Syncope Initial Evaluation and Management - …/media/Images/Swedish/CME1/SyllabusPDFs/...1 Syncope...
51
1 Syncope Initial Evaluation and Management John L. Petersen II, MD, MHS July 14, 2017 1
Transcript of Syncope Initial Evaluation and Management - …/media/Images/Swedish/CME1/SyllabusPDFs/...1 Syncope...

1
Syncope
Initial Evaluation and Management
John L. Petersen II, MD, MHS
July 14, 2017
1

2
Conflicts
• Stocks/Ownership
– Veravanti
• Speakers Bureau
– None
• Education Grants
– St Jude Medical
• Research Grants/Funding
– Abbott Vascular, Baxter, Biosensors, Reva Medical, Keystone
Medical, NIH
2

3
Question 1
• According to the ACC/AHA Guidelines, an appropriate
initial evaluation for all patients with syncope would
include
A. H and P Alone
B. H and P and ECG
C. H and P, ECG, and Transthoracic Echo
D. H and P, ECG, and Ambulatory ECG Monitor
3

4
Question 2
• Which of the following is not a prognosticator of
morbidity and mortality among patients with syncope
A. Age
B. Nausea and Vomiting
C. Palpitations
D. Cerebral Vascular Disease
4

5
Question 3
• Even with dedicated evaluations to investigate the
cause, the % of cases for which a cause cannot be
established is:
A. 70-80%
B. 50-60%
C. 20-40%
D. 1-10%
5

6
Objectives
• Discuss Definition and Causes of Syncope and other
Causes of Loss of Consciousness
• Review Initial Diagnostic Evaluation
• Identify Appropriate Patients for Additional Studies or
Referral for Specialty Evaluation
6

7
Overview
• Syncope
– Definition
– Classification of Causes
– Non Cardiac Causes of Loss of Consciousness
• Initial Evaluation and Risk Stratification
– History Elements
– Physical Exam Elements
– ECG Elements
– High Risk Features
• Appropriate Patients for Specialty Referral
– Which patients
– What Kind of Testing to Expect 7

8
Syncope
Abrupt, transient, complete loss of consciousness,
associated with inability to maintain postural tone, with
rapid and spontaneous recovery
8

9
What it is and what it is not
Syncope
• Orthostatic Hypotension
• Cardiac
– Bradycardia, tachycardia
– Structural Heart Disease
– Dissection
– Global Ischemia
– Heart Failure
• Pulmonary
– PE, pulmonary hypertension
• Reflex Syncope
– Vasovagal
– Carotid Sinus Syndrome
– Situational
– POTS
Not Syncope
• Coma
• Intoxication / Overdose
• Metabolic Derangements
• Trauma
• Massive Stroke
• Psychogenic Pseudo-
syncope
9

10
Epidemiology
Syncope is common ~ 20% of people will experience it
during a lifetime
The incidence increases with age > 70
10

11
Epidemiology
• Syncope is common ~ 20% of people will experience it
during a lifetime
• The incidence increases with age > 70
• Females are more likely to have syncope than males
• BUT – males are more likely to have high risk syncope
• The most common cause is reflex mediated syncope –
– Otherwise known as Vasovagal Syncope or Neurocardiogenic
syncope
• The etiology varies between studied but between 20-
40% of case no cause is identified
– BUT this has a good prognosis
11

12
Common Scenario
• 52 y.o. male patient presents to office on a Tuesday.
Over the weekend, had a passing out spell in the
afternoon at a barbeque. He woke up within a minute
or two and then felt better. The rest of the weekend
was uneventful
What do you do next?
12

13
General Principles
Transient loss of consciousness*
Suspected
syncope
Yes
Evaluation as clinically
indicatedNo
Risk assessmentCause of syncope
certain
Cause of syncope
uncertain
Further evaluationTreatment
Initial evaluation:
history, physical examination,
and ECG
(Class I)
Syncope Initial Evaluation
*See relevant terms and definitions in Table 3.
Colors correspond to Class of Recommendation in Table 1. This figure shows the
general principles for initial evaluation of all patients after an episode of syncope.
ECG indicates electrocardiogram.

14
History and Physical Examination
COR LOE Recommendation
I B-NRA detailed history and physical examination should be
performed in patients with syncope.
Electrocardiography
COR LOE Recommendation
I B-NRIn the initial evaluation of patients with syncope, a
resting 12-lead ECG is useful.

15
History
• So you say I need to do a good H and P
– What does that mean? Ask them about childhood
immunizations? Do a Weber-Rinne test?
• Targeted History
– Description of Episode(s)
• Important for clarifying etiology
– Number of Episodes
– Medications
– Comorbid Conditions
– Family History

16
Description of the Event
• Situation
– Decreased volume status,
ethanol and substance use
– Exercise/Exertion
– Anxiety provoking situation
– Fatigue, Sleep Depravation
– Postural changes
– Concomitant Body Functions
(Coughing, Valsalva,
Micturition, Defecation,
Deglutination)
• Prodrome
– Duration
– Nausea, Vomiting
– Flushing, Pallor
– Palpitations
– Dyspnea
• Recovery
– Bladder, Bowel
Function
– Trauma
– Evidence of Bleeding

17
Past History
• Prior Episodes
– Similarity and Age of Onset
• Medications
– Cardiac Medications
– Psychiatric Medications
– Antibiotics and other QT prolonging medications
• Known Cardiac History and Cardiac ROS
• Known Neurological History and Neurological ROS
17

18
Family History
• Cardiac Family History
– Early Atherosclerosis
– Cardiomyopathy
– Arrhythmia / ICD
placement
– Sudden Death
– Hypercoagulable State
– Aortic Dissection
• Neurologic Family History
– Seizures
– Degenerative Diseases
– Neuropathy
18

19
Detailed Exam
• Cardiac Exam
– Murmurs, Rhythm, Signs of R and L Heart Failure
– Bruits and evidence of atherosclerotic vascular disease
– Orthostatics – Including 3 minute recheck
• Neurological Exam
– Evidence of Degenerative Neurologic Disease
– Strength, Sensation, Balance, Tremors
19

20
ECG
• What to look for:
– Rhythm – Heart block, Atrial Arrhythmias, Wide Complex
Rhythm
– Conduction Disease – LBBB, RBBB, etc
– Pre-Excitation (WPW or short PR interval)
– Repolarization Abnormalities (hypertrophic CM)
– Chamber enlargement, including LAE
– Prior MI
– Long QT syndrome (QTc 500 msec without obvious cause)
– Brugada syndrome
20

21
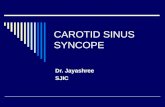
WPW (Wolfe-Parkinson-White)
21

22
Hypertrophic Cardiomyopathy
22

23
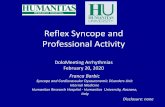
Long QT Syndrome
23

24
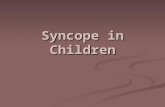
Brugada Syndrome
24

25
Risk Assessment
COR LOE Recommendations
I B-NR
Evaluation of the cause and assessment for the short-
and long-term morbidity and mortality risk of syncope
are recommended.
IIb B-NRUse of risk stratification scores may be reasonable in
the management of patients with syncope.

26
High/Moderate Risk – Short Term (< 30 days)
• History – Male
– Age > 60
– No prodrome
– Palpitations
– Exertion
– Structural Heart Disease
– Heart Failure
– Cerebrovascular Disease
– Family History of Sudden
Death
– Trauma
• Physical Exam / Lab
– Bleeding
– Persistently Abnormal
Vital Signs
– Abnormal ECG
– Positive Troponin
26

27
High/Moderate Risk – Long Term (> 30 days)
• History– Male
– Age
– Absence of nausea/vomiting
– Ventricular Arrhythmia
– Cancer
– Structural Heart Disease
– Heart Failure
– Cerebrovascular Disease
– Diabetes
– High CHADS2-Vasc
• Laboratory – Abnormal ECG
– Renal Failure
27

28
Back to our Patient
• 52 yo male passed out at a barbeque in the afternoon
– Ask about situation, prodrome, recovery, past history and
family history and perform exam
– Likely outside, warm
– Tells you he felt flush and bystanders said he looked pale.
– May have involved ethanol consumption and limited water
intake
– If no cardiac or neuro history, no risk factors, no family history,
Exam, vitals, orthostatics and ECG normal
– His only real risk factor is being male – so no further work up.
– Educate the patient about volume and dehydration
28

29
What if?
• He says:
– Father had MI at 48
– There were palpitations preceding the event
– It occurred moving a heavy box of supplies from the pickup to
the picnic table
– ECG has findings of LVH and left atrial enlargement
– This is not low risk
• Needs further evaluation
• Ambulatory ECG and Echo to start, consider stress test based on
additional symptoms of exertion
29

30
Examples Of High Risk Conditions
Warranting Hospitalization
• Cardiac Arrhythmia
– Sustained VT
– High Degree AV block
– Symptomatic Bradycardia
– Sinus Pauses
– Symptomatic SVT
– ICD Malfunction
– Genetic Conditions
• Other Cardiac
– Coronary Ischemia
– Severe AS
– Cardiac Tamponade
– Hypertrophic cardiomyopathy
– Severe prosthetic valve
dysfunction
– Pulmonary embolism
– Aortic Dissection
– Acute heart Failure
– Sytolic LV dysufnction
30
• Other Non Cardiac
– Severe Anemia / Bleeding
– Major Trauma
– Persistent Vital Sign
Abnormalities

31
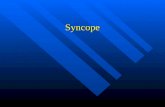
Patient Disposition After Initial Evaluation for Syncope
Syncope initial evaluation
Manage presumptive
reflex-mediated
syncope in
outpatient setting
(Class IIa)
Inpatient evaluation
(Class I)
Yes
Serious
medical conditions
present?
(Table 7)
Structured ED
observation protocol
for intermediate-
risk pts
(Class IIa)
Manage selected pts
with suspected
cardiac syncope in
outpatient setting
(Class IIb)
No
Colors correspond to Class of Recommendation in Table 1.
ED indicates emergency department; pts, patients.

32
Disposition After Initial Evaluation
COR LOE Recommendations
I B-NR
Hospital evaluation and treatment are recommended for
patients presenting with syncope who have a serious
medical condition potentially relevant to the cause of
syncope identified during initial evaluation.
IIa C-LDIt is reasonable to manage patients with presumptive
reflex-mediated syncope in the outpatient setting in the
absence of serious medical conditions.
IIa B-R
In intermediate-risk patients with an unclear cause of
syncope, use of a structured ED observation protocol
can be effective in reducing hospital admission.
IIb C-LD
It may be reasonable to manage selected patients with
suspected cardiac syncope in the outpatient setting in
the absence of serious medical condition.

33
When to Refer?
• Referral
– Clear evidence of
cardiac disease or
assessment that finds
patient is at risk for
cardiac disease
– Clear evidence
neurologic disease
– Intermediate risk –
reflex syncope with
other findings
– No findings at all – not
clearly reflex mediated
• When Not to Refer
– No findings of Cardiac
or Neuro disease
– No orthostasis
– ECG negative
– No family history
– Event history consistent
with reflex mediated
syncope (OH,
Vasovagal)
33

34
Additional Evaluation and Diagnosis
Initial
evaluation
suggests reflex
syncope
Initial evaluation
unclear
Targeted blood
testing
(Class IIa)†
Initial
evaluation
suggests
neurogenic OH
Initial
evaluation
suggests CV
abnormalities
Referral for
autonomic
evaluation
(Class IIa)†
TTE
(Class IIa)†
Stress testing
(Class IIa)†
Tilt-table
testing
(Class IIa)†
Cardiac monitor
selected based
on frequency
and nature
(Class I)
Implantable
cardiac monitor
(Class IIa)†
Ambulatory
external cardiac
monitor
(Class IIa)†
Options
Initial evaluation:
history, physical exam, ECG
(Class I)
EPS
(Class IIa)†
Initial evaluation
clear
MRI or CT
(Class Ilb)†
No additional
evaluation
needed*
Options
Syncope additional evaluation and diagnosis
Colors correspond to Class of Recommendation in Table 1.
*Applies to patients after a normal initial evaluation without significant injury or
cardiovascular morbidities; patients followed up by primary care physician as needed.
†In selected patients (see Section 1.4).
CT indicates computed tomography; CV, cardiovascular; ECG, electrocardiogram; EPS,
electrophysiological study; MRI, magnetic resonance imaging; OH, orthostatic
hypotension; and TTE, transthoracic echocardiography.

35
What about other tests?
• Labs
• Echo
• Stress Testing
• Holter and or Ambulatory ECG monitoring
• CT head / MRI Head
• EEG
• Carotid Ultrasound
35

36
COR LOE Recommendations
IIa B-NR
Targeted blood tests are reasonable in the evaluation
of selected patients with syncope identified on the
basis of clinical assessment from history, physical
examination, and ECG.
IIb C-LD
Usefulness of brain natriuretic peptide and high-
sensitivity troponin measurement is uncertain in
patients for whom a cardiac cause of syncope is
suspected.
III: No
BenefitB-R
Routine and comprehensive laboratory testing is not
useful in the evaluation of patients with syncope.
Blood Testing

37
Cardiac Imaging
COR LOE Recommendations
IIa B-NR
Transthoracic echocardiography can be useful in selected
patients presenting with syncope if structural heart
disease is suspected.
IIb B-NRCT or MRI may be useful in selected patients presenting
with syncope of suspected cardiac etiology.
III: No
BenefitB-R
Routine cardiac imaging is not useful in the evaluation of
patients with syncope unless cardiac etiology is
suspected on the basis of an initial evaluation, including
history, physical examination, or ECG.
Cardiovascular Testing

38
Stress Testing
COR LOE Recommendation
IIa C-LD
Exercise stress testing can be useful to establish the
cause of syncope in selected patients who experience
syncope or presyncope during exertion.

39
Cardiac Monitoring
COR LOE Recommendations
I C-EOThe choice of a specific cardiac monitor should be
determined on the basis of the frequency and nature of
syncope events.
IIa B-NR
To evaluate selected ambulatory patients with syncope of
suspected arrhythmic etiology, the following external
cardiac monitoring approaches can be useful:
1. Holter monitor
2. Transtelephonic monitor
3. External loop recorder
4. Patch recorder
5. Mobile cardiac outpatient telemetry.
IIa B-RTo evaluate selected ambulatory patients with syncope of
suspected arrhythmic etiology, an ICM can be useful.

40
Neurological and Imaging Diagnostics
COR LOE Recommendations
IIa C-LD
Simultaneous monitoring of an EEG and hemodynamic
parameters during tilt-table testing can be useful to
distinguish among syncope, pseudosyncope, and
epilepsy.
III: No
BenefitB-NR
MRI and CT of the head are not recommended in the
routine evaluation of patients with syncope in the absence
of focal neurological findings or head injury that support
further evaluation.
III: No
BenefitB-NR
Carotid artery imaging is not recommended in the routine
evaluation of patients with syncope in the absence of
focal neurological findings that support further evaluation.
III: No
BenefitB-NR
Routine recording of an EEG is not recommended in the
evaluation of patients with syncope in the absence of
specific neurological features suggestive of a seizure.

41
COR LOE Recommendations
I C-EOPatient education on the diagnosis and prognosis of VVS
is recommended.
IIa B-R
Physical counter-pressure maneuvers can be useful in
patients with VVS who have a sufficiently long prodromal
period.
IIa B-RMidodrine is reasonable in patients with recurrent VVS
with no history of hypertension, HF, or urinary retention.
IIb B-RThe usefulness of orthostatic training is uncertain in
patients with frequent VVS.
IIb B-R
Fludrocortisone might be reasonable for patients with
recurrent VVS and inadequate response to salt and fluid
intake, unless contraindicated.
Reflex Conditions
Vasovagal Syncope

42
IIb B-NRBeta blockers might be reasonable in patients 42 years of
age or older with recurrent VVS.
IIb C-LD
Encouraging increased salt and fluid intake may be
reasonable in selected patients with VVS, unless
contraindicated.
IIb C-LD
In selected patients with VVS, it may be reasonable to
reduce or withdraw medications that cause hypotension
when appropriate.
IIb C-LDIn patients with recurrent VVS, a selective serotonin
reuptake inhibitor might be considered.
Vasovagal Syncope (cont.)

43
Vasovagal Syncope
VVS
Education on
diagnosis and prognosis
(Class I)
Counter pressure
maneuvers
(Class IIa)
Salt and fluid
intake
(Class IIb)
VVS recurs
Selected serotonin
reuptake inhibitors
(Class IIb)
Midodrine
(Class IIa)
Beta blocker
(in patients >42 y)
(Class IIb)
Orthostatic training
(Class IIb)
Dual-chamber
pacemaker therapy
(Class IIb)
Fludrocortisone
(Class IIb)
Options
Options
Colors correspond to Class of Recommendation in Table 1.
VVS indicates vasovagal syncope.

44
Orthostatic
Hypotension
Colors correspond to Class
of Recommendation in
Table 1.
BP indicates blood pressure;
OH, orthostatic hypotension.
Continue to
evaluate
Syncope of suspected OH origin
Postural decrease in
BP ≥20/10 mm HgNo
Neurogenic OH
Compression
garments
(Class IIa)
Counter-pressure
maneuvers
(Class IIa)
Fludrocortisone
(Class IIa)
Midodrine
(Class IIa)
Droxidopa
(Class IIa)
Pydridostigmine
(Class IIb)
Drugs Dehydration
Options
Acute water
ingestion
(Class I)
Reduce or withdraw
medications
(Class IIa)
Reduce or withdraw
medications
(Class IIa)
Octreotide
(Class IIb)
Acute water
ingestion
(Class I)
Increase salt
and fluid intake
(Class IIb)
Increase salt and
fluid intake
(Class IIa)
Therapy options in
selected patients

45
Conclusions
• Syncope is common and incidence increases with age
• It is important to distinguish high risk and low risk
causes
• This is based mostly on history, exam, and ECG.
• Patients with clear reflex mediated syncope can be
managed conservatively
• Patients with clear cardiac or neurologic disease
should be referred – and possibly admitted
• Patients with intermediate risk should be referred with
directed additional testing based on findings
45

46
Question 1
• According to the ACC/AHA Guidelines, an appropriate
initial evaluation for all patients with syncope would
include
A. H and P Alone
B. H and P and ECG
C. H and P, ECG, and Transthoracic Echo
D. H and P, ECG, and Ambulatory ECG Monitor
46

47
Question 1
• According to the ACC/AHA Guidelines, an appropriate
initial evaluation for all patients with syncope would
include
A. H and P Alone
B. H and P and ECG
C. H and P, ECG, and Transthoracic Echo
D. H and P, ECG, and Ambulatory ECG Monitor
47

48
Question 2
• Which of the following is not a prognosticator of
morbidity and mortality among patients with syncope
A. Age
B. Nausea and Vomiting
C. Palpitations
D. Cerebral Vascular Disease
48

49
Question 2
• Which of the following is not a prognosticator of
morbidity and mortality among patients with syncope
A. Age
B. Nausea and Vomiting
C. Palpitations
D. Cerebral Vascular Disease
49

50
Question 3
• Even with dedicated evaluations to investigate the
cause, the % of cases for which a cause cannot be
established is:
A. 70-80%
B. 50-60%
C. 20-40%
D. 1-10%
50

51
Question 3
• Even with dedicated evaluations to investigate the
cause, the % of cases for which a cause cannot be
established is:
A. 70-80%
B. 50-60%
C. 20-40%
D. 1-10%
51