Syncope medical emergency
31
SYNCOPE BY: KRUTIKA D MISTRY
-
Upload
krutika-mistry -
Category
Healthcare
-
view
5.159 -
download
0
Transcript of Syncope medical emergency
SYNCOPE
BY: KRUTIKA D MISTRY
INTRODUCTION
• Syncope is referred as sudden, transient loss of consciousness that usually occurs secondary to a period of cerebral ischemia.
• Types of syncope– Vasovagal syncope– Cardiac syncope
PREDISPOSING FACTORS FOR VASODEPRESSOR SYNCOPE• PSYCHOGENIC
FACTORS– Fright– Anxiety– Emotional stress– Reciept of unwelcome news– Pain especially sudden
& unepected– Sight of blood or surgical or
other dental instruments.
• NON PSYCHOGENIC FACTORS– Erect siting or standing
positions– Hunger from dieting &
missing meals– Exhaustion– Poor physical condition – Hot humid crowded
environment– Male gender – Age group 16 to 35 years
PREVENTION• Prevention of vasodepressor syncope is directed at
eliminating those factors that predispose an individual to faint.
• Adequate air conditioning eliminates the heat factor.
• Patient hunger, a result of dieting or a missed meal before the dental appointment, also should be considered; all patients, but especially those who are anxious, should be requested to eat a light snack or meal before their dental appointment to minimize the risk of developing hypoglycemia in addition to a psychogenic response.
VASODEPRESSOR SYNCOPE CAN BE GROUPED AS:• PRESYNCOPE• SYNCOPE• POSTSYNCOPE

CLINICAL MANIFESTATIONS
PRESYNCOPE
EARLY• Feeling of warmth• Loss of color
– Pale or ashen- gray skin tone
• Heavy perspiration • Nausea• Blood pressure at
baseline level• Tachycardia
LATE• Pupillary dilation• Yawning • Cold hands & feet• Hypotension• Bradycardia • Visual disturbances • Dizziness • Loss of consciousness• Hypernea
SYNCOPE
• With The Loss Of Consciousness Breathing May:1. Become irregular, jerky, & gasping;2. Become quiet, shallow, and scarcely perceptible;3. Cease entirely- respiratory arrest or apnea.
• The pupils dilate, and the patient takes on deathlike appearance.
• Convulsive movements and muscular twitching of the hands, legs or facial and their brains become hypoxic, even for periods as short as 10 seconds.
• Bradycardia, which develops at the end of the presyncopal phase continues.
• A heart rate of less than 50 beats per minute is common during syncope.
• The blood pressure which falls precipitously to an extremely low level also remains low during this phase and often is difficult to obtain.
• The pulse becomes weak & thready. • Loss of consciousness is also associated with a
generalized muscular relaxation that commonly leads to partial or complete airway obstruction.
• Fecal incontinence may occur, particularly when systolic blood pressure falls below 70mm of Hg.
• Once the patient in supine position, the duration of syncope is extremely brief, ranging from several seconds to several minutes.
• If the patient remains unconscious for more than 5 min after proper positioning and management are achieved, or if the patient does not undergo a complete clinical recovery in 15 to 20 mins causes other than syncope should be considered
POST SYNCOPE( RECOVERY)
• With proper positioning recovery is rapid.• In the postsyncopal phase the patient may
demonstrate pallor, nausea, weakness and sweating, all of which last from a few minutes to several hours
• Symptoms persist 24hours. • During the immediate postsyncopal phase, the
patient may experience a short period of confusion or disorientation.
• Arterial blood pressure begins to rise at this time, it may not return to the baseline level several hours after the syncopal episode
• The heart rate, which is depressed, also returns slowly toward the baseline level and the pulse becomes stronger.
• In addition a point worth stressing is that once a patient loses consciousness the tendency for that patient to faint again may persist for many hours if the patient assumes a sitting position or stands too soon or quickly.
PATHOPHYSIOLOGY
PRESYNCOPE
This increase in catecholamines result in changes in tissue blood perfusion designed to prepare the individual for increased muscular activity.
Among many responses to catecholamine release are a decrease in peripheral vascular resistance and an increase in blood flow to many tissues particularly to peripheral skeletal muscles
In situation in which the this anticipated muscular activity occurs, the blood volume that was diverted to the muscles in the preparation for this movement is returned to the heart by pumping actions of the muscles.
In this case peripheral pooling of blood may occur ; the blood remains at or above the baseline level, signs and symptoms of vasodepressor syncope do not develop.
In situation in which the planned for muscular activity does not occur, the diversion of large volume of blood into the skeletal muscle causes a significant pooling of the blood in these muscles with an associated decrease in the volume of blood being returned to the heart.
This leads to relative decrease in circulating blood volume, a drop in arterial blood pressure, and a decrease in cerebral blood flow. Presyncopal signs & symptoms are related to decreased cardiac output, diminished cerebral blood flow and other physiologic alterations.
• As blood pools in peripheral vessels and arterial blood pressure begins to fall, compensatory mechanisms are activated that attempt to maintain adequate cerebral blood flow.
• These mechanisms include baroreceptors, which reflexely constrict peripheral blood vessels, increasing the return of venous blood to the heart, and the carotid and the aortic arch reflexes, which increases the heart rate.
• These mechanisms work to increase the cardiac output and the maintenance of a close to normal blood pressure, all of which are seen during early presyncopal period
• If the situation goes unmanaged these compensatory mechanisms fatigue, which is manifested through development of reflex bradycardia.
• Slowing of the heart rate to less than 50 beats/min is common & leads to a significant drop of cardiac output which is precipitous fall in blood pressure to levels below the critical for maintenance of consciousness.
• In such cases, cerebral ischemia results and the individual loses consciousness
SYNCOPE• The critical level of cerebral blood flow for the maintenance
of consciousness is established to be about 30 ml of blood per 100g of brain tissue per minute. The normal value of cerebral blood flow is 50-55ml per 100g per minute.
• In a fight or flight situation in which muscular movement is absent with the patient maintained in the upright position, the heart’s ability to pump this critical volume of blood flow is not reached, leading to syncope.
• Convulsive movements such as tonic, or clonic contractions of the arms and legs or turning of the head, may occur with onset of syncope.
• Cerebral ischemia lasting only 10 seconds can lead to seizure activity in patients with no prior histories of seizure disorders.
RECOVERY
• Recovery is usually hastened by placing the victim in the supine position with their legs elevated slightly, improving venous return to the heart and increasing blood flow to the brain so that cerebral blood flow once again exceeds the critical level necessary for maintenance of consciousness.
• Signs & symptoms such as weakness, sweating, & pallor may persist for hours.
• The body is fatigued and may require as long as 24 hrs to return to its normal functioning state after a syncopal episode.

MANAGEMENT
PRESYNCOPE
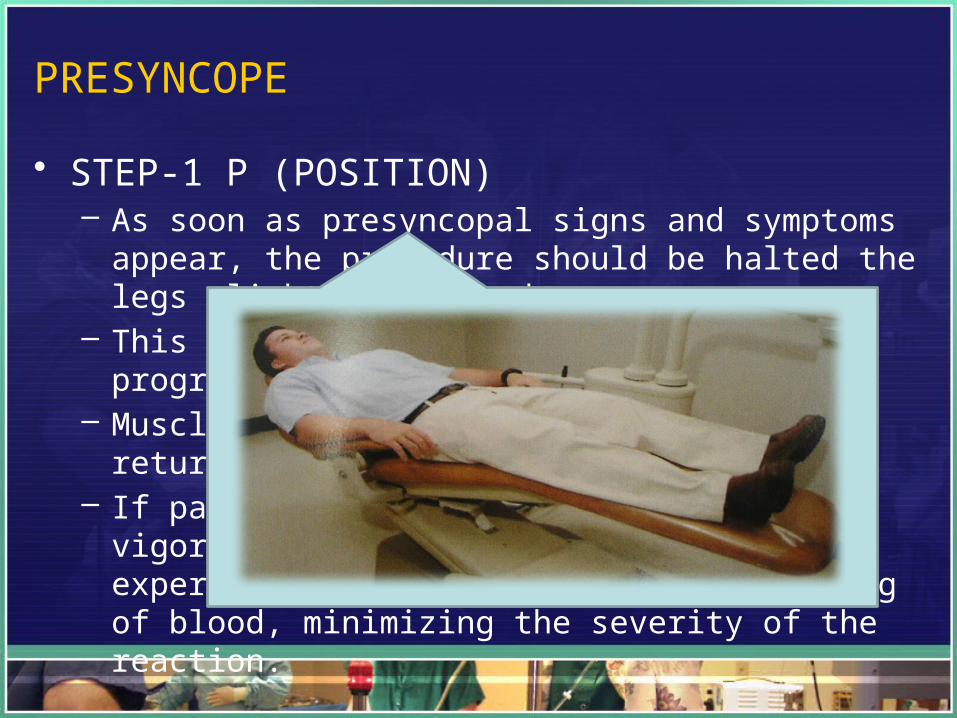
• STEP-1 P (POSITION)– As soon as presyncopal signs and symptoms appear, the
procedure should be halted the legs slightly elevated.– This position change usually halts the progression of
symptoms. – Muscle movement also helps increase the return of blood
from the periphery.– If patients can move their legs vigorously, they are less
likely to experience significant peripheral pooling of blood, minimizing the severity of the reaction.
• STEP-2: A B C– AIRWAY - BREATHING - CIRCULATION– The fairly common practice of placing the victim’s head
between his or her legs when presyncopal signs and symptoms develop should be discontinued.
– Bending over to such an extreme degree may actually further impede the return of blood from legs through a partial obstruction of the inferior vena cava, resulting in a greater decrease in blood flow to the brain.
– Furthermore, if patients lose consciousness while placing head between their legs, this position does not facilitate proper airway management.
– O2 may be administered through use of a full- face mask, or an ammonia ampule may be crushed under patient nose for speed recovery.
• STEP: 3 D( DEFINITIVE CARE)– Modifications in future dental treatment should be
considered to minimize the risk of recurrence – The planned dental treatment may proceed only if both
the doctor and the patient feel it is appropriate. – If either party remains doubtful, treatment should be
postponed.
SYNCOPE
• The basic management required for all unconscious patients: P A B C
Step 1 Assessment of consciousness
• The patient suffering vasodepressor syncoper demonstrates a lack of response to sensory stimulation.(Shake & shout)
Step 2 Activation of the dental office emergency system
• Office team members should perform their assigned duties.
STEP 3 P
• The placement of patient in supine position with slightly elevation of legs which helps in increase the return of blood from the periphery.
• Clinical manifestations during syncope are result of inadequate cerebral blood flow. • Failure to place the victim in the supine position may result in death or permanent
neurological damage secondary to prolonged cerebral ischemia• This damage occurs in as little as 2 to 3 mins if victim maintains an upright position.
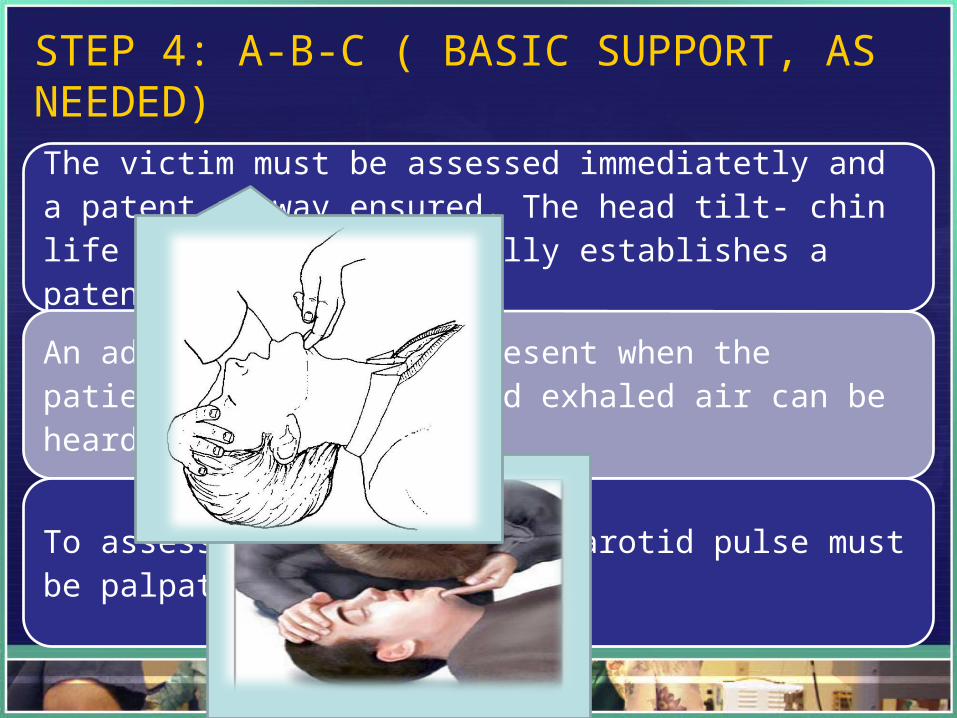
STEP 4: A-B-C ( BASIC SUPPORT, AS NEEDED)
The victim must be assessed immediatetly and a patent airway ensured. The head tilt- chin life position successfully establishes a patent airway.
An adequate airway is present when the patient’s chest moves and exhaled air can be heard and felt.
To assess circulation, the carotid pulse must be palpated.
STEP 5: D (DEFINITIVE CARE)
Adminsitration of oxygen
• Oxygen may be adminstered to the syncopal or postsyncopal patient at any time during the episode.
Monitoring of vital signs
• Blood pressure, heart rate, respiratory rate should be monitored.
Additional procedures
• Loosening of binding clothes such as ties, collars and belt.• Use of respiratory stimulant( aromatic ammonia) • If bradycardia persist an anticholinergic such as atropine administered either I.V OR I.M
DELAYED RECOVERY
• If the victim doesnot regain conciousness after the previous steps have been performed or doesnot recover completely in 15 to 20 minutes, a different cause for the syncopal episode should be considered and the emergency medical service system activated.
POST SYNCOPE• After recovery patient must not undergo any dental
treatment the remainder for that day. • Body requires up to 24 hours to return to its normal
state.• Prior to dismissal of the patient from the dental
office, the doctor should determine the primary precipitating event and any other factor that contributed to it.
• Arrangement must be made for a person with vested intrest in the health and safety of the patient to take the patient home

THANK YOU