRATEGIES KEY INTERVENTIONS
CONTRIBUTE TO: Improvement of maternal health Reduction of mortality & morbidity: • fetal & neonatal • infant • under-five Reduction of malnutrition
STRENGTHEN LGU MANAGEMENT OF QUALITY MCH SERVICES 1. DOH policy options on
TBAs & facility births articulated
2. 50% facilities certified SS MCH L2
3. 80% LGUs w/ protocols integrated MCH-FP
4. 70% health facilities with IMCI services
5. 90% of 6-59m children receiving Vit A q 6 months
IMPROVE HEALTH-CARING & HEALTH-SEEKING BEHAVIOR 1. 80% LGUs w/ community
models of integrated MCH -FP, varying TBA role in FP
2. 50% LGUs implemented integrated IEC on MCH-FP
3. 50% LGUS with system to monitor MCH –FP behavior indicators
4. 70% with HNPs among target communities
5. 50% illiterate caregivers completed LEAD FL classes
I
POLICY SUPPORT AND STANDARD SETTING
II
INCREASED ACCESS TO QUALITY INTEGRATED
MCH-FP SERVICES
III STRENGTHENING LGU /
COMMUNITIES TO IMPROVE HEALTH-
CARING AND HEALTH- SEEKING BEHAVIOR OF
FAMILIES.
Strategy I • Policy modeling: TBA changing
role (esp. FP) & facility births • Enhancement of SS standards
MCH Level 2 • Compliance w/ existing MCH
policies & regulations Strategy II • Systems improvements towards
integrated MCH-FP services • Development & implementation
of child care package: Vit. A supplemetation & expansion of IMCI
Strategy III • Development of LEAD
functional literacy courses • Strengthening of barangay multi-
sectoral committees • Expansion/ establishment of
HNPs in underserved/ unserved areas
• Community communication & participation in integrated MCH-FP
• Improvement of community level data & information systems
PERIODIC MONITORING AND EVALUATION
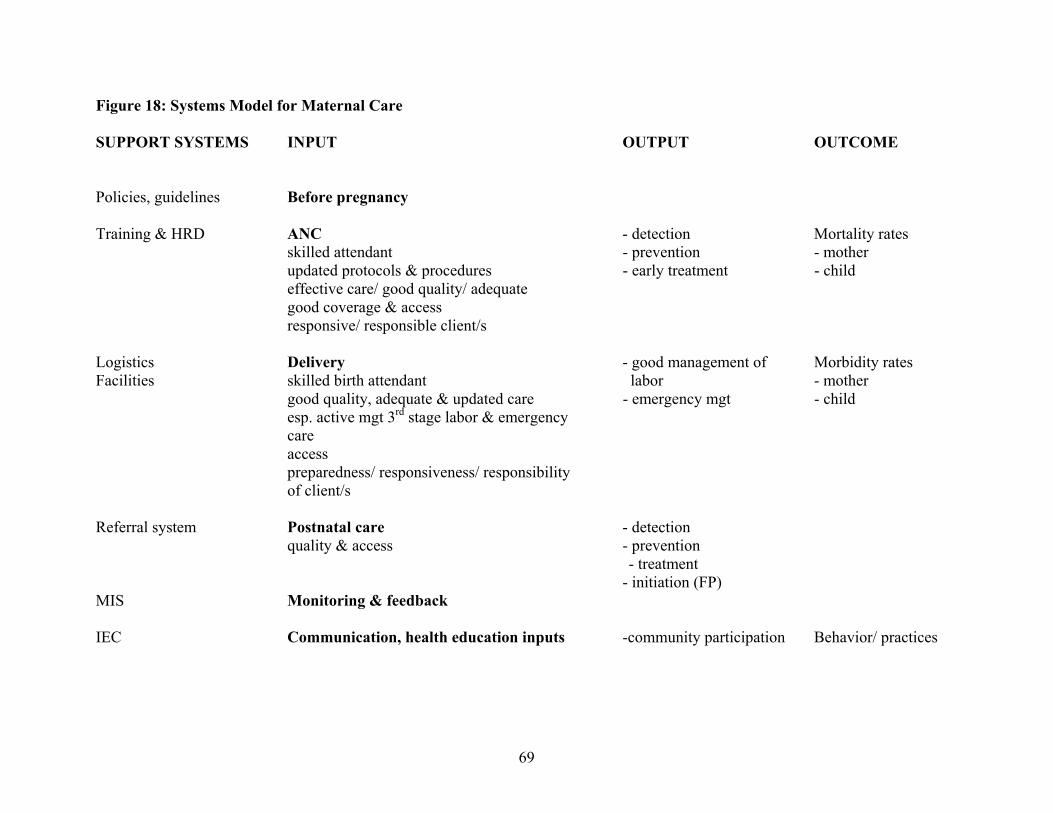
69
Figure 18: Systems Model for Maternal Care
SUPPORT SYSTEMS INPUT OUTPUT OUTCOME Policies, guidelines Before pregnancy Training & HRD ANC - detection Mortality rates
skilled attendant - prevention - mother updated protocols & procedures - early treatment - child effective care/ good quality/ adequate good coverage & access responsive/ responsible client/s
Logistics Delivery - good management of Morbidity rates Facilities skilled birth attendant labor - mother
good quality, adequate & updated care - emergency mgt - child esp. active mgt 3rd stage labor & emergency care access preparedness/ responsiveness/ responsibility of client/s
Referral system Postnatal care - detection quality & access - prevention - treatment - initiation (FP) MIS Monitoring & feedback IEC Communication, health education inputs -community participation Behavior/ practices

70
Figure 19 : General strategies in maternal care
New ANC Skilled BEmOC Quality model attendance EmOC postpartum at birth CEmOC care
*redirection *TBA role *place of *allocation of *adequate birth resources coverage

71
Figure 20: General strategies in childcare
Policy support (ECCD/ASIN Law, food fortification, etc)
Vitamin A Immunization (suppl/fortif)
breastfeeding, supplemental feeding
BRIGHT CHILD
adequate stimulation
newborn screening
Improve health-caring/ seeking behavior
Family and community The Bright Child is a concept of an integrated preventive and curative service package for children, of which IMCI, used when a child gets sick, is only one intervention. Vitamin A supplementation and fortification is specified apart from the other micronutrients in recognition of its proven, essential role in child health, almost as important as immunization for many children, especially those deficient in vitamin A.
M i c r o n u t. s u p p l.
H E A L T H F A C I L I T I E S
I M C I

72
Annex A Ten Action Messages of the Safe Motherhood Initiative
1. Advance Safe Motherhood through human rights
2. Empower women: Ensure choices
3. Safe Motherhood is a vital economic and social investment
4. Delay marriage and first birth
5. Every pregnancy faces risks
6. Ensure skilled attendance at delivery
7. Improve access to quality reproductive health services
8. Prevent unwanted pregnancy and address unsafe abortion
9. Measure progress
10. The power of partnership

73
Annex B New WHO Antenatal Care (ANC) Model
Classifying Form
Criteria for classifying women for the basic component of the new antenatal care model
Name of patient: ________________________________________________ Clinic record number: ____________________
Address: ______________________________________________________ Telephone: _____________________________
INSTRUCTIONS: Answer all of the following questions by placing a cross mark in the corresponding box .
OBSTETRIC HISTORY NO Yes
1. Previous stillbirth or neonatal loss?
2. History of 3 or more consecutive spontaneous abortions?
3. Birthweight of last baby < 2500g?
4. Birthweight of last baby > 2500g?
5. Last pregnancy: hospital admission for hypertension or pre-eclampsia/ eclampsia?
6. Previous surgery on reproductive tract? (myomectomy, removal of septum, cone biopsy, classical CS, cervical cerclage)
CURRENT PREGNANCY NO Yes
7. Diagnosed or suspected multiple pregnancy?
8. Age less than 16 years?
9. Age more than 40 years?
10. Isoimmunization Rh (-) in current or previous pregnancy?
11. Vaginal bleeding?
12. Pelvic mass?
13. Diastolic blood pressure 90mm Hg or more at booking?
GENERAL MEDICAL No Yes
14. Insulin-dependent diabetes mellitus?
15. Renal disease?
16. Cardiac disease?
17. Known “substance” abuse (including health alcohol drinking)?
18. Any other severe medical disease or condition? Please specify ____________________________________________________________________
A “Yes” to any ONE of the above questions (i.e. ONE shaded box marked with a cross) means that the woman is not eligible for the basic component of the new ANC model. Is the woman eligible? (circle) NO YES If NO, she is referred to ___________________________________________________________________________________ Date ______________ Name ________________________________ Signature ________________________________ (staff responsible for ANC)
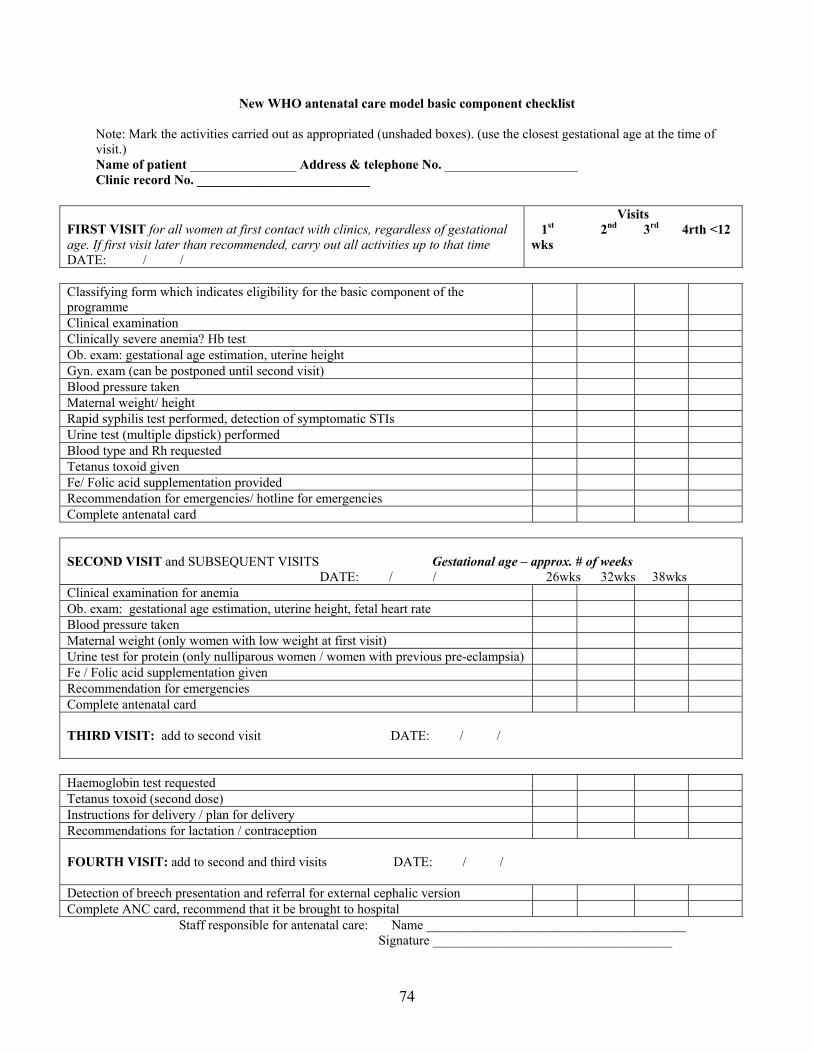
74
New WHO antenatal care model basic component checklist Note: Mark the activities carried out as appropriated (unshaded boxes). (use the closest gestational age at the time of visit.) Name of patient ________________ Address & telephone No. ____________________ Clinic record No. __________________________
FIRST VISIT for all women at first contact with clinics, regardless of gestational age. If first visit later than recommended, carry out all activities up to that time DATE: / /
Visits 1st 2nd 3rd 4rth <12 wks
Classifying form which indicates eligibility for the basic component of the programme
Clinical examination Clinically severe anemia? Hb test Ob. exam: gestational age estimation, uterine height Gyn. exam (can be postponed until second visit) Blood pressure taken Maternal weight/ height Rapid syphilis test performed, detection of symptomatic STIs Urine test (multiple dipstick) performed Blood type and Rh requested Tetanus toxoid given Fe/ Folic acid supplementation provided Recommendation for emergencies/ hotline for emergencies Complete antenatal card
SECOND VISIT and SUBSEQUENT VISITS Gestational age – approx. # of weeks DATE: / / 26wks 32wks 38wks Clinical examination for anemia Ob. exam: gestational age estimation, uterine height, fetal heart rate Blood pressure taken Maternal weight (only women with low weight at first visit) Urine test for protein (only nulliparous women / women with previous pre-eclampsia) Fe / Folic acid supplementation given Recommendation for emergencies Complete antenatal card THIRD VISIT: add to second visit DATE: / /
Haemoglobin test requested Tetanus toxoid (second dose) Instructions for delivery / plan for delivery Recommendations for lactation / contraception
FOURTH VISIT: add to second and third visits DATE: / / Detection of breech presentation and referral for external cephalic version Complete ANC card, recommend that it be brought to hospital
Staff responsible for antenatal care: Name _______________________________________ Signature ____________________________________

75
Annex C
Service Capability for Basic Emergency Obstetric Care (BEmOC)
In addition to the capability to handle normal spontaneous vaginal deliveries and provide routine newborn care, Basic Emergency Obstetric Care (BEmOC) includes: 1. Ability to recognize, stabilize and manage the majority of obstetric complications that
arise and threaten the life of the mother and her unborn child 2. Ability to administer intravenous fluids, oxytocin, magnesium sulfate and broad spectrum
antibiotics 3. Ability to do procedures that can be performed on site such as assisted vaginal delivery,
manual removal of the placenta, evacuation of an incomplete miscarriage and basic neonatal resuscitation
Annex D Service Capability for Comprehensive Emergency Obstetric Care (CEmOC)
In addition to the capability to handle normal spontaneous vaginal deliveries and provide routine newborn care and Basic Emergency Obstetric Care, Comprehensive Emergency Obstetric Care (CEmOC) includes: 1. Capability to perform surgical obstetric services in an operating room, such as a
caesarean section 2. Capability to provide blood transfusion 3. Capability to provide neonatal intensive care
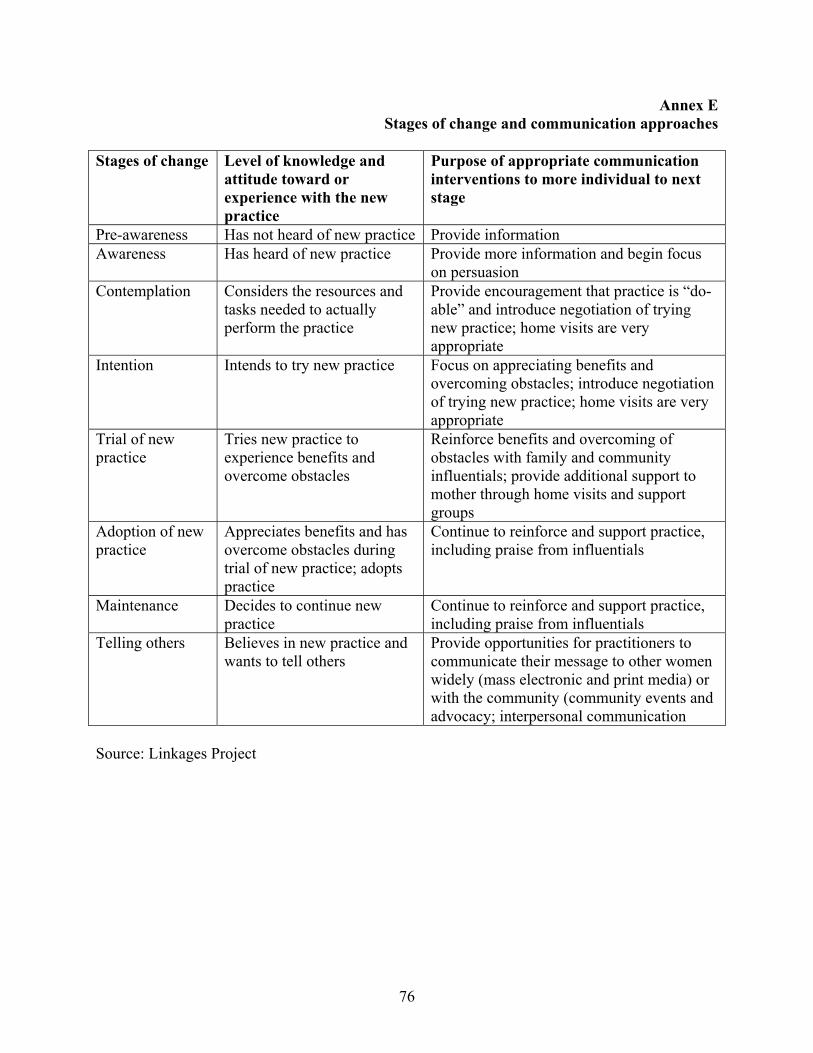
76
Annex E Stages of change and communication approaches
Stages of change Level of knowledge and
attitude toward or experience with the new practice
Purpose of appropriate communication interventions to more individual to next stage
Pre-awareness Has not heard of new practice Provide information Awareness Has heard of new practice Provide more information and begin focus
on persuasion Contemplation Considers the resources and
tasks needed to actually perform the practice
Provide encouragement that practice is “do-able” and introduce negotiation of trying new practice; home visits are very appropriate
Intention Intends to try new practice Focus on appreciating benefits and overcoming obstacles; introduce negotiation of trying new practice; home visits are very appropriate
Trial of new practice
Tries new practice to experience benefits and overcome obstacles
Reinforce benefits and overcoming of obstacles with family and community influentials; provide additional support to mother through home visits and support groups
Adoption of new practice
Appreciates benefits and has overcome obstacles during trial of new practice; adopts practice
Continue to reinforce and support practice, including praise from influentials
Maintenance Decides to continue new practice
Continue to reinforce and support practice, including praise from influentials
Telling others Believes in new practice and wants to tell others
Provide opportunities for practitioners to communicate their message to other women widely (mass electronic and print media) or with the community (community events and advocacy; interpersonal communication
Source: Linkages Project

77
Annex F UN indicators
1. Number of facilities providing emergency OB care 2. Proportion of women who deliver at the emergency OB facilities 3. Proportion of women with complications who deliver at the emergency OB facilities 4. Caesarean deliveries as a proportion of all births 5. Case fatality rate to measure and monitor availability, use and quality of emergency OB
care
Annex G Desirable Behaviors in Maternal Care
MATERNAL CARE Pre-pregnancy
• Girls and women know and practice proper balance between good nutrition and adequate activity
• Girls and women know and practice healthy lifestyle (active, no unhealthy habits like smoking or alcohol abuse)
• Girls and women know how, and do, protect themselves from diseases and injuries
• Girls and women know the danger signs of common illnesses, promptly consult and comply with treatment, especially for TB, malaria, HIV/AIDS, and other genito-urinary infections
Prenatal (with special attention to primigravidas) During pregnancy:
• Mothers consult early in their first trimester for prenatal care • Mothers comply with their scheduled prenatal care visits, TT vaccination, low dose
Vitamin A- iron/ folate supplementation and maintain good health and nutrition during pregnancy, including use of iodized salt, and do not observe traditional food taboos and dangerous traditional practices during pregnancy
• Mothers promptly consult and comply with the management of common pregnancy problems
• Mothers and their family members know the danger signs of pregnancy, and family members immediately bring the mothers to the appropriate health facilities when there are pregnancy complications
• Mothers and their families prepare adequately for childbirth, including preparing for emergencies Mothers and family members do kangaroo caring for newborns

78
Childbirth and immediate postpartum • Mothers who live in far flung communities temporarily transfer residence nearer a
referral hospital facility 1-2 weeks before their expected date of delivery • Mothers consult a trained health professional for the proper management of normal
delivery and postpartum • Mothers and their family members know the danger signs during childbirth and family
members promptly bring the mothers to the appropriate hospital facilities when there are complications during labor
• Mothers immediately feed their colostrum to their newborns and comply with exclusive breastfeeding
• Mothers and family members comply with counseling advice on immediate newborn care, such as kangaroo care
• Mothers and family members have the newborn weighed at birth Postnatal
• Mothers comply with proper perineal care, personal hygiene and newborn care, especially clean cord care, and maintain good health and nutrition
• Mothers practice demand breastfeeding following LAM guidelines • Mothers comply with their scheduled postnatal visits, TT vaccination (if any), Vitamin A
- iron/ folate supplementation and maintain good health and nutrition during postnatal • Mothers and their family members weigh the baby at the end of the first month after birth • Mothers and their family members know the danger signs during the postnatal period,
especially fever, foul vaginal discharge and bleeding; and family members promptly bring the mothers to the appropriate hospital facilities when there are complications during the postnatal period
• Mothers and their family members know the danger signs for newborns and promptly bring the newborns to the appropriate hospital facilities when there are danger signs, especially no/ poor suck, congenital anomalies, yellow baby or blue baby
Note: The same behaviors were proposed to UNICEF for inclusion in CPC VI. This will enhance convergence among various partners.

79
Annex H: Timetable The MCH component of the LEAD for Health Project will follow, as much as possible, the timetable of similar program components like TB-DOTS, FP and HIV/AIDS, as follows:
Activities Target dates Orientation and organization of pool of stakeholders June 2004 (already
conducted) Assessment of local situation with LGUs (health status, program status, facilities, resources, community profiles)
July 2004
Action planning with LGUs (specific targets, commitments)
August 2004
Development of tools (training modules, protocols, including monitoring indicators and proposals for LGU grants)
Sept-Dec 2004
Provision of technical and financial assistance for implementation
Sept 2004 – June 2006
Monitoring, supervision and consultation (continuing) Sept 2004 – Sept 2006 Evaluation Oct – Dec 2006

80
Annex I: Integrated Management on Childhood Disease
Sarangani Experience,2003
IMCI Outcome
Improvement in the case manage- ment skills of frontline workers
♦ Follow-up results showed improvement in the skills of HWs in assessing & managing sick children.
♦ As evidence of effective IMCI counseling,
85-90% caretakers interviewed can recall correctly the home treatment & instructions given to them
♦ Perception on the Quality of Care of Sick Child
received from Health Facility: Very Good- 24.8%; Good - 60.7%; Fair - 12.6%
Improvement in health care system ♦ Improved drug availability ♦ Improved referral pathways - No special days ♦ Increasing access to health in through establishment that limits the clinical care for children; More services; of 104 Health & Nutrition Post in hard to reach selective referrals areas / among Indigenous communities ♦ Improved service quality & organization in health facilities ♦ Improved key family practices ♦ Improved supervision / monitoring
Improvement in key family practices

81
IMPACT OF IMCI, SARANGANI EXPERIENCE
1. Reduction of deaths due to IMCI causes
Under-Five Deaths by Selected Causes, Sarangani Province, 1999-2003
Based on the review of the selected causes of under-five deaths, there was marked reduction of deaths due to pneumonia, measles and diarrhea in 2003 as compared to 1999. No deaths due to malnutrition or malaria was reported in 2003. The high number of measles deaths in 2001 was due to an outbreak .
0
5
10
15
20
25
30
35
40
45
1999 2000 2001 2002 2003
PnumoniaMeaslesDiarrheaMalariaMalnutrition

82
2. Reduction of under-five deaths
It was noted that there was a reduction of forty five percent of the percentage of under-five deaths to the total deaths in 2002 as compared to 1999.
2.171.96
1.90
1.18
0.0%
0.5%
1.0%
1.5%
2.0%
2.5%
1999 2000 2001 2002
Year
Underfive Deaths - Percentage to Total DeathsSarangani Province, 1999-2002

83
3. Improved nutritional status
Nutritional status of children below 6 years old have markedly improved. About 81% of children have normal weight for age. There is an increase of 18% compared to 68.4% in 2000.
68.469.6
73.6
80.5
62.0%
64.0%
66.0%
68.0%
70.0%
72.0%
74.0%
76.0%
78.0%
80.0%
82.0%
Percent
2000 2001 2002 2003
Year
Well-Nourished Underfive Years ChildrenSarangani Province, 2000-2003

84
List of Tables, Figures and Annexes
TABLE
TITLE PAGE
1 Maternal Mortality Ratio by Region, Philippines 1990-95 50 2 Infant and Under-Five Mortality Rates Differentials by Socio-
Economic and Demographic Factors, 1998 NDHS 51
3 Prenatal and Postnatal Care by Region, Philippines, FHSIS 2000 52 4 Livebirths by Attendance by Region, Philippines, FHSIS 2000 53 5 Deliveries by Type and Place by Region, Philippines, FHSIS 2000 54 6 Antenatal interventions known to be effective 55 7 Vitamin A Coverage by Province / City, 2003 56 8 Proposed Benchmarks for Childcare 57
FIGURE
TITLE PAGE
1 MMR, Philippines, 1990-98 58 2 Causes of Maternal Death, global 59 3 Causes of Maternal Death, Philippines, 1998 60 4 Trends in Infant and Under-five Mortality Rates, Philippines, 1988-
2002 61
5 IMR by Regions, NDHS1998 61 6 UFMR by Regions, NDHS 1998 62 7 Trend in the Prevalence of Malnutrition Among 0-5 children, 1989-
2001 62
8 Percentage Distribution of Underweight Children, Philippines, 1998 63 9 Prev. of Iron Deficiency Anemia Among Under-five Children,
Phil.1998 63
10 Exclusive Breastfeeding Status by age, Philippines, 1993, 1998, 2003
64
11 Diarrhea Case Management, Philippines, NDHS 1998 64 12 Global Coverage of Maternal Health Services 65 13 Immunization Status, Fully Immunized Infants, Philippines,
1993/1998/2003 66
14 Figure 14 Complete Immunization Status of Children According to Mothers’ Education, Philippines, NDHS 2003
66
15 Vitamin A Supplementation According to Mothers’ Education, Philippines, NDHS 2003
67
16 Iodized Salt Use Proportion, by Region, Philippines, 2001/2002/2003
67
17 MCH Component Strategic Framework 68 18 Systems model for maternal care 69 19 General strategies for maternal care 70 20 General Strategies in Child Care 71
85
ANNEX
TITLE PAGE
A Ten Action Messages of the Safe Motherhood Initiative 71 B ANC Form and checklist, new WHO ANC model 72 C Basic Emergency Obstetric Care 74 D Comprehensive Emergency Obstetric Care 74 E Communication Approaches 75 F UN process indicators 76 G Desirable behaviors in maternal care 76 H Shortened Version of MCH Strategy Component 78 I IMCI Experience in Sarangani Province 79

86
ACRONYMS ANC Antenatal care ARMM Autonomous Region of Muslim Mindanao ATUs Acute Respiratory Infection Training Units BHS Barangay Health Station BHWs Barangay Heal;th Workers BeMOC Basic Emergency Obstetric Care BNS BNS – Barangay Nutrition Scholar CARAGA region composed of Agusan Norte, Agusan Sur, Surigao Norte and
Surigao Sur CBMIS Community Based Management Information System CED Chronic Energy Deficiency CeMOC Comprehensive Emergency Obstetric Care CFL Caregiver Functional Literacy CHDs Center for Health Development CHOs City Health Offices CPC V Fifth Country Programme for Children CRS Catholic Relief Services DOH Department of Health DOST Department of Science and Technology DTUs Diarrheal Diseases Control Training Units ECCD Early Childhood Care and Development ECD Early Child Development ECG Enhanced Child Growth ENRICH Enhance and Rapid Improvement of Community Health in ARMM EPI Expanded Programme on Immunization FFL Female Functional Literacy FGD Focus Group Discussion FHSIS Field Health Service Information System FIC Fully Immunized Children FNRI Food and Nutrition Research Institute FP Family Planning FP-MCH Family Planning and Maternal and Child Health GAD Gender and Development GP Week Garantisadong Pambata Week HIS Health Intelligence Service HIV /AIDS Human Immunodeficiency Virus / Acquired Immune Deficiency
Syndrome HKI Helen Keller International HDP Hypertensive Diseases of Pregnancy HNP Health and Nutrition Posts IDA Iron Deficiency Anemia IFP-MHP Integrated Family Planning and Maternal Health Program IMCI Integrated Management of Childhood Illness

87
IRR Implementing Rules and Regulations KAP Knowledge, Attitude and Practices LAM Lactational Amenorrhea LCPCs Local Council for the Protection of Children LEAD for Health Local Enhancement and Development for Health LGUs Local Government Units MBFHI Mother Baby Friendly Hospital Initiatives MDG Millennium Decade Goals MCH Maternal and Child Health MCHS Maternal and Child Health Survey MHO Municipal Health Officer MIMAROPA Provinces of Mindoro, Marinduque, Romblon and Palawan MMR Maternal Mortality Rate MOST USAID Micronutrient Programme MICS Multiple Indicator Cluster Survey NCR National Capital Region NDHS National Demographic Health Survey NSO National Statistics Office PHOs Provincial Health Offices PHN Public Health Nurse PMEC Philippine Measles Elimination Campaign POGS Philippine Obstetric and Gynecology Society PPS Philippine Pediatric Society RHM Rural Health Midwife RHU Rural Health Unit SIO Service Institutions / Organizations SS Sentrong Sigla TB Tuberculosis TBA Traditional Birth Attendants UNICEF United Nations Children’s Fund USAID United States Agency for International Development USI Universal Salt Iodization VAD Vitamin A deficiency WHSMP2 Women’s Health and Safe-motherhood Project 2 WHT Women’s Health Team WHO World Health Organization

88
Acknowledgements
This MCH strategy was developed through consultations and focus group discussions of different stakeholders at national and sub-national level. Therefore, we would like to thank them for sharing their ideas, insights and lessons learned from their experiences: At national Level • Department of Health - Central Office
♦ Hon. Manuel M. Dayrit - Secretary of Health ♦ Dr. Milagros L. Fernandez – Undersecretary of Health ♦ Dr. Myrna Cabotaje – Director, National Center for Disease Prevention and Control ♦ Dr. Juanita Basilio – Chief, MCH, National Center for Disease Prevention and Control ♦ Dr, Joyce Ducusin – EPI Manager, National Center for Disease Prevention and Control ♦ Ms. Zenaida Decidoro – Nurse Coordinator, Safe Motherhood, NCDPC
• Helen Keller International
♦ Ms. Ellen Villate – Country Director
• United Nations Children’s Fund
♦ Dr. Martha Cayad-an – Maternal Health Program Officer At sub-national level • Department of Health – Centers for Health Development
♦ Dr. Rosario Benabaye – Director, CHD of Central Visayas; and Executive Committee & Program Coordinators
♦ Dr. Teogenes Baluma - Assistant Regional Director, Officer -in-Charge, CHD, Central Mindanao
♦ Dr. Dolores Castillo = Assistant Secretary, OIC, CHD Southern Mindanao
• Provincial Health Offices ♦ Dr. Edgardo Sandig - Provincial Health Officer of South Cotabato
♦ Dr. Antonio Yasana – Provincial Health Officer of Sarangani Province ♦ PHO Management Staff and technical staff of South Cotabato ♦ PHO Technical Staff of Sarangani Province

89
• City Health Offices
♦ Dr. Magdalena Meana – City Health Officer of Muntinlupa ♦ Dr. Stella Ygona – Officer-in – Charge, Cebu City Health Office ♦ Dr. Virginia Ramirez – Officer-in-Charge, City Health Office, General Santos City ♦ City Program coordinators of Muntinlupa City ♦ District Health Officers and Supervisors of Cebu City Health Office
• Municipal Health Offices
♦ Municipal Health Officer and other Rural Health Unit Personnel of Minglanilla Main Health Center of Cebu Province
♦ Municipal Health Officer and other Rural Health Unit Personnel of T’boli Main Health Center of South Cotabato
♦ Municipal Health Officer and other Rural Health Unit Personnel of Alabel Main Health Center of Sarangani Province
• Barangay Level
♦ Putatan Health Center of Muntinlupa – Medical Officers / Public Health Nurses / Midwives / BNS / BHWs / Hilots
♦ Mambaling Health Center of Cebu City – Medical Officer / PHN / Dentist / BHWs / BNS / Hilot
♦ Alaska Mambaling Health Center of Cebu City – Medical Officer/ Public Health Nurse / BHWs / BNS/ Hilot
♦ Tokawal Barangay Health Station of Alabel, Sarangani – Rural Health Midwife / BHWs / BNS / Hilots
• Communities
♦ Mothers in Pututan, Muntinlupa ♦ Badjao ( Muslim) mothers of Alaska, Mambaling, one of the slum areas of Cebu City ♦ Mothers of Minglanilla, Cebu ♦ Muslim and Christian Mothers of Tokawal, Alabel, Sarangani ♦ T’boli tribal leader / mothers in the municipality of T’boli.
Appreciation is also extended to the following LEAD for Health staff for their ideas and suggestions:
♦ Mr. William Goldman ♦ Ms. Joan Littlefield ♦ Dr. Jose Rodriguez
We would also like to thank all those LEAD staff who attended the presentation of the proposed strategy whose inputs facilitated improvement of this MCH component strategy. Likewise, we would like to thank the support staff of the FP and Health Services Unit of LEAD, especially Ms. Joan Manalo.

















![Welcome [s3.amazonaws.com]s3.amazonaws.com/zanran_storage/cbmwmixers.com/ContentPages/... · Welcome •Tough Industry 2010 •Laid a great foundation for success •Optimistic about](https://static.fdocuments.in/doc/165x107/5b50dcd87f8b9a056a8b5eb8/welcome-s3-s3-welcome-tough-industry-2010-laid-a-great-foundation.jpg)