Team Work in Neurorehab
13
Physiotherapy Research International Physiother. Res. Int. 11(2) 72–83 (2006) Published online in Wiley InterScience (www.interscience.wiley.com) DOI: 10.1002/pri.325 72 Physiother. Res. Int. 11: 72–83 (2006) Copyright © 2006 John Wiley & Sons, Ltd DOI: 10.1002/pri Therapists’ experiences and perceptions of teamwork in neurological rehabilitation: reasoning behind the team approach, structure and composition of the team and teamworking processes KITTY MARIA SUDDICK University of Brighton, UK LORRAINE DE SOUZA Centre for Research in Rehabilitation, School of Health Sciences and Social Care, Brunel University, UK ABSTRACT Background and Purpose. Teamwork and the interdisciplinary team approach have been strongly advocated for use in the provision of neurological rehabilita- tion services. However, whether teamwork has been adopted, and in what form, has yet to be established. The present study investigated therapists’ experiences and perceptions of the reasoning behind the team approach in neurological rehabilitation, the structure and composition of the team within which they worked and the teamworking process Method. This article reports part of an exploratory qualitative study. Five occupational therapists and five physiotherapists from three teams: a rehabilitation centre; a community team; and a stroke unit based within the UK. Semi-structured interviews were undertaken with each participant and then transcribed. Content and thematic analysis of the qualitative interview data was carried out, with respondents validating both the transcription and analysis stages. Results. Perceived composition and structure of the neurological rehabilitation team was variable across teams and between individual team members. There was disparity as to whether patients were included within the neurological team; the interdisciplinary team approach had not been consistently adopted and there were sub-teams and other team memberships in existence. Reasoning behind the team approach supported the perceived benefits of teamwork from a number of perspectives, and the activities reported as part of the team process were diverse. Conclusions. Different teams may choose to use different strategies depending on the aims and context of the team effort. In some instances inter- disciplinary teamwork and patient-centred approaches were not adopted consistently and the process of teamwork itself is both complex and diverse. Copyright © 2006 John Wiley & Sons, Ltd. Key words: neurological rehabilitation, team, team process, teamwork
-
Upload
dimitris698 -
Category
Documents
-
view
13 -
download
2
description
Team Work in Neurorehab
Transcript of Team Work in Neurorehab
Physiotherapy Research InternationalPhysiother. Res. Int. 11(2) 72–83 (2006)Published online in Wiley InterScience(www.interscience.wiley.com) DOI: 10.1002/pri.325
72
Physiother. Res. Int. 11: 72–83 (2006)Copyright © 2006 John Wiley & Sons, Ltd DOI: 10.1002/pri
L1
Therapists’ experiences and perceptions of teamwork in neurological rehabilitation: reasoning behind the team approach, structure and composition of the team and teamworking processes
KITTY MARIA SUDDICK University of Brighton, UKLORRAINE DE SOUZA Centre for Research in Rehabilitation, School of Health Sciences
and Social Care, Brunel University, UK
ABSTRACT Background and Purpose. Teamwork and the interdisciplinary team approach have been strongly advocated for use in the provision of neurological rehabilita-tion services. However, whether teamwork has been adopted, and in what form, has yet to be established. The present study investigated therapists’ experiences and perceptions of the reasoning behind the team approach in neurological rehabilitation, the structure and composition of the team within which they worked and the teamworking process Method. This article reports part of an exploratory qualitative study. Five occupational therapists and five physiotherapists from three teams: a rehabilitation centre; a community team; and a stroke unit based within the UK. Semi-structured interviews were undertaken with each participant and then transcribed. Content and thematic analysis of the qualitative interview data was carried out, with respondents validating both the transcription and analysis stages. Results. Perceived composition and structure of the neurological rehabilitation team was variable across teams and between individual team members. There was disparity as to whether patients were included within the neurological team; the interdisciplinary team approach had not been consistently adopted and there were sub-teams and other team memberships in existence. Reasoning behind the team approach supported the perceived benefits of teamwork from a number of perspectives, and the activities reported as part of the team process were diverse. Conclusions. Different teams may choose to use different strategies depending on the aims and context of the team effort. In some instances inter-disciplinary teamwork and patient-centred approaches were not adopted consistently and the process of teamwork itself is both complex and diverse. Copyright © 2006 John Wiley & Sons, Ltd.
Key words: neurological rehabilitation, team, team process, teamwork

Therapists’ experiences of teamwork in neurological rehabilitation 73
Physiother. Res. Int. 11: 72–83 (2006)Copyright © 2006 John Wiley & Sons, Ltd DOI: 10.1002/pri
INTRODUCTION
Teamwork has developed within the UK as a key component in healthcare delivery within the National Health Service (NHS). It has also been hailed as the cornerstone of rehabilitation (Diller, 1990) and has been supported by governmental directives (DoH, 2000) and professional bodies (Chartered Society of Physiotherapy, 2002; College of Occupational Therapists, 2000).
Within the provision of neurological rehabilitation services, teamwork has been reported to have a number of benefits:
• to provide comprehensive co-ordinated care to the neurologically impaired (LaRocca and Kalb, 1992; McGrath and Davis, 1992)
• to promote problem solving and goal-directed activity within the team (Feiger and Schmitt 1979)
• to improve the outcome of the interven-tion (Melvin, 1980)
• to promote motivation, generalization and a patient-centred service (McGrath and Davis, 1992).
Although these benefits have been presented within the literature they have not been sub-stantiated. Nor have the potential disadvan-tages, such as the resource and cost implications, been explored. There also remains a lack of transparency concerning the defining characteristics of the main team-work models: multidisciplinary and inter-disciplinary (Nieuwenhuis, 1993). A team whose members utilize more traditional methods of working in the confines of their own professional knowledge base whilst still co-operating is considered to be operating under a multidisciplinary framework (Diller, 1990; Barr, 1997). Interdisciplinary team-work requires greater collaboration and has
been defined as a model of care delivery and group interaction that will improve the outcome of the intervention far and beyond that of the summative effort of team members working in isolation (Melvin, 1980). The broadly defined characteristics of an interdis-ciplinary team which have been supported by the relevant literature include: an empha-sis on social- or handicap-related goals (role assumption) (McGrath and Davis, 1992); shared responsibility for goals across profes-sional disciplines (McGrath and Davis, 1992; Schut and Stam, 1994); commitment to shared working practices (collaboration) (Barr, 1997) and joint decision-making (Coopman, 2001); and an integrative client-centred service (Halstead et al., 1986; Davis et al., 1992). However, there have been no clear guidelines or substantive research that has clearly defined or characterized the dif-ferences between the two.
Despite a number of individually reported team cases from the UK (Davis et al., 1992; McGrath et al., 1995; Stead and Leonard, 1995; Newall et al., 1997) and the USA (Halstead et al., 1986), whether teamwork models have been adopted as a working framework for neurological rehabilitation teams has not been fully established. Ques-tions also remain about the specific compo-sition and structure of neurological rehabilitation teams in all varieties of setting. Each team has individual functions, charac-teristics and membership as well as environ-mental influences, and they can be geographically and organizationally diverse (Boaden and Leaviss, 2000).
Adding to the complex nature of team-work in neurological rehabilitation is the teamworking process: the functions and activities which a team carries out together, formal and informal, structured or non-structured, and the factors that influence these processes. To investigate teamwork in

Suddick and De Souza74
Physiother. Res. Int. 11: 72–83 (2006)Copyright © 2006 John Wiley & Sons, Ltd DOI: 10.1002/pri
L1
practice, researchers have explored the key activities that a team must carry out to opti-mize its effectiveness and the characteristics of effective or ineffective teams. The litera-ture has covered healthcare teams across a number of specialist areas. However, research which has focused on the neurological reha-bilitation teamwork process has been minimal, and has concentrated on a particu-lar aspect of the process, that is, communi-cation at ward meetings, role overlap (Booth and Hewison, 2002), the effect of using team notes and care pathways (Gibbon et al., 2002) or on a particular team in isolation (Halstead et al., 1986; Davis et al., 1992; McGrath et al., 1995; Stead and Leonard 1995; Dawson and Bartlett, 1996).
Research has not attempted to explore the teamworking process in its entirety, although some research on stroke units has attempted indirectly to support the contribution of teamwork to the stroke unit benefits reported in the literature (functional ability, survival and patients’ placement on discharge) (Stroke Unit Triallists Collaboration, 1997; Indredavik et al., 1999), it has not provided conclusive supporting evidence, and there has been limited discussion in the literature on the distinction between the different but related aspects of neurological rehabilitation team outcomes. Effectiveness can be consid-ered from the perspective of clients and from management and professional perspectives (Curry and Herbert, 1998); it may focus on the rehabilitation outcome, or on other factors such as the levels of satisfaction between the members of the neurological team and other quality of care indicators. Evaluating team effectiveness is the subject of another paper which is currently under review.
The aim of the present study was to explore the perceptions of occupational ther-apists and physiotherapists towards the
teams within which they worked. This explo-ration included the structure, composition and membership of the team, the reasoning behind the use of the teamwork approach in neurological rehabilitation and the types of activities that were carried out within the teams as part of the teamworking process.
METHOD
The physiotherapy and occupational therapy managers of 13 neurological rehabilitation teams were approached to ascertain whether they wished to participate in the study. The teams approached included stroke units, specialist inpatient or outpatient neurologi-cal services, specialist neurological rehabili-tation centres and community neurological rehabilitation teams based in the Thames region. Four responses, from the occupa-tional therapy and physiotherapy staff from two stroke units, one rehabilitation centre and one community team, were received. The first three teams which responded were selected to continue. Ethical approval for the study was then obtained from the relevant local research ethics committees.
The research procedure consisted of nine stages (Figure 1). Using a topic guide, semi-structured interviews were carried out involving five occupational therapists and five physiotherapists working within three teams involved with the neurological reha-bilitation of adults. The three teams were: a team at a neurological rehabilitation centre (Team A); a community neurorehabilitation team (Team B); and a specialist stroke unit team (Team C). The sample was purposive, and occupational therapists and physiothera-pists with less than one month’s experience of working within the teams were excluded.
Interviewees 1–6 were occupational ther-apists and physiotherapists from Team A; interviewees 7 and 8 were from Team B; and

Therapists’ experiences of teamwork in neurological rehabilitation 75
Physiother. Res. Int. 11: 72–83 (2006)Copyright © 2006 John Wiley & Sons, Ltd DOI: 10.1002/pri
L1
interviewees 9 and 10 were working in Team C. The number of years since qualification for the study population ranged from 1.5 to 13 years (mean 5.75 years, standard devia-tion (SD) 3.61 years) and length of time in the current job ranged from two months to five years (mean 1.9 years, SD 1.66 years). Eight participants were female, the remain-
ing two were a male occupational therapist and a male physiotherapist, both working within Team A.
All interviews were carried out by the researcher and a reflective account was completed after each interview (Keats, 2000) to minimize researcher bias (Stage 1). The interviews were tape-recorded and tran-
Stage 1
Stage 2
Stage 3
Stage 4
Stage 5
Stage 6
Stage 7
Stage 8
Stage 9 Final vaildated pamphlet (indicatingrespondent’s comments at validation)
Validation of analysis and pamphletdevelopment (Stage 6) byrespondent
Initial pamphlet
Content analysis and pamphletdevelopment
Interview transcript
Validated transcript
Validation of transcription (Stage 2)
Interview
Interview transcribed
FIGURE 1: Procedure for data collection and processing.
Suddick and De Souza76
Physiother. Res. Int. 11: 72–83 (2006)Copyright © 2006 John Wiley & Sons, Ltd DOI: 10.1002/pri
L1
scribed verbatim (Stage 2 and Stage 3). Respondents were then asked to validate the transcript (Stage 4). Each validated tran-script (Stage 5) was then organized through content analysis (Kvale, 1996) (Stage 6) by colour coding the information dealing with the main themes: team composition; mem-bership and structure; the teamwork process; and reasoning behind teamwork in neuro-logical rehabilitation. Each participant was sent a pamphlet (Stage 7) that summarized the main themes developed from the analy-sis of their transcript and was asked to vali-date the information presented (Stage 8). The original pamphlet was then amended to include the respondents comments (Stage 9).
RESULTS
Reasoning behind teamwork in neurological rehabilitation
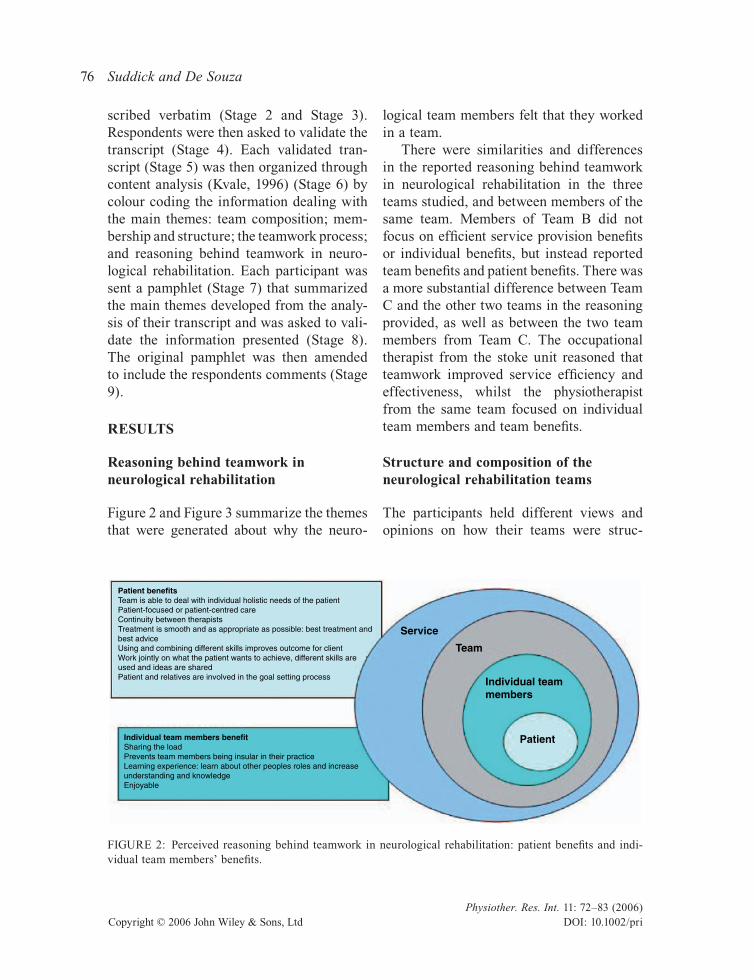
Figure 2 and Figure 3 summarize the themes that were generated about why the neuro-
logical team members felt that they worked in a team.
There were similarities and differences in the reported reasoning behind teamwork in neurological rehabilitation in the three teams studied, and between members of the same team. Members of Team B did not focus on efficient service provision benefits or individual benefits, but instead reported team benefits and patient benefits. There was a more substantial difference between Team C and the other two teams in the reasoning provided, as well as between the two team members from Team C. The occupational therapist from the stoke unit reasoned that teamwork improved service efficiency and effectiveness, whilst the physiotherapist from the same team focused on individual team members and team benefits.
Structure and composition of the neurological rehabilitation teams
The participants held different views and opinions on how their teams were struc-
Patient benefitsTeam is able to deal with individual holistic needs of the patientPatient-focused or patient-centred careContinuity between therapistsTreatment is smooth and as appropriate as possible: best treatment andbest adviceUsing and combining different skills improves outcome for clientWork jointly on what the patient wants to achieve, different skills areused and ideas are sharedPatient and relatives are involved in the goal setting process
Service
Team
Individual teammembers
PatientIndividual team members benefitSharing the loadPrevents team members being insular in their practiceLearning experience: learn about other peoples roles and increaseunderstanding and knowledgeEnjoyable
FIGURE 2: Perceived reasoning behind teamwork in neurological rehabilitation: patient benefits and indi-vidual team members’ benefits.

Therapists’ experiences of teamwork in neurological rehabilitation 77
Physiother. Res. Int. 11: 72–83 (2006)Copyright © 2006 John Wiley & Sons, Ltd DOI: 10.1002/pri
L1
tured, and who was included within each team. The study population consistently stated that the team included nurses and therapists (occupational therapy, physiother-apy and speech and language therapy). The inclusion of other team members (patients, doctors, social workers, physiotherapy assis-tants, occupational therapy technicians) was more variable. The occupational therapist and the physiotherapist from the community rehabilitation team felt that their team extended to include administration and cler-ical staff, and had even wider-ranging col-laborative links with community psychiatry, general practitioners, district nurses and another community domiciliary team. The occupational therapist and the physiothera-pist from the stroke unit included doctors, a dietician, a care manager and a specific stroke co-ordinator within their team.
Another difference reported across the three teams was the involvement of patients. Two respondents felt that patients’ cognitive ability limited how much they could be
included, others suggested that patients should be included but were not, or that patients were considered to be outside the team:
‘I would say with the way things are at the moment, yes, the patient and family are quite excluded. But it is partly because it is such an intense rehab environment, and it is partly just having access to the family for their involve-ment. Also, patients not necessarily knowing what their rehab needs are, because they haven’t got the expertise.’ (Occupational ther-apist, Team A)
There was a considerable consensus between participants from Team A and Team C that their teams were functioning as a multidis-ciplinary team. It was not clear whether Team B was working along a multidisci-plinary or interdisciplinary framework, although the occupational therapist and the physiotherapist from Team B did report the use of a number of interdisciplinary team-work processes.
Despite the occupational therapists and physiotherapists from Team A agreeing that
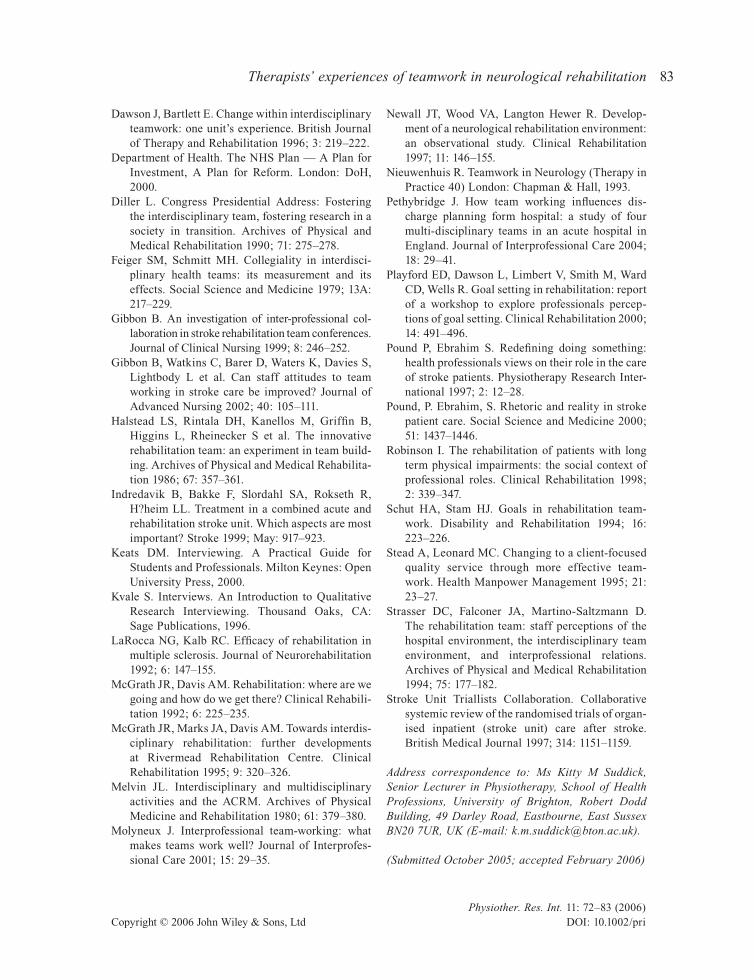
Team benefitsAllows sharing of knowledge and expertise or skillsCan manage gaps of knowledge by assisting each otherAllows integration and co-ordination of treatment across disciplinesAllows sharing of information and sharing of responsibilityTeam members can take on different roles within the teamEveryone is working towards common goalsNurturing and supportive roleAssists in the provision of 24-hour rehabilitation
Service
Team
Individual teammembers
Patient
Service benefitsEffective rehabilitation: knowing what everyone’s working on andwhere you can be most effectiveEffective service: achieving goalsSynergistic: more effective working togetherLimits repetition and improves efficiencyTime efficient: tasks delegated to right people and well co-ordinatedOrganises discharges betterTeam members are not doing in appropriate jobs or tasks
FIGURE 3: Perceived reasoning behind teamwork in neurological rehabilitation: service benefits and team benefits.

Suddick and De Souza78
Physiother. Res. Int. 11: 72–83 (2006)Copyright © 2006 John Wiley & Sons, Ltd DOI: 10.1002/pri
L1
their team functioned as a multidisciplinary team, they held differing perceptions about its specific structure: one participant intro-duced the concept of a core treating team and a secondary team. There was confusion as to whether there was a specific leader in place, and the existence of sub-teams and other team memberships were reported by a number of participants. Only one of the par-ticipants made no distinction, and held the opinion that they worked within a single team.
The teamworking process in neurological rehabilitation
Dimensions of the teamworking process which were reported across the three teams
included goal planning, meetings, joint working practices and social aspects. Some participants highlighted additional aspects: communication, organizational, service development and environmental factors, and discussed how these interrelated (Figure 4).
Goal planning
The three teams used goal planning but there were variations in how it was structured, organized and the level of involvement of patients and their families.
Team A participants discussed a goal-planning process with a specific protocol and a recognized Chair who co-ordinated patients’ admission, goal-planning meet-ings, liaised with patients, was responsible
FIGURE 4: Dimensions of the teamworking process in neurological rehabilitation. No parentheses = dimen-sion reported across all three teams; (A) = reported by Team A; (B) = reported by Team B; (C) = reported by Team C; arrows demonstrate interdependence and overlap between dimensions.

Therapists’ experiences of teamwork in neurological rehabilitation 79
Physiother. Res. Int. 11: 72–83 (2006)Copyright © 2006 John Wiley & Sons, Ltd DOI: 10.1002/pri
L1
for co-ordinating and leading professionals in the patient team, and could advise on the setting of long-term goals. This process also included a ‘plan of assessment’ meeting which clarified areas of assessment for the client, and which was carried out in the second week, in addition to meetings with patients and their families.
Team B had a separate allocated time each week to meet for goal-setting, but without the client.
The occupational therapist and physio-therapist based in Team C explained that patient goals were set and discussed within their weekly multidisciplinary team meeting using an multidisciplinary team goal-setting form, again without patient or family attendance.
Although Team A and Team B reported more interdisciplinary teamwork practices than Team C, team members from both Team A and Team B reported that they did not necessarily include patients and their fami-lies more within the goal-setting process.
Joint working practices
All participants reported the use of joint working practices in the teamworking process. However, a few participants sug-gested that these practices would not occur across the board of the multidisciplinary team in which they worked, with one par-ticipant reporting that joint working worked better with some team members than others. Team A and Team B had weekly team train-ing. Participants from Team C did not report team training as part of their teamworking process.
Communication
Three participants raised the issue of team communication as part of the teamworking
process. Interviewees 4, 6 and 7 reported the use of formal and informal aspects of com-munication, written and verbal. With regard to the informal aspects:
‘. . . and just informal liasons, you know, with people. I mean, they seem so critical to me, to sort of bonding, therapists to therapists and just sharing the load.’ (Occupational therapist, Team A)
Organizational structures, environmental and social factors
When discussing the teamworking process, three study participants also referred to envi-ronmental factors. Team B shared a team base and the physiotherapist from this team suggested that this encouraged more infor-mal team communication and reflection:
‘Because we sit in an open plan office, and a lot of things get discussed outside, someone, one of our locums earlier on this year called them “fringe meetings”, “In the office.”, sounds a bit like chatting, but it is quite sort of soft, but they are the really important things that get talked about often, I couldn’t really put my finger on what it is, but, just as impor-tant.’ (Physiotherapist, Team B)
Additional aspects of the teamworking process which were reported included social events between team members, the weekly timetabling of activities and treatment ses-sions for patients and the use of patient folders, the nursing diary and named nurses.
DISCUSSION
Reasoning behind teamwork in neurological rehabilitation
The findings suggest that teamwork is per-ceived to have benefits from a number of perspectives. The occupational therapists

Suddick and De Souza80
Physiother. Res. Int. 11: 72–83 (2006)Copyright © 2006 John Wiley & Sons, Ltd DOI: 10.1002/pri
L1
and physiotherapists studied reported diverse benefits to patients, the team, individual team members and in improving the effec-tiveness and efficiency of the service.
This reasoning may be influenced by the teams’ context, and, more specifically, the aims and priorities of the team. Team members of inpatient acute neurological services may work to different team priori-ties which focus on service efficiency. In addition, members of the same team may hold different perceptions of the possible rewards from teamwork. Pound and Ebrahim (1997) demonstrated that different views were held by team members caring for stroke patients in regard to their role, priori-ties and successful outcome from rehabilita-tion. These views may affect what the members of the team wish their teamwork to achieve. Lack of open discussion of these issues could lead to discord and disenchant-ment: the perceived rewards from teamwork may not be met, or other team members may be perceived to be working in opposition to those aims. Other influences may be team members’ own personal experience of team-work, the extent of their clinical experience and their profession.
Structure and composition of the neurological rehabilitation team
Occupational therapists and physiotherapists from the three teams discussed the structure and membership of their teams. With regard to the type of team that they worked in, 8/10 participants felt that they were working in a multi disciplinary team, suggesting that the use of inter disciplinary teamworking has not been adopted consistently within neuro-logical rehabilitation despite the literature advocating its use (Diller, 1990; LaRocca and Kalb, 1992; McGrath and Davis, 1992; Strasser et al., 1994). The participants
reported aspects of shared working prac-tices, decision-making and collaboration (Barr, 1997; Coopman, 2001) across the three teams. However, the additional char-acteristics of interdisciplinary working — whether the team was focusing on participation goals, sharing the responsibil-ity of the goals equally across all members of the team and whether it was providing a specific client-centred service — could not be clearly determined from the findings of the present study.
These findings support those of Pethy-bridge (2004), who discovered a number of different team approaches adopted by four different medical, stroke and discharge teams based in an acute hospital in the UK. The differences across the three teams in the present study may reflect the different team structure and composition required for the context in which that particular team works. A team may wish to be structured more in accordance with the social model of disabil-ity and functioning, and may choose to restrict the introduction of more ‘medical’ models of working (Robinson, 1998; Moly-neux, 2001). Variations between the reported team membership observed between the occupational therapists and physiotherapists from the same team may also be attributed to differing opinions about the composition of a team, and/or the perceived contribution or role of certain members of the team.
The findings from this project suggest that in some neurological rehabilitation teams patients and their carers are not per-ceived to be members of the team, and are excluded from contributing to aspects of the team work process. This finding concurs with the opinions of the medical and stroke team members studied by Pethybridge (2004). The neurological team members investigated in the present study considered this exclusion to be caused by the team’s

Therapists’ experiences of teamwork in neurological rehabilitation 81
Physiother. Res. Int. 11: 72–83 (2006)Copyright © 2006 John Wiley & Sons, Ltd DOI: 10.1002/pri
L1
needs, those of the client or additional factors and variables. These findings suggest that, in some instances, team members may be attempting to include patients in the team-working process more than other members of their team. Some team members may be aiming to work within a more patient-centred framework, which could be a source of discord for both patients and team relation-ships. Conversely, there may be appropriate decisions made about the exclusion of patients that have not yet been clearly addressed within the research literature.
The reasoning behind the perceived type of teamwork model used by the teams (both multi- and interdisciplinary) was beyond the scope of the present study. Whether the neu-rorehabilitation teams studied had chosen a specific framework or model of teamwork to meet their needs, whether they were limited to a specific model by other factors or whether they used a combination of models depending on the needs of clients (Nieuwenhuis, 1993) was unclear. The lack of clear guidelines on interdisciplinary working practices meant that no further conclusions could be drawn.
Perhaps the lack of clear guidance on the subject of teamwork in the neurological rehabilitation literature may be attributed to the complexity of the process. ‘Models of teamwork’ may be an outdated ideal in the provision of rehabilitation services which are attempting to adapt to each individual patient, and they may evolve alongside the varying demands of the systems and con-texts under which they work (Diller, 1990). This notion was supported by written feedback from one of the respondents at the pamphlet validation stage:
‘I suppose it is because teamwork is such a complex process to analyse. It is not a recipe of ingredients like food or objects. Teamwork
depends on a team made up of people. Person-alities are complex and changing. I think that a teamwork model only exists in theory. Each team has its own model.’ (Physiotherapist, Team C)
The continued reference to models of team-work in the provision of neurological ser-vices may therefore restrict the adequate description and investigation of the collab-orative methods by which the team approach is delivered.
The teamwork processes in neurological rehabilitation
These findings have provided a large amount of information which has begun to answer the research question about team functions and processes that are perceived to occur within the three teams studied. A large number of the teamworking processes that have been described in previous research were reportedly in use across the three teams. But there were also differences — suggesting that different teams may choose different strategies depending on the aims and context of the team effort. Correspond-ing with the findings of Playford et al. (2000), all three teams used goal planning when working in their team, but there were varia-tions in how it was structured, organized and in the level of patient involvement. These goal-planning processes did not relate to other multi- or interdisciplinary methods of working reported by the team members, or to the type of team (multi- or interdisciplin-ary) that they felt they worked in.
Investment in team training (Barr, 1997) or a lack of team training (Gibbon, 1999) have been discussed as influencing how a team works together, and regular staff train-ing was perceived to be an important con-tributor to the benefits of stroke unit care (Stroke Unit Triallists Collaboration, 1997).

Suddick and De Souza82
Physiother. Res. Int. 11: 72–83 (2006)Copyright © 2006 John Wiley & Sons, Ltd DOI: 10.1002/pri
L1
These findings may support greater invest-ment in the training of the neurological reha-bilitation team, and, in particular, in stroke unit teams. Having an opportunity to reflect on how well a team works together, either formally or informally, may ensure that a team and its members have the opportunity to evaluate their performance and learn together (Barr, 1997). Neurological teams that are not undertaking reflection may be limited in the development of the team and the service which it provides (Molyneux, 2001). The role of reflection in the develop-ment and sustaining of optimum methods of working within available team resources requires further investigation. Evaluating team effectiveness and the critical factors for effective and ineffective teamwork is the subject of another paper.
IMPLICATIONS
There has been no similar research under-taken on teamwork in neurological reha-bilitation within the UK. The present study has therefore provided a starting point for the development of hypotheses and future areas of research in this field. These study findings suggest that the occupational therapists and physiotherapists studied believed the rhetoric behind the benefits of teamwork in neurological rehabilitation (Pound and Ebrahim, 2000). Some of the participants had worked in neurological rehabilitation teams for a number of years and that they were still reporting these perceived benefits suggests that these neu-rorehabilitation team members’ percep-tions corresponded with the literature supporting the wide-ranging positive implications of teamwork. The present study has also demonstrated that interdis-ciplinary teamwork has not been adopted consistently by all neurological teams, that
there are differences in the structure and membership of teams and that there are an extensive and varied number of functions and processes which occur as part of working within different types of neuro-logical rehabilitation teams. There needs to be a deeper understanding of the nature of these processes before their effective-ness can be evaluated.
Further research must explore the issue of patient and carer involvement within teams, and whether the neurological reha-bilitation service users: patients, clients and family members, have similar or conflicting perceptions and experiences of neurological teamwork. The development of a more adap-tive and realistic neurological rehabilitation team model also needs to be evaluated and developed through future study.
REFERENCES
Barr O. Interdisciplinary teamwork: consideration of the challenges. British Journal of Nursing 1997; 6(17): 1005–1010.
Boaden N, Leaviss J. Putting teamwork in context. Medical Education 2000; 34: 921–927.
Booth J, Hewison A. Role overlap between occupa-tional therapy and physiotherapy during in-patient stroke rehabilitation: an exploratory study. Journal of Interprofessional Care 2002; 16: 31–40.
Chartered Society of Physiotherapy. Rules of Pro-fessional Conduct (second edition). London: CSP, 2002.
College of Occupational Therapists. Code of Ethics and Professional Conduct for Occupational Ther-apists. London: COT, 2000.
Coopman SJ. Democracy, performance, and out-comes in interdisciplinary health care teams. Journal of Business Communication 2001; 37: 261–286.
Curry A, Herbert D. Continuous improvement in public services — a way forward. Managing Service Quality 1998; 8: 339–349.
Davis A, Davis S, Moss N, Marks J, McGrath J, Hovard L et al. First steps towards an inter-disciplinary approach to rehabilitation. Clinical Rehabilitation 1992; 6: 237–244.
Therapists’ experiences of teamwork in neurological rehabilitation 83
Physiother. Res. Int. 11: 72–83 (2006)Copyright © 2006 John Wiley & Sons, Ltd DOI: 10.1002/pri
L1
Dawson J, Bartlett E. Change within interdisciplinary teamwork: one unit’s experience. British Journal of Therapy and Rehabilitation 1996; 3: 219–222.
Department of Health. The NHS Plan — A Plan for Investment, A Plan for Reform. London: DoH, 2000.
Diller L. Congress Presidential Address: Fostering the interdisciplinary team, fostering research in a society in transition. Archives of Physical and Medical Rehabilitation 1990; 71: 275–278.
Feiger SM, Schmitt MH. Collegiality in interdisci-plinary health teams: its measurement and its effects. Social Science and Medicine 1979; 13A: 217–229.
Gibbon B. An investigation of inter-professional col-laboration in stroke rehabilitation team conferences. Journal of Clinical Nursing 1999; 8: 246–252.
Gibbon B, Watkins C, Barer D, Waters K, Davies S, Lightbody L et al. Can staff attitudes to team working in stroke care be improved? Journal of Advanced Nursing 2002; 40: 105–111.
Halstead LS, Rintala DH, Kanellos M, Griffin B, Higgins L, Rheinecker S et al. The innovative rehabilitation team: an experiment in team build-ing. Archives of Physical and Medical Rehabilita-tion 1986; 67: 357–361.
Indredavik B, Bakke F, Slordahl SA, Rokseth R, H?heim LL. Treatment in a combined acute and rehabilitation stroke unit. Which aspects are most important? Stroke 1999; May: 917–923.
Keats DM. Interviewing. A Practical Guide for Students and Professionals. Milton Keynes: Open University Press, 2000.
Kvale S. Interviews. An Introduction to Qualitative Research Interviewing. Thousand Oaks, CA: Sage Publications, 1996.
LaRocca NG, Kalb RC. Efficacy of rehabilitation in multiple sclerosis. Journal of Neurorehabilitation 1992; 6: 147–155.
McGrath JR, Davis AM. Rehabilitation: where are we going and how do we get there? Clinical Rehabili-tation 1992; 6: 225–235.
McGrath JR, Marks JA, Davis AM. Towards interdis-ciplinary rehabilitation: further developments at Rivermead Rehabilitation Centre. Clinical Rehabilitation 1995; 9: 320–326.
Melvin JL. Interdisciplinary and multidisciplinary activities and the ACRM. Archives of Physical Medicine and Rehabilitation 1980; 61: 379–380.
Molyneux J. Interprofessional team-working: what makes teams work well? Journal of Interprofes-sional Care 2001; 15: 29–35.
Newall JT, Wood VA, Langton Hewer R. Develop-ment of a neurological rehabilitation environment: an observational study. Clinical Rehabilitation 1997; 11: 146–155.
Nieuwenhuis R. Teamwork in Neurology (Therapy in Practice 40) London: Chapman & Hall, 1993.
Pethybridge J. How team working influences dis-charge planning form hospital: a study of four multi-disciplinary teams in an acute hospital in England. Journal of Interprofessional Care 2004; 18: 29–41.
Playford ED, Dawson L, Limbert V, Smith M, Ward CD, Wells R. Goal setting in rehabilitation: report of a workshop to explore professionals percep-tions of goal setting. Clinical Rehabilitation 2000; 14: 491–496.
Pound P, Ebrahim S. Redefining doing something: health professionals views on their role in the care of stroke patients. Physiotherapy Research Inter-national 1997; 2: 12–28.
Pound, P. Ebrahim, S. Rhetoric and reality in stroke patient care. Social Science and Medicine 2000; 51: 1437–1446.
Robinson I. The rehabilitation of patients with long term physical impairments: the social context of professional roles. Clinical Rehabilitation 1998; 2: 339–347.
Schut HA, Stam HJ. Goals in rehabilitation team-work. Disability and Rehabilitation 1994; 16: 223–226.
Stead A, Leonard MC. Changing to a client-focused quality service through more effective team-work. Health Manpower Management 1995; 21: 23–27.
Strasser DC, Falconer JA, Martino-Saltzmann D. The rehabilitation team: staff perceptions of the hospital environment, the interdisciplinary team environment, and interprofessional relations. Archives of Physical and Medical Rehabilitation 1994; 75: 177–182.
Stroke Unit Triallists Collaboration. Collaborative systemic review of the randomised trials of organ-ised inpatient (stroke unit) care after stroke. British Medical Journal 1997; 314: 1151–1159.
Address correspondence to: Ms Kitty M Suddick, Senior Lecturer in Physiotherapy, School of Health Professions, University of Brighton, Robert Dodd Building, 49 Darley Road, Eastbourne, East Sussex BN20 7UR, UK (E-mail: [email protected]).
(Submitted October 2005; accepted February 2006)