Swan-Ganz Pacing TD Catheter - Edwards...
2
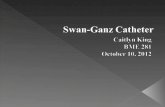
Swan-Ganz Pacing TD Catheter D200F7, D200HF7, D205HF7 Swan-Ganz Pacing TD Catheter D200F7, D200HF7, D205HF7 THE PACING-TD CATHETER CAN PERFORM: • RAP, PAP, and PAOP pressure measurements • Cardiac output measurements by thermodilution • Pacing atrial and ventricular pacing and atrioventricular (A-V) sequential pacing ATRIAL PROXIMAL ATRIAL CENTRAL ATRIAL DISTAL VENTRICULAR PROXIMAL VENTRICULAR DISTAL Proximal Injection Lumen Hub Gate Valve Distal Lumen Hub Thermistor Connector Proximal Atrial Central Atrial Distal Atrial Proximal Ventricular Distal Ventricular Balloon Thermistor (back side) 1 Ventricular Electrode 2 5 4 3 Stylet Anchor Brushing Atrial Electrodes Proximal Injection Port 1 2 3 4 5 ATRIAL PROXIMAL ATRIAL CENTRAL ATRIAL DISTAL VENTRICULAR PROXIMAL VENTRICULAR DISTAL ATRIAL PROXIMAL ATRIAL CENTRAL ATRIAL DISTAL VENTRICULAR PROXIMAL VENTRICULAR DISTAL ATRIAL PACING A-V SEQUENTIAL PACING 1. Connect the “distal atrial” electrode 3 to the negative pacemaker terminal. Connect the “central atrial” electrode 4 to the positive terminal. Notice: To facilitate a connection between the catheter and pacemaker, a cable adapter may be required. 2. Adjust the pacemaker output to 0.1 milliamps and the rate to 15% above the patient’s heart rate, or to a physiological rate. With the pacemaker turned on, slowly increase the output until atrial pacing occurs (see Figure 5). A typical atrial pacing current threshold is 5 milliamps. If atrial pacing does not occur, slowly advance or withdraw the catheter 0.5 cm at a time with the pacemaker operating at 5 milliamps and the balloon deflated. 3. Check the catheter position once again to make sure it has not been advanced to a permanent wedge position. 1. After achieving atrial and ventricular pacing, connect the two ventricular electrodes to the A-V sequential pacemaker; attempt pacing. Successful A-V sequential pacing is shown in above image. 1 2 3 5 4 ATRIAL VENT Pacemaker NEG POS ATRIAL VENT Pacemaker NEG POS EQUIPMENT 1. Swan-Ganz Pacing-TD catheter 2. Percutaneous sheath introducer and contamination shield 3. Compatible cardiac output computer, CO-Set injectate probe 4. External pacemaker (ventricular demand or A-V sequential) 5. External pacemaker cable adapters 6. Sterile flush system and pressure transducers 7. Bedside pressure monitor system PLACEMENT Standard pressure waveform showing RA-RV-PA-PAWP-progression 20 10 mmHg PAWP PA RV RA Surface ECG showing atrial pacing ATRIAL PROXIMAL ATRIAL CENTRAL ATRIAL DISTAL VENTRICULAR PROXIMAL VENTRICULAR DISTAL VENTRICULAR PACING 1. Connect the “distal ventricular” electrode 1 to the negative pacemaker terminal. Connect the “proximal ventricular” electrode 2 to the positive terminal. 2. Adjust the external generator R-wave sensitivity to approximately 3 millivolts to avoid competition between the pacemaker’s rate and the patient’s rate. 3. Repeat steps 1 and 2 to achieve ventricular pacing. Ventricular stimulation at 3 milliamps or less is generally obtainable. Check for adequate sensitivity once pacing is established. Successful ventricular capture is shown in above image. Unused electrode connectors must be capped to prevent their contact with a faulty ground. ATRIAL VENT Pacemaker NEG POS Surface ECG showing ventricular pacing Surface ECG showing A-V sequential pacing Catheter position before and after pulling back from initial wedge position Final Catheter Position A. Before B. After 1 2 3 4 5 1 2 3 4 5 Note: The Atrial Proximal Lead (5th lead) is used at the clinicians discretion when unable to capture or obtain satisfactory thresholds in the atrium using lead 3 and 4. Note: Diaphragmatic pacing may occasionally occur; it can usually be alleviated by advancing the catheter 0.5 to 1 cm. Precaution: If atrial and ventricular pacing occur only with the catheter in a permanent wedge position, withdraw the catheter to a pulmonary artery position. In this situation, pacing is sacrificed because of the likelihood of pulmonary infarction resulting from the catheter being permanently wedged.
Transcript of Swan-Ganz Pacing TD Catheter - Edwards...

Swan-Ganz Pacing TD CatheterD200F7, D200HF7, D205HF7
Swan-Ganz Pacing TD CatheterD200F7, D200HF7, D205HF7
THe PaCinG-TD CaTHeTer Can PerForm:• RAP, PAP, and PAOP pressure measurements
• Cardiac output measurements by thermodilution
• Pacing atrial and ventricular pacing and atrioventricular (A-V) sequential pacing
AT
RIA
L P
RO
XIM
AL
ATR
IAL
CEN
TRA
L
ATR
IAL
DIS
TAL
VEN
TRIC
ULA
R PRO
XIMAL
VENTRIC
ULAR DISTAL
Proximal Injection Lumen Hub
Gate Valve
Distal Lumen HubThermistor Connector
Proximal Atrial
CentralAtrial
DistalAtrial
ProximalVentricular
DistalVentricular
Balloon
Thermistor(back side)
1Ventricular Electrode
2
5 4 3 Stylet Anchor Brushing
Atrial Electrodes
Proximal InjectionPort
12
3
4
5
AT
RIA
L P
RO
XIM
AL
ATR
IAL
CEN
TRA
L
ATR
IAL
DIS
TAL
VEN
TRIC
ULA
R PRO
XIMAL
VENTRIC
ULAR DISTAL
AT
RIA
L P
RO
XIM
AL
ATR
IAL
CEN
TRA
L
ATR
IAL
DIS
TAL
VEN
TRIC
ULA
R PRO
XIMAL
VENTRIC
ULAR DISTAL
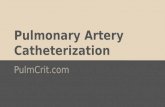
aTrial PaCinG a-V SequenTial PaCinG
1. Connect the “distal atrial” electrode 3 to the negative pacemaker terminal. Connect the “central atrial” electrode 4 to the positive terminal.
notice: To facilitate a connection between the catheter and pacemaker, a cable adapter may be required.
2. Adjust the pacemaker output to 0.1 milliamps and the rate to 15% above the patient’s heart rate, or to a physiological rate. With the pacemaker turned on, slowly increase the output until atrial pacing occurs (see Figure 5). A typical atrial pacing current threshold is 5 milliamps. If atrial pacing does not occur, slowly advance or withdraw the catheter 0.5 cm at a time with the pacemaker operating at 5 milliamps and the balloon deflated.
3. Check the catheter position once again to make sure it has not been advanced to a permanent wedge position.
1. After achieving atrial and ventricular pacing, connect the two ventricular electrodes to the A-V sequential pacemaker; attempt pacing. Successful A-V sequential pacing is shown in above image.
12
3
5
4
aTrial
VenT
Pacemaker
neGPoS
aTrial
VenT
Pacemaker
neGPoS
EquipmEnt1. Swan-Ganz Pacing-TD catheter2. Percutaneous sheath introducer and contamination shield3. Compatible cardiac output computer, CO-Set injectate probe4. External pacemaker (ventricular demand or A-V sequential)5. External pacemaker cable adapters6. Sterile flush system and pressure transducers7. Bedside pressure monitor system
PlaCemenT
Standard pressure waveform showing RA-RV-PA-PAWP-progression
20
10mm
Hg
PAWP
PARV
RA
Surface ECG showing atrial pacing
AT
RIA
L P
RO
XIM
AL
ATR
IAL
CEN
TRA
L
ATR
IAL
DIS
TAL
VEN
TRIC
ULA
R PRO
XIMAL
VENTRIC
ULAR DISTAL
VenTriCular PaCinG
1. Connect the “distal ventricular” electrode 1 to the negative pacemaker terminal. Connect the “proximal ventricular” electrode 2 to the positive terminal.
2. Adjust the external generator R-wave sensitivity to approximately 3 millivolts to avoid competition between the pacemaker’s rate and the patient’s rate.
3. Repeat steps 1 and 2 to achieve ventricular pacing. Ventricular stimulation at 3 milliamps or less is generally obtainable. Check for adequate sensitivity once pacing is established. Successful ventricular capture is shown in above image.
Unused electrode connectors must be capped to prevent their contact with a faulty ground.
aTrial
VenT
Pacemaker
neGPoS
Surface ECG showing ventricular pacing
Surface ECG showing A-V sequential pacing
Catheter position before and after pulling back from initial wedge position
Final Catheter Position
A. Before B. After
123
45
123
4
5
note: The Atrial Proximal Lead (5th lead) is used at the clinicians discretion when unable to capture or obtain satisfactory thresholds in the atrium using lead 3 and 4.
note: Diaphragmatic pacing may occasionally occur; it can usually be alleviated by advancing the catheter 0.5 to 1 cm.
Precaution: If atrial and ventricular pacing occur only with the catheter in a permanent wedge position, withdraw the catheter to a pulmonary artery position. In this situation, pacing is sacrificed because of the likelihood of pulmonary infarction resulting from the catheter being permanently wedged.

For professional use. CAUTION: Federal (United States) law restricts this device to sale by or on the order of a physician. See instructions for use for full prescribing information, including indications, contraindications, warnings, precautions and adverse events.
Edwards Lifesciences devices placed on the European market meeting the essential requirements referred to in Article 3 of the Medical Device Directive 93/42/EEC bear the CE marking of conformity.
Edwards, Edwards Lifesciences, the stylized E logo, AMC THROMBOSHIELD, Swan-Ganz are trademarks of Edwards Lifesciences Corporation. All other trademarks are the property of their respective owners.
© 2013 Edwards Lifesciences Corporation.All rights reserved. AR10036
Edwards Lifesciences | edwards.comOne Edwards Way | Irvine, California 92614 USASwitzerland | Japan | China | Brazil | Australia | India
PaCinG leaD-PaCemaker Cable ConneCTionimportant: Effective May 9, 2000, FDA regulation 21 CFR 898 requires changes affecting pacing catheters and probes. Your current external pacemaker cable may not be compatible with the modified catheter leads. Please follow these instructions to facilitate connection.
option 1: Use the universal adapters enclosed in this package with any external pulse generator cable equipped with a mechanism that mechanically secures the adapters in place.
option 2: Use cable models equipped with alligator clips option 3: Cables facilitating a direct connection between the catheter modified with shrouded pin connectors and external pulse generators may be available from other manufacturers.
Step 1. Insert and secure adapter to cable
Shrouded Pin Connector Universal AdapterPulseGeneratorCable
Step 2. Connect or disconnect shrouded pin connector and adapter
Shrouded Pin Connector Alligator Clip Connection
From Catheter
To PulseGeneratorCable
model number Computation Constants D200F7, D200HF7& D205HF7
Temp (°C) Volume (ml) Computation Constants (cc)*
0-5 10 0.542 5 0.247 3 0.132 19-22 10 0.578 5 0.274 3 0.154
Computation Constants for Co-Set+
Cold Injectate 10 0.561 10 ml: 6-12°C 5 0.2595 ml: 8-16°C 3 -
Room Temperature 10 0.608Injectate 5 0.3015 or 10 ml: 18-25°C 3 -
*CC = (1.08)CT(60)Vi
Function atrio-Ventricular Pacing and Thermodilution model number D200F7, D200HF7 D205HF7CoC Compatibility edwards edwards
Usable Length (cm) 110 110
Catheter Body French Size 7F 7F
Required Introducer Size 8F 8F
Body Color Yellow Yellow
Diameter of Deflated Balloon 8F 8F
Diameter of Inflated Balloon (mm) 13 13
Balloon Inflation Capacity (ml) 1.5 1.5
Injectate Port (cm from tip) 30 29.5
Injectate Lumen Volume (ml) 0.93 0.93
Electrode Material Elgiloy, 2 mm long Elgiloy, 2 mm long
Electrode Connector 0.40” x 0.080” dia pin plugs 0.40” x 0.080” dia pin plugs
Atrial Electrodes (cm from tip) 28.5, 31.0, 33.5 25.5, 28.0, 30.5
Ventricular Electrodes (cm from tip) 18.5, 19.5 15.5, 17.5
Permanent Stabilizing Stylet* Yes Yes
Compatible Guidewire Diameter (in) 0.020 0.020
Distal Lumen Natural Frequency/
Amplitude Radio 16 Hz 1.6:1
16 Hz 1.6:1
Thermistor Location (cm from tip) 4 4
Catheters are constructed from quadruple-lumen, polyvinylchloride, radiopaque extrusions; catheters with the AMC THROMBOSHIELD coating are denoted by an “H” in the model number.
* Catheters with permanent stabilizing stylets are not suitable for placement through the inferior vena cava. All specifications given are nominal values.
TD ComPuTaTion ConSTanTS CaTHeTer SPeCiFiCaTionS