
Systemic therapy: HER-2 update - · PDF fileSystemic therapy: HER-2 update ... • AND...
30
Hans Wildiers Multidisciplinair Borst Centrum/Algemene medische oncologie UZ Leuven Systemic therapy: HER-2 update
-
Upload
duongtuyen -
Category
Documents
-
view
220 -
download
4
Transcript of Systemic therapy: HER-2 update - · PDF fileSystemic therapy: HER-2 update ... • AND...

Hans Wildiers Multidisciplinair Borst Centrum/Algemene medische oncologie
UZ Leuven
Systemic therapy: HER-2 update
• New drugs
• Strategic issues
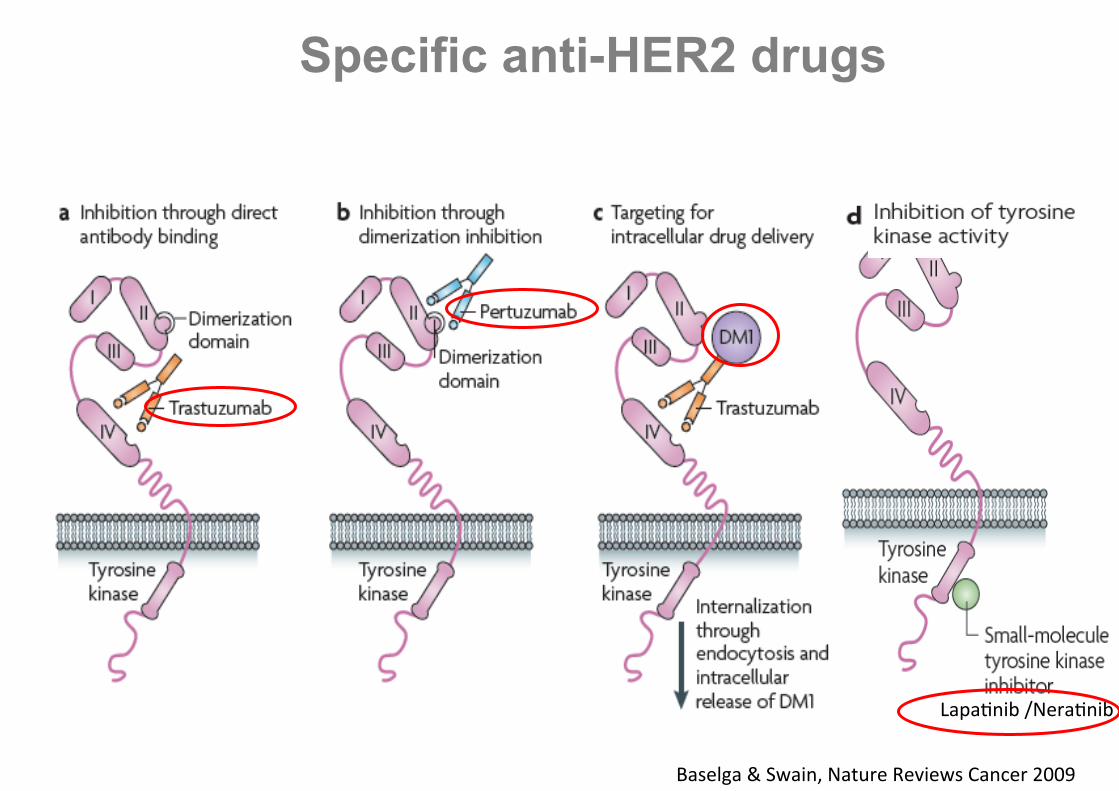
Specific anti-HER2 drugs
Lapa$nib /Nera$nib
Baselga & Swain, Nature Reviews Cancer 2009

Pertuzumab: NeoSphere
THP (n=107) docetaxel + trastuzumab + pertuzumab
HP (n=107) trastuzumab + pertuzumab
TP (n=96) docetaxel + pertuzumab
S
U
R
G
E
R
Y
docetaxel q3w x 4→FEC q3w x 3 trastuzumab q3w cycles 5–17
FEC q3w x 3 trastuzumab q3w cycles 5–17
FEC q3w x 3 trastuzumab q3w cycles 5–17
FEC q3w x 3 trastuzumab q3w cycles 5–21
Study dosing: q3w x 4
TH (n=107) docetaxel + trastuzumab
Patients with operable or
locally advanced /inflammatory*
HER2-positive BC
Chemo-naïve & primary tumors >2cm (N=417)
SABCS 2010 Lancet Oncol 2012

H, trastuzumab; P, pertuzumab; T, docetaxel
Pertuzumab: NeoSphere pCR rates
p = 0.0141 50
40
30
20
10
0 TH THP HP TP
pCR, % p = 0.0198
p = 0.003
29.0
45.8
16.8 24.0
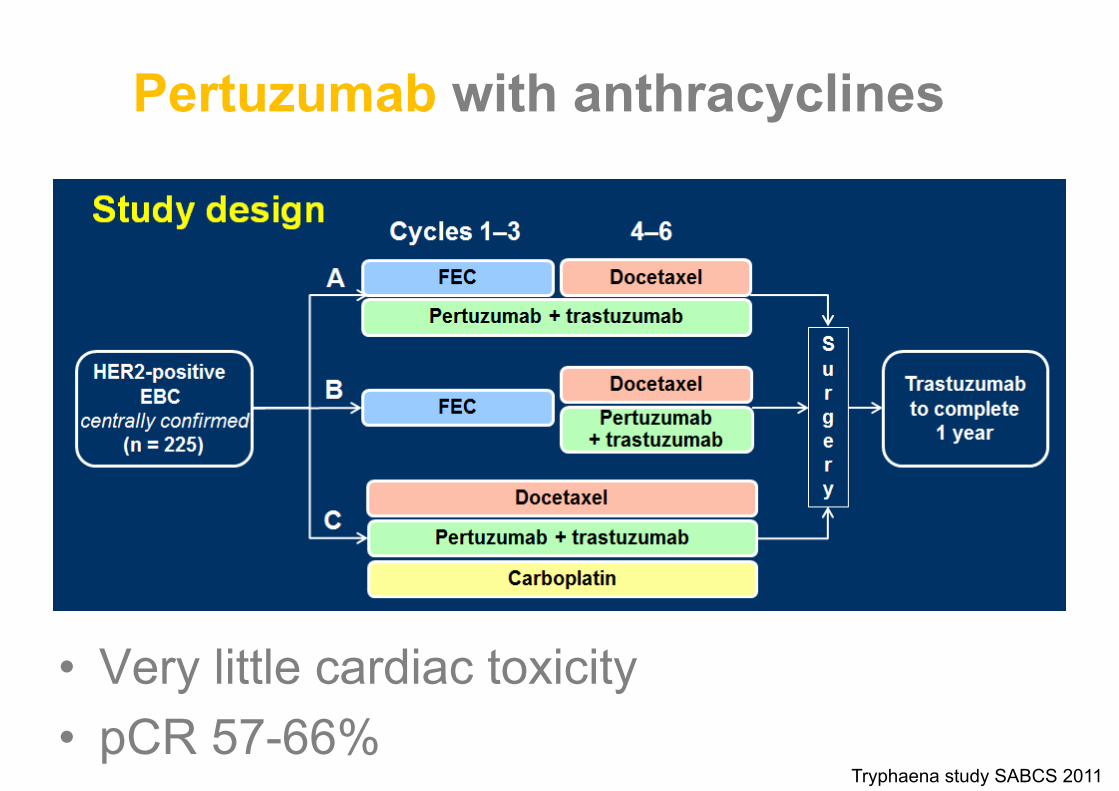
Pertuzumab with anthracyclines
• Very little cardiac toxicity • pCR 57-66%
Tryphaena study SABCS 2011
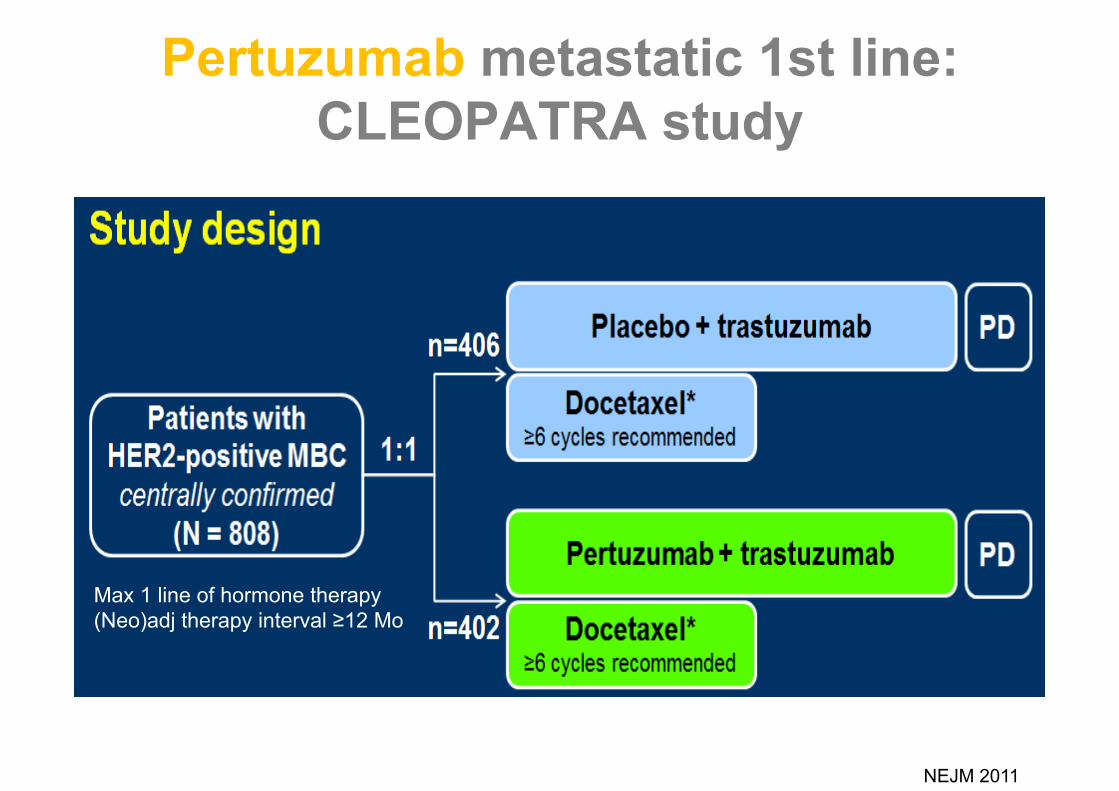
Pertuzumab metastatic 1st line: CLEOPATRA study
Max 1 line of hormone therapy (Neo)adj therapy interval ≥12 Mo
NEJM 2011

RR 80,2% vs 69,3%
Pertuzumab metastatic 1st line: CLEOPATRA study


Pertuzumab (P) after Trastuzumab (T)
• 29 pts progressive during T • Start P monotherapy:
– ORR 3% (1 pt), CBR 10% • Re-addition of T :
– ORR 17%, CBR 41%
JCO 212 Cortez.
→ P + T more active than monotherapy !

T-DM1
Single agent activity - 112 pts with progression after at least one line of
antiHER2 therapy (median of 5 prior systemic agents in metastatic setting)
- ORR 26% - PFS 4,6 months - Toxicity limited: hypokalemia, thrombocytopenia, liver
test disturbance JCO 2011 Burris

T-DM1 PFS
Hurvitz, ESMO 2011

EMILIA Study Design
1:1
HER2+ (central) LABC or MBC
(N=980)
• Prior taxane and trastuzumab
• Progression on metastatic tx or within 6 mos of adjuvant tx
PD
T-DM1
3.6 mg/kg q3w IV
Capecitabine 1000 mg/m2 orally bid, days 1–14, q3w
+ Lapatinib
1250 mg/day orally qd
PD
T-DM1
ESMO 2012

ORR 43,6% vs 30,8% Duration of Response 12,6 vs 6,5 months Much less toxic !
T-DM1 EMILIA results

Lapatinib: NEO-ALLTO trial
Stratification: • T ≤ 5 cm vs. T > 5 cm • ER or PgR + vs. ER & PgR – • N 0-1 vs. N ≥ 2 • Conservative surgery or not
Invasive operable HER2+ BC T > 2 cm (inflammatory BC excluded) LVEF ≥ 50% N=450
34 weeks 52 weeks of anti-HER2 therapy
lapatinib
trastuzumab
lapatinib trastuzumab
FEC X 3
S U R G E R Y
R A N D O M I Z E
lapatinib
trastuzumab
lapatinib trastuzumab
paclitaxel
paclitaxel
paclitaxel
+ 12 wks 6 wks
SABCS 2010

Lapatinib: Neo-ALLTO pCR rates
Lancet 2012

Lapatinib
• More toxic: diarrhea (21% gr III), rash, (liver)
• Waiting ALLTO trial: Lapatinib alone inferior!
• Other trials showing inferiority of L vs T (e.g. Capecitabine L vs T)
• L + T remains interesting
Neratinib
• Irreversible panHER TKI • High activity:
– RR 24% if prior Trast. – RR 56% in Trast-naïve pts
• Toxicity: up to 30% gr III-IV diarrhea
Ann Oncol 2010

• New drugs
• Strategic issues

Adjuvant treatment in HER2+
• Anthracycline–Taxane or TCH chemo • Trastuzumab
– 1y = standard – potentially useful from 0.5 cm (pT1bN0) – If chemo possible, best to combine T with chemo – T concomitant with Taxanes > sequential
• Other antiHER2 drugs: wait for ALLTO and Aphinity trial

Update on duration of Trast.
• HERA: 2y = 1y
• Phare: 6 Mo non inferior to 12 Mo
→ 1y Trast. remains standard
ESMO 2012

Increasing chaos …
• Number of drugs ↗ • Number of patients ↘ • Availability (reimbursement) =
‘suboptimal’
Metastatic

ER pos HER2 pos
• Chemo + T as efficient as in ER neg
• Hormone therapy – Tamoxifen: relative resistance? – Anastrozole +/- T: PFS 4.8 vs 2.4 mo – Letrozole +/- L: PFS 8.2 vs 3.0 mo PFS in HER2+ (no benefit in HER2 neg)
JCO 2005 Cui et al
R/ options • Taxane-T Monotherapie: RR ± 50-80% • Vinorelbine (30-35 mg/m2) –T vs Docetaxel (100 mg/m2)–T
TTP 15.3 vs 12.4 md OS 38.8 vs 35.7 md FN 10 % vs 36 % (p <0.05)
• Capecitabine + L < Capecitabine + H • L + T • platinum, gemcitabine, liposomal anthracycline (+/- T) • …
Andersson. JCO 2011
Metastatic: hormoneINsensitive/resistant

Near future
Cortes ESMO 2012
Reimbursement in Belgium • Taxanes: fortunately solved recently
• Trastuzumab: – Monotherapy after failure of anthracyclines and taxanes – With paclitaxel 1st line if ‘anthracycline are not considered’ – With docetaxel 1st line if docetaxel is reimbursed
• Aromatase inhibitors: ‘after anti-E’
• Lapatinib: – + Letrozole in ER+
• At this moment no indication for chemo • AND no previous trastuzumab or chemo for MBC • AND contraindication for anti-estrogeen • AND contraindication for trastuzumab (report from cardiologist)
– + Capecitabine, after failure of anthracycline-taxane-Trastuzumab
• Pertuzumab/T-DM1: let’s cross fingers !
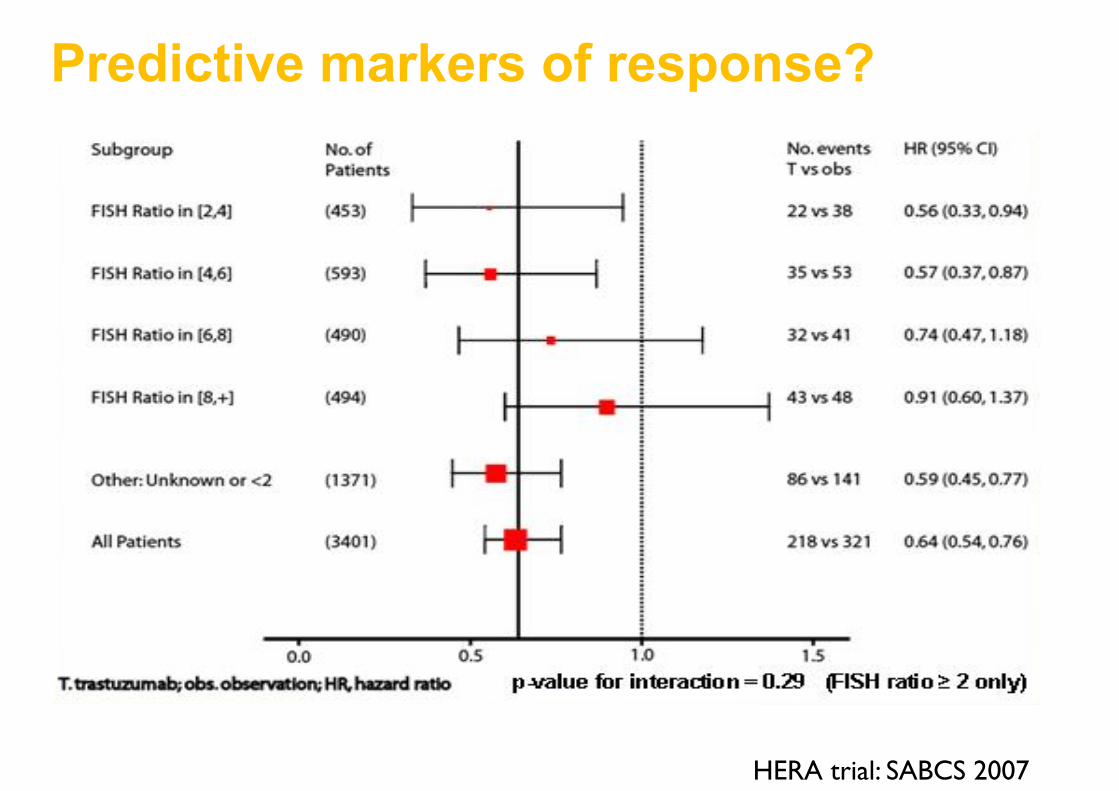
HERA trial: DFS by central FISH ratio
HERA trial: SABCS 2007)
Predictive markers of response?
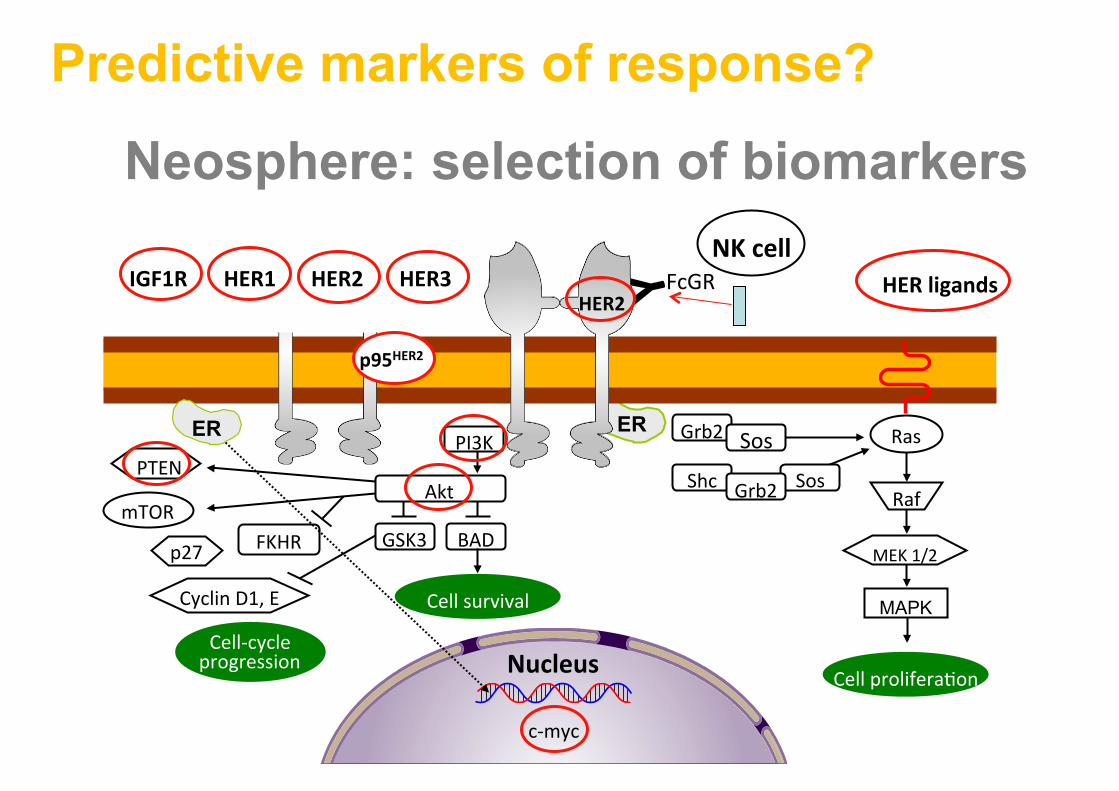
Neosphere: selection of biomarkers
ER
Nucleus
c-‐myc
Raf
MEK 1/2
MAPK
Akt
GSK3 BAD
Cell-‐cycle progression
PTEN
mTOR
p27
Cyclin D1, E
FKHR
Grb2 Sos
Cell survival
Ras
Shc Sos Grb2
PI3K
Cell prolifera$on
HER ligands NK cell
FcGR Y
ER
p95HER2
HER2 HER1 HER2 HER3 IGF1R
Predictive markers of response?

Conclusions from NeoSphere biomarker analyses • HER2 expression (H-score) associated with sensitivity to
pertuzumab • PIK3CA mutations in exon 9 linked to lack of sensitivity to
HER2-directed MAb’s • Intrinsic differences between HER2-positive tumors based
on hormone receptor status • No predictive role for truncated forms of the HER2 receptor
including p95HER2 • So far none of the analyses provided clinically useful
assays for patient and/or regimen selection in addition or alternative to the conventional assessment of HER2 by IHC or FISH
2
Predictive markers of response?

Conclusions: HER2+ breast cancer
• Wealth of drugs available (more and more specific with limited toxicity)
• Major challenge is how to use/combine/sequence these drugs
• Drug availability/reimbursement is a threat • Can we get rid of chemo?


















