T235 Bam! Pow! Wham! Algorithms & Case Studies: Flipped Classroom...
16
T235 Bam! Pow! Wham! Algorithms & Case Studies: Flipped Classroom Superpowers Ariel S. McGarry, MSPAS, PA-C Anne Schempp, MPAS, PA-C
Transcript of T235 Bam! Pow! Wham! Algorithms & Case Studies: Flipped Classroom...

T235 Bam! Pow! Wham! Algorithms & Case Studies: Flipped Classroom Superpowers
Ariel S. McGarry, MSPAS, PA-C Anne Schempp, MPAS, PA-C

Using Algorithms & Case Studies to Harness Teaching Superpowers in
the Flipped Classroom! Presented by:
Algorithm Girl (Ariel McGarry, MSPAS, PA-C)
Casewoman (Anne Schempp, MPAS, PA-C) Assembled in our underground lair at Shenandoah University
https://twitter.com/bamchallenge http://jrjp.org/just-say-pow/ http://www.cardboardsafari.com/products/wham-board/

Before We Get Started, Let’s Chat...
1.What do we know about CLINICAL DECISION MAKING in the didactic PA classroom?
a.How is clinical decision making defined? b.What are the components? c.Why is it difficult?
1.What do we know about the FLIPPED CLASSROOM? a.How is the flipped/inverted classroom defined? b.What are the components c.Why is it difficult?
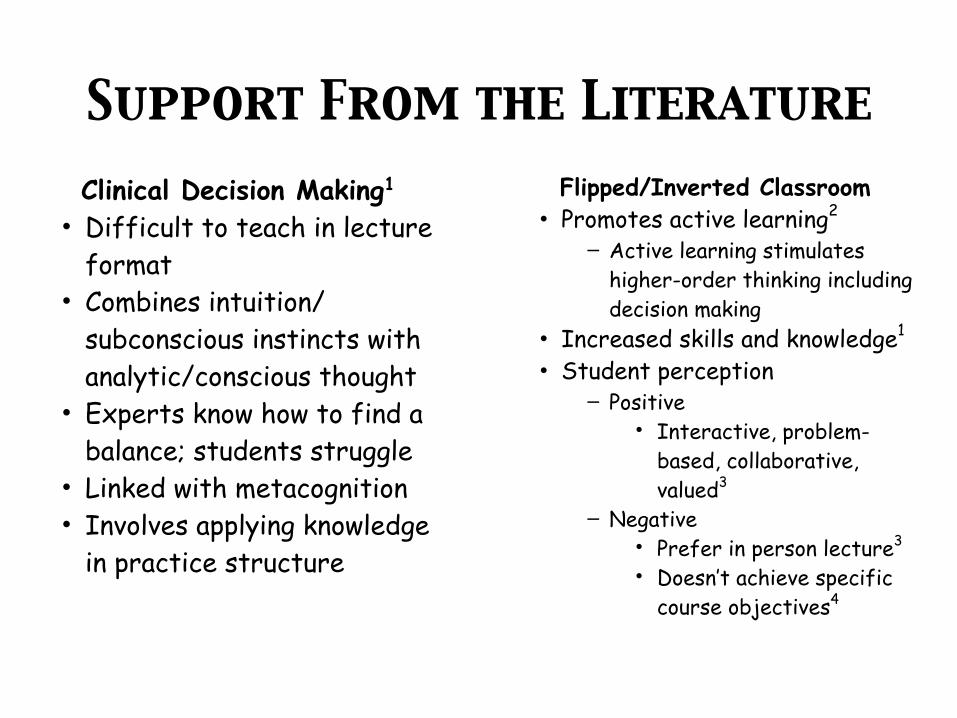
Support From the LiteratureClinical Decision Making1
• Difficult to teach in lecture format
• Combines intuition/subconscious instincts with analytic/conscious thought
• Experts know how to find a balance; students struggle
• Linked with metacognition • Involves applying knowledge
in practice structure
Flipped/Inverted Classroom • Promotes active learning2
– Active learning stimulates higher-order thinking including decision making
• Increased skills and knowledge1
• Student perception – Positive
• Interactive, problem-based, collaborative, valued3
– Negative
• Prefer in person lecture3
• Doesn’t achieve specific course objectives4
Today’s Evil Villain
The Differential Diagnosis
Why is the DDx so EVIL?
• It requires application of ALL medical knowledge (but using the DDx in cases increases skills in disease and clinical management).5
• It is CHALLENGING and often DAUNTING to students.3
• Without a good DDx, the students have NO IDEA where they are headed in the clinical decision-making process.
• It takes practice. Lots of practice.
http://www.keepcalm-o-matic.co.uk/p/keep-calm-and-create-a-differential-diagnosis-2/#
https://twitter.com/punchbampow

Here’s an Idea!
Goal: Development of clinical decision making skills through the development and modification of a differential
diagnosis based on presenting symptoms in the didactic classroom Steps:
1.Work through a symptom based algorithm a.Start with a presenting symptom b.Introduce new findings c.Illicit diagnoses that fit within the combination of symptoms
2.Work through an interactive case with the same presenting symptom
An Example
Algorithm: Hematemesis/Melena
Case: cc “vomiting blood”
Now Your Turn!
Discussion of Activity
What did you experience doing the activity?

Student Responses
“... thanks for using these
algorithms! I am a visual learner and I really like
them!”
“I really got a lot out of the recitations
when we made the algorithms and
discussed why each disease would fall under each step of
the algorithm.” “I love the algorithms!”

http://eternalremont.blogspot.com/2010_03_01_archive.html
Resources
1.The 5-Minute Clinical Consult
2.Algorithmic Diagnosis of Symptoms
and Signs
3.From Symptom to Diagnosis
4.Up-to-date
5.Case Files®

References1. Crebbin W, Beasley SW, Watters, DAK. Clinical decision making: how surgeons do it. ANZ Journal
of Surgery, January 2013;83:422-428. 2. McLaughlin J, Roth M, Mumper R, et al. The flipped classroom: a course redesign to foster learning
and engagement in a health professions school. Academic Medicine: Journal Of The Association Of American Medical Colleges [serial online]. February 2014;89(2):236-243. Available from: MEDLINE, Ipswich, MA. Accessed May 29, 2015.
3. Bösner S, Pickert J, Stibane T. Teaching differential diagnosis in primary care using an inverted classroom approach: student satisfaction and gain in skills and knowledge. BMC Medical Education [serial online]. April 1, 2015;15:63. Available from: MEDLINE, Ipswich, MA. Accessed May 27, 2015.
4. Strayer J. How learning in an inverted classroom influences cooperation, innovation and task orientation. Learning Environments Research [serial online]. July 2012;15(2):171-193. Available from: Education Research Complete, Ipswich, MA. Accessed May 27, 2015.
5. Macallan D, Kent A, Holmes S, Farmer E, McCrorie P. A model of clinical problem-based learning for clinical attachments in medicine. Medical Education [serial online]. August 2009;43(8):799-807. Available from: CINAHL Plus with Full Text, Ipswich, MA. Accessed May 27, 2015.
6. Stern SC, Cifu AS, Altkorn D. GI Bleeding. In: Stern SC, Cifu AS, Altkorn D. eds.Symptom to Diagnosis: An Evidence-Based Guide, 3e. New York, NY: McGraw-Hill; 2014. http://accessmedicine.mhmedical.com/content.aspx?bookid=1088&Sectionid=61698830. Accessed October 15, 2015.
7. Dambro M, Griffith H. Griffith's 5-Minute Clinical Consult, 2006. Philadelphia, Pa.: Lippincott Williams & Wilkins; 2006.
http://www.meridianschools.org/Eagle/Teachers/FifthGrade/Price/Pages/Price,Jake.aspx
How will YOU choose to HARNESS your
NEW TEACHING SUPERPOWERS?