![Uveitic macular edema: a stepladder treatment paradigm€¦ · of macular edema [1,3–4], this review will focus on uveitic macular edema specifically. Uveitic macular edema Macular](https://static.fdocuments.in/doc/165x107/5ed770e44d676a3f4a7efe51/uveitic-macular-edema-a-stepladder-treatment-paradigm-of-macular-edema-13a4.jpg)
SwixSPIEMI14-Microcystic Macular Edema Detection in Retina OCT Images
7
Microcystic macular edema detection in retina OCT images Emily K. Swingle a , Andrew Lang b , Aaron Carass b , Howard S. Ying c , Peter A. Calabresi d , and Jerry L. Prince b a Department of Biomedical Engineering, The Ohio State University b Department of Electrical and Computer Engineering, The Johns Hopkins University c Wilmer Eye Institute, The Johns Hopkins University School of Medicine d Department of Neurology, The Johns Hopkins University School of Medicine ABSTRACT Optical coherence tomography (OCT) is a powerful imaging tool that is particularly useful for exploring retinal abnormalitie s in oph thalmologic al disea ses. Recen tly , it has been used to trac k changes in the eye associa ted with neurological diseases such as multiple sclerosis (MS) where certain tissue layer thicknesses have been associated with disease progression. A small p ercen tage of MS patients also exhibit what has been called microcys tic macular edema (MME), where fluid collections that are thought to be pseudocysts appear in the inner nuclear layer. Very little is known about the cause of this condition so it is important to be able to identify precisely where these pseudocysts occur within the retina. This identification would be an important first step towards furthering our understanding. In this work, we present a detection algorithm to find these pseudocysts and to report on their spati al distributio n. Our approach uses a random forest classi fier trained on man ual segmen tation data to class ify each vo xel as pseudocyst or not. Despite having a small sample size of five subjects, the algorith m correctly iden tifies 84.6% of pseud ocysts as compared to manual delineation. Final ly , usin g our method, we show that the spatial distribution of pseudocysts within the macula are generally contained within an annulus around the fovea. Keywords: OCT, pseudocysts, segmentation, classification, microcystic macular edema 1. INTRODUCTION Optical Coherence Tomography (OCT) is becoming a useful imaging tool for estimating the severity of retinal pathology in both ophthalmology 1 and neurology. 2 Near-infrared light from the OCT scanner penetrates retinal lay ers at the back of the eye, and detects back scatte red light to create an imag e. In addition to displa ying the retinal layer s, these images can be used to iden tify structural abnormalities within each layer. One such abno rmali ty is the appearance of smal l fluid filled regio ns, sometimes called microcysts or pseud ocysts, found within the retinal tissue. In multip le sclerosis (MS) , these pseudocysts occur in about 5% of subjects; 3, 4 a condition that has been termed microcystic macular edema (MME). Specifically, MME is most commonly found in the inner nu cle ar laye r (INL ), see Fig. 1 for an exampl e. Little is kno wn about the appe ara nce of these pseudocysts, or their implications for disease prognosis, but they have been found to be correlated with disease severity, a reduction of visual acuity, and thinning of the retinal nerve fiber layer (RNFL). 4 It also seems that optic neuropathy may be associated with these pseudocystic changes. 5, 6 In addition to simp ly explo ring the appearance of these pseudocysts, trac king the longi tudin al changes may also prove to be useful to enhance our understanding of MME. In recent studies by Saidha et al. 3 and Gelfand et al., 4 longitudinally scanned OCT data were obtained from several patients with MME (ten patients in Ref. 3 and six patie nts in Ref. 4). In total, five of the affecte d eye s exhibited impro vement of MME, seven experie nced wor senin g of MME, and six showed either no apparent change or fluctuation s over time (noting that MME was bilateral in two of the patients). Although these studies indicate possible dynamic characteristics of MME over time, the volume and location of MME was not quantitatively evaluated and therefore much more can be learned about the pseudocyst volume and location over time in relation to MS. It is clear that studying the appearance of these pseudocysts, both cross-sectionally and longitudinally, is necessary to better help study this condition. With so much about MME still unknown, methods for detecting and quan tifying the size and distribu tion of these fluid-fi lled areas are essen tial. Due to the sheer amount of Medical Imaging 2014: Biomedical Applications in Molecular, Structural, and Functional Imaging, edited by Robert C. Molthen, John B. Weaver, Proc. of SPIE Vol. 9038, 90380G © 2014 SPIE · CCC code: 1605-7422/14/$18 · doi: 10.1117/12.2043910 Proc. of SP IE Vol. 9038 90380G-1 Downloaded From: http://spiedigitallibrary.org/ on 06/23/2014 Terms of Use: http://spiedl.org/terms
description
research
Transcript of SwixSPIEMI14-Microcystic Macular Edema Detection in Retina OCT Images
-
Microcystic macular edema detection in retina OCT images
Emily K. Swinglea, Andrew Langb, Aaron Carassb, Howard S. Yingc,Peter A. Calabresid, and Jerry L. Princeb
aDepartment of Biomedical Engineering, The Ohio State UniversitybDepartment of Electrical and Computer Engineering, The Johns Hopkins University
cWilmer Eye Institute, The Johns Hopkins University School of MedicinedDepartment of Neurology, The Johns Hopkins University School of Medicine
ABSTRACT
Optical coherence tomography (OCT) is a powerful imaging tool that is particularly useful for exploring retinalabnormalities in ophthalmological diseases. Recently, it has been used to track changes in the eye associated withneurological diseases such as multiple sclerosis (MS) where certain tissue layer thicknesses have been associatedwith disease progression. A small percentage of MS patients also exhibit what has been called microcystic macularedema (MME), where fluid collections that are thought to be pseudocysts appear in the inner nuclear layer. Verylittle is known about the cause of this condition so it is important to be able to identify precisely where thesepseudocysts occur within the retina. This identification would be an important first step towards furthering ourunderstanding. In this work, we present a detection algorithm to find these pseudocysts and to report on theirspatial distribution. Our approach uses a random forest classifier trained on manual segmentation data to classifyeach voxel as pseudocyst or not. Despite having a small sample size of five subjects, the algorithm correctlyidentifies 84.6% of pseudocysts as compared to manual delineation. Finally, using our method, we show thatthe spatial distribution of pseudocysts within the macula are generally contained within an annulus around thefovea.
Keywords: OCT, pseudocysts, segmentation, classification, microcystic macular edema
1. INTRODUCTION
Optical Coherence Tomography (OCT) is becoming a useful imaging tool for estimating the severity of retinalpathology in both ophthalmology1 and neurology.2 Near-infrared light from the OCT scanner penetrates retinallayers at the back of the eye, and detects backscattered light to create an image. In addition to displayingthe retinal layers, these images can be used to identify structural abnormalities within each layer. One suchabnormality is the appearance of small fluid filled regions, sometimes called microcysts or pseudocysts, foundwithin the retinal tissue. In multiple sclerosis (MS), these pseudocysts occur in about 5% of subjects;3,4 acondition that has been termed microcystic macular edema (MME). Specifically, MME is most commonly foundin the inner nuclear layer (INL), see Fig. 1 for an example. Little is known about the appearance of thesepseudocysts, or their implications for disease prognosis, but they have been found to be correlated with diseaseseverity, a reduction of visual acuity, and thinning of the retinal nerve fiber layer (RNFL).4 It also seems thatoptic neuropathy may be associated with these pseudocystic changes.5,6
In addition to simply exploring the appearance of these pseudocysts, tracking the longitudinal changes mayalso prove to be useful to enhance our understanding of MME. In recent studies by Saidha et al.3 and Gelfand etal.,4 longitudinally scanned OCT data were obtained from several patients with MME (ten patients in Ref. 3and six patients in Ref. 4). In total, five of the affected eyes exhibited improvement of MME, seven experiencedworsening of MME, and six showed either no apparent change or fluctuations over time (noting that MME wasbilateral in two of the patients). Although these studies indicate possible dynamic characteristics of MME overtime, the volume and location of MME was not quantitatively evaluated and therefore much more can be learnedabout the pseudocyst volume and location over time in relation to MS.
It is clear that studying the appearance of these pseudocysts, both cross-sectionally and longitudinally, isnecessary to better help study this condition. With so much about MME still unknown, methods for detectingand quantifying the size and distribution of these fluid-filled areas are essential. Due to the sheer amount of
Medical Imaging 2014: Biomedical Applications in Molecular, Structural, and Functional Imaging, edited by Robert C. Molthen, John B. Weaver, Proc. of SPIE Vol. 9038, 90380G
2014 SPIE CCC code: 1605-7422/14/$18 doi: 10.1117/12.2043910
Proc. of SPIE Vol. 9038 90380G-1
Downloaded From: http://spiedigitallibrary.org/ on 06/23/2014 Terms of Use: http://spiedl.org/terms
-
(a)
(b)
(c) (d)
(a)
(b)
(c) (d)(a)
(b)
(c) (d)
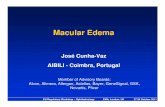
Figure 1: (a) Fundus image showing the location of acquired B-Scans; the red line represents the location ofthe B-scan portrayed in (b). (b) B-scan image containing pseudocysts which are shown with 3 zoom below.(c) and (d) shows areas with small and large pseudocysts, respectively.
data output from OCT, this analysis is only feasible with an automatic detection method. To the best of ourknowledge, there has been no previous research to automatically detect and analyze the spatial configuration ofthese pseudocysts within the retina for MME patients. Although a method for identifying closed-contour featuresin the retina has been investigated,7 and a 3D process has been analyzed to locate retinal abnormalities,8 thisresearch was not done to identify and analyze the types of cystic areas found in MME, specifically.
In this work, we created an algorithm to automatically identify pseudocysts in the retina. The algorithmuses a simple classification approach where each voxel is classified as pseudocyst or not based on the outputof a trained classifier. This detection allows us to both quantify the number of pseudocysts, and display theirspatial distribution across the retina. Overall, our method could be used to give more insight on the cause andprogression of these pseudocysts.
2. METHODS
In our analysis, we used OCT images of the retina acquired over the macular cube. A fundus image, illustratedin Fig. 1(a), displays the anterior portion of the retina where these images were obtained. The overall volumecomprises 49 OCT images, called B-scans (Fig. 1(b)). Each column of a B-scan is called an A-scan. These B-scansare acquired over the macula as shown in Fig. 1(a), with the horizontal blue lines representing the location ofeach B-scan. Each 2D image portrays details of the retinal layers, as well as abnormalities that may be locatedwithin these layers. Examples of small and large pseudocysts in the INL are shown in Figs. 1(c) and (d).
Our pseudocyst detection algorithm uses a pixel classification approach. Before the classification stage, weuse two preprocessing steps, which are summarized here and described in detail in Lang et al.9 In the first step,we normalize the intensities of the images; the intensity range of each B-scan is clamped and rescaled based ona robust estimate of the maximum intensity. The purpose of this step is to obtain a more consistent intensitydistribution to improve the performance of the classifier. Second, we estimate the location of the inner and outerretina boundaries, the inner limiting membrane (ILM) and Bruchs membrane (BM), respectively. Knowledge ofthese boundaries allows us to restrict the search area for the pseudocysts and also to incorporate the relativedistance of pseudocysts from the retina boundaries as a feature, as we only expect to see them in or near the INL.Briefly, these boundaries are found by looking for large vertical gradients in each image. The inner and outerboundaries are roughly estimated from the largest positive and negative gradients along each A-scan, respectively.Final boundary positions were constrained by an estimated position of the photoreceptor junction (a large positivegradient near the bottom of the retina), median filtered to remove outliers, and finally smoothed using a Gaussiankernel.
Proc. of SPIE Vol. 9038 90380G-2
Downloaded From: http://spiedigitallibrary.org/ on 06/23/2014 Terms of Use: http://spiedl.org/terms
-
With knowledge of where the retinal boundaries are, our pseudocyst detection algorithm uses a randomforest (RF) classifier.10 We use the RF classifier since it has a small number of parameters, is efficient, can extracthighly nonlinear correlations, and its performance is as good or better than other state-of-the-art methods. A RFworks by constructing a forest of multiple decision trees. Each tree is independently trained using a randomsample of the training data and, given an input feature vector, provides a decision about what class the inputbelongs to. By aggregating the classification result of each tree and using a majority vote rule, a final classificationestimate is obtained.
To use RF for our problem, we look at each pixel independently, using a set of 14 features to classify whetheror not each pixel is pseudocyst or non-pseudocyst. As the pseudocysts appear darker than the surrounding retinaltissue, we primarily use intensity-based features. For the first two features, we use the voxel intensity and voxelintensity after a gray-scale morphological closing operation (using a disk structuring element with a radius of5 pixels). Closing acts to remove the pseudocysts providing a contrast to the original intensity. The next ninefeatures are the voxel intensity after Gaussian filtering at various scales. The next two features are the Laplacianand Laplacian of Gaussian of the image as ways to enhance the smaller, narrow pseudocysts. Finally, we use therelative distance to the retina boundaries as a spatial feature to localize the position of the pseudocysts withinthe retina. Specifically, we look at the proportional distance of a pixel along each A-scan; for instance, looking atFig. 1(b), we might generally expect to find the pseudocysts at around 30% of the distance from the ILM to theBM.
To compute a final pseudocyst segmentation, we simply compute these features at each pixel and evaluatethem using the trained RF classifier. Since classification in this manner will produce several spurious pixelsclassified as pseudocyst, we simply remove all connected components below a specified threshold. The best valueof this threshold is explored in the next section.
3. EXPERIMENTS AND RESULTS
We used available data with pseudocysts from five MS subjects having MME. Additionally, we used twopseudocyst-free healthy controls to aid in training. The OCT scans (20 20) were imaged on a Spectralisscanner (Heidelberg Engineering, Heidelberg, Germany). The scans consisted of 49 B-scans with 1024 A-scanseach, imaging approximately 6 6 mm of the macula. Manual delineation of the pseudocysts in each subject wasperformed by two raters. Both raters independently delineated the scan with the most pseudocysts present, andthen separately delineated the remainder of the MS data.
To test our approach, the RF classifier was tested using a leave-one-out strategy on each of the five MSsubjects. Thus, one classifier was trained to evaluate each MME subject. Each classifier was trained on the datafrom four MME subjects and two healthy control subjects. From each training subject, we included ten randomlyselected B-scans from the MS subjects and twelve B-scans from the healthy controls. We used only a fraction ofthe training data because, at the resolution of the data, using the entire volume results in an excessive amount ofdata, both in terms of training time and memory requirements. All pseudocyst pixels and 75% of the backgroundpixels within the estimated retinal boundaries of the respective B-scan were included. We used 75 trees to buildthe RF, with the split decision at each node based on two randomly selected features.
Fig. 2 shows a comparison between the size of pseudocysts detected by our algorithm and those delineated byour human raters on the entire cohort of five MS subjects with MME. From this figure, it is clear that therewas broad agreement between the manual and automated segmentation for pseudocysts larger than 15 pixels,although below that level the algorithm detected vastly more pseudocysts. For purposes of this analysis, weconsider a single pseudocyst as a single connected component area.
In Table 1, we provide a direct comparison of the number of pseudocysts found by our algorithm and thenumber found by the manual raters. Listed are the number of pseudocysts found having an area above the statedpseudocyst threshold, with the area simply being the number of pixels within the connected component. Fivedifferent threshold values were compared. As we also see in Fig. 2, the performance of the algorithm improveswith a larger pseudocyst threshold. One explanation for this result is that the larger pseudocysts contain moredark intensities making the classification task simpler. Smaller pseudocysts generally have variable levels ofdark-to-bright intensities making them more difficult to classify.
Proc. of SPIE Vol. 9038 90380G-3
Downloaded From: http://spiedigitallibrary.org/ on 06/23/2014 Terms of Use: http://spiedl.org/terms
-
Manual SegmentationAlgorithmTogether
11L, n
Size of pseudocysts (pixels)
Numb
er of
pseud
ocysts
0 10 20 30 40 50 60 70 80 90 100 1100
100200300400
Manual SegmentationAlgorithmTogether
Figure 2: Histogram comparison of pseudocyst sizes for manual segmentation and algorithm identification.
Table 1: A comparison of pseudocysts segmented and correctly identified for different size thresholds of manualsegmentation. Values represent totals across all five MS patients.
Pseudocyst Size # Manual # Correctly % CorrectlyThreshold Segmented Segmented Detected
10 1869 1280 68.520 1325 1035 78.130 876 741 84.640 522 459 87.950 316 291 92.1
In Fig. 3, we show the result of our algorithm overlaid on a B-scan image. Looking closely at the results(Figs. 3(d) and 3(e)), we see good overall agreement in the larger pseudocysts, as well as the slight differencesin the boundaries when comparing the algorithm to our raters. Smaller pseudocysts show less agreement, withseveral pseudocysts found by the human rater and not by the algorithm (displayed in red). It should be noted,however, that manual delineation of these smaller pseudocysts is subjective due to the definition of what is and isnot a pseudocyst.
Next, we evaluated our algorithm on data that has no pseudocysts. To do this, we selected five healthy controlsubjects and five additional MS patients, which were all inspected and found to not have pseudocysts. The resultsof running our algorithm on this data are presented in Table 2. For this comparison, we removed all pseudocystsbelow a size threshold of 30 pixels. In this table, we see that the algorithm performs particularly well on thecontrol subjects, with a maximum of one pseudocyst detected in each subject. The same can be said for the MSsubjects without pseudocysts, having a maximum of two detected pseudocysts.
As a final comparison between the manual and automatic segmentation, we compared the spatial distributionof the pseudocysts within the macula. This was accomplished by projecting and smoothing the number ofpseudocysts found by both our algorithm and our human raters onto a fundus image of a retina, see Fig. 4. Weagain see good agreement between our algorithm and the manual segmentation, even when only a few pseudocystsare present, as shown in Figs. 4(c) and 3(d). We also notice a pattern in the distribution of the location of thepseudocysts around the fovea. Note that again, a pseudocyst size threshold of 30 pixels was used in these images.It is interesting to note that the distribution of these pseudocysts forms in an annulus around the fovea at thecenter of the macula.
4. DISCUSSION AND CONCLUSIONS
We have developed an algorithm for the detection of MME and the related pseudocysts in retinal OCT images.Our segmentation agrees closely with the results of manual raters on pseudocysts larger than 15 pixels in size,
Proc. of SPIE Vol. 9038 90380G-4
Downloaded From: http://spiedigitallibrary.org/ on 06/23/2014 Terms of Use: http://spiedl.org/terms
-
Pig orit hm Cyst Id enlif icati on
Manual vs. Algorithm Cyst Identification
..
t
L14a,
_
y+ 1
(a)
(b)
(c)
(d) (e)
(f) (g)
Figure 3: Performance of the pseudocyst segmentation algorithm on one B-scan, for pseudocysts above the 30pixel threshold. From top to bottom shows (a) the original B-scan, (b) the result of the algorithm overlaid ingreen, and (c) the ground truth and algorithm overlaid together (red = false negative, green = false positive, andblue = positive). The images in (d-g) show zoomed in portions of the images in (a) and (c).
with even better performance with a threshold of larger than 30 pixels. We believe that the errors below this levelrepresent the difficulty that human raters have in identifying small pseudocysts. This is evidenced by the factthat the raters had an overlap agreement (Dice score) of just 0.75 on the volume they both segmented. Despitethe small sample size for training and evaluation, our approach is able to locate 85% of the pseudocysts largerthan 30 pixels. Our method also did not identify pseudocysts in pseudocyst-free subjects, suggesting its specificity
Proc. of SPIE Vol. 9038 90380G-5
Downloaded From: http://spiedigitallibrary.org/ on 06/23/2014 Terms of Use: http://spiedl.org/terms
-
Table 2: Comparison of pseudocyst detection of our algorithm on three cohorts: healthy controls, MS patientswithout pseudocysts, and MS patients with pseudocysts. Each cohort consisted of five subjects. The mean, min,and max number of cysts per subject, and the mean number of cyst pixels identified per subject are reported bycohort.
Pseudocysts detected Pseudocyst Pixels
Mean Min Max Mean
Healthy Control 0.2 0 1 6.8MS Patients without Pseudocysts 0.6 0 2 24.8MS Patients with Pseudocysts 118.2 7 305 6288.6
Subject #1
(a) (b) (c)Subject #2
(d) (e) (f)Figure 4: (a, d) Fundus image for two subjects with the black lines indicating the extents of the OCT volume.Spatial distribution of pseudocysts overlaid on the fundus images of two subjects for (b, e) a manual rater,and (c, f) our algorithm. Similar annulus patterns and accuracy could be seen in all five MS subjects withpseudocysts.
is well suited for differentiating MME and non-MME patients. This detection capability would also be beneficialin improving layer segmentation algorithms9 which have difficulty when run on these MME patients. The spatialdistribution of the pseudocysts (Fig. 4) as an annulus around the fovea was unexpected and represents an excitingstep forward in our understanding of MME. This is a result that has only recently been found by others.6,11
Our approach could be improved in several ways including increasing the size of the training data andimproving the quality of the human rater segmentations. While the features we used worked well, incorporatingmore local information can help reduce the identification of smaller pseudocysts. However, there is some debateas to whether these are false positives or failures on the part of our raters. In addition, the apparent spatialdistribution of the pseudocysts (Fig. 4) informs us that we do not expect to find pseudocysts outside of an annulusaround the fovea. This information could be included in the classification.
Future work includes expanding our algorithm to other scanner manufacturers and a comprehensive study of
Proc. of SPIE Vol. 9038 90380G-6
Downloaded From: http://spiedigitallibrary.org/ on 06/23/2014 Terms of Use: http://spiedl.org/terms
-
the longitudinal behavior of MME. From this future work, a better understanding could be provided about thesepseudocysts; we will be able to learn more about the mechanisms by which these pseudocysts appear in additionto their changes with disease progression and severity.
REFERENCES
[1] Fujimoto, J. G., Drexler, W., Schuman, J. S., and Hitzenberger, C. K., Optical coherence tomography(OCT) in ophthalmology: introduction, Opt. Express 17(5), 39783979 (2009).
[2] Jindahra, P., Hedges, T. R., Mendoza-Santiesteban, C. E., and Plant, G. T., Optical coherence tomographyof the retina: applications in neurology, Curr. Opin. Neurol. 23(1), 1623 (2010).
[3] Saidha, S., Sotirchos, E. S., Ibrahim, M. A., Crainiceanu, C. M., Gelfand, J. M., Sepah, Y. J., Ratchford,J. N., Oh, J., Seigo, M. A., Newsome, S. D., Balcer, L. J., Frohman, E. M., Green, A. J., Nguyen, Q. D., andCalabresi, P. A., Microcystic macular oedema, thickness of the inner nuclear layer of the retina, and diseasecharacteristics in multiple sclerosis: a retrospective study, The Lancet Neurology 11(11), 963972 (2012).
[4] Gelfand, J. M., Nolan, R., Schwartz, D. M., Graves, J., and Green, A. J., Microcystic macular oedema inmultiple sclerosis is associated with disease severity, Brain 135(6), 17861793 (2012).
[5] Bhargava, P. and Calabresi, P. A., The expanding spectrum of aetiologies causing retinal microcysticmacular change, Brain 136(11), 32123214 (2013).
[6] Wolff, B., Basdekidou, C., Vasseur, V., Mauget-Faysse, M., Sahel, J.-A., and Vignal, C., Retinal inner nuclearlayer microcystic changes in optic nerve atrophy: A novel spectral-domain OCT finding, Retina 33(10),21332138 (2013).
[7] Chiu, S. J., Toth, C. A., Izatt, C. B.-R. J. A., and Farsiu, S., Automatic segmentation of closed-contourfeatures in ophthalmic images using graph theory and dynamic programming, Biomed. Opt. Express 3(5),11271140 (2012).
[8] Quellec, G., Lee, K., Dolejsi, M., Garvin, M. K., Abra`moff, M. D., and Sonka, M., Three-dimensionalanalysis of retinal layer texture: Identification of fluid-filled regions in SD-OCT of the macula, IEEE Trans.Med. Imag. 29(6), 13211330 (2010).
[9] Lang, A., Carass, A., Hauser, M., Sotirchos, E. S., Calabresi, P. A., Ying, H. S., and Prince, J. L., Retinallayer segmentation of macular OCT images using boundary classification, Biomed. Opt. Express 4(7),11331152 (2013).
[10] Breiman, L., Random forests, Machine Learning 45(1), 532 (2001).
[11] Abegg, M., Dysli, M., Wolf, S., Kowal, J., Dufour, P., and Zinkernagel, M., Microcystic macular edema:Retrograde maculopathy caused by optic neuropathy, Ophthalmology 121(1), 142149 (2014).
Proc. of SPIE Vol. 9038 90380G-7
Downloaded From: http://spiedigitallibrary.org/ on 06/23/2014 Terms of Use: http://spiedl.org/terms