![[Hyundai Glovis] Kis London Ndr](https://static.fdocuments.in/doc/165x107/55cf9c8c550346d033aa352f/hyundai-glovis-kis-london-ndr.jpg)
Swedish National Diabetes Register Annual report …Annual Report 2013 | 5 The NDR has established...
45
Swedish National Diabetes Register Annual report 2013 Time to pharmacological treatment has been reduced from year 2002 to 2011. 2011 2010 2009 2008 2007 2006 2005 2004 2003 2002 PATIENTS 100% 80% 60% 40% 20% 0% DAYS 0 500 1000 1500 2000 2500 3000 3500
Transcript of Swedish National Diabetes Register Annual report …Annual Report 2013 | 5 The NDR has established...

Swedish National Diabetes Register
Annual report 2013
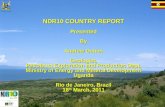
Time to pharmacological treatment has been reduced from year 2002 to 2011.
2011
20102009
20082007
2006
20052004
2003
2002
PATIENTS
100%
80%
60%
40%
20%
0%
DAYS
0 500 1000 1500 2000 2500 3000 3500
Time to pharmacological treatment has been reduced from year 2002 to 2011.

ISSN 2001-2632Print year 2014
Layout and production: Ibiz reklambyrå • Printing: Litorapid, Hisings Kärra • Photo: Björn Eliasson (cover photo), iStockhoto
AuthorsSoffía GuðbjörnsdóttirDirector, MD, PhD, Associate ProfessorSwedish National Diabetes Register (NDR) – Centre of Registers, Region Västra Götaland, Department of Medicine, University of Gothenburg413 45 Gothenburg, Sweden
Björn EliassonAssociate ProfessorDepartment of MedicineSahlgrenska University Hospital413 45 Gothenburg, Sweden
Jan CederholmAssociate ProfessorDepartment of Public Health and Caring Sciences Family Medicine and Clinical Epidemiology Uppsala University Uppsala, Sweden
Björn ZetheliusAssociate ProfessorDepartment of Public Health and Caring Sciences Geriatrics, Uppsala University Uppsala Sweden
Ann-Marie SvenssonAssociate Director, RN, PhDSwedish National Diabetes Register (NDR) – Centre of Registers, Region Västra Gö[email protected]
Pär SamuelssonDevelopment ManagerSwedish National Diabetes Register (NDR) – Centre of Registers, Region Västra Gö[email protected]
Statistician, MScMervete [email protected]
System developerHenrik [email protected]
CoordinatorIa [email protected]
DirectorSoffía Guðbjörnsdó[email protected]
EditorMarie RöllgårdhCentre of Registers, Region Västra Götaland413 45 Gothenburg, Sweden
Department HeadRegion Västra GötalandRegionens Hus462 80 Vänersborg, Sweden
Annual Report 2013: ResultsSwedish National Diabetes Register (NDR) – Centre of Registers, Region Västra Götaland www.ndr.nu

Contents
Introduction –
The NDR is a Tool for Improving Diabetes Care ............... 4
Participation and Reporting in 2013 .............................. 6
Observations by the Patient Advocacy Group ................. 8
National Results for 2009–2013 ................................... 9
Number of Patients and Classification of Diabetes ....................9
Lifestyle .........................................................................13
Young Adults with Type 1 Diabetes .....................................19
Diabetes Treatment ..........................................................20
Blood Pressure ................................................................21
Blood Lipids ....................................................................24
Impact on the Kidneys ......................................................25
Acetylsalicylic Acid (Aspirin) ...............................................26
Process Measures: Eye and Foot Examinations .......................26
Estimated 5-year Risk for Cardiovascular Disease ...................27
Patients with Recent Onset of Type 2 Diabetes ......................28
Percentage of Primary Care Patients
with Three or More High-risk Factors ...................................29
Women and Men ............................................................30
Facts about the NDR ..........................................................32
Example from specialist clinic ............................................38
Publications ........................................................................41
doi: 10.1111/j.1365-2796.2010.02265.x
New aspects of HbA1c as a risk factor for cardiovascular
diseases in type 2 diabetes: an observational study from the
Swedish National Diabetes Register (NDR)K. Eeg-Olofsson1, J. Cederholm2, P. M. Nilsson3, B. Zethelius4, A.-M. Svensson5, S. Gudbjornsdottir1& B. Eliasson1
Fromthe 1InstituteofMedicine,SahlgrenskaUniversityHospital,UniversityofGothenburg,Gothenburg; 2DepartmentofPublicHealthandCaring
Sciences ⁄ FamilyMedicineandClinicalEpidemiology,UppsalaUniversity,Uppsala; 3Department ofClinicalSciences,LundUniversity,University
Hospital,Malmo; 4DepartmentofPublicHealthandCaringSciences ⁄Geriatrics,UppsalaUniversity,Uppsala;and 5CenterofRegisters inRegion
VastraGotaland,Gothenburg,Sweden
Abstract. Eeg-Olofsson K, Cederholm J, Nilsson PM,
ZetheliusB,SvenssonA-M,GudbjornsdottirS,Elias-
son B (Institute of Medicine, Sahlgrenska University
Hospital, University of Gothenburg, Gothenburg;
Department of Public Health and Caring Sciences ⁄
FamilyMedicine andClinical Epidemiology, Uppsala
University, Uppsala; Department of Clinical Sci-
ences, Lund University, University Hospital, Malmo;
Department of Public Health and Caring Sciences ⁄
Geriatrics, Uppsala University, Uppsala; and Center
of Registers in Region Vastra Gotaland, Gothenburg,
Sweden) New aspects of HbA1c as a risk factor for
cardiovascular diseases in type 2 diabetes: an
observational study from the Swedish National
Diabetes Register (NDR). J Intern Med 2010; 268:
471–482.
Aims. To analyse the association between glycosylated
haemoglobin A1c (HbA1c) and cardiovascular dis-
ease (CVD) in patients with type 2 diabetes in the
SwedishNationalDiabetesRegister (NDR).Methods. An observational study of 18 334 patients
(age 30–79 years, previous CVD in 18%, baseline
HbA1c 5.0–10.9%) who were followed for 6 years
(mean5.6 years) from1997 ⁄1998until2003.Results.Hazard ratios per 1% unit increase in baseline
or updated mean HbA1c for fatal ⁄nonfatal coronary
heart disease (CHD), CVD and total mortality were
1.11–1.13, 1.10–1.11 and 1.09–1.10, respectively
(all P < 0.001), adjusted for several risk factors and
clinical characteristics inCox regression.Adjusted6-
year event rates increasedwithhigherbaselineorup-
dated mean HbA1c with no J-shaped risk curves, in
all patients and also when subgrouping by shorter
(mean 3 years) or longer (mean 14 years) diabetes
duration, by presence or absence of previousCVD, or
by treatment with oral hypoglycaemic agents (OHAs)
or insulin. Risk reductions of 20% for CHD and 16%
for CVD (P < 0.001) were found in patients with a
baseline mean HbA1c of 6.5%, compared to those
with amean level of 7.5%. Compared to OHA-treated
patients, insulin-treated patients had an increased
riskof totalmortality, duealmost exclusively toan in-
creased risk of non-CVDmortality, and due less to a
weakly significant increased risk of fatalCVD.HbA1c
wasnotassociatedwithnon-CVDmortality.Conclusions. This observational study showed progres-
sively increasing risks ofCHD,CVDand totalmortal-
ity with higher HbA1c, and no risk increase at low
HbA1c levels evenwith longer diabetes duration, pre-
vious CVD or treatment with either insulin or OHAs.
Patients achieving HbA1c <7% showed benefits for
risk reduction.
Keywords: cardiovascular disease, coronary heart dis-
ease,diabetes,HbA1c,myocardial infarction,stroke.
Abbreviations: ACCORD, action to control cardiovascu-
lar risk indiabetes;ADVANCE,action indiabetesand
vascular disease: preterax and diamicron modified
releasecontrolledevaluation;DCCT,diabetescontrol
and complications trial; HPLC, high-performance li-
quid chromatography; ICD, international classifica-
tion of diseases; OHA, oral hypoglycaemic agent; UK
GPRD, United Kingdom General Practice Research
Database; UKPDS, United Kingdom Prospective Dia-
betes Study; VADT, veterans affairs diabetes trial;
WHO,WorldHealthOrganization.
ª 2010 The Association for the Publication of the Journal of InternalMedicine 471
Original Article |
Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
Systolic blood pressure and risk of cardiovascular diseases intype 2 diabetes: an observational study from the Swedishnational diabetes registerJan Cederholma, Soffia Gudbjornsdottirb, Bjorn Eliassonb, Bjorn Zetheliusc,Katarina Eeg-Olofssonb and Peter M. Nilssond, on behalf of the NDRObjectives To estimate risks of fatal/nonfatal coronaryheart disease (CHD), stroke and cardiovascular disease(CVD) with SBP in an observational study of patients withtype 2 diabetes.
Methods Twelve thousand, six hundred and seventy-sevenpatients aged 30–75 years, treated with antihypertensivedrugs, without previous congestive heart failure, followedfor 5 years.
Results Risk curves of CHD and stroke increasedprogressively with higher baseline or updated mean SBP ina Cox model, in all participants, and in two subgroupswithout (nU10304) or with (nU2373) a history of CVD, withno J-shaped risk curves at low SBP levels. Hazard ratios forCHD and stroke per 10-mmHg increase in updated meanSBP in all participants, adjusting for clinical characteristicsand traditional risk factors, were 1.08 (1.04–1.13) and 1.20(1.13–1.27), P<0.001. With updated mean SBP of 110–129mmHg as reference, SBP of at least 140mmHg showedrisk increases of 37% for CHD, 86% for stroke and 44% forCVD (PU0.001 to <0.001), whereas SBP of 130–139mmHgshowed nonsignificant risk increases for these outcomes.With baseline SBP of 110–129mmHg, CHD and CVD risksincreased with further SBP reduction, hazard ratios were1.77 and 1.73 (PU0.002), but decreased considerably forCHD, stroke and CVD with higher baseline SBP.
Conclusion Risks of CHD and stroke increasedprogressively with higher SBP, with no J-shaped curves,although risk increase was significant only for SBP of atleast 140mmHg, but not comparing 130–139 and 110–129mmHg. Additionally, baseline SBP of 110–129mmHgshowed increased CHD and CVD risk with further SBPreduction during follow-up, whereas baseline SBP of atleast 130 showed benefits. J Hypertens 28:2026–2035 Q2010 Wolters Kluwer Health | Lippincott Williams & Wilkins.Journal of Hypertension 2010, 28:2026–2035
Keywords: blood pressure, cardiovascular diseases, diabetes, hypertension,myocardial infarction, stroke
Abbreviations: CHD, coronary heart disease; CVD, cardiovascular disease;NDR, National Diabetes RegisteraDepartment of Public Health and Caring Sciences/Family Medicine and ClinicalEpidemiology, Uppsala University, Uppsala, bDepartment of Medicine,Sahlgrenska University Hospital, Gothenburgh University, Goteborg,cDepartment of Public Health and Caring Sciences/Geriatrics, UppsalaUniversity, Uppsala and dDepartment of Clinical Sciences, Lund University,University Hospital, Malmo, Sweden
Correspondence to Peter M. Nilsson, MD, PhD, Professor of ClinicalCardiovascular Research, Department of Clinical Sciences, Lund University,University Hospital, S-205 02 Malmo, SwedenTel: +46 40 33 24 15; fax: +46 40 92 32 72; e-mail: [email protected] 4 February 2010 Revised 21 May 2010Accepted 27 May 2010
IntroductionHypertension is a well established risk factor for cardio-vascular disease (CVD) in patients with diabetes [1]. Anobservational analysis from the United Kingdom Pro-spective Diabetes Study (UKPDS) [2] has demonstrateda linear relationship between mean in-study SBP and therisk of macrovascular and microvascular complications.Tighter BP control in hypertensive type 2 diabeticpatients, by use of several antihypertensive drug classesversus placebo, has been documented to reduce the riskof both microvascular and macrovascular disease, in theUKPDS [3,4] as well as in several other interventionstudies [5–8]. Guidelines have, therefore, advocated atreatment target of BP below 130/80mmHg for patientswith type 2 diabetes [9–11]. However, the recent Euro-pean guidelines in 2009 from the European Society ofHypertension (ESH) [12] recommend that patients withdiabetes should lower SBP well below 140mmHg, with-out mentioning a specific lowest target.
Against this background, we assessed the associationbetween SBP and risk of coronary heart disease(CHD), stroke and CVD, also with regard to lower andhigher SBP levels, in an observational study of patientswith type 2 diabetes on routine treatment with antihy-pertensive drugs from a national diabetes register (NDR).Patients and methodsThe Swedish national diabetes registerThe NDR was initiated in 1996 as a tool for local qualityassurance and feedback in diabetes care. Annual reportingto theNDR is carried out by trained physicians and nursesvia the Internet or via clinical records databases, withinformation collected during patient visits at hospital out-patient clinics and primary healthcare centres nationwide.All included patients have agreed by informed consent toregister before inclusion. The Regional Ethics ReviewBoard at the University of Gothenburg approved thisstudy. Several reports [13–18] concerning trends in risk
2026 Original article
0263-6352 � 2010 Wolters Kluwer Health | Lippincott Williams & WilkinsDOI:10.1097/HJH.0b013e32833c8b75
© 2009 The Authors.
Journal compilation © 2009 Diabetes UK.
Diabetic Medicine
,
26
, 53–60
53
DIABETIC
Medicine
DOI: 10.1111/j.1464-5491.2008.02633.x
Blackwell Publishing Ltd
Original Article: Complications
Risk factor control in patients with Type 2 diabetes and
coronary heart disease: findings from the Swedish
National Diabetes Register (NDR)
S. Gudbjörnsdottir, K. Eeg-Olofsson, J. Cederholm*, B. Zethelius†, B. Eliasson and
P. M. Nilsson‡, on behalf of the Swedish National Diabetes Register (NDR)
Department of Medicine, Sahlgrenska University Hospital, Göteborg University, Göteborg, *Department of Public Health and Caring Sciences, Family Medicine and
Clinical Epidemiology and †Department of Public Health and Caring Sciences, Geriatrics, Uppsala University, Uppsala, and ‡Department of Clinical Sciences, Lund
University, University Hospital, Malmö, Sweden
Accepted 30 October 2008
Abstract
Aims
Patients with Type 2 diabetes and coronary heart disease (CHD) are infrequently treated to risk factor targets in current
guidelines. We aimed to examine risk factor management and control levels in a large sample of patients with Type 2 diabetes
with CHD.
Methods
This was an observational study of 1612 patients with first incidence of CHD before 2002, and of 4570 patients
with first incidence of CHD before 2005, from the Swedish National Diabetes Register (NDR).
Results
In patients with CHD 1–2 years before follow-up, the achievement of cardiovascular risk factor targets
(follow-up 2002/follow-up 2005) was: HbA
1c
<
7%, 47%/54% (
P
<
0.01); blood pressure
≤
130/80 mmHg, 31%/40%
(
P
<
0.001); total cholesterol
<
4.5 mmol/l, 47%/60% (
P
<
0.001); and low-density lipoprotein-cholesterol
<
2.5 mmol/l,
49%/65% (
P
<
0.001). Use of medication: antihypertensives, 90%/94% (
P
<
0.01); lipid-lowering drugs, 75%/86%
(
P
<
0.001); and aspirin, 85%/89% (
P
<
0.05). A high prevalence of adverse lifestyle characteristics prevailed (2002/
2005): overweight [body mass index (BMI)
≥
25 kg/m
2
], 86%/85%; obesity (BMI
≥
30 kg/m
2
), 41%/42%; smokers in age
group
<
65 years, 16–23%/18–19%; as well as waist circumference
≥
102 cm (men) or
≥
88 cm (women), 68% in 2005.
Conclusions
Patients with a combination of Type 2 diabetes and CHD showed an increased use of lipid-lowering drugs
over time, corresponding to improving blood lipid levels. A discrepancy existed between the prevalent use of antihypertensive
drugs and the low proportion reaching blood pressure targets. Regretfully, a high prevalence of adverse lifestyle characteristics
prevailed. Evidence-based therapy with professional lifestyle intervention and drugs seems urgent for improved quality
of secondary prevention in these patients.
Diabet. Med. 26, 53–60 (2009)
Keywords
coronary heart disease, diabetes mellitus, hyperlipidaemia, hypertension, secondary prevention
Abbreviations
BMI, body mass index; BP, blood pressure; CHD, coronary heart disease; DCCT, Diabetes Control and
Complications Trial; HDL, high-density lipoprotein; LDL, low-density lipoprotein; MI, myocardial infarction; NDR,
National Diabetes Register; PHC, primary healthcare; RIKS-HIA, Register of Information and Knowledge about Swedish
Heart Intensive Care Admission
Introduction
The risk of coronary heart disease (CHD) is substantially
increased in patients with Type 2 diabetes [1,2]. Furthermore,
mortality 1 year after CHD is higher in patients with vs.
without diabetes [3]. Glycaemic control can reduce the
risk of microvascular end-points [4], and myocardial infarc-
tion (MI) if metformin is used [5]. The importance of treat-
ment with antihypertensive, lipid-lowering and antiplatelet
drugs for primary prevention of cardiovascular disease has
also been documented [6–8]. Recently the benefit of statin
use in patients with diabetes was high-lighted in a meta-
analysis by the Cholesterol Treatment Trialists’ Collaborators
[9].
Correspondence to
: Peter M. Nilsson, MD, PhD, Department of Clinical
Sciences, Lund University, University Hospital, S-205 02 Malmö, Sweden.
E-mail: [email protected]
dme_2633.fm Page 53 Thursday, December 25, 2008 2:27 PM

4 | Annual Report 2013
The Swedish National Diabetes Register (NDR) serves as a useful tool for providers of everyday care Chronic diseases place a heavy burden not only on patients and their families, but on healthcare systems around the world. Such pressure on the infrastructure and organisation of the systems often leads to poor management of chronic conditions. The resulting complications reduce quality of life and dramatically increase healthcare costs. The personal and social repercussions are enormous. Diabetes management has a number of dimensions, each of which is multifaceted in itself. Thus, patients should receive advice from a wide range of skilled professionals who are working together. A diabetes centre is an important resource that permits a multidisciplinary team to communicate effectively while providing consistent, reliable counselling. In addition, an individual care plan should be set up on the basis of the patient’s particular needs and circumstances.
A clinical, practicebased population register can be used to support structural care and identify patients who may not be complying with their medication regimen, exposing them to risk of inadequate diabetes control.
The NDR was launched in 1996 for the purpose of promoting evidencebased development of diabetes care by offering uptodate information about changes in the treatment of glycaemia and other risk factors, as well as diabetic complications. Another aim is to support improvement in the quality of care provided by participating units at hospitals and primary care clinics. The overall objective is to reduce morbidity and mortality, as well as to maximise the costeffectiveness of diabetes care. The NDR is maintained by the Swedish Society for Diabetology on behalf, and with the financial support, and the Swedish Association of Local Authorities and Regions. The Swedish Diabetes Association, a patient advocacy group, actively uses the NDR as well.
The NDR has been online since April 2002 (www.ndr.nu), allowing individual clinics to quickly monitor their activities on a regular basis by virtue of immediate access to their own results, as well as national statistics for purposes of comparison.
The NDR, which has been an integral part of Swedish diabetes care for the past 18 years, has engaged the participation of both hospitals and primary care clinics. The register offers a unique opportunity to monitor the quality of care in terms of risk factors and the potential complications of diabetes, as well as the evolution of treatment methods. The results generated by the register have been presented at many international meetings and conferences. To our knowledge, the NDR is the largest diabetes register in the world.
Because the course of diabetes is complex and lifelong, both clinical practice and quality control of treatment measures must reflect systematic adherence to various guidelines. The NDR is an instrument to facilitate such monitoring and to disseminate findings in an accessible, transparent, comparable and timely manner. The register is both a repository of results and an educational tool for improving local quality assessment efforts. The register enables a focus on national quality indicators while following various process measures that are important at the local level. Diabetes care is largely selfmanaged. The NDR also promotes and facilitates the influence and participation of patients in their care and treatment. For example, patients can actively monitor data about their interactions with healthcare providers.
Improved diabetes care minimises risk factors and the incidence of complications. The result is less human suffering and greater social cost benefits. The findings of the proposed projects may prove highly useful during an implementation process that involves continuous monitoring of the performance of an individual diabetes care unit.

Annual Report 2013 | 5
The NDR has established itself as a wellfunctioning tool to promote improvement efforts in the field of diabetes care. Documented evidence suggests that use of the register leads to better longterm outcomes. The critical factors for success are the emergence of healthcare systems in which measuring results is integral to the overall process, as well as training the entire team to participate in the improvement effort. Another factor that is crucial to the effectiveness of the project is the commitment of providers to measuring results, collecting data and discussing what they have learned.
The NDR is used extensively throughout the country. NDRIQ and other ongoing improvement projects ensure the promulgation of new working methods, along with evidencebased approaches to ensuring progress and improvement.

6 | Annual Report 2013
Participation and reporting in 2013Participation rate Populationbased data were obtained from the Swedish National Diabetes Register (NDR). The Swedish NDR was initiated in 1996 as a tool for quality assurance in diabetes care. National results are published in yearly reports and the register is administrated from Centre of Registers in Region Västra Götaland, Gothenburg, Sweden (www.NDR.nu) Reporting to the register is not mandatory, but all specialist clinics and primary healthcare centres are encouraged to do so. Today 100% of specialist clinics and 95% of primary health care centres participate. More than 352,000 patients were reported to the register in 2013, representing approximately 88% of adult patients with diabetes in Sweden. Annual reporting to the NDR is carried out by trained physicians and nurses via the Internet or via clinical records databases, with information collected during patient visits at specialist clinics and primary health care centres nationwide. All included patients have agreed by informed consent to register before inclusion. In Sweden almost all patients with type 1 diabetes receive their treatment at specialist clinics. We estimate that approximately 90% of all adult patients with type 1 diabetes, were reported to the NDR in 2013. Furthermore, a recent study showed the prescribed drug register (PDR), which contains data on every prescription filled in Sweden since 1 July 2005 was matched with the NDR amongst the type 1 diabetes 18–34 age group with 91% precision for 2007–2009. (Rashwani et al. 2014. The incidence of diabetes among 034 year olds in Sweden: new data and better methods. Diabetologia. Apr 9.
Approximately 4% of Swedes have diabetes, though the prevalence varies from one county to another. Type 2 diabetes represents approximately 90% of all cases. On average men are younger when they develop the disease than women. Figure 1 shows the number of patients who participated in 1996–2013, broken down by primary care and specialist clinics. The total increased again in 2013 to 352,388. The register received reports in 2013 from all counties, all 90 specialist clinics and 1,246 primary care clinics (better than 90% altogether).
Thus, approximately 90% of all Swedish people with diabetes were entered in the register in 2013, allowing for highly representative data in general, though varying from county to county (see Figure 2). A number of diabetics in each county do not appear in the Prescribed Drug Register because they receive dietary treatment only.
Participation rate among people with diabetes receiving medication – comparison between the NDR and Prescribed Drug Register
To obtain an even more accurate estimate of the participation rate, we performed a comparison with the Prescribed Drug Register of the National Board of Health and Welfare. Figure 2 compares Swedes age 50–80 who picked up prescriptions for diabetes medications (tablets or insulin) in 2012 with the NDR for 2012 and 2013). The NDR contains more than 88% of patients nationwide and more than 90% in many counties.

Annual Report 2013 | 7
0
50,000
100,000
150,000
200,000
250,000
300,000
350,000
400,000
20132012201120102009200820072006200520042003200220011999199819971996
Primary care TotalSpecialist clinics
Figure 1. Number of patients entered in NDR, 1996–2013.
Number of patients
346,679 352,388
333,150
50,557 50,57649,199
301,812
283,951296,122
Source: NDR – Swedish National Diabetes Register.
0
10
20
30
40
50
60
70
80
90
100
Natio
nwid
e
Västra
Göta
land
Västm
anla
nd
Kronober
g
Kalm
ar
Österg
ötland
Örebro
Värm
land
Jäm
tland
Stock
holmSk
åne
Väste
rnorrl
and
Jönkö
ping
Sörm
land
Dalar
na
Väste
rbott
en
Gävle
borg
Bleki
nge
Halla
nd
Norrbott
en
Uppsala
Gotland
Figure 2. Comparison between the NDR and the Prescribed Drug Register. People age 50–80 entered in the Prescribed Drug Register on 1 January–31 December 2012 and in the NDR in 2012–2013. Matching based on unique Swedish personal identity numbers.
%
Source: NDR – Swedish National Diabetes Register.

8 | Annual Report 2013
Observations by the Patient Advocacy Group From the earliest days of the NDR, the Swedish Diabetes Association has been an active participant and vigorously promoted the inclusion of as many patients as possible. We are gratified to note that the participation rate has steadily grown to a very impressive level, We now have a means of verifying the quality of Swedish diabetes care and identifying areas for improvement at both the county and clinic level. The register serves as a solid foundation for setting priorities and designing various programmes. The results are useful not only for clinics and county councils, but for individual patients as a tool for evaluating the care and treatment they receive.
The traditional focus of the NDR on medical care is wholly understandable. While relatively unknown at one time, concepts such as empowerment and patient influence are now mandatory items on the healthcare agenda. Diabetes is a quintessential example of that trend, given that is predominantly a matter of selfcare and individual decision making on both everyday and special occasions when it comes to diet, medication, exercise, social activities and the full gamut of modern life. The NDR have done a number of patient reported outcome measure (PROM) projects. For that we can only be thankful, but the process is evolving much too slowly. The time has come to graduate from projects to the real world. From our point of view, the issue isn't the best way to ask patients what they think of their caregivers, but to explore the treatment options and tools they have at their disposal to manage their condition and maximise their quality of life. Such considerations determine not only the ultimate wellbeing and outcomes of each patient, but the successes and failures of diabetes care as a whole.
Another area that requires urgent attention is reporting of data about the use of insulin pumps, continuous glucose monitoring (CGM) systems and other medical devices. Entering such data will quickly generate facts about the impact of the devices on such variables as HbA1c levels and quality of life. There is no doubt in our minds that this information would rechannel public discussion from the current overemphasis on shortterm economic gain to the longterm benefits for patients, the healthcare system and the community at large. Above all, more Swedes would have the opportunity to share the fruits of technological progress.
The Diabetes Association wholeheartedly supports this year's decision to publish register results online and present them at the clinic level. At long last we will have access to hard data. In fact, the association would like to take the next step and publish the names of the individual clinics. We believe the fear that patients will switch clinics is considerably overblown. As is the case with all statistics, the challenge is to use common sense without losing sight of possible sources of error. The great majority of diabetics will continue to choose the primary care and specialist clinic closest to home. Ensuring that all patients have access to the same information is a democratic imperative. It goes without saying that we want to maximise our options for lobbying and advocacy, but protecting the right of individual patients to make choices and affect the care they receive is equally important. We have no interest in witch hunting or blacklisting clinics that report inferior results but rather in making a positive contribution to quality assessment efforts. The Diabetes Association is fully aware that the Swedish healthcare system is unaccustomed to the publication of data at the clinic level. Nevertheless, clear communication about the true import of the information should allay any concerns and fears that either we or the media may have.
Fredrik Löndahl, President Swedish Diabetes Association

Annual Report 2013 | 9
Nationwide results for 2009–2013This section presents nationwide results over time. We have selected a number of indicators – additional results appear on our website. For the first time, we have included a life expectancy analysis for type 1 diabetics, including a comparison with the general population.
The annual report of the NDR evaluates diabetes care in relation to the guidelines of the National Board of Health and Welfare while shedding light on patient populations, treatments, results and processes. The objectives of diabetes treatment should be individualised on the basis of each patient's circumstances.
Instead of a single target level, the following discussion often presents averages, proportions and several different targets. Particular patient populations are highlighted.
Number of patients and classification of diabetesThe results are presented for specialist clinics broken down by clinical classification of diabetes. All diabetics in primary care are reported as one group. A total of 97% of patients treated at specialist clinics have been clinically classified. A total of 97% of patients in primary care have been classified as type 2 diabetics, while only 3% developed the disease when they were younger than 40 and are receiving insulin treatment. Thus, the annual report regards patients in primary care as synonymous with type 2 diabetics.
NDR's scientific reports define type 1 diabetics epidemiologically as patients with onset when they were younger than 30 and have insulin treatment only. Type 2 diabetics, on the other hand, are defined epidemiologically as patients age 40 or older who are receiving 1) dietary treatment or taking tablets only, or 2) insulin treatment, whether or not they are taking tablets. This breakdown has proven to coincide very well with the clinical classification in the NDR. However, a few percent of patients whom the register classifies epidemiologically as type 2 diabetics have latent autoimmune diabetes in adults (LADA).
In Sweden almost all patients with type 1 diabetes attend specialist clinics, i.e., outpatient clinics with specialists in diabetology/endocrinology. These clinics also care for patients with complicated type 2 diabetes or many patients with secondary diabetes. Most patients with type 2 diabetes attend primary care, and are seen by general practitioners and diabetes nurses/educators.
The three patient populations are:
• All patients in primary care
• Type 1 diabetics treated at specialist clinics
• Type 2 diabetics treated at specialist clinics
Tables 1a–c describe the clinical characteristics of the three populations. Type 2 diabetics have a higher average age and shorter disease duration in primary care than at specialist clinics. The fact that specialist clinics are reporting fewer and fewer type 2 diabetics suggests that primary care is assuming increasing responsibility for this population.

10 | Annual Report 2013
Table 1a. Patients with diabetes in primary care: number, mean age, duration, men.
2009 2010 2011 2012 2013
Number 219,588 259,560 281,729 296,835 303,403
Mean age (SD) 67.8 (11.9) 67.9 (12.1) 68 (12.1) 68.1 (12.1) 68.2 (11.9)
Mean duration, years (SD) 8.7 (7.9) 8,8 (7.9) 8,9 (8) 9.2 (8.1) 9,5 (8,1)
Men (%) 121,639 (55.4) 143,961 (55.5) 157,263 (55.8) 166,848 (56.2) 172,081 (56.7)
Source: NDR – Swedish National Diabetes Register.
Table 1b. Patients with type 1 diabetes at specialist clinics: number, mean age, duration, men.
2009 2010 2011 2012 2013
Number 30,683 31,291 33,399 34,776 36,126
Mean age (SD) 46 (15.8) 45.9 (16.0) 45.7 (16.3) 45.7 (16.5) 45.9 (16.7)
Mean duration, years (SD) 23.1 (14.7) 23.1 (14.8) 23.2 (14.9) 23.2 (15.0) 23.5 (15.2)
Men (%) 17,069 (55.6) 17,421 (55.7) 18,790 (56.3) 19,491 (56) 20,170 (55.8)
Source: NDR – Swedish National Diabetes Register.
Table 1c. Patients with type 2 diabetes at specialist clinics: number, mean age, duration, men.
2009 2010 2011 2012 2013
Number 12,775 12,221 12,068 10,876 10,146
Mean age (SD) 62.4 (12.6) 62.6 (12.6) 62.5 (12.7) 62.6 (12.7) 62.6 (12.8)
Mean duration, years (SD) 13.9 (9.7) 14.2 (9.8) 14.5 (9.9) 15.2 (10.0) 15.4 (10.0)
Men (%) 8,216 (64.3) 7,922 (64.8) 7,757 (64.3) 7,062 (64.9) 6,505 (64.1)
Source: NDR – Swedish National Diabetes Register.

Annual Report 2013 | 11
Table 2a. Recently diagnosed patients in primary care. Clinical characteristics at onset.
2009 2010 2011 2012 2013
Number 13,391 16,676 16,964 16,614 14,416
Mean age (SD) 62.9 (12.5) 62.8 (12.6) 62.9 (12.5) 62.8 (12.5) 62.8 (12.7)
Number HbA1c 12,687 15,518 16,013 16,144 14,107
Mean HbA1c, mmol/mol (SD) 52.1 (14.9) 52.4 (14.9) 52.3 (15.5) 52.8 (15.7) 51.7 (15.5)
Number BMI 10,944 13,552 14,381 14,545 12,789
Mean BMI, kg/sq m (SD) 30.6 (5.7) 30.6 (5.7) 30.6 (5.6) 30.8 (5.7) 30.7 (5.7)
Source: NDR – Swedish National Diabetes Register.
Table 2b. Recently diagnosed adults with type 1 diabetes at specialist clinics. Clinical characteristics at onset.
2009 2010 2011 2012 2013
Number 403 397 398 409 356
Mean age (SD) 37.4 (14.8) 36.6 (15.1) 37.1 (15.4) 35.6 (14.8) 33.8 (13.3)
Number HbA1c 380 366 382 386 343
Mean HbA1c, mmol/mol (SD) 54.9 (17.1) 57.4 (19.9) 56.6 (18.4) 55.5 (17.8) 53.4 (16.8)
Number BMI 329 341 344 337 298
Mean BMI, kg/sq m (SD) 24.5 (4.4) 24.6 (3.7) 24.6 (4.3) 24.3 (4) 24.1 (4)
Source: NDR – Swedish National Diabetes Register.
Table 2c. Recently diagnosed adults with type 2 diabetes at specialist clinics. Clinical characteristics at onset.
2009 2010 2011 2012 2013
Number 339 347 307 229 214
Mean age (SD) 53.9 (13.3) 54.3 (14.1) 54.9 (14.1) 52.9 (14.4) 52.6 (15.8)
Number HbA1c 314 316 291 211 205
Mean HbA1c, mmol/mol (SD) 53.9 (15.2) 52.3 (15.3) 55.8 (19) 57 (20.9) 55.7 (18.8)
Number BMI 262 261 244 195 183
Mean BMI, kg/sq m (SD) 29.9 (5.4) 30 (5.7) 30 (5.4) 29.7 (5.9) 29.4 (5.6)
Source: NDR – Swedish National Diabetes Register.

12 | Annual Report 2013
Figure 3–5 shows the age breakdown for primary care, as well as type 1 and type 2 diabetics treated at specialist clinics, in 2013. As was the case in 2012, specialist clinics are treating many young adults with type 1 diabetes as a result of higher prevalence among children and adolescents.
Life expectancy of type 1 diabetics
The figure (Figure 6) shows the life expectancy among patients with type 1 diabetes (those who developed the disease before the age of 30 and are receiving insulin) for the six age groups between 40 to 69. Life expectancy increased for all groups from 2005 to 2010. For comparison purposes, the life expectancy of the general Swedish population, also broken down by age group, is presented for the same years. The greater increase in the life expectancy among patients with type 1 diabetes than of the general population was statistically significant.
One reason for the increased life expectancy among patients with type 1 diabetes may be improvements in the treatment of hypertension, high blood lipid levels and other risk factors for cardiovascular and kidney disease. Changes in BMI, physical activity and other lifestyle factors may also have played a role. Better control of HbA1c levels by means of injections or insulin pumps may also have contributed. The way that the healthcare system is structured to treat patients with type 1 diabetes is also important when it comes to both inpatient and outpatient care, including teams of professionals and specially trained diabetes nurses. The widespread use of the NDR by clinics since 2005 to report among patients with type 1 diabetes has created new opportunities for structured monitoring of the care provided at the local level.
Remaining life expectancy is based on actuarial tables. The basic variables are the size of the population and the number of deaths for various ages during the year in question.
0
3
4
1
2
5
6
7
8
%
Figure 4. Histogram by age. Patients with type 2 diabetes at specialist clinics, 2013.
15 19 23 27 31 35 39 43 47 51 55 59 63 67 71 75 79 83 87 91 95 99 103
N 10,146Mean 62.58269Std Deviation 12.83742Maximum 95Minimum 18
Age
Source: NDR – Swedish National Diabetes Register.
0
3
4
1
2
5
6
7
8
%
Age
Figure 3. Histogram by age. Patients with diabetes in primary care, 2013.
N 303,403Mean 68.19149Std Deviation 11.9385Maximum 104Minimum 18
15 19 23 27 31 35 39 43 47 51 55 59 63 67 71 75 79 83 87 91 95 99 103
Source: NDR – Swedish National Diabetes Register.
0
2
1
4
3
5
%
Figure 5. Histogram by age. Patients with type 1 diabetes at specialist clinics, 2013.
N 36,126Mean 45.9375Std Deviation 16.68745Maximum 94Minimum 18
15 19 23 27 31 35 39 43 47 51 55 59 63 67 71 75 79 83 87 91 95 99 103
Age
Source: NDR – Swedish National Diabetes Register.

Annual Report 2013 | 13
LifestylePrevalence of overweight and obesity not rising but very high
The proportion of women and men with type 2 diabetes who are overweight or obese has not risen significantly in recent years. Nevertheless, approximately 47% of women and 40.5% of men still suffer from obesity. Figures 7a–7b and Figure 8 show body mass index (BMI) trends in 2009–2013. Only 15.7% of type 2 diabetics treated at specialist clinics and 17.7% in primary care had normal weights (BMI < 25 kg/sq m).
0
10
20
30
40
65–6960–6455–5950–5445–4940–44Age
Type 1 diabetes, 2005 Type 1 diabetes, 2010 Entire population, 2005 Entire population, 2010
Figure 6. Life expectancy, type 1 diabetes.
%
2729
33 33
2325
28 28
1921
23 24
15 16
19 19
11 1214 14
8 9 10 10
Sources: Register Service, Swedish National Board of Health and Welfare, and NDR – Swedish National Diabetes Register.
0
10
20
30
40
50
20132012201120102009
Figure 7a. Mean BMI, women.
Primary care Specialist clinicstype 2 diabetes
Specialist clinicstype 1 diabetes
kg/sq m
25.5 25.6 25.7 25.7 25.8
30.6 30.7 30.8 30.6 30.5
30.1 30.2 30.2 30.2 30.1
Source: NDR – Swedish National Diabetes Register.
0
10
20
30
40
50
20132012201120102009
Figure 7b. Mean BMI, men.
Primary care Specialist clinicstype 2 diabetes
Specialist clinicstype 1 diabetes
kg/sq m
25.9 25.9 25.9 26.0 26.0
30.1 30.2 30.2 30.2 30.1
29.4 29.5 29.4 29.5 29.4
Source: NDR – Swedish National Diabetes Register.
Specialist clinics type 1 diabetes
Specialist clinics type 2 diabetes
Primary care
0
20
40
60
80
100
201320122011201020132012201120102013201220112010
Figure 8. BMI by intervals.
%
≥ 40 kg/sq m 35–39 kg/sq m 30–34 kg/sq m
25–29 kg/sq m < 25 kg/sq m
4.5 4.4 4.4
27.6 27.8 27.8
39.9 39.7 39.8
17.2 17.4 17.4
0.7 0.6 0.65.2 5.4 5.4
10.8 10.6 10.7
4.4
27.6
39.7
17.7
10.6
2.5 2.4 2.7
11.2 11.5 11.7
38.5 38.6 38.5
47.1 46.9 46.6
0.72.6
11.9
38.3
46.4
12.8 12.4 12.9
29.9 30.7 29.9
36.9 37.2 36.8
15.1 14.3 15.0
5.1
12.8
29.9
36.5
15.7
Source: NDR – Swedish National Diabetes Register.

14 | Annual Report 2013
0
20
40
60
80
100
120
20132012201120102009
Figure 9a. Mean waist circumference, women.
cm
Primary care Specialist clinicstype 2 diabetes
Specialist clinicstype 1 diabetes
86.0 86.2 86.2 86.4 86.2
102.0 102.5 102.9 102.5 102.1
100.2 100.7 100.8 101.0 101.0
Source: NDR – Swedish National Diabetes Register.
0
20
40
60
80
100
120
20132012201120102009
cm
Figure 9b. Mean waist circumference, men.
Primary care Specialist clinicstype 2 diabetes
Specialist clinicstype 1 diabetes
94.9 94.7 94.9 95.1 95.2
108.6 108.4 108.7 109.0 108.6
106.2 106.6 106.7 106.8 106.9
Source: NDR – Swedish National Diabetes Register.
Physical activity protects against risk factors
The largestever observational study, conducted by the NDR, of physical activity among patients with type 2 diabetes found that both women and men can substantially reduce the risk of cardiovascular disease and premature death by exercising regularly.
The results clearly indicated that these patients have the power to improve their own prognoses by staying physically active and eliminating sedentary habits.
Type 2 diabetes increases the risk of cardiovascular disease. Medical research has established that physical activity reduces the risk of myocardial infarct, stroke and a number of other diseases in the general population. We launched a study to quantify the extent to which patients with type 2 diabetes, who by definition are at elevated risk of cardiovascular disease, can take advantage of these positive health effects.
The study was based on NDR data for more than 15,000 women and men with type 2 diabetes. Responses to questions about level of physical activity are entered in the NDR each year. None of the participants had cardiac infarct, stroke or another cardiovascular disease at baseline, but 750 of them developed one within the fiveyear followup period. A total of 427 participants died during the period, most of them at age 60–70.
Both cardiovascular disease and premature death were much more common among participants who exercised no more than the equivalent of two 30minute walks per week than those with higher levels of physical activity. The results of the study showed that it is never too late to adopt a healthier lifestyle. Participants who exercised very little at baseline and became more physically active during the followup period exhibited the most pronounced protection against the risk factors for cardiovascular disease and premature death.
Their risk decreased by 50% compared with participants who remained physically inactive. In addition to a healthy diet, elimination of sedentary habits and regular physical activity are among the cornerstones of nonpharmacological treatment for type 2 diabetes. Because the disease is so common, greater awareness in this respect benefits public health as well. A number of international media, as well as the website of the European Society of Cardiology (www.escardio.org), featured the study.
Many are physically inactive
The trend line in Figure 10 goes between patients who exercise regularly (at least three times a week) and those who do not. Patients with type 1 and type 2 diabetes at specialist clinics trended slightly downward.
Specialist clinics type 1 diabetes
Specialist clinics type 2 diabetes
Primary care
0
20
40
60
80
100
201320122011201020132012201120102013201220112010
Figure 10. Physical leisure activities.
%
Never <1 time/week 1–2 times/week
3–5 times/week Daily
15.8 16.8 16.0
21.7 21.5 20.7
22.2 22.9 22.9
27.3 27.2 28.4
8.3 7.0 7.320.1 18.8 18.5
13.0 11.6 11.8
16.3
20.3
22.4
28.7
12.211.8 15.4 14.8
24.1 24.3 23.8
28.7 28.4 29.2
27.1 24.8 24.9
7.7
13.8
23.4
30.3
24.7
14.7 16.6 18.3
21.9 22.1 21.1
20.2 19.8 20.0
23.1 22.8 22.0
20.5
16.5
21.8
20.7
20.4
Source: NDR – Swedish National Diabetes Register.

Annual Report 2013 | 15
Patients with diabetes are smoking less
The percentage of smokers in primary care declined again in 2013 (Figures 11–12), regardless of gender or age (60, younger or older). Patients with diabetes are smoking less as well, but 13% of women and 10.8% of men have not quit yet.
0
5
10
15
20
25
30
20132012201120102009
Figure 11. Women and men in primary care < age 60 and ≥ age 60 who smoke.
%
Men ≥ age 60
Men < age 60
Women ≥ age 60
Women < age 60
25.2 25.5
25.624.0
22.8
12.9 13.3 13.4 12.8 12.2
25.7 25.7
25.323.1 22.6
11.7 12.1 12.4 12.0 11.7
Source: NDR – Swedish National Diabetes Register.
0
2
4
6
8
10
12
14
16
20132012201120102009
Figure 12. Type 1 diabetes patients at specialist clinics who smoke.
%
Men Women All
11.2 11.5 11.2 11.0 10.8
13.9
12.4 12.5 12.4 12.111.8
13.7 13.8 13.4 13.0
Source: NDR – Swedish National Diabetes Register.
Patients with type 2 diabetes who are relatively young
More than one in five 30–60 yearolds smoke and one in four are physically inactive (Figure 13). A total of 51.7% of men and 59.4% of women have BMI ≥ 30 kg/sq m.
Figure 13. Smokers, BMI ≥ 30 kg/sq m and physically inactive patients age 30–60 in primary care, 2013.
Men: 43,863 Women: 27,881
* Physical leisure activity ≤ 1 time/week
Smokers22.6%
Smokers22.7%
BMI ≥ 30 51.7% BMI ≥ 30
59.4%
Physically inactive*
25.7%
Physically inactive*
27.0%
Source: NDR – Swedish National Diabetes Register.

16 | Annual Report 2013
HbA1c trend
HbA1c levels have held steady or shown a negative trend in recent years. The negative trend reversed in 2013 (Figures 16–20) for all populations – with the exception of patients with type 2 diabetes treated at medical clinics who have had the disease for a short period of time, possibly reflecting the fact that their numbers have declined and that the ones who have remained have more severe cases. Thus, the trend has been positive both for patients with type 1 diabetes and for primary care as a whole.
Distribution of HbA1c levels
Figures 14–15 contain distribution curves and histograms for the most recent HbA1c levels among patients with type 1 and type 2 respectively.
0,0
2,5
7,5
5,0
10,0
12,5
15,0
%
HbA1c (mmol/mol)
25 30 35 40 45 50 55 60 65 70 75 80 85 90 95 100 105 110 115 120
N 43,799Mean 63.99934Std Deviation 14.50583Maximum 144Minimum 26
Figure 14. Histogram for HbA1c (mmol/mol). All patients with type 1 diabetes, 2013.
Source: NDR – Swedish National Diabetes Register.
0
5
10
15
20
%
HbA1c (mmol/mol)
25 30 35 40 45 50 55 60 65 70 75 80 85 90 95 100 105 110
N 28,7939Mean 54.13897Std Deviation 14.00891Maximum 145Minimum 26
Figure 15. Histogram for HbA1c (mmol/mol). All patients with type 2 diabetes, 2013.
Source: NDR – Swedish National Diabetes Register.
40
45
50
55
60
65
70
75
80
2013
2012
2011
2010
2009
2008
2007
2006
2005
2004
2003
2002
2001
2000
1999
1998
1997
1996
Figure 16. Mean for HbA1c (mmol/mol).mmol/mol
Specialist clinics, type 2 diabetes
Primary care Specialist clinics, type 1 diabetes
61.4
67.5
68.5
60.7
66.7
67.4
59.3
64.8
65.3
58.456.4
54.8 55.3 54.4 53.4 53.4 52.8 53.6 53.9 54.6 54.6 54.9 54.1
64.2
65.2
57.2
63.8 63 62 62.7 61.960.6 60.7 60.1 60.8 60.5 61 61.5 62.6 62
64.8 64.4 63.9 64.7 63.9 63.2 63.1 62.9 63.7 63.7 64.2 64.9 65.3 64.3
Source: NDR – Swedish National Diabetes Register.
30
40
50
60
70
20132012201120102009
Figure 17. Mean for HbA1c (mmol/mol). mmol/mol
Primary care Specialist clinics, type 2 diabetes
Specialist clinics, type 1 diabetes
63.7 64.2 64.9 65.3 64.3
60.5 61.0 61.5 62.6 62.0
53.9 54.6 54.6 54.9 54.1
Source: NDR – Swedish National Diabetes Register.

Annual Report 2013 | 17
0
20
40
60
80
100
20132012201120102009
Figure 18. HbA1c < 52 (mmol/mol). %
Primary care Specialist clinics, type 2 diabetes
Specialist clinics, type 1 diabetes
51.7
31.8
17.5
49.5
30.2
16.1
49.7
29.8
15.2
49.1
26.7
14.6
52.2
28.8
16.9
Source: NDR – Swedish National Diabetes Register.
0
10
20
30
40
50
20132012201120102009
Figure 19. HbA1c >73 (mmol/mol). %
Primary care Specialist clinics, type 2 diabetes
Specialist clinics, type 1 diabetes
7.7
18.1
20.3
8.6
18.7
21.6
9.0
19.7
23.3
9.6
22.1
24.0
9.3
21.6
22.1
Source: NDR – Swedish National Diabetes Register.
0
20
40
60
80
100
20132012201120102009
Figure 20. HbA1c < 52 (mmol/mol) among patients < age 70 and diabetes duration ≤ 3 years.
%
Primary care Specialist clinics, type 2 diabetes
60.0 58.2 57.1 55.9 58.6
67.1 65.6 66.0 65.5 68.5
Source: NDR – Swedish National Diabetes Register.

18 | Annual Report 2013
Patients with HbA1c levels above 73 mmol/mol
Tables 3ac show the clinical characteristics of this population.
Table 3b. Patients with HbA1c > 73 (mmol/mol). Type 1 diabetes at specialist clinics.
2009 2010 2011 2012 2013
Number 6,095 6,614 7,620 8,193 7,861
Mean age (SD) 44.2 (15.5) 44 (15.9) 43.6 (16.1) 43.8 (16.4) 44.1 (16.6)
Number (HbA1c) 6,095 6,614 7,620 8,193 7,861
Mean HbA1c, mmol/mol (SD) 83.7 (10.3) 83.5 (10.0) 83.8 (10.0) 84.1 (10.5) 84.3 (10.6)
Number (systolic blood pressure mm Hg) (SD) 5,818 6,341 7,252 7,780 7,546
Mean systolic blood pressure 127.6 (15.9) 127.2 (15.8) 126.7 (15.4) 126.6 (15.4) 126.9 (15.0)
Number (LDL) 4,716 5,095 5,875 6,399 6,048
Mean LDL, mmol/l (SD) 2.8 (0.9) 2.8 (0.9) 2.7 (0.9) 2.7 (0.9) 2.7 (0.9)
Number (BMI) 5531 6061 6827 7365 7071
Mean BMI, kg/sq m (SD) 26.2 (4.6) 26.2 (4.7) 26.2 (4.7) 26.2 (4.6) 26.4 (4.8)
Number of smokers (%) 1,078 (19.2) 1,210 (19.6) 1,341 (19.2) 1,447 (18.9) 1,399 (19.5)
Number of physically inactive patients (%) 1,259 (27.1) 1,531 (29.1) 1,907 (30.4) 2,039 (29.7) 2,004 (29.8)
Source: NDR – Swedish National Diabetes Register.
Table 3a. Patients with HbA1c > 73 (mmol/mol). Primary care.
2009 2010 2011 2012 2013
Number 16,079 21,158 24,067 27,376 27,139
Mean age (SD) 64.3 (13.1) 64.8 (13.4) 65 (13.3) 65.4 (13.4) 65.5 (13.3)
Number (HbA1c) 16,079 21,158 24,067 27,376 27,139
Mean HbA1c, mmol/mol (SD) 85.3 (11.6) 85.6 (11.8) 85.9 (11.7) 86 (11.9) 86.2 (12.0)
Number (systolic blood pressure mm Hg) (SD) 14,942 19,613 22,282 25,488 25,420
Mean systolic blood pressure 137.5 (17.6) 137.1 (17.5) 136.6 (17.2) 136.1 (17.0) 135.7 (16.6)
Number (LDL) 9,646 13,204 15,688 17,769 17,372
Mean LDL, mmol/l (SD) 2.8 (1.0) 2.8 (1.0) 2.8 (1.0) 2.7 (1.0) 2.7 (1.0)
Number (BMI) 13,409 17,574 20,671 23,708 23,712
Mean BMI, kg/sq m (SD) 31.2 (5.9) 31.2 (6.0) 31.1 (5.9) 31 (5.8) 31 (5.8)
Number of smokers (%) 2,635 (20.4) 3,410 (19.7) 4,054 (20.1) 4,391 (18.8) 4,142 (18.3)
Number of physically inactive patients (%) 4,563 (41.3) 5,949 (41.8) 6,887 (41.3) 7,893 (40.6) 8,564 (41.8)
Source: NDR – Swedish National Diabetes Register.
Table 3c. Patients with HbA1c > 73 (mmol/mol). Type 2 diabetes at specialist clinics.
2009 2010 2011 2012 2013
Number 2,251 2,186 2,324 2,359 2,151
Mean age (SD) 59.5 (12.5) 60.4 (12.5) 60.3 (12.9) 60.7 (12.5) 60 (13.0)
Number (HbA1c) 2,251 2,186 2,324 2,359 2,151
Mean HbA1c, mmol/mol (SD) 85.7 (11.5) 85.6 (11.0) 86.1 (11.5) 86.1 (11.4) 86.6 (11.6)
Number (systolic blood pressure mm Hg) (SD) 2,122 2,070 2,163 2,236 2,050
Mean systolic blood pressure 135.1 (17.6) 134 (16.6) 133.7 (16.6) 133.7 (17.0) 133.2 (16.1)
Number (LDL) 1,724 1,696 1,774 1,848 1,633
Mean LDL, mmol/l (SD) 2.5 (0.9) 2.5 (1.0) 2.5 (1.0) 2.4 (1.0) 2.4 (1.0)
Number (BMI) 1,997 1,970 2,048 2,098 1,921
Mean BMI, kg/sq m (SD) 32 (5.8) 31.8 (6.0) 31.6 (5.9) 31.5 (5.7) 31.4 (5.7)
Number of smokers (%) 329 (15.9) 314 (15.7) 361 (17.3) 361 (16.7) 310 (16.1)
Number of physically inactive patients (%) 764 (44.1) 794 (46.3) 837 (44.6) 930 (47.9) 843 (46.9)
Source: NDR – Swedish National Diabetes Register.

Annual Report 2013 | 19
Young adults with type 1 diabetesThey often have high HbA1c levels and are treated with insulin pumps.
While the youngest type 1 diabetics in the NDR have the highest HbA1c levels, their trend was positive in 2013 as well. The HbA1c levels of young adults declined steadily during their first ten years in the register but then increased. (Figure 21). They are also the patients who are treated with insulin pumps most often (30% of 18–21 yearold women, Figure 22). One reason is that the use of insulin pumps is a growing phenomenon among children. Figure 23 show that adults are trending in the right direction. The percentage with HbA1c levels below 52 is rising and fewer have levels above 70. Nevertheless, 12% of them still have blood pressure above 130/80, while 15% smoke. Adapting the healthcare system to this population and setting the stage for improved results represent a major challenge.
60
62
64
66
68
70
20132012201120102009
Figure 21. Mean for HbA1c (mmol/mol) among patients in various age groups with type 1 diabetes at specialist clinics.mmol/mol
Type 1 diabetes at specialist clinics, age > 30
Type 1 diabetes at specialist clinics, age 22–30
Type 1 diabetes at specialist clinics, age 18–21
64.0
63.3
67.4
64.7
63.8
67.7
65.5
64.4
68.7
66.0
64.8
69.1
64.9
63.9
67.6
Source: NDR – Swedish National Diabetes Register.
0
5
10
15
20
25
30
35
20132012201120102009
Figure 22. Insulin pump among patients in various age groups.%
Type 1 diabetes at specialist clinics, age > 30
Type 1 diabetes at specialist clinics, age 22–30
Type 1 diabetes at specialist clinics, age 18–21
18.3
16.2
25.3
19.6
16.4
25.9
22.2
17.5
29.8
23.4
18.7
29.5
25.4
19.2
30.7
Source: NDR – Swedish National Diabetes Register.
0
20
40
60
80
100
GFR >
60
Blood p
ressu
re
<140/8
5 mm
Hg
Blood p
ressu
re
≤ 130/8
0 mm
Hg
HbA1c
>70
mm
ol/mol
HbA1c
< 52 m
mol/m
ol
Figure 23. Percentage of patients at primary care clinics age 18–21 who reached their target levels.
%
20112013
15.8
37.0
88.092.0
99.8
Source: NDR – Swedish National Diabetes Register.

20 | Annual Report 2013
Diabetes treatmentMany patients with diabetes in primary care receive dietary treatment only
The proportion of patients with diabetes in primary care who receive dietary treatment only is declining but is still at approximately 20%. The proportion is also relatively high (almost 30%) among type 2 younger than 70 who have had the disease for less than 3 years, suggesting that treatment is not intense enough from the very beginning. Specialist clinics report that more than 9% of patients with type 2 they treat are receiving GLP1 receptor agonists. In other words, the percentage of patients taking tablets alone or in combination with insulin has declined.
Primary care still treats only a negligible proportion of diabetics with GLP1 receptor agonists, while the percentages have substantially increased for patients who take tablets and slowly decreased for those who receive dietary treatment.
The majority of patients with type 2 are receiving insulin treatment 15 years after onset.
As was the case early, the percentage of patients receiving combination treatment (tablets and insulin) or insulin alone is rising with duration of the disease (Figure 27). A total of 56% of patients in primary care are receiving one of these treatments 15 years after onset. Most type 2 diabetics with inadequate HbA1c control (>73 mmol/mol) are receiving combination treatment or insulin alone (Figure 29).
Period from onset of type 2 diabetes to start pharmacological treatment has become shorter
Diet and exercise are the cornerstones of treating type 2 diabetes. Meeting targets as soon as possible is very important, and the current recommendation is to prescribe tablets (Metformin as the firstline therapy) at an early stage of the disease. Consistent with the recommendations of the guidelines, the period from onset of diabetes until commencement of pharmacological treatment is starting to shorten.
0
10
20
30
40
50
GLP-1Oral agentsand insulin
Insulin onlyOral agentsonly
Figure 25. Hypoglycaemic treatment among patients with type 2 diabetes at specialist clinics.
%
20132012201120102009
19.4 19.3 19.317.0 17.1
43.9 43.341.4 42.2
40.6
36.3 35.8 35.333.7 33.0
0.5 1.64.0
7.19.2
Source: NDR – Swedish National Diabetes Register.
0
10
20
30
40
50
GLP-1Oral agentsand insulin
Insulin onlyOral agentsonly
Diet only
Figure 24. Various types of hypoglycaemic treatment. Primary care.
%
20132012201120102009
25.3
24.8
24.2
23.0
22.6
44.5 45
.3 46.3 47
.2 47.5
12.6
12.3
12.1
12.6
12.2
17.6
17.6
17.1
16.3
16.2
0.1 0.1 0.3 0.9 1.6
Source: NDR – Swedish National Diabetes Register.
0
20
40
60
80
100
Oral agentsand insulin
Insulin onlyOral agents onlyDiet only
Figure 26. Hypoglycaemic treatment among patients < age 70 and diabetes duration ≤ 3 years. Primary care.
%
20132012201120102009
38.836.434.0
30.1 29.4
47.750.553.257.0 57.5
5.3 4.9 4.7 4.9 4.68.2 8.1 7.8 7.3 7.3
Source: NDR – Swedish National Diabetes Register.
DAYS
2011
20102009
20082007
2006
20052004
2003
2002
PATIENTS
100%
80%
60%
40%
20%
0%
0 500 1000 1500 2000 2500 3000 3500
Time to pharmacological treatment has been reduced from year 2002 to 2011.

Annual Report 2013 | 21
More women than men use insulin pumps
Among patients with type 1, approximately 25% of women and only 17% of men use insulin pumps. Thus, one out of five patients with type 1 use insulin pumps, which represents a steady increase over the past few years.
Blood pressureIn the wake of positive trends over time, more than half of patients with diabetes in primary care have blood pressure below 140/85.
The trend of better control and increased antihypertensive treatment is continuing (Figures 31–39).
Approximately 80% of patients with type 2 and 44% of type 1 diabetics are taking antihypertensives. Two different targets have been set: < 130/80 (current guidelines) and < 140/85. Almost 55% of patients in primary care and 76.6% of patients with type 1 have blood pressure below 140/85.
The fact that a disproportionate percentage of patients have exactly 130/80 or 140/80 indicates that the results are generally rounded off, usually to the nearest ten. It is very important to measure blood pressure as accurately as possible. Blood pressure should be taken when the patient is in a sitting position after having rested for 5 minutes and rounded down to the nearest even number. If the measurement is automated, the exact numbers should be specified. There is also a great need for validated automated blood pressure monitors and a standardised measurement method. 24hour blood pressure is not entered in the NDR.
0
20
40
60
80
100
25+20–2415–1910–14 5–9 0–4
Figure 27. Various types of hypoglycaemic treatment by intervals of diabetes duration. Primary care, 2013.
Insulin onlyOral agents and insulin
Oral agents only Diet only Results for 2012
%
Diabetes duration (years)
5.4
56.8
56.5
13.5
12.823.9
34.0 36.729.5
4.48.0
48.5
34.424.2
14.733.4
22.714.1 9.6 8.9 9.7
22.030.2 46.0
Source: NDR – Swedish National Diabetes Register.
0
20
40
60
80
100
GLP-1Oral agentsand insulin
Insulin onlyOral agents only
Figure 29. Hypoglycaemic treatment among patients with HbA1c >73 (mmol/mol). Type 2 diabetes at specialist clinics.
%
20132012201120102009
7.7 5.4 7.0 6.3 6.4
45.9 47.6 44.9 43.6 41.345.9 45.2 43.9 41.7 40.1
0.5 1.8 4.38.4
12.2
Source: NDR – Swedish National Diabetes Register.
0
20
40
60
80
100
GLP-1Oral agentsand insulin
Insulin only
Oral agentsonly
Diet only
Figure 28. Hypoglycaemic treatment among patients with HbA1c >73 (mmol/mol). Primary care.
%
20132012201120102009
6.0 6.6 7.1 6.7 6.5
29.5
29.7
29.3
29.0
28.3
25.6
25.0
25.0 26
.525
.5
38.8
38.5
38.0
35.8
36.4
0.1 0.2 0.6 1.9 3.3
Source: NDR – Swedish National Diabetes Register.
0
5
10
15
20
25
30
20132012201120102009
Figure 30. Insulin pump among patients with type 1 diabetes at specialist clinics.
%
Men Women All
21.3 21.123.2
24.6 25.2
13.6 14.515.8 16.8 17.6
17.017.4
19.120.2 21.0
Source: NDR – Swedish National Diabetes Register.

22 | Annual Report 2013
60
70
80
90
100
110
120
130
140
150
20132012201120102009
Figure 33. Mean blood pressure (mm Hg).
mm Hg
Systolic
Diastolic
SystolicDiastolic
Primary care
Specialist clinics, type 2 diabetes
Specialist clinics, type 1 diabetes
Primary care
Specialist clinics, type 2 diabetes
Specialist clinics, type 1 diabetes
136.5 136.2 135.7 135.3 134.9
126.8 126.3 126.1 126.0 126.2
133.9
76.2 76.3 76.2 76.3 76.2
73.0 72.8 72.7 72.9 73.075.2
74.9 74.8 74.774.8
133.4 132.7 132.4 132.4
Source: NDR – Swedish National Diabetes Register.
0
10
20
30
40
50
60
20132012201120102009
Figure 32. Systolic blood pressure in various intervals. All patients with type 2 diabetes.
%
≥ 141 mm Hg 131–140 mm Hg ≤ 130 mm Hg
43.7
29.6
26.6 27.0 27.0
26.9 27.228.7 27.5
26.6 25.7
44.2 45.4 46.5 47.1
Source: NDR – Swedish National Diabetes Register.
0
20
40
60
80
100
20132012201120102009
Figure 35. Blood pressure ≤ 130/80 mm Hg.
%
Primary care Specialist clinics, type 2 diabetes
Specialist clinics, type 1 diabetes
67.2 68.1 68.2 68.3 67.0
48.2 48.9 49.7 50.7 49.3
39.4 39.9 41.1 41.9 42.4
Source: NDR – Swedish National Diabetes Register.
0
20
40
60
80
100
20132012201120102009
Figure 31. Antihypertensive drugs.
%
Primary care Specialist clinics, type 2 diabetes
Specialist clinics, type 1 diabetes
44.2 44.1 45.2 44.2 44.0
80.7 80.6 82.3 82.7 81.3
79.1 78.5 78.9 78.0 78.0
Source: NDR – Swedish National Diabetes Register.
0
20
40
60
80
100
20132012201120102009
Figure 34. Blood pressure <130/80 mm Hg.
%
Primary care Specialist clinics, type 2 diabetes
Specialist clinics, type 1 diabetes
44.2 45.5 46.5 47.1 47.0
27.3 27.9 29.6 31.1 31.1
21.5 21.7 23.0 23.6 23.8
Source: NDR – Swedish National Diabetes Register.
0
20
40
60
80
100
20132012201120102009
Figure 36. Blood pressure ≤140/85 mm Hg.
%
Primary care Specialist clinics, type 2 diabetes
Specialist clinics, type 1 diabetes
84.3 85.1 85.8 85.6 85.1
72.373.2 74.3 74.7
73.7
65.5 66.4 67.3 68.1 68.9
Source: NDR – Swedish National Diabetes Register.

Annual Report 2013 | 23
0
20
40
60
80
100
20132012201120102009
Figure 38. Blood pressure < 130/80 mm Hg among patients treated with antihypertensive drugs.
%
Primary care Specialist clinics, type 2 diabetes
Specialist clinics, type 1 diabetes
29.1 30.1 31.3 32.3 32.7
25.5 26.0 27.5 29.329.2
19.4 19.7 21.1 21.6 21.9
Source: NDR – Swedish National Diabetes Register.
0
20
40
60
80
100
20132012201120102009
Figure 39. Blood pressure < 140/85 mm Hg among patients treated with antihypertensive drugs.
%
Primary care Specialist clinics, type 2 diabetes
Specialist clinics, type 1 diabetes
59.6 62.0 62.6 63.5 63.7
54.1 55.9 58.8 59.559.2
47.3 48.1 49.9 50.9 52.0
Source: NDR – Swedish National Diabetes Register.
70 80 90 100 110 120 130 140 150 160 170 180 190
Systolic blood pressure (mm Hg)
2000
5
25
20
15
10
30
%
Figure 41. Histogram for systolic blood pressure (mm Hg). All patients with type 2 diabetes, 2013.
N 28,3444Mean 134.8331Std Deviation 15.69295Maximum 250Minimum 80
Source: NDR – Swedish National Diabetes Register.
70 80 90 100 110 120 130 140 150 160 170 180 190
Systolic blood pressure (mm Hg)
2000
5
25
20
15
10
30
%
Figure 40. Histogram for systolic blood pressure (mm Hg). All patients with type 1 diabetes, 2013.
N 43,084Mean 127.6564Std Deviation 15.27313Maximum 250Minimum 80
Source: NDR – Swedish National Diabetes Register.
0
20
40
60
80
100
20132012201120102009
Figure 37. Blood pressure <140/85 mm Hg.
%
Primary care Specialist clinics, type 2 diabetes
Specialist clinics, type 1 diabetes
74.4 75.9 76.6 76.6 76.6
57.2 58.7 61.1 61.6 61.5
50.5 51.1 52.7 53.7 54.6
Source: NDR – Swedish National Diabetes Register.
Distribution of blood pressure values

24 | Annual Report 2013
Blood lipidsA total of 60% of patients, in primary care are treated with blood lipid lowering drugs, less than half of those with type 1 diabetes.
Cholesterol levels are continuing to improve as well (Figures 42–44). Though most pronounced for LDL cholesterol, the changes are also evident for HDL and total cholesterol. Triglyceride levels, which are not significantly affected by statin treatment, are unchanged among all patient populations. With the exception of patients with type 2 at specialist clinics, however, the initial increase in lipid lowering treatment has levelled off in recent years. Altogether almost half of all patients – both patients with type 1 and those in primary care – have LDL cholesterol levels above 2.5mmol/l.
0
20
40
60
80
100
20132012201120102009
Figure 42. Lipid lowering drugs.
%
Primary care Specialist clinics, type 2 diabetes
Specialist clinics, type 1 diabetes
42.2 43.7 44.6 44.4 44.9
72.6 72.7 75.0 75.9 75.2
61.6 61.5 62.0 61.1 61.4
Source: NDR – Swedish National Diabetes Register.
0
20
40
60
80
100
20132012201120102009
Figure 43. LDL cholesterol < 2,5 mmol/l.
%
Primary care Specialist clinics, type 2 diabetes
Specialist clinics, type 1 diabetes
46.6 47.5 48.3 49.5 52.8
57.2 59.8 60.1 61.9 64.2
44.0 45.2 46.2 48.5 51.5
Source: NDR – Swedish National Diabetes Register.
0
20
40
60
80
100
20132012201120102009
Figure 44. LDL cholesterol < 2,5 mmol/l among patients treated with lipid lowering drugs.
%
Primary care Specialist clinics, type 2 diabetes
Specialist clinics, type 1 diabetes
54.5 55.9 56.4 57.9 61.3
64.267.9 68.0 69.8 71.6
55.456.2 57.5 60.4 63.7
Source: NDR – Swedish National Diabetes Register.

Annual Report 2013 | 25
Impact on the KidneysMany cases of proteinuria still not entered in the register
Almost one out of every five patients in primary care and more than one out of every ten patient with type 1 have microscopic proteinuria. The percentage of microscopic and macroscopic proteinuria cases rises the longer patients have diabetes (Figures 45–46).
Results for 2012
0
10
20
30
40
50
Specialist clinics,type 2 diabetes
Specialist clinics,type 1 diabetes
Primary care
Figure 45. Microalbuminuria (urine albumin excretion 20–200 microgram/min) by diabetes duration, 2013.
%
25+15–245–140–4
2.6 5.29.3
17.214.2
21.1
29.932.9
13.6
19.5
26.229.4
Source: NDR – Swedish National Diabetes Register.
0
10
20
30
40
50
Primary care Specialist clinics,type 2 diabetes
Specialist clinics,type 1 diabetes
%
Figure 46. Macroalbuminuria (urine albumin excretion > 200 μg/min) by diabetes duration, 2013.
Results for 201225+15–245–140–4
0.7 1.33.9
9.7 8.312.4
19.9
25.2
4.47.4
12.516.1
Source: NDR – Swedish National Diabetes Register.

26 | Annual Report 2013
Acetylsalicylic AcidLess treatment with aspirin for patients without ischaemic heart disease
Figures 47–49 present the use of acetylsalicylic acid (aspirin). Treatment with aspirin has gradually declined for both patients with type 1 and type 2 without ischaemic heart disease. Use of aspirin remains high for patients with ischaemic heart disease.
Process Measure: Eye and Foot ExaminationsWell-functioning processes
The national guidelines for diabetes care recommend a fundus examination every other year for type 1 diabetics and every three years for patients with type 2, or every year for patients with diabetes retinopathy. Figure 50 shows that specialist clinics are examining almost the same percentage of patients as before (95.5% of type 1 diabetics and 97.3% of type 2 diabetics) while primary care clinics are tending to examine somewhat fewer (90.3%). Approximately 93–95% of patients have had their foot examination done (Figure 51).
0
20
40
60
80
100
Coronaryheart disease
No coronaryheart disease
All
Figure 48. Acetylsalisylic acid for all type 1 diabetes patients and for all type 1 diabetes patients with coronary heart disease at specialist clinics.
%
2012 2013201120102009
25.722.123.4 20.5 19.6 19.6
15.717.3 14.4 13.5
90.2 89.388.4 87.1 86.8
Source: NDR – Swedish National Diabetes Register.
0
20
40
60
80
100
Coronaryheart disease
Ej ischemiskhjärtsjukdom
All
Figure 49. Acetylsalisylic acid for all type 2 diabetes patients and for all type 2 diabetes patients with coronary heart disease at specialist clinics.
%
2012 2013201120102009
56.852.952.6 52.0 49.5
45.240.141.9 38.6 36.3
84.7 83.180.6 83.7 82.2
Source: NDR – Swedish National Diabetes Register.
0
20
40
60
80
100
Coronaryheart disease
No coronaryheart disease
All
Figure 47. Acetylsalisylic acid for all patients and for patients with coronary heart disease in primay care.
%
2012 2013201120102009
48.042.944.8
40.5 38.9 36.831.333.7
28.8 27.0
78.7 75.776.9 74.5 73.4
Source: NDR – Swedish National Diabetes Register.
80
85
90
95
100
20132012201120102009
Figure 50. Monitoring of eye status during the last 2 years among patients with type 1 diabetes at specialist clinics and the last 3 years among patients with type 2 diabetes at specialist clinics and in primary care.
%
Primary care Specialist clinics, type 2 diabetes
Specialist clinics, type 1 diabetes
96.896.8 96.1 96.1 95.5
98.4 98.3 98.1 97.9 97.3
94.5 94.0 93.491.8
90.3
Source: NDR – Swedish National Diabetes Register.
80
85
90
95
100
20132012201120102009
Figure 51. Monitoring of foot status during the last year.
%
Primary care Specialist clinics, type 2 diabetes
Specialist clinics, type 1 diabetes
89.8
92.1
92.891.6
93.6
89.6
91.792.8
91.693.2
87.889.4
93.0 93.4
95.3
Source: NDR – Swedish National Diabetes Register.

Annual Report 2013 | 27
Estimated 5-year Risk for Cardiovascular DiseasePotential for improvements in multifactorial treatment
Based on the NDR risk model for type 2 diabetes (see website), Figure 52 shows the absolute risk of developing cardiovascular disease (myocardial infarct/stroke) in 5 years among primary care patients age 30–79 in 2013. The model proceeds from 12 cardiovascular risk factors: duration of diabetes, HbA1c levels, systolic blood pressure, total cholesterol levels, HDL cholesterol levels, smoking, BMI, microalbuminuri, macroalbuminuri, previous cardiovascular disease, age and gender. The model was satisfactorily validated by testing a large number of patients with type 2 throughout Sweden. The nationwide average for absolute 5year risk was 13.3%.
Figure 52 shows a countybycounty breakdown for 2013 of the percentage of patients with absolute risk greater than 10%, defined as medium risk – or 15%, defined as high risk – for cardiovascular disease in accordance with the NDR model. The countytocounty variations are moderate. The proportion of patients with greater than 10% risk ranges from 46% to 70%, for a nationwide average of 57%, while the proportion with greater than 15% risk ranges from 25% to 46%, for a nationwide average of 33%
We have also calculated a normal risk – the absolute risk of someone of the patient's age, gender and disease duration who has achieved normal levels for the modifiable risk factors: HbA1c (52 mmol/mol), systolic blood pressure (135 mmHg), total cholesterol (4.4 mmol/l), HDL cholesterol (1.1 mmol/l), BMI 25 kg/sq m, no proteinuria and nonsmoker. The nationwide fiveyear normal risk averaged 11.7%.
How much of the risk is modifiable?
Figure 53 shows the modifiable risk – the percentage of absolute risk that can be affected by the modifiable risk factors, calculated by dividing the difference between the absolute risk and normal risk by the normal risk. The nationwide average for modifiable risk was 18%. Figure 53 also shows the proportion of patients with modifiable risk above 10%, the counties varying from 34% to 68%, for a nationwide average of 49%.
The analysis is based on 143,157 patients with type 2 age 30–79 in the NDR for 2013 for whom data is available for all 12 risk factors that make up the estimated 5year risk for cardiovascular disease. HDL cholesterol and proteinuria are the risk factors for which data are most frequently missing.
0 10 20 30 40 50 60 70 80
Norrbotten
Västerbotten
Jämtland
Västernorrland
Gävleborg
Dalarna
Västmanland
Örebro
Värmland
Västra Götaland
Halland
Skåne
Blekinge
Gotland
Kalmar
Kronoberg
Jönköping
Östergötland
Sörmland
Uppsala
Stockholm
Figure 52. 5-year risk for cardiovascular disease, NDR riskmodel. Patients in primary care age 30–79 by county.
%
Absolute risk >15%Absolute risk >10%
52.0
58.0
54.0
50.0
54.0
55.0
62.0
70.0
59.0
54.0
56.0
51.0
46.0
54.0
55.0
63.0
56.0
57.0
60.0
56.0
66.0
28.0
34.0
32.0
29.0
32.0
32.0
39.0
46.0
34.0
33.0
33.0
29.0
25.0
32.0
28.0
39.0
33.0
34.0
36.0
35.0
44.0
Source: NDR – Swedish National Diabetes Register.

28 | Annual Report 2013
Patients with Recent Onset of Type 2 DiabetesThe better the levels, the lower the risk
Figure 54 shows the absolute 5year risk for cardiovascular disease (cardiac infarct or stroke) among patients age 30–79 in primary care who have developed type 2 diabetes within the past three years. The risk is based on the NDR
risk model for type 2 diabetes (see website), which proceeds from 12 cardiovascular risk factors: duration of diabetes, HbA1c levels, systolic blood pressure, total cholesterol levels, HDL cholesterol levels, smoking, BMI, microalbuminuri and macroalbuminuri, previous cardiovascular disease, age and gender. Crosssection analyses reveal that average absolute risk declined significantly from 10.4% in 2011 to 9.8% in 2013.
Figure 54 also shows the modifiable risk – the difference between the absolute risk and normal risk divided by the normal risk. The normal risk is based on a patient who has achieved the target levels for the modifiable risk factors. The fact that average modifiable risk declined significantly from 18.9% in 2011 to 15.2% in 2013 points to more intensive treatment following initial diagnosis.
Figure 55 shows average HbA1c, systolic blood pressure, BMI and LDL cholesterol levels shortly after onset of diabetes. HbA1c, systolic blood pressure and LDL cholesterol levels all declined significantly from 2011 to 2013, while BMI was unchanged.
Figure 56 shows the percentages of patients who have achieved the target levels for HbA1c levels, blood pressure, blood lipid levels, consumption of medication, smoking cessation and physical activity. The percentages increased significantly for HbA1c, blood pressure, LDL cholesterol and smoking cessation, while physical activity (no more than twice a week, or 30 minutes altogether) was unchanged.
This risk analysis uses the threshold for hypertension (140/85 mmHg) that is the latest target level specified by the European Societies of Cardiology and Hypertension. The switch from the previous target of 130/80 mm Hg is supported by the ACCORDBP randomised study of approximately 10,000 type 2 diabetics in the U.S., as well as the NDR BPII observational study of 35,000 type 2 diabetics under treatment for hypertension as published in the Journal of Hypertension in 2012. In accordance with the GRADE system, welldesigned observational studies like NDR BPII can be upgraded to evidence level A on a par with randomised studies. The study found that blood pressure of 140/80 mm Hg or higher substantially increased the risk of cardiovascular disease, whereas there was no significant difference between the 115–129 mm Hg and 130–139 mm Hg ranges.
0 10 20 30 40 50 60 70 80
Norrbotten
Västerbotten
Jämtland
Västernorrland
Gävleborg
Dalarna
Västmanland
Örebro
Värmland
Västra Götaland
Halland
Skåne
Blekinge
Gotland
Kalmar
Kronoberg
Jönköping
Östergötland
Sörmland
Uppsala
Stockholm
Figure 53. 5-year risk for cardiovascular disease, NDR riskmodel. Patients in primary care age 30–79 by county.
%Modifiable risk >10%
54.0
59.0
49.0
44.0
48.0
48.0
55.0
68.0
52.0
47.0
46.0
45.0
34.0
51.0
59.0
59.0
50.0
48.0
55.0
54.0
61.0
Source: NDR – Swedish National Diabetes Register.

Annual Report 2013 | 29
Percentage of Primary Care Patients with Three or More High-risk Factors May be identified with the “Button”.
Previous reports have presented the percentage of patients with decidedly high blood pressure and HbA1c levels in order to highlight the fact that they run a higher risk of diabetes complications. Describing the total impact of the various risk factors, as opposed to each one separately, is also a useful exercise. This indicator, as well as the 5year risk for diabetes complications, has been designed with that purpose in mind.
The indicator shows the percentage of primary care patients with three or more highrisk factors. The indicator could have been designed otherwise – no research has clearly established that three or more factors represent the most suitable criterion. Among other possible designs might be two or more factors, or three factors including smoking.
Thus, the indicator is accompanied by a countybycounty diagram broken down by the number of highrisk factors, as well as a diagram that shows the percentage of patients with three or more highrisk factors. The factors are LDL > 2,5 mmol/l, systolic blood pressure > 150 mm/Hg, HbA1c > 70 mmol/mol, smoking and microalbuminuri.
Fewer than 6% of patients nationwide have three or more highrisk factors, more than 31% have no factors and almost 44% have one factor.
In addition to the fact that the indicator can be designed in a number of different ways, the rate of data loss must be taken into consideration. A patient must have data in the NDR for all of the risk factors during the period in order to be included in the comparison. Only 142,364 of the more than 305,000 patients in primary care met those criteria. Given the probable correlation between working methods, monitoring and entry in the NDR, that sample is likely to have fewer risk factors than the entire population. The differences in data loss among the various counties further exacerbate the data loss to the point of unreliability.
0
4
8
12
16
20
Modifiable risk***Absolute 5-year risk
Figure 54. Cross section 2011 and 2013. 5-year risk for cardiovascular disease, NDR risk model. Patients in primary care age 30–79, duration no more than 3 years.
%
2013 2011 *** p < 0.001
10.49.8
18.9
15.2
Source: NDR – Swedish National Diabetes Register.
0
20
40
60
80
100
120
140
160
LDL x 10(mmol/l)
BMI (kg/sq )mSystolic blood pressure
(mm Hg)
HbA1c(mmol/mol)
***
Figure 55. Average HbA1c, systolic blood pressure and BMI. Patients in primary care age 30–79 with duration no more than 3 years.
Average
2013 2011 *** p < 0.001
50.249.3
135.0134.0
30.630.6 28.928.0
Source: NDR – Swedish National Diabetes Register.
Phys
ically
inac
tive
Smoke
r
Blood li
pid
low
erin
g dru
gs
LDL <
2.5 m
mol/l
***
Antihyp
erte
nsives
Blood p
ressu
re
< 140/8
5 mm
Hg
***
HbA1c
< 52 m
mol/m
ol
***
10
20
30
40
50
60
70
80
0
Figure 56. Patients in primary care age 30–79 with duration no more than 3 years.
%
2013 2011 *** p < 0.001
68.072.0
53.055.0
71.0
42.038.0
71.0
55.054.0
18.016.0
23.024.0
Source: NDR – Swedish National Diabetes Register.

30 | Annual Report 2013
Women and MenHigher blood lipid levels and less blood lipid lowering treatment among women with type 2 diabetes
Agestandardised results for patients with type 2 age 30–80 broken down by gender are available for several indicators. Women average lower HbA1c levels and more of them achieve the target of < 52. Similarly, women average lower diastolic blood pressure and more of then achieve the target of < 140/85 mmHg. However, there is no significant gender gap when it comes to systolic blood
pressure and only minor differences with respect to consumption of antihypertensives. Women have in average higher total cholesterol, LDL cholesterol and triglyceride levels, and significantly fewer achieve the targets of < 4.5 mmol/l and < 2.5 mmol/l respectively for the first two levels. Women also are less often treated with blood lipid lowering drugs. No difference in the percentage of non smokers Women average higher BMI (fewer are below 30) and are considerably less likely to exercise at least three times a week. The gender gap is statistically significant and is particularly pronounced with respect to BMI, total cholesterol and LDL cholesterol levels, as well as the target levels for HbA1c, blood pressure, total cholesterol and LDL cholesterol, plus consumption of blood lipid lowering drugs. The gap is similar to the situation for 2011–2012. Longitudinal studies can shed light on the implications of these differences for possible future complications.
0
10
20
30
40
50
20132012201120102009
Five risk factors
Four risk factors
Three risk factors
Two risk factors
One risk factor
No risk factors
Figure 58. Percentage of patients in primary care nationwide with risk factors (microscopic proteinuria, HbA1c >70, LDL > 2.5, BP >150, smoking).
%
25.7 26.6 27.5 28.831.4
45.6 44.8 44.6 44.2 43.5
22.1 21.9 21.3 20.8 19.4
5.6 5.8 5.7 5.4 4.9
0.8 0.8 0.9 0.8 0.70.1 0.1 0.1 0.10.0
Source: NDR – Swedish National Diabetes Register.
0
20
40
60
80
100
120
140
160
BMIDiastolicblood pressure
Systolicblood pressure
HbA1c
Figure 59. Average risk factors for women and men with type 2 diabetes age 30–80. Significant differences after age standardisation: ***p < 0.001.
Average
WomenMen
54.3 53.6
134.6 134.4
77.4 76.1
29.8 30.7
Source: NDR – Swedish National Diabetes Register.
0
1
2
3
4
5
6
TriglyceridesHDLLDLTotal cholesterol
Figure 60. Average blood lipid levels (mmol/l) for women and men with type 2 diabetes age 30–80. All differences are significant after age standardisation, p< 0.001.
Average
WomenMen
4.54.9
2.5 2.7
1.2 1.4
1.9 1.8
Source: NDR – Swedish National Diabetes Register.
0 20 40 60 80 100
GotlandVästmanland
NorrbottenStockholm
DalarnaUppsala
JämtlandKalmar
BlekingeGävleborg
VästerbottenNationwide
JönköpingHalland
Västra GötalandKronoberg
VästernorrlandSörmland
ÖrebroSkåne
VärmlandÖstergötland
%
Five risk factors
Four risk factors
Three risk factors
Two risk factors
One risk factor
No risk factors
40.6
36.5
35.6
34.7
34.5
33.8
33.7
33.6
32.8
32.2
31.4
31.1
29.8
29.8
28.5
26.4
26.0
25.9
25.6
25.3
23.7
22.7
41.2
41.5
42.1
44.0
44.5
44.1
44.5
42.4
44.4
45.1
43.5
44.0
46.4
45.3
45.5
44.9
46.2
44.9
43.9
44.7
46.3
42.1
14.9
17.5
17.6
17.4
16.7
17.2
17.5
18.7
17.8
17.5
19.4
18.2
19.2
19.4
20.3
21.2
21.4
22.2
23.0
22.7
23.1
26.8
3.0
4.0
4.1
3.4
3.8
4.5
3.7
4.6
4.3
4.6
4.9
5.7
4.0
4.7
5.1
6.3
5.7
6.3
6.4
6.2
5.8
5.9
0.3
0.5
0.6
0.4
0.5
0.5
0.5
0.7
0.6
0.6
0.7
1.0
0.5
0.7
0.6
1.1
0.7
0.8
1.0
1.0
1.1
2.3
0.0
0.0
0.0
0.0
0.0
0.0
0.1
0.0
0.1
0.0
0.0
0.0
0.0
0.1
0.0
0.1
0.0
0.0
0.1
0.1
0.0
0.2
Source: NDR – Swedish National Diabetes Register.
Figure 57. Breakdown of risk factors (microscopic proteinuria, HbA1c >70, LDL > 2.5, BP >150, smoking), primary care, county.

Annual Report 2013 | 31
Agestandardised results for people with type 1 diabetes age 18 and older broken down by gender are available for several indicators. Women have in average higher HBA1c levels and are less likely to achieve the target of < 52 mmol/mol. A somewhat lower percentage of women are nonsmokers. Average BMI is the same, though fewer women have BMI < 30. The same percentage of women and men exercise at least 3 times a week. Women have in average lower blood pressure and are more likely to achieve the target of <140/85 mm Hg despite the fact that they consume fewer antihypertensives. Women have higher HDL cholesterol and lower triglyceride levels. Women have in average the same LDL cholesterol levels as men and are just as likely to achieve the target of < 2.5 mmol/l despite the fact that they consume fewer blood lipid lowering drugs. The gender gap is statistically significant and particularly evident with respect to blood pressure, blood lipid levels, HDL cholesterol levels, triglyceride levels, BMI < 30 and nonsmoking. As was the case in 2011–2012, more women (22%) than men (15%) with type 1 diabetes are receiving insulin pump treatment. The overall situation is fairly consistent with 2011–2012. Longitudinal studies can shed light on the implications of these differences for possible future complications.
0
10
20
30
40
50
60
70
80
90
100
Figure 61. Percentage of women and men with type 2 diabetes age 30–80 who reached the target levels. Except for smokers, all differences are significant after age standardisation, p< 0.001.
%
WomenMen
47.9 50.954.5 57.156.7
49.453.8 51.1 53.4
39.5
54.948.2
55.2 54.3
65.4 62.4
78.177.184.3 84.2
Source: NDR – Swedish National Diabetes Register.
Non-smoke
rs
Antihyp
erte
nsives
Blood li
pid lo
wer
ing d
rugs
Trig
lycer
ides
1.7
LDL c
holeste
rol <
2.5
Tota
l chole
stero
l <4.5
Phys
ical a
ctivi
ty a
t lea
st
thre
e tim
es a
wee
k
BMI <
30
Blood p
ressu
re <
140/8
0
HbA1c <
52
0
20
40
60
80
100
120
140
BMIDiastolicblood pressure
Systolicblood pressure
HbA1c
Figure 62. Average risk factors for women and men with type 1 diabetes age 18 and older. Significant differences after age stadardisation: ***p <0.001
Average
WomenMen
63.6 64.5
129
74.3
126
71.9
26.4 26.2
Source: NDR – Swedish National Diabetes Register.
0
1
2
3
4
5
6
TriglyceridesHDLLDLTotal cholesterol
Figure 63. Average blood lipid levels (mmol/l) for women and men with type 1 diabetes, age 18 and older. All differences are significant after agestandardisation, p < 0.001.
Average
WomenMen
4.6 4.8
2.6
1.5
2.6
1.8
1.2 1.1
Source: NDR – Swedish National Diabetes Register.
0
10
20
30
40
50
60
70
80
90
100
Non-smoke
r
Antihyp
erte
nsives
Blood li
pid lo
wer
ing d
rugs
Trig
lycer
ides
1.7
LDL c
holeste
rol <
2.5
Tota
l chole
stero
l <4.5
Phys
ical a
ctivi
ty a
t lea
st
thre
e tim
es a
wee
k
BMI <
30
Blood p
ressu
re <
140/8
0
HbA1c <
52
Figure 64. Percentage of women and men with type 1 diabetes age 18 and older who reached target levls. Except for LDL (p=0.2) and physical activity (p=0.2) , all differences are significant.
%
WomenMen
17.0 15.1
70.6
83.376.5
80.2
54.5 55.147.5
36.2
52.5 52.8
82.586.7
49.042.9
50.245.5
88.186.2
Source: NDR – Swedish National Diabetes Register.

32 | Annual Report 2013
Facts about the NDRIntegral to Swedish diabetes careThe Swedish Association for Diabetology (SFD) established the National Diabetes Register (NDR) in 1996 in response to the St. Vincent Declaration, whose purpose was to persuade European countries to reduce the prevalence of diabetes complications. The NDR was designed to enable comparisons between the results achieved at all clinics treating diabetics and the nationwide average for a number of clinical variables. The register now offers online tools for comparisons over time, as well as among counties and clinics. The tools are intended for use as part of local improvement efforts.
The NDR has become integral to Swedish diabetes care, particularly since the late 1990s as research has increasingly demonstrated the importance of various risk factors for diabetes complications and cardiovascular disease, not to mention the efficacy of new treatments for high blood pressure, blood sugar and blood lipid levels. Thus, the register meets the indispensable need for an instrument that monitors treatment outcomes.
How the NDR is structuredThe SFD runs the NDR on behalf of the Swedish Association of Local Authorities and Regions. The register is financed by appropriations from the Executive Committee for National Quality Registers and the the Västra Götaland Register Centre. Refer to www.ndr.nu for the NDR regulations.
NDR Steering Committee
• President, SFD (Convenor): Professor Mona Landin Olsson, Lund University Affiliated with the specialist clinic in Helsingborg
• President, Swedish Diabetes Association Fredrik Löndahl
• Director: Soffia Guðbjörnsdóttir, Associate Professor, Director, Västra Götaland Register Centre, Gothenburg
• Ulf Samuelsson, Associate Professor, Director, Child and Adolescent Clinic, Linköping University Hospital
Representatives of:
• Swedish Society of Endocrinology Professor Mikael Rydén, Karolinska University Hospital, Huddinge
• Representative of primary care: Kristina Bengtsson Boström, Associate Professor, Billingen Health Centre, Skövde
• Section for Endocrinology and Diabetes, Swedish Association of Paediatricians Ulf Samuelsson, Associate Professor, Director, Child and Adolescent Clinic, Linköping University Hospital
• Swedish Association of Diabetes Nurses: Lars Berg, Diabetes Nurse, Southern Älvsborg Hospital/Borås
• UllaBritt Löfgren, Diabetes Nurse, Project Manager, NDR
• Pär Samuelsson, Development Manager, NDR
NDR Research group
The Research group is responsible for processing NDR data, as well as compiling annual and scientific reports for national and international conferences. The committee also promotes the use of the data in clinical research. The NDR has published a number of its scientific reports in national and international journals over the past few years.
• Soffia Guðbjörnsdóttir, Associate Professor
• Jan Cederholm, Associate Professor
• Björn Eliasson, Associate Professor
• Katarina EegOlofsson, Md, Specialist
• Björn Zethelius, Associate Professor
• AnnMarie Svensson, Associate Director
• Mervete Miftaraj, Biostatistician

Annual Report 2013 | 33
Maintenance and developmentVästra Götaland Register Centre
The national quality registers operate under the auspices of the various county councils and receive financial assistance from the Swedish Association of Local Authorities and Regions. The Västra Götaland Region is responsible for a number of registers, including the NDR.
Now that efforts to monitor the healthcare system are increasingly dependent on quality assessment data, there is a greater need to collaborate with the registers above and beyond basic reporting procedures.
The tasks of the Register Centre are to:
• supply the registers with various resources
• provide support and skills for launching and developing registers
• serve as a regional asset for improving quality register efforts
Technical development
The IT Division of the Register Centre is responsible for technical development and maintenance of the NDR website, software and online reports for each clinic. The division sets standards for ongoing technical development and improvement and has established a shared platform for all registers.
Data entry
Electronic data entry at www.ndr.nu provides a clinic with immediate access to its results, as well as countybycounty and nationwide comparison statistics. A patient’s data may be entered repeatedly throughout the course of a year. Approximately 86% of NDR users sign on with personnel cards.
Direct transmission of medical records
Information is also transmitted directly from medical record systems and through local extraction software to the NDR database. More than half of the entries are automated.
Input data
In addition to entry date, care provider code and Swedish personal identity number, the following data are requested: year of onset, type of diabetes, type of treatment, method of administering insulin, HbA1c levels, weight, height, waist circumference, blood pressure, blood lipid levels, serum creatinine levels, and 14 closed
questions: hypertension and lipid lowering treatment, aspirin or Waran treatment, microscopic and macroscopic proteinuria, history of stroke or myocardial infarct, fundus examination, retinopathy or visual impairment, foot examination, smoking status, physical activity and hypoglycaemia. The latest levels and care event are entered. Refer to reporting form.
Form for supplementing or revising entries in the most recent report.
Diabetes profile to be used in information for patients The profile is generated automatically on the basis of all mandatory data that has been entered, as well as the optional answers that the clinic has provided. Brief comments may also be entered. The profile may be printed out during an appointment and increase patient participation in treatment programmes.
An overview shows the clinic’s diabetes population (broken down by gender, current age, onset age, disease duration and treatment method), including national comparison figures for each level of care.
A search list is a tool that allows the user to combine the criteria to which a particular subpopulation is subject in order to process data, monitor quality and focus on patients – either individuals or groups – with special intervention needs.
A search can also be performed to identify patients for whom no data have been entered in relation to a particular variable. The purpose of the function is to obtain more complete information for use as part of the clinic’s monitoring and improvement efforts.
The statistics show the clinic’s outcomes, along with national comparison figures at each level of care. The results are based on input data for the period of time that the user selects.
Customised statistics show figures from a period of the user’s choice. The user can generate comparison data from two different time periods. The statistics can be presented as a cumulative diagram, a bar and pie chart, or a table. The function is under development.

34 | Annual Report 2013
Feedback
Each clinic has immediate access to its own outcomes, as well as nationwide comparison figures. The results are based on input data for the period of time that the user selects. A clinic can autonomously generate their annual report, including nationwide comparison figures. The NDR compiles and publishes a nationwide overview during the first half of the following year. The reports serve as a tool for monitoring and improvement efforts by individual clinics and the various county councils. The results are presented in an increasingly transparent manner as the register expands its coverage.
The “Button”
County coordinators and officials have exhibited growing interest in countybycounty and clinic outcomes. In response to this demand, the NDR designed and launched a brand new tool (the “Button”) during the year that permits a user to follow an indicator, as well as generate comparison figures, at the local, county and nationwide level.
The “Button” offers unprecedented options for monitoring outcomes and documenting improvement efforts at a clinic. The “Button” can be accessed on our website.

Annual Report 2013 | 35
Quality and validity
The online input software includes instructions and definitions, as well as a number of mandatory and builtin validation checks. Data entry is validated on a continual basis by means of required fields, fixed alternatives and automated plausibility checks built into the software. The database includes automated reporting of statistics for the percentage of completed variables so that the clinics can monitor the quality of their own data entry. Patients are assigned to the last clinic at which they had an appointment during the year, whether it be specialist or primary care.
Previous validation studies have found a high rate of agreement between medical records and NDR data for most variables. There were no systematic discrepancies between patients for whom data had or had not been entered. NDR data for primary care throughout the Västra Götaland Region have been validated against medical records, the Inpatient Register and the Prescribed Drug Register. Generally speaking, the data exhibit a very high rate of agreement.
Register data are always subject to methodological problems due to selection and measurement errors, as well as non participation. Measurement errors, the difference between a measured and true value, occur in all databases Such errors are caused by deficient instruments and methods, along with unreliable responses. Standardised measurement methods and secure data transmission reduce the risk of error. Given that the NDR is not comprehensive, it contains sampling errors. The selectivity of data loss, rather than the phenomenon itself, is the problem. The most effective antidote is to increase the participation rate at the country and regional levels. Nevertheless, variations in the participation rate at the clinic level affect assessments of the results. This report is representative of diabetes care at most specialist clinics, as well as primary care in many counties.

36 | Annual Report 2013
New developments and other NDR projects
• Insulin pump project. On behalf of the European Association for the Study of Diabetes (EASD) and for the purpose of enhancing traceability and patient safety, the NDR will add questions about insulin pumps and incidents that may be associated with their use. The goal for 2014 is to enter the indications, complications and reasons for termination of insulin pump treatment. Data entry is to be as simple as possible and hopefully become routine when treatment commences.
• A total of 18 external research projects were granted in 2013. The NDR published 15 articles in scientific journals and had 16 abstracts accepted at medical conferences. The NDR generates many statistical reports every year. Demand has decreased, however, since we launched our “Button” tool, which permits users to generate their own customised reports.
• The NDR is participating in a number of national and international research partnerships.
• Ten PhD students are affiliated with NDR in several different areas, including patient reported outcome measures (PROMs), health economics, cardiology, nephrology, general medicine, paediatric diabetology and clinical improvement methodology.
• The NDR Risk Engine, an online service for calculating the 5year risk of cardiovascular disease, is gaining in popularity. The annual report presents countybycounty results for the first time.
• The NDR website needs a comprehensive overhaul, and a new development project is under way. The goal is to make register data more graphically appealing and comprehensible, encouraging improvement efforts and reaching out to patients and other new target groups.
• The NDR participates regularly in various training activities initiated by the county councils.
• Representatives of the NDR deliver regular lectures about the register, improvement efforts and research in many different venues.
The NDR is involved in a host of projects concerning register efforts, including:
• National PROM Network.
• Västra Götaland Regional Quality Register for Primary Care.
• Diabetes and pregnancy: a working committee has launched a project to address register logistics and indicators.
• Quality register data at www.1177.se. The objective is to empower patients and their families, creating new opportunities for them to take action and assume control. Making administration and management of the healthcare system more transparent.
• SVEUS Project on outcomes, resource utilisation and compensation in diabetic care as part of the National Partnership for Development of Diagnostic Descriptive Systems and Valuebased Compensation Systems – Diabetes.
• Descriptive and compensation systems will be designed in close collaboration with participating county councils, the Swedish Association for Diabetology, Swedish Association of General Practice, Swedish Association of Diabetes Nurses and representatives of care providers. The overall purpose of the research project is to develop a new compensation system for diabetes care in participating counties on behalf of the Ministry of Health and Social Affairs. The goal of the partnership is to ensure that county councils have greater control over the care they provide while creating compensation systems that encourage costeffectiveness efforts (better outcomes for less money).
• Dialogue Project: development of a new feedback tool, introduction of selfreported data in interaction with diabetics and caregivers. The tool is to use stateoftheart visualisation technology and interactive design concepts to improve the ability of patients to participate in their care and learn about diabetes.
• National Platform for Improvement Research.
• A National Board of Health and Welfare project to address goal fulfilment in diabetes care.

Annual Report 2013 | 37
Typ 1 (inkl LADA) Typ 2 (inkl MODY)
Hypoglykemiförekomst svåra 6) (antal senaste året ) Ingen 1-2 3-5 >5
20.
Synnedsättning (P.g.a. diabetes <0,3 på bästa ögat med korr.) Ja Nej Okänt18.
Ja Nej Okänt Diagnos på sämsta ögat 8)
Laserbehandlad Ja Nej Okänt
Diabetesretinopati17b.
ASA (Eller annan tromb.aggregerings hämmare) Ja Nej Okänt Waran16.
Cerebrovaskulär sjukdom (Någonsin. TIA, stroke) Ja Nej Okänt15.
12b. S-kreatinin (µmol/l)
Vårdgivare (kod) Personnummer
Debutår (diagnos enl. WHO-kriterier; graviditetsdiabetes exkluderas)
1.
HbA1c (mmol/mol)4.
Vikt (kg, utan ytterplagg, kavaj och skor)5.
Midjeomfång (cm) 1)7.
Blodtryck (mm Hg. Sittande efter 5 minuters vila) /8.
Antihypertensiva läkemedel Ja Nej Okänt9.
Lipidsänkande läkemedel Ja Nej Okänt11.
Registreringsår 2014Gäller aktuella förhållanden
Version 1.0 2014-02-07
Längd (cm, utan skor)6.
3a. Diabetesbehandling Tabl. och insulinInsulin
Sekundär (t ex pancreatit) Oklart
Typ av diabetes (klinisk bedöming)2.
Datum
Metod att ge insulin Injektion Insulinpump
19a. Ja Nej Okänt DatumFotundersökning (Senaste året)
Ögonbottenundersökning (Ögonfoto eller insp. av ögonspecialist) Datum, År (ÅÅÅÅ) Månad (MM)17a.
Aldrig varit rökare Röker dagligen Röker, men ej dagligen
Slutat röka Slutat röka, År (ÅÅÅÅ) Månad (MM)
Rökvanor
21.
1) Midjeomfång: Tas med patienten stående efter normal utandning, horisontellt mellan nedersta revbensbågen och höftbenskammen (översta spetsen på höftbenet).2) Makroalbuminuri: För diagnos krävs kvantifiering dvs. alb/kreatininratio > 30 mg/mmol (eller U-albumin >200µg/min, eller > 300 mg/l)3) Mikroalbuminuri: För diagnos krävs kvantifiering där två av tre prov tagna inom ett år skall vara positiva dvs. alb/kreatininratio 3-30 mg/mmol (eller U-albumin 20-200µg/
min, eller 20-300 mg/l). Normaliserat värde efter farmakologisk behandling.4) Ischemisk hjärtsjukdom: Någonsin. Angina pectoris, genomgången hjärtinfarkt, PTCA, by-pass kirurgi.5) Riskkategori: Nivå 1: Frisk fot – Diabetes utan komplikationer; Nivå 2: Neuropati och/eller angiopati – perifer kärlsjukdom; Nivå 3: Tidigare diabetessår, fotdeformiteter,
grav callus, amputerad; Nivå 4: Pågående allvarlig fotsjukdom – sår, kritisk ischemi, infektion, grav osteoartropati, charcot-fot.6) Hypoglykemiförekomst svåra: hjälp av utomstående.7) LDL: behöver ej rapporteras då det beräknas automatiskt (enligt Friedewalds formel) om samtidig rapportering av Kolesterol, Triglycerider och HDL-kolesterol sker.
Manuell rapportering av LDL som beräknats enligt annan formel är möjlig.8) Diagnos på sämsta ögat: Simplex retinopati, PPDR= Preproliferativ diabetesretinopati, KSM= Kliniskt signifikant makulaödem, PDR= Proliferativ diabetesretinopati
Fysisk aktivitet (30 min promenad eller motsvarande. Individuellt anpassad och alla former av aktivitet räknas.)
Aldrig <1 ggr/vecka Regelbundet 1-2 ggr/vecka
Regelbundet 3-5 ggr/vecka Dagligen
22.
13. Ja Nej Okänt Normaliserat värdeMikroalbuminuri 3)
Ischemisk hjärtsjukdom 4) Ja Nej Okänt14.
10. HDL Blodlipider (mmol/l) Kolesterol Triglycerider
12a. Makroalbuminuri 2) Ja Nej Okänt
3b.
Riskkategori 5) 1 Frisk fot 2 Neuropati och/eller angiopati
3 Tidigare diabetessår 4 Pågående allvarlig fotsjukdom
19b.
Enb. kost Inj. GLP-1Tabl.
LDL7)

38 | Annual Report 2013
HbA1c
Systolic blood pressure
LDL-cholesterol
Non-smokerNo proteinuria
Fundus status
Foot status
Mean age 46, n=1,170
Year 2013
Sahlgrenska University Hospital/Sahlgrenska
Example from specialist clinic
Hospital views
Each hospital has a table, along with a “Target” snapshot of its results (mean and percentage) compared with the nationwide mean. The Target shows patients with type 1 diabetes at hospital.
The Target is not a comprehensive measure of the quality of diabetes care at the hospital, but rather an incentive for analysis, learning and improvement.
The three shades indicate:
• The hospital’s results are poorer than the nation- wide mean by a statistically significant margin.
• The hospital’s results are on a par with the nationwide mean.
• The hospital’s results are better than the nation- wide mean by a statistically significant margin.

Annual Report 2013 | 39
* the last 2 years among patients with type 1 diabetes at hospital, as well as the last 3 years among patients with type 2 diabetes at hospital and primary care ** last year
Primary care Specialist clinics, type 1 diabetes
Specialist clinics, type 2 diabetes
IndicationsNation-
wideCounty council
Nation-wide
County council
Nation-wide
County council
Mean value
HbA1c, mmol/mol 54.1 52.9 64.3 63.1 62 61.6
Systolic blood pressure, mm Hg
134.9 133.9 126.2 125.2 132.4 131.5
LDL-cholesterol, mmol/l 2.6 2.5 2.6 2.5 2.3 2.3
Proportion (%)
Non-smoker 85.7 85.8 88.2 90.0 86.8 88.0
No proteinuria 92.3 93.7 94.5 94.1 83.3 78.3
Fundus status* 90.3 89.5 95.5 96.9 97.3 98.0
Foot status** 95.3 96.9 93.6 90.2 93.2 90.2
0
20
40
60
80
100
20132012201120102009
Non-smoker
LDL-cholesterol <2.5 mmol/l
Blood pressure <130/80 mm Hg
HbA1c <52 mmol/mol
All dotted lines = Nation wide
Västra Götaland: primary care and nationwide.
%
0
20
40
60
80
100
20132012201120102009
Icke-rökare
LDL-kolesterol <2,5 mmol/l
Blodtryck <130/80 mm Hg
HbA1c <52 mmol/mol
Alla streckade linjer=Riket
Västra Götaland: specialist clinics type 1 diabetes and nationwide.
%
0
20
40
60
80
100
20132012201120102009
Icke-rökare
LDL-kolesterol <2,5 mmol/l
Blodtryck <130/80 mm Hg
HbA1c <52 mmol/mol
Alla streckade linjer=Riket
Västra Götaland: specialist clinics type 2 diabetes and nationwide.
%
Non-smoker
LDL cholesterol <2.5 mmol/l
Blood pressure <130/80 mm Hg
HbA1c <52 mmol/mol
Dashed lines =Nationwide
Coverage
LDL-cholesterol
Non-smoker
No proteinuria
HbA1c
Systolic blood pressure
Fundus status
Foot status
HbA1c
Systolic blood pressure
LDL-cholesterolNon-smoker
Fundus status
No proteinuria
Foot status
HbA1c
Systolic blood pressure
LDL-cholesterol
Non-smoker
No proteinuria
Fundus status
Foot status
Primary careN = 58,165Mean age = 68.3Mean duration = 9.3Men = 56.4%
Specialist clinics, type 1 diabetesN = 6,541Mean age = 45.6Mean duration = 22.9Män = 56.9%
Specialist clinics, type 2 diabetesN = 2,148Mean age = 63.6Mean duration = 16.0Män = 67.4%
Västra Götaland

40 | Annual Report 2013
IndicationsVästra
Götaland (%)
Nation- wide (%)
HbA1c < 52 mmol/mol 56.8 52.2
HbA1c ≤ 70 mmol/mol 89.6 88.3
Blood pressure ≤ 130/80 mmHg 44.3 42.4
Blood pressure < 140/85 mmHg 57.8 54.6
Systolic blood pressure < 150 mmHg 83.8 82.1
LDL < 2.5 mmol/l 54.2 51.5
BMI < 35 kg/sq m 85.1 85
Blood lipid lowering treatment 57.3 61.4
No macroscopic proteinuria 93.7 92.3
Foot status checked the past year 96.9 95.3
Fundus status checked the past three years 89.5 90.3
No diabetic retinopathy 80.5 72.4
Non-smoker 85.8 85.7
Physical activity * 75.4 71.5
*Physical activity, regularly 3–5 times/week or daily
0 20 40 60 80 100
Physical activity
Non-smoker
No diabetic retinopathy
Fundus status checkedthe past three years
Foot status checked the past year
No macroscopic proteinuria
Blood lipid lowering treatment
BMI < 35 kg/m2
LDL < 2.5 mmol/l
Systolic blood pressure < 150 mmHg
Blood pressure < 140/85 mmHg
Blood pressure ≤ 130/80 mmHg
HbA1c ≤ 70 mmol/mol
HbA1c < 52 mmol/mol
Västra Götaland, primary care
%Västra Götaland
0 20 40 60 80 100%
Nationwide
IndikatorerVästra
Götaland (%)
Nation- wide (%)
HbA1c < 52 mmol/mol 19.5 16.9
HbA1c ≤ 70 mmol/mol 75.0 71.3
Blood pressure ≤ 130/80 mmHg 69.1 67.0
Blood pressure < 140/85 mmHg 88.4 87.6
Systolic blood pressure < 150 mmHg 57.7 52.8
LDL < 2.5 mmol/l 90.6 90.9
BMI < 35 kg/sq m 42.8 44.9
Blood lipid lowering treatment 94.1 94.5
No macroscopic proteinuria 90.2 93.6
Foot status checked the past year 96.9 95.5
Fundus status checked the past three years 38.8 34.0
No diabetic retinopathy 90.0 88.2
Non-smoker 78.6 78.4
Physical activity * 21.7 21.0
*Physical activity, regularly 3–5 times/week or daily
Source: NDR – Swedish National Diabetes Register.
0 20 40 60 80 100
Insulin treatment
Physical activity
Non-smoker
No diabetic retinopathy
Fundus status checkedthe past 2 years
Foot status checked the past year
No macroscopic proteinuria
Blood lipid lowering treatment
eGFR > 60 ml/min/1.73 sq m
LDL < 2.5 mmol/l
Blood pressure < 140/85 mmHg
Blood pressure ≤ 130/80 mmHg
HbA1c ≤ 70 mmol/mol
HbA1c < 52 mmol/mol
Västra Götaland, specialist clinics, type 1 diabetes
%Västra Götaland
0 20 40 60 80 100%
Nationwide

Annual Report 2013 | 41
Publications1. Gudbjörnsdottir S, Cederholm J, Nilsson PM, Elias
son B. The National Diabetes Register in Sweden: An implementation of the St. Vincent Declaration for Quality Improvement in Diabetes Care. Diabetes Care 2003;26:12706.
2. Nilsson PM, Gudbjörnsdottir S, Eliasson B, Cederholm J. Hypertension in diabetes: trends in clinical control in repeated largescale national surveys from Sweden. J Hum Hypertens 2003;17:3744.
3. Nilsson PM, Gudbjörnsdottir S, Cederholm J, Eliasson B, for the Steering Committee of the Swedish National Diabetes Register. Smoking is associated with increased HbA1c values and microalbuminuria in patients with diabetes data from the National Diabetes Register in Sweden. Diabetes Metab. 2004;30:2618.
4. Cederholm J, Eliasson B, Nilsson PM, Weiss L, Gudbjörnsdottir S, for the steering committee of the Swedish National Diabetes Register. Microalbuminuria and risk factors in type 1 and type 2 diabetic patients. Diabetes Res Clin Pract. 2005;67:25866.
5. Eliasson B, Cederholm J, Nilsson P, Gudbjörnsdóttir S for the steering committee of the Swedish National Diabetes Register. The gap between guidelines and reality: Type 2 diabetes in a national diabetes register 19962003. Diabet Med 2005:22:14206.
6. Nilsson PM, Cederholm J, Gudbjörnsdóttir S, Eliasson B, for the Steering Committee of the Swedish National Diabetes Register. Predictors of successful longterm blood pressure control in patients with diabetes – data from the Swedish National Diabetes Register (NDR). J Hypertension 2005;23:230511.
7. Ridderstråle M, Gudbjörnsdóttir S, Eliasson B, Nilsson PM, Cederholm J for the Steering Committee of the Swedish National Diabetes Register (NDR). Obesity and cardiovascular risk factors in type 2 diabetes: Results from a national diabetes register. J Intern Med. 2006;259:31422.
8. EegOlofsson K, Cederholm J, Nilsson PM, Gudbjörnsdóttir S, Eliasson B for the Steering Committee of the Swedish National Diabetes Register (NDR). Glycemic and risk factor control in type 1 diabetes: Results from 13,612 patients in a national diabetes register. Diabetes Care 2007;30:496502.
9. Eliasson B, EegOlofsson K, Cederholm J, Nilsson PM, and Gudbjörnsdóttir S, for the Steering Committee of the Swedish National Diabetes Register (NDR). Antihyperglycaemic treatment of type 2 diabetes: Results from a national diabetes register. Diabetes Metab 2007;33:26976.
10. Cederholm J, EegOlofsson K, Eliasson B, Zethelius B, Nilsson PM, Gudbjörnsdóttir S. Risk prediction of cardiovascular disease in type 2 diabetes: A risk equation from the Swedish National Diabetes Register (NDR). Diabetes Care 2008;31:203843.
11. EegOlofsson K, Cederholm J, Nilsson PM, Zethelius B, Nunez L, Gudbjörnsdóttir S, Eliasson B. Risk of cardiovascular disease and mortality in overweight and obese patients with type 2 diabetes: an observational study in 13,087 patients. Diabetologia. 2009;52:6573.
12. Gudbjörnsdottir S, EegOlofsson K, Cederholm J, Zethelius B, Eliasson B, Nilsson PM, on behalf of the Swedish National Diabetes Register (NDR). Risk factor control in patients with type 2 diabetes and coronary heart disease: Findings from the Swedish National Diabetes Register (NDR). Diabetic Medicine 2009;26:53–60.
13. Gerdtham UG, Clarke P, Hayes A, Gudbjornsdottir S. Estimating the cost of diabetes mellitusrelated events from inpatient admissions in Sweden using administrative hospitalization data. Pharmacoeconomics. 2009;27:8190.
14. Nilsson PM, Cederholm J, EegOlofsson K, Eliasson B, Zethelius B, Fagard R, Gudbjörnsdottir S. Smoking as an independent risk factor for myocardial infarction or stroke in type 2 diabetes: A report from the Swedish National Diabetes Register (NDR). Eur J Cardiovasc Prev Rehabil 2009;16:506–12.

42 | Annual Report 2013
15. Jonasson JM, Ljung R, Talbäck M, Haglund B, Gudbjörnsdòttir S, Steineck G. Insulin glargine use and shortterm incidence of malignanciesa populationbased followup study in Sweden. Diabetologia. 2009;52:174554.
16. Cederholm J, Zethelius B, Nilsson PM, EegOlofsson K, Eliasson B, Gudbjörnsdottir S. Effect of tight control of HbA1c and blood pressure on cardiovascular diseases in type 2 diabetes: an observational study from the Swedish National Diabetes Register (NDR). Diabetes Res Clin Pract 2009;86:7481.
17. Nilsson PM, Cederholm J, EegOlofsson K, Eliasson B, Zethelius B, Gudbjörnsdóttir S, for the Swedish National Diabetes Register (NDR). Pulse pressure strongly predicts risk of cardiovascular disease in patients with type 2 diabetes from the Swedish National Diabetes Register (NDR). Diabetes Metab 2009;35:439–46.
18. EegOlofsson K, Cederholm J, Nilsson PM, Zethelius B, Svensson AM, Gudbjörnsdottir S, Eliasson B. Glycemic control and cardiovascular disease in 7454 patients with type 1 diabetes: an observational study from the Swedish National Diabetes Register (NDR). Diabetes Care 2010;33:16406.
19. Cederholm J, Gudbjörnsdottir S, Eliasson B, Zethelius B, EegOlofsson K, Svensson AM, Nilsson PM. Systolic blood pressure and risk of cardiovascular diseases in type 2 diabetes: an observational study from the Swedish National Diabetes Register. J Hypertens. 2010;28:202635.
20. EegOlofsson K, Cederholm J, Nilsson PM, Zethelius B, Svensson AM, Gudbjörnsdottir S, Eliasson B. New aspects of HbA1c as a risk factor for cardiovascular diseases in type 2 diabetes: an observational study from the Swedish National Diabetes Register (NDR). J Intern Med. 2010;268:47182.
21. Afghahi H, Cederholm J, Eliasson B, Zethelius B, Gudbjörnsdottir S, Hadimeri H, Svensson MK. Risk factors for the development of albuminuria and renal impairment in type 2 diabetesThe Swedish National Diabetes register (NDR). Nephrol Dial Transplant. 2011;26:123643.
22. Nilsson PM, Cederholm J, Zethelius BR, Eliasson B, EegOlofsson K, Gudbjörnsdottir S. Trends in blood pressure control in patients with type 2 diabetes: data from the Swedish National Diabetes Register (NDR). Blood Pressure 2011;20:348354
23. Eriksson M, Zethelius B, EegOlofsson K, Nilsson PM, Gudbjornsdottir S, Cederholm J, Eliasson B. Blood lipids in 75048 type 2 diabetic patients: a populationbased survey from the Swedish National Diabetes Register. Eur J Cardiovasc Prev Rehabil. 2011;18:97105.
24. Ljung R, Talbäck M, Haglund B, Jonasson JM, Gudbjörnsdòttir S, Steineck G. Insulin glargine use and shortterm incidence of malignancies a threeyear populationbased observation. Acta Oncol. 2011;50:68593.
25. Eliasson B, Svensson AM, Miftaraj M, Jonasson JM, EegOlofsson K, Sundell KA, Gudbjörnsdóttir S. Clinical use and effectiveness of lipid lowering therapies in diabetes mellitusan observational study from the Swedish National Diabetes Register. PLoS One. 2011 Apr 29;6(4):e18744. doi: 10.1371/journal.pone.0018744.
26. Cederholm J, EegOlofsson K, Eliasson B, Zethelius B, Gudbjörnsdottir S; Swedish National Diabetes Register. A new model for 5year risk of cardiovascular disease in Type 1 diabetes; from the Swedish National Diabetes Register (NDR). Diabet Med. 2011;28:121320.
27. Gudbjörnsdottir S, Eliasson B, EegOlofsson K, Zethelius B, Cederholm J; National Diabetes Register (NDR). Additive effects of glycaemia and dyslipidaemia on risk of cardiovascular diseases in type 2 diabetes: an observational study from the Swedish National Diabetes Register. Diabetologia. 2011;54:254451.
28. Lind M, Bounias I, Olsson M, Gudbjörnsdottir S, Svensson AM, Rosengren A. Glycaemic control and incidence of heart failure in 20,985 patients with type 1 diabetes: an observational study. Lancet. 2011;378:1406.
29. Zethelius B, Eliasson B, EegOlofsson K, Svensson AM, Gudbjörnsdottir S, Cederholm J. A new model for 5year risk of cardiovascular disease in type 2 diabetes, from the Swedish National Diabetes Register (NDR). Diab Res Clin Pract 2011;93:276284.
30. Eliasson B, Cederholm J, EegOlofsson K, Svensson AM, Zethelius B, Gudbjörnsdottir S. Clinical usefulness of different lipid measures for prediction of coronary heart disease in type 2 diabetes: a report from the Swedish National Diabetes Register. Diabetes Care 2011;34:20952100.

Annual Report 2013 | 43
31. Fhärm E, Cederholm J, Eliasson B, Gudbjörnsdottir S, Rolandsson O. Time trends in absolute and modifiable coronary heart disease risk in patients with Type 2 diabetes in the Swedish National Diabetes Register (NDR) 20032008. Diabet Med. 2012;29:198206.
32. Cederholm J, Zethelius B, Eliasson B, Gudbjörnsdottir S, Nilsson P. Different methods to present the effect of blood pressure on cardiovascular diseases at Cox regression (Correspondence). J Hypertens 2012;30:2357.
33. Ekström N, Miftaraj M, Svensson AM, Andersson Sundell K, Cederholm J, Zethelius B, Gudbjörnsdottir S, Eliasson B. Glucoselowering treatment and clinical results in 163 121 patients with type 2 diabetes: An observational study from the Swedish national diabetes register. Diabetes Obes Metab 2012;14:71726.
34. Ljung R, Talbäck M, Haglund B, Jonasson JM, Gudbjörnsdòttir S, Steineck G. Insulin glargine use and shortterm incidence of breast cancer a fouryear populationbased observation. Acta Oncol. 2012;51:4002.
35. Saleh N, Petursson P, Lagerqvist B, Skúladóttir H, Svensson AM, Eliasson B, Gudbjornsdottir S, EegOlofsson K, Norhammar A. Longterm mortality in patients with type 2 diabetes undergoing coronary angiography – the impact of glucoselowering treatment. Diabetologia 2012;55:210917.
36. Jonasson JM, Cederholm J, Eliasson B, Zethelius B, Eeg Olofsson K, Gudbjörnsdottir S. HbA1C and cancer risk in people with type 2 diabetes – a nationwide populationbased prospective cohort study in Sweden. PLoS One 2012;7(6):e38784.
37. Ekström N, Schiöler L, Svensson AM, Eeg Olofsson K, Jonasson JM, Zethelius B, Cederholm J, Eliasson, B, Gudbjörnsdottir S. Effectiveness and safety of metformin in 51 675 patients with type 2 diabetes and different levels of renal function: a cohort study from the Swedish National Diabetes Register. BMJ Open 2012;2:e001076. doi:10.1136/bmjopen2012001076.
38. Cederholm J, Gudbjörnsdottir S, Eliasson B, Zethelius B, EegOlofsson K, Nilsson PM. Blood pressure and risk of cardiovascular diseases in type 2 diabetes: further findings from the Swedish National Diabetes Register (NDRBP II). J Hypertens 2012;30:202030.
39. Lind M, Olsson M, Rosengren A, Svensson AM, Bounias I, Gudbjörnsdottir S. The relationship between glycaemic control and heart failure in 83,021 patients with type 2 diabetes. Diabetologia. 2012;55:294653.
40. Afghahi H, Miftaraj M, Svensson AM, Hadimeri H, Gudbjörnsdottir S, Eliasson B, Svensson M. Ongoing treatment with RAASblockade does not predict normoalbuminuric renal impairment in a general type 2 diabetes population. J Diabetes Compl 2013;27:229234.
41. B Eliasson, S Gudbjörnsdottir, B Zethelius, K EegOlofsson, J Cederholm, on behalf of the NDR. LDLcholesterol versus nonHDLtoHDLcholesterol ratio and risk for coronary heart disease in type 2 diabetes. Eur J Prev Cardiol 2013. doi: 10.1177/2047487313494292.
42. Ekström N, Cederholm J, Zethelius B, Eliasson B, Fhärm E, Rolandsson O, Niftaraj M, Svnesson AM, Gudjörnsdottir S. Aspirin treatment and risk of first incident cardiovascular diseases in type 2 diabetes: an observational study from the Swedish National Diabetes Register. BMJ Open 2013;3:e002688. doi:10.1136/bmjopen2013002688.
43. Svensson MK, Cederholm J, Eliasson B, Zethelius B, Gudbjörnsdottir S, for the Swedish National Diabetes Register. Albuminuria and renal function as predictors of cardiovascular events and mortality in a general population of patients with type 2 diabetes: a nationwide observational study from the Swedish National Diabetes Register. Diab Vasc Dis Res 2013;10:520529.
44. Zethelius B, Gudbjörnsdottir S, Eliasson B, EegOlofsson K, Cederholm J; (on behalf of the Swedish National Diabetes Register). Level of physical activity associated with risk of cardiovascular diseases and mortality in patients with type2 diabetes: report from the Swedish National Diabetes Register. Eur J Prev Cardiol. 2014;21:24451.

44 | Annual Report 2013
45. Fall K, Garmo H, Gudbjörnsdottir S, Stattin P, Zethelius B. Diabetes mellitus and prostate cancer risk; a nationwide casecontrol study within PCBaSe Sweden. Cancer Epidemiol Biomarkers Prev. 2013;22:11029.
46. Ahmad Kiadaliri A, Gerdtham UG, Nilsson P, Eliasson B, Gudbjörnsdottir S, Carlsson KS. Towards renewed health economic simulation of type 2 diabetes: risk equations for first and second cardiovascular events from Swedish register data. PLoS One. 2013;8:e62650. doi: 10.1371/journal.pone.0062650.
47. Ahmad Kiadaliri A, Clarke PM, Gerdtham UG, Nilsson P, Eliasson B, Gudbjörnsdottir S, Steen Carlsson K. Predicting changes in cardiovascular risk factors in type 2 diabetes in the postUKPDS era: Longitudinal analysis of the Swedish National Diabetes Register. J Diabetes Res. 2013;2013:241347. doi: 10.1155/2013/241347.
48. Vestberg D, Rosengren A, Olsson M, Gudbjörnsdottir S, Svensson AM, Lind M. Relationship between overweight and obesity with hospitalization for heart failure in 20,985 patients with type 1 diabetes: a populationbased study from the Swedish National Diabetes Registry. Diabetes Care. 2013;36:285761.
49. Glogner S, Rosengren A, Olsson M, Gudbjörnsdottir S, Svensson AM, Lind M. The association between BMI and hospitalization for heart failure in 83 021 persons with Type 2 diabetes: a populationbased study from the Swedish National Diabetes Registry. Diabet Med. 2013 Oct 22. doi: 10.1111/dme.12340.
50. Samuelsson U, Steineck I, Gudbjornsdottir S. A high meanHbA1c value 315 months after diagnosis of type 1 diabetes in childhood is related to metabolic control, macroalbuminuria, and retinopathy in early adulthooda pilot study using two nationwide population based quality registries. Pediatr Diabetes. 2013 Sep 30. doi: 10.1111/pedi.12085.
51. Hallgren Elfgren IM, Grodzinsky E, Törnvall E. Swedish Diabetes Register, a tool for quality development in primary health care. Prim Health Care Res Dev. 2013;14:2507.
52. Kelly PJ, Clarke PM, Hayes AJ, Gerdtham UG, Cederholm J, Nilsson P, Eliasson B, Gudbjornsdottir S. Predicting the mortality of people with type 2 diabetes mellitus following major complications: a study using Swedish National Diabetes Register data. 2014. Diabet Med. doi: 10.1111/dme.12468.
53. Eliasson B, Ekström N, Bruce Wirta S, Odén A, Pirouzi Fard M, Svensson AM. Metabolic effects of basal or premixed insulin treatment in 5,077 insulinnaïve type 2 diabetes patients: registrybased observational study in clinical practice. 2014. Diabetes Therapy. In press.
54. Kiadaliri AA, Gerdtham U, Eliasson B, Gudbjörnsdottir S, Svensson AM, Steen Carlsson K. Health utilities of type 2 diabetesrelated complications: a crosssectional study in Sweden. Int J Environ Res Public Health. 2014. In press.
55. Rawshani A, LandinOlsson M, Svensson AM, Nyström L, Arnqvist HJ, Bolinder J, Gudbjörnsdottir S. The incidence of diabetes among 0–34 year olds in Sweden: new data and better methods. Diabetologia 2014. DOI 10.1007/s0012501432259
Review articles in Läkartidningen (in Swedish)
1. Gudbjörnsdottir S, Nilsson, PM, Cederholm J, Eliasson B, Berne C. Förbättrad diabetesvård och sjunkande riskfaktorer i ny rapport från det nationella Diabetesregistret NDR. Läkartidningen. 2004;101:3790, 37937.
2. Cederholm J, Nilsson PM, Eliasson B, EegOlofsson K, Zethelius B, Gudbjörnsdottir S. Samband mellan riskfaktorer och komplikationer vid diabetes. Rapport efter 13 år med Nationella diabetesregistret (NDR). Läkartidningen 2009;42:26849.
3. Cederholm J, Eliasson B, Zethelius B, EegOlofsson K, Gudbjörnsdottir S. Riskfaktorer för hjärt–kärlsjukdom. Resultat från Nationella diabetesregistret jämförs med internationella studier. Läkartidningen 2013;1718:8825.

Centre of Registers Region Västra Götaland Centre for National Quality Registers
The Centre of Registers Region Västra Götaland is a repository of information for registers of healthcare quality. The Swedish Association of Local Authorities and Regions has charged the Centre with supporting the development, operation and use of national quality registers, as well as taking advantage of the registers to promote research and quality improvements.
www.registercentrum.se
Centre of Registers Region Västra GötalandSwedish National Diabetes Register413 45 Gothenburg, Sweden