Team Essentials for Preventing Acute Deterioration › files › 2016 › 09 ›...
75
Team Essentials for Preventing Acute Deterioration Reference Guide for Learners Version 1.0 March 2016
Transcript of Team Essentials for Preventing Acute Deterioration › files › 2016 › 09 ›...

Team Essentials for Preventing Acute Deterioration Reference Guide for Learners Version 1.0 March 2016

Pag
e1
Prepared by the Baycrest Centre for Learning, Research and Innovation in Long Term Care as part of
Team Essentials: Leading Practices for Long-Term Care.
This reference guide supports learners who have participated in the 1-day module on
Team Essentials for Preventing Acute Deterioration.
For more information, please contact the Lead Interprofessional Educator:
Jennifer Reguindin at [email protected]
Prepared by:
Jennifer Reguindin BScN MScN RN GNC(c)
Reviewers (alphabetically):
Faith Boutcher MN RN
David Conn MB BCh BAO FRCP
Shoshana Helfenbaum MSW RSW
Paul Katz MD
Monika Keri BScN MScN RN
Joyce Kuang BKin
Raquel Meyer PhD RN
Maria Nelson BScN RN GNC(c) ABA(c) CPMHN(c)
Disclaimer: This reference guide is not binding for users . It neither consti tutes a liability nor a discharge from
liability. While every effort has been made to ensure the accuracy of the contents at the time of publication,
nei ther the authors nor Baycrest Geriatric Centre give any guarantee as to the accuracy of the information
contained in the guide, nor accept any liability, with respect to loss , damage, injury or expense arising from any
such errors or omissions in the contents of this work. Any reference throughout the guide to specific products as
examples does not imply endorsement of any of these products.
Supported with funding from the Government of Ontario.
The views expressed are the views of the authors and do not necessarily reflect those of the Province.
© 2016 Baycrest Geriatric Centre. For indvidual use only.

Pag
e2
CONTENTS
Foreword ................................................................................................................................................................ 4
Introduction......................................................................................................................................................... 4
Core Frameworks ................................................................................................................................................ 6
The 3Rs Clinical Framework ............................................................................................................................. 6
SBAR Reporting Framework............................................................................................................................. 7
Abbreviations ...................................................................................................................................................... 8
A. BASELINE ............................................................................................................................................................ 9
Health History...................................................................................................................................................... 9
Social & Family History ...................................................................................................................................... 10
Personhood ....................................................................................................................................................... 10
Continuous Monitoring or Trending ................................................................................................................. 10
B. RECOGNIZE ....................................................................................................................................................... 11
Objective Observation....................................................................................................................................... 11
Common Conditions .......................................................................................................................................... 11
1. Delirium .................................................................................................................................................. 12
2. Dehydration............................................................................................................................................ 13
3. Urinary Tract Infection ........................................................................................................................... 14
4. Respiratory Infection .............................................................................................................................. 15
5. Chronic Obstructive Pulmonary Disease (COPD) Exacerbation ............................................................. 16
6. Septicemia .............................................................................................................................................. 17
7. Decompensated Heart Failure ............................................................................................................... 18
8. Myocardial Infarction (Heart Attack) ..................................................................................................... 19
9. Ischemic Stroke ...................................................................................................................................... 20
10. Diabetes: Hypoglycemia ..................................................................................................................... 21
10. Diabetes: Hyperglycemia .................................................................................................................... 22
Prioritize ............................................................................................................................................................ 23
A Note on Risk ................................................................................................................................................... 25
Basic Information for Any New Situation.......................................................................................................... 26
C. REFLECT............................................................................................................................................................. 27
Critical Thinking: Considerations with Any Change .......................................................................................... 27
Which Systems are Affected? ........................................................................................................................... 28
1. Safety ...................................................................................................................................................... 30
2. Neurological – Head, Nerves, & Pain ..................................................................................................... 31
3. Mood & Behaviour ................................................................................................................................. 34
4. Sensory – Eyes, Nose, Ears, Tongue ....................................................................................................... 36

Pag
e3
5. Respiratory – Breathing & Lungs............................................................................................................ 38
6. Cardiovascular – Heart & Circulation ..................................................................................................... 40
7. Integumentary – Skin & Touch............................................................................................................... 42
8. Gastrointestinal – Mouth, Digestion & Elimination ............................................................................... 45
9. Genitourinary – Renal & Elimination ..................................................................................................... 48
10. Musculoskeletal – Muscles & Bones .................................................................................................. 50
11. Function – ADLs, IADLs, Programs & Roles......................................................................................... 52
Systems Observed (Look & See) by Task........................................................................................................... 53
Considerations: Using SOS as a Reflective Checklist ......................................................................................... 54
D. RESPOND .......................................................................................................................................................... 55
Actions in the Moment ..................................................................................................................................... 55
Critical Sign or Symptom – Personal Support Staff ........................................................................................... 56
Critical Care Path – Nursing Staff ...................................................................................................................... 56
Sharing Actions & Assessments ........................................................................................................................ 57
Asking for or Recommending What is Needed ................................................................................................. 57
SBAR & Asking for Help: What to Include in Your Report................................................................................. 58
Introduction ................................................................................................................................................... 58
Situation ......................................................................................................................................................... 58
Background .................................................................................................................................................... 58
Action & Nursing Assessment........................................................................................................................ 59
Recommendations & Requests ..................................................................................................................... 59
Appendix A: SBAR Work Sheets........................................................................................................................... 61
PSW Worksheet................................................................................................................................................. 61
Nurse Worksheet .............................................................................................................................................. 62
Appendix B: Head-to-Toe Report Example ......................................................................................................... 63
Systematic Reporting Approach .................................................................................................................... 63
Sensory Observation Reporting Approach .................................................................................................... 63
Appendix C: What Does “OK” Mean?.................................................................................................................. 65
Neurological, Mood, Senses, Musculoskeletal & Function ........................................................................... 65
Respiratory..................................................................................................................................................... 65
Cardiovascular & Integumentary ................................................................................................................... 65
Gastrointestinal & Genitourinary .................................................................................................................. 65
References ............................................................................................................................................................ 66

Pag
e4
FOREWORD
Introduction
This reference guide was designed for staff and student healthcare providers who have participated in Team
Essentials – Leading Practices for Long-Term Care: Preventing Acute Deterioration. The purpose is to help long-
term care healthcare providers recognize, prioritize, reflect and respond to acute changes in the health status
of residents. Being more attuned to the changing needs of frail elders will improve the care provided and the
resident-provider relationship.
Some elderly residents have atypical signs or presentations of deterioration. To assist in identifying early acute
changes, this reference guide includes signs and symptoms of common conditions that may lead to the
transfer of elderly residents from long-term care to acute care emergency departments. This list of conditions
is specific to the geriatric population. The reference guide is based on current best and clinical practice
guidelines.
The Sensory Observation System (SOS) was created to help healthcare providers and students recognize,
prioritize and respond to subtle and acute changes in the health status of elderly residents. The SOS consists of
a head-to-toe assessment whereby senses (i.e., sight, touch, hearing and smell) are used to identify
observations and assessments which are grouped by system. It provides a systematic checklist to use when
observing and assessing physical, cognitive, emotional and functional changes in residents, in order to prevent
worsening of their condition.
The reference guide includes examples of:
Which systems may need to be considered
What information may need to be included
How the reporting term “OK” can be used by a team in a way that supports objective, specific and
concrete observations and reporting
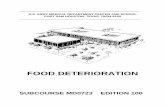
The SOS requires baseline knowledge of the resident and is used with a 3Rs clinical framework. The 3Rs ask
the healthcare provider to: Recognize, Reflect and Respond. Each step is based on professional readiness and
accountability. Figure 1 below depicts this process:

Pag
e5
Self/ Professional Readiness
Find Baseline
Continuous Monitoring
RECOGNIZE Priority
REFLECT
RECOGNIZE Change or Distress?
RESPONDEffective?
Team/SBAR Report
NO
YES
RESPOND: Pharm or Non-Pharm
Figure 1. Process Flow for the 3Rs Clinical Framework
All healthcare providers need to develop an understanding of the resident’s background and relevant
information in order to establish a baseline for future observations. Ensuring that the resident is safe in his or
her environment is always essential when observing or assessing a resident, but when a change in health
status is recognized, SOS is used systematically from head-to-toe starting with the neurological system and
ending with integumentary system. If the changes are localized to a system, SOS guides clinicians to perform a
focused system assessment. Finally, function, which is a great indicator of an elderly resident’s health
condition, is incorporated into the report to complete a picture of the resident’s situation.

Pag
e6
Core Frameworks
This module incorporates a clinical framework and a reporting framework.
The 3Rs Clinical Framework
Recognize: the signs, symptoms, risk and priority
Reflect: knowledge, observations and assessments
Respond: pharmacological, non-pharmacological or relational interventions and reporting
The 3Rs is a foundational clinical framework for healthcare providers to use in the face of any clinical situation
– whether it is responding to an acute emergency, understanding a resident’s responsive behaviours or
interacting with a concerned family. This framework is sequential, whereby healthcare providers are
encouraged to first recognize and understand the situation, then to reflect upon their observations and finally,
to respond appropriately.
Step 1 is to Recognize by:
i. Observing and assessing the change(s) based on risk and priority
ii. Identifying what may have triggered change(s).
iii. Identifying safety concerns that affect the resident and others.
Step 2 is to Reflect on:
i. The resident's known background and history to form a baseline.
ii. Systematic changes which may be connected to the original concern.
iii. The resident's function to create a fuller picture of the resident's current situation and overall health
condition.
Step 3 is to Respond by:
i. Providing appropriate interventions (pharmacological, non-pharmacological, relational).
ii. Describing the effectiveness of actions taken.
iii. Determining if further clinical diagnostic testing is needed.
iv. Reporting situation, background, actions and recommendations to the team.

Pag
e7
SBAR Reporting Framework
Situation – concern, risk/urgency
Background – baseline, observations/assessment
Action (unregulated & regulated staff) – intervention, outcomes
Assessment (regulated staff) – ruled out, overall picture
Recommendation/Request
The SBAR is a structured communication tool that is used to communicate any resident or family concerns
between team members. It has been tailored to allow personal support workers in long-term care to share
their knowledge, interventions and requests with the team. SBAR offers healthcare providers a thorough,
systematic and effective way of providing accurate information to the care team and beyond. This framework
allows information to be shared clearly and comprehensively in a short amount of time, thus making it critical
for urgent and emergency concerns. However, because clear communication is necessary for efficient
teamwork, SBAR is also suitable for non-urgent situations (e.g., action needed within hours, team rounds).

Pag
e8
Abbreviations
The following abbreviations are used in this Reference Guide.
ADLs Activities of Daily Living
3Rs Recognize, Reflect and Respond
BM Bowel Movement
Ca2+ Calcium
COPD Chronic Obstructive Pulmonary Disease
Fe+ Iron
GERD Gastroesophageal Reflux Disease
IADLs Instrumental Activities of Daily Living
kg Kilograms
LOC Level of Consciousness
PSW Personal Support Worker
SBAR Situation, Background, Action/Assessment, Recommendation/Request
SOS Sensory Observation System
UTI Urinary Tract Infection
VS Vital Signs
In this reference guide, the term ‘resident’ is used (instead of client or patient) to reflect the population living
in long-term care (i.e., persons who ‘reside’ in long-term care homes).

Pag
e9
Team Essentials for Preventing Acute Deterioration
A. BASELINE
In order to identify changes in a resident, there must be an initial reference point for comparison. This
reference point is referred to as the resident’s baseline. To establish a baseline, healthcare providers must
understand the resident’s background, health history and social history and must obtain relevant information
about the resident using a head-to-toe approach. All time spent with a resident is an opportunity to build on
or confirm baseline knowledge. The longer a healthcare provider knows a resident, the more comprehensive
baseline knowledge.
How do you get to know your resident?
What do you need to know?
Health History
Health history information is needed to establish baseline knowledge of your resident. Knowing this
information will allow you to anticipate what may go wrong when the health of the resident deteriorates or
what conditions may develop in the future. It also allows healthcare providers to understand the goals of care
that the healthcare team sets for the resident.
Questions to consider are:
What is the primary diagnosis?
What is the past medical history?
Are the changes being reported relevant to the primary diagnosis or to past medical history?
Does the resident have any allergies?
What is the resident’s code status?
Is there an advanced care plan?
What are the resident’s treatments and therapies?
Are there any recent changes?
Is it relevant to the advanced care plan?
What is written in the kardex? Is it up to date?
What is the care plan for this resident?

Pag
e1
0
Social & Family History
Social and family history can help healthcare providers to understand the resident’s current or past
environment. Some resident responses and interactions may be more easily understood in the context of this
information.
Questions to consider are:
Is there a relevant family practice or tradition that is important to the resident?
What stories do your colleagues, family members, volunteers or visitors share about the resident that are
significant to the care you are giving?
Personhood
For residents with cognitive decline or impairment such as Alzheimer’s Dementia, knowing the story of the
resident is key to creating solutions or interventions to many behaviours and psychological symptoms; also
known as “responsive behaviours”.
Questions to consider are:
Who was the resident before they came to the nursing home? What makes them tick?
What are their interests, needs, abilities and skills?
What are the resident’s culture, childhood, work life and education?
Are there any relevant or important stories or events?
Can you engage the resident in any activities based on this knowledge?
What would allow you to relate well with the resident?
How do you present yourself when relating with the resident?
Are there techniques that are relevant to caring for the resident?
Are there environmental factors that the resident prefers?
What is the resident able to do for him or herself?
Continuous Monitoring or Trending
Remember that the longer a healthcare provider knows the resident, the more the healthcare provider will
have developed a comprehensive baseline. Any time spent with a resident is an opportunity for the healthcare
provider to add to or confirm baseline knowledge of the resident. Each healthcare provider should consider the
trends observed in their own practice and by the team.
Consider what you know about the resident, from your baseline observations vs. over t ime.
Is there a trend?
Report any change.

Pag
e1
1
B. RECOGNIZE
This section will cover:
Recognizing and describing specific concerns objectively
Prioritizing new changes
All healthcare providers must be skilled in recognizing changes in resident condition. Communicating this
knowledge in a concise and specific manner is essential. In order to develop this skill, this section describes the
presentation of acute deterioration related to several conditions in the geriatric population. Also, prioritization
of these new changes will be discussed. Signs and symptoms that are localized (system-specific or easily
identifiable towards a body system) and general (non-localized) will be covered.
Objective Observation
It is important to maintain objectivity when noting signs and symptoms in order to plan and implement
interventions. The Sensory Observation System (SOS) developed for Team Essentials can guide healthcare
providers in determining the best method of assessment and encourages systematic observation. Based on
the senses, SOS directs the healthcare provider to:
Look and see
Listen and hear
Touch and feel
Smell
And consider further knowledge gathered
Common Conditions
Listed below are ten common conditions that may lead to an acute change in a resident’s condition. Note that
deterioration of chronic conditions in the frail elderly may present very differently compared to the general
population. Thus, the signs and symptoms listed below are specific to the elderly population. Many resources
were used to compile these signs and symptoms. In particular, practice guidelines from the former American
Medical Directors Association (now The Society for Post-Acute and Long-Term Care Medicine) were followed
and information from various sources was then added to complete the list (see References).
As a note, behavioural changes, mental status changes and change in functional status may be cues to
delirium, dementia or depression. Further assessment and intervention will only happen if changes are
recognized, prioritized and shared with the team.

Pag
e1
2
1. Delirium
Delirium is sudden change or acute disturbance of consciousness. A resident with delirium may show signs
such as reduced ability to focus, organize thoughts, or shift attention that may not be accounted for by a pre-
existing cognitive impairment like dementia. Most conditions that will be discussed may have signs of a mental
status change and appear as confusion but there are different types of delirium to consider. Note that if there
is a change from baseline behaviour, this may be related to a change in condition that needs to be addressed.
Signs of Delirium
Sudden onset or change in behaviour, symptoms come and go and is a change from baseline
Change in mental status or cognition (organizing information, planning, sequencing, perception,
memory, language)
Inattention, no focus
Easily distracted
Disorganized thinking
Disorientation (confusion)
Altered level of consciousness
Memory impairment (long-term and short-term memory problems)
Psychomotor changes or ADL function
Visuospatial problems (less able to see and understand the world around them)
Perceptual disturbances
Reports of feeling “cloudy”
Labile (always changing) affect
Hyperactive-Hyperalert Delirium
Sleep/wake cycle disturbance (most common)
Agitation, restlessness
Paranoid
Delusions or hallucinations
Hyperreactivity
Speech incoherence
Hypoactive-Hypoalert Delirium
Decreased level of consciousness and lethargy
Sluggish
Inactive or few spontaneous movements
Apathetic
Quiet, responds slowly to questions
Loss of facial reaction
Mixed Delirium
Shows and changes between hyper- and hypo- signs

Pag
e1
3
2. Dehydration
Elderly residents who are dehydrated are at higher risk for delirium and infection. Age-related changes, some
disease processes and medications also affect how water is retained or eliminated.
General Signs & Symptoms
Change in:
ADL function or engagement in activities
Intake of food or fluids
Mental status (increasing confusion and/or lethargy)
Skin temperature
General malaise
Dizziness
Fall or deterioration in balance or gait
Other Signs & Symptoms
Constipation
Decreased urine output
Postural hypotension
Postural pulse difference
Tachycardia
Weight loss (3-5 pounds in a 24-hour time frame)
Elevated body temperature

Pag
e1
4
3. Urinary Tract Infection
Urinary tract infections (UTIs) are common in long-term care residents. Although localized symptoms allow for
easier recognition and assessment, at times general signs are seen first.
General Signs & Symptoms
Change in:
ADL function or engagement in activities
Intake of food or fluids
Mental status (increasing confusion and/or lethargy)
Skin temperature and/or color
Sleep pattern
Vital signs
Increased or excessive perspiration
General malaise
Dizziness
Nausea and/or vomiting
Fall or deterioration in balance or gait
Fever or hypothermia
Generalized pain, myalgia
Localized Signs & Symptoms
Suprapubic or flank pain or tenderness
Painful urination
Gross hematuria
Foul smelling urine
Change in continence level (e.g., urgency or functional)

Pag
e1
5
4. Respiratory Infection
Recognizing respiratory signs is very helpful when addressing respiratory infections. Keep in mind the
differences in signs based on the location of infection.
General Signs & Symptoms
Change in:
ADL function or engagement in activities
Intake of food or fluids
Mental status (increasing confusion and/or lethargy)
Skin temperature and/or color
Sleep pattern
Vital signs
Tachypnea with or without shortness of breath
Increased or excessive perspiration
General malaise
Dizziness
Nausea and/or vomiting
Fall or deterioration in balance or gait
Fever or hypothermia
Generalized pain, myalgia
Localized Signs & Symptoms
Pneumonia
Tachypnea
Unlike the general population, coughing may be mild and without copious, purulent
sputum, especially in dehydrated elderly residents
Upper Respiratory Infections
Congestion
Sore throat
Nasal purulence
Lower Respiratory Infections
Increasing and/or productive cough
Shortness of breath
Adventitious lung sounds

Pag
e1
6
5. Chronic Obstructive Pulmonary Disease (COPD) Exacerbation
Residents with COPD may have acute exacerbation of the disease and if not treated early enough may lead to
a transfer to acute care services.
General Signs & Symptoms
Change in:
Mental status (increasing confusion and/or lethargy)
Behavioural changes (irritability and anxiety)
ADL function or engagement in activities
Sleeping pattern (chronic change or observed change over a prolonged period)
Intake of food or fluids
Vital signs
Oxygen saturation < 88%
Respiration > 28 breaths per minute
Fever
Peripheral edema
Acute Changes Likely When
Dyspnea is present
Increased cough
Increased sputum production, change in color or thickness
Chest tightness
Wheezing
Accessory muscle use

Pag
e1
7
6. Septicemia
The frail elderly with multiple comorbidities, decreased immunity, dehydration and other risk factors have a
higher chance to develop an inflammatory body response. These signs may be missed if the diagnos is of is not expected (Nasa et al., 2012).
General Signs & Symptoms
Change in:
ADL function or engagement in activities
Intake of food or fluids
Mental status (increasing confusion and/or lethargy)
Skin temperature and/or color
Sleep pattern
Vital signs
Increased or excessive perspiration
General malaise
Dizziness
Nausea and/or vomiting
Fall or deterioration in balance or gait
Fever or hypothermia
Generalized pain, myalgia
Fever, Infections & the Elderly
The febrile response is usually blunted in the elderly. However, using this guideline may
indicate fever in the elderly (AMDA, 2011):
Increase in temperature of equal to or greater than 1.1 oC from baseline
2 or more measurements of oral temperature equal to or greater than 37.2oC
Single measurement of temperature equal to or greater than 37.8oC

Pag
e1
8
7. Decompensated Heart Failure
A gradual onset of signs and symptoms of heart failure may lead to emergency transfers and hospitalizations.
General Signs & Symptoms
Change in:
ADL function or engagement in activities
Intake of food or fluids
Mental status (increasing confusion and/or lethargy)
Skin temperature and/or color
Vital signs
General malaise (lethargic, less active, weakness)
Nocturia or nocturnal incontinence
Sleep disturbance
Increased potential for falls
New or increasing edema
Lower-extremity swelling
Localized Signs & Symptoms
New or increasing edema
Sacral edema for bedbound residents
Abdominal swelling
Increased shortness of breath with or without exertion
Dyspnea (less likely if patient is sedentary)
Unexplained cough
Sudden night time dyspnea (difficulty breathing) during sleep
Orthopnea (breathing comfortably only when standing or sitting up)
Unexpected and sudden weight gain (example is 2 kgs over 3 days)

Pag
e1
9
8. Myocardial Infarction (Heart Attack)
Signs and symptoms of a heart attack may present as “atypical”, which means the classic signs of chest pain
that healthcare providers wait for may not be present.
General Signs & Symptoms
Change in mental status (increasing confusion and/or change in level of consciousness -
syncope)
Fatigue or weakness
Dizziness
Generalized pain, myalgia
Increased or excessive perspiration, cold sweats
Common Manifestations
Dyspnea
Upper abdominal distress
Syncope
Vomiting
Chest pain

Pag
e2
0
9. Ischemic Stroke
There is a higher incidence of stroke in the elderly population and knowing these signs may allow a healthcare
provider to recognize a change.
Acute Stroke
Sudden confusion, difficulty speaking (slurred), or difficulty understanding speech
Sudden difficulty seeing out of one eye
Sudden difficulty walking, severe dizziness, or loss of balance or coordination
Sudden numbness or weakness of face, arm, leg – confined to one side of the body
Sudden severe headache with no other readily identifiable cause
Subtle or Non-Specific Signs of Ischemic Stroke
Dramatic decline in muscle strength, speech, or level of consciousness
Decline in function
Difficulty judging distance or depth
Difficulty recognizing or paying attention to one side of the body
Difficulty with new learning
Impulsiveness or poor planning
Poor judgment
Poor safety awareness
Short attention span
Change in mental status (increasing confusion and/or lethargy)

Pag
e2
1
10. Diabetes: Hypoglycemia
The elderly population present differently when blood glucose levels decrease. The neuroglycopenic
symptoms listed below are more common changes in the elderly as opposed to the neurogenic symptoms that the younger diabetic population may present with (Clayton et al., 2013).
Neuroglycopenic Symptoms*
Change in mental status (cognition, increasing confusion and/or delirium)
Difficulty speaking
Weak, drowsy, lethargic
Change in psychomotor skills or function
Lack of coordination
Dizziness (increased potential for falls)
Headache
Vision changes
*Neuroglycopenic symptoms are more common in the elderly .
Neurogenic Symptoms
Trembling
Palpitations
Sweating
Anxiety
Hunger
Nausea
Tingling
Asymptomatic hypoglycemia occurs in the frail older resident.

Pag
e2
2
10. Diabetes: Hyperglycemia
Undiagnosed diabetes leads to further complications (AMDA, 2010b).
General Signs & Symptoms
Change in mental status (new or increasing confusion or delirium)
Weak, drowsy, lethargic
Blurred vision
Worsening incontinence
Fruity breath odour
Thirstier than usual
Hungrier than usual

Pag
e2
3
Prioritize
Prioritizing changes makes good use of team resources, time and interventions. Knowing the resident’s
baseline, making observations and conducting assessments are necessary to prioritize a change as an
emergency, urgent or non-urgent. Prioritizing concerns determines how quickly to respond to a concern. A
stoplight system of red, yellow and green can be used to help visually flag the priority (Table 1).
Table 1. Prioritization of Concerns
Priority Level Response Time Stoplight
Colour
Emergency Address Immediately Red
Non-Urgent Address Within Hours Green
Emergency concerns need to be addressed immediately to preserve life (or limb). For example, when a
resident presents with new signs of facial drooping, one-sided limb weakness and slurred speech, these would
be considered signs of an Ischemic Stroke and call for an immediate transfer.
. This prioritization refers to situations where a
resident’s status will not improve or will deteriorate if further interventions are not provided. For example,
consider a resident who continues to be short of breath upon exertion but remains on room air with no
oxygen support and only non-pharmacological interventions have been used. If oxygen saturation of greater
than 92% there are other interventions that could be used to ensure the resident remains stable like applying
oxygen by nasal prongs or giving medication. This is considered urgent because the resident saturation may
not improve if further interventions are not provided.

Pag
e2
4
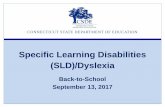
Figure 2 provides examples of emergency and urgent concerns by system.
Musculoskeletal
• Dramatic decline in muscle strength
• Falls
Integumentary
Skin looks gray or blue compared to
earlier appearance
Safety
Fall with fracture
Neurological
Sudden pain
Cardiovascular
Sudden edema or extensive bleeding
Function
Sudden decline in function compared
to earlier status
1
Neurological • Sudden change in LOC• Weakness on one side or seizure
Sensory
Sudden eye pain
Cardiovascular
• New/unrelieved chest pain,
tightness, pressure, discomfort with
known cardiac condition
• Hemodynamically unstable
Respiratory• Sudden or increased effort to
breathe at rest
• Respiration rate >28
• Obstruction
Gastrointestinal
• Rapid onset of abdominal pain or
distention
• Sudden weight gain
Genitourinary
Bleeding significantly
Mood & Behaviour
Sudden behaviour change
Photo Acknowledgement: Allen Cooper
Figure 2. Emergency and Urgent Concerns by System

Pag
e2
5
A non-urgent concern needs to be addressed within hours. Note: A non-urgent concern is still an important
concern (for example, you may take hours to further observe, assess, intervene and evaluate the change).
Prioritizing a concern as non-urgent allows the care team time to gather more information and to come up
with appropriate interventions. In some cases, non-urgent concerns may escalate if not addressed in a timely
manner. For example, when a stage 1 pressure ulcer is recognized and reported, the team then has time to
assess the new sore, identify contributing factors that led to the pressure sore and intervene as appropriate.
Figure 3 identifies some examples of non-urgent concerns by system (note: this is not a fully inclusive list).
Neurological• Lethargic
Sensory• Can’t perceive the same
Cardiovascular
• More swollen
Respiratory• Breathing faster (24-30), increased
secretions
Gastrointestinal• Decreased intake, change in continence
level
Genitourinary• Change in continence level or urine output
Musculoskeletal• Decline in muscle strength
Integumentary• New pressure ulcer, wound
Neurological
• Chronic painMood & Behaviour • Withdrawn
Function• Change in function compared
to earlier status
1
Figure 3. Non-Urgent Concerns by System
If the baseline established for the resident is known, then determining the priority of concerns is clear. If the
resident baseline is not known, a nurse should perform a head-to-toe assessment or focused assessment
(system specific assessment) to determine the priority.
A Note on Risk
Risk assessment of behaviors is necessary to keep residents and staff safe. It must be noted though that some
acute changes of conditions present as a sudden change in behavior. In this case, the sudden change must cue
a clinician into the urgency of the situation or a possible delirium. In some instances, these changes in
behavior may be seen as a responsive behavior due to dementia if a resident has this comorbidity. If so,
further assessment must be done by the team especially if new behaviours appear.

Pag
e2
6
Basic Information for Any New Situation
Table 2 can help organize communication about a concern and make it specific. Having this information right
at hand helps the healthcare provider highlight critical signs or symptoms and decide what additional
information is needed. See Appendix A for the full worksheet.
Table 2. RECOGNIZE: Situation Situation: What change requires the most attention?
Priority: Non-urgent, urgent or emergent Risk: Low, slight, moderate, high, potential to escalate
Trigger/Antecedent: What happened prior?
After reviewing Table 2, healthcare providers are encourage to practice using it with past clinical situations
experienced.

Pag
e2
7
C. REFLECT
This section will cover:
Thinking critically to compare the resident’s current status to background and baseline
Thinking critically to identify the potential source of the changes observed
Organizing signs and symptoms observed in a systematic manner
Critical Thinking: Considerations with Any Change
Drawing on the knowledge of the resident and his/her background and baseline, makes an important
difference in the care provided and allows healthcare providers to build a professional relationship that is
resident-centred.
When observing a change, consider:
1. Vital Signs (VS)
a) Are there significant changes in VS compared to the baseline?
b) If any of the VS are in the range listed in Table 3 below, act immediately, as the resident may be
hemodynamically compromised. If this is the case, the situation may be prioritized as urgent or
emergency.
c) With no change in VS, a healthcare provider has time to gather more data and the situation may be
prioritized as non-urgent.
Table 3. Critical Vital Sign Changes in the Elderly
TEMPERATURE 37.8 oC or 100.0oF
> or equal to 1.1oC from baseline
2 or more measurements of oral temperature = or >37.2oC
BLOOD PRESSURE Systolic: < 90 mmHg or > 200 mmHg
HEART RATE < 50bpm or >100 bpm
RESPIRATORY RATE <10/min or >28/min
OXYGEN SATURATION <90% (less than 88%, if COPD) or a 3% decrease from baseline
BLOOD GLUCOSE <3.9mmol or >16.6mmol
2. Is it delirium or delirium on dementia? Remember, there are numerous sources for delirium in elderly
residents.
a) Are basic needs being met?
Unmet needs may include: lack of food, lack of fluids, inability to void or defecate, lack of
sleep, presence of pain, or inability to breathe comfortably.
For example, a change in appetite may trigger hypoglycemia if food is not consumed but
diabetic medications are provided to the resident.
3. Is this a change due to disease progression or a new disease?
Some diseases have complications as it progresses. Also decompensations or deteriorations
happen in diseases such as heart failure or chronic obstructive pulmonary disorders.

Pag
e2
8
4. What other systems are affected or affecting the resident? Localized signs and symptoms may affect
other systems.
5. What is relevant about the change? Other considerations? Are there changes to treatment plans,
medications, any recent transfers or stressors?
6. Is it an increase in frailty or an age-related change?
Which Systems are Affected?
If a system is affected, you will find a signs and symptoms that can be grouped together. Organizing
observations by system may be helpful when working or communicating with the resident and the team. The
following section describes relevant information for each system in terms of:
Age-related changes
Systematic observations that healthcare providers may observe when working with the elderly
Examples of observations that require urgent attention
Examples of observations according to systems
Each system is reviewed as listed in figure 4 below:
1
Genitourinary
Kidneys, voiding
Neurological
Brain, mind, pain
Sensory
Eyes, ears, touch, taste,
smell
Cardiovascular
Heart
Respiratory
Breathing, lungs
Gastrointestinal
Mouth, digestion,
bowels
Mood & Behaviour
Musculoskeletal
Muscles, bones
Integumentary
Skin
Cardiovascular
Circulation
Function
ADL, IADL, programs,
roles
Safety &
Environment
Neurological
Pain
Background &
Baseline
Photo Acknowledgement: Allen Cooper
Figure 4. Review of the Descriptions of Each System

Pag
e2
9
With any changes to the resident, ask and consider, and then document and communicate: What is the change?
Be objective and specific
PSWs: What do you see, hear, smell, and feel that is different?
Nurses: What relevant systems are affected?
A sample head-to-toe report is found in Appendix B.

Pag
e3
0
1. Safety
Look & See
What does your safety environmental scan show?
Call bell in reach? Side rails up?
Non-slip shoes on resident?
Bed is low/near the ground?
Does the head of the bed facilitate better breathing and prevent skin breakdown?
Environment suited to reduce behaviours?
Feels like home?
How is the lighting?
Any excessive noise that may irritate the resident?
Bed/chair alarms on and working?
Restraints used?
Hip protectors on?
Could team offer more support for the resident’s memory?
Non-Urgent Concern (Act within Hours)
Reaction new to the environment
Reaction to sounds and loud environment
Reaction to warmth or coolness of environment
Reaction to new staff working with him or her
Some Safety Observations
Unable to follow safety precautions
Falling frequently

Pag
e3
1
2. Neurological – Head, Nerves, & Pain
Age-Related Changes
Less blood flow to brain leads to a decline in executive function – e.g., planning, attention and
problem solving abilities
Smaller and less brain size and neurons leads to slower speed of thinking, poorer short-term
memory, and a need for more time to reason things out
Slower nerve impulse (sensory and motor) changes movement and motor control
Slower movements, are not as balanced or coordinated
Bone thinning of the spine leads to less bones structure and may increase pressure to the spinal
cord and may lead to decreased response to stimuli and a need for a longer reaction time
Harder to choose words
More memory distraction
Less able to regulate heat
Less likely to show signs of elevated temperature typical of fevers when having an infection
Look & See
Level of consciousness?
Alert
Drowsy – lethargic, more tired or sleepier than usual
Confused - disoriented to person, time, place, altered perception
Drowsy and responding only to strong touch and verbal stimulation – stuporous
Not rousable and not responding - comatose
Mental responsiveness and orientation (name, time, place and purpose)?
Face even from left to right?
Listen & Hear
What is the resident saying?
Cognition - memory, recall, and identification
Complete and organized thoughts, understandable
No change in how the resident speaks
No word finding difficulty finding
Is there a positive or a negative theme?
Has sound judgment
Touch & Feel
Does not show new or sudden weakness
No reports of numbness to face, arm, trunk and/or leg
Equal strength and movement from both left and right limbs

Pag
e3
2
Ask & Consider Further
If there is pain present, consider the following:
Is it new or chronic?
What started it?
Where is the pain?
How long has the area been painful?
How much pain is the resident in?
What is the pain quality?
What treatment worked before?
Does the resident report any dizziness or lightheadedness?
If there are changes to energy levels:
How many hours of sleep has the resident had?
Was it enough for the resident to feel rested?
If the resident is non-verbal and/or cognitively impaired, consider history of painful chronic
disease and observe for:
Decreased interaction
Decreased food intake
Rocking movements
Grimacing
Negative language used
Physical or verbal aggression
Increased irritability
Breathing faster
Consider if there are physical changes related to pain and observe the following:
Gait
Posture
Appetite
Sleep patterns
Elevated BP
Increased respirations
Diaphoresis
Note the use of restraints and consider if there is a continued need for them
Urgent Concern (Act within 1 Hour)
Sudden change in level of consciousness – reduction in level of consciousness for example, from
alert to stuporous or non-responsive
Sudden confusion
Sudden change in speech – slurring or garbled speech
Sudden numbness limited to 1 side
New facial droop
New onset seizure

Pag
e3
3
Suicidal or homicidal thoughts
Non-Urgent Concern (Act within Hours)
Change in sleeping pattern
Worsening pain
New change in cognition
Decreased energy level—more lethargic, tired, weak, faint
Decrease in responsiveness
Chronic pain
Some Neurological Observations
Decreased alertness
Disoriented or confused
Pain present
Insomnia (not sleeping)
Fatigue

Pag
e3
4
3. Mood & Behaviour
Age-Related Changes
Less neurotransmitters and catecholamines that help with brain function such as cognition and
emotion
Poor sleep leads to an increased risk of major depression, memory problem and fewer social
interactions
Lethargy and hypo-alertness are NOT NORMAL in older adults with dementia
Look & See
Observe the resident’s affect (non-verbal reaction to environment)
Interactions with visitors, family, caregivers and staff
Positive or negative interaction?
Increased or decreased in quantity and/or quality?
Involvement in programs and activities
Is it more or less often than before?
Signs of boredom?
Is there any unexpected behaviour during care?
Is the resident hyperactive, more withdrawn (hypoactive) or resistant to care?
Listen & Hear
Interactions with visitors, family, caregiver and staff
Positive or negative theme when speaking?
Ask & Consider Further
What is the resident’s mood (what does resident say s/he is feeling)?
Is there a change?
Is there a presence or worsening of new responsive behaviours?
Is it: Delirium? Depression? Dementia?
Who is the behaviour affecting (staff, other residents, family)?
What is the behaviour and why might it be happening?
What happened beforehand?
What were the specific actions of the resident?
Describe and quantify
What or whom is around the resident at the time of the behaviour?
What is the resident saying?
When is this happening?
During the day or at night?
When is this NOT happening?
What can you do about it?
Has this behaviour occurred before?

Pag
e3
5
Which techniques were used? Which techniques were effective? Which techniques were
ineffective?
How long has this behaviour been happening?
Are there safety issues for staff, other residents, visitors, etc.?
Is there a behaviour that is now “normalized”?
Urgent Concern (Act within 1 Hour)
New delusions, paranoia, hallucinations
Violence or destructive tendencies to self and/or others
Suicidal or homicidal ideation present with or without a plan
Non-Urgent Concern (Act within Hours)
New onset behaviour or personality change or a significant change in behaviour:
Resisting or refusing care
Refusing to get up or move; staying in the same place
More withdrawn/sad or talking more than usual, negative themes
New or increased confusion/disorientation; delusions or hallucinations; severe depressed mood
Some Behaviour Observations
Increased motor activity or verbalization
Decreased interactions and participation
More withdrawn or more active than usual

Pag
e3
6
4. Sensory – Eyes, Nose, Ears, Tongue
Age-Related Changes
Eyes
Lens less flexible, which leads to decreased ability to focus on close objects (presbyopia)
and less able to adjust to changes in bright lighting (glare prevents seeing clearly)
Poorer night vision
Less sensitive cornea and conjunctiva
Less tear production
Less able to see colour differences
Cholesterol deposit lead to visual haziness
Ears
Outer ear enlargement
More ear wax impaction
Less elastic ear canal
Thinning and stiffening of the tympanic membrane
Less able to recognize speech
Less able to hear higher tones
Less able to follow conversations
Slower brain processes of auditory information
Inner ear structure – changes in vestibular system lead to more dizziness and falling
Nose
Less smell leads to less taste, which may lead to decreased appetite
Less able to identify odours
Higher chance of nose bleeds
Tongue
Less taste
Less saliva production
Look & See
Vision
Visual aids used – glasses, etc.?
Trouble seeing surroundings?
Blurred vision
With Hearing Aids
Comfortable fit
Batteries changed recently

Pag
e3
7
Listen & Hear
Hearing Deficits
Resident is responding to you
Ability to Communicate
Verbal or non-verbal
Ask & Consider Further
Vision
When was vision last checked and followed up on?
Seeing double?
Can’t see the same: decreased, blurry or lost vision?
New decreased or lost vision?
Any strain to see out of 1 eye?
Severe eye pain present?
Touch
Are there known tactile/touch risk issues?
Is there a loss of tactile sensation?
Urgent Concern (Act within 1 Hour)
Sudden change in vision (example, sudden change in visual fields or sudden inability to see out
of one eye)
Severe ear pain and bleeding or discharge from ear canal
Fast onset of hearing loss
Non-Urgent Concern (act within hours)
Seeing halos
Increasing glare from lights
Experiencing eye pain
Can’t see the same: new vision loss
Can’t hear, smell or taste the same
Some Sensory Observations
Can’t see, hear or taste the same

Pag
e3
8
5. Respiratory – Breathing & Lungs
Age-Related Changes
Stiffer chest wall and less lung muscle strength and elasticity
Decreased gas exchange
Drier mucus membranes
Decreased cough reflex leads to less ability to clear mucus/foreign matter and an increased risk
of infection and spasm of airway
Easier to lose breath when working harder than normal, which leads to less to tolerate exercise
Look & See
Depth
Deep or shallow
Rhythm
Regular or not
Respiratory rate
Fast or slow
Mouth breather
Discomfort when breathing
Any increased effort to breathe at rest or with activities
New or worsening shortness of breath only with activity
Increased need for more pillows to sleep in bed or a need to sit up to sleep
Listen & Hear
Wheezing
Coughing
Sneezing
Congestion
Ask & Consider Further
Is there a new cough?
How much and how often is the resident coughing?
What is the colour and quantity of sputum?
Urgent Concern (Act within 1 Hour)
Struggling to breathe
Short of breath at rest
Coughing up copious amounts of blood
Sudden or increased effort to breathe at rest
Non-Urgent Concern (Act within Hours)
Shortness of breath with activity or a change in breathing pattern

Pag
e3
9
Irregular or breathing fast
Slow breath recovery after an activity – e.g., ADLs or walking
New increased sputum production
New or worsened cough, wheezing
Sore throat
Some Respiratory Observations
Increased work of breathing at rest or during activities
New cough

Pag
e4
0
6. Cardiovascular – Heart & Circulation
Age-Related Changes
Thicker heart muscles, stiffer arteries and heart valves, thicker arterial walls and more fat
around the heart lead to more work for the heart
Less blood flow lead to cool arms, hands, legs and feet
Decreased number of white blood cells and decreased immune response resulting in higher risk
of infections
Lower maximum heart rate during exercise and a high risk of heart rhythm changes
Less cardiac reserve leads to more tiredness, shortness of breath and slower recovery from
higher heart rate – e.g., after exercise
Higher risk for a drop in blood pressure when changing positions (postural hypotension) – e.g.
Switching from laying down to sitting or sitting to standing
Look & See
Observe the overall colour of the resident
DIAPHORETIC – sweating too much
Edema or swelling
Where?
Legs, arms, sacrum, face, eyes and/or scrotum
How much?
Compare from left to right?
If subcutaneous lines are in use:
Where is it located?
What does the skin look like at the insertion site?
Is the dressing holding up?
Touch & Feel
Is the resident warm to touch?
Temperature – new fever?
Axilla drier than usual
Ask & Consider Further
Does the resident report:
Palpitations
Chest pain, chest tightness, pressure, discomfort and/or unusual sweating
(diaphoresis)?
Location of discomfort: neck, jaw, shoulder, arms, back and/or abdomen?
Some describe chest pressure as the sensation that “someone is sitting on my chest”
If needed, are the compression stockings on?

Pag
e4
1
Urgent Concern (Act within 1 Hour)
New or unrelieved chest pain, discomfort, pressure, heaviness or tightness with known cardiac
concerns
Sudden edema in only 1 leg with tenderness and redness
More than 5 lbs. weight gain in 3 days
No able to feel or sense touch in swollen legs
Non-Urgent Concern (Act within Hours)
Signs of dehydration:
Increasingly tired, sleepy, dry axilla
Signs of fever
Worsening edema in arms, legs, abdomen, sacrum or genitalia
Unable to sleeping laying down flat
Unable to stand without severe dizziness
Some Cardiovascular Observations
Chest pain or heaviness
Edema
Irregular heartbeats
Dizzy
Bleeding
Fatigued

Pag
e4
2
7. Integumentary – Skin & Touch
Age-Related Changes
Drier, more scaly and wrinkled
Less subcutaneous fat (under the skin) leads to less ability to stretch, and decease skin integrity
More visceral fat (deep)
Less able to sweat
Thinning and shrinking of the top layer of skin (epidermis) leads to slower healing
Fewer nerve cells leads to less ability to feel and sense
Less contact between dermis and epidermis (skin layers) lead to less nutrients exchange
Thinner scalp, pubic and axilla hair; also changes in colours
Higher risk of infection, trauma, cancerous les ions, and pressure ulcers
Thicker nasal and ear hair
More facial hair in women
Nails thicker, grow slower, become brittle and yellowed
Increased risk of splitting and infections of the nails due to less blood supply to nails
Look & See
Colour of skin
Pale, pink, yellow, flushed or bluish
Dry or DIAPHORETIC (excessive sweating)
Colour of legs
Pale, red, mottled
If there are wounds:
Is it a pressure ulcer? Rash? Hives? Blisters?
Boggy and/or red areas?
Is there any hardened skin around?
Any new changes to existing wounds?
Where is it?
Is there pain due to the wound?
How large is the area or wound?
What does it look like?
Red, yellow, black
Wet or dry
If there is drainage, what is its:
Quantity
Colour
What does the skin around the wound (PERIWOUND) look like?
Is there a dressing on it?
Dry and intact?
How often is it changed?

Pag
e4
3
Observe for:
Redness over pressure spots that does not blanch when touched
Visible scars
Bruises
Skin tears
New changes to moles
Touch & Feel
Warmth of skin
Drier or more clammy than usual
Smell
Any unusual smell to resident’s wound?
Ask & Consider Further
Are there positioning plans?
Is there use of special mattress or specialize cushions?
Presence of pressure sores depends on:
The ability to feel pressure-related changes
How often skin is wet
How often resident gets up and/or does physical activity
How much resident is eating and drinking
The risk of rubbing on a surface when being lifted or boosted
Urgent Concern (Act within 1 Hour)
Wound from a fall or trauma with significant bleeding
Colour of skin – gray or blue
Non-Urgent Concern (Act within Hours)
Some signs of dehydration
Tired or sleepy, dry skin, poor turgor in central locations (late sign)
Redness on and around pressure areas that don’t blanche when touched
A larger or worsening pressure ulcer or existing wound
A new skin tear
A lump that is felt in the breast area
Changes in skin colour – blue or yellow
Signs of chills
Showing excessive moisture due to incontinence
Diaphoresis – excessive sweating

Pag
e4
4
Some Integumentary Observations
Axilla drier than usual
Wounds larger and/or more drainage
Warm to touch
New reddened areas

Pag
e4
5
8. Gastrointestinal – Mouth, Digestion & Elimination
Age-Related Changes
Less able to taste
Diminished thirst drive
Less calories needed but same nutritional needs
Teeth sockets wearing away and decreasing gums leads to tooth loss
Risk of chewing problems contributing to poor nutrition
Decreased strength of chewing muscles
Thinner mucus lining in the mouth (less protection) leads to dry mouth
Weaker mucosal barrier lead to more risk of infection
Swallowing muscles are less effective leading to risk of swallowing difficulty (dysphagia)
Weaker peristalsis and weaker esophageal sphincters lead to GERD (heartburn)
Change in ability to absorb nutrients (Ca2+, Fe2+) and medications leads to further
considerations for pharmacological interventions
Higher risk of adverse drug reactions due to decrease in liver size, blood flow and cardiac
reserve
Less able to digest starch
Less bile production leads to less tolerance for fats
Less able to feel the need to defecate BUT constipation is NOT normal
Risk of fecal incontinence with disease (not when resident is healthy)
Look & See
Nutrition
Appetite (meals and snacks)
Appropriate diet and texture
Able to eat independently
Drinking enough
Intake is the same as usual
Oral condition
Condition of membranes in the mouth, lips and tongue
See if appearance is dry or moist, and pink or covered in white
Teeth (own or dentures)
Dentures fit comfortably
Appearance of abdomen
Not unusually bloated (DISTENDED)
Rounded
Flat
If there is nausea or vomiting:
How much, how often and what is vomited?
Elimination
Size and quality of stool

Pag
e4
6
No change in frequency, size, type and consistency of bowel movement
Ostomy: stoma, appliance, skin, effluent
Touch & Feel
Pain is present when touching abdomen
Listen & Hear
Voice is clear and there are no changes such as gurgling or wet voice
If there is a concern with swallowing
Coughing before, during or after swallowing
Pocketing food in mouth when eating
Choking concerns are addressed
More flatus (gas)
Smell
No unusual smell to resident’s breath (e.g., fruity odour)
No unusual smell to resident’s BM
Ask & Consider Further
Nutrition:
Too much salt or sugar or fat intake?
Indigestion
Appearance:
Sudden distention of abdomen?
Unexpected weight gain or loss?
Any sudden onset of abdominal pain or cramps?
If there is a feeding tube, consider:
Location
Placement of the tube
Amount of feeds
Type of feeds ordered
Volume and rate of feeds
If resident is diabetic:
How often do they have signs of hypoglycemia or hyperglycemia?
When was the date of last bowel movement?
Is a bowel routine needed?
Are laxatives used?
Change in frequency, size, type and consistency of the bowel movement?
Change to the continence level?
Toileting plan? How often?
Any unplanned weight loss or weight gain in the last month or quarter to consider?
Need Registered Dietitian or Speech Language Pathology assessment?

Pag
e4
7
Urgent Concern (Act within 1 Hour)
Rapid weight gain or weight loss (example 2 kg over 3 days)
Coffee ground-like or bloody emesis
Rapid onset of abdominal pain, distention, weight gain and rigid stomach, with or without
vomiting, but with known constipation
Choking during meals
Non-Urgent Concern (Act within Hours)
Change in appetite or intake pattern – decreased oral intake over past 24-48 hours
Dry mouth, lips and tongue
Reporting denture pain or a burning sensation in mouth
Nausea and/or episodes of vomiting
Swallowing difficulty: coughing, wet voice, voice changes when eating; pocketing food in mouth
Blood in stool (without history of hemorrhoids)
Acute onset of diarrhea or multiple episodes
Change in stool pattern (frequency, size, type and consistency of BM)
New constipation or no BM for 3 days (start planning intervention)
Abdominal pain or any sign of pain when abdomen is touched, bloating
Weight loss or gain – 5% over last 30 days or 10% over last 6 months?
Some Gastrointestinal Observations
Not eating or drinking
Nausea and/or vomiting
Pain or stomach tenderness
No BM or watery BM

Pag
e4
8
9. Genitourinary – Renal & Elimination
Age-Related Changes
Kidneys
Decreased kidney size, less blood flow and function leads to lesser ability to clear body
of drugs and toxic substances, resulting in higher risk of electrolyte imbalance
Leaves body in a more acidic environment
Lead to more risk of kidney injury and significant reactions from drugs
Higher risk of water retention in body (in heart failure)
Higher risk of dehydration
Bladder
Less elastic, has less muscle tone and less capacity
Bladder volume decreases from 500-600 ml to 150-250 ml
More urine left in bladder after voiding
More night time urine produced and need to void (nocturia and polyuria) – higher
risk of urinary urgency
Incontinence is NOT a normal finding
In females
Shorter urethra in women lead to a higher risk of UTI
Remember the relationship between UTI and increased potential for falls
Decreased estrogen lead to tissue shrinkage and less lubricating secretions
In males
Prostate enlargement, testicular shrinkage, less sperm count and decreased
testosterone
Larger prostate in men compresses the urethra and leads to difficulty or painful voiding
Look & See
Method of urination
Spontaneous
Continent or incontinent
If incontinent, check size and fit of incontinence prevention tool
Foley catheter
Condom catheter
Suprapubic catheter
A leg bag is attached with catheters
The resident is not ANURIC (does not void)
No dialysis needed
Frequency of resident’s voiding
Frequency does not increase at night
No urgency, pain when voiding or straining to void

Pag
e4
9
Quality of urine
Amount
Colour
Odour
Clear
No signs of blood in the urine
Smell
No unusual smell to resident’s urine
Ask & Consider Further
If there is a change to continence level, is there a toileting plan?
Is there:
Vaginal discharge or bleeding?
Itchiness to pubic area?
Burning on urination?
Blood in urine?
Is there any history of:
UTI?
Urinary retention?
Urgent Concern (Act within 1 Hour)
Bleeding significantly from vagina
Non-Urgent Concern (Act within Hours)
Blood in urine or more sediments in urine
Change in urination pattern (urgency, frequency or continence level)
Foul smelling or concentrated urine
Reporting pain or difficulty when voiding
Pain in lower abdomen, flank
Less urine output than usual
Some Genitourinary Observations
Incontinence
Pain when voiding
Frequency and/or urgency of voiding
Unusual smell
Not voiding

Pag
e5
0
10. Musculoskeletal – Muscles & Bones
Age-Related Changes
Less muscle mass and coordination (sarcopenia) leads to weakness and poor exercise tolerance
Leads to less strength
Leads to higher risk of disability, falls and unstable gait
Less cartilage-forming cells leads to more joint damage
Less lean body mass, more fat and less able to absorb calcium leads to bone thinning
Bone loss in women and men (after peak mass at ages 30 to 35 years) leading to higher risk of
fractures and/or osteoporosis
Less ligament and tendon strength, elasticity and flexibility
Cartilage erodes and leads to changes in how resident stands and his/her height; range of
motion limited, more joint instability, higher risk of osteoarthritis, less flexibility and less
mobility
Look & See
If the resident has resident fallen before:
Any changes in balance and gait, weight bearing, transfer, ambulation, and posture?
Any dramatic or ongoing decline in muscle strength?
How often are these falls?
Is the resident able to weight bear?
Are transfers or mobility aids needed and within reach?
Movement
No change in exercise or activity tolerance
No shuffling when walking
No tremors, rigidity
Coordinated movement
Observe feet and toenails to see if there is anything that may cause pain
Touch & Feel
Compare limb strength from left to right
Limbs equal in strength
No 1-sided weakness to face, arm, truck and/or leg
Joints moving normally for the resident
No evidence of pain on movement or at rest
No increase in rigidity or decrease in coordination
No changes to muscle tone
No odd bumps on the joints
Ask & Consider Further
Is the resident part of a:
Physiotherapy program?

Pag
e5
1
Occupation Therapy program?
Exercise/cardiac rehabilitation program?
Could this resident benefit from more range of motion or joint loading exercises –
active/passive?
Are hip protectors on for high risk fallers who have a history of frequent falls?
Is there a falls prevention plan in place?
If the resident is on bed rest, is there a positioning schedule?
Urgent Concern (Act within 1 Hour)
New onset one-sided weakness (face, arm, trunk, leg) – unequal limb strength
Fall with obvious broken bones or known blood thinner use
Dramatic decline in muscle strength
Non-Urgent Concern (Act within Hours)
Change in balance, weight bearing, transfer, ambulation, postural ability or gait
Change when walking, moving or joint range of motion
Increased weakness, tremors or rigidity
Decreased exercise /activity tolerance
Repeatedly falling
Known unequal limb strength from left to right
Some Musculoskeletal Observations
Pain
Stiffer when moved or moving
Weaker strength
New or increasing tremors or rigidity
Falling (new or frequent)

Pag
e5
2
11. Function – ADLs, IADLs, Programs & Roles
Age-Related Changes
Function is a resident’s ability to carry out his/her activities of daily living (ADLs), instrumental
activities of daily living (IADLs) and roles
Increased engagement in ADLs prevents excess disability
Providing an agenda for the day or task breakdowns with cue cards leads to better engagement
and positive benefits
Ensure activities and roles are based on the assessment of resident’s needs, interest, skills and
ability
Ask & Consider Further
Is there a sudden decline in function?
Is there a decrease in tolerance for one or more activities?
Is the resident participating more or less than usual?
What is the resident’s ability to do an ADL independently? (capacity)
E.g., Toileting, feeding, dressing, grooming, teeth brushing, ambulation and bathing
Will you be able to support the resident with a task breakdown?
Is there a change in the level of assistance required for the activities?
What is the resident’s capacity for IADLs?
E.g., Shopping, meal planning and preparation, housekeeping, laundry, transit, financial
management, using a telephone, medication management and driving
What Therapeutic Recreation programs does the resident enjoy?
Urgent Concern (Act within 1 Hour)
Sudden decline in function – ADLs, activity or engaging with others
Non-Urgent Concern (Act within Hours)
Showing signs of boredom or loneliness
Hesitation to do a simple task
Refusing programs or activities
Showing a steady decline in function (ADLs) and requiring increasing help
Decreased exercise or activity intolerance
Some Observations about Function
Not able to function in ADLs as before
Not participating in activities as per usual

Pag
e5
3
Systems Observed (Look & See) by Task
Some healthcare providers have deemed that a systematic head-to-toe observation is not always feasible
unless time is set aside. This section categorizes some systems that may be observed during an activity of daily
living when a healthcare provider is continuously monitoring the resident and using these instances to build
up on or confirm baseline knowledge of the resident.
Table 4. Summary of Systems Observed by Activity of Daily Living Safety Neuro Mood/Behaviour Sensory Resp CV Integumentary GI GU MSK Function
Bathing
Feeding
Dressing
Oral Care
Toileting
Ambulation
Transfers
Activities
Periodic
Checks
Remember that if a resident is able to speak and respond, then healthcare provider is able to collect more
information to trend and observe the systems. This will lead to a comprehensive definition of what is “ok” for
a resident (See Appendix C: What Does “OK” Mean? for sample descriptions of an “OK” system).

Pag
e5
4
Considerations: Using SOS as a Reflective Checklist
Table 5 can be used as a reflective checklist to put together what is known about the resident. Remember to
prioritize the affected system and act on it based on your knowledge, skill, judgment and scope of practice as a
healthcare provider. Please see Appendix A for the full worksheet.
Table 5. REFLECT: Background
Background & Baseline (vs. Current Presentation)
Personal and medical history:
Basic needs (intake, sleep, toileting, pain):
Sensory Observation System
Which system(s) are affected? How? Local? Systemic?
Safety/Environment:
Vital Signs:
Neurological:
Mood, Affect or Behaviour:
Respiratory:
Cardiovascular:
Gastrointestinal:
Genitourinary:
Musculoskeletal:
Integumentary:
Function:

Pag
e5
5
D. RESPOND
This section will cover:
Initiating appropriate actions and assessments
Highlighting needs, requests or recommendations to the team
Reporting systematically with SBAR
Planning for follow up
When encountering a resident with a change in condition, the healthcare provider must support the resident
to their best of ability in the moment so that the resident can be safe, supported and receive appropriate
interventions according to the care plan or level of care. Responding to a resident’s change, in the moment,
requires a few considerations, especially if the first observer is alone. If alone, consider the following:
Is the resident safe and comfortable before setting out to find a co-worker or equipment?
What resources are at available here/now?
Are there medications ordered for this specific event? If not know, does the nurse know?
Are there medical directives, policies, or orders that outline the diagnostics and laboratory testing
required?
Is there an advanced care plan that is documented that will prevent or guide further interventions?
Actions in the Moment
If providing a non-pharmacological intervention, consider the following:
Interventions – What was done?
Here are some examples:
If a resident is not waking up, was verbal communication or light touch tried?
If a resident is short of breath, are they safe and sitting? Were deep breathing exercises
tried?
How many times was the intervention tried?
For how long?
The number of attempts and duration of attempts are valuable pieces of information that may contribute to
the plan of care for a resident and should be shared with the team.
Outcome of Intervention (Consequences) – Did it work?
Effective: concern modified or stopped
Ineffective: concern accelerated or continued
Sharing the outcome of the intervention will be useful as the team changes or builds new interventions
based on the information shared.
Was there a noticeable trigger, antecedent or unmet need?

Pag
e5
6
Clinical interventions may vary between a medical condition and a concern based on a responsive behavior.
Consider these questions:
Is it an acute change due to a medical condition OR a delirium? Think about:
Medication, supplementary oxygen, increased VS checks, blood work, diagnostic testing,
consults or further observations by the team
Assess the need for transfer to acute care or further interventions
Is there a known responsive behaviour due to dementia or depression?
If yes, attempt the following non-pharmacological interventions: distract, engage in activity,
assist, redirect, instruct verbally, re-approach and monitor; if pharmacological intervention,
monitor
Consider milieu management
Critical Sign or Symptom – Personal Support Staff
When a PSW identifies multiple concerns, signs, or symptoms of a change in condition, it is imperative to be
precise and concise when reporting these changes to the registered staff. Highlighting the priority of the
change as non-urgent, urgent or an emergency will help registered staff pay attention to your concern.
If multiple concerns are present, use Figure 2to highlight and report observations to a nurse. This may assist in
the nurse’s further clinical assessment and intervention. If there is more than one emergent or urgent change,
list these systematically from head-to-toe, if possible. An example: A resident is coughing, breathing fast, has
repetitive vocalizations about not being able to breathe and appears anxious. The critical sign of breathing fast
and the symptom of repetitive vocalization about not being able to breathe should be reported first.
A carefully established baseline offers a clearer description of what changes are present in a resident.
Critical Care Path – Nursing Staff
After a registered nurse or physician completes an assessment, a critica l care path may be determined. All the
initial observations, prioritizations and interventions (pharmacological, non-pharmacological, relational) made
by the team lead to this determination.
After careful consideration of the change, identification of a care path provides guidance on how a resident
should be monitored and future monitoring and interventions that may be required as well as may set the
parameters for transfers to acute care emergency as needed.
For example, a new concern of a cough may lead to a respiratory infection, an exacerbation of chronic
obstructive pulmonary disorder or a decompensation of a congestive heart failure. Therefore, careful
assessment and evaluation are the keys to ensuring that the correct interventions are implemented by the
team.

Pag
e5
7
Sharing Actions & Assessments
Table 6 can help organize communication about specific actions or interventions taken and the resulting
outcomes. Nurses should provide an overall assessment of the potential critical care path. Please see
Appendix A for the full worksheet.
Table 6. RESPOND: Action, Safety & Assessment Interventions (Pharmacological or Non-Pharmacological)
• Number of trials • Duration of intervention
• Outcome (effective or ineffective) Nursing Assessment:
“I have ruled out …” (basic needs, delirium or other system change); “I think the problem may be …”
Asking for or Recommending What is Needed
Table 7 can help organize communication about any recommendations or requests. It helps you to be specific
about what the resident needs or what you need to help the resident. Please see Appendix A for the full
worksheet.
Table 7. RESPOND: Recommendation/Request PSW:
“I recommend …” (specific action, non-pharm interventions, further observation, monitoring and/or referrals); “Can I ask you to … / What can I do in the next __ minutes/hour?”
Nursing: “I recommend …” (non-pharm or pharm interventions, labs, consults,further assessment, review of medication side effects, monitoring and/or transfer); “Can I ask you to …?” (specific action)

Pag
e5
8
SBAR & Asking for Help: What to Include in Your Report
There are probably times when you ask for help, but you don’t get the response you desire. As a healthcare
provider, many elements need to be communicated concisely to help team members gain insight into your
knowledge of the resident. The SBAR communication tool has been tailored to assist healthcare providers in
long-term care in reporting to the team.
SBAR stands for:
Situation – concern, risk/urgency
Background – baseline, observations/assessment
Action (unregulated & regulated staff) – intervention, outcomes
Assessment (regulated staff) – ruled out, overall picture
Recommendation/Request
Introduction
When communicating with a new team member, be sure to introduce yourself. This will help avoid confusion
in the beginning. If on the phone, let the team member know where you work do they can identify your
specific location.
Situation
Always highlight the reason for the call according to priority, followed by specifics about the concern. This will
paint the picture for the other team member. Stating the priority helps team members to manage their time
and workload. If you were able to determine or observe what triggered the new concern, then share this too.
In short, let the team member know the main concern and whether it is an emergency, urgent or non-urgent?
Background
Share what you know in a systematic way using SOS. Pull together information from what you and the team
have observed and/or assessed and consider trends and relevant information. This is where systematic
observations or assessments and accurate prioritization are relevant. Comparing what is known from baseline
to how the resident is presenting now helps to figure out the next steps. Preparing this ahead of time
increases team efficiency and quality of care for the resident.
Always consider if basic needs are being met (e.g., eating, drinking, sleeping, toileting, oxygen, no presence
of pain). Pain is a common concern for the elderly. So with respect to basic needs, consider if the resident is
experiencing any pain, pressure, or discomfort that can be relieved without medications.
Pain is a commonly missed change that leads to complications, such as delirium.

Pag
e5
9
Action & Nursing Assessment
When you ask for help, always highlight some of the actions that you have done based on the signs or
symptoms that you’ve observed. Let the other team member(s) know if it was effective, so there is no
duplication of efforts.
Nurses should also communicate their overall assessment of the situation, which is the critical care path, to
ensure that the care provided is consistent and the goals of care are clear with the team. PSWs are
encouraged to share the critical sign or symptom observed.
Recommendations & Requests
It is always helpful for the other team member to understand why you need his or her help. In emergency or
urgent cases, relating what you need from your team also speeds up the process of achieving quality care for
the resident.
Consider the interventions listed below and your scope of practice. What clinical actions could another
member of the team assist, ordering, perform or evaluate?
Acute change due to a medical condition OR a delirium?
Medication, supplementary oxygen, increased VS checks, blood work, diagnostic testing,
consults or further observations by the team
Transfer to acute care
Responsive behavior due to dementia or depression?
Non-pharmacological interventions: distract, engage in activity, assist, redirect, instruct
verbally, re-approach and monitor
Milieu management, medications and monitoring, further consultation, organized assessments
and observations

Pag
e6
0
Table 8 summarizes the elements to be included in an SBAR report for acute deterioration.
Table 8. SBAR for Acute Deterioration in the Elderly
Introduction
Name, Position, Location, Resident
Situation (Recognize)
Situation: What change requires the most attention?
Priority: Non-urgent, urgent or emergent
Risk: Low, slight, moderate, high, potential to escalate
Trigger/Antecedent: What happened prior?
Background (Reflect)
Background & Baseline (vs. Current Presentation)
• Personal and medical history
• Basic needs (example, intake, sleep, toileting, pain)
Sensory Observation System
• Which system(s) are affected? How? Local? Systemic?
Action, Safety & Assessment (Respond)
Interventions (Pharmacological or Non-Pharmacological)
• Number of trials
• Duration of intervention
• Outcome (effective or ineffective)
Nursing Assessment:
“I have ruled out …” (basic needs, delirium or other system change);
“I think the problem may be …”
Recommendation / Request (Respond)
PSW:
“I recommend …” (specific action, non-pharm interventions, further observation, monitoring
and/or referrals);
“Can I ask you to … / What can I do in the next __ minutes/hour?”
Nursing:
“I recommend …” (non-pharm or pharm interventions, labs, consults, further assessment,
review of medication side effects, monitoring and/or transfer);
“Can I ask you to …?” (specific action)

Pag
e6
1
APPENDIX A: SBAR WORK SHEETS
PSW Worksheet
PSW Introduction Name, Position, Location, Resident
S
Situation (Recognize)
Current Concern: What change requires the most attention?
Priority: Non-urgent, urgent or emergency?
Risk: Low, slight, moderate, high, potential to escalate
Trigger/Antecedent: What happened prior?
B
Background (Reflect)
Background & Baseline (vs. Current Presentation)
- Personal and medical history - Basic needs (intake, sleep, toileting, pain)
Sensory Observation System
Which system(s) are affected? How? Local? Systemic? - Safety & Environment - Neurological - Mood & Behaviour - Sensory - Respiratory - Cardiovascular - Integumentary - Gastrointestinal - Genitourinary - Musculoskeletal - Function (ADL &IADLs)
A
Action & Safety (Respond)
Interventions
Number of trials
Duration of intervention
Outcome of intervention (consequence) Effective: concern modified or s topped
Ineffective: concern accelerated or continued
R Recommendation / Request (Respond) “I recommend … ” (specific action, non-pharm interventions,
further observation, monitoring and/or referrals)
“Can I ask you to … ” “What can I do in the next _____ min/hr?”
© 2016 Baycrest Geriatric Centre.

Pag
e6
2
Nurse Worksheet
Nurse Introduction
Name, Position, Location, Resident
S
Situation (Recognize)
Current Concern: What change requires the most attention?
Priority: Non-urgent, urgent or emergency?
Risk: Low, slight, moderate, high, potential to escalate
Trigger/Antecedent: What happened prior?
B
Background (Reflect)
Background & Baseline (vs. Current Presentation)
- Personal and medical history - Basic needs (intake, sleep, toileting, pain)
Sensory Observation System Which system(s) are affected?
How? Local? Systemic? - Safety & Environment - Neurological - Mood & Behaviour - Sensory - Respiratory - Cardiovascular - Integumentary - Gastrointestinal - Genitourinary - Musculoskeletal - Function (ADL &IADLs)
A
Action & Safety (Respond)
Interventions
Number of trials & duration
Outcome of intervention (consequence) Effective: behaviour modified or s topped Ineffective: behaviour accelerated or continued
Nursing Assessment (Respond) “ I have ruled out …” (basic needs, delirium or other body
system change, deterioration of a chronic condition)
“I think the problem may be ________.”
R Recommendation / Request (Respond) “I recommend … ” (non-pharm or pharm interventions , labs,
consults , further assessment, review of medication side effects,
monitoring, and/or transfer)
“Can I ask you to … ?” (specific action)
© 2016 Baycrest Geriatric Centre.

Pag
e6
3
APPENDIX B: HEAD-TO-TOE REPORT EXAMPLE
Remember: Look up, down and around
The following examples are based on a case study shown during the education day. The first example is listed
in a systemic reporting approach and the second is arranged in a sensory observation approach. In both types
of reports, descriptions written in bold blue represent a sign or symptom that a healthcare provider might
report to the team.
Situation Description:
When it was time for activities, Mr. Smith was lethargic with negative affect and interaction with staff.
Resident declined participating in his usual programs and reports being uninterested in them. He is more
withdrawn than usual.
Patient Background:
Mr. Smith is an 85-year old resident, who likes to eat and attend sing-a-long activities. He is usually pleasant
and his wife visits regularly in the evenings.
Table 9. Comparison of the Systematic Reporting and Sensory Observation Reporting Approaches
Systematic Reporting Approach Sensory Observation Reporting Approach
Safety
Resident sitting in armchair with no safety issues
noted.
Neurological/ Psychological
Awake, lethargic, but converses appropriately. Face is
even from left to right. Complete and organized
thoughts, understandable but has negative theme.
Unable to observe limb strength. The resident was
not asked verbally if he was in pain, but no non-verbal
signs of pain were present.
Mood & Behaviour
Negative affect observed. Negative interaction with
staff. Resident declines to participate in the
programs he usually attends. No restlessness but
more withdrawn than usual.
Sensory
He does not wear glasses or hearing aids. He can hear
Look & See: (Neuro, Mood, Sensory, Respiratory, CV,
Integumentary, GI, GU, MSK, Safety)
Awake, lethargic but converses appropriately.
Non-verbal signs of pain not present but resident
was not asked verbally.
Negative in his affect and is interacting more
negatively with staff.
Regular breathing. No noted discomfort with
breathing.
No edema observed. Not diaphoretic.
Skin pink. No wounds seen at this time.
Resident sitting in chair. Able to turn his head
from side to side with no noted discomfort.
Resident sitting in armchair with no safety issues
noted.
Listen & Hear: (Neuro, Sensory, Resp, GI)
Complete and organized thoughts,
understandable but has a negative theme.

Pag
e6
4
well. No known tactile risk issues.
Respiratory
Regular breathing. No noted discomfort. No cough.
Cardiovascular
No edema observed. No subcutaneous lines. Not
diaphoretic. Unable to feel warmth of skin at this
time.
Skin
Skin pink. No noted wounds at this time. No excessive
sweating noted.
Gastrointestinal
Unable to observe oral mucosa, teeth, abdomen or
elimination.
Genitourinary
Unable to observe elimination at this time.
Musculoskeletal
Resident sitting in chair. Able to turn his head from
side to side with no noted discomfort.
Function: ADLs, IADLs, Programs, and Roles
Resident is reporting that he is not interested in his
usual activity at this time.
Smell: (Integumentary, GI, GU)
Unable to smell
Touch & Feel: (Neuro, Sensory, CV, Integumentary,
GI, MSK)
Unable to test limb strength.
Unable to feel warmth of skin at this time.
Consider Further: (Neurological, Respiratory,
Cardiac, Skin, Sensory, Musculoskeletal,
Gastrointestinal, Genitourinary, Mood/Behaviour,
Safety, ADLs)
Also, Mr. Smith...
Declines to participate in the programs he
usually attends.
Is reporting that he is not interested in his usual
activities at this time.
The systematic approach gathers all observable data under a system and the sensory observation reporting
allows for multiple systems observation grouped under how the resident was observed.

Pag
e6
5
APPENDIX C: WHAT DOES “OK” MEAN?
It is helpful for healthcare teams to establish normal baseline functioning of residents as a reference point for
reporting that they are “OK.” This allows caregivers to prioritize changes in residents as they occur. Below, one
such list of normal baseline functioning by system is suggested for a general resident population. It is
important that the team agrees on the meaning of “OK” and normal baseline functioning.
Neurological, Mood, Senses, Musculoskeletal & Function
Awake, alert, converses appropriately
Speaks in complete and organized thoughts
No behavioural or psychological symptoms of dementia observed
Positive affect, no sad mood reported
Using glasses, hearing aid, and mobility aids appropriately and safely
Moves without difficulty or discomfort
Equal limb strength from left to right
Steady gait
No dizziness when moving
Non-verbal signs of pain not observed, no pain reported
No change in ADL level
Engaging in activities as per usual
Respiratory
Breathing on room air
Equal rise and fall of chest
No cough or wheezing heard
No increased work of breathing observed
Cardiovascular & Integumentary
No change in skin color
No new swelling to arms, legs, abdomen
Denies chest pain, pressure or discomfort
No wounds, skin tears, pressure ulcers, bruises
No excessive sweating
Gastrointestinal & Genitourinary
No change in appetite
Mouth clear, no observed sores
Eating by mouth and taking in 100% of offered food and drinks
Abdomen not swollen; soft when touched
Passing flatus; last bowel movement less than 3 days ago
No changes to continence level
Toileting routine effective

Pag
e6
6
REFERENCES
1. Ahmed, A. (2009). DEFEAT – Heart Failure: A Guide to Management of Geriatric Heart Failure by
Generalist Physicians. Minerva Medica, 100(1), 39–50. Retrieved from:
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2914573/
2. Alzheimer’s Ontario. (2011). The U-First! Wheel. Retrieved from http://u-first.ca/about-u-first/the-u-
first-wheel/
3. American Medical Directors Association. (2003). Acute change of condition. Columbia, MD: AMDA.
Retrieved from http://www.guidelines.gov/popups/pop-algorithm.aspx?id=4950&file=3518/NGC-
3518.html&title=Acute+Change+of+Condition
4. American Medical Directors Association. (2009a). Heart failure in the long term care setting clinical
practice guideline. Columbia, MD: AMDA.
5. American Medical Directors Association. (2009b). Dehydration and fluid maintenance in the long term
care setting clinical practice guideline. Columbia, MD: AMDA.
6. American Medical Directors Association. (2010a). COPD management in the long term care setting
clinical practice guideline. Columbia, MD: AMDA.
7. American Medical Directors Association. (2010b). Diabetes management in the long term care setting
clinical practice guideline. Columbia, MD: AMDA.
8. American Medical Directors Association. (2011a). Common infections in the long term care setting
clinical practice guideline. Columbia, MD: AMDA.
9. American Medical Directors Association. (2011b). Stroke management in the long term care setting
clinical practice guideline. Columbia, MD: AMDA.
10. American Medical Directors Association. (2012). Urinary incontinence in the long term care setting
clinical practice guideline. Columbia, MD: AMDA.
11. Amodeo, J. (2013, January). Ontario’s health human resources: Leveraging the value of personal
support workers. Teleconference at the Alzheimer’s Knowledge Exchange. Toronto, Ontario.
12. Andrade, M., & Knight, J. (2008). Exploring the anatomy and physiology of ageing; part 4: The renal
system. Nursing Times, 104(34), 22-23.
13. Baycrest Centre for Education & Knowledge Exchange in Aging. (2012). Baycrest toolkit for
interprofessional education and care. Toronto, ON: Baycrest.
14. Blazer, D.G., & van Nieuwenhuizen, A. (2012). Evidence for the diagnostic criteria of delirium. Current
opinion in Psychiatry, 25(3), 239-243. Retrieved from
http://www.medscape.com/viewarticle/761823_3
15. Borlaug, B. A., & Colucci, W. S. (2015). Treatment and prognosis of heart failure with preserved ejection
fraction. In T.W. Post (Ed.), UptoDate. Waltham, MA: UptoDate. (Accessed on January 14, 2016).
Retrieved from http://www.uptodate.com/contents/treatment-and-prognosis-of-heart-failure-with-
preserved-ejection-fraction?source=see_link
16. Breall, J. A., Aroesty, J. M., & Simons, M. (2015). Overview of the acute management of unstable angina
and non-ST elevation myocardial infarction. In T.W. Post (Ed.), UptoDate. Waltham, MA: UptoDate.
(Accessed on January 12, 2016). Retrieved from http://www.uptodate.com/contents/overview-of-the-
acute-management-of-unstable-angina-and-non-st-elevation-myocardial-infarction#H23

Pag
e6
7
17. Bryan, E. D. (2015, December 27). Abdominal pain in elderly persons. Medscape. (Accessed on
February 12, 2016). Retrieved from http://emedicine.medscape.com/article/776663-workup
18. Buhr, G.T., Genao, L., & White, H.K. (2011). Urinary tract infections in long-term care residents. Clinics
in Geriatric Medicine, 27(2), 229-239.
19. Canadian Coalition for Seniors’ Mental Health. (n.d.). Tool on depression: Assessment and treatment for
older adults. Toronto, ON: Canadian Coalition for Seniors’ Mental Health. (Accessed on January 14,
2016). Retrieved from http://www.ccsmh.ca/pdf/CCSMH_depressionBrochure.pdf
20. Canadian Coalition for Seniors’ Mental Health. (2006). National guidelines for senior’s mental health:
The assessment and treatment of delirium. Toronto, ON: Canadian Coalition for Seniors’ Mental Health.
Retrieved from http://www.ccsmh.ca/en/natlGuidelines/delirium.cfm
21. Canadian Thoracic Society. (n.d.). Facts about COPD. Retrieved from
http://www.respiratoryguidelines.ca/sites/all/files/COPD_fact_sheet.pdf
22. Canadian Thoracic Society. (2008). Recommendations for the management of chronic obstructive
pulmonary disease 2008 update. Retrieved from
http://www.respiratoryguidelines.ca/sites/all/files/2008_CTS_Slide_Kit_COPD.pdf
23. Carro, A., & Kaski, J. C. (2011). Myocardial Infarction in the Elderly. Aging and Disease, 2(2), 116–137.
Retrieved from: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3295051/
24. Cefalu, C.A. (2011). Theories and mechanisms of aging. Clinics in Geriatric Medicine, 27(4), 493-506.
25. Centre for the Advancement of Interprofessional Education. (2002). Defining IPE. Retrieved from
http://www.caipe.org.uk/resources/
26. Clayton, D., Woo, V., & Yale, J. F. (2013). Hypoglycemia. In Canadian Diabetes Association Clinical
Practice Guidelines Expert Committee (Chapter 14). (Accessed on January 11, 2016). Retrieved from
http://guidelines.diabetes.ca/browse/chapter14
27. Clement, M., & Leung, F. (2009). Diabetes and the Frail Elderly in Long-Term Care. Canadian Journal of
Diabetes, 33(2), 114-121.
28. Cohen-Mansfield, J., Marx, M. S., & Rosenthal, A. S. (1989). A description of agitation in a nursing
home. Journal of Gerontology: Medical Sciences, 44(3), M77-M84.In S. Davidson. (Ed.). (2011). Living
with Alzheimer's disease and related dementias: A manual of resources, references and information
(2nd ed.). Ottawa, Ontario: CAOT Publications ACE.
29. Cole, M., McCusker, J., Voyer, P., Monette, J., Champoux, N., Ciampi, A., Vu, M., Dyachenko, A.,&
Belzile, E. (2012). Symptoms of delirium occurring before and after episodes of delirium in older long -
term care residents. Journal of the American Geriatrics Society, 60(12), 2302-2307.
30. College of Nurses of Ontario. (2013). Statistics. Retrieved from
http://www.cno.org/Global/ms/annualreport/statistics.html
31. Colucci, W.S. (2015a). Treatment of acute decompensated heart failure: General considerations. In
T.W. Post (Ed.), UptoDate. Waltham, MA: UptoDate. (Accessed on January 12, 2016). Retrieved from
http://www.uptodate.com/contents/treatment-of-acute-decompensated-heart-failure-general-
considerations?source=see_link
32. Colucci, W.S. (2015b). Evaluation of the patient with suspected heart failure. In T.W. Post (Ed.),
UptoDate. Waltham, MA: UptoDate. (Accessed on January 12, 2016). Retrieved from
http://www.uptodate.com/contents/evaluation-of-the-patient-with-suspected-heart-failure

Pag
e6
8
33. Colucci, W. S. (2015c). Overview of the therapy of heart failure with reduced ejection fraction. In T.W.
Post (Ed.), UptoDate. Waltham, MA: UptoDate. (Accessed on January 14, 2016). Retrieved from
http://www.uptodate.com/contents/overview-of-the-therapy-of-heart-failure-with-reduced-ejection-
fraction?source=see_link
34. Dante Yeh, D., & Bordeianou, L. (2015). Overview of mechanical colorectal obstruction. In T.W. Post
(Ed.), UptoDate. Waltham, MA: UptoDate. (Accessed on January 13, 2016). Retrieved from
http://www.uptodate.com/contents/overview-of-mechanical-colorectal-
obstruction?source=search_result&search=constipation+and+impaction+geriatric&selectedTitle=8%7E
150#H76779339
35. Day, J., Higgins, I., & Keatinage. (2011). Orientations strategies during delirium: Are they helpful?
Journal of Clinical Nursing, 20, 3285-3294.
36. Dellinger, R.P., Levy, M. M., Rhodes, A., Annane, D., Gerlach, H., Opal, S. M., … Moreno, R. (2012).
Surviving sepsis campaign: International guidelines for management of severe sepsis and septic shock.
(Accessed on January 14, 2016). Retrieved from
http://www.idsociety.org/uploadedFiles/IDSA/Guidelines-
Patient_Care/IDSA_Practice_Guidelines/Fever_and_Infections/2013%20Sepsis%20Guidelines.pdf
37. Douglas, P. S. (2014). Clinical features and diagnosis of coronary heart disease in women. In T.W. Post
(Ed.), UptoDate. Waltham, MA: UptoDate. (Accessed on January 12, 2016). Retrieved from
http://www.uptodate.com/contents/clinical-features-and-diagnosis-of-coronary-heart-disease-in-
women?source=see_link
38. Elliot, G. (2012). Montessori Methods for DementiaTM: Focusing on the person and the prepared
environment. Hamilton, ON: McMaster University.
39. Espinoza, R.T., & Unützer, J. (2016). Diagnosis and management of late-life unipolar depression. In T.W.
Post (Ed.), UptoDate. Waltham, MA: UptoDate. (Accessed on January 11, 2016). Retrieved from
http://www.uptodate.com/contents/diagnosis-and-management-of-late-life-unipolar-
depression?source=search_result&search=geriatric+depression&selectedTitle=1%7E150
40. Fink, D. L. (2013). Creating significant learning experiences: An integrated approach to designing
college courses. San Francisco, CA: Jossey-Bass.
41. Florida Atlantic University. (2011). Interventions to reduce acute care transfers. Retrieved from
http://interact2.net/tools.html
42. Glenny, C., Heckman, G., & McKElvie, R. (2012). Heart failure in older persons: Considerations for the
primary care physician. Canadian Geriatrics Society Journal of Continuing Medical Education, 2(1), 9-
17.
1. Gauer, R.L. (2013). Early recognition and management of sepsis in adults. American Family Physician,
1(88), 44-53. (Accessed on January 14, 2016). Retrieved from
http://www.aafp.org/afp/2013/0701/p44.html
2. Goguen, J., & Gilbert, J. (2013). Hyperglycemic emergencies in adults. In Canadian Diabetes Association
Clinical Practice Guidelines Expert Committee (Chapter 15). Retrieved from:
http://guidelines.diabetes.ca/Browse/Chapter37
3. Han, M. K., Dransfield, M. T., & Martinez, F. J. (2015). Chronic obstructive pulmonary disease:
Definition, clinical manifestations, diagnosis, and staging. In T.W. Post (Ed.), UptoDate. Waltham, MA:
UptoDate. (Accessed on January 12, 2016). Retrieved from

Pag
e6
9
http://www.uptodate.com/contents/chronic-obstructive-pulmonary-disease-definition-clinical-
manifestations-diagnosis-and-
staging?source=search_result&search=COPD+in+elderly&selectedTitle=1%7E150
4. Hanania, N. A., Sharma, G., & Sharafkhaneh, A. (2010). COPD in the elderly patient. Seminars in
Respiratory and Critical Care Medicine, 31(5), 596-606.
5. Hennekens, C. H. (2015). Secondary prevention of cardiovascular disease. In T.W. Post (Ed.), UptoDate.
Waltham, MA: UptoDate. (Accessed on January 12, 2016). Retrieved from
http://www.uptodate.com/contents/secondary-prevention-of-cardiovascular-
disease?source=see_link#H49
6. Hickey, L. (2012). Patterns in the sky. Requested with permission by Monika Keri, RN.
http://www.lisadhickey.ca/site/portfolio/Pages/look_up_.html#20
7. Horwitz L., & Krumholz, H. (2015). Heart failure self management. In T.W. Post (Ed.), UptoDate.
Waltham, MA: UptoDate. (Accessed on January 12, 2016). Retrieved from
http://www.uptodate.com/contents/heart-failure-self-management?source=see_link
8. Joseph, S. M., Cedars, A. M., Ewald, G. A., Geltman, E. M., & Mann, D. L. (2009). Acute Decompensated
Heart Failure: Contemporary Medical Management. Texas Heart Institute Journal, 36(6), 510–520.
Retrieved from: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2801958/
9. Kitabchi, A.E., Hirsch, I.B., & Emmett, M. (2014). Diabetic ketoacidosis and hyperosmolar hyperglycemic
state in adults: Clinical features, evaluation and diagnosis. In T.W. Post (Ed.), UptoDate. Waltham, MA:
UptoDate. Retrieved from http://www.uptodate.com/contents/diabetic-ketoacidosis-and-
hyperosmolar-hyperglycemic-state-in-adults-clinical-features-evaluation-and-
diagnosis?source=search_result&search=diabetic+ketoacidosis&selectedTitle=2%7E150
10. Knight, J., & Nigam, Y. (2008a). Exploring the anatomy and physiology of ageing; part 1: The
cardiovascular system. Nursing Times, 104(31), 26-27.
11. Knight, J., & Nigam, Y. (2008b). Exploring the anatomy and physiology of ageing; part 2: The respira tory
system. Nursing Times, 104(32), 24-25.
12. Knight, J., & Nigam, Y. (2008c). Exploring the anatomy and physiology of ageing; part 5: The nervous
system. Nursing Times, 104(35), 18-19
13. Knight, J., & Nigam, Y. (2008d). Exploring the anatomy and physiology of ageing; part 7: The endocrine
system. Nursing Times, 104(45), 24-25.
14. Knight, J., & Nigam, Y. (2008e). Exploring the anatomy and physiology of ageing; part 8: The
reproductive system. Nursing Times, 104(46), 24-25.
15. Knight, J., & Nigam, Y. (2008f). Exploring the anatomy and physiology of ageing; part 10: Muscle and
Bone. Nursing Times, 104(48), 21-22.
16. Larzelere, M.M., Campbell, J., & Adu-Sarkodie, N.Y. (2011). Psychosocial factors in aging. Clinics in
Geriatric Medicine, 27(4), 645-660.
17. Mandel, J., & Palevsky, P.M. (2005). Treatment of severe hypovolemia or hypovolemic shock in adults.
In T.W. Post (Ed.), UptoDate. Waltham, MA: UptoDate. (Accessed on January 15, 2016). Retrieved from
http://www.uptodate.com/contents/treatment-of-severe-hypovolemia-or-hypovolemic-shock-in-
adults?source=see_link#H1
18. McGreer, M.A., & Carter, P.J. (2011). Lippincott’s textbook for personal support workers: A humanistic
approach to caregiving. Philadelphia, PA: Lippincott Williams & Wilkins.

Pag
e7
0
19. Merck Manual for Health Care Professionals. (2012). Unusual presentation of illness in the elderly.
Retrieved from
http://www.merckmanuals.com/professional/print/geriatrics/approach_to_the_geriatric_patient/unu
sual_presentations_of_illness_in_the_elderly.html
20. Meneilly, G.S., Knip, A., & Tessier, D. (2013). Diabetes in the elderly. In Canadian Diabetes Association
Clinical Practice Guidelines Expert Committee (Chapter 37). (Accessed on January 12, 2016). Retrieved
from http://guidelines.diabetes.ca/Browse/Chapter37
21. Ministry of Training, Colleges and Universities. (2014). Personal support worker program standard.
Ontario, Canada: Queen’s Printer for Ontario. Retrieved from
http://www.tcu.gov.on.ca/pepg/audiences/colleges/progstan/health/41469.pdf
22. Moorhouse, P., & Rockwood, K. (2012). Frailty and its quantitative clinical evaluation. The Journal of
Royal College of Physicians of Edinburgh, 42(4) 333-340. Retrieved from
http://www.rcpe.ac.uk/journal/issue/journal_42_4/moorhouse.pdf
23. Namirah, J., Woods, C., Desai, S., Dhanani, S., & Taler, G. (2011). Pneumonia in the long-term resident.
Clinics in Geriatric Medicine, 27(2), 117-133.
24. Nasa, P., Juneja, D., & Singh, O. (2012). Severe sepsis and septic shock in the elderly: An
overview. World Journal of Critical Care Medicine, 1(1), 23–30. http://doi.org/10.5492/wjccm.v1.i1.23
25. National Association of Career Colleges. (2010). Personal support worker. Retrieved from
http://www.nacc.ca/w_personal_support_worker.aspx
26. National Institute for Health and Care Excellence. (2015). Urinary tract infections in adults. Retrieved
from http://www.nice.org.uk/guidance/qs90/chapter/Quality-statement-1-Diagnosing-urinary-tract-
infections-in-adults-aged-65-years-and-over
27. Neviere, R. (2015). Sepsis and the systemic inflammatory response syndrome: Definitions,
epidemiology, and prognosis. In T.W. Post (Ed.), UptoDate. Waltham, MA: UptoDate. (Accessed on
January 14, 2016). Retrieved from http://www.uptodate.com/contents/sepsis-and-the-systemic-
inflammatory-response-syndrome-definitions-epidemiology-and-prognosis?source=see_link
28. Nigam, Y., & Knight, J. (2008a). Exploring the anatomy and physiology of ageing; part 3: The digestive
system. Nursing Times, 104(33), 22-23.
29. Nigam, Y., & Knight, J. (2008b). Exploring the anatomy and physiology of ageing; part 6: The eye and
ear. Nursing Times, 104(36), 22-23.
30. Nigam, Y., & Knight, J. (2008c). Exploring the anatomy and physiology of ageing; part 9: The immune
system. Nursing Times, 104(47), 22-23.
31. Nigam, Y., & Knight, J. (2008d). Exploring the anatomy and physiology of ageing; part 11: The skin.
Nursing Times, 104(48), 24-25.
32. Ontario Community Support Association. (2009). Ministry of health and long term care personal
support worker training standards (1997). Retrieved from
http://www.psno.ca/uploads/1/0/1/9/10197937/psw_training_standards.pdf
33. Philips, L. A. (2013). Delirium in geriatric patients: Identification and prevention. Medsurg Nursing,
22(1), 9-12.
34. Physical changes with aging. (2009). In R.S. Porter, J.L. Kaplan, K.A.G. Lane, S.T. Schindler, S.C.Short, &
S. Steigerwald (Eds.). The Merck manual for healthcare professionals. Retrieved from

Pag
e7
1
http://www.merckmanuals.com/professional/geriatrics/approach_to_the_geriatric_patient/physical_c
hanges_with_aging.html
35. P.I.E.C.E.S. Canada. (2010). User guideline for the job aid putting it all together: RAI-MDS© and
P.I.E.C.E.S.TM integration. Retrieved from http://piecescanada.com/RAI-
MDS_PIECES_JobAidGuide_20100206_v1.0_LTCHCAP.pdf
36. Pinto, D. S., & Kociol, R. D. (2015). Evaluation of acute decompensated heart failure. In T.W. Post (Ed.),
UptoDate. Waltham, MA: UptoDate. (Accessed on January 12, 2016). Retrieved from
http://www.uptodate.com/contents/evaluation-of-acute-decompensated-heart-
failure?source=see_link
37. Preyra, C. (2013, February 14). Designing for the future: What kind of long term care does Ontario
need? Presentation at the 2013 OLTCA Applied Research Day. Retrieved from
http://www.oltca.com/library/events/ARD2013/Research%20Day%202013%20Presentations%20(3).zi
p
38. Psychogeriatric Resource Consultant. Presented by Thomas, J. (2011, August). The thinking problems of
dementia: 7As. Staff session at Baycrest. Toronto, ON.
39. Rao, S.S.C. (2015). Constipation in the older adult. In T.W. Post (Ed.), UptoDate. Waltham, MA:
UptoDate. (Accessed on January 13, 2016). Retrieved from
http://www.uptodate.com/contents/constipation-in-the-older-
adult?source=search_result&search=gi+fecal+impaction&selectedTitle=2%7E150#H523121797
40. Reeder, G. S., & Kennedy, H. L. (2014). Criteria for the diagnosis of acute myocardial infarction. In T.W.
Post (Ed.), UptoDate. Waltham, MA: UptoDate. (Accessed on January 12, 2016). Retrieved from
http://www.uptodate.com/contents/criteria-for-the-diagnosis-of-acute-myocardial-
infarction?source=see_link#H8
41. Registered Nurses’ Association of Ontario. (n.d. a). Guidelines for nurses on how to manage
hypoglycemia. Toronto, Canada: Registered Nurses’ Association of Ontario. (Accessed on January 12,
2016). Retrieved from http://pda.rnao.ca/content/guidelines-nurses-how-manage-hypoglycemia
42. Registered Nurses’ Association of Ontario. (n.d.b). Clinical signs and symptoms of dehydration.
Toronto, Canada: Registered Nurses’ Association of Ontario. (Accessed on January 13, 2016). Retrieved
from http://pda.rnao.ca/content/clinical-signs-and-symptoms-dehydration
43. Registered Nurses’ Association of Ontario. (n.d.c). Assessment and management of pain in the elderly.
Toronto, Canada: Registered Nurses’ Association of Ontario. (Accessed on January 14, 2016). Retrieved
from http://rnao.ca/sites/rnao-ca/files/Assessment_and_Management_of_Pain_in_the_Elderly_-
_Learning_Package_for_LTC.pdf
44. Registered Nurses’ Association of Ontario. (2005a). Stroke assessment across the continuum of care.
Toronto, Canada: Registered Nurses’ Association of Ontario. Retrieved from http://rnao.ca/sites/rnao-
ca/files/Stroke_Assessment_Across_the_Continuum_of_Care.pdf
45. Registered Nurses’ Association of Ontario. (2005b). Health Education facto Sheet: Chronic obstructive
pulmonary disease (COPD)- Helping you Breathe Easier. Retrieved from http://rnao.ca/sites/rnao-
ca/files/Chronic_Obstructive_Pulmonary_Disease_COPD_-_Helping_You_Breathe_Better.pdf
46. Registered Nurses’ Association of Ontario. (2007). Assessment & management of pain. Toronto,
Canada: Registered Nurses’ Association of Ontario. Retrieved from http://rnao.ca/sites/rnao-
ca/files/Assessment_and_Management_of_Pain.pdf

Pag
e7
2
47. Registered Nurses’ Association of Ontario. (2008). Oral Health: Nursing assessment and interventions.
Toronto, Canada: Registered Nurses’ Association of Ontario. Retrieved from http://rnao.ca/sites/rnao-
ca/files/Oral_Health_-_Nursing_Assessment_and_Interventions.pdf
48. Registered Nurses’ Association of Ontario. (2009a). Nursing care of dyspnea: The 6th vital sign in
individuals with chronic obstructive pulmonary disease. Toronto, Canada: Registered Nurses’
Association of Ontario. Retrieved from http://rnao.ca/sites/rnao-ca/files/Nursing_Care_of_Dyspnea_-
The_6th_Vital_Sign_in_Individuals_with_Chronic_Obstructive_Pulmonary_Disease.pdf
49. Registered Nurses’ Association of Ontario. (2009b). Nursing management of hypertension. Toronto,
Canada: Registered Nurses’ Association of Ontario. Retrieved from http://rnao.ca/sites/rnao-
ca/files/Nursing_Management_of_Hypertension.pdf
50. Registered Nurses’ Association of Ontario. (2010). Caregiving strategies for older adults with delirium,
dementia and depression. Toronto, Canada: Registered Nurses’ Association of Ontario. Retrieved from
http://rnao.ca/sites/rnao-
ca/files/Caregiving_Strategies_for_Older_Adults_with_Delirium_Dementia_and_Depression.pdf
51. Registered Nurses’ Association of Ontario. (2011a). Prevention of falls and fall injuries in the older
adult. Toronto, Canada: Registered Nurses’ Association of Ontario. Retrieved from
http://rnao.ca/sites/rnao-ca/files/Prevention_of_Falls_and_Fall_Injuries_in_the_Older_Adult.pdf
52. Registered Nurses’ Association of Ontario. (2011b). Prevention of constipation in the older adult
population. Toronto, Canada: Registered Nurses’ Association of Ontario. Retrieved from
http://rnao.ca/sites/rnao-ca/files/Prevention_of_Constipation_in_the_Older_Adult_Population.pdf
53. Registered Nurses’ Association of Ontario. (2011c). Risk Assessment & Prevention of Pressure Ulcers.
Toronto, Canada: Registered Nurses’ Association of Ontario. Retrieved from http://rnao.ca/sites/rnao-
ca/files/Assessment__Management_of_Stage_I_to_IV_Pressure_Ulcers.pdf
54. Registered Nurses’ Association of Ontario. (2011d). Best practice guideline: Prevention of constipation
in the older adult population. Toronto, Canada: Registered Nurses’ Association of Ontario. (Accessed on
January 13, 2016). Retrieved from http://rnao.ca/sites/rnao-
ca/files/Constipation_supplement_2011.pdf
55. Rehman, H., & Qazi, S. (2013). Atypical manifestations of medical conditions in the elderly. Canadian
Geriatrics Society Journal of Continuing Medical Education, 3(1), 17-24.
56. Rhodes-Kropf, J., Cheng, H., Castillo, E.C., & Fulton, A.T. (2011). Managing the patient with dementia in
long-term care. Clinics in Geriatric Medicine, 27(2), 135-152.
57. Rosenquist, E.W.K., & Aronson, M.D. (2015). Overview of the treatment of chronic pain. In T.W. Post
(Ed.), UptoDate. Waltham, MA: UptoDate. (Accessed on January 8, 2016). Retrieved from
http://www.uptodate.com/contents/overview-of-the-treatment-of-chronic-
pain?source=search_result&search=Overview+of+the+treatment+of+chronic+pain&selectedTitle=1%7
E150
58. Robichaud, S., & Blondeau, J. (2008). Urinary tract infections in older adults: Current issues and new
therapeutic options. Geriatrics and Aging, 11(10), 582-588.
59. Rockwood, K., Song, X., MacKnight, C., Bergman, H., Hogan, D.B., McDowell, I., & Mitnitski, A. (2005). A
global clinical measure of fitness and frailty in elderly people. Canadian Medical Association Journal.
173(5), 489-495.

Pag
e7
3
60. Schmidt, G.A., & Mandel, J. (2016). Evaluation and management of severe sepsis and septic shock in
adults. In T.W. Post (Ed.), UptoDate. Waltham, MA: UptoDate. (Accessed on January 14, 2016).
Retrieved from http://www.uptodate.com/contents/evaluation-and-management-of-severe-sepsis-
and-septic-shock-in-adults?source=search_result&search=septicemia&selectedTitle=2%7E150#H31
61. Shah, N., Afridi, M.H., Jamal, S., & Marwat, M.A. (2012). Prevalence, risk factors and outcomes of
hypoglycemia in elderly diabetic patients. Journal of Postgraduate Medical Institute, 26(3), 272-276.
62. Sharkey, S. (2008). People caring for people: Impacting the quality of life and care of residents of long-
term care homes. Ontario, Canada: Ontario Ministry of Health and Long-Term Care. Retrieved from
http://tools.hhr-
rhs.ca/index.php?option=com_mtree&task=att_download&link_id=5987&cf_id=68&lang=en
63. Sources of potentially avoidable emergency department visits. (2014). Ottawa, ON: Canadian Institute
for Health Information. Retrieved from
https://secure.cihi.ca/free_products/ED_Report_ForWeb_EN_Final.pdf
64. Sterns, R. H. (2014). Etiology, clinical manifestations, and diagnosis of volume depletion in adults. In
T.W. Post (Ed.), UptoDate. Waltham, MA: UptoDate. (Accessed on January 14, 2016). Retrieved from
http://www.uptodate.com/contents/etiology-clinical-manifestations-and-diagnosis-of-volume-
depletion-in-adults?source=search_result&search=dehydration+in+elderly&selectedTitle=1%7E150
65. Stoller, J. K. (2015). Management of exacerbations of chronic obstructive pulmonary disease. In T.W.
Post (Ed.), UptoDate. Waltham, MA: UptoDate. (Accessed on January 12, 2016). Retrieved from
http://www.uptodate.com/contents/management-of-exacerbations-of-chronic-obstructive-
pulmonary-disease?source=see_link
66. Stone, N. D., Ashraf, M. S., Calder, J., Crnich, C. J., Crossley, K., Drinka, P. J., … for the Society for
Healthcare Epidemiology Long-Term Care Special Interest Group. (2012). Surveillance Definitions of
Infections in Long-Term Care Facilities: Revisiting the McGeer Criteria. Infection Control and Hospital
Epidemiology, 33(10), 965–977. http://doi.org/10.1086/667743
67. University of Toronto. (2010). Framework for Interprofessional Competencies. Toronto, Canada: Centre
for Interprofessional Education.
68. UptoDate. (2016). UpToDate’s rapid overview: Management of acute coronary syndrome (ACS). In T.W.
Post (Ed.), UptoDate. Waltham, MA: UptoDate. Retrieved from
http://www.uptodate.com/contents/image?imageKey=CARD%2F75032&topicKey=CARD%2F68&sourc
e=see_link&utdPopup=true
69. Vancouver Island Health Authority. (2012). Age-related changes. In Delirium Resources. Retrieved from
http://www.viha.ca/NR/rdonlyres/E925275F-3EF0-420F-8244-
9D5884BA914E/0/age_related_changes_09.pdf
70. Way, D., Jones, L., & Busing, N. (2000). Implementation strategies: "Collaboration in primary care –
family doctors and nurse practitioners delivering shared care". Discussion paper for the Ontario College
of Family Physicians.
71. Wenger, N. K. (2015). Cardiac rehabilitation in older adults. In T.W. Post (Ed.), UptoDate. Waltham, MA:
UptoDate. (Accessed on January 12, 2016). Retrieved from
http://www.uptodate.com/contents/cardiac-rehabilitation-in-older-
adults?source=search_result&search=myocardial+infarction+elderly&selectedTitle=5%7E150

Pag
e7
4
72. White-Chu, E.F., Flock, P., Struck, B., & Aronson, L. (2011). Pressure ulcers in long-term care. Clinics in
Geriatric Medicine, 27(2), 241-258.
73. Whytock, S. (2013). Geriatric vicious circles. [Web log post]. Retrieved from:
http://blogs.ubc.ca/geronursing/resources/geriatric-syndromes/
74. Woo, V., & Yale, J. (2013). Clinical Practice Guidelines: Hypoglycemia. Canadian Journal of Diabetes, 37,
69-71.