
Table of Contents Document Page 7 06.1 MCCG … PCCC...Table of Contents Document Page 1 01 PT1 PCCC...
104
Table of Contents Document Page 1 01 PT1 PCCC October 2018 AGENDA 3 2 02 MPCCC Register of Interest 2018-19 August 2018 5 3 03.1 PT1 PCCC June 2018 minutes 11 4 03.2 PMCPG_Executive summary 15 5 05.1 PART 1 Integrated Primary Care Commissioning Update 21 6 05.2 M5 Merton Primary Care Committee Finance Update 29 7 06.1 MCCG PCC GP Pt Survey 2018 37 8 06.2 08R - NHS MERTON CCG GP Survey 47 9 07.1 Merton Primary Care Committee Estates Update_cover 99 10 07.2 Merton CCG_PCCC_ Estates Update.docx 101
Transcript of Table of Contents Document Page 7 06.1 MCCG … PCCC...Table of Contents Document Page 1 01 PT1 PCCC...
Table of Contents
Document Page
1 01 PT1 PCCC October 2018 AGENDA 32 02 MPCCC Register of Interest 2018-19 August 2018 53 03.1 PT1 PCCC June 2018 minutes 114 03.2 PMCPG_Executive summary 155 05.1 PART 1 Integrated Primary Care Commissioning Update 216 05.2 M5 Merton Primary Care Committee Finance Update 297 06.1 MCCG PCC GP Pt Survey 2018 378 06.2 08R - NHS MERTON CCG GP Survey 479 07.1 Merton Primary Care Committee Estates Update_cover 9910 07.2 Merton CCG_PCCC_ Estates Update.docx 101

This page has been left blank

1
MERTON CLINICAL COMMISSIONING GROUP PRIMARY CARE COMMISSIONING COMMITTEE
Tuesday 2rd October 2018
13.00 – 14:00
Rm. 6.2, 6th Floor. 120 The Broadway, Wimbledon, SW19 1RH
Part 1
Questions from the public are received at the discretion of the Chair.
Closure of Part 1 To resolve that the public now be excluded from the meeting, on the basis that publicity would be prejudicial to the public interest by reason of the confidential nature of the business to be conducted in the second part of the agenda.
Chair: Clare Gummett
No. Item Description Lead For Att./
Verbal
1 Welcome and Apologies CG Note Verbal
2 Conflicts of Interest All Note Att 1
3 Minutes of Part 1 of the Primary Care Commissioning Committee 05.06.18
All Approval Att 2
4 Matters Arising All Note Verbal
5 Integrated Primary Care Commissioning Update inc. Finance Report
KS & NM
Information Att 3
6 GP Patient Survey Report EG Note
7 Primary Care Estates Update LL Note
8 Any Other Business All Note Verbal
3 of 104

This page has been left blank

Name
Current position (s) held in the
CCG i.e. Governing Body
member; Committee member;
Member practice; CCG employee
or other
Do you
have any
interests
to
declare?
(Y or N)
Declared Interest
(Name of the organisation and nature of business)
Fin
an
cia
l In
tere
st
No
n-F
ina
nc
ial
pro
fes
sio
na
l
Inte
res
t
No
n-F
ina
nc
ial
Pe
rso
na
l In
tere
st
Ind
ire
ct
Inte
res
t
Nature of Interest
From To
Action taken to
mitigate risk
Dr Andrew Murray Clinical Chair of MCCG
Chair of Governing Body
Joint Chair Clinical Oversight Group
Member of Remuneration Committee
Member of Executive Management
Team
Member of Finance Committee in
Common
Member (non-voting) of Primary Care
Commissioning Committee
Chair of South West London Clinical
Senate
Chair of Merton Planned Care
Programme Board
Co-Chair Integrated Governance and
Quality Committee
Y
1. GP Partner in The Nelson Medical Practice operating out of the Nelson
Health Centre.
2. Chair of Executive Management Team at Nelson.
3. Wife helped establish Merton Against Trafficking (local anti-people
trafficking) for which I have done some volunteer work.
4. A close friend set up Chapel Street (Charity) – this runs some services
for NHS, but not in Merton.
5. Same friend also set up “For Refugees” – a national initiative aimed at
supporting refugees moving to UK.
6. Regular attendee of Raynes Park Community Church, a member of
Merton Citizens, a community movement whose campaign areas include
mental health services for children and young.
1
6
3
4
5
1. Apr 2015
2. Apr 2015
3. Sept 2008
4. 2010
5. 2016
4. March
2017
Adherence to COI
policy
James Blythe Managing Director
Governing Body Member
Member of Executive Management
Team
Member of Primary Care
Commissioning Committee
Member of Finance Committee in
Common
Member of Integrated Governance
Quality Committee
Y
1. Wife is an employee of St George's University Hospitals NHS
Foundation Trust and has a specialist training number with HEE South
London
1 1. May 2017 1. I am not present
at specific
discussions relating
to the relevant
service.
Register of Interests 2018/19 (updated September 2018)
5 of 104

Name
Current position (s) held in the
CCG i.e. Governing Body
member; Committee member;
Member practice; CCG employee
or other
Do you
have any
interests
to
declare?
(Y or N)
Declared Interest
(Name of the organisation and nature of business)
Fin
an
cia
l In
tere
st
No
n-F
ina
nc
ial
pro
fes
sio
na
l
Inte
res
t
No
n-F
ina
nc
ial
Pe
rso
na
l In
tere
st
Ind
ire
ct
Inte
res
t
Nature of Interest
From To
Action taken to
mitigate risk
Clare Gummett Governing Body Lay Member for
Patient & Public Engagement
Member of Integrated Governance and
Quality Committee
Chair of Primary Care Commissioning
Committee
Member of Audit & Governance
Committee
Member of Remuneration Committee
Member of Sutton & Merton CCGs
Charitable Trust
Member of Patient Engagement Group
Member of Merton Equality & Diversity
Group
Y
1. Age UK Merton – Chair of Trustees 1. Jan 2014 Adherence to COI
policy
Andrew Leigh Governing Body Lay Member for Audit
& Governance
Chair of Audit & Governance
Committee
Member of Governing Body
Member of Remuneraton committee
Member of Primary Care
Commissioning Committee
Member of Integrated Governance
Quality Committee
Y
1. Director of Maynard Leigh Associates (MLA), and Chair of Leadership
Team. MLA runs training courses; NHS employees occasionally attend.
2. Manage a non for profit web site called Ethical Leadership.
3. Wife is Deputy Chair of Sustainable Merton
1
2?
3
1. Nov 2017
2. Nov 2017
3. Current
all ongoing 1. Avoid voting on
items about
Leadership Training
contracts for which
Maynard Leigh
might bid.
2. A not-for profit
site; does not trade
commercially.
6 of 104

Name
Current position (s) held in the
CCG i.e. Governing Body
member; Committee member;
Member practice; CCG employee
or other
Do you
have any
interests
to
declare?
(Y or N)
Declared Interest
(Name of the organisation and nature of business)
Fin
an
cia
l In
tere
st
No
n-F
ina
nc
ial
pro
fes
sio
na
l
Inte
res
t
No
n-F
ina
nc
ial
Pe
rso
na
l In
tere
st
Ind
ire
ct
Inte
res
t
Nature of Interest
From To
Action taken to
mitigate risk
Dr Tim Hodgson GP Governing Body Member
Joint West Merton Locality Lead
Member of Integrated Governance and
Quality Committee
Member of Finance Committee in
Common
Member of Clinical Oversight Group
Member of Primary Care
Commissioning CommitteeY
1. GP Partner – Wimbledon Village Surgery (Member of Merton
Federation)
1 Apr-17 Apr-19 Adherence to COI
policy
Dr Karen
Worthington
GP Governing Body Member
Member of Clinical Oversight Group
Member of Integrated Governance and
Quality Committee
Member of Finance Committee in
Common
Clinical Director for transforming
Primary care
Member of Merton Health and
Wellbeing board
Y
1. Part time salaried GP at Central Medical Centre. 2 days per week
2. Part time staff bank member-clinical support to clinical harm review
at St Georges Hospital. Training undertaken but no work done.
1.
2.
1.12/06/16
2. 24/4/17 2. 24/04/18
Adherence to COI
policy
Dr Mike Greenberg Governing Body Secondary Care
Member
Member of Primary Care
Commissioning Committee
Member of Audit & Governance
Committee
Y
1. Medical Director of Barnet Hospital (part of Royal Free London Group)
2. Member of Wellington Diagnostics and Outpatient Centre LLP
3. Wife is a GP in Barnet and a Board member of Barnet Federation of
GPs.
2
1
3
1. 01/04/2018
2. 01/04/2018
3. 01/04/2018
Adherence to COI
policy
7 of 104

Name
Current position (s) held in the
CCG i.e. Governing Body
member; Committee member;
Member practice; CCG employee
or other
Do you
have any
interests
to
declare?
(Y or N)
Declared Interest
(Name of the organisation and nature of business)
Fin
an
cia
l In
tere
st
No
n-F
ina
nc
ial
pro
fes
sio
na
l
Inte
res
t
No
n-F
ina
nc
ial
Pe
rso
na
l In
tere
st
Ind
ire
ct
Inte
res
t
Nature of Interest
From To
Action taken to
mitigate risk
Dagmar Zeuner Director of Public Health (LBM)
Member of Governing Body
Director for Preventative and Proactive
Care
Member of Clinical Oversight Group
Member of CCG Clinical Cabinet
Member of Primary Care Committee Y
1. Director of Public Health, LBM
In this role potential / perceived conflict of interest re any decision
about future of St Helier’s Hospital.
2. Partner is owner of ZG publishing (publishes the magazine: “Outdoor
Swimmer”).
3. Honorary senior lecturer at the London School of Hygiene and
Tropical Medicine.
4. Research advisor (occasional) for University of London/Institute of
Child Health.
1
3
2
1. Feb 2016
2. Feb 2011
3. Apr 2006
4. Apr 2010
1. Not being a
member of the CIC,
being excluded
from any decision
making on the
future of St Helier,
which includes
circulation of
related
unpublished
papers.
Neil McDowell Director of Finance
Member of Governing Body
Member of Finance Committee
Member of Audit & Governance
Committee
Member of Primary Care
Commissioning Committee
Member of Executive Management
Committee
Member of Integrated Governance and
Quality Committee
Y
1. Spouse employed by Guildford and Waverley CCG as CFO Adherence to COI
policy
Julie Hesketh Director of Quality and Corporate
Governance
Member of Governing Body
Member of Executive Management
Committee
Member of Integrated Governance and
Quality Committee
Member of Audit and Governance
Committee
Y
1. Personal involvement in Richmond Education Network (not for profit
organisation). This is done outside of CCG hours.
Adherence to COI
policy
Katharine Denton Director of Primary Care
Transformation
N
No interests declared Adherence to COI
policy
8 of 104

Name
Current position (s) held in the
CCG i.e. Governing Body
member; Committee member;
Member practice; CCG employee
or other
Do you
have any
interests
to
declare?
(Y or N)
Declared Interest
(Name of the organisation and nature of business)
Fin
an
cia
l In
tere
st
No
n-F
ina
nc
ial
pro
fes
sio
na
l
Inte
res
t
No
n-F
ina
nc
ial
Pe
rso
na
l In
tere
st
Ind
ire
ct
Inte
res
t
Nature of Interest
From To
Action taken to
mitigate risk
John Atherton Director of Performance Improvement
Member of Governing Body
Member of Primary Care
Commissioning Committee
Member of Integrated Governance and
Quality Committee
Member of Executive Management
Committee
N
No interests declared Adherence to COI
policy
Josh Potter Director of Commissioning Member
of Governing Body
Member of Executive Management
Committee
Member of Primary Care
Commissioning Committee
Member of Integrated Governance
and Quality Committee
N
No interests declared Adherence to COI
policy
Dr Marek
Jarzembowski
Local Medical Committee
Representative
Chair of Merton Local Medical
Committee
Y
1. Partner in the Nelson Medical Practice partnership, operating from
the Nelson Health Centre.
2. Member of Merton Health Ltd (Federation) by dint of being a partner
in the Nelson Medical Practice.
3. Member of the Board of Directors of Londonwide LMCs.
4. Chair of Merton Local Medical Committee.
1 1. April 2015
3. March 2015
4. 2016
Adherence to COI
policy
9 of 104

Name
Current position (s) held in the
CCG i.e. Governing Body
member; Committee member;
Member practice; CCG employee
or other
Do you
have any
interests
to
declare?
(Y or N)
Declared Interest
(Name of the organisation and nature of business)
Fin
an
cia
l In
tere
st
No
n-F
ina
nc
ial
pro
fes
sio
na
l
Inte
res
t
No
n-F
ina
nc
ial
Pe
rso
na
l In
tere
st
Ind
ire
ct
Inte
res
t
Nature of Interest
From To
Action taken to
mitigate risk
10 of 104

Page 1 of 4
Minutes of the Merton Clinical Commissioning Group
Primary Care Commissioning Committee Meeting
Tuesday 5th June 2018, 120, The Broadway, Wimbledon, SW19 1RH
Chair: Clare Gummett
Members:
Clare Gummett (CG) Chair, Governing Body Lay Member for PPI
Neil McDowell (NM) Director of Finance
Andrew Leigh (AL) Governing Body Lay Member for Audit & Governance
Andy McMylor (AMc) Director of Primary Care Transformation
Julie Hesketh (JH) Director of Quality & Governance
Dr Mike Greenberg (MG) Secondary Care Governing Body Member
Attendees:
Dr Dagmar Zeuner (DZ) Director of Public Health
Dr Tim Hodgson (TH) Clinical Locality Lead, West Merton
Dr Marek Jarzembowski (MJ) Chair, Merton Local Medical Committee
Dr Andrew Murray (AM) Chair of the Governing Body
Nora Simon (NS) Deputy Head of Primary Care Commissioning, NHSE
Rebecca Blackburn (RB)
Lucy Lewis (LL) Head of Estates, Merton and Wandsworth CCGs
Apologies:
James Blythe (JB) Managing Director
Kate Symons (KS) Acting Head of Delegated Primary Care Commissioning
Officer in Attendance:
Tony Foote (TF) NELCSU
Muna Ahmed (MA) Interim Governance Officer
11 of 104

Page 2 of 4
No. Item Action
1.
Welcome and Apologies
CG welcomed all and noted the apologies as above. The meeting was quorate. CG thanked TF for all his hard work in managing the committee and introduced MA, who will be taking this role on from TF.
2. Conflicts of Interest
DZ declared that she works for Merton Council and would be conflicted if there were any decisions to be made regarding Epsom and St Helier.
3. Notes of Meeting on 24th April 2018
The minutes of 24th April 2018 were APPROVED as a full and accurate record, subject to the attendees list being updated to include DZ, who was in attendance.
4. Matters Arising and Action Log
There were no matters arising from the minutes. Action log Action 5 – AMc confirmed that as part of the Primary Care at Scale, there will be practice support teams. The overarching contract will now include complaints.
5. Integrated Primary Care Commissioning Update including Finance Report
Rowans Surgery CQC report The Rowans Surgery was inspected by the CQC on 27th February 2018. The current provider Streatham Common Practice had only been in place for four months. Four of the five key domains were identified as “Requires improvement”. It was acknowledged that there were legacy issues with the practice. The domain “Effective” was rated as “Good”. The practice has since recruited 2.6 WTE GPs and has a good medicines management system in place. CCG and NHSE team will visit the practice to address quality areas of concern. A follow up inspection is usually carried out after 6 months and is likely to be a desktop inspection. The practice will develop an improvement action plan which is monitored at the Primary Care Quality Committee. DZ advised the committee to ensure participation of the local authority is included in the action plan, for assurance around safeguarding. JH confirmed an update on safeguarding goes to the Safeguarding Committee. Updates to the NHS England Primary Care Policy Guidance Manual (PGM) NS provided a brief summary of the PGM and explained that existing policies were pulled together into one document. NS highlighted what is in the manual:
- NHS England’s responsibilities
- CCG delegated commissioning responsibilities
12 of 104

Page 3 of 4
- Contract Management
- Assurance Framework
- Issuing breach notices
- Local payments and reimbursements
There was a discussion about the new chapter on discretionary payments. NS explained that this relates to the section 96 payment. Sickness and maternity leave is no longer discretionary and will be an entitlement. Joint Primary Care Quality Review Group (PCQRG) Update There was a review on how the joint PCQRG is going. There was general consensus that it is a helpful and useful forum to discuss how we communicate with the membership, provided input and made changes to “Make a difference”, contract management and going forward, formulate which areas to target in quality. It was felt that there is scope for learning from Wandsworth. AMc added that it is useful to review the CQC inspections with the expertise in the meeting. With the quality contract starting, AMc would like to invite the Federation to the meetings. Learning events for Merton will be held over the summer. There was a discussion about a dashboard for quality in Primary Care. The CSU has been asked to develop a dashboard for primary care which incorporates practice variation and quality contracts. The aim is to have data in one place. Primary Care contracting decisions NS highlighted an error in the paper, as the contract variations are for the whole of 2017/18 and not for quarter 1, as stated.
Action: An executive summary of the NHS England Primary Care Policy Guidance Manual to be circulated to the committee.
The Committee NOTED the Integrated Primary Care Commissioning Paper.
Finance Report NM presented this report and highlighted the following points:
- The end of year 2017/18 position for primary care was an under spend of
£1m.
- The primary care budget has been approved by the Board.
- James O’Riordan practice transfer with Sutton is ongoing. 1st July is the
official move date.
- Month 12 position is similar to month 11. Prescribing performed well
overall with an under spend of £704k, despite the “No Cheaper Stock”
13 of 104

Page 4 of 4
(NCSO) issue. MJ advised that a reduction in cost for prescribing should
not mean a reduction in the quality of prescribing.
- Out of hours had an unusual under spend. NM will look into why this is
the case. AMu queried whether the under spend in out of hours is due to
the GP Access Hubs. AMc will ask STP to provide more information on
this.
- There has been an increase in locum fees and will be a cost pressure in
2018/19.
MJ queried the over spend of £102k in Quality and Outcomes Framework (QOF) payments. It was explained that there was temporary protection for Rowans and also the QOF final achievement is based on the list size, as it is on 1st January.
2018/19 budget report:
- Going forward, NM will make a distinction in the report between
transformation funding and business as usual funding.
- NM asked for feedback on how the finance report can be improved and
what the committee would like to see that is different from Board finance
report. A committee member asked for the “Other” category in the
finance report to be broken down, for transparency and clarity.
The Committee NOTED the Finance Report on the Primary Care Budgets. -
6. Any Other Business
There was a discussion about how the committee is publicised to the public. It was queried whether this meeting should be filmed, like the Governing Body. There was no additional business for consideration. CG thanked all present for their input and declared Part 1 of the meeting closed.
Date of Next Meeting: Tuesday 2nd October 2018, 1-3pm
14 of 104

1 | P a g e
Executive summary - Primary Medical Care Policy and
Guidance Manual (PGM) This policy and guidance manual has been updated to reflect the changing landscape in
primary care co-commissioning.
In 2016, the ‘Policy Book’ for Primary Medical Services was published (Gateway Ref 04171),
which provided commissioners of GP services with the context, information and tools to
commission and manage GP contracts.
As part of the co-commissioning strategy, as at 1 April 2017, 176 Clinical Commissioning
Groups (CCGs) have responsibility for commissioning and contract monitoring GP services in
their locality, with NHS England maintaining overall accountability. Local Offices of NHS
England retain responsibility for commissioning and monitoring the performance of GP
services for the remaining CCGs.
Recognising the need to strengthen guidance for CCG commissioners, NHS England
reviewed its Policy Book and the feedback received since its first publication and has made
the following additions and amendments and published herewith in this ‘Primary Medical Care
Policy and Guidance Manual (PGM).
The PGM has been divided into 4 parts (A-D). The language throughout has been amended
to cover all commissioners, recognising 85% of CCGs are now operating under fully delegated
authority or joint arrangements. Reflecting feedback, templates have been embedded as
extractable documents for easier onward use.
Part A – Excellent Commissioning and Partnership Working 1 Introduction – providing some background information to updated policy
2 Abbreviations and Acronyms – List of abbreviations and acronyms used throughout
the document
3 Commissioning Described – in this section co-commissioning and delegated
commissioning arrangements are explained
4 General Duties of NHS England (including addressing health inequalities) This chapter
outlines the general duties that NHS England must comply with that are likely to affect
the decisions it takes regarding the provision of primary care. CCGs carrying out co-
commissioning under delegated authority do so on behalf of NHS England. Such
CCGs need to comply with NHS England's legal duties when doing this – this is set
out in the co-commissioning Delegation Agreement. Therefore, this chapter is also
relevant to co-commissioning CCGs.
Summary of duties covered by this chapter
Equality and Health Inequalities duties
a) Equality Act 2010
15 of 104

2 | P a g e
b) NHS Act 2006
Other non-equality and health inequalities related duties
The "Regard Duties"
The "View To Duties"
The "Promote Duties"
The "Involvement Duty"
Duty to act fairly & reasonably
Duty to "obtain appropriate advice"
Duty to exercise functions effectively
Duty not to prefer one type of provider
Equality and Health Inequalities duties
a) Equality Act 2010 b) NHS Act 2006 (as amended by the Health and Social Care Act
2012)
5 Working Together – Commissioning and Regulating – This chapter is intended to
inform commissioners of existing and ongoing work to establish a robust and practical
joint working framework by CQC and NHS England, with wider clinical commissioners,
in light of CCGs taking on full delegation and as CQC moves to its next phase of
inspection process.
Part B – General Contract Management 1 Contracts Described – This chapter includes a comparison of the various contracting
models and the list of eligibility requirements for persons entering the GMS/PMS and
APMS contract.
2 Assurance Framework Contract Review – Commissioners of Primary Medical Care are
responsible for the quality, safety and performance of services delivered by providers,
within their area of responsibility. This chapter outlines the approach to be taken by
commissioners when overseeing primary medical care contracts to ensure compliance
with quality and safety standards and replaces the Primary Medical Services
Assurance Management Framework guidance and policy documents first published
April 2013.
3 Managing Patient Lists – This chapter explains practice and commissioner’s
responsibility with regards to managing patient lists (open/closed/patient assignments)
and the process of list maintenance. It also describes the Primary Care Support (PCS)
Services delivered nationally through Primary Care Support England (PCSE).
4 GP Patient Registration Standard Operating Principles for Primary Medical Care – A
new chapter in the PGM, but which updates existing registration guidance published
by NHS England in November 2015 (Gateway Ref 04448). There has not been any
change in national policy in respect of patient registration for primary medical care
services – this guidance clarifies the rights of patients and the responsibilities of
16 of 104

3 | P a g e
providers in registering with a GP practice. It also clarifies the contractual rules in
respect of patient registration for patients, practices, CCGs and NHS England’s
regional teams.
5 Temporary suspension to patient registration – These guidelines for commissioners,
describe the process for closing the practice list and the circumstances where a
temporary suspension by the contractor of patient registration may be appropriate and
the conditions that should govern that decision such that the roles and responsibilities
of both parties are not compromised.
6 Special Allocation Scheme (SAS) – This chapter provides guidance to Commissioners
and providers of essential primary medical care services in relation to the removal of
patients who are violent from their practice list and the Special Allocation Schemes
(SAS) intended to ensure such patients receive primary care services. Provision for
SAS is set out in the GMS Regulations and the PMS Regulations (together, the
Regulations). This guidance focuses on a number of key themes, such as
commissioning the service, provider and service requirements, eligibility criteria and
the process of requesting immediate removal of a patient, which are intended to
support implementation of, and commissioning and monitoring of a SAS.
7 Contract Variations - This policy describes the process to determine any contract
variation, whether by mutual agreement or required by regulatory amendments, to
ensure that any changes reflect and comply with legislation so as to maintain robust
contracts. An existing chapter that has been strengthened and refined by the Legal
team and provides increased guidance in relation to Practice Mergers.
8 Managing a PMS Contractor’s Right to a GMS Contract – A contractor holding a PMS
agreement which is providing essential services, has the right to a GMS contract in
accordance with Regulation 19 of the PMS Regulations. This policy sets out the
decision-making process that the Commissioner will follow, together with refusal
(where eligibility is not satisfied), appeal processes and discussions regarding any
actions that are required.
9 Practice Closedown (Planned / Scheduled) - This chapter outlines the approach to be
taken when a time-limited primary medical services contract is coming to an end.
10 Discretionary Payments (made under Section 96) – this section does not cover locum
payments. A new chapter drafted jointly with NHS England’s Legal and Finance
Teams. Section 96 of the NHS Act (2006) (as amended) makes provisions for
commissioners to provide assistance and support to primary medical services
contractors, including financial support. S.96 exceptional discretionary funding is
intended to be used to safeguard patients’ interests by providing additional funding to
support practices facing a crisis situation.
Part C – When things go wrong 1 Contract Breaches, Sanctions and Terminations – This policy chapter outlines the
approach to be taken by the Commissioner when a contract is considered to have
been breached. The GMS Regulations, the PMS Regulations and the APMS Directions
make a clear distinction between the process to be followed where a breach is capable
of remedy and the process where a breach is not capable of remedy. The chapter also
17 of 104

4 | P a g e
describes the circumstances where the commissioner may apply contract sanctions.
The third part of this chapter deals with contract terminations.
2 Unplanned / Unscheduled and Unavoidable Practice Closedown – When a GP
Practice closes at short notice, it is important that commissioners respond and act in a
timely way. Such closures may be as result of actions by the CQC, for example
voluntary closure in response to an adverse inspection or cancellation of the practice’s
registration, or due to the sudden inability of a provider to continue providing a service
for some other reason such as bankruptcy. This guidance clarifies the role of the
commissioner and the engagement required with patients and any partner
organisations (e.g. NHS England or CQC).
3 Death of a Contractor (excluding single handers – see adverse events) – The aim of
this policy is to provide consistency when dealing with the death of a contractor,
whether they are a single-handed contractor, in a partnership or a corporate
organisation and includes consideration of GMS, PMS, APMS and where appropriate
MCP/PACS contracts. This policy outlines the procedure to follow when the death of a
contractor occurs. This is a rare occurrence, but there are certain steps to follow within
agreed timescales that are laid down in legislation.
4 Managing Disputes – This policy describes the process to determine the action
required when a contractor has requested to follow the NHS dispute resolution process
or where the Commissioner elects to follow the NHS dispute resolution procedure.
5 Adverse Events (e.g. flood fire) – Adverse incidents are dealt with in the force majeure
provisions of the standard GMS, PMS, APMS and where appropriate MCP/PACS
contracts. Although these provisions are not required by the GMS Regulations, the
PMS Regulations or the APMS Directions, the majority of GMS, PMS, APMS and
where appropriate MCP/PACS contracts will include them. A force majeure event is
one which is caused by circumstances beyond the reasonable control of either the
Commissioner or the contractor that could not have been avoided or mitigated with
reasonable care and where the event has had a material effect on the fulfilment of the
contract. All contractors will likely be obliged under the terms of their contracts to
promptly notify the Commissioner of a force majeure event, detailing the cause or
event, what service provision is being delayed or prevented and what action(s) within
their power they are taking in order to comply with the terms of the contract as fully
and promptly as possible.
Part D – General 1 GP IT Operating Model: Data and Cyber Security Arrangements – A new chapter
drafted by the GPIT team. This chapter provides an overview of GP IT Operating
Arrangements, as outlined in the GP IT Operating Model, ‘Securing Excellence in GP
IT Services’ 2016/18, published by NHS England. Particular reference is made to data
and cyber security arrangements, following the publication of the National Data
Guardian Review in July 2016 which included key recommendations and proposed ten
data security standards.
2 Protocol in respect of locum cover or GP performer payments for parental and sickness
leave – A new chapter in the PGM but previously published in April 2017 with Gateway
Ref 06791. The General Medical Services Contracts Statement of Financial
Entitlement Directions 2013 (SFE) as amended in the SFE (amendment) Directions
18 of 104

5 | P a g e
2017 set out the provisions, conditions and payments relating to reimbursement to GP
practices for GP performers covering parental leave and sickness leave. This protocol
applies only to GMS practices, but commissioners should ensure they treat Primary
Medical Services (PMS) practices equitably.
3 Guidance Note: GP Practices serving Atypical Populations – A new chapter in the PGM
but previously published in December 2016 with Gateway Ref 06265). The General
Medical Services (GMS) funding formula (Carr-Hill formula) is an attempt to fund
practice workload, regardless of the population they serve. It is applicable to the vast
majority of the UK, but there are some practice populations that are so significantly
atypical that using the GMS funding formula would not ensure the delivery of an
adequate general practice service. This working group has looked at three such
atypical populations: unavoidably small and isolated; university practices and; those
with a high ratio of patients who do not speak English.
This document was produced to assist NHS England and delegated Clinical
Commissioning Group (CCG) commissioners of 3 such atypical ‘populations’ by
detailing the particular challenges faced by providers and offering examples of either
provider or commissioner reports that may help either articulate or address these
pressures. The chapter also talks about the GMS funding formula review.
NHS England recognises the scale and pace of change in Primary Medical Care
commissioning, service delivery and redesign. As such it is committed to reviewing this policy
and guidance regularly, to ensure it supports the commitments set out in the General Practice
Forward View, the Five Year Forward View and with changes in legislation and regulation.
References NHS England. (2017, November 15). Primary Medical Care Policy and Guidance Manual
(PGM) . Retrieved from NHS England: https://www.england.nhs.uk/publication/primary-
medical-care-policy-and-guidance-manual-pgm/
19 of 104

This page has been left blank

General Purpose – Integrated Primary Care
Commissioning Paper Author: Kate Symons & Emma Gillgrass Sponsor: Katie Denton Date: October 2018
Executive Summary
Context
This is report provides the Primary Care Committee with an update on how delegated
Primary Care commissioning is being managed in Merton; providing an update on some of
the key programmes of work.
Question(s)/ topics this paper addresses 1. Monitoring PMS KPIs
2. Ravensbury Park Update
3. Joint Primary Care Quality Review Group (PCQRG) Update
4. What general contracting decisions have been made in the last quarter?
Conclusion 1. The Committee are asked to note the proposals for monitoring the PMS KPIs in Merton,
including the development of a PMS KPI Review Group.
2. Ravensbury Park Practice have recently been respected by the CQC and we are
awaiting the outcome.
3. The PCQRG update focussed specifically on the Quality, Support and Education
contract and the GP Resilience Funding update.
4. The Committee are asked to note the decisions taken over the last quarter.
Input Sought The Committee are asked to note the detail included within this paper, and the progress
made under delegate commissioning arrangements.
21 of 104

The Report
A N A L Y S I S
1. Monitoring the PMS KPIs
In 2016/17 the CCG undertook a review of the PMS Premium indicators in Merton as part
of a nationally directed review process. As part of this process we had the opportunity to
review the old PMS indicators and engage clinicians in the development of new service
specification requirements that were clinically appropriate and strategically important, whilst
also ensuring that we continued to support sustainability across practices in Merton.
A PMS Working Group was established and regular meetings took place with the Local
Medical Council (LMC) in order to develop and refine our approach; as well as agreeing
what we will be included in our local PMS Premium Offer. We utilised the opportunity
afforded to us under delegated primary care commissioning to look at the quality of the
previous indicators and work in a more broader sense to ensure that the new indicators are
fit for purpose, provide value for money, and clinical appropriate for the population of Merton.
In total there are 22 Practices in Merton; 20 of which are PMS Practices, with 1 GMS and 1
APMS Practice.
We rolled out the developed PMS Premium indicators to all our PMS practices during the
end of 2017, early 2018 with all PMS Practices signing up to the new PMS Contract and
local Premium. One practice decided to revert back to a GMS Contract, although agreed to
sign up to the PMS Premium indicators.
As part of our delegated commissioning responsibility the CCG is responsible for the
oversight of the PMS KPIs and the performance management of practices achieving these
indicators.
As such we are now in a position to begin to review these locally developed indicators as
part of the process of continuous improvement, review and reflection of the suitability of
each of those implemented.
What are the PMS Premium Indicators in Merton?
The Merton PMS Premium Indicators are made up of the following:
Improving access for Carers
Opening Hours, Appointment Numbers and facilitations of access to Local Access Hubs
Working with the CCGs Medicines Optimisation Team
Medicines Management Uptake of Electronic Prescribing System (EPS)
Uptake and utilisation of advice and guidance tool (kinesis)
Peer review for referrals
Reducing unscheduled admissions for mild to moderate frailty
22 of 104

Diabetes exception reporting
Ten High Impact Actions
Prevention – Bowel cancer screening
Prevention – Improve uptake of childhood immunisations
Prevention – Improve uptake of Influenza Vaccinations in Primary Care
Wound Care
Administering non-contraceptive hormonal implants or injections
What about the GMS Practices?
As part of the PMS Review Process one Merton Practice reverted back to a GMS practice;
although signed up to delivering the PMS premium indicators and therefore aligned with the
other PMS practices in relation to the services now offered.
How do we propose to monitor these indicators?
A standardised data collection template has been designed by the SWL Primary Care
Contracting Team, as they will be collecting the data on our behalf. This template details
the reporting requirements for each indicator, and as well as the format for reporting on
action planning, or where further performance feedback on the indicator is required.
It is the monitoring of areas that the SWL Team require input in from a local perspective; in
terms of the content on the action or implementation plans, and deciding on the best way to
follow up these area where required.
The Area’s that will be monitored via an Action or implementation Plan include:
Reviewing the uptake of EPC and documenting any valid factors that have impacted on
progress
Evidencing how peer reviews have been undertaken
Annual 360 degree feedback template for the reducing unplanned admissions KPI
Annual Diabetes Action Plan to improve rates of exception reporting
Annual report detailing the changes implemented as a result of the Dementia Friends
Training
Annual report of how non responders to the bowel cancer screening invite will be
identified and the methods used to contact them
Sharing learning from these reports will also be an important way of adding value to the
PMS Indicators. It may be through local review that examples of good practice are identified,
or learning can be shared where practices have made significant progress in increasing
certain rates, i.e bowel screening uptake. Ensuring that we have a local intelligence when
reviewing the data will provide a more robust review of these data returns, allowing for local
context where appropriate.
23 of 104

Who will review the indicators? It is proposed that a local PMS KPI Review Group will be established to look at the KPI
returns, on a quarterly and annual basis as required by the specific indicator. This group
will include;
SWL primary care team lead
Locality Manager
Head of Primary Care Quality
Locality clinicians as appropriate
Head of delegated commissioning
Where zero returns are made, or practices report a reduction towards meeting a target then
the group can review this data in light of any other local intelligence and agree whether there
should be any follow-up support provided to the practice. Conversely, where practice may
show significant improvements then the group can agree an approach to sharing good
practice/learning.
It is anticipated that the initial review meetings will focus on the baseline returns and any
action plans, as well as ensuring the practice are able to provide the required information.
This will give an initial review as to the suitability of the KPIs as well as the use of the
searches and templates by each practice.
Subsequent review of the returns will enable the review of the suitability of the KPI indicators,
to ensure that we are getting full value and realising the anticipated benefits of each
indicator.
How do we plan to share the learning? It is anticipated that learning will be shared more widely on an annual basis, as practice may
choose to implement improvements in a staged approach and therefore the full impact
and/or benefit of the indicators will not be realised until the full year.
We will however be mindful where early feedback indicators that certain KPIs may not be
appropriate or suitable to monito, or where searches do not provide the appropriate data i.e
regular zero returns.
Learning from reviewing the KPI indicators will be reported into both the Primary Care
Quality Review Group and well as the Primary Care Ops group as appropriate, with the final
oversight of performance undertaken by the Primary Care Committee. Where areas of good
and even poor practice can be identified, then these groups can agree the best approach to
share this learning more widely.
Working with the LMC One of the key success points of the PMS Review in Merton was the engagement with our
local LMC colleagues to develop locally driven, fit for purpose indicators. With this is mind
the CCG aims to continue this engagement with the LMC in the review of the KPIs on an
annual basis to ensure that we continuously review the suitability of each indicator. Local
24 of 104

LMC colleagues will be asked to feed into the review process and where indicators may be
retired or refreshed, engage with the CCG in the development of alternative replacements.
The LMC will also be asked to contribute to the process in particular where early indicators
identify a particular issue or concern with a specific KPI.
2. Ravensbury Park Update
The Committee will be aware of previous updates made in relation to the CQC Inadequate
Rating given to the Practice, and the work undertaken over the last 12 months as a result of
the Practice being placed into ‘Special Measures’. The practice have been supported by
both the CCG, NHS England and a local practice (through a new partnership arrangement)
in order to implement the required improvements at the practice. The Practice received a
further CQC inspection on the 18th September; and we are awaiting the formal outcome and
rating.
3. Joint Primary Care Quality Review Group (PCQRG) Update
The Joint Merton and Wandsworth Primary Care Quality Review Group (PCQRG) is a
clinically led group with responsibility for overseeing the quality of services provided by GP
practices across both boroughs through the core GP contracts. It reviews a range of data
and information in order to seek assurance on the quality of services and also identify any
areas, or individual practices that may require support. The PCQRG then identifies what
support is available, what further work may be required and monitors progress.
The PCQRG monitors national and local quality standards as well as holding Providers to
account for any contractual requirements relating to clinical quality and safety of the
services. This group review a range of areas such as patient experience and clinical
indicators to direct areas of focus and inform decisions about practices, as well as identifying
support for practices where required.
Quality, Support, Education Contract
A Quality, Support and Education contract has recently been agreed with Merton Health Ltd.
(the Merton GP Federation). As part of this contact a Primary Care Support Team be
established to support practices with quality improvement, reducing variation and
developing resilience.
The team will facilitate discussion within practices, to identify areas of good practice and
also areas where improvements could be made. This will be tailored to each individual
practice. The team will then be able to support the practice implement actions for
improvement. This may include linking in with other teams or services which will be able to
provide expert advice and support. The team will also provide direct support to the practices.
A key area for support will be in ensuring practices are CQC compliant, and responding to
requests for support ahead of inspections or where areas of improvement are identified by
the CQC.
25 of 104

GP Resilience Funding
In 2017-18 12 Merton practices were identified as part of the resilience scheme and received
support which included practice management and back office support, and I.T. support and
training.
2018-19 is now the third year of GP Resilience funding and as in 2017-18, due to the small
amount of funding available (approximately £170,000 for SWL) it has been agreed to
manage this at a South West London level.
A heat map for SWL was produced which included data around Quality and safety,
Workforce, Patient Experience and Efficiency for all practice. This was used as the basis for
local discussions as to which practices should be put forward for the 2018-19 scheme. In
Merton this was through the Primary Care Quality Review Group. Using the heat map and
other local data and knowledge a list of 7 Merton practices was agreed to be put forward for
the scheme.
Practices were also offered the opportunity to self-nominate for the 2018-19 scheme and 1
practices put themselves forward, which had already been identified by the CCG.
The process for identifying and agreeing the specific packages for support is being managed
across all the SWL resilience practices and CCGs will be provided with regular update
reports.
4. What general Primary Care Contracting decisions have been made in the last quarter?
The following details the primary care contracting decision made to date; under business as
usual arrangements. Where the contractual changes are detailed these decision would
have been made through the usual governance arrangements; and therefore taken at
Committee level.
26 of 104

C O N C L U S I O N
The Committee are asked to note the ongoing work that has been jointly implemented
across Primary Care under delegated commissioning arrangements.
27 of 104

This page has been left blank

Primary Care Finance Report
Produced by Finance
August 2018 (2018/19 Month 5)
29 of 104

Contents
1. Month 5 Background & Overview
2. Month 5 Primary Care Overall Position
3. Primary Care Narrative
4. Recommendations
August 2018
Primary Care Finance Report
30 of 104

1. Month 5 Background & Overview• Background
Primary Care Delegated Commissioning was introduced on 1st April 2016.
The financial accounting for this area is done with NHS England staff working exclusively for South West London
CCGs.
This paper reflects information available to the CCG to support the financial position for the five months ended
31st August 2018.
For prescribing we are relying on 3 months’ data for forecasting purposes.
It should be noted that this position includes general primary care commissioning that has always been the
responsibility of the CCG as well as picking up other areas of primary care expenditure which have always been
under the responsibility of their CCG from its programme allocation.
• Overview
Primary care expenditure overall had an underspend of £81k year to date.
This is the net impact of a prescribing overspend of £46k and an overspend in Local Enhanced Services of £106k,
offset by an underspend in Primary Care Delegated Budgets of £25k, and an underspend of £206k relating to
other primary care expenditure.
We are currently reporting a forecast net overspend of £77k which includes risk of £256k for NCSO, but there are
significant risks to prescribing for category M drugs (£500k) and further NCSO risk (£100k) which are not currently
reflected in the reported forecast outturn.
The following slides give more detail behind these numbers.
August 2018
Primary Care Finance Report
31 of 104

2. Primary Care Position
August 2018
Primary Care Finance Report
Full Year
Budget
Budget to
Date
Actual to
Date
Variance to
Date
Forecast
Actual
Forecast
Variance
£000's £000's £000's £000's £000's £000's
PRESCRIBING 21,694 9,039 9,083 -44 21,800 -105
MEDICINES OPTIMISATION 75 31 28 3 67 8
CENTRAL DRUGS 669 279 283 -5 680 -12
Total Prescribing 22,438 9,349 9,395 -46 22,547 -109
HOME OXYGEN SERVICE 220 92 88 4 220 0
TB PROJECT 30 13 13 0 30 0
TOTAL LONG TERM CONDITIONS 250 104 100 4 250 0
PRIMARY CARE CONTRACT VALUE AND KPI'S 21,295 7,052 7,065 -13 21,493 -198
PRIMARY CARE OTHER DELEGATED BUDGET 7,791 4,879 4,841 39 7,561 230
Total Primary Care Delegated Budgets 29,086 11,931 11,906 25 29,054 32
Total Local Enhanced Services 531 221 327 -106 531 0
Total Out Of Hours 1,808 753 756 -3 1,808 -0
GP - STATUTORY MEDICAL FEES 108 45 75 -29 108 0
QUALITY PREMIUM 0 0 0 0 0 0
GPSI'S COMMISSIONING - MINOR SURGERY 77 32 0 32 77 0
OPHTHALMOLOGY (LOW VISION SERVICE) 9 4 0 4 9 0
GPFV GP DEV RECEPTION & CLERICAL TRAINING (S1017) 38 16 16 0 38 0
GPFV ONLINE CONSULT SOFTWARE SYSTEMS (S1018) 75 31 31 0 75 0
GPFV IMPROVED GP ACCESS INIT SCHEME (S1019) 948 395 395 0 948 0
PRIMARY CARE TRANSFORMATION FUND 0 -0 -0 -0 0 -0
PRIMARY CARE INVESTMENTS 157 65 69 -3 157 0
PRIMARY CARE OTHER 1,938 808 754 54 1,938 0
Access Local Incentive Scheme 1,180 492 342 149 1,180 0
WALK IN CENTRE (UNREGISTERED PATIENTS) 0 0 0 0 0 0
Total Primary Care Other 4,530 1,888 1,681 206 4,530 0
TOTAL PRIMARY CARE 58,643 24,247 24,166 81 58,720 -77
32 of 104
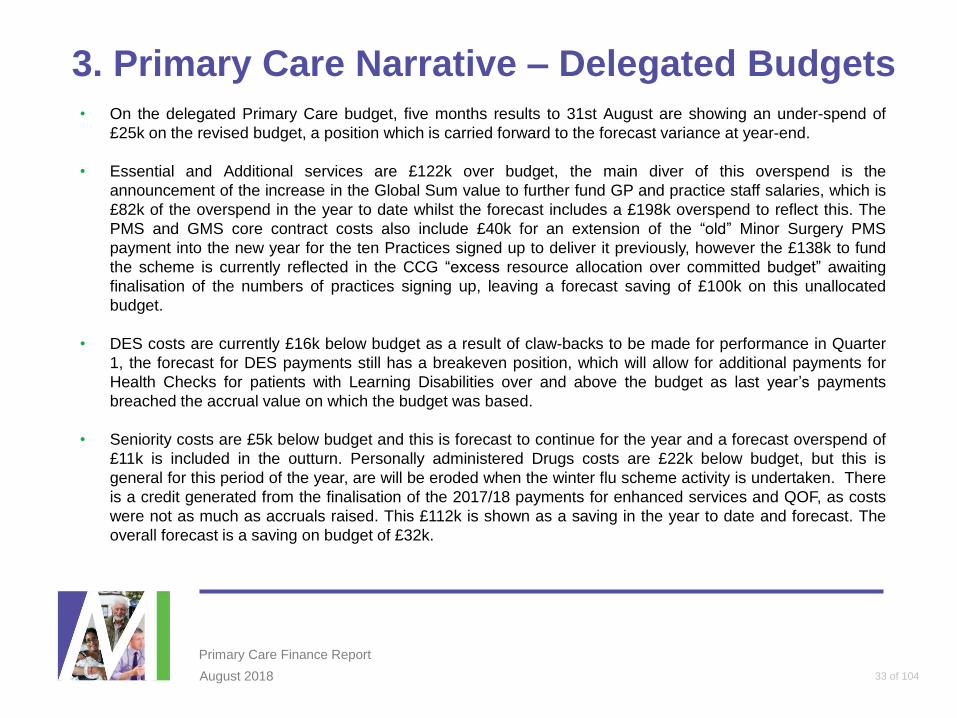
3. Primary Care Narrative – Delegated Budgets• On the delegated Primary Care budget, five months results to 31st August are showing an under-spend of
£25k on the revised budget, a position which is carried forward to the forecast variance at year-end.
• Essential and Additional services are £122k over budget, the main diver of this overspend is the
announcement of the increase in the Global Sum value to further fund GP and practice staff salaries, which is
£82k of the overspend in the year to date whilst the forecast includes a £198k overspend to reflect this. The
PMS and GMS core contract costs also include £40k for an extension of the “old” Minor Surgery PMS
payment into the new year for the ten Practices signed up to deliver it previously, however the £138k to fund
the scheme is currently reflected in the CCG “excess resource allocation over committed budget” awaiting
finalisation of the numbers of practices signing up, leaving a forecast saving of £100k on this unallocated
budget.
• DES costs are currently £16k below budget as a result of claw-backs to be made for performance in Quarter
1, the forecast for DES payments still has a breakeven position, which will allow for additional payments for
Health Checks for patients with Learning Disabilities over and above the budget as last year’s payments
breached the accrual value on which the budget was based.
• Seniority costs are £5k below budget and this is forecast to continue for the year and a forecast overspend of
£11k is included in the outturn. Personally administered Drugs costs are £22k below budget, but this is
general for this period of the year, are will be eroded when the winter flu scheme activity is undertaken. There
is a credit generated from the finalisation of the 2017/18 payments for enhanced services and QOF, as costs
were not as much as accruals raised. This £112k is shown as a saving in the year to date and forecast. The
overall forecast is a saving on budget of £32k.
August 2018
Primary Care Finance Report
33 of 104

3. Primary Care Narrative – Prescribing
• Currently only three months of prescribing data is available. Expenditure at Merton CCG for
the first three months is slightly higher than that of last year.
• There is an additional risk to the position relating to Category M reimbursement prices which
are due to increase from August 2018. This is a national issue due to the Department of
Health and Social Care agreeing to cease a £15 million per month reduction in prices that had
been in place to recover estimated excess margin delivered to pharmacies in 2015/16 and
2016/17. This decision was a result of negotiations with PSNC (Pharmaceutical Services
Negotiating Committee) in which concerns were raised about the impact of price reductions on
contractors’ cash flow.
• We expect this issue to translate locally into a cost pressure of approximately £75k per month
for the CCG, which if this continues for the rest of the year from August, could mean an over-
spend of around £600k by year end. We will continue to monitor the situation as the actual
data comes through in ePACT and start to recognise this risk in the forecast position as we
gain greater certainty over its value and likelihood.
August 2018 6
Primary Care Finance Report
34 of 104

The Primary Care Committee are asked to note the financial position as
reported in this paper for the four months ended 31st August 2018.
August 2018
Primary Care Finance Report
4. Recommendations
35 of 104

This page has been left blank

M E R T O N C C G P A G E 1 O F 9
Strictly Confidential Board Intelligence Hub template
GP Patient Survey 2018 Author: Emma Gillgrass Sponsor: Katie Denton Date: 10/2018
Executive Summary
Context
The GP Patient Survey (GPPS) is an England-wide survey, providing practice-level data
about patients’ experiences of their GP practices. Ipsos MORI administer the survey on
behalf of NHS England.
The most recent data, reviewed in this report was collected in the survey period January –
March 2018.
Question(s) this paper addresses
1. What does the survey show about GP practices in Merton?
2. What areas need further work?
Conclusion
1. The survey shows the variation in services between GP practices, however overall
there is a high level of satisfaction with GP practices in Merton.
2. The areas with the lowest results, and widest variation between practices which may
need further consideration are linked to making appointments.
Input Sought
The Primary Care Committee is asked to review and note the survey results.
M E R T O N C C G
37 of 104

M E R T O N C C G P A G E 2 O F 9
Strictly Confidential Board Intelligence Hub template
The Report
F U R T H E R C O N T E X T
The GP Patient Survey (GPPS) is an England-wide survey, providing practice-level data
about patients’ experiences of their GP practices. Ipsos MORI administer the survey on
behalf of NHS England.
The most recent data, reviewed in this report was collected in the survey period January –
March 2018. Full results and CCG level packs can also be accessed at: https://www.gp-
patient.co.uk/surveysandreports
(Please note the Merton CCG slide pack includes data on the GP Led Health Centre which
has now closed and James O’Riordan Medical Centre which now comes under Sutton CCG)
Survey questions come under a number of headings:
Your local GP service
Making an appointment
Your last appointment
Overall experience
Your health
When your GP practice is closed
Some questions about you
The sample sizes for individual practices are very small so this should be taken into account when analysing the data.
Within Merton 3.8% of the registered list was sent a survey. The response rate was 27.9%
in Merton which equates to 1% of the total registered list sizes.
Population (May 2018)
Forms distributed
Completed forms
returned
% Pop. sent form
Response
rate (%)
%
Response
Total Pop.
Merton 226,482 8,687 2,422 3.8% 27.9% 1.1%
Wandsworth 404,441 15,779 3,818 3.9% 24.2% 0.9%
SW London 1,665,262 68,606 19,845 4.1% 28.9% 1.2%
London 9,863,204 485,814 125,270 4.9% 25.8% 1.3%
England 59,085,088 2,221,068 758,165 3.8% 34.1% 1.3%
38 of 104

M E R T O N C C G P A G E 3 O F 9
Strictly Confidential Board Intelligence Hub template
A N A L Y S I S
1) What does the survey show about GP practices in Merton?
1.1) 2018 Results – Borough level
In 2018 82% of patients in Merton rated their experience of their GP practice as Good.
The table below highlight some of the key questions from the survey and provides
comparisons for Merton with South West London (SWL), London and England. In general
Merton is in line with the London average.
2018 – Averages Merton
CCG
South West
London London England
Overall how would you describe your experience of your GP surgery? (% Good)
82% 85% 81% 84%
Generally how easy is it to get through to someone at your GP surgery on the phone? (% Easy)
65% 75% 70% 70%
How helpful do you find the receptionists at your GP surgery? (% Helpful)
87% 90% 88% 90%
Overall how would you describe your experience of making an appointment? (% Good)
67% 72% 66% 69%
How easy is it to use your GP practice’s website to look for information or access services? (% easy)
79% 78% 73% 78%
During last general practice appointment did you have confidence and trust in the healthcare professional (% yes)
94% 95% 94% 96%
How satisfied are you with the general practice appointment times that are available to you? (% satisfied)
67% 69% 65% 66%
1.2) Trends – Borough level
Many of the questions in the 2018 survey had changes to previous surveys so trends could
not be seen. The table below sets out some questions that had not changed to show trends
over the last few years at borough and national level, and two questions where there was a
slight change in the wording so both the previous questions and the new question are
shown. For the majority of questions Merton has seen improvements since the 2017 survey.
39 of 104

M E R T O N C C G P A G E 4 O F 9
Strictly Confidential Board Intelligence Hub template
Jun-13 Jul-14 Jul-15 Jul-16 Jul-17 Aug-18
Change from Jul-17 to Aug-18
Overall how would you describe your experience of your GP surgery? (% Good)
MCCG 82% 79% 79% 80% 80% 82%
England 85% 85% 84%
Generally how easy is it to get through to someone at your GP surgery on the phone? (% Easy)
MCCG 66% 61% 57% 60% 60% 65%
England 70% 68% 70%
How helpful do you find the receptionists at your GP surgery? (% Helpful)
MCCG 86% 84% 84% 85% 84% 87%
England 87% 87% 90%
Overall how would you describe your experience of making an appointment? (% Good)
MCCG 70% 66% 66% 67% 66% 67%
England 73% 73% 69%
How satisfied are you with the hours that your GP surgery is open? (% Satisfied)
MCCG 76% 74% 70% 73% 75%
England 76% 76%
How satisfied are you with the appointment times that are available to you? (% Satisfied)
MCCG 67%
England 66%
Did you have confidence and trust in the GP you saw or spoke to? (% Yes)
MCCG 94% 94% 95% 94% 94%
England 95% 95%
Did you have confidence and trust in the nurse you saw or spoke to? (% Yes)
MCCG 96% 96% 96% 95% 96%
England 97% 97%
During your last general practice appointment did you have confidence and trust in the healthcare professional? (%yes)
MCCG 94%
England 96%
1.3) Practice Level Results
Results for the survey are also available at practice level, although again the small sample
size needs to be taken in to consideration. The number of completed surveys per practice
ranged from 83 to 132, reflecting an average of 1% of the practice population.
Friends and Family Test (FFT)
The GP Patient survey is just one way in which patient experience is captured. Another route
that all practices are expected to engage with is the Friends and Family Test. As with the
patient survey the FT often had small numbers of responses which needs to be considered
when analysing the results.
40 of 104

M E R T O N C C G P A G E 5 O F 9
Strictly Confidential Board Intelligence Hub template
The Friends and Family Test question is “How likely are you to recommend our service to
friends and family if they needed similar care or treatment?”
When the results of the Overall Experience GP Patient Survey Question and the FFT
question are compared, most practices are rated fairly similarly across both question,
although the majority have a slightly higher scores for their most recent Friends and Family
Test (June 2018 data), where data was submitted.
Practice Level Charts – Appendix 1
The charts below show for each practice:
Overall experience: – Overall how would you describe your experience of your GP
surgery? (% Good)
Use of Services: Practice level results across 9 questions
GP Patient Survey: Overall Experience compared to Friends and Family Test (June
2018) results
2) What areas need further work?
Merton generally rates similarly to the London average. There are still areas for
improvement, and areas where there is significant variation between practices.
The questions with the lowest results:
How easy is it to get through to someone on the phone
Offered choice of appointment
Satisfied with the general practice appointment times that are available
Over all experience of making an appointment
Questions with the widest variation between practices:
How easy is it to get through to someone on the phone
Offered choice of appointment
Over all experience of making an appointment
Satisfied with the general practice appointment times that are available
3) Next Steps
The survey results are being reviewed by the Primary Care Quality Review Group where
practices requiring additional support will be identified as well as areas across the borough
where improvement can be made. The PCQRG will also look to identify what support can
be provided in order to make improvements.
C O N C L U S I O N
The Primary Care Committee are asked to review and note the survey results.
41 of 104

M E R T O N C C G P A G E 6 O F 9
Strictly Confidential Board Intelligence Hub template
Appendix 1
Merton Practice Level Data: Overall how would you describe your experience of your GP surgery? (% Good)
42 of 104

M E R T O N C C G P A G E 7 O F 9
Strictly Confidential Board Intelligence Hub template
Merton Practice Level Data: Use of services
Practice Name List Size
Overall
experience
Over all
experience of
making an
appointment
How satisfied
are you with
the general
practice
appointment
times that are
available to
you?
How easy is it
to get through
to someone on
the phone
How helpful do
you find the
receptionists
Offered choice
of appointment
Satisfied with
type of
appointments
offered
How easy is it
to use your GP
practice’s
website to look
for information
or access
services?
During your last
general practice
appointment
did you have
confidence and
trust in the
healthcare
professional
Jun-18 % Good % Good % Satisfied % Easy % Helpful % Yes % Satisfied % Easy % Yes
E Rowans Surgery 7,220 53% 40% 43% 32% 68% 48% 60% 60% 83%
E Tamworth House Medical Centre 9,345 68% 51% 56% 41% 79% 42% 53% 52% 85%
E Mitcham Family Practice 3,608 70% 74% 64% 78% 90% 71% 64% 81% 88%
E The Mitcham Medical Centre 9,040 77% 48% 49% 36% 82% 53% 58% 76% 87%
E Figges Marsh Surgery 7,989 80% 60% 68% 60% 90% 78% 76% 76% 91%
W Morden Hall Medical Centre 14,524 80% 64% 74% 57% 88% 81% 73% 83% 92%
E Ravensbury Park Medical Centre 5,336 80% 74% 67% 71% 88% 69% 74% 88% 93%
W Grand Drive Surgery 8,850 81% 70% 66% 88% 92% 65% 69% 90% 96%
W Lambton Road Medical Practice 17,646 81% 68% 67% 58% 85% 63% 70% 85% 92%
E Colliers Wood Surgery 10,546 82% 75% 72% 72% 85% 61% 78% 51% 93%
W The Nelson Medical Practice 28,975 82% 61% 70% 68% 87% 66% 63% 81% 100%
E Wide Way Medical Centre 9,196 83% 72% 77% 76% 91% 69% 80% 91% 87%
E Cricket Green Medical Practice 11,605 85% 66% 64% 49% 87% 54% 81% 71% 94%
W The Merton Medical Practice 8,007 85% 78% 76% 86% 88% 70% 82% 79% 89%
W The Vineyard Hill Road Surgery 4,210 85% 82% 73% 94% 91% 80% 85% 72% 93%
W Stonecot Surgery 8,481 87% 69% 70% 42% 90% 67% 79% 90% 94%
W Princes Road Surgery 9,448 87% 76% 68% 77% 93% 65% 81% 80% 98%
W Central Medical Centre 8,740 87% 72% 74% 64% 73% 75% 80% 65% 96%
W Francis Grove Surgery 13,436 87% 70% 65% 67% 94% 67% 70% 81% 96%
W Wimbledon Village Practice 12,177 89% 81% 63% 89% 95% 68% 80% 86% 97%
W Alexandra Surgery 5,536 90% 71% 83% 75% 94% 86% 86% 72% 100%
W Riverhouse Medical Practice 5,819 91% 78% 73% 89% 83% 85% 87% 90% 100%
Range: Minimum 40% 43% 32% 68% 42% 53% 51% 83%
Range: Maximum 82% 83% 94% 95% 86% 87% 91% 100%
43 of 104

M E R T O N C C G P A G E 8 O F 9
Strictly Confidential Board Intelligence Hub template
Merton Practice Level Data: GP Patient survey Overall Experience Compared to Friends and Family Results
44 of 104

M E R T O N C C G P A G E 9 O F 9
Strictly Confidential Board Intelligence Hub template
For Reference Edit as appropriate:
1. The following were considered when preparing this report:
The long-term implications [Yes]
The risks [Not applicable]
Impact on our reputation [Yes]
Impact on our patients [Yes]
Impact on our providers [Yes]
Impact on our finances [Not applicable]
Equality impact assessment [Not applicable]
Patient and public involvement [Yes]
2. This paper relates to the following corporate objectives:
Commission high quality services which improve outcomes and reduce
inequalities [Yes]
Make the best use of resources, continually improve performance and deliver
statutory responsibilities [Not applicable]
Continually improve delivery by listening to and collaborating with our patients,
members, stakeholders and communities [Yes]
Transform models of care to improve access, ensuring that the right model of care
is delivered in the right setting [Yes]
Develop the CCG as a continuously improving and effective commissioning
organisation [Yes]
3. Executive Summaries should not exceed 1 page. [My paper does comply]
4. Papers should not ordinarily exceed 10 pages including appendices.
[My paper does comply]
45 of 104

This page has been left blank

17-043177-06 Version 1 | Public© Ipsos MORI
1
Version 1| Public
17-043177-06 Version 1 | Public© Ipsos MORI
NHS MERTON CCG
Latest survey resultsAugust 2018 publication
47 of 104

17-043177-06 Version 1 | Public© Ipsos MORI
2
Contents
This slide pack provides results for the following topic areas:
Background, introduction and guidance …………………………….……………………………………….. Slide 3
Overall experience of GP practice ………………………………………………………………..…..……….. Slide 8
Local GP services ………………………………………………………………………………………………... Slide 13
Access to online services ………………………………………………………………………………………. Slide 18
Making an appointment …………………………………………………………………………………………. Slide 23
Perceptions of care at patients’ last appointment …………………………………………….……………. Slide 31
Managing health conditions …………………………………………………………………………….............Slide 35
Satisfaction with general practice appointment times …………………………………………………….. Slide 38
Services when GP practice is closed ……….………………………………………………………………… Slide 41
Statistical reliability ………………………………………………………………………………………………. Slide 46
Want to know more? …………………………………………………………………………………………...... Slide 48
48 of 104

17-043177-06 Version 1 | Public© Ipsos MORI
3
17-043177-06 Version 1 | Public© Ipsos MORI
Background, introduction
and guidance
49 of 104

17-043177-06 Version 1 | Public© Ipsos MORI
4
Background information about the survey
• The GP Patient Survey (GPPS) is an England-wide survey, providing practice-level
data about patients’ experiences of their GP practices.
• Ipsos MORI administers the survey on behalf of NHS England.
• For more information about the survey please refer to the end of this slide pack or visit
https://gp-patient.co.uk/.
• This slide pack presents some of the key results for NHS MERTON CCG.
• The data in this slide pack are based on the August 2018 GPPS publication.
• In NHS MERTON CCG, 8,687 questionnaires were sent out, and 2,422 were returned
completed. This represents a response rate of 28%.
• Prior to 2015 these slide packs presented Area Team averages for each CCG. These
are no longer included following the integration of Area Teams into the four existing
Regional Teams. However, CCGs can still see how their results compare to those of
other local CCGs.
• The questionnaire has been redeveloped for 2018 in response to significant changes to
primary care services as set out in the GP Forward View, and to provide a better
understanding of how local care services are supporting patients to live well, particularly
those with long-term care needs. The questionnaire (and past versions) can be found
here: https://gp-patient.co.uk/surveysandreports.
50 of 104
17-043177-06 Version 1 | Public© Ipsos MORI
5
Introduction
• The GP Patient Survey measures patients’ experiences across a range of topics, including:
- Making appointments
- Perceptions of care at appointments
- Managing health conditions
- Practice opening hours
- Services when GP practices are closed
• The GP Patient Survey provides data at practice level using a consistent methodology, which means it is comparable across organisations.
• The survey has limitations:
- Sample sizes at practice level are relatively small.
- The survey does not include qualitative data which limits the detail provided by the results.
- The data is provided once a year rather than in real time.
• However, given the consistency of the survey across organisations, GPPS can be used as one element of evidence.
• It can be triangulated with other sources of feedback, such as feedback from Patient Participation Groups, local surveys and the Friends and Family Test, to develop a fuller picture of patient journeys.
• This slide pack is intended to assist this triangulation of data. It aims to highlight where there may be a need for further exploration.
• Practices and CCGs can then discuss the findings further and triangulate them with other data – in order to identify potential improvements and highlight best practice.
• The following slide suggests ideas for how the data can be used to improve services.
• Given the extensive changes to the questionnaire in 2018, this pack does not include trends over time.
51 of 104
17-043177-06 Version 1 | Public© Ipsos MORI
6
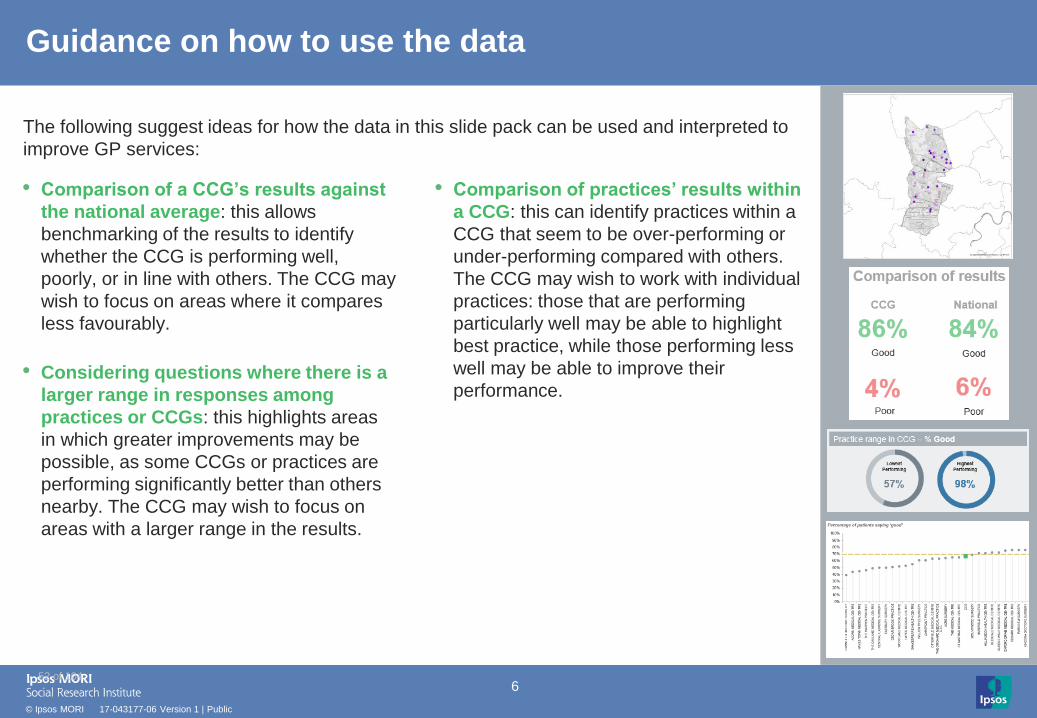
Guidance on how to use the data
• Comparison of a CCG’s results against
the national average: this allows
benchmarking of the results to identify
whether the CCG is performing well,
poorly, or in line with others. The CCG may
wish to focus on areas where it compares
less favourably.
• Considering questions where there is a
larger range in responses among
practices or CCGs: this highlights areas
in which greater improvements may be
possible, as some CCGs or practices are
performing significantly better than others
nearby. The CCG may wish to focus on
areas with a larger range in the results.
• Comparison of practices’ results within
a CCG: this can identify practices within a
CCG that seem to be over-performing or
under-performing compared with others.
The CCG may wish to work with individual
practices: those that are performing
particularly well may be able to highlight
best practice, while those performing less
well may be able to improve their
performance.
The following suggest ideas for how the data in this slide pack can be used and interpreted to
improve GP services:
52 of 104

17-043177-06 Version 1 | Public© Ipsos MORI
7
Interpreting the results
• The number of participants answering (the
base size) is stated for each question. The
total number of responses is shown at the
bottom of each chart.
• All comparisons are indicative only.
Differences may not be statistically
significant – particularly when comparing
practices due to low numbers of
responses.
• For guidance on statistical reliability, or for
details of where you can get more
information about the survey, please refer to
the end of this slide pack.
• Maps: CCG and practice-level results are
also displayed on maps, with results split
across 5 bands (or ‘quintiles’) in order to
have a fairly even distribution at the national
level of CCGs/practices across each band.
• All data is taken from the latest / August
2018 publication (fieldwork January to
March 2018).
• For further information on using the data
please refer to the end of this slide pack.
*More than 0% but less
than 0.5%
100%Where results do not sum to
100%, or where individual
responses (e.g. fairly good;
very good) do not sum to
combined responses
(e.g. very/fairly good) this is
due to rounding, or cases
where multiple responses
are allowed.
When fewer than 10
patients respond
In cases where fewer than 10
patients have answered a
question, the data have been
suppressed and results will
not appear within the charts.
This is to prevent individuals
and their responses being
identifiable in the data.
53 of 104

17-043177-06 Version 1 | Public© Ipsos MORI
8
17-043177-06 Version 1 | Public© Ipsos MORI
Overall experience of GP practice
54 of 104

17-043177-06 Version 1 | Public© Ipsos MORI
9
84%
7%
Overall experience of GP practice
42%
40%
11%
5%Very good
Fairly good
Neither good nor poor
Fairly poor
Very poor
Q31. Overall, how would you describe your experience of your GP practice?
Practice range in CCG – % Good Local CCG range – % Good
National
6%
Good
Poor
Lowest
Performing
Highest
Performing
39% 93%
Lowest
Performing
Highest
Performing
74% 87%
%Good = %Very good + %Fairly good
%Poor = %Very poor + %Fairly poor
Base: All those completing a questionnaire: National (746,847); CCG (2,396);
Practice bases range from 24 to 131; CCG bases range from 2,174 to 7,142
CCG’s results Comparison of results
82%Good
Poor
CCG
55 of 104

17-043177-06 Version 1 | Public© Ipsos MORI
10
Results range from
to
Overall experience:
how the CCG’s results compare to other local CCGs
Comparisons are indicative only: differences may not be statistically significant
74%
87%
Percentage of patients saying ‘good’
Base: All those completing a questionnaire: CCG bases range from 2,174 to 7,142 %Good = %Very good + %Fairly good
Q31. Overall, how would you describe your experience of your GP practice?
The CCG represented by this pack is highlighted in red
56 of 104

17-043177-06 Version 1 | Public© Ipsos MORI
11
Overall experience: how the CCG’s practices compare
Percentage of patients saying ‘good’
Base: All those completing a questionnaire: Practice bases range from 24 to 131 %Good = %Very good + %Fairly good
Q31. Overall, how would you describe your experience of your GP practice?
Comparisons are indicative only: differences may not be statistically significant
Results range from
to
39%
93%
57 of 104

17-043177-06 Version 1 | Public© Ipsos MORI
12
Overall experience: how the CCG’s practices compare
Percentage of patients saying ‘good’ CCGPractices National average
Comparisons are indicative only: differences may not be statistically significant, particularly at practice level due to low numbers of responses
Base: All those completing a questionnaire: National (746,847); CCG (2,396);
Practice bases range from 24 to 131
%Good = %Very good + %Fairly good
Q31. Overall, how would you describe your experience of your GP practice?
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
GP
LE
D H
EA
LT
H C
EN
TR
E
RO
WA
NS
SU
RG
ER
Y
TA
MW
OR
TH
HO
US
E M
ED
ICA
LC
EN
TR
E.
MIT
CH
AM
FA
MIL
Y P
RA
CT
ICE
TH
E M
ITC
HA
M M
ED
ICA
L C
EN
TR
E.
MO
RD
EN
HA
LL M
ED
ICA
L C
EN
TR
E
FIG
GE
S M
AR
SH
SU
RG
ER
Y
RA
VE
NS
BU
RY
PA
RK
ME
DIC
AL
CE
NT
RE
LA
MB
TO
N R
OA
D M
ED
ICA
L P
RA
CT
ICE
GR
AN
D D
RIV
E S
UR
GE
RY
CC
G
TH
E N
ELS
ON
ME
DIC
AL P
RA
CT
ICE
CO
LLIE
RS
WO
OD
SU
RG
ER
Y
WID
E W
AY
ME
DIC
AL
CE
NT
RE
CR
ICK
ET
GR
EE
N M
ED
ICA
L P
RA
CT
ICE
TH
E V
INE
YA
RD
HIL
L R
OA
D S
UR
GE
RY
TH
E M
ER
TO
N M
ED
ICA
L P
RA
CT
ICE
FR
AN
CIS
GR
OV
E S
UR
GE
RY
PR
INC
ES
RO
AD
SU
RG
ER
Y
CE
NT
RA
L M
ED
ICA
L C
EN
TR
E
ST
ON
EC
OT
SU
RG
ER
Y
WIM
BLE
DO
N V
ILLA
GE
PR
AC
TIC
E
ALE
XA
ND
RA
SU
RG
ER
Y
RIV
ER
HO
US
E M
ED
ICA
L P
RA
CT
ICE
JA
ME
S O
'RIO
RD
AN
ME
DIC
AL
CE
NT
RE
58 of 104

17-043177-06 Version 1 | Public© Ipsos MORI
13
17-043177-06 Version 1 | Public© Ipsos MORI
Local GP services
59 of 104

17-043177-06 Version 1 | Public© Ipsos MORI
14
35%
70%65%
Not easy
Easy
Ease of getting through to GP practice on the phone
18%
47%
23%
12% Very easy
Fairly easy
Not very easy
Not at all easy
Easy
Practice range in CCG - % Easy Local CCG range - % Easy
Lowest
Performing
Highest
Performing
32% 94%
Lowest
Performing
Highest
Performing
52% 86%
%Easy = %Very easy + %Fairly easy
%Not easy = %Not very easy + %Not at all easyBase: All those completing a questionnaire excluding ‘Haven’t tried’: National (729,884); CCG (2,313);
Practice bases range from 20 to 129; CCG bases range from 2,127 to 6,975
CCG
Q1. Generally, how easy is it to get through to someone at your GP practice on the phone?*
National
30%
*Those who say ‘Haven't tried’ have been excluded from these results.
CCG’s results Comparison of results
Not easy
60 of 104

17-043177-06 Version 1 | Public© Ipsos MORI
15
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
RO
WA
NS
SU
RG
ER
Y
TH
E M
ITC
HA
M M
ED
ICA
L C
EN
TR
E.
TA
MW
OR
TH
HO
US
E M
ED
ICA
LC
EN
TR
E.
ST
ON
EC
OT
SU
RG
ER
Y
CR
ICK
ET
GR
EE
N M
ED
ICA
L P
RA
CT
ICE
GP
LE
D H
EA
LT
H C
EN
TR
E
MO
RD
EN
HA
LL M
ED
ICA
L C
EN
TR
E
LA
MB
TO
N R
OA
D M
ED
ICA
L P
RA
CT
ICE
FIG
GE
S M
AR
SH
SU
RG
ER
Y
CE
NT
RA
L M
ED
ICA
L C
EN
TR
E
CC
G
FR
AN
CIS
GR
OV
E S
UR
GE
RY
TH
E N
ELS
ON
ME
DIC
AL P
RA
CT
ICE
RA
VE
NS
BU
RY
PA
RK
ME
DIC
AL
CE
NT
RE
CO
LLIE
RS
WO
OD
SU
RG
ER
Y
ALE
XA
ND
RA
SU
RG
ER
Y
WID
E W
AY
ME
DIC
AL
CE
NT
RE
PR
INC
ES
RO
AD
SU
RG
ER
Y
MIT
CH
AM
FA
MIL
Y P
RA
CT
ICE
JA
ME
S O
'RIO
RD
AN
ME
DIC
AL
CE
NT
RE
TH
E M
ER
TO
N M
ED
ICA
L P
RA
CT
ICE
GR
AN
D D
RIV
E S
UR
GE
RY
WIM
BLE
DO
N V
ILLA
GE
PR
AC
TIC
E
RIV
ER
HO
US
E M
ED
ICA
L P
RA
CT
ICE
TH
E V
INE
YA
RD
HIL
L R
OA
D S
UR
GE
RY
Ease of getting through to GP practice on the phone:
how the CCG’s practices compare
Percentage of patients saying it is ‘easy’ to get through to someone on the phone
Comparisons are indicative only: differences may not be statistically significant, particularly at practice level due to lower numbers of responses
Base: All those completing a questionnaire excluding ‘Haven’t tried’: National (729,884); CCG (2,313);
Practice bases range from 20 to 129%Easy = %Very easy + %Fairly easy
Q1. Generally, how easy is it to get through to someone at your GP practice on the phone?
CCGPractices National average
61 of 104

17-043177-06 Version 1 | Public© Ipsos MORI
16
Not helpful
Helpfulness of receptionists at GP practice
39%
49%
10%3% Very helpful
Fairly helpful
Not very helpful
Not at all helpful
Practice range in CCG - % Helpful Local CCG range - % Helpful
National
Not helpful
90%
10%
Helpful
Lowest
Performing
Highest
Performing
68% 95%
Lowest
Performing
Highest
Performing
81% 92%
%Helpful = %Very helpful + %Fairly helpful
%Not helpful = %Not very helpful + %Not at all helpful
Base: All those completing a questionnaire excluding ‘Don’t know’: National (738,543); CCG (2,352);
Practice bases range from 22 to 127; CCG bases range from 2,155 to 7,099
87%
13%
Helpful
CCG
Q2. How helpful do you find the receptionists at your GP practice?*
*Those who say ‘Don't know’ have been excluded from these results.
CCG’s results Comparison of results
62 of 104

17-043177-06 Version 1 | Public© Ipsos MORI
17
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
RO
WA
NS
SU
RG
ER
Y
CE
NT
RA
L M
ED
ICA
L C
EN
TR
E
TA
MW
OR
TH
HO
US
E M
ED
ICA
LC
EN
TR
E.
GP
LE
D H
EA
LT
H C
EN
TR
E
TH
E M
ITC
HA
M M
ED
ICA
L C
EN
TR
E.
RIV
ER
HO
US
E M
ED
ICA
L P
RA
CT
ICE
LA
MB
TO
N R
OA
D M
ED
ICA
L P
RA
CT
ICE
CO
LLIE
RS
WO
OD
SU
RG
ER
Y
CC
G
TH
E N
ELS
ON
ME
DIC
AL P
RA
CT
ICE
CR
ICK
ET
GR
EE
N M
ED
ICA
L P
RA
CT
ICE
MO
RD
EN
HA
LL M
ED
ICA
L C
EN
TR
E
RA
VE
NS
BU
RY
PA
RK
ME
DIC
AL
CE
NT
RE
TH
E M
ER
TO
N M
ED
ICA
L P
RA
CT
ICE
ST
ON
EC
OT
SU
RG
ER
Y
MIT
CH
AM
FA
MIL
Y P
RA
CT
ICE
FIG
GE
S M
AR
SH
SU
RG
ER
Y
WID
E W
AY
ME
DIC
AL
CE
NT
RE
TH
E V
INE
YA
RD
HIL
L R
OA
D S
UR
GE
RY
GR
AN
D D
RIV
E S
UR
GE
RY
PR
INC
ES
RO
AD
SU
RG
ER
Y
FR
AN
CIS
GR
OV
E S
UR
GE
RY
JA
ME
S O
'RIO
RD
AN
ME
DIC
AL
CE
NT
RE
ALE
XA
ND
RA
SU
RG
ER
Y
WIM
BLE
DO
N V
ILLA
GE
PR
AC
TIC
E
Helpfulness of receptionists at GP practice:
how the CCG’s practices compare
Percentage of patients saying receptionists at the GP practice are ‘helpful’
Comparisons are indicative only: differences may not be statistically significant, particularly at practice level due to low numbers of responses
Base: All those completing a questionnaire excluding ‘Don’t know’: National (738,543); CCG (2,352);
Practice bases range from 22 to 127%Helpful = %Very helpful + %Fairly helpful
Q2. How helpful do you find the receptionists at your GP practice?
CCGPractices National average
63 of 104

17-043177-06 Version 1 | Public© Ipsos MORI
18
17-043177-06 Version 1 | Public© Ipsos MORI
Access to online services
64 of 104

17-043177-06 Version 1 | Public© Ipsos MORI
19
Awareness of online services
52%
37%
16%
9%
34%
41%38%
13%8%
42%
0
10
20
30
40
50
60
70
80
90
100
Bookingappointmentsonline
Ordering repeatprescriptionsonline
Accessing mymedical recordsonline
None of these Don't know
CCG
National
Comparisons are indicative only: differences may not be statistically significant
Pe
rcen
tage a
wa
re o
f o
nlin
e s
erv
ices o
ffe
red b
y
GP
pra
ctice
Base: All those completing a questionnaire: National (735,717); CCG (2,351);
Practice bases range from 24 to 125
Q4. As far as you know, which of the following online services does your GP practice offer?
Practice range
within CCG
65 of 104

17-043177-06 Version 1 | Public© Ipsos MORI
20
Online service use
20%
10%6%
74%
13% 14%
3%
79%
0
10
20
30
40
50
60
70
80
90
100
Booking appointmentsonline
Ordering repeatprescriptions online
Accessing my medicalrecords online
None of these
CCG
National
Pe
rcen
tage u
se
d o
nlin
e s
erv
ices in p
ast 1
2 m
on
ths
Comparisons are indicative only: differences may not be statistically significant
Practice range
within CCG
Base: All those completing a questionnaire: National (742,492); CCG (2,376);
Practice bases range from 24 to 128
Q5. Which of the following general practice online services have you used in the past 12 months?
66 of 104

17-043177-06 Version 1 | Public© Ipsos MORI
21
78%
22%
79%
21%
Base: All those completing a questionnaire excluding 'Haven't tried': National (234,144); CCG (893);
Practice bases range from 22 to 64; CCG bases range from 871 to 2,390
Ease of use of online services
24%
55%
14%
7% Very easy
Fairly easy
Not very easy
Not at all easy
Practice range in CCG - % Easy Local CCG range - % Easy
National
Easy
Not easy
Lowest
Performing
Highest
Performing
51% 91%
Lowest
Performing
Highest
Performing
66% 82%
CCG
Easy
Not easy
Q6. How easy is it to use your GP practice’s website to look for information or access services?*
%Easy = %Very easy + %Fairly easy
%Not easy = %Not very easy + %Not at all easy
*Those who say ‘Haven’t tried’ have been excluded from these results.
CCG’s results Comparison of results
67 of 104

17-043177-06 Version 1 | Public© Ipsos MORI
22
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
CO
LLIE
RS
WO
OD
SU
RG
ER
Y
TA
MW
OR
TH
HO
US
E M
ED
ICA
LC
EN
TR
E.
RO
WA
NS
SU
RG
ER
Y
CE
NT
RA
L M
ED
ICA
L C
EN
TR
E
CR
ICK
ET
GR
EE
N M
ED
ICA
L P
RA
CT
ICE
TH
E V
INE
YA
RD
HIL
L R
OA
D S
UR
GE
RY
ALE
XA
ND
RA
SU
RG
ER
Y
TH
E M
ITC
HA
M M
ED
ICA
L C
EN
TR
E.
FIG
GE
S M
AR
SH
SU
RG
ER
Y
CC
G
TH
E M
ER
TO
N M
ED
ICA
L P
RA
CT
ICE
PR
INC
ES
RO
AD
SU
RG
ER
Y
TH
E N
ELS
ON
ME
DIC
AL P
RA
CT
ICE
FR
AN
CIS
GR
OV
E S
UR
GE
RY
JA
ME
S O
'RIO
RD
AN
ME
DIC
AL
CE
NT
RE
MIT
CH
AM
FA
MIL
Y P
RA
CT
ICE
MO
RD
EN
HA
LL M
ED
ICA
L C
EN
TR
E
LA
MB
TO
N R
OA
D M
ED
ICA
L P
RA
CT
ICE
WIM
BLE
DO
N V
ILLA
GE
PR
AC
TIC
E
RA
VE
NS
BU
RY
PA
RK
ME
DIC
AL
CE
NT
RE
ST
ON
EC
OT
SU
RG
ER
Y
RIV
ER
HO
US
E M
ED
ICA
L P
RA
CT
ICE
GR
AN
D D
RIV
E S
UR
GE
RY
WID
E W
AY
ME
DIC
AL
CE
NT
RE
Ease of use of online services
Percentage of patients saying it is ‘easy’ to use their GP practice’s website
Comparisons are indicative only: differences may not be statistically significant, particularly at practice level due to low numbers of responses
%Easy = %Very easy + %Fairly easy Base: All those completing a questionnaire excluding 'Haven't tried': National (234,144); CCG (893);
Practice bases range from 22 to 64
Q6. How easy is it to use your GP practice’s website to look for information or access services?
CCGPractices National average
68 of 104

17-043177-06 Version 1 | Public© Ipsos MORI
23
17-043177-06 Version 1 | Public© Ipsos MORI
Making an appointment
69 of 104

17-043177-06 Version 1 | Public© Ipsos MORI
24
62%
38%
66%
34%
*Those who say ‘Doesn’t apply’ or ‘Can’t remember’ have been excluded from these results. The ‘Yes’ options are multi-code and so the summation of the three ‘Yes’ options does not equal the combined
‘Yes’ offered a choice statistic.
Choice of appointment
Practice range in CCG - % Yes Local CCG range - % Yes
National
Yes
No
Lowest
Performing
Highest
Performing
42% 86%
Lowest
Performing
Highest
Performing
57% 73%
CCG
Yes
No
Q16. On this occasion (when you last tried to make a general practice appointment), were you
offered a choice of appointment?*
%Yes = either offered a ‘Choice of place’, a ‘Choice of time or day’
or a ‘Choice of healthcare professional’
Base: All tried to make an appointment since being registered excluding ‘Doesn’t apply’ and ‘Can’t remember’: National (586,602); CCG (1,868);
Practice bases range from 16 to 106; CCG bases range from 1,750 to 5,473
9%
59%
10%
34%
Yes, a choice of place
Yes, a choice of time orday
Yes, a choice ofhealthcare professional
No, I was not offered achoice of appointment
CCG’s results Comparison of results
70 of 104

17-043177-06 Version 1 | Public© Ipsos MORI
25
Choice of appointment
Percentage of patients saying ‘yes’ they were offered a choice of appointment
Comparisons are indicative only: differences may not be statistically significant, particularly at practice level due to low numbers of responses
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
TA
MW
OR
TH
HO
US
E M
ED
ICA
LC
EN
TR
E.
RO
WA
NS
SU
RG
ER
Y
TH
E M
ITC
HA
M M
ED
ICA
L C
EN
TR
E.
CR
ICK
ET
GR
EE
N M
ED
ICA
L P
RA
CT
ICE
CO
LLIE
RS
WO
OD
SU
RG
ER
Y
GP
LE
D H
EA
LT
H C
EN
TR
E
LA
MB
TO
N R
OA
D M
ED
ICA
L P
RA
CT
ICE
PR
INC
ES
RO
AD
SU
RG
ER
Y
GR
AN
D D
RIV
E S
UR
GE
RY
CC
G
TH
E N
ELS
ON
ME
DIC
AL P
RA
CT
ICE
FR
AN
CIS
GR
OV
E S
UR
GE
RY
ST
ON
EC
OT
SU
RG
ER
Y
WIM
BLE
DO
N V
ILLA
GE
PR
AC
TIC
E
WID
E W
AY
ME
DIC
AL
CE
NT
RE
JA
ME
S O
'RIO
RD
AN
ME
DIC
AL
CE
NT
RE
RA
VE
NS
BU
RY
PA
RK
ME
DIC
AL
CE
NT
RE
TH
E M
ER
TO
N M
ED
ICA
L P
RA
CT
ICE
MIT
CH
AM
FA
MIL
Y P
RA
CT
ICE
CE
NT
RA
L M
ED
ICA
L C
EN
TR
E
FIG
GE
S M
AR
SH
SU
RG
ER
Y
TH
E V
INE
YA
RD
HIL
L R
OA
D S
UR
GE
RY
MO
RD
EN
HA
LL M
ED
ICA
L C
EN
TR
E
RIV
ER
HO
US
E M
ED
ICA
L P
RA
CT
ICE
ALE
XA
ND
RA
SU
RG
ER
Y
Base: All tried to make an appointment since being registered excluding ‘Doesn’t apply’ and ‘Can’t remember’: National (586,602); CCG (1,868);
Practice bases range from 16 to 106
Q16. On this occasion (when you last tried to make a general practice appointment), were you
offered a choice of appointment?
%Yes = %Choice of place + %Choice of time or day
+ %Choice of healthcare professional
CCGPractices National average
71 of 104

17-043177-06 Version 1 | Public© Ipsos MORI
26
6%
21%
7%
74%
20%
73%
No, took appt
Base: All tried to make an appointment since being registered: National (701,961); CCG (2,230);
Practice bases range from 21 to 121; CCG bases range from 2,074 to 6,713
Satisfaction with appointment offered
73%
21%
7% Yes, and I accepted anappointment
No, but I still took anappointment
No, and I did not take anappointment
Practice range in CCG - % Yes Local CCG range - % Yes
National
Yes, took appt
No, took appt
Lowest
Performing
Highest
Performing
48% 87%
Lowest
Performing
Highest
Performing
63% 78%
CCG
Yes, took appt
Q17. Were you satisfied with the type of appointment (or appointments) you were offered?
No, didn’t take apptNo, didn’t take appt
CCG’s results Comparison of results
72 of 104

17-043177-06 Version 1 | Public© Ipsos MORI
27
Satisfaction with appointment offered
Percentage of patients saying ‘yes’ they were satisfied with the appointment offered
Comparisons are indicative only: differences may not be statistically significant, particularly at practice level due to low numbers of responses
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
GP
LE
D H
EA
LT
H C
EN
TR
E
TA
MW
OR
TH
HO
US
E M
ED
ICA
LC
EN
TR
E.
TH
E M
ITC
HA
M M
ED
ICA
L C
EN
TR
E.
RO
WA
NS
SU
RG
ER
Y
TH
E N
ELS
ON
ME
DIC
AL P
RA
CT
ICE
MIT
CH
AM
FA
MIL
Y P
RA
CT
ICE
GR
AN
D D
RIV
E S
UR
GE
RY
FR
AN
CIS
GR
OV
E S
UR
GE
RY
LA
MB
TO
N R
OA
D M
ED
ICA
L P
RA
CT
ICE
CC
G
MO
RD
EN
HA
LL M
ED
ICA
L C
EN
TR
E
RA
VE
NS
BU
RY
PA
RK
ME
DIC
AL
CE
NT
RE
FIG
GE
S M
AR
SH
SU
RG
ER
Y
CO
LLIE
RS
WO
OD
SU
RG
ER
Y
JA
ME
S O
'RIO
RD
AN
ME
DIC
AL
CE
NT
RE
ST
ON
EC
OT
SU
RG
ER
Y
WIM
BLE
DO
N V
ILLA
GE
PR
AC
TIC
E
WID
E W
AY
ME
DIC
AL
CE
NT
RE
CE
NT
RA
L M
ED
ICA
L C
EN
TR
E
PR
INC
ES
RO
AD
SU
RG
ER
Y
CR
ICK
ET
GR
EE
N M
ED
ICA
L P
RA
CT
ICE
TH
E M
ER
TO
N M
ED
ICA
L P
RA
CT
ICE
TH
E V
INE
YA
RD
HIL
L R
OA
D S
UR
GE
RY
ALE
XA
ND
RA
SU
RG
ER
Y
RIV
ER
HO
US
E M
ED
ICA
L P
RA
CT
ICE
Base: All tried to make an appointment since being registered: National (701,961); CCG (2,230);
Practice bases range from 21 to 121
Q17. Were you satisfied with the type of appointment (or appointments) you were offered?
CCGPractices National average
73 of 104

17-043177-06 Version 1 | Public© Ipsos MORI
28
14%
6%
17%
4%
12% 14%
6%11%
34%
14%
7%11% 10% 11%
22%
11% 11%
28%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Got anappointment fora different day
Called an NHShelpline, suchas NHS 111
Went to A&E Spoke to apharmacist
Went to orcontacted
another NHSservice
Decided tocontact my
practice anothertime
Looked forinformation
online
Spoke to afriend or family
member
Didn’t see or speak to anyone
CCG
National
What patients do when they are not satisfied with the
appointment offered and do not take it
Comparisons are indicative only: differences may not be statistically significant
Perc
enta
ge
wh
o w
ent
on to
do s
om
eth
ing
els
e w
hen
did
not ta
ke the a
ppoin
tment off
ere
d
Base: All who did not take the appointment offered (excluding those who haven't tried to make one): National (32,326); CCG (121)
Q19. What did you do when you did not take the appointment you were offered?
74 of 104

17-043177-06 Version 1 | Public© Ipsos MORI
29
69%
15%
67%
15%Poor
Overall experience of making an appointment
26%
41%
18%
9%5% Very good
Fairly good
Neither good nor poor
Fairly poor
Very poor
Practice range in CCG - % Good Local CCG range - % Good
National
Good
Poor
Lowest
Performing
Highest
Performing
40% 82%
Lowest
Performing
Highest
Performing
58% 76%
%Good = %Very good + %Fairly good
%Poor = %Fairly poor + %Very poor
Base: All tried to make an appointment since being registered: National (693,912); CCG (2,215);
Practice bases range from 21 to 121; CCG bases range from 2,062 to 6,696
CCG
Q22. Overall, how would you describe your experience of making an appointment?
CCG’s results Comparison of results
Good
75 of 104

17-043177-06 Version 1 | Public© Ipsos MORI
30
Overall experience of making an appointment:
how the CCG’s practices compare
Percentage of patients saying they had a ‘good’ experience of making an appointment
Comparisons are indicative only: differences may not be statistically significant, particularly at practice level due to low numbers of responses
Base: All tried to make an appointment since being registered: National (693,912); CCG (2,215);
Practice bases range from 21 to 121
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
RO
WA
NS
SU
RG
ER
Y
GP
LE
D H
EA
LT
H C
EN
TR
E
TH
E M
ITC
HA
M M
ED
ICA
L C
EN
TR
E.
TA
MW
OR
TH
HO
US
E M
ED
ICA
LC
EN
TR
E.
FIG
GE
S M
AR
SH
SU
RG
ER
Y
TH
E N
ELS
ON
ME
DIC
AL P
RA
CT
ICE
MO
RD
EN
HA
LL M
ED
ICA
L C
EN
TR
E
CR
ICK
ET
GR
EE
N M
ED
ICA
L P
RA
CT
ICE
JA
ME
S O
'RIO
RD
AN
ME
DIC
AL
CE
NT
RE
CC
G
LA
MB
TO
N R
OA
D M
ED
ICA
L P
RA
CT
ICE
ST
ON
EC
OT
SU
RG
ER
Y
FR
AN
CIS
GR
OV
E S
UR
GE
RY
GR
AN
D D
RIV
E S
UR
GE
RY
ALE
XA
ND
RA
SU
RG
ER
Y
WID
E W
AY
ME
DIC
AL
CE
NT
RE
CE
NT
RA
L M
ED
ICA
L C
EN
TR
E
MIT
CH
AM
FA
MIL
Y P
RA
CT
ICE
RA
VE
NS
BU
RY
PA
RK
ME
DIC
AL
CE
NT
RE
CO
LLIE
RS
WO
OD
SU
RG
ER
Y
PR
INC
ES
RO
AD
SU
RG
ER
Y
RIV
ER
HO
US
E M
ED
ICA
L P
RA
CT
ICE
TH
E M
ER
TO
N M
ED
ICA
L P
RA
CT
ICE
WIM
BLE
DO
N V
ILLA
GE
PR
AC
TIC
E
TH
E V
INE
YA
RD
HIL
L R
OA
D S
UR
GE
RY
%Good = %Very good + %Fairly good
Q22. Overall, how would you describe your experience of making an appointment?
CCGPractices National average
76 of 104

17-043177-06 Version 1 | Public© Ipsos MORI
31
17-043177-06 Version 1 | Public© Ipsos MORI
Perceptions of care at patients’
last appointment
77 of 104

17-043177-06 Version 1 | Public© Ipsos MORI
32
Perceptions of care at patients’ last appointment with a
healthcare professional
Base: All had an appointment since being registered with current GP practice excluding 'Doesn't apply’:
National (706,895; 705,167; 706,882); CCG (2,239; 2,236; 2,236)
CCG’s results
*Those who say ‘Doesn’t apply’ have been excluded from these results.
Nationl results %
Poor (total)
CCG results
% Poor (total)
%Poor (total) = %Very poor + %Poor
Q26. Last time you had a general practice appointment, how good was the healthcare professional
at each of the following*
41% 47% 45%
42%40% 38%
12% 9% 12%3% 3% 3%
Giving you enough time Listening to you Treating you with care and concern
Very good Good Neither good nor poor Poor Very poor
National results
% ‘Poor’ (total)
CCG results
% ‘Poor’ (total)
Very poor
Very good
4% 3% 4%
5% 4% 5%
Giving you enough time Listening to you Treating you with care and concern
78 of 104

17-043177-06 Version 1 | Public© Ipsos MORI
33
Perceptions of care at patients’ last appointment with a
healthcare professional
Base: All had an appointment since being registered with current GP practice excluding 'Doesn't apply’:
National (628,938; 695,421; 696,267); CCG (1,987; 2,190; 2,190)
CCG’s results
Nationl results %
Poor (total)
CCG results
% Poor (total)
Q28-30. During your last general practice appointment…*
55%64% 60%
36%29% 34%
9% 6% 6%
Felt involved in decisions about care andtreatment
Had confidence and trust in thehealthcare professional
Felt their needs were met
Yes, definitely Yes, to some extent No, not at all
National results
% ‘No, not at all’
CCG results
% ‘No, not at all’
No, not at all
Yes, definitely
*Those who say ‘Don’t know / doesn’t apply’ or ‘Don’t know / can’t say’ have been excluded from these results.
7% 4% 5%
9% 6% 6%
Felt involved in decisions about care
and treatment Had confidence and trust in the
healthcare professional
Felt their needs were met
79 of 104

17-043177-06 Version 1 | Public© Ipsos MORI
34
87%
13%18%
82%
Mental health needs recognised and understood
50%
32%
18% Yes, definitely
Yes, to some extent
No, not at all
Practice range in CCG - % Yes Local CCG range - % Yes
National
Yes
No
Lowest
Performing
Highest
Performing
54% 94%
Lowest
Performing
Highest
Performing
76% 89%
%Yes = %Yes, definitely + %Yes, to some extentBase: All had an appointment since being registered with current GP practice excluding ‘I did not have any mental health needs’ or ‘Did not apply
to my last appointment’: National (277,497); CCG (905); Practice bases range from 11 to 56; CCG bases range from 817 to 3,013
*Those who say ‘I did not have any mental health needs’ or ‘Did not apply to my last appointment’ have been excluded from these results.
No
CCG
Q27. During your last general practice appointment, did you feel that the healthcare professional
recognised and/or understood any mental health needs that you might have had?*
CCG’s results Comparison of results
Yes
80 of 104

17-043177-06 Version 1 | Public© Ipsos MORI
35
17-043177-06 Version 1 | Public© Ipsos MORI
Managing health conditions
81 of 104

17-043177-06 Version 1 | Public© Ipsos MORI
36
79%
21%
74%
26%
Base: All with a long-term condition excluding ‘I haven’t needed support’ and ‘Don’t know / can’t say’: National (284,887); CCG (776);
Practice bases range from 25 to 46; CCG bases range from 704 to 2,286
Support with managing long-term health conditions
38%
36%
26%Yes, definitely
Yes, to some extent
No
Practice range in CCG - % Yes Local CCG range - % Yes
National
Yes
No
Lowest
Performing
Highest
Performing
61% 93%
Lowest
Performing
Highest
Performing
64% 84%
CCG
Yes
No
Q38. In the last 12 months, have you had enough support from local services or organisations to
help you to manage your condition (or conditions)?*
%Yes = %Yes, definitely + %Yes, to some extent
*Those who say ‘I haven’t needed support’ and ‘Don’t know / can’t say’ have been excluded from these results.
CCG’s results Comparison of results
82 of 104

17-043177-06 Version 1 | Public© Ipsos MORI
37
Percentage of patients saying ‘yes’ they have had enough support to manage their condition(s)
Comparisons are indicative only: differences may not be statistically significant, particularly at practice level due to low numbers of responses
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
MO
RD
EN
HA
LL M
ED
ICA
L C
EN
TR
E
TH
E V
INE
YA
RD
HIL
L R
OA
D S
UR
GE
RY
WIM
BLE
DO
N V
ILLA
GE
PR
AC
TIC
E
RA
VE
NS
BU
RY
PA
RK
ME
DIC
AL
CE
NT
RE
TA
MW
OR
TH
HO
US
E M
ED
ICA
LC
EN
TR
E.
ALE
XA
ND
RA
SU
RG
ER
Y
RO
WA
NS
SU
RG
ER
Y
FIG
GE
S M
AR
SH
SU
RG
ER
Y
GR
AN
D D
RIV
E S
UR
GE
RY
RIV
ER
HO
US
E M
ED
ICA
L P
RA
CT
ICE
PR
INC
ES
RO
AD
SU
RG
ER
Y
TH
E M
ER
TO
N M
ED
ICA
L P
RA
CT
ICE
CC
G
TH
E N
ELS
ON
ME
DIC
AL P
RA
CT
ICE
ST
ON
EC
OT
SU
RG
ER
Y
MIT
CH
AM
FA
MIL
Y P
RA
CT
ICE
FR
AN
CIS
GR
OV
E S
UR
GE
RY
CO
LLIE
RS
WO
OD
SU
RG
ER
Y
TH
E M
ITC
HA
M M
ED
ICA
L C
EN
TR
E.
CR
ICK
ET
GR
EE
N M
ED
ICA
L P
RA
CT
ICE
WID
E W
AY
ME
DIC
AL
CE
NT
RE
LA
MB
TO
N R
OA
D M
ED
ICA
L P
RA
CT
ICE
JA
ME
S O
'RIO
RD
AN
ME
DIC
AL
CE
NT
RE
CE
NT
RA
L M
ED
ICA
L C
EN
TR
E
Base: All with a long-term condition excluding ‘I haven’t needed support’ and ‘Don’t know / can’t say’: National (284,887); CCG (776);
Practice bases range from 25 to 46
Q38. In the last 12 months, have you had enough support from local services or organisations to
help you to manage your condition (or conditions)?
%Yes = %Yes, definitely + %Yes, to some extent
Support with managing long-term health conditions
CCGPractices National average
83 of 104

17-043177-06 Version 1 | Public© Ipsos MORI
38
17-043177-06 Version 1 | Public© Ipsos MORI
Satisfaction with general
practice appointment times
84 of 104

17-043177-06 Version 1 | Public© Ipsos MORI
39
66%
17%
67%
16%Dissatisfied
Satisfaction with appointment times
22%
46%
17%
10%
6%Very satisfied
Fairly satisfied
Neither satisfied nordissatisfied
Fairly dissatisfied
Very dissatisfied
Practice range in CCG - % Satisfied Local CCG range - % Satisfied
National
Satisfied
Dissatisfied
Lowest
Performing
Highest
Performing
34% 83%
Lowest
Performing
Highest
Performing
58% 73%
Base: All those completing a questionnaire excluding ‘I’m not sure when I can get an appointment’: National (689,659); CCG (2,209);
Practice bases range from 20 to 124; CCG bases range from 2,055 to 6,729
%Satisfied = %Very satisfied + %Fairly satisfied
%Dissatisfied = %Very dissatisfied + %Fairly dissatisfied
Satisfied
CCG
Q8. How satisfied are you with the general practice appointment times that are available to you?*
*Those who say ‘I’m not sure when I can get an appointment’ have been excluded from these results.
CCG’s results Comparison of results
85 of 104

17-043177-06 Version 1 | Public© Ipsos MORI
40
Satisfaction with appointment times:
how the CCG’s practices compare
Percentage of patients saying they are ‘satisfied’ with the appointment times available
Comparisons are indicative only: differences may not be statistically significant, particularly at practice level due to low numbers of responses
Base: All those completing a questionnaire excluding ‘I’m not sure when I can get an appointment’: National (689,659); CCG (2,209);
Practice bases range from 20 to 124
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
GP
LE
D H
EA
LT
H C
EN
TR
E
RO
WA
NS
SU
RG
ER
Y
TH
E M
ITC
HA
M M
ED
ICA
L C
EN
TR
E.
TA
MW
OR
TH
HO
US
E M
ED
ICA
LC
EN
TR
E.
WIM
BLE
DO
N V
ILLA
GE
PR
AC
TIC
E
CR
ICK
ET
GR
EE
N M
ED
ICA
L P
RA
CT
ICE
MIT
CH
AM
FA
MIL
Y P
RA
CT
ICE
FR
AN
CIS
GR
OV
E S
UR
GE
RY
GR
AN
D D
RIV
E S
UR
GE
RY
CC
G
LA
MB
TO
N R
OA
D M
ED
ICA
L P
RA
CT
ICE
RA
VE
NS
BU
RY
PA
RK
ME
DIC
AL
CE
NT
RE
PR
INC
ES
RO
AD
SU
RG
ER
Y
JA
ME
S O
'RIO
RD
AN
ME
DIC
AL
CE
NT
RE
FIG
GE
S M
AR
SH
SU
RG
ER
Y
TH
E N
ELS
ON
ME
DIC
AL P
RA
CT
ICE
ST
ON
EC
OT
SU
RG
ER
Y
CO
LLIE
RS
WO
OD
SU
RG
ER
Y
RIV
ER
HO
US
E M
ED
ICA
L P
RA
CT
ICE
TH
E V
INE
YA
RD
HIL
L R
OA
D S
UR
GE
RY
MO
RD
EN
HA
LL M
ED
ICA
L C
EN
TR
E
CE
NT
RA
L M
ED
ICA
L C
EN
TR
E
TH
E M
ER
TO
N M
ED
ICA
L P
RA
CT
ICE
WID
E W
AY
ME
DIC
AL
CE
NT
RE
ALE
XA
ND
RA
SU
RG
ER
Y
%Satisfied = %Very satisfied + %Fairly satisfied
Q8. How satisfied are you with the general practice appointment times that are available to you?
CCGPractices National average
86 of 104

17-043177-06 Version 1 | Public© Ipsos MORI
41
17-043177-06 Version 1 | Public© Ipsos MORI
Services when GP practice is closed
• The services when GP practice is closed questions are only asked of those who have recently used an NHS service when they wanted to see
a GP but their GP practice was closed. As such, the base size is often too small to make meaningful comparisons at practice level; practice
range within CCG has therefore not been included for these questions.
• Please note that patients cannot always distinguish between out-of-hours services and extended access appointments. Please view the results
in this section with the configuration of your local services in mind.
87 of 104

17-043177-06 Version 1 | Public© Ipsos MORI
42
62%
21%
6%
44%
12%
11%
2%
6%
62%
25%
5%
36%
12%
18%
5%
8%
I contacted an NHS service by telephone
A healthcare professional called me back
A healthcare professional visited me at home
I went to A&E
I saw a pharmacist
I went to another general practice service
I went to another NHS service
Can't remember
CCG National
Use of services when GP practice is closed
Base: All those who have contacted an NHS service when GP practice closed in past 12 months: National (138,025); CCG (461)
Q45. Considering all of the services you contacted, which of the following happened on that
occasion?
88 of 104

17-043177-06 Version 1 | Public© Ipsos MORI
43
36%
65%
35%
64%
64%
36%It was about right
It took too long
Time taken to receive care or advice when GP practice is closed
About right
Took too long
Local CCG range – % About right
Base: All those who have contacted an NHS service when GP practice closed in past 12 months excluding ‘Don’t know / doesn’t apply’:
National (129,429); CCG (430); CCG bases range from 394 to 1,182
Lowest
Performing
Highest
Performing
50% 69%
NationalCCG
About right
Took too long
Q46. How do you feel about how quickly you received care or advice on that occasion?*
*Those who say ‘Don’t know / doesn’t apply’ have been excluded from these results.
CCG’s results Comparison of results
89 of 104

17-043177-06 Version 1 | Public© Ipsos MORI
44
8%
91%
9%
92%
47%
45%
8% Yes, definitely
Yes, to some extent
No, not at all
Confidence and trust in staff providing services when GP
practice is closed
%Yes = %Yes, definitely + % Yes, to some extent
Yes
No
Local CCG range – % Yes
*Those who say ‘Don’t know / can’t say’ have been excluded from these results.
Lowest
Performing
Highest
Performing
86% 94%
NationalCCG
Yes
No
Q47. Considering all of the people that you saw or spoke to on that occasion, did you have
confidence and trust in them?*
Base: All those who have contacted an NHS service when GP practice closed in past 12 months excluding 'Don't know / can't say’:
National (132,710); CCG (443); CCG bases range from 401 to 1,248
CCG’s results Comparison of results
90 of 104

17-043177-06 Version 1 | Public© Ipsos MORI
45
19%
69%
15%
69%27%
42%
13%
11%
7%Very good
Fairly good
Neither good nor poor
Fairly poor
Very poor
Overall experience of services when GP practice is closed
%Good = %Very good + %Fairly good
%Poor = %Fairly poor + %Very poor
Base: All those who have contacted an NHS service when GP practice closed in past 12 months excluding 'Don't know / can't say:
National (133,444); CCG (445); CCG bases range from 405 to 1,260
Good
Poor
Local CCG range - % Good
Lowest
Performing
Highest
Performing
54% 70%
Good
Poor
NationalCCG
Q48. Overall, how would you describe your last experience of NHS services when you wanted to
see a GP but your GP practice was closed?*
*Those who say ‘Don’t know / can’t say’ have been excluded from these results.
CCG’s results Comparison of results
91 of 104

17-043177-06 Version 1 | Public© Ipsos MORI
46
17-043177-06 Version 1 | Public© Ipsos MORI
Statistical reliability
92 of 104

17-043177-06 Version 1 | Public© Ipsos MORI
47
Statistical reliability
Participants in a survey such as GPPS represent only a sample of the total population of interest – this means we cannot be certain that the results of
a question are exactly the same as if everybody within that population had taken part (“true values”). However, we can predict the variation between
the results of a question and the true value by using the size of the sample on which results are based and the number of times a particular answer is
given. The confidence with which we make this prediction is usually chosen to be 95% – that is, the chances are 95 in 100 that the true value will fall
within a specified range (the “95% confidence interval”).
The table below gives examples of what the confidence intervals look like for an ‘average’ practice and CCG, as well as the confidence intervals at
the national level.
Average sample size on
which results are based
Approximate confidence intervals for percentages at or near
these levels
Level 1:
10% or 90%
Level 2:
30% or 70%
Level 3:
50%
+/- +/- +/-
National 758,165 0.09 0.15 0.16
CCG 4,000 1.32 2.02 2.20
Practice 100 6.93 10.21 11.08
An example of confidence intervals (at national, CCG and practice level) based on the average number of responses to the question
“Overall, how would you describe your experience of your GP practice?”
For example, taking a CCG where 4,000 people responded and where 30% answered ‘Very good’ in response to ‘Overall, how would you describe
your experience of making an appointment’, there is a 95% likelihood that the true value (which would have been obtained if the whole population had
been interviewed) will fall within the range of +/-2.02 percentage points from that question’s result (i.e. between 27.98% and 32.02%).
When results are compared between separate groups within a sample, the difference may be “real” or it may occur by chance (because not everyone
in the population has been interviewed). Confidence intervals will be wider when comparing groups, especially where there are small numbers e.g.
practices where 100 patients or fewer responded to a question. These findings should be regarded as indicative rather than robust.
93 of 104

17-043177-06 Version 1 | Public© Ipsos MORI
48
17-043177-06 Version 1 | Public© Ipsos MORI
Want to know more?
94 of 104

17-043177-06 Version 1 | Public© Ipsos MORI
49
Further background information about the survey
• The survey was sent to c.2.2 million adult patients registered with a GP practice.
• Participants are sent a postal questionnaire, also with the option of completing the
survey online or via telephone.
• Past results dating back to 2007 are available for every practice in the UK. From 2017
the survey has been annual; previously it ran twice a year (June 2011 – July 2016), on a
quarterly basis (April 2009 – March 2011) and annually (January 2007 – March 2009).
• For more information about the survey please visit https://gp-patient.co.uk/.
• The overall response rate to the survey is 34.1%, based on 758,165 completed surveys.
• Weights have been applied to adjust the data to account for potential age and gender
differences between the profile of all eligible patients in a practice and the patients who
actually complete a questionnaire. Since the first wave of the 2011-2012 survey the
weighting also takes into account neighbourhood statistics, such as levels of deprivation,
in order to further improve the reliability of the findings.
• Further information on the survey including questionnaire design, sampling,
communication with patients and practices, data collection, data analysis, response
rates and reporting can be found in the technical annex for each survey year, available
here: https://gp-patient.co.uk/surveysandreports.
758,165Completed surveys in
the August 2018
publication
c.2.2mSurveys to adults
registered with an
English GP practice
34.1% National response
rate
95 of 104

17-043177-06 Version 1 | Public© Ipsos MORI
50
Where to go to do further analysis …
• For reports which show the National results broken down by CCG and Practice, go to
https://gp-patient.co.uk/surveysandreports - you can also see previous years’ results here.
• To look at the survey data at a national, CCG or practice level, and filter on a specific participant group (e.g. by
age), break down the survey results by survey question, or to create and compare different participant
‘subgroups’, go to https://gp-patient.co.uk/analysistool
• For general FAQs about the GP Patient Survey, go to https://gp-patient.co.uk/faq
96 of 104

17-043177-06 Version 1 | Public© Ipsos MORI
51
17-043177-06 Version 1 | Public© Ipsos MORI
For further information about the GP Patient Survey, please
get in touch with the GPPS team at Ipsos MORI at
We would be interested to hear any feedback you have on
this slide pack, so we can make improvements for the next
publication.
97 of 104

This page has been left blank

Cover Sheet Template for Committee Meetings Final Version 1.2 July 2018 Page 1 of 2
Merton Primary Care Commissioning Committee Date Tuesday, 02 October 2018
Document Title Estates Update
Lead Director (Name and Role)
Neil McDowell, Director of Finance
Clinical Sponsor (Name and Role)
N/A
Author(s) (Name and Role)
Lucy Lewis, Head of Estates
Agenda Item No. Attachment No.
Purpose (Tick as Required) Approve Discuss Note
Executive Summary Background: Merton CCG has four improvement schemes underway. These projects have been in the pipeline for some years and are now if the planning and delivery phase. Schemes are being funded through Estates and Transformation Technology Funding, Section 106 and Local Improvement Finance Trust (LIFT) respectively. In addition the CCG has 8 practices who have applied for Improvement Grant funding 2019/20. The report provides the committee with a high level update on progress to date and next steps. Purpose: Note Reason for Committee Review: Regular update to the committee
Key Issues: 1. The delay to the Wilson project 2. The delivery of Patrick Doody scheme in November 3. The progress with the Colliers Wood and Rowan Park schemes
Conflicts of Interest: N/A.
Mitigations: N/A
Recommendation: The Committee is asked to: Note the report and feedback any comments or areas of concern.
XX
99 of 104

Cover Sheet Template for Committee Meetings Final Version 1.2 July 2018 Page 2 of 2
Corporate Objectives This document will impact on the following CCG Objectives:
Under delegated commissioning the CCG needs to be assured that practices are providing services to patients from safe and suitable premises that are fit for purpose. Meets objectives of the STP as part of wider SWL estates strategy and feeds into London Capital Estates project reporting via that forum.
Risks This document links to the following CCG risks:
N/A
Mitigations Actions taken to reduce any risks identified:
N/A
Financial/Resource/ QIPP Implications
Financial impacts have been explored and approved through CCG’s internal financial governance processes. No further details required for this update.
Has an Equality Impact Assessment (EIA) been completed?
Yes relevant to each individual project.
Are there any known implications for equalities? If so, what are the mitigations?
None known
Patient and Public Engagement and Communication
Relevant to each individual project.
Previous Committees/ Groups Enter any Committees/ Groups at which this document has been previously considered:
Committee/Group Name: Date Discussed:
Outcome:
Click here to enter a date.
Click here to enter a date.
Click here to enter a date.
Supporting Documents
100 of 104

Merton CCG Estates Update
1. Patrick Doody Estates & Technology Transformation Fund (ETTF) Scheme
Background
An NHS England ETTF scheme to refurbish the ground floor and part first floor of
Patrick Doody Clinic 79 Pelham Road, London SW19 1NX for occupation by
Princes Road Surgery. The new site is 0.2 mile from the current premises at 51
Princes Road. Patients and staff are supportive of the refurbishment which will
provide additional ground floor consulting and treatment rooms, and dedicated
staff breakout and office space on the first floor.
The CCG approved the scheme in 2016 because the current premises, a
converted end terrace house was no longer fit for purpose for a growing list size,
and the scheme met ETTF requirements for transformation of primary care. The
CCG has taken a number of business cases through internal and external
governance to enable the scheme to be completed in 2018/19 financial year and
worked with the ETTF Programme Management Office (PMO) and NHS England
Director of Finance on obtaining 100% allocation of funds direct to NHS Property
Services for the cost of the works required.
Position to date
NHS Property Services (NHSPS) are in possession of the allocation of funds
for the works and have raised the purchase order for the contractor;
A Project Manager has been engaged by NHS Property Services to manage
the works and the move;
Primary Care colleagues are working to ensure the project plan for the move
is implemented. This is being monitored via MCCG’s Primary Care
Commissioning Operations Group (PCCOG);
The building contractor started on site Monday 24th September and has
confirmed completion of works by 24th November 2018.
Next steps
A letter will be sent to all Princes Road Surgery patients informing them of
the move date.
And update will be shared with the Wimbledon Community Forum.
Information will be shared on practice website and notice board;
CCG Estates and finance lead continue to remain actively involved in
oversight of the scheme until, and beyond completion.
101 of 104

2 | P a g e
2. Rowan Park – Section 106 Scheme
Background
Between 2012 and 2014 the former Rowan High School site, Rowan Road
Mitcham was redeveloped as part of a joint project with the Homes and
Communities Agency (HCA), Crest Nicholson Homes and Merton Council. At the
time a Section 106 (S106) agreement was put in place for a scout hall and
community facility, new medical centre and pharmacy. Rowan Park development
has been complete since 2014 however the medical centre and community
facilities are yet to be built.
Rowans Surgery plans to relocate to the new site from their existing site in Stirling
Close, Mitcham which is 0.5 miles from Rowan Park. The CCG supports the
scheme because the existing surgery premises is no longer fit for purpose and
cannot support further growth and meets our obligations to improve primary care
estate
The scheme is a high profile scheme in Mitcham with interest from local residents,
ward councillor and MP.
Position to date
The CCG approved a business case to proceed in 2016/17. Since then we have
been meeting regularly with the Council, Crest Nicholson and their delivery
partner, CMS Developments to ensure the scheme meets all the local stakeholder
requirements and remains deliverable.
Next Steps
Crest have recently put forward a series of options which are currently being
considered by all partners, this includes some further value engineering to the
medical centre specification and the addition of two residential units on the site.
We have committed to review all available options by end November 2018.
3. Colliers Wood Estates & Technology Transformation (ETTF) Scheme
Background
An ETTF Scheme to the value of £1.01m to consolidate two current outdated
separate Colliers Wood Surgery premises into one new, purpose built facility at
the current Merton Vision site at 67, Clarendon Road, Colliers Wood, SW19 2DX.
The GP practice is working with third party developer, Octopus Health and Merton
Vision’s board of trustees on the design and planning for the new building which
includes a two storey GP surgery and 200 square metres of additional clinical
space for out of hospital services.
102 of 104

3 | P a g e
The outline business case for the scheme was submitted to ETTF Programme
Management Office in August 2017. Approval on revenue implications and rent
from MCCG Finance Committee was obtained on 28th March. The CCG, GP
Partners, Merton Vision Trustees and Octopus Health hosted an event for local
councillors earlier in 2018 and followed up by sharing the outcome of the
discussion and a Q&A.
Position to date
In 2018 Octopus Healthcare focussed on engagement with Ward Councillors,
London Borough of Merton as Planning Authority and landowner, along with
engagement with Colliers Wood Residents’ Association in order to prepare the
scheme for the planning process:
As a result of successful stakeholder activity the scheme now has a set of
proposals which are in principle supported by Ward Councillors and the Residents’
Association, are capable of getting planning permission and in principle fit with the
Council’s legal framework for the site.
Next Steps
The planning application is planned to be submitted later this year with a
construction commencement date of April 2019 (subject to planning).
4. The Wilson Health & Wellbeing Campus – Local Improvement Finance
Trust (LIFT) Scheme
Background
Following an economic appraisal in 2015 it was decided that a new build on the
Wilson Hospital site was the preferred option for providing the estate to support
the delivery of new models of care. The chosen procurement route for the delivery
of the scheme is NHS LIFT (Local Improvement Finance Trust).
The Wilson will become a Health & Wellbeing Campus, addressing particular
needs of residents in the east of the borough, but available for all residents of
Merton. The Wilson will be deliberately different from a traditional health centre.
The space will support residents to stay healthy and develop stronger links with
their community, as well as deliver local wellbeing services that support people to
lead healthier lives.
Position to date
At the time of writing the CCG has reported a delay to the opening date for the
redeveloped Wilson Health and Wellbeing Campus due to discussions at a
national level between HM Treasury and Department of Health and Social Care
about policy change. As is the case for all other similar projects across England,
we must now wait for the outcome of these discussions as they will have an impact
103 of 104

4 | P a g e
on the plans and agreements we make with the developers of the Wilson. Until
then, we are unable progress with the building design and planning element of the
project with the developers. In addition, the estimated construction period for the
scheme was 20 months, however developers have further information about the
site and construction resulting in a revision of this time to 24 months.
Despite delays, our service development work and community engagement
activity is continuing as planned. Over the summer CCG colleagues attended a
range of community events and meetings to talk to people about developing the
campus. We also asked for feedback to inform the initial design for the site. A
report on the feedback we heard this summer and is being factored into the design
brief to be published in the coming weeks.
Next steps
Wilson Community Reference Group (WCRG), made up of local residents and
community organisations, to support and advise us throughout the programme’s
lifetime. We hope to hold the first meeting in early November.
A Social Enterprise will be set up that will have oversight of the wellbeing services
and we plan this to be in place by the end of March 2019.
Merton CCG’s Wilson Service Design & Commissioning Group continues to work
on the detailed design of the services and commissioning model for the campus.
5. Improvement Grant Funding
Merton has 8 applications pending approval by NHS England’s Improvement
Grant (IG) funding programme management office. Funding can be applied for a
wide variety of practice improvements from large extensions to replacement doors.
All applications must meet the criteria set out by the IG team and practices will be
required to contribute 34% towards the cost of the works.
Practices will receive notification of whether or not their scheme has been
approved from January 2019 onwards following a process of prioritisation across
the STP.
Last year Wide Way Medical Centre and Central Medical Centre both successfully
used IG funding to improve and extend their current premises.
104 of 104


















