FISHERIES CONTROL AT THE ELY-CENTRE Lars Sundqvist Fisheries inspector Ostrobothnian ELY-centre
1 | P a g e V 1 3
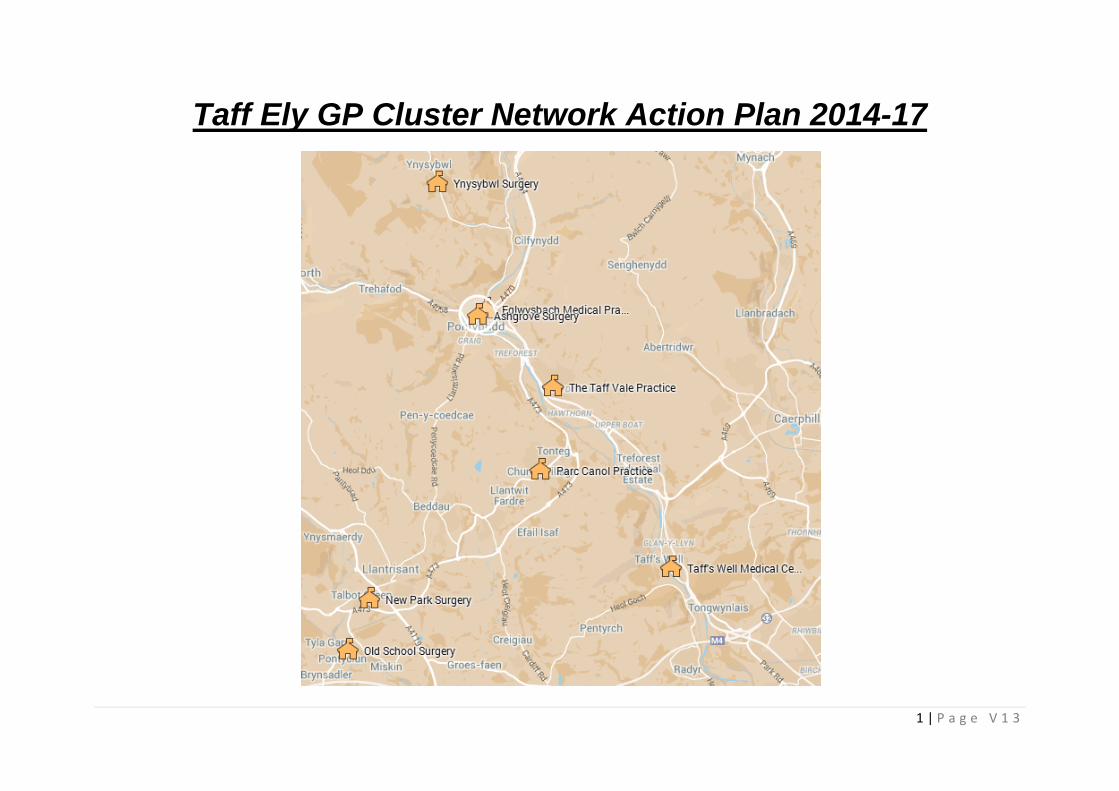
Taff Ely GP Cluster Network Action Plan 2014-17
2 | P a g e V 1 3
TAFF ELY NETWORK CLUSTER ACTION PLAN 2014-17
This plan has been developed by the following 8 practices which operate in the Taff Ely Cluster Area, through facilitated discussion with the Local Clinical
Director and Primary care LHB Locality Management :-
• Ashgrove Surgery
• Eglwysbach Surgery
• New Park Surgery
• Old School Surgery
• Parc Canol Surgery
• Taff Vale Surgery
• Taffs Well Surgery
• Ynysybwl Surgery
3 | P a g e V 1 3
The plan The plan has been informed by the practice development plans produced by practices; public health information on key health needs within the
area; information provided by Cwm Taf uHB re current activity/referral patterns; an understanding of our localities baseline services (current service
provision) and identification of potential service provision unmet needs. The plan also embraces key UHB priorities for the next three years. The plan details
cluster objectives for years 1-3 (2014/2017) that have been agreed by consensus across practices, providing where relevant background to current position,
planned objectives and outcomes and actions required to deliver improvements. The plan is by its very nature fluid /flexible and evolving over the next 3
years the plan itself will be reviewed and updated in response to changes in cluster planning.
The RAG rating score indicates progress against planned action:
Red- future work
Amber- work in progress
Green – work completed.
A number of key principles underpin the plan:
• Management of variation/reducing harm/sharing good practice: in acknowledgement of the fact that healthcare must be delivered on the basis of
safety, effectiveness and efficiency, the practices have considered and analysed variation in performance and where appropriate have considered
steps by which to map standardise practice based on clinical guidelines.
• Maximising use of local cluster resources: practices have taken into account the capacity, capability and expertise that exists within primary care,
community services and voluntary/third sector services to deliver more care closer to home and reduce unnecessary demands within the acute care
services.
• Promoting integration/better use of health, social care and third sector services to meet local needs: practices have considered current
arrangements/links with RCT CBC and the voluntary sector and will also consider any action plans from stakeholders that evolve over the 3 year
cycle of this plan.
4 | P a g e V 1 3
• Considering and embedding new approaches to delivering primary care: this includes increased use of technology, new roles and service models
considering an embedding new approaches to delivering primary care: this includes increased use of technology new roles
• Maximising opportunities for patient participation: this includes consideration of models of good practice that exist with within/locality/cluster
and nationally and within the rest of the UK.
• Maximising opportunities for more efficient and effective use of resources: this includes consideration of current resources, opportunities to
utilise and current and new services more efficiently and effectively
Additional contributors to the plan/potential evolving contributors to the plan subject to evolution of plan
• Health and social care facilitators.
• Primary care practice managers.
• Practice Nursing and allied health professions representatives.
• Local voluntary sector providers and third sector.
• Prescribing advisers.
• Potential educator partners including third sector TEDS for brief alcohol intervention training, podiatry for foot assessment training for Health careassistants.
• Primary Care Support Unit Nursing advisory expertise/local university school of health care re Health care assistant initiatives and informingcommunity care planning e.g. diabetes.
• Public Health
• Acknowledgements Cynon cluster plan authors re layout.
5 | P a g e V 1 3
Strategic Aim 1: to understand the needs of the population served by the Cluster Network
Outline of cluster population profile
The Cwm Taf uHB population estimate in 2007 was 289.4 thousand with 233.7 thousand in the RCT locality .Approximately 10% of the population of Wales
live within Cwm Taf uHB, the uHB locality is the second smallest in Wales but the second most densely populated area (Cardiff is first) The Taff Ely Valley in
recent CMO for Wales reports and based on recent Public Health Wales data is an area of high social deprivation .We also due to our high deprivation status
have high rates of mental health issues long term disability/morbidity ,a high rate of poverty/benefits uptake and high rates of chronic illness from legacy
heavy industry particularly mining. Recent CMO reports have indicated a low level of car ownership with an obvious impact on service planning. The
neighbourhood has a higher proportion of persons aged 0-15 and 30-44 than the Cardiff average. Public Health Wales indicate that our area consists mainly
of most deprived and next most deprived classifications. 34% of Cwm Taf as a whole is designated most deprived on the Welsh Index Multiple Deprivation
Scale (WIMD). Within our cluster this figure rises to 38.2% in the Taff Ely Valley. The Public Health Observatory for Wales publications in the field of child
health highlight for our locality that: our rate of low birth weights is significantly higher than the Welsh average 1 in 15 c.f. all Wales 1 in 18; and the % of
children (<20 years old) living in poverty is 26.6% c.f. all Wales 22.2%. Particularly relevant to our area is the identification of Rhydfelen and Glyncoch as
areas of greatest deprivation in Wales by the public health observatory (ranked 17th and 27th respectively). All Wales public health observatory data on
levels of unemployment in the 16-24 yr old age group show a rate of 18.4% for CwmTaf c.f. all Wales 15.7%.With regard to our older population the data for
those living alone at 43.9% is near to the all Wales average of 43%.Our localities Black and ethnicity population data suggest an LHB rate of 1.1% lower than
the all Wales average of 2.1 % which in turn is lower than England’s data. Finally Public Health Wales Data indicates that for Cwm Taf’s population as a
whole, life expectancy is reduced by 1.5 years for males c.f. the welsh national average i.e. 75.3yrs as opposed to 77 years old. Our locality has in recent
years seen and will see several large scale residential developments with obvious impacts on primary care provision planning. Recent public health
presentations to our locality identify several top challenges to morbidity and mortality:
• Malignancy (Cancer survival levels in Cwm Taf are amongst the lowest in Wales)
• Cardiovascular disease/circulatory disease
• Smoking levels
Subsequent review of Welsh statistics highlighted further areas of concern (see next page)
6 | P a g e V 1 3
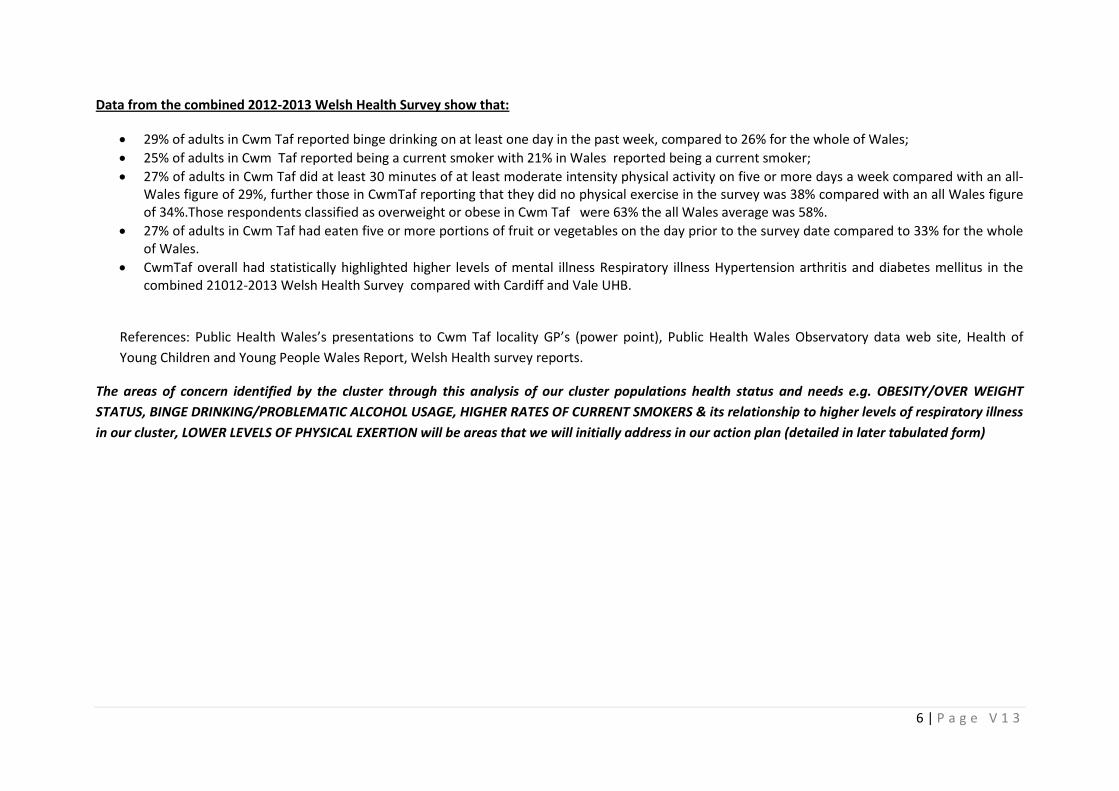
Data from the combined 2012-2013 Welsh Health Survey show that:
• 29% of adults in Cwm Taf reported binge drinking on at least one day in the past week, compared to 26% for the whole of Wales;
• 25% of adults in Cwm Taf reported being a current smoker with 21% in Wales reported being a current smoker;
• 27% of adults in Cwm Taf did at least 30 minutes of at least moderate intensity physical activity on five or more days a week compared with an all-Wales figure of 29%, further those in CwmTaf reporting that they did no physical exercise in the survey was 38% compared with an all Wales figureof 34%.Those respondents classified as overweight or obese in Cwm Taf were 63% the all Wales average was 58%.
• 27% of adults in Cwm Taf had eaten five or more portions of fruit or vegetables on the day prior to the survey date compared to 33% for the wholeof Wales.
• CwmTaf overall had statistically highlighted higher levels of mental illness Respiratory illness Hypertension arthritis and diabetes mellitus in thecombined 21012-2013 Welsh Health Survey compared with Cardiff and Vale UHB.
References: Public Health Wales’s presentations to Cwm Taf locality GP’s (power point), Public Health Wales Observatory data web site, Health of
Young Children and Young People Wales Report, Welsh Health survey reports.
The areas of concern identified by the cluster through this analysis of our cluster populations health status and needs e.g. OBESITY/OVER WEIGHT
STATUS, BINGE DRINKING/PROBLEMATIC ALCOHOL USAGE, HIGHER RATES OF CURRENT SMOKERS & its relationship to higher levels of respiratory illness
in our cluster, LOWER LEVELS OF PHYSICAL EXERTION will be areas that we will initially address in our action plan (detailed in later tabulated form)
7 | P a g e V 1 3
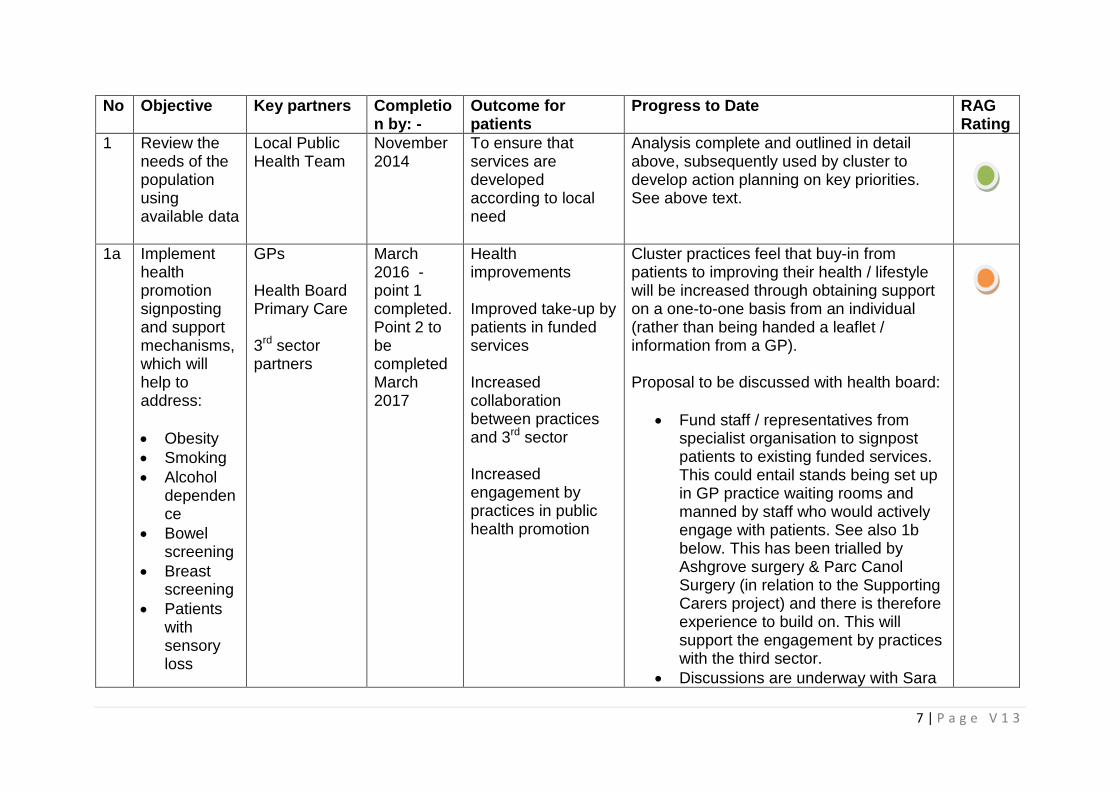
No Objective Key partners Completion by: -
Outcome forpatients
Progress to Date RAGRating
1 Review theneeds of thepopulationusingavailable data
Local PublicHealth Team
November2014
To ensure thatservices aredevelopedaccording to localneed
Analysis complete and outlined in detailabove, subsequently used by cluster todevelop action planning on key priorities.See above text.
1a Implementhealthpromotionsignpostingand supportmechanisms,which willhelp toaddress:
• Obesity• Smoking• Alcohol
dependence
• Bowelscreening
• Breastscreening
• Patientswithsensoryloss
GPs
Health BoardPrimary Care
3rd sectorpartners
March2016 -point 1completed.Point 2 tobecompletedMarch2017
Healthimprovements
Improved take-up bypatients in fundedservices
Increasedcollaborationbetween practicesand 3rd sector
Increasedengagement bypractices in publichealth promotion
Cluster practices feel that buy-in frompatients to improving their health / lifestylewill be increased through obtaining supporton a one-to-one basis from an individual(rather than being handed a leaflet /information from a GP).
Proposal to be discussed with health board:
• Fund staff / representatives fromspecialist organisation to signpostpatients to existing funded services.This could entail stands being set upin GP practice waiting rooms andmanned by staff who would activelyengage with patients. See also 1bbelow. This has been trialled byAshgrove surgery & Parc CanolSurgery (in relation to the SupportingCarers project) and there is thereforeexperience to build on. This willsupport the engagement by practiceswith the third sector.
• Discussions are underway with Sara
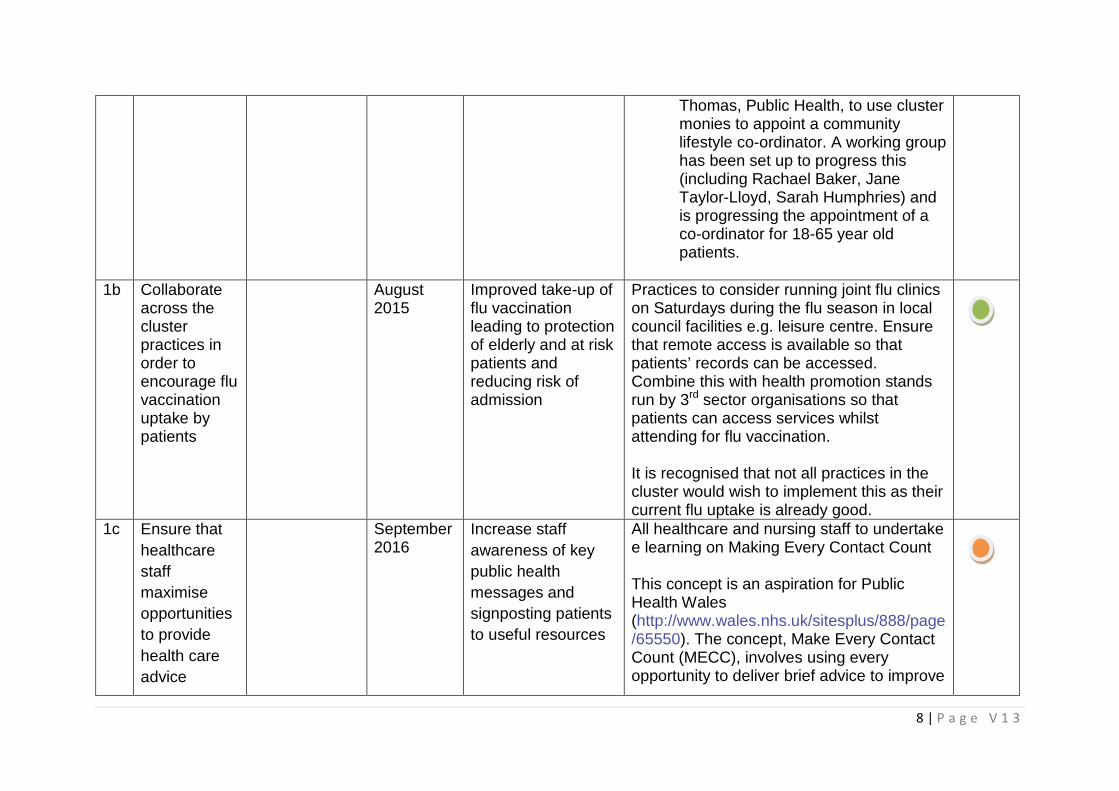
8 | P a g e V 1 3
Thomas, Public Health, to use clustermonies to appoint a communitylifestyle co-ordinator. A working grouphas been set up to progress this(including Rachael Baker, JaneTaylor-Lloyd, Sarah Humphries) andis progressing the appointment of aco-ordinator for 18-65 year oldpatients.
1b Collaborateacross theclusterpractices inorder toencourage fluvaccinationuptake bypatients
August2015
Improved take-up offlu vaccinationleading to protectionof elderly and at riskpatients andreducing risk ofadmission
Practices to consider running joint flu clinicson Saturdays during the flu season in localcouncil facilities e.g. leisure centre. Ensurethat remote access is available so thatpatients’ records can be accessed.Combine this with health promotion standsrun by 3rd sector organisations so thatpatients can access services whilstattending for flu vaccination.
It is recognised that not all practices in thecluster would wish to implement this as theircurrent flu uptake is already good.
1c Ensure that
healthcare
staff
maximise
opportunities
to provide
health care
advice
September2016
Increase staff
awareness of key
public health
messages and
signposting patients
to useful resources
All healthcare and nursing staff to undertakee learning on Making Every Contact Count
This concept is an aspiration for PublicHealth Wales(http://www.wales.nhs.uk/sitesplus/888/page/65550). The concept, Make Every ContactCount (MECC), involves using everyopportunity to deliver brief advice to improve
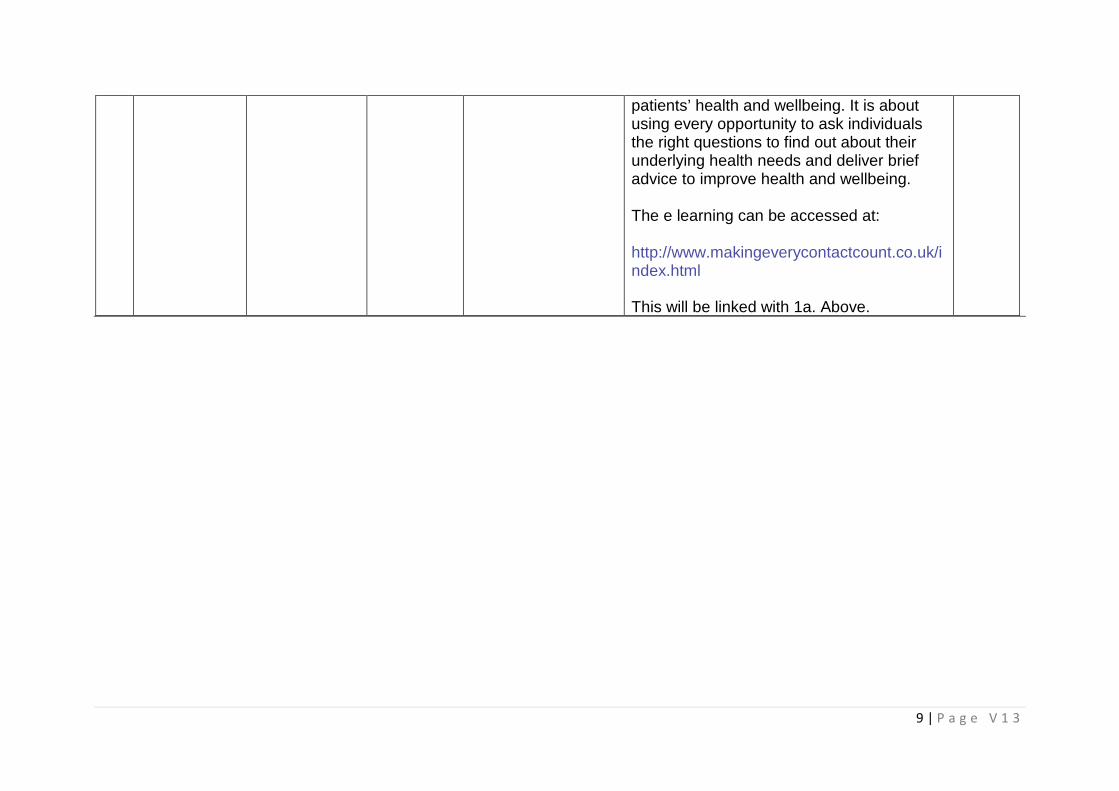
9 | P a g e V 1 3
patients’ health and wellbeing. It is aboutusing every opportunity to ask individualsthe right questions to find out about theirunderlying health needs and deliver briefadvice to improve health and wellbeing.
The e learning can be accessed at:
http://www.makingeverycontactcount.co.uk/index.html
This will be linked with 1a. Above.
10 | P a g e V 1 3
Strategic Aim 2: To ensure sustainability of core GP services and access arrangements that meet
reasonable need (including new approaches to delivering primary care)
Cluster practice members have considered this area already in their individual Practice Development Plans, with a range of access and sustainability issues
considered including number of GP appointments provided, hours of services, inappropriate use of A+E, unscheduled admissions +GP Out of Hours services
by patients, DNA rates, Promoting use of technology such as My Health on Line/Texts messaging etc. Further WAG briefing on primary care clusters also
advocates use of new technology including ultimately via My Health patient access to their records online repeat prescription ordering, online appointment
booking as well as new technologies for consultation, practices are at various stages with these developments within the cluster. In addition to practices
individual development plans in this area those areas of common interest across the Cluster are identified in this section.
No Objective Keypartners
For completionby: -
Outcome forpatients
Progress to Date RAG Rating
2a Develop
transfer of
appropriate
services from
secondary to
primary care
cluster hub
once the LHB
have created
proposed
“Hub” at Dewi
Sant
including
relevant
infrastructure
Healthboard
Secondarycare
GPs
NWIS &DigitalDevelopmentTeam
Health board toconfirmtimescales ofthe setting up of“Hub”.
Cluster grouptimelines aredependant uponthe LHB DewiSant Parkprogramme
Improved
efficiency in
delivering
services in
primary care with
improved access
for patients closer
to patient’s home
Progress will be dependant upon thesetting up of the “Hub” and relevantinfrastructure with the initial roll out ofservices as outlined belowMSK Service – which will consist ofboth Consultant, GPWSI, PhysioServices, and MRI services to providepatients with a “one stop shop”
Supporting the LHB with the creationof a Primary Care Support Unit whichwould be based at the “Hub” and toinclude GPs (using the academicfellowship model), Pharmacists,Nurse Practitioners, Nurses, HCP andPhlebotomists. The cluster groupwould help with the recruitmentprocess
11 | P a g e V 1 3
It should be noted that any servicesoffered at the “Hub” should notconflict with current or thedevelopment of new services withinthe confines of a GP practiceenvironment, they should remainthere.
Central patient record access will bekey to making these services viable,and will form part of the coreinfrastructure required in the settingup of the “Hub”.The project is currently progressingslowly
2b Facilitate
increased
use of My
Health
Online
(MHOL) by
patients to
improve
access to
appointment
booking and
repeat
prescription
requests
NWIS
GPpractices
August 2016 There is varying
patient and
practice uptake of
technology to
improve access.
Increased uptake
will improve
access to
services for
patients.
Discuss within the cluster and worktowards agreement for all practices toimplement MHOL for bothappointments and repeatprescriptions.
Collaborate across practices onpromoting the service to patients.
NWIS is progressing furtherdevelopments to MHOL to provideeasier registration and use of an App.
12 | P a g e V 1 3
2d Work withthe healthboard ondevisingsolutions forthe currentissue of GPrecruitmentandsuccessionplanning
Healthboard
Dr MairHopkins –lead
GPs asrequired
Health board toconfirmtimescales
The issue is asignificant onewithin the clusteras manypractices arestruggling to fillvacancies andreplace retiringpartners
Dr Mair Hopkins has volunteered toact as lead for the cluster on a healthboard committee to review this issue.
As an interim solution, the healthboard should consider how GPs canbe shared across practices, which areshort of resource.
The issue has also led to a significantand unsustainable increase in locumrates, which is having a severedetrimental impact on those practices,which are forced throughcircumstances to employ locums.Note that the Cwm Taf practicemanager forum is discussing theagreement of consistent locum termsand conditions across practices toensure that a standard of locum tasksrequired by practices will be put inplace (avoiding the current practice oflocums dictating their own varyingterms to practices). We would alsolook to link with neighbouring healthboards to ensure regionalconsistency.
KB to chase June Williams forupdate.
2e Improveretention of
Practicemanagers
March 2017 Maintaining afully trained and
Health board funding is available tobackfill practice nurse positions to
13 | P a g e V 1 3
practicenursing staffand facilitatereplacementof retiringstaff
Healthboard
Practicenurses
resourced healthcare team withinpractices willensure thatpatients’ chronicdiseasemanagement issustained andthat a fullyresourced rangeof nursetreatments isavailable forpatients
enable them to train nursing staff insecondary care, who wish to work inprimary care.
This issue needs to be discussedfurther within the cluster to identifywhich practices are able to take onthis option.
June Williams will need to gather datafrom practice nurse population inconfidence to honest feedback.
2f Developfurther GPswith SpecialInterests(GPwSIs) tosupport 2a
Healthboard
GPs
March 2017 Develop animproved rangeof servicesavailable topatients withincluster practices
Practices have already submitteddata to the health board on currentGP and nurse specialist interests aspart of their practice developmentplans.
The next stages are:
• Health board to identify gaps inskill sets across the cluster
• Health board to identify GPs,who would be interested indeveloping as GwPSI for gapspecialist areas
• Health board to review andincrease GPwSI rate andshare revised pay scale with
14 | P a g e V 1 3
practices, as current rate doesnot cover backfill requirement
• Health board to identify GPs,who can provide training forthe gap specialist areas andfacilitate training. This could bethrough health board fundedtraining sessions in practice,via formal observation or bybackfilling.
It is proposed that a similar schemebe investigated for healthcare staffe.g. cryotherapy training for practices,who wish to offer this service.
2g Review GPvisitingguidelinesprepared bySouthStaffordshireLMC
GPsPracticemanagers
September2015
Consistentapproach to GPvisiting acrosscluster practices,ensuring thatpriority is given topatients withsame day /urgent visitingneed
Guidelines to be reviewed bypractices and discussed at clustermeeting before consideredimplementation – review at nextcluster meeting 09 September.
Practices have agreed in principle toimplement and to utilise informationprovided by third sector regardingpatient transport (to overcome keyperceived issue).
15 | P a g e V 1 3
Strategic Aim 3: Planned care- to ensure that patient’s needs are met through prudent care pathways,
facilitating rapid, accurate diagnosis and management and minimising waste and harm.
No Objective Keypartners
Forcompletionby: -
Outcome forpatients
Progress to Date RAGRating
3a Standardiseuse ofelectronicand non-electronicreferralforms.Maximiseease ofaccess anduse
Integration offorms withclinicalsystems
Healthboard
INPS
EMIS
Directorateleads
NWIS
December2015
More efficientreferral process withimprovedcommunication andimprovedgovernance
A number of templates have been stored onthe Cwm Taf GP portal. These need to bereviewed and added to, to ensure that acomprehensive library of forms is available.
This should be coupled with communicationto practices of where and how to access anda process, which will ensure that practicesno longer use locally stored copies.
Accountability will need to be assigned bythe health board for maintaining the library,which will require liaison with secondarycare, as a central point of contact for anynew / amended forms to be used by primarycare.
Current paper-based forms should bereplaced by electronic version – this willrequire health board / IT resource.• Provide central repository of templates
for clinical systems (Vision & EMIS) thatwould be accessed via the Portal.
16 | P a g e V 1 3
• This should include approval by the LMCwith input from secondary care wherenecessary to agree pathways
• Use INPS & EMIS to create and maintaintemplate versions
3b Improveaccess tominor surgeryserviceswithin thecommunity
Linked to 2aabove.
HealthBoard
GPs
March 2017 Reduced waitingtimes and provisionof care closer to thepatient’s home
A number of improvements can be made tothe minor surgery enhanced servicesprocess in order to improve servicesavailable to patients, namely:
• Add carpal tunnel decompression tothe enhanced service (alreadyavailable within the Enhanced MinorSurgery agreement
• Referral centre to route referrals inprimary care i.e. other organisations(e.g. podiatrists) could use this routeto refer procedures (e.g. toe nailremoval) to practices signed up todeliver certain services (this hasalready been proposed by Ashgrovesurgery to the Health Board)
• Identify further procedures which canbe transferred to primary care, byinvolving consultants to agreetransfer and deliver training
A first phase has been rolled out to extendminor surgery but there is still a significantlimit to what services can be delivered inprimary care.
17 | P a g e V 1 3
The GP Portal should be used to makepractices aware of which practices deliverwhat services and then enable referral to bemade via WCCG (as already happens forvasectomy referrals to Ashgrove andPontcae surgeries). LHB to ensure this iskept up to-date as more services are rolledout by the practices/hub.
Data provided to June Williams regardingpractice specialities via Hayley Pugh.
3d Extendsexual healthservicesacrosspractices
Linked to 2aabove
HealthboardGPs
November2016
Reduced waitingtimes and provisionof care closer to thepatient’s home
Some practices within the cluster alreadydeliver services for other practices and havethe capacity to extend this. Extending thisservice could allow provision of temporaryservices, whilst a GP is on maternity leave,for example, or to cover other staffing issuese.g. retirement.
In order to implement this, the following willneed to be in place:
• Treatment pathways will need to bealigned across the cluster
• Referral documents will need to bereviewed and agreed (pathwayalready drafted and submitted byAshgrove surgery)
• Processes will need to be defined,documented and communicated
• Referral mechanism will need to be inplace, using WCCG for consistency
18 | P a g e V 1 3
LHB to ensure this is kept up to-dateas more services are rolled out by thepractices/hub
See 3b.3e Develop a
shared carerecord for usebetweenPrimary andCommunityServices
NWISLHBGP Systemsuppliersi.e. INPS &EMIS
By March2017
Prevention ofduplication andimprovement ofcommunication.
Reducing risk topatients
This a dependency for a number of itemswithin the cluster plan
This development can be aligned to thework required by NWIS/Digital Developmentteam in 2a
19 | P a g e V 1 3
Strategic Aim 4: To provide high quality, consistent care for patients presenting with urgent care needsand to support the continuous development of services to improve patient experience, coordination ofcare and the effectiveness of risk management
No Objective Keypartners
Forcompletionby: -
Outcome forpatients
Progress to Date RAGRating
Re Strategic Aim 4:
All Taff Ely cluster practices are engaged with care pathways aimed at reducing emergency and elective unnecessary referrals to
Secondary Care/attendances at the Emergency Care Centre/Clinical decisions units. This follows on from prior annual Qof work.
20 | P a g e V 1 3
Strategic Aim 5: Improving the delivery of end of life care
No Objective Key partners Forcompletion by: -
Outcome forpatients
Progress to Date RAGRating
5a All practicesin the clusterto analysetheir palliativecarepresentations2014-2015QOF yearanddisseminatelessons learntandeducationalneedsidentified(seeAppendix 1below)
LHB
Individualcluster primarycare practiceteams
End March2016
Lessons learntfrom practiceanalysis of casesof palliativecare/end of lifecare analysedduring QOF year2014-2015 fedback into servicedevelopment andeducationaldevelopment whenrequired
All practices in the cluster engaged on inpractice national priority work on SEA ofend of life care presentations as pernationally agreed national priority work
Completed for 2014/15.
Completed for 2015/16
21 | P a g e V 1 3
5b Considereffectiveanalysis atpractice levelof end of lifecare andpalliative careregisters
Macmillan localcharityfundedresources
Clusterpractices
LHB resources
Third sectororganisations
September2015
Improved adoptedof EOL carepathways will leadto improved EOLcare for patients
• Implement an EOL care checklist acrossthe cluster, to ensure that all elements ofthe pathway have been considered andaddressed, where appropriate, for apalliative patient (template provided byOld School practice)
• Target early involvement by Macmillanstaff in the care of palliative patients –measure to be agreed with Macmillanteam
• Implement a communication skillsframework (to be developed incollaboration with Macmillan staff) acrossthe cluster for GPs to use whendiscussing EOL care with palliativepatients, to ensure that GPs are usingappropriate communication techniques
General guidance is available on Cwm Tafhealth board intranet. Discuss with healthboard replicating this advice on the GPportal and ensure that this includes usefulphone numbers / websites.
5c ContinueQOF 2014-2015individualclustermemberspracticepalliative care
IndividualCluster primarycare practiceteamsDistrict Nursingrepresentativesand palliativecare team
Ongoingindividualpracticework
Case reviewpatients identifyproactive end oflife planning forindividuals andadvice refuture/additionalmanagement of
Continues in progress every QOF year
22 | P a g e V 1 3
teammeetings
representatives the individual.Lessons learnedfor individualpatients will benefitand inform futurepatients care.
5d Increase useof JIC boxes
September2015
More timely controlof symptoms andmay reduce crisisadmissions andunplanned care
Check that all practices in cluster haveaccess to JIC system and that all relevantstaff are aware of the process.
.
23 | P a g e V 1 3
Strategic Aim 6: Targeting the prevention and early detection of cancers
No Objective Keypartners
Forcompletionby: -
Outcome forpatients
Progress to Date RAGRating
6a All practicesin the clusterto analysetheir cancerpresentations2014-2015QOF yearanddisseminatelessons learntandeducationalneeds (seeAppendix 3below)
LHB
ClusterGP’s andclusterprimary carehealthteams
End March2016
Lessons learnt frompractice analysis ofcases of canceranalysed duringQOF year 2014-2015 fed back intoservicedevelopment andeducationaldevelopment whenrequired
All practices in the cluster engaged on inpractice national priority work on SEA ofcancer presentations as per nationallyagreed national priority work.
Completed for 2014/15.
Completed for 2015/16
24 | P a g e V 1 3
Strategic Aim 7: Minimising the risk of poly-pharmacy
No Objective Keypartners
Forcompletionby: -
Outcome forpatients
Progress to Date RAGRating
7a Identify and
report the
number /% of
patients aged
86 years or
more
receiving 6 or
more
medications
(see
Appendix 2
below)
Lead GP ineach clusterpractice
LHBpharmacyadvisoryteam
End March2016
Decrease thepotential formedicationinteractions/morbidityby reviewing themedications currentlyprescribed againstpatients’ currentmedical conditionsand changes incondition relatedprescribingpractice/guidelinesi.e. optimisemedication andcondition.
Undertake face to face medication reviewsusing the NO TEARS approach or similartool for at least 60% of the cohort definedabove. Use the agreed read code forpolypharmacy review. All practices in thecluster are committed to completion of thiswork by end March 2015.
Completed for 2014/15.
Completed for 2015/16
25 | P a g e V 1 3
Strategic Aim 8: Deliver consistent, effective systems of Clinical Governance
No Objective Keypartners
Forcompletionby: -
Outcome forpatients
Progress to Date RAGRating
8a Engage witha robustvalidatedclinicalgovernanceprocessspecificallydesigned withclusterplanning inmind
Individualclusterpractices
PublicHealthWales
End March2016
Allmeasures/proposalsoutlined andassessed in avalidated all Walesclinical governancetool
Clinical Governance Practice SelfAssessment Tool(CGPSAT) each individual cluster memberwill be entering their areas of responsibilityinto their PDP’s (practice developmentplans) and CGPSAT.
Aspiration level 4/5 maturity on CGPSAT recluster network work.
Completed for 2014/15.
Completed for 2015/16
26 | P a g e V 1 3
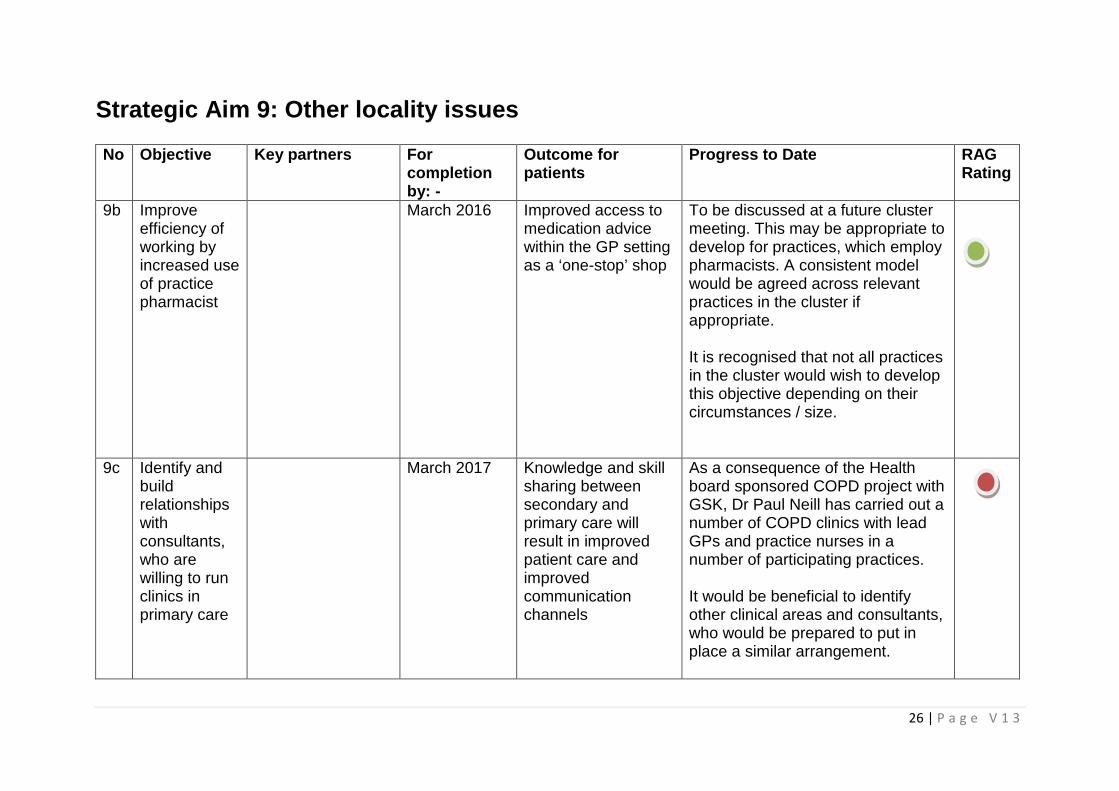
Strategic Aim 9: Other locality issues
No Objective Key partners Forcompletionby: -
Outcome forpatients
Progress to Date RAGRating
9b Improveefficiency ofworking byincreased useof practicepharmacist
March 2016 Improved access tomedication advicewithin the GP settingas a ‘one-stop’ shop
To be discussed at a future clustermeeting. This may be appropriate todevelop for practices, which employpharmacists. A consistent modelwould be agreed across relevantpractices in the cluster ifappropriate.
It is recognised that not all practicesin the cluster would wish to developthis objective depending on theircircumstances / size.
9c Identify andbuildrelationshipswithconsultants,who arewilling to runclinics inprimary care
March 2017 Knowledge and skillsharing betweensecondary andprimary care willresult in improvedpatient care andimprovedcommunicationchannels
As a consequence of the Healthboard sponsored COPD project withGSK, Dr Paul Neill has carried out anumber of COPD clinics with leadGPs and practice nurses in anumber of participating practices.
It would be beneficial to identifyother clinical areas and consultants,who would be prepared to put inplace a similar arrangement.
27 | P a g e V 1 3
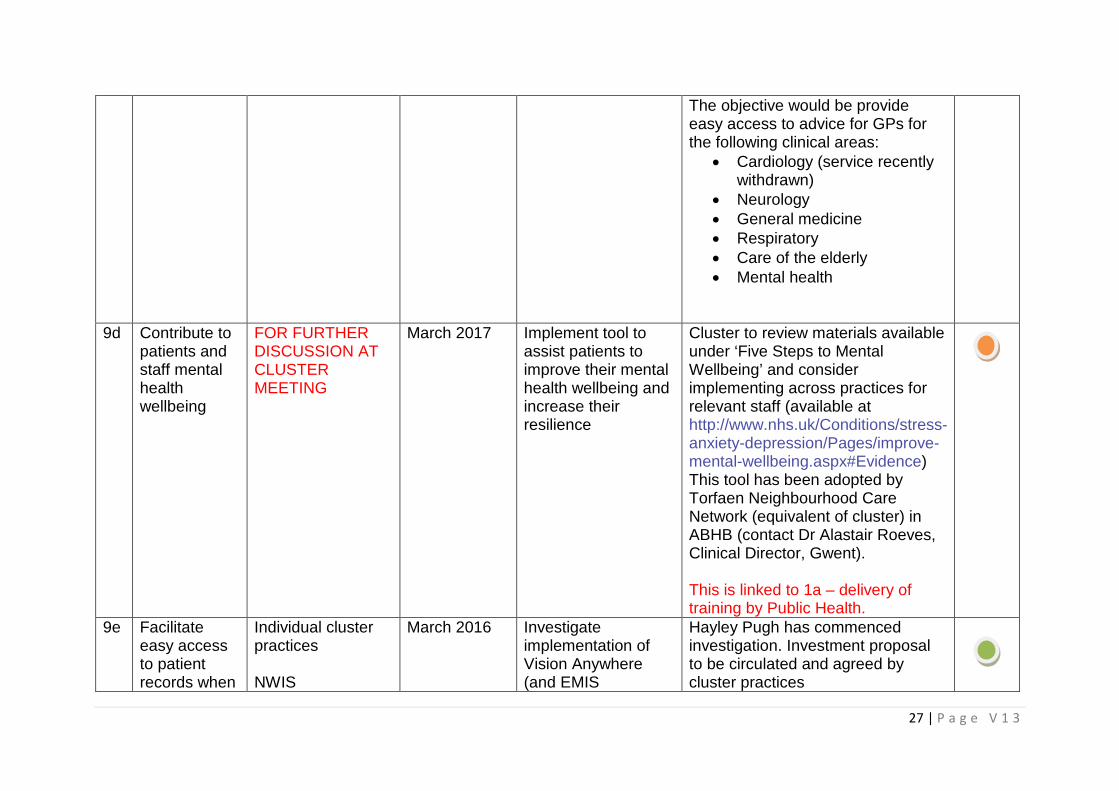
The objective would be provideeasy access to advice for GPs forthe following clinical areas:
• Cardiology (service recentlywithdrawn)
• Neurology• General medicine• Respiratory• Care of the elderly• Mental health
9d Contribute topatients andstaff mentalhealthwellbeing
FOR FURTHERDISCUSSION ATCLUSTERMEETING
March 2017 Implement tool toassist patients toimprove their mentalhealth wellbeing andincrease theirresilience
Cluster to review materials availableunder ‘Five Steps to MentalWellbeing’ and considerimplementing across practices forrelevant staff (available athttp://www.nhs.uk/Conditions/stress-anxiety-depression/Pages/improve-mental-wellbeing.aspx#Evidence)This tool has been adopted byTorfaen Neighbourhood CareNetwork (equivalent of cluster) inABHB (contact Dr Alastair Roeves,Clinical Director, Gwent).
This is linked to 1a – delivery oftraining by Public Health.
9e Facilitateeasy accessto patientrecords when
Individual clusterpractices
NWIS
March 2016 Investigateimplementation ofVision Anywhere(and EMIS
Hayley Pugh has commencedinvestigation. Investment proposalto be circulated and agreed bycluster practices
28 | P a g e V 1 3
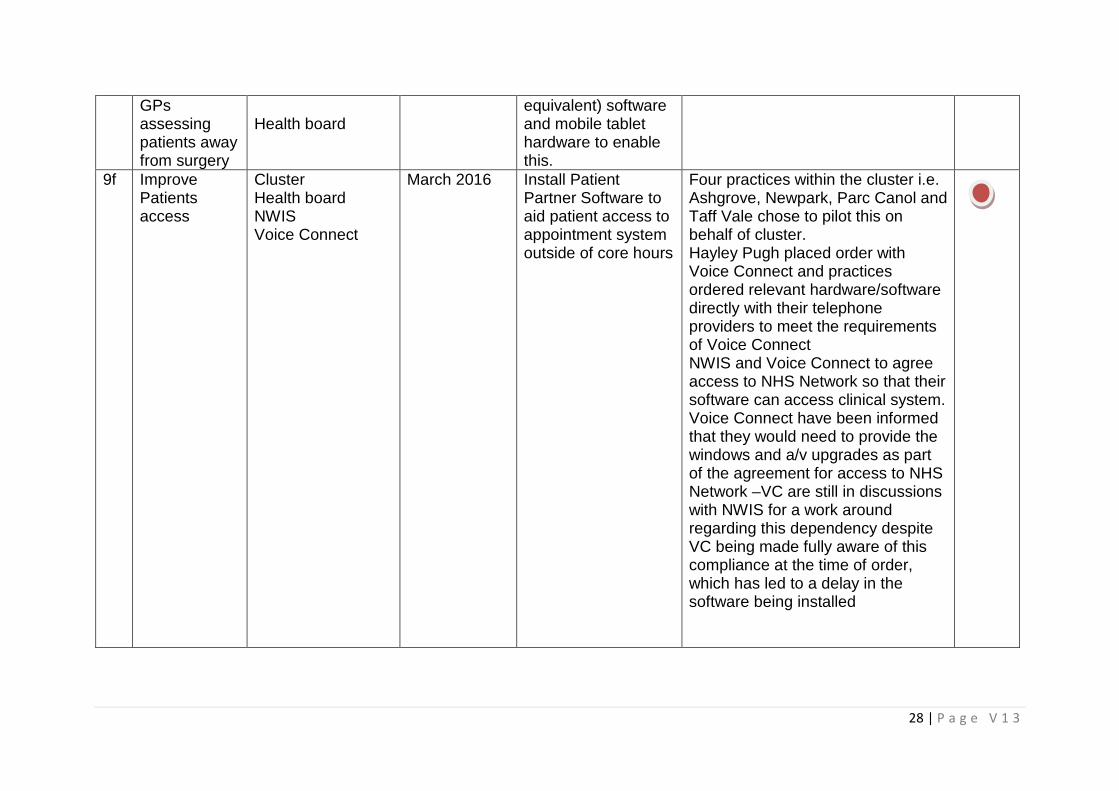
GPsassessingpatients awayfrom surgery
Health boardequivalent) softwareand mobile tablethardware to enablethis.
9f ImprovePatientsaccess
ClusterHealth boardNWISVoice Connect
March 2016 Install PatientPartner Software toaid patient access toappointment systemoutside of core hours
Four practices within the cluster i.e.Ashgrove, Newpark, Parc Canol andTaff Vale chose to pilot this onbehalf of cluster.Hayley Pugh placed order withVoice Connect and practicesordered relevant hardware/softwaredirectly with their telephoneproviders to meet the requirementsof Voice ConnectNWIS and Voice Connect to agreeaccess to NHS Network so that theirsoftware can access clinical system.Voice Connect have been informedthat they would need to provide thewindows and a/v upgrades as partof the agreement for access to NHSNetwork –VC are still in discussionswith NWIS for a work aroundregarding this dependency despiteVC being made fully aware of thiscompliance at the time of order,which has led to a delay in thesoftware being installed
29 | P a g e V 1 3
Appendix 1Lessons learnt from practice analysis of cases of palliative care/end of life care
No. Key issues Actions
1 Refer to submission for 2015-16
Appendix 2Lessons learnt from practice analysis minimising the risk of polypharmacy
No. Key issues Actions
1 Refer to submission for 2015-16
Appendix 3Lessons learnt from practice analysis of understanding cancer care pathways
No. Key issues Actions
1 Refer to submission for 2015-16
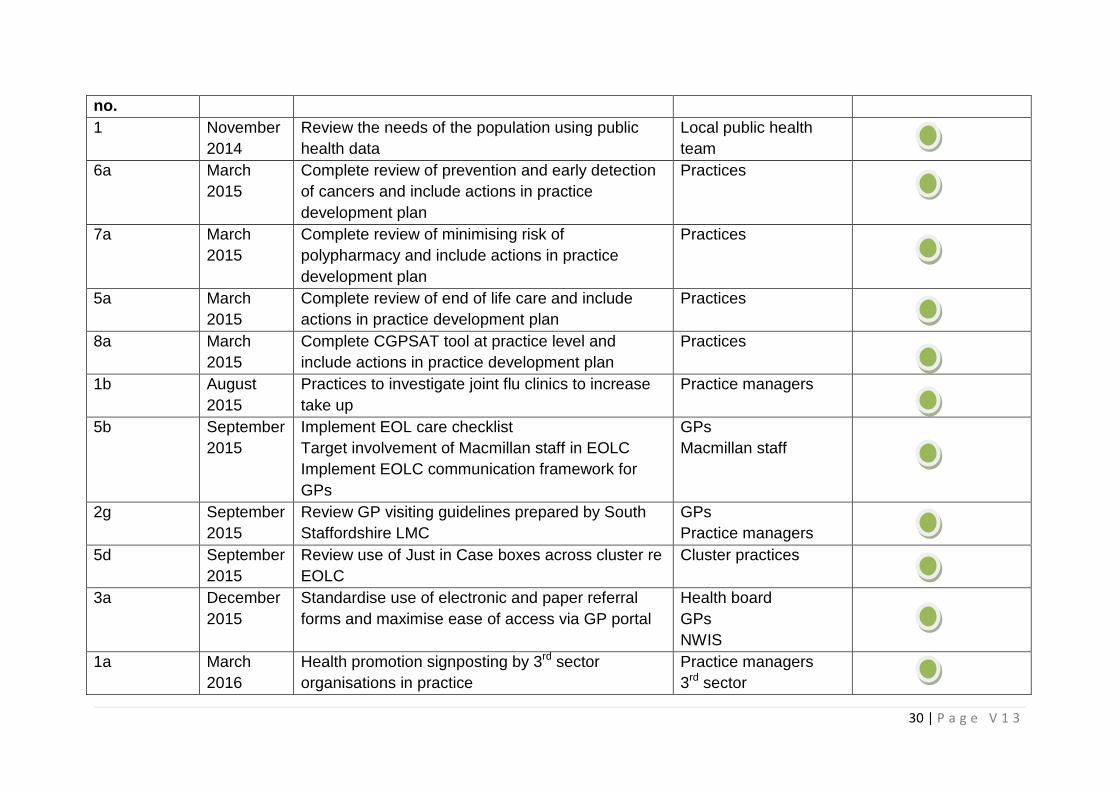
Appendix 3Action plan
Objective Date Action Responsible Status
30 | P a g e V 1 3
no.
1 November
2014
Review the needs of the population using public
health data
Local public health
team
6a March
2015
Complete review of prevention and early detection
of cancers and include actions in practice
development plan
Practices
7a March
2015
Complete review of minimising risk of
polypharmacy and include actions in practice
development plan
Practices
5a March
2015
Complete review of end of life care and include
actions in practice development plan
Practices
8a March
2015
Complete CGPSAT tool at practice level and
include actions in practice development plan
Practices
1b August
2015
Practices to investigate joint flu clinics to increase
take up
Practice managers
5b September
2015
Implement EOL care checklist
Target involvement of Macmillan staff in EOLC
Implement EOLC communication framework for
GPs
GPs
Macmillan staff
2g September
2015
Review GP visiting guidelines prepared by South
Staffordshire LMC
GPs
Practice managers
5d September
2015
Review use of Just in Case boxes across cluster re
EOLC
Cluster practices
3a December
2015
Standardise use of electronic and paper referral
forms and maximise ease of access via GP portal
Health board
GPs
NWIS
1a March
2016
Health promotion signposting by 3rd sector
organisations in practice
Practice managers
3rd sector
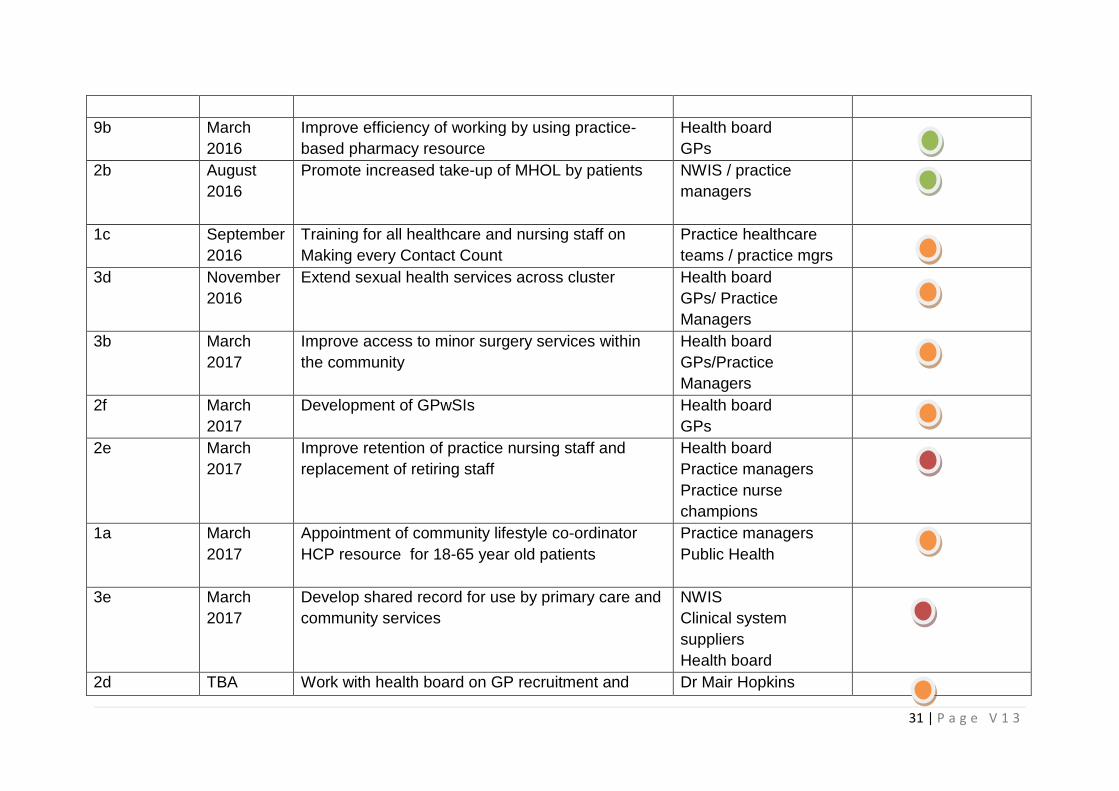
31 | P a g e V 1 3
9b March
2016
Improve efficiency of working by using practice-
based pharmacy resource
Health board
GPs
2b August
2016
Promote increased take-up of MHOL by patients NWIS / practice
managers
1c September
2016
Training for all healthcare and nursing staff on
Making every Contact Count
Practice healthcare
teams / practice mgrs
3d November
2016
Extend sexual health services across cluster Health board
GPs/ Practice
Managers
3b March
2017
Improve access to minor surgery services within
the community
Health board
GPs/Practice
Managers
2f March
2017
Development of GPwSIs Health board
GPs
2e March
2017
Improve retention of practice nursing staff and
replacement of retiring staff
Health board
Practice managers
Practice nurse
champions
1a March
2017
Appointment of community lifestyle co-ordinator
HCP resource for 18-65 year old patients
Practice managers
Public Health
3e March
2017
Develop shared record for use by primary care and
community services
NWIS
Clinical system
suppliers
Health board
2d TBA Work with health board on GP recruitment and Dr Mair Hopkins
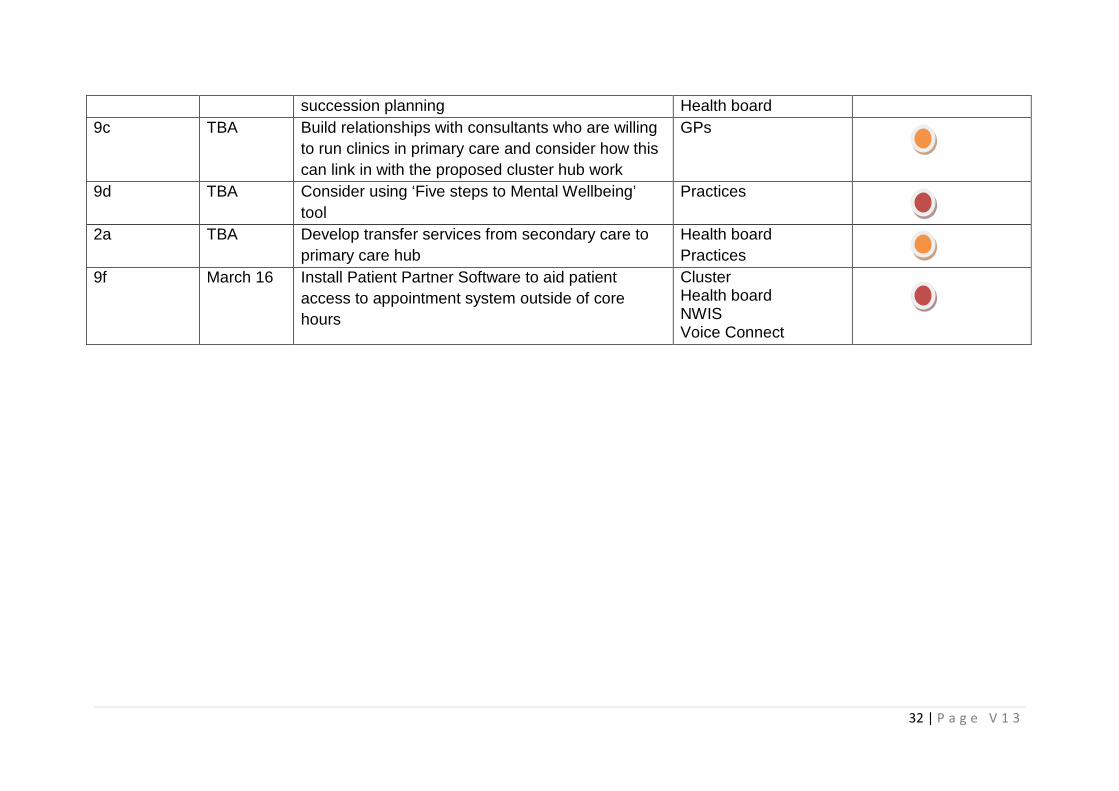
32 | P a g e V 1 3
succession planning Health board
9c TBA Build relationships with consultants who are willing
to run clinics in primary care and consider how this
can link in with the proposed cluster hub work
GPs
9d TBA Consider using ‘Five steps to Mental Wellbeing’
tool
Practices
2a TBA Develop transfer services from secondary care to
primary care hub
Health board
Practices
9f March 16 Install Patient Partner Software to aid patient
access to appointment system outside of core
hours
ClusterHealth boardNWISVoice Connect