Team 3 presentation2
56
Team Members Tina Fulbright – Slides #2 – 12 Christy Smith – Slides #13 – 23 Jali Jackson – Slides # 24 – 35 Todd MacDonald – Slides #36 - 51
-
Upload
toddmacdonald -
Category
Education
-
view
866 -
download
2
description
Transcript of Team 3 presentation2

Team MembersTina Fulbright – Slides #2 – 12
Christy Smith – Slides #13 – 23
Jali Jackson – Slides # 24 – 35
Todd MacDonald – Slides #36 - 51

As you will see in the following compilation of research, Clinical Information Systems are multifaceted with the ultimate goal of providing clinical decision information to the clinician. This information allows the clinician to make decisions about patient care and can enhance patient outcome.

CIS Overview CIS refers to a Clinical Information System.
The system requires multiple technology applications which are used at the point of care. The CIS is capable of acquiring, processing, retaining, and retrieving information related to patient care.
(McGonigle & Mastrian, 2009)

Choosing, Implementing, Revising the CIS The choice of systems is one made between
multiple departments. A collaborative effort is required in order to ensure that the needs of all departments are met by the system chosen for the facility. Various committees are formed to gather information in an effort to focus the goals of the system, to oversee clinical quality as well as evaluate design of the system and hardware. (Al Mallah, Guelpa, Marsh & van Rooij, 2010)

Choosing, Implementing, Revising the CIS (Cont) Some of the team players would include
administration and executive staff as well as representatives from clinical specialty areas, support services, and the information technology department. Software vendors are also called upon for their input and recommendations.
(Al Mallah, Guelpa, Marsh, & van Rooij, 2010)

Some of the team players would include administration and executive staff as well as representatives from clinical specialty areas, support services, and the information technology department. Software vendors are also called upon for their input and recommendations. After implementation of the CIS, revisions are made based upon the needs and input of the users.
(Al Mallah, Guelpa, Marsh, & van Rooij, 2010)

Clinical Decision Support Clinical decision support (CDS) is a program
which is computer-based. It is intended to help clinicians make clinical decision. Large amounts of information are integrated or filtered during this process and give clinicians suggestions in regard to clinical intervention. (The Design, 2001)

CDS Infrastructure• A quality infrastructure would include a depository of
medical knowledge that would require “standardization of CDS and genomic medicine information”. This information would need to be computer-processable;
• In order for it to be computer interpretable, there must be a standard format of patient data. An example would be Health Level (HL) 7 and extensible markup language (XML);
• The approach used to acquire medical knowledge and find and recapture patient data in order to form patient-specific guidance by bringing together both the personal data of the patient and medical knowledge.
(Al Mallah, Guelpa, Marsh & van Rooij, 2010)

The American National Standard Institute HIT Standards Panel (HITSP) champions “the standardization of health information technology through the American Health Information Community.”
(Al Mallah, Guelpa, Marsh & van Rooij, 2010)

Structure and Updates The design of the CDS should be easy to use
for the clinician. It should contain quality up-to-date medical information that will help the clinician make the best decision for each individual patient. The system should be updated as new information becomes available.

Clinical Decision Support Systems There are multiple systems available on the
market. Listed below are just a few of the CDS systems available and their design companies.
TheraDoc, Inc/HospiraVisualDx/Logical ImagesQMR/First Data Bank
(Clinical Decision, 2003)

Conclusion
Obviously, when considering a CIS, one must look at multiple factors. There must be a team assembled to determine what is needed by that particular facility. The HER, CDS, safety of the system, cost and the education for staff must all be considered in great detail before one can begin to work towards implementing a successful system into their facility.


The EHR Component The HIMSS(Healthcare Information
and Management Systems Society, 2006) defines an EHR as a “longitudinal electronic record of patient information produced by encounters in one or more care setting” (McGonigle & Mastrian, 2009).
The IOM(Institute of Medicine) defines the EHR as “health information and data that is the patient data required to make sound clinical decisions including demographics, medical and nursing diagnoses, medication lists, allergies and test results” (McGonigle & Mastrian, 2009).

Eight Components to the EHR

Health Information and Data The patient data required to make sound
clinical decisions including demographics, medical and nursing diagnoses, medication lists, allergies and test results(IOM,2003) (McGonigle & Mastrian, 2009).
All personnel that have a sign on, password and credentials(for most facilities) have access to this information. Doctors, nurses, PA’s, NP’s, etc… There is a demographic view available for admission staff.

Results Management The ability to manage results of all types
electronically including laboratory and radiology procedure reports both current and historical(IOM, 2003)((McGonigle & Mastrian, 2009).
Laboratory and radiology personnel have the ability to view and enter results here. Authorized staff have the ability to view results here. Any personnel with the credentials to view patient records has access to this information. Without this component, results are delayed and hard to compare with archived records.

Order Entry Management The ability of a clinician to enter medication and
other care orders, including laboratory, microbiology, pathology, radiology, nursing, supply orders, ancillary services, and consultations directly into a computer(IOM,2003) (McGonigle &Mastrian, 2009).
Personnel are given rights according to their credentials. Orders and medications are signed by physicians electronically when needed. Without this component, there are several extra steps that must be taken to complete the task of placing an order for a patient.

Decision Support The computer reminders and alerts to improve the
diagnosis and care of a patient including screening for correct drug selection and dosing, medication interactions with other medications, preventative health reminders in areas such as vaccinations, health risk screenings and detection, and clinical guidelines for patient disease treatment(IOM,2003)(Mcgonigle & Mastrian, 2009)
This component helps us to monitor what the patient has and has not had completed according to their medical record. It also aids in the faster prescribing of medications for physicians and keeping patients safe from possible deadly interactions from their medications. This is a powerful tool for both the healthcare team and patient satisfaction.

Electronic Communication and Connectivity The online communication among healthcare
team members, their care partners, and patients including E-mail, Web messaging, and an integrated health record within and across settings, institutions, and telemedicine (IOM, 2003) (McGonigle & Mastrian, 2009).
This component is important for access to patients records when they are being seen by a physician other than their primary care and history can be easily accessed. Not all parts of this system are utilized by all healthcare facilities, but they are available and helpful tools for accurate patient care.

Patient Support The patient education and self-monitoring tools,
including interactive computer-based patient education, home telemonitoring and telehealth systems(IOM,2003) (Mcgonigle & Mastrian, 2009).
These are very helpful for patients to be taken care of on an out-patient basis. Blood pressure monitoring for home health that reports immediately if there are any problems is a good example of one system used through a patient’s phone line. The report of the patient’s vitals is sent to the agency and they can call if something is not right or if the patient doesn’t respond to the machine telling them it is time for their vital signs to be checked.

Administrative Processes
The electronic scheduling, billing, and claims management systems including electronic scheduling for inpatient and outpatient visits and procedures, electronic insurance eligibility validation, claim authorization and prior approval, identification of possible research study participants and drug recall support (IOM, 2003) (McGonigle & Mastrian, 2009).
This helps the organization not double book patients for appointments and to get authorization for procedures and admits almost immediately. Of coarse not everything is automatic but it helps speed the process for both the institution and the patient. If your sign on has the credentials needed for this process, you have access to work in these sections.

Reporting and Population Health Management The data collection tools to support public
and private reporting requirements including data represented in a standardized terminology and machine-readable format (IOM, 2003) (Mcgonigle & Mastrian, 2009).
This is part of every healthcare system and is required by law. The reporting is done to evaluate EHR systems for functionality, security, and interoperability. This is regulated by the Certification Commission for Healthcare Information Technology or CCHIT.

The EMR/EHR was created to limit mistakes, cut
down expenses, and improve care.
EMR/EHR’s provide direct access to patient records,
improve order legibility, have built in safety
features, and use of standardized nomenclature.
Like with anything new, there is a need for
protection and education.
The following slides will show how safety and
education will be implemented regarding the
EMR/HER.
(Buppert, 2010)

Backup Due to private and sensitive patient information, it is necessary to
back-up the EMR/EHR frequently (Buppert, 2010).
Not only does the system need to be backed up, but the method in
which the system is backed up needs to be assessed frequently to
ensure that a back up is taking place (Buppert, 2010).
It is necessary to ensure that the network storage or hard drive is
efficient in terms of space and function (Buppert, 2010)
Common back up programs include Legato and Net-backup
software (Rosenfeld, 2006).
A cheaper, yet slower, option is hierarchical storage
management software (Rosenfeld, 2006).

Storage
“The key driver leading to the need for healthcare institutions to pay attention to storage and archival resources is the dramatic growth in healthcare digital information” (Rosenfeld, 2006)
A cost efficient choice for storage management are enterprisewide storage architectures. This architecture “…expedite[s] management of
storage resources, enhance[s] the ability to share application data with other systems, and facilitate[s] automated data backup and redundancy/continuity” (Rosenfeld, 2006)

EMR/EHR AccessImplement password protected log-
ins.
Automatic log out if no activity after 2
minutes.
Have designated staff to handle
breaches in security.
Have staff change their password every 6
months to ensure only employees have
access to sensitive records.
(Buppert, 2010)

HIPAA Considerations The HIPAA rule book is 1,500 pages long. Although this
is a massive amount of information, “…it is a well-
thought-out, clear set of rules about the accepted use of
protected health information” (McDonald, 2009).
HIPAA requires all organizations using EMR/EHR to
maintain an audit trail.
Other rules implemented by HIPAA regarding the
EMR/EHR took effect April 14, 2003.
These rules are to help maintain each and every patients
privacy.
(Medscape, 2010)

Protection of Files It is important to protect the privacy of sensitive patient
information.
With EMR/EHR comes the increased opportunity for security
breaches and viruses.
Because of this, there needs to be increased security and
awareness when charts are pulled up on the computer.
Built in automatic shut off and password protected screen
savers are a must have.
Antivirus and malware programs also need to be installed
on all computers to ensure that privacy is maintained
(Fetter, 2009)

Protection of Files (cont…) Due to the frequent occurrence of power surges, there is a chance
for disruptions in computer systems and network damage.
This risk can cause a loss of patient information and aggravated
staff members.
Uninterruptible power supplies (UPS) can be installed to prevent
this from occurring.
A great option to use because it is generator friendly and removes
the problems associated with generator frequency synchronization
problems.
(Reisz, et al., 2010)

Education Anyone who will be operating or charting in the EMR/EHR
needs to be properly educated on the proper way of doing so.
IT workers who are familiar with the program and all that it
entails are great resources to the facility and it employees.
An important aspect of EMR/EHR education is developing a
plan that will enhance computer literacy and competency of
the staff.
It is “…critical to assess, develop, and maintain staff
competency to ensure quality of care in all nursing areas”
(Miller & Arquiza, 1999).

Education Strategies Select members from each unit to
be trained in a way that they would
be able to train others- “Super
users”
Structure classes based on
position/level (i.e. Nurses, doctors,
CNA would be in three different
classes)
Conduct annual competency
checks to evaluate if more training
is needed.
Have employees perform self
assessments and compare with
comments made by “super-users”
(Miller & Arquiza, 1999)

Education Strategies (cont…) Depending on whether weekly or monthly training
sessions are needed, there needs to be an adequate number of IT personnel available to “…answer questions and give impromptu training on [various units], and receive feedback on…problems in return” (Transitioning to, 2006).
Organizational planning and shared resources combined with a well thought out mission, vision, and yearly objectives can help advance knowledge and competency (Fetter, 2009).
Provide refreshments and support to facilitate participation.

Principles to Improve Effectiveness Assess training needs
Don’t rush training time
Have a low student-to-instructor ratio
Allow staff to practice their new knowledge in the
classroom before use on real charts.
(Fetter, 2009)

Principles (cont…) Have paper versions of screen shots available to aid
in learning how to navigate through the EMR/EHR.
Allow extra practice time
Have extra trainers available to answer individual
questions.
Technical support needs to be available for each
unit.
(Fetter, 2009)

Costs Associated With CIS

Taking into consideration all aspects of implementing a CIS is a daunting task. Genesis, the joint initiative task force from St. Johns, has been responsible for the research and implementation of EPIC at St. Johns.
The total installation cost, Mercy-wide, has been approximately $500,000,000.
The following presentation discusses where the costs were incurred.
Micki Struckhoff, RN – VP Systems Integration, St. Johns Springfield.

What Is A Computer Network? Simply stated, a computer network “is two or
more computers connected so that they can communicate with each other and share information, software, peripheral devices, and/or processing power.” The most common of which is called a LAN (local area network) and a WAN (wide area network).
highered.mcgraw-hill.com/sites/0072464011/student_view0/chapter6/glossary.html

Hardware and SoftwareHardware & software for a computer
network involves several components. Keep in mind, when a large network is installed, the hardware & software needs can increase significantly.
An upgrade to existing computer networks typically accompanies the addition of a CIS package.

ComponentsHardware
Robust computer workstation
Network CablesRouter with firewallServers & BackupsRepeater (if signal
attenuation an issue)Peripheral EquipmentFiber optic connection
to internet
SoftwareCompatible OS
(operating system & license)
CIS Software & license for each server (usually based on size of network involved)
Internet accessSoftware firewallAntivirus

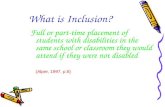
Classic Network Bandwidth &
Hardware Map
The picture on the left is a great depiction of what a typical wide area networks bandwidth looks like without hardware. The right is a very basic map of a LAN.

Support PersonnelRelevant to the discussion is the number of
support technicians available and their associated salaries. According to indeed.com, the average salary for a computer technician in Springfield, MO is $33,000 per year. Depending on the size of network, this cost could multiply very quickly. The network manager will average $66,000.

Support Personnel ContinuedAs is the case with EPIC, there are groups of IT
Technicians within the IT Department that strictly support the CIS, according to Micki Struckhoff, RN.
Anyone supporting the software must be certified through EpicCare, the company that supplies St. Johns’ CIS software.
Micki Struckhoff, RN. – VP Systems Integration for St. Johns Springfield.

Multiple redundancies are required for this type of market. Several ISPs are involved in making this system as failsafe as possible to achieve maximum stability.

WorkstationsWorkstations are the PCs that everyone does
their work.
St. John’s needed to upgrade each PC that the hospital had to support the new software.

Part of the purchase of any CIS will be to train those utilizing the system. With EPIC, Certified Trainers were sent to Wisconsin for training by the company, EpicCare. As it was during the CIS implementation at St. John’s, those who would help the remainder of the system to become trained were the “Credential Trainers” for the next site for training, which included retired teachers.

ImplementationPrior to implementing a CIS, a committee
known as Genesis at St. John’s, gathered information from all aspects from the hospital end-users. This committee represented a cross-section of all areas of the system. The needs from the end-user was translated into what the software was going to accomplish for our healthcare system. Going “live” would be done in phases as to eliminate potential unforeseen issues.

Implementation Other aspects needing to be considered is the
“transitional time and problems associated with switching over to a new clinical software.”
http://informatics.umdnj.edu/clinical/information_systems.htm

Challenge To ImplementationMercy wanted to standardize all areas to
reduce the cost of building software. Most common challenge was to standardize all order sets collaboratively across all regions.
Micki Struckhoff, RN – VP Systems Integration, St. Johns Springfield

Updates for the software are twice per year. This year will be a full system upgrade in December. Those wishing to improve their skills have the opportunity to work in a computer lab setting prior to utilizing the upgraded software.

SummaryWhile the costs associated with this CIS were
considerable, a massive upgrade to the network backbone was the costliest portion. Thousands of due diligence and man hours went into the implementation of the CIS to ensure the most stable, reliable and user-friendly software would run seamlessly in our health care system.

ReferencesAl Mallah, A., Guelpa, P., Marsh, S & van Rooij, T., (2010). Integrating genomic-based clinical decision
support into electronic health records. Personalized Medicine. 7(2), 163-170.
Barey, E.B.,(2009). The Electronic Health Record and Clinical Informatics. In McGonigle, D., & Mastrian, K.
(Eds.), Nursing Informatics and the Foundation of Knowledge(pp.219-237). Boston: Jones and Bartlett
Publishers.
Buppert, C. (2010, January 13). Medscape. Retrieved October 1, 2010, from Authors and Disclosures:
http://www.medscape.com/viewarticle/714812
Clinical Decision Support Systems. (2003). Retrieved October 6, 2010, from
http://www.informatics-review.com/decision-support/index.html
Fetter, M. (2009). Improving information technology competencies: implications for psychiatric mental
health nursing. Issues in Mental Health Nursing, 30(1), 3-13. Retrieved from CINAHL Plus with Full Text
database.

References ContinuedIndeed.com. Salaries for computer technicians in Springfield, MO. Retrieved
October 23, 2010. http://www.indeed.com/salary?q1=Computer+Technician&l1=springfield%2C+mo
Institute of Medicine. (2003). Key capabilities of an electronic
health system: Letter report. Washington, DC: National
Academics Press.
Informatics Institute: University of Medicine & Dentistry of New Jersey . Retrieved October 20, 2010
http://informatics.umdnj.edu/clinical/information_systems.htm

References ContinuedMcDonald, C. (2009). Protecting patients in health information exchange: A defense of the HIPAA
privacy rule. Health Affairs , 447-449.
McGonigle, D. & Mastrian, K. (2009). Nursing Informatics: and the foundation of knowledge ( pp. 193).
Massachusetts: Jones and Bartlett Publishers, LLC.
McGraw-Hill Online Learning Center. Retrieved October, 21, 2010. http://highered.mcgraw-hill.com/sites/0072464011/student_view0/chapter6/glossary.html
Medscape. (2010, September 10). Retrieved October 1, 2010, from OJIN: The Online Journal of Issues
in Nursing: http://www.medscape.com/viewarticle/723608
Miller, E., & Arquiza, E. (1999). Improving computer skills to support hospital restructing. Journal of
Nursing Care Quality, 13(5), 44-56. Retrieved from CINAHL Plus with Full Text database.

References ContinuedReisz, T., Denny, J., Nguyen, D., Braun, D., Merkel, R., Kuhn, P., et al.
(2010). 2010: change & progress: our panel of experts offers
readers their take on what to look for in healthcare technology in
the year ahead. Health Management Technology, 31(1), 12.
Retrieved from CINAHL Plus with Full Text database.
Rosenfeld, K. (2006). What is application-attached storage costing your
facility? As electronic healthcare databases grow, traditional
backup systems may become inadequate. Is information lifecycle
management the future of data storage? Health Management
Technology, 27(8), 22-25. Retrieved from CINAHL Plus with Full
Text database.

References ContinuedStruckhoff, Micki RN – VP Systems Integration, St. John’s Springfield. Personal interview October 25, 2010.
Ten commandments for implementing clinical information systems Proc (Bayl Univ Med Cent). 2004 July; 17(3): 265–269. Retrieved October 23, 2010 www.ncbi.nlm.nih.gov/pmc/articles/PMC1200662/
Transitioning to electronic medical records: the move to electronic records presents
opportunities and challenges for physicians. (2006). AMIA Annu Symp Proc , 629-
633.
University of California, Irvine, Donald Bren School of Information and Computer Sciences. Retrieved October 22, 2010. http://www.ics.uci.edu/.../Tech-EC/EC-EB/index.html
The design and implementation of a computerized patient record at the Ohio State University health system-a success story. (n.d.)
Retrieved from http://www.himss.org/content/files/davies_2001_osuhs.pdf