Synergism between Topiramate and Budipine in Refractory Status Epilepticus in the Rat
8
Epilepsia, 45(11):1300–1307, 2004 Blackwell Publishing, Inc. C 2004 International League Against Epilepsy Laboratory Research Synergism between Topiramate and Budipine in Refractory Status Epilepticus in the Rat Andrew Fisher, Xiaolan Wang, Hannah R. Cock, Maria Thom, Philip N. Patsalos, and Matthew C. Walker Department of Clinical and Experimental Epilepsy, Institute of Neurology, UCL, London, United Kingdom Summary: Purpose: To evaluate the antiepileptic and neuropro- tective properties of topiramate (TPM) alone and with coadmin- istration of the N-methyl-D-aspartate (NMDA)-receptor antago- nist budipine in a rat model of refractory status epilepticus. Methods: Male Sprague–Dawley rats had electrodes im- planted into the perforant path and dentate granule cell layer of the hippocampus under halothane anesthesia. Approximately 1 week after surgery, the perforant path of each animal was elec- trically stimulated for 2 h to induce self-sustaining status epilep- ticus. Successfully stimulated rats were given intraperitoneally vehicle (n = 6), TPM (20–320 mg/kg; n = 28), budipine (10 mg/kg; n = 5), or budipine (10 mg/kg) and TPM (80 mg/kg; n = 6) 10 min after the end of the stimulation and monitored behaviorally and electroencephalographically for a further 3 h. The animals were killed 14 days later, and histopathology was assessed. Results: Neither budipine alone nor TPM at any dose termi- nated status epilepticus. Despite this, TPM resulted in various degrees of neuroprotection at doses between 40 and 320 mg/kg. Coadministration of budipine with TPM terminated the status epilepticus in all rats. This combination also significantly im- proved the behavioral profile and prevented status-induced cell death compared with control. Conclusions: Budipine and TPM are an effective drug combination in stopping self-sustained status epilepticus, and TPM alone was neuroprotective, despite the continuation of seizure activity. Key Words: Topiramate—Budipine—Status epilepticus—Perforant path—Neuroprotection. Status epilepticus is a medical emergency with a high morbidity and mortality. Existing pharmacotherapeutic approaches successfully treat fewer than 70% of patients with status epilepticus (1), and there thus remain a substan- tial proportion of individuals whose condition is refractory to conventional treatments. Status epilepticus is associated with severe neuronal damage. The degree of excitotoxic neuronal damage that occurs during status epilepticus is dependent on the presence and duration of electrographic seizure activity (2). Therefore the most effective way to minimize neuronal damage is to stop seizures as soon as possible after their onset. Furthermore, status epilepticus becomes progressively more difficult to treat as the time between seizure manifestation and pharmacologic inter- vention increases (3,4). In the 40% of cases that are esti- mated to be unresponsive to first-line treatment (1), gen- eral anesthesia in an intensive care unit can often be the Accepted June 23, 2004. Address correspondence and reprint requests to Dr. M.C. Walker at Department of Clinical & Experimental Epilepsy, Institute of Neurol- ogy, Queen Square, London, WC1N 3BG, U.K. E-mail: m.walker@ ion.ucl.ac.uk only option available to treat refractory status epilepticus. However, this approach is associated with increased risks of hypotension and infection and with a high morbidity and mortality (5,6). Administration of neuroprotective compounds offers an alternative approach to combat the neuronal dam- age that occurs with continual seizure activity. Activa- tion of ionotropic glutamate receptors has been thought to play an integral role in the pathophysiology of status- induced neuronal damage (7). Therefore glutamate antag- onists would be expected to be effective in combating the initiation and propagation of seizure-induced excitotox- icity and its associated neuropathology. Several groups have confirmed this hypothesis in rodents that have been treated with glutamate-receptor antagonists either before (8–10) or after the induction of status epilepticus (11,12). Furthermore, N-methyl-D-aspartate (NMDA)-receptor antagonists enhance the effect of diazepam (DZP) in the treatment of status epilepticus (13) and prevent the de- velopment of DZP refractoriness (14). NMDA-receptor antagonists exhibit limited clinical effectiveness on ac- count of their psychotomimetic side effects. However, 1300
-
Upload
andrew-fisher -
Category
Documents
-
view
212 -
download
0
Transcript of Synergism between Topiramate and Budipine in Refractory Status Epilepticus in the Rat

Epilepsia, 45(11):1300–1307, 2004Blackwell Publishing, Inc.C© 2004 International League Against Epilepsy
Laboratory Research
Synergism between Topiramate and Budipine in RefractoryStatus Epilepticus in the Rat
Andrew Fisher, Xiaolan Wang, Hannah R. Cock, Maria Thom, Philip N. Patsalos,and Matthew C. Walker
Department of Clinical and Experimental Epilepsy, Institute of Neurology, UCL, London, United Kingdom
Summary: Purpose: To evaluate the antiepileptic and neuropro-tective properties of topiramate (TPM) alone and with coadmin-istration of the N-methyl-D-aspartate (NMDA)-receptor antago-nist budipine in a rat model of refractory status epilepticus.
Methods: Male Sprague–Dawley rats had electrodes im-planted into the perforant path and dentate granule cell layerof the hippocampus under halothane anesthesia. Approximately1 week after surgery, the perforant path of each animal was elec-trically stimulated for 2 h to induce self-sustaining status epilep-ticus. Successfully stimulated rats were given intraperitoneallyvehicle (n = 6), TPM (20–320 mg/kg; n = 28), budipine (10mg/kg; n = 5), or budipine (10 mg/kg) and TPM (80 mg/kg;n = 6) 10 min after the end of the stimulation and monitoredbehaviorally and electroencephalographically for a further 3 h.
The animals were killed 14 days later, and histopathology wasassessed.
Results: Neither budipine alone nor TPM at any dose termi-nated status epilepticus. Despite this, TPM resulted in variousdegrees of neuroprotection at doses between 40 and 320 mg/kg.Coadministration of budipine with TPM terminated the statusepilepticus in all rats. This combination also significantly im-proved the behavioral profile and prevented status-induced celldeath compared with control.
Conclusions: Budipine and TPM are an effective drugcombination in stopping self-sustained status epilepticus, andTPM alone was neuroprotective, despite the continuation ofseizure activity. Key Words: Topiramate—Budipine—Statusepilepticus—Perforant path—Neuroprotection.
Status epilepticus is a medical emergency with a highmorbidity and mortality. Existing pharmacotherapeuticapproaches successfully treat fewer than 70% of patientswith status epilepticus (1), and there thus remain a substan-tial proportion of individuals whose condition is refractoryto conventional treatments. Status epilepticus is associatedwith severe neuronal damage. The degree of excitotoxicneuronal damage that occurs during status epilepticus isdependent on the presence and duration of electrographicseizure activity (2). Therefore the most effective way tominimize neuronal damage is to stop seizures as soon aspossible after their onset. Furthermore, status epilepticusbecomes progressively more difficult to treat as the timebetween seizure manifestation and pharmacologic inter-vention increases (3,4). In the 40% of cases that are esti-mated to be unresponsive to first-line treatment (1), gen-eral anesthesia in an intensive care unit can often be the
Accepted June 23, 2004.Address correspondence and reprint requests to Dr. M.C. Walker at
Department of Clinical & Experimental Epilepsy, Institute of Neurol-ogy, Queen Square, London, WC1N 3BG, U.K. E-mail: [email protected]
only option available to treat refractory status epilepticus.However, this approach is associated with increased risksof hypotension and infection and with a high morbidityand mortality (5,6).
Administration of neuroprotective compounds offersan alternative approach to combat the neuronal dam-age that occurs with continual seizure activity. Activa-tion of ionotropic glutamate receptors has been thoughtto play an integral role in the pathophysiology of status-induced neuronal damage (7). Therefore glutamate antag-onists would be expected to be effective in combating theinitiation and propagation of seizure-induced excitotox-icity and its associated neuropathology. Several groupshave confirmed this hypothesis in rodents that have beentreated with glutamate-receptor antagonists either before(8–10) or after the induction of status epilepticus (11,12).Furthermore, N-methyl-D-aspartate (NMDA)-receptorantagonists enhance the effect of diazepam (DZP) in thetreatment of status epilepticus (13) and prevent the de-velopment of DZP refractoriness (14). NMDA-receptorantagonists exhibit limited clinical effectiveness on ac-count of their psychotomimetic side effects. However,
1300

TOPIRAMATE AND BUPIDINE SYNERGISM 1301
evidence suggests that low-affinity NMDA-receptor an-tagonists such as budipine and memantine may displaybeneficial effects in the early treatment of some clini-cal conditions such as Parkinson’s disease (15,16) andepilepsy (17).
Topiramate [TPM;2,3:4,5-bis-O-(1-methylethylidene)-β-D-fructopyranose sulphamate] is a novel anticon-vulsant that displays multiple mechanisms of actionincluding antagonism of α-amino-3-hydroxy-5-methyl-4-isoxazolepropionate (AMPA) and kainate receptors;blockade of voltage-activated Na+ and L-type Ca2+
channels; potentiation of γ -aminobutyric acid (GABA)-mediated inhibitory neurotransmission, and the activationof K+ channels (18,19). The actions of TPM on GABAA
receptors are not mediated through the benzodiazepine(BZD) or barbiturate sites. This is an important distinc-tion, as drugs that act at these loci within the GABAA
receptor–ionophore complex experience a loss of efficacyduring status epilepticus (3).
The aim of the current study was to investigate the ef-fectiveness of TPM alone and in combination with budip-ine (1-tert-butyl-4,4-diphenylpiperidine), a low-affinityNMDA-receptor antagonist, in a rodent model of refrac-tory status epilepticus (20) and to assess its role as aputative neuroprotectant when administered once statusepilepticus has been established.
METHODS
AnimalsMale Sprague–Dawley rats (Tuck, Battlesbridge, Essex,
England) weighing 250 to 320 g were used. Rats were indi-vidually housed in a temperature-controlled environmentunder a 12-h light/dark cycle with food and water availablead libitum. All animal procedures strictly adhered to local(Institute of Neurology, London, U.K.) and Home Officeregulations under the Animal (Scientific Procedures) Act,1986.
DrugsTPM (R.W. Johnson Pharmaceutical Research Institute,
Spring House, PA, U.S.A.) was dissolved in deionized wa-ter containing 1 M NaOH (2–5% vol/vol) and protectedfrom light. Budipine (Byk Gulden, Konstanz, Germany)was dissolved in warm deionized water. Both drugs wereprepared in solution immediately before injection. Alldrugs were administered intraperitoneally in an injectionvolume of 0.1 ml/100 g body weight.
Electrode implantationThis procedure has been previously described in de-
tail (21). In brief, animals were fully anaesthetized withhalothane in oxygen (3% vol/vol induction; 1.5% vol/volmaintenance) and placed into a stereotaxic frame (DavidKopf Instruments, Tujunga, CA, U.S.A.). Before elec-trode placement, ventral measurements were recorded for
bregma and lambda to ensure that the skull was as level aspossible while in the frame. Fine adjustments of the nosebar were made until differences in ventral coordinates be-tween bregma and lambda were ≤0.1 mm. A bipolar stim-ulating electrode was then slowly lowered into the angularbundle (coordinates, 8.1 mm caudal to bregma; 4.4 mm lat-eral; 3.5–4.0 mm ventral from brain surface) to stimulatethe perforant pathway, and a unipolar recording electrodewas lowered into the ipsilateral hippocampal dentate gran-ule cell layer (coordinates, 4.0 mm caudal to bregma; 2.5mm lateral; 3.5–4.0 mm ventral from brain surface). Allstereotaxic coordinates were in reference to the stereotaxicrat brain atlas of Paxinos and Watson (22). The depths ofthe electrodes were finely adjusted to maximize the slopeof the field potential.
After 7 to 10 days’ recovery from surgery, each animalwas challenged with a single monopolar pulse (2 mA, 50µs) to ensure continual functional competency of the elec-trodes after the postoperative recovery period. Rats thatdisplayed a population spike of <2 mV were not includedfor further study.
The perforant pathway was stimulated in freely movingrats with a Neurolog stimulator (Digitimer Ltd., WelwynGarden City, U.K.) delivering 2-mA, 50-µs monopolarpulses at 20 Hz for 2 h to induce self-sustaining statusepilepticus (SSSE). EEG signals were transferred via anNB-MIO-16 interface (National Instruments, Newbury,Berkshire, U.K.) to a computer equipped with LabViewsoftware. Drugs were administered intraperitoneally (i.p.)10 min after electrical stimulation was terminated. Ani-mals that failed to display self-sustaining chronic limbicstatus 10 min after the electrical stimulation was stoppedwere excluded from further analysis. We assessed the de-gree of sedation by using a well-established scale: 0, spon-taneous movement; 1, intermittent spontaneous move-ment; 2, no spontaneous movement; 3, loss of auditoryreflex; 4, loss of corneal reflex; 5, loss of response to tailpinch (20,23). We assessed the seizure severity by usingthe classification of Racine (24). For the purposes of thesedation score, the presence of only seizure-related move-ments was scored as no spontaneous movements. We con-tinually monitored the EEG recordings for a further 3 h.Seizure severity, level of sedation, spike frequency, andmaximal spike amplitude were recorded every 10 min.
Animals that displayed seizure activity 3 h after drugadministration had their seizures terminated by i.p. admin-istration of 20 mg/kg DZP.
HistologyFourteen days after stimulation, all animals were
deeply anaesthetized and transcardially perfused with 4%buffered paraformaldehyde (pH 7.2). The brains were re-moved and stored in 4% paraformaldehyde before be-ing embedded in paraffin wax. Coronal sections (5 µmfor hematoxylin and eosin staining and 20 µm for Nissl
Epilepsia, Vol. 45, No. 11, 2004

1302 A. FISHER ET AL.
labeling) were taken every 200 µm to assess semiquan-titively acute neuronal injury (eosinophilic and pyknoticneurons on H&E sections) and cell density, respectively.Within the hippocampus, the dentate granule (DG) celllayer, the hilus, and the CA1 and the CA3 regions wereindependently graded. The investigator was blinded to thetreatment that the rat had received. In all slides, three ran-dom areas within each hippocampal subregion were se-lected, and the number of neurons (distinguished fromother cell types on the basis of their size, the presence ofNissl granules in the cytoplasm, and a large pale-stainingnucleus with one or more nucleoli) partly or wholly con-tained within a 50-µm2 area was counted by using anOlympus CK inverted microscope with a ×20 objectivelens and a 10 × 10 eyepiece graticule (grid area, 0.5 ×0.5 mm2).
Statistical methodsSpike frequencies between drug groups were analyzed
by using a general linear model with repeated-measuresanalysis of variance (ANOVA) on SPSS for Windows withalterations in spike frequency and spike amplitude overtime as the within-subject factors. Where significance wasreached, post hoc analysis was conducted by using Tukey’sHSD test. Results for cell density and acute neuronal dam-age were determined by using a multifactorial ANOVA onSPSS for Windows, and significance was determined byusing Pillai’s trace. Variables included brain hemisphere,
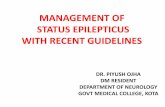
FIG. 1. Topiramate (TPM, 20–320mg/kg, i.p.) has no effect on the spikefrequency (A) or amplitude (B) in ani-mals 10 min after self-sustaining sta-tus epilepticus had been established.Each point is expressed as the mean± SEM of at least four individualsper treatment group. C: Typical sam-ples of EEG after drug administration.Recordings are continually analyzedbut are represented here at time 0, 30,60, and 180 min after the onset of self-sustaining status epilepticus.
brain region, and drug treatment. Behavioral assessmentwas quantified by using the Kruskal–Wallis H test for sig-nificance between groups. Significant behavioral differ-ences from control were subsequently assessed by usingthe Mann–Whitney U test. In all statistical tests, a valueof p < 0.05 was taken as the level of significance.
RESULTS
EEG/behavioral analysisAfter the stimulation protocol, all rats that went into
status epilepticus (n = 45) had an initial spike frequencyof 1.0–2.1 Hz and exhibited marked behavioral seizures(Racine score, ≥3).
TPM at doses of 20, 40, 80, 160, and 320 mg/kg failed toabolish EEG seizure activity (Fig. 1). Differences in spikefrequency over time between treatment groups was notsignificant [F(5, 26) = 0.8; p = 0.570]. Despite the lackof effect of TPM on seizure frequency, a trend was notedtoward a reduction of spike amplitude after high-dose ad-ministration (160 and 320 mg/kg), but this effect did notreach statistical significance at any TPM dose tested [F(5,26) = 2.3; p = 0.078]. High-dose administration of TPMwas accompanied by profound ataxia and sedation in allanimals tested at these doses (Table 1). Moreover, TPMat 320 mg/kg induced severe respiratory depression in allrats tested and exhibited lethal toxicity in two rats. We thenasked whether an NMDA-receptor antagonist would en-
Epilepsia, Vol. 45, No. 11, 2004

TOPIRAMATE AND BUPIDINE SYNERGISM 1303
TABLE 1. The effect of topiramate (TPM, 40–320 mg/kg, i.p), budipine (BDP, 10 mg/kg), or BDP and TPM treatment (10 and 80mg/kg, respectively) on sedation scores
Sedation Score DrugTime afterdrug (min) Saline TPM 40 TPM 80 TPM 160 TPM 320 BDP 10 BDP +TPM
0 Mean 3.00 3.00 3.00 3.00 3.00 3.00 3.00SEM 0.00 0.00 0.00 0.00 0.00 0.00 0.00
30 Mean 3.00 2.00 3.00 3.00 3.25 2a 1.5a
SEM 0.00 0.24 0.00 0.00 0.25 0.32 0.3460 Mean 3.00 2.00 3.00 3.17 3.75 1.8a 0.5a
SEM 0.00 0.24 0.26 0.17 0.25 0.37 0.34120 Mean 3.00 1.50 3.00 3.17 3.50 1.4a 0.33a
SEM 0.00 0.21 0.26 0.17 0.29 0.24 0.21180 Mean 3.00 1.33 3.00 3.17 3.25 1.6a 0.33a
SEM 0.00 0.31 0.26 0.17 0.25 0.24 0.21
See Methods: 0, no sedation; 5, deep anesthesia. Behavioral assessment represents the means ± SEM of at least four individuals per treatment group.The nonparametric Kruskal–Wallis test was used to assess between-group significance. Significant deviations from control were subsequently quantifiedby using the Mann–Whitney U test.
ap < 0.05.
hance the antiepileptic effect of TPM. We first confirmedthat the low-affinity NMDA-receptor antagonist budipinealone at low dose (10 mg/kg; i.p.) failed to exhibit any sig-nificant effect on spike frequency [F(3.4, 30.2) = 2.4; p =0.085 vs. saline control]. However, the behavioral scoreof all budipine-treated animals tested was significantlyimproved compared with those of animals receiving ve-hicle alone (see Table 1). We next tested the combinedeffect of TPM and low-dose budipine. Status epilepti-cus was terminated in all animals that received budip-
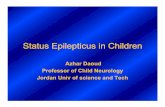
FIG. 2. The effect of combiningbudipine (BDP, 10 mg/kg, i.p.) andtopiramate (TPM, 80 mg/kg, i.p.) onspike frequency (A) and amplitude(B) in perforant path–stimulatedrats. Spike frequency was signif-icantly reduced by 50 min, andseizure activity stopped in all ani-mals by 90 min after drug admin-istration. Significant attenuation ofspike amplitude was reached 10min after combination therapy. Thelack of effect of TPM (80 mg/kg)and BDP (10 mg/kg) given aloneand the effect of saline are includedfor comparison. Each point is ex-pressed as the mean ± SEM of atleast five individuals per treatmentgroup. ∗p < 0.05 compared withcontrol (repeated measures analy-sis of variance with post hoc TukeysHSD test). C: Representative 10-sEEG traces from rats given BDP (10mg/kg) and TPM (80 mg/kg).
ine, 10 mg/kg, as an adjunct to TPM, 80 mg/kg, therapy.In all cases, the EEG returned to baseline levels within90 min after drug administration (Fig. 2). A significantdrug effect was found between the groups [F(4.8, 90.9) =6.4; p < 0.001, with a significant reduction in spike fre-quency attained 50 min after treatment with both drugs].Behavioral seizure activity was terminated in all animalssubjected to budipine and TPM coadministration withoutcompromising the motility or alertness of the animals (seeTable 1).
Epilepsia, Vol. 45, No. 11, 2004

1304 A. FISHER ET AL.
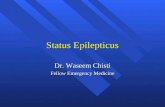
FIG. 3. Neuronal damage in the CA1 region of the hippocampus secondary to status epilepticus is ameliorated by topiramate (TPM; 80mg/kg) and by the combination of budipine (10 mg/kg) and TPM (80 mg/kg). Examples of CA1 regions from unstimulated rat (A), rat withstatus epilepticus given saline (B) demonstrating marked neuronal loss with increase in microglia and reactive astrocytes, rat with statusepilepticus given TPM (C), and rat with status epilepticus given budipine and TPM (D). Examples are from 5-µm H&E sections.
NeuroprotectionIn all saline-treated animals, histologic examination re-
vealed severe bilateral neuronal damage, as previously de-scribed (21). In all cases, almost complete neuronal losswas seen in the CA1 region on the stimulated hemisphere,with an accompanying marked increase in microglia andreactive astrocytes (Fig. 3). The CA3 and hilus regionsalso were affected, with the area of the hilus reduced insaline-treated animals compared with those rats treatedwith TPM (data not shown).
TABLE 2. The effect of topiramate (TPM, 40–320 mg/kg, i.p), budipine (BDP, 10 mg/kg), or BDP and TPM treatment (10 and 80mg/kg, respectively) as a neuroprotectant against status-induced neuronal loss compared with animals given saline
Right DG Left DG Right hilus Left hilus Right CA3 Left CA3 Right CA1 Left CA1
Saline 10.9 ± 1.5 11.8 ± 0.8 1.0 ± 0.6 2.3 ± 0.1 1.5 ± 0.7 2.6 ± 0.2 0.8 ± 0.6 1.4 ± 0.3TPM 40 10.0 ± 0.6 9.7 ± 0.5 2.4 ± 0.2 2.5 ± 0.2 2.9 ± 0.2a 2.8 ± 0.1 3.6 ± 0.5a 3.4 ± 0.4TPM 80 15.8 ± 0.6a 16.0 ± 0.7a 4.5 ± 0.4a 4.7 ± 0.3a 5.9 ± 0.3a 6.7 ± 0.8a 8.5 ± 0.5a 8.1 ± 0.7a
TPM 160 11.5 ± 1.0 9.6 ± 0.6 1.7 ± 0.5 2.6 ± 0.1 2.8 ± 0.3 2.4 ± 0.3 1.1 ± 0.4 4.8 ± 0.5a
TPM 320 10.3 ± 0.6 9.3 ± 0.8 2.9 ± 0.2a 3.0 ± 0.3 3.3 ± 0.3a 4.8 ± 0.6 5.2 ± 0.3a 5.0 ± 0.7a
BDP 10 11.0 ± 0.5 11.1 ± 0.5 3.4 ± 0.2a 3.3 ± 0.2 4.3 ± 0.4a 4.4 ± 0.5 5.4 ± 0.5a 5.8 ± 0.6a
BDP+TPM 11.1 ± 0.4 10.6 ± 0.3 2.9 ± 0.2a 2.8 ± 0.2 3.4 ± 0.2 3.1 ± 0.1 5.3 ± 0.2a 5.3 ± 0.2a
Cell densities were quantified from three random areas (each 50 µm2) within each hippocampal subregion. Values are expressed as mean ± SEM,n = 6, for all groups except TPM, 320 mg/kg (n = 4, as two animals died during status epilepticus) and budipine (n = 5).
ap < 0.05 for difference from saline (Tukey’s HSD test; see Methods)
Significant variability was seen in the cell density ofrats treated with TPM at doses of 40–320 mg/kg [F(40,175) = 3.23; p < 0.01; Pillai’s trace, 2.12]. Further anal-ysis revealed that TPM at 80 mg/kg was the minimal dosethat prevented the marked reduction in hilar, CA1, andCA3 cell densities after saline administration (Table 2,Fig. 3). Administration of budipine at 10 mg/kg eitheralone or concurrent with TPM at 80 mg/kg significantlyprotected against neuronal loss compared with controls[F(32, 152) = 3.13; p < 0.01; Pillai’s trace = 1.59] in
Epilepsia, Vol. 45, No. 11, 2004

TOPIRAMATE AND BUPIDINE SYNERGISM 1305
the hilus, CA1, and CA3 brain regions (Table 2, Fig. 3).The level of neuroprotection offered by TPM alone versuscombined budipine and TPM was found to be not signifi-cantly different in any brain region studied (Table 2).
DISCUSSION
The purpose of this study was to evaluate the anticon-vulsant and neuroprotective actions of TPM in an estab-lished experimental model of refractory status epilepticus(21). The TPM doses selected in our study were basedon preclinical data (19,25) that allowed us to examinedoses that are above and below the reported median ef-fective dose (ED50) of the drug. Our experimental pro-tocol ensured that the duration and intensity of electricalstimulation was identical for all animals included in thestudy. This methodologic approach allowed direct com-parisons to be made between all experimental groups withregard to the effectiveness of the drug(s) and their abilityto afford neuroprotection or a cessation of seizure activ-ity or both. The results suggest that although TPM is aneffective AED in the clinic (26–29), and despite clinicalreports of its use in status epilepticus (30), monoadmin-istration of the drug (20–320 mg/kg, i.p.) does not stopcontinual seizure activity in perforant path –stimulatedrats. However, a single dose of TPM (80 mg/kg, i.p.)did provide a significant reduction in acute neuronal in-jury in the CA1 region of the hippocampus comparedwith control, an effect that supports previous findings inboth status epilepticus (31,32), and ischemia (33,34). Thisalso demonstrates a dissociation between the neuropro-tective and antiepileptic effects of TPM, as neuroprotec-tion was maximal at a dose (80 mg/kg, i.p.) that had nosignificant effect on spike frequency or amplitude. Thisdissociation is similar to that seen with other neuropro-tective compounds (35) and with budipine in this study.The mechanisms underlying this neuroprotective effectare unknown. The loss of the neuroprotective effect athigher TPM doses (160 and 320 mg/kg) can be partlyexplained by the respiratory depression and increasedsedation at these doses (two animals died at the high-est TPM dose). Undoubtedly such physiologic compro-mise during status epilepticus can contribute to neuronaldamage (36).
Combining TPM with the low-affinity NMDA-receptorantagonist budipine (1-tert-butyl-4, 4-diphenylpiperidine)provided no additional neuroprotection (no significant dif-ference was found between the neuroprotection with TPMalone and that when given in combination), but stoppedseizure activity in all animals tested. Moreover, all an-imals undergoing this polypharmacy regimen exhibiteda marked improvement in their behavioral profile 30 minafter drug administration (compared with sole administra-tion of either drug) that appeared to be directly correlatedwith their EEG recordings.
We used budipine in this study, as it offers advantagesover other NMDA-receptor antagonists. Noncompetitive,dissociative anesthetic agents (MK-801, ketamine) havelimited clinical use on account of their sympathomimeticand behavioral side effects (37–39). The binding sites forketamine and MK-801 are located within the ion channelof the NMDA receptor. Because these sites are availableto these ligands only when the NMDA receptor is acti-vated, and the ion channel is in its open conformation,these drugs should be effective in targeting NMDA re-ceptors that are activated, while having little or no ef-fect on NMDA receptors that remain quiescent. How-ever, high-affinity NMDA-receptor antagonists such asMK-801 [Ki = 3 nM; (39)] are associated with slow disso-ciation rates from their binding sites and low voltage de-pendency (40). Consequently, drugs such as MK-801 failto distinguish between NMDA receptors that are patholog-ically activated and those undergoing phasic physiologicstimulation.
In contrast, low-affinity NMDA-receptor antagonistssuch as budipine [Ki = 12 µM (41)] are clinically toleratedand are not typically associated with psychotomimeticside effects (42) on account of their fast dissociation ki-netics [offset rate of budipine, 0.63 s−1 (43)] that are ≥2orders of magnitude faster than that of MK-801 (44). Dur-ing strong depolarization, low-affinity NMDA-receptorion channel antagonists are thought to mimic Mg2+ byrapidly leaving the ion channel after its physiologic acti-vation, but differ from Mg2+in that it does not exit the ionchannel after moderate prolonged synaptic depolarization,as seen with chronic excitotoxicity (40). These propertiesof budipine may afford protection against pathologic ac-tivation of NMDA receptors while sparing any significantinfluence by transient physiologic stimulation.
Typically, low-affinity NMDA-receptor antagonists areadministered in concentrations that do not limit their activ-ity to NMDA receptors but also are likely to interact withbinding sites other than the NMDA receptor. This is notnecessarily a limitation of these drugs, especially when itis considered that the usefulness of TPM as an anticonvul-sant possibly stems from its broad pharmacologic mecha-nisms of action. The pharmacologic profile of budipine hasbeen well characterized (16,45). It has been shown to in-teract with the dopaminergic (46,47), cholinergic (17,48),serotonergic (49), and GABAergic systems (50). Any orall of these interactions with other neurotransmitter sys-tems could contribute to the drug’s synergistic effects withTPM seen in the current study. However, the observed syn-ergistic effects of TPM with MK-801 on seizure activity(n = 3, data not shown) suggest that budipine’s effective-ness may stem from its ability to inhibit NMDA recep-tors. The mechanism underlying the synergistic effect ofNMDA-receptor antagonists in status epilepticus remainslargely unexplained but could be partly due to the role ofNMDA receptors in regulating refractoriness (14).
Epilepsia, Vol. 45, No. 11, 2004

1306 A. FISHER ET AL.
These results show that the use of low-affinity NMDA-receptor antagonists as adjuncts to AEDs could offer clin-ical benefits in patients who have persistent seizure activ-ity that proves to be intractable to first-line AED therapy.TPM also could have an important role as an adjunctivetreatment, especially because it seems to afford significantneuroprotection, even if it does not terminate the statusepilepticus.
Acknowledgment: We thank Johnson & Johnson for sup-porting this work. We also thank Dr. Peter Whitton for the giftof budipine, Derek Marson for assistance with the preparationof the brain slices for histologic assessment, and Hannah Slevenfor assistance with in vivo work.
REFERENCES
1. Treiman DM, Meyers PD, Walton NY, et al. A comparison of fourtreatments for generalized convulsive status epilepticus: VeteransAffairs Status Epilepticus Cooperative Study Group. N Engl J Med1998;339:792–8.
2. Sloviter RS. “Epileptic” brain damage in rats induced by sustainedelectrical stimulation of the perforant path, I: acute electrophysiolog-ical and light microscopic studies. Brain Res Bull 1983;10:675–97.
3. Kapur J, Macdonald RL. Rapid seizure-induced reduction of benzo-diazepine and Zn2+ sensitivity of hippocampal dentate granule cellGABAA receptors. J Neurosci 1997;17:7532–40.
4. Mazarati AM, Baldwin RA, Sankar R, et al. Time-dependent de-crease in the effectiveness of antiepileptic drugs during the courseof self-sustaining status epilepticus. Brain Res 1998;814:179–85.
5. Claassen J, Hirsch LJ, Emerson RG, et al. Treatment of refractorystatus epilepticus with pentobarbital, propofol, or midazolam: a sys-tematic review. Epilepsia 2002;43:146–53.
6. Walker MC. Status epilepticus on the intensive care unit. J Neurol2003;250:401–6.
7. Meldrum BS. Excitatory amino acid receptors and their role inepilepsy and cerebral ischaemia. Ann N Y Acad Sci 1995;757:492–505.
8. Clifford DB, Olney JW, Benz AM, et al. Ketamine, phencyclidine,and MK801 protect against kainic acid-induced seizure-related braindamage. Epilepsia 1990;31:382–90.
9. Fariello RG, Golden GT, Smith GG, et al. Potentiation of kainic acidepileptogenicity and sparing from neuronal damage by an NMDAreceptor antagonist. Epilepsy Res 1989;3:206–13.
10. Penix LP, Wasterlain CG. Selective protection of neuropeptide con-taining dentate hilar interneurons by non-NMDA receptor blockadein an animal model of status epilepticus. Brain Res 1994;644:19–24.
11. Borris DJ, Bertram EH, Kapur J. Ketamine controls prolonged statusepilepticus. Epilepsy Res 2000;42:117–22.
12. Prasad A, Williamson BA, Bertram EH. Phenobarbital and MK-801, but not phenytoin, improve the long-term outcome of statusepilepticus. Ann Neurol 2002;51:175–81.
13. Walton NY, Treiman DM. Motor and electroencephalographic re-sponse of refractory experimental status epilepticus in rats to treat-ment with MK-801, diazepam, or MK-801 plus diazepam. BrainRes 1991;553:97–104.
14. Rice AC, DeLorenzo RJ. N-methyl-D-aspartate receptor activationregulates refractoriness of status epilepticus to diazepam. Neuro-science 1999;93:117–23.
15. Siegfried J, Fischer R. Budipine: a new chemical substance in thetreatment of Parkinson’s disease. In: Gerstenbrand F, Poewe W,Stern G, eds. Clinical experiences with budipine in Parkinson ther-apy. New York: Springer-Verlag, 1985:152–7.
16. Eltze M. Multiple mechanisms of action: the pharmacological pro-file of budipine. J Neural Transm 1999(suppl); 56:83–105.
17. Klockgether T, Wullner U, Steinbach JP, et al. Effects of the an-tiparkinsonian drug budipine on central neurotransmitter systems.Eur J Pharmacol 1996;301:67–73.
18. Glauser T. Topiramate. Epilepsia 1999;40(suppl 5):S71–80.19. Shank RP, Gardocki JF, Vaught JL, et al. Topiramate: preclin-
ical evaluation of a structurally novel anticonvulsant. Epilepsia1994;35:450–60
20. Holtkamp M, Tong X, Walker MC. Propofol in subanestheticdoses terminates status epilepticus in a rodent model. Ann Neurol2001;49:260–3.
21. Walker MC, Perry H, Scaravilli F, et al. Halothane as a neuropro-tectant during constant stimulation of the perforant path. Epilepsia1999;40:359–64.
22. Paxinos G, Watson C. The rat brain in stereotaxic coordinates. Syd-ney: Academic Press, 1986.
23. Lee VC, Moscicki JC, DiFazio CA. Propofol sedation producesdose-dependent suppression of lidocaine-induced seizures in rats.Anesth Analg 1998;86:652–57.
24. Racine RJ. Modification of seizure activity by electrical stimu-lation, II: motor seizure. Electroencephalogr Clin Neurophysiol1972;32:281–94.
25. Shank RP, Gardocki JF, Streeter AJ, et al. An overview of the pre-clinical aspects of topiramate: pharmacology, pharmacokinetics, andmechanism of action. Epilepsia 2000;41(suppl 1):S3–9.
26. Sharief M, Viteri C, Ben-Menachem E, et al. Double-blind, placebo-controlled study of topiramate in patients with refractory partialepilepsy. Epilepsy Res 1996;25:217–24.
27. Faught E. Efficacy of topiramate as adjunctive therapy in re-fractory partial seizures: United States trial experience. Epilepsia1997;38(suppl 1):S24–7.
28. Coppola G, Caliendo G, Terracciano MM, et al. Topiramatein refractory partial-onset seizures in children, adolescents andyoung adults: a multicentric open trial. Epilepsy Res 2001;43:255–60.
29. Reuber M, Evans J, Bamford JM. Topiramate in drug-resistant com-plex partial status epilepticus. Eur J Neurol 2002;9:111–2.
30. Towne AR, Garnett RN, Waterhouse EJ, et al. The use of topiramatein refractory status epilepticus. Neurology 2003;60:332–4.
31. Niebaurer M, Gruenthal M. Topiramate reduces neuronal injury afterexperimental status epilepticus. Brain Res 1999;837:263–9.
32. Rigoulot MA, Koning E, Ferrandon A, et al. Neuroprotective prop-erties of topiramate in the lithium-pilocarpine model of epilepsy.J Pharmacol Exp Ther 2004;308:787–95.
33. Lee S-R, Kim S-P, Kim J-E. Protective effect of topiramate againsthippocampal neuronal damage after global ischaemia in the gerbils.Neurosci Lett 2000;281:183–6.
34. Yang Y, Suaib A, Li Q, et al. Neuroprotection by delayed admin-istration of topiramate in a rat model of middle cerebral artery em-bolization. Brain Res 1998;804:169–76.
35. Brandt C, Potschka H, Loscher W, et al. N-methyl-D-aspartate re-ceptor blockade after status epilepticus protects against limbic braindamage but not against epilepsy in the kainate model of temporallobe epilepsy. Neuroscience 2003;118:727–40.
36. Meldrum BS, Brierley JB. Prolonged epileptic seizures in primates:ischemic cell change and its relation to ictal physiological events.Arch Neurol 1973;28:10–7.
37. Williamson JM, Lothman EW. The effects of MK801 on kindledseizures: implications for use and limitations as an antiepileptic drug.Ann Neurol 1989;26:85–90.
38. Carter A. Many agents that antagonize the NMDA receptor-channelcomplex in vivo also cause disturbances of motor coordination.J Pharmacol Exp Ther 1994;269:573–80.
39. Geter-Douglass B, Witkin JM. Behavioural effects and anticonvul-sant efficacies of low-affinity, uncompetitive NMDA antagonists inmice. Psychopharmacology 1999;146:280–9.
40. Parsons CG, Quack G, Bresink I, et al. Comparison of the po-tency, kinetics and voltage-dependency of a series of uncompetitiveNMDA receptor antagonists in vitro with anticonvulsive and mo-tor impairment activity in vivo. Neuropharmacology 1995;34:1239–58.
41. Kornhuber J, Herr B, Thome J, et al. The antiparkinsonian drugbudipine binds to NMDA and sigma receptors in post-mortem braintissue. J Neural Transm Suppl 1995;46:131–7.
42. Jellinger K, Bliesath H. Adjuvant treatment of Parkinson’s dis-ease with budipine: a double-blind trial versus placebo. J Neurol1987;234:280–2.
Epilepsia, Vol. 45, No. 11, 2004

TOPIRAMATE AND BUPIDINE SYNERGISM 1307
43. Parsons CG, Hartmann S, Spielmanns P. Budipine is a low affin-ity, N-methyl-D-aspartate receptor antagonist: patch clamp studiesin cultured striatal, hippocampal, cortical and superior colliculusneurones. Neuropharmacology 1998;37:719–27.
44. MacDonald JF, Bartlett MC, Mody I, et al. Actions of ketamine,phencyclidine and MK-801 on NMDA receptor currents in culturedmouse hippocampal neurones. J Physiol 1991;432:483–508.
45. Przuntek H, Stasch JP. Biochemical and pharmacologic aspects ofthe mechanism of action of budipine. In: Gerstenbrand F, PoeweW, Stern G, eds. Clinical experiences with budipine in Parkinsontherapy. New York: Springer-Verlag, 1985:107–12.
46. Biggs CS, Fisher A, Starr MS. The antiparkinsonian drug budipinestimulates the activity of aromatic L-amino acid decarboxylase andenhances L-DOPA-induced dopamine release in rat substantia nigra.Synapse 1998;30:309–17.
47. Biggs CS, Starr MS. Microdialysis study of the effects of theantiparkinsonian drug budipine on L-Dopa-induced release ofdopamine and 5-hydroxytryptamine by rat substantia nigra and cor-pus striatum. Synapse 1999;34:36–46.
48. Keim C, Mutschler E, Lambrecht G, et al. Affinity of the antiparkin-sonian drug, budipine, on native muscarinic M1-M3 and human re-combinant m1-m5 receptors. Naunyn Schmiedeberg Arch Pharma-col 1998;357(suppl S):79.
49. Mihatsch W, Russ H, Przuntek H. Intracerebroventricular admin-istration of 1-methyl-4-phenylpyridinium ion in mice: effects ofsimultaneously administered nomifensine, deprenyl and 1-t-butyl-4,4-diphenylpiperidine. J Neural Transm 1988;71:177–88.
50. Jackisch R, Huang HY, Reimann W, et al. Effects of the antiparkin-sonian drug budipine on neurotransmitter release in central nervoussystem tissues in vitro. J Pharmacol Exp Ther 1993;264:207–11.
Epilepsia, Vol. 45, No. 11, 2004