Syncope Due to Idiopathic Paroxysmal Atrioventricular Block · Syncope Due to Idiopathic Paroxysmal...
7
Syncope Due to Idiopathic Paroxysmal Atrioventricular Block Long-Term Follow-Up of a Distinct Form of Atrioventricular Block Michele Brignole, MD,* Jean-Claude Deharo, MD,† Luc De Roy, MD,‡ Carlo Menozzi, MD,§ Dominique Blommaert, MD,‡ Lara Dabiri, MD,‡ Jean Ruf, MD, Regis Guieu, MD¶ Lavagna and Reggio Emilia, Italy; Marseille, France; and Yvoir, Belgium Objectives We present data on patients with syncope due to paroxysmal atrioventricular (AV) block unexplainable in terms of currently known mechanisms. Background Paroxysmal AV block is known to be due to intrinsic AV conduction disease or to heightened vagal tone. Methods We evaluated 18 patients presenting with unexplained syncope who had: 1) normal baseline standard electro- cardiogram (ECG); 2) absence of structural heart disease; and 3) documentation, by means of prolonged ECG monitoring at the time of syncopal relapse, of paroxysmal third-degree AV block with abrupt onset and absence of other rhythm disturbances before or during the block. Results The study group consisted of 9 men and 9 women, mean age 55 19 years, who had recurrent unexplained syncope for 8 7 years and were subsequently followed up for as long as 14 years (4 4 years on average). The patients had no structural heart disease, standard ECG was normal, and electrophysiological study was neg- ative. In all patients, prolonged ECG monitoring documented paroxysmal complete AV block with 1 or multiple consecutive pauses (mean longest pause: 9 7 s at the time of syncope); AV block occurred without P-P cycle lengthening or PR interval prolongation. During the observation time, no patient had permanent AV block; on permanent cardiac pacing, no patient had further syncopal recurrences. Conclusions Common clinical and electrophysiological features define a distinct form of syncope due to idiopathic paroxys- mal AV block characterized by a long history of recurrent syncope, absence of progression to persistent forms of AV block, and efficacy of cardiac pacing therapy. (J Am Coll Cardiol 2011;58:167–73) © 2011 by the American College of Cardiology Foundation Paroxysmal third-degree atrioventricular (AV) block is a known cause of syncope. Paroxysmal AV block that occurs in patients with underlying heart disease and/or abnormal standard electrocardiogram (ECG) is usually regarded as a manifestation of an intrinsic disease of the AV conduction system (Stokes-Adams attack). This is usually confirmed by abnormal electrophysiological findings (1,2). Well-defined clinical and electrophysiological features allow differentiat- ing intrinsic AV block from the other known form of block, namely, vagal (extrinsic) paroxysmal AV block. Differenti- ation between the often benign and reversible causes of vagal AV block from intrinsic AV block is of practical importance because the benefit of permanent cardiac pacing for vagal AV block is controversial (3,4). See page 174 In this study, we present data on patients with syncope due to paroxysmal AV block unexplainable in terms of currently known mechanisms. Methods In this 4-center study, we evaluated 18 patients presenting with unexplained syncope who had: 1) normal baseline standard ECG; 2) absence of structural heart disease; and 3) documentation, by means of prolonged ECG monitoring at the time of syncopal relapse, of paroxysmal third-degree AV block with abrupt onset (and delayed emergence of an adequate escape rhythm) and absence of other rhythm disturbances before or during the block (type 1C according to the ISSUE [International Study of Syncope of Uncertain Etiology] study classification [5]). From the *Department of Cardiology, Arrhythmologic Centre, Ospedali del Tigullio, Lavagna, Italy; †Department of Cardiology, Timone University Hospital, Marseille, France; ‡Department of Cardiology, UCL Mont-Godinne, Yvoir, Belgium; §De- partment of Cardiology, Arcispedale S Maria Nuova, Reggio Emilia, Italy; Labora- tory of Biochemistry and Molecular Biology, Timone University Hospital, Marseille, France; and the ¶Université de la Méditerranée, Ministère de la Défense, Marseille, France. The authors have reported that they have no relationships to disclose. Manuscript received September 17, 2010; revised manuscript received December 6, 2010, accepted December 21, 2010. Journal of the American College of Cardiology Vol. 58, No. 2, 2011 © 2011 by the American College of Cardiology Foundation ISSN 0735-1097/$36.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2010.12.045
Transcript of Syncope Due to Idiopathic Paroxysmal Atrioventricular Block · Syncope Due to Idiopathic Paroxysmal...

Journal of the American College of Cardiology Vol. 58, No. 2, 2011© 2011 by the American College of Cardiology Foundation ISSN 0735-1097/$36.00
Syncope Due to IdiopathicParoxysmal Atrioventricular BlockLong-Term Follow-Up of a Distinct Form of Atrioventricular Block
Michele Brignole, MD,* Jean-Claude Deharo, MD,† Luc De Roy, MD,‡ Carlo Menozzi, MD,§Dominique Blommaert, MD,‡ Lara Dabiri, MD,‡ Jean Ruf, MD,� Regis Guieu, MD�¶
Lavagna and Reggio Emilia, Italy; Marseille, France; and Yvoir, Belgium
Objectives We present data on patients with syncope due to paroxysmal atrioventricular (AV) block unexplainable in termsof currently known mechanisms.
Background Paroxysmal AV block is known to be due to intrinsic AV conduction disease or to heightened vagal tone.
Methods We evaluated 18 patients presenting with unexplained syncope who had: 1) normal baseline standard electro-cardiogram (ECG); 2) absence of structural heart disease; and 3) documentation, by means of prolonged ECGmonitoring at the time of syncopal relapse, of paroxysmal third-degree AV block with abrupt onset and absenceof other rhythm disturbances before or during the block.
Results The study group consisted of 9 men and 9 women, mean age 55 � 19 years, who had recurrent unexplainedsyncope for 8 � 7 years and were subsequently followed up for as long as 14 years (4 � 4 years on average).The patients had no structural heart disease, standard ECG was normal, and electrophysiological study was neg-ative. In all patients, prolonged ECG monitoring documented paroxysmal complete AV block with 1 or multipleconsecutive pauses (mean longest pause: 9 � 7 s at the time of syncope); AV block occurred without P-P cyclelengthening or PR interval prolongation. During the observation time, no patient had permanent AV block; onpermanent cardiac pacing, no patient had further syncopal recurrences.
Conclusions Common clinical and electrophysiological features define a distinct form of syncope due to idiopathic paroxys-mal AV block characterized by a long history of recurrent syncope, absence of progression to persistent formsof AV block, and efficacy of cardiac pacing therapy. (J Am Coll Cardiol 2011;58:167–73) © 2011 by theAmerican College of Cardiology Foundation
Published by Elsevier Inc. doi:10.1016/j.jacc.2010.12.045
Paroxysmal third-degree atrioventricular (AV) block is aknown cause of syncope. Paroxysmal AV block that occursin patients with underlying heart disease and/or abnormalstandard electrocardiogram (ECG) is usually regarded as amanifestation of an intrinsic disease of the AV conductionsystem (Stokes-Adams attack). This is usually confirmed byabnormal electrophysiological findings (1,2). Well-definedclinical and electrophysiological features allow differentiat-ing intrinsic AV block from the other known form of block,namely, vagal (extrinsic) paroxysmal AV block. Differenti-ation between the often benign and reversible causes ofvagal AV block from intrinsic AV block is of practical
From the *Department of Cardiology, Arrhythmologic Centre, Ospedali del Tigullio,Lavagna, Italy; †Department of Cardiology, Timone University Hospital, Marseille,France; ‡Department of Cardiology, UCL Mont-Godinne, Yvoir, Belgium; §De-partment of Cardiology, Arcispedale S Maria Nuova, Reggio Emilia, Italy; �Labora-tory of Biochemistry and Molecular Biology, Timone University Hospital, Marseille,France; and the ¶Université de la Méditerranée, Ministère de la Défense, Marseille,France. The authors have reported that they have no relationships to disclose.
Manuscript received September 17, 2010; revised manuscript received December 6,2010, accepted December 21, 2010.
importance because the benefit of permanent cardiac pacingfor vagal AV block is controversial (3,4).
See page 174
In this study, we present data on patients with syncopedue to paroxysmal AV block unexplainable in terms ofcurrently known mechanisms.
Methods
In this 4-center study, we evaluated 18 patients presentingwith unexplained syncope who had: 1) normal baselinestandard ECG; 2) absence of structural heart disease; and3) documentation, by means of prolonged ECG monitoringat the time of syncopal relapse, of paroxysmal third-degreeAV block with abrupt onset (and delayed emergence of anadequate escape rhythm) and absence of other rhythmdisturbances before or during the block (type 1C accordingto the ISSUE [International Study of Syncope of Uncertain
Etiology] study classification [5]).
dah
q2pt
168 Brignole et al. JACC Vol. 58, No. 2, 2011Idiopathic Paroxysmal AV Block July 5, 2011:167–73
These patients underwent afull cardiological work-up thatexcluded structural heart disease.In particular, a conventional in-vasive electrophysiological evalu-ation, which included rapid atrialpacing and ajmaline drug chal-lenge, was performed in 15 pa-tients; 3 patients denied theirconsent for the examination.Further additional nonconven-
tional electrophysiological tests included measurement ofbaseline adenosine plasma level (APL) as described previ-ously (J.C. Deharo et al., personal communication, 2011)(6–8) and adenosine or adenosine triphosphate (ATP) test(9–11). An increased susceptibility to the ATP test has beensuspected in patients with syncope due to paroxysmal AVblock (9). Syncope work-up was completed by means oftilt-table testing and carotid sinus massage.
The APL was also determined in 9 control patients (6men and 3 women, mean age 58 � 17 years) with syncope
ue to reflex long pauses (mean 19 � 16 s) due to sinusrrest documented by implantable loop recorder, and in 81ealthy subjects matched for age and sex.Data are reported as mean � SD or as median (inter-
uartile range [IQR]), as appropriate. Comparison betweencontinuous variables with a non-Gaussian distribution waserformed by applying the Mann-Whitney nonparametricest.
Patient Characteristics, Test Results, and OutcomeTable 1 Patient Characteristics, Test Results, and Outcome
Patient#
Age (yrs),Sex
Syncope
Total No.Duration
(yrs)
1 73, M 20 8.0
2 85, F 4 1.0
3 69, M 2 0.5
4 63, F 3 7.0
5 50, F 20 20.0
6 63, F 6 13.0
7 66, F 25 8.0
8 57, F Very frequent 5.0
9 68, M 6 18.0
10 62, M 4 2.0
11 70, F 100 20.0
12 20, M 4 4.0
13 41, M 10 8.0
14 57, M 21 4.0
15 13, M 1 0.0
16 49, F 2 0.5
17 52, M 1 0.5
18 26, F 10 16.0
Abbreviationsand Acronyms
APL � adenosine plasmalevel
ATP � adenosinetriphosphate
AV � atrioventricular
ECG � electrocardiogram
IQR � interquartile range
Results
The study group consisted of 9 men and 9 women (meanage 55 � 19 years) who had had recurrent unexplainedsyncope and pre-syncope for 8 � 7 years (median 6 years,IQR: 3 to 12 years, range 0 to 20 years) (Table 1). Mostsyncopal episodes were unpredictable, in that prodromeswere absent or very short (a few seconds of dizziness orblurred vision). Only 3 patients had some episodes withfeatures that suggested autonomic activation: during a mealpreceded by prodromes (Patient #4), triggered by unex-plained cough or by emotion (Patient #11), and preceded bynausea and prodromes (Patient #16). The patients did nothave structural heart disease, and standard ECG was nor-mal. Prolonged ECG monitoring (implantable loop re-corder in 10 patients, Holter in 5 patients, and in-hospitaltelemetry in 3 patients) at the time of syncope or pre-syncope documented paroxysmal complete AV block with 1or multiple consecutive pauses (longest pause 9 � 7 s) dueto absence or depression of escape rhythm in all patients;AV block occurred without P-P cycle lengthening (n � 12)or with minimal P-P cycle lengthening (n � 6); PR intervalremained stable before and at the end of the pause (Figs. 1,2, and 3). One patient had advanced AV block, whichpersisted for 2 days, followed by first-degree AV block for afew days and then normal conduction. An electrophysiolog-ical study performed at the time of first-degree AV blockshowed impaired AV nodal conduction. Multiple episodesof AV block (2 to 20) were also documented in 11 patients
Spontaneous AVB
rodromes, AutonomicActivation, Triggers Diagnostic Tool Max Pause, s
o ILR 5.0
o (all while sitting) ILR 13.0
o ILR 3.5
es (meal, prodromes) ILR 5.0
o ILR 22.0
o ILR 10.0
o ILR 28.0
o In-hospital telemetry 4.5
o ILR 17.0
o (1 while driving) ILR 8.0
es (tussive, emotional) 7-day Holter 8.0
o In-hospital telemetry 3.6
o Holter 3.4
o Holter 11.0
o Holter 3.5
es (nausea,rodromes)
Holter 4.8
o (while driving) ILR 4.5
o In-hospital telemetry 5.0
P
N
N
N
Y
N
N
N
N
N
N
Y
N
N
N
N
Yp
N
N
Continued on next page

pitftLstbfs
oc[piAm
169JACC Vol. 58, No. 2, 2011 Brignole et al.July 5, 2011:167–73 Idiopathic Paroxysmal AV Block
in whom monitoring was continued after the first docu-mented syncope; these were always similar to the firstdocumented episode.
After the diagnosis, the patients were followed up for atotal of 4 � 4 years (range 0.6 to 14 years). Seventeen
atients underwent permanent dual-chamber cardiac pac-ng, and no patient had recurrence of syncope. The totalime from the first syncopal symptom to the end ofollow-up was 12 � 8 years (range 1.6 to 34 years). Duringhis period, no patient had permanent AV block.aboratory findings. Electrophysiological study did not
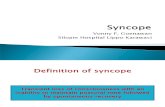
how any impairment of AV conduction in 14 patients; in 1 ofhese, mild sinus dysfunction was detected. The medianaseline APL of these patients was significantly lower than thatound in the age- and sex-matched population of 81 healthyubjects: 0.33 �M (IQR: 0.20 to 0.56 �M) versus 0.49 �M
(IQR: 0.38 to 0.68l �M, p � 0.017). The median APL valuef the patients was also 4-fold lower than that found in 9ontrol patients with syncope due to reflex sinus arrest (1.2 �MIQR: 1.0 to 1.7 �M]; p � 0.001) (Fig. 4). In 15 (83%)atients with paroxysmal AV block, the rapid intravenousnjection of 18 mg adenosine or 20 mg ATP caused completeV block similar to the spontaneous AV block and a meanaximum pause of 10 � 6 s (Table 1, Fig. 3B). Finally,
tilt-table testing induced a vasovagal syncope in 7 (41%) ofcases, but never reproduced AV block, and carotid sinusmassage was negative in all patients in whom it was performed.
Discussion
The common clinical and electrophysiological features ofthese patients define a distinct form of syncope character-
ContinuedTable 1 Continued
APL(�M)
ATP Test: AVB(Max Pause, s) EPS
Tilt TableTesting
0.91 Yes (7.5) Normal DOH
0.45 Sinus arrest Mild SND Mixed
0.20 Yes (8.0) Normal Mixed
0.28 Yes (3.3) Normal Mixed
0.89 Yes (11.0) Normal Negative
0.40 Yes (8.6) Not done Negative
0.20 Yes (7.6) Normal Negative
0.29 Yes (8.0) * Not done
0.36 Yes (4.0) Not done Mixed
0.70 Yes (5.0) Not done Negative
0.38 Yes (10.0) Normal Negative
0.12 Yes (9.3) Normal Mixed
0.11 Negative Normal Negative
0.11 Yes (13.7) Normal Negative
0.89 Yes (8.0) Normal Negative
0.74 Yes (18.0) Not done Sinus arrest
0.34 Negative Normal Negative
0.12 Yes (25.0) Normal Sinus arrest
*Patient #8 had advanced-degree atrioventricular block (AVB) that persisted for 2 days, then first
time of the block showed impaired AV nodal conduction.APL � adenosine plasma level; ATP � adenosine triphosphate; DOH � delayed orthostatic hypotension;
ized by a long history of recurrent syncope due to idiopathicparoxysmal AV block with long pauses, absence of cardiacand ECG abnormalities, absence of progression to persis-tent forms of AV block, and efficacy of cardiac pacingtherapy. These patients have low baseline APL values andshow an increased susceptibility to exogenous adenosine.
Similar ECG features have been occasionally described inindividual patients in clinical studies (9,11,12) and in a fewcase reports (13–16); no follow-up is reported.
In our patients, the paroxysmal AV block had differentclinical and electrophysiological features from those of the 2other known types of paroxysmal AV block: intrinsic AVblock due to AV conduction disease and extrinsic vagal AVblock.
Intrinsic AV block due to AV conduction disease wasunlikely in our population. The absence of any evidence ofcardiac abnormalities, the young age of several of thesepatients, and the outcome showing no progression of theblock toward permanent forms for several years argueagainst an intrinsic cardiac etiology. Furthermore, the AVblock was never initiated by atrial, His, or ventricularpremature extrasystole, increased heart rate (tachy-dependent AV block), or decreased heart rate (brady-dependent AV block), all features that support a diagnosisof intrinsic AV block (1,2).
The clinical features of our patients were also differentfrom those of a typical population of patients affected byvasovagal syncope. Specifically, historical findings of auto-nomic activation, triggering, and predisposing factors thatcould suggest a diagnosis of reflex syncope were encounteredonly in 3 of our patients, whereas the etiology remained
Carotid SinusMassage
PMTherapy
Follow-UpDuration
(yrs) Symptoms
Not done Yes 4.4 No
Not done Yes 4.0 No
Negative Yes 8.0 No
Negative Yes 1.7 No
Negative Yes 14.0 No
Negative Yes 10.0 No
Negative Yes 2.0 No
Not done No 1.7 No
Negative Yes 1.0 No
Negative Yes 5.0 No
Negative Yes 0.8 No
Negative Yes 2.0 No
Negative Yes 5.6 No
Negative Yes 2.3 No
Negative Yes 10.7 No
Negative Yes 1.1 No
Not done Yes 1.3 No
Negative Yes 0.6 No
AVB for few days, then normal conduction. An electrophysiological study (EPS) performed at the
-degreeILR � implantable loop recorder; Max � maximum; PM � pacemaker; SND � sinus node disease.

170 Brignole et al. JACC Vol. 58, No. 2, 2011Idiopathic Paroxysmal AV Block July 5, 2011:167–73
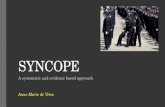
Figure 1 Case #14
(A, B) Holter recording of 2 episodes of spontaneous syncope that occurred a few minutes apart. The 2 episodes were very similar and were characterized by sudden-onset complete atrioventricular (AV) block without changes in P-P cycle length, which constantly remained 720 ms and long ventricular asystole of 7 and 11 s(top and bottom, compressed traces, respectively).
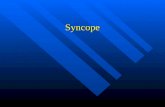
Figure 2 Case #10
The 4 strips are continuous and show a spontaneous syncope recorded by implantable loop recorder. Initial minimal sinus slowing (P-P cycle increased by 80 ms) wasfollowed by 2:1 atrioventricular (AV) block and finally complete AV block with a very long asystolic pause. During AV block, the P-P cycle progressively shortened, indicat-ing a compensatory reflex sympathetic activation.

171JACC Vol. 58, No. 2, 2011 Brignole et al.July 5, 2011:167–73 Idiopathic Paroxysmal AV Block
unexplained in the others. Also, the electrophysiologicalfeatures of our patients were against a vagally mediated AVblock. Indeed, a classic vagal effect on the conduction systemincludes gradual slowing of the sinus rate (P-P interval) andAV conduction (prolonging PR), which are occasionallyfollowed by sinus arrest or complete AV block. The 2conditions frequently coexist, indicating a simultaneousvagal action on sinus node and AV node. Even when a moreprominent AV response occurs, vagally mediated AV blockis usually preceded by significant PR prolongation orWenckebach; the P-P interval is prolonged markedly alsoduring asystole, and there is significant PR prolongation onresumption of AV conduction (1,4,5,17). These featureswere absent in our patients, who were affected by abrupt-onset AV block without significant rhythm disturbancesbefore or during the attack (type 1C block).
Paroxysmal type 1C AV block is very rare during tilt-induced vasovagal syncope. Apart from 2 case reports(14,18), AV block with a constant P-P cycle has never beenobserved in large series of tilt-table tests (17,19). In thepresent study, tilt-table testing, which induced a vasovagalsyncope in 7 cases, never reproduced AV block. Carotid
Figure 3 Case #7
(A) The 2 strips are continuous and show a spontaneous syncope recorded by imblock, followed by complete AV block without changes in P-P cycle length. (B) Adeadenosine, complete AV block with constant P-P cycle and ventricular asystole of 7
sinus massage was invariably negative. In addition, low APL
values clearly differentiated our patients from patients withdocumented spontaneous reflex sinus arrest, who had amedian APL value 4 times higher than patients with AVblock (Fig. 4). High APL values seem to characterizevasovagal syncope as they were also found in 3 studies
ble loop recorder. The episode was characterized by 2:1 atrioventricular (AV)test. A few seconds after rapid intravenous (i.v.) injection of a bolus of 18 mgas induced.
Figure 4 Individual APL in Patients and Controls
The individual values of adenosine plasma level (APL) in patients andcontrols are plotted. The median APL value of each group is also shown.AV � atrioventricular.
plantanosine.6 s w

mnn
(eisph(gimumStfltis
sitbpwt
C
Imsiacodhfrtcpme
Tpddtswp
ittpscmpcasdAsp
172 Brignole et al. JACC Vol. 58, No. 2, 2011Idiopathic Paroxysmal AV Block July 5, 2011:167–73
involving patients with a diagnosis of vasovagal syncopeconfirmed by positive tilt-table testing (J.C. Deharo et al.,personal communication, 2011) (6,7). Thus, a differentplasmatic adenosine background seem to be present inpatients with idiopathic AV block and in patients withvasovagal syncope. Finally, permanent cardiac pacing wascompletely successful in preventing syncopal recurrencesduring long-term follow-up. This suggests that paroxysmalAV block was the main determinant of syncope in ourpatients. Conversely, cardiac pacing has been reported to beless efficacious in patients affected by reflex cardioinhibitorysyncope, even if a spontaneous asystolic reflex has beendocumented, with syncope recurring in 9% to 45% ofpatients (3,4). The cause of persistence of syncopal recur-rence in reflex syncope is attributed to the coexistence of avasodepressor reflex, which, to some degree, is present invirtually all patients.Pathophysiological observations. We found that our pa-tients had a low baseline APL value (compared with controlsubjects and with patients with reflex asystolic syncope) anda rate of positive ATP test much higher than that found inthe literature in normal control subjects (9) and in patientswith unexplained syncope (9–12,20), indicating an in-creased susceptibility of the AV node to adenosine. Theseobservations may lead to hypothesize some relationshipbetween the adenosine pathway and the genesis of the AVblock.
The effect of adenosine on the AV node is mainly due tothe stimulation of high-affinity A1 receptors, which are
uch more numerous in the AV node than in the sinoatrialode (21–23). Like many other cell surface receptors, theumber of cardiac adenosine A1 receptors undergoes up-
regulation and down-regulation when cardiac tissues arechronically exposed to low or elevated concentrations ofadenosine receptor agonist (i.e., adenosine), respectively. Atransient release of endogenous adenosine could be sufficientto block conduction in the AV node when a high number offree high-affinity A1 receptors in the AV node are availablelow-APL patients). The cause of the transient release ofndogenous adenosine responsible for paroxysmal AV blockn our patients is unknown. Adenosine is a ubiquitousubstance, which is released under several physiological andathological conditions (e.g., in the case of myocardialypoxia or during reflex beta-adrenergic stimulation)24,25). Even if a role of the adenosine pathway in theenesis of the AV block may be possible, these data arensufficient to prove a causal relationship. Therefore, the
echanism of the block in our patients remains largelynexplained (idiopathic AV block). The above observationsight be of interest for the planning of future studies.
tudy limitations. Three patients had historical featureshat suggest the activation of vasovagal or situational re-exes. Seven patients had a vasovagal response duringilt-table testing. Apart these features, these patients werendistinguishable from the others. The absence of sinus
lowing along with AV block does not definitely rule outome role of exogenous hypervagotonia in causing the blockn these patients. Probably are the very different APL valueshat differentiate better the patients with idiopathic AVlock from patients with typical vasovagal syncope. In someatients, the follow-up period after pacemaker implantationas too short to allow evaluating the efficacy of pacing
herapy in preventing symptomatic recurrences.
onclusions
n clinical practice, paroxysmal AV block without or withinimal changes in the P-P cycle, as was observed in our
tudy patients, is usually regarded as a manifestation of anntrinsic disease of the AV conduction system, and inccordance with current guidelines (26), a diagnosis ofardiac syncope (primary arrhythmia) is made. Conversely,n the basis of their clinical features and the absence of anyetectable cardiac abnormality, our patients would probablyave been categorized as possibly affected by an atypicalorm of neurally mediated syncope if they had not had theather fortuitous documentation of paroxysmal AV block athe time of syncope (26). Therefore, 2 opposite diagnosesould be made in the same patients, depending on whetheraroxysmal AV block during a spontaneous attack is docu-ented on ECG. We were able to give an alternative
xplanation.How frequent is syncope due to idiopathic AV block?
ype 1C block was found to be present in 8% of syncopeatients with normal ECG and absence of structural heartisease (corresponding to 15% of those who had ECGocumentation of syncope) (11). We can only speculate thathese figures may represent the prevalence of this newyndrome among patients without structural heart diseaseho are affected by unexplained syncope. However, arospective study is needed to confirm this hypothesis.Given that ECG documentation of idiopathic AV block
s the gold standard for diagnosis, is there some other testhat could anticipate diagnosis? The adenosine test appearedo be sensitive enough to identify the patients with idio-athic AV block in this study, but it showed a very lowpecificity in other studies in which there was a lack oforrelation between the responses to the test and theechanism of spontaneous syncope documented by im-
lantable loop recorder (11,12). There is not a clear-cututoff of APL value between idiopathic AV block patientsnd normal control subjects. In patients with unexplainedyncope, normal ECG, and absence of structural heartisease, low-to-normal APL values suggest an idiopathicV block whereas high APL values suggest a typical reflex
yncope. That is probably likely for patients (30% of ouropulation) who have an APL value �0.24 �M, which is
the fifth lower percentile in normal healthy subjects. How-ever, the specificity of APL value in identifying idiopathic
AV block is unknown and a matter of future studies.
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
173JACC Vol. 58, No. 2, 2011 Brignole et al.July 5, 2011:167–73 Idiopathic Paroxysmal AV Block
Reprint requests and correspondence: Dr. Michele Brignole,Arrhythmologic Center, Department of Cardiology, Ospedali delTigullio, Via Don Bobbio 25, 16033 Lavagna, Italy. E-mail:[email protected].
REFERENCES
1. Lee S, Wellens JJ, Josephson M. Paroxysmal atrioventricular block.Heart Rhythm 2009;6:1229–34.
2. El-Sherif N, Jalife J. Paroxysmal atrioventricular block: are phase 3 andphase 4 block mechanisms or misnomers? Heart Rhythm 2009;6:1514–21.
3. Brignole M, Sutton R, Menozzi C, et al. Early application of animplantable loop recorder allows effective specific therapy in patientswith recurrent suspected neurally mediated syncope. Eur Heart J2006;27:1085–92.
4. Sud S, Klein G, Skanes A, Gula L, Yee R, Krahn A. Implications ofmechanism of bradycardia on response to pacing in patients withunexplained syncope. Europace 2007;9:312–8.
5. Brignole M, Moya A, Menozzi C, Garcia-Civera R, Sutton R.Proposed electrocardiographic classification of spontaneous syncopedocumented by an implantable loop recorder. Europace 2005;7:14–8.
6. Saadjian A, Lévy S, Franceschi F, Zouher I, Paganelli F, Guieu RP.Role of endogenous adenosine as a modulator of syncope inducedduring tilt testing. Circulation 2002;106:569–74.
7. Carrega L, Saadjian AY, Mercier L, et al. Increased expression ofadenosine A2A receptors in patients with spontaneous and head-up-tilt-induced syncope. Heart Rhythm 2007;4:870–6.
8. Saadjian AY, Gerolami V, Giorgi R, et al. Head-up tilt inducedsyncope and adenosine A2A receptor gene polymorphism. Eur Heart J2009;30:1510–5.
9. Brignole M, Gaggioli G, Menozzi C, et al. Adenosine-inducedatrioventricular block in patients with unexplained syncope: the diag-nostic value of ATP testing. Circulation 1997;96:3921–7.
0. Flammang D, Erickson M, McCarville S, Church T, Hamani D,Donal E. Contribution of head-up tilt test and ATP testing inassessing the mechanisms of vasovagal syndrome: preliminary resultsand potential therapeutic implications. Circulation 1999;99:2427–33.
1. Brignole M, Sutton R, Menozzi C, et al. Lack of correlation betweenthe responses to tilt testing and adenosine triphosphate test and themechanism of spontaneous neurally mediated syncope. Eur Heart J2006;27:2232–9.
2. Deharo JC, Jego C, Lanteaume A, Djiane P. An implantable loop
recorder study of highly symptomatic vasovagal patients. J Am CollCardiol 2006;47:587–93.3. Strasberg B, Lam W, Swiryn S, et al. Symptomatic spontaneousparoxysmal AV nodal block due to localized hyperresponsiveness ofthe AV node to vagotonic reflexes. Am Heart J 1982;103:795–801.
4. Sra JS, Singh B, Blanck Z, Dhala A, Akhtar M. Sinus tachycardia withatrioventricular block: an unusual presentation during neurocardio-genic (vasovagal) syncope. J Cardiovasc Electrophysiol 1998;9:203–7.
5. Mendoza IJ, Castellanos A, Lopera G, Moleiro F, Mitrani RD,Myerburg RJ. Spontaneous paroxysmal atrioventricular block in pa-tients with positive tilt tests and negative electrophysiologic studies.Am J Cardiol 2000;85:893–6.
6. Sanjuan R, Facila L, Blasco ML, Garcıa-Civera R, Ruiz Granell R,Morell Cabedo S. Case 13. Neuromediated syncope presenting as highgrade AV block. In: Garcia-Civera R, Baron-Esquivias G, Blanc JJ, etal., editors. Syncope Cases. Oxford: Blackwell Futura, 2006:38–40.
7. Zysko D, Gajek J, Koúluk E, Mazurek W. Electrocardiographiccharacteristics of atrioventricular block induced by tilt testing. Euro-pace 2009;11:225–30.
8. Paravolidakis KE, Apostolou TS, Theodorakis G, Vartela VG, Kre-mastinos D. Accelerated sinus rhythm with high grade A-V blockduring head-up tilt testing. Europace 2006;8:128.
9. Brignole M, Gaggioli G, Menozzi C, et al. Clinical features ofadenosine sensitive syncope and tilt induced vasovagal syncope. Heart2000;83:24–8.
0. Perennes A, Fatemi M, Borel ML, Lebras Y, L’Her C, Blanc JJ.Epidemiology, clinical features, and follow-up of patients with syncopeand a positive adenosine triphosphate test result. J Am Coll Cardiol2006;47:594–7.
1. Burnstock G, Kennedy C. Purinergic receptors in the cardiovascularsystem. Prog Pharmacol 1986;6:111–32.
2. Shryock JC, Belardinelli L. Adenosine and adenosine receptors in thecardiovascular system: biochemistry, physiology and pharmacology.Am J Cardiol 1997;79:2–10.
3. Wu L, Belardinelli L, Zablocki JA, Palle V, Shryock JC. A partialagonist of the A(1)-adenosine receptor selectively slows AV conduc-tion in guinea pig hearts. Am J Physiol Heart Circ Physiol 2001;280:334–43.
4. Lerman B, Belardinelli L. Cardiac electrophysiology of adenosine.Basic and clinical concepts. Circulation 1991;83:1499–507.
5. Clemo H, Belardinelli L. Effect of adenosine on atrioventricularconduction. I: site and characterization of adenosine action in theguinea pig atrioventricular node. Circ Res 1986;59:427–36.
6. Moya A, Sutton R, Ammirati F, et al. Guidelines for the diagnosis andmanagement of syncope (version 2009). Eur Heart J 2009;30:2631–71.
Key Words: adenosine y AV block y ECG monitoring y
electrocardiography y syncope.