TACTIC PROJECT 2: THE ROLE OF FACTOR XI IN TIC LEAD INVESTIGATOR: SAULIUS BUTENAS (UNIVERSITY OF...
20
TACTIC PROJECT 2: THE ROLE OF FACTOR XI IN TIC LEAD INVESTIGATOR: SAULIUS BUTENAS (UNIVERSITY OF VERMONT) CO-INVESTIGATOR: JAMES H MORRISSEY (UNIVERSITY OF ILLINOIS AT URBANA- CHAMPAIGN) PHILADELPHIA, SEPTEMBER 10, 2014 a
-
Upload
ginger-dickerson -
Category
Documents
-
view
215 -
download
0
Transcript of TACTIC PROJECT 2: THE ROLE OF FACTOR XI IN TIC LEAD INVESTIGATOR: SAULIUS BUTENAS (UNIVERSITY OF...

TACTIC PROJECT 2: THE ROLE OF FACTOR XI IN TIC
LEAD INVESTIGATOR: SAULIUS BUTENAS (UNIVERSITY OF VERMONT)
CO-INVESTIGATOR: JAMES H MORRISSEY (UNIVERSITY OF ILLINOIS AT URBANA-CHAMPAIGN)
PHILADELPHIA, SEPTEMBER 10, 2014
a

The Coagulation CascadeIntrinsic Pathway
Factor XIIPrekallikrein
HMW Kininogen“Surface”
Factor XIaHMW Kininogen
MembraneCa2+, Zn2+
Intrinsic Tenase
AT-III
AT-III
IIa
XIa
Vai
VIIIai
XIIa
IXa
Extrinsic Pathway
Factor VIIaTissue Factor
MembraneCa2+
Factor IXaFactor VIIIaMembrane
Ca2+
Factor XaFactor Va
MembraneCa2+
ThrombinThrombomodulin
MembraneCa2+
Fibrin Clot Formation
Extrinsic Tenase
Prothrombinase
Cross-LinkedFibrin Clot
Soluble Fibrin Peptides
TFPIAT-III
PAI-1
AT-III
TAFIa
Plasmin
APC
2-AP
AT-III
XIIIa
FibrinIIa
Xa Xa
IXa
TFPIAT-III
Red = EnzymesYellow = Inhibitors
VascularInjury
Tissue Factor
IIaVaVIIIa

FXIa-Initiated Clotting of Whole Blood
5 pM TF 50 pM XIa 10 pM XIa 5 pM XIa 1 pM XIa 0.5 pM XIa 0.1 pM XIa0
125
250
375
500
625
750
Clot
Tim
e (s
)
Initiator Concentration

Assays for FXIa
Clotting and thrombin generation (TGA) assays were developed.
Both assays are based on the response of contact pathway-inhibited (corn trypsin inhibitor; CTI) plasma to the inhibitory anti-FXI monoclonal antibody.
No exogenous initiator of thrombin
generation is added. No thrombin generation/clot formation is
observed in plasma from healthy individuals

Study #1(In collaboration with Dr. M. Park from Mayo Clinic)
Multiple time-points from 98 patients: Burn 34 Blunt 47 Penetrating 17
Clotting assay was used for the quantitation of FXIa
Supported by DoD and PO1 HL46703
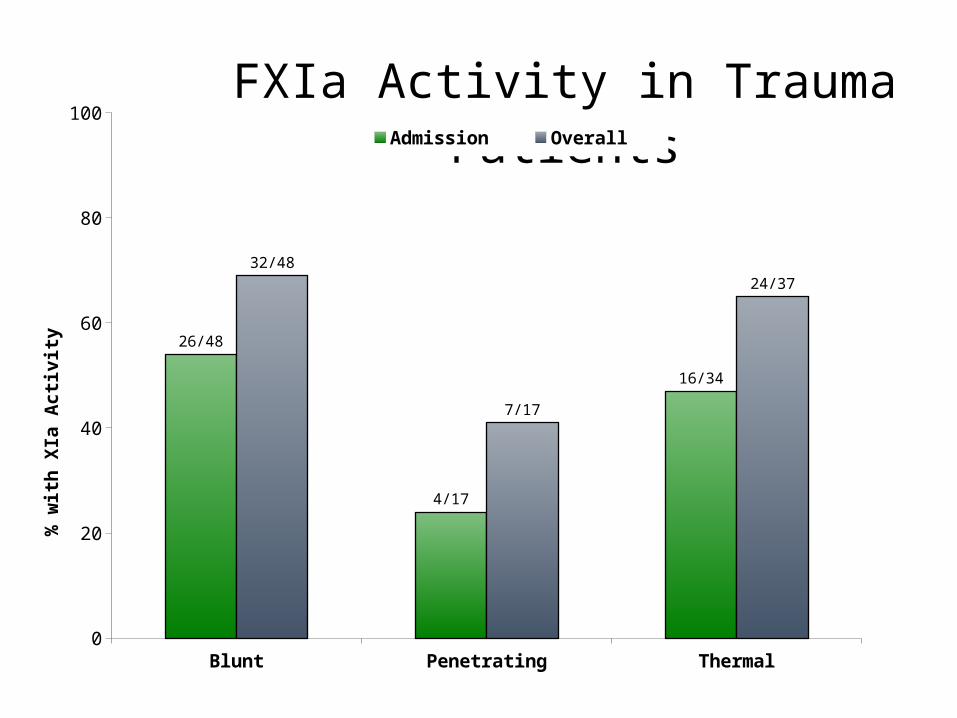
Blunt Penetrating Thermal0
20
40
60
80
100
26/48
4/17
16/34
32/48
7/17
24/37
FXIa Activity in Trauma PatientsAdmission Overall
% w
ith
XIa
Acti
vity
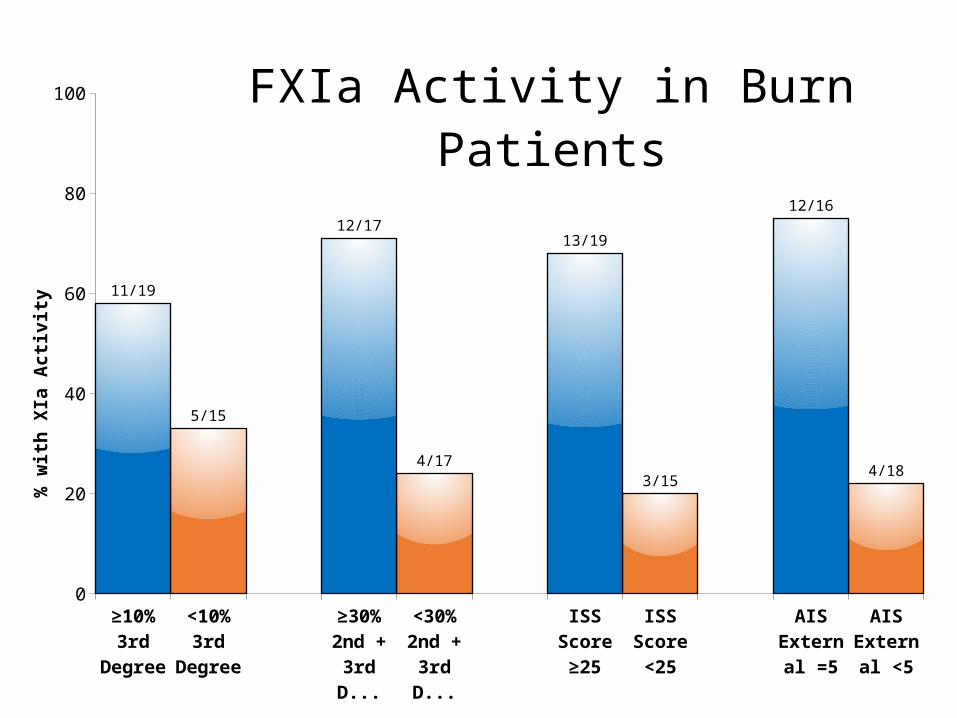
≥10% 3rd
Degree
<10% 3rd
Degree
≥30% 2nd + 3rd
Degree
<30% 2nd + 3rd
Degree
ISS Score ≥25
ISS Score <25
AIS Ex-ternal =5
AIS Ex-ternal <5
0
20
40
60
80
100
11/19
5/15
12/17
4/17
13/19
3/15
12/16
4/18
FXIa Activity in Burn Patients%
wit
h XI
a A
ctivi
ty

ISS Score ≥25 ISS Score <25 Head/Neck ≥4 Head/Neck <40
20
40
60
80
100
18/27
8/20
18/27
8/20
FXIa Activity in Blunt Patients%
wit
h XI
a A
ctivi
ty

Blunt Penetrating Thermal0
20
40
60
80
100
3/4
0/1
6/1120/36
4/10
9/203/7
0/2 0/0
FXIa Activity in All PatientsD L T
% w
ith
XIa
Acti
vity

*ISS – injury severity score.**Average ± SD for patients with FXIa ≥ 10 pM. Detectabiliy limit of FXIa in this clotting time-based assay is 10 pM.
S. Butenas, M. Park, K. Mann (unpublished data).
Active Factor XIa at Admission
Injury
ISS* > 25 ISS ≤ 25
XIa
Frequency (pM)** Frequency (pM)
Burn 13/19 (68%) 38±36 3/15 (20%) 47±7
Blunt 19/31 (61%) 39±28 7/16 (44%) 37±26
Penetrating 3/7 (43%) 55±65 1/10 (10%) 160

Conclusion #1
The occurrence of FXIa correlates with the severity of trauma


Study #2 (In collaboration with Dr. J. Shupp from Washington Burn Center)
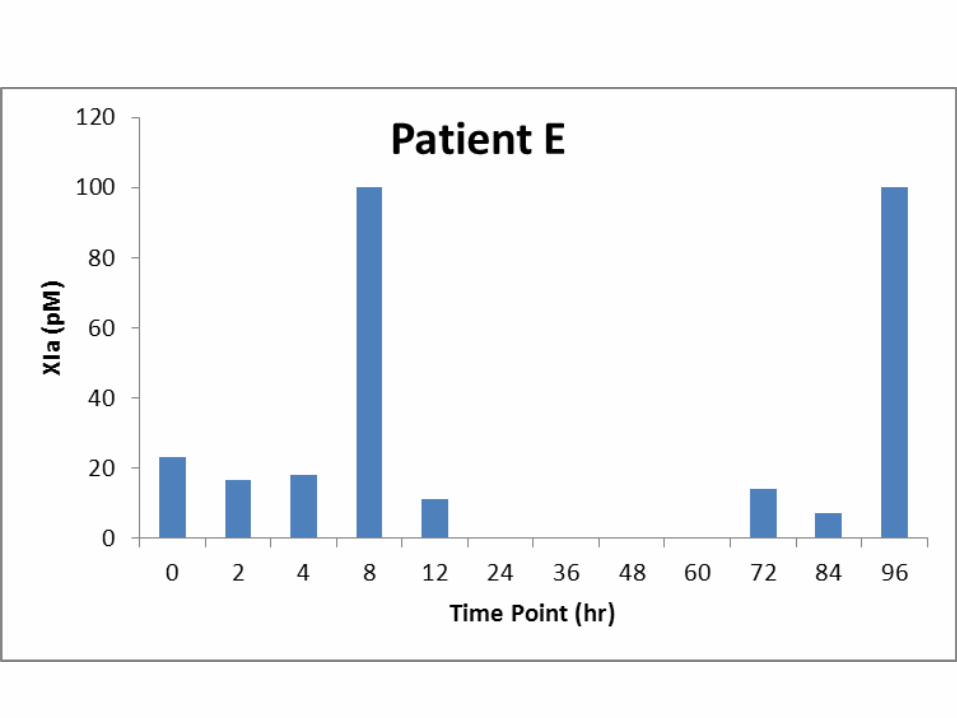
56 Burn patients 463 time-points Up to 20 time-points per patient from 0 to 504
hours (3 weeks)
Thrombin Generation assay was used for the quantitation of FXIa
Supported by Systems Biology grant




Conclusion #2
Of 56 burn patients analyzed:62% had TF and 100% had FXIa at at least one time-point.
TF activity was observed in 21% and FXIa in 90% time-point samples.
Study #3 (In collaboration with Dr. K. Freeman from FAHC, Burlington VT)
Multiple time-point plasma samples from 66 patients (no burn patients; 187 time-points)
56% of them had TF and 94% had FXIa at at least one time-point.
TF activity was observed in 30% and FXIa in
79% time-point samples.
Thrombin Generation assay was used for the quantitation of FXIa
Supported by Systems Biology grant
Final Conclusions
The majority of trauma patients have circulating FXIa, which correlates with trauma severity.
FXIa concentration over observation time varies in a wide range.
The frequency of FXIa in burn patients is higher than in other trauma patient categories
FXIa could be a potential marker of trauma severity