
SYSTEMATIC REVIEW Patient complaints in healthcare systems: a systematic review … · Patient...
12
Patient complaints in healthcare systems: a systematic review and coding taxonomy Tom W Reader, Alex Gillespie, Jane Roberts Department of Social Psychology, London School of Economics, London, UK Correspondence to Dr Tom Reader, Department of Social Psychology, London School of Economics, Houghton Street, London WC2A 2AE, UK; [email protected] Received 27 August 2013 Revised 14 March 2014 Accepted 4 May 2014 Published Online First 29 May 2014 To cite: Reader TW, Gillespie A, Roberts J. BMJ Qual Saf 2014;23:678–689. ABSTRACT Background Patient complaints have been identified as a valuable resource for monitoring and improving patient safety. This article critically reviews the literature on patient complaints, and synthesises the research findings to develop a coding taxonomy for analysing patient complaints. Methods The PubMed, Science Direct and Medline databases were systematically investigated to identify patient complaint research studies. Publications were included if they reported primary quantitative data on the content of patient- initiated complaints. Data were extracted and synthesised on (1) basic study characteristics; (2) methodological details; and (3) the issues patients complained about. Results 59 studies, reporting 88 069 patient complaints, were included. Patient complaint coding methodologies varied considerably (eg, in attributing single or multiple causes to complaints). In total, 113 551 issues were found to underlie the patient complaints. These were analysed using 205 different analytical codes which when combined represented 29 subcategories of complaint issue. The most common issues complained about were ‘treatment’ (15.6%) and ‘communication’ (13.7%). To develop a patient complaint coding taxonomy, the subcategories were thematically grouped into seven categories, and then three conceptually distinct domains. The first domain related to complaints on the safety and quality of clinical care (representing 33.7% of complaint issues), the second to the management of healthcare organisations (35.1%) and the third to problems in healthcare staff–patient relationships (29.1%). Conclusions Rigorous analyses of patient complaints will help to identify problems in patient safety. To achieve this, it is necessary to standardise how patient complaints are analysed and interpreted. Through synthesising data from 59 patient complaint studies, we propose a coding taxonomy for supporting future research and practice in the analysis of patient complaint data. INTRODUCTION Patient complaints provide a valuable source of insight into safety-related pro- blems within healthcare organisations. 1 Patients are sensitive to, and able to recog- nise, a range of problems in healthcare delivery, 2 some of which are not identified by traditional systems of healthcare moni- toring (eg, incident reporting systems, retrospective case reviews). 3 Thus, patient complaints can provide important and additional information to healthcare orga- nisations on how to improve patient safety. 4 Furthermore, analysing data on negative patient experiences strengthens the ability of healthcare organisations to detect systematic problems in care. This has recently been highlighted in the UK through the Francis report 5 on 1200 unnecessary deaths that occurred over 3 years at Mid-Staffordshire NHS Foundation hospital. The report found that, over the duration of the incident, written patients complaints had identified the problems of neglect and poor care at the trust. Yet, deficiencies in complaint handling meant critical warning signs were missed, and numerous challenges in using patient complaint data to improve patient safety were highlighted. 6 Healthcare organisations receive huge volumes of complaints (eg, over 100 000 annually on hospital care in the NHS), and complaints can focus on diverse pro- blems (from car parking to prescribing errors), describe different types of harm (eg, physical, emotional), have legal or malpractice implications, and have differ- ent underlying aims (eg, resolving dissatis- faction, creating change, preventing future issues). 7–9 The level of standardisation of techniques used to analyse patient com- plaints is unclear, and there may be benefit in developing a standardised and Open Access Scan to access more free content SYSTEMATIC REVIEW 678 Reader TW, et al. BMJ Qual Saf 2014;23:678–689. doi:10.1136/bmjqs-2013-002437 on April 13, 2020 by guest. Protected by copyright. http://qualitysafety.bmj.com/ BMJ Qual Saf: first published as 10.1136/bmjqs-2013-002437 on 29 May 2014. Downloaded from
Transcript of SYSTEMATIC REVIEW Patient complaints in healthcare systems: a systematic review … · Patient...
Patient complaints in healthcaresystems: a systematic reviewand coding taxonomy
Tom W Reader, Alex Gillespie, Jane Roberts
Department of SocialPsychology, London School ofEconomics, London, UK
Correspondence toDr Tom Reader, Department ofSocial Psychology, LondonSchool of Economics, HoughtonStreet, London WC2A 2AE, UK;[email protected]
Received 27 August 2013Revised 14 March 2014Accepted 4 May 2014Published Online First29 May 2014
To cite: Reader TW,Gillespie A, Roberts J. BMJQual Saf 2014;23:678–689.
ABSTRACTBackground Patient complaints have beenidentified as a valuable resource for monitoringand improving patient safety. This article criticallyreviews the literature on patient complaints, andsynthesises the research findings to develop acoding taxonomy for analysing patient complaints.Methods The PubMed, Science Direct andMedline databases were systematically investigatedto identify patient complaint research studies.Publications were included if they reported primaryquantitative data on the content of patient-initiated complaints. Data were extracted andsynthesised on (1) basic study characteristics; (2)methodological details; and (3) the issues patientscomplained about.Results 59 studies, reporting 88 069 patientcomplaints, were included. Patient complaintcoding methodologies varied considerably (eg, inattributing single or multiple causes to complaints).In total, 113 551 issues were found to underlie thepatient complaints. These were analysed using 205different analytical codes which when combinedrepresented 29 subcategories of complaint issue.The most common issues complained about were‘treatment’ (15.6%) and ‘communication’(13.7%). To develop a patient complaint codingtaxonomy, the subcategories were thematicallygrouped into seven categories, and then threeconceptually distinct domains. The first domainrelated to complaints on the safety and quality ofclinical care (representing 33.7% of complaintissues), the second to the management ofhealthcare organisations (35.1%) and the third toproblems in healthcare staff–patient relationships(29.1%).Conclusions Rigorous analyses of patientcomplaints will help to identify problems in patientsafety. To achieve this, it is necessary to standardisehow patient complaints are analysed andinterpreted. Through synthesising data from 59patient complaint studies, we propose a codingtaxonomy for supporting future research andpractice in the analysis of patient complaint data.
INTRODUCTIONPatient complaints provide a valuablesource of insight into safety-related pro-blems within healthcare organisations.1
Patients are sensitive to, and able to recog-nise, a range of problems in healthcaredelivery,2 some of which are not identifiedby traditional systems of healthcare moni-toring (eg, incident reporting systems,retrospective case reviews).3 Thus, patientcomplaints can provide important andadditional information to healthcare orga-nisations on how to improve patientsafety.4 Furthermore, analysing data onnegative patient experiences strengthensthe ability of healthcare organisations todetect systematic problems in care. Thishas recently been highlighted in the UKthrough the Francis report5 on 1200unnecessary deaths that occurred over3 years at Mid-Staffordshire NHSFoundation hospital. The report foundthat, over the duration of the incident,written patients complaints had identifiedthe problems of neglect and poor care atthe trust. Yet, deficiencies in complainthandling meant critical warning signswere missed, and numerous challenges inusing patient complaint data to improvepatient safety were highlighted.6
Healthcare organisations receive hugevolumes of complaints (eg, over 100 000annually on hospital care in the NHS),and complaints can focus on diverse pro-blems (from car parking to prescribingerrors), describe different types of harm(eg, physical, emotional), have legal ormalpractice implications, and have differ-ent underlying aims (eg, resolving dissatis-faction, creating change, preventing futureissues).7–9 The level of standardisation oftechniques used to analyse patient com-plaints is unclear, and there may bebenefit in developing a standardised and
Open AccessScan to access more
free content
SYSTEMATIC REVIEW
678 Reader TW, et al. BMJ Qual Saf 2014;23:678–689. doi:10.1136/bmjqs-2013-002437
on April 13, 2020 by guest. P
rotected by copyright.http://qualitysafety.bm
j.com/
BM
J Qual S
af: first published as 10.1136/bmjqs-2013-002437 on 29 M
ay 2014. Dow
nloaded from

reliable taxonomy for analysing and interpreting (interms of patient safety) complaint data. To achieve this,we provide the first systematic review of empiricalresearch on patient complaints. The aim of the reviewis to outline the practices used to code and analysepatient complaints, and to describe the types andprevalence of issues underlying patient complaints.Furthermore, through data synthesis, we develop a tax-onomy for guiding and standardising the future ana-lysis of patient complaints, with the purpose being tosupport research and practice on analysing and usinginformation reported in letters of patient complaints.
Patient letters of complaintPatient complaints usually refer to an ‘expression ofgrievance’ and ‘dispute within a health care setting’.10
They are often formal letters written to a healthcareorganisation (or regulator) after a threshold of dissatis-faction with care has been crossed.11 Typically, com-plaints are made by patients or families.12 To resolvecomplaints, healthcare institutions usually create dia-logue on the complaint, investigate it and reach aresolution for the individual patient (eg, apologise,reject, compensate).10 In considering how patientcomplaint data might be used to identify or reduceproblems in patient safety, a number of distinguishingfeatures of patient complaints require discussion.First, patient complaints do not reflect a systematic
investigation of failure; instead, they represent individ-ual patient experiences. Complaints are unstandar-dised, although can report incidences of physical ormental harm.10 Second, patient complaints are oftenemotive. They can describe anger and distress, withthe skills and attitudes of individual healthcare profes-sionals being criticised. Third, patient complaints maynot be put forward to improve healthcare provision,and thus may not explicitly highlight key learningpoints that could be used to improve healthcare ser-vices. Fourth, patient complaints often prioritiseproblems in interactions with healthcare staff,7 13
leading to a focus on subjective and less procedura-lised aspects of treatment (eg, compassion anddignity), and how they interact with quality andsafety.14 Fifth, patient complaints can be madewithout an awareness of the wider system pressuresinfluencing care (eg, staff workloads), meaning theymay not identify all of the contributory factorsleading to a problem in care.Nonetheless, patient complaint data can provide
unique patient-centred insights into aspects of carethat may not be easily captured through traditionalquality and safety metrics (eg, dignity). Crucially,when patient complaints are considered at an aggre-gate level (eg, a hospital), they potentially indicateproblematic trends in healthcare provision. Rigorousand systematic analytical procedures are essential iflearning from patient complaints is to be facilitated.For example, in understanding the causes of adverse
events, highly systematic and standardised investiga-tory techniques have been developed for analysingmedical errors (eg, using human factors frameworksto identify causal factors15). These have facilitated the(i) generation of normative data on the frequency,nature and causes of adverse events;16 (ii) identifica-tion of challenges for different healthcare organisa-tions/specialities;17 and (iii) interventions based oncausal analyses.15 Similar rigour may be beneficial inextracting safety-related data from patient complaints.To contribute to future patient complaint research(and the patient safety literature more generally) ourreview has two aims.The first aim is to systematically review quantitative
articles reporting primary data on patient complaintsin order to assess the nature and quality of the patientcomplaint research literature. We do this through:1. Describing the characteristics of patient complaint
studies.2. Describing the methodologies used to collect and
analyse patient complaint data.The second aim is to synthesise quantitative data on
the type and prevalence of issues that underlie patientcomplaints, and to propose a patient complaintcoding taxonomy for guiding future research andpractice. We do this through:3. Reporting on and consolidating the issues identified as
underlying patient complaints across the literature.4. Sorting and thematically grouping the issues identified as
underlying patient complaints in order to develop a data-driven patient complaint coding taxonomy.
METHODStudy selectionThis is the first systematic literature review on patientcomplaints in healthcare institutions. Accordingly, noprotocol exists to guide the review, and so standard pro-tocols for systematic review were applied.18 The startingeligibility criteria were articles reporting primary dataon patient complaints in English. A search strategy toselect relevant papers was then applied. Figure 1describes the study selection procedure.For stage 1, the search terminology was designed to
limit the number of studies with the term ‘complaint’in order that a relevant and manageable number ofpapers could be identified (‘complaint’ is a verycommon medical term). Studies were only identified ifthe word ‘complaint’ featured (or a common synonym,such as grievance or letter, or antonym such as satisfac-tion) alongside the words ‘care’, ‘quality’ or ‘safety’ inthe title or abstract. This meant papers referring to theterm ‘complaint’ only were not included.For stage 2, the abstracts of articles with titles of
relevance were inspected. For stage 3, the inclusioncriteria identified articles with complaints submittedby patients on poor healthcare experiences (or repre-senting third-parties), and excluded those where com-plaints were not initiated by patients or significant
Systematic review
Reader TW, et al. BMJ Qual Saf 2014;23:678–689. doi:10.1136/bmjqs-2013-002437 679
on April 13, 2020 by guest. P
rotected by copyright.http://qualitysafety.bm
j.com/
BM
J Qual S
af: first published as 10.1136/bmjqs-2013-002437 on 29 M
ay 2014. Dow
nloaded from
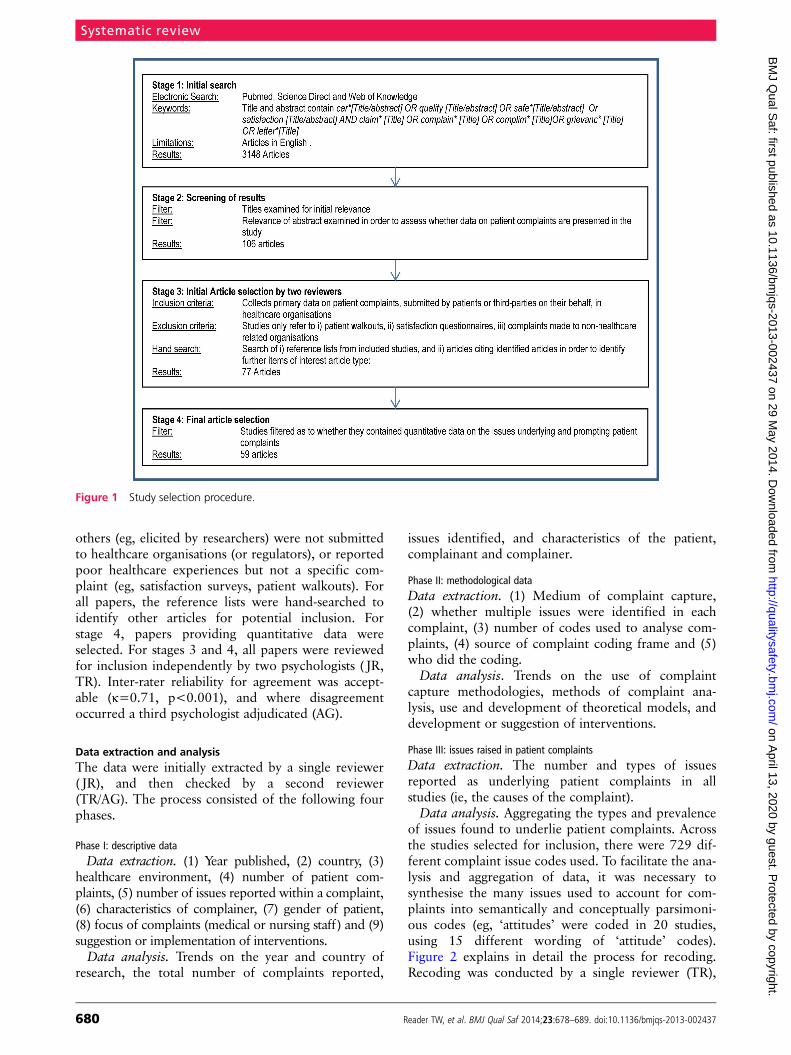
others (eg, elicited by researchers) were not submittedto healthcare organisations (or regulators), or reportedpoor healthcare experiences but not a specific com-plaint (eg, satisfaction surveys, patient walkouts). Forall papers, the reference lists were hand-searched toidentify other articles for potential inclusion. Forstage 4, papers providing quantitative data wereselected. For stages 3 and 4, all papers were reviewedfor inclusion independently by two psychologists ( JR,TR). Inter-rater reliability for agreement was accept-able (κ=0.71, p<0.001), and where disagreementoccurred a third psychologist adjudicated (AG).
Data extraction and analysisThe data were initially extracted by a single reviewer( JR), and then checked by a second reviewer(TR/AG). The process consisted of the following fourphases.
Phase I: descriptive dataData extraction. (1) Year published, (2) country, (3)
healthcare environment, (4) number of patient com-plaints, (5) number of issues reported within a complaint,(6) characteristics of complainer, (7) gender of patient,(8) focus of complaints (medical or nursing staff) and (9)suggestion or implementation of interventions.Data analysis. Trends on the year and country of
research, the total number of complaints reported,
issues identified, and characteristics of the patient,complainant and complainer.
Phase II: methodological dataData extraction. (1) Medium of complaint capture,(2) whether multiple issues were identified in eachcomplaint, (3) number of codes used to analyse com-plaints, (4) source of complaint coding frame and (5)who did the coding.Data analysis. Trends on the use of complaint
capture methodologies, methods of complaint ana-lysis, use and development of theoretical models, anddevelopment or suggestion of interventions.
Phase III: issues raised in patient complaintsData extraction. The number and types of issuesreported as underlying patient complaints in allstudies (ie, the causes of the complaint).Data analysis. Aggregating the types and prevalence
of issues found to underlie patient complaints. Acrossthe studies selected for inclusion, there were 729 dif-ferent complaint issue codes used. To facilitate the ana-lysis and aggregation of data, it was necessary tosynthesise the many issues used to account for com-plaints into semantically and conceptually parsimoni-ous codes (eg, ‘attitudes’ were coded in 20 studies,using 15 different wording of ‘attitude’ codes).Figure 2 explains in detail the process for recoding.Recoding was conducted by a single reviewer (TR),
Figure 1 Study selection procedure.
Systematic review
680 Reader TW, et al. BMJ Qual Saf 2014;23:678–689. doi:10.1136/bmjqs-2013-002437
on April 13, 2020 by guest. P
rotected by copyright.http://qualitysafety.bm
j.com/
BM
J Qual S
af: first published as 10.1136/bmjqs-2013-002437 on 29 M
ay 2014. Dow
nloaded from
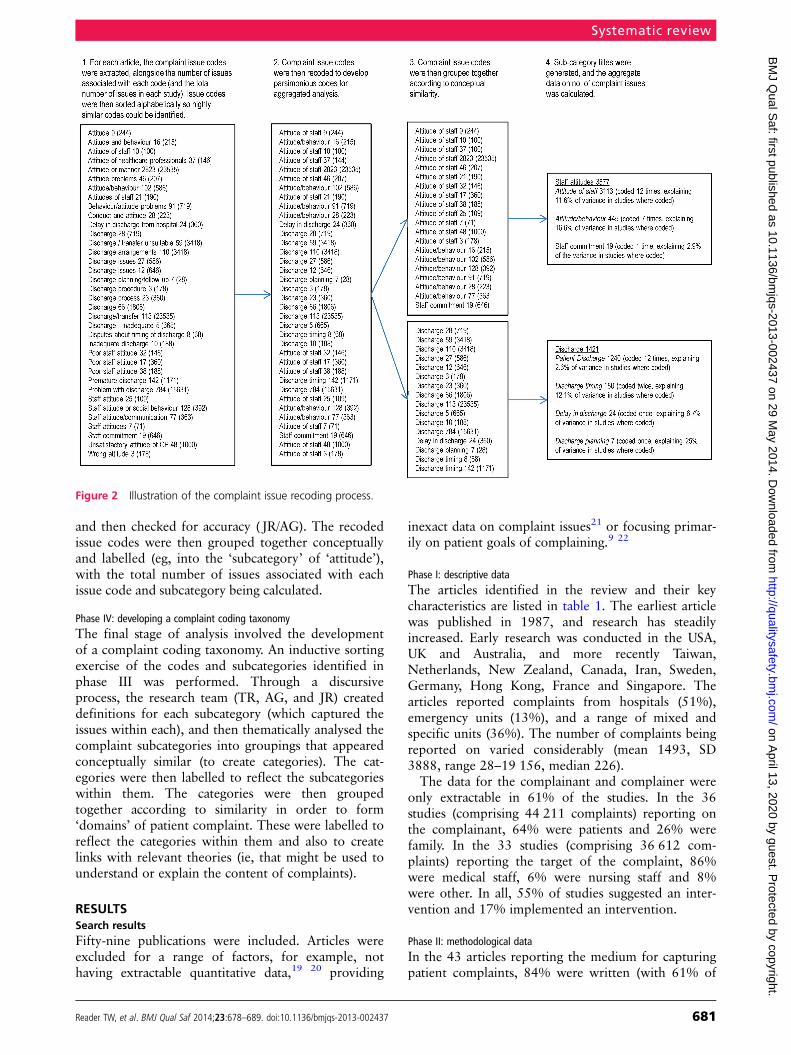
and then checked for accuracy ( JR/AG). The recodedissue codes were then grouped together conceptuallyand labelled (eg, into the ‘subcategory’ of ‘attitude’),with the total number of issues associated with eachissue code and subcategory being calculated.
Phase IV: developing a complaint coding taxonomyThe final stage of analysis involved the developmentof a complaint coding taxonomy. An inductive sortingexercise of the codes and subcategories identified inphase III was performed. Through a discursiveprocess, the research team (TR, AG, and JR) createddefinitions for each subcategory (which captured theissues within each), and then thematically analysed thecomplaint subcategories into groupings that appearedconceptually similar (to create categories). The cat-egories were then labelled to reflect the subcategorieswithin them. The categories were then groupedtogether according to similarity in order to form‘domains’ of patient complaint. These were labelled toreflect the categories within them and also to createlinks with relevant theories (ie, that might be used tounderstand or explain the content of complaints).
RESULTSSearch resultsFifty-nine publications were included. Articles wereexcluded for a range of factors, for example, nothaving extractable quantitative data,19 20 providing
inexact data on complaint issues21 or focusing primar-ily on patient goals of complaining.9 22
Phase I: descriptive dataThe articles identified in the review and their keycharacteristics are listed in table 1. The earliest articlewas published in 1987, and research has steadilyincreased. Early research was conducted in the USA,UK and Australia, and more recently Taiwan,Netherlands, New Zealand, Canada, Iran, Sweden,Germany, Hong Kong, France and Singapore. Thearticles reported complaints from hospitals (51%),emergency units (13%), and a range of mixed andspecific units (36%). The number of complaints beingreported on varied considerably (mean 1493, SD3888, range 28–19 156, median 226).The data for the complainant and complainer were
only extractable in 61% of the studies. In the 36studies (comprising 44 211 complaints) reporting onthe complainant, 64% were patients and 26% werefamily. In the 33 studies (comprising 36 612 com-plaints) reporting the target of the complaint, 86%were medical staff, 6% were nursing staff and 8%were other. In all, 55% of studies suggested an inter-vention and 17% implemented an intervention.
Phase II: methodological dataIn the 43 articles reporting the medium for capturingpatient complaints, 84% were written (with 61% of
Figure 2 Illustration of the complaint issue recoding process.
Systematic review
Reader TW, et al. BMJ Qual Saf 2014;23:678–689. doi:10.1136/bmjqs-2013-002437 681
on April 13, 2020 by guest. P
rotected by copyright.http://qualitysafety.bm
j.com/
BM
J Qual S
af: first published as 10.1136/bmjqs-2013-002437 on 29 M
ay 2014. Dow
nloaded from

Table 1 Descriptive and methodological characteristics of identified article
Authors Year CountryHealthcareenvironment
No. ofcomplaintsreported
System-levelintervention
Single ormultiplecoding
No. ofcodesused
Source ofcodingframe
Complaintcoded by
Schwartz and Overton23 1987 USA Emergency 244 Suggested Single 12 NR Secretarial staff
Chande et al24 1991 USA Hospital 176 Suggested Single 11 NR Healthcare staff
Owen25 1991 UK Primary care 1000 NR* Single 13 NR Author(s)
Burstein and Fleisher26 1991 USA Hospital 67 Suggested Multiple 4 NR Unit manager
Hunt and Glucksman27 1991 UK Emergency 122 Suggested Multiple 11 NR Author(s)
Donaldson andCavanagh28
1992 UK Hospital 71 Suggested Multiple 6 NR Healthcare staff
Kadzombe and Coals29 1992 UK Emergency 66 NR Multiple 8 NR Unit manager
Hanson et al30 1994 Australia Child A&E 71 Suggested Single 5 NR Parents
Allsop31 1994 UK Surgery 110 NR Multiple 6 Literature Author(s)
Bark et al7 1994 UK Hospital 491 Suggested Multiple 9 Literature Author(s)
Lloyd-Bostock andMulcahy10†
1994 UK Hospital 399 Implemented Multiple 36 Developed Author(s)
Nettleton and Harding32 1994 UK Multiple 107 NR Multiple 43 NR Author(s)
Curka et al33 1995 USA Emergency 371 Suggested Single 8 NR Unit manager
Webb34 1995 UK Hospital 188 Suggested Single 18 NR Healthcare staff
Ingram and Roy35 1995 UK Psychiatric 47 NR Multiple 10 NR Author(s)
Mulholland andDawson36
1998 NZ Multiple 146 Suggested Single 5 NR Author(s)
Mace37 1998 USA Hospital 28 Implemented Single 5 NR Healthcare staff
Lim et al38 1998 Singapore Clinics 226 NR Multiple 38 NR Complaint staff
Daniel et al39 1999 Australia Multiple 290 NR Single 12 NR Complaint staff
Pichert et al40† 1999 USA Hospital 6419 Implemented Multiple 15 Developed Complaint staff
Allen et al41‡ 2000 USA Hospital 3984 Implemented Single 5 Developed Patients
Halperin42 2000 USA Multiple 29 NR Single 5 NR Complaint staff
Anderson et al43 2000 Australia Hospital 127 NR Multiple 17 NR Patient advisor
Pitarka-Carcani et al44 2000 UK Psychiatric 100 Implemented Multiple 23 NR NR
Anderson et al45 2001 Australia Hospital 1308 NR Multiple 8 NR Patient advisor
Powers andBendall-Lyon46
2002 USA Hospital 211 NR Single 5 Literature Complaint staff
Taylor et al47 2002 Australia Emergency 2419 Suggested Multiple 43 NR Complaint staff
Colwell et al48 2003 USA Emergency 286 Suggested Single 10 NR Unit manager
Choy et al49 2004 Hong Kong Hospital 241 Suggested Multiple 4 NR NR
Taylor et al50 2004 Australia Hospital 19 156 Suggested Multiple 7 NR Complaint staff
Wofford et al51 2004 USA Hospital 222 Suggested Multiple 7 Developed Author(s)
Stelfox et al52 2005 USA Hospital 483 NR Single 2 NR NR
Friele and Sluijs53 2006 Netherlands Hospital 424 NR Multiple 4 Literature Patients
Chavan et al54 2007 UK Eye infirmary 94 Implemented Single 6 NR Complaint staff
Cowan and Wilson55† 2007 UK Surgery 526 Suggested Single 6 NR Healthcare staff
Kline et al56 2007 Canada Hospital 586 Suggested Single 11 NR Complaint staff
Saravanan et al57 2007 UK Hospital 100 Suggested Single 6 NR NR
Siyambalapitiya et al58† 2007 UK Hospital 183 Suggested Single 6 NR Complaint staff
Natangelo59 2007 Italy Hospital 151 Suggested Multiple 6 Literature Healthcare staff
Wong et al60 2007 Singapore Emergency 175 Suggested Multiple 16 NR Author(s)
Haw et al61 2008 UK Psychiatric 392 Implemented Single 15 NR Complaint staff
Friele et al62 2008 Netherlands Hospital 279 Suggested Multiple 5 Literature Patients
Montini et al63 2008 USA Hospital 1216 Implemented Multiple 22 Developed Author(s)
Giugliani et al64 2009 France Hospital 164 NR Single 6 NR Healthcare staff
Parry and Hewage65 2009 Australia Hospital 101 Suggested Single 4 NR Complaint staff
Jangland et al13 2009 Sweden Hospital 105 Implemented Multiple 14 Literature Author(s)
Levtzion-Korach et al3 2010 USA Hospital 4722 Suggested Multiple 8 Literature Author(s)
Continued
Systematic review
682 Reader TW, et al. BMJ Qual Saf 2014;23:678–689. doi:10.1136/bmjqs-2013-002437
on April 13, 2020 by guest. P
rotected by copyright.http://qualitysafety.bm
j.com/
BM
J Qual S
af: first published as 10.1136/bmjqs-2013-002437 on 29 M
ay 2014. Dow
nloaded from
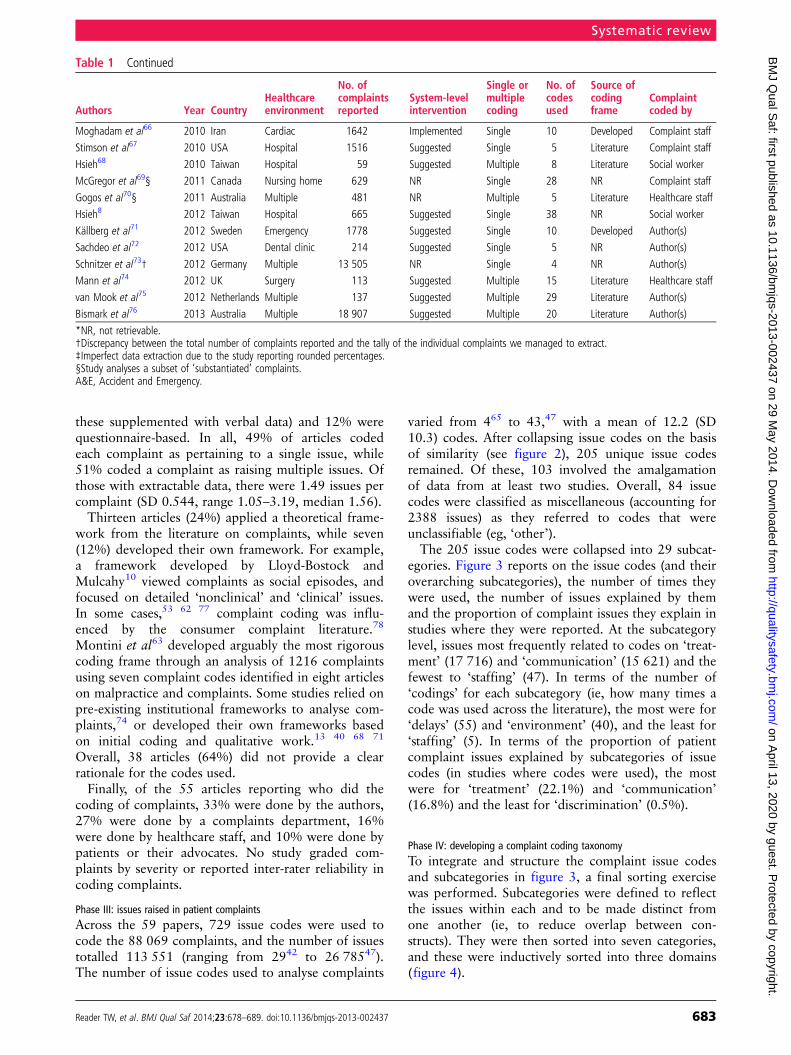
these supplemented with verbal data) and 12% werequestionnaire-based. In all, 49% of articles codedeach complaint as pertaining to a single issue, while51% coded a complaint as raising multiple issues. Ofthose with extractable data, there were 1.49 issues percomplaint (SD 0.544, range 1.05–3.19, median 1.56).Thirteen articles (24%) applied a theoretical frame-
work from the literature on complaints, while seven(12%) developed their own framework. For example,a framework developed by Lloyd-Bostock andMulcahy10 viewed complaints as social episodes, andfocused on detailed ‘nonclinical’ and ‘clinical’ issues.In some cases,53 62 77 complaint coding was influ-enced by the consumer complaint literature.78
Montini et al63 developed arguably the most rigorouscoding frame through an analysis of 1216 complaintsusing seven complaint codes identified in eight articleson malpractice and complaints. Some studies relied onpre-existing institutional frameworks to analyse com-plaints,74 or developed their own frameworks basedon initial coding and qualitative work.13 40 68 71
Overall, 38 articles (64%) did not provide a clearrationale for the codes used.Finally, of the 55 articles reporting who did the
coding of complaints, 33% were done by the authors,27% were done by a complaints department, 16%were done by healthcare staff, and 10% were done bypatients or their advocates. No study graded com-plaints by severity or reported inter-rater reliability incoding complaints.
Phase III: issues raised in patient complaintsAcross the 59 papers, 729 issue codes were used tocode the 88 069 complaints, and the number of issuestotalled 113 551 (ranging from 2942 to 26 78547).The number of issue codes used to analyse complaints
varied from 465 to 43,47 with a mean of 12.2 (SD10.3) codes. After collapsing issue codes on the basisof similarity (see figure 2), 205 unique issue codesremained. Of these, 103 involved the amalgamationof data from at least two studies. Overall, 84 issuecodes were classified as miscellaneous (accounting for2388 issues) as they referred to codes that wereunclassifiable (eg, ‘other’).The 205 issue codes were collapsed into 29 subcat-
egories. Figure 3 reports on the issue codes (and theiroverarching subcategories), the number of times theywere used, the number of issues explained by themand the proportion of complaint issues they explain instudies where they were reported. At the subcategorylevel, issues most frequently related to codes on ‘treat-ment’ (17 716) and ‘communication’ (15 621) and thefewest to ‘staffing’ (47). In terms of the number of‘codings’ for each subcategory (ie, how many times acode was used across the literature), the most were for‘delays’ (55) and ‘environment’ (40), and the least for‘staffing’ (5). In terms of the proportion of patientcomplaint issues explained by subcategories of issuecodes (in studies where codes were used), the mostwere for ‘treatment’ (22.1%) and ‘communication’(16.8%) and the least for ‘discrimination’ (0.5%).
Phase IV: developing a complaint coding taxonomyTo integrate and structure the complaint issue codesand subcategories in figure 3, a final sorting exercisewas performed. Subcategories were defined to reflectthe issues within each and to be made distinct fromone another (ie, to reduce overlap between con-structs). They were then sorted into seven categories,and these were inductively sorted into three domains(figure 4).
Table 1 Continued
Authors Year CountryHealthcareenvironment
No. ofcomplaintsreported
System-levelintervention
Single ormultiplecoding
No. ofcodesused
Source ofcodingframe
Complaintcoded by
Moghadam et al66 2010 Iran Cardiac 1642 Implemented Single 10 Developed Complaint staff
Stimson et al67 2010 USA Hospital 1516 Suggested Single 5 Literature Complaint staff
Hsieh68 2010 Taiwan Hospital 59 Suggested Multiple 8 Literature Social worker
McGregor et al69§ 2011 Canada Nursing home 629 NR Single 28 NR Complaint staff
Gogos et al70§ 2011 Australia Multiple 481 NR Multiple 5 Literature Healthcare staff
Hsieh8 2012 Taiwan Hospital 665 Suggested Single 38 NR Social worker
Källberg et al71 2012 Sweden Emergency 1778 Suggested Single 10 Developed Author(s)
Sachdeo et al72 2012 USA Dental clinic 214 Suggested Single 5 NR Author(s)
Schnitzer et al73† 2012 Germany Multiple 13 505 NR Single 4 NR Author(s)
Mann et al74 2012 UK Surgery 113 Suggested Multiple 15 Literature Healthcare staff
van Mook et al75 2012 Netherlands Multiple 137 Suggested Multiple 29 Literature Author(s)
Bismark et al76 2013 Australia Multiple 18 907 Suggested Multiple 20 Literature Author(s)
*NR, not retrievable.†Discrepancy between the total number of complaints reported and the tally of the individual complaints we managed to extract.‡Imperfect data extraction due to the study reporting rounded percentages.§Study analyses a subset of ‘substantiated’ complaints.A&E, Accident and Emergency.
Systematic review
Reader TW, et al. BMJ Qual Saf 2014;23:678–689. doi:10.1136/bmjqs-2013-002437 683
on April 13, 2020 by guest. P
rotected by copyright.http://qualitysafety.bm
j.com/
BM
J Qual S
af: first published as 10.1136/bmjqs-2013-002437 on 29 M
ay 2014. Dow
nloaded from

Figure 4 was developed in a bottom-up mannerand develops a tri-level system of complaint coding.At the top-level, it distinguishes among the domains
of ‘clinical’, ‘management’ and ‘relationship’ for ana-lysing patient complaints. The ‘clinical’ domain(33.7% of complaint issues) pertains to patient
Figure 3 List of complaint issue codes and subcategories.
Systematic review
684 Reader TW, et al. BMJ Qual Saf 2014;23:678–689. doi:10.1136/bmjqs-2013-002437
on April 13, 2020 by guest. P
rotected by copyright.http://qualitysafety.bm
j.com/
BM
J Qual S
af: first published as 10.1136/bmjqs-2013-002437 on 29 M
ay 2014. Dow
nloaded from

reports on poor quality care (23 414 issues) and safetyincidents (14 929 issues), and conceptually thesecategories relate to the human factors and safety lit-erature.79 80 The ‘management’ domain (35.1%) per-tains to problems in waiting times/access to care(16 043 issues) and institutional management (23 787issues), and may be understood in terms of literatureson service and organisational management.81–83
Finally, the ‘relationship’ domain (29.1%) considerspatient complaints on interactions and experiences ofhealthcare professionals. These refer to communica-tory acts between patients and staff (20 683 issues),the humaneness and caring nature of staff (7955issues), and failures to fulfil basic patient rights(4352 issues). These categories reflect psychology lit-eratures on communication and dialogue,84 compas-sion and emotional care,85 86 and workplace ruleviolations.87–89 It is notable that for the subcategoriesof ‘communication’ and ‘patient rights’ reported infigure 3, these were incorporated into the ‘category’level as they did not provide insight at the subcategorylevel (ie, they were umbrella terms and highlygeneral), and the subcategory of ‘miscellaneous’ wasnot included (meaning the taxonomy has 26subcategories).Finally, using the taxonomy to reflect on the patient
complaint studies, it was found that there were differ-ent distributions of complaints between studies thatcoded complaints as having a single (29 studies) ormultiple (30) issues. Single coded complaints reportedmore ‘institutional issues’ (35.6% vs 16.3%) andfewer problems in ‘communication’ (14.3% vs 19.4%)and ‘quality’ (12.5% vs 23.1%).
DISCUSSIONInvestigations of patient complaints are increasing,both in total number and countries represented.Analyses of patient complaints serve two key functions
within healthcare organisations. First, they allow forthe concerns of specific patients to be met, for redressto occur and for solutions to be designed for solvingcase-specific safety problems. Second, they canprovide insight into system-wide problems in patientcare and allow for comparisons between healthcareorganisations. The latter requires aggregate analyses ofpatient complaints in order that patient complaintdata can be used to identify safety and quality issueswithin healthcare systems or conditions (eg, manage-ment problems) that increase the likelihood of poorcare. Of the 59 papers reviewed in this study, patientswere found to complain almost equally on thedomains of ‘clinical’, ‘management’ and ‘relation-ships’. Some institutional factors appear morespecific to certain healthcare systems (eg, finance andbilling in the USA), while others are more generic(eg, delays). Overall, 39% of complaint issues focuson two of the seven categories, ‘communication’ and‘treatment’, and a further 13% of complaint issuesrelate to ‘safety’.
Methodological issues in coding patient complaintsThe review highlights a lack of standardised codifica-tion or analytical techniques for analysing complaints.System-wide analyses of patient complaint data willremain difficult unless the following inconsistenciesare addressed.First, there is little standardisation of the procedures
for analysing complaints (eg, training) or the purposeof data collection (ie, for redressing individual com-plaints or system-wide issues). In addition, the processof who handles and codes complaints differs consider-ably between studies, with little data on coding reli-ability. Second, the process of complaint coding varieswidely, with different codes and frameworks (or noneat all) being used. Research studies code and mix dataat both the category and subcategory level, and often
Figure 4 Patient complaint taxonomy.
Systematic review
Reader TW, et al. BMJ Qual Saf 2014;23:678–689. doi:10.1136/bmjqs-2013-002437 685
on April 13, 2020 by guest. P
rotected by copyright.http://qualitysafety.bm
j.com/
BM
J Qual S
af: first published as 10.1136/bmjqs-2013-002437 on 29 M
ay 2014. Dow
nloaded from

do not apply a theoretical framework. Third, thecodes used sometimes pertain to the stage of health-care (ie, referral, examination, treatment) and some-times to problems at a more general level (ie, safetyincident, delays, staff attitudes). Fourth, in some cases,patient complaints are treated as representing oneissue, and in others multiple issues (51% of studies).Multiple coding is more rigorous, and reveals patientcomplaints to focus on several interconnected aspectsof healthcare. Fifth, where multiple issues are coded,complaint studies do not link issues within complaintstogether (eg, staff attitudes as precursors to adverseevents), meaning complaints about one issue (eg, com-munication) cannot be linked to another (eg, clinicalharm). Sixth, complaint studies do not typicallycollect data on the reliability of complaint analyses oron the severity of patient complaint (standard withinadverse event studies).90 Seventh, because patientcomplaint letters are usually focused on the initialcommunique to healthcare providers, additional infor-mation found through follow-up studies (eg, inter-views) are rarely incorporated into analyses. Finally,safety issues were only coded in 60% of the studies,yet where coded they often accounted for a consider-able proportion of complaints, indicating the potentialutility of analysing patient complaints to identifysafety-specific data.
Patient complaint coding taxonomyTo overcome some of the issues highlighted above, wehave developed a three-level complaint coding tax-onomy (figure 4). It is designed to provide a standar-dised and comprehensive system for aiding researchersand practitioners to identify, code and interpret theissues raised within a letter of complaint. Trends onbroader constructs can be then developed (eg, pro-blems in bureaucracy and safety incidents), anddetailed at a more specific level (ie, subcategory).Furthermore, patient complaint data can be inter-preted and analysed through concepts and literaturesthat appear associated with the category and domainlevels. For example, theory on communication anddialogue,84 compassion and caring,85 86 and rule vio-lations87–89 may facilitate analysis of ‘relationship’problems. Alternatively, human factors theory appearsessential for understanding issues relating to safetyproblems.79 80 It is notable that the separation of therelational and clinical/management issues correspondsto the sociological literature which describes health-care in terms of a clash between ‘system’ (clinical andmanagement) factors and ‘lifeworld’ (relationship)concerns.90 91 Examining the tensions between‘relationships’ and ‘system’ issues within healthcareorganisations may be useful for understanding andlearning from patient complaints (eg, on how‘systems’ shape patient perspectives of care).91 92
The taxonomy draws on previous research, forexample that which attempted to develop
parsimonious codes for analysing patient complaints,63
and the conceptual distinctions made between thetypes of issues raised within a patient complaint.10 78 Itcombines these different approaches, and uses thecoded content of 88 069 complaints (and the 113 551issues within them) to ensure comprehensiveness.Inconsistencies found across the set of studies, forexample, the coding of communication at category andsubcategory levels and the use of ’umbrella’ concepts,are reduced.The taxonomy may be beneficial for developing
international standards to analyse patient complaints,and would emulate work conducted on adverse eventanalysis standardisation.93–95 For example, systematicframeworks have been developed to standardise theidentification and analysis of contributory factorsleading to adverse events.96 Contributory factorsunderlying adverse events show them having a highcommonality internationally,97 and developing a simi-larly universal taxonomy and procedure for analysingpatient complaints would allow for international learn-ing and benchmarking (eg, at present consensus isoften lacking between studies on the concepts used toanalyse complaints). As indicated by the patient safetyliterature,3 this is likely to focus on different issuesthan those capture by adverse event analysis taxon-omies; for example, subjective concepts such as com-passion and sensitivity, which patients view asimportant, but cannot be easily managed by the organ-isation98 and are not typically investigated throughadverse event taxonomies.99
Future investigations of patient complaintsIn developing and implementing the codingtaxonomy described in figure 4, three stages may beundertaken.First, the reliability and usability of the complaint
coding taxonomy should be assessed; for example,through having different raters use the taxonomy tocode a sample of patient complaints. This wouldallow an assessment of the extent to which informa-tion on each domain, category and subcategory can bereliably coded with a letter of complaint.Second, the taxonomy should be used to structure the
analysis and interpretation of patient complaint data.For example, in understanding where within the careprocess problems occurred (ie, identified by the use ofthe taxonomy to analyse patient complaints), theirseverity (eg, threat to patient safety) and their impactupon patient outcomes (eg, harm). An underlying flawin patient complaint research is the mixing of data onstages of care (eg, examinations, treatment) and moregeneric problems (eg, communication, staff skills), andfurther conceptual development is required to betterunderstand how these interact within the taxonomy.Third, using the taxonomy, patient complaint
data might be subject to more sophisticated analysesat the aggregate level; for example, analysing a national
Systematic review
686 Reader TW, et al. BMJ Qual Saf 2014;23:678–689. doi:10.1136/bmjqs-2013-002437
on April 13, 2020 by guest. P
rotected by copyright.http://qualitysafety.bm
j.com/
BM
J Qual S
af: first published as 10.1136/bmjqs-2013-002437 on 29 M
ay 2014. Dow
nloaded from

sample of complaints (to collect norm data, makeassociations between complaints and care quality athealthcare institutions, compare against existing frame-works). This would allow for healthcare organisationsto be compared and for deviations (in comparison withthe norm) in particular types of complaint to be identi-fied. The build-up of lower level complaint issues (eg,staff attitudes) within a unit or hospital might be bettercaptured, and used as a potential (or ‘early-warning’)indicator of poor quality care, as shown with near missdata in the medical error literature.100
Study limitationsThe review has a number of limitations. Primarily, ouranalysis of the issues underlying complaints involvedsecondary interpretation of the data reviewed in thispaper. This was necessary for performing an analysisof trends within the literature, yet involved recodingconcepts that in some cases had minimal qualificationor definition.Our analysis of the issues underlying patient com-
plaints is also skewed towards larger studies, andthose with multiple patient complaint issue codes aremore fully represented. This reflects the differences insize of studies and the depth of their analyses. Thecomplaint coding taxonomy only represents thedomains and categories of complaints coded withinthe literature, and there may be unidentified ones.Additionally, as described above, some categories andsubcategories overlap (eg, poor attitudes may belinked to poor communication), and subcategoriescannot be completely exclusive.The literature review largely focuses on studies
which presented quantitative data, and future workmay wish to incorporate the qualitative studies.19 20
In particular, development of the concepts underlyingthe relationships categories is required, and the use ofthe safety and quality literature to expand the ‘clinical’domain may be beneficial. Furthermore, in somecases, data in patient complaint studies were not fullyreported or described clearly, leading to data beingnot retrievable (table 1). Finally, for the study selec-tion, only the later stages (3 and 4) were performedby two raters, with the potential for error or biasbeing heightened in stages 1 and 2.
ConclusionsA range of clinical, management and relationshipissues underlie patient complaints. The systematiccollation of data on patient complaints potentiallyprovides a mechanism through which the standardof healthcare can be monitored and system-levelinterventions developed. Although patient com-plaints provide a unique and unvarnished insightinto the problems that occur during healthcareepisodes, challenges remain in using the dataheld within them. In comparison with otherforms of quality and safety data (eg, accident and
incident data), the methodologies used to analysepatient complaints are inconsistent or do notprovide an optimal level of depth into complaints.Furthermore, there is considerable variation in theframeworks used to guide the coding of issuesunderlying patient complaints. This means that dataare unstandardised, difficult to make comparisons ofand problematic to demonstrate relationships with.Improvements in the methodology used to codifycomplaints will help to overcome these issues.
Contributors TWR led the writing of the paper and the analysisof complaint issues. AG led the synthesis of the 59 studies, theamalgamation of their results and contributed to the writing ofthe paper. JR ran the literature searchers, extracted the data andparticipated in the writing.
Funding A small grant from the London School of Economics.
Competing interests None.
Provenance and peer review Not commissioned; externallypeer reviewed.
Data sharing statement Data from the literature review will beavailable online.
Open Access This is an Open Access article distributed inaccordance with the Creative Commons Attribution NonCommercial (CC BY-NC 3.0) license, which permits others todistribute, remix, adapt, build upon this work non-commercially,and license their derivative works on different terms, provided theoriginal work is properly cited and the use is non-commercial.See: http://creativecommons.org/licenses/by-nc/3.0/
REFERENCES1 Donaldson L. An organisation with a memory: Learning from
adverse events in the NHS. London: Department of Health,2000.
2 Weingart SN, Pagovich O, Sands DZ, et al. Patient-reportedservice quality on a medicine unit. Int J Qual Health Care2006;18:95–101.
3 Levtzion-Korach O, Frankel A, Alcalai H, et al. Integratingincident data from five reporting systems to assess patientsafety: making sense of the elephant. Jt Comm J Qual PatientSaf 2010;36:402–10.
4 Weingart SN, Pagovich O, Sands DZ, et al. What canhospitalized patients tell us about adverse events? Learning frompatient-reported incidents. J Gen Intern Med 2005;20:830–6.
5 Francis R. Report of the mid-Staffordshire NHS FoundationTrust Public Inquiry. London: The Stationary Office, 2013.
6 Clwyd A, Hart T. A review of the NHS hospitals complaintssystem: putting patients back in the picture. London, England:Department of Health, 2013.
7 Bark P, Vincent C, Jones A, et al. Clinical complaints: a means ofimproving quality of care.Qual Health Care 1994;3:123–32.
8 Hsieh SY. An exploratory study of complaints handling andnature. Int J Nurs Pract 2012;18:471–80.
9 Bismark M, Dauer E, Paterson R, et al. Accountabilitysought by patients following adverse events from medical care:the New Zealand experience. CMAJ 2006;175:889–94.
10 Lloyd-Bostock S, Mulcahy L. The Social Psychology ofmaking and responding to hospital complaints: anaccount model of complaint processes. Law Policy1994;16:123–47.
11 Mulcahy L, Tritter J. Pathways, pyramids and icebergs?Mapping the links between dissatisfaction and complaints.Sociol Health Illn 1998;20:825–47.
Systematic review
Reader TW, et al. BMJ Qual Saf 2014;23:678–689. doi:10.1136/bmjqs-2013-002437 687
on April 13, 2020 by guest. P
rotected by copyright.http://qualitysafety.bm
j.com/
BM
J Qual S
af: first published as 10.1136/bmjqs-2013-002437 on 29 M
ay 2014. Dow
nloaded from

12 Carmel S. Patient complaint strategies in a general hospital.Hosp Health Serv Adm 1990;35:277–88.
13 Jangland E, Gunningberg L, Carlsson M. Patients’ andrelatives’ complaints about encounters and communication inhealth care: evidence for quality improvement. Patient EducCouns 2009;75:199–204.
14 Reader T, Gillespie A. Patient neglect in healthcareinstitutions: a systematic review and conceptual model. BMCHealth Serv Res 2013;13:156.
15 Taylor-Adams S, Vincent C, Stanhope N. Applying humanfactors methods to the investigation and analysis of clinicaladverse events. Saf Sci 1999;31:143–59.
16 Gawande AA, Studdert D, Zinner M, et al. Analysis of errorsreported by surgeons at three teaching hospitals. Surgery2003;133:614–21.
17 Reader T, Flin R, Lauche K, et al. Non-technical skills in theIntensive Care Unit. Br J Anaesth 2006;96:551–9.
18 Moher D, Liberati A, Tetzlaff J, et al. Preferred reportingitems for systematic reviews and meta-analyses: the PRISMAstatement. PLoS Med 2009;6:e1000097.
19 Alemi F, Hurd P. Rethinking satisfaction surveys: time to nextcomplaint. Jt Comm J Qual Improv 2009;35:156–61.
20 Mailis-Gagnon A, Nicholson K, Chaparro L. Analysis ofcomplaints to a tertiary care pain clinic over a nine-yearperiod. Pain Res Manag 2010;15:17.
21 Allsop J, Mulcahy L. Dealing with clinical complaints. QualHealth Care 1995;4:135–43.
22 Bismark MM, Spittal MJ, Gogos AJ, et al. Remedies soughtand obtained in healthcare complaints. BMJ Qual Saf2011;20:806–10.
23 Schwartz LR, Overton DT. Emergency department complaints:a one-year analysis. Ann Emerg Med 1987;16:857–61.
24 Chande VT, Bhende MS, Davis HW. Pediatric emergencydepartment complaints: a three-year analysis of sources andtrends. Ann Emerg Med 1991;20:1014–16.
25 Owen C. Formal complaints against general practitioners: astudy of 1000 cases. Br J Gen Pract 1991;41:113.
26 Burstein J, Fleisher GR. Complaints and compliments in thepediatric emergency department. Pediatr Emerg Care1991;7:138–40.
27 Hunt M, Glucksman M. A review of 7 years of complaints inan inner-city accident and emergency department. Arch EmergMed 1991;8:17–23.
28 Donaldson LJ, Cavanagh J. Clinical complaints and theirhandling: a time for change?Qual Saf Health Care 1992;1:21–5.
29 Kadzombe E, Coals J. Complaints against doctors in anaccident and emergency department: a 10-year analysis. ArchEmerg Med 1992;9:134–42.
30 Hanson R, Clifton-Smith B, Fasher B. Patient dissatisfaction ina paediatric accident and emergency department. J Qual ClinPract 1994;14:137–43.
31 Allsop J. Two sides to every story: complainants’ and doctors’perspectives in disputes about medical care in a generalpractice setting. Law Policy 1994;16:149–83.
32 Nettleton S, Harding G. Protesting patients: a study ofcomplaints submitted to a family health service authority.Sociol Health Illn 1994;16:38–61.
33 Curka PA, Pepe PE, Zachariah BS, et al. Incidence,source, and nature of complaints received in a large, urbanemergency medical services system. Acad Emerg Med1995;2:508–12.
34 Webb B. A study of complaints by patients of different agegroups in an NHS trust. Nurs Stand 1995;9:34.
35 Ingram K, Roy L. Complaints against psychiatrists: a five yearstudy. Psychiatric Bulletin 1995;19:620–2.
36 Mulholland J, Dawson K. A complaints management system:strengths and weaknesses. N Engl J Med 1998;111:77.
37 Mace S. An analysis of patient complaints in an observationunit. J Qual Clin Pract 1998;18:151.
38 Lim H, Tan C, Goh L, et al. Why do patients complain?A primary health care study. Singapore Med J 1998;39:390–5.
39 Daniel A, Burn R, Horarik S. Patients’ complaints aboutmedical practice. Med J Aust 1999;170:598–602.
40 Pichert JW, Federspiel C, Hickson G, et al. Identifyingmedical center units with disproportionate shares of patientcomplaints. Jt Comm J Qual Improv 1999;25:288.
41 Allen LW, Creer E, Leggitt M. Developing a patient complainttracking system to improve performance. Jt Comm J QualImprov 2000;26:217–26.
42 Halperin EC. Grievances against physicians: 11 years’experience of a medical society grievance committee. West JMed 2000;173:235.
43 Anderson K, Allan D, Finucane P. Complaints concerning thehospital care of elderly patients: a 12-month study of onehospital’s experience. Age Ageing 2000;29:409–12.
44 Pitarka-Carcani I, Szmukler G, Henderson C. Complaints aboutcare in a mental health trust. Psychiatric Bulletin 2000;24:372–6.
45 Anderson K, Allan D, Finucane P. A 30 month study ofpatient complaints at a major Australian hospital. J Qual ClinPract 2001;21:109–11.
46 Powers TL, Bendall-Lyon D. Using complaint behavior toimprove quality through the structure and process of servicedelivery. J Consum Satisfaction Dissatisfaction ComplainingBehav 2002;15:13–21.
47 Taylor DM, Wolfe R, Cameron PA. Complaints from emergencydepartment patients largely result from treatment andcommunication problems. Emerg Med 2002;14:43–9.
48 Colwell CB, Pons PT, Pi R. Complaints against an EMSsystem. J Emerg Med 2003;25:403–8.
49 Choy K, Lau A, Li E, et al. The evolution of complaintmanagement in the Hong Kong Hospital Authority. Part 1:complaints management—a tool for system change? HongKong Med J 2004;10:290.
50 Taylor DM, Wolfe RS, Cameron PA. Analysis of complaintslodged by patients attending Victorian hospitals, 1997–2001.Med J Aust 2004;181:31–5.
51 Wofford MM, Wofford JL, Bothra J, et al. Patient complaintsabout physician behaviors: a qualitative study. Acad Med2004;79:134–8.
52 Stelfox HT, Gandhi TK, Orav EJ, et al. The relation ofpatient satisfaction with complaints against physicians andmalpractice lawsuits. Am J Med 2005;118:1126–33.
53 Friele RD, Sluijs EM. Patient expectations of fair complainthandling in hospitals: empirical data. BMC Health Serv Res2006;6:106.
54 Chavan R, Porter C, Sandramouli S. Formal complaints at aneye hospital: a three-year analysis. Clinical Governance: AnInternational Journal 2007;12:85–92.
55 Cowan J, Wilson J. Complaints in primary care arising frombereavement. Clinical Governance: An International Journal2007;12:296–304.
56 Kline T, Willness C, Ghali W. Predicting patient complaints inhospital settings. Qual Saf Health Care 2008;17:346–50.
57 Saravanan B, Ranganathan E, Jenkinson L. Lessons learntfrom complaints by surgical patients. Clinical Governance:An International Journal 2007;12:155–58.
Systematic review
688 Reader TW, et al. BMJ Qual Saf 2014;23:678–689. doi:10.1136/bmjqs-2013-002437
on April 13, 2020 by guest. P
rotected by copyright.http://qualitysafety.bm
j.com/
BM
J Qual S
af: first published as 10.1136/bmjqs-2013-002437 on 29 M
ay 2014. Dow
nloaded from
58 Siyambalapitiya S, Caunt J, Harrison N, et al. A 22 monthstudy of patient complaints at a National Health Servicehospital. Int J Nurs Pract 2007;13:107–10.
59 Natangelo R. Clinicians’ and managers’ responses to patients’complaints: a survey in hospitals of the Milan area. ClinicalGovernance: An International Journal 2007;12:260–6.
60 Wong L, Ooi S, Goh L. Patients’ complaints in a hospitalemergency department in Singapore. Singapore Med J2007;48:990–5.
61 Haw C, Collyer J, Sugarman P. Patients’ complaints at a largepsychiatric hospital: can they lead to better patient services?Int J Health Care Qual Assur 2010;23:400–9.
62 Friele RD, Sluijs EM, Legemaate J. Complaints handling inhospitals: an empirical study of discrepancies betweenpatients’ expectations and their experiences. BMC Health ServRes 2008;8:199.
63 Montini T, Noble AA, Stelfox HT. Content analysis of patientcomplaints. Int J Qual Health Care 2008;20:412–20.
64 Giugliani C, Gault N, Fares V, et al. Evolution of patients’complaints in a French university hospital: is there acontribution of a law regarding patients’ rights? BMC HealthServ Res 2009;9:141.
65 Parry J, Hewage U. Investigating complaints to improve practiceand develop policy. Int J Health Care Qual Assur 2009;22:663–9.
66 Moghadam JM, Ibrahimipour H, Akbari AS, et al. Study ofpatient complaints reported over 30 months at a large heartcentre in Tehran. Qual Saf Health Care 2010;19:1–5.
67 Stimson C, Pichert JW, Moore IN, et al. Medical malpracticeclaims risk in urology: an empirical analysis of patientcomplaint data. J Urol 2010;183:1971–6.
68 Hsieh SY. The use of patient complaints to drive qualityimprovement: an exploratory study in Taiwan. Health ServManage Res 2010;23:5–11.
69 McGregor MJ, Cohen M, Stocks-Rankin C-R, et al.Complaints in for-profit, non-profit and public nursing homesin two Canadian provinces. Open Med 2011;5:e183.
70 Gogos AJ, Clark RB, Bismark MM, et al. When informedconsent goes poorly: a descriptive study of medical negligenceclaims and patient complaints. Med J Aust 2011;195:340–4.
71 Källberg A-S, Göransson KE, Östergren J, et al. Medicalerrors and complaints in emergency department care inSweden as reported by care providers, healthcare staff, andpatients–a national review. Eur J Emerg Med 2013;20:33–8.
72 Sachdeo A, Konfino S, Icyda RU, et al. An analysis of patientgrievances in a dental school clinical environment. J DentEduc 2012;76:1317–22.
73 Schnitzer S, Kuhlmey A, Adolph H, et al. Complaints asindicators of health care shortcomings: which groups of patientsare affected? Int J Qual Health Care 2012;24:476–82.
74 Mann CD, Howes JA, Buchanan A, et al. One-year audit ofcomplaints made against a University Hospital SurgicalDepartment. ANZ J Surg 2012;82:671–4.
75 van Mook WN, Gorter SL, Kieboom W, et al. Poorprofessionalism identified through investigation of unsolicitedhealthcare complaints. Postgrad Med J 2012;88:443–50.
76 Bismark MM, Spittal MJ, Gurrin LC, et al. Identification ofdoctors at risk of recurrent complaints: a national study ofhealthcare complaints in Australia. BMJ Qual Saf2013;22:532–40.
77 Doron I, Gal I, Shavit M, et al. Unheard voices: complaintpatterns of older persons in the health care system. Eur JAgeing 2011;8:63–71.
78 Powers T, Bendall-Lyons D. Using complaint behaviour toimprove quality through the structure and process of servicedelivery. J Consum Satisf Dissatisf Complain Behav2002;15:14–21.
79 Pronovost P, Wachter R. Balancing “no blame” withaccountability in patient safety. N Engl J Med 2010;361:1401–6.
80 Vincent C. Patient safety. London: Elsevier, 2006.81 Ferlie E, Shortell S. Improving the quality of health care in
the United Kingdom and the United States: a framework forchange. Milbank Q 2001;79:281–315.
82 Swayne LE, Duncan WJ, Ginter PM. Strategic management ofhealth care organizations. John Wiley & Sons, 2012.
83 Kenagy J, Berwick D, Shore M. Service quality in health care.JAMA 1999;281:661–5.
84 Gillespie A, Cornish F. Intersubjectivity: towards a dialogicalanalysis. J Theory Soc Behav 2010;40:19–46.
85 Bradshaw A. Measuring nursing care and compassion: theMcDonaldised nurse? J Med Ethics 2009;35:465–8.
86 Maslach C, Jackson S. Burnout in organizational settings.Appl Soc Psychol 1984;5:133–53.
87 Jewkes R, Abrahams N, Mvo Z. Why do nurses abusepatients? Reflections from South African obstetric services.Soc Sci Med 1998;47:1781–95.
88 Robinson S, Bennett R. A typology of deviant workplacebehaviors: A multidimensional scaling study. Acad Manage J1995;38:555–72.
89 Lawton R. Not working to rule: understanding proceduralviolations at work. Saf Sci 1998;28:77–95.
90 de Vries E, Ramrattan M, Smorenburg S, et al. The incidenceand nature of in-hospital adverse events: a systematic review.Qual Saf Health Care 2008;17:216–23.
91 Greenhalgh T, Robb N, Scambler G. Communicative andstrategic action in interpreted consultations in primary healthcare: A Habermasian perspective. Soc Sci Med 2006;63:1170–87.
92 Habermas J. The theory of communicative action: Volume 2:lifeword and system: a critique of functionalist reason. Beaconpress, 1985.
93 Runciman W, Hibbert P, Thomson R, et al. Towards aninternational classification for patient safety: key concepts andterms. Int J Qual Health Care 2009;21:18–26.
94 Runciman WB, Baker GR, Michel P, et al. Tracing thefoundations of a conceptual framework for a patient safetyontology. Qual Saf Health Care 2010;19:1–5.
95 Sherman H, Castro G, Fletcher M, et al. Towards aninternational classification for patient safety: the conceptualframework. Int J Qual Health Care 2009;21:2–8.
96 Lawton R, McEachan RR, Giles SJ, et al. Development of anevidence-based framework of factors contributing to patientsafety incidents in hospital settings: a systematic review. BMJQual Saf 2012;21:369–80.
97 Pham JC, Aswani MS, Rosen M, et al. Reducing medical errorsand adverse events. Annu Rev Med 2012;63:447–63.
98 Reader T, Gillespie A, Mannell J. Patient neglect in 21stcentury healthcare institutions: a community healthpsychology perspective. J Health Psychol 2014;19:137–48.
99 Chang A, Schyve PM, Croteau RJ, et al. The JCAHO patientsafety event taxonomy: a standardized terminology andclassification schema for near misses and adverse events. Int JQual Health Care 2005;17:95–105.
100 Catchpole K, Giddings A, Wilkinson M, et al. Improvingpatient safety by identifying latent failures in successfuloperations. Surgery 2007;142:102–10.
Systematic review
Reader TW, et al. BMJ Qual Saf 2014;23:678–689. doi:10.1136/bmjqs-2013-002437 689
on April 13, 2020 by guest. P
rotected by copyright.http://qualitysafety.bm
j.com/
BM
J Qual S
af: first published as 10.1136/bmjqs-2013-002437 on 29 M
ay 2014. Dow
nloaded from


















