Synovial Joints PTP 521 Musculoskeletal Diseases and Dysfunctions.
83
Synovial Joints PTP 521 Musculoskeletal Diseases and Dysfunctions
-
Upload
jeffrey-ross -
Category
Documents
-
view
218 -
download
2
Transcript of Synovial Joints PTP 521 Musculoskeletal Diseases and Dysfunctions.

Synovial Joints
PTP 521 Musculoskeletal Diseases and Dysfunctions

Objectives
• Review the embryological development of joints
• Review the components of a joint• Discuss the histological makeup of joint
components • Discuss diseases and disorders that stem from
particular joint dysfunctions• Discuss healing rates of joint components

Embryonic Development of Human Joints
• Joints appear as intervals of less concentrated mesenchymal cells
• These cells become flattened in the center.
• At the ends, the flattened cells are continuous with the investing perichondrium
• The perichondrial investment becomes the joint capsule
• 6th week: joints develop
• 8th week: joints resemble adult joints

• As soon as joint cavity appears during development, it contains watery fluid
• Joint capsule develops into an outer fibrous portion lined with an inner portion which is the highly vascularized synovial membrane
• Articular Cartilage is formed from the original cartilagenous template

Articular Cartilage
Embryological Development:– Develops during week 5– Mesenchymal cells
condense, enlarge, proliferate to form compact mass
– Cells (Chondrocytes) become rounded, secrete matrix

Synovial Joint Components
• Joint Capsule
• Synovium
• Synovial Fluid
• Articular Cartilage

Joint Capsule A. Completely encloses the synovial joint and covers all surfaces except
for articulating surfaces and contact surface of any intra-articular structure such as a meniscus– Hydrated, water content of ~70%
B. Forms a cuff around the joint with collagen fibers, Type I– Variability in thickness and attachment of capsule, some are thin attachments and
some are thick– Capsular redundancy
D. Fiber diameter varies, organized in parallel bundles
E. Capsular thickenings or intrinsic ligaments are present, reinforce the capsule.

Capsule Inflammatory Response
• High potential for adhesion formation
• Loss of Glycoaminoglycogen content and water
• Fiber-fiber distance decreases, folds of synovial fluid adhere together limiting mobility

Capsule InjuryA. Joint Effusion: Signs: joint moves to position of
comfort Symptoms: tight sensation in
joint
B. Capsular Fibrosis: Thickened capsule,
collagen fibers have decreased extensibility Signs: decrease in ROM,
capsular pattern present

BECKY IS Re-Posting this section on MECHANORECEPTORS

Joint Mechanoreceptors• Sensory receptor
located within the joint capsule and articular ligaments
• Responds to mechanical pressure or deformation
• 4 Main types– Pacinian Corpusles– Ruffini Corpusles– Golgi – like tendon
organs– Free nerve endings –
type C

Joint Mechanoreceptors:Capsule and Ligaments
• Ruffini Corpuscles– Located superficial joint capsules– Postural receptors– Low threshold, easy to stimulate,
slow to adapt– Stimulated by a change in
mechanical stress about the joint– Give information on static and
dynamic position, sense of velocity, direction and amplitude of movement
– Responds by increasing tone in muscle being stretched, relaxing antagonistic muscle
• Pacinian Corpuscles– Located in small groups in joint
capsule– Low threshold, rapidly adapting,
active with oscillation techniques rather than traction
– Stimulated by sudden changes in movement, pressure changes within the joint
– Give a sense of joint acceleration and deceleration
– Increases tone in muscle being stretched and relaxes antagonistic muscle

Joint Mechanoreceptors• Golgi-Tendon Like
– Inhibitive– NOT in joint capsule but rather
found in ligaments– High threshold, slowly adapting,
more active with high velocity techniques
– Stimulated by stretch at end range
– Function is to prevent excessive stresses at joint by reflexively inhibiting muscle
– Sense of dynamic movement and direction of movement
• Nociceptors: Unmyelinated free nerve endings: Type C– Found in capsule, ligament,
articular fat pads, periosteum, walls of blood vessels
– Burning, aching pain that is difficult to localize
– tonic receptors – responds by producing a tonic muscle contraction
– no significant peripheral adaptation, but central adaptation can occur(perception of pain may decrease)
– High threshold, non adaptive– Stimulated by excessive movement

Joint Mechanoreceptors:Capsule and Ligaments
• Pacinian Corpuscles• Located in small
groups in joint capsule• Low threshold,
reapidly adapting active with ocillation techniques rather than traction
• Stimulated by
• Ruffini• Located superficial to joint capsule• Postural receptors• Low threshold, easy to stimulate,
slow to adapt• Stimulated by a change in
mechanical stress about the joint• Give info on static and dynamic
position, sense of velocity, direction and amplitude movement
• Responds to stretch by increasing muscle tone, relaxing antagonistic mucles

Joint Mechanoreceptors
• Golgi-Tendon Like– Inhibitive, Not in joint
capsule but rather found in ligaments.
– Stimulated by stretch at end range.
– Sense of dynamic movemnent and direction of movemnet
• Nociceptors: Unmyelinated free nerve endings: Type C– Found in capsule, ligament,
fat pads, periosteum, walls of blood vessels
– Burning aching pain that is difficult to localize
– Tonic receptors-responds b producing a tonic muscle contraction
– High threshold, non adaptive– Stimulated by excessive
movements

Synovium
Synoviocytes: Specialized layer of connective tissue cells • Covers the inner surface of the joint capsule to the
margins of the articular cartilage.
• Does not cover weight bearing surfaces.

Synovium:Two Layers of Cells
1) Intima • Layer of specialized fibroblasts, 1-
3 deep, set within a matrix
• Contain both macrophages derived type A cells and fribroblast-derived type B cells
• Synthesizes hyaluronic acid and other cells which help lubricate the joint
• Line the joint cavity

2) Subsynovial tissue• Produces collagen
matrix
• Fibrous, areolar, and adipose tissue
• Contains lymphatics and blood vessels

Vascularity
• Varies between joints
• Varies within a joint
• Lowest in fibrous subsynovial tissues
• Greatest in areolar or adipose subsynovial tissue

Functions of the Synovium
1) Joint Lubrication: provides a low friction lining
2) Transportation – nutrition
3) Joint Stability
4) Other: 1) Regulation of intra-articular temperature2) May have an anti-microbial effect

Synovium: Reaction to Injury
1) Proliferation of Surface Cells
2) Increase in vascularization
3) Gradual Fibrosis of Subsynovial Tissue
4) Granular Surface appears
5) Alteration in synovial fluid

Disease Processes
1) Post Traumatic SynovitisPathophysiology:• Intima layers increase to 8-10 and as much as 15• Increase in lymphatics, protein synthesis
Clinical Manifestations• Signs: joint effusion• Symptoms: tight sensation around joint

Hemarthrosis
• Fracture must be ruled out first– Signs: rapid swelling within 15 min to 2 hours
after injury, loss of range due to increase in swelling
– Symptoms: increase in pain, tight sensation

Pigmented Villonodular Synovitis
• Nodules formed in the synovial tissue due to blood clots attaching to the synovium.
• 1.8 cases/million• Women > Men• 20-50 years of age• Theory: auto immune response or benign
neoplastic process

PVS:
• During joint motion, the nodules are crushed and cause further hemorrhage. This leads to more nodules and more pain occurring.– Inflammatory signs and
symptoms – Signs: Pain with
compression of joint surfaces
• Medical RX: synovectomy
Illustrated by Dave Klemm

26
Rheumatoid Arthritis:
Definition:chronic systemic
inflammatory disease which can result in severe deformities and disabilities.
http://www.emedicine.com/RADIO/topic877.htm

27
R.A. Cont.
• Cervical spine and PIP joints of the hand are commonly involved.
• Incidence: affects all races and ages. 1-2% of the adult population have RA

28
Risk Factors:
a. Women are 2-3 times more likely to develop RA than men
b. Age: 30 to 40 years of age is peak onset time c. RA incidence is lower in women who have
had children and in women who have taken oral contraceptives

29
R.A. Cont.
1. Etiology: unknown
2. Pathology: 80% have a positive rheumatoid factor

30
R.A. Cont.
3. SX: joint stiffness 98% are stiffer after inactivity and better with activity.
• Joint pain: severity of synovitis – may not be a factor at rest
• Fatigue onset about 4 ½ hours after rising
• Weakness out of proportion to activity

31
Signs:
• Swelling in the small joints and tendon sheaths in the hands wrists and forefeet is most common. Can affect any area of the body.
• Palmar erythema is very common, (palms and thenar eminences)

32
R.A. Cont.
• Cool moist skin
• Atrophy of muscles in hands and feet
• Can get extensive joint contractures at later stages
http://www.emedicine.com/RADIO/topic877.htm

33
Treatment goals:
• Reduce pain, maintain mobility, minimize stiffness, edema and joint destruction, aggressive treatment is contraindicated.

34
R.A. Cont.
Medical management: diagnosis is made with lab tests and is also based on history, physical examination.
• Surgery is indicated if conservative care is not sufficient to control pain and maintain functional status.

35
American Rheumatism Association
4/7 conditions with the first 4 present at least 6 weeks
1. morning stiffness greater than 1 hour2. arthritis in 3 or more joints with swelling3. arthritis of hands, joints with swelling4. symmetric arthritis5. rheumatoid nodules6. x-ray findings are typical for RA7. + lab tests – serum rheumatoid factor

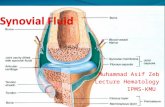
Synovial Fluid Blood plasma with additions of
proteins and hyaluronic acid
Analysis of synovial fluid involves process of arthrocentesis which is the surgical withdrawal of fluid from the cavity

Categories
1) Normal2) Group I: Non-inflammatory3) Group II: Inflammatory4) Group III: Purulent5) Group IV: Hemorrhagic


• Group IV: Hemorrhagic: presence of blood in the synovial fluid. If blood is present at all, it is in this grouping.
– Examples: trauma, fracture, charcot joint, hemophilia, tumor, joint prosthesis, sickle cell trait or disease, internal derangement, major ligament tear
• Other: Fat – indicates a fracture
– Cloudy Synovial Fluid: usually caused by leukocytes. If greater than 2000, will be concerned about an inflammatory joint disease

Articular Cartilage:
• Composition: Water, Collagen, Proteoglycans
• Nutritional Supply: occurs with diffusion and osmosis
• Functions: Carry a heavy load

Histological Composition
• Cells:– Chondroblasts: young cell
– Fibroblasts
– Fibrocytes
– Chondrocytes 2-5% of volume,

Chondrocyte Function
Synthesizes Matrix composed of proteoglycans, growth factors, cytokines, collagen fibers
Anabolic activity and catabolic activity
Common for cells to be multinucleated
Every cell contains a monocillium (mechanotransductory function)

Articular Cartilage Zones

Articular Cartilage Zones
• Zone 1: superficial tangential zone
• Zone 2: transitional zone
• Zone 3: deep radial layer
• Zone 4: cartilage zone– tidemark

Joint Lubrication
Boundary Lubrication: – low load, – prevents direct surface contact– eliminates surface wear, – dependent on Lubricin

Fluid Film Lubrication: high load
A. squeeze film lubrication: perpendicular movement, high loads, short duration occurs with synovial fluid viscosity
Zachazewski JE, Magee DJ, Quillen WS. Athletic Injuries and Rehabilitation. W.B.
Saunders Co. 1996

Fluid Film Lubrication
B. hydrodynamic lubrication: tangential movement, lifting pressure
Zachazewski et al, 1996

Fluid Film Lubrication
C. Elastohydrodynamic: mixed mode of lubrication
• Articular cartilage operates under this type of lubrication
Zachazewski et al, 1996

Fluid Film Lubrication
D. Boosted Lubrication: mixture of both boundary and squeeze film lubrication
Zachazewski et al, 1996

Zachazewski et al, 1996

Response to Injury: Articular Cartilage (AC)
• Causes: – mechanical injuries blunt trauma– penetrating wound– frictional abrasion– biomechanical stress - alteration in weight bearing
forces

Cycle of Degenerative Changes in a Joint
1. Initial changes– Fibrillation: fracturing of collagen fibers
– Depletion of ground substance


Cycle of Degeneration of AC
2. Begins after fibrillation and depletion of ground substance has occurred. – Loss of ground substance
– Softening of the surface layer of cartilage,
– Death of local chondrocytes.
– Death leads to release of proteolytic enzymes

Tissue Healing Factors: AC1. Depth of injury
A. Partial Thickness
B. Full thickness injury: extends into subchondral bone
2. Volume and surface area of articular cartilage involved
3. Immobilization will delay healing, defect most likely filled in with connective tissue.

Summary:
• Components of synovial joints• Lubrication of the joints under normal
circumstances• Healing Times and response to immobilization • Common Injuries to these components

57
Osteoarthritis (Degenerative Joint Disease)
• Definition: loss of articular cartilage with secondary changes in the subchondral bone.
• Non-inflammatory– May be some subsets
that have inflammatory episodes

58
Two Types of Osteoarthritis
1. Primary Osteoarthritis: idiopathic: – develops spontaneously in middle age,
progresses slowly– occurs without any pre-existing joint disease

59
Secondary OA
2. Secondary Osteoarthritis: – Most common type. – Generally occurs following a joint dysfunction/trauma. – Can occur at any age. – Usually occurs due to abnormal stresses placed on a joint– Associated Factors: obesity, high degree of physical
activity, physical disabilities– Look for a history of injury, surgery, or high stress activity
(recreation or occupational) – No direct link of obesity to OA, however increased joint
stress.

60
Incidence• Common disease in elderly
• Affects nearly 21 million people in the United States
• Accounting for 25% of visits to primary care physicians
• Half of all NSAID (Non-Steroidal Anti-Inflammatory Drugs) prescriptions
• It is estimated that 80% of the population will have radiographic evidence of OA by age 65, although only 60% of those will be symptomatic
• If you can catch the OA early enough, then you can change some of the abnormal stress angles and prevent or delay its development.

61
Etiology
• Trauma
• Family: Up to 60% of OA cases are thought to result from genetic factors.
Commonly affected joints; hip, knee, cervical and lumbar spine, first MTP-Joints that are used in posture and have constant stress on them.

62
Risk Factors
• Age
• Overuse
• Theories1. Defect in articular cartilage matrix leads to
premature failure2. Primary abnormality is in bone and cartilage
failure is secondary

63
Pathology
• Cartilage becomes worn, thin, frayed. Subchondral bone is exposed and compressed. – Shape: changes occur with addition of new bone – Each joint has a characteristic location for
osteophyte formation

64
• Hand: Heberden’s nodes

65
Onset
• > age 40
• Women more than men (75% women over 60) – (McCarthy, Frassica1998)
• By age 65, most everyone has some radiographic evidence of OA

66
Clinical Manifestations
• Symptoms: Pain– Relieved by rest
• Signs:– Crepitus– Joint Deformity– Loss of function
• Medical Tests: Radiographs, Class one synovial fluid analysis

67
Radiologic Features of OA
• Subchondral sclerosis– Sclerosis: formation of
new bone in areas of stress
• Osteophyte formationA: Alignment 5 is shifted posteriorB:

68
Radiologic Features of OA
• Joint space narrowing– Loss of proteoglycans
from the matrix
• Bony cyst formation

69
Classification of Articular Cartilage Defects
• Normal Joint
• Macroscopic changes: Grade I: softening of the cartilage –Outerbridge (1961)
Medcohealth

70
Grade 2
• Fragmentation and fissuring cartilage
• Area is .5 inch or less in diameter

71
Grade 3
• Area of involvement is greater than .5 in in diameter
• Won’t want to walk or move a lot.

72
Grade IV
• Full thickness injury with exposed bone

73
Grade V
• Full exposed bone, in need of a knee replacement.

74
Nonoperative management:
Look for areas of loss of ROM and work on getting movement back
a. chondroitin sulfate and glucosaminepreliminary research indicates some benefit but best results are for those who are in the early stages of OA
b. injections of hyaluronic acid substitutes also gave best
results in those patients with early stages of OA-First injections work well (3-6 months) but affect wears off.

75
Pharmacological Interventions• Medications: NSAIDS drugs help to increase joint
motion, decrease joint warmth. • These drugs, including aspirin, ibuprofen, Naprosyn
and others may be effective in decreasing pain, but there is no indication that they decrease the progression of joint breakdown in osteoarthritis.
• Moreover, nonsteroidal anti-inflammatories may be associated with side effects, such as stomach pain and gastrointestinal bleeding. They should be used with caution in elderly patients.
• The new nonsteroidal anti-inflammatory COX II drugs Celebrex and Vioxx have fewer gastrointestinal side effects.

76
Surgical Management
• Cartilage Repair– Problems with repair process• Filling the defect with a material that will have the
same mechanical properties as cartilage• Consolidation of material with native articular cartilage

77
Autologous Condrocyte Implantation
• Patients between 15 and 55 with minor damage to the articular cartilage
• Procedure;– Sample of cartilage removed from a NWB area– Sample sent to a lab where the chondrocytes are
separated from the cell matrix

78
– Cells are cultured for 4-5 weeks and then returned (5-10 million cells)
– Then, patient returns and has a surgical implantation of the cells sutured by a periosteal membrane flap
– NWB status for 10 – 12 weeks
– Good results in about 72% of patients» Beris, 2005

79
Periosteal/Perichondreal Grafts
• Transplant periosteum and perichondrium in full thickness defects
• Poor clinical results
• Complete restoration of hyaline cartilage layer and long-term stability of repair tissue didn’t occur.

80
Surgical Management1. Osteoarticular Transfer System (OATS) Mosaicplasty One stage procedure Cylindrical osteochondral pieces removed from
non-weight bearing areas of the AC and transferred into debrided full thickness defects.

81
OATS Procedure
• Low Cost• Not Lab Dependent• Minimally invasive• Works well for small to medium amount oA
• Most effective for small and medium size full thickness defects– Less than 25 mm in diameter– Chondral defect with stable surrounding cartilage

82
Surgical Treatments
• Hemi or Total Joint Replacements
– Typical Joints: Knee’s Shoulders, Hips, Hands

Compare and Contrast
• RA • OA