TAP Depression Anxiety

of 72
-
Upload
arlette-derizka -
Category
Documents
-
view
254 -
download
0
Transcript of TAP Depression Anxiety
-
8/9/2019 TAP Depression Anxiety
1/721
Depression and Anxiety
For internal use only
Therapeutic Area PackDepression and
Anxiety
Psychiatry andNeurology
Psychiatry andNeurology Therapeutic Area Pack
Depression and
Anxiety
Last update: August 2007
-
8/9/2019 TAP Depression Anxiety
2/72
-
8/9/2019 TAP Depression Anxiety
3/723
Depression and Anxiety
For internal use only
1. Marketing Overview 71.1. Situation Analysis 7
1.2. Antidepressants Classes 14
1.3. Antidepressants INN Specific
171.4. Comparison of 10 Leading Antidepressants 20
1.5. Our Portfolio of Antidepressants 22
2. Depressive Disorders Medical Overview 262.1. Etiology and Pathophysiology 26
2.2. Classification 26
2.3. Epidemiology 27
2.4. Disease Description
272.5. Course of the Disease 28
2.6. Comorbidities 29
2.7. Disease Management 31
3. Anxiety Disorders Medical Overview 333.1. Etiology and Pathophysiology 33
3.2. Classification 33
3.3. Epidemiology 343.4. Disease Description 34
3.5. Disease Management 37
4. Treatment Methods 394.1. Pharmacotherapy 39
4.2. Tricyclic Antidepressant Agents (TCAs) 43
4.3. Monoamine Oxidase Inhibitors (MAOIs) 44
4.4. Selective Serotonin Reuptake Inhibitors (SSRIs) 45
4.5. Selective Serotonin and Noradrenalin Reuptake Inhibitors (SNRIs) 49
-
8/9/2019 TAP Depression Anxiety
4/72
-
8/9/2019 TAP Depression Anxiety
5/725
Depression and Anxiety
For internal use only
Dear reader,
After reading this overview you should become more familiar with the area of depressionand anxiety, its specifics and treatments available. You should also be able to makeinformed choices about the drugs to be included in you portfolio and choose the beststrategy possible to promote the antipsychotic drugs already chosen for your countrysportfolio. This pack provides you with the basic knowledge to make these decisions,however this area is so wide and fast changing that it should be closely followed at alltimes. Additionally, please do not forget that after gaining initial guidance and learningabout global trends, it is essential to investigate the situation in your market throughinterviews with doctors and reports on competitors activities. Also, do not forget to adaptthe strategy to your local situation, if necessary.
Enjoy the read.
-
8/9/2019 TAP Depression Anxiety
6/726
Depression and Anxiety
For internal use only
-
8/9/2019 TAP Depression Anxiety
7/72
-
8/9/2019 TAP Depression Anxiety
8/728
Depression and Anxiety
For internal use only
An overview worldwide vs. EuropeThe N6A antidepressants group has been experiencing slower growth in Europe than ithas globally in 2006. This is mostly due to the fact that the majority of the sales in theN6A group are generated in the US, which is a well developed market. Europe has beenslowly approaching the US development level in the past years. However we believe that
due to cultural reasons, it will never quite reach the level of development of the US, whereit is quite normal to be depressed and where its almost fashionable to have a shrink is that what we would wish for ourselves?
Source: PADDS
Figure 2: Comparison of N and N6A worldwide vs. European data
So what are the key growth drivers of the worldwideantidepressant market?
Growing number of people with mood disorders, mostly due toaging and changes in lifestyle,
N in USD N6A in USD
European DATA30.000 MIO
25.000 MIO
20.000 MIO
15.000 MIO
10.000 MIO
5.000 MIO
0 MIO
N Growth N6AGrowth N6A MS in N
2002 2003 2004 2005 2006
5.2 %7.1 %
18.1 %29.1 %
-2.7 % -3.7 %13.5 %23.6 %
22.1% 21.1%18.4%
20.3% 16.9%
N in USD N6A in USD
WW DATA
120.000 MIO
100.000 MIO
80.000 MIO
60.000 MIO
40.000 MIO
20.000 MIO
0 MIO
N Growth N6AGrowth N6A MS in N
2002 2003 2004 2005 2006
7.2 %5.5 %13.8 %
20.7 %
-3.6 % 3.6 %4.8 %15.9 %
26.3%
25.2%
21.2%
23.2%
20.5%
-
8/9/2019 TAP Depression Anxiety
9/729
Depression and Anxiety
For internal use only
Decrease in social stigma more people presenting increase indiagnosed and treated patients,
Increasing awareness of mood disorders (in general public andhealth professionals),
Shift of market towards GP level, Movement of products into non-traditional markets comorbidity
with various anxiety and non-anxiety disorders, Leading antidepressant therapies reaching blockbuster status
originators are among the major players present in the CNS seg-ment (Pfizer, GSK, Eli Lilly, Lundbeck),
Current blockbusters prolonging life-cycle through introduction of new formulations which have advantages over existing ones mostlywith regard to compliance (e.g. Effexor ER, Remeron SolTab),
Launch of new molecules with blockbuster potential (e.g.escitalopram, duloxetine);
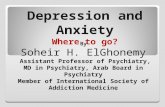
The situation is very different on CEE marketsThe N6A antidepressant group is fast growing and set to further expand in the coming
years. It is expected to become 3rd largest sub-group within CNS by 2010, after analgesicsand antipsychotics. The reasons why it is not expected to experience a boom as in thewestern markets are mostly area specific (lifestyle, stigma). However, the graph presentedbelow shows that there is still immense potential for growth in our markets.
Sources: PADDS, PhMIS, CEGEDIM, RMBC
Figure 3: N6A DDD per capita consumption in various markets
US
Canada
Germany
Spain
France
UK
Czech
Republic
Italy
Poland
Japan
Argentina
Brazil
Romania
Mexico
Russia
Philippines
45.00000
40.00000
35.00000
30.00000
25.00000
20.00000
15.00000
10.00000
5.00000
0.00000 2 0 0 2
2 0 0 3
2 0 0 4
2 0 0 5
2 0 0 6
2 0 0 2
2 0 0 3
2 0 0 4
2 0 0 5
2 0 0 6
2 0 0 2
2 0 0 3
2 0 0 4
2 0 0 5
2 0 0 6
2 0 0 2
2 0 0 3
2 0 0 4
2 0 0 5
2 0 0 6
2 0 0 2
2 0 0 3
2 0 0 4
2 0 0 5
2 0 0 6
2 0 0 2
2 0 0 3
2 0 0 4
2 0 0 5
2 0 0 6
2 0 0 2
2 0 0 3
2 0 0 4
2 0 0 5
2 0 0 6
2 0 0 2
2 0 0 3
2 0 0 4
2 0 0 5
2 0 0 6
2 0 0 2
2 0 0 3
2 0 0 4
2 0 0 5
2 0 0 6
2 0 0 2
2 0 0 3
2 0 0 4
2 0 0 5
2 0 0 6
2 0 0 2
2 0 0 3
2 0 0 4
2 0 0 5
2 0 0 6
2 0 0 2
2 0 0 3
2 0 0 4
2 0 0 5
2 0 0 6
2 0 0 2
2 0 0 3
2 0 0 4
2 0 0 5
2 0 0 6
2 0 0 2
2 0 0 3
2 0 0 4
2 0 0 5
2 0 0 6
2 0 0 2
2 0 0 3
2 0 0 4
2 0 0 5
2 0 0 6
2 0 0 2
2 0 0 3
2 0 0 4
2 0 0 5
2 0 0 6
N6A (DDD per capita)
DDD per capita
SSRI old new SNRI herbals
-
8/9/2019 TAP Depression Anxiety
10/7210
Depression and Anxiety
For internal use only
The current situation in our markets is as follows:
All markets are experiencing growth in units. Markets are largely underdeveloped and using old therapies (mar-
ket as other on the graph below). The two main reasons for this
situation are low presentation and treatment rates and low reim-bursement levels combined with high prices by originators. Marketsare expected to expand with the entry of lower priced generics.
Market expansion is expected due to changes in lifestyle ! it is theright time to enter the antidepressant markets in the CEE region.
High level of social stigma associated with depression and allmental illnesses people are associated or associate themselveswith going mad. Fortunately, this is slowly changing, but its along-lasting process.
Competition level is low to medium at the moment, but it is currentlychanging, as new players are continuously entering the antidepres-sants market. A very high competition level is expected in the future.
The generic market is forecasted to become dominated by a smallnumber of strong players, having wide portfolios.
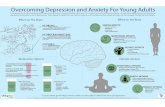
The following figure shows the forecasted evolution of CNS and within it a N6A marketin the CEE region.
Source: PADDS, authors estimation
Figure 4: Trends in ATC N in East Europe
S
ales (mio USD)
4.000
3.500
3.000
2.500
2.000
1.500
1.000
500
0
Trends in EE in ATC N
2002 2003 2004 2005 2006 2007 2008 2009 2010Year
Others NO7D NO6A NO5C NO5B NO5A NO4A NO3A NO2C NO2B NO2A
-
8/9/2019 TAP Depression Anxiety
11/72
-
8/9/2019 TAP Depression Anxiety
12/72
-
8/9/2019 TAP Depression Anxiety
13/72
-
8/9/2019 TAP Depression Anxiety
14/7214
Depression and Anxiety
For internal use only
correct treatment is the fact that the patients often discontinue their therapy when feelingbetter and do not continue it for the recommended duration of time. This in turn leads toa higher level of recurrence of depressive episodes.
All of above mentioned facts lead us to conclude, that the marketing approach is necessaryfor success in the antidepressants market.
GPs are main prescribers (in some countries specialists are stillmain prescribers) they dont often perform therapeutic sub-stitution, if patients are satisfied with current therapy, but aremore likely to carry out substitution within INN.
Pharmacists are more cautious when substituting antidepres-sants in comparison to certain other medicine.
Patients attach themselves to a drug; high placebo effect. Large unexploited market potential market will grow fur-
ther. Low recognition of depression among GPs, improper treat-ment of anxiety.
Possibility of co-promotion with other brands in other diseaseareas i.e. Bipolar Disorder.
DTC opportunity low awareness of disease. OTC cooperation possible Deprim, Persen.
1.2. Antidepressants Classes1.2.1. Classes of Antidepressants
As already mentioned in the medical part, antidepressants are divided into various classes(listed above), according to their mode of action. These classes have been introducedonto the market through time, each bringing certain advantages over the previous one
1996 RemeronWellbutrin SR2001 Remeron
SolTab
1953 1959 1987 1994 1996 2001 2002 2004
TCA MAOI SSRI SNRI Others
1983 Fevarin1987 Prozac1989 Cipramil1990 Zoloft
1991 Seroxat2002 Cipralex
1994 Effexor2004 Cymbalta
-
8/9/2019 TAP Depression Anxiety
15/72
-
8/9/2019 TAP Depression Anxiety
16/72
-
8/9/2019 TAP Depression Anxiety
17/7217
Depression and Anxiety
For internal use only
If we take a look at the classes of antidepressants from a different, most important, aspect the therapeutic one, we can further understand the current doctrine trends, the treatmentguidelines (see medical part, page 57), which in turn allow us to bring more weigheddecisions about our portfolio of drugs. (Various comparisons are summarized in the tablesabove.)
From the comparisons made above, we can deduce why SSRIs are drugs of first choicefor treatment of both depression and anxiety disorders. They cover the whole range of various indications associated with mood disorders and have various therapeutic benefitsover TCAs. TCAs are used as a second-line treatment, after poor treatment response orwhen intolerability to SSRIs adverse effects is observed in an individual patient. They areparticularly effective in treatment of severe and resistant depression, are cheap and wellknown by doctors, due to their long-term presence on the market and extensive clinicalexperience. SSRIs exhibit no therapeutic advantage over SNRIs, however due to the factthat SNRIs are new on the market and also have higher prices than SSRIs, they arepositioned as a second-line therapy. It is predicted that in the future they will establish
themselves as first-line therapy, as they gain wider range of indications and positiveclinical experience among psychiatrists. Antidepressants in the Other group are usuallyused as second-line therapy in specific cases, which best suit individual drug profilesfrom that group (e.g. mirtazapine sedation, bupropion less sexual dysfunction). MAOIsare positioned as third-line therapy in cases of non-responsive depression and areprescribed rather rarely.
1.3. Antidepressants INN Specific
In this part, we will focus on the ten leading antidepressants worldwide, which are:1. Venlafaxine* (Effexor/Effectin, Wyeth),2. Sertraline* (Zoloft, Pfizer),3. Paroxetine* (Seroxat/Paxil, GSK),4. Escitalopram (Cipralex/Lexapro, Lundbeck/Forest),5. Bupropion (Wellbutrin, GSK),6. Citalopram* (Cipramil/Celexa, Lundbeck/Forest),
7. Fluoxetine* (Prozac, Eli Lilly),8. Mirtazapine* (Remeron, Organon),9. Duloxetine (Cymbalta, Eli Lilly),10. Fluvoxamine* (Fevarin/Luvox, Solvay);
The molecules denoted with * are the ones that are available for you to include into yourlocal portfolio at present. They are presented in the order as they rank financially on theworldwide scale, as shown in the graph below.
-
8/9/2019 TAP Depression Anxiety
18/7218
Depression and Anxiety
For internal use only
4.500
4.000
3.500
3.000
2.500
2.000
1.500
1.000
500
0 2002 2003 2004 2005 2006
Venlaflaxine Sertraline EscilatopramBupropion Paroxetine DuloxetineFluoxetine CitalopramMirtazapine Fluvoxaminex
x
MIO USD
year
10 leading molecules within N6A (by sales in US $, WW)
x x x
x
x
x x x x x
Source: PADDS
Figure 5: 10 leading antidepressants worldwide by sales in US dollars
In Figure 5, we can clearly see how much patent expiry affects the sales of a certainproduct, even in this therapeutic area. Fluoxetine experienced the greatest decline insales, when it lost patent protection in 2001. However its successors have preparedbetter defence strategies against generic competition, which can be seen in lower decliningof sales of citalopram and paroxetine. Venlafaxine has taken a lead during 2005, as
SSRIs come under increased generic pressure. From this we can also forecast thatvenlafaxine will soon become the drug of 1st choice. Bupropion and mirtazapine arestruggling to keep up the sales through introduction of various line-extensions, but theywill never become the leading ones, which is also a consequence of the fact that they aresecond-line therapy. Duloxetine has only just been launched and first-signs of its forecastedsuccess can already be observed. However a true star is escitalopram, which managedto almost fully substitute citalopram and in a very short period of time become the 4thantidepressant worldwide. This was achieved only through a very well planned marketingstrategy from Lundbeck, where they have greatly expanded the market for both escitalopramand citalopram without extensive cannibalization.
If we take a look at the consumption of antidepressants expressed in kg per DDD, whichis shown in graph below, we can get a better overview of which antidepressants areactually most prescribed.
-
8/9/2019 TAP Depression Anxiety
19/7219
Depression and Anxiety
For internal use only
4.500
4.000
3.500
3.000
2.500
2.000
1.500
1.000
500
0 2002 2003 2004 2005 2006
Venlaflaxine Sertraline EscilatopramBupropion Paroxetine DuloxetineFluoxetine CitalopramMirtazapine Fluvoxaminex
x
MIO USD
year
10 leading molecules within N6A (by No DDD WW)
x x xx
xx x x x
x
Source: PADDS
Figure 6: 10 leading antidepressants worldwide by DDD consumption worldwide
We can see that the most prescribed antidepressants are SSRIs, which is in line with ourexpectations, as they are defined as first-line therapy by the guidelines. We can alsoconclude that patent expiry does not actually affect the consumption of certain moleculesvery much (see fluoxetine in the above graph), which can also be expected, as afterpatent expiry the product becomes even more widely available on the market. The order
of the molecules is entirely in line with the prescribing guidelines, which is a good indicationof prescribing habits of doctors being in line with the guidelines. With our portfolio, wewill cover five out of the first six leading molecules, which are by consumption largelyahead of the remaining ones. All of these molecules are keeping their positions, which ispositive information for us patients are continuing to take these drugs and the prescriptionsare continuously generated.
Why is the order of the molecules such and why are some experiencing high financialgrowth while others stay on the same level? These answers can be attained from the datain the following table, where in-depth analysis of the 10 molecules is given.
-
8/9/2019 TAP Depression Anxiety
20/7220
Depression and Anxiety
For internal use only
1.4. Comparison of 10 Leading Antidepressants
INN
1. Originator global
product name
launch yearline-extensions
importance ofproduct in orig.portfoliosales mioUSD/growth 2006expected sales1 IMSDatamonitor
2. INN globalSales INN mioUSD/growth (2006)Position INN/MSINN
3. Dosage forms2 present worldwide
4. DDD (WHO ATC/DDD Index 2006)
5. Patent status3USA/EU15CEE markets
6. Genericspresent inCEE/SEE/CIS
7. Indications4
8. Contraindications5
CitalopramSSRI
Lundbeck/
ForestCipramil,Celexa1989Escitalopram
No. 2/19%
385 m$/ 32%7 m$ (2010)
73 m$ (2010)
786 m$/ 19%
No. 8/4%
FCT 10mg,20mg, 25mg,30mg, 40mg,60mg; oraldrops, oralliquid,ampoules
20 mg
ex.04/ex.02expired
Torrex,Biovena,Ratiopharm,Zentiva,Lannacher,Desitin,Alpharma,Pliva, Merck
- Depression- PD*
- Concurrentuse of MAOI- Hyper-sensitivity tocitalopramproducts
SertralineSSRI
Pfizer
Zoloft
1990
No. 3/7%
2845 m$ / 21%772 m$ (2009)
287 m$ (2010)
3,864 m$ / 11%
No. 2/18%
FCT 25mg,50mg, 100mg;TABS 10mg,25mg, 50mg,75mg, 100mg;oral liquid, oraldrops,suspension
50 mg
ex.06/ex.05expired
Egis, Irex Labs,Krka, Pliva,Ranbaxy,Ratiopharm,VeropharmZAO, Winthrop,Dr. Reddy
- Depression- OCD- PD- PTSD- Social phobia- PMDD
- Concurrentuse of MAOI- Concurrentuse ofpimozide
ParoxetineSSRI
GSK
Seroxat, Paxil
1991Paxil CR
No. 4/5%
1136 m$/ 7%626 m$ (2009)
153 m$ (2010)
2,045 m$/ 9%
No. 5/11%
FCT 10mg,20mg, 30mg,40mg; FCTRETARD (CRform) 12,5mg, 25mg,37,5mg; oralliquid, oraldrops,suspension
20 mg
ex.03 / ex.01expired
Apotex, A/SGea, Duiven,GedeonRichter,Keripharma,Merck, Pliva,Ratiopharm
Depression- GAD- OCD- PD- PTSD- Social phobia- PMDD
- Concurrentuse of MAOI- Concurrentuse ofpimozide- Concurrentuse ofthioridazine- Hyper-sensitivity toparoxetine
FluoxetineSSRI
Eli Lilly
Prozac
1987Prozac ODT,Prozac WeeklyNo. 7/4%
339 m$/ 20%419 m$ (2009)
42 m$ (2010)
865 m$/ 14%
No. 7/5%
CAPS 10mg,20mg, 40mg,60mg, 90mg;ODT 10mg,20mg;RETARDCAPS (weeklyfrom) 90mg;oral liquid, oraldrops, syrup,suspension
20 mg
ex.01/ex.00expired
Apotex,GedeonRichter,Grindex, Krka,Pliva, Ranbaxy,Ratiopharm,Teva, Zentiva,and manyothers
- Depression- OCD- PD- PMDD(Sarafem )- Bulimianervosa- PTSD*- Bodydysmorphicdisorder- Fibromyalgia- Rynaudsphenomenon
- Concurrentuse of MAOI- Concurrentuse ofthioridazine- Hyper-sensitivity tofluoxetine
MirtazapineNaSSA
Organon/
Akzo NobelRemeron,Zispin1996RemeronSolTab (ODT)No. 1/18%
308 m$/ 13%220 m$(2010)
583 m$/ 9%
No. 9/3%
FCT 7,5mg,15mg, 30mg,45mg; ODT 7,5mg,15mg, 30mg,45mg, oralliquid,ampoules
30 mg
ex.03/ex.04expired
Krka
-Depression
- Concurrentuse of MAOI- Hyper-sensitivity tomirtazapine
VenlafaxineSNRI
Wyeth
Effexor
1994Effexor ER
No. 1/26%
3,931 m$/+3%2,130 m$(2009)2,353 m$(2010)
4,109 m$/+6%
No. 1/22%
TABS 25mg,37,5mg, 50mg,75mg, 100mg,150mg; CAPSRETARD (ERform) 37,5mg, 75mg,150mg
100 mg
2008/20082008??
Pliva
- Depression- GAD- Social phobia
- Concurrentuse of MAOI- Hyper-sensitivity tovenlafaxine
EscitalopramSSRI
Lundbeck/
ForestCipralex,Lexapro2002
No. 1/54%
2,868 m$/+18%2,500 m$(2009)3,487 m$(2010)
2,998 m$/+20%
No. 3/16%
FCT 5mg,10mg, 15mg,20mg; oralliquid, oraldrops
10 mg
2009/20142007??
- Depression- GAD- Mixed anxietyand depressivedisorder*
- Concurrentuse of MAOI- Hyper-sensitivity toescitalopram orcitalopramproducts
DuloxetineSNRI
Eli Lilly
Cymbalta
2004
No. >10
1,327 m$/+95%3,800 m$(2010)
1,365 m$/+99%
No. 6/7%
CAPS 20mg,30mg, 40mg,60mg
60 mg
2009/20142014??
- Majordepressivedisorder- Diabeticneuropathy- Pain- Urinaryincontinence*
- Concurrentuse of MAOI- Hyper-sensitivity toany ingredientof product- Uncon-trollednarrow-angleglaucoma
BupropionNDRI
GSK
Wellbutrin
1985Wellbutrin SR,Wellbutrin XRNo. 6/4%
1,932 m$/+23%2,210 m$(2010)807 m$ (2010)
2,507 m$/+16%
No. 4/13%
TABS 5mg,75mg, 100mg,150mg; FCTRETARD 100mg, 150mg,200mg, 300mg;CAPS 250mg,ampoules,syrup
300 mg
ex.94/ex.89expired
- Depression- Smokingcessationassistance(Zyban )
- Seizuredisorders- Patientsundergoingabruptdiscontinuationof alcohol orsedatives (incl.benzodiaz-epines)- Prior orcurrentdiagnosis ofbulimia oranorexia- Con-comitantMAOI- Hyper-
sensitivity tobupropionproducts
FluvoxamineSSRI
Solvay
Fevarin,Luvox1983
No. >10
43 m$/ 11%70 m$(2007)
260 m$/ 1%
No. 10/1%
FCT 25mg,50mg, 100mg
100 mg
ex. 97/ex. 96expired
- OCD- Depression*- PD*- Social phobia*
- Co-administrationof alosetron,astemizole,cisapride,pimozide,terfenadine,thioridazine,or tizanidine-Hyper-sensitivity tofluvoxaminemaleate
Source: IMS Knowledge Link, IMS Life Cycle, PADDS, Newport Horizon, Datamonitor
-
8/9/2019 TAP Depression Anxiety
21/7221
Depression and Anxiety
For internal use only
BupropionNDRI
- In Europe stillnot used asanti-depressant(with a fewexceptioncountries)- Anti-depressant infocus for GSK,as paroxetinelosing patentprotection- XLformulationsupposed tohaveadvantages inless weightgain and lesssex. disf.
Reconnectingwith life.
- Proven first-line efficacy indepression withlong-termprevention ofrelapse/recurrence, lowrisk of sexualdysfunction, lowrisk of weightgain, proventolerabilityprofile, simpletitration anddosing flexibility.- ConsiderWellbutrin SRfor your patientsconcernedaboutdepression-related fatigueor low energy,sexual function,weight gain.
www.wellbutrin-xl.com
DuloxetineSNRI
- Newest SNRI a futureblockbuster- Lilly focusingon treating thephysicalsymptoms pain indepression- Also focusingon area ofneuropathicpain.
The relief youneed.
www.cymbalta.com
EscitalopramSSRI
- Supposed tobe supraSSRI- Highlyselective,supposed to beeven moreselective thancitalopram withless sideeffects due tolower doses- Studies tryingto show that ithas a fasteronset of action- Lack ofclinicalexperience incomparison toother SSRIs.
Power to enjoylife.
- One effectivetherapy fordepression andanxiety- Improvedquality andenjoyment of lifein adults sufferingfrom depressionand GAD.- Unique mode ofACTION has aunique mode ofaction by which itpotentiates itsown binding tothe Serotonintransporter- A super-selective SRI super selectiveand efficientbinding to theserotonintransporterresults in higherextra-cellularserotoninconcentrations-Escitalopramspre-clinicalbenefits arereflected by afaster and betterefficacy thanobserved forcitalopram
www.lexapro.com,www.cipralex.com
1 Expected sales differences between IMS and Datamonitor forecasts, show that this market is verydifficult to predict;
2 FCT film coated tablets, TABS tablets, CR controlled release form, ODT oral disintegratingtablet, ER extended release, CAPS capsules, SR sustained release, XR extended release;
3 Patent status taken from IMS Knowledge link and Newport Horizon many patents unclear. For exactpatent status please check your local situation.
4 Indications and Contraindications source: Physicians Desk Reference;5 Indications listed are FDA labeled indications. The ones denoted with * are Non-FDA labeled indications.
FluvoxamineSSRI
- First SSRI.
VenlafaxineSNRI
- The mainSNRI- Dualmechanism ofaction actson bothserotonin andnoradrenalinreceptors dueto supposedlyhaving higherefficacy inhigher numberof patients- Leadingantidepressantworldwidefinancially - Believed tobecome first-line therapy infuture- Highlyeffective indepressiontreatment
Anantidepressantwith a dualmechanism ofaction it actson bothserotonin andnoradrenalinreceptors.Second-linetherapy intreatment ofbothdepression andanxiety.
The changeyou deserve.
www.effexorxr.com
MirtazapineNaSSA
- 2nd linetherapy- Causes lesssex. disf.- Has astrongersedative effectthan the otherantidepres-sants- ODT formsupposedly hasa faster onsetof action- Weight gain
Specific modeof action(serotonin andnoradrenalinreceptors).Especiallysuitable forpatients whodesire a normalsexual life. Dueto sedativeeffect it is mostsuitable fordepressivepatients withsleepdifficulties.
Simply rewardsyour confidence.(SolTab)
- It begins tohelp quickly- It enhancespatientconvenienceand compliance- It providesfast andsustained reliefyour patientsare looking for- Is suitable forall your patients- May be takenwith or withoutwater.- Dissolves onthe tongue inless than 30sec.- Has a pleasantorange-flavoured taste- Simple once-a-day eveningdose of 30mg- It will improveyour success inmanagingdepression- The worldsfirst and onlyfast dissolvingantidepressant
www.remeron.com
FluoxetineSSRI
- Gold standardin depressiontreatment- Prozac asynonym foranti-depressant- Indication forchildren under18 - PMDDindication
The goldstandard intreatment ofdepression.Many years ofpositive clinicalexperience.The only SSRIwith indicationfor treatment ofdepression inchildren under18 years. Alsoused astreatment forbulimicpatients.
- Most widelyprescribed anti-depressant inhistory.- Gives doctorsand patients asafe andeffective choicefor treatment ofdepression,OCD, bulimiaand PD.
www.prozac.com
ParoxetineSSRI
- Largestnumber ofregisteredanxietyindications- Largestnumber ofoverdosereports- Largestnumber ofreportedwithdrawalsymptoms
The SSRI withthe largestnumber ofregisteredindications.First linetherapy forbothdepression andanxieties.
www.paxil.com
SertralineSSRI
- Wide off-labeluse- 1st linetherapy choicein US Pfizersmarketingstrength
Anantidepres-sant withlargestnumber ofprescriptionsin the world.First-linetherapy for allpatients withdepressionand/or anyform ofanxiety. Itcan also beused forchildren intreatment ofOCD.
#1 prescribedbrand of itskind.
- No. 1 formillions ofreasons.Its the #1doctor-prescribedbrand fordepression andanxiety.- It has treatedmore peoplewith moretypes ofdepression andanxiety thanany brand of itskind.- It has treatedmillions ofpeople for over12 years.- Doctors havewritten over250 millionprescriptionsfor Zoloft.
www.zoloft.com
CitalopramSSRI
- Most selectiveSSRI- Especiallysuitable forelderly- Less sex. disf.and weight gain- More rapidonset of action- Lundbeck didnot developcitalopram verywell in this area poorpresence
Highly potentSSRI, safe interms of sideeffects and withfewerinteractionsthan oldertherapies andother SSRIsdue to its highselectivity. 1stchoice therapyin treatment ofdepression anditscomorbidities.Especiallysuitable forolder patientsand for thepoly-morbidpatients
Helps patientssuffering fromdepression.
- One of worldsmostprescribedSSRIs for thetreatment ofdepression,OCD andanxietydisorders.
www.celexa.comwww.cipramil.com
INN
9. Importantfeatures
10. Positioning proposals for ourproducts
11. Originatorslogan
12. Originator keymessages
13. Web pages
-
8/9/2019 TAP Depression Anxiety
22/7222
Depression and Anxiety
For internal use only
1.5. Our Portfolio of AntidepressantsThe molecules that are currently available for you to include into your portfolio are:
Citalopram (Citalon) reg. file available for FCT, Sertraline (Sertiva) reg. file available for FCT, Paroxetine (Paluxon) reg. file available for FCT, Mirtazapine (Mirzalux) reg. file available for FCT and ODT forms, Venlafaxine (Efexiva) reg. file available for TABS and for XR
CAPS6;Please note that some of these molecules are currently available from both Sandoz andHexal sources. If you have the opportunity to choose, you should first be guided by TTM(time to market). If this is the same for both, then please make sure to check the SmPC andchoose the product with a wider array of indications in registration documentation. The
availability of strengths is also greatly important. It should be decided in each individualcase, should it come to that, whether a wider availability of strengths or a greater arrayof indications is more important and the decision made based on that. If you choose tolaunch a branded product, please check the local situation regarding the registration of the chosen trade mark. The ones listed above are trademarks proposed by Sandoz forthe corresponding molecules.
The existing portfolio might consist of some of the following molecules: Fluoxetine (Portal) CAPS, DISP TABS, oral solution, Fluvoxamine FCT,
Amitriptyline (Amyzol) FCT and MR TABS, Moclobemide FCT, Maprotiline FCT, sol. for inj., Mianserin FCT,
You might have the majority of these products already present in your portfolio or perhapsnone. The decision whether to include additional products from this group into your futureportfolio should be made based on the local situation.
With the available molecules, all the different classes of antidepressants are covered:
TCA MAOI SSRI SNRI OtherAmitriptyline Moclobemide Citalopram Venlafaxine MirtazapineMaprotiline SertralineMianserin Paroxetine
Fluoxetine
Fluvoxamin e6XR CAPS Extended Release CapsulesODT Orally Dispersible TabletDISP TABS Dispersible TabletsMR TABS Modified Release Tablets
The existing portfolio consists mostly of older antidepressants from TCA, MAOI and theearly SSRIs. However, the future portfolio is based on the newer molecules, which arealso therapeutically drugs of first choice.
-
8/9/2019 TAP Depression Anxiety
23/7223
Depression and Anxiety
For internal use only
1.5.1. Portfolio Assessment
When evaluating molecules and deciding how to structure the portfolio, we suggest youto take the following criteria into account:
The global medico-marketing potential of the molecule.
Local treatment guidelines, local prescribing situation (who is al-lowed to prescribe specific INN/class, who starts the therapy),prescription habits of doctors, etc.
Try to predict the development of the molecule on your market willit follow the global trend? Try to predict the level of competition(high medium low), identify the major competitors expected/present (also analyze their portfolios and the importance of CNSgroup), try to predict which generic will enter first (if none arepresent yet) and try to evaluate the possibility of us being the firstgeneric (look at other markets for predicting the competition).
Reimbursement status, pricing of the product and connection withthe reimbursement levels, comparison with other products in thesame class (do not forget about a class effect of antidepressants).
Transfer price and profitability of the product.There are many new products expected to arrive in a rather short time period, andtherefore we advise you differentiate among them in order to achieve the highest result.It is suggested that you prioritize among products and determine the type of promotionfor each product, based on the local market situation and considering the following:
Product assessment, potential, the other products/portfolio; Market local characteristics, development in terms of therapy (i.e.
how much is depression treated, overall market development) andin terms of doctrine (i.e. which classes are used the most, level of development of modern therapies);
Sales team size, organization; Company strategy;
1.5.2. Which Strategies Can be Employed?
In most of the markets we already have certain products in the antidepressant portfolio.However, in the majority of the countries they have not been promoted in the past few
years. In those cases, when launching new antidepressants, we are in the same situationas if opening a completely new group of drugs.
When entering the CNS group, it is highly advisable to start with Sanval (zolpidem,hypnotic), as that is the product which relies mostly on prescriptions by GPs, and is agood introduction into CNS group. Through Sanval we can start to slowly build therelationship with Psychiatrists (PSY) and Neurologists (NEU), without having to rely ontheir prescriptions heavily.
Antidepressants are the next CNS sub-group advisable to enter. Here the main prescribersare GPs in the majority of the markets, however the PSY also play a very important role
-
8/9/2019 TAP Depression Anxiety
24/7224
Depression and Anxiety
For internal use only
and should not be left out. It is actually the case that in some markets, the majority of antidepressant prescriptions come from PSY (sometimes due to restrictions in prescribing),however that is expected to change with time, as the market shifts to GPs.
The first products to be launched will be citalopram, sertraline, paroxetine all SSRIs(selection of products and the launch order varies among markets). Depending on thetype of market and the market situation, the following strategies can be employed:Offensive strategy tailored to the development stage of each individual market. (Thesemarkets can be identified from Figure 3.)
Antidepressants market expansionIn the case of an underdeveloped market of antidepressants, we must try to build themarket by educating doctors and patients about the problem of depression and the needfor its pharmacological treatment with modern new drugs, which have numerousadvantages. Later we can spread the problem by adding anxiety disorders and expanding
the market into that segment as well. By offering SSRIs, which are first-line treatment forboth conditions, we can ideally cover both segments. The examples of this type of marketare Bulgaria, Romania, Russia, and CIS.
Building the market of SSRIs, attacking old therapies (mostly TCAs)In the event that the antidepressant market is rather well developed but the consumptionof TCAs is still extremely high, we should stress the advantages of SSRIs over TCAs. Ourstrategy should be to widen the SSRI segment, mainly the promoted SSRI (i.e. citalopram).We have a great advantage over all TCA drugs, since SSRIs are the first-line treatment forboth depression and anxiety, and we can hence ideally cover both segments with one
drug. This is a great advantage for doctors, as very often these two conditions areinterrelated. This, together with other advantages (i.e. improved adverse-effect profile)should be continuously stressed in all our messages. The examples of this type of marketare Poland and Latvia.
Stressing the advantages of certain SSRI (e.g. citalopram) over allother currently available SSRIs
In the event that the market is well developed and the use of SSRI drugs is at the expectedlevel, we should stress the advantages that a certain SSRI (e.g. citalopram most selectiveSSRI, especially suitable for elderly) has over all other currently available SSRIs. This waywe should aim at increasing the usage of that particular SSRI. At the same time we shouldlook for and expose the advantages that we have over other available products with thesame INN if we can find them.
When we enter the market, it will be in one of the above stages. We should apply thestrategy that is appropriate for that market at that time, but it is also possible that a mix of strategies will be required, if the market fits more than one stage description.
Considering the fact that there are many new products and that portfolio of antidepressantswill be wide, we should utilize the advantages that a wide portfolio offers. High competitionis expected in the antidepressants market, however not all players will have such wide
portfolios. This will certainly be one of our advantages, together with the fact that we willoffer CNS drugs from other segments, besides antidepressants. The advantage of havinga wide portfolio should definitely be utilized in the sales segment approach to wholesalers
-
8/9/2019 TAP Depression Anxiety
25/7225
Depression and Anxiety
For internal use only
and pharmacists, however portfolio can also be promoted to doctors. Possible approachesto portfolio promotion are the following:
1. Building a wide portfolio and maximization of the potential of eachmolecule through offering multiple molecules from the same antide-pressant class. In this case a microtargeting approach should beemployed. A highly skilled and educated sales force with thoroughknowledge of the customers and habits is needed in order for thisapproach to be successful. Through this approach the doctor canprescribe the best suited drug, from Sandozs portfolio, to theirpatient.
2. Focus on one main molecule in each class (choose according toportfolio assessment criteria), while other molecules in the class aretreated as supported products. They can be positioned in specificindications (if possible) or be offered as an alternative to the mainpromoted product, but they are mainly supported through activitiesat the pharmacy and wholesaler level. In this way, we cannot fullyexploit the advantage of a wide portfolio.
3. Promote just one molecule from each class, with no activities onother products from that class.
You should choose one of these approaches according to your local market situation.When bringing this decision, the specifics of the antidepressant market, which areexplained earlier in this overview, should be taken into account. You should particularlykeep in mind the fact that in the majority of the markets, pharmacists are rather reluctantto substitute generics in this filed; this is often a long-term treatment, patients for various
reasons develop a high affinity for their particular drug and even in rather developedmarkets there is a large unexploited market potential. Keeping all of those things in mind,we are certain that you will make the best decision for your market, which will lead to themost success with the antidepressant portfolio.
-
8/9/2019 TAP Depression Anxiety
26/7226
Depression and Anxiety
For internal use only
2. Depressive Disorders A Medical Overview 2.1. Etiology and Pathophysiology
The etiology of depression is unknown. Today it is believed that there are environmental stressors that trigger depression ingenetically susceptible people.
Serious risk factors for depression include: Family history. Serious negative events. Illness.
Positive family history is the strongest risk factor for depression. Serious negativeevents (such as the death of a loved one or a divorce) may trigger depression inpeople who are susceptible to the disorder because of their genetic background or becauseof other risk factors. Most initial episodes of depression are preceded and probablyprovoked by a negative event. Chronic illness is another significant risk factorassociated with depression. Some disorders, such as Alzheimers disease, Parkinsonsdisease, and ischemic stroke, are thought to induce depression through their effect onneurochemistry and/or direct damage to the brain.
PathophysiologyLooking back to the history of antidepressant medication, researchers in the 1960shypothesized that low concentrations of monoamine neurotransmitters (serotonin,noradrenalin, and dopamine) caused depression.
The scientific clarification of abnormal chemical processes in the brain of patients withdepression is known as the monoamine hypothesis. The monoamines have provedeffective targets for antidepressant therapies.
2.2. ClassificationAmerican Psychiatric Association (APA) has developed a precise classification system forpsychiatric diseases, known as the Diagnostic and Statistical Manual of MentalDisorders, Fourth Edition (DSM-IV). The DSM-IV classification is used worldwide and istherefore also referred to in this TAP.
Depressive disorders include:
Major depression, single episode. Major depression, recurrent.
Dysthymic disorder. Depressive disorders not otherwise specified.
-
8/9/2019 TAP Depression Anxiety
27/7227
Depression and Anxiety
For internal use only
2.3. Epidemiology The percentage of the general population aged 15 or older who have at least one of these conditions ranges from9% to 19%.Women experience depression about twice as often as men.
Prevalence of major depression: 5% to 12%.Prevalence of dysthymia: 2% to 4%.Prevalence of other depressive conditions: 6% to 24%.One in 5 individuals suffers from a mood disorder during his or her lifetime.
2.4. Disease DescriptionMajor Depression
The typical symptoms of depression are divided in two groups:emotional and physicalsymptoms. They are listed in the table below.
Spectrum of Symptoms in Depression
Emotional Symptoms Physical SymptomsSadness, tearfulness Tiredness, fatigueLoss of interest Sleep disturbancesAnxiety/irritability HeadachesHopelessness Psychomotor agitation/retardation
Concentration difficulties GI disturbancesGuilt Appetite changesSuicidal ideation Body aches and pain
The physical symptoms of depression are often less appreciated, even though thesesymptoms may dominate the clinical picture. In primary care settings, the physical symptomsmay be the chief complaint of depressed patients.
The DSM-IV classifies major depression as a mood disorder that manifests either as asingle episode or as recurrent episodes. Five or more of the following symptoms must bepresent during the same two-week period and must represent a change from previous
functioning (at least one of the symptoms must be either depressed mood or loss of interest or pleasure).DSM-IV criteria for Major Depression:
Depressed mood most of the day, nearly every day. Markedly diminished interest or pleasure in all, or almost all, activities most of the day, nearly every day. Significant weight loss or gain when not dieting, or decreased or increased appetite nearly every day. Insomnia or hypersomnia nearly every day. Psychomotor agitation or retardation nearly every day (observable by others). Fatigue or loss of energy nearly every day. Feelings of worthlessness or excessive or inappropriate guilt (which may be delusional) nearly every day. Diminished ability to think or concentrate, or indecisiveness, nearly every day. Recurrent thoughts of death (not just fear of dying), recurrent suicidal ideation without a specific plan, and a specific
plan for committing suicide, or a suicide attempt.
-
8/9/2019 TAP Depression Anxiety
28/7228
Depression and Anxiety
For internal use only
Dysthymia
Dysthymia is defined as achronic mood disorder characterized by a depressed feelingthat occurs for most of the day, on most days, for at least two years. Two or more of thefollowing symptoms have to be present: poor appetite or overeating, insomnia orhypersomnia, low energy or fatigue, low self-esteem, poor concentration or difficultymaking decisions, feeling of hopelessness.Dysthymia is distinguished from major depression bythe number of symptoms, theirseverity, and the chronic course of the illness. Dysthymic symptoms usually last for
years, while major depressive episodes are typically measured in weeks or months.
Other Depressive Disorders
In addition to major depression and dysthymia, several other categories of depressivedisorders are defined in the DSM-IV system. They includeminor depression, brief
recurrent depression, and a miscellaneous category referred to as sub-thresholddepressions. These disorders share symptoms with major depression and dysthymia.
2.5. Course of the DiseaseA depressive episode may begin either suddenly or gradually. The duration of an untreatedepisode may range from a few weeks to months or even years, although most depressiveepisodes clear spontaneously within approximately 6 months. The prognosis for everysingle depressive episode is quite good, particularly in the view of the efficacy of the
available antidepressant medications.Many, if not most, people who suffer from one episode of depression will suffer a recurrenceat some point in their lives.
REMISSION: A complete or partial disappearance of the signs and symptoms of disease in response to treatment.RELAPSE: Reappearance of symptoms within one year of treatment initiation.RECURRENCE: Reappearance of symptoms after one year of treatment initiation.
The best predictor ofrelapse or recurrence is the level of recovery between two consecutiveepisodes.
Even with continuation therapy,only 3050% of patients reach full remission on agiven drug. Patients who do not achieve full remission those who experience residualsymptoms (i.e., persistent sub-threshold symptoms) following partial recovery have beenfound to experience a recurrence three times faster and relapse five times faster thanasymptomatic patients.
Approximately 3035% of all cases of depression are considered chronic, meaningthat symptoms persist (to varying degrees of severity) for two years or more.
Suicide is the most serious complication of depression. Approximately 10% to 15% of all
patients hospitalized with depression will eventually take their own lives. Suicidal riskshould always be carefully evaluated in any patient with depression.
-
8/9/2019 TAP Depression Anxiety
29/7229
Depression and Anxiety
For internal use only
2.6. Comorbidities2.6.1.Comorbidity of Depression with Anxiety
Disorders
Comorbidity (i.e. the presence of more than one psychiatric disorder or somatic illness) isa well-recognized aspect of major depression that has important implications for treatment,quality of life, and prognosis.
75% of people with a depressive episode have at least one other psychiatric disorder in their lifetimes.
On a lifetime basis, sssssome 4060% of people with major depression also have ananxiety disorder. Anxiety disorders tend to precede the first episode of depression.
The figure below shows some of the symptoms common to major depression and anxiety.
Common psychiatric conditions that are co-morbid with MDD
Source: Authors analysis Business Insight Ltd.
Panic DisorderObsessiveComplusiveDisorder
GeneralizedAnxietyDisorder (GAD)
AgoraphobiaPremenstrual
DysphoricDisorder (PMDD)Depression
Social AnxientyDisorder (SAD)
Attention DeficitHyperactivity
Disorder (ADHD)Post Traumatic
StressDisorder (PTSD) Bulimia Nervosa
Source: Authors estimates, Business Insights Business Insight Ltd.
MDD and anxiety disorders patient population, 2003
49.4%of MDDpatients
50.6%of MDDpatients
36.8%of anxietypatients
63.2%of anxietypatients
Depression Comorbid Anxiety
-
8/9/2019 TAP Depression Anxiety
30/7230
Depression and Anxiety
For internal use only
Source: Decision Resources, Inc.
Symptomps Common to Major Depression and Anxiety
Major Depression
AnxietyWeight lossDepressed moodSusidical ideationInappropriate guiltDimnished pleasure
FearFatigue
InsomniaAgitation
Chronic painApprehension
AgoraphobiaPanic attacs
Muscle tensionExcessive worry
Fear of social sitations
Two competitive variables in the market are those of cost of the treatment and efficacy of treating comorbidities. Comorbidities associated with major depression representanimportant target for drug makers, facilitating prescription growth and lifecycle extensionfor existing treatments.
2.6.2.Comorbidity of Depression with PhysicalIllnesses
Depression is more common in patients with physical illness than in those without, but isvery hard to diagnose.
The rate of comorbid depression and medical illness varies from10 to 40%.
Although data are limited, the available evidence suggests that depression concomitantwith medical illness can be treated. SSRIs have demonstrated potential usefulness indepressed patients with medical illnesses.
Cardiovascular Disorders
Major depression is a common problem in patients with coronary heart disease and isassociated with an increased risk for cardiac morbidity and mortality. Treatment of depression in cardiac patients is complicated by concerns regarding effects of medicationson heart rhythm, blood pressure and other cardiovascular functions.
Diabetes MellitusThe presence of depression may be associated with deterioration in glucose utilization.Patients exhibit insulin resistance and decreased glucose tolerance.
Neurology Depression is a common, but often unrecognized complication occurring aftercerebrovascular accident or stroke, or along with epilepsy, Parkinsons disease, Alzheimersdisease or multiple sclerosis.
-
8/9/2019 TAP Depression Anxiety
31/7231
Depression and Anxiety
For internal use only
Cancer
Patients with major depression were found to improve with treatment after usingantidepressants.
Patients with depression in each of these conditions should be treated we must not assume that they ought to be de-
pressed. The symptoms of both depression and comorbid disorder should improve.
2.7. Disease Management
Depression is under diagnosed and undertreated largely owing to the social stigma historically associated with psychiatricillnesses.
Awareness of depression has been increased in recent years all over the world.Consequently, much of the social stigma associated with depression has been eliminated.More and more people are presenting their problems to their doctors and the diagnosisof depression is improving.
2.7.1.Who Treats Depression?
When patients do present, 90% are first seen by a general practitioner (GP). Many of these physicians are inadequately trained in the diagnosis of depression. In mostcountries, no more than 1015% of diagnosed patients are referred for psychiatrist and usually, only after their GP has attempted to treat them, but with no success.
Patients, whose depression is associated with an underlying chronic illness, are usuallytreated for depression by the specialist, who is treating the basic disease.
Studies in primary care settings have found that approximately 50% of the patients who meet criteria for major depressionare recognized; half of those (25%) receive antidepressant treatment; but fewer than half of those (12%) receive adequatedoses and duration of therapy. Major depression is under diagnosed; and even when diagnosed, depression is often nottreated correctly.
Another significant problem ispatient compliance. They often stop taking theantidepressant soon after the beginning of treatment. The primary reason forearly discontinuation is intolerance of the medications side effects; for patients who stay onmedication, side effects are a major reason for skipped doses. Other common reasonsfor discontinuation within the first few months of therapy include patients belief that theydo not need the medication (usually because they start to feel better) or that the medicationis not working.
Reducing the dose or discontinuing treatment early significantly increases the risk of a return of depressive symptoms.
-
8/9/2019 TAP Depression Anxiety
32/7232
Depression and Anxiety
For internal use only
Source: Decision Resources, Inc.
Recommended Time for Continuation and Maintenance Therapy in PatientsWith Chronic Depression
Greatest risk of relapse
Risk of recurrence
Acute612 weeks
Continuation49 months
Maintenance1 or more years
High
Low
Magnitude of treatment response,
riskof relapse/recurrence
2.7.2.Pharmacotherapy of Depressive Disorders
Main therapeutic approaches: Pharmacotherapy. Non-pharmacological measures (psychotherapy, electroconvulsive therapy ECT).
Definition of Adequate Antidepressant Drug Therapy
In the last decade several national guidelines for the treatment of major depression havebeen published that define an adequate dose and duration of drug therapy.
Nowadays depression is treated to the point of remission of symptoms, not justto the point of reduction of severity of symptoms.
Key Recommendations in Antidepressant Treatment: Antidepressants take several weeks of continuous use before symptoms improve. Taking them on an as-needed
basis is of no benefit. Antidepressants must usually be taken for 6 to 12 months. Stopping treatment as soon as the symptoms improve
greatly increases the risk of symptoms returning. Antidepressants have specific effects on the bodys chemicals to improve depressive symptoms. Depression is a
medical illness, not a character flaw or weakness. Antidepressants are not addictive, are not stimulants or uppers, and do not cause physical dependence. Common adverse effects should be mentioned, along with specific instructions about what to do if an adverse effect
occurs.
-
8/9/2019 TAP Depression Anxiety
33/7233
Depression and Anxiety
For internal use only
3. Anxiety Disorders Medical Overview
Physicians must recognize the difference between pathological anxiety and anxiety as anormal or adaptive response.
Anxiety disorders are: Common. Chronic. The cause of considerable distress and disability. Often unrecognized and untreated.
3.1. Etiology and Pathophysiology The biology of panic disorder is being intensively studied. Among the biologicaldisturbances possibly underlying panic are increased catecholamine levels in the centralnervous system, an abnormality in the locus ceruleans (an area in the brainstem), andabnormalities of the gamma-aminobutyric acid (GABA) neurotransmitter system.
Phobic disorders tend to run in families.
Research has shown that serotonergic pathways may play a role insocial phobia orsocial anxiety disorder.
Over the years, obsessive-compulsive disorder has been explained in genetic,psychodynamic, behavioural, and neurobiological terms.
The cause ofgeneralized anxiety disorder is unknown. One family study showed thatnearly 25% of the first degree relatives of these patients are affected with this disordertoo. Several different neurotransmitter systems have been implicated in the disorder,including the noradrenergic, GABA, and serotonergic systems in the frontal lobe andlimbic system.
The major etiological event leading toposttraumatic stress disorder is a stressor. Bydefinition, a stressor must be severe enough to be outside the range of normal humanexperience.
3.2. ClassificationAccording to theDSM-IV system, anxiety disorders are the following:
Panic disorder with or without agoraphobia. Social anxiety disorder (social phobia). Obsessive-compulsive disorder.
-
8/9/2019 TAP Depression Anxiety
34/7234
Depression and Anxiety
For internal use only
Generalized anxiety disorder. Posttraumatic stress disorder. Acute stress disorder. Anxiety disorder due to a general medical condition.
Substance-induced anxiety disorder. Anxiety disorder not otherwise specified.
3.3. Epidemiology Approximately 23% of women and 0.51.5% of men have a panic disorder. Theprevalence of agoraphobia is slightly higher.
Social anxiety disorder is reported to affect 35% of the population. It affects men andwomen equally.23% of the general population met the criteria forobsessive-compulsive disorder atsome point during their lives. Men and women are equally likely to develop this disorder.Patients have a normal range of intelligence, despite early reports that they possessabove-average intellect.
Generalized anxiety disorder is relatively common. Its life-time prevalence is between4 and 7% in the general population. Rates are higher in women and persons youngerthan 30 years.
The prevalence ofposttraumatic stress disorder in the general population is estimatedat about 0.5% in men and 1.2% in women. The disorder can occur at any age. Thefrequency among survivors of catastrophes varies, e.g., 57% of persons 1 year later.
3.4. Disease DescriptionPanic Disorder (PD)
PD consists ofrecurrent, unexpected panic (or anxiety) attacks accompanied by at
least a month or more of persistent concern about having another attack, worry about theimplications of having an attack, or significant behavioural change related to the attacks.
According to DSM-IV criteria for PD, at least 4 of 13 characteristic symptoms must occurduring the attack. The 13 characteristic symptoms are:
Palpitations or accelerated heart rate. Sweating. Trembling or shaking. Sensations of shortness of breath. Feeling of choking. Chest pain or discomfort. Nausea or abdominal distress.
-
8/9/2019 TAP Depression Anxiety
35/7235
Depression and Anxiety
For internal use only
Feeling dizzy, unsteady, lightheaded, or faint. Derealization (feelings of unreality) or depersonalization (being detached from oneself). Fear of losing control or going crazy. Fear of dying. Paresthesias (numbness or tingling sensations). Chills or hot flushes.
Complications: The most common complications of PD are depression and alcohol
abuse. PD patients are at increased risk for peptic ulcer disease and
hypertension. Agoraphobia is a disabling complication of panic disorder. Pa-
tients fear having a panic attack in a public place and embarrass-ing themselves. They tend to avoid crowded places and at its mostsevere, agoraphobia leads many patients to become housebound.
Panic attacks usually have sudden onset, peak within minutes, and last 5 to 30 minutes.PD and agoraphobia each typically have an onset in mid-20s. Panic disorder andagoraphobia generally are considered chronic and life-long. The severity and intensity of symptoms can fluctuate, total remission is uncommon.
Social Anxiety Disorder (SAD)
SAD is a marked and persistent fear of humiliation or embarrassment in public places.
These individuals fear situations in which they might be observed by other people. Theperson recognizes that the fear is excessive or unreasonable. The symptoms are not dueto a substance or another medical condition.
SAD begins during adolescence. It tends to develop slowly, is chronic and has no obviousprecipitating stressors. Many patients with SAD become dependent on alcohol or sedativedrugs they use them to reduce their anxiety in feared situations.
Obsessive-Compulsive Disorder (OCD)
The hallmarks of OCD are obsessions or compulsions, or more commonly, both.
According to DSM-IV,obsessions are recurrent and persistent ideas, thoughts, impulses, or images that are experienced asintrusive and inappropriate and that cause marked anxiety and distress.Compulsions are repetitive, purposeful, and intentional behaviors or mental acts performed in response to obsessions oraccording to certain rules that must be applied rigidly.
Common obsessions include fears of harming other persons or sinning against God.Examples of compulsions include repetitive hand washing or ritualistic checking. Theseare meant to neutralize or reduce discomfort or to prevent a dreaded event or situation.In short,obsessions create anxiety, which is relieved by compulsive rituals.
The symptoms are not due to another disorder, and they are not caused by the effects of a substance or general medical condition.
-
8/9/2019 TAP Depression Anxiety
36/7236
Depression and Anxiety
For internal use only
OCD typically begins in the late teens or early 20s. Onset is generally gradual but mayoccur suddenly over a period of one month in the absence of any obvious stressor.
Obsessive-compulsive symptoms are usually worsened by depressed mood and stressfulevents. In fact, it is often depression that leads the OCD patient to seek help, not theobsessions and compulsions.
General Anxiety Disorder (GAD)GAD is characterized by excessive anxiety and worry that is difficult to control,without the specific symptoms that characterize either phobic disorders, PD or OCD. Thisworry is central to the diagnosis of GAD.
Patients with GAD worry excessively about life circumstances, including their health,finances, social acceptance, job performance, and marital adjustment.
The criteria also require that the individual have at least three of the following six symptoms:
Feeling restless or keyed up. Being easily fatigued. Having poor concentration. Being irritable. Having muscle tension. Experiencing poor sleep.
The condition must persistfor 6 months or longer.
The disorder appears to have chronic course, with symptoms that fluctuate over time.About one quarter of patients with GAD develop panic disorder. The most frequentcomplications of GAD are major depression and substance abuse.
Posttraumatic Stress Disorder (PTSD)PTSD occurs in persons who have experienced a trauma in which they experienced,witnessed, or were confronted with an event involving actual or threatened death, seriousphysical injury, or a threat to ones physical integrity. Examples include combat, physicalassault, rape, and disasters such as home fires.
The three major elements in PTSD include: Re-experiencing the trauma through dreams or recurrent and intrusive thoughts. Showing emotional numbing such as feeling detached from others. Having symptoms of autonomic hyper arousal such as irritability and exaggerated startle response.
Many patients with PTSD develop frank major depression, other anxiety disorders, alcoholand drug abuse, anger and irritability, and poor impulse control.
-
8/9/2019 TAP Depression Anxiety
37/7237
Depression and Anxiety
For internal use only
3.5. Disease ManagementFew persons with anxiety disorders seek psychiatric treatment, although many seekevaluations from medical specialists for specific symptoms, such as palpitations or shortnessof breath. When no cause for physical symptoms is determined, patients are advised to
go to the psychiatrist.The disorders appear to have a chronic course, with symptomsthat fluctuate in severity over time.
The treatment of anxiety disorders usually involves individual psychotherapy andmedication. The patient should be educated about the chronic nature of the disorder andthe tendency of symptoms to wax and wane, often along with external stressors that thepatient may be experiencing.
Treatment methods Cognitive behavioural therapy may help the patient recognize
and control anxiety symptoms. Pharmacological therapy the most commonly used drugs: SSRIs,
benzodiazepines, buspirone. Self-help bibliotherapy: the use of written material to help people
understand their psychological problem.
Appendix: Premenstrual Dysphoric Disorder (PMDD)
PMDD is a mood disorder with symptoms sufficiently severe that they result in significantdisruption of a womans normal level of functioning across family, social, and occupationaldomains. The degree of disability and impairment in quality of life is very similar to whatis reported by patients with other depressive or anxiety disorders. Antidepressants,especially SSRIs, are considered first-line treatment for severepremenstrual syndrome(PMS) and PMDD.
MD
PD
SAD
OCD
GAD
PTSD
Disease descriptionEmotional and physical symptoms.
Recurrent, unexpected anxiety attacks.Agoraphobia: avoiding public places.
A marked and persistent fear of humiliation orembarrassment in public places.Obsessions recurrent and persistent ideas thatcause distress.Compulsions repetitive, purposeful behaviours inresponse to obsessions or rigid rules.Excessive anxiety that is difficult to control about lifecircumstances for 6 months or longer.
In persons who have experienced severe trauma.
Epidemiology9 to 19% of the population over15 years old.Women: 2 to 3%Men: 0.5 to 1.5%
Women = men,3 to 5% of the population.Women = men,2 to 3% of the population.
Women, persons younger than30, 4 to 7% of the population.
Women: 1.2%Men: 0.5%
ComplicationsSuicide.
Increased risk forpeptic ulcer andhypertension.Depression.Alcohol abuse.Alcohol and sedativeabuse.Depression.
PD.Depression.Substance abuse.Depression.Other anxietydisorders.Substance abuse.Poor impulse control.
-
8/9/2019 TAP Depression Anxiety
38/7238
Depression and Anxiety
For internal use only
Etiology
Etiology of PMDD is unknown. The current predominant hypothesis is that women whodevelop PMDD have an underlying vulnerability in CNS neurotransmitter systems, mostnotably the serotonergic system. Typically, the disorder is present in families.
Epidemiology The prevalence of PMDD is estimated at 3 to 8% of females in the reproductive age.
Disease Description
PMDD is considered a severe form of PMS. Symptoms are severe enough to impairsocial, sexual, school and/or occupational functioning.
This disorder can begin anytime after menarche, but usually in the late teens or early 20s.
DSM-IV criteria for PMDD:
Presence of 5 of 11 depressive, anxiety, cognitive or physicalsymptoms experienced in most of the menstrual cycles for the past year.
The symptoms begin 3 to 10 days before menstruation begins. Thesymptoms resolve spontaneously within 3 days of the onset of menses, and the patients then remain free of symptoms until at leastpast the halfway point of their cycle.
The symptoms of PMDD are significant dysphoria (depression,anxiety, suddenly feeling sad or tearful, with increased sensitivity topersonal rejection) with fatigue, difficulty in concentration, de-creased interest in usual activities, sleep change (insomnia or hyper-somnia), irritability, anger and appetite change (loss or more com-monly, increase, often sweets). Concurrently, patients could alsohave headache, bloating, breast swelling or tenderness, joint ormuscle pain, nausea, or constipation.
Symptoms are discretely related to the menstrual cycle and are notmerely a worsening of pre-existing depression, anxiety or personal-ity disorder.
Over the years or decades, the premenstrual episodes typically gradually become longer
and more severe. Episodes cease after menopause. The symptoms tend to remit duringpregnancy.
Differential Diagnosis
The following underlying psychiatric or medical disorders may present with pattern of premenstrual exacerbation that mimics the monthly pattern of PMDD:
1. Psychiatric disorders: major depression, dysthymic disorder,bipolar II, cyclothymic disorder, PD, GAD, bulimia, PTSD, victimsof abuse.
2. Medical disorders: endocrine disorders (hypothyroidism,diabetes), autoimmune or collagen vascular disorders, anaemia,chronic fatigue syndrome, endometriosis.
-
8/9/2019 TAP Depression Anxiety
39/7239
Depression and Anxiety
For internal use only
Disease Management
Initial management includesnon-medical interventions such as education and support,counselling, stress management, relaxation techniques, exercise, cognitive therapy andsleep deprivation. Caffeine and salt restriction are of unproven benefit. The herbal remedyAgnus castus, calcium carbonate and vitamin B6 supplementation has been found to beof benefit.In women with predominantly psychological symptoms, thecontinuous or intermittentadministration ofSSRIs can be helpful. Fluoxetine (Portal by Lek Sandoz),citalopram(Citalon by Lek Sandoz),sertraline and venlafaxine have been shown in controlledtrials to alleviate both the psychological and physical symptoms in women with PMS.Clomipramine, a nonselective serotonin reuptake inhibitor, has also been tried withsome success.
The anxiolyticalprazolam has also been used, but use of this and other benzodiazepinesshould be restricted to the luteal phase of the cycle in selected patients to minimize therisk of dependence and tolerance.Abdominal bloating and swelling associated with PMDD has traditionally been thoughtto be due to sodium and water retention. However, in most women with these symptomsthere is no evidence of an increase in body-weight or in body sodium or total water, anduse of diuretics is therefore not justified. Nevertheless, in women with appreciable weightgain in the luteal phase, diuretics may be useful.
Symptoms of PMDD may remit ifovulation is suppressed. The adverse effects of thattreatment make this third-line treatment for PMDD.
4. Treatment Methods4.1. Pharmacotherapy
Available drug therapies for depression include:
Augmentation therapies (to enhance the effects of antidepressants). Adjunctive therapies (to ameliorate antidepressant-induced sideeffects).
Antidepressants.When patients do not respond well to antidepressants alone, physicians sometimes useaugmentation therapies to enhance the antidepressants effects before switching toanother class of antidepressant.
-
8/9/2019 TAP Depression Anxiety
40/7240
Depression and Anxiety
For internal use only
Augmentation Therapies Used in Conjunction with AntidepressantsAugmentation Therapy Clinical IntentMood stabilizers To potentiate antidepressant effect in patients who have severe depression or are
unresponsive to TCAs, MAOIs, and SSRIs; mood stabilizers used include lithium, valproicacid, and carbamazepine. Lithium requires at least twice yearly blood testing becausetherapeutic doses closely approach toxic doses.
Pindolol To accelerate response to antidepressant therapy (anecdotal evidence) or to addresssymptoms of anxiety.
Stimulants To potentiate antidepressant effect of TCAs or MAOIs in patients withno symptoms of anxietyor agitation; agents used include methylphenidate or dextroamphetamine (this approach is notwidely used).
Thyroid augmentation To potentiate antidepressant effect in refractory patients; T3 is the preferred form of thyroid.
Adjunctive therapies are also used to treat antidepressant-induced side effects or comorbidsymptoms such as anxiety or delusions that are often seen in patients with depression.The tables below list some commonly used augmentation therapies and adjunctive
therapies.Adjunctive Therapies Used in Conjunction with Antidepressants
Adjunctive Therapy Clinical IntentAntipsychotics To treat psychotic symptoms in patients with delusional depression.Benzodiazepines To reduce antidepressant-induced activation during first few weeks of therapy; commonly used
agents include alprazolam, clonazepam, and diazepam.Bupropion To address antidepressant-induced sexual dysfunction (bupropion is also used as
monotherapy for depression).Buspirone To address antidepressant-induced sexual dysfunction or symptoms of anxiety.Dopaminergic agents To address antidepressant-induced sexual dysfunction; antiparkinsonian agent amantadine
(Endo Pharmaceuticals Symmetrel) and pramipexole (Pharmacias Mirapex) are sometimesused.
The exact mechanism of how antidepressant drugs work to treat major depression is notknown. However, a consistent finding is that drugs with potent agonist effects onnoradrenergic and serotonergic receptors possess antidepressant activity. Differences inefficacy between antidepressant drug classes are very subtle anddifferences in safety and tolerability are much more pronounced. Drugs that have the best safety andtolerability profiles are generally used as first-line agents.
Antidepressant drug classes are: Tricyclic antidepressants (TCAs). Monoamine oxidase inhibitors (MAOIs). Selective serotonin re-uptake inhibitors (SSRIs). Multiple-mechanism antidepressants.
Some physicians also consider herbal remedies such asSt. Johns Wort ( Hypericum perforatum ), Leks OTC productDeprim, to be effective in treatment of depression.
Figure below depicts the mechanism of action of SSRIs, TCAs and MAOIs in treatment of depression. SSRIs selectively inhibit the presynaptic reuptake of serotonin while exerting
little effect on norepinephrine reuptake.SSRIs as a class have little effect on histaminergic,cholinergic, dopaminergic, or alpha-adrenergic receptors. So, they have lower incidenceof side effects compared to older antidepressants.
-
8/9/2019 TAP Depression Anxiety
41/7241
Depression and Anxiety
For internal use only
Mechanism of Antidepressant Drug Action in the Treatment of Depression
Source: Decision Resources, Inc.
Chronologic overview Aside from herbal preparations, TCAs have been on the market longest (since the 1950s),followed by MAOIs and second-generation antidepressants.
Tricyclic antidepressants (TCAs), with diverse effects on many neurotransmitters andreceptor systems, have well-established clinical efficacy in treating major depression since1953.
Their effectiveness is due at least in part to their effects on both norepinephrine (NE) andserotonin (5-HT). Their very broad mechanisms of action also includemany unwantedeffects related to their potent activity on histaminic, muscarinic, and alpha-adrenergic
receptors.Monoamine oxidase inhibitors (MAOIs) inhibit monoamine oxidase (MAO), an enzymeresponsible for the degradation of serotonin, dopamine, and norepinephrine, which arethe primary neurotransmitters involved in etiology of depressive disorders. Blocking thisenzymatic process leads to an increase in CNS levels of these monoamines.
MAOIs produceserious side effects and interactions with many other medicines andfoods. Therefore, their use is limited to the patients with heavy forms of depression, non-responding to other treatments.
Selective serotonin reuptake inhibitors (SSRIs) show prominent serotonin agonistactivity, do not possess most of the significant adverse effects seen with TCAs and offermuch greater safety in overdose. They became the most widely prescribed antidepressantsrapidly after their introduction to the market.
-
8/9/2019 TAP Depression Anxiety
42/7242
Depression and Anxiety
For internal use only
Multiple-mechanism antidepressants include: Selective serotonin and noradrenalin reuptake inhibitors
(SNRIs) such as venlafaxine and duloxetine. Venlafaxine is a potentserotonin reuptake inhibitor, and at higher doses also inhibits nore-pinephrine reuptake.
Selective noradrenalin reuptake inhibitors (SNARIs) such asreboxetine. Other agents such as mirtazapine and bupropion. By a different
mechanism, mirtazapine enhances both serotonin and norepineph-rine, and in addition, selectively blocks several postsynaptic seroto-nin receptor subtypes primarily responsible for the gastrointestinaladverse effects and sexual dysfunction seen with SSRIs.
Current Therapies Used for the Treatment of Depression
Substance Originator/Brand (US/EU) Daily Dosea
Tricyclic Antidepressant Agents (TCA) b
amytriptiline Astra Zeneca Elavil 75150 mgclomipramine Novartis Anafranil 30150 mgimipramine Novartis Tofranil 100 mgmaprotiline Novartis Ludiomil 2575 mgnortriptyline Novartis Pamelor 75100 mglofepramine Merck Gamanil 140210 mg
Monoamine Oxidase Inhibitors (MAOI)
phenelzine Warner-Lambert Nardil 1560 mgmoclobemidec Roche Aurorix/Maclamine 150600 mgisocarbixazid Roche Merplan 100200 mgtranylcypromine GlaxoSmithKline Parnate 1030 mg
Selective Serotonin Reuptake Inhibitors (SSRI) fluvoxamine Solvay/Fujisawa Luvox 100 mgfluoxetine Ely Lilly Prozac 2060 mgfluoxetine weekly Prozac Weekly 90 mgparoxetine GlaxoSmithKline Paxil/Seroxat 2060 mgparoxetine CR Paxil CR 25 mgsertraline Pfizer Zoloft 50200 mgcitalopram Lundbeck/Forest Cipramil/Celexa 2060 mgescitalopram Lundbeck/Forest Cipralex/Lexapro 1020 mg
Selective Serotonin and Noradrenaline Reuptake Inhibitors (SNRI)
milnacipran BioMerieux-Pierre Fabre Dalcipran 100 mgvenlafaxine Wyeth Effexor 75-375mgvenlafaxine XL Effexor XL 75-225 mg
duloxetine Lilly/BMS Cymbalta 60120 mgSelective Noradrenaline Reuptake Inhibitors (SNaRI)
reboxetine Pfizer Edronax/Vestra 812 mg
Other agents
mirtazapine Organon Remeron 1545 mgRemeron SolTab
trazodone Bristo-Myers Squibb Desyrel 150600 mgBupropiond GlaxoSmithKline Wellbutrin 300 mgBupropion XL Wellbutrin XL 300 mg
OTC medicinal products
Hypericum perforatum Lek Pharmaceuticals Deprim
a. Dose shown is the suggested total daily dose.b. Only a representative sample of TCAs are included in this table because of the multitude of agents available;other TCAs include amoxapine (Wyeth-Ayersts Asendin), dothiepin (Knolls Prothiaden), doxepin (Roerigs Sinequan), protriptyline (Mercks Concordin),trimipramine (Aventiss Surmontil), and desipramine (Aventiss Norpramin).c . Moclobemide is a reversible MAO inhibitor.d. Bupropion has been launched in theUnited Kingdom, France, Germany, Italy, and Spain for smoking cessation, not depression.Source: Decision Resources, Inc.
-
8/9/2019 TAP Depression Anxiety
43/7243
Depression and Anxiety
For internal use only
4.2. Tricyclic Antidepressant Agents (TCAs)Mechanism of Action
TCAs block the synaptic reuptake of serotonin and norepinephrine to varying degrees.They have little effect on dopamine and are potent blockers of muscarinic, histaminergicH1, and 1-adrenergic receptors.
The Most Commonly Used TCAs Include: the tertiary amines:
amitriptyline (AstraZenecas Elavil/Roches Laroxyl, generics,Leks Amyzol ),
imipramine (Novartiss Tofranil, generics), the secondary amines:
desipramine (Aventiss Norpramin), nortriptyline (Novartiss Pamelor, generics),
tetracyclic antidepressants: maprotiline, mianserin;
Most TCAs can be given in a single daily dose and are usually administered at bedtimebecause of their sedating effect.
Safety
TCAs are associated with ahigh incidence of side effects, because they are nonselectiveinhibitors of various receptors:
inhibition of histaminergic receptors causes long-term weight gainand sedation,
muscarinic receptor blockade can cause anticholinergic effects suchas dry mouth, constipation, blurred vision, urinary retention, andcognitive impairment,
1-adrenergic blockade can lead to postural hypotension, reflextachycardia, dizziness, and sexual dysfunction,
potential for cardiotoxicity in overdose;Therefore they are generally reserved for patients who fail to respond to SSRIs. Even so,many specialists consider TCAs the most effective agents for severe depression,and no newer class of agents has proved more effective in the treatment of majordepression.
The general rule when prescribing a TCA is to start at a very low dose and increase itslowly until plasma levels reach a therapeutic point. Routine monitoring of patients isinconvenient and expensive; therefore, physicians generally administer TCAs insubtherapeutic doses.
Interactions
TCAs are highly protein-bound and metabolized primarily by the 2D6 subset of the CYP-450 system; therefore, several other drugs can affect TCA metabolism, with potentiallyharmful results:
-
8/9/2019 TAP Depression Anxiety
44/7244
Depression and Anxiety
For internal use only
drugs increasing plasma levels of TCAs: SSRIs, oral contraceptives,acetaminophen, cimetidine, isoniazid, and valproic acid,
drugs decreasing plasma levels of TCAs: the anticonvulsantscarbamazepine and phenytoin, and barbiturates,
combining TCAs with MAOIs or sympathomimetics can lead tohypertension and CNS toxicity,
concurrent use of TCAs and warfarin puts patients at risk of haemorrhage;
Maprotiline (NovartissLudiomil, generics)
Maprotiline, a tetracyclic antidepressant, is considered as effective as commonly usedTCAs such as amitriptyline and imipramine. This drug is sometimes referred to as asecond-generation antidepressant.
Maprotiline acts primarily by blocking the reuptake of norepinephrine. The drug alsoshares the TCAs anticholinergic properties to a lesser extent and toxicity in overdose.Maprotiline is generally prescribed assecond- or third-line therapy for patients withsevere depression who are refractory to or intolerant of TCAs.
Place in Therapy
Although TCAs are no less effective than other classes of available antidepressants thatis, they benefit 60 to 80% of patients who take them their high incidence of side effects,slow onset of action, and potentially dangerous effects at high doses preclude their useas first-line agents. They are primarily prescribed by specialists and are generally reserved
as second-line treatment for patients who are refractory to more than one drug from theother classes of antidepressant drugs.Recently they have been used for treatment ofneuropathic pain.
4.3. Monoamine Oxidase Inhibitors(MAOIs)
Mechanism of Action
MAOIs restore serotonin and norepinephrine function by blocking monoamine oxidase(MAO), a naturally occurring enzyme that metabolizes monoamines such as serotoninand norepinephrine.
MAO exists in two major forms MAO-A and MAO-B which are distinguished by theirsubstrate affinities for norepinephrine and serotonin (MAO-A) or dopamine (MAO-B).The original MAOIs were nonselective, irreversible inhibitors of both MAO-A and MAO-B. Extensive research has revealed thatMAO-A inhibition is primarily responsible forthe MAOIs antidepressant effects and that the accompanying dangerous tyramine-MAOIinteractions can be significantly attenuated by usingselective reversible inhibitors ofMAO-A (RIMAs).
-
8/9/2019 TAP Depression Anxiety
45/7245
Depression and Anxiety
For internal use only
The Most Commonly Used MAOIs Include: Moclobemide (Roches Aurorix/Maclamine/Manerix). Phenelzine (Warner-Lamberts Nardil, generics). Tranylcypromine (GlaxoSmithKlines Parnate, generics).
Safety The original MAOIs (phenelzine, tranylcypromine) are associated with potentially seriousside effects:
weight gain, oedema, insomnia, muscle cramps, dizziness, sexual dysfunction, orthostatic hypotension and cardiotoxicity;
Interactions
MAOI have dangerous interactions with tyramine-containing foods which can causehypertensive episodes and possibly lethal brain haemorrhage. They have also interactionswith numerous other drugs.
Moclobemide (Roches Aurorix/Maclamine /Manerix)
Moclobemide is one of the most well-known RIMAs and the most widely used.
Moclobemide is marketed for depression in Europe, Canada, and other countries, but isnot available in the United States. Clinical data indicate that moclobemide is equivalentin efficacy to other available antidepressants Including SSRIs and TCAs andmay beparticularly useful in the elder