TAVR SPRING 2017 - Bryan Health...4/13/2017 Nithin P G 1 Matthew Johnson, MD TAVR SPRING 2017 The...
22
4/13/2017 Nithin P G 1 Matthew Johnson, MD TAVR SPRING 2017 The evolution of TAVR Disclosers None Evolution of the Balloon- Expandable Transcatheter Valves * Sheath compatibility for a 23 mm valve 2002 Cribier 2006 SAPIEN 2009 SAPIEN XT 2013 SAPIEN 3
Transcript of TAVR SPRING 2017 - Bryan Health...4/13/2017 Nithin P G 1 Matthew Johnson, MD TAVR SPRING 2017 The...

4/13/2017
Nithin P G 1
Matthew Johnson, MD
TAVR SPRING 2017The evolution of TAVR
Disclosers
None
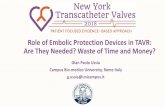
Evolution of the Balloon-Expandable Transcatheter Valves
* Sheath compatibility for a 23 mm valve
2002
Cribier
2006
SAPIEN
2009
SAPIEN XT
2013
SAPIEN 3

4/13/2017
Nithin P G 2
Introduction
AV
R
High risk for
surgery
Complications30-40% do not undergo Sx
•Advanced age
•LV dysfunction
•Multiple co-morbidities
•Pt. preference
•Physician assessment
“Symptomatic Severe Aortic
Stenosis” Prohibitive risk
Inoperability
•~3% mortality (STS, EuroSCORE)
•~2% Stroke
•~11% prolonged ventilation
•Organ failure
•Thromboembolic Complications
•Bleeding
•Prosthetic valve DysfunctionJ. Am. Coll. Cardiol. 2012;59;1200-1254
Indications 2012
• A Symptomatic severe calcific Aortic Stenosis [trileaflet] who
have aortic and vascular anatomy suitable for TAVR and a
predicted survival >12 months, and who have a prohibitive
surgical risk as defined by an estimated 50% or greater risk of
mortality or irreversible morbidity at 30 days or other factors such as frailty, prior radiation therapy, porcelain aorta, and severe hepatic
or pulmonary disease.
• TAVR is a reasonable alternative to surgical AVR in patients at
high surgical risk (PARTNER Trial Criteria: STS >8)
J. Am. Coll. Cardiol. 2012;59;1200-1254
Indications
Patient selection in clinical trials
Logistic EuroSCORE >20% or STS Score > 10.
J. Am. Coll. Cardiol. 2012;59;1200-1254

4/13/2017
Nithin P G 3
Indications
J. Am. Coll. Cardiol. 2012;59;1200-1254
Requisites
• ‘Heart team’ approach– Specific team leader
– Close communication
– ‘Preplanning procedure’
• Large cathlabs/ ‘hybrid’ rooms– Fluoroscopic imaging
– TEE capabilities
– GA/ CPB
– Vascular intervention
– Urgent AVR, CABG, Vascular complications
• Anesthesia
– Conscious sedation/ GA
– CPB facility
– Hemodynamic monitoring
and management
Work up
• Pre-anesthetic work up
• Cardiothoracic evaluation [access, AVR, risk assessment]
• Imaging– AS severity, morphology, calcification, annular size and shape
– Aortic root, annulus to coronary ostia (>8mm), Atheroma burden, calcification
– Other valvular disease, sub aortic obstruction
– LV function
– Vascular anatomy from access site to annulus
– Cerebro vascular imaging

4/13/2017
Nithin P G 4
Work upRole of imaging in pre-procedural and post procedural assessment
J. Am. Coll. Cardiol. 2012;59;1200-1254
Transcatheter Aortic Valve
Intervention
Procedure & Hardware
Procedure & Hardware• LA + Conscious sedation/ GA, hemodynamic stability [ SBP~120 mm
Hg / MAP >75 mm Hg]
• Vascular access
– Sites
• Transfemoral
• Transapical
– Left ant. thoracotomy
– More direct, shorter catheter
– Septal hypertrophy
– Ascendra2, Sapien valve
• Transaortic
– Upper partial sternotomy
– Mini-sternotomy 2/3 RICS
– Aorta 5 cm above valve
– Less painful, familiar approach
– Manipulation of ascending aorta
• Subclavian
Percutaneous
or Cut-down
technique
J. Am. Coll. Cardiol. 2012;59;1200-1254

4/13/2017
Nithin P G 5
Procedure & Hardware
• Pacing leads – Trans venous or epicardial
• Anticoagulation
– Large sheaths
– Heparin [ACT>300]
• Intra-procedural TEE
– Guidewire placement
– Valve placement
• Stable position
• No coronary obstruction
• No interference with mitral valve function
• No conduction system impingement
• No overhanging native aortic leaflets
• Avoidance of aortic root complications (rupture & dissection)
– Post deployment assessment [MR, AR]
TEE- Mid esophageal
long axis view
J. Am. Coll. Cardiol. 2012;59;1200-1254
Procedure & Hardware‘Sapien XT’ device ‘CoreValve’ device
Self expandable
Nitinol frame
Porcine
Pericardial
Tissue
European Heart Journal (2011) 32, 140–147
Cardiol Clin 29 (2011) 211–222
•Superior hemodynamics
•Lower risk for PPM
Procedure & HardwarePressure tracings before and after TAVR
European Heart Journal (2011) 32, 140–147

4/13/2017
Nithin P G 6
Procedure & Hardware
European Heart Journal (2011) 32, 140–147
Post-Operative Care & Monitoring
• Immediate or early extubation, early mobilization
• Adequate analgesia, control postoperative hypertension,
monitor for any bleed
• Monitor vital parameters including fluid balance, renal status,
and AV conduction system.
• Pre-discharge TTE, DAPT,Coumadin vs NOAC
J. Am. Coll. Cardiol. 2012;59;1200-1254
Complications & Management

4/13/2017
Nithin P G 7
Complications & Management
Left main stem compromise with semi-occlusive displacement of
calcified nodule from aortic valve.
Treated with CPB� device explantation � AVR
Also PCI/CABG
Cardiol Clin 29 (2011) 211–222
J. Am. Coll. Cardiol. 2012;59;1200-1254
Complications & Management
• Incidence of CHB requiring permanent pacemaker implantation has been higher with the CoreValve (19.2% to 42.5%) than with the Sapien valve (1.8% to 8.5%) [larger profile and extension low into the LVOT
• Occurrence of CHB/LBBB
– BAV 46%
– Balloon/prosthesis positioning &wire-crossing of the aortic valve 25%
– Prosthesis expansion 29%.
• Pre-existing RBBB risk factor for CHB
J. Am. Coll. Cardiol. 2012;59;1200-1254
Complications & Management
Aortic Regurgitation
•Typically paravalvular mild or
mild-moderate severity
•Most of AR disappears or reduces
at 1 yr follow-up [13% absent, 80%
mild AR]
J. Am. Coll. Cardiol. 2012;
59;1200-1254
Cardiol Clin 29 (2011) 211–222

4/13/2017
Nithin P G 8
Complications & Management
Paravalvular AR
Central valvular AR
Post-deployment balloon dilation, rapid RV
pacing for stabilization, ‘valve in valve’
implantation
Usually self-limited, Gentle probing of leaflets
with a soft wire or catheter
Delivery of a 2nd TAVR device, ‘valve in valve’
J. Am. Coll. Cardiol. 2012;59;1200-1254
Complications & Management Rapid Pacing for stabilization
‘Valve in Valve’ Implantation
Reduction
of diastole
Cardiol Clin 29
(2011) 211–222
Complications & Management
Causes of hypotension after TAVI
•Vascular complications—iliac rupture
•Ventricular rupture
•Acute valve dysfunction
•Coronary artery obstruction
•Multiple rapid pacing episodes in pts with poor LV function
•‘Suicidal’ LV in severe LVH [After removing AV obstruction LV
decompresses to such an extent that the subvalvular hypertrophy
obstructs outflow] treated with fluids & avoiding diuretics
Cardiol Clin 29 (2011) 211–222 J. Am. Coll. Cardiol. 2012;59;1200-1254

4/13/2017
Nithin P G 9
Complications & Management
Significant annular rupture
Ventricular perforation
•Pericardial drainage, auto-transfusion
•Conversion to open surgical closure
Device malposition
Device embolization
Overlapping ‘valve in valve’
Urgent endovascular/ surgical
management
Major ischemic stroke
Minor ischemic stroke
Hemorrhagic stroke
Catheter-based, mechanical embolic retrieval
Aspirin, anticoagulants
Anticoagulation reversal, coagulopathy correction
J. Am. Coll. Cardiol. 2012;59;1200-1254
Complications & Management
Atrial fibrillationRate control/ rhythm control via
pharmacological or electrical
cardioversion
Shock, low cardiac output
Major bleeding
Vascular complications
•Careful systemic pressure management,
inotropic support, IABP, or CPB
•Hemodynamic support, blood transfusion
•Urgent endovascular repair/surgery
J. Am. Coll. Cardiol. 2012;59;1200-1254
Transcatheter Aortic Valve
Intervention
Review of evidence

4/13/2017
Nithin P G 10
Review of Evidence
Registry data
•Age> 80 years
•EuroSCORE [> 23 ‘Sapien’, >16 ‘CoreValve’]
•Route of implantation no difference in procedural success rate b/w
TF & TA accesses
•Major bleeding more in TA vs. more vascular complications in TF
J. Am. Coll. Cardiol. 2012;59;1200-1254
Review of EvidencePARTNER Trial Design
Cohort A
84 yrs
N=699
Cohort B
83 yrs
N=358
J. Am. Coll. Cardiol. 2012;59;1200-1254www.nejm.org
Background
• Based on randomized trials with first generation devices,
transcatheter aortic valve replacement (TAVR) has been
incorporated into the treatment strategy for high-risk and
inoperable patients with severe AS.
• Procedural complications remain a concern with TAVR,
including stroke, vascular complications, paravalvular leak
(PVL) and conduction disturbances.
• Addressing these limitations will support TAVR use in lower
risk populations.

4/13/2017
Nithin P G 11
Evolution of the Balloon-Expandable Transcatheter Valves
* Sheath compatibility for a 23 mm valve
2002
Cribier
2006
SAPIEN
2009
SAPIEN XT
2013
SAPIEN 3
SAPIEN 3 Transcatheter Heart ValveDistinguishing Features
Bovine pericardial
tissue
Outer skirt to reduce PVL
Low frame height
Enhanced frame geometry for
ultra-low delivery profile
SAPIEN 3 Commander Delivery SystemDistinguishing Features
• Accurate positioning
Fine control of valve positioning Distal flex
SAPIEN 3 Valve Size 20 mm 23 mm 26 mm 29 mm
Expandable Sheath 14F 14F 14F 16F
Minimum Access Vessel Diameter 5.5 mm 5.5 mm 5.5 mm 6.0 mm
• Improved coaxial alignment

4/13/2017
Nithin P G 12
The PARTNER II ProgramPurpose
To evaluate the safety and efficacy of the SAPIEN 3
transcatheter heart valve system at 30 days in
inoperable, high-risk, and intermediate-risk patients.
Intermediate Risk
Operable(PII S3i)
High Risk Operable /
Inoperable (PII S3HR)
Symptomatic Severe Aortic Stenosis
ASSESSMENT by Heart Valve Team
n = 1076
Patients
n = 583
Patients
ASSESSMENT:
Optimal Valve
Delivery Access
ASSESSMENT:
Optimal Valve
Delivery Access
SAPIEN 3
2 Single Arm Non-Randomized
Historical-Controlled Studies
Transfemoral (TF)
TF TAVR
SAPIEN 3TAA TAVR
SAPIEN 3
Transapical /
Transaortic (TA/TAo)
TF TAVR
SAPIEN 3
PI A
SAPIEN
PII A
SAVR
Transfemoral (TF)
TAA TAVR
SAPIEN 3
Transapical /
Transaortic (TA/TAo)
The PARTNER II S3 TrialStudy Design
Key Inclusion Criteria
• Risk determined by STS score and heart team:
– High Risk / Inoperable (S3HR): STS score > 8 or heart team
determination
– Intermediate Risk (S3i): STS score between 4 and 8 or heart
team determination
• Severe aortic stenosis determined by echocardiography:
– Valve area < 0.8 cm2 or Valve area index < 0.5 cm2/m2 and mean
gradient > 40mmHg or peak velocity > 4 m/s

4/13/2017
Nithin P G 13
Key Exclusion Criteria
• MI within one month
• Bicuspid aortic valve
• Severe aortic regurgitation
• Prior prosthetic valve in any position
• Untreated significant CAD (S3HR only)
• LVEF < 20%
• Stroke or TIA within 6 months
• Upper GI bleed within 3 months
• Creatinine > 3.0 or dialysis
• Estimated life expectancy< 24 months
Study Methodology
• All patients presented on a screening call for approval prior to
implant.
• 3D imaging of annulus (CT or 3D TEE) recommended for S3HR and
required for majority of S3i with core lab analysis prior to implant.
• All patients evaluated by a neurologist at baseline and at follow-up
time points.
• Primary Analysis: As treated patients
• S3HR and S3i combined for echocardiographic analyses (valve
implant patients).
Study Flow: S3HR & S3i30 Day Patient Status
0 Withdrawal
3 LTFU
13 Deaths
0 Withdrawal
5 LTFU
12 Deaths
S3HR S3i
n = 583n = 583
n = 570
SAPIEN 3
n = 570
SAPIEN 3
567 / 570 or 99.5% follow-upvisits performed at 30 Days 567 / 570 or 99.5% follow-upvisits performed at 30 Days
n = 1076n = 1076
n = 1064
SAPIEN 3
n = 1064
SAPIEN 3
1059 / 1064 or 99.5% follow-upvisits performed at 30 Days
1059 / 1064 or 99.5% follow-upvisits performed at 30 Days

4/13/2017
Nithin P G 14
Baseline Patient CharacteristicsS3HR Patients
Average STS =
8.6%(Median 8.4%)
N = 583Average Age =
82.6yrs
Baseline Patient CharacteristicsS3i Patients
Average STS =
5.3%(Median 5.2%)
N = 1076Average Age =
81.9yrs
Baseline Patient CharacteristicsDemographics
Characteristic (%)S3HR(n=583)
S3i(n=1076)
NYHA Class III or IV 90.1 72.6
Previous CABG 33.1 28.0
Previous CVA 11.0 8.9
Peripheral Vascular Disease 35.2 28.3
Diabetes 34.5 34.1
COPD - O2 Dependent 11.7 5.0
CKD - Creat. ≥ 2mg/dL 12.0 7.5
Atrial Fibrillation 43.7 36.0
Permanent Pacemaker 16.3 13.2
Frailty 30.9 8.6

4/13/2017
Nithin P G 15
Baseline Echocardiography
CharacteristicS3HR(n=583)
S3i(n=1076)
AV Area - cm2 (mean ± SD) 0.67 ± 0.18 0.70 ± 0.17
Annulus Diam. - cm (mean ± SD) 2.2 ± 0.2 2.2 ± 0.2
AV Gradient - mmHg (mean ± SD) 45.5 ± 14.3 46.3 ± 12.7
LV Ejection Fraction (%) 56.4 ± 14.8 58.6 ± 13.3
Mod-Severe MR (%) 3.0 2.3
Procedural Factors
S3HR(n=583)
S3i(n=1076)
Post-Dilatation (%) 14.8 11.3
>1 Valve Implanted (%) 0.9 0.4
Valve Embolization (%) 0.2 0.1
IABP During Procedure (%) 0.5 0.4
Cardiopulmonary Bypass (%) 1.2 0.6
Conscious Sedation (%) 13 17
Median LOS – Days (Min, Max) 5 (1, 33) 4 (1, 64)
Mortality and Stroke: S3HRAt 30 Days (As Treated Patients)
% O:E = 0.26
(STS 8.6%)
Mortality Stroke
%

4/13/2017
Nithin P G 16
Mortality and Stroke: S3iAt 30 Days (As Treated Patients)
O:E = 0.21
(STS 5.3%)
Mortality Stroke
% %
Transfemoral Transapical / Transaortic
%
Mortality: S3HR & S3iAt 30 Days (As Treated Patients)
491 947 92 125
All-Cause Mortality at 30 DaysSAPIEN Valves (As Treated Patients)
175 344 240 271 282 583 491 1072 947
SAPIEN SXT SAPIEN 3
PARTNER I and II Trials
Overall and TF Patients

4/13/2017
Nithin P G 17
104 125 94 92 125
SAPIEN SAPIEN XT SAPIEN 3
Nested Registries
All-Cause Mortality at 30 DaysSAPIEN Valves (As Treated Patients)
PARTNER I and II Trials
TA/TAo Patients
StrokesAt 30 Days (As Treated Patients)
Events (%)
S3HROverall(n=583)
S3HRTF
(n=491)
S3HRTA/TAo(n=92)
S3iOverall(n=1076)
S3iTF
(n=951)
S3iTA/TAo(n=125)
All 1.54 1.63 1.09 2.60 2.42 4.00
Disabling* 0.86 0.81 1.09 1.02 0.95 1.60
Non-Disabling 0.69 0.81 0 1.58 1.47 2.40
TIA 0.69 0.61 1.09 0.37 0.42 0
*CEC adjudicated or Modified Rankin Score ≥ 2 at 30 days
All Strokes at 30 DaysSAPIEN Valves
SAPIEN SAPIEN XT SAPIEN 3
PARTNER I and II Trials
Neurologist evaluations (pre- and post)

4/13/2017
Nithin P G 18
Other Clinical EventsAt 30 Days (As Treated Patients)
Events (%)
S3HROverall(n=583)
S3HRTF
(n=491)
S3HRTA/TAo(n=92)
S3iOverall(n=1076)
S3iTF
(n=951)
S3iTA/TAo(n=125)
Major Vascular Comps. 5.0 5.3 3.3 5.6 5.9 3.2
Bleeding - Life Threatening 6.3 5.5 10.9 5.4 4.4 12.9
Annular Rupture 0.3 0.2 1.1 0.2 0.2 0
Myocardial Infarctions 0.5 0.4 1.1 0.3 0.3 0
Coronary Obstruction 0.2 0 1.1 0.4 0.4 0
Acute Kidney Injury 1.0 0.8 2.2 0.5 0.3 1.6
New Permanent Pacemaker 13.0 13.2 12.0 10.1 10.4 7.2
Aortic Valve Re-intervention 1.0 0.8 2.2 0.7 0.8 0
Endocarditis 0.2 0.2 0 0.1 0.1 0
%
Baseline 30 Days
90%
73%
13%6%
583 10495501075
I
II
III
IV
NYHA Functional ClassAt 30 Days (As Treated Patients)
Echo Findings: S3HR & S3iAortic Valve Area (Valve Implant Patients)
No. of EchosOverall 1546 1461

4/13/2017
Nithin P G 19
0.69
1.67
0.75
1.90
0.70
1.74
0.63
1.46
0.62
1.22
0
0.2
0.4
0.6
0.8
1
1.2
1.4
1.6
1.8
2
Baseline 30 Days
Va
lve A
rea
(cm
²)
Overall
29 mm
26 mm
23 mm
20 mm
No. of EchosOverall 1546 1461
Echo Findings: S3HR & S3iAortic Valve Area (Valve Implant Patients)
No. of EchosOverall 1602 1531
Echo Findings: S3HR & S3iMean Gradients (Valve Implant Patients)
46.0
11.3
50.1
16.7
47.6
13.0
45.5
10.8
43.9
9.1
0.0
10.0
20.0
30.0
40.0
50.0
60.0
Baseline 30 Days
Gra
die
nt
(mm
Hg
)
Overall
20 mm
23 mm
26 mm
29 mm
No. of Echos
Echo Findings: S3HR & S3iMean Gradients (Valve Implant Patients)
Overall 1602 1531

4/13/2017
Nithin P G 20
Paravalvular Leak: S3HR & S3i(Valve Implant Patients)
1504No. of Echos
0.1%
Moderate/Severe PVL at 30 DaysSAPIEN Valves
PARTNER I and II Trials
SAPIEN SAPIEN XT SAPIEN 3

4/13/2017
Nithin P G 21
Conclusions (1)
• In high-risk and inoperable patients (S3HR), the SAPIEN 3
TAVR system demonstrated low mortality and stroke and
excellent clinical outcomes at 30 days:
– Mortality: 2.2% (TF 1.6%, TA/TAo 5.4%)
– Disabling Stroke: 0.9%
• In intermediate-risk patients (S3i), SAPIEN 3 was
associated with strikingly low mortality and strokes at 30
days:
– Mortality: 1.1% (TF 1.1%, TA/TAo 1.6%)
– Disabling Stroke: 1.0%

4/13/2017
Nithin P G 22
Conclusions (2)
• Other important clinical findings with SAPIEN 3
(both S3HR & S3i) include:
– Major vascular complications: ~5%
– Annular rupture: ~0.2%
– Coronary obstruction: ~0.3%
– New pacemakers: ~10%
• Significant paravalvular regurgitation with SAPIEN 3 (both
S3HR & S3i) was rare:
– Severe: 0.1%
– Moderate: 3.7%
Implications
• The rapid evolution of balloon-expandable TAVR,
both procedural developments and technical
enhancements, represented in the SAPIEN 3 clinical
and echo results, indicates at least parity with the
best surgical outcomes in comparable patients.
• SAPIEN 3 TAVR should now be considered as an
alternative to surgery, even in lower risk patients with
aortic stenosis.
Thank YouThank YouThank YouThank You