Task-Shifting in HIV/AIDS Care in a Rural District of Malawi Some successes and lessons learnt from...
24
Task-Shifting in HIV/AIDS Care in a Rural District of Malawi Some successes and lessons learnt from Thyolo Moses Massaquoi, Rony Zachariah, Ulrike von Pilar Médecins Sans Frontières (Operational research) – Brussels District Health Services, Thyolo, Malawi Ministry of Health and Population, Malawi
-
Upload
dorthy-bennett -
Category
Documents
-
view
218 -
download
0
Transcript of Task-Shifting in HIV/AIDS Care in a Rural District of Malawi Some successes and lessons learnt from...

Task-Shifting in HIV/AIDS Care in a Rural District
of Malawi
Some successes and lessons learnt from Thyolo
Moses Massaquoi, Rony Zachariah, Ulrike von Pilar
Médecins Sans Frontières (Operational research) – Brussels
District Health Services, Thyolo, MalawiMinistry of Health and Population, Malawi
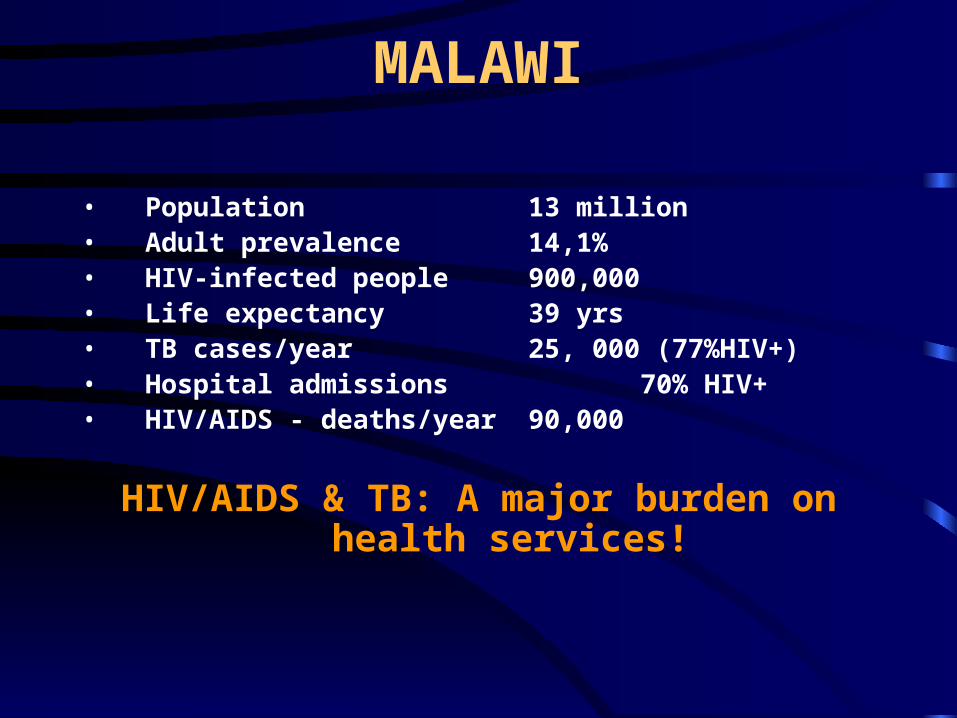
MALAWI
• Population 13 million• Adult prevalence 14,1%• HIV-infected people 900,000 • Life expectancy 39 yrs• TB cases/year 25, 000 (77%HIV+)• Hospital admissions 70% HIV+• HIV/AIDS - deaths/year 90,000
HIV/AIDS & TB: A major burden on health services!
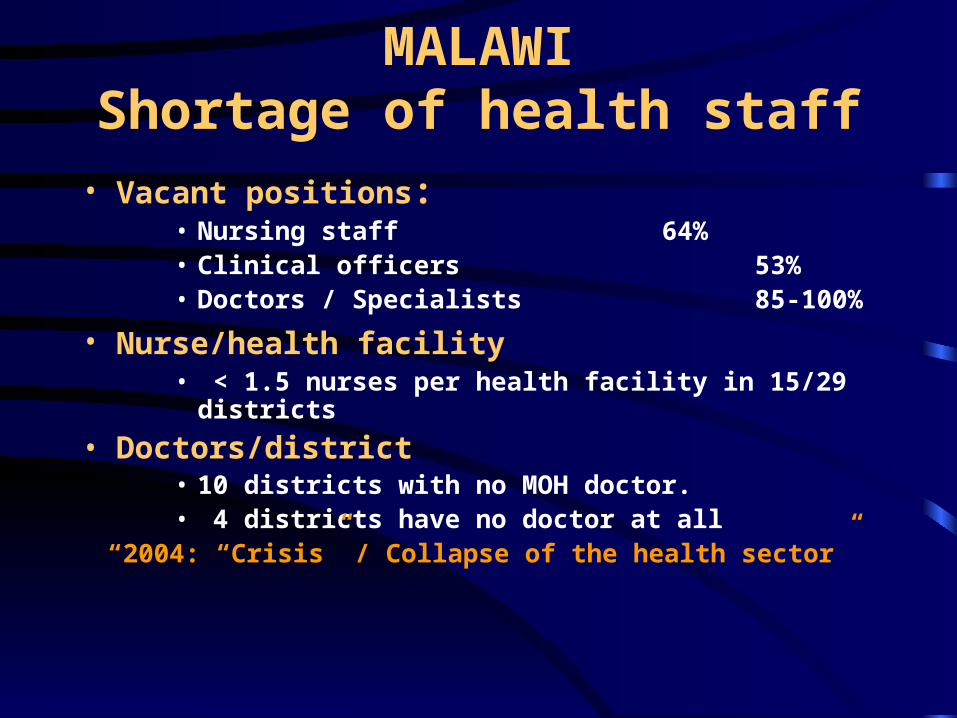
MALAWIShortage of health staff
• Vacant positions:• Nursing staff 64%• Clinical officers 53%• Doctors / Specialists 85-100%
• Nurse/health facility • < 1.5 nurses per health facility in 15/29
districts
• Doctors/district• 10 districts with no MOH doctor.• 4 districts have no doctor at all
“2004: “Crisis” / Collapse of the health sector”
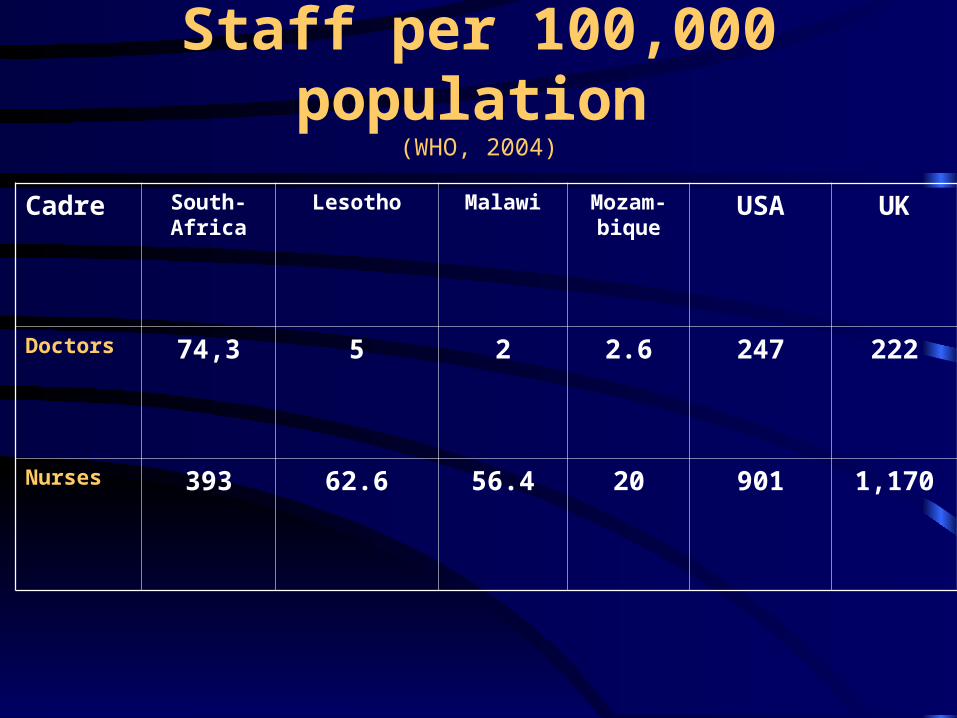
Staff per 100,000 population
(WHO, 2004)
Cadre South-Africa
Lesotho Malawi Mozam-bique
USA UK
Doctors 74,3 5 2 2.6 247 222
Nurses 393 62.6 56.4 20 901 1,170

Background: Thyolo district
OBJECTIVES
To highlight some successes and lessons learnt in “task
shifting” to achieve Universal ART Access in Thyolo.

METHODS (1)Scale up: HIV-testing/ Clinic
services
CT: • Increase sites: from 3 to 26
(trained lay PLWA counsellors)
HIV/AIDS clinics:• Drastically improve efficiency of
“delivery systems” particularly for ART.

METHODS (2) : Clinics “One track” doctor centred “multiple
flow tracks”
• Screening & track allocation - Nurse• Slow track - Medical assistant
• Complicated opportunistic infections (OI)• Side effects/referred patients
• Medium track - Nurse• Less severe OI (eg candida, diarrhoea)• ART initiation /ART follow up (< 1month)
• Fast track - PLWA counsellor• Stable patients & drug refills
Doctor/Clinical officer – Supervision and support
METHODS (3) Community: Involvement & Activities
Community network : (Volunteers/PLWA’s)
– Treatment : diarrhoea, fever, oral thrush….– Community based counselling (ART)– Support to family care givers at home – Referral : drug reactions and “risk signs”.– Cough screening (TB)– Social mobilisation.

METHODS (4) Community: Volunteers

METHODS (5) Community: Home care “kit”

METHODS (6)
Community: Nurses
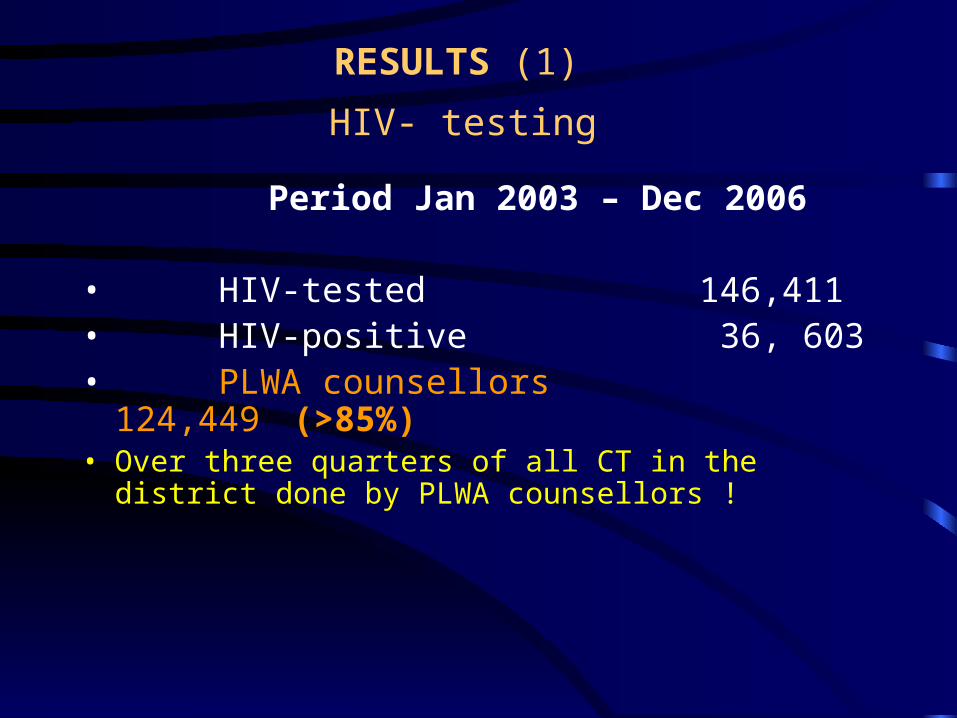
RESULTS (1)
HIV- testing Period Jan 2003 – Dec 2006
• HIV-tested 146,411• HIV-positive 36, 603• PLWA counsellors 124,449
(>85%)• Over three quarters of all CT in the district
done by PLWA counsellors !
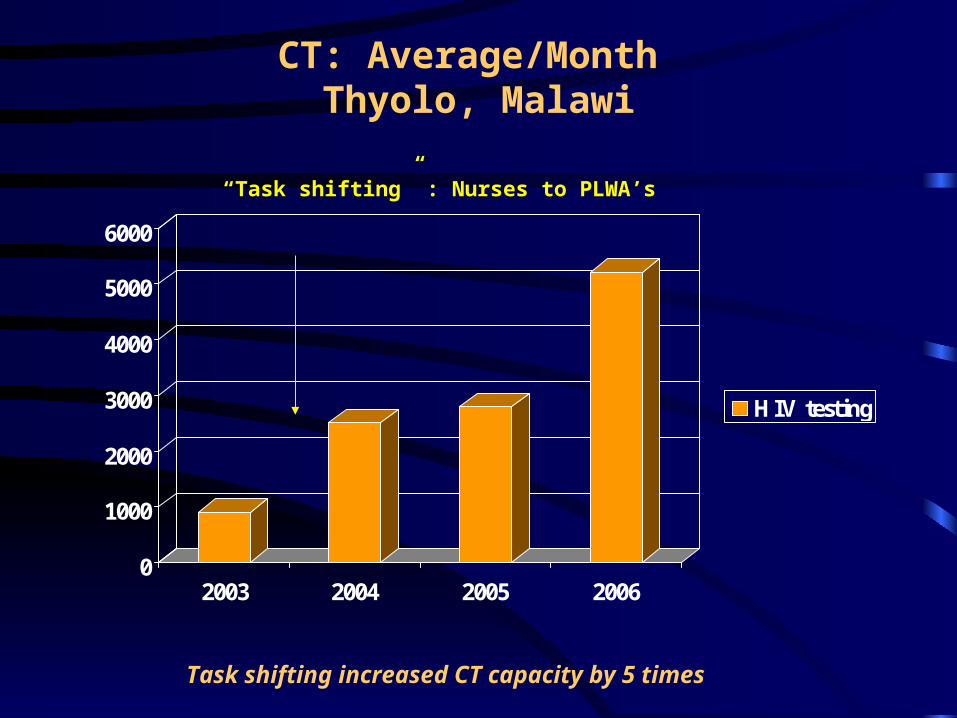
CT: Average/Month Thyolo, Malawi
0
1000
2000
3000
4000
5000
6000
2003 2004 2005 2006
HIV testing
“Task shifting” : Nurses to PLWA’s
Task shifting increased CT capacity by 5 times
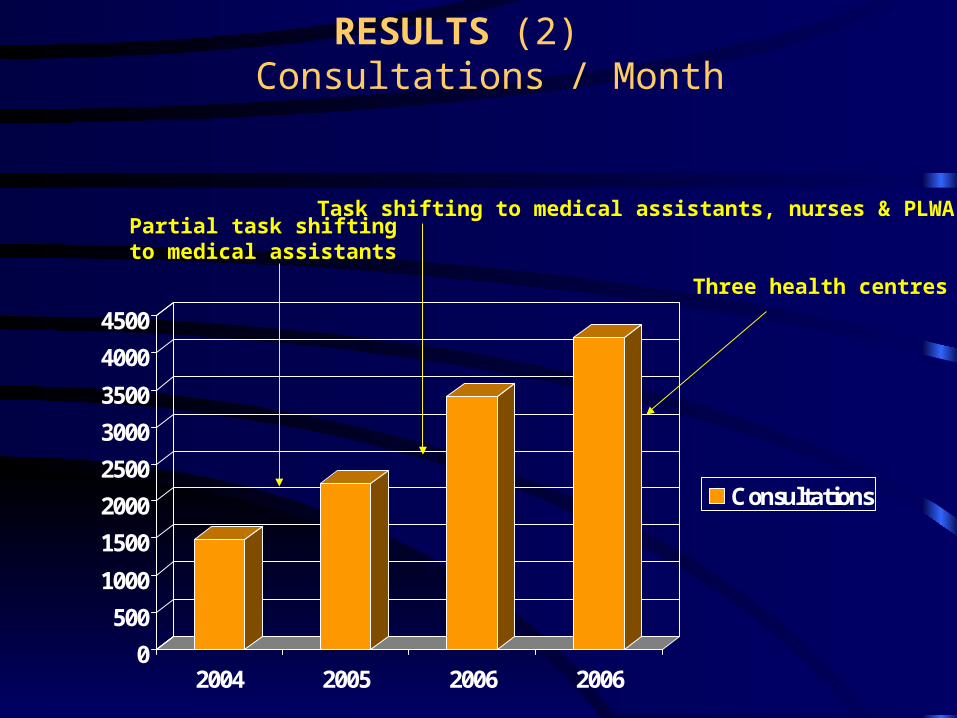
RESULTS (2) Consultations / Month
0
500
1000
1500
2000
2500
3000
3500
4000
4500
2004 2005 2006 2006
Consultations
Task shifting to medical assistants, nurses & PLWA’s Partial task shifting to medical assistants
Three health centres ++
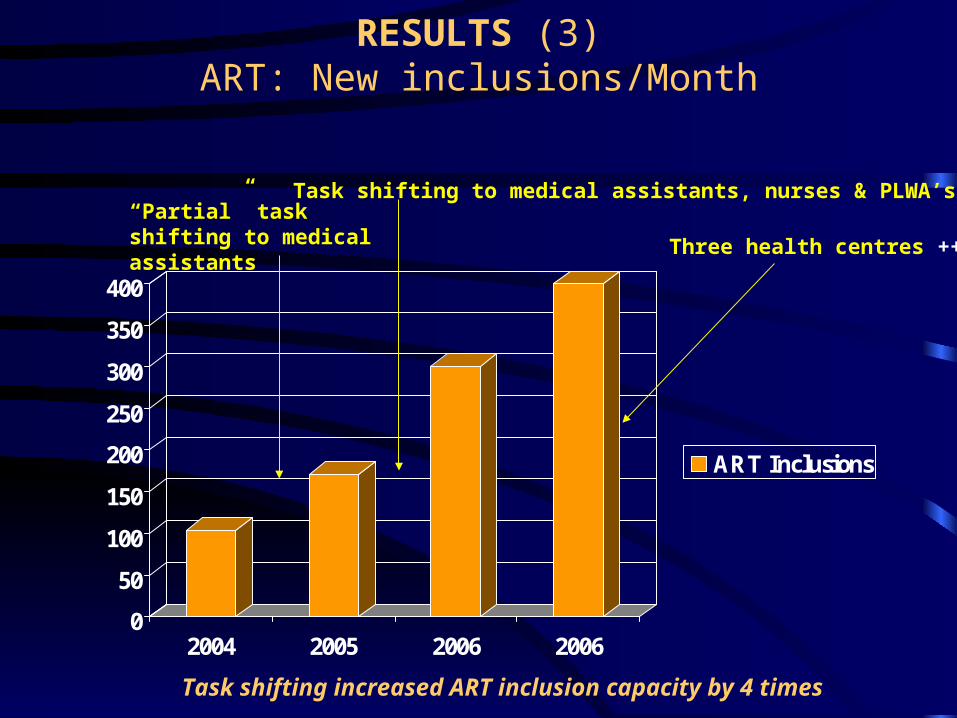
RESULTS (3)ART: New inclusions/Month
0
50
100
150
200
250
300
350
400
2004 2005 2006 2006
ART Inclusions
Three health centres ++
“Partial” task shifting to medical assistants
Task shifting to medical assistants, nurses & PLWA’s
Task shifting increased ART inclusion capacity by 4 times
ART - Thyolo Universal Access - Dec 2007 ?
• ART Target: 10,000 (+-1000)• On ART 6285 (March 2007)• ART initiations/Month 400• Target Nov 2007
Without task shifting, this target would only have been achieved by 2012 !

RESULTS (4)Community: Active TB case finding
(Jan 2003-Dec 2004)
Chronic cough: 3 weeks
No referred (chronic cough) 806 No with Smear + PTB 161 (20%)Annual TB incidence (Households) 1997/100,000Reported TB incidence (Malawi) 265/100,000
“Active” cough screening detects 8 times more infectious TB cases !
RESULTS (5) Antiretroviral treatment (ART)
Period Jan 2003-Dec 2004
• Total placed on ART 1634 • with community support 895
(55%)• without community support 739
(45%)
Compare: ART outcomes among patients
living in areas with and without community support

CONCLUSIONS (1)
• Universal access: Develop a Public Health ART scale-up model, standardize, keep it simple, be inclusive, use lower cadres & community.
“Good for many” instead of “best for a few”
CONCLUSIONS (2)
Be innovative..
Challenge established practices, rules and regulations
“professional turf protection”

ACKNOWLEDGEMENTS
• PLWA associations and groups• District health services, Thyolo • Ministry of Health - Malawi• Financial support:
– G.D of Luxembourg, – DFID, NORAD, Global FUND, EU,
USAID, FHI, KNCV TB foundation, CIFF, WHO STOP-TB….