Sympathovagal imbalance in transsexual subjects
6
1014 J. Endocrinol. Invest. 31: 1014-1019, 2008 ABSTRACT. Context: Autonomic nervous system imbalance is related to cardiovascular risk. Heart rate variability (HRV) in- dexes are associated with age, race, and sex, but the role of sex hormones is still unknown. Objective: To evaluate sym- pathovagal balance (SB) in transsexuals. Patients: Eighteen transsexual subjects, 12 male-to-female (group 1) and 6 fe- male-to-male (group 2), compared with 34 age-matched con- trols: 17 males (group 3) and 17 females (group 4). Auto- nomic testing of SB was performed by Power Spectral Anal- ysis (PSA) of HRV in clinostatism (c) and orthostatism (o). PSA identifies power peaks: high frequency (HF) expresses vagal activity, while low frequency (LF) expresses sympathetic ac- tivity. Results: Group 1 showed lower LFc than groups 2, 3, and 4 (p<0.001, p=0.05, p<0.001, respectively), and lower LFo than groups 3 and 4 (p=0.01); HFc was lower than in groups 2, 3, and 4 (p=0.02, p=0.02, p<0.001, respectively), and HFo was lower than in groups 3 and 4 (p<0.001). LFo/HFo ratio was higher in group 1 than in group 4 (p<0.001). No differences emerged between groups 2 and 3. Group 2 showed lower HFo than group 4 (p=0.03), and a higher LFo/HFo ratio (p=0.01). Group 3 showed lower HFo and HFc than group 4 (p=0.02, p=0.05, respectively), and a higher LFo/HFo ratio (p=0.03). Conclusion: In this study we found a sympathovagal imbalance due to a reduced sympa- thetic and parasympathetic influence on heart rate. Sex hor- mone therapy per se may play a role in this imbalance, and HRV measurement could be useful in detecting cardiovascu- lar risk in transsexuals. (J. Endocrinol. Invest. 31: 1014-1019, 2008) © 2008, Editrice Kurtis INTRODUCTION A significant relationship has been reported between au- tonomic nervous system imbalance and cardiovascular mortality (1, 2). Electrocardiographic RR intervals fluctuate cyclically, modulated by ventilation, baroreflexes, and other ge- netic and environmental factors that are mediated through the autonomic nervous system (3). The evalua- tion of RR intervals from Holter recordings yields a use- ful index of global heart rate variability (HRV) (4). Of the different methods of measuring HRV, spectral analysis has the greatest ability to differentiate between vagal and sympathetic modulation of the heart rate (5). HRV constitutes a quantitative marker of autonomic ac- tivity (6) and is also a useful, well-recognized tool in the diagnosis of cardiovascular pathologies (7). Long-term, 24-h recording can usually be used to assess autonom- ic nervous responses during normal daily activities in conditions of health or disease. Short-term electrogar- diogram (ECG) recordings (5-15 min) made under con- trolled conditions (lying supine or standing or tilted up- right) can elucidate physiological, pharmacological or pathological changes in autonomic nervous system function. Sympathovagal imbalance is a common finding in dia- betes, and the utility of standard cardiovascular tests in diagnosing cardiac autonomic neuropathy in diabetes has been well documented (8-10). The early subclinical detection of autonomic dysfunction is therefore impor- tant for risk stratification and subsequent management (7). Moreover, we have recently demonstrated that sym- pathovagal imbalance is a new cardiovascular risk factor in acromegaly (11). HRV spectral indices are associated with age, race, and sex. While in HRV parameters differences between the sexes are reported, with females displaying a lower sym- pathetic activity and a higher vagal activity than males, the role of sex hormones in this difference is still unknown (12-14). These gender-related autonomic differences dis- appear in elderly subjects. It has been shown that estrogen replacement therapy may facilitate vagal and attenuate sympathetic regula- tion of heart rate in post-menopausal women (15). More- over, estrogens may directly modulate ventricular repo- larization (16). In addition, they may play an important role in gender-related autonomic differences (17). A number of cardiovascular diseases, such as myocardial infarction, hypertension, and heart failure are associated with alterations in the autonomic nervous system, with an increase in sympathetic activity and a consequent worsening in prognosis (18, 19). The cardiac vagotonic and sympatholytic effects of es- trogen may explain, at least in part, why pre-menopausal women have a lower incidence of coronary heart disease (CHD) and mortality than post-menopausal women (19). More recent data, however, have shown that estrogen therapy is actually associated with an increased risk of cardiovascular events (20). No data are available on the sympathovagal balance in transsexuals. Cardiovascular risk in transsexual subjects is not clearly understood. Though no clear data are avail- able, these subjects could have a thrombotic risk factor, changed body composition (21) etc, that can explain the cardiovascular risk due to the metabolic balance. HRV evaluation is a well-recognized method of evaluating car- Key-words: Heart rate variability, sympathovagal balance, transsexual subjects. Correspondence: E. Resmini, MD, Department of Endocrinology and Metabolism University of Genoa, Viale Benedetto XV, 6, 16132 – Genova, Italia. E-mail: [email protected] Accepted March 21, 2008. Sympathovagal imbalance in transsexual subjects E. Resmini 1 , M. Casu 2 , V. Patrone 2 , A. Rebora 1 , G. Murialdo 2 , F. Minuto 1 , and D. Ferone 1 1 Department of Endocrinology and Medical Sciences and Center of Excellence for Biomedical Research; 2 Division of Internal Medicine, San Martino University Hospital, Genoa, Italy
Transcript of Sympathovagal imbalance in transsexual subjects

1014
J. Endocrinol. Invest. 31: 1014-1019, 2008
ABSTRACT. Context: Autonomic nervous system imbalance isrelated to cardiovascular risk. Heart rate variability (HRV) in-dexes are associated with age, race, and sex, but the role ofsex hormones is still unknown. Objective: To evaluate sym-pathovagal balance (SB) in transsexuals. Patients: Eighteentranssexual subjects, 12 male-to-female (group 1) and 6 fe-male-to-male (group 2), compared with 34 age-matched con-trols: 17 males (group 3) and 17 females (group 4). Auto-nomic testing of SB was performed by Power Spectral Anal-ysis (PSA) of HRV in clinostatism (c) and orthostatism (o). PSAidentifies power peaks: high frequency (HF) expresses vagalactivity, while low frequency (LF) expresses sympathetic ac-tivity. Results: Group 1 showed lower LFc than groups 2, 3,and 4 (p<0.001, p=0.05, p<0.001, respectively), and lowerLFo than groups 3 and 4 (p=0.01); HFc was lower than in
groups 2, 3, and 4 (p=0.02, p=0.02, p<0.001, respectively),and HFo was lower than in groups 3 and 4 (p<0.001).LFo/HFo ratio was higher in group 1 than in group 4(p<0.001). No differences emerged between groups 2 and 3.Group 2 showed lower HFo than group 4 (p=0.03), and ahigher LFo/HFo ratio (p=0.01). Group 3 showed lower HFoand HFc than group 4 (p=0.02, p=0.05, respectively), and ahigher LFo/HFo ratio (p=0.03). Conclusion: In this study wefound a sympathovagal imbalance due to a reduced sympa-thetic and parasympathetic influence on heart rate. Sex hor-mone therapy per se may play a role in this imbalance, andHRV measurement could be useful in detecting cardiovascu-lar risk in transsexuals.(J. Endocrinol. Invest. 31: 1014-1019, 2008)©2008, Editrice Kurtis
INTRODUCTION
A significant relationship has been reported between au-tonomic nervous system imbalance and cardiovascularmortality (1, 2).Electrocardiographic RR intervals fluctuate cyclically,modulated by ventilation, baroreflexes, and other ge-netic and environmental factors that are mediatedthrough the autonomic nervous system (3). The evalua-tion of RR intervals from Holter recordings yields a use-ful index of global heart rate variability (HRV) (4). Of thedifferent methods of measuring HRV, spectral analysishas the greatest ability to differentiate between vagaland sympathetic modulation of the heart rate (5).HRV constitutes a quantitative marker of autonomic ac-tivity (6) and is also a useful, well-recognized tool in thediagnosis of cardiovascular pathologies (7). Long-term,24-h recording can usually be used to assess autonom-ic nervous responses during normal daily activities inconditions of health or disease. Short-term electrogar-diogram (ECG) recordings (5-15 min) made under con-trolled conditions (lying supine or standing or tilted up-right) can elucidate physiological, pharmacological orpathological changes in autonomic nervous systemfunction.Sympathovagal imbalance is a common finding in dia-betes, and the utility of standard cardiovascular tests indiagnosing cardiac autonomic neuropathy in diabeteshas been well documented (8-10). The early subclinicaldetection of autonomic dysfunction is therefore impor-
tant for risk stratification and subsequent management(7). Moreover, we have recently demonstrated that sym-pathovagal imbalance is a new cardiovascular risk factorin acromegaly (11).HRV spectral indices are associated with age, race, andsex. While in HRV parameters differences between thesexes are reported, with females displaying a lower sym-pathetic activity and a higher vagal activity than males,the role of sex hormones in this difference is still unknown(12-14). These gender-related autonomic differences dis-appear in elderly subjects.It has been shown that estrogen replacement therapymay facilitate vagal and attenuate sympathetic regula-tion of heart rate in post-menopausal women (15). More-over, estrogens may directly modulate ventricular repo-larization (16). In addition, they may play an importantrole in gender-related autonomic differences (17).A number of cardiovascular diseases, such as myocardialinfarction, hypertension, and heart failure are associatedwith alterations in the autonomic nervous system, withan increase in sympathetic activity and a consequentworsening in prognosis (18, 19).The cardiac vagotonic and sympatholytic effects of es-trogen may explain, at least in part, why pre-menopausalwomen have a lower incidence of coronary heart disease(CHD) and mortality than post-menopausal women (19).More recent data, however, have shown that estrogentherapy is actually associated with an increased risk ofcardiovascular events (20).No data are available on the sympathovagal balance intranssexuals. Cardiovascular risk in transsexual subjectsis not clearly understood. Though no clear data are avail-able, these subjects could have a thrombotic risk factor,changed body composition (21) etc, that can explain thecardiovascular risk due to the metabolic balance. HRVevaluation is a well-recognized method of evaluating car-
Key-words: Heart rate variability, sympathovagal balance, transsexual subjects.
Correspondence: E. Resmini, MD, Department of Endocrinology and MetabolismUniversity of Genoa, Viale Benedetto XV, 6, 16132 – Genova, Italia.
E-mail: [email protected]
Accepted March 21, 2008.
Sympathovagal imbalance in transsexual subjectsE. Resmini1, M. Casu2, V. Patrone2, A. Rebora1, G. Murialdo2, F. Minuto1, and D. Ferone1
1Department of Endocrinology and Medical Sciences and Center of Excellence for Biomedical Research;2Division of Internal Medicine, San Martino University Hospital, Genoa, Italy

Sympathovagal imbalance in transsexuals
1015
diovascular risk due to autonomic balance and we be-lieve that it could also be useful in evaluating this risk intranssexual subjects.The aim of the present study was to evaluate the sym-pathovagal balance in transsexuals by means of powerspectral analysis of HRV, by comparison with both maleand female subjects. We hypothesize that sympathovagalimbalance may also be a cardiovascular risk factor intranssexual subjects.
MATERIALS AND METHODSPatients and protocolWe studied the sympathovagal balance (SB) in 18 non-diabetictranssexual subjects, without dyslipidemia, with normal bodymass index: 12 male-to-female (M-to-F) (mean age 36.58±14.99yr) and 6 female-to-male (F-to-M) (mean age 32.17±6.24 yr).Thirty-four age-matched subjects, 17 males (mean age36.18±14.77 yr) and 17 females (mean age 34.59±8.21 yr)served as controls. We compared each group of transsexualswith both male and female controls: each group of transsexu-als was, therefore, compared with two control groups (malesand females). The duration of sex hormone therapy was6.00±5.41 yr for M-to-F and 3.83±2.85 yr for F-to-M.The subjects were divided into 4 groups: group 1=M-to-F, group2=F-to-M, group 3=males, group 4=females.All the transsexuals and controls had normal blood pressure andnormal ECG. The controls were not taking any hormonal or non-hormonal treatment.The hormonal profiles of patients and controls are shown inTable 1. The protocol was approved by the local Ethics Com-mittee, and written informed consent was obtained from thetranssexuals and controls.Two M-to-F previously underwent surgery for sex reassignmentand are now in therapy with estradiol (E2); 10 M-to-F were treat-ed with antiandrogen (9 with cyproterone acetate, 100 mg/dayand 1 with spironolactone, 200 mg/day) and estrogen (E2 hemi-hydrate in gel or oral tablets, 4 mg/day). Regarding concomi-tant treatments, 2 were in therapy with levo-T4 (LT4) for nodulargoiter.One F-to-M had previously undergone surgery for sex reas-signment and all were in therapy with depot testosterone (250mg im every 21 days). Regarding concomitant treatments, onlyone was taking LT4 for nodular goiter.
HRV analysisAutonomic tests were performed by means of power spectralanalysis of HRV in clinostatism (c) and orthostatism (o), using afrequency domain method. HRV is a measure of autonomic ner-vous system balance. An electrocardiographic recording of R-Rintervals was made at 10:00 h in a quiet room reserved for thispurpose, at least 1 h after venopuncture for routine hormonalevaluation. Subjects were placed supine on a mechanically driv-en tilt-table and instructed to relax, stay awake, breathe regular-ly, and not to speak. After supine resting for about 10 min to sta-bilize blood pressure and heart rate, clinostatic R-R intervals wereacquired. Immediately thereafter, the patient was passivelybrought into the upright position by raising the table over a 30-sec period, and the recording was repeated. For both clinostat-ic and orthostatic postures, the ECG was consecutively recordedfor 330 sec by means of an electrocardiograph connected to a PCequipped with software which sampled the analogical signal atabout 200 Hz using an analogical/digital converter. Each R-R in-terval was measured in milliseconds and memorized as atachogram (R-R interval duration vs no. of heartbeats). Two seriesof data, corresponding to clinostatic (tachogram A) and ortho-static (tachogram B) R-R intervals, were analyzed in all subjectsby means of a parametric method based on the autoregressivemodel for the quantification of HRV signals.The main power densities in the high-frequency (HF) (0.15-0.4 Hz)and low-frequency (LF) (0.04-0.15 Hz) bands were identified foreach density spectrum. In addition, LF/HF ratios were calculated inboth clinostatism and orthostatism. An LF/HF greater than 1 is ev-idence of a normal SB. Power spectral analysis identifies 3 peaks ofpower: a peak of HF, which expresses vagal activity; a peak of LF,which expresses sympathetic activity; and a peak of very LF, whichis of uncertain significance. LF and HF are quantitative indicators ofneural control of the sinoatrial node; in particular, the LF compo-nent is a marker of sympathetic modulation, whereas the HF com-ponent is a marker of vagal modulation. LF/HF is regarded as anindex of sympathovagal balance in the frequency domain (22, 23).All HRV parameters were measured in milliseconds squared.
Statistical analysisMann-Whitney U test for unpaired data was used for data com-parison between transsexuals and controls. Comparison withingroups was made by the non-parametric Wilcoxon test, usingSPSS program v.11.00. Graphics were elaborated by theSigmaplot 9.0 program (Systat Software, Inc., Richmond, CA).
M-to-F F-to-M Males Females(no.12) (no.6) (no.17) (no.17)
BMI (kg/cm2) (mean±SD) 21.4±2.41 21.45±2.20 20.21±1.99 21.06±2.50
Age (mean±SD) 36.58±14.99 32.17±6.24 36.18±14.77 34.59±8.21
LH (UI/l) 0.19 2.6 4.20 5.20median (25th-75th percentile) (0.10-0.66) (1.56-6.12) (2.15-5.50) (3.20-6.80)
FSH (UI/l) 0.74 6.02 5.80 6.95median (25th-75th percentile) (0.10-6.6) (3.02-10.4) (4.5-7.40) (4.25-7.90)
Estradiol (pg/ml) 74.30 29.25 18.05 68.50median (25th-75th percentile) (27-83) (22.40-37.40) (15.05-25.40) (50.45-78)
Total testosterone (ng/ml) 0.50 3.30 5.40 0.50median (25th-75th percentile) (0.3-2) (1.5-5.9) (1.20-7.80) (0.2-0.80)
Normal ranges: LH 0.6-16 UI/l; FSH 1.5-13 UI/l (follicular phase); total testosterone 0.2-0.8 ng/ml for females and 3.5-10 ng/ml for males; estradiol 20-80 pg/ml for females and <50 pg/ml for males. M: male; F: female; BMI: body mass index.
Table 1 - Clinical and hormonal parameters in transsexual and control subjects.

E. Resmini, M. Casu, V. Patrone, et al.
1016
RESULTS
The HRV variables are expressed as median (25th-75th
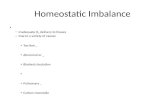
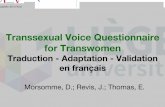
percentile).Group 1 showed significantly lower LFc [474.66 (301.54-819.56)] than groups 2 [1185.52 (881.78-1837.73)], 3[1292.62 (1139.45-1723.49)], and 4 [1630.98 (1397.98-2019.30)], (p<0.001, p=0.05, p<0.001, respectively) andsignificantly lower LFo [951.18 (543.82-1091.31)] thangroups 3 [1452.34 (993.38-1638.30)], p=0.01 and 4[1394.92 (1146.93-1487.91)], p=0.01. HFc in group 1[211.68 (125.54-363.47)] was significantly lower than ingroups 2 [514.83 (421.46-563.80)], 3 [437.72 (276.45-714.17)], and 4 [819.36 (536.82-1073.64)] with p=0.02,p=0.02, and p<0.001, respectively. HFo in group 1 [94.11(50.53-217.13)] was lower than in group 2 [265.60(186.10-318.89)], p=0.06, and significantly lower than ingroups 3 [309.83 (191.43-464.90)], p<0.001 and 4 [578.32(340.18-714.39)], p<0.001. LFo/HFo ratio in group 1 wassignificantly higher [7.79 (6.00-10.75)] than in group 4[2.61 (2.09-4.55)], p<0.001. There were no statisticallysignificant differences between groups 2 and 3.Group 2 showed significantly lower HFo [265.60 (186.10-
318.89)] than group 4 [578.32 (340.18-714.39)], p=0.03,and a significantly higher LFo/HFo ratio [5.86 (5.06-7.59)]than group 4 [2.61 (2.09-4.55)], p=0.01.Group 3 showed significantly lower HFo [309.83 (191.43-464.90)] than group 4 [578.32 (340.18-714.39)], p=0.02.HFc [437.72 (276.45-714.17)] was significantly lower thanin group 4 [819.36 (536.82-1073.64)], p=0.05. TheLFo/HFo ratio [6.91 (2062-8.28)] was significantly higherthan in group 4 [2.61 (2.09-4.55)], p=0.03.These results are summarized graphically in Figures 1 and 2.Statistical analysis within the groups was done to showthe trend in autonomic parameters on passing from cli-nostatism to orthostatism. In group 1, LFc was signifi-cantly lower than LFo (p=0.01) and HFc was significantlyhigher than HFo (p=0.003). In group 2 there were no dif-ferences between LFc and LFo, while HFc was signifi-cantly higher than HFo (p=0.004).
DISCUSSION
The relationship between HRV and CHD has recentlybeen explored following the development of HRV tech-
LFC
3000
2000
1000
Group
AH
FC3000
2000
1000
0
-1000No. 12 6 17 17
1 2 3 4Group
BH
FO
1400
1200
1000
800
600
400
200
0
-200No. 12 6 17 17
1 2 3 4Group
D
LFO
5000
4000
3000
2000
1000
0
-1000No. 12 6 17 17
1 2 3 4Group
C
No. 12 6 17 171 2 3 4
Fig. 1 - Box-and-whisker plot of heart rate variability parameters in the four groups enrolled in this study. Group 1: M-to-F; Group 2: F-to-M; Group 3: males; Group 4: females; C: clinostatism; O: orthostatism. A) LFC: sympathetic activity in clinostatism; B) HFC: vagal ac-tivity in clinostatism; C) LFO: sympathetic activity in orthostatism; D) HFO: vagal activity in orthostatism. ***p<0.001, **p<0.05, *p=0.05.

Sympathovagal imbalance in transsexuals
1017
niques. A consensus has emerged that diminishedparasympathetic and/or increased sympathetic controlof heart rate contributes to increasing the risk of cardio-vascular events.Lower HRV has been demonstrated to be associated witha greater risk of developing hypertension among nor-motensive men (24). Moreover, lower HRV has beenfound to be related to sudden cardiac death (1, 2). Acutemyocardial infarction is associated with decreased HRV,which is due to reduced vagal or increased sympatheticoutflow to the heart (25). It has thus been proposed thatHRV be used as a prognostic factor for myocardial in-farction risk stratification and management (17). Resultsfrom population-based follow-up studies also suggestthat lower HRV is associated with the risk of developingCHD (26).It is known that HRV indexes are associated with age,race, and sex, with a predominance of sympathetic con-trol in men and a dominant parasympathetic influenceon heart rate regulation in women, and that these gen-der-related autonomic differences disappear in the el-derly. However, the role of sex hormones in this differ-ence is as yet unknown (12-14).Sex-related differences in the neurohumoral control ofthe cardiovascular system have been demonstrated dur-ing physical effort and in the hemodynamic adaptationto orthostatism. They have been postulated to explainthe lower mortality in women than in men among hyper-tensive or chronic heart failure patients (27).In addition to parasympathetic dominance in the control ofheart rate, women have been seen to display less LF spec-tral power of muscle sympathetic nerve activity and arteri-al blood pressure than men of the same age (28). These re-sults, together with epidemiological studies, suggest thata significant component of women’s cardiovascular ad-vantage over men may result not only from greater relativeparasympathetic input to the heart, but also from lessersympathetic input to vascular regulation (29).Cardiovascular risk factors in transsexual subjects are notclearly understood. The cardiovascular risk due to auto-
nomic balance in these subjects has not been previous-ly investigated. HRV could be a useful tool in the diag-nosis of cardiovascular pathologies in these subjects, andthe early subclinical detection of autonomic dysfunctionis therefore important for risk stratification and subse-quent management.While transsexualism is not a pathology, it constitutes anew and challenging field of research for endocrinolo-gists, and is able to shed new light on the use and role ofsex hormone therapy. Firstly, detecting the presence ofan autonomic imbalance in this population reveals a pos-sible cardiovascular risk due to the autonomic influenceon the heart. Secondly, it is important to classify the grav-ity of the risk in order to manage this population. Oncethe problem has been detected, risk stratification enablesus to identify those patients at greatest risk and to findproper solutions for their clinical management. For ex-ample, a deteriorated autonomic balance in a transsexu-al should suggest the re-modulation of the hormonaltherapy, namely reduction of the doses or the use of pro-tective strategies.Our data demonstrate that M-to-F transsexuals displaysignificantly lower sympathetic activity, both in clinos-tatism and in orthostatism, than males and females, andsignificantly lower sympathetic activity in clinostatism thanF-to-M transsexuals. Moreover, M-to-F have lowerparasympathetic activity, both in clinostatism and in or-thostatism, than males and females, and significantly low-er parasympathetic activity in clinostatism than F-to-M.The prevalence of sympathetic activity in males is associ-ated with higher cardiovascular risk. Our data indicate thatM-to-F display reduced sympathetic activity both in cli-nostatism and in orthostatism, which could reduce thespecific cardiovascular risk due to the higher sympathet-ic influence on the heart. This could be mediated by theeffect of hexogen estrogens, since these subjects do nothave other protective factors. Moreover, there are no da-ta regarding the possible interference of cyproterone ac-etate with the HRV parameters. Estrogen therapy may at-tenuate sympathetic regulation of heart rate, as reported
LF
/HF
o
20
10
0
-10No. 12 6 17 17
1 2 3 4Group
LF
/HF
c12
10
8
6
4
2
0
-2No. 12 6 17 17
1 2 3 4Group
Fig. 2 - Heart rate variability ratios in the 4 groups. A) Sympathetic activity (LF)/vagal activity (HF) in clinostatism (c); B) LF/HF in or-thostatism (o). ***p<0.001, **p<0.05.

E. Resmini, M. Casu, V. Patrone, et al.
1018
(15). The estrogen therapy seems to have changed theautonomic features of this population and no differencesin the autonomic parameters between M-to-F patientstaking oral E2 and transdermal E2 were found. Moreover,this lowering of sympathetic activity showed that M-to-Fsubjects have been seen to reach HRV indexes that aremore similar to those recorded in females.Regarding parasympathetic activity, M-to-F transsexualsdo not attain parasympathetic dominance in the controlof heart rate, a protective feature typical of females.It has been reported that estrogens have a facilitating ef-fect on cardiac vagal function (12, 30), but this did notappear in our patients. Regarding the sympathovagal in-fluence on the heart, M-to-F transsexuals are totally dif-ferent from both females and males.F-to-M transsexuals display a lower parasympathetic ac-tivity than females and therefore lose the protective fea-ture of parasympathetic dominance in the control of heartrate, which is typical of females. This potential disadvan-tage could be due to the administration of hexogentestosterone, as they do not have other autonomic in-terfering factors. Diminished parasympathetic control ofheart rate contributes to increasing the risk of cardiovas-cular events. Moreover, F-to-M transsexuals do not dis-play different HRV parameters from those of males. In-deed, in F-to-M, cardiovascular risk, due to the auto-nomic influence on the heart, may be higher than in fe-males and become more similar to that of males.In this study we also analyzed the mechanism of posturaladaptation by making a comparison within groups. Incontrol subjects in clinostatism, LF prevails over HF, in-dicating a prevalence of sympathetic activity. On pass-ing from clinostatism to orthostatism, a mechanism ofpostural adaptation occurs, producing a decrease in va-gal activity (HF) and a further increase in sympathetic ac-tivity (LF). Indeed, in both categories of transsexuals, themechanism of postural adaptation is partially conserved.Finally, our data confirm the gender differences in HRVdescribed in literature, namely a prevalence of vagal tonein females. Detailed mechanisms linking estrogens andHRV warrant further exploration.In conclusion, our data revealed a sympathovagal imbal-ance in transsexual patients, due to a reduction in bothsympathetic and parasympathetic influence on heart rateregulation, irrespective of the type of hormone adminis-tered. Sex hormone therapy per se may therefore play arole in this imbalance. Transsexual subjects display fea-tures which are different from those of their genetic sex.The sympathetic reduction in M-to-F may lead to a low-er cardiovascular risk due to autonomic influence on heartrate. The parasympathetic reduction in F-to-M may leadto a higher cardiovascular risk due to autonomic influ-ence on heart rate.Our study involved a small number of patients, owing tothe difficulty of recruiting this kind of patient; moreover,our data are only preliminary. Nevertheless, we believe thatthis method could be applied to the study of cardiovascu-lar risk in transsexuals, which is not clearly understood, be-cause evaluating HRV is a well-recognized method of as-sessing cardiovascular risk due to autonomic activity. Wewould therefore like to open a new area of research intocardiovascular risk among transsexual patients.
Further longitudinal studies, with a larger number of pa-tients, are needed in order to ascertain the clinical mean-ing and the role of sympathovagal imbalance in trans-sexuals.
ACKNOWLEDGMENTSThis study was partially supported by grants from MIUR (2002067251-001) and the University of Genoa, and by an educational grant fromCARIGE Foundation to D.F. (research funding).
REFERENCES1. Malliani A, Lombardi F, Pagani M, Cerutti S. Power spectral analy-
sis of cardiovascular variability in patients at risk for sudden car-diac death. J Cardiovasc Electrophysiol 1994, 5: 274-86.
2. Vanoli E, Schwartz PJ. Sympathetic-parasympathetic interactionand sudden death. Basic Res Cardiol 1990, 85 (Suppl 1): 305-21.
3. Lombardi F, Malliani A, Pagani M, Cerutti S. Heart rate variabili-ty and its sympatho-vagal modulation. Cardiovasc Res 1996, 32:208-16.
4. Sosnowski M, Clark E, Latif S, Macfarlane PW, Tendera M. Heartrate variability fraction--a new reportable measure of 24 h R-R in-terval variation. Ann Noninvasive Elettrocardiol 2005, 10: 7-15.
5. Malliani A. Heart rate variability: from bench to bedside. Eur JIntern Med 2005, 16: 12-20.
6. Heart rate variability. Guidelines. Standards of measurements, phys-iological interpretation and clinical use. Task Force of the Europeansociety of Cardiology and The North American Society of Pacingand Electrophysiology. Eur Heart J 1996, 17: 354-81.
7. Kleiger RE, Stein PK, Bigger JT Jr. Heart rate variability: measure-ment and clinical utility. Ann Noninvasive Elettrocardiol 2005, 10:88-101.
8. Spallone V, Uccioli L, Menzinger G. Diabetic autonomic neuropa-thy. Diabetes Metab Rev 1995, 11: 227-57.
9. Aring AM, Jones DE, Falko JM. Evaluation and prevention of dia-betic neuropathy. Am Fam Physician 2005, 71: 2123-8.
10. Low PA, Benrud-Larson LM, Sletten DM, et al. Autonomic symp-toms and diabetic neuropathy: a population-based study. DiabetesCare 2004, 27: 2942-7.
11. Resmini E, Casu M, Patrone V, et al. Sympathovagal imbalance inacromegalic patients. J Clin Endocrinol Metab 2006, 91: 115-20.
12. Evans JM, Ziegler MG, Patwardhan AR, et al. Gender differences inautonomic cardiovascular regulation: spectral, hormonal, andhemodynamic indexes. J Appl Physiol 2001, 91: 2611-8.
13. Stein PK, Kleiger RE, Rottman JN. Differing effects of age on heartrate variability in men and women. Am J Cardiol 1997, 80: 302-5.
14. Bonnemeier H, Richardt G, Potratz J, et al. Circadian profile of car-diac autonomic nervous modulation in healthy subjects: differing ef-fects of aging and gender on heart rate variability. J CardiovascElectrophysiol 2003, 14: 791-9.
15. Liu CC, Kuo TB, Yang CC. Effects of estrogen on gender-relatedautonomic differences in humans. Am J Physiol Heart Circ Physiol2003, 285: H2188-93.
16. Rosano GM, Panina G. Oestrogens and the heart. Thérapie 1999,54: 381-5.
17. La Rovere MT, Bigger JT Jr, Marcus FI, Mortara A, Schwartz PJ.Baroreflex sensitivity and heart-rate variability in prediction of to-tal cardiac mortality after myocardial infarction. ATRAMI(Autonomic Tone and Reflexes After Myocardial Infarction)Investigators. Lancet 1998, 351: 478-84.
18. Mortara A, La Rovere MT, Pinna GD, et al. Arterial baroreflex mod-ulation of heart rate in chronic heart failure: clinical and hemody-namic correlates and prognostic implications Circulation 1997, 18:3450-8.
19. Bush TL, Barrett-Connor E, Cowan LD, et al. Cardiovascular mor-tality and noncontraceptive use of estrogen in women: results fromthe Lipid Research Clinics Program Follow-up Study. Circulation1987, 75: 1102-9.

Sympathovagal imbalance in transsexuals
1019
20. Rossouw JE, Anderson GL, Prentice RL, et al; Writing Group forthe Women’s Health Initiative Investigators. Risks and benefits ofestrogen plus progestin in healthy postmenopausal women: prin-cipal results for the Women’s Health Initiative randomized con-trolled trial. JAMA 2002, 288: 321-33.
21. Elbers JM, Giltay EJ, Teerlink T, et al. Effects of sex steroids oncomponents of the insulin resistance syndrome in transsexual sub-jects. Clin Endocrinol (Oxf) 2003, 58: 562-71.
22. Malliani A, Pagani M, Lombardi F, Cerutti S. Cardiovascular neuralregulation explored in the frequency domain. Circulation 1991, 84:482-92.
23. Cowan MJ. Measurement of heart rate variability. West J Nurs Res1995,17: 32-48.
24. Singh JP, Larson MG, Tsuji H, Evans JC, O'Donnell CJ, Levy D.Reduced heart rate variability and new-onset hypertension: insightsinto pathogenesis of hypertension: the Framingham Heart Study.Hypertension 1998, 32: 293-7.
25. Casolo GC, Stroder P, Signorini C, et al. Heart rate variability dur-
ing the acute phase of myocardial infarction. Circulation 1992, 85:2073-9.
26. Janszky I, Ericson M, Mittleman MA, et al. Heart rate variability inlong-term risk assessment in middle-aged women with coronaryheart disease: The Stockholm Female Coronary Risk Study. J InternMed 2004, 255: 13-21.
27. Conte MR. Gender differences in the neurohumoral control of thecardiovascular system. Ital Heart J 2003, 4: 367-70.
28. Matsukawa T, Sugiyama Y, Watanabe T, Kobayashi F, Mano T.Gender difference in age-related changes in muscle sympathet-ic nerve activity in healthy subjects. Am J Physiol 1998, 275:R1600-4.
29. Evans JM, Ziegler MG, Patwardhan AR, et al. Gender differences inautonomic cardiovascular regulation: spectral, hormonal, andhemodynamic indexes. J Appl Physiol 2001, 91: 2611-8.
30. Du XJ, Riemersma RA, Dart AM. Sex differences in the parasym-pathetic nerve control of rat heart. Clin Exp Pharmacol Physiol1994, 21: 485-93.