Taylor J Greenwood, MD, Adam Wallace, MD, Aseem Sharma, MD, Jack Jennings, MD, PhD.
23
Imaging of Spinal Metastases after Percutaneous Ablation Taylor J Greenwood, MD, Adam Wallace, MD, Aseem Sharma, MD, Jack Jennings, MD, PhD
-
Upload
malcolm-jordan -
Category
Documents
-
view
220 -
download
0
Transcript of Taylor J Greenwood, MD, Adam Wallace, MD, Aseem Sharma, MD, Jack Jennings, MD, PhD.

Imaging of Spinal Metastases after Percutaneous AblationTaylor J Greenwood, MD, Adam Wallace, MD, Aseem Sharma, MD, Jack
Jennings, MD, PhD
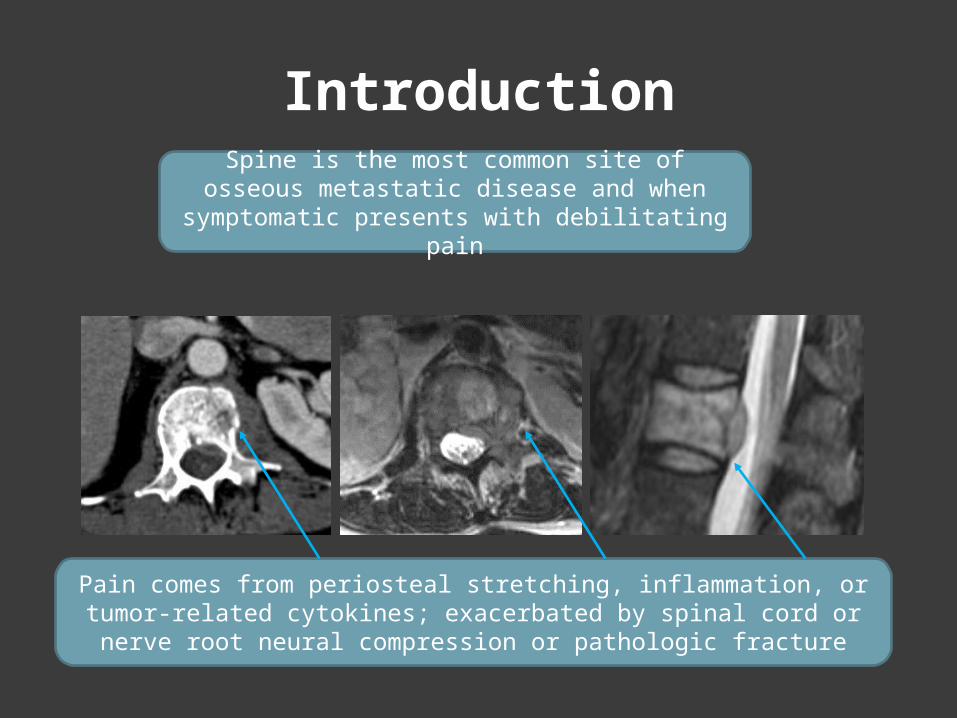
IntroductionSpine is the most common site of osseous metastatic disease and when symptomatic
presents with debilitating pain
Pain comes from periosteal stretching, inflammation, or tumor-related cytokines; exacerbated by spinal cord or nerve root neural
compression or pathologic fracture

First line for symptomatic metastases
-NSAIDS-Acetomenophen-Opioids
-High doses often required-Drowsiness, altered mental status and limits independence (no driving)
Analgesics
Treatment Options

Treatment Options
Cytotoxic and Targeted Therapy
-Improved survival-Side effects sometimes not tolerated-Pain relief variable, often takes weeks to months
Chemotherapy

Treatment Options
Conventional external beam radiation therapy-Partial (~60%) and complete (23%) palliation rates
Stereotactic body radiation therapy-May have better longer lasting pain and tumor control
Radiation
Treatment Options
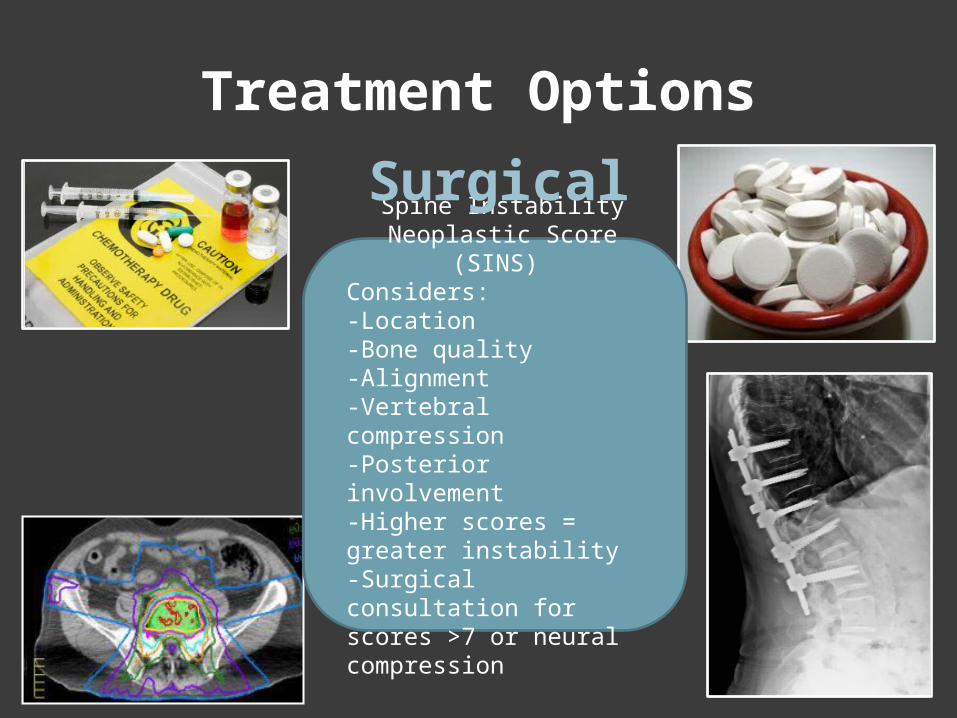
Spine Instability Neoplastic Score (SINS)
Considers:-Location-Bone quality-Alignment-Vertebral compression-Posterior involvement -Higher scores = greater instability-Surgical consultation for scores >7 or neural compression
Surgical
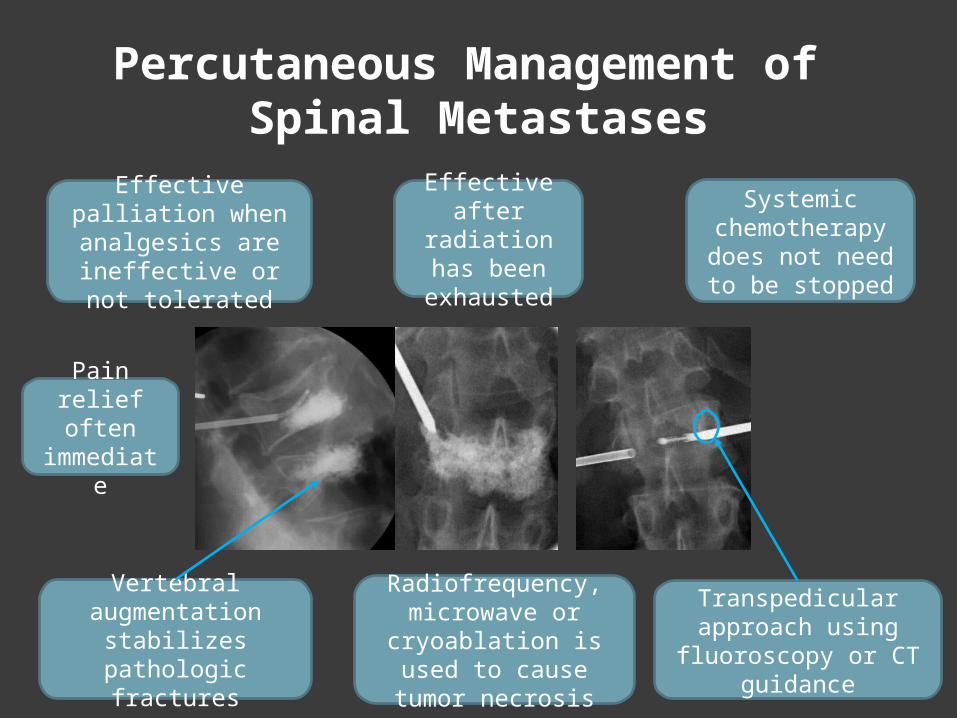
Percutaneous Management of Spinal Metastases
Transpedicular approach using
fluoroscopy or CT guidance
Radiofrequency, microwave or
cryoablation is used to cause tumor
necrosis
Vertebral augmentation
stabilizes pathologic fractures
Effective palliation when analgesics are ineffective or
not tolerated
Effective after
radiation has been
exhausted
Systemic chemotherapy does not need to be stopped
Pain relief often
immediate

Imaging for Treatment Planning
CT Cortical integrity
Posterior vertebral wall
Pedicle medial cortex
Tumor may retract,Osseous canal stenosis
will not
When intact: it is a firm backstop during transpedicular acces
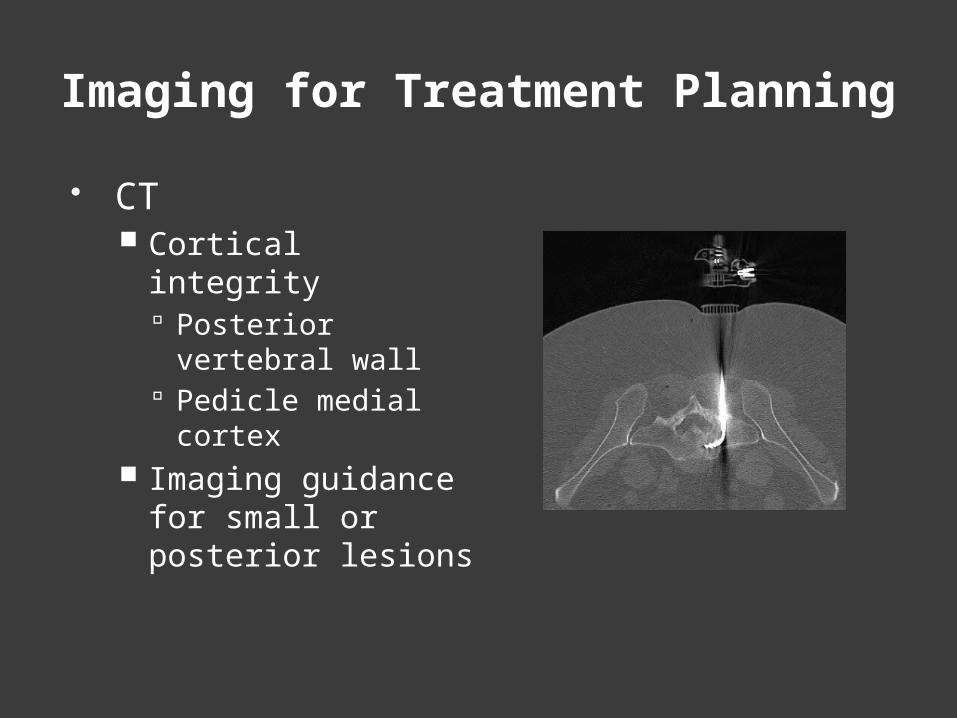
Imaging for Treatment Planning
CT Cortical integrity
Posterior vertebral wall
Pedicle medial cortex
Imaging guidance for small or posterior lesions
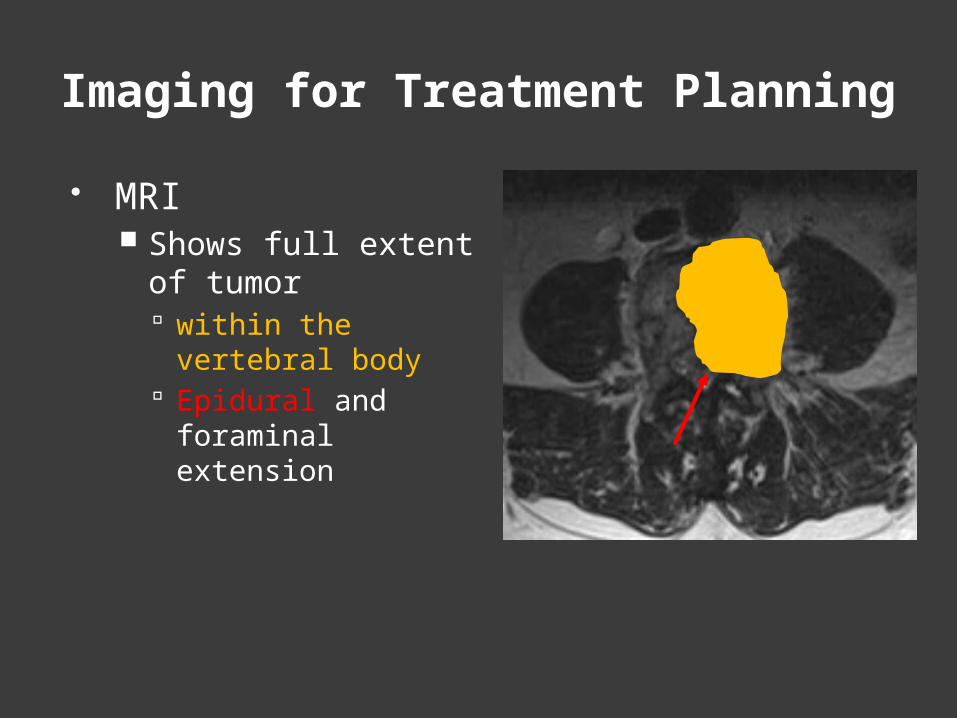
MRI Shows full extent of
tumor within the vertebral
body Epidural and
foraminal extension
Imaging for Treatment Planning

MRI Shows full extent of
tumor within the vertebral
body Epidural and
foraminal extension Reveals tumor at
adjacent levels
Imaging for Treatment Planning
Pain cannot be localized to a single level when contiguous
levels are involved.MRI changed management to a 2
level procedure ?
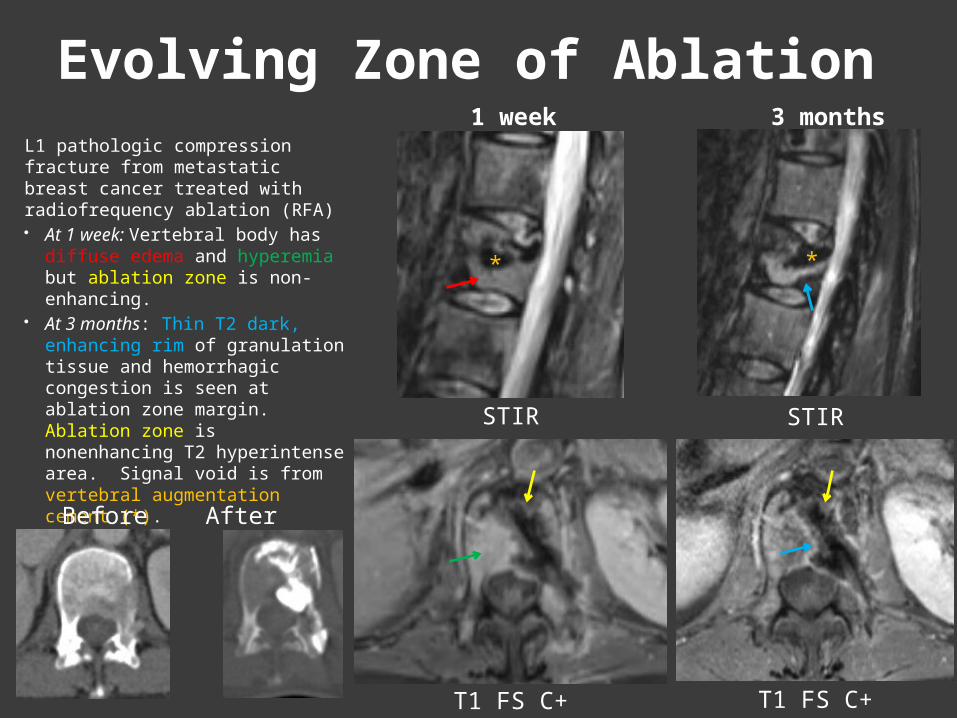
Evolving Zone of AblationL1 pathologic compression fracture from metastatic breast cancer treated with radiofrequency ablation (RFA) At 1 week: Vertebral body
has diffuse edema and hyperemia but ablation zone is non-enhancing.
At 3 months: Thin T2 dark, enhancing rim of granulation tissue and hemorrhagic congestion is seen at ablation zone margin. Ablation zone is nonenhancing T2 hyperintense area. Signal void is from vertebral augmentation cement (*).
STIR STIR
T1 FS C+T1 FS C+
**
Before After
1 week 3 months

Margin of EnhancementL3 metastatic renal cell carcinoma treated with stereotactic radiation followed 10 months later by RFA Lytic metastasis has central non-
enhancement consistent with tumor necrosis centrally and viable tumor peripherally
At 2 months after RFA: Paraspinal muscle inflammation is seen, likely from the percutaneous ablation. There is mild residual hyperemia of the vertebral body and signal void from cement. T2 hyperintense smoothy enhancing margin was stable for > 1 year, therefore likely granulation tissue.
Granulation response can be variable in thickness, smooth contour favors fibrosis
T2
T1 FS C+
T2
T1 FS C+
Before After
2 months

Margin of Enhancement
In contrast to the previous example . . .
L1 small cell lung cancer metastasis treated with RFA Zone of ablation is
non enhancing but nodular enhancing soft tissue outside the zone of ablation has increased, indicating residual tumor
Salvage Radiation Therapy resulted in tumor retraction
*
*
T1 FS C+
T2T2
T1 FS C+
Pre-Tx 2 months
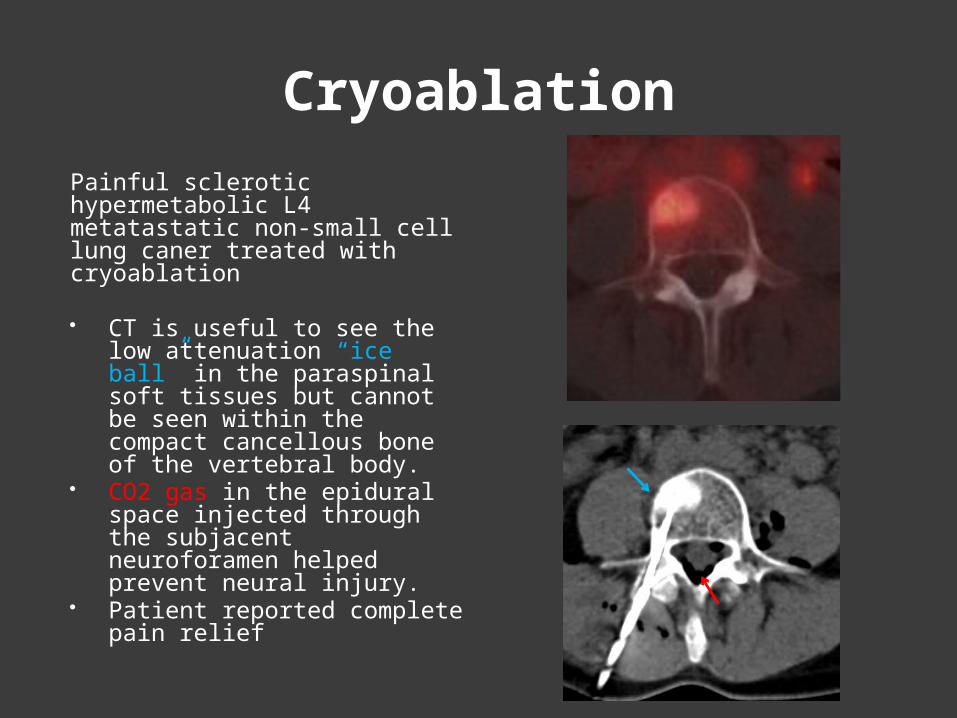
Cryoablation
Painful sclerotic hypermetabolic L4 metatastatic non-small cell lung caner treated with cryoablation
CT is useful to see the low attenuation “ice ball” in the paraspinal soft tissues but cannot be seen within the compact cancellous bone of the vertebral body.
CO2 gas in the epidural space injected through the subjacent neuroforamen helped prevent neural injury.
Patient reported complete pain relief

Tumor Recurrence
MRI 10 months after cryoablation showed tumor recurrence Ablation tract and T2
dark rim of hemorrhagic congestion are clearly seen
Nodular enhancement is seen within the ablation zone and in the right psoas muscle
T2 dark enhancing marrow is due to the blastic metastasis
Axial T1 FS C+ T2
Sag T1 FS C+ T2

Imaging Correlation
S4 rectal cancer metastasis treated with cryoablation CT guidance shows the “ice
ball” delineating the ablation zone.
At 4 months: MRI and PET/CT correlate with the original ablation zone
Central T1 hypointense, T2 hyperintense coagulation necrosis with T2 hypointense, T1 hyperintense rim of hemorrhagic congestion is seen just like RFA
PET/CT shows no uptake in the ablation zone, but disease progression was seen at contiguous levels
Cryoablation Sag T2
Axial T1 FS Pre-C PET/CT
*
*

Post contrast images show tumor enhancement at S3 and necrosis from ablation
at S4
Diffusion Weighted Images
DWI can be helpful adjunct tool in evaluating post treatment changes from tumor. Particularly if contrast in
contraindicated and tumor restricted initially
Coagulation necrosis has rapid diffusion (relatively lower high b value signal and increased ADC)
Metastases often have restricted diffusion
DWI
ADC
S3 No Tx S4 s/p cryoablation
T2T1 FS C+

Pitfall: T1 hyperintensity
Sacral rectal cancer metastasis 1 month after RFA. T2 heterogeneous,
T1 hyperintensity within the ablation zone: hemorrhage or tumor?
Subtraction images are helpful in differentiating residual tumor from hemorrhage.
T1 FS C+
T2 FS T1
CTSubtraction

PET/CTOligometastatic Ewing’s sarcoma to L4 treated with RFA Follow up PET/CT 3 weeks after
RFA showed residual hypermetabolic lesion
Despite attempted retreatment tumor progression was seen 2 months later Patients symptoms also
returned
Baseline 3 weeks later
2 months after 2nd RFA
2nd RFA
PET/CT can detect residual hypermetabolic
disease before symptoms return and
helps differentiate tumor from granulation tissue

Tumor or Fibrosis?
L5 = RFA treated lesion with marrow fibrosisL4 = viable metastatic disease
Tumor
Fibrosis
T1 T2 T1 FS C+PET/CT
When to Biopsy
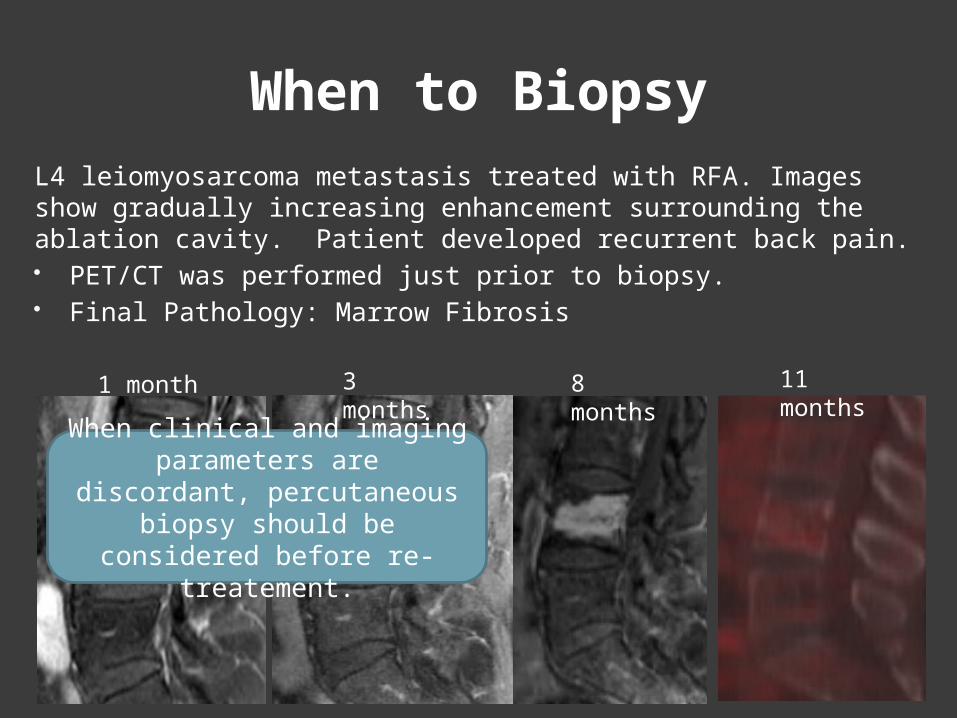
1 month 11 months
3 months
8 months
L4 leiomyosarcoma metastasis treated with RFA. Images show gradually increasing enhancement surrounding the ablation cavity. Patient developed recurrent back pain. PET/CT was performed just prior to biopsy. Final Pathology: Marrow Fibrosis
When clinical and imaging parameters are discordant, percutaneous biopsy should
be considered before re-treatement.

Summary
Post Ablation changes evolve over the first several months due to an inflammatory response
Margin of Enhancement: Thin, smooth = expected treatment change Thick or increasing enhancement does not always
equal tumor When clinical and imaging parameters are
discordant, biopsy should be considered before re-treatment.
PET/CT and DWI are useful in evaluation of residual or recurrent hypermetabolic disease.